 Waad Alfawaz
Waad Alfawaz Reem S. Albassam
Reem S. Albassam Noura Almuharib1
Noura Almuharib1- 1Department of Community Health Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia
- 2Department of Scientific Research, King Saud University, Riyadh, Saudi Arabia
Background: A balanced diet and active lifestyle are key factors influencing health and quality of life (QoL). This study examined the relationships between eating patterns, physical activity, and QoL among Arab healthcare professionals.
Methodology: A cross-sectional study included 353 healthcare workers in Riyadh, Saudi Arabia. Data were collected through face-to-face interviews, where participants were briefed on the study objectives and provided voluntary informed consent. The WHOQOL-BREF tool was used to evaluate QoL, while the Rapid Diet Quality Screener assessed dietary habits. The Global Physical Activity Questionnaire was used to measure physical activity. Statistical analysis included independent samples t-tests, one-way ANOVA, and Pearson correlation.
Results: Among participants, 47.6% had a normal weight, 44.7% were overweight or obese, and 7.6% were underweight. While those with normal weight had the highest QoL scores across all domains, differences across BMI categories were not statistically significant. Regular physical activity was linked to high QoL, particularly in social relationships (p = 0.037). Participants who exercised regularly also reported healthier eating habits (p < 0.001). Weak but significant positive correlations were found between diet quality and QoL, particularly physical health (r = 0.219, p < 0.001) and psychological health (r = 0.184, p = 0.002). No significant diet quality differences were found between genders (p = 0.677).
Conclusion: Healthcare professionals who exercise regularly exhibit a better QoL, especially in social relationships, and maintain healthier eating habits. While normal BMI was associated with improved QoL, differences across BMI categories were not statistically significant. These findings highlight the need for interventions promoting physical activity and healthy eating to enhance QoL in healthcare workers.
1 Introduction
A balanced diet has long been recognized as a key factor in maintaining good health and an overall quality of life (QoL) (1). Physical inactivity and unhealthy eating behaviors contribute significantly to economic burdens, including lost productivity at work. When healthcare workers are affected, it can indirectly impact the efficiency of the healthcare sector (2).
Several studies have assessed the healthy lifestyle and cardiometabolic risk among healthcare staff and found that the majority adhere to unhealthy diets and engage in low levels of physical activity (2, 3). A study from United Kingdom evaluated the incidence of cardiovascular risk factors and adherence to dietary and physical activity recommendations among National Health Service staff (2). It reported that half of the participants were overweight or obese, with low compliance with dietary and physical activity guidelines (2). Another study from South Africa indicated that nurses are at a higher risk of non-communicable diseases, with a high prevalence of poor dietary habits, obesity, and insufficient physical activity (3). Sharma et al. (4) conducted a study in India examining the prevalence of risk factors for lifestyle diseases among healthcare professionals. The study reported that the prevalence of diabetes and hypertension in this population was 5 and 10%, respectively, both of which are associated with lifestyle and dietary factors (4). A study conducted in Saudi Arabia revealed that a significant proportion of healthcare professionals across various specialties and practice settings exhibit unhealthy dietary behaviors both in the workplace and in their personal lives. These behaviors are characterized by excessive consumption of sweets and coffee, along with frequent episodes of binge eating. The study identified key contributing factors, including demanding workloads, insufficient break times, and limited availability of nutritious food options within hospital environments (5). A cohort study comprised 11,128 individuals from a cohort known as “Seguimiento Universidad de Navarra” (SUN). Dietary practices were evaluated using a validated food frequency questionnaire. QoL was measured using the validated Spanish version of the SF-36 Health Survey. This study aimed to determine the relationship between dietary habits and emotional and physical quality of life, following a 4-year follow-up period. The researchers found that after 4 years of follow-up, baseline adherence to a Mediterranean dietary pattern was directly associated with higher QoL scores in the SUN Project, while baseline adherence to a Western dietary pattern was inversely associated with self-perceived QoL (6). Phiri et al. (3) observed that nurses who exercised regularly experienced lower stress levels, better physical health, and improved social interactions, all contributing to enhanced QoL. A recent study assessing the QoL among healthcare workers in the Arab world found that the majority reported suboptimal QoL scores across various domains, including physical, psychological, social, and environmental aspects. However, general QoL scores remained relatively satisfactory (7). A study in Saudi Arabia also reported poor QoL among healthcare professionals working in four primary cares centers (8). Doctors frequently neglect their physical and mental health and exhibit higher levels of anxiety, burnout, depression, and substance misuse than other occupational groups (9, 10).
Our research is pioneering in its examination of the interconnections between dietary habits, physical activity, and QoL among healthcare professionals in Saudi Arabia. This study provides region-specific insights and adds to the sparse body of research on Middle Eastern healthcare populations, where previously these factors were often investigated in isolation. By integrating nutrition, physical activity, and QoL within a single healthcare cohort, providing a holistic approach unlike to the previous regional research that often examines these factors separately. Analyzing these interconnected lifestyle dimensions offers a more comprehensive perspective of well-being. Workplace interventions to improve nutrition and quality of life, including work-related outcomes, are complex and challenging to implement owing to a lack of understanding (1). The association between diet and QoL among medical staff is a crucial area of study since healthcare professionals’ well-being directly influences their ability to provide effective patient care and educate medical students (2). However, the specific relationship between dietary choices, lifestyle factors and QoL among medical staff remains unclear. Understanding this relationship is essential for identifying potential interventions and strategies to enhance the well-being and work-life balance of medical professionals. Based on the findings of our study, targeted interventions, such as providing healthy food options in the workplace, promoting healthy eating habits, and implementing stress management programs, can be developed to improve dietary habits and QoL among medical staff. These efforts are expected to improve patient outcomes and increase the effectiveness of health care systems. The current study aimed to determine the association between diet quality and QoL among medical staff, taking their lifestyle into account.
2 Materials and methods
2.1 Study design
This cross-sectional study was conducted at the King Saud University Medical City (KSUMC), Riyadh, Saudi Arabia. A total of 353 healthcare professionals were included in the study. The sample size was determined using the Epi calculator and Raosoft software (11) with a 95% confidence level, resulting in a sample of 353 participants. Data were collected through face-to-face interviews, which provided participants with information on the study objectives and ensured their voluntary consent to participate. Ethical approval was obtained from the Institutional Review Board (IRB) of King Saud University (KSU-HE-24-091) to ensure adherence to ethical standards and safeguard the rights and well-being of the participants.
2.2 Assessment tools
The World Health Organization QoL Instrument (WHOQOL-BREF) was used to assess the QoL of study participants. The WHOQOL-BREF is a self-administered questionnaire comprising 26 items measuring four keys QoL domains defined by the World Health Organization: physical health, psychological health, social relationships, and environment. The scores were transformed into a linear scale from 0 to 100, where 0 represented the lowest QoL, and 100 represented the highest (12). The first two items independently assessed overall perceptions of QoL and general health. Each question is rated on a 5-point Likert scale, ranging from 1 (very poor/very dissatisfied/none/never) to 5 (very good/very satisfied/extremely/always), with scores across the four domains summed and positively scaled, indicating higher QoL with higher scores (13). Numerous studies have validated the reliability of the WHOQOL-BREF as a QoL assessment tool (14, 15). The Arabic version has also been tested and shown to be valid and highly reliable among Arabic-speaking populations (Cronbach’s alpha > 0.867) (12).
The Rapid Diet Quality Screener (RDQS) developed by Kotecki et al. (16) was used to evaluate diet quality. This tool begins with the question, “In a typical week, how often do you:” and is followed by 12 questions regarding the frequency of consumption of certain foods and beverages associated with either reducing or increasing chronic disease risk. Six questions addressed high-quality foods (e.g., minimally processed vegetables, fruits, whole grains, protein-rich foods, and healthy fats), whereas the remaining six assessed low-quality foods (e.g., processed items, those high in added sugars, saturated and trans fats, and sodium, such as desserts, sugary drinks, red meat, and alcohol). For each item, responses are categorized into three frequency columns: “never/rarely,” “sometimes,” and “often/always.” This three-level frequency system minimizes recall and calculation errors. Responses were scored by dietary healthfulness, with the healthiest behavior scored as 2, a moderately healthful behavior as 1, and the least healthful behavior as 0. The total score represents the overall diet quality, ranging from 0 to 24. Higher scores reflect healthier dietary habits, whereas lower scores indicate areas requiring improvement. The score is then categorized into five diet quality levels for easy interpretation, each represented by a specific color: 21–24 (excellent, green), 17–20 (very good, light green), 14–16 (good, yellow), 7–13 (fair, orange), and 0–6 (poor, red). Effective screening tools such as the RDQS are designed not to quantify exact food and nutrient intake but rather to classify diets as relatively high or low in specific dietary qualities (16).
The Global Physical Activity Questionnaire (GPAQ), developed by the World Health Organization, was used to assess participants’ physical activity levels. GPAQ evaluates physical activity through a series of structured questions organized into three domains: occupational (work-related), transportation (such as walking and cycling), and recreational (leisure-time activities). Each domain assesses the frequency of these activities during a typical week, as well as the duration spent on each activity per day. Activity intensity is classified as either moderate or vigorous, with assigned Metabolic Equivalent Task (MET) values of 4.0 for moderate activities and 8.0 for vigorous activities. The total physical activity for each participant was calculated by multiplying these MET values by the reported duration of each activity (minutes per week), providing a continuous indicator of weekly energy expenditure expressed in MET-minutes per week. Then, categorical indicators of physical activity (insufficiently active, sufficiently active) were established following WHO recommendations. Participants were classified as sufficiently active if they engaged in at least 150 min of moderate-intensity physical activity, 75 min of vigorous-intensity physical activity, or an equivalent combination achieving at least 600 MET-minutes per week (17).
2.3 Statistical analyses
The data were preprocessed prior to analysis, including data cleaning; the dataset was examined for missing values, outliers, and consistency, and only complete cases were included in the final analysis. Descriptive statistics were employed to summarize the demographic variables, including sex, BMI categories, income levels, living area, walking activity, and physical activity. Independent samples t-tests were conducted to evaluate differences in mean scores by sex and physical activity status, while one-way ANOVA was used to compare mean differences across BMI categories. Additionally, the Pearson correlation coefficient was calculated to determine the strength and direction of the relationships between QoL domains and diet quality. Furthermore, multiple linear regression analysis was conducted to identify significant predictors of each QoL domain, using diet quality, physical activity levels, and relevant demographic variables as independent factors. Statistical significance was set at a p-value of <0.05. All data analyses were performed using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY, United States).
3 Results
3.1 General characteristics of the study sample
The study participants consist of 353 healthcare professionals employed at King Saud University’s Medical City. Among the participants, 56.9% were male and 43.1% were female. Nearly half (47.6%) of the respondents maintained a normal weight (BMI 18.5–24.9), while over 44% were overweight or obese.
The majority (52.1%) of participants earned ≤10,000 Saudi Riyals (SR) monthly, with 33.2% earned 10,000–20,000 SR, and 14.7% earned >20,000 SR. Most resided in Central (37.4%) and North Riyadh (30.3%).
Regarding walking activity, 13.9% did not walk in the past week. Among walkers, the most common frequency was 5 days (19%). Overall, 65.2% sufficiently active, whereas 34.8% insufficiently active. Among those participants, 15.6% exercised for 5 days a week, 14.4% for 3 days, and only 3.4% exercised daily (Table 1).
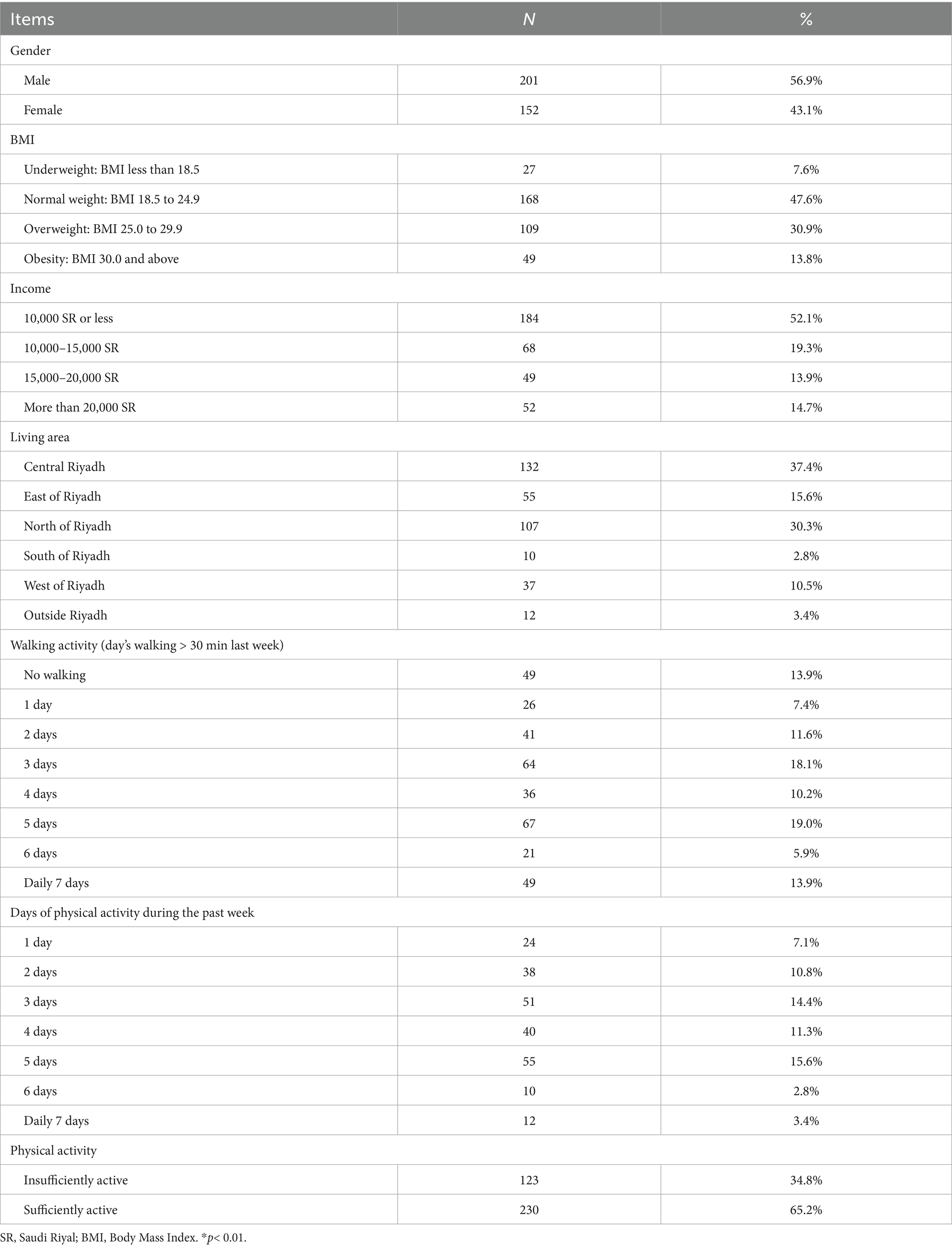
Table 1. Socio-demographic characteristics of the population (n = 353).
3.2 Quality of life and RDQS according to impact factors
Table 2 illustrates the influence of gender, physical activity, and BMI on QoL domains and diet quality. The gender-based analysis showed that males scored slightly higher across all QoL domains (physical health, psychological health, social relations, and environment), with a significant advantage in social relations (68.0 ± 22.7 vs. 63.6 ± 18.1, p = 0.049). Diet quality did not differ significantly between sexes (p = 0.677).
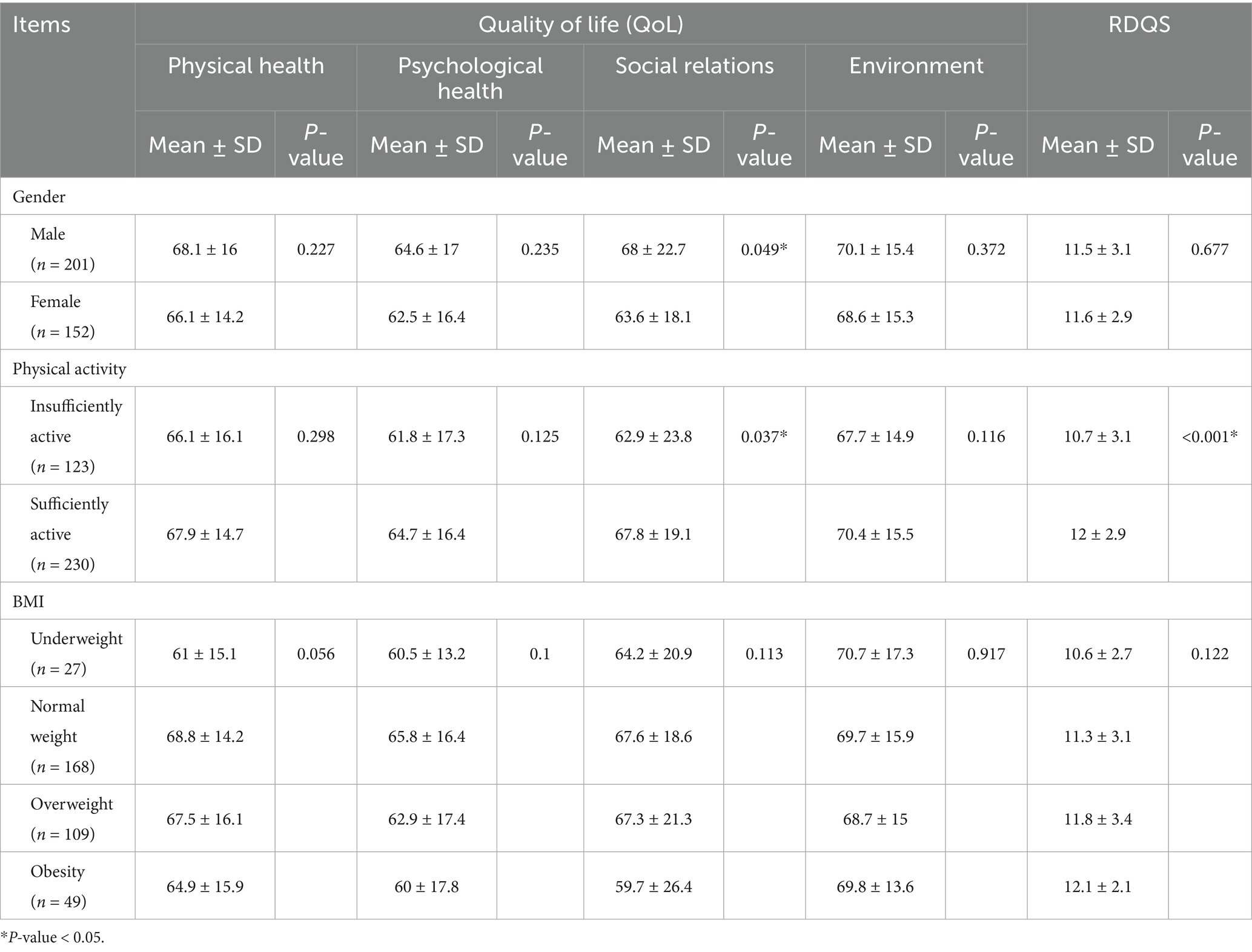
Table 2. QoL and RDQS according to impact factors (n = 353).
Physical activity was positively correlated with QoL. Participants engaged in physical activity had higher scores in all domains, with A significant impact on social relations (p = 0.037). Sufficiently active participants also had higher diet quality scores (p < 0.001), linking exercise to healthier eating habits.
BMI trends indicated higher QoL scores for those with normal weight, though differences were not statistically significant (p = 0.056–0.917).
For diet quality, obese participants had the highest diet quality scores (12.1 ± 2.1), while underweight individuals had the lowest (10.6 ± 2.7), but the difference was not significant (p = 0.122) (Table 2).
3.3 Association of diet quality, physical activity, and demographic variables with quality of life
The relationship between QoL domains and the diet quality (RDQS) scores is displayed in Table 3. All correlation coefficients were weak (r < 0.4), but significant positive associations were observed. Physical health correlated with RDQS (r = 0.219, p < 0.001), suggesting that better diet quality may enhanc the physical well-being of this population. Psychological health also showed a positive correlation (r = 0.184, p = 0.002), supporting the inclusion of dietary improvements as a part of broader mental health strategies. Social relations had a modest but significant correlation (r = 0.109, p = 0.041), implying that diet quality influence social interactions. The environment domain also correlated positively (r = 0.134, p = 0.012), indicating individuals with healthier diets may perceive their surroundings more favorably.
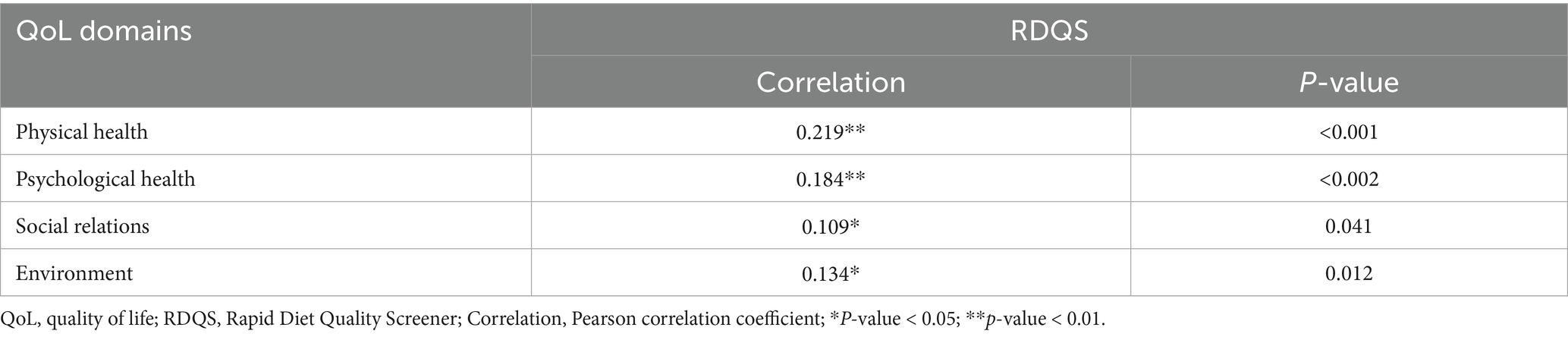
Table 3. The relationship between quality of life and diet quality (n = 353).
Table 4 shows that diet quality (RDQS) consistently emerged as the strogest significant predictor across all dimensions of quality of life, including physical (B = 1.132, t = 4.152, p < 0.001), psychological (B = 1.002, t = 3.341, p = 0.001), social relationship (B = 0.710, t = 1.891, p = 0.059, marginally significant), environmental (B = 0.690, t = 2.465, p = 0.014), and overall QoL (B = 0.883, t = 3.620, p < 0.001). In addition, BMI significantly and negatively predicted the psychological (B = −0.372, p = 0.013), social relationship (B = −0.584, p = 0.002), and overall QoL dimensions (B = −0.296, p = 0.015). Gender also showed a significant negative effect on the social (B = −6.087, p = 0.009) and overall QoL domains (B = −3.391, p = 0.026), indicating lower scores for females. Other variables, including age and physical activity, did not show significant associations across most QoL domains. All models except for the environmental dimension were statistically significant at p < 0.05, with explained variances ranging from 5.9% (physical, psychological, social) to 6.7% (overall QoL), while the environmental model was not significant (p = 0.10), explaining only 2.6% of the variance.
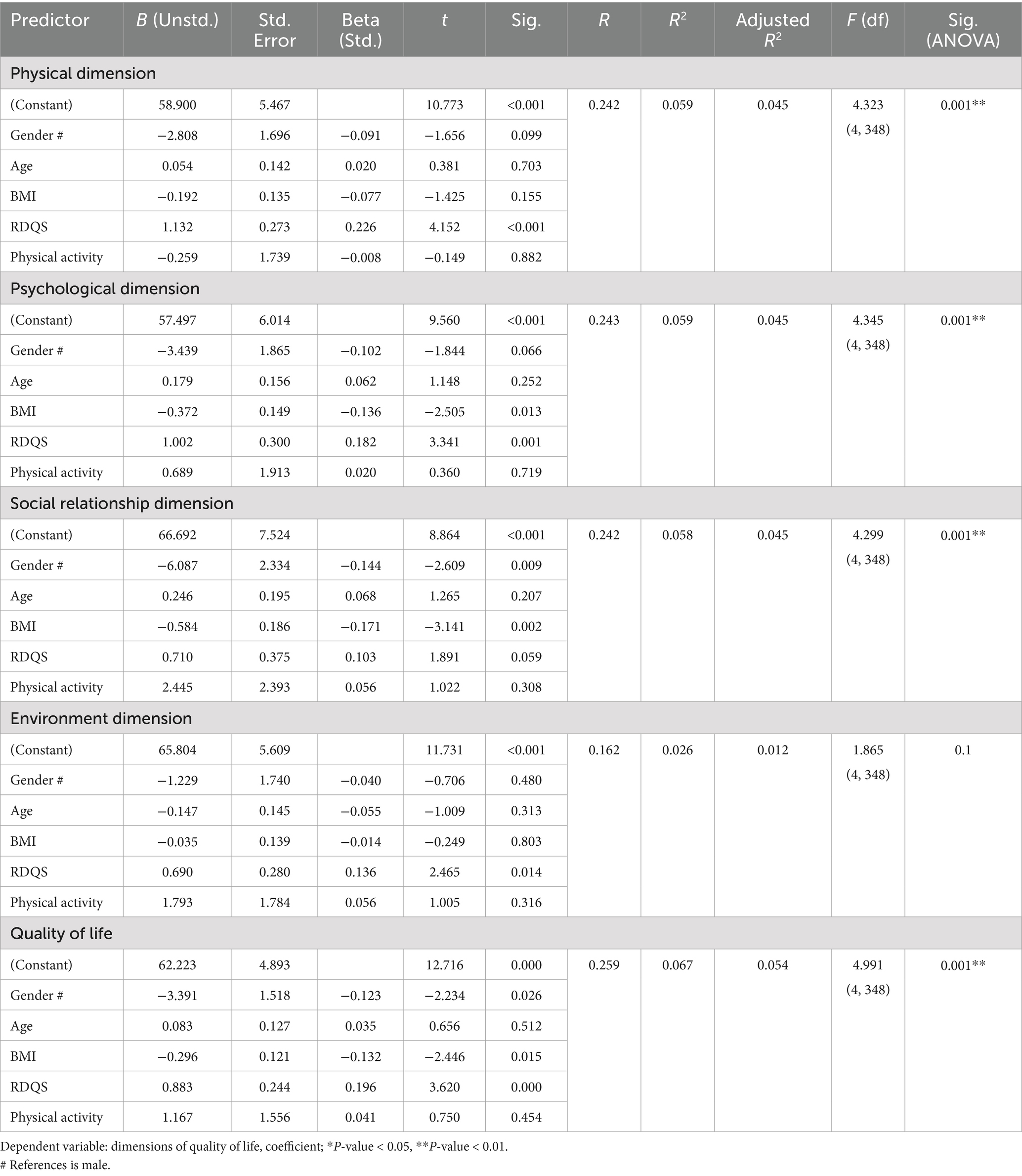
Table 4. Multiple regression analysis of quality of life domains in relation to diet quality, physical activity levels, and demographic variables (n = 353).
4 Discussion
To the best of the authors’ knowledge, this is the first Arab study that examines the relationship between quality of life, diet quality, and personal characteristics among healthcare professionals. In Saudi Arabia, healthcare professionals frequently encounter substantial workloads, irregular work schedules, and restricted access to nutritious food options within hospital environments. Additionally, cultural norms may shape gender roles, social expectations, and dietary behaviors, thereby influencing health outcomes (18). A comprehensive understanding of these contextual factors is essential for developing effective interventions specifically tailored to the local healthcare system.
Our findings reveal significant positive correlations between diet quality and various QoL domains. Notably, the social relations domain demonstrated significant differences based on physical activity and gender. Furthermore, participants who regularly engaged in exercise exhibited healthier dietary habits. Diet quality was the strongest and most consistent predictor across all dimensions of quality of life. Lower BMI significantly predicted better psychological, social, and overall QoL, while male gender was a significant predictor of higher social and overall QoL.
Numerous studies have been conducted among healthcare professionals; however, they primarily focus on assessing QoL or lifestyle factors separately. A recent study aimed to evaluate the QoL among 3,170 healthcare workers from 19 Arab countries using the WHOQOL-BREF instrument. It reported that most healthcare workers in the Arab world exhibited unsatisfactory QoL scores across various domains: physical (59.2%), psychological (84.6%), social (73.8%), and environmental (77.7%), except for general QoL, where the score was 38.8%. This underscores the need to focus attention on this group to enhance their productivity and quality of service provision (7). Our study revealed weak but significant positive correlations between healthcare professionals’ diet quality, as measured by the RDQS, and QoL domains, particularly physical (r = 0.219) and psychological health (r = 0.184), suggesting a diet’s role in overall well-being. Additionally, improved diet quality reliably predicted enhanced quality of life across all domains. These findings align with those of previous studies, suggesting that better diet quality is associated with improved health outcomes, stressing the importance of dietary habits in overall well-being (6, 19). Al Hazmi et al. (18), who investigated dietary habits among healthcare workers in Riyadh, found widespread unhealthy dietary behaviors. A notable percentage of healthcare professionals frequently consume sweets (46.6%) and coffee (66.2%). The study also revealed that Saudis had higher rates of binge eating at home compared to non-Saudis (61.9% vs. 22.5%) (18). Another study on manufacturing employees, not centered on healthcare professionals, has revealed that adherence to a healthy diet is linked to enhanced QoL (20). Additionally, the 2025 systematic review by Godos et al., which incorporated 13 studies of the general population and 15 studies of various patient groups, indicated a significant positive correlation between adherence to the Mediterranean diet and health-related quality of life (HRQoL), particularly in the physical domains (21). Conversely, another study has reported conflicting findings regarding the relationship between healthier dietary habits and quality of life. A cross-sectional study in France assessed the dietary patterns and health-related quality of life (HRQoL) of 308 adult females using three 24-h dietary recalls and a Food Benefit Assessment (FBA) questionnaire. Cluster analysis was employed to identify dietary patterns, while the FBA questionnaire was used to evaluate HRQoL. The study reported no significant differences in QoL based on dietary patterns in a sample of adult females, which they attributed to potential limitations in dietary assessment methods (22).
Nutritional behavior is intricately shaped by various factors, among which nutritional knowledge stands out. Consistent and effective nutrition education is crucial for promoting health and transforming eating habits across all age groups (23). Furthermore, health literacy plays a critical role as a determinant of health-enhancing behaviors (24). Poor health literacy hinders one’s ability to detect and address health problems. A key part of health literacy, nutrition literacy, involves understanding, interpreting, and utilizing basic nutritional information to make informed dietary decisions. The impact of an individual’s knowledge, attitudes, skills, and behaviors related to food and nutrition on their dietary choices is widely recognized. Research has consistently shown that many people struggle to understand information on food labels, and those with limited health literacy or numerical skills often experience adverse health outcomes (25).
In addition, it is believed that physical activity can enhance social well-being, potentially by fostering greater community involvement or promoting social interaction (26); indeed, the findings of our study confirm this, by showing that healthcare professionals who engaged in regular physical activity reported healthier dietary habits and achieved higher scores across all QoL domains, with social relations showing a statistically significant improvement (p = 0.037). Although physical activity was not a significant predictor of QoL domains, and no significant differences were observed in the physical health, psychological health, and environmental domains, the trends indicate a general enhancement in QoL for those who are physically active. Also, several studies have revealed that higher physical activity level is related to better QoL (16, 17, 22, 23). Gill et al. (27) demonstrated that engaging in physical activity positively affects all domains of quality of life, extending beyond mere physical improvements to enhance social and emotional well-being, which may primarily motivate community participants. In consistence, Di Bartolomeo and Papa (26) found that regular physical activity significantly improved trust and social connectedness among participants engaged in structured sports activities. Their research highlights the cooperative nature of sports, emphasizing how teamwork, communication, and shared goals foster trust and build stronger social networks. However, this study primarily focused on team sports, which may limit its applicability to other forms of physical activity, such as yoga or walking, that lack structured group dynamics. Additionally, individual differences such as personality traits or preexisting social skills were not considered, which may moderate the social benefits derived from physical activity (26).
Further evidence supporting the beneficial effects of physical activity on health care professionals’ QoL can be seen in a study by Grimani et al. (1), who demonstrated that workplace exercise programs enhanced not only physical health but also mental well-being and work performance among health care staff (3). However, some studies have reported inconsistent results. For example, Sharma et al. (4) found that while physical activity improved physical health indicators in healthcare professionals, its impact on psychological well-being was limited due to ongoing work-related stress factors. Similarly, Zubair et al. (28) stated no significant correlation between physical activity levels and QoL among surgical residents, attributing this lack of impact to extended working hours, irregular schedules, and burnout, which could potentially overshadow the benefits of exercising. These findings suggest that, although physical activity is generally advantageous, its positive effects may be diminished by occupation-specific factors in healthcare environments.
Another interesting finding of this study is the variability of the scores by gender. Being male significantly predicted better the social and overall quality of life. Male participants demonstrated marginally higher scores than female participants across all QoL domains (physical health, psychological health, social relations, and environment), with a statistically significant difference observed in social relations. This suggesting that gender influences the social aspects of QoL among medical staff. This finding is consistent with those of other studies conducted in Greece, Italy, the USA, and Oman (29–31). Tountas et al. (29) linked gender disparities in health-related quality of life to the lower social status of female in a male-dominated society, particularly in Greece, a Mediterranean country where traditional norms further diminish female’s standing. These disparities may also reflect professional differences, as most males in this study were medical doctors, whereas women primarily held nursing or auxiliary positions (29). As previously mentioned, our study found that males generally scored higher than females in all QoL domains. However, the only statistically significant difference occurred in social relations. The lack of significant results in other areas may reflect substantial ongoing efforts to empower females, aligning with one of the objectives of Saudi Vision 2030 (32).
In our study, dietary quality did not show significant differences between the genders, indicating that both maintain comparable dietary practices (3, 16). However, previous research has highlighted poor dietary habits among healthcare workers in Riyadh, with females consuming more fruits and vegetables than males (47.1%, 18.6%, p < 0.000) (18).
Although previous research has suggested that maintaining a normal BMI is linked to improved QoL outcomes (29, 30), our findings revealed that lower BMI significantly predicted better psychological, social relationship, and overall QoL dimensions. Additionally, our study observed a trend where participants with normal weight had the highest mean scores across QoL domains. In contrast, those who were underweight or obese had lower scores. However, no statistically significant differences were observed in the mean scores across various BMI categories and QoL domains. This aligns with the existing literature that does not establish a definitive correlation between BMI and QoL (33).
Finally, numerous studies have highlighted that the well-being of healthcare practitioners significantly impacts the quality and safety of patient care (34, 35). Enhanced well-being among healthcare professionals is associated with improved care delivery (34). Additionally, the well-being and quality of work environment have been identified as critical factors affecting patient care outcomes (31). This emphasizes the importance for hospital management and policymakers to focus on improving work-related factors, thereby boosting healthcare professionals’ well-being and, consequently, elevating the standard of patient care.
This study has several strengths marks a significant contribution to the literature on diet quality and QoL among this population. First, diet, QoL, and physical activity were evaluated using validated instruments (12–17). Second, we used structured interviews to collect data (considered more reliable than self-administered questionnaires for assessing behaviors). Third, both sexes were included in the present study. However, there are some limitations that should be considered. First, it employed a cross-sectional design that precludes causal inferences. Finally, weight and height were self-reported, which could have created recall bias due to over- or under-reporting, potentially affecting the accuracy of our results.
5 Conclusions and future implications
Our findings highlight the interrelation between physical activity, diet quality, and QoL, suggesting that interventions aimed at improving dietary habit and lifestyle choices among medical staff could enhance individual health outcomes, improve social and psychological well-being, and ultimately enhancing the quality of patient care. With growing global attention on the well-being of healthcare workers, these findings have broad international relevance, reinforcing the role of dietary interventions in enhanceing QoL in healthcare settings. It is also important to consider potential confounding variables not fully accounted for in this analysis, such as occupational stress, sleep patterns, specific job roles, and work hours. These factors may influence dietary habits and QoL and should be explored using multivariate approaches in future studies.
Future research should investigate these relationships more comprehensively through longitudinal studies to establish stronger causal links. Such studies would provide more comprehensive insights, forming the basis for evidence-based policies aimed at improving healthcare professionals’ QoL in Saudi Arabia and beyond.
Incorporating nutrition education into public health initiatives and promoting awareness of nutrition and sustainability are essential for supporting informed dietary choices. Implementing evidence-based practices and policies supported by collaborative efforts is crucial for improving the diet quality and overall well-being of healthcare professionals. Integrating physical activity facilities within a medical institution can encourage staff to engage in physical activity during breaks and working hours. This enhancement can positively impact the emotional, social, and potentially spiritual aspects of life, contributing to a fulfilling experience. Ultimately, this could lead to improved QoL for healthcare professionals.
Finally, this study highlights the importance of implementing policies and initiatives to enhance healthcare professionals’ well-being and quality of work life. Strengthening these areas can contribute to a healthier workforce, ultimately enhancing patient care and the overall effectiveness of healthcare systems.
Data availability statement
The datasets generated during and/or analyzed during this study are not publicly available due to data protection requirements. Requests to access the datasets should be directed to WA, V2FsZmF3YXpAa3N1LmVkdS5zYQ==.
Ethics statement
The study protocol was approved by the local institutional ethics committee of King Saud University (No. KSU-HE-24-091). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
WA: Conceptualization, Formal analysis, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. RA: Formal analysis, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. NA: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing. SA: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. WM: Data curation, Software, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported by the Ongoing Research Funding program (ORF-2025-840), King Saud University, Riyadh, Saudi Arabia.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Grimani, A, Aboagye, E, and Kwak, L. The effectiveness of workplace nutrition and physical activity interventions in improving productivity, work performance and workability: a systematic review. BMC Public Health. (2019) 19:1676. doi: 10.1186/s12889-019-8033-1
2. Mittal, TK, Cleghorn, CL, Cade, JE, Barr, S, Grove, T, Bassett, P, et al. A cross-sectional survey of cardiovascular health and lifestyle habits of hospital staff in the UK: do we look after ourselves? Eur J Prev Cardiol. (2018) 25:543–50. doi: 10.1177/2047487317746320
3. Phiri, LP, Draper, CE, Lambert, EV, and Kolbe-Alexander, TL. Nurses’ lifestyle behaviours, health priorities and barriers to living a healthy lifestyle: a qualitative descriptive study. BMC Nurs. (2014) 13:38. doi: 10.1186/s12912-014-0038-6
4. Sharma, S, Anand, T, Dey, B, Ingle, G, and Kishore, J. Prevalence of modifiable and non-modifiable risk factors and lifestyle disorders among health care professionals. Astrocyte. (2014) 1:178. doi: 10.4103/2349-0977.157757
5. Abdulrahman, M, Nair, SC, Farooq, MM, Al Kharmiri, A, Al Marzooqi, F, and Carrick, FR. Burnout and depression among medical residents in the United Arab Emirates: a multicenter study. J Family Med Prim Care. (2018) 7:435–41. doi: 10.4103/jfmpc.jfmpc_199_17
6. Ruano, C, Henriquez, P, Martínez-González, MÁ, Bes-Rastrollo, M, Ruiz-Canela, M, and Sánchez-Villegas, A. Empirically derived dietary patterns and health-related quality of life in the SUN project. PLoS One. (2013) 8:e61490. doi: 10.1371/journal.pone.0061490
7. Ghazy, RM, Abubakar Fiidow, O, Abdullah, FSA, Elbarazi, I, Ismail, II, Alqutub, ST, et al. Quality of life among health care workers in Arab countries 2 years after COVID-19 pandemic. Front Public Health. (2022) 10:917128. doi: 10.3389/fpubh.2022.917128
8. AlAteeq, MA, and AlArawi, SM. Healthy lifestyle among primary health care professionals. Saudi Med J. (2014) 35:488–94.
9. Brooks, SK, Gerada, C, and Chalder, T. Review of literature on the mental health of doctors: are specialist services needed? J Ment Health. (2011) 20:146–56. doi: 10.3109/09638237.2010.541300
10. Firth-Cozens, J. Doctors, their wellbeing, and their stress. BMJ. (2003) 326:670–1. doi: 10.1136/bmj.326.7391.670
11. Raosoft Inc. RaoSoft® sample size calculator. Available online at: http://www.raosoft.com/samplesize.html (Accessed November 5, 2023).
12. Malibary, H, Zagzoog, MM, Banjari, MA, Bamashmous, RO, and Omer, AR. Quality of life (QoL) among medical students in Saudi Arabia: a study using the WHOQOL-BREF instrument. BMC Med Educ. (2019) 19:344. doi: 10.1186/s12909-019-1775-8
13. Zhang, Y, Qu, B, Lun, S, Wang, D, Guo, Y, and Liu, J. Quality of life of medical students in China: a study using the WHOQOL-BREF. PLoS One. (2012) 7:e49714. doi: 10.1371/journal.pone.0049714
14. Rondung, E, Oliveira, S, and Esteves, F. Validity and reliability of the WHOQOL-BREF in a pregnant population. Health Qual Life Outcomes. (2023) 21:96. doi: 10.1186/s12955-023-02166-2
15. Almarabheh, A, Salah, AB, Alghamdi, M, Al Saleh, A, Elbarbary, A, Al Qashar, A, et al. Validity and reliability of the WHOQOL-BREF in the measurement of the quality of life of sickle disease patients in Bahrain. Front Psychol. (2023) 14:1219576. doi: 10.3389/fpsyg.2023.1219576
16. Kotecki, JE, Greene, MA, Khubchandani, J, and Kandiah, J. A brief dietary screening and counseling tool for health educators. Am J Health Educ. (2021) 52:111–6. doi: 10.1080/19325037.2021.1902886
17. World Health Organization. Global physical activity questionnaire (GPAQ): Analysis guide. Geneva: World Health Organization (2004).
18. Al Hazmi, TM, AlGhamdi, A, and Abdulmajeed, I. Eating habits among healthcare providers during working hours at National Guard Health Affairs-Riyadh, Saudi Arabia. Int J Med Res Health Sci. (2018) 7:1–14.
19. Dello Russo, M, Formisano, A, Lauria, F, Ahrens, W, Bogl, LH, Eiben, G, et al. Dietary diversity and its association with diet quality and health status of European children, adolescents, and adults: results from the I.Family study. Food Secur. (2023) 12:4458. doi: 10.3390/foods12244458
20. Nasab, SJ, Hamedani, SG, Roohafza, H, Feizi, A, Clark, CCT, and Sarrafzadegan, N. The association between dietary patterns and quality of life: a cross-sectional study among a large sample of industrial employees. BMC Public Health. (2023) 23:2016. doi: 10.1186/s12889-023-16898-9
21. Godos, J, Guglielmetti, M, Ferraris, C, Frias-Toral, E, Domínguez Azpíroz, I, Lipari, V, et al. Mediterranean diet and quality of life in adults: a systematic review. Nutrients. (2025) 17:577. doi: 10.3390/nu17030577
22. Holmes, BA, Habi-Rachedi, F, Trotin, B, Paineau, D, Guyonnet, D, Rondeau, P, et al. Dietary patterns, digestive symptoms, and health-related quality of life in women reporting minor digestive symptoms. Nutrition. (2017) 35:132–8. doi: 10.1016/j.nut.2016.10.020
23. Carvalho, GP, Costa-Camilo, E, and Duarte, I. Advancing health and sustainability: a holistic approach to food production and dietary habits. Food Secur. (2024) 13:3829. doi: 10.3390/foods13233829
24. Carrara, A, and Schulz, PJ. The role of health literacy in predicting adherence to nutritional recommendations: a systematic review. Patient Educ Couns. (2018) 101:16–24. doi: 10.1016/j.pec.2017.07.005
25. Draper, AK, Adamson, AJ, Clegg, S, Malam, S, Rigg, M, and Duncan, S. Front-of-pack nutrition labelling: are multiple formats a problem for consumers? Eur J Public Health. (2013) 23:517–21. doi: 10.1093/eurpub/ckr144
26. Di Bartolomeo, G, and Papa, S. The effects of physical activity on social interactions: the case of trust and trustworthiness. J Sports Econom. (2019) 20:50–71. doi: 10.1177/1527002517717299
27. Gill, DL, Hammond, CC, Reifsteck, EJ, Jehu, CM, Williams, RA, Adams, MM, et al. Physical activity and quality of life. J Prevent Med Public Health. (2013) 46:S28–34. doi: 10.3961/jpmph.2013.46.S.S28
28. Zubair, MH, Hussain, LR, Williams, KN, and Grannan, KJ. Work-related quality of life of US general surgery residents: is it really so bad? J Surg Educ. (2017) 74:e138–46. doi: 10.1016/j.jsurg.2017.09.018
29. Tountas, Y, Demakakos, PT, Yfantopoulos, Y, Aga, J, Houliara, L, and Pavi, E. The health related quality of life of the employees in the Greek hospitals: as-sessing how healthy are the health workers. Health Qual Life Outcomes. (2003) 1:61. doi: 10.1186/1477-7525-1-61
30. Messina, G, Quercioli, C, Troiano, G, Russo, C, Barbini3, E, Nisticò, F, et al. Italian medical students quality of life: years 2005-2015. Ann Ig. (2016) 28:245–51. doi: 10.7416/ai.2016.2103
31. Al Wahaibi, N, Al Kindi, R, and Al Hinai, M. Quality of life among postgraduate medical residents in Oman: a cross-sectional survey. Oman Med J. (2023) 38:e568. doi: 10.5001/omj.2023.115
32. Saudi Arabia’s Vision 2030. Available online at: https://www.vision2030.gov.sa/en (accessed January 24, 2025)
33. Apple, R, Samuels, LR, Fonnesbeck, C, Schlundt, D, Mulvaney, S, Hargreaves, M, et al. Body mass index and health-related quality of life. Obes Sci Pract. (2018) 4:417–26. doi: 10.1002/osp4.292
34. Mohammadi-Bolbanabad, A, Shirkhani, B, Mohammadi, S, Asadi, H, and Aghaei, A. Relationship between quality of work life of medical staff and quality of patient care. Hosp Pract Res. (2016) 1:61–3. doi: 10.20286/hpr-010261
Keywords: diet, quality of life, healthcare professionals, WHOQOL, RDQS
Citation: Alfawaz W, Albassam RS, Almuharib N, Alghafis S and Mahfouz W (2025) Association between diet and quality of life among healthcare professionals in King Saud University Medical City. Front. Public Health. 13:1595412. doi: 10.3389/fpubh.2025.1595412
Edited by:
Radwan Qasrawi, Al-Quds University, PalestineReviewed by:
Rute F. Meneses, Fernando Pessoa University, PortugalKarolina Sobczyk, Medical University of Silesia, Poland
Copyright © 2025 Alfawaz, Albassam, Almuharib, Alghafis and Mahfouz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Reem S. Albassam, cmVlbS5hbGJhc3NhbUBnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship