 Grecia Victoria Vivas-Colmenares
Grecia Victoria Vivas-Colmenares Jose Ruben Ramírez-Iglesias
Jose Ruben Ramírez-Iglesias Ana M. Martínez-Pérez
Ana M. Martínez-Pérez- 1Health Sciences Faculty, School of Medicine, Universidad Internacional SEK (UISEK), Quito, Ecuador
- 2International Doctoral School, Universidad Rey Juan Carlos, Madrid, Spain
- 3Department of Communication and Sociology, Faculty of Communication, Universidad Rey Juan Carlos, Madrid, Spain
Introduction: Telemedicine reduces in-person appointments and extends healthcare services to rural areas. Despite its extended use after the COVID-19 pandemic, further analysis of educational applications and strategies is needed to better prepare parents and caregivers for postoperative pediatric care beyond routine clinical follow-up. Therefore, this review systematically evaluates the effectiveness of telemedicine interventions in educating parents or caregivers after pediatric surgery, with respect to caregiver knowledge and self-efficacy in postoperative care, caregiver satisfaction, and postoperative clinical outcomes.
Methods: Following the PRISMA guidelines, we searched three databases, PubMed, Scopus, and LILACS, for articles published between 2013 and 2023 that involved patients aged 0–18 years who underwent surgery and caregivers who received some form of education through telemedicine. We evaluated the effectiveness of telemedicine for educational purposes by assessing caregiver knowledge, satisfaction, and patient morbidities. Bias was analyzed using the RoB2 and ROBINS-I tools. The certainty of the presented evidence was assessed using the GRADE guidelines. The SWiM guideline was employed to report a structured narrative synthesis from the combined results. The protocol was registered in the International Prospective Register of Systematic Reviews (CRD42024545858).
Results: Four studies were included from 2,163 records initially registered: two randomized controlled trials (RCTs) and two uncontrolled before–after (UCBAs) studies. In the RCTs, caregiver knowledge was significantly higher in the telemedicine intervention group (p < 0.05); in one UCBA, caregiver knowledge increased over time. All studies reported high satisfaction with telemedicine, with the RCTs showing significantly higher satisfaction levels than control groups (p < 0.05). One UCBA also reported a significant improvement in patient continence. Bias was assessed as moderate in the RCTs and high in the UCBAs. The GRADE criteria indicate a certainty of evidence moderate for satisfaction and caregiver knowledge, and very low for morbidity and rate of complications or adverse events.
Discussion: Telemedicine-based educational tools show promise as a strategy for healthcare systems, achieving high acceptance levels. However, further research is required to refine the methodological approaches for implementing telemedicine in caregiver education within the postoperative setting.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024545858, identifier [CRD42024545858].
1 Introduction
The implementation of several technological tools and resources has contributed to strengthening a wide range of aspects associated with health services, from remote attention for routine checks to caregiver-focused education to improve the rehabilitation process (1). Under this approach, the terms telemedicine and telehealth include using medical information delivered via electronic communications to improve the clinical status of the patients (2). Specifically, the remote health approach for rehabilitation is based on providing services for prevention, monitoring, intervention, supervision, and education to overcome geographic, temporal, social, and financial barriers (3). Although the use of basic devices such as telephones for monitoring patients at distance was already implemented around 1960 and medical telehealth as a specific term was established more than 30 years ago (4, 5), the recent COVID-19 pandemic context has significantly piqued the interest in improving and extending the application of these resources. Telemedicine was implemented to avoid exposure to potentially infectious environments and provide continuous care for long-term conditions without in-person encounters (6, 7).
The restrictions associated with the non-pharmaceutical measures taken globally against the SARS-CoV-2 affected the health services offered to vulnerable populations, including pediatric patients. These effects were observed at several levels, such as a decrease in general child life services (8), reduced routine vaccination coverage (9) and postponed non-emergency surgeries (10), together with the classical in-person follow-up appointments (11). One of the critical areas where monitoring and control policies have changed is in the rehabilitation and post-operative care for pediatric patients (12). The high demand for pediatric surgical interventions highlights the need to implement telemedicine for this population. In the USA, approximately 3.9 million pediatric surgeries were performed annually from 2016 to 2019, with 4.7% of children undergoing at least one surgery (13). In lower-middle-income countries, nearly 50% of the population is under 20 years old, indicating a significant need for pediatric surgical services (14). Surgical interventions are crucial for achieving universal health coverage (SDG 3). Insufficient access to safe surgery maintains poverty and hampers economic development, linking to SDGs 1 and 8 (15, 16).
The management related to rehabilitation for these patients includes aspects of patient education, which comprises all materials and strategies for improving literacy and betterment of patient care (17), and high-quality communication focused on Family-Centered Rounds to support decision-making, which increases the involvement of the family during the processes and plan the discharge of the patient for subsequent follow-up and recovery from home (18). The following process of postoperative management at home plays a key role in achieving an adequate recovery and monitoring of multiple aspects associated with surgical trauma, from the commonly expected side effects of postoperative pain (19) to the specific care depending on the surgical intervention. From this point of view, telemedicine has allowed the implementation of dual applications to both educate parents and caregivers to improve rehabilitation management and for a flexible follow-up, which is ideal for rural contexts, to reduce the stress of mobilization to the hospital and, more recently, as valuable tools during the situation of global health emergencies (2, 20, 21).
While various strategies utilizing commercial and customized technologies, as well as applications designed for different devices, have been explored for postoperative follow-up, there is a shortage of studies that consolidate these resources and analyze their use in, specifically, telemedicine focused on education for guiding parents or caregivers during the recovery process of pediatric patients. Based on this, the aim of the present study was to systematically evaluate the effectiveness of telemedicine interventions in educating parents or caregivers after pediatric surgery, with respect to caregiver knowledge and self-efficacy in postoperative care, caregiver satisfaction, and postoperative clinical outcomes.
2 Methods
2.1 Criteria for study selection
The systematic review was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions (22) and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (23). The eligibility criteria for study selection were defined a priori and applied during the screening process. Studies were included if they were published between 2013 and 2023, involved patients aged 0 to 18 years, and reported surgically treated conditions. The search period was established based on global trends in telemedicine research, highlighting 2013 as an inflection point in the telemedicine literature, with annual mHealth output first exceeding 100 papers and a rapid increase in citations associated with telecare, suggesting a patient-centered telemedicine (24, 25). The primary intervention of interest was the use of telemedicine with an educational focus, delivered through various communication platforms to perform remote interaction. The review included only educational strategies delivered exclusively using telemedicine, with no hybrid components involving in-person clinical care. Eligible interventions had to educate parents or caregivers to support postoperative recovery in pediatric patients. We excluded studies that did not focus on a pediatric postoperative population or that combined telemedicine education with additional clinical interventions. The following study designs were eligible for inclusion: randomized controlled trials (RCTs) and non-randomized controlled trials (NRCTs) where the comparator was a standard not telemedicine-related intervention, uncontrolled before–after (UCBA) studies and interrupted time-series (ITS) with 3 or more data points before and after the intervention. Eligible studies reported at least one of the following outcomes in a quantitative manner: parental or caregiver knowledge, satisfaction with the telemedicine intervention, or reduction in post-surgical morbidity in patients.
Articles were excluded if they focused solely on telemedicine for routine follow-ups or appointments or used a hybrid model combining education and clinical teleconsultation. Additionally, letters to the editor, single case reports, narrative reviews, systematic reviews, meta-analyses, and studies involving patients older than 18 years or with psychiatric, cognitive, or neurological disorders were excluded. Only studies published in English or Spanish were considered. The compliance of all eligibility items was independently checked by three reviewers (G.V.V.C., J.R.R.I., and A.M.P.), followed by revising the full text for the selected articles. Following recommendations of the Cochrane handbook and to ensure transparency in this review, a removal of duplicates was performed after the database search, using the Zotero software. Differences in judgment between reviewers were resolved by consensus through case-by-case discussions among the three authors.
2.2 Search strategy and study selection
A systematic literature search was conducted, using PubMed,1 renowned for its extensive coverage of health, medicine, and related disciplines, including telemedicine (26); SCOPUS,2 which offers broad interdisciplinary coverage (27); and Literatura Latinoamericana y del Caribe en Ciencias de la Salud (LILACS),3 which encompasses regional and grey literature to enhance geographical diversity (26). The electronic search strategy was structured in three blocks: population, intervention, and outcomes. The PubMed search string was developed first and then translated to Scopus and LILACS, according to the syntax rules and search manuals for each database. For the case of LILACS, the search was conducted using Spanish terms. The complete search strategies for all three databases are provided in Supplementary Table 1. The studies were retrieved based on selection criteria, checking the title and abstract, and a subsequent evaluation of the full text. The search was concluded on 28/05/2025.
2.3 Data management and quality assessment
Data was extracted from the original articles into Excel sheets (Microsoft Windows) and the Cochrane RevMan 7.2.0 version. The generally considered variables were study design, geographical location, application or platform used for interaction with the caregivers, type of surgery, time of measure, questionnaires used, and level of satisfaction with the implemented strategy. The methodological quality of the randomized trials and non-randomized studies was assessed by the Risk of Bias 2 (RoB2) and Risk of Bias in Non-randomised Studies of Interventions (ROBINS-I) tools of Cochrane, respectively (28, 29). All considered results and variables were compiled into a summary table of findings. The methodological approach for explaining and carrying out the telemedicine intervention was also considered. Similarly, the certainty of presented evidence derived from this systematic review was performed by implementing a Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, based on the Cochrane handbook for grading the certainty of the evidence (30). General data extraction and the implementation of tools for article analysis were carried out by G.V.V.C. and J.R.R.I. Similar to the screening processes, disagreements between the two authors regarding data and bias analysis were resolved through discussion among the three authors.
The implemented protocol for this systematic review was registered and can be accessed on the international database of prospectively registered systematic reviews in health and social care (PROSPERO) under the registration number CRD42024545858.
2.4 Synthesis of results
Data synthesis was conducted following the Cochrane Handbook (22) and the SWiM guideline (Synthesis Without Meta-analysis) (31). Studies were grouped a priori by design and, within each design, by outcome: caregiver knowledge, satisfaction, and postoperative complications and benefits in the quality of life of patients. Because methodological heterogeneity ruled out a meta-analysis, a structured narrative synthesis with vote counting based on the direction of the point estimate was applied. An upward arrow (↑) was assigned when the point estimate favored tele-medicine, a downward arrow (↓) when it favored the comparator, and a horizontal arrow (↔) when the direction was unclear. Effect estimates are presented in their original units. p-values are reported for context only.
Heterogeneity was explored qualitatively by comparing population characteristics, intervention components and risk-of-bias judgments across studies. Certainty of the evidence was assessed with the GRADE framework and summarised. No study or outcome was prioritised. All results received equal interpretative weight because each addressed the evaluated outcomes. The results were presented in a summary table describing the characteristics of the included studies, as well as in an additional table showing the certainty of the evidence for each outcome analyzed. Limitations of this synthesis approach are discussed in the Discussion section.
2.5 Appraisal of included studies
Ethics committee approval was not required as this manuscript is a systematic review article.
3 Results
The initial searches yielded 994 studies in Scopus, 395 in PUBMED, and 773 in LILACS, for 2,163 records registered at the identification stage. After excluding the duplicates and a subsequent title and abstract screening, 95 papers remained for full-text review. An additional 91 studies were excluded during the full-text review, considering the inclusion criteria and the specificity of the educational purpose, and no hybrid interventions (telemedicine and in-person), or interventions with purposes other than educational, such as those focused on providing patient care. Therefore, most of the articles excluded at this stage were studies on telemedicine for routine consultations. A smaller proportion involved adult populations or interventions aimed at patient self-care. The final review comprised 4 articles, consisting of 2 UCBA (32, 33) and 2 RCTs studies (34, 35), published between 2020 and 2022 (Figure 1).
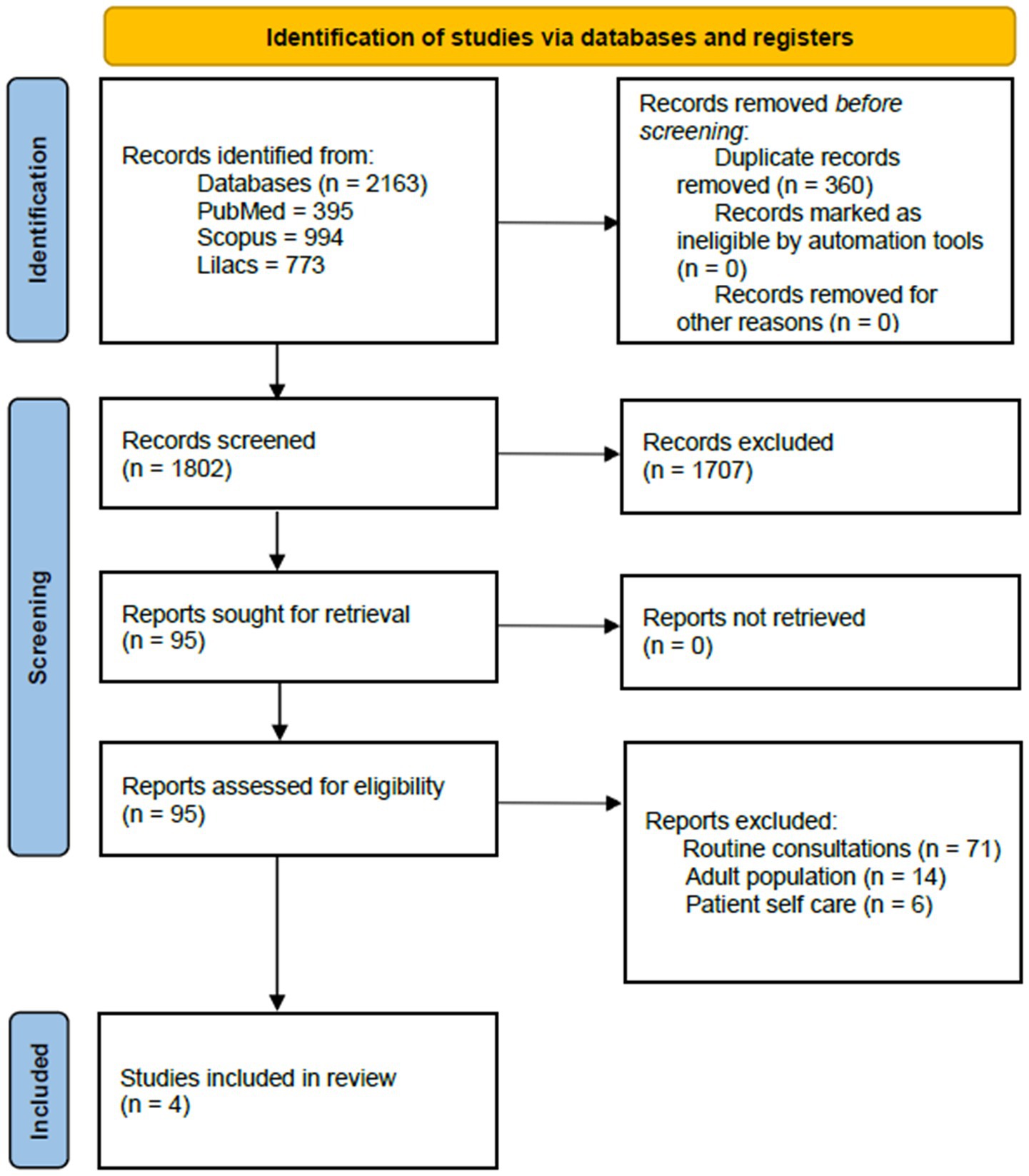
Figure 1. PRISMA flow diagram.
3.1 General characteristics of included studies
The population assessed in the included studies varied from 2 to 74 participants, with follow-up durations ranging from 1 to 4 months and documenting four types of surgical conditions. Among the platforms employed for remote health aimed at education, the WeChat app was used in the 2 RCTs, and only one study indicated the use of mixed tools, including video and phone calls. The comparator (control groups for RCT) utilized information provided through manuals and leaflets. The resources for reporting the main outcomes were also diverse, with several surveys used to estimate caregiver knowledge. Two studies employed the Patient Satisfaction Questionnaire Short Form 18 (PSQ-18) for satisfaction quantification. Additionally, from the four included studies, only Yu et al. offered a more detailed explanation of how the telemedicine intervention was implemented (34). This was based on the WeChat platform and consisted of an attending physician and two nursing supervisors to distribute information on breastfeeding, including its importance, operational skills, and hygiene practices. A summary of the main criteria and extracted data from the included works is provided in Table 1.
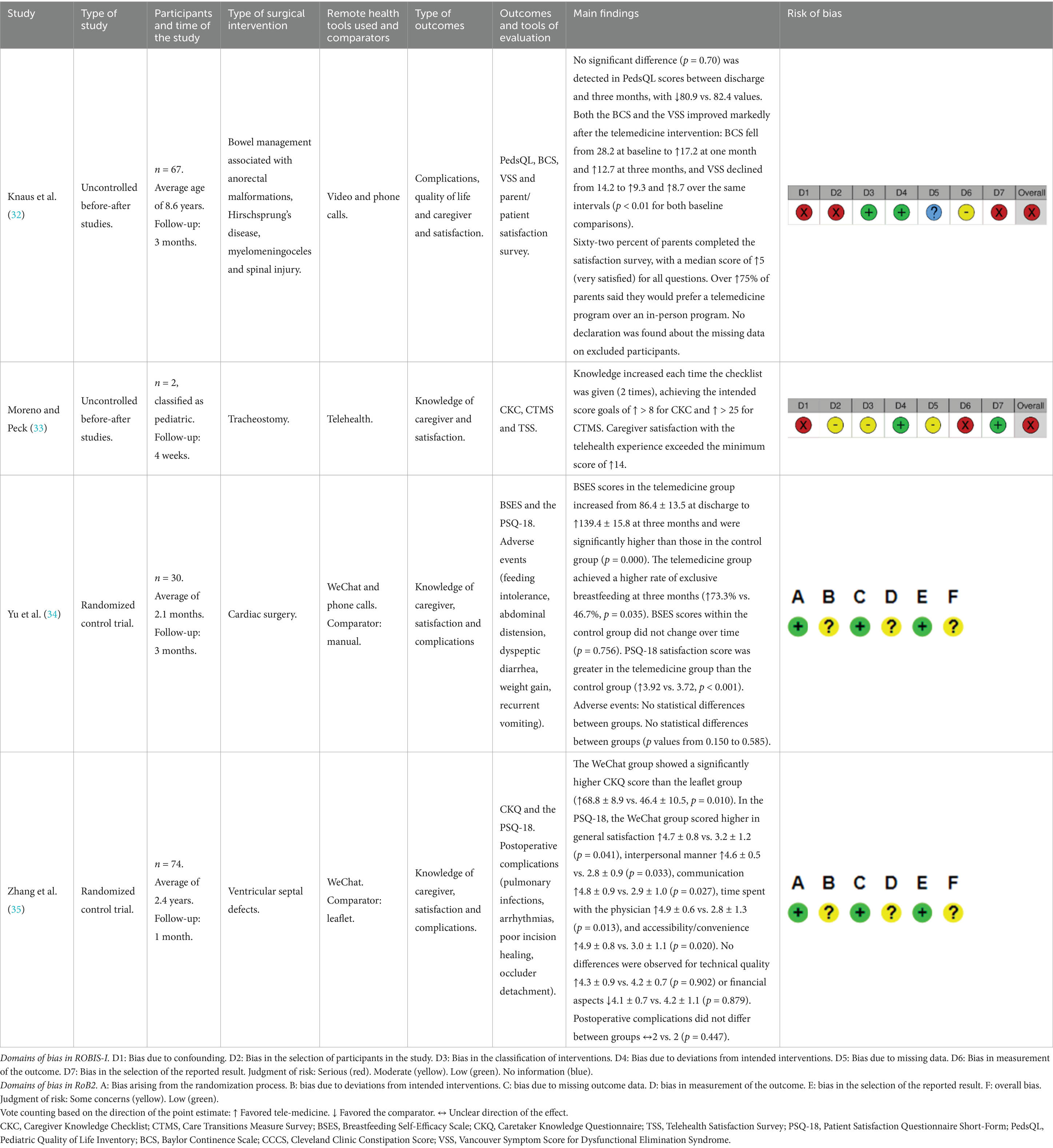
Table 1. Characteristics of the studies included in the revision (n = 4).
3.2 Risk of bias assessment
Among the analyzed randomized trial studies, there were some concerns about the design of the studies, as overall judgment. Specifically, Yu et al. (34) and Zhang et al. (35) raised concerns about the risk of bias due to the potential participant awareness of their assignment during the trial, impacting two domains of bias. In the case of non-randomized studies, UCBAs studies, the general risk of bias was serious. Knaus et al. (32) and Moreno and Peck (33) demonstrated a serious risk due to a lack of adjustments for confounding factors related to patient or caregiver baseline characteristics. Additionally, other classifications of serious risks or biases included participant awareness of the intervention received (33) and the lack of equivalence in the analysis applied to intervention groups (32). One study was classified as “No Information” in one of the domains due to a need for more information about missing data on excluded participants (Table 1).
3.3 Certainty of evidence
Due to the heterogeneity of the studies, not all retrieved articles were included to evaluate the certainty of each outcome. The level of satisfaction with the intervention was assessed in all four included studies. Knowledge level was evaluated in three of them (33–35), while complications and benefits in quality of life were assessed in three studies as well (32, 34, 35). Table 2 shows the results of applying the GRADE tool for judgment of the certainty of evidence. Morbidity is downgraded by the inconsistency, indirectness, and imprecision criteria. This is due to mixed results, where Knaus et al. report favorable outcomes, while the other studies do not report significant results with the telemedicine intervention. Additionally, different clinical outcomes are reported between the four studies, and imprecision is due to the inconsistent reporting of confidence intervals in the two RCTs. Moreover, imprecision impacts the satisfaction and knowledge outcomes because a small “n” of participants reported in one study. The risk of bias also affects all outcomes. After applying the GRADE criteria, the certainty of evidence is moderate for satisfaction and knowledge, and very low for morbidity.
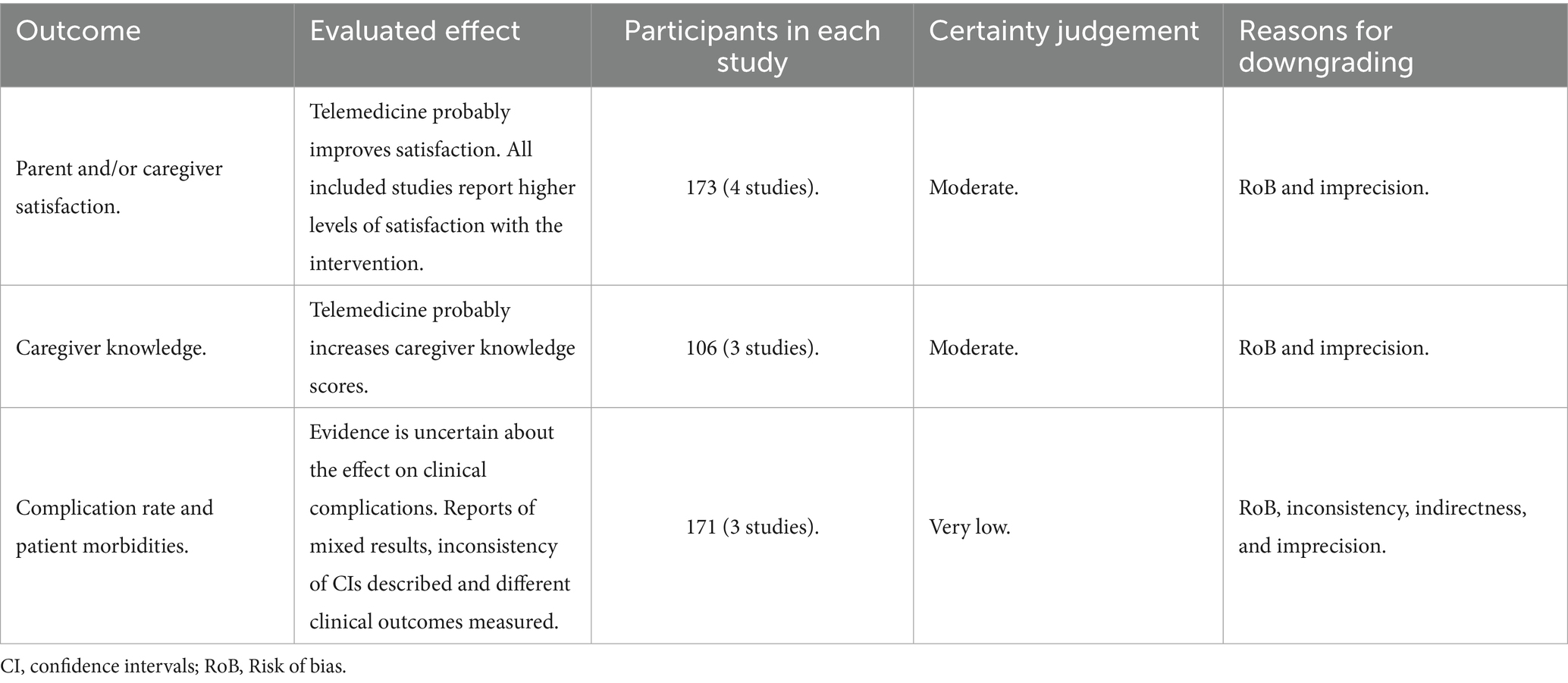
Table 2. Evaluation of the certainty of evidence using the GRADE tool.
3.4 Main outcomes analyzed
For the analysis of the various elements evaluated in this systematic review, the authors of the included studies used a series of standardized questionnaires. These included: The Caregiver Knowledge Checklist (CKC), used to assess caregivers’ knowledge. The Care Transitions Measure Survey (CTMS) evaluates caregiver preparedness during the care transition process. The Breastfeeding Self-Efficacy Scale (BSES), designed to measure the confidence of the mother in her ability to breastfeed. The Caretaker Knowledge Questionnaire (CKQ) indicates the level of knowledge of the caregiver. The Telehealth Satisfaction Survey (TSS), used to assess satisfaction or dissatisfaction with telehealth interventions. The Patient Satisfaction Questionnaire Short-Form (PSQ-18) measures multiple dimensions of patient satisfaction, including general satisfaction, technical quality, interpersonal manner, communication, financial aspects, time spent with the physician, accessibility, and convenience. The Pediatric Quality of Life Inventory (PedsQL), a tool designed to measure health-related quality of life in children and adolescents. The Baylor Continence Scale (BCS) assesses the impact of fecal incontinence on quality of life in pediatric populations. The Cleveland Clinic Constipation Score (CCCS), also known as the Wexner Constipation Score, quantifies the severity of chronic constipation in both adults and children. The Vancouver Symptom Score for Dysfunctional Elimination Syndrome (VSS), used to identify symptoms of dysfunctional elimination syndrome in children, including both urinary and defecatory problems.
3.4.1 Parent and caregiver knowledge
Moreno and Peck used the CKC, which includes items for evaluating tracheostomy management skills (33). A CTMS was also used in this study to evaluate the preparedness of the caregiver. These surveys were applied during the 2-week telehealth visit and in a face-to-face visit 4 weeks later. The results indicated that knowledge increased each time the checklist was given, achieving the intended score goals of >8 for CKC and >25 for CTMS. The other UCBA study, Knaus et al. did not assess the level of prior knowledge of the subject (32).
Yu et al. applied the BSES, which contained 33 items in total, with a 5-point Likert scale, associated with skill and psychological dimensions, for measuring the breastfeeding self-efficacy, after congenital cardiac surgery (34). The knowledge measured by this tool was similar among the evaluated groups at discharge. However, during the 3-month follow-up, the BSES in the telemedicine group increased markedly, from 86.4 ± 13.5 at discharge to 139.4 ± 15.8 points, whereas the control group showed no significant change, from 85.5 ± 9.7 to 92.3 ± 9.4. Consequently, at 3 months postdischarge, the telemedicine group demonstrated significantly (p = 0.00) higher breastfeeding self-efficacy and greater confidence in caring for their infants than the standard care group.
In the case of the second RCT study conducted by Zhang et al., the CKQ is a survey comprising 18 items, with possible scores ranging from 0 to 4 points (35). Different score ranges indicate the level of knowledge: a score < 44 is classified as a low knowledge level, 44 to 58 is classified as an intermediate knowledge level, and > 58 is classified as a high knowledge level. The reported CKQ scores in the WeChat group (68.8 ± 8.9) were significantly higher than those in the leaflet group (46.4 ± 10.5) during the perioperative period.
3.4.2 Patient satisfaction
The satisfaction survey used by Knaus et al. consisted of 10 questions evaluated using a Likert scale ranging from 1 (very dissatisfied) to 5 (very satisfied) (34). Additionally, the survey included multiple-choice queries and a section for free-text comments. The results describe 91% (39/43) of parents indicating that the telemedicine appointments were less stressful for their child compared to in-person visits, and over 75% (33/43) of parents said they would choose a telemedicine program over an in-person program. Additionally, over 75% of parents said they would choose a telemedicine program over an in-person program. In Moreno and Peck study, the TSS consisted of 10 questions with dichotomous responses of satisfied or unsatisfied and a result of >14 as an intended score goal (33). At each patient encounter, caregivers expressed gratitude for ongoing communication and continuity of quality care.
The PSQ-18, employed in the two analyzed RCTs, is a validated form comprising 18 questions. It utilizes a five-point Likert scale (1–5) to measure various dimensions, including general satisfaction, technical quality, interpersonal manner, communication, financial aspects, time spent with the physician, accessibility, and convenience. Yu et al. reported significantly higher satisfaction in the study group (p < 0.001), compared to the control group (34). In this study, all dimensions analyzed in the survey were significantly higher in the remote health intervention group. Similarly, Zhang et al. reported higher general satisfaction in the WeChat group than in the leaflet group and described better satisfaction in five out of seven dimensions using the app (35).
3.4.3 Complication rate
Knaus et al. applied the PedsQL, and PROMs were collected for each patient at the first clinic visit before the program (intake), at the 1-month follow-up, and at the 3-month follow-up after the BMP (34). The recorded PROMs included the BCS, CCCS, and the VSS. Before the BMP, stool continence data were available for 42 patients aged 4 or older. Of these patients, 28.6% (12/42) were continent of stool at intake. At the 1-month follow-up, 45.1% (23/51) were continent of stool, and at the 3-month follow-up, 68.9% (31/45) were continent of stool (p = 0.1 and p < 0.01, respectively). Before the BMP, urine continence data were available for 47 patients, and 55.3% (26/47) were continent of urine at intake. There was a significant improvement in the BCS and VSS scores after undergoing the telemedicine BMP (p < 0.01 for 1-month and 3-month follow-up compared to baseline). Urinary continence improved to 63.6% (28/44) at the 1-month follow-up, with further improvement to 73.7% (28/38) at the 3-month follow-up, although these differences were not statistically significant (p = 0.42 and p = 0.09, respectively).
Zhang et al. mention no significant difference between the two groups in postoperative complications (such as pulmonary infections, arrhythmias, poor incision healing, residual shunts, and occlude detachment) (35). Yu et al. describe that there was no significant difference in the incidence of feeding intolerance, abdominal distension, dyspeptic diarrhea, weight gain, or recurrent vomiting between the two groups during the 3-month follow-up period (p > 0.05) (34). The prevalence of these adverse events was smaller in the study group. Moreno and Peck did not evaluate morbidity or complications.
4 Discussion
Communication technologies have advanced for decades, presenting an unprecedented opportunity to overcome the limitations imposed by traditional medical services, where both the provider and the recipient must be physically present in the same location simultaneously. Information and communication technologies, including telemedicine, are pivotal for improving healthcare services (36).
Interestingly, most of the published articles on telemedicine for pediatric patients are focused on the postoperative classical follow-up rather than specifically on education for caregivers. In addition to the PRISMA screening applied in our research to exclude studies involving the typical use of telemedicine for routine checks, this aspect can also be noted in a recent systematic review of pediatric orthopedic trauma patients. This review assessed the satisfaction of both patients and surgeons with telemedicine remote care during the COVID-19 pandemic, as reported in the included articles (37). On the other hand, our systematic review found a few studies that specifically analyze telemedicine focused on the education of caregivers about postoperative care. Overall, the data we have reviewed suggests that implementing a remote health approach can improve the knowledge of caregivers to attend to the patients at home, with increased satisfaction compared to the use of manuals and documents for education, and also decreasing the complication rates.
However, when analyzing the mechanism for carrying out parental and caregiver education in the postoperative environment, there is a lack of detailed information for explaining the designed and implemented methodological approach, such as the use of videos, apps, the employment of management guides, and simulation strategies, among others. This hinders the efficient replication of this type of intervention by medical groups interested in applying this method. It also does not allow for assessing the potential and effectiveness of these strategies in achieving caregiver education. One of the studies in our review describes the use of dedicated personnel and the WeChat app to educate parents and share experiences in the postoperative context (34). Beyond the articles reviewed here, other studies have suggested developing specific instructional programs. These programs, supported by the WeChat app, would provide content on basic and advanced knowledge regarding patient conditions and how to conduct appropriate care procedures to prevent infections, using clear and understandable language (38). Furthermore, this social media tool has been described in China for general patient care education in several areas related to stroke patients (39) and coronary artery disease (40).
Regarding the bias analysis conducted in this systematic review, there is potential for improvement in both RCT and UCBA studies, particularly in clearly defining the groups receiving the telemedicine intervention and those that do not, as well as establishing the patient baseline information, which is primarily lacking in non-randomized studies. Other serious risks or biases classifications included the participant awareness of the intervention received and the lack of equivalence in the analysis applied to the intervention group. Including information about the studied population, such as age group, the level of education and knowledge of the caregiver, and easy access to technological tools, may enable the creation of more homogeneous groups for comparison or enhance the before-and-after study approach. Regarding the certainty of the presented evidence analysis, moderate certainty evidence suggests that the telemedicine interventions improve the knowledge of the caregivers about postoperative care in the home setting and increase their overall satisfaction with the intervention. These findings indicate that telemedicine can provide parents with additional resources to manage the postsurgical needs of patients and may promote a wider adoption of such programs. However, the evidence for clinical morbidity and complications is of very low certainty. Therefore, we cannot determine whether telemedicine reduces postsurgical complications or adverse postoperative events that require a classical assessment. Further well designed trials with uniform outcome measures are needed before firm conclusions can be drawn about safety and clinical effectiveness.
To assess caregivers satisfaction with telemedicine programs, the validated PSQ-18 survey was employed, which also allowed for determining the general satisfaction, technical quality, interpersonal manner, communication, financial aspects, time spent with the physician, accessibility, and convenience, providing more comprehensive information about the various elements involved in the satisfaction of a program, not just a single value, but enabling the determination of areas for improvement in future research. Patient satisfaction is becoming increasingly important in healthcare, encompassing numerous aspects that warrant evaluation. Valdes et al. conducted a study to determine if the PSQ-18 was an appropriate outcome measure for assessing patient satisfaction among individuals undergoing hand therapy (41). The findings suggest that the PSQ-18, when adapted for hand therapy, is a suitable outcome measure for assessing patient satisfaction in this context, as it evaluates multiple subscales of the phenomenon. In the case of UCBA studies, they focused exclusively on providing numerical information regarding the overall satisfaction of the caregiver. They did not focus on the social component linked to patient care, represented by economic, communicative, and accessibility aspects. The aspects assessed in these scales include important variables that must be considered when selecting a telemedicine or in-person program.
Regarding postoperative complications and morbidity, despite not obtaining statistically significant results in 2 RCTs studies where this variable was evaluated, it can be highlighted that with the support of the intestinal management program, the percentage of digestive incontinence decreased progressively during follow-up, which was statistically significant for Knaus et al. (32).
It is important to highlight that telemedicine is subdivided into different areas, with teleassistance being the most widely developed in the scientific literature. Its benefits regarding the reduction of space–time variables are clear. However, the area of telemedicine aimed at education for caregivers has not been as extensively developed. The literature reflects its utility more for educational purposes within the medical community, rather than directed towards mothers, fathers, and caregivers, which still needs to be explored. The applicability of telemedicine includes an important social component, which can be evidenced in this systematic review. For example, despite the lack of statistically significant differences in complications or morbidity between groups in some of the studies, treated in person and those managed via telemedicine, there is evident satisfaction among caregivers regarding telemedicine programs for educational purposes.
Factors such as the availability of staff, educational materials, and savings in terms of travel or mobility potentially contribute to user satisfaction. As healthcare professionals, we understand how overwhelming a hospital admission can be, and doubts about managing a particular condition often arise at home when we do not have the presence of healthcare personnel. Having the educational support of healthcare professionals, or their availability to address any doubts that may arise at home, is a subjective but highly relevant variable provided by remote practices. An example of this is the statistically significant improvement in continence observed in patients enrolled in intestinal management programs. Yang et al. conducted a systematic review to assess the effects of telemedicine on the burden, anxiety, depression, and quality of life of informal caregivers of patients receiving palliative care (42). They included 9 randomized controlled trials and concluded that telemedicine statistically significantly reduced the caregiving burden and anxiety of informal caregivers. However, it had no significant effect on depression or quality of life.
Beyond clinical outcomes, the implementation of telemedicine related to pediatric postsurgical care also carries implications for optimizing sustainability within healthcare structures. Maia et al. (43) described a Pediatric Telecardiology Service in Portugal, whose implementation resulted in cost savings of approximately 1.1 million euros and 419 euros per patient for the healthcare system. Other studies emphasize three fundamental pillars of telemedicine sustainability: cost reduction, improved service utilization, and enhanced quality of care. These aspects align directly with Sustainable Development Goals (SDGs) 3 and 10, promoting well-being and reducing inequalities (44). Achieving SDGs related to telemedicine also involves overcoming challenges to facilitate broader adoption. Critical factors include robust digital infrastructure, sustainable financing models supported by public-private partnerships, and continuous professional training (45).
The main limitation of this review was the inability to conduct a quantitative synthesis or meta analysis. Despite the creation of a summary of findings table and assessing certainty with GRADE, substantial methodological heterogeneity, including differences in study design, outcome instruments, and the outcomes themselves, prevented statistical pooling and reduced the overall certainty of the evidence. Another potential limitation was the heterogeneity of outcome metrics across studies. To address this, we report the exact p-values and present each result in the original units of its measurement tool, therefore strengthening the narrative synthesis, supported by the vote counting method. Nonetheless, the findings of this study suggest the advantages and satisfaction of telemedicine for the education of caregivers, considering the context in which it is applied and the general necessity for well-described methodologies for training parents and caregivers. Similarly, the implementation of the remote health education process in postoperative care is highly dependent on the context, given potential limitations related to access to technology. This necessitates the use of platforms and resources based on the availability of devices. Consequently, changes need to be instituted through regulations and policies that incorporate this new service modality centered on education, ensuring its authorization by insurers (46).
Although there are few publications about the use of telemedicine for educational purposes in the field of pediatrics, specifically in pediatric surgery, this approach is increasingly common in adult care, due to the public health benefits these interventions can offer. A cluster-randomized controlled trial conducted in Guangzhou, China, showed that a six-month self-management intervention, including health education, health promotion, group chat, and blood pressure monitoring, and delivered via WeChat, could feasibly and effectively help patients reduce blood pressure and improve self-management effectiveness (47). Digital health has shown its reach not only in the context of chronic diseases and surgical conditions, but also in the development of strategies such as reducing tobacco consumption. For example, the study published by Cupertino et al. (48) Vive Sin Tabaco. ¡Decídete!, a web-based (e-health) decision aid designed to help Mexican smokers create a quit plan and access cessation resources. The intervention included 164 smokers from two primary care clinics who presented with both physical and psychological dependence on nicotine. Two out of ten smokers who used the tool successfully quit smoking, with a 3-month follow-up rate of 81.5% and a 7-day point prevalence abstinence rate of 19.1%.
Lastly, from a prospective point of view, this review was used as a starting point for developing a telemedicine program aimed at mothers, fathers, and caregivers of pediatric post-surgical patients with gastrostomies, ileostomies, and colostomies in the provinces of Pichincha, Guayas, and Manabí in the South American country of Ecuador. The goal is to provide tools to caregivers for vulnerable populations who may benefit from telemedicine follow-up for educational purposes due to socioeconomic, geographical, and even healthcare system saturation issues. This program is intended to be delivered by healthcare professionals, and it aims to reduce patient morbidity, seeking to contribute to the scientific literature in an area that is currently under-researched.
5 Conclusion
The results showing increased caregiver knowledge and higher satisfaction with the remote approach indicate that telemedicine tools represent a promising strategy for patients and healthcare systems in the education and care of postoperative pediatric patients. Despite the intrinsic limitations, it is a valid strategy that adapts to the day-to-day lives of patients and their caregivers. However, more studies with detailed explanations of the methodological forms are needed to adjust the telemedicine strategy, reduce biases and reinforce the attention of government policies to facilitate its implementation in society beyond remote care, favoring the utilization of the tool for educational purposes.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Author contributions
GV-C: Investigation, Conceptualization, Funding acquisition, Resources, Supervision, Software, Writing – original draft, Project administration, Validation, Data curation, Methodology, Visualization, Formal analysis. JR-I: Validation, Writing – review & editing, Funding acquisition, Investigation, Formal analysis, Conceptualization, Methodology. AM-P: Formal analysis, Validation, Writing – review & editing, Investigation, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by DII-P23233_4 (GVVC) and DII-P011617_2 (JRRI), Directorate of Research and Innovation, Universidad Internacional SEK (UISEK).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1606211/full#supplementary-material
Footnotes
References
1. Waller, M, and Stotler, C. Telemedicine: a primer. Curr Allergy Asthma Rep. (2018) 18:54. doi: 10.1007/s11882-018-0808-4
2. Burke, BL Jr, and Hall, RWSection on Telehealth Care. Telemedicine: pediatric applications. Pediatrics. (2015) 136:e293–308. doi: 10.1542/peds.2015-1517
3. Galea, MD. Telemedicine in rehabilitation. Phys Med Rehabil Clin N Am. (2019) 30:473–83. doi: 10.1016/j.pmr.2018.12.002
4. Craig, J, and Patterson, V. Introduction to the practice of telemedicine. J Telemed Telecare. (2005) 11:3–9. doi: 10.1177/1357633X0501100102
5. Standing, C, Standing, S, McDermott, M, et al. The paradoxes of telehealth: a review of the literature 2000–2015. Syst Res Behav Sci. (2018) 35:90–101. doi: 10.1002/sres.2442
6. Arshad Ali, S, Bin Arif, T, Maab, H, Baloch, M, Manazir, S, Jawed, F, et al. Global interest in telehealth during COVID-19 pandemic: an analysis of Google trends. Cureus. (2020) 12:e10487. doi: 10.7759/cureus.10487
7. Vorenkamp, KE, Kochat, S, Breckner, F, and Dimon, C. Challenges in utilizing telehealth for chronic pain. Curr Pain Headache Rep. (2022) 26:617–22. doi: 10.1007/s11916-022-01067-1
8. Penwill, NY, Roessler De Angulo, N, Pathak, PR, et al. Changes in pediatric hospital care during the COVID-19 pandemic: a national qualitative study. BMC Health Serv Res. (2021) 21. doi: 10.1186/s12913-021-06947-7
9. Suárez-Rodríguez, GL, Salazar-Loor, J, Rivas-Condo, J, Rodríguez-Morales, AJ, Navarro, JC, and Ramírez-Iglesias, JR. Routine immunization programs for children during the COVID-19 pandemic in Ecuador, 2020—hidden effects, predictable consequences. Vaccines. (2022) 10:857. doi: 10.3390/vaccines10060857
10. Nasher, O, Sutcliffe, JR, and Stewart, RJ. Pediatric surgery during the COVID-19 pandemic: an international survey of current practice. Eur J Pediatr Surg. (2021) 31:407–13. doi: 10.1055/s-0040-1714714
11. Metzger, G, Jatana, K, Apfeld, J, Deans, KJ, Minneci, PC, and Halaweish, I. State of telemedicine use in pediatric surgery in the USA—where we stand and what we can gain from the COVID-19 pandemic: a scoping review. World J Pediatr Surg. (2021) 4:e000257. doi: 10.1136/wjps-2020-000257
12. Farrell, S, Schaeffer, EK, and Mulpuri, K. Recommendations for the care of pediatric orthopaedic patients during the COVID-19 pandemic. J Am Acad Orthop Surg. (2020) 28:e477–86. doi: 10.5435/JAAOS-D-20-00391
13. Rabbitts, JA, and Groenewald, CB. Epidemiology of pediatric surgery in the United States. Paediatr Anaesth. (2020) 30:1083–90. doi: 10.1111/pan.13993
14. Ozgediz, D, Langer, M, Kisa, P, and Poenaru, D. Pediatric surgery as an essential component of global child health. Semin Pediatr Surg. (2016) 25:3–9. doi: 10.1053/j.sempedsurg.2015.09.002
15. Bouchard, ME, Tian, Y, Justiniano, J, Linton, S, DeBoer, C, Abdullah, F, et al. A critical threshold for global pediatric surgical workforce density. Pediatr Surg Int. (2021) 37:1303–9. doi: 10.1007/s00383-021-04939-6
16. Kids Operating Room. Paediatric surgery: a global health crisis. Global Report 2022. KidsOR; (2022). Available online at: https://www.kidsor.org/assets/uploads/files/downloads/EN__KIDSOR_PAEDIATRIC_SURGERY_GLOBAL_REPORT.pdf
17. Bhattad, PB, and Pacifico, L. Empowering patients: promoting patient education and health literacy. Cureus. (2022) 14:e27336. doi: 10.7759/cureus.27336
18. Murphy, M, O'Brien, P, and Gates, M. Postoperative management of pediatric patients. Adv Pediatr. (2021) 68:103–19. doi: 10.1016/j.yapd.2021.05.010
19. Sng, QW, He, HG, Wang, W, Taylor, B, Chow, A, Klainin-Yobas, P, et al. A meta-synthesis of children's experiences of postoperative pain management. Worldviews Evid-Based Nurs. (2017) 14:46–54. doi: 10.1111/wvn.12185
20. Kohler, JE, Falcone, RA Jr, and Fallat, ME. Rural health, telemedicine and access for pediatric surgery. Curr Opin Pediatr. (2019) 31:391–8. doi: 10.1097/MOP.0000000000000763
21. Dedeilia, A, Esagian, SM, Ziogas, IA, Giannis, D, Katsaros, I, and Tsoulfas, G. Pediatric surgery during the COVID-19 pandemic. World J Clin Pediatr. (2020) 9:7–16. doi: 10.5409/wjcp.v9.i2.7
22. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. PLoS Med. (2021) 18:e1003583. doi: 10.1371/journal.pmed.1003583
23. Higgins, JPT, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, et al. Cochrane handbook for systematic reviews of interventions version 6.5 (updated august 2024). Cochrane (2024). Available online at: https://training.cochrane.org/handbook/current
24. Cao, J, Lim, Y, Sengoku, S, Guo, X, and Kodama, K. Exploring the shift in international trends in Mobile Health Research from 2000 to 2020: bibliometric analysis. JMIR Mhealth Uhealth. (2021) 9:e31097. doi: 10.2196/31097
25. Feng, H, Kurata, K, Cao, J, Itsuki, K, Niwa, M, Aoyama, A, et al. Telemedicine research trends in 2001-2022 and research cooperation between China and other countries before and after the COVID-19 pandemic: bibliometric analysis. Interact J Med Res. (2024) 13:e40801. doi: 10.2196/40801
26. Gusenbauer, M, and Haddaway, NR. Which academic search systems are suitable for systematic reviews or meta-analyses? Evaluating retrieval qualities of Google scholar, PubMed, and 26 other resources. Res Synth Methods. (2020) 11:181–217. doi: 10.1002/jrsm.1378
27. Mongeon, P, and Paul-Hus, A. The journal coverage of web of science and scopus: a comparative analysis. Scientometrics. (2016) 106:213–28. doi: 10.1007/s11192-015-1765-5
28. Sterne, JA, Hernán, MA, Reeves, BC, Savović, J, Berkman, ND, Viswanathan, M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
29. Sterne, JAC, Savović, J, Page, MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
30. Higgins, JPT, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated February 2024). Cochrane, 2024. Chapter 14: Completing “Summary of findings” tables and grading the certainty of the evidence. Available from: https://training.cochrane.org/handbook/current/chapter-14 (Accessed 5 June 2025).
31. Campbell, M, McKenzie, JE, Sowden, A, Katikireddi, SV, Brennan, SE, Ellis, S, et al. Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ (Clin Res Ed). (2020) 368:l6890. doi: 10.1136/bmj.l6890
32. Knaus, ME, Ahmad, H, Metzger, GA, Beyene, TJ, Thomas, JL, Weaver, LJ, et al. Outcomes of a telemedicine bowel management program during COVID-19. J Pediatr Surg. (2022) 57:80–5. doi: 10.1016/j.jpedsurg.2021.09.012
33. Moreno, L, and Peck, JL. Nurse practitioner-led telehealth to improve outpatient pediatric tracheostomy management in South Texas. J Pediatr Health Care. (2020) 34:246–55. doi: 10.1016/j.pedhc.2019.11.008
34. Yu, XR, Xie, WP, Liu, JF, Yu, X‐R, Xie, W‐P, Liu, J‐F, et al. Effect of WeChat follow-up education on breastfeeding efficiency of infants after congenital cardiac surgery and parents' satisfaction: a short-term follow-up study. J Paediatr Child Health. (2021) 57:1899–904. doi: 10.1111/jpc.15605
35. Zhang, QL, Xu, N, Huang, ST, Chen, Q, and Cao, H. Effect of using the WeChat platform on the perioperative health education of parents of children who underwent transthoracic device closure of VSDs. J Cardiothorac Surg. (2020) 15:256. doi: 10.1186/s13019-020-01282-0
36. Ren, X, Wang, Z, Wu, Y, Li, Y, Chen, M, Zhai, Y, et al. Design and implementation of a message-based regional telemedicine system to achieve high availability and scalability. Telemed J E Health. (2019) 25:243–9. doi: 10.1089/tmj.2018.0047
37. Chaudhry, H, Nadeem, S, and Mundi, R. How satisfied are patients and surgeons with telemedicine in orthopaedic care during the COVID-19 pandemic? A systematic review and meta-analysis. Clin Orthop Relat Res. (2021) 479:47–56. doi: 10.1097/CORR.0000000000001494
38. Liu, J, Zheng, X, Zhang, X, Feng, Z, Song, M, and Lopez, V. The evidence and future potential of WeChat in providing support for Chinese parents of pediatric patients undergoing herniorrhaphy. J Transcult Nurs. (2020) 31:114–20. doi: 10.1177/1043659619841672
39. Kang, K, and Li, S. A WeChat-based caregiver education program improves satisfaction of stroke patients and caregivers, also alleviates poststroke cognitive impairment and depression: a randomized, controlled study. Medicine. (2022) 101:e29603. doi: 10.1097/MD.0000000000029603
40. Kang, G, Zhang, H, Zhou, J, and Wan, D. The WeChat platform-based health education improves health outcomes among patients with stable coronary artery disease. Patient Educ Couns. (2023) 111:107704. doi: 10.1016/j.pec.2023.107704
41. Valdes, K, Kannas, S, Kakar, S, Veneziano, J, Dake, T, and Sierra, F. Patient satisfaction of hand therapy services. J Hand Ther. (2021) 34:585–90. doi: 10.1016/j.jht.2020.07.006
42. Yang, X, Li, X, Jiang, S, and Yu, X. Effects of telemedicine on informal caregivers of patients in palliative care: systematic review and meta-analysis. JMIR Mhealth Uhealth. (2024) 12:e54244. doi: 10.2196/54244
43. Maia, MR, Castela, E, Pires, A, and Lapão, LV. How to develop a sustainable telemedicine service? A pediatric telecardiology service 20 years on—an exploratory study. BMC Health Serv Res. (2019) 19:681. doi: 10.1186/s12913-019-4511-5
44. Palozzi, G, Schettini, I, and Chirico, A. Enhancing the sustainable goal of access to healthcare: findings from a literature review on telemedicine employment in rural areas. Sustainability. (2020) 12:3318. doi: 10.3390/su12083318
45. Jerjes, W, and Harding, D. Telemedicine in the post-COVID era: balancing accessibility, equity, and sustainability in primary healthcare. Front Digit Health. (2024) 6:1432871. doi: 10.3389/fdgth.2024.1432871
46. Hincapié, MA, Gallego, JC, Gempeler, A, Piñeros, JA, Nasner, D, and Escobar, MF. Implementation and usefulness of telemedicine during the COVID-19 pandemic: a scoping review. J Prim Care Community Health. (2020) 11:2150132720980612. doi: 10.1177/2150132720980612
47. Li, X, Li, T, Chen, J, Xie, Y, An, X, Lv, Y, et al. A WeChat-based self-management intervention for community middle-aged and elderly adults with hypertension in Guangzhou, China: a cluster-randomized controlled trial. Int J Environ Res Public Health. (2019) 16:4058. doi: 10.3390/ijerph16214058
48. Cupertino, AP, Cartujano-Barrera, F, Perales, J, Formagini, T, Rodríguez-Bolaños, R, Ellerbeck, EF, et al. Vive sin Tabaco… ¡Decídete! Feasibility and acceptability of an e-health smoking cessation informed decision-making tool integrated in primary healthcare in Mexico. Telemed J E-Health. (2019) 25:425–31. doi: 10.1089/tmj.2017.0299
Keywords: pediatric surgery, follow-up, telemedicine, post-operative care, satisfaction
Citation: Vivas-Colmenares GV, Ramírez-Iglesias JR and Martínez-Pérez AM (2025) Telemedicine for educating parents or caregivers for postoperative care of pediatric patients: a systematic review. Front. Public Health. 13:1606211. doi: 10.3389/fpubh.2025.1606211
Edited by:
Shengdi Lu, Shanghai Jiao Tong University, ChinaReviewed by:
Birgitte Espehaug, Western Norway University of Applied Sciences, NorwayRyan Davidson, Harvard Medical School, United States
Copyright © 2025 Vivas-Colmenares, Ramírez-Iglesias and Martínez-Pérez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Grecia Victoria Vivas-Colmenares, Z3JlY2lhLnZpdmFzQHVpc2VrLmVkdS5lYw==