 Eman A. Abduljawad
Eman A. Abduljawad Buthaina M. Aljehany
Buthaina M. Aljehany Haya Aljadani
Haya Aljadani Howeida Abusalih
Howeida Abusalih- 1Food and Nutrition Department, Human Sciences and Design Faculty, King Abdulaziz University, Jeddah, Saudi Arabia
- 2Department of Health Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Aim: This study examines the determinants of fruit and vegetable consumption among Saudi adults using an extended Theory of Planned Behavior (TPB) model. The model incorporates core TPB constructs—attitudes, subjective norms, and perceived behavioral control (PBC)—along with sociodemographic, behavioral, and knowledge-related factors.
Methods: A cross sectional study was conducted on a sample of adult Saudis (n = 471). Data were analyzed using structural equation modeling, comparing a basic TPB model with an extended model that included additional predictors such as knowledge about World Health Organization (WHO) dietary recommendations, diet, family meals, and physical activity.
Results: PBC has is a strong predictor of behavior compared to intention. For intention, attitude (unstandardized coefficients [coeff] = 0.29, standard error [se] = 0.13, p = 0.025), subjective norm (coeff = 0.37, se = 0.11, p = 0.001), and PBC (coeff = 1.29, se = 0.17, p = 0.000) are all significant predictors. The extended model explained slightly more variance in behavior (R2 = 0.45) and intention (R2 = 0.78) compared to the basic model (behavior: R2 = 0.40; intention: R2 = 0.74), highlighting the added value of these factors. PBC emerged as the strongest predictor of behavior (coeff = 0.71, se = 0.26, p = 0.006), while knowledge (coeff = 0.29, se = 0.05, p < 0.001) and family meals (coeff = 0.19, se = 0.05, p < 0.001) significantly predicted attitudes. Moderate physical activity was associated with subjective norms (coeff = 0.08, se = 0.03, p = 0.009), suggesting a synergistic relationship between physical activity and dietary behavior.
Conclusion: These findings underscore the importance of addressing both psychological and practical factors in interventions to promote fruit and vegetable consumption among Saudi population, with a focus on enhancing self-efficacy, leveraging family dynamics, and integrating physical activity promotion.
1 Introduction
It is well established that the consumption of fruits and vegetables is widely recognized as a cornerstone of a healthy diet, playing a critical role in preventing chronic diseases such as obesity, cardiovascular diseases, diabetes, hypertension, coronary heart disease, and stroke World Health Organization (WHO) (1, 2), with recent meta-analyses demonstrating dose-dependent mortality reductions (3). Beyond chronic diseases prevention, adequate intake of fruits and vegetables has been associated with the prevention of weight gain, the delay of geriatric conditions (4), modification the gut microbiota composition and reducing the pro-inflammatory response (5). Considering this scientific evidence, the WHO and the Food and Agriculture Organization (FAO) advise a minimum daily consumption of 400 grams of fruits and vegetables per person, excluding starchy tubers (6), recently reaffirmed in updated global guidelines (40). This guideline is frequently promoted through public health campaigns like the “Five-a-Day” initiative, which advocates for the daily intake of at least five servings of fruits and vegetables (7). Despite these widely recognized recommendations, global compliance with dietary guidelines remains inadequate, as many populations do not achieve the advised levels of intake (2). Emerging solutions include food system approaches (8), digital interventions (9), and fiscal policies (10) to address these persistent challenges.
To better understand and encourage healthier eating habits, researchers have increasingly relied on psychological and behavioral theories, such as the Theory of Planned Behavior (TPB) (11). According to the TPB, behavior is shaped by three core constructs: attitudes, subjective norms, and perceived behavioral control (PBC). Attitudes represent an individual’s positive or negative evaluation of a behavior, subjective norms reflect the perceived social pressure to engage in the behavior, and PBC refers to the perceived ease or difficulty of performing the behavior (11). The TPB has been extensively used to predict and analyze health-related behaviors, including dietary choices, across diverse cultural settings (12, 13, 39). Recent meta-analyses confirm its robustness in explaining dietary intentions, particularly for fruit and vegetable consumption (14, 15). For instance, research has shown that TPB constructs explain a significant portion of the variance in both the intention to consume fruits and vegetables and actual consumption levels (12). Moreover, interventions based on the TPB have proven effective in increasing fruit and vegetable intake while positively impacting TPB-related factors such as attitudes and perceived control (Kothe et al., 2012). In addition to the constructs of the Theory of Planned Behavior (TPB), sociodemographic and behavioral factors—such as age, gender, education, income, nutrition knowledge, family habits, and physical activity—have also been identified as significant predictors of dietary behavior (16–19). For example, studies have found that greater nutrition knowledge and regular family meals are positively associated with higher fruit and vegetable consumption (18, 20). Similarly, physical activity has been shown to correlate with healthier dietary patterns, indicating a synergistic relationship between these two health-promoting behaviors (17).
In Saudi Arabia, the prevalence of diet-related non-communicable diseases has surged in recent years, driven by rapid urbanization, increasingly sedentary lifestyles, and a shift toward Westernized dietary patterns (21, 22). National health surveys highlight a concerning trend: 97.4% of Saudi adults consume fewer than five servings of fruits and vegetables per day, with only 2.6% meeting the recommended intake (23). More recent data from Riyadh further emphasize this issue, revealing that 91.6% of participants consume fewer than two servings daily (24). These alarming statistics underscore the urgent need to address dietary behaviors in the country. Research has identified several factors influencing fruit and vegetable consumption among the Saudi population, including fitness consciousness, self-efficacy, perceived benefits and barriers to healthy eating, and meal planning (25–27). However, despite the widespread application of the TPB in understanding dietary choices, few studies have explored its utility in the Saudi context, where cultural and social norms may uniquely determine dietary practices (28). This study aims to address this gap by examining the factors influencing fruit and vegetable consumption among adult Saudis using an extended TPB model. By incorporating sociodemographic factors, behavioral variables, and knowledge related to fruit and vegetable consumption, the study seeks to provide a comprehensive understanding of the determinants of this dietary behavior in the Saudi population. The findings will contribute to the development of culturally tailored interventions to promote healthy eating habits, with a particular focus on increasing fruit and vegetable consumption. Specifically, the study proposes several hypotheses grounded in the TPB: (1) a positive attitude will significantly predict the intention to consume fruits and vegetables, (2) subjective norms will play a significant role in shaping these intentions, (3) PBC will significantly predict both the intention to consume fruits and vegetables and the actual behavior, (4) intention will be a strong predictor of actual fruit and vegetable consumption, and (5) lifestyle behaviors, knowledge related to fruit and vegetable consumption, and sociodemographic factors will be associated with the PBC construct.
2 Methods
2.1 Study population and study design
This study adopted a cross-sectional design and was carried out in Saudi Arabia, covering the five regions (Northern, South, East, Western and Middle). Data was collected over 6 months from May to October 2024. To be included in the study, the participant should be a Saudi citizen, living in Saudi Arabia during the time of the study, and adult aged from 18 to 59 years old. Adults aged 60 years and above were excluded from the study due to significant physiological, psychological, and behavioral differences in dietary patterns and health determinants compared to younger adults (29). In addition, this age group might introduce heterogeneity that may confound the applicability of the TPB model, as older adults tend to rely less on intention and more on habitual behavior and environmental factors when it comes to dietary choices (14, 30). Pregnant or lactating women, individuals on special diets, or those with chronic diseases affecting their fruit and vegetable intake were also excluded from the study.
The study was conducted after obtaining the ethical approval granted by the Institutional Review Board (IRB) of King Abdulaziz University (IRB Log number 15–24).
2.2 Sampling technique and sample size calculation
Due to the nature of online distribution, a non-probability convenience sampling technique was employed. Although El Bcheraoui et al. (23) reported that 97.4% of Saudi adults consumed fewer than five servings of fruits and vegetables per day, based on data from the 2013 Saudi Health Interview Survey, this information is outdated and may not accurately reflect current consumption patterns. Therefore, in the absence of current and specific national data, a conservative estimate of 50% prevalence was used. This standard approach is widely accepted when the actual population proportion is uncertain or outdated (31), as it yields to the maximum sample size and statistical power. The adult population of Saudi Arabia was estimated at approximately 13 million, as reported in The Saudi Census (45). The sample size was calculated using the following standard formula:
where:
• n = required sample size
• Z = Z-score corresponding to the desired confidence level (1.96 for 95%)
• p = estimated proportion (set at 0.50 to maximize sample size)
• d = margin of error (set at 0.05)
Thus, an initial target of 385 participants was determined. To account for potential challenges such as incomplete submissions or non-responses, an extra 10% was included, raising the minimum required sample size to 422. Ultimately, the study successfully recruited 471 participants.
2.3 Data collection
Data were collected through an online, self-administered questionnaire hosted on Google Forms. Participants were recruited through the support of the Scientific Research Committee at King Abdulaziz University. This committee distributed a formal email to all staff and students, which included the study objective and a link to the online questionnaire, inviting them to participate. Additionally, the email encouraged recipients to share the link with their social networks via platforms such as Twitter, Telegram, and WhatsApp. Upon accessing the survey, participants were presented with an informed consent page. Only those who consented were able to proceed to complete the questionnaire. Participant were also informed of the study’s objectives, the voluntary nature of their participation, and their right to withdraw at any time without consequences. Confidentiality was strictly maintained, and no personally identifiable information was collected. The data gathered were used exclusively for research purposes. The questionnaire was provided in Arabic, the native language of the participants, to ensure clarity and ease of understanding.
2.4 Instrument for data collection
A structured questionnaire was used in the study and was divided into three distinct sections:
Section 1—General Information: This segment gathered general details about the participants, such as their age, gender, marital status, educational background, region of residence, and monthly income in Saudi Riyals (SAR). It also included questions on height (m) and weight (kg) These anthropometric parameters were used to calculate the body mass index (kg/m2).
Section 2—Assessment of Nutrition Knowledge: One targeted question was included to evaluate participants knowledge related to the recommended daily intake (5 portions) of fruits and vegetables, as outlined by the Saudi Ministry of Health (46).
Section 3—Evaluation of Lifestyle Behaviors: This section explored participants’ overall lifestyle habits through a series of questions covering aspects such as physical activity levels, family meal-sharing practices, the description of their diet (healthy, balanced, calorie content), and their involvement in purchasing and preparing fruits and vegetables.
Section 4—TPB Constructs: The study was grounded in Ajzen’s conceptual framework for developing a TPB questionnaire (11, 47). The Target, Action, Context, and Time (TACT) strategy was employed to define the behavior under investigation, which was “consuming 5 servings of fruits and vegetables daily over the next week.” The TACT elements were determined in accordance with the recommendations of the Saudi Arabian Ministry of Health. Following the WHO guidelines, starchy roots such as potatoes and sweet potatoes were excluded from the vegetable category. Attitude was measured using four semantic differential scales. Participants were asked to rate statements such as, “Eating at least 5 servings of fruits and vegetables daily next week is very bad/bad/neutral /good/very good,” “Eating at least 5 servings of fruits and vegetables daily next week is not all pleasant/not pleasant/neutral/pleasant/very pleasant,” “Eating at least 5 servings of fruits and vegetables daily next week is very unhealthy/unhealthy/neutral/healthy/very healthy,” and “Eating at least 5 servings of fruits and vegetables daily next week is very difficult to digest/difficult to digest/neutral/easy to digest/very easy to digest.” Subjective Norms were assessed through two items: “My family expects me to eat 5 servings of fruits and vegetables per day next week” and “My friends expect me to eat 5 servings of fruits and vegetables per day next week.” PBC was measured using two items: “I think that eating 5 servings of fruits and vegetables daily next week is something possible” and “I am sure that I can eat 5 servings of fruits and vegetables per day next week.” Intention was evaluated using three items: “I intend to eat 5 servings of fruits and vegetables per day next week,” “I am sure to eat 5 servings of fruits and vegetables per day next week,” and “My aim is to eat 5 servings of fruits and vegetables per day next week.” Behavior was assessed by measuring the actual consumption of 5 servings of fruits and vegetables daily. Two questions were used: “How many servings of fruits and vegetables have you eaten daily in the last week?” and “How many times have you eaten 5 servings of fruits and vegetables daily in the last week?”
The items of the TPB were assessed using a 5-points Likert scale. Attitude toward the behavior was assessed with four differentials. Two measures of subjective norms were used and PBC was measured with two items. Three items were used to assess behavioral intention. Two items were employed to measure the behavior.
2.5 Validity
After finalizing the questionnaire, it was reviewed by a panel of 11 experts specializing in nutrition, public health, and psychology to assess its face validity, following the guidelines outlined by Mokkink et al. (41). Content validity aims to ensure that the questionnaire adequately covers the construct of interest and is conceptually appropriate. This process requires the input of subject-matter experts who can judge clarity, and comprehensiveness of each item based on theoretical and practical knowledge, and the estimated time required to complete the survey (32, 42). Hence, expert validation is considered the gold standard in assessing content validity. The results indicated that 88.9% of the experts considered the content comprehensive, 88.9% found the questions easy to understand, and the average completion time was 8.9 ± 1.4 min. Additionally, the experts were invited to provide feedback on the questionnaire’s usability, identifying any potential ambiguities in wording or content that might require refinement, in accordance with the recommendations of Janssens et al. (43). Their suggestions were incorporated to improve the instrument’s validity and user-friendliness.
Content validity was also evaluated alongside face validity. The Individual Content Validity Index (I-CVI) for each item ranged between 0.82 and 1, with a 97.1% agreement rate among experts. The Scale Content Validity Index (S-CVI)/Average was calculated at 93.3%, while the S-CVI/Universal Agreement stood at 77.4%. These metrics demonstrate the questionnaire’s strong content validity, confirming its effectiveness as a reliable measurement tool.
2.6 Internal consistency reliability
The reliability testing consisted in measuring the internal consistency by calculating the Cronbach’s alpha. It was performed on individuals who are representative of the actual study population. This is because the purpose is to assess how consistently the respondents interpret and respond to the items over time or within the same measurement, which would not be generalizable if only experts (who are not the target audience) were used (33, 44). The internal consistency of the scales (Cronbach’s alpha) suggests that the scales are reasonably homogenous.
2.7 Statistical analysis
All data analyses were conducted using the R software. Descriptive data were presented as mean ± standard deviation, % and frequencies. A structural equation modeling (SEM) approach was used to test the research hypotheses 1–4. The model fit was assessed with Chi-square (χ2), comparative fit index (CFI), the Tucker-Lewis Index (TLI), and root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR), and the coefficient of determination (R2) was used to measure the explained variance of the endogenous variables (intention and behavior). An adequate model fit is obtained when the CFI and TLI are >0.90 and the RMSEA and SRMR <0.08. The models were estimated using the Maximum Likelihood estimator. To test hypothesis 5, extension of the model was performed by including the lifestyle behaviors, knowledge, sociodemographic factors, in addition to the TPB construct. A bivariate Pearson test were also conducted in a separate analysis than SEM to assess the correlation of the studied parameters. Significance was set at a p-value <0.05.
3 Results
3.1 Descriptive analysis
The sociodemographic characteristics and lifestyle habits of a studied population are summarized in Table 1. The average age of participants is 34.53 ± 13.86 years, with a majority being female (74.58%). Most participants fall within the normal BMI range (43.56% with BMI 18.5–24.9), though a significant portion are overweight (25.95%) or obese (23.11%). Over half of the population was not married (53.18%), and the majority had a bachelor’s degree or higher (88.99%). Geographically, most participants originated from the Western region (62.50%). Income levels were relatively evenly distributed, with the largest group earning 11,000–20,000 monthly (34.32%).

Table 1. Sociodemographic characteristics of the studied population.
Regarding dietary habits, 38.77% of participants had moderate knowledge of WHO dietary recommendations, and nearly half reported having family meals daily (46.19%). A significant portion frequently purchased (62.29% often/always) and prepared (52.12% often/always) fruits and vegetables. Dietary intake was described as moderately healthy (44.70% middle, 33.69% healthy) and balanced (32.20% middle, 39.62% balanced), with calorie intake mostly moderate (45.76%). Physical activity levels were generally low, with 60.48% never engaging in intense activity and 34.32% never engaging in moderate activity. Light physical activity was more common, though 30.30% still report never participating. Overall, the findings indicate moderate awareness of fruit and vegetable consumption but low levels of physical activity.
Table 2 presents the reliability (Cronbach’s alpha), mean scores, and standard deviations for various constructs related to the consumption of five servings of vegetables and fruits per day. The Cronbach’s alpha values indicate good to excellent internal consistency for all constructs, ranging from 0.72 (Behavior) to 0.92 (Intention). Participants generally held positive attitudes toward consuming five servings of vegetables and fruits daily, with the highest mean score for the item “healthy” (4.35 ± 0.79). Subjective norms showed moderate agreement, with family expectations (3.50 ± 1.08) slightly higher than friends’ expectations (3.25 ± 1.05). PBC was also moderately high, with participants expressing confidence in their ability to consume the recommended servings (3.68 ± 0.94). Intentions to consume five servings were moderately strong, with mean scores ranging from 3.25 ± 1.09 to 3.56 ± 1.06. In terms of actual behavior, participants reported consuming an average of 3.27 ± 0.93 servings daily in the past week, with a frequency of consumption averaging 2.42 ± 1.23.
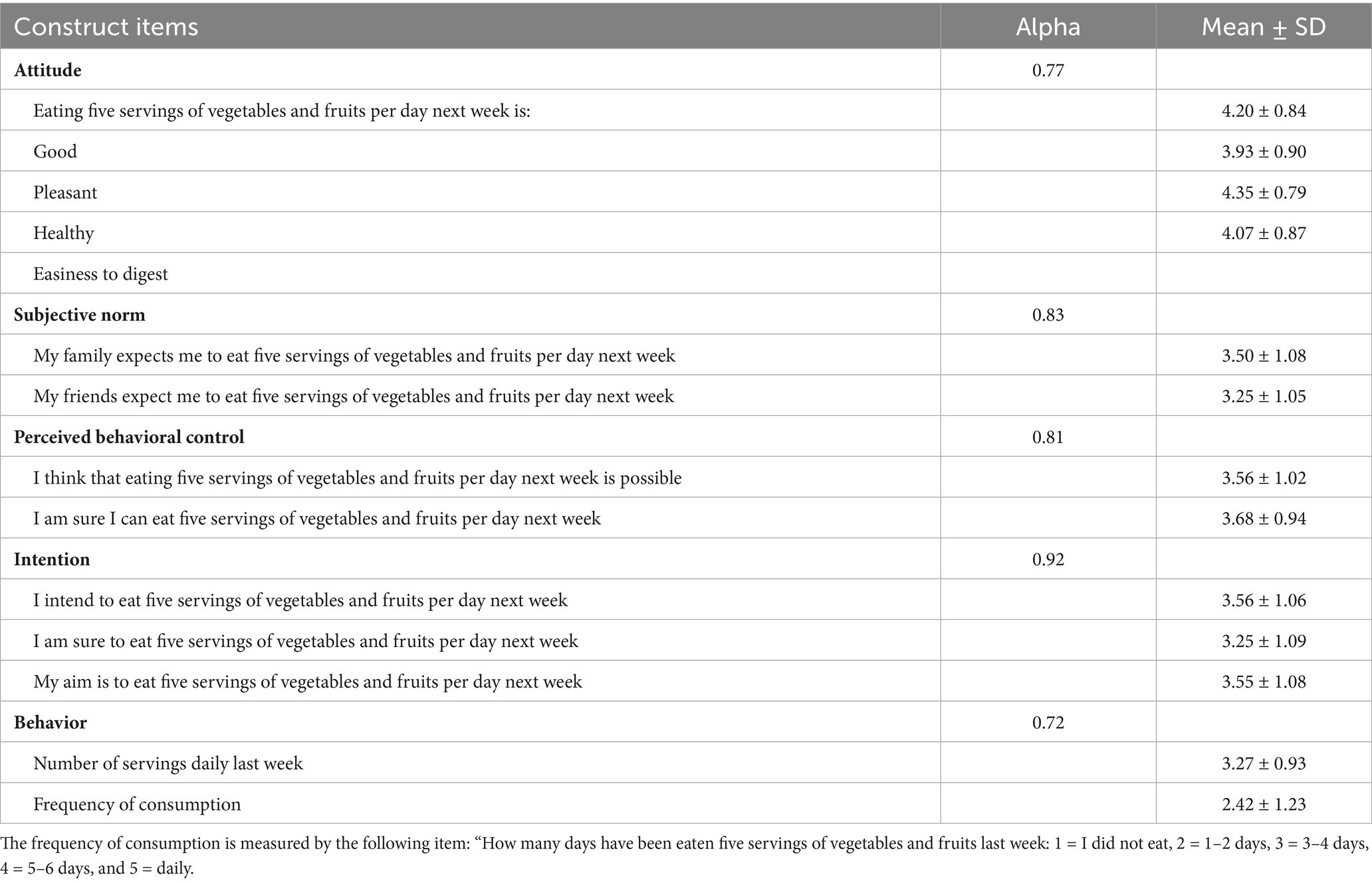
Table 2. Constructs Cronbach’s alpha, mean scores, and standard deviations.
3.2 Predicting fruits and vegetables consumption
Table 3 presents the results of the TPB model, including unstandardized coefficients (coeff), standard errors (se), standardized coefficients (std), and p-values for predicting behavior and intention. The model explains 40% of the variance in behavior and 74% of the variance in intention. For behavior, both intention (coeff = 0.16, se = 0.06, p = 0.012) and PBC (coeff = 0.54, se = 0.14, p = 0.000) are significant predictors. PBC is a strong predictor of behavior compared to intention. For intention, attitude (coeff = 0.29, se = 0.13, p = 0.025), subjective norm (coeff = 0.37, se = 0.11, p = 0.001), and PBC (coeff = 1.29, se = 0.17, p = 0.000) are all significant predictors. PBC is the strongest predictor of intention, followed by subjective norm and attitude. The covariances and correlations among the constructs are also significant. All these parameters of the construct are positively correlated and interrelated. The model fit measures indicate a good fit: χ2 (78) = 2,597.468; CFI = 0.969; TLI = 0.958; RMSEA (95% CI) = 0.054 (0.043–0.064); SRMR = 0.042. These values suggest that the TPB model is well-suited to explain the relationships between the constructs and the observed behavior and intention.
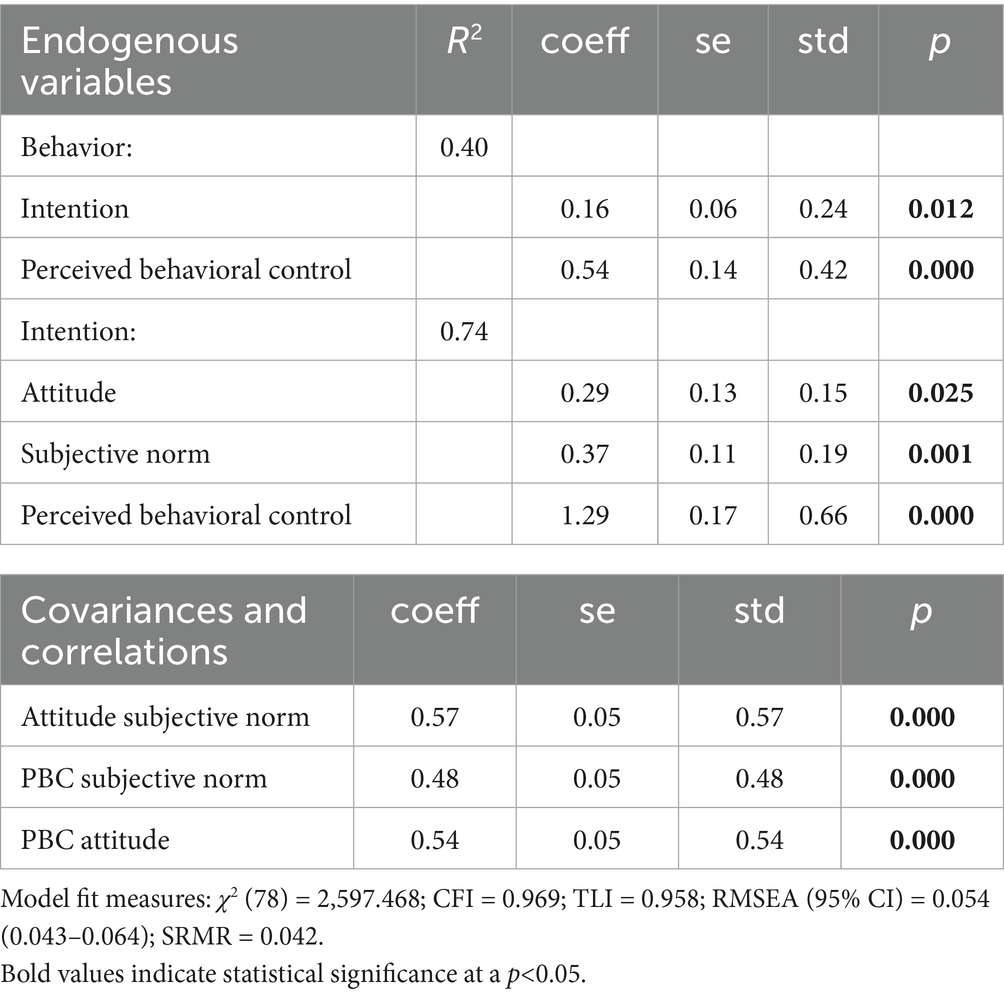
Table 3. TPB model unstandardized coefficients (coeff), standard error (se), standardized coefficients (std), and p-values.
Table 4 shows the findings of the extended TPB model, which integrates additional predictors such as sociodemographic variables, dietary habits, and physical activity levels. The model accounts for 78% of the variance in intention, 45% in behavior, 21% in attitudes, 12% in subjective norms, and 24% in PBC. The model demonstrates a good fit, as indicated by the following measures: χ2 (237) = 430.966; CFI = 0.955; TLI = 0.912; RMSEA (95% CI) = 0.045 (0.039–0.052); SRMR = 0.042.
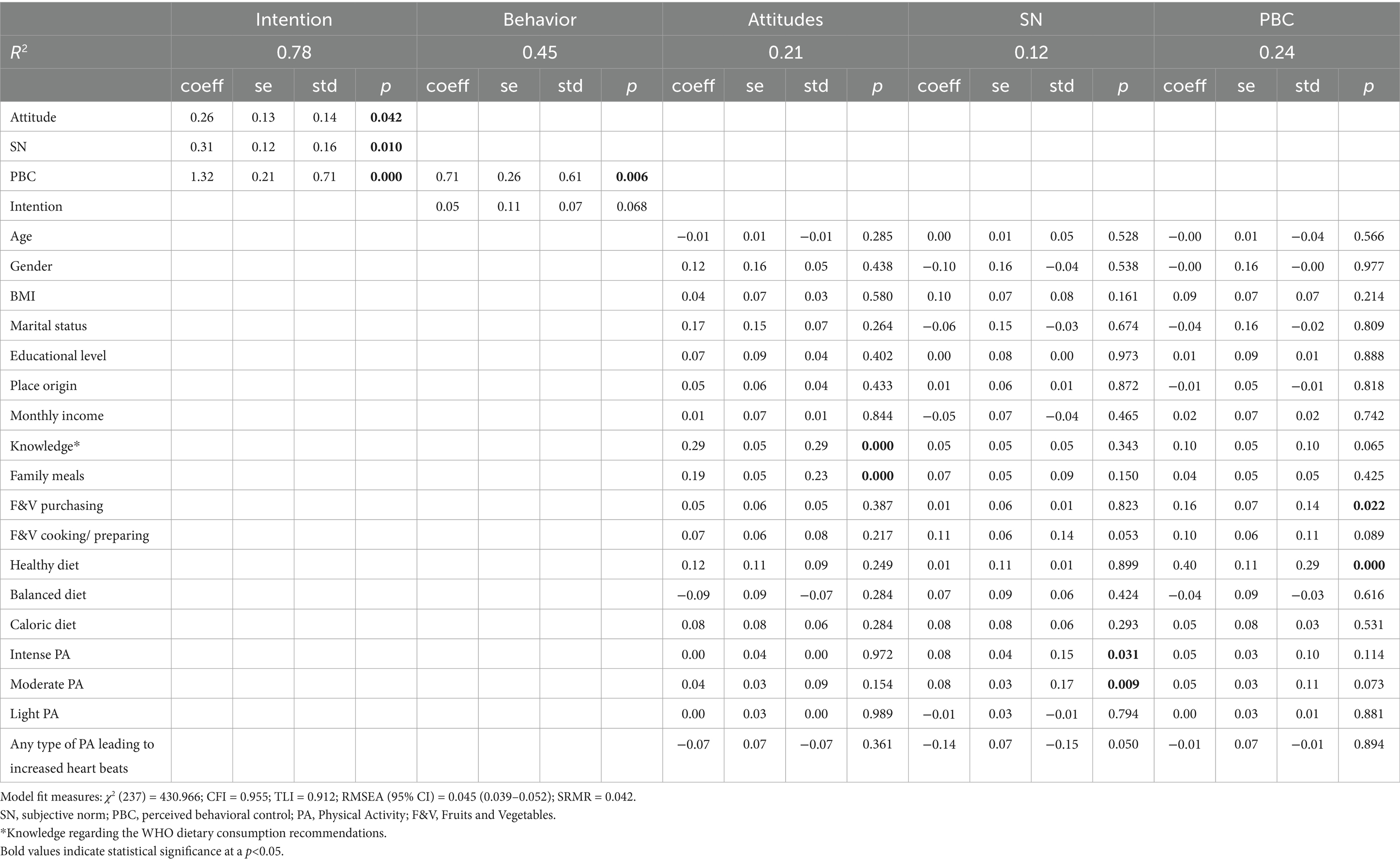
Table 4. TPB-extended model unstandardized coefficients (coeff), standard error (se), standardized coefficients (std), and p-values.
The results indicated that intention is significantly predicted by attitude (coeff = 0.26, se = 0.13, p = 0.042), subjective norm (coeff = 0.31, se = 0.12, p = 0.010), and PBC (coeff = 1.32, se = 0.21, p = 0.000). Among these, PBC was the strongest predictor, followed by subjective norm and attitude. Notably, none of the sociodemographic variables significantly predict intention. For behavior, it is significantly predicted by PBC (coeff = 0.71, se = 0.26, p = 0.006). Attitudes toward fruits and vegetables consumption are significantly predicted by knowledge of WHO dietary recommendations (coeff = 0.29, se = 0.05, p = 0.000) and family meals (coeff = 0.19, se = 0.05, p = 0.000). Subjective norms are not significantly predicted by most sociodemographic or behavioral factors, except for intense physical activity (coeff = 0.08, se = 0.04, p = 0.031) and moderate physical activity (coeff = 0.08, se = 0.03, p = 0.009). In terms of PCB, this construct is significantly predicted by fruits and vegetables purchasing habits (coeff = 0.16, se = 0.07, p = 0.022) and perceptions of healthy dietary intake (coeff = 0.40, se = 0.11, p = 0.000). Main results are presented in Figure 1.
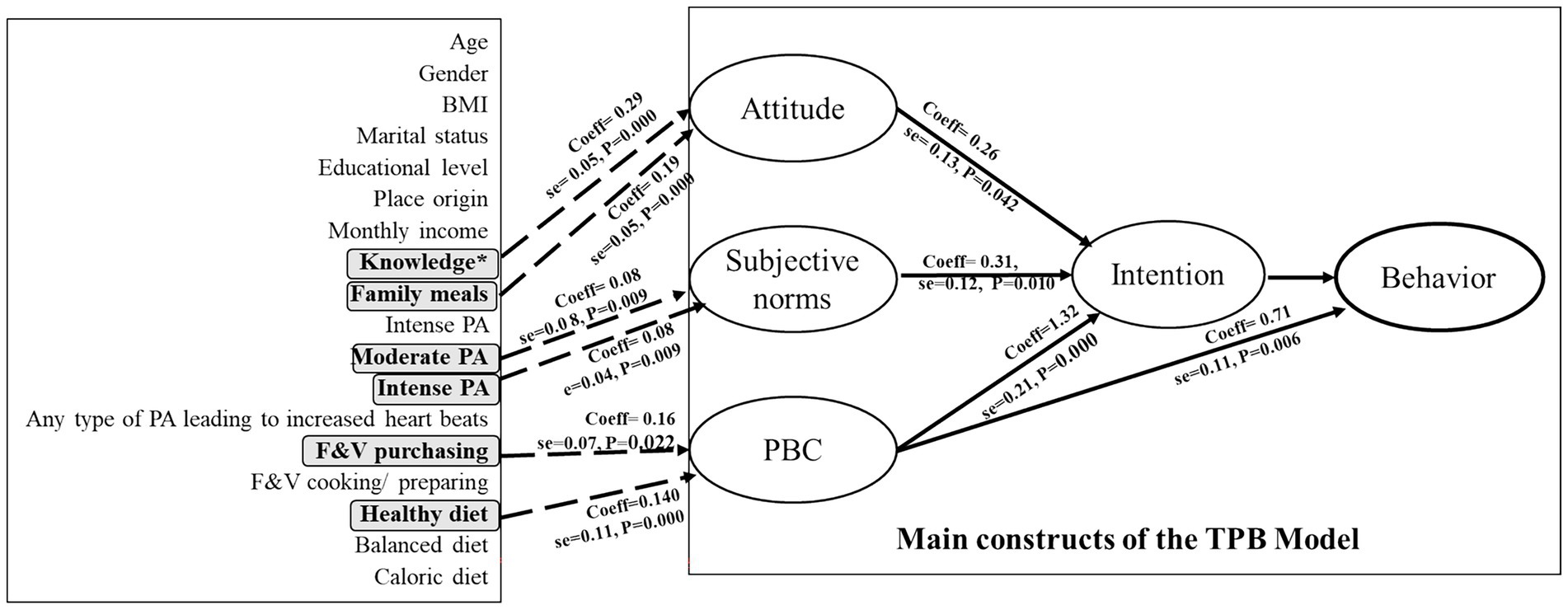
Figure 1. TPB-extended model and significant predictions. BMI, Body mass index; PA, Physical Activity; F&V, Fruits and Vegetables; *knowledge regarding the WHO dietary consumption recommendations.
Table 5 highlights the interrelationships between sociodemographic variables, behavioral factors, and TPB constructs. Main findings indicate that among the TPB constructs, attitude is positively correlated with subjective norms (cov = 0.53, se = 0.05 corr = 0.48) and PBC (cov = 0.51, se = 0.06 corr = 0.48). Subjective norms is also positively correlated with PBC (cov = 0.41, se = 0.07, corr = 0.40), suggesting that social expectations and perceived control are interrelated. Knowledge regarding WHO dietary recommendations is positively correlated with family meals (covariance = 0.15, se = 0.05, correlation = 0.15) and fruits and vegetables purchasing (covariance = 0.18, se = 0.05, correlation = 0.18). In addition, family meals are positively correlated with fruits and vegetables purchasing (covariance = 0.23, se = 0.05, correlation = 0.24) and fruits and vegetables cooking/preparing (covariance = 0.25, se = 0.05, correlation = 0.27). Fruits and vegetables purchasing shows strong correlations with fruits and vegetables cooking/preparing (covariance = 0.29, se = 0.05, correlation = 0.30) and dietary intake (healthy wise) (covariance = 0.44, se = 0.04, correlation = 0.43). These findings highlight the role of family eating habits in promoting the consumption of fruits and vegetables.
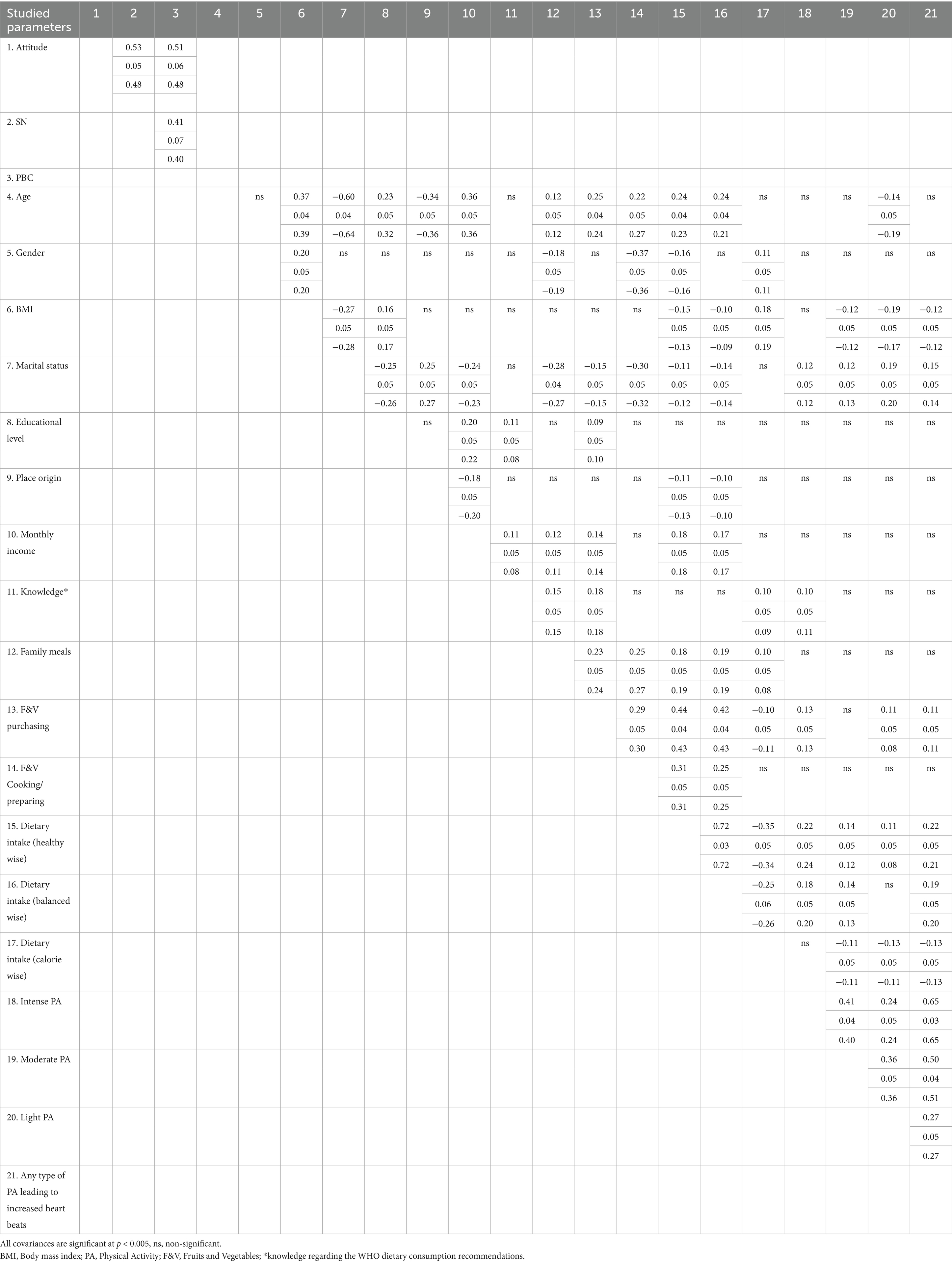
Table 5. TPB-extended model, covariances, standard error, correlations.
Healthy diet is strongly correlated with balanced (covariance = 0.72, se = 0.03, correlation = 0.72), suggesting that individuals who perceive their diet as healthy also perceive it as balanced. Intense physical activity is positively correlated with moderate physical activity (covariance = 0.41, se = 0.04, correlation = 0.40) and light physical activity (covariance = 0.24, se = 0.05, correlation = 0.24). Moderate physical activity is strongly correlated with light physical activity (covariance = 0.36, se = 0.05, correlation = 0.36) and any type of physical activity leading to increased heartbeats (covariance = 0.50, se = 0.04, correlation = 0.51). These correlations suggest a consistent pattern of physical activity across different intensity levels, reflecting a holistic approach to maintaining an active lifestyle.
4 Discussion
The objective of this study is to conduct a comprehensive analysis of fruit and vegetable consumption among Saudi adults using the extended TPB. The findings provide critical insights into the determinants of dietary behavior in this population, emphasizing the roles of attitudes, SN, PBC, and additional behavioral and sociodemographic factors. The results confirm earlier findings indicating low levels of fruit and vegetable intake among Saudi adults (24, 26) and further highlight that both the average daily servings and the frequency of meeting the recommended five servings per day remain significantly inadequate. Overall, the results suggest that while participants hold positive attitudes, moderate perceived control, and intentions to consume fruits and vegetables, their actual consumption falls short of the recommended daily intake.
In line with the TPB framework, PBC emerged as the strongest predictor of both intention and behavior, followed by subjective norms and attitudes. This indicates that individuals’ beliefs about their capability, social expectations, and personal attitudes collectively shape their intentions to consume fruits and vegetables. These findings align with previous research, which highlights the central role of PBC in health-related behaviors, including dietary choices (11, 34). For example, studies in other populations have also identified PBC as the most significant predictor of fruit and vegetable consumption, while subjective norms and attitudes had a weaker direct impact on behavior (35, 36) (Kothe et al., 2012).
The comparison of R2 values between the basic TPB model (Table 3) and the TPB-extended model (Table 4) reveals important insights into the determinants of fruit and vegetable consumption among Saudi adults. The TPB-extended model explains slightly more variance in behavior (R2 = 0.45) compared to the basic TPB model (R2 = 0.40), indicating that the inclusion of additional predictors—such as sociodemographic factors, knowledge about WHO dietary recommendations, family meals, and physical activity—enhances the model’s ability to explain dietary behavior. However, the modest improvement suggests that while these factors contribute, the core TPB constructs (intention and PBC) remain the primary drivers of behavior (11, 34). Similarly, the extended model explains slightly more variance in intention (R2 = 0.78) compared to the basic model (R2 = 0.74), with knowledge and family meals strengthening the predictive power by influencing attitudes and subjective norms (18, 20). The extended model also provides insights into the variance explained for attitudes (R2 = 0.21), subjective norms (R2 = 0.12), and PBC (R2 = 0.24). These relatively low values suggest that these constructs are predicted by factors not fully captured in the model, such as cultural or contextual elements specific to Saudi Arabia (26, 28). For example, family influence and social norms may play a significant role in shaping dietary habits but are not explicitly accounted for in the current model. The enhanced explanatory power of the extended model is evident in the significant role of key predictors. Knowledge about WHO dietary recommendations strongly predicted attitudes (coeff = 0.29, se = 0.05, p < 0.001), highlighting the importance of education in shaping dietary intentions (37). Family meals were a significant predictor of attitudes (coeff = 0.19, se = 0.05, p < 0.001), emphasizing the role of family dynamics in promoting healthy eating (20). Additionally, moderate physical activity was associated with subjective norms (coeff = 0.08, se = 0.03, p = 0.009), suggesting a synergistic relationship between physical activity and dietary behavior (17).
In contrast, sociodemographic variables (e.g., age, gender, income) had minimal direct predictive effect behavior or intention, as reflected in their non-significant p-values. This suggests that dietary habits in Saudi Arabia may be more strongly determined by psychological and behavioral factors than by sociodemographic characteristics (16). The relatively low R2 values for subjective norms and attitudes further highlight the need to explore cultural and contextual factors, such as family influence and accessibility of fruits and vegetables, to enhance the model’s explanatory power (26).
From a practical perspective, the higher R2 for behavior in the extended model underscores the importance of addressing both psychological (e.g., PBC, intention) and practical factors (e.g., knowledge, family meals, physical activity) in interventions aimed at promoting fruit and vegetable consumption. The strong predictive effect of PBC (coeff = 0.71, se = 0.26, p = 0.006) on behavior highlights the need to enhance individuals’ confidence in their ability to consume fruits and vegetables, such as through cooking classes or meal planning workshops (38). Additionally, the significant role of family meals suggests that interventions should engage families and promote shared meals as a strategy to improve dietary habits (20).
The study found that physical activity levels, particularly intense and moderate activity, were positively associated with healthier dietary attitudes and behaviors. This aligns with research demonstrating a synergistic relationship between physical activity and healthy eating. For example, a study in Canada found that individuals who engaged in regular physical activity were more likely to consume fruits and vegetables (17). These findings suggest that interventions promoting both physical activity and healthy eating may be more effective than those targeting diet alone, as they address multiple health behaviors simultaneously.
This study has several strengths, including the use of an extended TPB model to explore a wide range of predictors and the inclusion of respondents from the different age groups and regions of Saudi Arabia. However, there are also limitations. The cross-sectional design limits the ability to establish causal relationships, and self-reported data may be subject to bias. Future research should consider longitudinal designs and objective measures of the reported parameters.
5 Conclusion
This study provides valuable insights into the factors influencing vegetable and fruit consumption among Saudi adults. Utilizing an extended TPB model, the findings highlight the importance of PBC, knowledge, family habits, and physical activity in shaping dietary behavior. Interventions that address these factors while considering sociodemographic contexts are likely to be most effective in promoting healthy eating habits in this population. By fostering a supportive environment and empowering individuals with the skills and confidence to make healthier choices, public health initiatives can contribute to reducing the burden of diet-related diseases in Saudi Arabia. Despite its strengths—including a diverse sample and comprehensive theoretical framework—this study has some limitations. The cross-sectional design restricts the ability to infer causality, and reliance on self-reported data may introduce response bias. Future research should employ longitudinal designs and incorporate objective measures of dietary intake and related behaviors to validate and expand upon these findings. Addressing these limitations will help refine strategies aimed at reducing the burden of diet-related diseases in Saudi Arabia and beyond.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, under reasonable request.
Ethics statement
Ethical approval for the study was granted by the Institutional Review Board (IRB) of King Abdulaziz University (IRB Log number 15-24). Informed consent was obtained online from all participants, who confirmed their agreement to participate by clicking ‘I accept to participate in the study’ before accessing the questionnaire.
Author contributions
EA: Methodology, Project administration, Investigation, Writing – original draft, Conceptualization, Resources. BA: Data curation, Methodology, Investigation, Resources, Supervision, Writing – review & editing, HaA: Supervision, Conceptualization, Writing – original draft, Investigation, Validation, Data curation. Project administration, Conceptualization. HoA: Writing – review & editing, Software, Writing – original draft, Conceptualization, Supervision, Funding acquisition, Project administration, Methodology.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Authors would like to acknowledge Princess Nourah Bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R804), Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia for funding this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Boeing, H, Bechthold, A, Bub, A, Ellinger, S, Haller, D, Kroke, A, et al. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr. (2012) 51:637–63. doi: 10.1007/s00394-012-0380-y
2. World Health Organization. Healthy diet. (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/healthy-diet (Accessed January 15, 2024).
3. Aune, D, Giovannucci, E, Boffetta, P, Fadnes, LT, Keum, N, Norat, T, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. (2017) 46:1029–56. doi: 10.1093/ije/dyw319
4. Nicklett, EJ, and Kadell, AR. Fruit and vegetable intake among older adults: a scoping review. Maturitas. (2013) 75:305–12. doi: 10.1016/j.maturitas.2013.05.005
5. Lakshmanan, AP, Mingione, A, Pivari, F, Dogliotti, E, Brasacchio, C, Murugesan, S, et al. Modulation of gut microbiota: the effects of a fruits and vegetables supplement. Front Nutr. (2022) 9:930883. doi: 10.3389/fnut.2022.930883
6. FAO/WHO. Fruit and vegetables for health: Report of a joint FAO/WHO workshop. World Health Organization. (2004). Available online at: https://www.who.int/publications/i/item/9241592818 (Accessed January 15, 2024).
7. Naska, A, Vasdekis, VGS, and Trichopoulou, A. Fruit and vegetable availability among ten European countries: how does it compare with the ‘five-a-day’ recommendation? Br J Nutr. (2000) 84:549–56. doi: 10.1017/S0007114500001931
8. Fanzo, J, Haddad, L, Schneider, KR, Béné, C, Covic, NM, Guarin, A, et al. Rigorous monitoring is necessary to guide food system transformation in the countdown to the 2030 global goals. Food Policy. (2021) 104:102163. doi: 10.1016/j.foodpol.2021.102163
9. Livingstone, KM, Rawstorn, JC, Partridge, SR, Godrich, SL, McNaughton, SA, Hendrie, GA, et al. Digital behaviour change interventions to increase vegetable intake in adults: a systematic review. Int J Behav Nutr Phys Act. (2023) 20:36. doi: 10.1186/s12966-023-01439-9
10. Dogbe, W, Akaichi, F, Rungapamestry, V, and Revoredo-Giha, C. Effectiveness of implemented global dietary interventions: a scoping review of fiscal policies. BMC Public Health. (2024) 24:2552. doi: 10.1186/s12889-024-19988-4
11. Ajzen, I. The theory of planned behavior. Organ Behav Hum Decis Process. (1991) 50:179–211. doi: 10.1016/0749-5978(91)90020-T
12. Sjoberg, S, Kim, K, and Reicks, M. Applying the theory of planned behavior to fruit and vegetable consumption by older adults. J Nutr Educ Behav. (2004) 36:304–11. doi: 10.1300/J052v23n04_03
13. Solhi, M, and Shirzad, M. Situation of fruits and vegetables consumption in the dormitory female students based on the theory of planned behavior. J. Health Lit. (2016) 1:129–136. doi: 10.22038/jhl.2016.10973
14. McDermott, MS, Oliver, M, Simnadis, T, Beck, EJ, Coltman, T, Iverson, D, et al. The theory of planned behaviour and dietary patterns: a systematic review and meta-analysis. Prev Med. (2015) 81:150–6. doi: 10.1016/j.ypmed.2015.08.020
15. Scalco, A, Noventa, S, Sartori, R, and Ceschi, A. Predicting organic food consumption: a meta-analytic structural equation model based on the theory of planned behavior. Appetite. (2017) 112:235–48. doi: 10.1016/j.appet.2017.02.007
16. Darmon, N, and Drewnowski, A. Does social class predict diet quality? Am J Clin Nutr. (2008) 87:1107–17. doi: 10.1093/ajcn/87.5.1107
17. Larson, NI, Story, MT, and Nelson, MC. Neighborhood environments: disparities in access to healthy foods in the U.S. Am J Prev Med. (2006) 36:74–81. doi: 10.1016/j.amepre.2008.09.025
18. Spronk, I, Kullen, C, Burdon, C, and O'Connor, H. Relationship between nutrition knowledge and dietary intake. Br J Nutr. (2014) 111:1713–26. doi: 10.1017/S0007114514000087
19. Yee, AZ, Lwin, MO, and Ho, SS. The influence of parental practices on child promotive and preventive food consumption behaviors: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. (2017) 14:1–14. doi: 10.1186/s12966-017-0501-3
20. Videon, TM, and Manning, CK. Influences on adolescent eating patterns: the importance of family meals. J Adolesc Health. (2003) 32:365–73. doi: 10.1016/S1054-139X(02)00711-5
21. DeNicola, E, Aburizaiza, OS, Siddique, A, Khwaja, H, and Carpenter, DO. Obesity and public health in the Kingdom of Saudi Arabia. Rev Environ Health. (2015) 30:191–205. doi: 10.1515/reveh-2015-0008
22. Elgaili, EO, Mohamed, AM, and Abdullah, ASH. Food transition in the Gulf cooperation council region. Afr J Agric Res. (2020) 15:297–311. doi: 10.5897/AJAR2019.14592
23. El Bcheraoui, C, Basulaiman, M, AlMazroa, MA, Tuffaha, M, Daoud, F, Wilson, S, et al. Fruit and vegetable consumption among adults in Saudi Arabia, 2013. Nutr Diet Suppl. (2015):41–9. doi: 10.2147/NDS.S77460
24. Albrahim, T, Alotaibi, N, Alharbi, M, Alrasheedi, KR, Aldosari, HA, and Albarqi, HM. Exploring the association between nutritional knowledge and fruit and vegetable consumption among young adults: a cross-sectional study. Curr. Res. Nutr. Food Sci. (2023) 11:617–626. doi: 10.12944/CRNFSJ.11.2.13
25. Al Otaibi, HH. Measuring self-efficacy and barriers to healthy eating among Saudi adolescents. J Family Community Med. (2014) 21:165–70. doi: 10.4103/2230-8229.142972
26. Al-Otaibi, HH. The pattern of fruit and vegetable consumption among Saudi university students. J. Health Sci. (2013) 6:155. doi: 10.5539/gjhs.v6n2p155
27. Alsunni, AA, and Badar, A. Fruit and vegetable consumption and its determinants among Saudi university students. J. Taibah Univ. Med. Sci. (2015) 10:201–207. doi: 10.1016/j.jtumed.2014.11.003
28. Hala Hazam, AO. Psychosocial factors associated with fruit and vegetable consumption among Saudi University Students. J Fud Nutr. (2014) 1:1–10.
29. Shlisky, J, Bloom, DE, Beaudreault, AR, Tucker, KL, Keller, HH, Freund-Levi, Y, et al. Nutritional considerations for healthy aging and reduction in age-related chronic disease. Adv Nutr. (2017) 8:17–26. doi: 10.3945/an.116.013474
30. Raats, MM, de Groot, LCPGM, and van Asselt, D. Food for the ageing population. UK: Woodhead Publishing (2011).
31. Lwanga, S. K., and Lemeshow, S. Sample size determination in health studies: a practical manual. World Health Organization. (1991). Available online at: https://apps.who.int/iris/handle/10665/40062 (Accessed January 15, 2024).
32. Polit, DF, and Beck, CT. The content validity index: are you sure you know what's being reported? Critique and recommendations. Res Nurs Health. (2006) 29:489–97. doi: 10.1002/nur.20147
33. Boateng, GO, Neilands, TB, Frongillo, EA, Melgar-Quiñonez, HR, and Young, SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. (2018) 6:149. doi: 10.3389/fpubh.2018.00149
34. Armitage, CJ, and Conner, M. Efficacy of the theory of planned behaviour: a meta-analytic review. Br J Soc Psychol. (2001) 40:471–99. doi: 10.1348/014466601164939
35. Menozzi, D, Sogari, G, and Mora, C. Explaining vegetable consumption among young adults: an application of the theory of planned behaviour. Nutrients. (2015) 7:7633–50. doi: 10.3390/nu7095357
36. Pawlak, R, and Malinauskas, B. Predictors of intention to eat 2.5 cups of vegetables among ninth-grade students attending public high schools in eastern North Carolina. J Nutr Educ Behav. (2008) 40, 392–398. doi: 10.1016/j.jneb.2007.11.002
37. Wardle, J, Parmenter, K, and Waller, J. Nutrition knowledge and food intake. Appetite. (2000) 34:269–75. doi: 10.1006/appe.1999.0311
38. Reicks, M, Trofholz, AC, Stang, JS, and Laska, MN. Impact of cooking and home food preparation interventions among adults: outcomes and implications for future programs. J Nutr Educ Behav. (2014) 46:259–76. doi: 10.1016/j.jneb.2014.02.001
39. Kothe, EJ, and Mullan, BA. A randomised controlled trial of a theory of planned behaviour to increase fruit and vegetable consumption. Appetite. (2014) 78:68–75. doi: 10.1016/j.appet.2014.03.010
40. WHO. Healthy diet recommendations. Available online at: https://www.who.int/health-topics/healthy-diet#tab=tab_2 (Accessed April 18, 2025).
41. Mokkink, LB, Terwee, CB, Patrick, DL, Alonso, J, Stratford, PW, Knol, DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J. Clin. Epidemiol. (2010) 63:737–745. doi: 10.1016/j.jclinepi.2010.02.006
42. Ehrenbrusthoff, K, Ryan, CG, Grüneberg, C, Wand, BM, and Martin, DJ. The translation, validity and reliability of the German version of the Fremantle Back Awareness Questionnaire. PLoS One, (2018) 13:e0205244. doi: 10.1371/journal.pone.0205244
43. Janssens, L, Goossens, N, Wand, BM, Pijnenburg, M, Thys, T, and Brumagne, S. The development of the Dutch version of the Fremantle Back Awareness Questionnaire. Musculoskelet Sci Pract. (2017) 32, 84–91. doi: 10.1016/j.msksp.2017.09.003
45. Census The Saudi. Available at: https://portal.saudicensus.sa/portal (Accessed 27 November, 2023).
46. Ministry of Health, Saudi Arabia. Healthy eating habits. Awareness platform: healthy lifestyle (in Arabic). (n.d.). Available at: https://www.moh.gov.sa/awarenessplateform/HealthyLifestyle/Pages/HealthyEatingHabits.aspx (Accessed March 16, 2024).
47. Ajzen, I. Constructing a TPB questionnaire: conceptual and methodological considerations. (2002). Available at: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=0574b20bd58130dd5a961f1a2db10fd1fcbae95d (Accessed August 16, 2025)
Keywords: fruits and vegetables, consumption, Theory of Planned Behavior, Saudi Arabia, adults
Citation: Abduljawad EA, Aljehany BM, Aljadani H and Abusalih H (2025) Determinants of fruit and vegetable consumption among Saudi adults: an extended Theory of Planned Behavior approach. Front. Public Health. 13:1593625. doi: 10.3389/fpubh.2025.1593625
Edited by:
Haleama Al Sabbah, Abu Dhabi University, United Arab EmiratesReviewed by:
Archana Kumari, University of Delhi, IndiaRobert Akparibo, The University of Sheffield, United Kingdom
Copyright © 2025 Abduljawad, Aljehany, Aljadani and Abusalih. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haya Aljadani, aGhhbGphZGFuaUBrYXUuZWR1LnNh