 John Whitebrook
John Whitebrook Caroline Lafarge
Caroline Lafarge Jamie S. Churchyard
Jamie S. Churchyard- Department of Psychology, School of Human and Social Sciences, University of West London, Ealing, United Kingdom
Introduction: The annual suicide death rate is c.760,000 therefore, using the widely accepted estimate of 135 people being exposed to each suicide, the worldwide annual exposure rate is over 100 million. While male suicide-loss survivors (SLSs) are equally exposed, the vast majority of suicide bereavement research includes a large majority of female participants.
Methods: Following the eMERGe and PRISMA guidelines, a meta-ethnography (systematic review of qualitative studies) was carried out to assess historical research into suicide-loss survivorship. Seven data sources were searched, up to 30-Nov-2022, for peer-reviewed studies, written in English, that used identifiable and interpretative qualitative methods, had at least 50% male participation, and offered a valuable contribution to the synthesis.
Results: Overall, 1,645 records were screened, and 15 reports of included studies assessed. Eight main themes were identified: changed forever, trauma, stigmatization, protector, lost futures, lost in plain sight, societal norms, and dualities. Via line of argument synthesis, and considering the broader literature, a model for suicide bereavement, applicable to all, is proposed that brings together the gamut of pertinent factors into an integrated framework.
Discussion: The model could be used in practice (clinical, therapy/counseling, education) to enable better understanding of the highly complex and interwoven components of suicide bereavement, thereby facilitating improved and extended services available to SLSs that are more in-tune with their needs. While the model cannot confer full comprehension of suicide bereavement, it can go a long way to assist those looking to assist SLSs by providing a platform for dialogue and empathy.
Introduction
This study was carried out as part of an overall research program investigating postvention (bereavement support) uptake and effectiveness in UK and Ireland adult males bereaved by suicide. The term “suicide loss survivor” (SLS) is utilized in this article as it is being increasingly used for those who have experienced the suicide of a close family member, or a friend, and face persistent, distressing trauma (1). It is thereby differentiated from survivors of suicide attempts. Against a backdrop of c. 760,000 annual suicide deaths globally (2), based on UK (3–5) and Ireland (6) government suicide statistics, annual suicides total approximately 7,500 with male suicide being three to four times more prevalent than female suicide. However, the UK is one of several countries where it has been suggested that the coronial system could result in a 15–50% underestimation of suicide as the officially determined cause of death. This has been associated with SLS pressure on the coroner, the coroner's inherent wish to protect SLS from the associated stigma and, most importantly, coronial reticence to declare deaths as suicide reflective of the legacy of deemed criminality (7). This may have been mitigated, more recently, by the standard of proof for suicide deaths, in England and Wales, being lowered to the civil standard of being on “the balance of probabilities,” from “beyond all reasonable doubt,” in 2018 (8). In the period 2000–2019, Ireland was in keeping with a global trend of declining suicide rates but the numbers for the UK increased, although not statistically significantly (2). The number of people bereaved by suicide annually, across the world, has been estimated at 48 million (9). Using an annual global suicide figure of 700,000 (noted in the same paper) the corresponding annual suicide exposure level, on a ratio basis, would be approximately 480,000 for the UK and Ireland. Using the estimate of 135 people being exposed to each suicide (10), the UK and Ireland annual exposure rate to suicide is 945,000. Results of a UK-wide survey indicated that 77% of participants (including professionals and those that lost friends) were majorly affected by losing a loved one to suicide, with half reporting mental health issues, 38% contemplating suicide, and 8% attempting suicide, directly related to their bereavement by suicide (11). Similarly, a survey conducted in Ireland found that 93% of SLS noted a moderate or major impact on their lives with mental health issues (56%), relationship struggles and alcohol abuse being typical factors, and 35% considering self-harm or suicide (12). A recent systematic review of the psychosocial impact of suicide bereavement on men highlighted their increased risk of suicide and mental health problems, plus issues with relationships and social interactions, over men not bereaved by suicide (13). Furthermore, a systematic review of postvention service models, between 2014 and 2019, found that, generally, studies of suicide bereavement support services had 80–91% female participation (14). However, evidence also suggests that there is no correlation between parental gender (or that of a child lost to suicide) and depression and grief (15). Similarly, no gender differences were found relating to siblings' suicide loss (16) or partner suicide loss, with both genders experiencing reduced life expectancy, higher rates of divorce, children in care, sick leave, and unemployment (17). Yet, despite encountering similar levels of grief and emotional distress to female SLS, male SLS seek help far less frequently. It has also been noted that the impact and management approaches of suicide bereavement interventions vary by gender, with the inadvertent emphasis on the effectiveness of postvention in largely female samples, thereby introducing a major gap in both postvention activities and the literature regarding men (18). In addition to SLS being prone to mental health issues and at increased risk of suicide themselves (19), understanding psychosocial influences, with appropriate interventions, has also been shown to be effective in lessening both suicidal behaviors and the likelihood of attempts (20). Therefore, men are typically not receiving much needed, proven, support to help them cope with their losses.
The purpose of this meta-ethnography was to identify qualitative research which summarizes current knowledge on how adult males experience, cope with, and adapt to, bereavement by suicide. Factors influencing this could be cultural, socioeconomic, educational, demographic, psychological, as well as previous history of trauma, which are implicated in postvention being available, taken up, and impacting its effectiveness. Based on a gained comprehension of adult male postvention research findings in the broad literature, the intent was to frame further novel research pertinent to the target population of UK and Ireland adult male SLS.
There are several approaches to qualitative evidence synthesis which have been collated, summarized, and “the state of the method” assessed (21). To achieve the intended objectives of this study, a method was required that goes beyond aggregation of themes but, rather, one which is interpretive of the underlying concepts facilitating creation of an overview regarding the fundamental issues faced by adult males bereaved by suicide. This reflects the two essential components of meta-ethnography, in viewing the source information as metaphorical, rather than literal, and translation of studies into each other during the synthesis (22). This approach allows for a derivation of commonality and the development of constructs that represent the dataset, as a whole, but may not individually be apparent in any of the studies included (23).
The goal was to assess prior research regarding how men have experienced, coped, or struggled with bereavement by suicide, along with any prevailing attitudes or perspectives reported. A secondary objective was to systematically review the level of male involvement in, and contributions to, relevant research. Finally, the intent was to consider whether the literature indicates male-specific factors relevant to the provision, and uptake, of postvention services.
Method
Search strategy
The search strategy involved retrieving records that describe the lived experience of adult males bereaved by suicide. The purpose of the search terms was to capture records covering suicidality, aspects of grief or bereavement, relationships to those lost, male involvement, and various types of qualitative study. Wildcards were used to capture linguistic variations, for example “grie*” allowing retrieval of records that describe grief or grieving. The search strategy was honed via multiple searches of the Academic Elite database. In conjunction with the research team and the [University of West London] specialist librarian, the following data sources were searched: Academic Search Elite, CINAHL Complete (Cumulated Index to Nursing and Allied Health Literature), Medline, PsycARTICLES, PsycINFO, ProQuest, and Google Scholar. These were selected as they are frequently used in psychological research and provide a broad coverage of relevant publishers. Each data source was searched independently, as they are indexed differently, and the search strategy was refined based on the initial output generated from the individual sources (see Supplementary material A for the complete search strategy).
Search criteria
The searching of ProQuest was constrained by two of the primary terms, relating to suicidality and bereavement, plus limited to abstracts and the Google Scholar searches were of article titles only. Both measures were necessary to eliminate many thousands of extraneous hits and home in on the target records. The searches were set to return only English language records, to avoid interpretation bias, but no timeframe was set other than a publication date up to and including the end of November 20221. There was no exclusion based on geography. All the studies included in this meta-ethnography had a significant level of male participation (50% or above) and similar aims, in terms of looking to elucidate how the experiences related to suicide-loss shape those left behind (see Supplementary material A for the complete search criteria).
Approach
The overall approach adopted is compliant with that advocated by the “STARLITE” guidance which calls for the clear definition of the “sampling strategy, type of study, approaches, range of years, limits, inclusion and exclusions, terms used, electronic sources,” reflecting the mnemonic and intended to provide a standard for reporting literature searches (24).
To mitigate any inherent bias, in their consideration, the studies included in this meta-ethnography have been presented alphabetically by author [save for Ross et al. (25), which is embedded under Entilli et al. (26), as it is an earlier report of the same study]. The comparison of papers was then initiated by using the first study with each of the following studies being assessed against all those preceding (27). The analysis was conducted by Author #1 and cross-validated by Authors #2 and #3. All authors agreed that the themes and interpretative framework were embedded in the data and provided a meaningful interpretation of SLS's experiences2.
Studies were included that offered a valuable contribution to the synthesis. This is a subjective appraisal but is in keeping with meta-ethnographic practice (28). When conducting a meta-ethnography, it is common for the quality of the included studies not to be a basis for exclusion prior to the synthesis (27) and this was the case herein. There is no defined standard for assessing the quality of studies included in a meta-ethnography (29). For the purposes of this meta-ethnography, the CASP Qualitative Studies Checklist (30) was employed which consists of 10 questions. Application of these questions facilitated evaluation of studies based on key parameters, including methods, congruity of method with the aims and analysis, ethics, comprehensibility, and value in terms of adding to existing knowledge. Questions reflect three aspects of the quality review with items one to six focused on validity, seven to nine on the results, and 10 on the study value. This framework has been effectively used in other meta-ethnographies (27) where each study is assessed against nine questions, for specific aspects of quality, with ratings of “yes,” “can't tell,” or “no,” plus observations on the value of the research undertaken and overall comments. The studies were all assessed by Author #1 with the other two members of the team each reviewing a random sample. Any divergence of opinion was resolved through dialogue.
Meta-ethnography is a method for synthesis of purely qualitative studies, but it allows for a range of study designs to be included. Its systematic approach facilitates generation of insights into experiences and derivation of impressions and models that can inform both future research and real-world policy and practice (31). While meta-ethnography is an intricate method, and time-consuming, it is well suited for application to primary studies that contain rich data and are highly interpretative (31).
Transparency and openness
This meta-ethnography adhered to the PRISMA 2020 guidelines for systematic reviews (32). All data and research materials (including our manual coding scheme) are available upon request. This review was not preregistered. Historically, meta-ethnographies have often lacked an audit trail, but standards, such as the eMERGe reporting guidance (33) employed herein, providing structure and aimed to enhance quality, robustness, and reliability, address that potential limitation (21).
Research team
The full research team (of three) was involved at key stages (search strategy, extraction, translation, and synthesis) as well as the supporting researchers conducting randomly assigned, independent reviews where appropriate (10% studies post de-duplication, 10% full text review, and 50% quality assessment). Any differences in opinion, arising from such checkpoints, were collated for discussion at face-to-face team meetings and consensus reached prior to each stage being finalized.
Positionality and reflexivity
The lead researcher is an SLS and is a trustee/volunteer with a UK peer-support group [Survivors of Bereavement by Suicide]. It is with that lens that the research described herein has been conducted and with an acknowledgment of the consequential potential for inherent bias. That said, the charity work has facilitated the lead researcher interacting with many other SLS who have lost a cross-section of loved ones, who come from a broad range of backgrounds, and their losses span from the very recent to 10 or more years ago. This has provided an expansive perspective beyond personal experience. Other members of the research team have not been bereaved by suicide and so brought a balanced viewpoint and provided a check regarding any intrinsic bias of the lead researcher, regarding the findings of this meta-ethnography.
As the primary executor of this meta-ethnography, the lead researcher inevitably perceived the development of the proposed model in the content of both personal experience and the interplay with a broad cross-section of other SLS. This was mitigated by the extensive experience of the overall team, with various qualitative research approaches, and the rigorous methodological approach employed herein to bring structure and transparency. The make-up of the research team facilitated the combination of academic rigor and real-life awareness of the impacts of suicide bereavement to inform the interpretation of the analysis of the studies included in this meta-ethnography. Thereby producing a novel and informative model that holistically depicts suicide loss survivorship and its overarching, life-changing complexity.
Ethics
British Psychological Society ethical considerations were adhered to, including obtaining ethical approval from the [University Research and Ethics Committee (UREC) at the University of West London].
Findings
The initial search yielded 1,645 records. After de-duplication, there were 1,189 records remaining. After the exclusion of gray literature, systematic reviews, quantitative studies, clinical trials, viewpoints, non-scientific records or those relating to fiction, studies lacking a focus on suicide bereavement, and studies with minimal adult male involvement, or where the findings are not attributable to the adult men that participated, a further 1,090 records were eliminated, leaving 99 to be sought for full text retrieval. During the review of articles obtained via the database searches (including Google Scholar) a number of papers were manually identified or cited in studies that were candidates for retention. In total these numbered 36, making the overall total to be sought for retrieval at 135. From both the database and manual search routes, a few papers were unavailable from the university library, therefore Inter-Library Loan requests were made. All but one (from the manual search path) were obtained, such that 134 records were retrievable overall.
Figure 1 depicts the full screening process in line with the current PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guideline (32). It is based on the 2020 version of the PRISMA Flow Diagram template. One report retrieved (26) describes a longitudinal study of parents bereaved by suicide assessed at 6, 12 and 24 months after their losses. A prior report (25) is based on the same study but only covered the 6- and 12-month assessments. Both studies met the inclusion criteria set for the review but, following the latest PRISMA guidance on how this should be reported on the flow diagram, this represents a single included study and increases the “Reports of included studies” by one (34). Overall, based on consensus reached by the review team, 13 papers were included in the meta-ethnography arising from the database searches and two from the manual searches.
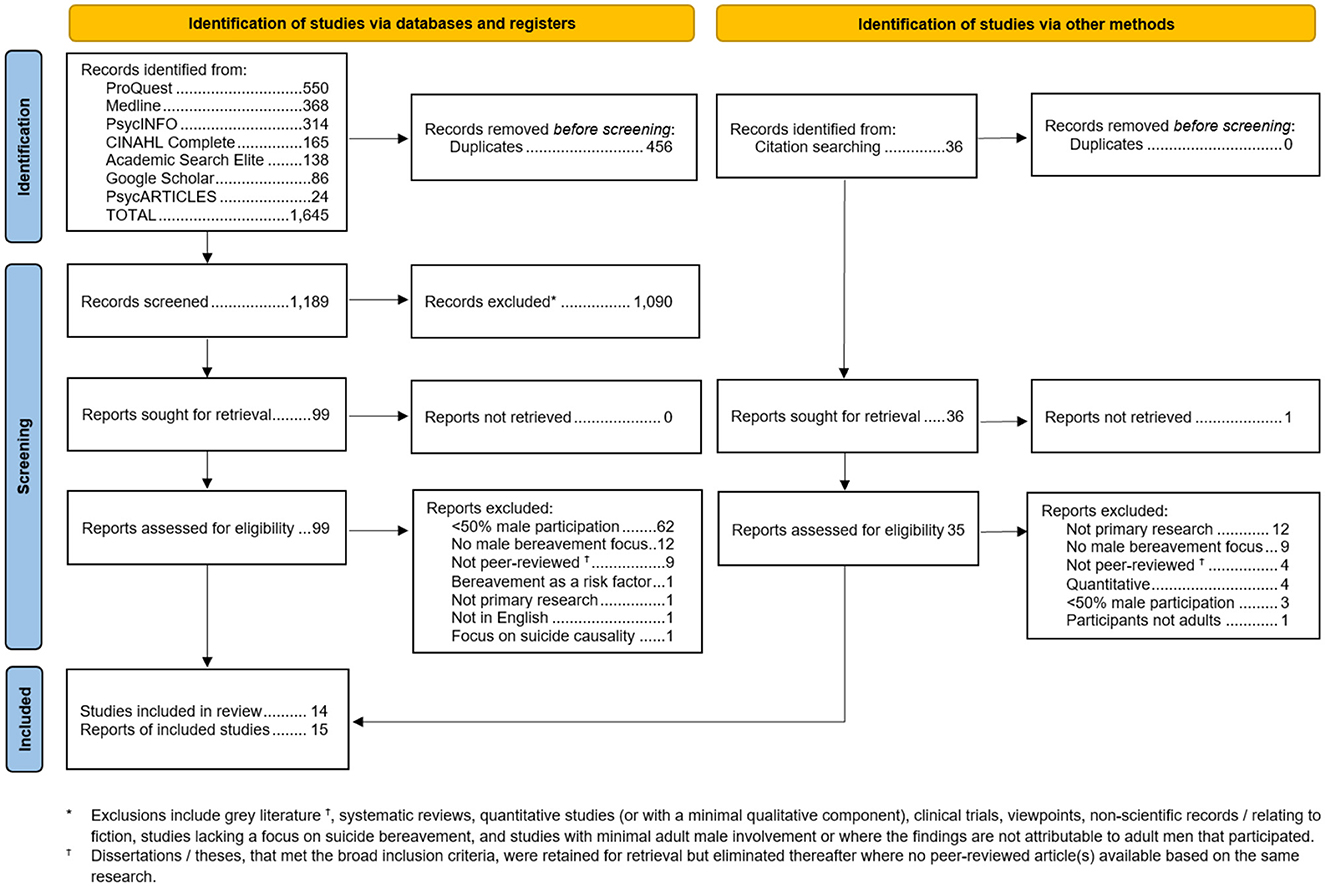
Figure 1. PRISMA flow diagram depicting the overall steps for identifying reports for inclusion in the meta-ethnography.
The quality assessment of the 14 studies indicated that, despite minor issues, all of them can be relied upon as valid data sources3.
Study characteristics
All the included studies were conducted since 2010, with most (10/14) being from 2017 onwards. A summary of the key characteristics, from each included study, is presented in Table 1. Together, the two articles mapping to a single study are one of three Australian papers (#6 plus #7, and #1). Other geographies represented are Africa (1: Nigeria (#13)), Asia (4: China (#5), Hong Kong (#4), South Korea (#11), and Pakistan (#2)), Europe (4: England (#12), Germany (#3), Ireland (#9), and Poland (#15)) and North America (2: Canada (#8 and #14)). Cultures vary across these regions and/or sub-populations within them and, of the countries represented, suicide remains illegal in two countries (Nigeria and Pakistan). Eight of the 14 studies (#1, #2, #6 plus #7, #9, #12, #13, and #15) had both male and female participants while the remainder (#3, #4, #5, #8, #10, #11, and #14) included only men, with four of them based on a single participant (#3, #5, #10, and #11). The ages of participants were not supplied for three of the studies (#2, #5, and #12). Where ages were provided, many (6/14) included middle-aged to older participants (#3, #6 plus #7, #8, #11) with some (#4, #9, #13, #14, and #15) including a broad range of ages (4/14), and only two having exclusively younger participation (#1, and #10). Socio-economic background was not provided in most studies, but some did include specific information on the participant(s). In one (#10), it was noted that the individual was part of a family that had immigrated from a non-English speaking country and that they had experienced domestic violence, with a backdrop of financial difficulties. In the Nigerian study (#13) it was recorded that population, from which the sample was drawn, had strong literacy and religiosity, with employment primarily across agriculture, commerce, and the civil service. In the study conducted in China (#5), it was recorded that the participant was recruited from a bereavement support group in a city which is economically developed.
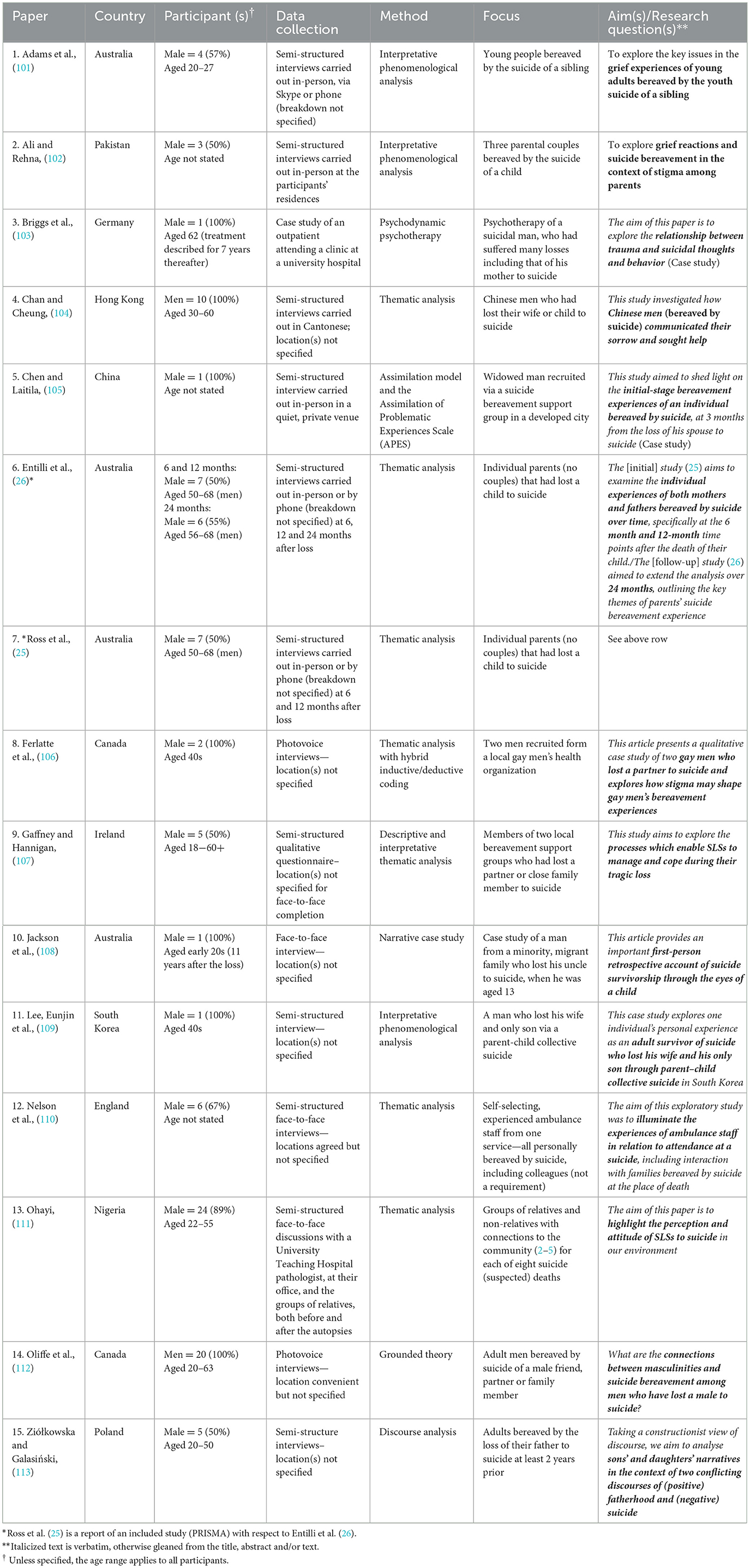
Table 1. Key characteristics of the studies included in the meta-ethnography.
Most studies (#1, #2, #4, #5, #6 plus #7, #9, #11, #12, #13, and #15) collected data via semi-structured interviews (10/14). Data collection for one (#9) was unclear but an examination of the larger study of which it is a component (but not part of this meta-ethnography) implies that this was also via semi-structured interviews (35). Two studies (#8 and #14) employed photovoice interviews, and one was based on the psychotherapy notes for an individual (#3). The procedure, for the psychotherapy study (#3), also notes that the verbatim transcript was translated into English but no issues with this were mentioned. The authors of the study conducted in Poland (#15) noted that the participant quotes were translated from Polish into English and that some fidelity may have been lost due to the resulting text losing a degree of coherence, in some instances.
In terms of data analysis, Thematic Analysis (TA) was used in four of the studies (#4, #6 plus #7, #12, and #13), another used a hybrid of deductive and inductive TA (#8), and another noted the use of “descriptive and interpretative thematic analysis” (#9). Interpretive Phenomenological Analysis was employed in three studies (#1, #2, and #11). The remaining five studies each approached the analysis differently, one being based on a case study of psychodynamic psychotherapy (#3), with others employing grounded theory (#14) and discourse analysis (#15). Uniquely, in this set, one study (#5) applied ratings from the Assimilation of Problematic Experiences Scale (APES) to textual passages derived from the transcript. One paper describes a narrative case study (#9) but did not define an analysis approach, nor did it articulate any themes. It does, though, contain a rich set of participant quotes from which concepts can be gleaned.
Analysis
The outcome of the translation process, involving iterative review of all the studies to assess for concepts consistent across them (reciprocal) or those that differ or are conflicting (refutational) and the subsequent interpretation to create novel themes (line of argument), is encapsulated in Table 2, in which, after a synopsis of each individual study, the cumulative concepts are listed. This reflects the research program's aim of understanding the broad impacts of suicide bereavement. Importantly, this table is not merely a list of themes, but attempts to portray the underlying, cohesive concepts arising from each study, and an amalgamation thereof.

Table 2. Main themes of the studies and cumulative concepts derived.
When considering how studies are related to each other, originally characterized as metaphors to capture derived meaning across studies (28), more recently, such amalgamations have been described as storylines, which can help identify sub-sets, commonalities, and conflicts (22). No concepts, across the 15 papers, were found to refute each other. Concepts shared across papers were mostly reciprocal. A line of argument (28), or framework for interpretation was developed which is described below.
Following a method described elsewhere (27, 36), the 14 studies were tabulated to facilitate comparisons of the main concepts identified in each one (Table 3). For ease of review, only the main themes from each study have been included in the table and their descriptions abbreviated and/or paraphrased for fit. However, the full articles, including detailed analyses, findings and discussions, were examined during the translation process. With the proviso that, by their very nature, published studies included a selected set of quotations intended to represent the participants' experiences, such reflections in meta-ethnography are considered first-order constructs, and are typically located in the analysis or results sections of the articles. How participants' perceptions were interpreted by the study authors, are considered as second-order constructs, and usually described in the discussion sections. New concepts, synthesized from first and second order constructs, are deemed third-order constructs (37) and derived as part of the meta-ethnography analysis. From first, second and third order constructs, a line of argument can be generated: a framework of interpretation. Generation of a line of argument comprises an expanded comprehension of the underlying constructs to produce an extended or novel concept (22, 36). To illustrate the analysis, participants' quotations (first-order constructs) are presented in italics using quotations marks, whilst the authors' interpretations (second-order construct) are displayed using quotations marks only:
“I got quite protective of Dad and Mum…but I think they were more worried about protecting me.”/“Most participants reported that the death highlighted for them and their parents the fragility of life, triggering a pattern of reciprocal protection and anxiety for each other's safety” (Paper #1).
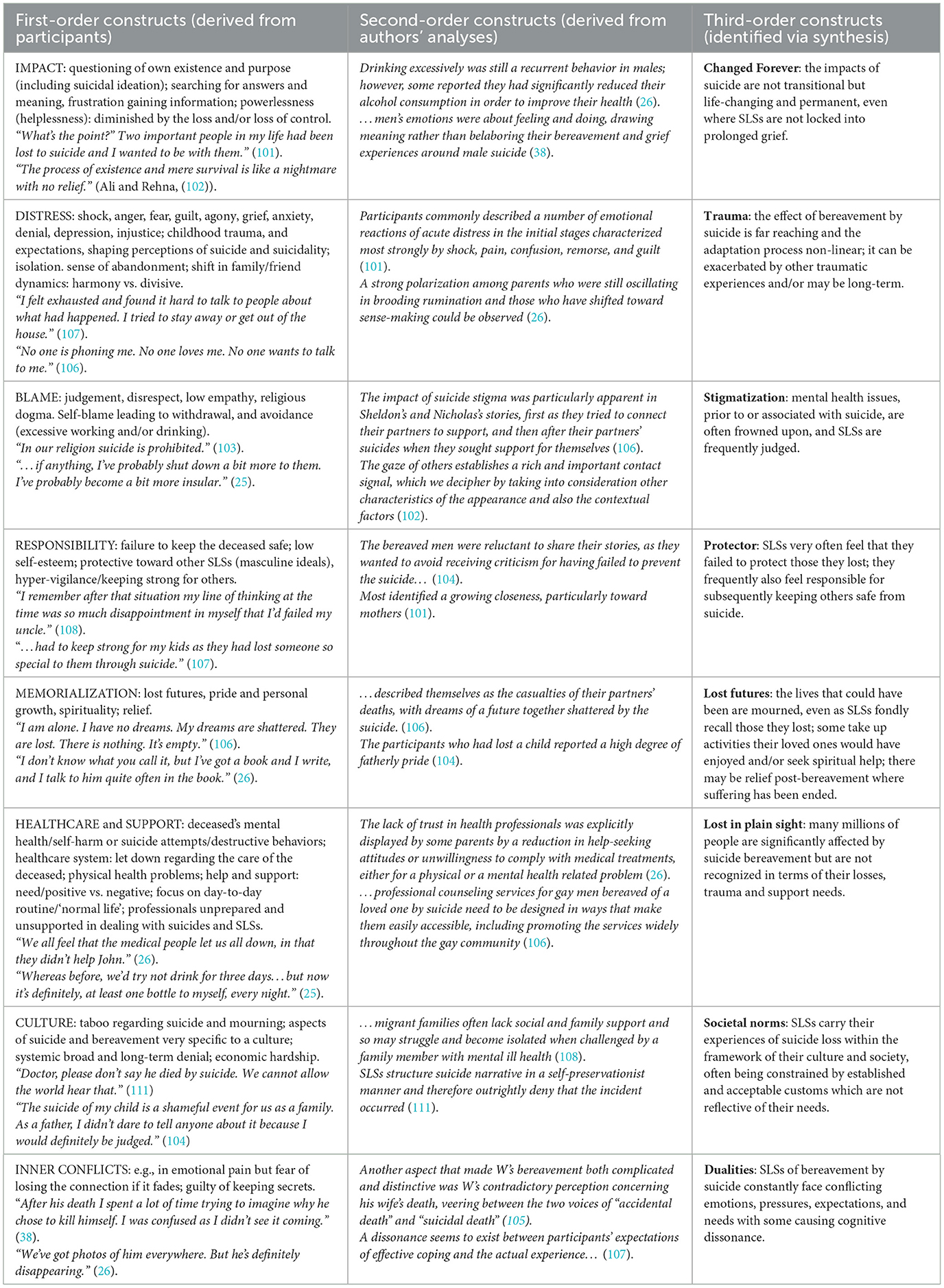
Table 3. Synthesis of concepts based on second- and third-order interpretations.
Table 3 reflects the reciprocal translations of the 14 contributing studies (15 papers). The first- and second-order constructs, included in the table, are representative and not exhaustive. The analysis identified eight concepts (third-order constructs), derived from eight themes (second-order constructs) which were used to generate an all-encompassing new “Suicide Bereavement Model” (line of argument). These concepts (themes) are: changed forever (impact), trauma (distress), stigmatization (blame), protector (responsibility), lost futures (memorialization), lost in plain sight (healthcare and support), societal norms (culture), and dualities (inner conflicts). The model demonstrates how these concepts interplay to reflect a shared core, inherent continuum of devastation mediated, and moderated, by external elements and competing drivers and factors such as relationships (to those lost and fellow SLS), culture, and timeframe (Figure 2). Other research has modeled aspects of the grief associated with suicide loss, from the perspectives of meaning-making and relationships to the deceased, the self and others (39) but the authors are not aware of any model that has holistically encompassed the multitude of factors associated with suicide bereavement.
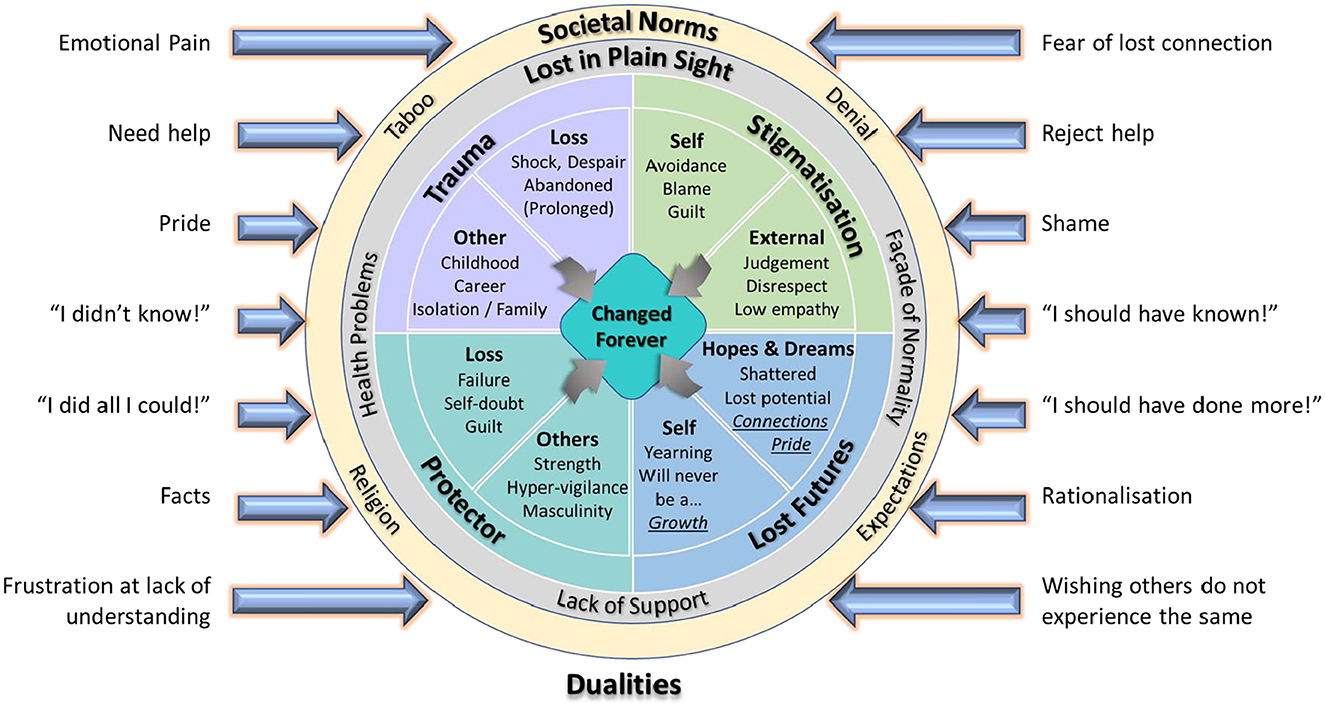
Figure 2. A proposed model of suicide bereavement impact on SLSs.
Changed forever
A universal experience is that SLS' lives are permanently and irrevocably changed (Impact): “It's a thing I still constantly see when I'm asleep and I think of it every day while I'm awake...”; first-order (Paper #6). There are many facets to this, including existential crisis, issues with trust, relationships, avoidance, withdrawal/isolation, and suicide risk. In keeping with the broader literature, from these studies it appears common for SLS to constantly struggle with trying to make sense of the suicide and derive some essence of meaning from their loss. They may be frustrated with a lack of hard information: “Some parents described their frustrations at trying to obtain information from coroners, psychologists and doctors in order to gain some understanding of the reasons for the suicide.”; second-order (Paper #7). Given the breadth, and gravity, of the upheaval and instability created by suicide bereavement, it seems reasonable to conclude that SLS are ‘changed forever'; “I was fragmented...broken that day when [Name] died. The process of existence and mere survival is like a nightmare with no relief.”; first-order (Paper #2).
Trauma
Another recurring thread was the intense emotional turmoil experienced by SLS, encompassing the immediate shock and horror but also angst and longer-term issues such as anxiety and depression (Distress); “Participants acknowledged initial feelings of depersonalization, detachment, blur, isolation/solitude, feeling robotic, and using strategies which created distance with the reality of the loss.”; second-order (Paper #8). Disbelief often propagates a sense of removal and detachment from reality such that SLS are overwhelmed and struggle to relate their level of devastation to those not in the same situation: “… participants in this study reported their feelings of comfort and relief in being understood and talking to others who had shared experiences.”; second-order (Paper #7).. ‘Trauma' associated with suicide bereavement can be long-term and potentially debilitating affecting not only individuals but whole families: “…but Dad and I definitely got further apart. I was resentful toward him and I didn't understand his process [of grieving], it made me really angry.”; first-order (Paper #1).
Stigmatization
Often SLS feel judged by others (Blame) and treated with a lack of empathy: “After the death of my son, I felt ignored by my family. They simply ignored my mourning. They always offer me unhelpful advice like it's time to move on, no one even tried to ask me how I was feeling from inside.”; first-order (Paper #2). Being considered somehow liable for the factors that led to the death of their loved ones amplifies the trauma and distress with which they were already burdened: “…a mother reported feeling her living child directly blamed her for the suicide of her brother.”; second-order (Paper #6). There are also instances where those bereaved hold others liable for the death of their loved ones, within the family or outside of it, and were hostile toward them: “I suppose I'll always question why the medical system had to let her down. I'm looking for somebody to blame, somebody's ass to kick. How did this happen? What could you do to prevent it?”; first-order (Paper #7). Thus, ‘stigmatization' remains a pervasive issue that those bereaved by suicide frequently encounter: “Will people stop asking questions? And if people do not ask questions now then what kind of stories will they fabricate?”; first-order (Paper #2).
Protector
Related to suicide stigma, it also appears common for SLS to hold themselves, at least in part, accountable for the suicide of their loved ones (Responsibility) as they considered it a failure to safeguard them: “As much as people tell you that it's not your fault, it's impossible to not feel wrong for not being able to protect someone you love.”; first-order (Paper #8). This is one area where some aspects of stereotypical masculine expectations were observed but was also noted as a factor for some female SLS: “Another example of avoidance was shown in fathers who reported working excessively in order to avoid the pain of thinking about their loss.”; second-order (Paper #7). The sense that they let down those they lost often leads to low self-esteem and low mood. At the same time, SLS often see themselves as being responsible for the safety and wellbeing of others impacted by the same bereavement: “Even as an adolescent, as the lone male in his immediate family, Joseph felt a responsibility to protect his female family members”; second-order (Paper #10). This includes being stoic to shelter others from their own emotions, assuming responsibility for the emotional care of others impacted by the suicide, and/or extends to hypervigilance due to an innate fear that others close to them may also be at risk of suicide. Both prior to the suicide they experienced, and thereafter, SLS frequently perceive themselves as being in the role of ‘protector': “They redefined their responsibilities to protect the rest of the family and educate others about mental disorders.”; second-order (Paper #4).
Lost futures
The way in which SLS recall those they lost to suicide and commemorate them (Memorialization) seems multi-faceted. Some are left with a sense of emptiness and that their hopes and dreams have been crushed. Some embrace spirituality whilst others have their faith challenged. The latter may relate to the loss but also the way in which their faith, and other followers, view and treat suicide. In some instances, SLS embrace the hopes and wishes of those lost and attempt to emulate them and their goals. A positive aspect is that SLS can maintain, or enhance, strong connections, both to those they lost and other surviving friends and family, and often become driven to help others: “I feel a lot better myself, it helps me by helping other people… I have finally got to a place where I can channel it into something constructive.”; first-order (Paper #1). In one instance (Paper #14) a SLS noted a sense of relief, when they recollect their loved one, because the person lost to suicide was suffering and self-destructive. Some bereaved individuals recall their loved ones with pride, which may be psychologically protective. How SLS experience continuing bonds with their decedents varies depending upon the relationship to the person lost and their gender, the expectations of others, whether they had been able to come to terms with the loss, time since bereavement, and the gender of the bereaved. There are cases where, in addition to their bereavement, SLS mourn “lost futures” such as their decedents being present at a meaningful family event or that they will never be known to younger family members or those yet to be born: “What could they be doing now? Could they have got married and had kids?”; first-order (Paper #1).
Lost in plain sight
Discontent with the provision of healthcare can pre-date bereavement, and was not uncommon, where those lost were seeking or were under treatment prior to their suicide. SLS relate that they considered that their decedents were let down and services were lacking or insufficient: “I suppose I'll always question why the medical system had to let her down.”; first-order (Paper #7). It was also noted that professionals are often unprepared, and unsupported, in dealing with suicides and SLS and, in some cases, SLS find the attitude and abilities of professionals inappropriate and inadequate. SLS also note a lack of transparency regarding the support available to them (Healthcare and Support). They can feel alienated by those within their social network actively avoiding them, but may also contribute to their isolation by maintaining a façade of normality, and feigning coping, whilst enduring inner turmoil: “I'm afraid to talk to my friends because they will ask me about my children, so I avoid them. If we do see each other, I avoid the topic by changing the subject.”; first-order (Paper #4). Whether externally or internally imposed, issues with obtaining professional support, and/or the distancing of SLS from people they interact with daily, can result in them being ‘lost in plain sight' as their plight goes largely unnoticed, or disregarded, by those around them: “I did go to pieces when alone at night.”; first-order (Paper #9).
Societal norms
Beyond the broad stigma associated with suicide, SLS also may have to cope with taboos and systemic denial within the communities in which they live (Culture): “In terms of time of the suicide, the cultural factors present may influence how an individual reacts and copes in the aftermath, as stigma and cultural attitudes about suicide and grief seem to have a key role.”; second-order (Paper #2). Within suicide-bereaved families, there may be unspoken conventions of never discussing the event, and some people even attempt to hide the cause of death from others. This can create an atmosphere of secrecy, such that those not present or very young, at the time of the suicide, are never given a true account of events. Men can be especially prone to regarding suicide as a taboo subject. External to the immediate family, there may be taboos surrounding suicide that arise from religious beliefs or are specific to certain ethnicities: ”In our religion suicide is prohibited. In Islamic law, it is forbidden. I believe that he has reached his destination but he is not in peace. We prepare ourselves for the real-life [life after death] but not this way.”; first-order (Paper #2). In addition to the taboo of suicide, in some cases SLS face, or are party to, outright denial and secrecy regarding the manner in which their loved one died: “Doctor, please don't say he died by suicide.... No, doctor, please, nobody must hear that. You can say anything but... please just don't say that.”; first-order (Paper #13). Pressures on SLS, to withhold their losses, vary by culture and religiosity but, in all cases, the extent to which their bereavement is shared, acknowledged, and accepted falls within ‘societal norms'. A lack of certainty, regarding how their struggles are perceived, can exacerbate avoidant behaviors and contribute to their sense of the world, as they know it, being undermined: “While they felt that men should not seek help, they also felt that if suicide was not a taboo topic in their support group, they could more easily share their feelings within the group.”; second-order (Paper #4).
Dualities
Collectively, the concepts indicate that SLS often experience opposing emotions or viewpoints simultaneously (Inner Conflicts), and this is exemplified by the study of those bereaved by the suicide of their fathers: “Founded by a conflict between two social metanarratives: stigmatizing suicide and strong fatherhood, we argue that it is underpinned by ambiguity.”; second-order (Paper #15). This can be extended, as part of the line of argument, that is characteristic of meta-ethnography, to cover other “dualities” faced by SLS. These include aspects such as SLS logically knowing there was nothing they could have done to prevent the suicide, but feeling guilty nonetheless, or feeling guilt that they let their loved one(s) down even though they know they did all they could for them prior to their deaths: “…my line of thinking at the time was so much disappointment in myself that I'd failed my uncle. That was a burden that I carried with me just forever. Probably last year or this year was the first time in which I sort of now realized that maybe I shouldn't be so hard on myself.”; first-order (Paper #10). One of the studies (Paper #5) describes vacillations between acceptance and denial of suicide plus the struggle to maintain an outward control while constantly dealing with “uncontrollable emotions.” SLS can also be stuck between wanting to mitigate their feelings of loss and being constantly reminded of their trauma: “Whenever I thought of reducing the grief, I remembered my son, and more than that the way he died never get away from my eyes.”; first-order (Paper #2). They can also perceive a disconnect between their own expectations of coping in contrast to the persistence of their grief (Paper #9). Overall, there seem to be a number of dualities, that those bereaved by suicide perceive, such that they often encounter conflicting notions concurrently.
Summary—A novel model for suicide bereavement
The far-reaching, and long-standing, impacts of suicide bereavement with, at its core, the permanency of its life-changing implications, are the basis of the model (line of argument) constructed to describe, and contextualize, the synthesis of concepts gleaned from the 14 studies. This is encapsulated visually in Figure 2, and is proposed to be transferable, fitting suicide bereavement regardless of gender, demographics, relationship to the person lost, timeframe and culture. The proposed model is intended to represent the factors that influence adult SLS' cognitive and behavioral changes when experiencing bereavement by suicide, based on the 14 studies assessed. The deep-seated and fundamental modification to SLS' world view is manifestly impacted by key factors that pervade their lives. There is the emotional shock, often exacerbated by underlying issues and/or prior events, and entrenched grief, intensified by blame (externally and/or internally generated) which frequently results in stigmatization. While SLS struggle to cope with their losses, they may also constantly yearn for futures they can never attain with an associated sense of failure, regarding the safety of those lost, and foreboding, regarding others close to them, which can lead to a constant self-doubt of their capabilities to shield those they love. Surrounding all these very strong reactions, SLS may not get appropriate support, or acknowledgment of the impacts on their health, and feel constrained to outwardly project a level of normality, in their everyday lives, that masks their real, and deep-rooted, psychological state. This is driven by factors including culture, religion, and what they perceive to be expected of them by society, as a whole, or components thereof, such as family members, the workplace and community leaders. The combined pressure of all of these factors, bearing on them in unison, can result in SLS experiencing constantly competing perspectives regarding the circumstances of their bereavements.
The primary objective of this meta-ethnography was to investigate aspects of male suicide bereavement, whereas the model is not gender specific. This is because the analysis did not identify any characteristics that could be exclusively attributed to male participants and most of the studies also included female participants. The secondary objective of this review, to gain insight into how those factors impact SLS' inclination to seek or avoid support, and to continue or not continue with support involvement, is addressed to some extent by the model, but an apparent lack of evidence, from the 14 studies assessed, reinforces the need for further research to elucidate the barriers and enablers relevant to postvention uptake and continuance.
Discussion
The aim of this meta-ethnography was to identify prior qualitative research which summarizes current knowledge on how adult males cope with, and adapt to, bereavement by suicide. Overall, the findings suggested that men coped by both extracting meaningfulness and protecting themselves by emotionally separating from the event. While these studies suggest recognized “masculine-style” of grieving, such as stoicism, fatalism, anger, and over-working, they did not get to the essence of what makes men deal with suicide differently from a “conventional-style” of grieving, typified by women, whereby grievers more openly share their feelings and, consequently, received greater support (40). The Suicide Bereavement Model, described herein, is proposed as being applicable to all adults due to the translation synthesis, core to the meta-ethnography, indicating that the included studies support a pertinent line of argument, from which the model is derived, regardless of gender. Of the papers where participation was limited to men (#3, #4, #5, #8, #10, #11, and #14) the focus was on individuals or narrowly targeted groups. Of the studies including males and females (with at least 50% male participation), very little was noted as specifically attributable to men, and the nature of thematic illumination lends itself to inclusion of participants quotes that best exemplify each theme, often masking whether, or at least not amplifying, any trends in gender alignment with the aspects under review. Overall, based on the information gleaned from the 14 studies that fell into the meta-ethnography, despite some instances of male survivors demonstrating stoicism and assuming the role of protector, it was considered that the syntheses and line of argument are equally applicable to men and woman, as some papers indicated the similar traits emerged in female participants. Therefore, the discussion, and associated Suicide Bereavement Model, is proposed to be applicable regardless of gender.
Changed forever
The review findings reveal that suicide bereavement is complex and has many interwoven facets. These wax and wane, interact, and can have differing individual or collective impacts on SLS' capabilities to adapt and cope, in the immediate term after their loss, but also for many years to come, as they struggle to derive any meaning. In that, the overall impact of bereavement by suicide changes SLS' view of the world, and is interwoven into their belief system, attitudes, and daily behaviors, it can be regarded as a form of embodied biographical disruption (41). The complexity regarding SLS' drives and needs, with respect to making meaning out of their losses, has been noted elsewhere (42). That said, even as those bereaved by suicide process their losses and re-shape their lives, the evidence, herein and in the literature, suggests how they handle their grief is far from linear (43, 44). Rather grief intensity can fluctuate and be reactivated by both internal and external stimuli. While some SLS demonstrate personal growth, partly characterized by strengthening existing relationships and facilitating forging new ones (45), over time, some are often fundamentally lonely (46) and locked into negative patterns of “prolonged grief” (47)—now recognized as a mental health condition, evolving from what was previously described as “complicated grief” (48). Indeed, the combined shifts in SLS' perceptions, experiences, and personal reassessments of every aspect of their lives, are very common resulting in their lives being changed forever.
Trauma
Following suicide bereavement, typically “acute grief” manifests as powerful and disturbing trauma. Psychological shock can be protective, in the short to mid-term, and prevent an individual from being overwhelmed with gloom and desolation. This can allow them to deal with the administrative aspects of death such as registrars, funeral directors, travel, and finances (49). While it has been suggested the difference between suicide bereavement and other types is negligible (50), others have argued that it is very much different, supporting that those bereaved by suicide experience psychological distress above and beyond that associated with other types of loss (19, 51). Men's expression of grief may be delayed, with respect to that of women (52). SLS can feel as if they also lost part of themselves when their loved ones took their own lives (53, 54). In keeping with some of the studies that form part of this meta-ethnography (Papers #3, #10, and #12), it has been observed that other traumas, in the lives of the those bereaved, can significantly impact how they deal with a loss to suicide (55). The trauma, related to suicide, is not limited to individuals but plays out within, and across, family and social constructs (56, 57). However, the majority of studies on suicide focus on specific relationships to those lost (58). Little is known regarding the overall dynamics and how suicide loss impacts generationally (59). Suicide-related trauma can be exacerbated by the bereaved feeling isolated individually (60) or as a family (61) and can be compounded by pre-existing trauma (62). Bereavement by suicide can lead some SLS to question their own existence and undermine their prior value systems (43, 63).
Stigmatization
The stigma associated with suicide is widely recognized as an issue for SLS (64). Where decedents had known mental health issues and/or prior suicide attempts, stigmatization can be prevalent even before their losses (65). SLS sense that, generally, people do not perceive suicide as something that can happen in their families, and the families where it does occur are somehow blighted (66). The bereaved can be viewed as sullied by their loved one's suicide, with outsiders assuming mental illness pervades the family, and that it must be prone to suicidality (67). In some cultures, stigmatization of SLS can arise, and be very strong, within families and communities, as noted in a couple of the studies included is this meta-ethnography (Papers #2 and #13) and elsewhere (61, 68). The potential sequelae of suicide bereavement can further lead to stigmatization, as noted for sufferers of prolonged grief disorder (69). Not only are SLS subject to external stigma, but they may also internalize the unempathetic and judgmental opinions of others (70), thereby attributing to themselves blame, and subsequently shame; such self-stigmatization can lead to SLS adopting non-adaptive thinking and behavior (67). Perceived blame can intensify the negative connotations of suicide loss and magnify the suffering of SLS (71, 72). All facets of blame, in combination, can be exacerbated by inaccurate and inconsiderate media coverage (73).
Protector
As noted in the findings of several of the 14 included studies, SLS often berate themselves for failing to protect their decedents (Papers #3, #4, #8 and #10). This has also been reported elsewhere (74). The assumption of the role as protector, to other SLS, was also noted (Papers #1, #4, #6, #9, #10, #12, and #13) and has been observed more broadly, including female SLS “directing from the shadows” (75) and SLS looking to rescue others in potential suicidal stress (76). With respect to parents that had lost a child, one paper (#6) reported that fathers assumed the role of protector, with respect to their partners, as they perceived the latter requiring support above and beyond their own needs. Elsewhere, men have also been noted to assume the role of carer, toward their female SLS partners and families (13). Where striving for such safeguarding results in SLS becoming hypervigilant, or overprotective, there is an increased emotional burden to bear, on top of individual's own grief (56).
Lost futures
While SLS grieve intensely, related to the loss of a loved one to suicide, and its aftermath, they also speculate on what might have been in terms of their decedent's potential achievements, time and activities they could have shared, and the children they will never have (53, 54). These aspects can also cause an extension and prolongation to their grief (43). SLS often have a strong desire to keep the memories of those they have lost alive and close to them. While generally beneficial, this has been found to add distress where they could not maintain a cohesive bond, due to loss of mementos, waning memories, or a sense that they have lost control of how their relationship to their decedent is manifested (77). Increasingly, memorialization of those lost to suicide is via social media and online platforms (44). While this aspect of grief management is relatively new, there has been research suggesting mixed effects, with indications that SLS can both find an outlet for their emotions and maintain a virtual relationship with the loved one lost via dynamic media (78), but that commemorative internet sites can exacerbate anguish due to a resulting exacerbation of emotional stress (79).
Lost in plain sight
Somewhat as a result of the persistent taboo around suicide, SLS tend to adopt a façade of normality hiding, or even denying, their true feelings (54) with men being more prone to, or even primed for, emotional concealment (80). Such a persona may be maintained in public, but the mask sometimes drops in the context of peer support (81). SLS can be overwhelmed and struggle to relate their level of devastation to those not in the same situation (82) and maintenance of a pretense of not needing help, or a lack of trust in the provider, may result in those bereaved lacking much needed support (83). Men are often unwilling to consult professionals for fear of being perceived as ineffectual and incapable (52). Also, due to suicide not being openly discussed, SLS may be unaware of its prevalence thereby missing the opportunity of support from others similarly afflicted (84). Men are generally assumed to be outwardly more stoic and are noted to use avoidance, such as a focus on work (85) or increased alcohol consumption (86), as part of their grieving pattern. This, though, can be the perpetuation of a gender stereotype and lead to them perceiving that their needs are being ignored (52). Overall, the lack of attention to SLS' needs can create a scenario where they live “under the radar” as they continue to be faced with significant turmoil, in relation to both themselves and those around them, encompassing their role as a protector, the potential futures lost to them by the suicide, stigmatization, and on-going trauma. SLS are prone a variety of mental health issues that have been found to vary by gender, with men being less likely to seek help (87) and their needs not being identified in healthcare policy setting (80). Research has also identified an increased risk of physical ailments in SLS (88) however, they may be less likely to engage with healthcare services if they perceive that those providers did not meet the needs of those lost to suicide (38, 89). In some cases, organizations can lack empathy (46) and be misaligned with the requirements of the bereaved, with healthcare professionals demonstrating a lack of thought and awareness (90) or frustrating SLS by not providing much needed information (91).
Societal norms
The model depicting the multi-faceted negative experiences of SLS, presented herein, does strongly disagree with the notion of a linear nature to grief and bereavement, and other studies have also indicated that suicide bereavement is very much non-linear (92), despite SLS being pressurized, by external expectations to adhere to a broadly accepted sequence of stages exemplified by linear grief models (93). A recent systematic review of male suicide bereavement studies noted that men often experience marked grief responses but are constrained by the accepted customs and anticipated masculine behaviors in society (13). Several of the 14 included studies noted contextual social and cultural taboos, regarding openness and acknowledgment of suicide, with some highlighting deeply rooted negativity and denial (Papers #4 and #13). The level of repudiation seemed to reflect cultural hostility toward suicide, and SLS, and encompassed religiosity. Taboos can be faced at a family level, where members refuse to engage in a dialogue regarding a suicide (71), or can be at a cultural level, driven by the fear of repercussions and/or religious dogma (68, 94). The latter is exacerbated with suicide remaining an illegal act in many countries (95). Losing someone to suicide has been found to both enhance religious beliefs and diminish them, depending on the individual (96). Lack of empathy toward SLS, as a broad cohort, can lead to disenfranchised grief (44) and the judgement by others may be part of an overall stereotyping of bereaved families as being somehow broken or dysfunctional (61, 67). The need for better education, and a shift in societal attitudes, has been noted as necessary for SLS to receive both compassion and meaningful support (97).
Dualities
Some of the papers assessed (Papers #2, #6, #8 and #9) suggested their findings exemplified the Dual Process Model of Bereavement's oscillation between factors associated with loss and those that help restore the bereaved to a level of normality (98). The model herein is not in conflict with it, as the “dualities” described here could reflect the “oscillations,” between “loss-oriented” and “restoration-oriented” behaviors, portrayed in the Dual Process Model. That said, the proposed model suggests that the experience may in fact be more intricate, in that SLS may not necessarily find themselves gravitating to either pole, at any given point in time, but may experience both concurrently. For example, they may intellectually accept that they did not have prior knowledge of their loved ones' struggles but, at the same time, still carry guilt because they cannot escape the feeling that they should have known. Whilst not wishing anyone else to experience the trauma of suicide bereavement, at the same time SLS frequently feel that they are not understood (81) or recognized (99). One of the included studies (#4) contains multiple examples of this type of conflicting emotions/experiences, such as emotional regulation vs. uncontrollable emotional responses, which fight for dominance. So, instead of merely oscillating between aspects of bereavement, the proposed model supports that SLS often experience both faces of the dualities at the same time, that is, they co-exist in perpetual contention. Elsewhere, such opposing drivers have been described as leaving SLS in a perpetual liminal state (100).
Implications
The proposed Suicide Bereavement Model brings together perspectives across both the studies included in this meta-ethnography and the broader literature. It could be used in practice (clinical, therapy/counseling, education, peer support) to better understand the highly complex and interwoven components of suicide bereavement, thereby facilitating improved and extended services available to SLS that are more in-tune with their needs. A common perception, among SLS, is that those not bereaved by suicide can never understand their situation. While the model cannot confer full comprehension of suicide bereavement, it can go a long way to assist those looking to assist SLS by providing a platform for dialogue and empathy.
Strengths, limitations, and reflexivity
The 14 primary studies are all relatively recent (2010 and after), demonstrating modern approaches, and adopted recognized qualitative research methods. Adopting the eMERGe project guidance (33) provided structure and rigor to the process of conducting this meta-ethnography. A simplistic (alphabetical by author) approach for synthesizing the studies was adopted to mitigate any potential bias regarding the study locations, demographics, methods, and findings. Throughout its development, the team focused on a clear rationale, distillation of appropriate insights and extrapolation of concepts, a pragmatic and critical assessment of findings, and the creation of a clear model, that describes the output, to achieve high quality at each process stage, and overall (29). There was a strong accord within the research team throughout the stages of the meta-ethnography and the derivation of the model that describes suicide bereavement holistically. The model proposed is novel, with its generally applicability bolstered by the inclusion of studies with a high proportion of male participation, and it seems to resonate with the broader literature on the impacts of suicide bereavement.
Assessment of the 14 studies highlighted some stereotypical male behaviors, such as stoicism and assumption of gender specific roles, but did not elucidate detailed gender variations in terms of accessing and embracing support. However, that emphasizes that this remains an under-researched area. Another potential limitation is that study authors selectively include quotes, from participants, to illustrate a theme, but there may be numerous other quotes, that were not included, from participants. It is possible that papers with lower male involvement (excluded from the present review) could contain information of relevance to male attitudes to suicide bereavement and support. As is the case with most psychology research, the majority of participants originated in ethnically European dominated locations, with limited cultural homogeneity, potentially limiting the transferability of the model more broadly. Overall, this meta-ethnography emphasized the dearth of research into postvention in general, and especially regarding its applicability to men, indicating the need for further research.
Conclusion
The research team is not aware of any other model that comprehensively describes suicide bereavement. It portrays that suicide bereavement is highly complex with many interwoven facets that are constantly interacting and can be in contention. It is therefore important that those providing support services to SLS are aware of this complexity and recognize that, while addressing individual components of suicide bereavement, such as the initial grief and guilt, may make sense pragmatically, they need to be considered in the context of the totality of SLS' long-term needs, and not seen as isolated goals or endpoints. SLS strongly believe that suicide bereavement is different to other types of loss, which is supported by qualitative studies, and thus healthcare professionals, emergency service personnel and coroners should acknowledge this and act accordingly. Suicide bereavement permanently shifts SLS' perspectives and any improvement in coping, or personal regrowth, is not a linear process but cyclical in nature with the likelihood of many setbacks, often triggered by anniversaries, birthdays, holidays and other key dates or events, such as a family celebration from which the person lost is conspicuously absent. Those that deal with the suicide bereaved need appropriate training to be able to interact with them effectively, and with sensitivity and empathy, to meet their needs.
Most of the research into suicidology has a focus on prevention, which is highly important but does not cover the impact of suicide on those left behind. Research into the implications for men bereaved by suicide remains a rarity and understanding the needs of men plus, crucially, the reasons why many men do not engage with support services is an under-investigated aspect. The numbers of men that have historically participated in suicide research are low and those that do so may be atypical due to their willingness to share their experiences. Papers published where participants are mixed gender may mask factors especially pertinent to men as researchers chose quotes best suited, to make a given point, which may come from a female participant even though the issue in question may have been predominately a concern to the men in the study. More evidence is needed on why men mostly avoid suicide support/research and how they can be encouraged to participate. Some studies identify avoidance behaviors in male SLS, including over-working and excessive alcohol consumption, but these are symptomatic and do not get to the underlying motivators. Studies often reinforce male gender stereotypes which might perpetuate their grief being masked or even suppressed. Hence the Suicide Bereavement Model is being proposed as being equally applicable to men and women, as there is insufficient evidence to differentiate at this point in time.
Data availability statement
The data analyzed were from publicly available published academic papers.
Author contributions
JW: Data curation, Formal analysis, Methodology, Resources, Writing – original draft, Writing – review & editing. CL: Conceptualization, Methodology, Supervision, Validation, Writing – review & editing. JC: Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1596961/full#supplementary-material
Footnotes
1. ^The Chen and Laitila paper met the criteria at the time, as a pre-publication, but has since been formally published in 2024.
2. ^Further methodological details are available from the corresponding author.
3. ^Further quality assessment details are available from the corresponding author.
References
1. Levi-Belz Y, Birnbaum S. Depression and suicide ideation among suicide-loss survivors: a six-year longitudinal study. Int J Environ Res Public Health. (2022) 19:16561. doi: 10.3390/ijerph192416561
2. Ilic M, Ilic I. Worldwide suicide mortality trends (2000–2019): a joinpoint regression analysis. World J Psychiatry. (2022) 12:1044. doi: 10.5498/wjp.v12.i8.1044
3. National Records of Scotland. Probable Suicides (2024). Available online at: https://www.nrscotland.gov.uk/publications/probable-suicides-2023/ (accessed October 29, 2024).
4. Northern Ireland Statistics and Research Agency. Suicide Deaths (2023). Available online at: https://www.nisra.gov.uk; https://www.nisra.gov.uk/publications/suicide-statistics-2022 (accessed October 29, 2024).
5. Office of National Statistics. Suicides in England and Wales (2024). Available online at: https://www.ons.gov.uk; https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/suicidesintheunitedkingdomreferencetables (accessed October 29, 2024).
6. Central Statistics Office. Open Data Platform (2023). Available online at: https://data.cso.ie/. https://data.cso.ie/ (accessed October 31, 2023).
7. Tait G, Carpenter B. The continuing implications of the ‘crime' of suicide: a brief history of the present. Int J Law Context. (2016) 12:210–24. doi: 10.1017/S1744552316000021
8. Anthony G, Aronson JK, Brittain R, Heneghan C, Richards GC. Preventable suicides involving medicines: a systematic case series of coroners' reports in England and Wales. Public Health Pract. (2024) 7:100491. doi: 10.1016/j.puhip.2024.100491
9. Quayle K, Jones P, Di Simplicio M, Kamboj S, Pitman A. Exploring the phenomenon of intrusive mental imagery after suicide bereavement: a qualitative interview study in a British sample. PLoS ONE. (2023) 18:e0284897. doi: 10.1371/journal.pone.0284897
10. Cerel J, Brown MM, Maple M, Singleton M, Van de Venne J, Moore M, et al. How many people are exposed to suicide? Not six. Suicide Life Threat Behav. (2019) 49:529–34. doi: 10.1111/sltb.12450
11. McDonnell S, Flynn S, Shaw J, Smith S, McGale B, Hunt IM. Suicide bereavement in the UK: descriptive findings from a national survey. Suicide Life Threat Behav. (2022) 52:887–97. doi: 10.1111/sltb.12874
12. O'Connell S, Tuomey F, O'Brien C, Daly C, Ruane-McAteer E, Khan A, et al. AfterWords: A Survey of People Bereaved by Suicide in Ireland. Cork; Dublin: National Suicide Research Foundation and HUGG (2022).
13. Logan N, Krysinska K, Andriessen K. Impacts of suicide bereavement on men: a systematic review. Front Public Health. (2024) 12:1372974. doi: 10.3389/fpubh.2024.1372974
14. Andriessen K, Krysinska K, Kõlves K, Reavley N. Suicide postvention service models and guidelines 2014–2019: a systematic review. Front Psychol. (2019) 10:2677. doi: 10.3389/fpsyg.2019.02677
15. Harper M, O‘Connor RC, O'Carroll RE. Factors associated with grief and depression following the loss of a child: a multivariate analysis. Psychol Health Med. (2014) 19:247–52. doi: 10.1080/13548506.2013.811274
16. Dyregrov K, Dyregrov A. Siblings after suicide-the forgotten bereaved. Suicide Life Threat Behav. (2005) 35:714–24. doi: 10.1521/suli.2005.35.6.714
17. Erlangsen A, Runeson B, Bolton JM, Wilcox HC, Forman JL, Krogh J, et al. Association between spousal suicide and mental, physical, and social health outcomes: a longitudinal and nationwide register-based study. JAMA Psychiatry. (2017) 74:456–64. doi: 10.1001/jamapsychiatry.2017.0226
18. Andriessen K, Krysinska K, Hill NTM, Reifels L, Robinson J, Reavley N, et al. Effectiveness of interventions for people bereaved through suicide: a systematic review of controlled studies of grief, psychosocial and suicide-related outcomes. BMC Psychiatry. (2019) 19:1–15. doi: 10.1186/s12888-019-2020-z
19. Bellini S, Erbuto D, Andriessen K, Milelli M, Innamorati M, Lester D, et al. Depression, hopelessness, and complicated grief in survivors of suicide. Front Psychol. (2018) 9:198. doi: 10.3389/fpsyg.2018.00198
20. Zortea TC, Cleare S, Melson AJ, Wetherall K, O'Connor RC. Understanding and managing suicide risk. Br Med Bull. (2020) 134:73–84. doi: 10.1093/bmb/ldaa013
21. Flemming K, Noyes J. Qualitative evidence synthesis: where are we at? Int J Qual Methods. (2021) 20:1–13. doi: 10.1177/1609406921993276
22. Noblit GW. Meta-ethnography in Education. Oxford: Oxford University Press (2019). doi: 10.1093/acrefore/9780190264093.013.348
23. Soundy A, Heneghan NR. Meta-ethnography. Int Rev Sport Exerc Psychol. (2022) 15:266–86. doi: 10.1080/1750984X.2021.1966822
24. Booth A. “Brimful of STARLITE”: toward standards for reporting literature searches. J Med Libr Assoc. (2006) 94:421.
25. Ross V, Kõlves K, Kunde L, De Leo D. Parents' experiences of suicide-bereavement: a qualitative study at 6 and 12 months after loss. Int J Environ Res Public Health. (2018) 15:618. doi: 10.3390/ijerph15040618
26. Entilli L, Ross V, De Leo D, Cipolletta S, Kõlves K. Experiences of parental suicide-bereavement: a longitudinal qualitative analysis over two years. Int J Environ Res Public Health. (2021) 18:564. doi: 10.3390/ijerph18020564
27. Campbell R, Pound P, Morgan M, Daker-White G, Britten N, Pill R, et al. Evaluating meta-ethnography: systematic analysis and synthesis of qualitative research. Health Technol Assess. (2011) 15:1–164. doi: 10.3310/hta15430
28. Noblit GW, Hare RD. Meta-ethnography: Synthesizing Qualitative Studies. Newbury Park, CA: Sage (1988). doi: 10.4135/9781412985000
29. Toye F, Seers K, Allcock N, Briggs M, Carr E, Andrews J, et al. ‘Trying to pin down jelly'-exploring intuitive processes in quality assessment for meta-ethnography. BMC Med Res Methodol. (2013) 13:1–12. doi: 10.1186/1471-2288-13-46
30. Critical Appraisal Skills Programme. CASP Qualitative Studies Checklist (2018). Available online at: https://casp-uk.net/images/checklist/documents/CASP-Qualitative-Studies-Checklist/CASP-Qualitative-Checklist-2018.pdf (accessed May 9, 2023).
31. Sattar R, Lawton R, Panagioti M, Johnson J. Meta-ethnography in healthcare research: a guide to using a meta-ethnographic approach for literature synthesis. BMC Health Serv Res. (2021) 21:1–13. doi: 10.1186/s12913-020-06049-w
32. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. (2021) 134:178–89. doi: 10.1016/j.jclinepi.2021.03.001
33. France EF, Cunningham M, Ring N, Uny I, Duncan EAS, Jepson RG, et al. Improving reporting of meta-ethnography: the eMERGe reporting guidance. BMC Med Res Methodol. (2019) 19:25. doi: 10.1186/s12874-018-0600-0
34. Rethlefsen ML, Page MJ. PRISMA 2020 and PRISMA-S: common questions on tracking records and the flow diagram. J Med Libr Assoc. (2022) 110:253. doi: 10.5195/jmla.2022.1449
35. Peters K, Murphy G, Jackson D. Events prior to completed suicide: perspectives of family survivors. Issues Ment Health Nurs. (2013) 34:309–16. doi: 10.3109/01612840.2012.751639
36. Atkins S, Lewin S, Smith H, Engel M, Fretheim A, Volmink J. Conducting a meta-ethnography of qualitative literature: lessons learnt. BMC Med Res Methodol. (2008) 8:1–10. doi: 10.1186/1471-2288-8-21
37. Britten N, Campbell R, Pope C, Donovan J, Morgan M, Pill R. Using meta ethnography to synthesise qualitative research: a worked example. J Health Serv Res Policy. (2002) 7:209–15. doi: 10.1258/135581902320432732
38. Oliffe JL, Broom A, Rossnagel E, Kelly MT, Affleck W, Rice SM. Help-seeking prior to male suicide: bereaved men perspectives. Soc Sci Med. (2020) 261:113173. doi: 10.1016/j.socscimed.2020.113173
39. Sands D. A tripartite model of suicide grief: meaning-making and the relationship with the deceased. Grief Matters. (2009) 12:10–17. https://search.informit.org/doi/epdf/10.3316/INFORMIT.995255247342864
40. Zinner ES. Being a man about it: the marginalization of men in grief. Illn Crisis Loss. (2000) 8:181–8. doi: 10.1177/105413730000800206
41. Engman A. Embodiment and the foundation of biographical disruption. Soc Sci Med. (2019) 225:120–7. doi: 10.1016/j.socscimed.2019.02.019
42. Post E, Vis J, Boynton HM. The clinical utility of spirituality and religion in meaning-making theory for suicide loss survivors: a scoping review. Religions. (2023) 14:73. doi: 10.3390/rel14010073
43. Kaur R, Stedmon J. A phenomenological enquiry into the impact of bereavement by suicide over the life course. Mortality. (2022) 27:53–74. doi: 10.1080/13576275.2020.1823351
44. Mathieu S, Todor R, De Leo D, Kõlves K. Coping styles utilized during suicide and sudden death bereavement in the first six months. Int J Environ Res Public Health. (2022) 19:14709. doi: 10.3390/ijerph192214709
45. Gilo T, Feigelman W, Levi-Belz Y. Forgive but not forget: from self-forgiveness to posttraumatic growth among suicide-loss survivors. Death Stud. (2022) 46:1870–9. doi: 10.1080/07481187.2020.1864064
46. Nilsson C, Blomberg K, Bremer A. Existential loneliness and life suffering in being a suicide survivor: a reflective lifeworld research study. Int J Qual Stud Health Well-being. (2022) 17:2122157. doi: 10.1080/17482631.2022.2122157
47. Grafiadeli R, Glaesmer H, Wagner B. Loss-related characteristics and symptoms of depression, prolonged grief, and posttraumatic stress following suicide bereavement. Int J Environ Res Public Health. (2022) 19:10277. doi: 10.3390/ijerph191610277
48. Lenferink LIM, Van Den Munckhof MJA, De Keijser J, Boelen PA. DSM-5-TR prolonged grief disorder and DSM-5 posttraumatic stress disorder are related, yet distinct: confirmatory factor analyses in traumatically bereaved people. Eur J Psychotraumatol. (2021) 12:1–14. doi: 10.1080/20008198.2021.2000131
49. Tal Young I, Iglewicz A, Glorioso D, Lanouette N, Seay K, Ilapakurti M, et al. Suicide bereavement and complicated grief. Dialogues Clin Neurosci. (2012) 14:177. doi: 10.31887/DCNS.2012.14.2/iyoung
50. Carmassi C, Calderani E, Pocai B, Gemignani S, Menichini M, Manni C, et al. Suicide survivors with complicated grief (CG) - do they differ from other kinds of bereaved with CG. Eur Neuropsychopharmacol. (2013) 23:S626–7. doi: 10.1016/S0924-977X(13)70996-9
51. Nam I. Suicide bereavement and complicated grief: experiential avoidance as a mediating mechanism. J Loss Trauma. (2016) 21:325–34. doi: 10.1080/15325024.2015.1067099
52. Grad OT, Treven M, Krysinska K. “Suicide bereavement and gender.” In: Andriessen K, Krysinska K, Grad O, , editors. Postvention in Action: The International Handbook of Suicide Bereavement Support. Göttingen: Hogrefe Publishing GmbH (2017). p. 39–49. doi: 10.1027/0227-5910/a000502
53. Kalischuk RG, Hayes VE. Grieving, mourning, and healing following youth suicide: a focus on health and well being in families. Omega. (2004) 48:45–67. doi: 10.2190/UA8F-Q4QK-AM1Q-HAHJ
54. Whitebrook J, Churchyard JS. ‘You just wear a mask': an interpretative phenomenological analysis study to explore the impacts of bereavement by suicide among peer support group members. Pre-Print, In Press (2025). Available online at: https://repository.uwl.ac.uk/id/eprint/11256/
55. Macdonald D, Nicolopoulos A, McLachlan K, Habak S, Christensen H, Boydell KM. Tragedies, fates, furies and fuels: narratives of individuals bereaved by suicide. Int J Environ Res Public Health. (2022) 19:8715. doi: 10.3390/ijerph19148715
56. Azorina V, Morant N, Nesse H, Stevenson F, Osborn D, King M, et al. The perceived impact of suicide bereavement on specific interpersonal relationships: a qualitative study of survey data. Int J Environ Res Public Health. (2019) 16:1801. doi: 10.3390/ijerph16101801
57. Contessa JC, Padoan CS, Silva JLGD, Magalhães PV. A qualitative study on traumatic experiences of suicide survivors. OMEGA. (2023) 87:730–44. doi: 10.1177/00302228211024486
58. Andriessen K, Krysinska K, Rickwood D, Pirkis J. “It changes your orbit”: the impact of suicide and traumatic death on adolescents as experienced by adolescents and parents. Int J Environ Res Public Health. (2020) 17:9356. doi: 10.3390/ijerph17249356
59. Cerel J, Jordan JR, Duberstein PR. The impact of suicide on the family. Crisis. (2008) 29:38–44. doi: 10.1027/0227-5910.29.1.38
60. McDaniel BM, Daly P, Pacheco CL, Crist JD. Experiences with suicide loss: a qualitative study. Clin Nurs Res. (2022) 31:1491–9. doi: 10.1177/10547738221119344
61. Lee E. Experiences of bereaved families by suicide in South Korea: a phenomenological study. Int J Environ Res Public Health. (2022) 19:2969. doi: 10.3390/ijerph19052969
62. Hafford-Letchfield T, Hanna J, Grant E, Ryder-Davies L, Cogan N, Goodman J, et al. “It's a living experience”: bereavement by suicide in later life. Int J Environ Res Public Health. (2022) 19:7217. doi: 10.3390/ijerph19127217
63. Castelli Dransart DA. Reclaiming and reshaping life: patterns of reconstruction after the suicide of a loved one. Qual Health Res. (2017) 27:994–1005. doi: 10.1177/1049732316637590
64. Pitman A, Stevenson F, Osborn DPJ, King MB. The stigma associated with bereavement by suicide and other sudden deaths: a qualitative interview study. Soc Sci Med. (2018) 198:121–9. doi: 10.1016/j.socscimed.2017.12.035
65. Sheehan LL Corrigan PW Al-Khouja MA Stigma Stigma of Suicide Research Team. Stakeholder perspectives on the stigma of suicide attempt survivors. Crisis. (2017) 38, 73–81. doi: 10.1027/0227-5910/a000413
66. Peters K, Cunningham C, Murphy G, Jackson D. ‘People look down on you when you tell them how he died': qualitative insights into stigma as experienced by suicide survivors. Int J Ment Health Nurs. (2016) 25:251–7. doi: 10.1111/inm.12210
67. Sheehan LL, Corrigan PW, Al-Khouja M, Lewy SA, Major DR, Mead J, et al. Behind closed doors: the stigma of suicide loss survivors. OMEGA. (2018) 77:330. doi: 10.1177/0030222816674215
68. Khan AR, Ratele K, Helman R, Dlamini S, Makama R. Masculinity and suicide in Bangladesh. OMEGA. (2020). 86:218–240. doi: 10.1177/0030222820966239
69. Eisma MC. Public stigma of prolonged grief disorder: an experimental study. Psychiatry Res. (2018) 261:173–7. doi: 10.1016/j.psychres.2017.12.064
70. Testoni I, Francescon E, De Leo D, Santini A, Zamperini A. Forgiveness and blame among suicide survivors: a qualitative analysis on reports of 4-year self-help-group meetings. Community Ment Health J. (2018) 55:360–8. doi: 10.1007/s10597-018-0291-3
71. Creuzé C, Lestienne L, Vieux M, Chalancon B, Poulet E, Leaune E. Lived experiences of suicide bereavement within families: a qualitative study. Int J Environ Res Public Health. (2022) 19:13070. doi: 10.3390/ijerph192013070
72. Spillane A, Matvienko-Sikar K, Larkin C, Corcoran P, Arensman E. How suicide-bereaved family members experience the inquest process: a qualitative study using thematic analysis. Int J Qual Stud Health Well-being. (2019) 14:1563430. doi: 10.1080/17482631.2018.1563430
73. Gregory P, Stevenson F, King M, Osborn D, Pitman A. The experiences of people bereaved by suicide regarding the press reporting of the death: qualitative study. BMC Public Health. (2020) 20:1–14. doi: 10.1186/s12889-020-8211-1
74. Royden LJ. Forgotten but not gone: a heuristic literature review of sibling suicide bereavement. Aotearoa N Z Soc Work. (2021) 33:19–31. doi: 10.11157/anzswj-vol33iss2id862
75. Gordon E, McElvaney R. Directing from the shadows: women's experiences of male relative suicide bereavement. J Fam Ther. (2022) 44:396–407. doi: 10.1111/1467-6427.12388
76. Praetorius RT, Rivedal J. Navigating out of the ocean of “Why”—a qualitative study of the trajectory of suicide bereavement. Illn Crisis Loss. (2020) 28:347–62. doi: 10.1177/1054137317741714
77. Goodall R, Krysinska K, Andriessen K. Continuing bonds after loss by suicide: a systematic review. Int J Environ Res Public Health. (2022) 19:2963. doi: 10.3390/ijerph19052963
78. Shoib S, Chandradasa M, Nahidi M, Amanda TW, Khan S, Saeed F, et al. Facebook and suicidal behaviour: user experiences of suicide notes, live-streaming, grieving and preventive strategies—a scoping review. Int J Environ Res Public Health. (2022) 19:13001. doi: 10.3390/ijerph192013001
79. Abbate L, Chopra J, Poole H, Saini P. Evaluating postvention services and the acceptability of models of postvention: a systematic review. OMEGA. (2024) 90:00302228221112723. doi: 10.1177/00302228221112723
80. River J, Flood M. Masculinities, emotions and men's suicide. Sociol Health Illn. (2021) 43:910–27. doi: 10.1111/1467-9566.13257
81. Hybholt L, Higgins A, Buus N, Berring LL, Connolly T, Erlangsen A, et al. The spaces of peer-led support groups for suicide bereaved in Denmark and the Republic of Ireland: a focus group study. Int J Environ Res Public Health. (2022) 19:9898. doi: 10.3390/ijerph19169898
82. Näppä U, Björkman-Randström K. Experiences of participation in bereavement groups from significant others' perspectives; a qualitative study. BMC Palliat Care. (2020) 19:1–10. doi: 10.1186/s12904-020-00632-y
83. GeleŽelyte O, Gailiene D, Latakiene J, MaŽulyte-Rašytine E, Skruibis P, Dadašev S, et al. Factors of seeking professional psychological help by the bereaved by suicide. Front Psychol. (2020) 11:592. doi: 10.3389/fpsyg.2020.00592
84. Feigelman W, Cerel J, McIntosh JL, Brent D, Gutin N. Suicide exposures and bereavement among American adults: evidence from the 2016 general social survey. J Affect Disord. (2018) 227:1–6. doi: 10.1016/j.jad.2017.09.056
85. Andriessen K, Krysinska K. Essential questions on suicide bereavement and postvention. Int J Environ Res Public Health. (2012) 9:24–32. doi: 10.3390/ijerph9010024
86. Rivart P, Wainwright V, Flynn S, Hunt IM, Shaw J, Smith S, et al. Ethnic minority groups' experiences of suicide bereavement: a qualitative exploratory study. Int J Environ Res Public Health. (2021) 18:11860. doi: 10.3390/ijerph182211860
87. van de Venne J, Cerel J, Moore M, Maple M. Sex differences in mental health outcomes of suicide exposure. Arch Suicide Res. (2019) 24:158–85. doi: 10.1080/13811118.2019.1612800
88. Spillane A, Larkin C, Corcoran P, Matvienko-Sikar K, Riordan F, Arensman E. Physical and psychosomatic health outcomes in people bereaved by suicide compared to people bereaved by other modes of death: a systematic review. BMC Public Health. (2017) 17:1–16. doi: 10.1186/s12889-017-4930-3
89. Pettersen R, Omerov P, Steineck G, Dyregrov A, Titelman D, Dyregrov K, et al. Suicide-bereaved siblings' perception of health services. Death Stud. (2015) 39:323–31. doi: 10.1080/07481187.2014.946624
90. Peters K, Cunningham C, Murphy G, Jackson D. Helpful and unhelpful responses after suicide: experiences of bereaved family members. Int J Ment Health Nurs. (2016) 25:418–25. doi: 10.1111/inm.12224
91. De Leo D, Guarino A, Congregalli B, Zammarrelli J, Valle A, Paoloni S, et al. Receiving notification of unexpected and violent death: a qualitative study of italian survivors. Int J Environ Res Public Health. (2022) 19:10709. doi: 10.3390/ijerph191710709
92. Watson C, Cutrer-Párraga EA, Heath M, Miller EE, Young TA, Wilson S. Very young child survivors' perceptions of their father's suicide: Exploring bibliotherapy as postvention support. Int J Environ Res Public Health. (2021) 18:11384. doi: 10.3390/ijerph182111384
93. Maple M, Edwards HE, Minichiello V, Plummer D. Still part of the family: the importance of physical, emotional and spiritual memorial places and spaces for parents bereaved through the suicide death of their son or daughter. Mortality. (2013) 18:54–71. doi: 10.1080/13576275.2012.755158
94. Shakil M. A qualitative analysis of suicides committed by the students in Pakistan. Pak J Med Res. (2019) 58:35–40.
95. Scocco P, Preti A, Totaro S, Ferrari A, Toffol E. Stigma and psychological distress in suicide survivors. J Psychosom Res. (2017) 94:39–46. doi: 10.1016/j.jpsychores.2016.12.016
96. Abossein S, Santurri L, Borrero L, Shaw L. Lived experiences of individuals bereaved by the suicide death of a sibling. J Ment Health Couns. (2022) 44:133–52. doi: 10.17744/mehc.44.2.03
97. Marek F, Oexle N. Supportive and non-supportive social experiences following suicide loss: a qualitative study. BMC Public Health. (2024) 24:1190. doi: 10.1186/s12889-024-18545-3
98. Stroebe MS, Schut HAW. The dual process model of coping with bereavement: a decade on. Omega. (2010) 61:273–89. doi: 10.2190/OM.61.4.b
99. Pitman A, De Souza T, Khrisna Putri A, Stevenson F, King M, Osborn D, et al. Support needs and experiences of people bereaved by suicide: qualitative findings from a cross-sectional british study of bereaved young adults. Int J Environ Res Public Health. (2018) 15:666. doi: 10.3390/ijerph15040666
100. Bristowe K, Timmins L, Pitman A, Braybrook D, Marshall S, Johnson K, et al. Between loss and restoration: the role of liminality in advancing theories of grief and bereavement. Soc Sci Med. (2024) 344:116616. doi: 10.1016/j.socscimed.2024.116616
101. Adams E, Hawgood J, Bundock A, Kõlves K. A phenomenological study of siblings bereaved by suicide: a shared experience. Death Stud. (2019) 43:324–32. doi: 10.1080/07481187.2018.1469055
102. Ali U, Rehna T. Grief reactions and suicide bereavement in the context of stigma among parents: an interpretative phenomenological analysis. Ann Méd Psychol. (2023) 18:598–603. doi: 10.1016/j.amp.2022.04.016
103. Briggs S, Goldblatt MJ, Lindner R, Maltsberger JT, Fiedler G. Suicide and trauma: a case discussion. Psychoanal Psychother. (2012) 26:13–33. doi: 10.1080/02668734.2011.652657
104. Chan TS, Cheung M. The “men in grief” phenomenon among suicide bereaved Chinese men in Hong Kong. Death Stud. (2020) 46:1845–52. doi: 10.1080/07481187.2020.1855609
105. Chen Y, Laitila A. Initial-stage suicide bereavement experiences: a case study. OMEGA J. Death Dying. (2024) 89:1514–34. doi: 10.1177/00302228221095905
106. Ferlatte O, Oliffe JL, Salway T, Knight R. Stigma in the bereavement experiences of gay men who have lost a partner to suicide. Cult Health Sex. (2019) 21:1273–89. doi: 10.1080/13691058.2018.1556344
107. Gaffney M, Hannigan B. Suicide bereavement and coping: a descriptive and interpretative analysis of the coping process. Proc Soc Behav Sci. (2010) 5:526–35. doi: 10.1016/j.sbspro.2010.07.137
108. Jackson D, Peters K, Murphy G. Suicide of a close family member through the eyes of a child: a narrative case study report. J Child Health Care. (2015) 19:495–503. doi: 10.1177/1367493513519297
109. Lee E, Kim SW, Enright RD. Case study of a survivor of suicide who lost all family members through parent-child collective suicide. Crisis. (2015) 36:71–5. doi: 10.1027/0227-5910/a000286
110. Nelson PA, Cordingley L, Kapur N, Chew-Graham C, Shaw J, Smith S, et al. 'We're the first port of call' - perspectives of ambulance staff on responding to deaths by suicide: A qualitative study. Front Psychol. (2020) 11:722. doi: 10.3389/fpsyg.2020.00722
111. Ohayi SR. “Doctor, please don't say he died by suicide”: exploring the burden of suicide survivorship in a developing country. Egypt J For Sci. (2019) 9:1–7. doi: 10.1186/s41935-019-0153-3
112. Oliffe JL, Broom A, Kelly MT, Bottorff JL, Creighton GM, Ferlatte O. Men on losing a male to suicide: a gender analysis. Qual Health Res. (2018) 28:1383–94. doi: 10.1177/1049732318769600
Keywords: suicide loss survivors, suicide bereavement model, meta-ethnography, qualitative research, postvention
Citation: Whitebrook J, Lafarge C and Churchyard JS (2025) A suicide bereavement model: based on a meta-ethnography of the experiences of adult suicide loss survivors. Front. Public Health 13:1596961. doi: 10.3389/fpubh.2025.1596961
Received: 01 April 2025; Accepted: 13 June 2025;
Published: 14 July 2025.
Edited by:
Ricardo Gusmão, University of Porto, PortugalReviewed by:
Molnar Rebeca Isabela, Emergency County Hospital Targu Mures, RomaniaRafailia Zavrou, Cyprus University of Technology, Cyprus
Copyright © 2025 Whitebrook, Lafarge and Churchyard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: John Whitebrook, am9obi53aGl0ZWJyb29rQHJlc2VhcmNoLnV3bC5hYy51aw==