 Sujin Choi1
Sujin Choi1 Eunjeong Kang2*
Eunjeong Kang2*- 1Department of Nursing, College of Medicine, Soonchunhyang University, Asan-si, Republic of Korea
- 2Department of Health Administration and Management, Soonchunhyang University, Asan-si, Republic of Korea
Introduction: This scoping review investigates the cultural factors influencing the health of immigrants by applying Donabedian’s structure-process-outcome (SPO) model. While immigrant health has been extensively studied, cultural factors have not been systematically analyzed within a comprehensive healthcare quality framework.
Methods: Following the Arksey and O’Malley’s scoping review framework, 42 studies were identified and analyzed using the SPO model to categorize cultural factors into structural, process, and outcome dimensions.
Results: Structural factors included social support, discrimination, ethnicity, language barriers, cultural competence, and parents’ culturalism. Process factors included acculturation to new cultures, while outcome factors encompassed acculturative stress and an ethnic identity crisis. Social support and cultural competence were crucial for mitigating health challenges, whereas discrimination and language barriers were significant obstacles.
Conclusion: This study highlights the importance of an integrated approach to understanding immigrant health by addressing cultural factors within a structured health model. Our findings provide actionable insights for planning culturally sensitive policies and services to enhance immigrant health outcomes.
1 Introduction
Immigrant populations have grown significantly worldwide, reshaping societies into multicultural landscapes. According to the Organization for Economic Cooperation and Development, a country is considered multicultural when its immigrant population, including naturalized citizens, second-generation immigrants, and foreign nationals, exceeds 5% of its total population (1). In 2024, 281 million international immigrants constituted 3.6% of the global population (2). This trend suggests that the world is moving toward establishing more multicultural societies.
In response to the emerging multicultural society, previous research has focused on education, discrimination, integration, and immigrant health. The rapid surge in immigration driven by the pursuit of improved economic opportunities, education, and public health for their families (3) has shaped perspectives on immigrants’ health issues. Although recent studies have elucidated the barriers to and facilitators of health among immigrants, they have not comprehensively identified the factors that influence health using an integrated approach. An integrated approach that acknowledges the interdependence of physical, mental, and social well-being in defining health is crucial, as stated by the World Health Organization (4). Despite this definition, research on immigrant health has traditionally focused on physical and mental health. Consequently, the holistic investigation of the factors influencing immigrants’ health remains critically underexplored.
Numerous studies have reported that immigrants face a myriad of obstacles to effective healthcare, including language barriers, legal complications, stigma, limited access to health insurance, and socioeconomic disadvantages (5, 6). However, previous studies have analyzed each influencing factor in isolation, failing to explore their interconnections within a health model (7). These factors are intricately related (8), necessitating a structural framework for their presentation. Donabedian’s model, which evaluates healthcare service quality through three components-‘structure,’ ‘process,’ and ‘outcome’ (SPO) (9), offers a robust framework to analyze the interconnected factors influencing immigrant health. By applying this model, this study sought to investigate the factors influencing physical, mental, and social well-being and provide insights into enhancing healthcare service quality.
Among the myriad factors related to immigrant health, this study focuses on cultural factors. The term culture refers to the dynamic system of shared values, beliefs, behaviors, and customs that shape how individuals perceive, interpret, and respond to health and illness (10, 11). Cultural factors shape protective behaviors and have been assessed based on immigrants’ perceptions and behaviors within specific contexts (12). Thus, an improved understanding of cultural factors is essential for developing culturally and linguistically sensitive health services that minimize health disparities among immigrants.
This study aims to systematically identify and classify cultural factors influencing the physical, mental, and social health of immigrants through a scoping review, and presents these factors using Donabedian’s SPO model (9). These findings can inform the implementation of health policies that enhance health equity in multicultural contexts.
2 Methods
For The methodology used in this review was based on the framework developed in 2005 by Arksey and O’Malley. A scoping review aims to clarify the research question by broadly analyzing the available materials (13). This type of review consists of five main steps and one additional optional step depending on availability (13, 14). The five main steps included identifying the research question; relevant studies; study selection; analyzing the data; and organizing, summarizing, and reporting the findings. An optional step, which is not considered in this review, involves consulting stakeholders for further insights (13). The collated, summarized, and reported factors were categorized based on Donabedian’s SPO model (9).
In this model (9), the structure included the attributes of material resources domain (such as equipment and money), human resources domain (such as the number and qualifications of personnel), and organizational resources domain (such as medical staff organization and methods of peer review and reimbursement). The process encompasses the client’s activities in seeking and receiving care as well as the provider’s efforts in making a diagnosis and recommending or implementing treatment. Outcomes included the effects of care on clients’ health status.
In this study, we define the structural category as the system or environmental factors of society, individuals, and organizations related to immigrants’ health. The process category refers to immigrants’ interactive health experiences while navigating distinct cultures. The outcome category included the consequences of immigrants’ interactive health processes. All these terms are explained along with the factors in the Results section. Ethical approval was not required due to the nature of this review.
In this study, the term “immigrant” refers to individuals who have experienced cross-national migration and resettlement, regardless of generational status. Inclusion criteria was based on whether participants had a lived experience of migration and whether cultural factors related to that migration were central to the study’s objectives. Studies focusing on long-established ethnic minority groups without migration experience were excluded.
2.1 Search strategies
This study provides a scoping review that explores the various cultural influences on health. The sources used in this review included ScienceDirect, CINAHL, ProQuest, PsycInfo, PubMed, Embase, Web of Science, RISS, KMbase, KoreaMed, and the Cochrane Library. Journal papers and peer-reviewed articles were searched using keywords such as (“emigrant” OR “immigrant” OR “international migrant”) AND (“health” OR “health care” OR “healthcare” OR “medical”) AND (“culture” OR “cultur” OR “acculturation” OR “ethnic*” OR “acculturation” OR “cultural belief*” OR “cultural competence”). The literature search was conducted between September 29 and October 9, 2023. During this period, iterative testing and refinement of search terms were performed to improve relevance and comprehensiveness. The final database search using the finalized keyword set was completed on October 9, 2023. The final database search was conducted by a single researcher using the finalized search strategy. Title and abstract screening, as well as full-text review, were performed independently by two researchers. Any discrepancies in study inclusion decisions were resolved through discussion and consensus.
We adopted a broad understanding of culture to capture the multifaceted influences on immigrant health. Only studies published in English or Korean in full-text were included. Exclusion criteria were: (1) studies without international migration experiences, and (2) non-original publications (e.g., editorials, letters). No restrictions were placed on study design; both qualitative and quantitative studies were included. A total of 5,236 papers were screened (based on titles and abstracts), and 85 were evaluated to determine their relevance to the research topic. Finally, 42 studies were included in the analysis.
2.2 Charting data
After selecting the final set of studies, the pertinent data addressing the research questions were extracted. Data charting was also conducted independently by two reviewers who extracted relevant information and cross-checked results, resolving any inconsistencies by agreement. The data charting approach used is illustrated in the flowchart shown in Figure 1. The extracted data, including factors, titles, target groups, health variables, and countries, are summarized in Table 1.
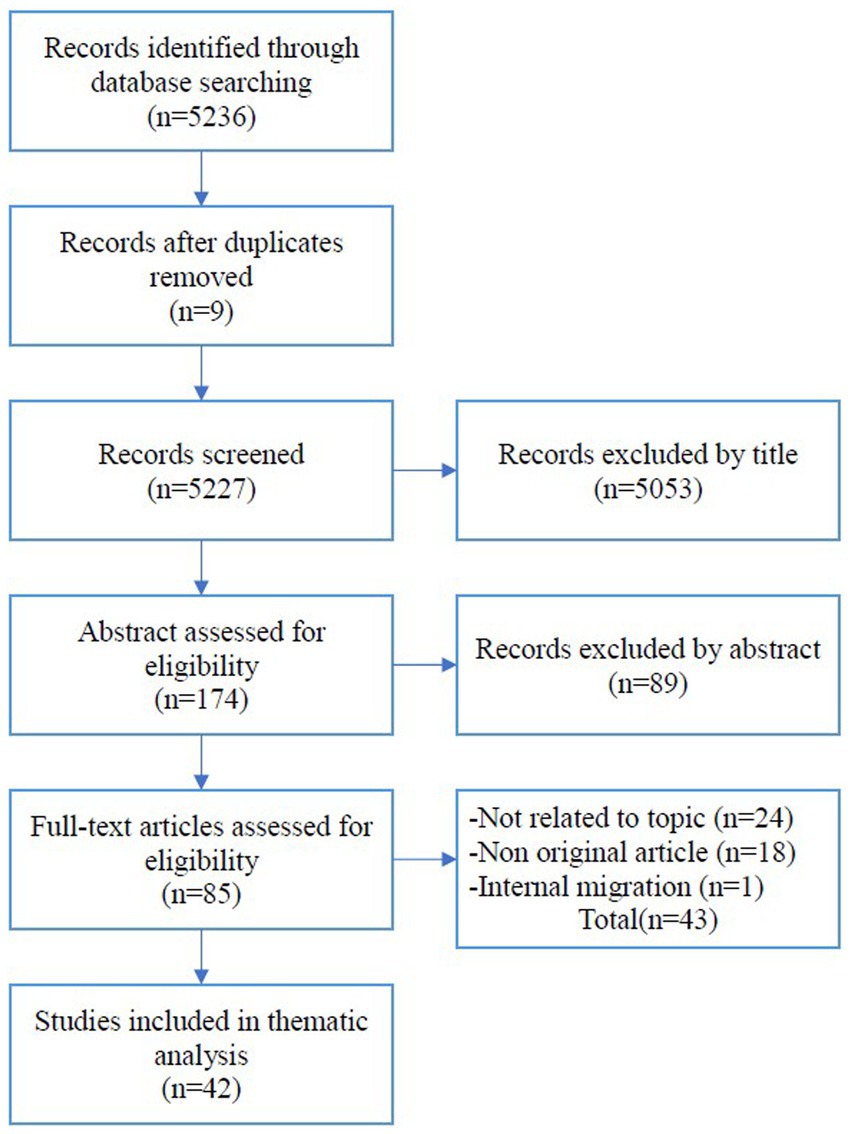
Figure 1. Strategy used for article selection.

Table 1. Analysis of selected articles.
3 Results
Through a scoping review, 42 studies were examined to identify cultural factors influencing immigrants’ health and were categorized using the Donabedian SPO model (9). The literature for this analysis is represented by year. Between 2010 and 2023, many studies emphasized cultural factors influencing the health of immigrants (Figure 2). The numbers of studies examining physical and mental health are shown in Figure 3. Of the 42 studies, 15 (50%) focused on physical health, 15 (40%) focused on mental health, and 12 (10%) focused on both. No studies have addressed the cultural factors that influence immigrants’ social health. Previous studies were conducted primarily in the United States of America [n = 25 (57.8%)], Canada [n = 5 (11.9%)], Australia [n = 4 (9.5%)], Norway [n = 2 (4.8%)], New Zealand [n = 1 (2.4%)], Taiwan [n = 1 (2.4%)], Thailand [n = 1 (2.4%)], Israel [n = 1 (2.4%)], the Netherlands [n = 1 (2.4%)], and South Korea [n = 1 (2.4%)].
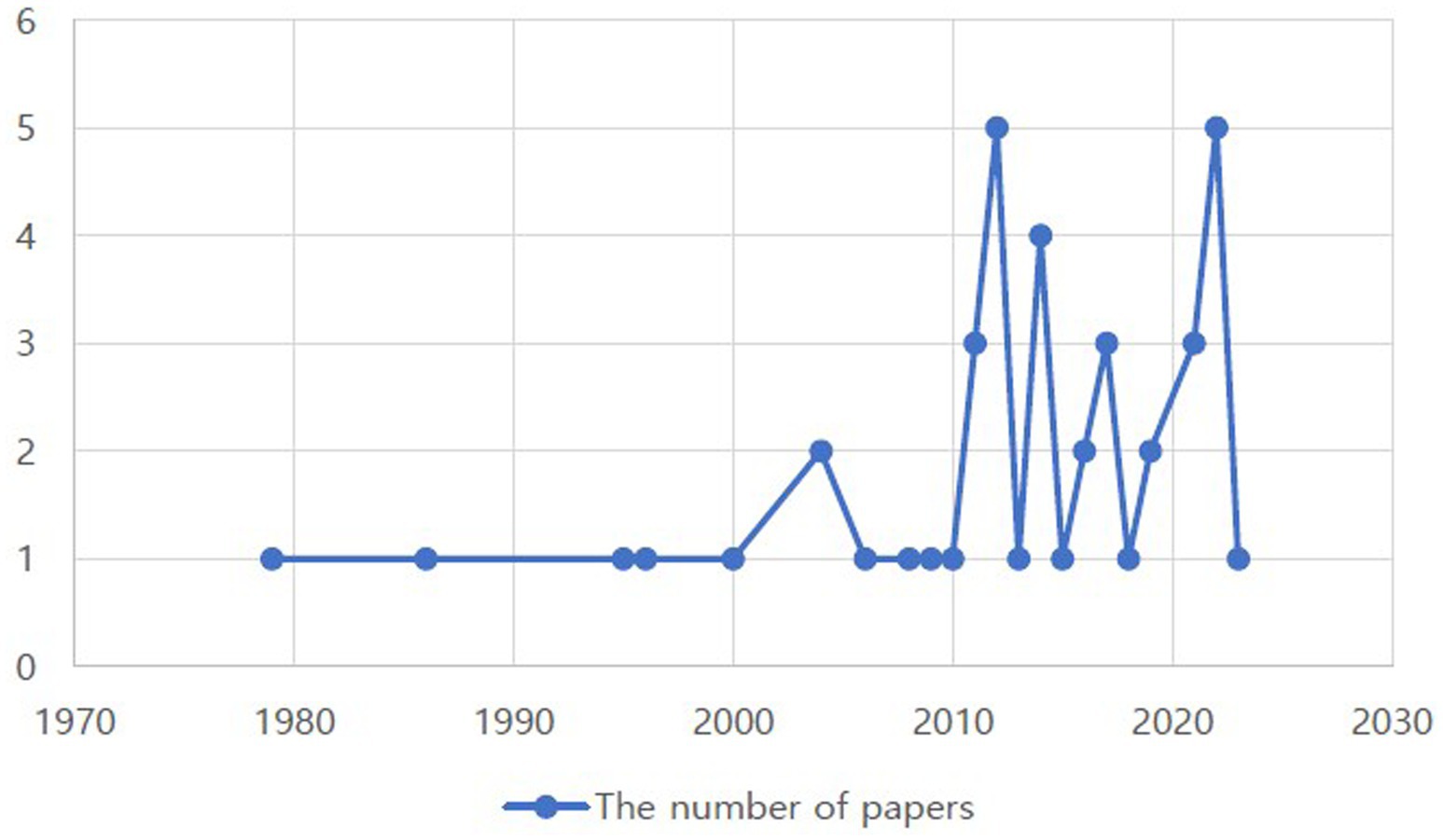
Figure 2. Distributions of papers regarding cultural factors influencing immigrants’ health.
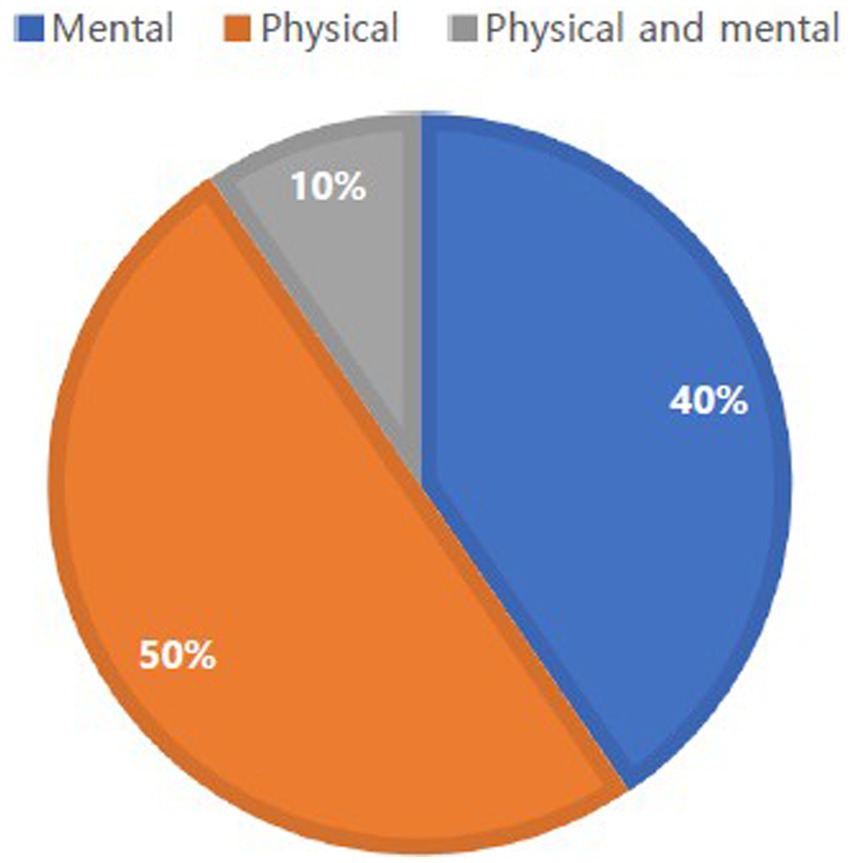
Figure 3. The number of papers investigating physical and mental health of immigrants.
3.1 Structural factors
Structural factors consisted of social (support systems and social discrimination) and personal factors (ethnicity, language barriers, cultural competence, and parents’ culturalism) that affected the inherent conditions of immigrants.
3.1.1 Support system
Social support is considered a significant factor in promoting immigrants’ mental health and participation in preventive health behaviors, especially for those affected by a lack of appropriate support (15) in their host society. According to Lubben (16), social support is an emotional and instrumental aid derived from interpersonal relationships. Familial and informal social networks of immigrants are often critical for obtaining the information, resources, and emotional support required to adapt to new environments. Social network support is associated with reduced levels of depressive symptoms in older Korean immigrants (17) and fewer mental health issues (18) among African immigrant youths (19). As an example of a social network, Trovato and Jarvis (20) demonstrated that immigrants with religious backgrounds have high levels of social integration, mitigating acculturative stress.
3.1.2 Social discrimination
Social discrimination affects the physical activity and mental health of immigrants. Discrimination has been described in various forms, ranging from microaggression to bullying and ignorance (19). Racist bullying–mostly menacing, insulting, and offending–has been identified as a stressful barrier to physical activity among South Asian immigrants in Australia (21). The experience of discrimination affects anxiety, depression (22), distress, and self-esteem among immigrants (23).
3.1.3 Ethnicity
Ethnicity influences mental health and risky health behaviors. Immigrant patients who rated their ethnicity or culture as important in the context of healthcare decision-making were significantly satisfied with the health guidance they received (24). Hispanic cultural values moderate trauma-health relationships exclusively for adults (25). Mexican American females with high levels of ethnic pride reported elevated levels of family support, which predicted lower levels of mental health issues (26). The authors highlighted ethnic pride as another important cultural factor that should be considered in research on ethnic minority populations (27). For instance, heritage practices and collectivist values are generally protective against health-risk behaviors (27). Chinese immigrants who maintain cultural beliefs about luck and fate were more likely to consume herbal remedies (28).
3.1.4 Language barriers
Language barriers are common challenges for effective healthcare, as reported by immigrants and healthcare providers. In a study investigating the negative experiences of healthcare in Sydney, Australia, immigrant patients with little or no understanding of English reported an inability to communicate effectively (29). Low levels of English proficiency are significantly associated with an increased risk of depression among older Chinese immigrant older adults in Arizona (30) and are more likely to die in hospital (31).
3.1.5 Cultural competence
Cultural competence affects immigrant health. Ethnic cultural competence is assumed to increase adaptation within one’s ethnic and cultural dimension (23). Additionally, cultural competence includes complex cognitive, affective, and behavioral processes, obtaining information about languages, motivational and attitudinal issues, and skills to utilize the acquired knowledge in an appropriate way and situation (32). Oppedal et al. (23) highlighted that ethnic and host competencies promote socio-cultural integration and mental health. Similarly, the construct of cultural consonance is defined as the “degree to which individuals approximate, in their own beliefs and behaviors, the prototypes of beliefs and behaviors encoded in cultural models” (33). Mexican immigrant females in Birmingham, Alabama, with low consonance are likely to be affected by diabetes (34).
3.1.6 Parents’ culturalism
Parenting cultural values and behaviors are related to various aspects of children’s mental health. Banerjee et al. (35) described South Asian immigrant parents’ cultural beliefs about childhood cancer as incurable, rare, unspeakable, and understood through religion, including practicing religious rituals and prayers, indicating the importance of healthcare providers in understanding immigrant parents’ culturalism. Parents’ cultural value of independence appears to be especially salient and negatively related to the behavioral problems associated with immigrant children (36). Baker et al. (37) reported that parents of Hmong origin in California perceived immunization as unimportant for their children, resulting in immunization inequality.
3.2 Process factors
The process factor was acculturation, which embraces emotional, behavioral, and affective aspects.
3.2.1 Acculturation
Acculturation has been described positively as a developmental process toward gaining competence within multiple sociocultural settings (23). Acculturation is also the degree to which an individual acquires new culture in terms of cultural behaviors, beliefs, and values (38). Acculturation is positively associated with the identification of mental disorders and negatively associated with personal stigma across generations of immigrants (39). Consedine et al. (40) focused on emotional acculturation because adapting to new cultural contexts requires massive and complete reconfiguration and recalibration of basic systems. In their study, female immigrants in the USA, who were emotionally different (less acculturated), reported significant somatic symptoms. Behavioral and affective acculturation are indirectly associated with depressive symptoms through perceived discrimination (41).
3.3 Outcome factors
Outcome factors included acculturative stress and ethnic identity crisis.
3.3.1 Acculturative stress
Acculturative stress is the physiological and psychological state of an individual caused by culture-specific stressors rooted in the acculturation process (42). Elevated levels of acculturative stress are significantly associated with high levels of C-reactive protein and soluble tumor necrosis factor receptor 2 in Chinese immigrant females (43). Mui and Kang (44) investigated older American and Asian populations in the US and Asia and reported that acculturative stress caused by older people’s perception of a cultural gap between themselves and their adult children was associated with high levels of depression. A study on Asian Americans in the US reported that acculturative stress was a significant predictor of mental health (45).
3.3.2 Ethnic identity crisis
Ethnic identity crises have been largely assessed among immigrant youth. During acculturation, individuals go through the process of developing their migrant youth identity. A significant ethnic identity crisis has been correlated with great distress and low self-esteem among immigrant youth in Norway (23). In Canada, the mental health of American immigrant youth is affected by their struggles with their identity (19).
4 Discussion
This study analyzed the cultural factors related to immigrants’ integrated health, encompassing physical, mental, and social aspects. Cultural factors were categorized and presented using Donabedian’s SPO model to provide a structured understanding of these factors.
First, social (social support and discrimination) and personal (ethnicity, language barriers, cultural competence, and parenting) factors were identified as structural factors. This finding is consistent with those of previous studies (46). Structural and social factors play important roles in immigrants’ health outcomes (17–19). Individual health resources such as health knowledge and self-efficacy have been associated with improved health outcomes in newly resettled refugee migrants, emphasizing the importance of support systems that buffer structural barriers to health (46). These similarities can be attributed to enhancing social support and addressing social discrimination to improve immigrants’ health and well-being. Social support can be obtained from inside (17) and outside of family (19). Religious involvement has been introduced as the largest source of social support (19). Therefore, in order to improve immigrants’ health outcomes, developing various religious activity program based on their religious needs should be considered as a strategy.
Other structural factors include ethnicity, language barriers, cultural competence and parental culture. Cultural competence and parental cultural orientation have been identified as personal factors among immigrants. Previous studies highlighted the importance of cultural competence as an essential skill for medical professionals, with training programs suggested to enhance this competency for physicians, nurses, and mental health professionals (47, 48). Relatively few studies have analyzed cultural competence in immigrant health. However, considering that immigrants with low levels of cultural competence are likely to suffer from diabetes (32), cultural competence has emerged as a crucial factor affecting their health. This highlights the need for future studies to explore strategies for enhancing cultural competence.
Acculturation is a key factor in this process. Research on the cultural adaptation of immigrants demonstrates that acculturation and enculturation are multidimensional and context-dependent cultural socialization processes, highlighting the intricate nature of cultural adaptation (49). Acculturation is regarded as a process factor in studies that does not specifically address immigrant health. Recent studies have demonstrated that acculturation can have ambivalent effects on the mental, physical, and cognitive health of immigrant populations (50, 51). Additionally, acculturation is closely linked to the experience of racism, which is a significant social determinant of immigrant health (52). That is, addressing acculturation pathways is important to mitigate the impact of racism on immigrants’ health. Acculturation manifests initially through behavioral changes (e.g., language use, diet), followed by changes in values or identity (49, 53). This sequential pattern suggests that lifestyle changes such as dietary life that occur in the early acculturation phase may have important implications for immigrant health. Thus, early intervention in the behavioral adaptation phase may have important policy implications for advancing health equity and shaping preventive health policies.
The outcome factors were acculturative stress and ethnic identity crisis. The negative effects of acculturation and acculturative stress, when not managed effectively, can result in adverse health consequences such as hypertension and obesity, particularly affecting Black and Hispanic immigrants (54). Mui and Kang (44) revealed that acculturative stress causes generational gaps between parents and children, indicating that stressors can originate from both intercultural and intrafamilial differences. Psychological strain is associated with adverse mental health outcomes and stress-related physical conditions, highlighting the need for culturally sensitive support systems and interventions (54, 55). Culturally tailored services such as family-based acculturation intervention have been reported to reduce acculturation stress and improve immigrants’ health outcomes (56). These findings support the need for policies that ensure access to culturally competent, family-focused health care for immigrants populations.
Although this study attempted to analyze the cultural factors that affect overall health, many studies have focused on physical and mental health. However, social health issues have not been addressed yet. Social health is defined as the adequate quantity and quality of relationships within a specific context to fulfill an individual’s need for meaningful human connections (57). Furthermore, social health plays a significant role in addressing health inequalities among marginalized groups and is essential for understanding population health concerns (57, 58). Given the pivotal role of social health, future research should prioritize the underexplored areas of immigrants’ social health. Addressing social health as an integral component of immigrant well-being can lead to more inclusive and equitable public health systems.
5 Limitations
This study was limited by the disproportionate number of studies written in English (41 out of 42), with only one study published in Korean. As a result, the findings may be less generalizable to non- English-speaking contexts. Cultural factors that affect immigrants’ health may differ in the early, middle, and late stages of settlement, or by era; however, this study could not distinguish between these gaps. Further studies are required to identify these gaps. Additionally, one notable limitation of this review lies in the search strategy, which primarily relied on terms such as “health,” “healthcare,” and “medical.” As a result, studies that conceptualize social health using alternative terms such as “well-being,” “social connection,” or “loneliness” may have been unintentionally excluded. Future reviews could consider including the keywords to more comprehensively capture the multidimensional nature of health, including its social components. Lastly, this study focused on cultural factors and did not include socioeconomic conditions, which may also influence immigrant health but fall outside the scope of our conceptual framework. Future research may benefit from exploring how cultural and socioeconomic factors interact to shape health outcomes in immigrant populations.
6 Conclusion
This scoping review underscores the critical role of cultural factors in shaping the health outcomes of immigrant populations. By applying Donabedian’s SPO model, this study revealed structural factors, such as social support, social discrimination, ethnicity, language barriers, cultural competence, and parenting, all of which significantly influence immigrant health. These findings are consistent with previous studies and highlight the critical role of structural factors in mitigating immigrants’ health problems. This study emphasizes the importance of fostering social support systems and addressing social discrimination to enhance immigrant populations’ overall well-being, thereby informing the development of culturally responsive policies and providing a robust evaluative framework grounded in the SPO model.
Additionally, this study identified acculturation as a crucial process factor and explored its complex relationship with health risks and racism. This study highlights the adverse health effects of acculturative stress and ethnic identity crises, and emphasizes the need for culturally sensitive support systems. Despite the extensive focus on physical and mental health, this study revealed a notable gap in the research on immigrants’ social health. Given the pivotal role of social health in mitigating health inequalities and enhancing the quality of life, future research should prioritize this area to develop comprehensive strategies that address the holistic health needs of immigrants. By expanding the scope of the research to include social health, policymakers and healthcare providers can reduce health disparities and promote equity of immigrant communities.
Author contributions
SC: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. EK: Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Soonchunhyang Research Fund (20231164).
Acknowledgments
We would like to thank the student assistants (Minah Baek, Gyeongchan Kim, Subin Jeong, Sunwoo Kang) for their help during data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Park, HR. 2.51 million foreigners in Korea. Entering a multicultural society in sight. South Korea: Korean Culture and Information Service (2024). Available online at: https://www.kocis.go.kr/koreanet/view.do?seq=1047344 (Accessed May 15, 2024).
2. Interactive World Migration Report. Chapter 2 - migration and migrants: a global overview. International Organization for Migration (2025). Available online at: https://publications.iom.int/books/world-migration-report-2024-chapter-2 (Accessed January 7, 2025).
3. Hus, N.. (2022). Unknown immigrants in Nordic countries. Nordic cooperation. Available online at: https://www.norden.org/en/statistics/immigrants-nordic-countries-0 (Accessed November 14, 2023).
4. World Health Organization. Preamble to the constitution of the World Health Organization as adopted by the international health conference, vol. 2. New York: Official Records of the World Health Organization (1946). 100 p.
5. Derose, KP, Escarce, JJ, and Lurie, N. Immigrants and health care: sources of vulnerability. Health Aff. (2007) 26:1258–68. doi: 10.1377/hlthaff.26.5.1258
6. Woodgate, RL, Busolo, DS, Crockett, M, Dean, RA, Amaladas, MR, and Plourde, PJ. A qualitative study on African immigrant and refugee families’ experiences of accessing primary health care services in Manitoba, Canada: it’s not easy! Int J Equity Health. (2017) 16:5. doi: 10.1186/s12939-016-0510-x
7. Qiu, Y, Meng, G, and Wei, Y. Factors influencing immigrants’ satisfaction in Danjiangkou reservoir based on logistic regression model. Water Policy. (2016) 18:1384–98. doi: 10.2166/wp.2016.255
8. Bacong, A, and Sohn, H. Disentangling contributions of demographic, family, and socioeconomic factors on associations of immigration status and health in the United States. J Epidemiol Community Health. (2020) 75:214245. doi: 10.1136/jech-2020-214245
9. Donabedian, A. The quality of care. How can it be assessed? JAMA. (1988) 260:1743–8. doi: 10.1001/jama.1988.03410120089033
10. Kroeber, AL, and Kluckhohn, C. Culture: A critical review of concepts and definitions. Cambridge (MA): Harvard University Press (1952).
11. Betancourt, H, and López, SR. The study of culture, ethnicity, and race in American psychology. Am Psychol. (1993) 48:629–37. doi: 10.1037/0003-066X.48.6.629
12. Karl, JA, and Fischer, R. More than yes and no: predicting the magnitude of non-invariance between countries from systematic features. In: Klicperova-Baker, M, and Friedlmeier, W. Xenophobia vs. patriotism: Where is my home? Proceedings from the 25th congress of the International Association for Cross-Cultural Psychology 2022. Michigan: Grand Valley State University (2022).
13. Arksey, H, and O’Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
14. Levac, D, Colquhoun, H, and O’Brien, KK. Scoping studies: advancing the methodology. Implement Sci. (2010) 5:1–9. doi: 10.1186/1748-5908-5-69
15. Bliatout, B, Ben, R, Do, VT, Keopraseuth, KO, Bliatout, HY, and Lee, DTT. Mental health and prevention activities targeted to southeast Asian refugees. In T. C. Owan (Ed.), Southeast Asian mental health: Treatment, prevention, services, training, and research. Rockville, MD: National Institute of Mental Health (1985) 183–207.
16. Lubben, JE. Assessing social networks among elderly populations. Fam Community Health. (1988) 11:42–52. doi: 10.1097/00003727-198811000-00008
17. Kim, BJ, Sangalang, CC, and Kihl, T. Effects of acculturation and social network support on depression among elderly Korean immigrants. Aging Ment Health. (2012) 16:787–94. doi: 10.1080/13607863.2012.660622
18. Khanlou, N, Bender, A, Mill, C, Vazquez, LM, and Rojas, L. Youth experiences of cultural identity and migration: a systems perspective In: S Pashang, N Khanlou, and J Clarke, editors. Today’s youth and mental health: Hope, power, and resilience. Advances in mental health and addiction. New York: Springer (2018). 57–76.
19. Olawo, O, Pilkington, B, and Khanlou, N. Identity-related factors affecting the mental health of African immigrant youth living in Canada. Int J Ment Health Addict. (2021) 19:701–13. doi: 10.1007/s11469-019-00177-z
20. Trovato, F, and Jarvis, GK. Immigrant suicide in Canada: 1971 and 1981. Soc Forces. (1986) 65:433–57. doi: 10.2307/2578681
21. Nisar, M, Khan, A, and Kolbe-Alexander, TL. “Cost, culture and circumstances”: barriers and enablers of health behaviours in south Asian immigrants of Australia. Health Soc Care Community. (2022) 30:e3138–49. doi: 10.1111/hsc.13759
22. Pernice, R, and Brook, J. Refugees’ and immigrants’ mental health: association of demographic and post-immigration factors. J Soc Psychol. (1996) 136:511–9. doi: 10.1080/00224545.1996.9714033
23. Oppedal, B, Røysamb, E, and Sam, DL. The effect of acculturation and social support on change in mental health among young immigrants. Int J Behav Dev. (2004) 28:481–94. doi: 10.1080/01650250444000126
24. Schutt, RK, and Mejía, C. Health care satisfaction: effects of immigration, acculturation, language. J Immigr Minor Health. (2017) 19:1372–8. doi: 10.1007/s10903-016-0409-z
25. Mercado, A, Venta, A, Henderson, C, and Pimentel, N. Trauma and cultural values in the health of recently immigrated families. J Health Psychol. (2021) 26:728–40. doi: 10.1177/1359105319842935
26. Dinh, KT, Castro, FG, Tein, JY, and Kim, SY. Cultural predictors of physical and mental health status among Mexican American women: a mediation model. Am J Community Psychol. (2009) 43:35–48. doi: 10.1007/s10464-008-9221-9
27. Schwartz, SJ, Weisskirch, RS, Zamboanga, BL, Castillo, LG, Ham, LS, Huynh, QL, et al. Dimensions of acculturation: associations with health risk behaviours among college students from immigrant families. J Couns Psychol. (2011) 58:27–41. doi: 10.1037/a0021356
28. Chun, KM, and Chesla, CA. Cultural issues in disease management for Chinese Americans with type 2 diabetes. Psychol Health. (2004) 19:767–85.doi: 10.1080/08870440410001722958
29. Garrett, PW, Dickson, HG, Young, L, and Whelan, AK. “The happy migrant effect”: perceptions of negative experiences of healthcare by patients with little or no English: a qualitative study across seven language groups. Qual Saf Health Care. (2008) 17:101–3. doi: 10.1136/qshc.2007.022426
30. Kang, SY, Boyas, J, and Salehin, M. Correlates of depression among Chinese immigrant elders in Arizona: the role of acculturative stress and social support. J Hum Behav Soc Environ. (2012) 22:334–50. doi: 10.1080/10911359.2012.655609
31. Basic, D, Shanley, C, and Gonzales, R. The impact of being a migrant from a non-English-speaking country on healthcare outcomes in frail older inpatients: an Australian study. J Cross Cult Gerontol. (2017) 32:447–60. doi: 10.1007/s10823-017-9333-5
32. Kim, YY. Facilitating immigrant adaptation: ethnic support systems In: TL Albrecht and M Adelman, editors. Communicating social support. Newbury Park: Sage Publications (1987). 192–211.
33. Dressler, WW. Culture and the individual: Theory and method of cultural consonance. London: Routledge (2017).
34. Andrews, C, Oths, KS, and Dressler, WW. Time in the United States and diabetes among Mexican immigrant women: the moderating role of culture. J Migr Health. (2022) 6:100118. doi: 10.1016/j.jmh.2022.100118
35. Banerjee, AT, Watt, L, Gulati, S, Sung, L, Dix, D, Klassen, R, et al. Cultural beliefs and coping strategies related to childhood cancer: the perceptions of south Asian immigrant parents in Canada. J Pediatr Oncol Nurs. (2011) 28:169–78. doi: 10.1177/1043454211408106
36. Huang, KY, Calzada, E, Cheng, S, Barajas-Gonzalez, RG, and Brotman, LM. Cultural adaptation, parenting and child mental health among English-speaking Asian American immigrant families. Child Psychiatry Hum Dev. (2017) 48:572–83. doi: 10.1007/s10578-016-0683-y
37. Baker, DL, Dang, MT, Ly, MY, and Diaz, R. Perception of barriers to immunization among parents of Hmong origin in California. Am J Public Health. (2010) 100:839–45. doi: 10.2105/AJPH.2009.175935
38. Williams, CL, and Berry, JW. Primary prevention of acculturative stress among refugees. Application of psychological theory and practice. Am Psychol. (1991) 46:632–41. doi: 10.1037/0003-066X.46.6.632
39. Knaifel, E, Youngmann, R, and Neter, E. Immigrant generation, acculturation, and mental health literacy among former Soviet Union immigrants in Israel. Int J Soc Psychiatry. (2023) 69:724–34. doi: 10.1177/00207640221134236
40. Consedine, NS, Chentsova-Dutton, YE, and Krivoshekova, YS. Emotional acculturation predicts better somatic health: experiential and expressive acculturation among immigrant women from four ethnic groups. J Soc Clin Psychol. (2014) 33:867–89. doi: 10.1521/jscp.2014.33.10.867
41. Cano, MÁ, de Dios, MA, Castro, Y, Vaughan, EL, Castillo, LG, Lorenzo-Blanco, EI, et al. Alcohol use severity and depressive symptoms among late adolescent Hispanics: testing associations of acculturation and enculturation in a bicultural transaction model. Addict Behav. (2015) 49:78–82. doi: 10.1016/j.addbeh.2015.06.002
42. Berry, JW, Kim, U, Minde, T, and Mok, D. Comparative studies of acculturative stress. Int Migr Rev. (1987) 21:491–511. doi: 10.1177/019791838702100303
43. Fang, CY, Ross, EA, Pathak, HB, Godwin, AK, and Tseng, M. Acculturative stress and inflammation among Chinese immigrant women. Psychosom Med. (2014) 76:320–6. doi: 10.1097/PSY.0000000000000065
44. Mui, AC, and Kang, SY. Acculturation stress and depression among Asian immigrant elders. Soc Work. (2006) 51:243–55. doi: 10.1093/sw/51.3.243
45. Miller, MJ, Yang, M, Farrell, JA, and Lin, LL. Racial and cultural factors affecting the mental health of Asian Americans. Am J Orthopsychiatry. (2011) 81:489–97. doi: 10.1111/j.1939-0025.2011.01118.x
46. Al-Adhami, M, Berglund, E, Wångdahl, J, and Salari, R. A cross-sectional study of health and well-being among newly settled refugee migrants in Sweden—the role of health literacy, social support, and self-efficacy. PLoS One. (2022) 17:e0279397. doi: 10.1371/journal.pone.0279397
47. Ogundu, C. Cultural competence training program for African immigrants. Unpublished manuscript. Chidinma Ogundu papers. Henderson, NV: Touro University Nevada Archives (2021).
48. Zartaloudi, A. Cultural competence of mental health professionals. Eur Psychiatry. (2022) 65:S547–8. doi: 10.1192/j.eurpsy.2022.1402
49. Yoon, E, Cabirou, L, Galvin, S, Hill, L, Daskalova, P, Bhang, C, et al. A meta-analysis of acculturation and enculturation: bilinear, multidimensional, and context-dependent processes. Couns Psychol. (2020) 48:342–76. doi: 10.1177/0011000019898583
50. Jiang, Y, Tang, F, and Wu, B. Impacts of acculturation on the health of US older Chinese immigrants. Innov Aging. (2023) 7:148. doi: 10.1093/geroni/igad104.0485
51. Ryu, S, Morey, BN, Shi, Y, and Lee, S. Acculturation and self-rated health among Chinese and Korean immigrants aged 49 to 75. Front Public Health. (2023) 11:1272428. doi: 10.3389/fpubh.2023.1272428
52. Naidu, J, Paolucci, EO, and Turin, TC. Racism as a social determinant of health for newcomers towards disrupting the acculturation process. Soc. (2022) 13:2. doi: 10.3390/soc13010002
53. Miller, MJ, Yang, M, Lim, RH, Hui, K, Choi, N, Fan, X, et al. A test of the domain-specific acculturation strategy hypothesis. Cult Divers Ethnic Minor Psychol. (2013) 19:1–12. doi: 10.1037/a0030499
54. Cokley, K, McClain, S, Enciso, A, and Martinez, M. An examination of the impact of minority status stress and impostor feelings on the mental health of diverse ethnic minority college students. J Multicult Couns Dev. (2013) 41:82–95. doi: 10.1002/j.2161-1912.2013.00029.x
55. Salas-Wright, CP, Pérez-Gómez, A, Maldonado-Molina, MM, Mejia-Trujillo, J, García, MF, Bates, MM, et al. Cultural stress and mental health among Venezuelan migrants: cross-national evidence from 2017 to 2024. Soc Psychiatry Psychiatr Epidemiol. (2024). doi: 10.1007/s00127-024-02796-x
56. Estrada, Y, Lee, TK, and Prado, G. (2025). SER familia: a family-based intervention addressing syndemic health conditions by decreasing acculturative stress and promoting resilience. NIH Reporter. Available online at: https://reporter.nih.gov/project-details/11142466 (Accessed May 19, 2025).
57. Doyle, DM, and Link, BG. On social health: history, conceptualization, and population patterning. Health Psychol Rev. (2024) 18:619–48. doi: 10.1080/17437199.2024.2314506
Keywords: immigrants, health equity, cultural factors, Donabedian model, public health
Citation: Choi S and Kang E (2025) Cultural factors related to immigrants’ health: a scoping review. Front. Public Health. 13:1606772. doi: 10.3389/fpubh.2025.1606772
Edited by:
Mireia Faus, University of Valencia, SpainReviewed by:
Karen Lau, St George’s University of London, United KingdomKazuo Araki, Kyoto University, Japan
Copyright © 2025 Choi and Kang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eunjeong Kang, bWFyY2hlajcyQHNjaC5hYy5rcg==