 Raquel Prieto-García1,2,3,4*†
Raquel Prieto-García1,2,3,4*† Joan Pau Millet2,3,4
Joan Pau Millet2,3,4 Antonio Soriano-Arandes5María Espiau5Claudia Broto5Mar Ronda6Núria López7
Antonio Soriano-Arandes5María Espiau5Claudia Broto5Mar Ronda6Núria López7 Antoni Noguera-Julian8,9,10Eva Masdeu Corcoll2,3Cristina Domingo Jimenez2,3Miriam Ros Samsó2,3Maria Isabel Marcos Arroita2,3Jesús Edison Ospina Valencia2,9Carmen García Rebollo8
Antoni Noguera-Julian8,9,10Eva Masdeu Corcoll2,3Cristina Domingo Jimenez2,3Miriam Ros Samsó2,3Maria Isabel Marcos Arroita2,3Jesús Edison Ospina Valencia2,9Carmen García Rebollo8 Pere Simon Viván1,2,3,4Cristina Rius Gibert1,2,3,4
Pere Simon Viván1,2,3,4Cristina Rius Gibert1,2,3,4- 1Departament de Ciències Experimentals i de la Salut (DCEXS). Universitat Pompeu Fabra, Barcelona, Spain
- 2Servei d’Epidemiologia (SEPID), Agència de Salut Pública de Barcelona (ASPB), Barcelona, Spain
- 3Institut de Recerca de l'Hospital de la Santa Creu i Sant Pau (IIB Sant Pau), Barcelona, Spain
- 4CIBER de Epidemiología y Salud Pública (CIBERESP), Barcelona, Spain
- 5Unitat de Patologia Infecciosa i Immunodeficiències de Pediatria, Hospital Universitari Vall d'Hebron, Barcelona, Spain
- 6Departament de Malalties Infeccioses, Hospital Universitari de Bellvitge, l’Hospitalet del Llobregat, Barcelona, Spain
- 7Servicio de Pediatría, Hospital del Mar, Barcelona, Spain
- 8Malalties Infeccioses i Resposta Inflamatòria Sistèmica en Pediatria, Servei de Malalties Infeccioses i Patologia Importada, Institut de Recerca Pediàtrica Sant Joan de Déu, Barcelona, Spain
- 9Centro de Investigación Biomédica en Red de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain
- 10Departament de Cirurgia i Especialitats Medicoquirúrgiques, Facultat de Medicina i Ciències de la Salut, Universitat de Barcelona, Barcelona, Spain
Children under 15 years of age living in the household of a tuberculosis case constitute a very vulnerable group to tuberculosis infection (TBI). The objective of this study was to determine the prevalence of TBI and the risk factors associated with presenting TBI in this group, considering sex, age, and migratory status as axes of inequality. A population-based, analytical, cross-sectional observational study was carried out in the city of Barcelona in the period 2003–2022. The study population was household contacts under 15 years of age with index cases of pulmonary TB reported to the Barcelona Public Health Agency in the period 2003–2022. The analyses were performed using Generalized Estimating Equations (GEE) to predict the risk of TBI among these cohabiting contacts and were stratified considering the inequality axes of sex and migratory status. A total of 1084 contacts under 15 years of age were studied from 693 cases of tuberculosis. TBI prevalence among contacts was 24.5%. The factors associated with the presence of TBI in the contacts were having a smear positive in the index case, being older than 5 years in the contacts ([5,10], [10–15]) and the case and the contact being migrants; smear positive when the index case was native women and being from a municipal district with a lower incidence of tuberculosis when the index case was native women and the men. The results of the study confirm the importance of carrying out contact tracing and follow-up of household children, especially if the index case is smear positive. Contact tracing should be carried out as soon as possible to assess the prescription of primary chemoprophylaxis and TBI treatment to avoid rapid TB progression in children.
Introduction
Tuberculosis (TB) was declared a public health emergency in 1993 by the World Health Organization (WHO) and still poses a significant global health challenge (1). In 2021 in Spain, the incidence of TB was 7.4 cases per 100,000 inhabitants in the whole population, and 4.1 cases per 100,000 among children under 15 (2). In 2022 in Barcelona, the incidence of TB among children under 15 was 5.3 cases per 100,000 (3). In Barcelona, the current measures include the implementation of the Barcelona Tuberculosis Prevention and Control Program, which focuses on early diagnosis, epidemiological surveillance, contact tracing, and treatment management. However, significant challenges remain, such as drug resistance, the identification and treatment of latent infections, and the need to improve intersectoral coordination, especially in vulnerable populations such as children.
TB transmission is primarily airborne and depends on factors like cohabitation and shared activities with the index case (IC), the bacillary load and the disease severity of the IC, and poor home ventilation, among others (3–5). The progression from initial TB infection to TBI involves the immune response. Mycobacterium tuberculosis enters a dormant state due to factors like a weakened immune system as occurs in children. Unlike acute TB infection, individuals with TBI do not exhibit symptoms and cannot transmit the disease. This distinction is crucial. Active TB is characterized by symptoms like persistent cough, chest pain, and weight loss, and can spread to others. The burden of TBI is less than one-quarter of the world’s population (6). It is estimated that 5–10% of individuals develop TB within 2 to 5 years from infection (7–9), with the risk being even higher in children under the age of five (3, 10). To reduce this risk, contact tracing and treatment of latent tuberculosis infection (TBI) are essential measures recommended by the WHO’s End-TB Strategy for TB elimination (11–13). These should begin immediately after diagnosis of the IC, especially if the IC has a high bacillary load (14, 15).
Barcelona, like other large European cities, has extensive social heterogeneity, with vulnerable populations concentrated in specific neighborhoods where health inequalities are significant (16). These inequalities stem directly from urban health determinants, such as governance, physical context, socioeconomic factors, and physical environment. In addition, these determinants can affect people differently depending on several axes of inequality including sex, age, and migratory status (17). These axes are critical for understanding the disparities in the burden of TBI and for designing targeted interventions to improve TB prevention and control in the most vulnerable populations.
This study aimed to determine the prevalence and risk factors of TBI in children under 15 years old living with an IC in Barcelona from 2003 to 2022, considering axes of inequality: sex, age, and migratory status.
Methods
Study design and population
We conducted a population-based cross-sectional analytical observational study in the city of Barcelona from 1 January 2003 to 31 December 2022. This study was a secondary analysis of routinely collected data.
The study included household contacts under 15 years of age of ICs with pulmonary TB infection reported to the ASPB in the period 2003–2022. The exclusion criteria for these contacts were having had a history of TB or TBI. Contacts were removed from the study if they did not attend the tuberculin skin test (TST) or the TST reading or were lost of follow-up in the tuberculosis unit if the test was positive.
Contact tracing and testing procedure
The Epidemiology Service of the ASPB carried out the contact tracing in collaboration with community health agents. We conducted a structured interview with the TB case and the identified contacts as a part of routine surveillance, prevention, and control activities from the Barcelona TB Prevention and Control Program. The TST was performed on the latter, considering positive those who presented an induration larger than 5 mm. If the result was negative, a second TST was performed 8–12 weeks later. All study data were recorded and analyzed anonymously. Access to these data, for subsequent analysis, was carried out between November 3, 2023, and March 30, 2024, and at the time of data extraction, they were anonymized so that the people who carried out the statistical analysis did not have access to information that could individually identify the participants.
Contacts with a positive TST or symptoms compatible with TB were referred to one of the designated TB clinical units in Barcelona where they underwent a chest X-ray and interferon-gamma release assay based on medical criteria. These units also managed any necessary treatment and follow-up for TBI or active TB.
Variables
The explanatory variables of the IC were sex, migratory status, age, municipal district (MD) of residence, and smear positive. The MD variable was classified into two categories based on the prevalence of TB in Barcelona: high prevalence with more than 10 cases per 100,000 inhabitants (MD of Ciutat Vella, Sant Martí, and Nou Barris districts) and low prevalence with less than or equal to 10 cases per 100,000 inhabitants (MD of Sants-Montjuïc, Sant Andreu, Eixample, Horta-Guinardó, Gràcia, Les Corts, and Sarrià districts) (18).
The explanatory variables of the contacts were sex, age, and migratory status. The stratification of age groups into 3 categories ([0–5], [5–10], [10–15]) was done to reflect key stages of child development and TB risk, consistent with prior pediatric TB literature and clinical practice. Children under 5 are considered at higher risk for rapid progression and severe forms of TB, often guiding prioritization in contact tracing and preventive treatment. The [5–10] and [10–15] age groups were defined to reflect school-age and early adolescent populations, which differ in terms of exposure patterns, immunological maturity, and likelihood of adherence to preventive treatment (19, 20). The migratory status and the MD variables serve as reliable indicators for determining socioeconomic level.
The response variable was the diagnosis of TBI, recorded as either present or absent for each investigated contact.
Statistical analysis
We performed a descriptive analysis of the sociodemographic and clinical characteristics of the IC and the sociodemographic variables of the contacts. The age distribution of the ICs was analyzed using the Shapiro–Wilk test, as it did not follow a normal distribution. Therefore, for this variable, we used the median as a measure of central tendency and the interquartile range as a measure of dispersion. For all the analyses, the ICs were stratified by sex and migratory status. In all tests, the level of significance was set at 0.05.
We used the Pearson chi-squared test to determine the association between qualitative variables and the prevalence of TBI among contacts, and the Mann–Whitney U test to determine the association between quantitative variables and the prevalence of TBI among contacts.
Considering that our outcomes were not independent across contacts of the same IC, we used Generalized Estimating Equations (GEE) (21), an extension of generalized linear models that allows regression analysis of outcomes that may not be normally distributed or independent. We performed a bivariate analysis to select the demographic variables of ICs and contacts that best predict the risk of TBI among contacts. The variables showing statistical significance were included in the stratified multivariate analysis.
We used the statistical program RStudio Version 1.3.1093.
Ethical considerations
Demographic and clinical data were obtained from the epidemiological questionnaire used by the Barcelona Tuberculosis Prevention and Control Program. All study data were recorded and analyzed anonymously. Data were collected routinely according to the National Tuberculosis Plan approved by the Spanish Ministry of Health and the statistical analysis was carried out retrospectively between March 1, 2023, and September 30, 2023. At the time of data extraction, people who performed the analysis did not have access to information that could individually identify the participants. Therefore, informed consent was not required. The project was approved by the Parc de Salut Mar Drug Research Ethics Committee (CEIm-PSMAR, 2023/11081). All data were treated strictly confidential under the regulations: the ethical principles of the Declaration of Helsinki (22); the Organic Law 7/2021 (23), of May 26, on the protection of personal data processed for prevention, detection, investigation and prosecution of criminal offenses and the execution of criminal penalties; and the Directive (EU) 2016/680 of the European Parliament and of the Council, April 27, 2016 (24).
Results
In Barcelona, between January 2003 and December 2022, 770 cases of pulmonary TB were reported with 1,222 cohabiting contacts under 15 years of age. During the study, 22 (1.8%) of these contacts were lost to follow-up and were therefore removed from the statistical analysis. After applying the selection criteria, the study population included 1,084 contacts of 700 TB cases. The number of contacts who tested positive for the TST was 237 at the first screening and 29 at the second screening, for a total of 266 (Figure 1). The median age of TB IC with contacts with TBI was lower in migrants, both for females and males (Figure 2).
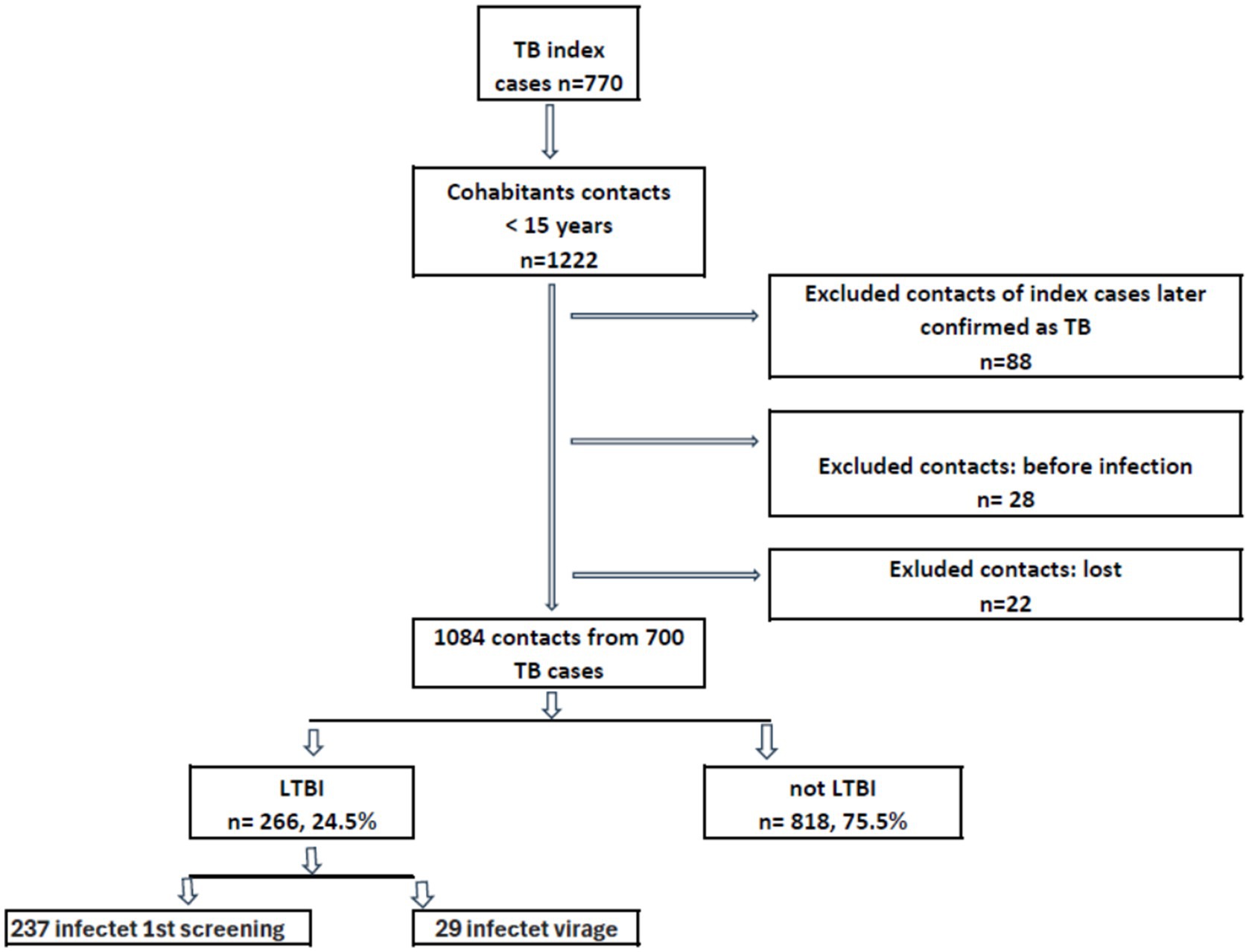
Figure 1. Flowchart of tuberculosis cases and their cohabiting contacts younger than 15 years reported to the Epidemiological Surveillance Service of the Public Health Agency of Barcelona. Barcelona, 2003–2022.
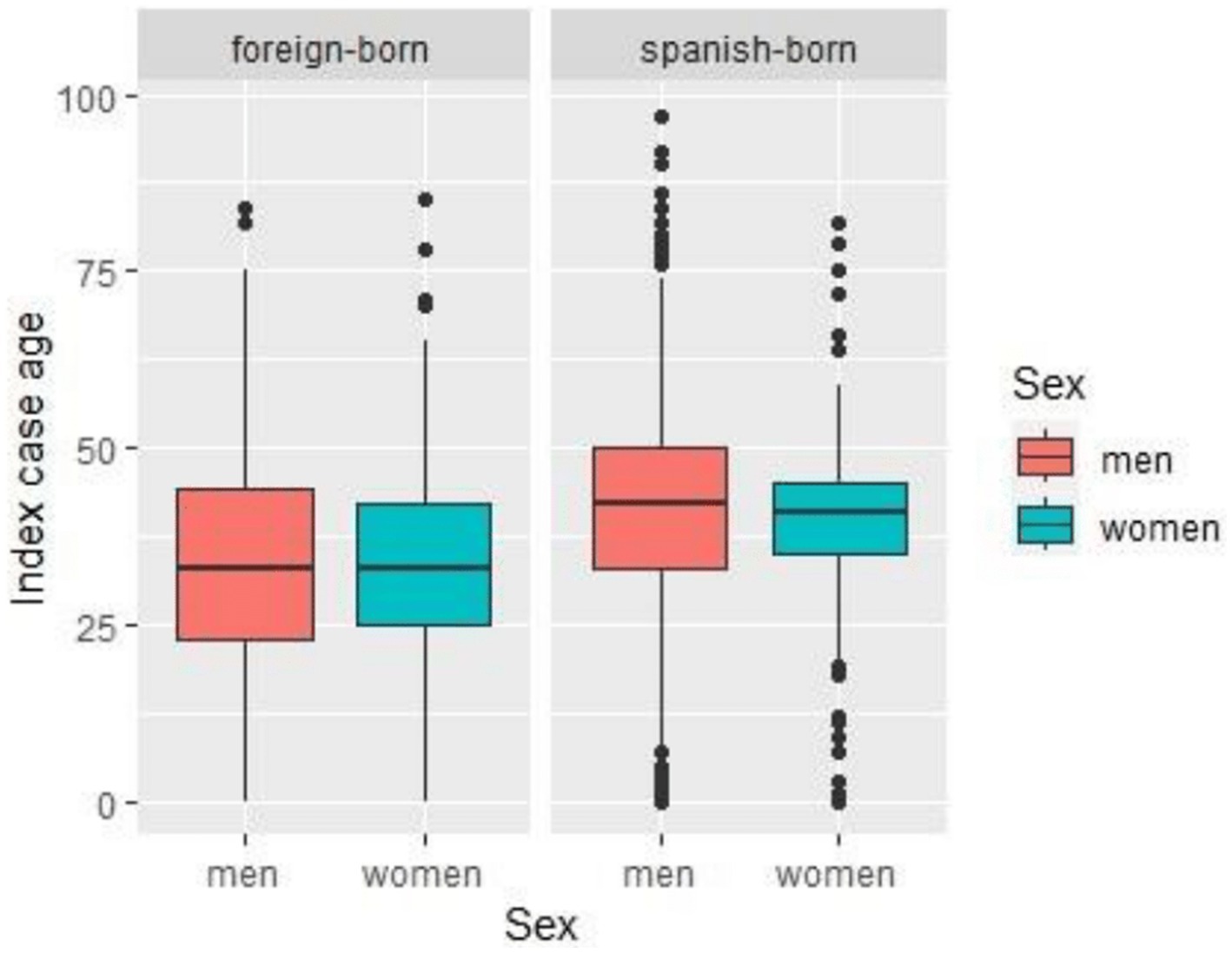
Figure 2. Distribution of ICs age by sex in foreign-born (left) and Spanish-born (right). Age distribution is shown in males (red) and females (teal) ICs. The median age, interquartile range, and outliers are displayed for each group.
Figure 3 illustrates the geographic distribution of TBI cases according to the MD of residence of the IC without statistical significance.
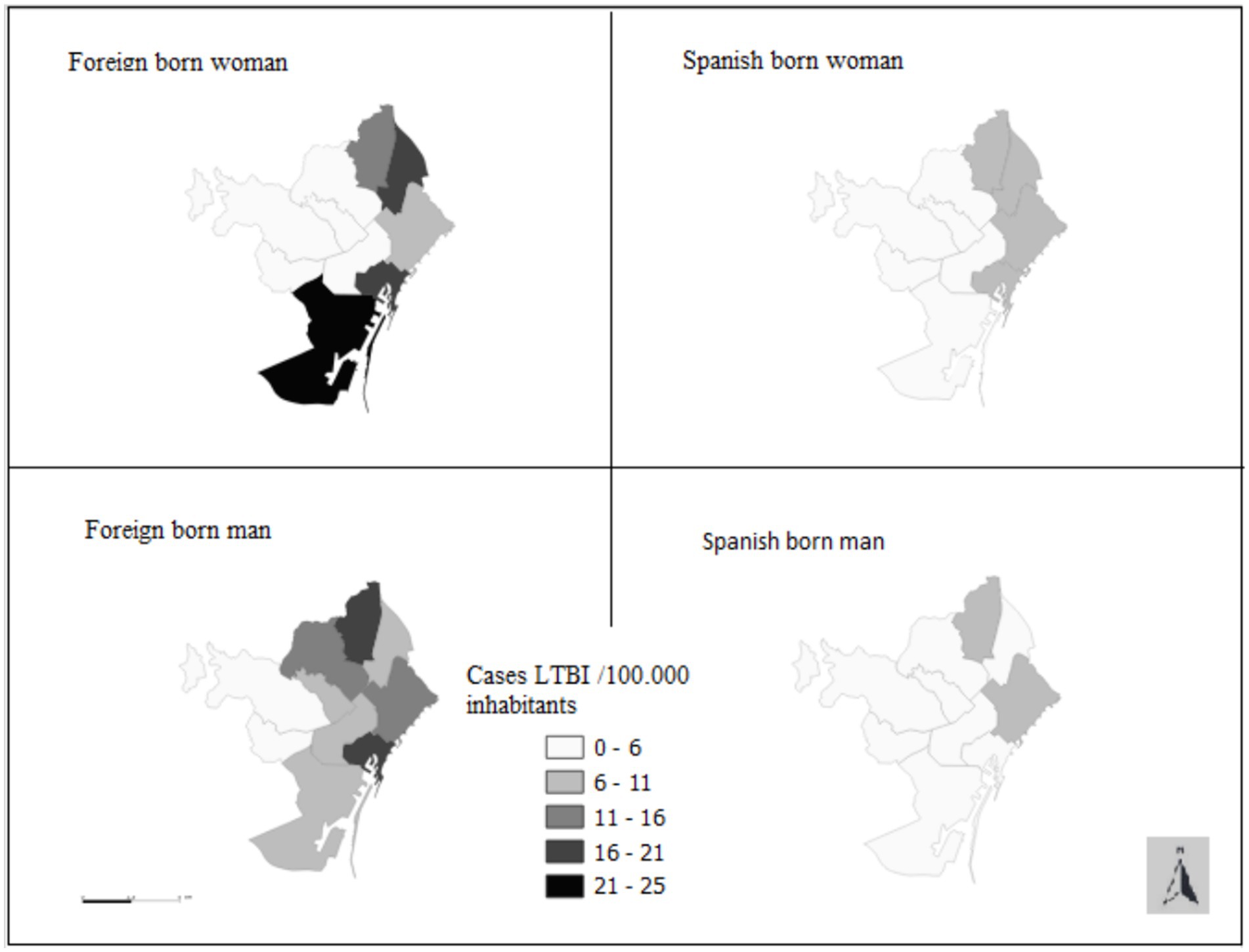
Figure 3. Distribution of TBI Cases Among Contacts by Residential MD of the Index Case, Stratified by Sex and Migratory Status (Barcelona, 2003–2022).
The mean number of cohabiting contacts under 15 years of age per case was 1.61 when the IC was a female and 1.49 when the IC was a male (Tables 1.1, 1.2). Among contacts, the prevalence of TBI was 24.5% (Tables 1.1, 1.2) and the prevalence of TB was 7.5%.
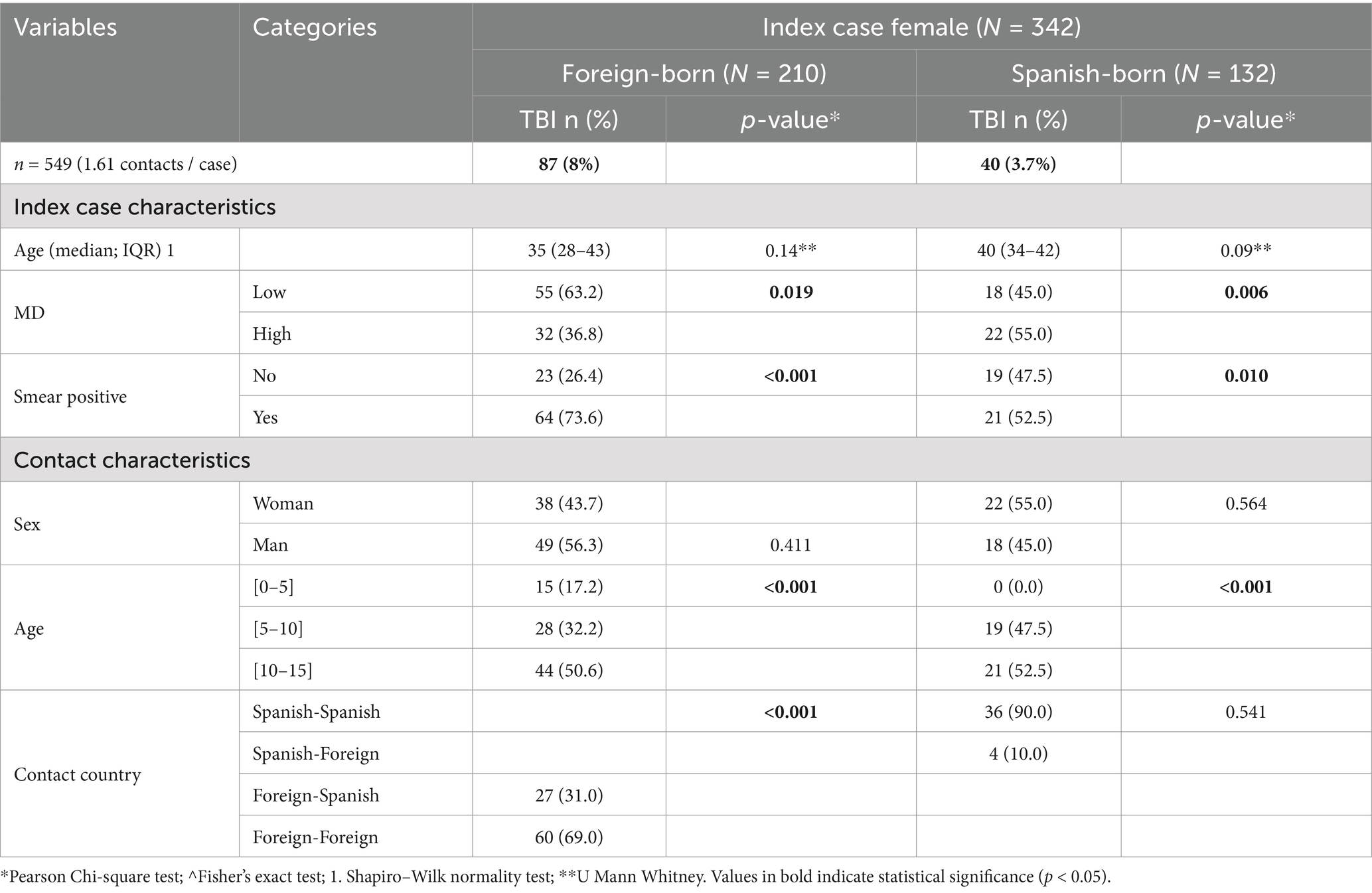
Table 1.1. Characteristics and TBI prevalence among contacts of female ICs, by IC and contact demographics, Barcelona 2003–2022.
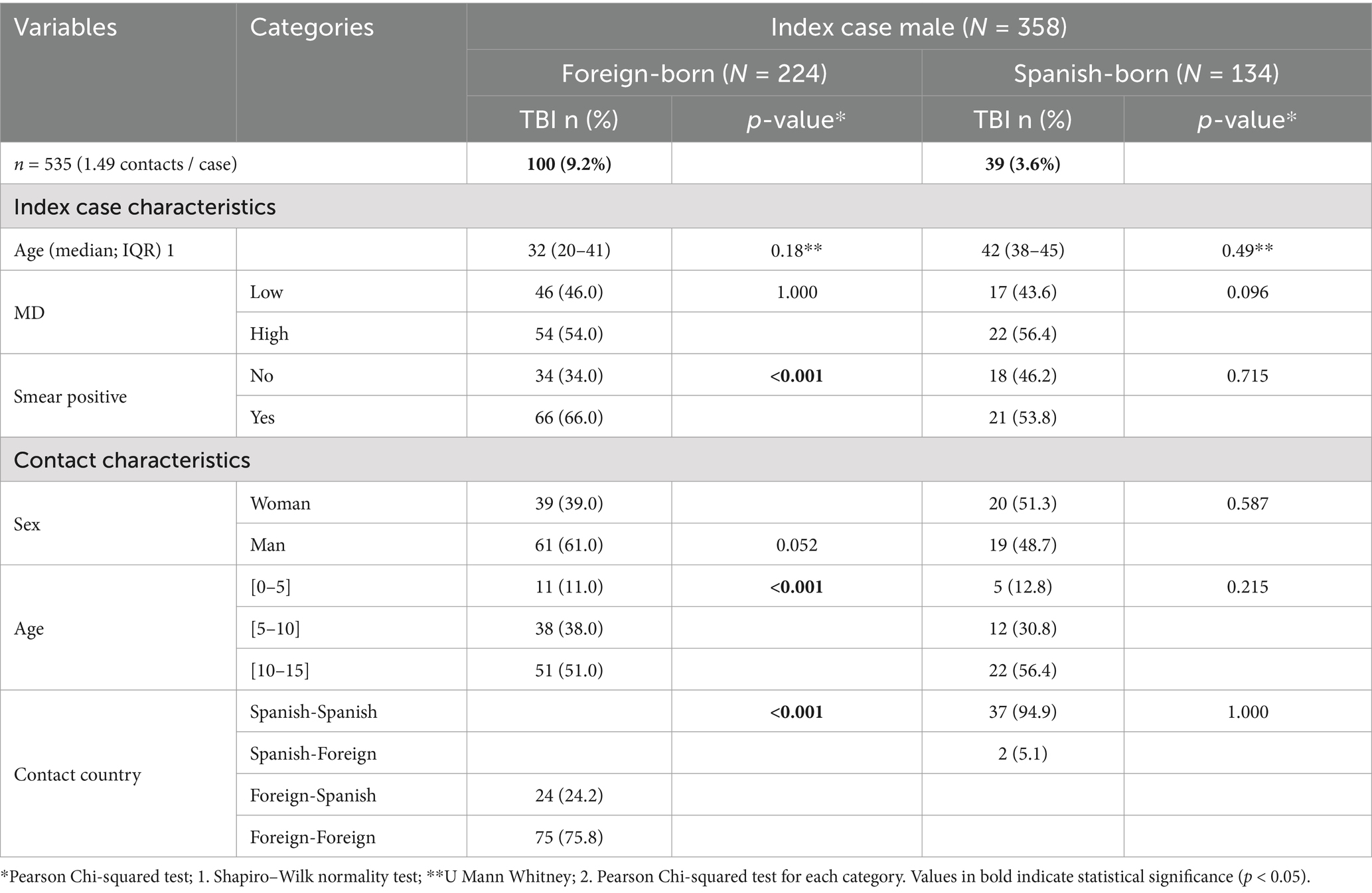
Table 1.2. Characteristics and TBI prevalence among contacts of male ICs, by IC and contact demographics, Barcelona 2003–2022.
Among the contacts of female ICs, the variables significantly associated with TBI were a smear positive of the IC and an age range of 10 to 15 years of the contacts (Table 1.1). In the case of migrant female ICs, other variables significantly associated with TBI were the following: MD with a high prevalence of TB, and the concomitant migrant status of the case and the contact. In the case of native female ICs, there was a significant association between TBI and living in an MD with a low prevalence of TB (Table 1.1; Figure 3).
Among the contacts of migrant male ICs, the variables significantly associated with TBI were a smear positive, an age range of 10 to 15 years, and the concomitant migrant status of the case and the contact (Table 1.2). In the case of native male ICs, none of the variables studied presented significant differences (Table 1.2). Among migrants, both females and males and especially when the IC was a male, we observed that the older the age of the contact, the greater the presence of TBI.
In the bivariate analysis, among the contacts of migrant ICs, both females and males, the following factors were significantly predicting TBI: a smear positive of the IC, older contact age, and the migratory status of both the IC and the contact. For contacts of native ICs, both females and males, TBI was predicted by residing in an MD with a lower incidence of TB and smear positive when the ICs were native females.
The multivariate analysis confirmed the results of the bivariate analysis, except for MD in the case of native female ICs (Tables 2.1, 2.2). As we describe in the bivariate analysis, among the contacts of migrant ICs, both females and males, the following factors were significantly predictive: smear positive of the IC and older contact age. For contacts of native females’ ICs, the migratory status of both the IC and the contact was significant too.
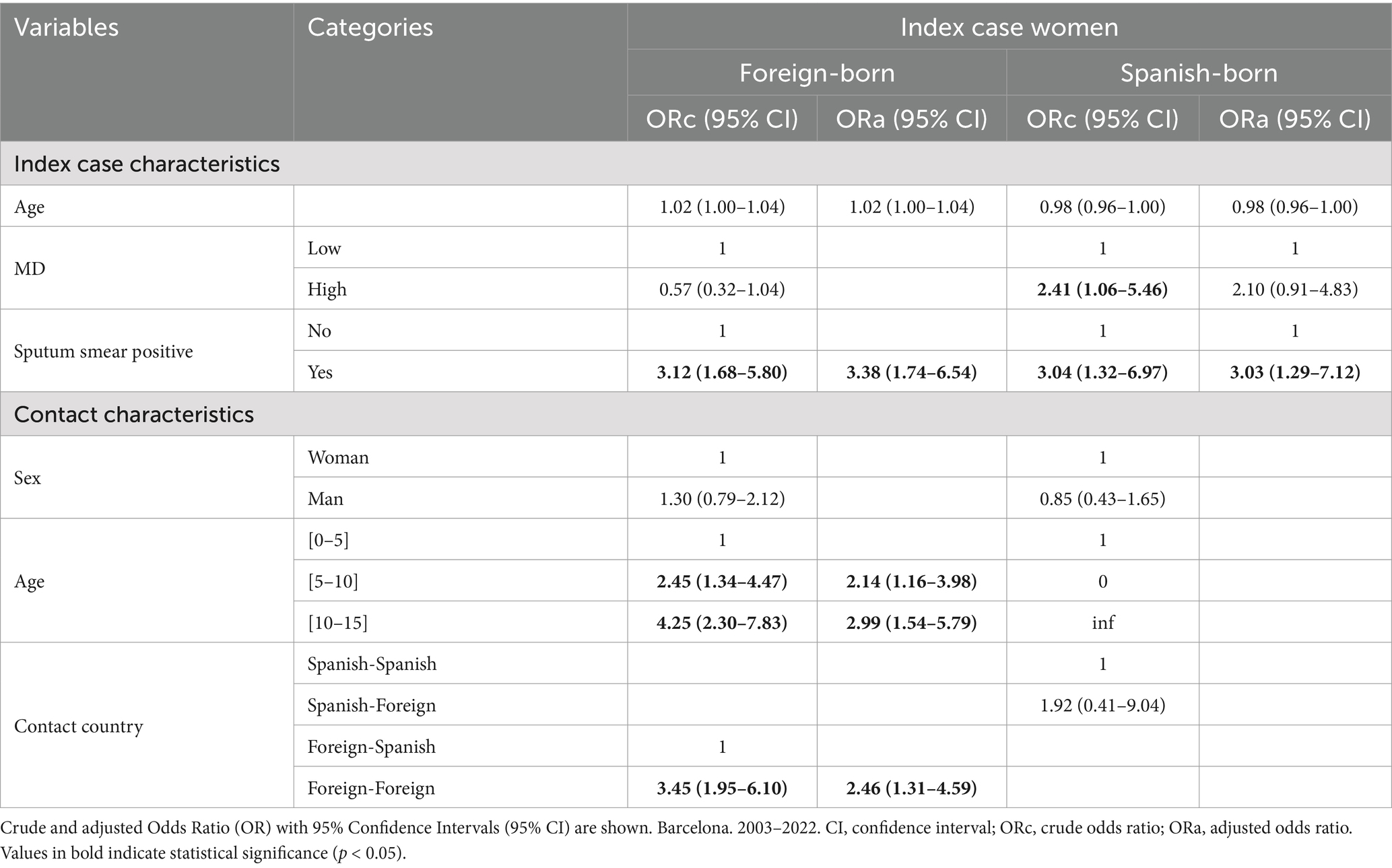
Table 2.1. Multivariate model (GEE) predicting TBI risk among contacts of female ICs, by IC and contact demographics.
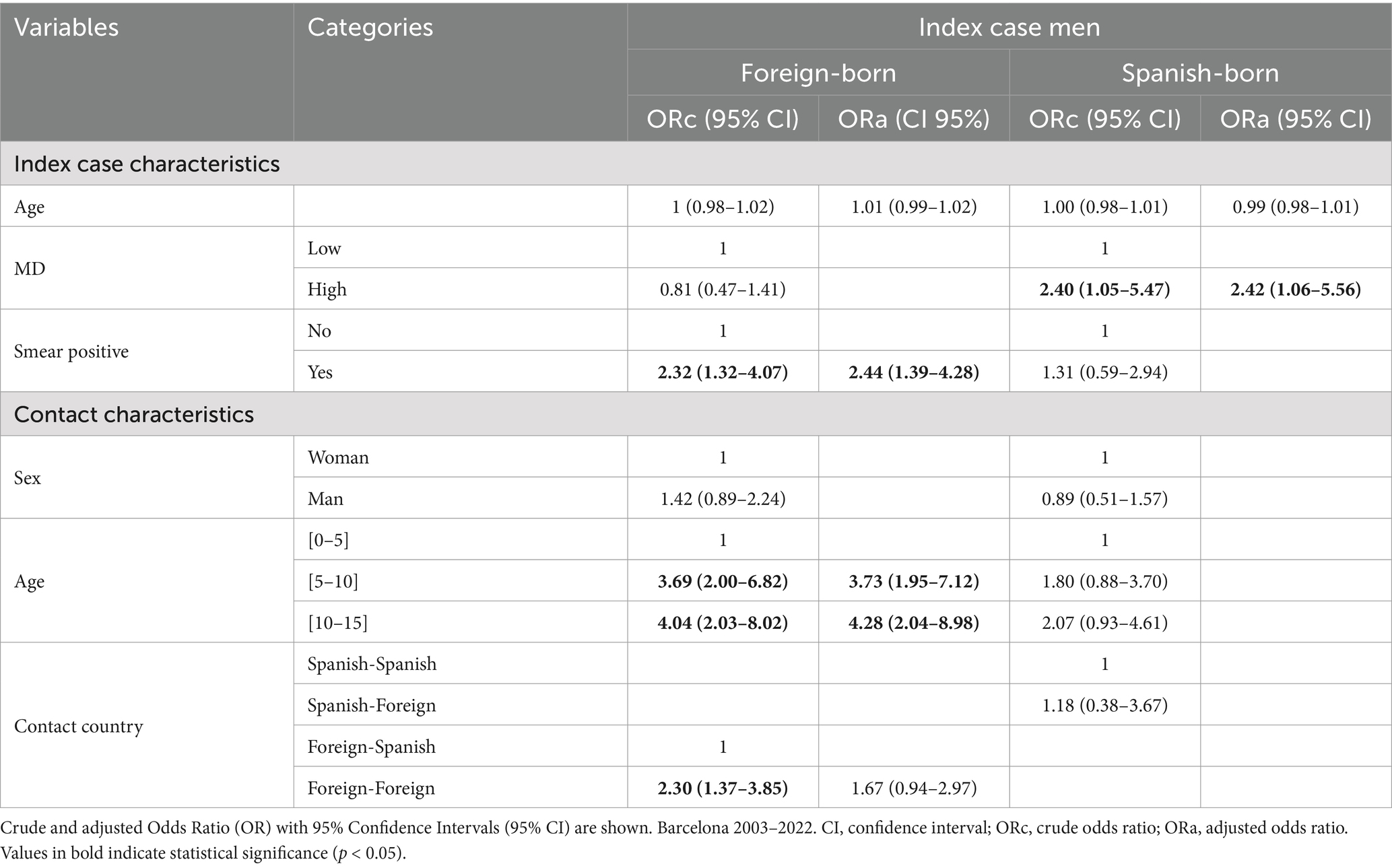
Table 2.2. Multivariate model (GEE) predicting TBI risk among contacts of male ICs, by IC and contact demographics.
We also performed an analysis of the age distribution of contacts that developed TB compared to the ones presenting TBI. This analysis found that younger age was directly associated with the presence of TB in the case of the migrant and native female ICs and the migrant male ICs (Tables 3.1, 3.2).
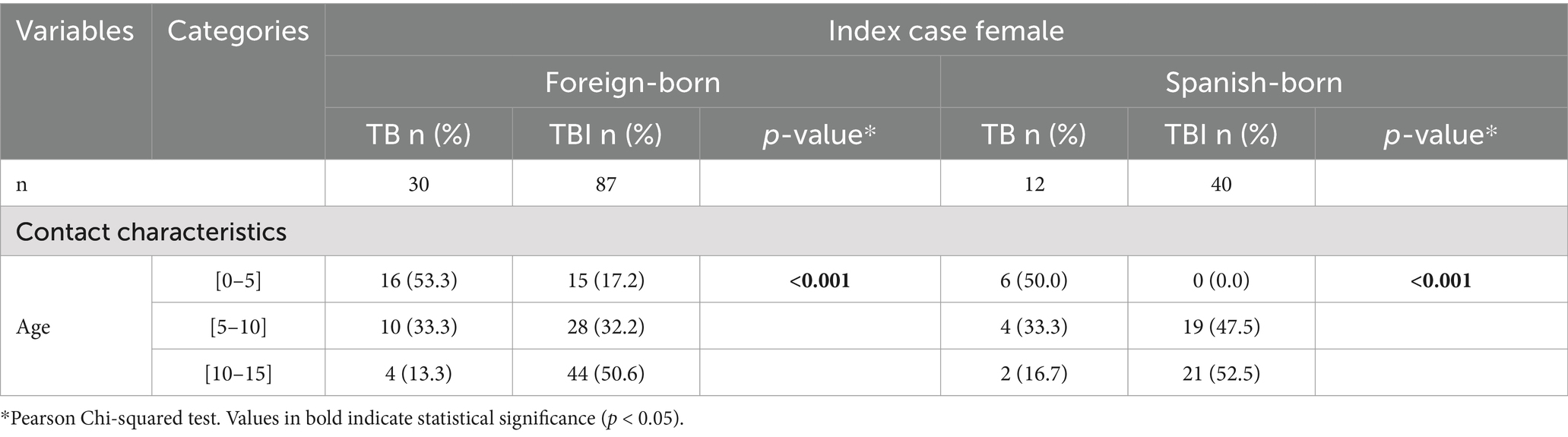
Table 3.1. Age distribution of contacts of female ICs, stratified by migratory status, Barcelona 2003–2022.
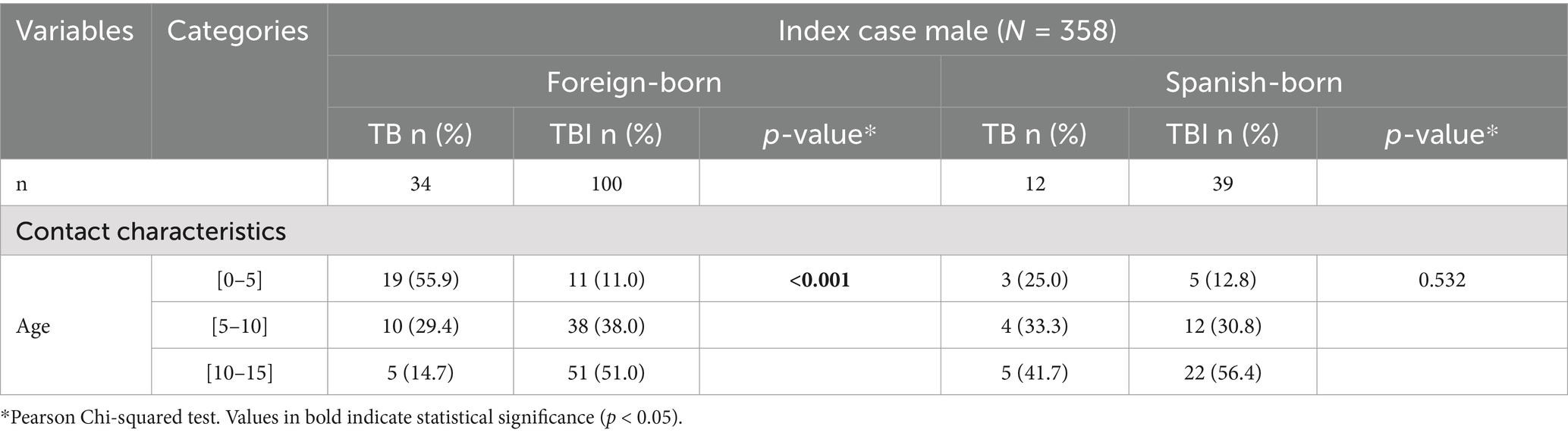
Table 3.2. Age distribution of contacts of male ICs, stratified by migratory status, Barcelona 2003–2022.
Figure 4 illustrates the results of the multivariate analysis among contacts of migrant ICs, females and males, according to the significant variables.
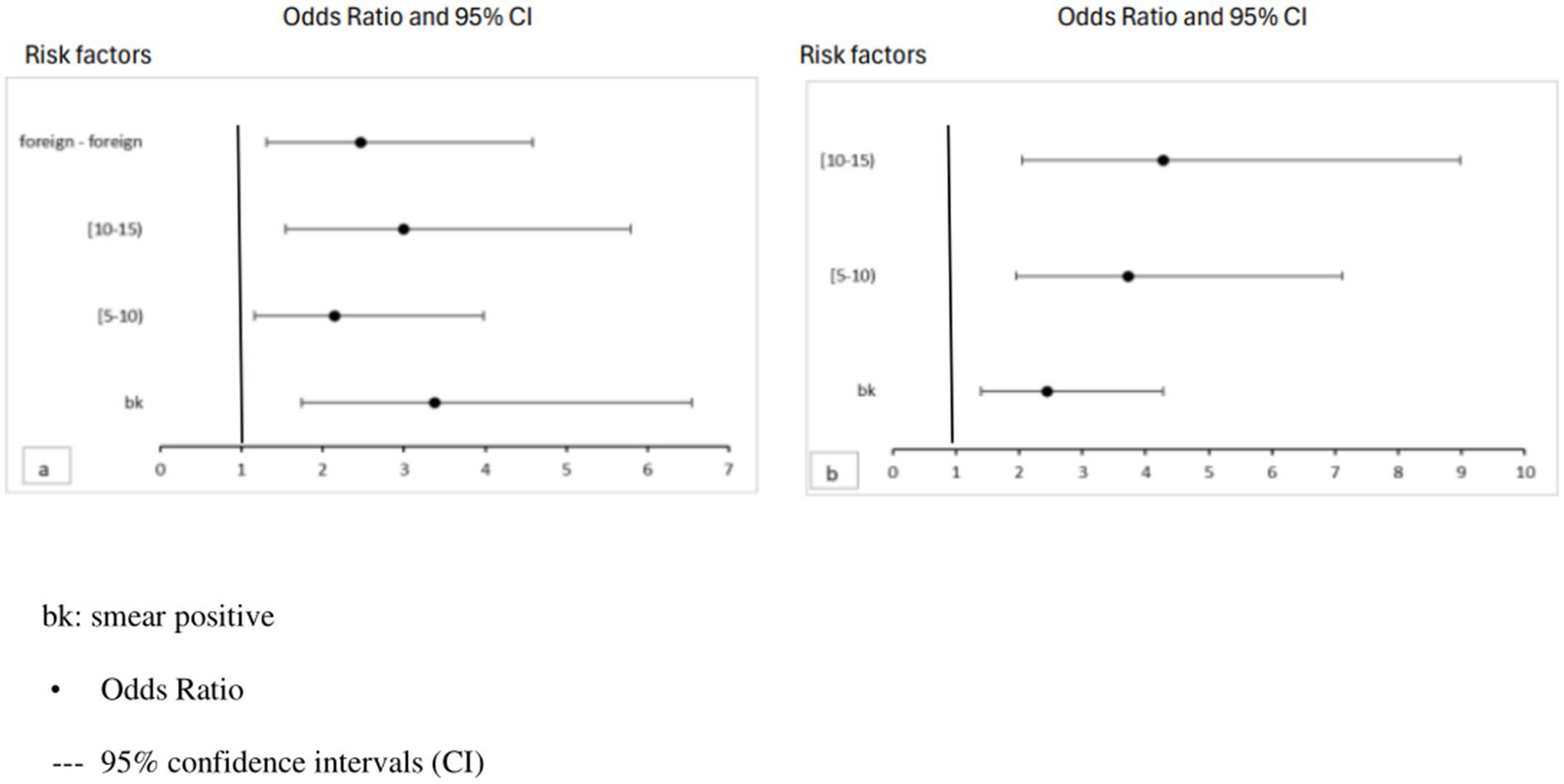
Figure 4. Risk factors for TBI in contacts of foreign-born female (a) and male (b) ICs by age. Data are presented as odds ratios with 95% CIs.
Discussion
During the study period (2003–2022), the prevalence of TBI among cohabiting contacts of TB ICs under 15 years of age was 24.5%, higher than the estimated 3% among the population under 15 years of age in Europe (1) and similar to the 27.9% found in contacts under 5 years of age in a systematic review of 17 studies in low TB burden countries (25). Other research in high-income countries has reported TBI prevalence in children under 15 years old ranging from 16 to 41% (26). The mean age of ICs was highest in male natives, followed by female natives, migrant males, and migrant females.
Contacts of native male ICs from MDs with lower TB incidence were at higher risk of TBI compared to other contacts. This elevated risk may be related to delays in the diagnosis and treatment of these ICs, possibly because of limited awareness and perception of TB risk in ICS males (21). Additionally, males may be influenced by social constructs of strength, leading to delays in seeking medical care. They are less likely to report their symptoms and may reject interventions, particularly in the context of low-qualified and low-wage informal jobs, and of the idealization of harmful masculinities (27, 28). Similarly, in the unadjusted analysis, contacts of native female ICs from MDs with lower TB incidence showed a higher risk of TBI, although this was not statistically significant.
Contacts of smear positive TB patients, likely at a more advanced disease stage, had a higher risk of developing TBI. This risk was highest among contacts of migrant female ICs, followed by contacts of native female ICs and contacts of migrant male ICs. This diagnostic delay for female ICs could be linked to gender-related health inequalities, most likely due to their role as primary family caregivers (29, 30). This has been observed in national health surveys (31) and qualitative studies conducted in high TB burden settings (32). This delay is even higher among migrant women, for whom the interrelated challenges of being a woman and a migrant exacerbate the situation, according to other studies (33).
Another factor contributing to delayed diagnosis is the stigma associated with TB, which may lead ICs to fear job loss, eviction, or restricted access to education. Stigma, as a social determinant of health, also creates barriers to accessing health care systems (34). For migrant populations, these barriers contribute to increased diagnostic delays and increased transmission of TB within the community and among close contacts, as reported in previous studies (35). Additional research has linked TB to a lack of family support, arising from fears of infection and social blame, further exacerbating diagnostic delays (36).
Contacts of migrant men with IC, followed by contacts of migrant women with IC in contacts older than 5 years, showed a higher risk of TBI, with a positive gradation of risk. This same gradation has been observed in other studies (37) and may be explained by greater exposure to possible TB cases in the contacts’ countries of origin, although this explanation has not been verified. To explore this hypothesis, in the future, the time elapsed between the contacts’ arrival in the country and their diagnosis could be evaluated in different age groups.
Being both the IC and the contact migrants represented a risk factor for TBI in contacts, possibly because of increased exposure from travel to their countries of origin (6, 38).
One limitation of this study is the exclusion or inaccuracies in data collection of some important variables, such as diagnostic delay, symptom presence, and income. Additionally, the data obtained in this study may overestimate TBI prevalence, as in many contacts the screening of migrated patients has not been carried out as required by the 2015 “Recommendations for the prevention and control of pediatric tuberculosis in Catalonia” (6, 39).
Another limitation of our study is that some stratification resulted in small groups, and this could lead to a loss of statistical power in the multivariate analysis.
This population-based study’s findings could be extrapolated to other large cities with high migrant populations and similar TB burden and incidence profiles to Barcelona. Such population characteristics are likely to become increasingly common because of demographic changes and displacements driven by climate change (40).
Although not specifically analyzed in our study, effective contact studies in migrant populations require support from community health agents, especially in groups facing strong language barriers (41).
The results of our study underscore the importance of contact studies to promptly detect and treat TBI in children under 15 years of age, aiming to prevent progression to active TB. Our study supports the current recommendations for contact tracing in pulmonary TB ICs. It also highlights the need for additional measures, such as providing primary chemoprophylaxis for contacts under 5, patient and family education, home visits, minimizing delays in diagnosing ICs, conducting active case surveillance, and addressing axes of inequality (sex, age, and migratory status), treatment monitoring, and the involvement of the health system, especially tuberculosis units (42). Incorporating these strategies can improve the effectiveness of contact tracing and ensure proper follow-up for treatment adherence.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: dataset from epidemiological surveillance databases. Requests to access these datasets should be directed to cnByaWV0b0Bhc3BiLmNhdA==.
Ethics statement
The studies involving humans were approved by Comité de Ética de la Investigación con medicamentos del Parc de Salut MAR. 2023/11081. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because the tuberculin test in children within the tuberculosis contact tracing did not require informed consent, as it is a mandatory public health strategy for detecting and preventing the disease. Its application was supported by national and international regulations, it was a safe and low-risk procedure, and it served the best interests of the child by preventing the progression to active tuberculosis. Additionally, in the context of epidemiological surveillance, its implementation was considered a necessary measure to protect both individual and community health.
Author contributions
RP-G: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. JM: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. AS-A: Validation, Writing – review & editing. ME: Validation, Writing – review & editing. CB: Validation, Writing – review & editing. MR: Validation, Writing – review & editing. NL: Validation, Writing – review & editing. AN-J: Validation, Writing – review & editing. EM: Visualization, Writing – review & editing. CD: Visualization, Writing – review & editing. MR: Visualization, Writing – review & editing. MM: Visualization, Writing – review & editing. JO: Visualization, Writing – review & editing. CG: Visualization, Writing – review & editing. PS: Visualization, Writing – review & editing. CR: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. With the support of the Industrial Doctorate Plan of the Department of Research and Universities of the Generalitat de Catalunya.
Acknowledgments
The authors would like to thank all the health care and administrative staff of the Epidemiology Service, Barcelona Public Health Agency (PHAB) and all physicians and TB nurses from the Catalonia hospitals. Without them, this work would not have been possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ASPB, Public Health Agency of Barcelona (Agència de Salut Pública de Barcelona); CEIC, Clinical Research Ethics Committee; IC, Index case; MD, Municipal District; TBI, Tuberculosis infection; ORc, Crude Odds Ratio; ORa, Adjusted Odds Ratio; TB, Tuberculosis; TST, Tuberculin skin test.
References
1. WHO Global Tuberculosis Programme. TB: a global emergency, WHO report on the TB epidemic [Internet]. (1994). Available online at: https://iris.who.int/handle/10665/58749 (Accessed April 5, 2025).
2. European Centre for Disease Prevention and Control, & WHO Regional Office for 324 Europe. Tuberculosis surveillance and monitoring in Europe 2023-2021 data. 325 Stockholm: European Centre for Disease Prevention and Control; Copenhagen: WHO 326 Regional Office for Europe. (2023).
3. Martinez, L, Shen, Y, Mupere, E, Kizza, A, Hill, PC, and Whalen, CC. Transmission of Mycobacterium Tuberculosis in households and the community: a systematic review and Meta-analysis. Am J Epidemiol. (2017) 185:1327–39. doi: 10.1093/aje/kwx025
4. Narasimhan, P, Wood, J, Macintyre, CR, and Mathai, D. Risk factors for tuberculosis. Pulm Med. (2013) 2013:11. doi: 10.1155/2013/828939
5. Wood, R, Johnstone-Robertson, S, Uys, P, Hargrove, J, Middelkoop, K, and Lawn, SD, et al. Tuberculosis transmission to young children in a south African community: Modeling household and community infection risks. (2010). Available online at: https://academic.oup.com/cid/article/51/4/401/477332 (Accessed June 3, 2024).
6. Houben, RMGJ, and Dodd, PJ. The global burden of latent tuberculosis infection: a re-estimation using mathematical modelling. PLoS Med. (2016) 13:e1002152. doi: 10.1371/journal.pmed.1002152
7. Pediatría Integral.Tuberculosis pulmonar en Pediatría. (2021). Available online at: https://www.pediatriaintegral.es/publicacion-2021-03/tuberculosis-pulmonar-en-pediatria/ (Accessed July 18, 2023).
8. Gowrishankar, NC. Tuberculosis: Natural History. (2019). Available online at: https://www.pidjournal.com/doi/PID/pdf/10.5005/jp-journals-10081-1102
9. Gong, W, and Wu, X. Differential diagnosis of latent tuberculosis infection and active tuberculosis: a key to a successful tuberculosis control strategy. Front Microbiol. (2021) 12. doi: 10.3389/fmicb.2021.745592
10. WHO consolidated guidelines on tuberculosis: module 2: screening: systematic screening for tuberculosis disease [Internet]. Available online at: https://www.who.int/publications/i/item/9789240022676 (Accessed July 11, 2024).
11. Heemskerk, D, Caws, M, Marais, B, and Farrar, J. Tuberculosis in adults and children. (2015) 2. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK344402/ (Accessed July 4, 2024).
12. Martinez, L, Cords, O, Horsburgh, CR, Andrews, JR, Acuna-Villaorduna, C, Desai Ahuja, S, et al. The risk of tuberculosis in children after close exposure: a systematic review and individual-participant meta-analysis. Lancet. (2020) 395:973–84. doi: 10.1016/S0140-6736(20)30166-530166-5
13. WHO. Aplicación de la estrategia fin de la TB: Aspectos esenciales [implementing the end TB strategy: The essentials]. Ginebra: Organización Mundial de la Salud (2016). Available online at: http://apps.who.int/iris
14. María, J, and García, G. estudio de contactos de tuberculosis. Medicina respiratoria. (2012) 37:37–47.
15. Barrabeig-Fabregat, I, Clotet-Romero, L, Mercè, R, Orcau-Palau, À, Parrón-Bernabé, I, Rodés-Monegal, A, et al. Recomanacions per a la realització d’estudis de contactes de malalts amb tuberculosi a Catalunya. Scientia. (2018) 12–34.
16. Borrell, C, Pasarín, MI, Díez, E, Pérez, K, Malmusi, D, Pérez, G, et al. Las desigualdades en salud como prioridad política en Barcelona. Gac Sanit. (2020) 34:69–76. doi: 10.1016/j.gaceta.2020.01.003
17. Borrell, C, Pons-Vigués, M, Morrison, J, and Díez, È. Factors and processes influencing health inequalities in urban areas. J Epidemiol Community Health. (2013) 67:389–91. doi: 10.1136/jech-2012-202014
19. Nolt, D, and Starke, JR. Tuberculosis infection in children and adolescents: testing and treatment. Pediatrics. (2021) 148. doi: 10.1542/peds.2021-054663
20. Nevada Division of Public and Behavioral Health. Pediatric Tuberculosis and LTBI: Diagnosis and Treatment of Latent Tuberculosis Infection (LTBI) and Tuberculosis Disease in Children (under 15 years of age). In: Tuberculosis Program Manual (2020) 12.1–12.34.
21. Bailey, WC, Gerald, LB, Kimerling, ME, Redden, D, Brook, N, Bruce, F, et al. Predictive model to identify positive tuberculosis skin test results during contact investigations. JAMA. (2002) 287:996–1002. doi: 10.1001/jama.287.8.996
22. Declaración de Helsinki de la AMM. Principios éticos para las investigaciones médicas en seres humanos, WMA. The World Medical Association. (2024). Available online at: https://www.wma.net/es/policies-post/declaracion-de-helsinki-de-la-amm-principios-eticos-para-las-investigaciones-medicas-en-seres-humanos/ (Accessed July 1, 2024).
23. BOE.es - BOE-A-2021-8806 Ley Orgánica 7/2021, de 26 de mayo, de protección de datos personales tratados para fines de prevención, detección, investigación y enjuiciamiento de infracciones penales y de ejecución de sanciones penales [Internet]. (2021). Available online at: https://www.boe.es/buscar/act.php?id=BOE-A-2021-8806
24. Parlamento Europeo y Consejo de la Unión Europea. Directiva (UE) 2016/680 relativa a la protección de las personas físicas en lo que respecta al tratamiento de datos personales por parte de las autoridades competentes para fines de prevención, investigación, detección o enjuiciamiento de infracciones penales o de ejecución de sanciones penales, y a la libre circulación de dichos datos. (2016). Available online at: https://eur-lex.europa.eu/legal-content/ES/TXT/HTML/?uri=CELEX:32016L0680&from=ES (Accessed July 1, 2024).
25. Hamada, Y, Glaziou, P, Sismanidis, C, and Getahun, H. Prevention of tuberculosis in household members: estimates of children eligible for treatment. Bull World Health Organ. (2019) 97:534–547D.
26. Fox, GJ, Barry, SE, Britton, WJ, and Marks, GB. Contact investigation for tuberculosis: a systematic review and meta-analysis. Eur Respir J. (2012) 41:140–56. doi: 10.1183/09031936.00070812
27. Chikovore, J, Hart, G, Kumwenda, M, Chipungu, GA, Desmond, N, and Corbett, L. Control, struggle, and emergent masculinities: a qualitative study of men’s care-seeking determinants for chronic cough and tuberculosis symptoms in Blantyre. Malawi BMC Public Health. (2014) 14:1–12. doi: 10.1186/1471-2458-14-1053
28. Wysocki, AD, Ponce, MAZ, and Scatolin, BE. Atraso na procura pelo primeiro atendimento para o diagnóstico da tuberculose. Rev Esc Enferm USP. (2013) 47:440–7. doi: 10.1590/S0080-62342013000200024
29. Fonseca Mardones, I, and Clave, P. Influencia del género en la salud de las mujeres cuidadoras familiares. Revista Chilena de Terapia Ocupacional. (2020) 20:211–9. doi: 10.5354/0719-5346.2020.51517
30. Carla Da Silva, T, Lima Pinto, M, Orlandi, GM, Maria, T, Monteiro De Figueiredo, R, De Siqueira, O, et al. A tuberculose na perspectiva do homem e da mulher. Rev Esc Enferm USP. (2022) 56:e20220137. doi: 10.1590/1980-220X-REEUSP-2022-0137en
31. Artazcoz, L, Borrell, C, and Benach, J. Gender inequalities in health among workers: the relation with family demands. J Epidemiol Community Health. (2001) 55:639–47. doi: 10.1136/jech.55.9.639
32. Gosoniu, GD, Ganapathy, S, Kemp, J, Auer, C, Somma, D, Karim, F, et al. Gender and socio-cultural determinants of delay to diagnosis of TB in Bangladesh, India and Malawi. Int J Tuberc Lung Dis. (2008) 12:848–55.
33. Moynihan, C. Theories in health care and research: theories of masculinity. BMJ Br Med J. (1998) 317:1072.
34. Bertolín, EG, Seises, JAQ, Morales, EM, and Antolín, EF. Papel del estigma social, la radiografía de tórax y la Atención Primaria en la detección de casos de Tuberculosis: a propósito de un caso. Rev Esp Salud Publica. (2020) 19–34. doi: 10.1590/RESP202010120
35. Sánchez-Montalvá, A, Salvador, F, Molina-Morant, D, and Molina, I. Tuberculosis e inmigración. Enferm Infecc Microbiol Clin. (2018) 36:446–55.
36. Miranda López, JJ, and Ochoa Soto, R. Desigualdades de género y las redes de apoyo social en pacientes con tuberculosis. Rev. cuba. hig. epidemiol [Internet]. (2023) 60. Available online at: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1561-448 30032023000100014&lng=es (Accessed April 29, 2025).
37. Reichler, MR, Khan, A, Yuan, Y, Chen, B, McAuley, J, Mangura, B, et al. Duration of exposure among close contacts of patients with infectious tuberculosis and risk of latent tuberculosis infection. Clin Infect Dis. (2020) 71:1627–34. doi: 10.1093/cid/ciz1044
38. Perez-Porcuna, TM, Noguera-Julian, A, Riera-Bosch, MT, Macià-Rieradevall, E, Santos-Santiago, J, Rifà Pujol, MÀ, et al. Tuberculosis among children visiting friends & relatives. J Travel Med. (2024) 31. doi: 10.1093/jtm/taae037
39. Asensio, O, Domínguez-Benítez, JA, Altet-Gómez, N, Follia-Alsina, N, Font, R, Noguera-Julián, A, et al. Recomanacions per a la prevenció i el control de la tuberculosi pediàtrica a Catalunya. Scientia. (2015) 45–67.
40. Ferrero-Turrión, R. Desplazamientos medioambientales. Revista Diecisiete: Investigación Interdisciplinar para los Objetivos de Desarrollo Sostenible. (2022) 6:107–19. Available online at: https://plataforma2030.org/es/desplazamientos-medioambientales
41. Vargas Urpi, M, Gil Bardají, A, and Arumí, Ribas M. Inmigrantes en Cataluña: ¿una comunicación efectiva en los servicios públicos? (2013). Available online at: http://repositori.upf.edu/handle/10230/23656 (Accessed April 10, 2025).
Keywords: latent tuberculosis infection, contact tracing, children, axes of inequality, tuberculosis
Citation: Prieto-García R, Millet JP, Soriano-Arandes A, Espiau M, Broto C, Ronda M, López N, Noguera-Julian A, Masdeu Corcoll E, Domingo Jimenez C, Ros Samsó M, Marcos Arroita MI, Ospina Valencia JE, García Rebollo C, Simon Viván P and Rius Gibert C (2025) Tuberculosis household contact tracing in children: axes of inequality, Barcelona 2003–2022. Front. Public Health. 13:1591552. doi: 10.3389/fpubh.2025.1591552
Edited by:
Ying Luo, University of Texas Southwestern Medical Center, United StatesReviewed by:
Pui Yeung Lee, Yale University, United StatesXutong Xue, Boston Children’s Hospital and Harvard Medical School, United States
Li Meng, University of Texas Southwestern Medical Center, United States
Da Chen, University of Texas Southwestern Medical Center, United States
Yanan Wu, University of Michigan, United States
Copyright © 2025 Prieto-García, Millet, Soriano-Arandes, Espiau, Broto, Ronda, López, Noguera-Julian, Masdeu Corcoll, Domingo Jimenez, Ros Samsó, Marcos Arroita, Ospina Valencia, García Rebollo, Simon Viván and Rius Gibert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Raquel Prieto-García, cnByaWV0b0Bhc3BiLmNhdA==
†These authors have contributed equally to this work