 Mohamed Ali Boujelbane1,2†
Mohamed Ali Boujelbane1,2† Achraf Ammar1,2,3*†‡
Achraf Ammar1,2,3*†‡ Atef Salem1,2
Atef Salem1,2 Mohamed Kerkeni2,4
Mohamed Kerkeni2,4 Khaled Trabelsi4,5
Khaled Trabelsi4,5 Bassem Bouaziz6,7
Bassem Bouaziz6,7 Liwa Masmoudi2‡
Liwa Masmoudi2‡ Juliane Heydenreich8Christiana Schallhorn9‡
Juliane Heydenreich8Christiana Schallhorn9‡ Gabriel Müller1Ayse Merve Uyar1
Gabriel Müller1Ayse Merve Uyar1 Hadeel Ali Ghazzawi10
Hadeel Ali Ghazzawi10 Adam Tawfiq Amawi5
Adam Tawfiq Amawi5 Bekir Erhan Orhan11Giuseppe Grosso12‡
Bekir Erhan Orhan11Giuseppe Grosso12‡ Osama Abdelkarim13,14
Osama Abdelkarim13,14 Tarak Driss15
Tarak Driss15 Kais El Abed2,4
Kais El Abed2,4 Piotr Zmijewski16Frédéric Debeaufort17,18‡Nasreddine Benbettaieb17,18‡Clément Poulain18‡Laura Reyes19
Piotr Zmijewski16Frédéric Debeaufort17,18‡Nasreddine Benbettaieb17,18‡Clément Poulain18‡Laura Reyes19 Amparo Gamero20Marta Cuenca-Ortolá20
Amparo Gamero20Marta Cuenca-Ortolá20 Antonio Cilla20
Antonio Cilla20 Nicola Francesca21
Nicola Francesca21 Concetta Maria Messina22Enrico Viola21‡Björn Lorenzen23Stefania Filice23Aadil Bajoub24‡El-Mehdi Ajal24,25El Amine Ajal26‡Majdouline Obtel25
Concetta Maria Messina22Enrico Viola21‡Björn Lorenzen23Stefania Filice23Aadil Bajoub24‡El-Mehdi Ajal24,25El Amine Ajal26‡Majdouline Obtel25 Sadjia Lahiani27
Sadjia Lahiani27 Taha Khaldi28
Taha Khaldi28 Nafaa Souissi2Omar Boukhris29,30‡
Nafaa Souissi2Omar Boukhris29,30‡ Haitham Jahrami31,32
Haitham Jahrami31,32 Waqar Husain33
Waqar Husain33 Evelyn Frias-Toral34,35
Evelyn Frias-Toral34,35 Walid Mahdi6,7
Walid Mahdi6,7 Hamdi Chtourou2
Hamdi Chtourou2 Wolfgang I. Schöllhorn1
Wolfgang I. Schöllhorn1- 1Department of Training and Movement Science, Institute of Sport Science, Johannes Gutenberg-University Mainz, Mainz, Germany
- 2High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia
- 3Research Laboratory, Molecular Bases of Human Pathology, LR19ES13, Faculty of Medicine of Sfax, University of Sfax, Sfax, Tunisia
- 4Research Laboratory, Education, Motricity, Sport and Health, EM2S, LR19JS01, High Institute of Sport and Physical Education of Sfax, University of Sfax, Sfax, Tunisia
- 5Department of Movement Sciences and Sports Training, School of Sport Science, The University of Jordan, Amman, Jordan
- 6Multimedia InfoRmation Systems and Advanced Computing Laboratory (MIRACL), University of Sfax, Sfax, Tunisia
- 7Higher Institute of Computer Science and Multimedia of Sfax (ISIMS), University of Sfax, Sfax, Tunisia
- 8Department of Experimental Sports Nutrition, Faculty of Sports Sciences, Leipzig University, Leipzig, Germany
- 9Department of Sports Economics, Sociology and History, Institute of Sport Science, Johannes Gutenberg-University Mainz, Mainz, Germany
- 10Department of Nutrition and Food Technology, School of Agriculture, The University of Jordan, Amman, Jordan
- 11Faculty of Sports Sciences, Istanbul Aydın University, Istanbul, Türkiye
- 12Department of Biomedical and Biotechnological Sciences, University of Catania, Catania, Italy
- 13Faculty of Sport Sciences, Assiut University, Assiut, Egypt
- 14ESLSCA University Egypt, Giza, Egypt
- 15Interdisciplinary Laboratory in Neurosciences, Physiology, and Psychology: Physical Activity, Health, and Learning (LINP2), UFR STAPS, Paris Nanterre University, Nanterre, France
- 16Jozef Pilsudski University of Physical Education in Warsaw, Warsaw, Poland
- 17Department BioEngineering, Institut Universitaire de Technologie IUT-Dijon-Auexrre-Nevers, University Burgundy Europe, Dijon, France
- 18Joint Research Unit UMR PAM-Food Processing and Microbiology, Université Bourgogne Europe, INRAE, Institut AgroDijon, Dijon, France
- 19Vitagora Innovation Cluster, Dijon, France
- 20Department of Preventive Medicine and Public Health, Food Science, Toxicology and Forensic Medicine, Faculty of Pharmacy and Food Sciences, University of Valencia, Valencia, Spain
- 21Department of Agricultural Food and Forest Sciences, University of Palermo, Palermo, Italy
- 22Laboratory of Marine Biochemistry and Ecotoxicology, Department of Earth and Marine Sciences DiSTeM, University of Palermo, Trapani, Italy
- 23Microtarians SIS, Société d’Impact Societal, Luxembourg, Luxembourg
- 24Laboratory of Food and Food By-Products Chemistry and Processing Technology, National School of Agriculture in Meknès, Meknès, Morocco
- 25Laboratory of Social Medicine, Department of Epidemiology and Public Health, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco
- 26UPR of Pharmacognosy, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University, Rabat, Morocco
- 27VALCORE Laboratory, Department of Biology, Faculty of Science, University of M’hamed Bougara Boumerdes, Boumerdes, Algeria
- 28Biotechnology Research Center C.R.Bt Constantine ALGERIA, Constantine, Algeria
- 29SIESTA Research Group, School of Allied Health, Human Services and Sport, La Trobe University, Melbourne, VIC, Australia
- 30Sport, Performance, and Nutrition Research Group, School of Allied Health, Human Services and Sport, La Trobe University, Melbourne, VIC, Australia
- 31Government Hospitals, Manama, Bahrain
- 32Department of Psychiatry, College of Medicine and Medical Sciences, Arabian Gulf University, Manama, Bahrain
- 33Department of Humanities, COMSATS University Islamabad, Islamabad, Pakistan
- 34Escuela de Medicina, Universidad Espíritu Santo, Samborondón, Ecuador
- 35Division of Research, Texas State University, San Marcos, TX, United States
Introduction: The Mediterranean diet (MedDiet) is acknowledged for its health advantages; however, compliance with its principles differs by region and is influenced by geographical, cultural, economic, and life-style factors. This research examines regional differences in sociodemographic and lifestyle factors between Mediterranean (MC) and non-Mediterranean (NMC) countries, with a particular focus on adherence to the Mediterranean diet and lifestyle, as well as the associated barriers in each region.
Methods: The MEDIET4ALL international survey was conducted across 10 countries, and data were collected from 4,010 participants. Dietary adherence was assessed via the MedLife Index, and additional lifestyle measures included physical activity (IPAQ-SF), sleep patterns (PSQI), mental health (DASS-21), and social participation (SSPQL). Statistical analyses included chi-square tests, Mann–Whitney U tests, and standardized residual analyses to identify significant regional variations.
Results: The study revealed distinct dietary patterns, with MC participants showing stronger adherence to traditional MedDiet components (legumes, fish) while NMC participants favored modern adaptations (whole grains). Both regions exhibited low physical activities dominance (60%–62%), although MC participants engaged more (21.1% vs. 18.5%) in moderate physical activity. MC maintained higher proportions of “sometimes socially active” individuals, NMC showed greater representation in the “always socially active” category. Sleep quality was poorer in MC (45% below recommended duration vs. 40% in NMC), while NMC reported higher insomnia rates. Mental health symptoms were comparable (33%–35% moderate depression/anxiety in both), reflecting post-pandemic global trends. Barriers differed regionally with MC faced economic/access constraints while NMC struggled with knowledge gaps and time limitations.
Conclusion: Our findings highlight that while Mediterranean regions maintain traditional dietary patterns, globalization and modern lifestyle shifts are narrowing regional health behaviors. Public health strategies should address region-specific barriers, including economic constraints in MC regions and knowledge gaps in NMC regions, while promoting MedDiet adherence. Future research should explore the impact of cultural, socio-economic, and digital factors on dietary behaviors and mental health to develop tailored, effective interventions for improving overall well-being.
1 Introduction
The scientific community has increasingly focused on assessing the risk factors associated with dietary practices and their potential associations with public health (1). Current evidence suggests that traditional dietary patterns are undergoing a profound transformation due to globalization and the increased availability of processed, ready-to-eat, high-calorie foods (2). This transition has led to a decline in locally sourced, nutrient-dense foods and an increase in diets characterized by high levels of added sugars, saturated and hydrogenated fats, and a deficiency in fiber and micronutrients. Such dietary changes are linked to the increasing prevalence of noncommunicable diseases (NCDs), including obesity, diabetes, cardiovascular diseases, and certain cancers (3).
While numerous traditional dietary patterns worldwide are associated with health benefits, the MedDiet stands out as one of the most extensively researched (4). Rooted in the eating habits of Greece and Italy during the early 1960s, the MedDiet is characterized by high consumption of olive oil, fruits, vegetables, whole grains, nuts, and legumes; moderate intake of fish and dairy; and low consumption of red meat and processed foods (5). Its nutritional composition is rich in bioactive compounds with antioxidant and anti-inflammatory properties, is associated with its low glycemic index and potential health benefits (6).
Numerous systematic reviews and meta-analyses of population-based and prospective epidemiological studies have demonstrated that adherence to the MedDiet is associated with a reduced risk of obesity (7), hypertension (8), type 2 diabetes (9), metabolic syndrome (10), primary (11) and secondary prevention of cardiovascular diseases (12), certain types of cancer (13), and neurodegenerative disorders, such as cognitive decline and Alzheimer’s disease (14). Besides, higher adherence to this dietary pattern has also been associated with better physical and mental quality of life in the general population and in individuals with a variety of health conditions (15). Finally, the Mediterranean diet is also considered an ideal dietary model supporting the balance among people, environment, and society (16).
Adherence to the MedDiet varies across regions due to geographical, cultural, economic, and lifestyle factors (17). Traditionally, MC including those in Southern Europe (Spain, Italy, France, Turkey), North Africa (Tunisia, Algeria, Morocco), and the Middle East (Jordan), have followed a diet rich in plant-based foods, seafood, and olive oil, which aligns with the MedDiet model. However, globalization and urbanization have led to a shift away from these dietary habits, resulting in the increasing adoption of Westernized diets in these regions (18). This transition coincides with a steady decline in MedDiet adherence, despite its well-documented health benefits (19). Socioeconomic factors play a crucial role in dietary choices, as individuals with higher socioeconomic status are more likely to consume nutrient-dense foods such as fruits, vegetables, and whole grains, whereas those with lower socioeconomic status often rely more on refined grains and processed foods owing to cost and accessibility (20). Additionally, lifestyle behaviors, including smoking and physical inactivity, are linked to lower adherence to the MedDiet, often coinciding with increased fast-food consumption (21). In contrast, non-Mediterranean regions, such as Central and Northern Europe (Germany, Luxembourg), exhibit distinct dietary patterns shaped by local food availability, cultural traditions, and economic conditions. The consumption of diets in these regions tends to be greater for processed foods, red meat, and dairy products, with lower consumption rates of olive oil and fresh produce (22). Nonetheless, the growing global awareness of the health benefits of the MedDiet has led to efforts to promote its adoption in NMC. However, barriers such as food availability, affordability, and ingrained culinary traditions continue to affect the extent to which individuals in these regions can integrate MedDiet principles into their daily eating habits (23, 24). As part of the broader MEDIET4ALL PRIMA project, which is supported by the European Union, this research aligns with the initiative’s goal of promoting the MedDiet and its associated lifestyle as a sustainable and health-focused model (25). This study aims to evaluate regional variations in the MedDiet adherence by analyzing sociodemographic and lifestyle factors across the Mediterranean and non-Mediterranean regions.
2 Materials and methods
2.1 Survey design and participants recruitment
The MEDIET4ALL survey was conducted as an international online study over a period of 4 months, starting in the summer of 2024, to assess adherence to the Mediterranean Diet across multiple countries and regions. Designed by a multidisciplinary team of specialists in public health, nutrition, psychology, and social sciences, the survey prioritized representativeness in regional comparisons while acknowledging inherent limitations of digital recruitment (e.g., higher participation from younger, urban populations). The study targeted participants from Tunisia, Algeria, Morocco, France, Spain, Germany, Luxembourg, Italy, Turkey, and Jordan, ensuring proportional representation across Mediterranean and non-Mediterranean regions. To facilitate regional comparisons, countries were grouped as Mediterranean (MC)—including Tunisia, Algeria, Morocco, France, Spain, Italy, and Turkey—or non-Mediterranean (NMC)—including Germany, Luxembourg, and Jordan, based on strict geographic and historical definitions of the Mediterranean (26).
The survey was developed in multiple languages, including English, German, French, Italian, Spanish, Arabic, and Turkish, to maximize accessibility. Validated instruments were used to assess adherence to the Mediterranean diet and associated lifestyle factors. Items without official translations underwent rigorous translation and back-translation processes, ensuring high reliability coefficients (r = 0.81–0.94). The survey was hosted on the GDPR-compliant SoSci Survey platform, with support from Johannes Gutenberg University Mainz.
The MEDIET4ALL survey was disseminated through various channels, including email invitations, university and consortium websites, and social media platforms such as ResearchGate™, LinkedIn™, Facebook™, WhatsApp™, and X™ (formerly Twitter™). The MEDIET4ALL consortium and collaborators (e.g., Bilendi solution) facilitated distribution, and the general public was encouraged to share the survey within their networks.
Initially, more than 8,000 individuals participated in the survey. To ensure high-quality data, responses underwent logical screening to detect inconsistencies, such as reporting no vigorous physical activity while simultaneously claiming daily engagement in such exercises. Duplicate entries were identified and removed based on criteria including matching IP addresses, closely timed submissions, and highly similar demographic and response patterns. Implausible values, such as reporting unrealistic sleep durations (e.g., 24 h) or improbable dietary intake, were also excluded to enhance data reliability. After applying rigorous data filtering for accuracy and completeness, 4,010 valid responses were included in the final analysis.
The survey collected demographic, socio-economic, and behavioral data, including dietary behaviors, physical activity, social participation, sleep quality, mental health, and lifestyle characteristics. Several validated questionnaires were used, including the MedLife Index for dietary adherence (27), the International Physical Activity Questionnaire Short Form (IPAQ-SF) for physical activity (28), the Depression Anxiety Stress Scales-21 (DASS-21) for mental health assessment (29), and the Short Life Satisfaction Questionnaire (SLSQ) for well-being evaluation (30).
The survey began with an introductory page detailing the study’s objectives, ethical considerations, data privacy policies, and consent information. The participants were required to select one of the seven available languages before proceeding. The estimated completion time was 15–20 min. Participation was entirely voluntary, and no personal identifiable information was collected. Withdrawal was possible at any stage without any negative consequences.
This study involved human subjects, and all ethical guidelines, including informed consent, were strictly adhered to in accordance with the ethical principles of the Declaration of Helsinki. The protocol and consent form were approved by the Ethics Committee of the Faculty of Medicine at the University of Sfax (approval identification code: 066/24). Participation was entirely voluntary, and participants were informed that all data would be used solely for research purposes and kept anonymous and confidential. The survey complied with the SoSci Survey privacy policy,1 the Federal Data Protection Act (BDSG), and the EU General Data Protection Regulation (GDPR).
Participants were not asked to provide personally identifiable information, and their responses were recorded only upon survey submission. They were informed that they could withdraw from the study at any stage with no negative consequences. By completing the survey, participants provided informed consent for the anonymous use of their data for research purposes. Data confidentiality was rigorously maintained in compliance with applicable privacy regulations.
2.2 Measures and questionnaires
The survey used a variety of validated questionnaires to collect data on adherence to the MedDiet and associated lifestyle factors.
2.2.1 MedLife Index
The MedDiet adherence scores were recently evaluated in a systematic review con-ducted by Zaragoza-Martí et al. (31). Among the 28 scores analyzed, 12 were applied to the general population, and five adhered to the principles of the MedDiet Pyramid (32, 33). However, only the “MedLife index,” developed by Sotos-Prieto et al. (27), demonstrated good internal consistency with a Cronbach’s α coefficient of 0.75. Based on these findings, the MedLife Index was selected for inclusion in the MedLife 4ALL e-survey.
The MedLife Index is a validated instrument that measures adherence to the MedDiet and associated lifestyle practices (27). Based on the MedDiet Pyramid (33), the index includes 28 items divided into three categories: food consumption frequency (15 items), dietary habits (7 items), and lifestyle behaviors (6 items). The first category, food consumption frequency, includes 15 items that evaluate adherence to MedDiet patterns, such as consuming adequate amounts of fruits, vegetables, whole grains, and healthy fats, while limiting the intake of pastries and red meat. The second category, MedDiet habits, consists of 7 items assessing behaviors such as minimizing salt and sugar use and avoiding snacking between meals. The third category, lifestyle behaviors, contains 6 items measuring physical activity (e.g., engaging in at least 150 min of moderate activity per week), sleep duration (6–8 h), social habits, and conviviality.
Each item in the index is scored as 0 for non-adherence or 1 for adherence, with the total score ranging from 0, representing the lowest adherence, to 28, indicating the highest adherence. To facilitate interpretation, scores are classified into three levels: low adherence for scores below 12, medium adherence for scores between 12 and 16, and high adherence for scores above 16. These thresholds are determined based on tertiles of the total score distribution within the dataset. The MedLife Index thus offers a comprehensive measure of adherence to the MedDiet and lifestyle model.
2.2.2 Four items from the Pittsburgh Sleep Quality Index
Four items from the Pittsburgh Sleep Quality Index (PSQI) were included in the survey to assess sleep quality and disturbances (34), focusing on sleep efficiency, sleep latency, sleep quality, and sleep du-ration. Sleep efficiency was defined as the ratio of time asleep to time in bed, categorized as good when exceeding 85% or poor when below 85%. Sleep latency referred to the time taken to fall asleep, classified as good if less than 20 min or delayed if greater than 20 min. Sleep quality was self-rated on a 4-point Likert scale ranging from “very good” to “very bad.” Sleep duration was evaluated based on age-specific recommendations, with 7 to 9 h considered adequate for individuals younger than 65 years and 7 to 8 h for those aged 65 or older (35). The total PSQI score ranged from 0 to 21, with higher scores indicating poorer sleep quality.
2.2.3 Insomnia Severity Index
The Insomnia Severity Index (ISI) is a self-reported questionnaire designed to assess the severity and impact of insomnia symptoms (36). It includes seven items that evaluate difficulties with falling asleep, staying asleep, waking too early, satisfaction with sleep, interference with daily functioning, noticeability of sleep problems, and the personal distress caused by these difficulties. Each item is rated on a 0–4 scale, producing a total score range of 0 to 28. Based on the total score, insomnia is categorized into four levels: absence of insomnia (0–7), sub-threshold insomnia (8–14), moderate insomnia (15–21), or severe insomnia (22–28). The ISI is widely recognized for its reliability and ease of use, making it a valuable tool for clinical assessments, research, and monitoring treatment outcomes (36).
2.2.4 Depression Anxiety Stress Scales-21
The Depression Anxiety Stress Scales-21 (DASS-21) is a validated self-report questionnaire designed to measure the se-verity of symptoms related to depression, anxiety, and stress over the past week. It consists of 21 items, with seven items allocated to each of the three scales. Responses are rated on a 4-point Likert scale, and the scores for each scale are summed and then multiplied by two to reflect the overall severity. The scores categorize symptoms into five levels: normal, mild, moderate, severe, and extremely severe, offering valuable in-sights for clinical assessment and research into mental health (37).
2.2.5 Short Life Satisfaction Questionnaire-lockdown
The Short Life Satisfaction Questionnaire (SLSQ) is a modified version of the Satisfaction with Life Scale (SWLS) that focuses on three items closely associated with emotional well-being. Validated during the COVID-19 lockdown period (38, 39). The SLSQ allows participants to evaluate their life satisfaction based on personal criteria. Participants rate their agreement with each item on a 7-point Likert scale, ranging from 1 (“Strongly disagree”) to 7 (“Strongly agree”), producing a total score between 3 and 21. Higher scores indicate greater life satisfaction and are categorized as follows: 3 (“Extremely dissatisfied”), 4–6 (“Dissatisfied”), 7–9 (“Slightly dissatisfied”), 10–12 (“Neutral”), 13–15 (“Slightly satisfied”), 16–18 (“Satisfied”), and 19–21 (“Extremely satisfied”).
2.2.6 International Physical Activity Questionnaire Short Form
The International Physical Activity Questionnaire Short Form (IPAQ-SF) is a self-reported tool designed to quantify physical activity levels across various intensities, including vigorous, moderate, and walking activities, over the past 7 days. It calculates the total activity in MET-minutes per week (Metabolic Equivalent Task), where activities are classified into three levels: low activity (<1,500 MET-minutes/week), moderate activity (1,500–2,999 MET-minutes/week), and high activity (≥3,000 MET-minutes/week). The IPAQ-SF is widely used for evaluating physical activity patterns in diverse populations and supports both clinical assessments and research studies on physical activity and health outcomes (40, 41).
2.2.7 Short Social Participation Questionnaire-Lockdowns
The Short Social Participation Questionnaire (SSPQ) is a short modified version of the Social Participation Questionnaire (SPQ) designed to assess social participation behaviors during the last 12 months and previously validated and used during the COVID-19 home confinement period (38, 39). It includes 14 items, with 10 items rated on a 5-point scale from “never” to “all the time,” and 4 items requiring binary “yes” or “no” responses. The total score ranges from 14 to 70, with higher scores indicating greater levels of social participation. Scores are categorized as follows: 14 (“Never socially active”), 15–28 (“Rarely socially active”), 29–42 (“Sometimes socially active”), 43–56 (“Often socially active”), and 57–70 (“Socially active at all times”).
2.2.8 Short Technology-Use Questionnaire-Lockdowns
The Short Technology-Use Questionnaire-Lockdowns (STuQL) was developed to assess technology use for social participation, dietary practices, and physical activity. The questionnaire was previously validated and used during the COVID-19 home confinement period (38, 39). The questionnaire consists of three items rated on a 5-point scale ranging from “never” to “all the time.” Scores range from 3, indicating minimal technology use, to 15, indicating extensive use, with intermediate scores reflecting varying levels of engagement with technology.
2.2.9 The MedDiet Barriers Questionnaire
The MedDiet Barriers Questionnaire (MBQ) is a newly developed tool designed to assess barriers and limitations to adherence to the MedDiet. The questionnaire includes 13 items exploring the presence (answered as “Yes”) or absence (answered as “No”) of various potential barriers identified in the literature. Specifically, the MBQ addresses: (i) barriers related to food allergies and intolerances; (ii) barriers related to cultural and/or religious limitations; (iii) barriers related to medical or health-related limitations; (iv) barriers related to individual beliefs (e.g., vegan or vegetarian diets); (v) barriers related to taste dislike; (vi) barriers related to attitudes, such as suitability, taste, restrictiveness, or food waste concerns; (vii) barriers related to social norms (e.g., food culture); (viii) barriers related to low motivation; (ix) barriers related to price unaffordability; (x) barriers related to time or effort-consuming meal preparation; (xi) barriers related to low accessibility or availability of Mediterranean food; (xii) barriers related to lack of knowledge and cooking skills; and (xiii) other barriers. Responses are scored as “No” = 0 and “Yes” = 1, with the total score calculated as the sum of all items, ranging from 0 to 13. A score of 0 indicates the absence of barriers, while a score of 13 reflects severe barriers to adherence.
2.2.10 Additional data
Additional geo-demographic, socio-economic, and health-related data were collected, along with information on participants’ awareness of the MedDiet. Demographic variables included age, gender, marital status, education, employment, living environment, and ethnicity. Health status was categorized into healthy, at risk of disease, or living with diseases.
2.3 Statistical analysis
All analyses were performed using SPSS version 25. Descriptive statistics summarized the distribution of MedLife adherence categories across MC and NMC regions, with results expressed as respondents number as well as percentages of respondents within each region. A chi-square test of independence (χ2) was performed to assess the overall associations between regional and each categorical variable. Then, to assess whether the proportion of participants in each categorical variable differed significantly between regions, a Z-test for two proportions was conducted using the following pooled variance formula:
where:
• and are the observed proportions of a given category in the NMC and MC groups, respectively;
• (NMC: 1416) and (MC: 2594) represent the sample sizes for each region;
• is the pooled proportion, calculated as where and are the counts of participants in the category of interest for NMC and MC.
This test accounts for the imbalanced sample sizes between regions, with significance thresholds set at ∣Z∣ ≥ 1.96 (p < 0.05), ∣Z∣ ≥ 2.58 (p < 0.01), and ∣Z∣ ≥ 3.29 (p < 0.001). For continuous variables, the Shapiro–Wilk test confirmed non-normality, prompting the use of Mann–Whitney U tests. Effect sizes were reported using Cohen’s h for proportional differences (interpreted as: trivial ≤ 0.20; small > 0.20; medium > 0.50; large > 0.80) and Cohen’s d for mean comparisons, per Hopkins’ criteria. All tests were two-tailed with α = 0.05.
3 Results
3.1 Demographic characteristics of the participants
The demographic characteristics of the participants are presented in Table 1. Of the 4,010 participants, 2,594 (64.7%) resided in Mediterranean countries (MC), while 1,416 (35.3%) were from non-Mediterranean countries (NMC). Among NMC participants, 682 (48.2%) were from Asia, whereas MC participants were predominantly from Europe (n = 1,552, 58.7%) and Africa (n = 476, 18.4%) (p < 0.001).
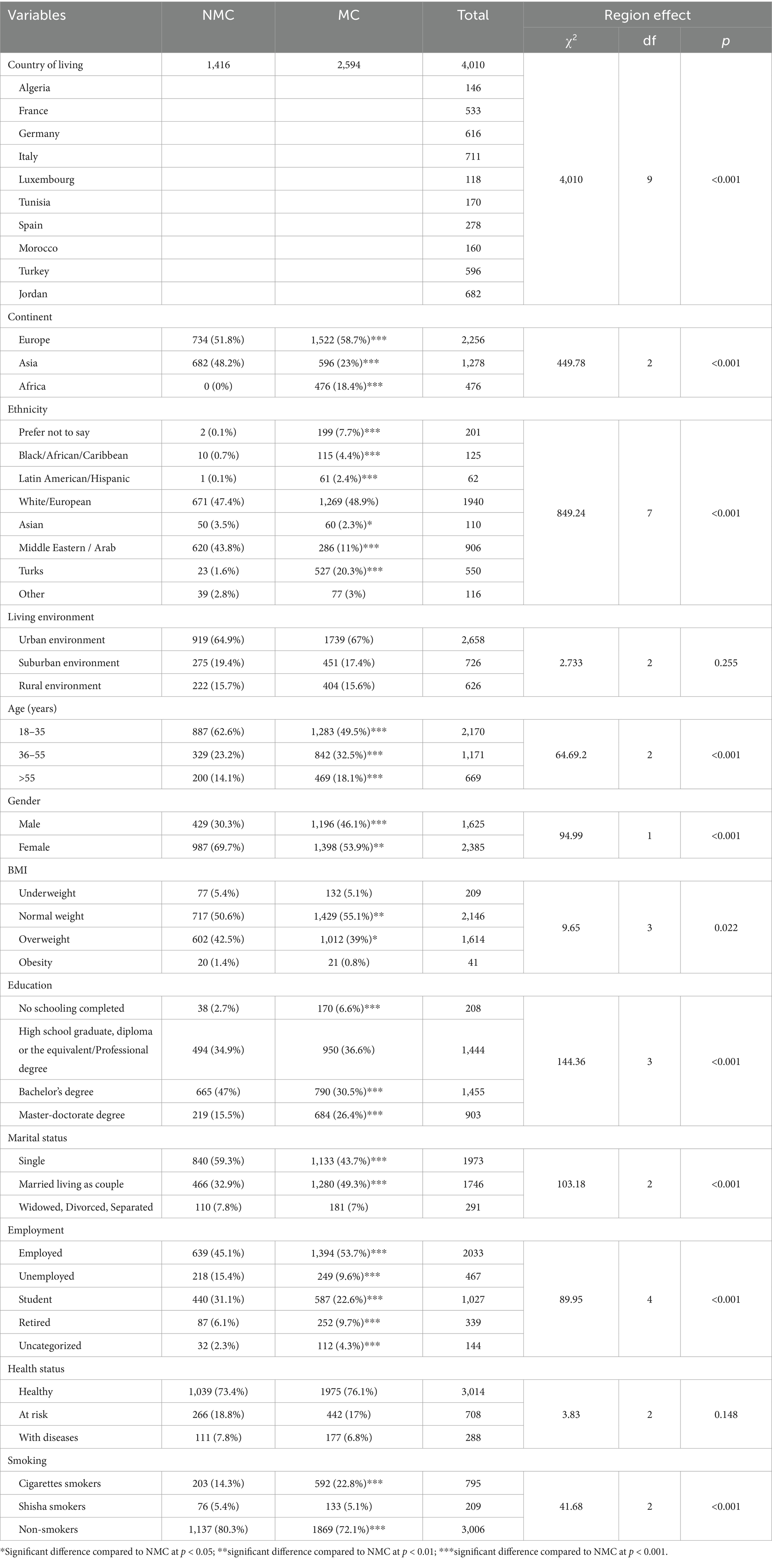
Table 1. Sociodemographic characteristics of the study population (n = 4,010) stratified by regions.
Ethnic background varied significantly across regions (p < 0.001), with only the white/European ethnic group being the largest group in both MC and NMC, showing comparable proportions (≈50%). Middle Eastern/Arab participants (43.8%) were significantly more represented in the NMC (p < 0.001), while Turkish participants (20.3%) were significantly more represented in the MC (p < 0.001).
The age and gender distribution revealed significant regional differences (p < 0.001), with younger individuals (18–35 years) and females representing the largest categories in both regions. However, the proportions were higher in the NMC compared to the MC (62.6% vs. 49.5% for younger individuals and 69.7% vs. 53.9% for females) (p < 0.001). BMI classification showed significant variation (p = 0.022), with normal weight being the most common category in both regions, where MC participants had a higher prevalence of normal weight (55.1% vs. 50.6%; p < 0.01) and a lower prevalence of overweight individuals (39% vs. 42.5%; p < 0.05).
Educational attainment differed significantly across regions (p < 0.001), with individuals holding bachelor’s degrees being more prominent in the NMC, showing a higher proportion than in the MC (47% vs. 30.5%). Conversely, a higher proportion of individuals with a master’s or doctorate degree was found in the MC (26.4% vs. 15.5%). Marital status also varied significantly (p < 0.001), with a greater proportion of single individuals in the NMC (59.3% vs. 51.5%) and more married or cohabiting individuals in the MC (49.3% vs. 32.9%; p < 0.001).
Employment status showed significant regional differences (p < 0.001). MC participants had higher employment (53.7% vs. 45.1%; p < 0.001) and retirement (9.7% vs. 6.1%; p < 0.001) rates, whereas NMC participants had a greater proportion of unemployed (15.4% vs. 9.6%; p < 0.001) and students (31.1% vs. 22.6%; p < 0.001) participants. Smoking behavior exhibited notable regional disparities (p < 0.001), with non-smokers presented higher proportion in NMC (80.3% vs. 72.1%; p < 0.001).
Living environment and health status showed comparable subgroup prevalences between MC and NMC, with no significant differences (p > 0.05).
3.2 Observational results for all parameters
3.2.1 MedLife Index and perceived barriers
The Mann–Whitney test revealed significant differences in total MedLife Index scores across regions (Z = 5.03, p < 0.001, Cohen’s d = 0.17), with MC participants scoring higher (mean = 14.2 ± 3.18) than NMC participants (mean = 13.66 ± 3.18) (Table 2).
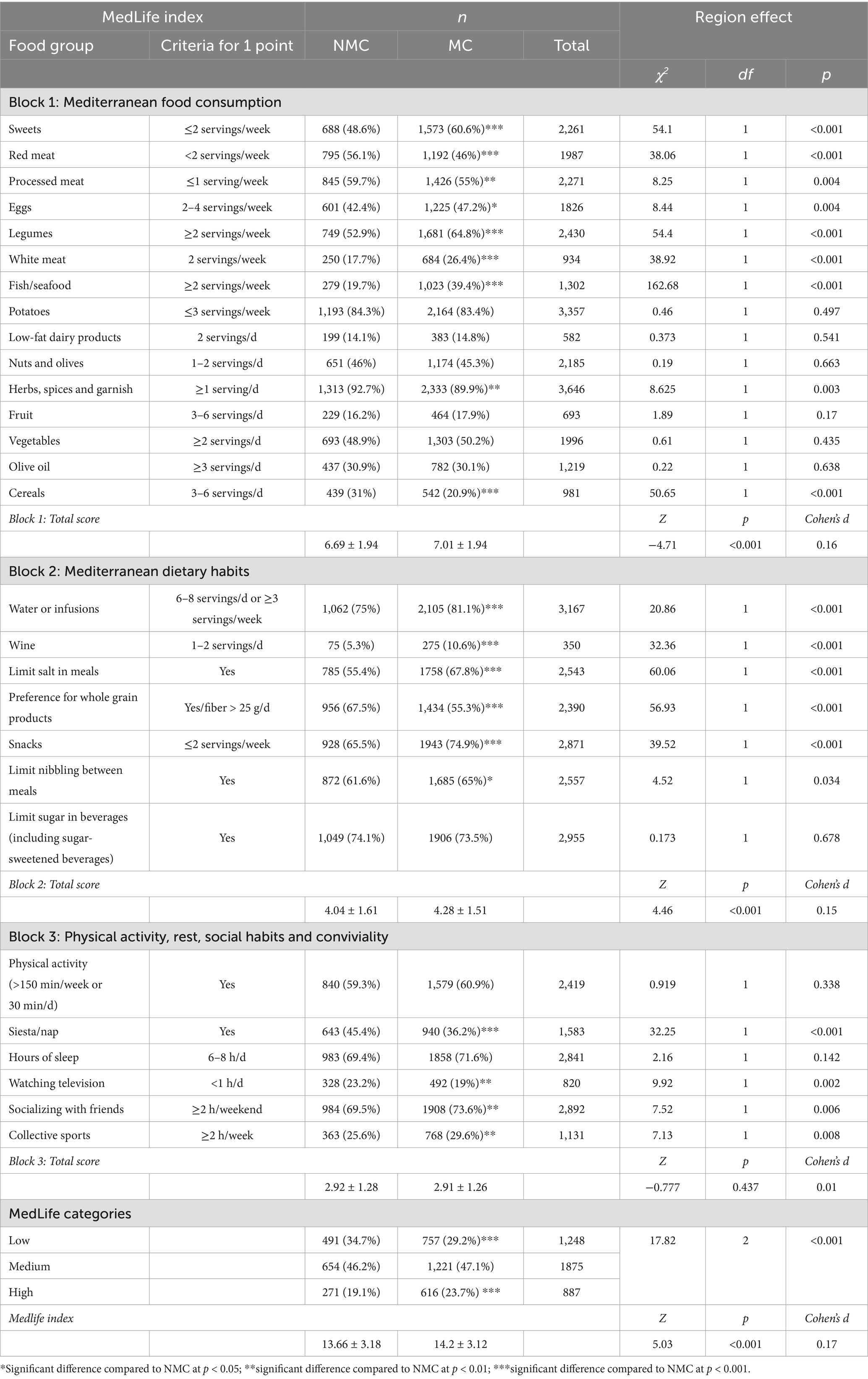
Table 2. Analysis of the MedLife Index: Mediterranean diet adherence, dietary habits, and consumption patterns by regions.
Participants in MC presented significantly higher scores in Block 1 (Mediterranean Food Consumption) (Z = −4.71, p < 0.001, Cohen’s d = 0.16), with greater adherence to recommended intake in key food groups: sweets (60.6% vs. 48.6%; p < 0.001), eggs (47.2% vs. 42.4%; p < 0.05), legumes (64.8% vs. 52.9%; p < 0.001), white meat (26.4% vs. 17.7%; p < 0.001), and fish/seafood (39.4% vs. 19.7%, p < 0.001). However, NMC reported higher adherence to recommended intake of red meat (56.1% vs. 46%; p < 0.001), processed meat (59.7% vs. 55%; p < 0.01), herbs, spices and garnish (92.7% vs. 89.9%; p < 0.01), and cereals (31% vs. 20.9%; p < 0.001).
Block 2 (Mediterranean Dietary Habits) showed significant regional differences (Z = 4.46, p < 0.001, Cohen’s d = 0.15) with higher scores in MC. MC participants presented higher proportions in water (81.1% vs. 75%; p < 0.001), wine (10.6% vs. 5.3%; p < 0.001), limited salt in meals (67.8% vs. 55.4%; p < 0.001), limited snacks (74.9% vs. 65.5%; p < 0.001) and limited nibbling between meals (65% vs. 61.6%; p < 0.05), while NMC participants reported stronger preference for whole grains (67.5% vs. 55.3% p < 0.001).
Block 3 (physical activity, rest, social habits, and conviviality) score did not significantly differ between MC and NMC (Z = −0.777, p = 0.437, Cohen’s d = 0.01). Looking at the individual items, the Z-test for two proportions showed significantly greater participation in socializing with friends and engaging in collective sports practices for MC participants (73.6% vs. 69.5% and 29.6% vs. 25.6%; p < 0.01 for both), while NMC participants demonstrated significantly greater participation in napping (45.4% vs. 36.2%; p < 0.001) and limiting television watching (23.2% vs. 19%; p < 0.01). Regarding the MedLife Index categories (low, medium, and high adherence), MC participants reported a lower proportion in the low adherence category (29.2% vs. 34.7%; p < 0.001) and a higher proportion in the high adherence category (23.7% vs. 19.1%; p < 0.001).
For perceived barriers, there was no significant difference between MC and NMC (Z = −0.93, p = 0.356, Cohen’s d = 0.06). However, the Z-test for two proportions revealed a higher proportion of barriers related to awareness (59.8% vs. 44.8%; p < 0.001), attitudes (83% vs. 79.7%; p < 0.05), price unaffordability (72.9% vs. 69.6%; p < 0.05), low accessibility (87.4% vs. 84.3%; p < 0.01), and individual beliefs (91.6% vs. 89.7%; p < 0.05) among MC participants. In contrast, a higher proportion of NMC participants reported barriers related to low motivation (19.3% vs. 16.4%; p < 0.05), time effort consumption (28.3% vs. 22.1%; p < 0.001), and lack of knowledge (20% vs. 17%; p < 0.05) (Table 3).
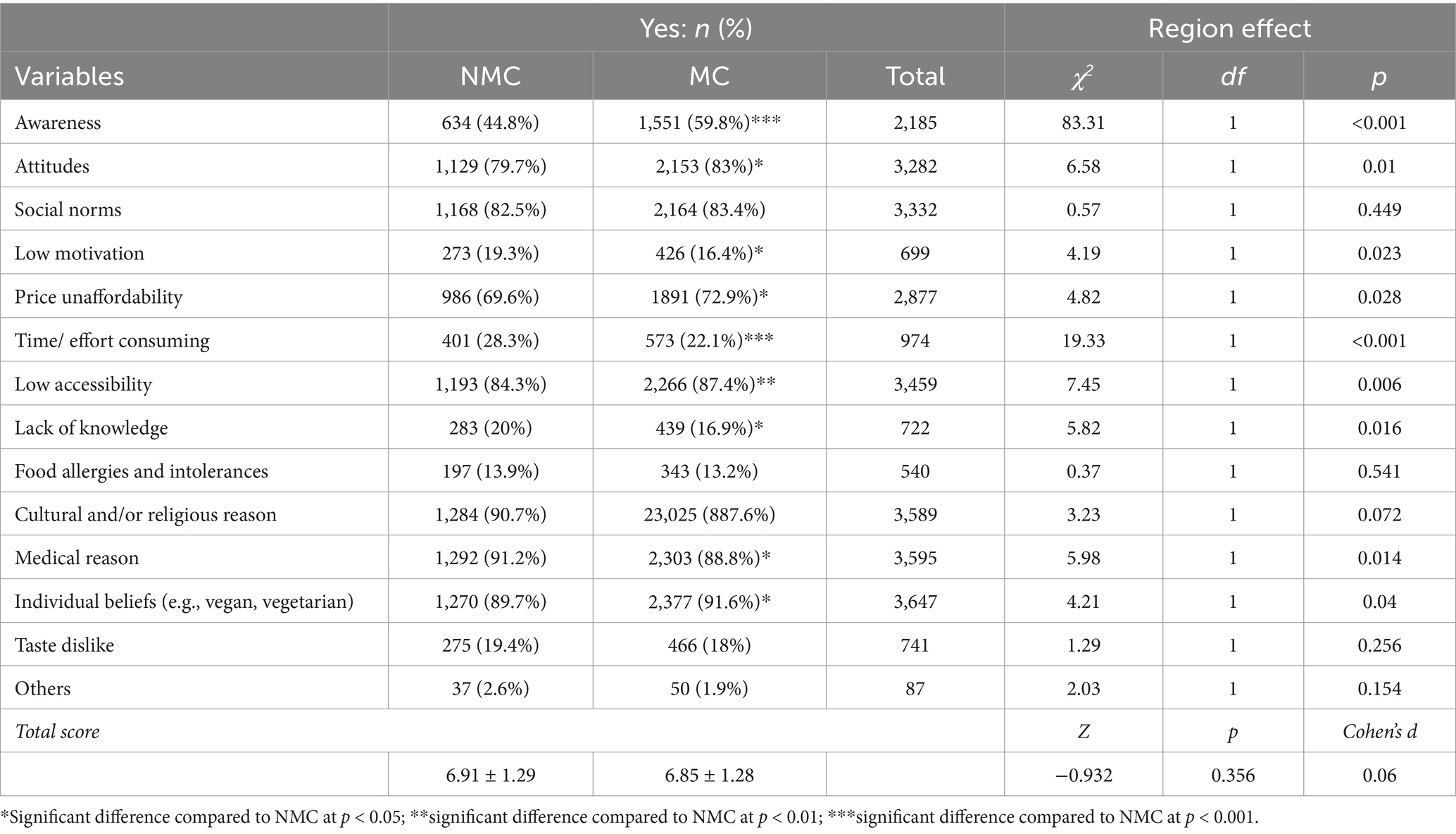
Table 3. Regions differences in awareness and potential barriers influencing their adherence to MedLife.
3.2.2 Physical and social activities, sleep patterns, and technology use behavior
There was no significant difference between regions in overall physical activity behavior (Z = 0.31, p = 0.758, Cohen’s d = 0.01), with the majority of participants from both regions (60–62%) primarily engaging in low physical activity. However, the Z-test for two proportions showed a higher proportion of participants engaging in moderate activities in MC compared to NMC (21.1% vs. 18.5%; p < 0.05). Regarding social participation behaviors, the majority of participants from both regions were classified as “sometimes socially active,” with a higher proportion in MC (52.2%) compared to NMC (48.1%). In contrast, NMC showed a significantly higher proportion, albeit small, of individuals categorized as “always socially active” (5.9%) compared to MC (3.2%). Overall, the SSPQ score was slightly higher in NMC compared to MC (Z = −2.48, p = 0.013, Cohen’s d = 0.1) (Table 4).
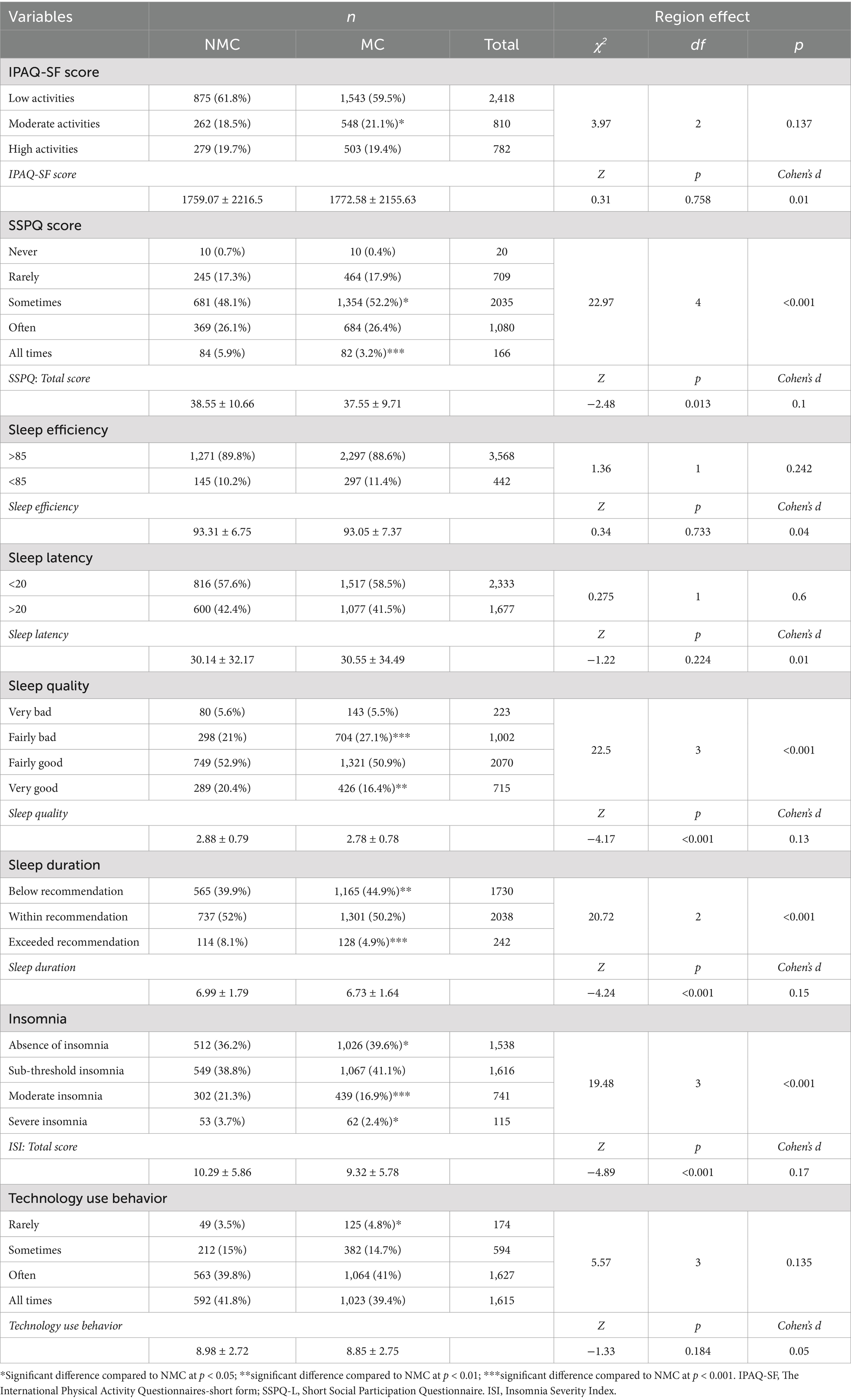
Table 4. Behavioral and sleep outcomes by regions.
Regarding sleep patterns, no significant differences were found in sleep efficiency (Z = 0.34, p = 0.733, Cohen’s d = 0.04) and sleep latency (Z = −1.22, p = 0.224, Cohen’s d = 0.01). However, sleep quality was significantly lower in MC (Z = −4.17, p < 0.001, Cohen’s d = 0.13), with MC participants reporting higher proportions of “Fairly bad” sleep quality (27.1% vs. 21%; p < 0.001) and lower proportions of “Very good” sleep quality (16.4% vs. 20.4%; p < 0.01) compared to NMC. Additionally, MC had significantly lower sleep duration (Z = −4.24; p < 0.001; Cohen’s d = 0.15), with a higher proportion of participants reporting sleep durations below the recommended amount (44.9% vs. 39.9%; p < 0.01) and a lower proportion exceeding the recommended sleep duration (4.9% vs. 8.1%; p < 0.001). Regarding insomnia, MC had a lower insomnia score (Z = −4.89; p < 0.001; Cohen’s d = 0.17), with a greater proportion reporting no insomnia (39.6% vs. 36.2%; p < 0.05). In contrast, NMC participants showed higher proportions of moderate and severe insomnia (21.3% vs. 16.9% and 3.7% vs. 2.4%; p < 0.001 and p < 0.05, respectively).
There was no significant regional effect on technology use behavior scores (Z = −1.33, p = 0.184, Cohen’s d = 0.01), with the majority of participants from both regions reporting frequent (often) to constant (all times) technology use (≈80%).
3.2.3 Life satisfaction, mental health (DASS-21), and the need for psychosocial, physical, and nutritional support
There were no significant regional differences in terms of life satisfaction, depression, anxiety, and stress (p > 0.05). However, it should be noted that the highest proportion in both regions were declaring moderate depression and anxiety (33–35%) (Table 5).
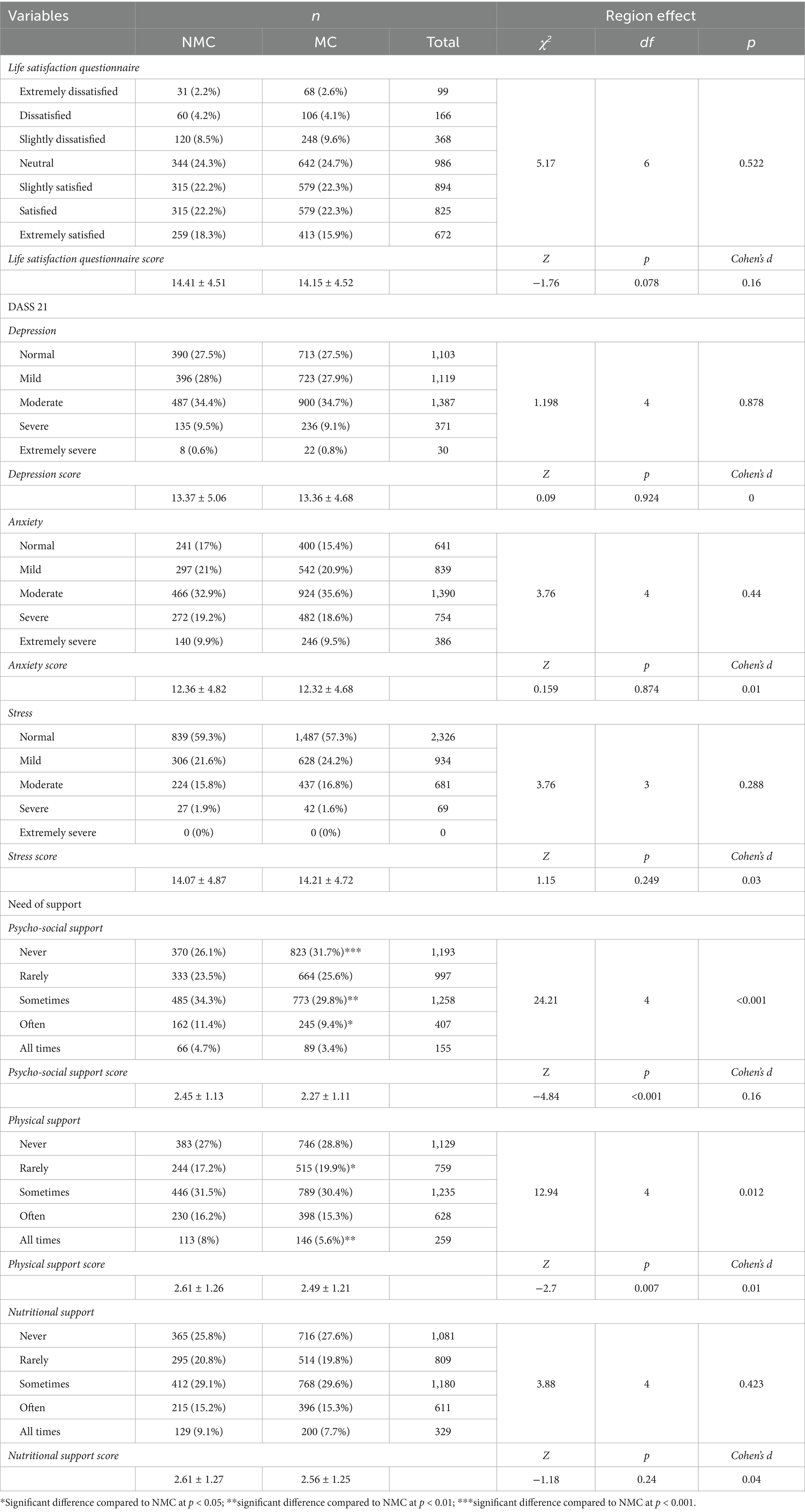
Table 5. Assessment of life satisfaction, mental health (DASS-21), and the demand for psychosocial, physical, and nutritional support.
Regarding the need for support, NMC participants reported a significantly greater demand for psychosocial (Z = −4.84, p < 0.001, Cohen’s d = 0.16) and physical (Z = −2.7 p = 0.007, Cohen’s d = 0.01) supports. In psychosocial support NMC reported a significantly lower proportion for “Never” (26.1%vs. 31.7%; p < 0.001) and significantly higher proportion for “Sometimes” (34.3% vs. 29.8%; p < 0.01) and “Often” (11.4% vs. 9.4%; p < 0.05). Similarly for physical support, NMC presented significantly lower significant proportions for “Rarely” (17.2%vs. 19.9%; p < 0.05) and higher proportion for “All times” (8% vs. 5.6%; p < 0.01).
4 Discussion
The present study aims to evaluate regional variations in MedDiet adherence by analyzing socio-demographic and lifestyle factors across MC and NMC regions. The main findings highlight regional differences in adherence to the MedDiet and its associations with physical and mental health across MC and NMC regions. While MC participants showed greater adherence to traditional MedDiet components such as legumes and fish, NMC participants focused more on whole grains and modern adaptations of the diet. Distinct yet overlapping barriers to MedDiet adherence were identified across regions, with MC participants faced economic and accessibility challenges, while NMC participants struggled with knowledge gaps, behavioral hurdles, and time constraints. No significant differences in overall physical activity were observed, although MC participants engaged more in moderate physical activities and social participation. Sleep patterns varied, with MC participants reporting poorer sleep quality and shorter sleep duration compared to NMC. Mental health symptoms, particularly depression and anxiety, were moderate in both regions, likely reflecting global trends in mental health following the COVID-19 pandemic.
4.1 Demographic characteristics
The demographic differences observed between the MC and NMC populations are consistent with established regional patterns in various studies. Our findings reveal significant differences in age distribution, gender, BMI, educational attainment, marital status, and employment patterns between the two regions. These differences align with previous research, including that of Obeid et al. (26), who observed distinct demographic trends between Mediterranean and non-Mediterranean regions, including variations in education levels and employment patterns. The greater representation of MC participants from Europe and Africa, compared to the predominantly Asian background of NMC participants, reflects both geographic proximity to the Mediterranean Sea and historical definitions of Mediterranean populations. These definitions traditionally include regions with shared cultural and agricultural practices, particularly olive cultivation across the Mediterranean basin (26, 42). The higher proportion of younger individuals (18–35 years) and females in the NMC cohort contrasts with trends typically reported in Mediterranean populations, where younger demographics often dominate due to higher birth rates and delayed transitions to adulthood (43). However, our findings align with demographic studies highlighting a younger population in non-Mediterranean regions, as well as with global trends where females in these regions are more likely to participate in higher education and the workforce, particularly in Western and Central Europe (44, 45). The present findings suggest that the NMC’s younger demographic may be influenced by selective migration, where younger individuals relocate for education or employment opportunities—a phenomenon well-documented in high-income European nations like Germany and Luxembourg (46). This hypothesis is supported by the high proportion of students and employees in the NMC region studied, compared to the MC. A pattern which may reflect national policies prioritizing access to tertiary education, aimed at improving workforce competitiveness and fostering economic development (43). The greater proportion of single individuals in the NMC further supports this notion, as delayed marriage is often linked to urbanization and economic mobility (47). Conversely, the MC’s higher rate of married/cohabiting individuals aligns with cultural norms that prioritize familial ties, particularly in North African and Southern European societies (48). In contrast, in non-Mediterranean countries, particularly in Western societies, there is a trend toward later marriage and a greater acceptance of non-traditional living arrangements (49).
Regarding the educational and employment disparities, the NMC’s higher bachelor’s degree attainment contrasts with the MC’s greater proportion of master/doctoral degrees. These disparities reveal distinct socioeconomic strategies. The NMC’s higher bachelor’s degree attainment reflects policy emphasis on workforce-ready education, where countries like Germany and Luxembourg have aligned undergraduate programs with industrial demands through dual education systems (50). Conversely, the MC’s greater proportion of advanced degrees signals an adaptive response to economic challenges—graduate education expansion in countries like Spain and Italy functions both as a buffer against youth unemployment (reaching 27.2% in Mediterranean EU nations in 2023) and a mechanism to enhance competitiveness in knowledge-based sectors (43, 51). This educational divergence is mirrored in employment patterns: the MC’s higher employment rate reflects economic necessity driving earlier workforce entry, particularly in service and agricultural sectors where education-occupation mismatches are prevalent (52). Meanwhile, the NMC’s larger student population and higher retirement rates illustrate the demographic and economic privilege of extended education in aging, high-income societies (53, 54). These trends suggest that while NMC regions optimize education for immediate labor market integration, MC nations employ advanced education as both an economic adaptation strategy and social stabilizer amidst unemployment crises.
The observed differences in body weight profiles between Mediterranean (MC) and non-Mediterranean (NMC) populations reflect both persistent dietary advantages and concerning behavioral trends. The MC’s higher prevalence of normal-weight individuals (55.1% vs. 50.6%; p < 0.01) and lower overweight rates (39% vs. 42.5%; p < 0.05) confirm the enduring protective effects of traditional Mediterranean dietary patterns, characterized by high consumption of olive oil, fish, and plant-based foods (42, 55). However, the narrowing gap suggests nutritional transition, where globalization has increased processed food consumption in MC regions by approximately 27% since 2010, diluting the diet’s protective effects (56). This dietary convergence is particularly evident among younger MC cohorts, who show BMI trends approaching NMC levels. The NMC’s significantly higher smoking abstinence (80.3% vs. 72.1%; p < 0.001) demonstrates the success of comprehensive tobacco control policies in countries like Germany, where smoke-free legislation and advertising bans reduced smoking prevalence by 35% between 2005 and 2020 (57, 58). Conversely, the MC’s persistent tobacco use reflects both the cultural entrenchment of shisha in social practices—with 42% of Lebanese and 28% of Tunisian adults reporting regular use (59, 60)—and slower implementation of WHO Framework Convention on Tobacco Control measures in Mediterranean nations. These findings highlight the need for culturally adapted public health strategies that address both emerging nutritional challenges and traditional risk behaviors. The living environment and health status did not show significant regional differences, suggesting that similarities exist between the studied Mediterranean and non-Mediterranean countries in terms of environmental stressors and access to healthcare.
4.2 Mediterranean diet and lifestyle adherence and perceived barriers
The regional disparities in MedLife Index scores highlight greater adherence to the Mediterranean diet (MedDiet) and lifestyle among participants from Mediterranean countries (MC) compared to those from non-Mediterranean countries (NMC), reflecting enduring cultural dietary patterns. These findings align with previous research, which has shown that Mediterranean populations are more likely to adhere to the principles of the MedDiet (26, 42). However, these disparities also suggest cultural and economic influences in NMC regions, where access to fresh, healthy Mediterranean foods may be limited or more expensive, leading to a greater reliance on processed foods (61, 62). It is important to note that the modest Cohen’s d value (0.17) for differences in the MedLife Index, despite statistical significance, indicates that while traditional dietary patterns persist in MC regions, their distinctiveness is eroding, likely due to globalization-driven homogenization of food systems (63). While MC populations continue to show higher adherence to core MedDiet elements like fish and legumes, the rise of processed foods and shifting agricultural economies have reduced the historical gaps. This convergence is particularly evident among younger cohorts in MC regions, whose snacking behaviors (with only 65% limiting nibbling) now reflect globalized eating patterns (64).
The regional variations in specific food groups shown in the present findings further support these suggestions. Indeed, MC participants showed superior adherence to traditional MedDiet pillars, including (i) plant-based proteins with higher legume consumption, aligning with the MedDiet’s emphasis on pulses as primary protein sources (42); (ii) lean animal proteins, with greater adherence to fish/seafood and white meat recommendations, consistent with coastal dietary traditions (65); and (iii) sugar moderation, with lower sweets intake, reflecting cultural preferences for fresh fruits as desserts (66). In contrast, NMC participants demonstrated stronger adherence to modern MedDiet adaptations, including (i) meat moderation, with better compliance with limiting red and processed meat, likely influenced by Northern European public health campaigns (67); (ii) whole grains and herbs, with higher cereal and herb/spice use, which align with the MedDiet’s plant-centric ethos and locally available ingredients (68). This dichotomy suggests that while MC regions preserve traditional MedDiet practices rooted in local food systems, they face challenges in adopting newer evidence-based recommendations, such as the reduction of red meat consumption. Conversely, NMC regions appear to adopt MedDiet principles selectively, emphasizing aspects that are compatible with their food environments (e.g., whole grains over seafood), demonstrating the diet’s adaptability beyond its geographic origins (69).
Regarding Mediterranean dietary habits, MC participants scored significantly higher in several categories, including water and wine consumption, and limiting salt intake in meals. These findings reflect the lifestyle choices typically associated with the Mediterranean region, where hydration, moderate alcohol consumption, and low sodium intake are common components of the traditional diet (70). On the other hand, NMC participants reported a stronger preference for whole grains, which aligns with global trends of increasing whole grain consumption in response to growing health awareness (71). However, the higher adherence to whole grains in NMC compared to MC could also be influenced by the broader availability and cultural acceptance of whole grains in non-Mediterranean regions.
The absence of significant regional differences in overall Block 3 scores suggests growing global lifestyle homogenization, yet nuanced behavioral patterns persist. MC participants maintained stronger engagement in culturally rooted social practices, demonstrating higher rates of both socializing with friends and collective sports participation. These findings align with traditional Mediterranean lifestyle models emphasizing communal physical activity and face-to-face interaction as integral to wellbeing (65, 72). The preservation of these practices likely reflects deeper cultural values prioritizing social cohesion, even amidst dietary transitions (64). Conversely, NMC participants exhibited distinct compensatory behaviors: more frequent napping and stricter television time management. While these patterns may initially appear contradictory, they potentially represent adaptive responses to Northern Europe’s productivity-oriented cultures—where napping serves as a stress-regulation strategy in high-demand work environments (73), and conscious screen limitation counters sedentary office lifestyles (74). The MC’s comparatively lower TV restriction may paradoxically reflect stronger outdoor leisure traditions reducing screen dependence (75). These findings collectively suggest that while globalization has diminished overt lifestyle disparities (evidenced by comparable Block 3 scores), region-specific coping mechanisms and cultural priorities continue to shape health behaviors in subtle but meaningful ways. This has important implications for public health strategies, suggesting that MedDiet interventions should leverage existing social networks to reinforce dietary changes through community-based programs in MC contexts and compensatory behaviors like napping as potential gateways to broader lifestyle modification in NMC contexts.
The analysis of perceived barriers reveals distinct yet overlapping obstacles to MedDiet adoption across regions. While no significant difference emerged in overall barrier perception, MC participants faced more pronounced structural challenges. Economic constraints (i.e., price unaffordability) were particularly salient, reflecting inflationary pressures on traditional foods like olive oil and fish most probably in Southern Europe (76). Accessibility barriers were also more prevalent in MC, likely due to urban food deserts limiting fresh produce availability in rapidly modernizing cities (77). Cultural factors further complicated adherence, as 91.6% of MC participants reported belief-related barriers, mirroring generational shifts toward convenience foods despite strong dietary traditions (64). These findings align with prior research showing that even in Mediterranean countries, socioeconomic factors increasingly undermine dietary quality (78). In contrast, NMC participants encountered primarily knowledge-and behavior-related hurdles, suggesting limited familiarity with MedDiet principles in regions without cultural exposure to this eating pattern (71). Practical implementation challenges were equally significant, with time constraints and motivation deficits reflecting the demands of Northern Europe’s fast-paced work culture (74). These behavioral barriers align with the theory of planned behavior, which identifies intention and perceived control as critical factors in dietary adoption (79). Together with knowledge gaps, these obstacles create a dual challenge for NMC populations: comprehending MedDiet principles while adapting them to incompatible lifestyles. Despite these regional differences, the high prevalence of accessibility and belief barriers in both groups (exceeding 84% overall) signals universal challenges in contemporary food environments. The persistence of such obstacles, even in traditional MedDiet heartlands, highlights the need for targeted interventions: price stabilization and retail access improvements in MC regions, paired with education and behavior-change strategies in NMC contexts. Future research should explore how these barriers interact with demographic factors like income and urbanization to better inform policy solutions.
4.3 Physical and social activities, sleep patterns, and technology use behavior
Although MC participants exhibited greater engagement in lifestyle-integrated physical activities—such as walking, household chores, and active socializing, as assessed by Block 3 of the MedLife Index—this did not translate into higher overall physical activity levels. Data from the more comprehensive IPAQ questionnaire, which measures total physical activity, including structured exercise, occupational movement, and recreational activities, revealed the absence of significant differences in overall physical activity levels between regions, with 60–62% of participants in both areas engaging in low activity, underscores a global trend more in gavour of sedentarization that transcends cultural boundaries (80). However, the higher proportion of moderate activity in MC suggests residual cultural practices of lifestyle-embedded movement—such as walking for transportation or social purposes—that persist despite broader activity declines (65). This aligns with the Mediterranean lifestyle model that traditionally integrates physical activity into daily routines rather than structured exercise (42), though its protective effects may be weakening in contemporary urban environments.
Regarding the social participation patterns the present findings report a cultural paradox. While MC maintained higher proportions of “sometimes socially active” individuals, NMC showed greater representation in the “always socially active” category and higher SSPQ scores (Cohen’s d = 0.1). This likely reflects divergent social models—MC’s informal, frequent interactions versus NMC’s more organized but less frequent engagements (81). The Mediterranean pattern of sustained but variable social connectivity may derive from cultural norms prioritizing familial and community bonds (64), whereas Northern European societies may favor scheduled social commitments within individualistic frameworks (82). Similarly, sleep analyses uncovered clinically relevant contrasts. Indeed, despite equivalent sleep efficiency and latency, MC participants reported poorer sleep quality and shorter duration, with 45% sleeping below recommended levels versus 40% in NMC. These findings implicate cultural factors like late-night dining (83) and evening-oriented social rhythms (84) as potential contributors. Paradoxically, NMC showed higher insomnia rates (moderate/severe: 25% vs. 19.3%), suggesting that while Mediterranean lifestyles may disrupt sleep quantity, Northern European work cultures might exacerbate sleep disorders through productivity-related stress (73). This dissociation between subjective sleep quality and clinical insomnia warrants further investigation into cultural perceptions of sleep health (85).
Technology use showed striking homogeneity, with ≈80% of both groups reporting frequent-to-constant engagement. This universal digital saturation reflects technology’s role as a cultural equalizer, potentially eroding traditional lifestyle distinctions while creating new health challenges (86). The lack of regional differences contradicts assumptions about the Mediterranean “digital lag” and underscores technology’s pervasive influence on modern lifestyles.
4.4 Life satisfaction, mental health (DASS-21), and the need for psychosocial, physical, and nutritional support
Our findings challenge the traditional idea that mental health issues are significantly different across regions. We found no significant differences in life satisfaction, depression, anxiety, or stress between participants from MC and NMC. In both regions, about 33–35% of people reported moderate symptoms, which reflects global trends in mental health after the COVID-19 pandemic, where mental health issues have become widespread across different economic contexts (87). These findings contradict earlier studies that suggested Mediterranean populations suffer from worse mental health due to economic instability (88). This discrepancy could be due to differences in research methods when applying mental health assessments across cultures (89), or perhaps the increasing globalization is contributing to similar levels of psychological distress worldwide due to common digital and economic challenges (90). The present findings suggest that traditional risk factors for mental health, like economic difficulties (26), may be counterbalanced by cultural factors such as strong family support networks (48). Alternatively, it may indicate that economic measures no longer reflect individual psychological well-being in modern welfare states (91).
Surprisingly, participants from the studied NMC in the present study (suggested to have low economic challenges) reported a significantly greater need for both psychosocial and physical support compared to MC. This difference likely reflects three factors: (i) NMC countries have established systems for seeking help, where robust social welfare programs (like Germany’s Pflegeversicherung) make it normal to request support (92); (ii) in MC regions, people tend to rely on informal family support networks, reducing the need for formal assistance (93); and (iii) NMC countries have older populations, which creates more demand for physical care (43). The lower demand for support in MC regions might also reflect underreporting due to stigma—a common issue in collectivist societies, where acknowledging a need for help can risk family honor (94). These findings call for a reassessment of the “Mediterranean paradox,” which suggests that despite economic hardship, Mediterranean countries often show lower formal support utilization. Instead of viewing this as a sign of resilience, it may reflect cultural resourcefulness—where people rely on family and community networks rather than formal services (95). This finding highlights the need to understand cultural contexts better when evaluating support systems and mental health in different regions.
4.5 Public health implications
Our findings reveal both the resilience of traditional health behaviors and the growing pressures of modernization across Mediterranean (MC) and non-Mediterranean (NMC) regions. These insights point to three critical pathways for public health action that balance cultural preservation with contemporary adaptation.
4.5.1 Region-specific dietary preservation and promotion
The study’s most urgent policy imperative lies in safeguarding Mediterranean dietary traditions while making them accessible in modern contexts. For MC regions, this requires dual interventions: economic support for traditional food systems through agricultural subsidies (particularly for olive oil, fish, and legumes under CAP reforms) paired with urban planning regulations to combat food deserts (96). Successful models like Barcelona’s “Eat Mediterranean” program demonstrate how municipal kitchens can deliver affordable MedDiet meals while creating local employment (97). Simultaneously, digital platforms could reinvigorate cultural pride in traditional diets among younger generations—Spain’s “Mediterranean Diet Virtual Museum” shows how gamification can make heritage appealing to digital-native youth (98).
In NMC regions, adoption strategies must address the knowledge-motivation gap through behavioral “nudge” techniques. German workplace trials where cafeterias positioned Mediterranean options at eye-level increased selection by 38% without restricting choice (99). Supermarket partnerships could extend this approach through ready-to-cook MedDiet meal kits, addressing time barriers identified in our study. Primary care systems in Northern Europe should integrate dietitian referrals—following the UK’s “Social Prescribing” model that links clinical care with community cooking classes (100).
4.5.2 Mental health system innovation
The paradox of higher formal support requests in NMC despite comparable mental health metrics suggests systemic inefficiencies in addressing mild-to-moderate cases. Stepped-care models piloted in the Netherlands—where digital CBT precedes specialist referral—reduced treatment delays by 60% while maintaining outcomes (101). These could be adapted to Mediterranean contexts by training community health workers as “culture brokers” who connect formal services with existing familial support networks, as successfully trialed in southern Italy’s “Mental Health Bridges” program (102).
4.5.3 Lifestyle integration and digital integration
The universal physical activity decline and technology saturation demand reimagining healthy living in digital societies. Urban design must prioritize “movement-friendly” environments: Barcelona’s “superblocks” initiative increased neighborhood walking by 22% through traffic calming (103), while Copenhagen’s bicycle infrastructure serves as a model for active commuting. For screen-dominated lifestyles, app-based interventions like Greece’s “MedMove” demonstrate how smartphone reminders can convert sedentary time into micro-activity breaks without requiring gym access (104).
By anchoring interventions in cultural strengths while addressing modernization’s challenges, policymakers can develop sustainable approaches to health promotion that respect regional identities while meeting global health targets. The Mediterranean diet’s evolutionary history—adapting over millennia while retaining core principles—offers a powerful metaphor for this balanced approach to 21st century public health.
4.6 Limitations
This study possesses multiple strengths, including its multinational design and diverse population (N = 4,010), which enhance the generalizability of findings across cultural contexts. The use of validated assessment tools provides a comprehensive evaluation of demographic, behavioral, and psychosocial factors influencing MedDiet adherence. However, several limitations warrant discussion. First, the online recruitment method, while enabling efficient multinational data collection, may have favored participation from more health-conscious, urban, and technologically adept populations, particularly underrepresenting older adults and rural residents. Furthermore, the sample size disparity between Mediterranean (MC: n = 2,594, 64.7%) and non-Mediterranean (NMC: n = 1,416, 35.3%) groups represent a significant limitation. While we employed robust statistical methods such as the proportional analyses (focusing on relative distributions (%) rather than absolute counts) and Z-tests for two proportions that explicitly account for unequal group sizes through pooled variance estimation, the imbalance may still reduce precision for detecting small effect size in NMC subgroups. Future studies should prioritize balanced recruitment across regions while maintaining proportional analytical approaches to optimize comparability. Second, cross-sectional design inherently limits causal interpretation of the observed associations between MedDiet adherence and health outcomes. While our findings identify important regional patterns, they cannot establish temporal relationships or directionality. Longitudinal or intervention studies would be valuable to confirm whether improved MedDiet adherence leads to better health outcomes across different cultural contexts. Third, reliance on self-reported data introduces potential measurement biases, including recall bias (particularly for dietary assessments) and social desirability bias. Although we used validated instruments (MedLife Index, IPAQ-SF), the subjective nature of these measures may have affected accuracy. Incorporating objective measures such as biomarkers of dietary intake or device-based physical activity monitoring in future research would strengthen the evidence. Fourth, while we examined numerous covariates, unmeasured confounders may have influenced our results. For instance, variations in local food policies, agricultural practices, or genetic predispositions across regions could affect both dietary patterns and health outcomes but were not accounted for in our analyses. Additionally, the study did not assess potential mediators (e.g., food insecurity, cultural identity) that might explain regional differences in MedDiet adherence. Fifth, our country-level grouping (MC vs. NMC) may have masked important within-region heterogeneity. For example, significant cultural and socioeconomic differences exist between Southern European (e.g., Spain, Italy) and North African (e.g., Tunisia, Morocco) Mediterranean countries that were not explored in depth. Similarly, non-Mediterranean countries like Germany and Luxembourg may differ substantially in food environments and health policies. Future research with larger samples could examine these subgroups separately to identify more nuanced patterns. Finally, the study’s recruitment methods, primarily through online platforms and social networks, may have introduced selection bias toward more health-conscious or technologically adept populations. This could limit the generalizability of findings to broader populations, particularly in regions with lower internet penetration or among older adults less likely to participate in online surveys.
5 Conclusion
This multinational study reveals both persistent cultural patterns and converging trends in MedDiet and lifestyle adherence across MC and NMC regions. While significant differences persist in dietary practices—with MC populations maintaining stronger traditional food consumption but facing erosion from processed foods, and NMC regions selectively adopting MedDiet components—our findings demonstrate surprising similarities in mental health outcomes and physical activity levels. These results underscore how globalization is reshaping health behaviors while cultural resilience preserves key dietary distinctions. These findings suggest that public health strategies must be tailored to each region’s cultural, economic, and environmental contexts, promoting MedDiet adherence while addressing barriers such as economic constraints, lifestyle incompatibility, and psychological support needs. Future research should explore the complex relationships between diet, physical activity, mental health, and social support, while also examining the influence of cultural and socio-economic factors on dietary behaviors. This will help develop tailored interventions that address region-specific challenges, considering the role of digital tools in shaping health outcomes. By respecting regional identities while addressing shared modern challenges—from economic pressures to digital lifestyle shifts—public health strategies can preserve the MedDiet’s proven benefits while ensuring its relevance in modern society.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available at this time as further analyses are ongoing, and additional publications based on these data are in preparation. Data may be made available upon reasonable request to the corresponding author once all planned analyses and publications are completed.
Author contributions
MB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. AcA: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. AS: Conceptualization, Data curation, Formal analysis, Investigation, Validation, Visualization, Writing – review & editing. MK: Conceptualization, Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. KT: Conceptualization, Data curation, Investigation, Methodology, Resources, Validation, Visualization, Writing – review & editing. BB: Conceptualization, Data curation, Investigation, Methodology, Resources, Validation, Visualization, Writing – review & editing. LM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. JH: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. CS: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. GM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. HG: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AdA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. BO: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. GG: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. OA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. TD: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. KA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. PZ: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. FD: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. NB: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. CP: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. LR: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AG: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. MC-O: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AC: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. NF: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. CM: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. EV: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. BL: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. SF: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. AB: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. E-MA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. EA: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. MO: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. SL: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. TK: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. NS: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. OB: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. HJ: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. WH: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. EF-T: Data curation, Investigation, Resources, Validation, Visualization, Writing – review & editing. WM: Data curation, Investigation, Resources, Supervision, Validation, Visualization, Writing – review & editing. HC: Data curation, Investigation, Methodology, Resources, Validation, Visualization, Writing – review & editing. WS: Data curation, Investigation, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work is part of the MEDDIET4ALL PRIMA PROJECT, supported by the European Union (Section 2-Multi-topic 2022, thematic Area 3—Food Value Chain, Topic 2.3.1–202-RIA) and multiple national organizations, including the Federal Ministry of Education and Research (BMBF) (grant no. 02WPM1681) and the national research agencies in France (ANR) (grant no. ANR-23-P012-0008-04).
Acknowledgments
We sincerely thank all MEDIET4ALL project collaborators for their valuable contributions to this study.
Conflict of interest
BL and SF were employed by Microtarians SIS, Société d’impact societal.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Afshin, A, Sur, PJ, Fay, KA, Cornaby, L, Ferrara, G, Salama, JS, et al. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2019) 393:1958–72. doi: 10.1016/S0140-6736(19)30041-8
2. Srour, B, and Touvier, M. Ultra-processed foods and human health: what do we already know and what will further research tell us? EClinicalMedicine. (2021) 32:100747. doi: 10.1016/j.eclinm.2021.100747
3. Silva Meneguelli, T, Viana Hinkelmann, J, Hermsdorff, HHM, Zulet, MÁ, Martínez, JA, and Bressan, J. Food consumption by degree of processing and cardiometabolic risk: a systematic review. Int J Food Sci Nutr. (2020) 71:678–92. doi: 10.1080/09637486.2020.1725961
4. Godos, J, Scazzina, F, Paternò Castello, C, Giampieri, F, Quiles, JL, Briones Urbano, M, et al. Underrated aspects of a true Mediterranean diet: understanding traditional features for worldwide application of a "Planeterranean" diet. J Transl Med. (2024) 22:294. doi: 10.1186/s12967-024-05095-w
5. Sikalidis, AK, Kelleher, AH, and Kristo, AS. Mediterranean diet In: Encyclopedia (2021). 1:371–87. doi: 10.3390/encyclopedia1020031
6. Martínez-González, M, Hershey, M, Zazpe, I, and Trichopoulou, A. Transferability of the Mediterranean diet to non-Mediterranean countries: what is and what is not the Mediterranean diet. Nutrients. (2017) 9:1226. doi: 10.3390/nu9111226
7. Lotfi, K, Saneei, P, Hajhashemy, Z, and Esmaillzadeh, A. Adherence to the Mediterranean diet, five-year weight change, and risk of overweight and obesity: a systematic review and dose–response meta-analysis of prospective cohort studies. Adv Nutr. (2022) 13:152–66. doi: 10.1093/advances/nmab092
8. Nissensohn, M, Román-Viñas, B, Sánchez-Villegas, A, Piscopo, S, and Serra-Majem, L. The effect of the Mediterranean diet on hypertension: a systematic review and meta-analysis. J Nutr Educ Behav. (2016) 48:42–53.e1. doi: 10.1016/j.jneb.2015.08.023
9. Schwingshackl, L, Missbach, B, König, J, and Hoffmann, G. Adherence to a Mediterranean diet and risk of diabetes: a systematic review and meta-analysis. Public Health Nutr. (2015) 18:1292–9. doi: 10.1017/S1368980014001542
10. Esposito, K, Kastorini, C-M, Panagiotakos, DB, and Giugliano, D. Mediterranean diet and metabolic syndrome: an updated systematic review. Rev Endocr Metab Disord. (2013) 14:255–63. doi: 10.1007/s11154-013-9253-9
11. Rosato, V, Temple, NJ, La Vecchia, C, Castellan, G, Tavani, A, and Guercio, V. Mediterranean diet and cardiovascular disease: a systematic review and meta-analysis of observational studies. Eur J Nutr. (2019) 58:173–91. doi: 10.1007/s00394-017-1582-0
12. Molani-Gol, R, and Rafraf, M. Effects of the mediterranean diet on the secondary prevention of cardiovascular diseases: a systematic review of randomised controlled trials. Int J Food Sci Nutr. (2025) 26:1–13. doi: 10.1080/09637486.2025.2466111
13. Schwingshackl, L, Schwedhelm, C, Galbete, C, and Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: an updated systematic review and meta-analysis. Nutrients. (2017) 9:1063. doi: 10.3390/nu9101063
14. Fekete, M, Varga, P, Ungvari, Z, Fekete, JT, Buda, A, Szappanos, Á, et al. The role of the Mediterranean diet in reducing the risk of cognitive impairment, dementia, and Alzheimer's disease: a meta-analysis. Geroscience. (2025) 47:1–13. doi: 10.1007/s11357-024-01488-3
15. Godos, J, Guglielmetti, M, Ferraris, C, Frias-Toral, E, Domínguez Azpíroz, I, Lipari, V, et al. Mediterranean diet and quality of life in adults: a systematic review. Nutrients. (2025) 17:577. doi: 10.3390/nu17030577
16. Tolomeo, M, De Carli, L, Guidi, S, Zanardi, M, Giacomini, D, Devecchi, C, et al. The mediterranean diet: from the pyramid to the circular model. Med J Nutr Metab. (2023) 16:257–270. doi: 10.3233/MNM-230014
17. Damigou, E, Faka, A, Kouvari, M, Anastasiou, C, Kosti, RI, Chalkias, C, et al. Adherence to a Mediterranean type of diet in the world: a geographical analysis based on a systematic review of 57 studies with 1, 125, 560 participants. Int J Food Sci Nutr. (2023) 74:799–813. doi: 10.1080/09637486.2023.2262781
18. Kamiński, M, Skonieczna-Żydecka, K, Nowak, JK, and Stachowska, E. Global and local diet popularity rankings, their secular trends, and seasonal variation in Google trends data. Nutrition. (2020) 79-80:110759. doi: 10.1016/j.nut.2020.110759
19. Vilarnau, C, Stracker, DM, Funtikov, A, da Silva, R, Estruch, R, and Bach-Faig, A. Worldwide adherence to mediterranean diet between 1960 and 2011. Eur J Clin Nutr. (2019) 72:83–91. doi: 10.1038/s41430-018-0313-9
20. Darmon, N, and Drewnowski, A. Does social class predict diet quality? Am J Clin Nutr. (2008) 87:1107–17. doi: 10.1093/ajcn/87.5.1107
21. Dunneram, Y, and Jeewon, R. A scientific assessment of sociodemographic factors, physical activity level, and nutritional knowledge as determinants of dietary quality among indo-Mauritian women. J Nutr Metab. (2013) 2013:1–9. doi: 10.1155/2013/572132
22. Kihlstrom, L, Long, A, and Himmelgreen, D. Barriers and facilitators to the consumption of fresh produce among food pantry clients. J Hunger Environ Nutr. (2019) 14:168–82. doi: 10.1080/19320248.2018.1512923
23. Holgado, B, De Irala-Estévez, J, Martínez-González, M, Gibney, M, Kearney, J, and Martínez, J. Barriers and benefits of a healthy diet in Spain: comparison with other European member states. Eur J Clin Nutr. (2000) 54:453–9. doi: 10.1038/sj.ejcn.1600996
24. Knight, CJ, Jackson, O, Rahman, I, Burnett, DO, Frugé, AD, and Greene, MW. The Mediterranean diet in the stroke belt: a cross-sectional study on adherence and perceived knowledge, barriers, and benefits. Nutrients. (2019) 11:1847. doi: 10.3390/nu11081847
25. Ammar, A. A transnational movement to support the sustainable transition towards a healthy and eco-friendly Agri-food system through the promotion of MEDIET and its lifestyle in modern society: MEDIET4ALL. Eur J Pub Health. (2024) 34:ckae144.643
26. Obeid, CA, Gubbels, JS, Jaalouk, D, Kremers, SPJ, and Oenema, A. Adherence to the Mediterranean diet among adults in Mediterranean countries: a systematic literature review. Eur J Nutr. (2022) 61:3327–44. doi: 10.1007/s00394-022-02885-0
27. Sotos-Prieto, M, Moreno-Franco, B, Ordovás, JM, León, M, Casasnovas, JA, and Peñalvo, JL. Design and development of an instrument to measure overall lifestyle habits for epidemiological research: the Mediterranean lifestyle (MedLife) index. Public Health Nutr. (2015) 18:959–67. doi: 10.1017/S1368980014001360
28. Craig, CL, Marshall, AL, Sjöström, M, Bauman, AE, Booth, ML, Ainsworth, BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
29. Lovibond, PF, and Lovibond, SH. The structure of negative emotional states: comparison of the depression anxiety stress scales (DASS) with the Beck depression and anxiety inventories. Behav Res Ther. (1995) 33:335–43. doi: 10.1016/0005-7967(94)00075-U
30. Diener, E, Emmons, RA, Larsen, RJ, and Griffin, S. The satisfaction with life scale. J Pers Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
31. Zaragoza-Martí, A, Cabañero-Martí, M, Hurtado-Sánchez, J, Laguna-Pérez, A, and Ferrer-Cascales, R. Evaluation of mediterranean diet adherence scores: a systematic review. BMJ Open. (2018) 8:e019033. doi: 10.1136/bmjopen-2017-019033
32. Bach-Faig, A, Berry, EM, Lairon, D, Reguant, J, Trichopoulou, A, Dernini, S, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. (2011) 14:2274–84. doi: 10.1017/S1368980011002515
33. Davis, C, Bryan, J, Hodgson, J, and Murphy, K. Definition of the Mediterranean diet: a literature review. Nutrients. (2015) 7:9139–53. doi: 10.3390/nu7115459
34. Buysse, DJ, Reynolds, CF, Monk, TH, Berman, SR, and Kupfer, DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213.
35. Watson, NF, Badr, MS, Belenky, G, Bliwise, DL, Buxton, OM, Buysse, D, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of sleep medicine and Sleep Research Society. J Clin Sleep Med. (2015) 38:843–844. doi: 10.5665/sleep.4716
36. Bastien, C. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. (2001) 2:297–307. doi: 10.1016/s1389-9457(00)00065-4
37. Coker, AO, Coker, OO, and Sanni, D. Psychometric properties of the 21-item depression anxiety stress scale (DASS-21). Afr Res Rev. (2018) 12:135–42. doi: 10.4314/afrrev.v12i2.13
38. Ammar, A, Brach, M, Trabelsi, K, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB-COVID19 international online survey. Nutrients. (2020) 12:1583. doi: 10.3390/nu12061583
39. Ammar, A, Trabelsi, K, Brach, M, Chtourou, H, Boukhris, O, Masmoudi, L, et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: insight from the ECLB-COVID19 multicenter study. Biol Sport. (2021) 38:9–21. doi: 10.5114/biolsport.2020.96857
40. Lavelle, G, Noorkoiv, M, Theis, N, Korff, T, Kilbride, C, Baltzopoulos, V, et al. Validity of the international physical activity questionnaire short form (IPAQ-SF) as a measure of physical activity (PA) in young people with cerebral palsy: a cross-sectional study. Physiotherapy. (2020) 107:209–15. doi: 10.1016/j.physio.2019.08.013
41. Lee, PH, Macfarlane, DJ, Lam, T, and Stewart, SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. (2011) 8:115. doi: 10.1186/1479-5868-8-115
42. Trichopoulou, A, Martínez-González, MA, Tong, TY, Forouhi, NG, Khandelwal, S, Prabhakaran, D, et al. Definitions and potential health benefits of the Mediterranean diet: views from experts around the world. BMC Med. (2014) 12:112. doi: 10.1186/1741-7015-12-112
43. Eurostat. Eurostat Population projections in the EU European Commission (2023). Available online at: https://ec.europa.eu/eurostat/statistics-explained/index.php?oldid=497115 (accessed December 20, 2024).
44. Rebollo-Sanz, YF, and De la Rica, S. Gender gaps in skills and labor market outcomes: evidence from the PIAAC. Rev Econ Household. (2022) 20:333–71. doi: 10.1007/s11150-020-09523-w
45. Cipollone, A, Patacchini, E, and Vallanti, G. Female labour market participation in Europe: novel evidence on trends and shaping factors. IZA J Eur Labor Stud. (2014) 3:18. doi: 10.1186/2193-9012-3-18
46. Mau, S, Gülzau, F, Laube, L, and Zaun, N. The global mobility divide: how visa policies have evolved over time. J Ethn Migr Stud. (2015) 41:1192–213. doi: 10.1080/1369183X.2015.1005007
47. Lesthaeghe, R. The second demographic transition: a concise overview of its development. Proc Natl Acad Sci USA. (2014) 111:18112–5. doi: 10.1073/pnas.1420441111
48. Calzada, I, and Brooks, C. The myth of mediterranean familism: family values, family structure and public preferences for state intervention in care. Eur Soc. (2013) 15:514–34. doi: 10.1080/14616696.2013.836402
49. Brons, MD, Liefbroer, AC, and Ganzeboom, HB. Parental socioeconomic status and the timing of first marriage: what is the role of unmarried cohabitation? Results from a cross-national comparison. Demogr Res. (2021) 45:469–516. doi: 10.4054/DemRes.2021.45.15
50. OECD. Education policy outlook 2022: Transforming pathways for lifelong learners. (2022). OECD Publishing. Available online at: https://www.oecd.org/en/publications/education-policy-outlook-2022_c77c7a97-en.html (accessed December 20, 2024).
51. OECD Education at a glance 2020: OECD indicators OECD Publishing (2020). Available online at: https://www.oecd.org/en/publications/education-at-a-glance-2020_69096873-en.html (accessed December 20, 2024).
52. International Labour Organization (ILO). Global employment trends for youth: Investing in transforming futures for young people. (2022). Available online at: https://www.ilo.org/publications/major-publications/global-employment-trends-youth-2022-investing-transforming-futures-young (accessed December 20, 2024).
53. Schofer, E, and Meyer, JW. The worldwide expansion of higher education in the twentieth century. Am Sociol Rev. (2005) 70:898–920. doi: 10.1177/000312240507000602
54. Parniak, S, DePaul, V, Frymire, C, DePaul, S, and Donnelly, C. Naturally occurring retirement communities: scoping review. JMIR Aging. (2022) 5:e34577. doi: 10.2196/34577
55. Dinu, M, Pagliai, G, Casini, A, and Sofi, F. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur J Clin Nutr. (2018) 72:30–43. doi: 10.1038/ejcn.2017.58
56. Fanzo, J, and Miachon, L. Harnessing the connectivity of climate change, food systems and diets: taking action to improve human and planetary health. Anthropocene. (2023) 42:100381. doi: 10.1016/j.ancene.2023.100381
57. Feliu, A, Filippidis, FT, Joossens, L, Fong, GT, Vardavas, CI, and Baena, A. Impact of tobacco control policies on smoking prevalence and quit ratios in 27 European Union countries from 2006 to 2014. Tob Control. (2019) 28:101–9. doi: 10.1136/tobaccocontrol-2017-054119
58. World Health Organization (WHO) WHO report on the global tobacco epidemic 2021. (2021). Available online at: https://www.who.int/publications/i/item/9789240032095 (accessed December 20, 2024).
59. Jawad, M, Khader, A, and Millett, C. Waterpipe tobacco smoking prevalence and correlates in 25 eastern Mediterranean and eastern European countries: cross-sectional analysis of the global youth tobacco survey. Nicotine Tob Res. (2018) 20:482–91. doi: 10.1093/ntr/ntv101
60. Maziak, W. The global epidemic of waterpipe smoking. Addict Behav. (2011) 36:1–5. doi: 10.1016/j.addbeh.2010.08.030
61. Kromhout, D, Spaaij, CJ, de Goe, J, and Weggemans, RM. The 2015 Dutch food-based dietary guidelines. Eur J Clin Nutr. (2018) 72:665–73. doi: 10.1038/ejcn.2016.52
62. Fiolet, T, Srour, B, Sellem, L, Kesse-Guyot, E, Allès, B, Méjean, C, et al. Consumption of ultra-processed foods and cancer risk: results from Nutri net-santé prospective cohort. BMJ. (2018) 360:k322. doi: 10.1136/bmj.k322
63. Baker, P, Machado, P, Santos, T, Sievert, K, Backholer, K, Hadjikakou, M, et al. Ultra-processed foods and the nutrition transition: global, regional and national trends, food systems transformations and political economy drivers. Obes Rev. (2020) 21:e13126. doi: 10.1111/obr.13126
64. Bonaccio, M, Di Castelnuovo, A, Ruggiero, E, Costanzo, S, Grosso, G, De Curtis, A, et al. Joint association of food nutritional profile by Nutri-score front-of-pack label and ultra-processed food intake with mortality: Moli-sani prospective cohort study. BMJ. (2022) 378:e070688. doi: 10.1136/bmj-2022-070688
65. Bonaccio, M, Ruggiero, E, Di Castelnuovo, A, Costanzo, S, Persichillo, M, De Curtis, A, et al. Fish intake is associated with lower cardiovascular risk in a Mediterranean population: prospective results from the Moli-sani study. Nutr Metab Cardiovasc Dis. (2017) 27:865–73. doi: 10.1016/j.numecd.2017.08.004
66. Yesildemir, O, Guldas, M, Boqué, N, Calderón-Pérez, L, Degli Innocenti, P, Scazzina, F, et al. Adherence to the mediterranean diet among families from four countries in the mediterranean basin. Nutrients. (2025) 17:1157. doi: 10.3390/nu17071157
67. Springmann, M, Clark, M, Mason-D'Croz, D, Wiebe, K, Bodirsky, BL, Lassaletta, L, et al. Options for keeping the food system within environmental limits. Nature. (2018) 562:519–25. doi: 10.1038/s41586-018-0594-0
68. EFSA Nutrition, novel foods and food allergens (2021). Available online at: https://www.efsa.europa.eu/en/science/scientific-committee-and-panels/nda (accessed December 20, 2024).
69. Dernini, S, Berry, EM, Serra-Majem, L, La Vecchia, C, Capone, R, Medina, FX, et al. Med diet 4.0: the Mediterranean diet with four sustainable benefits. Public Health Nutr. (2017) 20:1322–30. doi: 10.1017/S1368980016003177
70. Lopez-Garcia, E, Rodriguez-Artalejo, F, Li, TY, Fung, TT, Li, S, Willett, WC, et al. The mediterranean-style dietary pattern and mortality among men and women with cardiovascular disease. Am J Clin Nutr. (2004) 79:379–85. doi: 10.3945/ajcn.113.068106
71. Micha, R, Khatibzadeh, S, Shi, P, Andrews, KG, Engell, RE, and Mozaffarian, D. Global, regional and national consumption of major food groups in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open. (2017) 5:e008705. doi: 10.1136/bmjopen-2015-008705
72. Pitt, E, Gallegos, D, Comans, T, Cameron, C, and Thornton, L. Exploring the influence of local food environments on food behaviours: a systematic review of qualitative literature. Public Health Nutr. (2017) 20:2393–405. doi: 10.1017/S1368980017001069
73. Hublin, C, Lehtovirta, M, Partinen, M, Koskenvuo, M, and Kaprio, J. Napping and the risk of type 2 diabetes: a population-based prospective study. Sleep Med. (2016) 17:144–8. doi: 10.1016/j.sleep.2015.11.004
74. Eurofound. Working time and work-life balance. (2022). Available online at: https://www.eurofound.europa.eu/en/working-time-and-work-life-balance (accessed December 20, 2024).
75. Evaristo, OS, Moreira, C, Lopes, L, Abreu, S, Agostinis-Sobrinho, C, Oliveira-Santos, J, et al. Associations between physical fitness and adherence to the mediterranean diet with health-related quality of life in adolescents: results from the lab med physical activity study. Eur J Pub Health. (2018) 28:631–5. doi: 10.1093/eurpub/cky043
76. OECD OECD economic outlook. (2023). Available online at: https://www.oecd.org/en/publications/oecd-economic-outlook/volume-2023/issue-1_ce188438-en.html (accessed December 20, 2024).
77. Prosperi, P, Allen, T, Padilla, M, Peri, I, and Cogill, B. Sustainability and food & nutrition security: a vulnerability assessment framework for the Mediterranean region. SAGE Open. (2014) 4:1–17. doi: 10.1177/2158244014539169
78. Bonaccio, M, Donati, M, Iacoviello, L, and de Gaetano, G. Socioeconomic determinants of the adherence to the Mediterranean diet at a time of economic crisis: the experience of the MOLI-SANI study. Agric Agric Sci Procedia. (2016) 8:741–7. doi: 10.1016/j.aaspro.2016.02.059
79. Ajzen, I. The theory of planned behavior: frequently asked questions. Hum Behav Emerg Technol. (2020) 2:314–24. doi: 10.1002/hbe2.195
80. Guthold, R, Stevens, GA, Riley, LM, and Bull, FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. (2018) 6:e1077–86. doi: 10.1016/S2214-109X(18)30357-7
81. Palaz, FS. The social networks and engagements of older Turkish migrants in Germany. Open J Sociol Stud. (2020) 4:79–92. doi: 10.32591/coas.ojss.0402.03079p
82. Swader, CS. Loneliness in europe: personal and societal individualism-collectivism and their connection to social isolation. Soc Forces. (2019) 97:1307–36. doi: 10.1093/sf/soy088
83. Lopez-Minguez, J, Gómez-Abellán, P, and Garaulet, M. Timing of breakfast, lunch, and dinner. Effects on obesity and metabolic risk. Nutrients. (2019) 11:2624. doi: 10.3390/nu11112624
84. Kuriyama, K. Social determinants of sleep quality: association between sleep quality and living environment among older individuals. Sleep Biol Rhythms. (2024) 22:301–2. doi: 10.1007/s41105-024-00533-0
85. Grandner, MA, and Fernandez, FX. The translational neuroscience of sleep: a contextual framework. Science. (2021) 374:568–73. doi: 10.1126/science.abj8188
86. Valkenburg, PM, Meier, A, and Beyens, I. Social media use and its impact on adolescent mental health: an umbrella review of the evidence. Curr Opin Psychol. (2022) 44:58–68. doi: 10.1016/j.copsyc.2021.08.017
87. World Health Organization (WHO) World mental health report: transforming mental health for all. (2022). Available online at: https://www.who.int/publications/i/item/9789240049338 (accessed December 20, 2024).
88. Safaei Lari, M, and Emamgholipour Sefiddashti, S. Socio-economic, health and environmental factors influencing suicide rates: a cross-country study in the eastern Mediterranean region. J Forensic Leg Med. (2023) 93:102463. doi: 10.1016/j.jflm.2022.102463
89. Gopalkrishnan, N. Cultural diversity and mental health: considerations for policy and practice. Front Public Health. (2018) 6:179. doi: 10.3389/fpubh.2018.00179
90. Sharma, S, and Sharma, M. Globalization, threatened identities, coping and well-being. Psychol Stud. (2010) 55:313–22. doi: 10.1007/s12646-010-0048-8
91. Howarth, RB, and Kennedy, K. Economic growth, inequality, and well-being. Ecol Econ. (2016) 121:231–6. doi: 10.1016/j.ecolecon.2015.10.005
92. Nadash, P, Doty, P, and von Schwanenflügel, M. The German Long-term care insurance program: evolution and recent developments. Gerontologist. (2018) 58:588–97. doi: 10.1093/geront/gnx018
93. Dunst, CJ. A meta-analysis of informal and formal family social support studies: relationships with parent and family psychological health and well-being. Int J Caring Sci. (2023) 16:514.
94. Pines, AM, Ben-Ari, A, Utasi, A, and Larson, D. A cross-cultural investigation of social support and burnout. Eur Psychol. (2002) 7:256–64. doi: 10.1027//1016-9040.7.4.256
95. Porcel-Gálvez, AM, Allande-Cussó, R, Fernández-García, E, Essawi, S, Salama, M, Saad, SS, et al. Priorities and challenges in social and healthcare policies for older people living in the Mediterranean basin: a Delphi panel study. BMC Geriatr. (2024) 24:845. doi: 10.1186/s12877-024-05430-2
96. Al Sharjabi, SJ, Al Jawaldeh, A, Hassan, OEH, and Dureab, F. Understanding the food and nutrition insecurity drivers in some emergency-affected countries in the eastern Mediterranean region from 2020 to 2024. Nutrients. (2024) 16:3853. doi: 10.3390/nu16223853
97. Parish, J, Perić, M, Čipčić Paljetak, H, Matijašić, M, and Verbanac, D. Translating the mediterranean diet: from chemistry to kitchen. Period Biol. (2011) 113:303–10.
98. Vera, L, Coma, I, Pérez, M, Riera, JV, Martínez, B, and Gimeno, J. The mediterranean forest in a science museum: engaging children through drawings that come to life in a virtual world. Multimed Tools Appl. (2024) 83:76851–72. doi: 10.1007/s11042-024-18606-0
99. Naicker, A, Shrestha, A, Joshi, C, Willett, W, and Spiegelman, D. Workplace cafeteria and other multicomponent interventions to promote healthy eating among adults: a systematic review. Prev Med Rep. (2021) 22:101333. doi: 10.1016/j.pmedr.2021.101333
100. NHS England Social prescribing: applying all our health (2023). Available online at: https://www.gov.uk/government/publications/social-prescribing-applying-all-our-health (accessed December 20, 2024).
101. Hageman, D, Fokkenrood, HJP, Essers, PPM, Koelemay, MJW, Breek, JC, Vahl, AC, et al. Improved adherence to a stepped-care model reduces costs of intermittent claudication treatment in the Netherlands. Eur J Vasc Endovasc Surg. (2017) 54:51–7. doi: 10.1016/j.ejvs.2017.04.011
102. Sultan, MA, Miller, E, Tikkanen, RS, Singh, S, Kullu, A, Cometto, G, et al. Competency-based education and training for community health workers: a scoping review. BMC Health Serv Res. (2025) 25:263. doi: 10.1186/s12913-025-12217-7
103. Puig-Ribera, A, Arumí-Prat, I, Cirera, E, Solà, M, Codina-Nadal, A, Palència, L, et al. Use of the superblock model for promoting physical activity in Barcelona: a one-year observational comparative study. Arch Public Health. (2022) 80:257. doi: 10.1186/s13690-022-01005-y
Keywords: Mediterranean regions differences, MedLife Index, physical activity, mental health, public health, psychological distress, health predictors
Citation: Boujelbane MA, Ammar A, Salem A, Kerkeni M, Trabelsi K, Bouaziz B, Masmoudi L, Heydenreich J, Schallhorn C, Müller G, Merve Uyar A, Ghazzawi HA, Amawi AT, Orhan BE, Grosso G, Abdelkarim O, Driss T, El Abed K, Zmijewski P, Debeaufort F, Benbettaieb N, Poulain C, Reyes L, Gamero A, Cuenca-Ortolá M, Cilla A, Francesca N, Messina CM, Viola E, Lorenzen B, Filice S, Bajoub A, Ajal E-M, Ajal EA, Obtel M, Lahiani S, Khaldi T, Souissi N, Boukhris O, Jahrami H, Husain W, Frias-Toral E, Mahdi W, Chtourou H and Schöllhorn WI (2025) Regional variations in Mediterranean diet adherence: a sociodemographic and lifestyle analysis across Mediterranean and non-Mediterranean regions within the MEDIET4ALL project. Front. Public Health. 13:1596681. doi: 10.3389/fpubh.2025.1596681
Edited by:
Suman Chakrabarty, West Bengal State University, IndiaReviewed by:
Héctor Armando Rincón León, Mexican Social Security Institute, MexicoHolly Huye, University of Southern Mississippi, United States
Copyright © 2025 Boujelbane, Ammar, Salem, Kerkeni, Trabelsi, Bouaziz, Masmoudi, Heydenreich, Schallhorn, Müller, Merve Uyar, Ghazzawi, Amawi, Orhan, Grosso, Abdelkarim, Driss, El Abed, Zmijewski, Debeaufort, Benbettaieb, Poulain, Reyes, Gamero, Cuenca-Ortolá, Cilla, Francesca, Messina, Viola, Lorenzen, Filice, Bajoub, Ajal, Ajal, Obtel, Lahiani, Khaldi, Souissi, Boukhris, Jahrami, Husain, Frias-Toral, Mahdi, Chtourou and Schöllhorn. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Achraf Ammar, YWNhbW1hckB1bmktbWFpbnouZGU=
†These authors share first authorship
‡ORCID: Achraf Ammar, orcid.org/0000-0003-0347-8053
Liwa Masmoudi, orcid.org/0000-0002-9628-1585
Christiana Schallhorn, orcid.org/0000-0003-1564-2658
Giuseppe Grosso, orcid.org/0000-0003-3930-5285
Frédéric Debeaufort, orcid.org/0000-0002-4760-0500
Nasreddine Benbettaieb, orcid.org/0000-0001-8454-2218
Clément Poulain, orcid.org/0009-0004-6370-1581
Enrico Viola, orcid.org/0000-0003-3980-528X
Aadil Bajoub, orcid.org/0000-0002-3665-5223
El Amine Ajal, orcid.org/0000-0003-3946-5246
Omar Boukhris, orcid.org/0000-0002-2861-0164