 Julio Cesar Quispe Mamani1*
Julio Cesar Quispe Mamani1* Santotomas Licimaco Aguilar Pinto2Amira Carpio Maraza3Yethy Melixa Poma Palma4Lucas Ponce Quispe3
Santotomas Licimaco Aguilar Pinto2Amira Carpio Maraza3Yethy Melixa Poma Palma4Lucas Ponce Quispe3 Nelly Beatriz Quispe Maquera5
Nelly Beatriz Quispe Maquera5 Balbina Esperanza Cutipa Quilca3
Balbina Esperanza Cutipa Quilca3 Betsy Quispe Quispe5Paola Huarca Flores6
Betsy Quispe Quispe5Paola Huarca Flores6 Dominga Asunción Calcina Álvarez7Lycet Maria Caceres Bustinza8
Dominga Asunción Calcina Álvarez7Lycet Maria Caceres Bustinza8- 1Faculty of Economic Engineering, National University of Altiplano, Puno, Peru
- 2Faculty of Administrative Sciences, Andean University Nestor Caceres Velasquez, Juliaca, Peru
- 3Faculty of Accounting and Administrative Sciences, National University of Altiplano, Puno, Peru
- 4Faculty of Administrative and Human Sciences, National University of Altiplano, Puno, Peru
- 5Faculty of Health Sciences, Professional School of Dentistry, National University of the Altiplano, Puno, Peru
- 6Faculty of Social Sciences and Humanities, Santa Maria Catholic University, Arequipa, Peru
- 7Academic Department of Education and Humanities, Faculty of Education, Amazon National University of Madre of Dios, Puerto Maldonado, Peru
- 8Professional School of Agroindustrial Engineering, Micaela Bastidas National University of Apurímac, Abancay, Peru
Introduction: Infant mortality is one of the most sensitive indicators of a country’s social and health development. Despite advances in public policies aimed at maternal and child health, significant challenges remain in sustainably reducing mortality rates among children under one year of age. The objective of this study was to analyze the impact of women’s literacy rate and educational level on infant mortality across the 24 departments and the constitutional province of Peru between 2001 and 2022.
Materials and methods: Data provided by the National Institute of Statistics and Informatics (INEI) were used, and a statistical analysis was conducted to explore the relationship between female literacy rate, educational attainment, and infant mortality across different regions of the country. A panel data model was employed, allowing for the assessment of both temporal variations and regional differences.
Results: The findings reveal a significant and inverse relationship between women’s educational level— as measured by literacy rate and average years of schooling—and the infant mortality rate in Peru from 2001 to 2022. Higher levels of female education are associated with lower infant mortality, highlighting the central role of education as a determinant of child health. Furthermore, substantial regional disparities persist, particularly in rural and impoverished areas, where educational levels are lower and infant mortality rates are higher.
Discussion and conclusions: These results underscore the need for comprehensive public policies that improve both access to and the quality of education, strengthen infrastructure in health and education, and prioritize targeted interventions to reduce territorial gaps. A multisectoral and inclusive approach is essential to achieve sustainable improvements in child health indicators and promote social equity in the country.
1 Introduction
Infant mortality, understood as the number of deaths of children under 5 years old per 1,000 live births, is a key indicator of a country’s social and economic development (1, 2). Its reduction is directly linked to various factors, among which the quality of the healthcare system, access to basic services, and especially the educational level of women plays a decisive role in maternal and child health. Over the years, it has been shown that mothers with higher educational levels are more likely to adopt effective health practices, such as prenatal care, vaccination, and proper nutrition, which directly influence the reduction of infant mortality (1–3).
Globally, studies have revealed a strong correlation between the educational level of women and infant mortality. According to the World Health Organization (WHO), countries with higher female education levels have significantly lower infant mortality rates. In 2019, the global infant mortality rate in countries with low education for women was 62 deaths per 1,000 live births, while in countries with high educational levels for women, this rate dropped to 10 deaths per 1,000 live births. This finding demonstrates the importance of education in improving child health by providing mothers with the tools necessary to make informed decisions about their children’s health (4–8).
In Latin America, the relationship between education and child health is equally evident. Despite progress in educational coverage, disparities remain, particularly in rural areas. According to the UNESCO 2020 report, the female literacy rate in Latin America increased from 89.2% in 2000 to 94.3% in 2020. However, this progress has not been uniform, as rural women continue to face significant barriers to accessing education (9–15). In countries like Peru, educational gaps between urban and rural areas persist, directly impacting child health (16–18).
In Peru, the analysis period of this study (2001–2022) has witnessed notable progress in female literacy and reductions in infant mortality, although these advances have been uneven at the territorial level. According to the National Institute of Statistics and Informatics (INEI), the female literacy rate in Peru rose from 88.5% in 2001 to 94.4% in 2021, an increase that reflects the country’s efforts to improve access to education, particularly for women. However, this progress has not been homogeneous, as regional disparities remain significant. In 2021, the female literacy rate in urban areas reached 98.1%, while in rural areas it was 87.3%; this gap of over 10 percentage points highlights inequality in access to education, which negatively affects child health, particularly in the most disadvantaged areas (19–21).
On the other hand, infant mortality in Peru has shown a considerable decrease in the first two decades of the 21st century. In 2001, the infant mortality rate in the country was 34.3 deaths per 1,000 live births. By 2022, this rate had dropped to 12.3 deaths per 1,000 live births, according to data from the Ministry of Health of Peru; this 64% reduction in infant mortality is a positive indicator of the country’s progress in terms of child health. However, regional inequalities remain a concern. In regions such as Puno and Apurímac, the infant mortality rate in 2022 was 22.5 and 20.1 deaths per 1,000 live births, respectively, well above the national average (21–25).
In this context, the present study aims to analyze how access to education and female literacy levels have influenced infant mortality rates in Peru between 2001 and 2022. Specifically, it seeks to evaluate the impact that female literacy rates and educational levels have had on the reduction of infant mortality, and determine whether these factors have been decisive in the observed improvements. Additionally, it explores how educational disparities between urban and rural areas have contributed to differences in infant mortality, with a particular focus on the most vulnerable regions (24–29).
This analysis not only contributes to understanding the fundamental role of education in reducing infant mortality but also helps identify areas where public policies need to be strengthened to close the educational gap and improve child health in the country. In this way, it aims to provide evidence-based recommendations to continue reducing infant mortality rates in the most disadvantaged areas of Peru.
2 Theoretical framework
2.1 Infant mortality as a social and health indicator
Infant mortality, defined as the number of deaths of children under 5 years of age per 1,000 live births, is one of the most sensitive indicators of the social and economic development levels of a nation. It is a direct reflection of factors such as access to healthcare services, nutrition, sanitary conditions, and particularly the educational level of mothers. This indicator is closely linked to poverty, malnutrition, preventable diseases, lack of access to quality medical care, and low literacy, all of which limit the ability of mothers to make informed decisions that promote the health and well-being of their children (30).
The World Health Organization (WHO) asserts that one of the main causes of infant mortality are preventable diseases such as diarrhea, pneumonia, and respiratory infections, which are more common in areas with poor living conditions and low educational levels. According to various international studies, infant mortality rates tend to be higher in regions where women have less access to education, highlighting the importance of female literacy and education in reducing infant mortality (31).
2.2 Theories and models relevant to the study of infant mortality
2.2.1 Epidemiological transition theory
This theory was proposed by Abdel Omran in 1971, suggesting that as countries progress socially and economically, they experience changes in mortality patterns, reflected in a decrease in infant mortality and a reduction in mortality from infectious diseases (32). This process is classified into three phases:
• Phase of high mortality and low life expectancy: Characterized by high rates of infant and general mortality due to infectious diseases and limited access to healthcare services.
• Transition phase: Improvements in public health conditions occur, such as access to vaccines, better nutrition, and healthcare, which reduce infant mortality.
• Phase of low mortality: Significant improvements in living conditions, education, public health, and medicine reduce infant mortality drastically.
In the specific case of infant mortality, this model suggests that female education and literacy are fundamental in the first two phases of the transition process, as educated women have a better understanding of the importance of maternal and child health, which directly impacts the reduction of infant mortality (32).
2.2.2 Social determinants of health model
This model, developed by Wilkinson and Marmot, focuses on how social and economic factors affect people’s health. According to this model, factors such as education level, housing quality, employment, nutrition, and social support networks are key determinants of health. In the case of infant mortality, this approach emphasizes that women with higher education levels are better able to access healthcare services, adopt healthy child-rearing practices, and make informed decisions that directly impact their children’s health (33).
Wilkinson and Marmot highlight that women’s education not only improves their employment and socioeconomic opportunities but is also linked to better health practices in the home. Educated mothers, for example, are more likely to breastfeed their children, follow vaccination recommendations, and seek medical attention when their children are ill, all of which reduce the risk of infant mortality (34).
2.2.3 Education as a strategy of liberation theory (Paulo Freire)
This theory, proposed by Paulo Freire, is fundamental to understanding how literacy and education empower women. Freire argues that education should be a process that allows individuals to develop critical consciousness and transform their social and economic reality. Through education, women not only acquire knowledge but also gain the ability to question power structures that perpetuate social inequalities (35).
In the context of infant mortality, education, according to Freire, provides women with the tools to make decisions that improve their children’s lives, from accessing healthcare to improving dietary habits. Literacy enables mothers to better understand health-related information, actively participate in the care of their children, and utilize available healthcare services to prevent diseases and reduce mortality (35).
2.2.4 The feminist empowerment theory and its relationship with maternal and child health
This theory posits that access to education and knowledge enables women to gain greater agency, autonomy, and decision-making capacity across various spheres of their lives, including reproductive health and the well-being of their children. It also recognizes that structural gender inequalities limit women’s access to resources, power, and information, thereby negatively affecting their health and that of their families (36, 37).
From this perspective, education is not only of instrumental value but also transformational, as it provides women with the tools to challenge restrictive social norms and to exercise control over their bodies, fertility, and parenting. Through knowledge, women acquire skills to identify symptoms of childhood illnesses, adhere to vaccination schedules, ensure proper nutrition, and seek health services when necessary (38).
The key components of empowerment in this theory include the following (39):
• Agency, defined as the capacity to set goals and act upon them. Women with formal education show greater initiative in seeking medical care for themselves and their children.
• Autonomy, referring to increased control over reproductive decisions, including birth spacing, number of children, and use of contraceptive methods.
• Access to information, where literacy allows women to correctly interpret medical instructions, medication labels, vaccination cards, and educational health materials.
Therefore, empowered women—especially those with higher levels of education—are more likely to access and utilize maternal and child health services such as prenatal care, institutional childbirth, child immunization, and treatment for common illnesses (40).
2.3 Determinants of infant mortality
2.3.1 Endogenous and exogenous factors
Factors influencing infant mortality are classified into endogenous and exogenous. Endogenous factors relate to the child’s physical constitution, such as congenital malformations or inherited conditions, which affect the child’s viability at birth. Exogenous factors are external to the child, such as infections, inadequate nutrition, accidents, and lack of access to appropriate healthcare services (41).
It is important to note that infant mortality is particularly influenced by exogenous factors, which are more easily controlled through public policies. Factors such as access to prenatal and postnatal care, nutrition, vaccination, and maternal education play a crucial role in reducing infant mortality (41).
2.3.2 The role of female literacy and education
Female education and literacy have a direct impact on infant mortality, as educated mothers tend to make more informed decisions about their children’s health. Education improves women’s ability to access healthcare services, understand the importance of nutrition and hygiene, and prevent diseases. Therefore, infant mortality rates are significantly lower in countries where women have access to secondary and higher education, demonstrating that education can be a powerful tool in reducing infant mortality (41).
2.4 Public policies and strategies to reduce infant mortality
Public policies in health and education have played a crucial role in reducing infant mortality, especially in rural areas and vulnerable populations. In Peru, programs such as Universal Health Insurance (SIS), Growing with Our Children, the Milk Glass Program, and the strengthening of Primary Health Care (PHC) have proven effective in improving child health and nutrition. These programs have reduced infant mortality rates by ensuring access to medical care, proper nutrition, and health education for mothers. However, challenges persist, particularly in rural areas where access to education and healthcare services remains limited. Public policies must focus on reducing these inequalities by promoting women’s education and literacy as a key strategy to improve child health (42, 43).
3 Materials and methods
3.1 Approach, type, and research design
The approach of this study is quantitative, as it seeks to measure the relationships between the variables considered in the research: literacy rate and years of female education in relation to infant mortality. Statistical methods are used to analyze the variables, identify patterns, and determine the magnitude of their impact on infant mortality in Peru (44). The research type is descriptive-correlational, as the study aims to describe the characteristics of the variables of interest (literacy and female education) and explore the relationships between these variables and infant mortality. The goal is not to establish causal relationships but to analyze how the variables are correlated with each other. Additionally, the research design is non-experimental and longitudinal with a panel approach, where the variables are observed in their natural environment without manipulation or intervention. Furthermore, as it is a longitudinal panel design, data from multiple periods over time (2001–2022) are analyzed, allowing the observation of changes and trends at both the national and regional levels (45).
3.2 Research method
The research method used is quantitative, based on statistical techniques, where descriptive analyses were conducted to characterize the variables under study and correlational analyses were performed to identify the relationship between the literacy rate, years of female education, and infant mortality. This allowed for an understanding of whether there is a significant relationship between these factors (44).
3.3 Population and sample
The study population consists of the 25 departments of Peru during the period from 2001 to 2022. The sample used includes 535 observations, as those observations lacking complete data on the variables of interest were excluded from the study.
3.4 Variable analysis
The following variables were identified and described in the study:
• Endogenous Variable: Infant Mortality Rate, which measures the number of deaths of children under 1 year of age per 1,000 live births during a specific period.
• Exogenous Variables: Female Literacy Rate: Represents the percentage of women aged 15 and older who can read and write.
• Years of Female Education: Reflects the average number of years of schooling completed by the female population aged 15 and older.
The econometric model used is as follows:
This panel data model allows for evaluating how the independent variables affect the infant mortality rate, considering both regional differences and changes over time (see Table 1).

Table 1. Operationalization of variables.
3.5 Statistical tests
To analyze the relationships between the variables, the following statistical tests were used:
• Pearson Correlation: This test was employed to measure the strength and direction of the linear relationship between female literacy and education with infant mortality.
• Fixed Effects Regression: Using the function xtreg Infant Mortality Rate Female Literacy Rate Average Years of Education, fe, the impact of literacy and education variables on infant mortality was evaluated, controlling for specific characteristics of each department and the effects over time.
Through these tests, the coefficients of the variables were analyzed to determine their significance and the impact they have on the infant mortality rate, thus establishing the relevance of female education in reducing infant mortality in Peru.
4 Results
4.1 Descriptive analysis of the variables
Below is a detailed analysis of the descriptive statistics for the three key variables in this study: infant mortality rate, literacy rate among women aged 15 years and older, and the average years of education attained by women aged 15 years and older:
In the case of the infant mortality rate, it averages 26 deaths per 1,000 live births, meaning that, on average, approximately 26 children under the age of one die for every thousand births in Peru. However, the standard deviation of 7.86 indicates considerable variability in the data. The range of values is wide, with a minimum of 10.5 and a maximum of 64, reflecting significant regional or temporal disparities in infant mortality rates. It is important to highlight that this dispersion may be influenced by differences in access to healthcare services, socioeconomic conditions, sanitary infrastructure, and public program coverage. The high variability is a relevant indicator for analysis, as it points to the existence of structural inequalities between departments or time periods within the country—factors that are essential to understanding the differentiated impact of public policies on maternal and child health (Table 2).
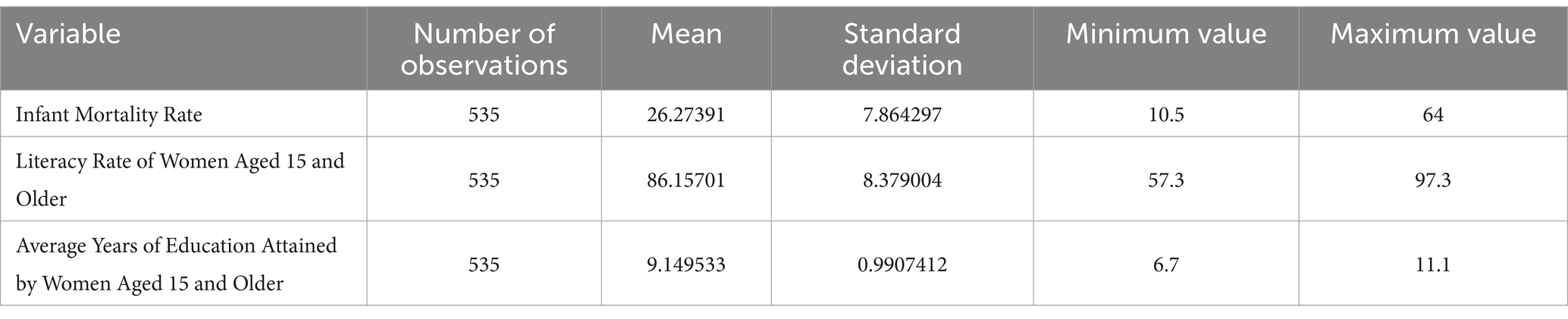
Table 2. Descriptive statistics of the model.
Regarding the literacy rate among women aged 15 and older, the national average stands at 86.16%, which means that, on average, more than 86% of adult women in Peru can read and write. With a standard deviation of 8.38, this shows moderate variability in female literacy levels across regions. The minimum recorded value is 57.3%, while the maximum reaches 97.3%, highlighting significant territorial disparities. It is likely that the lowest rates correspond to rural, Amazonian, or Indigenous communities with limited access to education. In contrast, the highest figures are probably concentrated in urban areas or regions with higher economic and educational development. Additionally, this dispersion suggests that factors such as educational quality, school infrastructure, mother tongue, and targeted policies directly influence women’s educational attainment (Table 2).
As for the average years of schooling among women aged 15 and older, the national average is 9 years, indicating that, in general, women have completed primary education and part of secondary education. This is supported by a low standard deviation of 0.99, showing a relatively homogeneous distribution of years of schooling among the population analyzed. The minimum value of 6.7 years reflects contexts with lower educational access, possibly associated with poverty, rural areas, or structural inequalities. Meanwhile, the maximum value of 11.1 years approaches the level of completed secondary education or even the beginning of higher education, indicating that in some regions, a portion of women attain more advanced educational levels. This variable therefore reinforces the importance of female education as a critical factor for human development and child health (Table 2).
These results clearly show that while educational variables (literacy and years of schooling) have a relatively high national average, they also reveal significant regional inequalities. These educational disparities are directly linked to the behavior of infant mortality in the country, which supports the study’s hypothesis regarding the influence of female education on maternal and child health outcomes (Table 2).
4.2 Correlational analysis of the variables
The negative correlation between the infant mortality rate and the female literacy rate is −0.7044, which shows that as the female literacy rate increases, the infant mortality rate decreases. This suggests that literate women are more likely to access essential information regarding health, nutrition, and childcare. This result aligns with previous studies highlighting the crucial role of literacy in making informed decisions, which directly impacts the reduction of infant mortality. Literate women tend to seek better medical care for their children, understand public health campaigns, and have greater knowledge of preventive practices such as hygiene, nutrition, and prenatal care (Table 3).
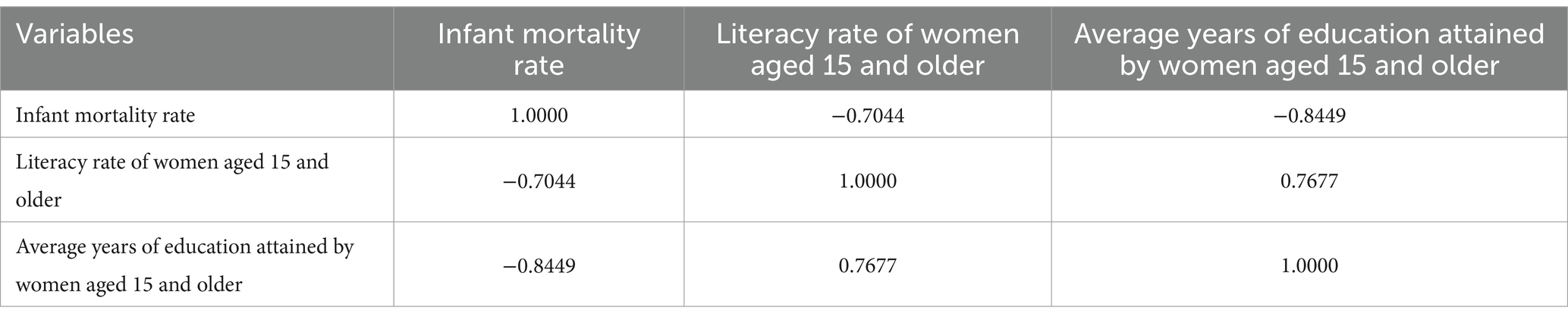
Table 3. Correlation between variables.
The negative correlation between the infant mortality rate and the average years of education attained is even stronger, with a value of −0.8449. This relationship indicates that as the number of years of education for women increases, infant mortality decreases, underscoring the significant impact of formal education on child health. Women with more years of schooling tend to be better informed and empowered to make decisions that promote the well-being of their children. These results support the importance of long-term education as a key determinant in improving health outcomes, particularly regarding infant mortality (Table 3).
Additionally, the positive correlation of 0.7677 between the female literacy rate and the average years of education attained demonstrates a direct relationship between educational level and literacy. As women gain more years of education, their literacy rates also increase. This result is expected, as literacy is a fundamental skill that underpins the ability to pursue higher education. The higher the education level, the greater the likelihood that women will be literate, reinforcing the connection between basic education and subsequent educational outcomes (Table 3).
4.3 Econometric model analysis
To provide a more detailed analysis of the regression results, below is an overview of each component of the model, delving into the economic and social implications of the estimated coefficients, as well as the interpretation of the goodness of fit and the relevance of the model. The regression results are as follows:
4.3.1 Analysis of statistical tests
The Hausman test, applied to determine the appropriate model between the fixed effects (FE) and random effects (RE) models, yielded a Chi-squared statistic of 15.07 with 2 degrees of freedom and a p-value of 0.00053. Since this p-value is below the 5% significance threshold, the null hypothesis—that the individual effects are uncorrelated with the explanatory variables—is rejected. Therefore, it is concluded that the fixed effects model is more appropriate for this analysis, as it provides consistent estimates by controlling for unobserved factors that vary across departments but remain constant over time. This methodological decision is crucial because it ensures that the effects of literacy and years of female education on infant mortality are not biased by structural characteristics unique to each region (Table 4).
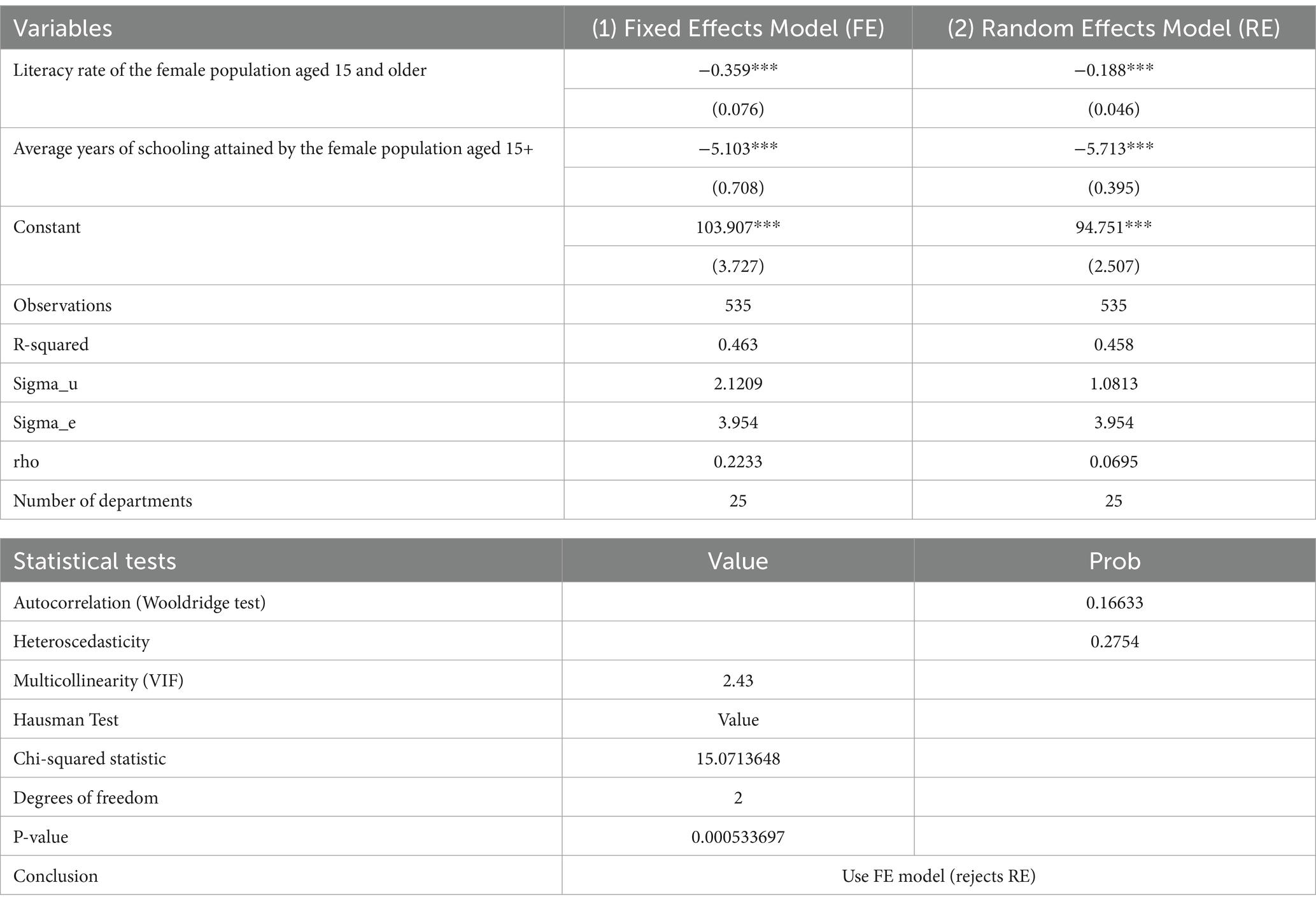
Table 4. Regression model of the effect of literacy rate and years of education on infant mortality rate.
Additionally, the Wooldridge test for autocorrelation shows a p-value of 0.16633, indicating sufficient evidence to conclude that there is no autocorrelation in the residuals—a desirable condition for fixed effects panel data models. The p-value for the heteroscedasticity test is 0.2754, which is above the common threshold of 0.05; this result indicates that there is no evidence of heteroscedasticity in the model’s residuals. Regarding multicollinearity, the Variance Inflation Factor (VIF) is 2.43, well below the critical threshold of 10 commonly used to detect significant multicollinearity. This suggests that there is no problematic multicollinearity between the independent variables—namely, the literacy rate and the average years of schooling (Table 4).
Therefore, the fixed effects (FE) model, selected based on the Hausman test, successfully passes all relevant statistical tests. No issues of autocorrelation or heteroscedasticity are detected, supporting the model’s validity and reliability. Furthermore, the absence of multicollinearity among the variables ensures the precision of the coefficient estimates. In summary, these results reinforce the decision to use the fixed effects model, which is well-suited for analyzing how female literacy and education variables impact the infant mortality rate while controlling for unobserved differences between departments (see Figure 1).
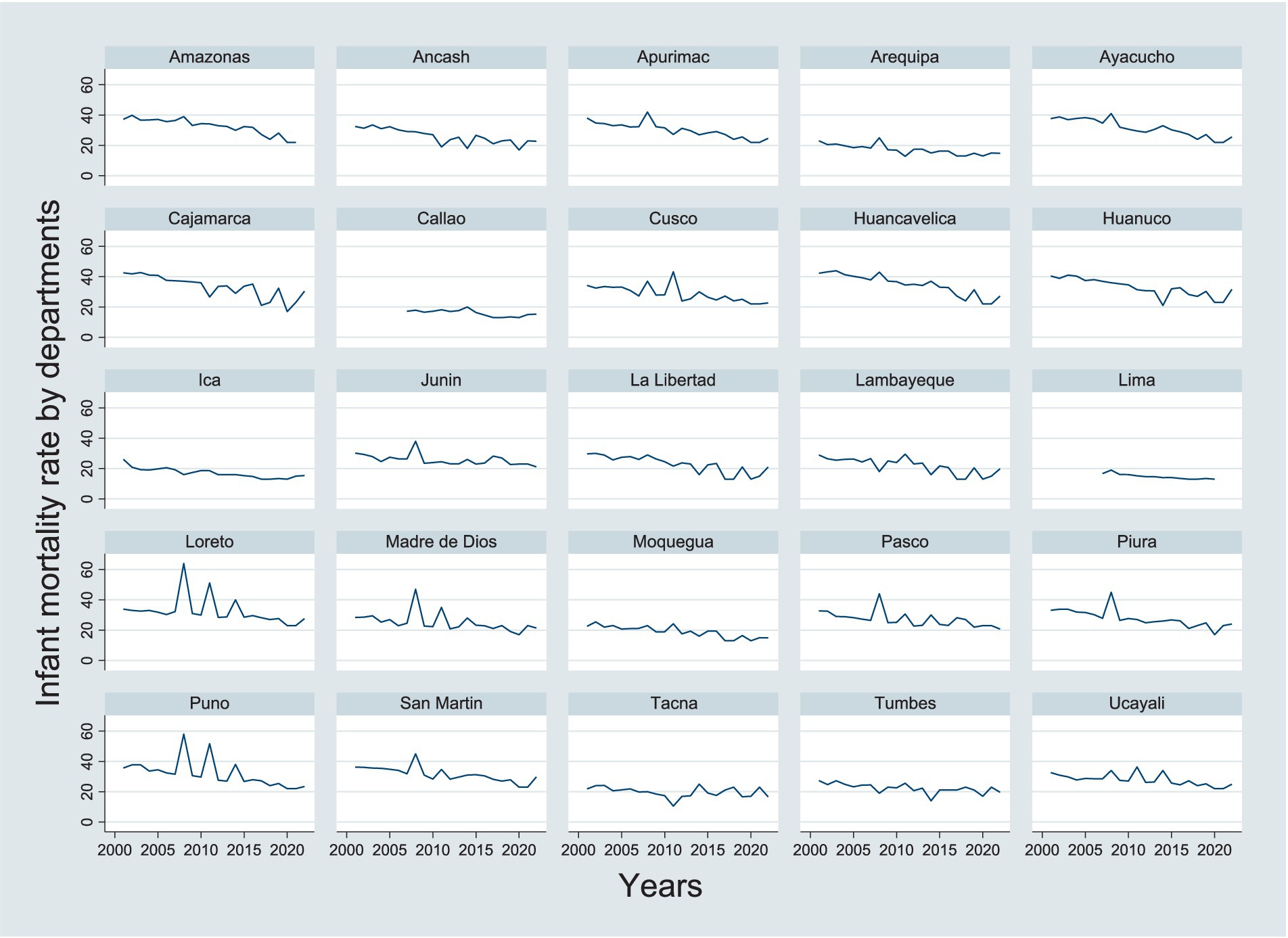
Figure 1. Infant mortality rate by departments.
4.3.2 Analysis of the coefficients of the explanatory variables
According to Table 4, the estimated coefficients for the variables in the model represent the expected change in the infant mortality rate for a unit change in the explanatory variables, holding other variables constant.
For the literacy rate of women aged 15 and older, the coefficient is −0.3591204, indicating that for each 1 percentage point increase in the female literacy rate, the infant mortality rate would decrease by 0.36 units (for every 1,000 live births). This coefficient is highly significant with a p-value of 0.000, leaving no doubt that the female literacy rate is negatively related to the infant mortality rate. This result shows that increasing the female literacy rate is an effective strategy to reduce infant mortality, as literacy may be linked to better access to health, nutrition, and childcare information, which directly impacts reducing infant mortality (Figure 2). Furthermore, literate women are more likely to seek appropriate medical care during pregnancy and childbirth, which also reduces infant mortality rates.
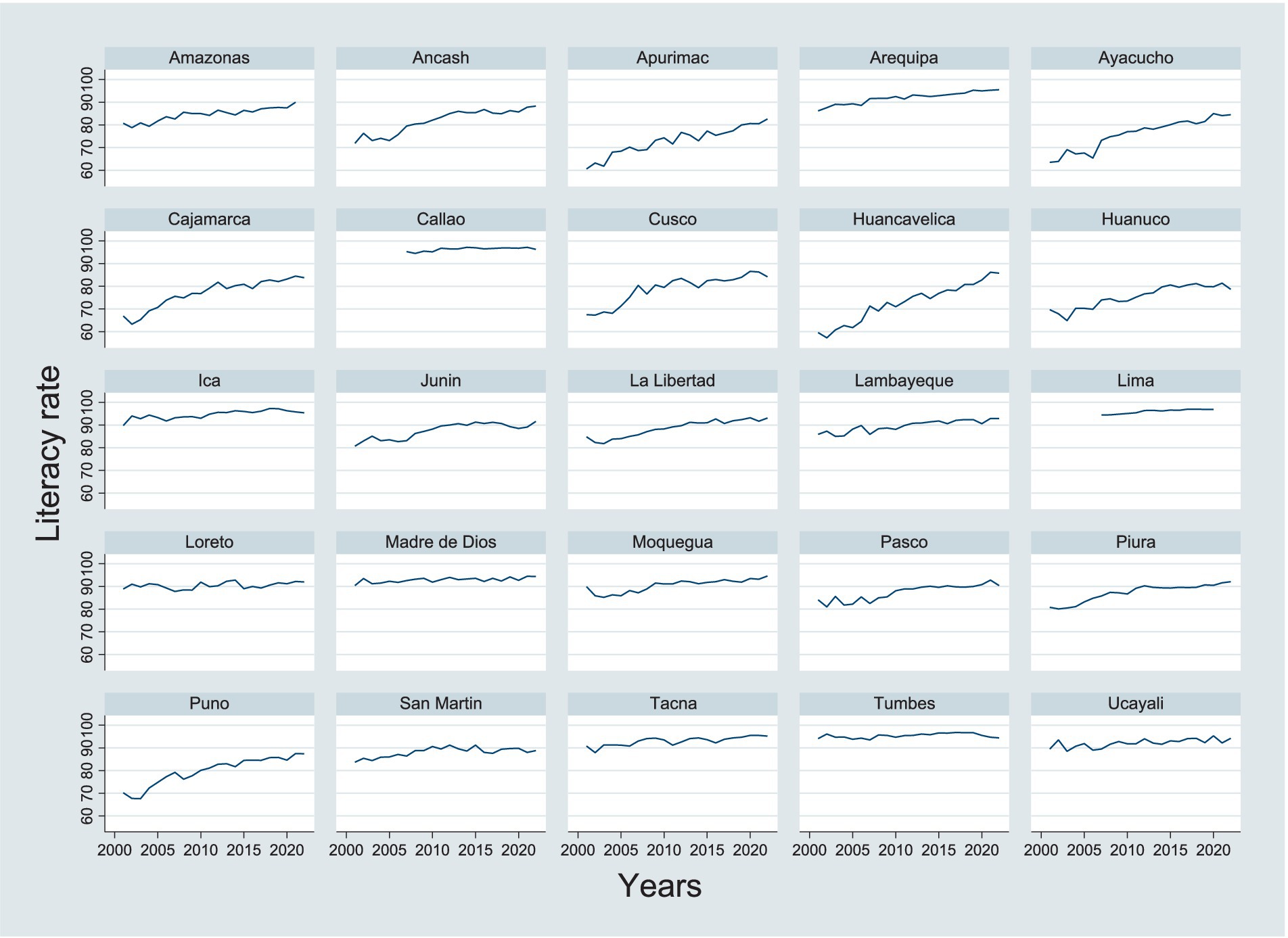
Figure 2. Literacy rate of the female population aged 15 and over by departments.
Regarding the average years of education attained by women aged 15 and older, the coefficient is −5.103285, demonstrating that for each additional year of education attained by women, the infant mortality rate would decrease by 5.10 units (for every 1,000 live births). Like the literacy rate, the coefficient for years of education is highly significant with a p-value of 0.000, confirming that education has a robust and clear effect on reducing infant mortality. Formal education, beyond literacy, has an even deeper impact on women’s health decisions. Educated women are more likely to make informed decisions about family planning, prenatal care, nutrition, and hygiene, which directly improves their children’s health. Additionally, women with higher education levels have more access to well-paying jobs, which improves family quality of life and reduces the risk of infant mortality related to poverty (Figure 3).
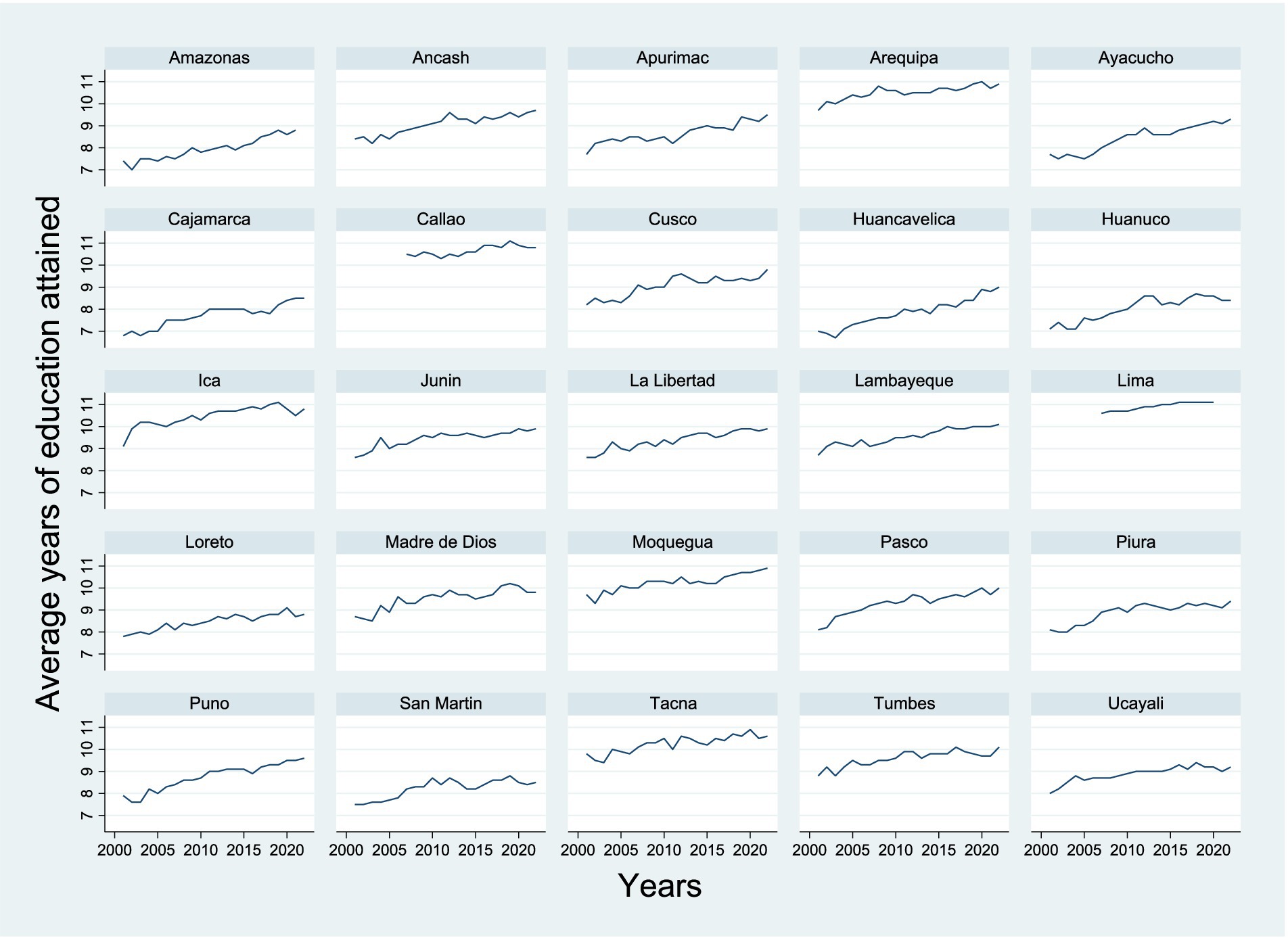
Figure 3. Average years of education attained by the female population aged 15 and over by departments.
Therefore, the results of the econometric model demonstrate that both female literacy and years of education have a negative and significant effect on the infant mortality rate in Peru. The findings strongly suggest that improving the educational level of women is crucial for reducing infant mortality in the country. The model shows a good fit, explaining a considerable amount of the variability both within and between departments, highlighting the importance of educational policies targeted at women as a key strategy for improving child health indicators. Furthermore, the fixed effects and significance tests reinforce the idea that the specific characteristics of each department play an important role in infant mortality, indicating that tailored interventions at the local level should be designed to maximize the impact on reducing infant mortality.
5 Discussion
The results of this research confirm a negative and significant relationship between the female literacy rate and infant mortality in Peru, which is consistent with the findings of López-Leyva (46), who highlight the fundamental role of women’s literacy in improving child health. A literate mother is better equipped to access, understand, and apply information related to health, nutrition, and medical care. As a result, these women tend to make more informed decisions about their children’s well-being, seek timely medical attention, and adopt healthy practices at home. These mechanisms directly contribute to the reduction of infant mortality, as also pointed out by Cleland and Ginneken (47), who emphasize that women with higher literacy levels make better use of child health services, positively impacting their children’s survival.
Likewise, the findings regarding the average years of female education also show a negative and significant association with infant mortality, supporting studies such as those by Medina and Cerda (48), who argue that education is one of the most influential factors in child survival. Mothers with more years of education tend to have greater knowledge about health practices, family planning, nutrition, and prenatal care, which reduces risks associated with preventable childhood diseases. This empirical evidence also aligns with the findings of Cancelo et al. (49), who assert that an increase of 1 year in women’s average schooling can lead to a significant reduction in the infant mortality rate. Although the magnitude of the effects may vary across contexts, the direction of the impact is consistent and supports the need to strengthen investment in women’s education as a central public policy strategy for child health.
One of the most relevant findings of this study is the presence of marked regional inequalities in the relationship between female education and infant mortality. Regions such as Huancavelica and Huánuco exhibit high levels of infant mortality associated with low levels of female literacy. This finding aligns with the analysis of Beltrán and Zárate (19), who point out that structural factors such as poverty, regional inequality, deficient educational and health infrastructure, and geographic marginalization limit access to both education and basic health services. These conditions perpetuate high levels of infant mortality in certain regions, suggesting that the positive impact of education cannot be understood in isolation, but rather within a broader framework of socioeconomic conditions.
Moreover, while this study focuses on female education as the main variable, it is important to recognize that infant mortality is a multifactorial phenomenon. Factors such as access to quality healthcare services, malnutrition, extreme poverty, and public health policies are also relevant determinants. In this regard, as Beltrán and Zárate (19) once again highlight, improvements in educational levels must be accompanied by policies aimed at reducing poverty, improving sanitation, and strengthening the coverage and quality of medical services. This reinforces the need to adopt comprehensive and cross-sectoral approaches in the fight against infant mortality.
Finally, the evidence presented is consistent with the arguments of Rojas and Hernández (5), who underscore that poverty and socioeconomic inequalities remain critical barriers to improving child health indicators, especially in rural and marginalized areas. Poverty not only limits access to education and healthcare but also directly affects living conditions, increasing children’s vulnerability to disease and malnutrition. Therefore, it is concluded that in order to effectively and sustainably reduce infant mortality, public policies must be multifaceted, addressing not only access to and quality of female education but also the structural determinants of child health and well-being.
6 Conclusion
There is an inverse and statistically significant relationship between female education levels—measured through the literacy rate and the average years of schooling—and the infant mortality rate in Peru during the period 2001–2022. Specifically, as both literacy and women’s years of education increase, a considerable reduction in infant mortality is observed. This confirms that female education serves as a key determinant of child health, by enhancing mothers’ ability to make informed decisions about prenatal care, nutrition, vaccination, and timely use of healthcare services. These findings strongly support the design and implementation of public policies focused on strengthening women’s education, recognizing it as an empowerment tool that directly impacts child well-being. Furthermore, the fixed effects econometric model employed—validated by the Hausman test—demonstrates that this relationship holds even when controlling for unobserved structural differences across departments, which reinforces the robustness of the results.
In addition, the analysis reveals that this positive trend is not uniformly distributed across the country. Significant regional inequalities persist, especially in rural or impoverished areas such as Huancavelica and Huánuco, where infant mortality remains high and female education levels continue to lag behind. These disparities reflect structural gaps in access to educational and healthcare services, stemming from factors such as poverty, geographic marginalization, and limited public investment in infrastructure.
Therefore, to achieve a sustained and equitable reduction in infant mortality, it is essential that public policies not only promote access to education but also ensure its quality and relevance, particularly in the most vulnerable regions. This requires investment in educational infrastructure, teacher training, and school programs that integrate content on health, nutrition, and family planning. Likewise, the coordination between the education and health sectors must be strengthened through integrated interventions that improve access to medical services, living conditions, and community empowerment. Only through a territorial, inclusive, and multisectoral approach can Peru make meaningful progress toward a sustainable and equitable reduction in infant mortality.
Data availability statement
The data used in this research are freely accessible, and can be accessed through the statistical information platform of the National Institute of Statistics and Informatics of Peru, whose URL is: https://www.gob.pe/institucion/inei/tema/informacion-estadistica.
Author contributions
JQ: Supervision, Writing – original draft, Writing – review & editing. SA: Conceptualization, Writing – original draft. AC: Conceptualization, Writing – original draft. YP: Methodology, Writing – original draft. LP: Software, Writing – original draft. NQ: Validation, Writing – original draft. BC: Validation, Writing – original draft. BQ: Formal analysis, Writing – original draft. PH: Methodology, Writing – original draft. DC: Resources, Writing – original draft. LC: Data curation, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Armstrong, D. The invention of infant mortality. Sociol Health Illn. (1986) 8:211–32. doi: 10.1111/j.1467-9566.1986.tb00298.x
2. Wise, PH. The anatomy of a disparity in infant mortality. Annu Rev Public Health. (2003) 24:341–62. doi: 10.1146/annurev.publhealth.24.100901.140816
3. Rechtman, LR, Colvin, JD, Blair, PS, and Moon, RY. Sofas and infant mortality. Pediatrics. (2014) 134:e1293–300. doi: 10.1542/peds.2014-1543
4. Esmaeilzadeh, F, Alimohamadi, Y, Sepandi, M, Khodamoradi, F, and Jalali, P. The comparing of infant mortality rate in different World Health Organization regions during 1990–2017. Egypt Pediatr Assoc Gaz. (2021) 69:1–7. doi: 10.1186/s43054-020-00048-6
5. Rojas, YLR, and Hernández, AR. Análisis de la mortalidad materna desde los determinantes sociales en los países de latinoamérica y el caribe. Mov Científico. (2014) 6:132–43.
6. Qamar, K, Essar, MY, Siddiqui, JA, Salman, A, Salman, Y, and Head, MG. Infant and child mortality in Afghanistan: a scoping review. Health Sci Rep. (2024) 7:e2224. doi: 10.1002/hsr2.2224
7. Geruso, M, and Spears, D. Heat, humidity, and infant mortality in the developing world. National Bureau of Economic Research. (No. w24870) (2018). Available at: https://www.nber.org/papers/w24870.
8. Baird, S, Friedman, J, and Schady, N. Aggregate income shocks and infant mortality in the developing world. Rev Econ Stat. (2011) 93:847–56. doi: 10.1162/REST_a_00084
9. Palloni, A, and Rafalimanana, H. The effects of infant mortality on fertility revisited: new evidence from Latin America. Demography. (1999) 36:41–58. doi: 10.2307/2648133
10. Betrán, AP, De, OM, Lauer, JA, and Villar, J. Ecological study of effect of breast feeding on infant mortality in Latin America. BMJ. (2001) 323:303. doi: 10.1136/bmj.323.7308.303
11. Bähr, J, and Wehrhahn, R. Life expectancy and infant mortality in Latin America. Soc Sci Med. (1993) 36:1373–82. doi: 10.1016/0277-9536(93)90230-2
12. Ortigoza, A, Braverman, A, Hessel, P, Di Cecco, V, Friche, AA, Teixeira Caiaffa, W, et al. Women’s empowerment and infant mortality in Latin America: evidence from 286 cities. Cities Health. (2023) 7:93–101. doi: 10.1080/23748834.2021.1908794
13. Ortigoza, AF, Granados, JAT, Miranda, JJ, Alazraqui, M, Higuera, D, Villamonte, G, et al. Characterising variability and predictors of infant mortality in urban settings: findings from 286 Latin American cities. J Epidemiol Community Health. (2021) 75:264–70. doi: 10.1136/jech-2020-215137
14. Validova, A, Uruchima, J, Yamada, G, Vives, A, Schnake-Mahl, A, de Lima Friche, AA, et al. Are extensions in paid parental leave associated with lower infant and neonatal mortality in Latin American cities? Evidence from 148 cities in Chile, Mexico, and Colombia (2000–2015). Soc Sci Med. (2025) 372:117971. doi: 10.1016/j.socscimed.2025.117971
15. Sáfadi, MAP, Asturias, EJ, Colomar, M, Gentile, A, Miranda, J, Sáez-Llorens, X, et al. Identifying gaps and opportunities for maternal and neonatal immunization research and implementation in Latin America Pediatr Infect Dis J. Available online at: https://journals.lww.com/pidj/fulltext/2025/02001/identifying_gaps_and_opportunities_for_maternal.7.aspx?context=latestarticles (Accessed April 2, 2025).
16. Young, FW, Edmonston, B, and Andes, N. Community-level determinants of infant and child mortality in Peru. Soc Indic Res. (1983) 12:65–81. doi: 10.1007/BF00428861
17. Paxson, C, and Schady, N. Child health and economic crisis in Peru. World Bank Econ Rev. (2005) 19:203–23. doi: 10.1093/wber/lhi011
18. Dammert, AC. Acceso a servicios de salud y mortalidad infantil en el Perú. Lima: Consorcio de Investigación Económica y Social: GRADE, Grupo de Análisis para el Desarrollo (2001). 60 p.
19. Beltrán, A, and Zárate, ARG. Políticas efectivas para reducir la mortalidad infantil en el Perú: ¿Cómo reducir la mortalidad infantil en las zonas más pobres del país? Apuntes Rev Cienc Soc. (2008) 5–54. doi: 10.21678/apuntes.62.570
20. Ticona, R. M, and Huanco, A. D. Mortalidad perinatal hospitalaria en el Perú: Factores de riesgo. Available online at: https://www.scielo.cl/scielo.php?pid=S0717-75262005000500006&script=sci_arttext (Accessed April 2, 2025).
21. Torres, GY, and Mujica, RF. Criterios de medición de la mortalidad infantil y la vigencia de los derechos a la salud de los pueblos indígenas. Rev Fac Med Hum. (2017) 17:55–63. doi: 10.25176/RFMH.v17.n2.832
22. Paredes Mamani, RP, Yapuchura Saico, C, Arpi Mayta, R, Pelayo Calatayud Mendoza, A, Paredes Mamani, RP, Yapuchura Saico, C, et al. Determinantes socioeconómicos y próximos de la mortalidad de niños menores de cinco años en el Perú (2015-2018). Available online at: http://www.scielo.org.pe/scielo.php?pid=S0252-18652021000100085&script=sci_arttext&tlng=en (Accessed April 2, 2025).
23. Vargas-Machuca, Á, and Giselle, J. Desigualdad en la mortalidad neonatal del Perú generada por la pobreza y educación, 2011–2019. Rev. Peru Med. Exp. Salud Publica. (2022) 39:178–84. doi: 10.17843/rpmesp.2022.392.10629
24. Gutiérrez, W. La desnutrición en la niñez en el Perú: Factores condicionantes y tendencias. Rev. Peru Med. Exp. Salud Publica. (2011) 28:390. doi: 10.17843/rpmesp.2011.282.514
25. Díaz, AA, Gallestey, JB, Vargas-Machuca, R, and Velarde, RA. Desarrollo infantil en zonas pobres de Perú Desarrollo infantil en zonas pobres de Perú. Available online at: https://www.scielosp.org/article/rpsp/2017.v41/e71 (Accessed April 2, 2025).
26. Tavera Salazar, M. La atención primaria de salud y la salud materno infantil. Available online at: http://www.scielo.org.pe/scielo.php?pid=S2304-51322018000300011&script=sci_arttext&tlng=en (Accessed April 2, 2025).
27. Maravi, VT. La Mortalidad infantil en la Ciudad de Huancayo. Perú en los años 1995-2005. Rev Peru Pediatr. (2010) 63:7–12. doi: 10.61651/rped.2010v63n3p07-12
28. Velásquez Hurtado, JE, Kusunoki Fuero, L, Paredes Quiliche, TG, Hurtado La Rosa, R, Rosas Aguirre, AM, and Vigo Valdez, WE. Mortalidad neonatal, análisis de registros de vigilancia e historias clínicas neonatales del año 2011 en Huánuco y Ucayali, Perú. Rev Peru Med Exp Salud Publica. (2014) 31. doi: 10.17843/rpmesp.2014.312.39
29. Avila-Jaquez, C. Disminución de la mortalidad materna en Perú y el enfoque de capacidades. Convergencia. (2019) 26:1. doi: 10.29101/crcs.v26i80.10790
30. Ospina, AG, Lozano, GB, and Jaramillo, HM. Relación entre la salud y el ingreso per cápita: revisión de literatura y elaboración del marco teórico. Rev Gest Reg (2011)133–158. Available online at: https://revistas.ucp.edu.co/index.php/gestionyregion/article/view/864 (Accessed April 2, 2025).
31. Longhi, F. Pobreza y mortalidad infantil: Una aproximación teórica al estudio de sus relaciones. (2011) Available online at: https://www.scielo.org.ar/scielo.php?pid=S1668-80902013000200002&script=sci_arttext&tlng=en (Accessed April 2, 2025).
32. Gómez Redondo, RM. La mortalidad infantil española en el siglo XX. Centro de Investigaciones Sociológicas (CIS) (1992). Available online at: https://portalcientifico.uned.es/documentos/5f88ea5429995259ef290a89 (Accessed April 2, 2025).
33. Hernández-Bringas, HH, Narro-Robles, J, Hernández-Bringas, HH, and Narro-Robles, J. Mortalidad infantil en México: logros y desafíos. Available online at: https://www.scielo.org.mx/scielo.php?pid=S1405-74252019000300017&script=sci_arttext (Accessed April 2, 2025).
34. Kaempffer, R A, and Medina, L E. Mortalidad infantil reciente en Chile: Éxitos y desafíos. Available online at: https://www.scielo.cl/scielo.php?pid=S0370-41062006000500007&script=sci_arttext&tlng=en (Accessed April 2, 2025).
35. Carreño, M. Teoría y práctica de una educación liberadora: el pensamiento pedagógico de Paulo Freire. (2010) Available online at: https://revistascientificas.us.es/index.php/Cuestiones-Pedagogicas/article/view/9922 (Accessed April 2, 2025).
36. Pratley, P. Measuring Women’s empowerment and its associations with maternal and child health outcomes. (2016) Available online at: https://www.proquest.com/openview/784a9e26c80ca9f5a529a3a9fbb5170f/1?cbl=18750&pq-origsite=gscholar
37. Parker, B, and McFarlane, J. Feminist theory and nursing: An empowerment model for research. Adv Nurs Sci. Available online at: https://journals.lww.com/advancesinnursingscience/abstract/1991/03000/feminist_theory_and_nursing__an_empowerment_model.8.aspx (Accessed May 6, 2025).
38. Robinson, F. Discourses of motherhood and women’s health: maternal thinking as feminist politics. J Int Polit Theory. (2014) 10:94–108. doi: 10.1177/1755088213507189
39. O’Reilly, A. Maternal theory: Patriarchal motherhood and empowered mothering. In: O’Brien Hallstein L, O’Reilly A, and Vandenbeld Giles M. The Routledge companion to motherhood. Routledge. (2019) 19–35. Available at: https://www.taylorfrancis.com/chapters/edit/10.4324/9781315167848-2/maternaltheoryandrea-reilly
40. Maschi, T, Turner, SG, Dewan, SE, Kaye, A, and Hintenach, AM. Feminist and empowerment theory and practice: a powerful alliance. In: Rethinking feminist theories for social work practice. Cham: Springer International Publishing. (2022) pp. 37–57. Available at: https://link.springer.com/chapter/10.1007/978-3-030-94241-0_3.
41. Mojarro, O, and Núñez, L. Mortalidad infantil en México: tendencias y factores determinantes. Salud Publica Mex (1988) 30:329–345. Available online at: https://saludpublica.mx/index.php/spm/article/view/174 (Accessed April 2, 2025).
42. Del Carpio, AL. Situación de la mortalidad materna en el Perú, 2000-2012. Rev Peru Med Exp Salud Publica. (2014) 30. doi: 10.17843/rpmesp.2013.303.284
43. Urdaneta, J.R., and Baabel-Zambrano, N. Una mirada bioética a la mortalidad materna en Venezuela. Gac Med Caracas (2025) Available online at: http://saber.ucv.ve/ojs/index.php/rev_gmc/article/view/30363 (Accessed April 2, 2025).
44. Hernández, F, Fernández, C, and Baptista, L. Metodología de la investigación. 5th ed. México: McGraw. (2010). Available at: https://www.esup.edu.pe/wp-content/uploads/2020/12/2.%20Hernandez,%20Fernandez%20y%20Baptistametodolog%C3%ADa%20Investigacion%20Cientifica%206ta%20ed.pdf
45. Mendoza, W. Cómo investigan los economistas: Guía para elaborar y desarrollar un proyecto de investigación. 1st Ed. Lima - Perú: Fondo Editorial de la Pontificia Universidad Católica del Perú (2014) 234 p.
46. López-Leyva, S. educación de América Latina percibida desde el objetivo 4 de los objetivos del desarrollo sostenible (ODS). Inf Tecnol. (2024) 35:23–36. doi: 10.4067/s0718-07642024000200023
47. Cleland, JG, and van Ginneken, JK. Maternal education and child survival in developing countries: the search for pathways of influence. Soc Sci Med. (1988) 27:1357–68. doi: 10.1016/0277-9536(88)90201-8
48. Medina, L M, and Cerda, L J Nivel de Educación Parental y Mortalidad Infantil. Available online at: https://www.scielo.cl/scielo.php?pid=S0370-41062010000300005&script=sci_arttext&tlng=pt (Accessed April 2, 2025).
49. Cancelo, M, Lamelas, N, Cancelo, M, and Lamelas, N. Análisis econométrico de la relación entre la educación y la mortalidad infantil en la comunidad andina. 1960-2000. Estudios económicos de desarrollo Internacional (2003) 3:1–20. Available online at: https://investigacion.usc.es/documentos/5ec464b2299952379f6e0494 (Accessed April 2, 2025).
Keywords: infant mortality, literacy, education, women, Peru
Citation: Quispe Mamani JC, Aguilar Pinto SL, Carpio Maraza A, Poma Palma YM, Ponce Quispe L, Quispe Maquera NB, Cutipa Quilca BE, Quispe Quispe B, Huarca Flores P, Calcina Álvarez DA and Caceres Bustinza LM (2025) Effect of female literacy rate and education on infant mortality in Peru, 2001–2022. Front. Public Health. 13:1605790. doi: 10.3389/fpubh.2025.1605790
Edited by:
Daniel Robert Neuspiel, Atrium Healthcare, United StatesReviewed by:
Francisco Palencia-Sánchez, Pontifical Javeriana University, ColombiaMamadou Abdoulaye Diallo, Consortium pour la recherche économique et sociale, Senegal
Copyright © 2025 Quispe Mamani, Aguilar Pinto, Carpio Maraza, Poma Palma, Ponce Quispe, Quispe Maquera, Cutipa Quilca, Quispe Quispe, Huarca Flores, Calcina Álvarez and Caceres Bustinza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julio Cesar Quispe Mamani, amNxdWlzcGVAdW5hcC5lZHUucGU=