 Andrew McNeely1
Andrew McNeely1 Alexandra MacMillan Uribe1Gabrielli T. De Mello1Andres Herrero-Loza2Mahak Ali3Kaitlyn Nguyen4
Alexandra MacMillan Uribe1Gabrielli T. De Mello1Andres Herrero-Loza2Mahak Ali3Kaitlyn Nguyen4 Yetunde Olawuyi5
Yetunde Olawuyi5 Chad D. Rethorst1
Chad D. Rethorst1 Rebecca A. Seguin-Fowler1
Rebecca A. Seguin-Fowler1 Jacob Szeszulski1*
Jacob Szeszulski1*- 1Institute for Advancing Health through Agriculture, Texas A&M AgriLife Research, Dallas, TX, United States
- 2Department of Biomedical Sciences, Texas A&M University, College Station, TX, United States
- 3Department of Economics, Texas A&M University, College Station, TX, United States
- 4Department of Nutrition, Texas A&M University, College Station, TX, United States
- 5Institute for Advancing Health through Agriculture, Prairie View A&M University, Prairie View, TX, United States
Introduction: Strong Teens for Healthy Schools (STHS) is a middle school program that focuses on improving healthy eating habits, physical activity, and engages students in civic engagement projects to promote healthy environments within schools. As a novel approach to school-based health interventions, this program faces numerous intervention implementation challenges.
Methods: To assess potential barriers and facilitators to implementing STHS, interviews with Texas Cooperative Extension staff (n = 20) and middle school staff (n = 15) were conducted prior to implementing the program to inform program delivery. Participants (89% female, 71% white, mean age 41 ± 9.2 years old) reviewed sections of the curriculum and provided feedback in semi-structured interviews. Open inductive coding, followed by deductive categorization of codes within the Consolidated Framework for Implementation Research framework, grouped responses into themes.
Results: Themes found in the response were: (1) Trainings should emphasize using STHS in a structured setting and highlight the core components of the curriculum to ensure consistent delivery. (2) Variations in capabilities may affect how information is delivered by implementers, as well as how it is received by students. (3) Participants discussed how the physical infrastructure required for STHS could be a challenge in some school contexts. (4) The STHS curriculum received positive feedback for its design, relative advantage compared to other curricula, and evidence-base. (5) Local partners' attitudes and conditions may affect the adoption and implementation of STHS.
Discussion: Overall, participants supported implementation of the STHS but noted several potential challenges that could be addressed prior to implementation.
Introduction
There is strong evidence for the many benefits of children engaging in physical activity (PA) and developing healthy eating habits, including reduced risks of depression, anxiety, cancer, type 2 diabetes, obesity, and cardiovascular disease (1–3). However, most American youth do not meet PA recommendations, and most school-aged students do not consume enough fruits and vegetables to meet the dietary guidelines (4–6). The discrepancy between PA and healthy eating recommendations and the reality of children's lack of engagement in these behaviors supports the ongoing need for interventions that promote behavior change. Schools are an important setting for promoting health, given their ability to reach many children, regardless of ethnicity, background, or gender. They also provide an opportunity for continuous, intensive interventions over long periods of time (7, 8). Children spend a large proportion of their time in schools—over 6 h per day for nearly 180 days per year (7–9). Additionally, school programs have demonstrated effectiveness in increasing PA (10, 11), positively affecting the consumption of vegetables, fruits, sugar sweetened drinks, and fast food (12–14) and promoting positive youth development among youth (15). However, when developing a novel program for the school setting it is important to understand potential program specific barriers that may promote or impede delivery (e.g., adoption, implementation, sustainment) (16–18).
School-based PA, healthy eating, and positive youth development programs face critical challenges to implementation (19). Several reviews found that some of the most prevalent barriers to program implementation include staff beliefs that conflict with the program's aim (e.g., underlying value of the intervention or program), lack of access to necessary resources, lack of access to necessary resources, supportive leadership, staff buy-in, and understanding of the program's principles and purpose, as well as other specific school characteristics (e.g., school size, high school vs. elementary school) (20, 21). Another study that examined school-based interventions found that ‘inner contextual factors' (i.e., factors within the school) were predominately related to sustainability, including availability of facilities or equipment, continued executive or leadership support, and implementation team cohesion (22). Furthermore, these results are supported by numerous other studies that identify additional barriers to various aspects of implementing school-based interventions, including managing students, inadequate resources, and a lack of time, knowledge, skills, competence, and training (22–24). Conversely, access to resources to support implementation, presence of effective and supportive leadership, access to ongoing training, effective communication about the purpose and outcomes of the program, teacher support, good training, and technical assistance can all facilitate the delivery of school-based programs (20, 22, 25).
Strong Teens for Healthy Schools (STHS) is a middle school program that was adapted from an adult civic engagement and health behavior program, the Change Club, which was created to empower people to take an active role in creating healthier eating and PA environments in their community (26). The STHS curriculum, which uses the theory of planned behavior (27–29), the socioecological model (30–32), and the whole school, whole community, whole child (WSCC) model (33, 34) to address PA, healthy eating habits, and positive youth development, is comprised of 16 one hour sessions, with half devoted to civic engagement skills and half alternating between PA and nutrition topics. One novel component of the curriculum is the student-led project to promote healthy environments within schools. Creating a health-focused change to the built environment through civic engagement is an evidence-based method that has been implemented in both rural and urban communities (35–38). These programs have demonstrated success in facilitating environmental change (39, 40) and have been integrated successfully into evidence-based, multilevel interventions as well (38). STHS adapts its civic engagement curriculum from these prior iterations to target adolescent cardiometabolic health in the school environment. STHS is also aligned with the Texas Essential Knowledge and Skills (TEKS) (41)—curriculum standards set by the state board of education—to help improve adoption of the program in Texas schools.
Achieving behavioral changes and promoting health benefits in educational settings requires a comprehensive understanding of factors that may impede or support the delivery of effective programs within school settings (22). Given the novelty of this approach in a school setting, understanding potential barriers and facilitators to its implementation in schools is essential to informing the development of implementation strategies that can enhance the delivery and sustainment of programs over time (22, 42). The Consolidated Framework for Implementation Research (CFIR) (43) is a conceptual model that divides the implementation of a given program into five domains (Figure 1)—the innovation (i.e., the program being implemented); the individuals involved with delivering the innovation, including implementers, leadership, support staff, administrators, recipients, etc.; the inner setting where the innovation is implemented; the outer setting, which includes the surrounding community and context beyond of the inner setting; and the process (i.e., how implementation occurs). Given the complex, multi-level nature of STHS, CFIR provides the most comprehensive understanding of factors that may affect program delivery throughout all phases of implementation (adoption, implementation, and sustainment), whereas many other models are more limited in their focus. Additionally, CFIR has been previously used to help identify and categorize barriers and facilitators to the implementation of other programs in the school setting (44–47) and has successfully helped to generate implementation of other programs and generate implementation strategies that aim to improve program delivery (48).
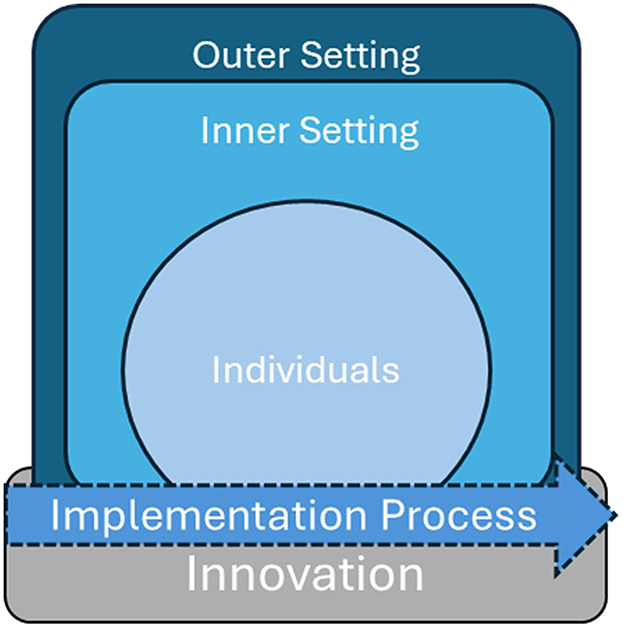
Figure 1. Adapted from the consolidated framework for implementation research (CFIR).
Overall, school-based interventions to promote health face a number of implementation challenges that can adversely impact the outcomes of such programs (20, 22, 24), but frameworks such as CFIR allow implementers to anticipate and adapt their interventions to overcome barriers (44, 45). However, STHS uses a novel civic engagement approach to school-based health and poses challenges to implementation in the school setting. Therefore, this study investigated the perceived barriers and facilitators to implementing STHS from the perspective of Texas Cooperative Extension staff (i.e., health educators) and middle school staff before it was delivered in schools to inform program delivery.
Methods
Overview of setting
The state of Texas school system encompasses more than 9,000 campuses, including 1,475 middle-schools (32). Students in middle-schools comprise about 18% of the total number of enrolled students in Texas schools, and are typically between the ages of 11 and 13 years old. In addition to resources and education about health provided directly by the school, external organizations and agencies can be utilized to implement beneficial programs. In the United States, Cooperative Extension is a nationwide, educational network, operating through land-grant universities in partnership with federal, state, and local governments, that translates research into practical knowledge and action to address public needs. In Texas, this system is collectively referred to as AgriLife Extension, and has a presence in all 254 counties of the state (33). Extension personnel include agents who provide a range of programs and services to the public, and 4H staff that specialize in delivering youth development programs to schools.
Design
Qualitative interviews were conducted to assess barriers and facilitators to the implementation of STHS. Interview questions were based on CFIR domains. Questions prompted participants for feedback about the innovation (e.g., benefits and drawbacks to the STHS program), its delivery (e.g., usefulness of the materials in aiding instruction), as well as factors that could affect implementation of the STHS program (e.g., perceptions of school leadership support, physical design of the school). Participants were provided with a high-level overview of the STHS program and assigned two (out of 16 total) lessons of STHS to review. Lessons to be reviewed were assigned sequentially (i.e., the first participant received lessons one and two). Participants reviewed their assigned lessons using digital copies of the curriculum and were provided with an evaluation sheet to document their impressions and prompt discussion during the interview. Participants were asked to complete their review within 1 week of assignment but were given additional time if needed. Upon finishing their self-paced review, participants completed a demographic survey assessing gender, race/ethnicity, and years of experience in respective roles (i.e., extension/schools), and scheduled a time to complete a 45-min semi-structured interview with a research team member. This study was approved by the institutional review board at Texas A&M (IRB2022-1159D).
Recruitment
The research team recruited potential implementers of STHS using a multi-pronged approach beginning with Texas Cooperative Extension staff members (48). Staff members of the Texas AgriLife Extension system (hereafter, Extension staff) that were recruited for this study include county extension agents and 4H staff members, which were identified using AgriLife extension website and word of mouth referral.
Educators were recruited by sending informational emails to contact email addresses on Texas school websites. Convenience sampling was also used to recruit educators directly at school health conference. For both Extension staff and educators, snowball sampling was used, in which participants could share research team contact information with their colleagues who may have been interested in participating in the study. Inclusion criteria for educators were adults (≥18 years old) with any number of years of education experience in a Texas public or private middle school settings (past or present). Participants were provided with an electronic copy of the study information and informed consent information sheet. They provided verbal consent to the researcher prior to beginning the interview. Participants were compensated for their time with a $50 Amazon gift card.
Data collection
Interviews were conducted online (Microsoft Teams version 25) and recorded by AMU and JS. Audio recordings of the interviews were uploaded to a secure web-based transcription service (NVivo Transcription 2024, Lumivero LLC). Transcript files were cleaned and reviewed for accuracy against the audio recording by a research team member. Final transcripts were then uploaded to qualitative analysis software (ATLAS.ti 25), and copies of the project were shared with coding team members.
Analysis
All data analysis was led by the first author (AM). Analysis team members (AH-L, MA, KN, GTDM) met with the team leader as well as principal investigators (JS, AMU) regularly to discuss progress and findings. Coding proceeded in three stages. In the first stage, members of the analysis team performed open coding on the transcripts to capture a priori ideas and patterns. Second, the same team members applied axial coding to the analysis to sort and refine codes into conceptual content areas (49). The analysis team then engaged in focused, deductive coding, applying the CFIR domain and subdomains to the codes established in the first two rounds of coding. An additional round of line-by-line focused coding for CFIR concepts was performed to ensure all data was accounted for in the analysis. Coded transcript excerpts, categorized by CFIR domain and subdomain, were then reviewed by the analysis team members and the principal investigators, and final analytic themes were developed, reviewed, and approved for each CFIR domain by all team members. Demographic surveys were collected via Qualtrics (Qualtrics, LLC 2024), and exported for analysis in Microsoft Excel (Version 2403).
The use of inductive and deductive methods in the analysis also influenced the method of determining an appropriate cessation of data analysis, also known as saturation in qualitative studies. Following the analysis model, inductive thematic saturation (50), in which no new codes or themes could be derived from the data, was first established. Then, this coding was organized under CFIR domains and subdomains until all data had been accounted for in this framework, achieving a form of a priori thematic saturation (50). As expected, inductively derived codes sometimes crossed into multiple CFIR domains and could not be easily organized into these deductive categories. In these cases, the analysis team lead (AM) and the principal investigators (JS and ALMU) discussed the relevant topics and quotations, and made decisions for categorization on a case by case basis.
Research team characteristics
The research team represents a professionally and individually diverse group. This study was led by faculty members with Texas A&M Institute for Advancing Health through Agriculture (IHA) JS, AMU, CDR, and RAS-F. At the time of interviews, analysis, and writing, AM, GTDM, and YO were postdoctoral researchers with IHA, and AH-L, MA, and KN were undergraduate student researchers at Texas A&M University. All faculty and postdoctoral researchers have had professional experience and a current research agenda in community health, and training and professional experience in qualitative research methods; student researchers were trained in qualitative research methods by AM.
Results
Extension staff (n = 20) and school staff members (n = 15) completed qualitative interviews between March of 2023 and March of 2024. Most participants were female, non-Hispanic White, with 6 or more years of experience in their respective roles (Table 1). The average age of participants was 41 years old (standard deviation ± 9.2 years). The interviews lasted an average of 33 min (rounded to nearest minute), with a standard deviation of ±11 min. The shortest interview was 16 min, and the longest interview was 59 min.
Implementation process theme—Trainings should emphasize using STHS in a structured setting and highlight the core components of the curriculum to ensure consistent delivery.
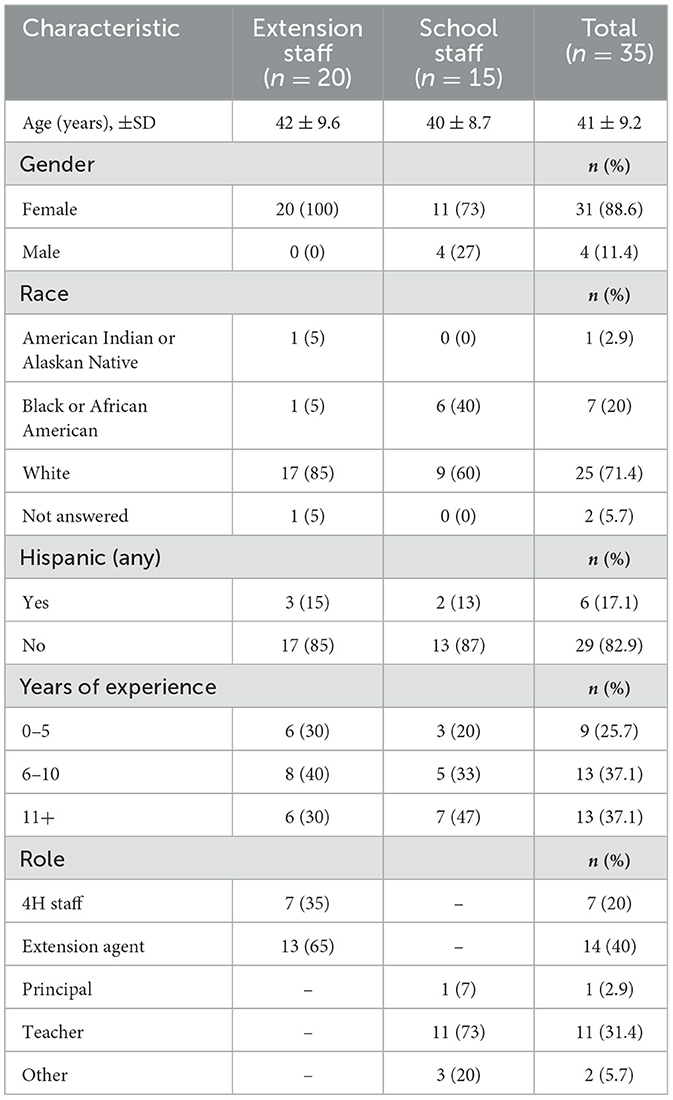
Table 1. Demographic characteristics of interview participants (n = 35).
Although STHS is designed to be deliverable either by school staff members or by extension agents, participants emphasized the necessity of training the implementer on the program components, particularly its most critical components, to ensure fidelity. These comments were often made in reference to implementer time constraints and their need for clear expectations about their role (Table 2, Quote 1); implementers balancing multiple demands on their time may inadvertently skip important pieces of the curriculum if they are not emphasized in training. Aside from training, however, participants noted that the curriculum itself was appealing in that it would require very little expert knowledge or preparation time, thereby promoting its consistent use by implementers (Table 2, Quote 2).
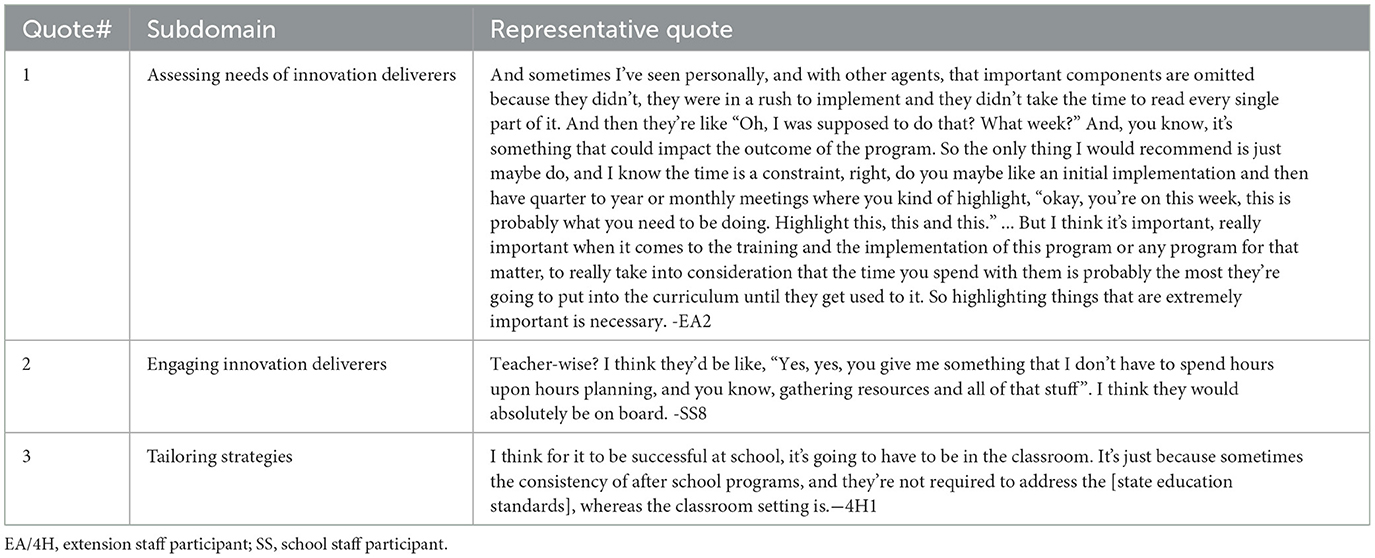
Table 2. Implementation process theme—trainings should emphasize using STHS in a structured setting and highlight the core components of the curriculum to ensure consistent delivery.
In regard to fitting STHS into the school's programming, participants noted that although after school programs can be beneficial for students, after-school programs lacked consistency in terms of delivery (e.g., student might not attend every day) and educational standards (e.g., after school programs may not align with the same educational standards required in the classroom) that participants believed would be necessary to successfully implement STHS (Table 2, Quote 3). According to the participants, implementing STHS inside a classroom setting, such as an elective or part of physical education or health courses, would be more suitable for consistency of delivery.
Individuals theme—Variations in capabilities may affect how information is delivered by implementers, as well as how it is received by students.
For the implementers of the program, interview participants generally affirmed that the STHS curriculum itself was easy to understand and could be adequately delivered by teachers of any experience level. Some participants noted that the educator's level of experience, however, could influence delivery in subtle ways that, while not hindering adequate delivery, might result in varied experiences and engagement. Veteran teachers may be better equipped through training and experience to manage the pace of the sessions to fit allotted times, where novice teachers may struggle with ensuring all content was covered in the same amount of time. Participants also mentioned that in classes with shorter sessions, experienced teachers would know how to add supplemental material to fill out the time, whereas new teachers may be left with gaps in their schedule (Table 3, Quote 1). It was also noted that Extension staff may struggle with the timing more than schoolteachers, as their experiences with program delivery do not always involve middle-school education settings, and thus they may need more guidance on classroom management (Table 3, Quote 2).
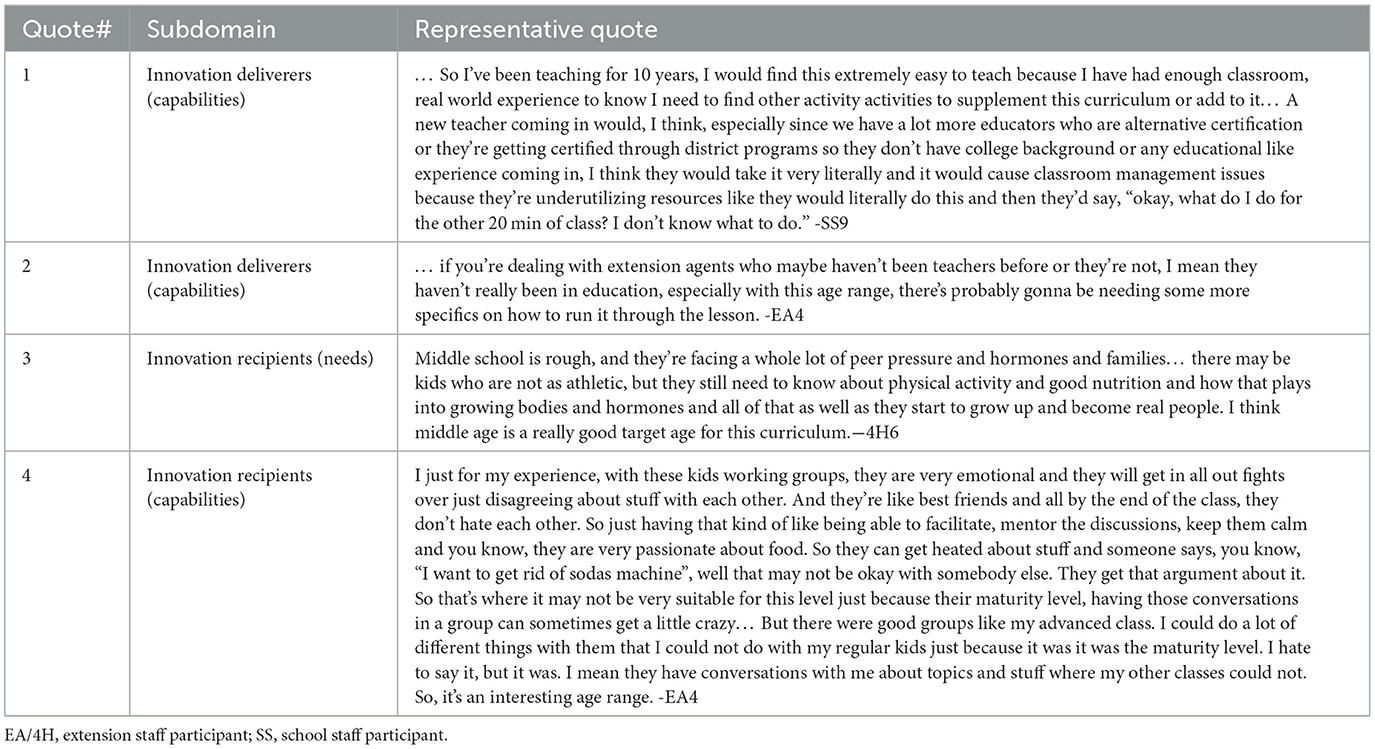
Table 3. Individuals theme—variations in capabilities may affect how information is delivered by implementers, as well as how it is received by students.
Participants viewed STHS as a source of critical information and skills for middle-school students. Specifically, the connection between nutrition, PA, and mental health, particularly during this critical developmental age, was a topic from which participants thought many students would benefit (Table 3, Quote 3). Participants also discussed the civic engagement components of STHS as a needed skill for this age group, asserting that such material could be helpful in identity formation for middle school students as they progress through adolescence. On the other hand, aspects of the developmental stage of these years could create an added challenge for engaging middle school students in the curriculum. For example, the wide range of maturity levels among potential students could make it difficult to present the material or expect students to engage appropriately (Table 3, Quote 4).
Inner setting theme—Participants discussed how the physical infrastructure required for STHS could be a challenge is some school contexts.
Structural characteristics regarding the layout and facilities of the school were mentioned primarily by school staff participants as being important for the implementation of STHS. In most cases, school staff had no concerns about accommodating the program's physical activities. In some cases, however, implementers who described their school settings as smaller and/or in rural areas, noted that interior space was often multi-purpose, such as gyms combined with cafeterias, which might limit their ability to use those spaces. However, these schools often had abundant outdoors space, which participants noted as a possibility for supplementing the program's space requirements (Table 4, Quote 1).
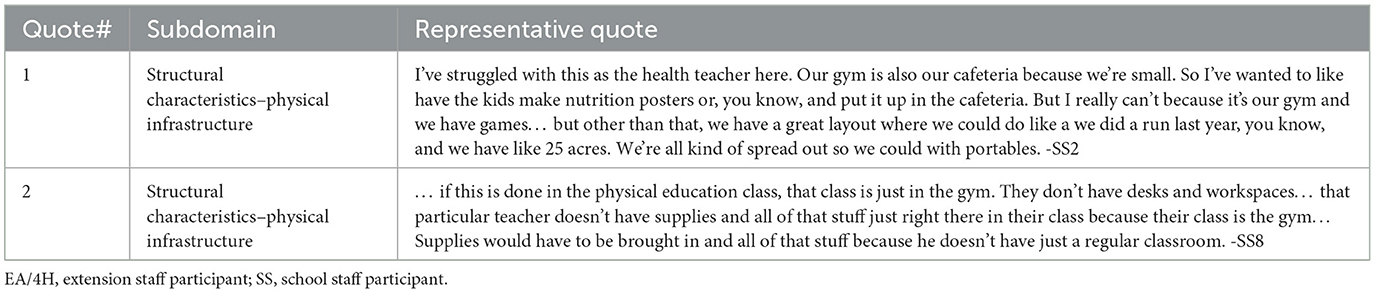
Table 4. Inner setting theme—participants discussed how the physical infrastructure required for STHS could be a challenge is some school contexts.
In addition, the use of classroom lessons and physical activities was seen as an effective, but logistically tricky, combination. For example, although nearly all schools had adequate physical education space, such as a gym, participants discussed how moving between the gym and the classroom during the instructional period may be cumbersome to the implementers. On the other hand, if the program were implemented in a gym by default, additional considerations or planning would be needed to make sure the gym was equipped with the necessary items to facilitate the curriculum's classroom lesson (e.g., desks, screens) that are not typically a part of the physical education space (Table 4, Quote 2).
Innovation theme—The STHS curriculum received positive feedback for its design, relative advantage compared to other curricula, and evidence-base.
Participants suggested that STHS would only be feasible to implement if it did not create any new demands for the school staff. For many participants, this was emphasized in the fact that they saw STHS alignment with the TEKS as a benefit of the curriculum. Class time in almost all subjects must be dedicated to meeting the TEKS standards, which are evaluated in statewide standardized testing. Thus, STHS aligned with the requirements and processes already in place in the schools and would not be perceived as taking anything away or adding additional burden to staff (Table 5, Quote 1). It is worth noting that alignment with TEKS was seen as a facilitator to implementation, but several Extension staff members expressed that it was not a guarantee of program adoption by the school due to difficulty implementing any kind of program in schools during state-mandated testing season.
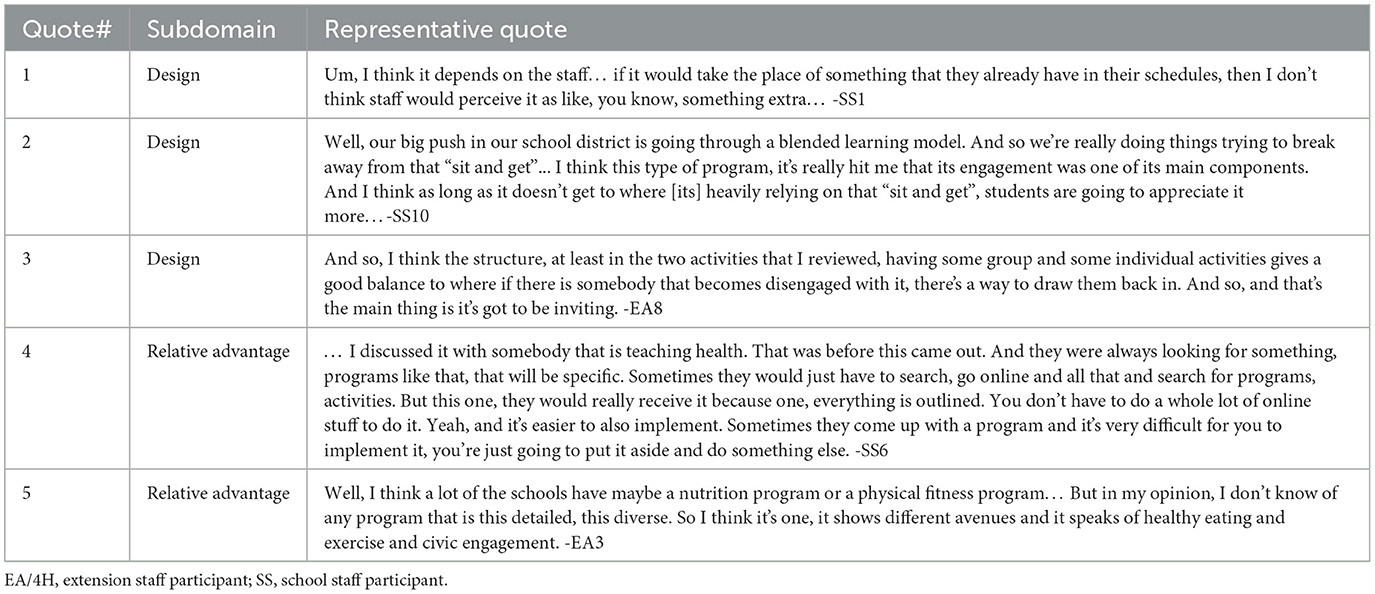
Table 5. Innovation theme—The STHS curriculum received positive feedback for its design, relative advantage compared to other curricula, and evidence-base.
Participants voiced a nearly unanimous positive reception to the design of the STHS curriculum in terms of its usability (e.g., clear, simple instructions) and thoroughness (e.g., self-contained, all materials provided). In addition, participants thought that the variety of activities and lesson structures would appeal to all types of students and a variety of learning styles. The curriculum was also praised for its minimization of “sit and get” learning, described as students simply sitting and listening to traditional, formal lectures (Table 5, Quote 2). Instead, participants discussed how STHS favored group-based activities, active learning, and physical engagement. The balance of activities was also considered a high point, in that no single learning style or teaching format (e.g., group vs. individual tasks, video vs. reading) stood out above the rest (Table 5, Quote 3).
STHS was also discussed in reference to other programs (or the lack thereof) that addressed similar topics. The nutrition and/or PA information covered by STHS was considered to be specific and actionable by participants, whereas the lessons in comparable programs were often too vague or generalized to be particularly useful to students (Table 5, Quote 4). Furthermore, participants asserted that STHS was overall more comprehensive in its approach, covering a variety of topics relating to nutrition, as well as connecting them to health and social connections in a way that is not typically done within school-based curricula (Table 5, Quote 5).
Outer setting theme—Local partners' attitudes and conditions may affect the adoption and implementation of STHS.
In reference to the context in which the school operates, a frequent topic of discussion by Extension staff was the Student Health Advisory Councils (SHACs), which are required by Texas law to be established in each school district and are required to meet at least four times per year. Texas SHACs are comprised of educators and administrators, county extension agents, and local residents. Interview participants cited the SHAC as a logical partner in adopting and delivering the STHS program into schools (Table 6, Quote 1), though some noted that SHACs can be inconsistently administered, understaffed, or overburdened with existing obligations. Comments regarding SHACs—both positive and cautionary—came from Extension staff, consistent with their role as health and education promotion agents within the county who regularly partner with community advisory and steering committees such as SHACs.
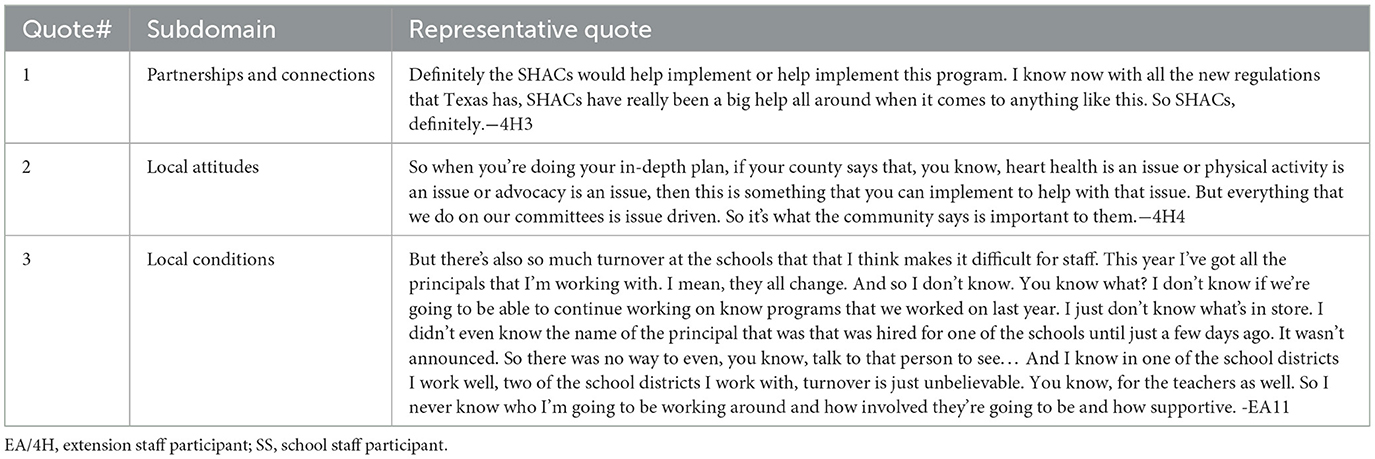
Table 6. Outer setting theme—local partners' attitudes and conditions may affect the adoption and implementation of STHS.
The mandate of the SHAC is to ensure that school district health priorities reflect the priorities and values of community residents. In this regard, participants noted that in their preparation for the academic year, local priorities are given precedence, meaning that programs such as STHS must align with not only the implementer's objectives, but the goals of stakeholders in the broader context as well (Table 6, Quote 2). The implementation challenge for STHS, then, would be in the assumption that SHACs would be a consistent source of support between years. Finally, participants noted that factors outside of their influence or control, such as staff turnover at the district or school administrator level (Table 6, Quote 3), could impede implementation of programs like STHS.
Discussion
Implementation of evidence-based innovations requires identification of barriers and facilitators to using that program with a specific population in a specific setting. To this end, the CFIR framework was preemptively applied to interviews conducted with Texas middle-school educators and extension staff regarding the STHS program at their respective school(s). The study found that participants provided generally positive comments, with some specific caveats and hesitations, about the potential for implementation of STHS. These findings align with much of the literature on barriers and facilitators to school-based programs; programs are more likely to be successfully implemented when there is support and training available from the program developers25, which the participants noted as a positive strategy to promote buy-in from school staff and leadership.
Additionally, aligning programs with state-mandated testing requirements, which several participants mentioned as a strength of STHS, reduces the competition in school priorities, a documented barrier to implementation (25). Based on these findings, it will be important for researchers, and eventually, Extension staff working with schools to adopt STHS to discuss the types of training and resources that will be available to teachers and emphasize the alignment of STHS with TEKS as a way to enhance curricular alignment, and potential academic outcomes. These findings also echo prior implementation evaluation of civic engagement interventions to create health-focus changes to the built environment; important facilitators for success of these types of programs include securing stakeholder support (e.g., partners in the community that can mobilize resources to facilitate change) and being able to negotiate around time constraints (26, 39, 40).
Participants also noted, however, specific circumstances and contexts in four of the five domains that could act as barriers to implementation if not considered. A notable example is the continually shifting priorities of external partners such as SHACs, which as noted are obligated to reflect the values and priorities of local community residents. This is in line with previous research that identifies socio-political contexts and the priorities of the surrounding environment as possible barriers to implementation of school-based programs (22). This is also the space in which Texas Extension staff operate, as many of them serve on their SHAC. By working with extension agents to implement STHS, the research team can identify when schools and communities are interested in implementing health and positive youth development programs, as well as other circumstances where STHS may align with the needs and values of communities (e.g., wanting to offer an after school program). By providing unique insight into the priorities and amenability of their local SHACs and other potential implementation support, extension agents will thus be critical partners in tailoring STHS implementation plan to local contexts.
Another finding was that variability in teachers' or extension agents' experience was a potential barrier to implementing STHS. More specifically, participants stated that newer teachers and extension agents may not be as prepared to manage classroom time and/or students, and these topics were not covered in the curriculum materials. These results corroborate previous studies that also identified managing time and students as a challenge during the implementation of behavioral programs in schools (14, 15, 20). Some methods of addressing this concern may be to provide optional additional training, ancillary support materials, or additional implementation support from an experienced educator to help less experienced implementers with the program. Providing training for the STHS program was perceived as positive implementation support and is widely supported as a facilitator to successful school-based programs (22–24), both in the United States as well as international contexts (51, 52). By providing additional time management and classroom management strategies, the research team may be able to provide a more comprehensive and tailored training regimen that addresses potential barriers. In addition, training models that address diverse experience levels could be proposed.
The application of CFIR to these interviews yielded useful information to contextualize the program and provide potential ways to improve the implementation of STHS at different levels of influence, which can lead to designing programs that are more practical, scalable, and impactful for the school context. Although the study revolved around one specific evidence-based program (i.e., STHS), the findings may be applied to a wider array of school-based programs that focus on PA, healthy eating, and/or positive youth development. For example, identified challenges that result in variations in implementation fidelity of after-school programs or inconsistency of community boards, such as SHACs, are likely to be issues that are encountered by many researchers and practitioners delivering programs in the school setting. Additionally, the need for training to implement programs, sensitivity to limited instructional time, and accommodation of varying teacher experience levels are also factors found here that are not unique to STHS or the Texas public education system. However, future research is needed to better understand and test the relationships between the barriers identified here and various implementation outcomes (e.g., adoption, fidelity, sustainability).
Limitations
Participants in this study reviewed only two sessions of the full STHS curriculum to provide feedback, and provided with a verbal overview of the entire program. Their perceptions of the program's usefulness, barriers, and facilitators of implementation are limited in this way. However, given the consistency in the comments across interviews that formed, and the themes discussed here, the authors are confident that the findings reflect the overall STHS curriculum and its potential for implementation. Interviews did not consider the perspectives of all people involved with STHS's delivery (e.g., students, parents, school health advisory council members). Although these individuals' perspectives are important, they may not apply to all aspects of the implementation process (e.g., use of the implementation guide, classroom management), and as a result, they are not included here. Future studies providing a more comprehensive perspective of all stakeholders are needed.
Strengths
Despite not including all pertinent stakeholder groups, as mentioned above, interview participants presented a useful sampling of potential innovation deliverers, facilitators, and support personnel that gave comprehensive feedback on all aspects of the CFIR framework. Another strength was the use of inductive coding, followed by deductive CFIR coding, which allowed the research team to find emergent barriers and facilitators that may not have been captured by an exclusively deductive coding process, which may be overly constrained by a priori categories and ideas. Finally, having participants identify potential barriers before STHS implementation and evaluation allowed the team to pre-emptively change the curriculum and the implementation strategies (e.g., developing additional classroom management training materials) before evaluating it in a randomized controlled trial.
Conclusion
According to Extension staff and school staff members, STHS provides a comprehensive and accessible intervention for improving middle-schooler nutrition and PA knowledge. Many aspects of the program address existing needs and are tailored to overcome implementation barriers for school-based interventions, as recognized by participants who felt the useability of the curriculum and the alignment with teaching standards were advantageous. Further refinement of the implementation process of STHS could be accomplished through additional strategizing with local community advisory boards (e.g., SHACs) and targeted training that is more responsive to educators' needs.
Data availability statement
Data are available from Jacob Szeszulski (SmFjb2IuU3plc3p1bHNraUBhZ25ldC50YW11LmVkdQ==) upon completion of a satisfactory data sharing agreement.
Ethics statement
The studies involving humans were approved by Texas A&M University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AMc: Investigation, Writing – original draft, Writing – review & editing, Formal analysis. AMa: Conceptualization, Writing – review & editing, Supervision. GD: Writing – review & editing. AH-L: Formal analysis, Writing – review & editing. MA: Writing – review & editing, Formal analysis. KN: Formal analysis, Writing – review & editing. YO: Writing – review & editing. CR: Supervision, Writing – review & editing. RS-F: Supervision, Writing – review & editing. JS: Writing – review & editing, Supervision.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported in part by the NIH/NIMHD (R01MD018214).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Jebeile H, Kelly AS, O'Malley G, Baur LA. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. (2022) 10:351–65. doi: 10.1016/S2213-8587(22)00047-X
2. U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025. (2020). Available online at: https://www.dietaryguidelines.gov/sites/default/files/2021-03/Dietary_Guidelines_for_Americans-2020-2025.pdf (accessed June 11, 2025).
3. Szeszulski J, Lanza K, Dooley EE, Johnson AM, Knell G, Walker TJ, et al. Y-PATHS: a conceptual framework for classifying the timing, how, and setting of youth physical activity. J Phys Act Health. (2021) 18:310–7. doi: 10.1123/jpah.2020-0603
4. Lange SJ, Moore LV, Harris DM, Merlo CL, Lee SH, Demissie Z, et al. Percentage of adolescents meeting federal fruit and vegetable intake recommendations — youth risk behavior surveillance system, United States, 2017. MMWR Morb Mortal Wkly Rep. (2021) 70:69–74. doi: 10.15585/mmwr.mm7003a1
5. Katzmarzyk PT, Denstel KD, Carlson J, Crouter SE, Greenberg J, Pate RR, et al. The 2022 United States Report Card on Physical Activity for Children & Youth Acknowledgements Results. (2022). Available online at: https://paamovewithus.org/wp-content/uploads/2022/10/2022-US-Report-Card-on-Physical-Activity-for-Children-and-Youth.pdf (accessed March 19, 2025).
6. Rock CL, Thomson C, Gansler T, Gapstur SM, McCullough ML, Patel AV, et al. American cancer society guideline for diet and physical activity for cancer prevention. CA Cancer J Clin. (2020) 70:245–71. doi: 10.3322/caac.21591
7. World Health Organization. Global Action Plan on Physical Activity 2018–2030. Geneva: World Health Organization (2019).
8. Brener ND, McManus T, Shanklin SL, Queen B. School Health Profiles 2020: Characteristics of Health Programs Among Secondary Schools. (2020). Available online at: https://www.cdc.gov/healthyyouth/data/profiles/results.htm (accessed March 19, 2025).
9. Goodway J Getchell N Raynes D National Association for Sport and Physical Education. Active Start : A Statement of Physical Activity Guidelines for Children from Birth to Age 5. Annapolis Junction, MD: National Association for Sport and Physical Education (2009). 48 p.
10. Faries MD, Lopez ML, Faries E, Keenan K, Green SD. Evaluation of walk across Texas! - a web-based community physical activity program. BMC Public Health. (2019) 19:1588. doi: 10.1186/s12889-019-7918-3
11. Lopez ML, Faries MD, Lankford EG, Green SD. Sustained effectiveness of the walk across Texas program: a follow-up study. Am J Health Behav. (2023) 47:1271–80. doi: 10.5993/AJHB.47.6.19
12. Wolfe WS, Scott-Pierce M, Dollahite J. Choose health: food, fun, and fitness youth curriculum promotes positive behaviors. J Nutr Educ Behav. (2018) 50:924–30. doi: 10.1016/j.jneb.2017.09.008
13. Wolfe WS, Dollahite J. Evaluation of the choose health: food, fun, and fitness 3rd- to 6th-grade curriculum: changes in obesity-related behaviors. J Sch Health. (2021) 91:9–18. doi: 10.1111/josh.12970
14. Wolfe W, Dollahite J, Scott-Pierce M. Practice-Based Evidence for Cornell's Choose Health: Food, Fun, and Fitness (CHFFF) Youth Curriculum. Ithaca. (2016). Available online at: https://cfacaa.human.cornell.edu/dns.fnec/files/chfff/CHFFF_Practice-Based_Evidence_Report_2016.pdf (accessed March 19, 2025).
15. Curran T, Wexler L. School-based positive youth development: a systematic review of the literature. J Sch Health. (2017) 87:71–80. doi: 10.1111/josh.12467
16. Szeszulski J, Walker TJ, Robertson MC, Cuccaro P, Fernandez ME. School staff's perspectives on the adoption of elementary-school physical activity approaches: a qualitative study. Am J Health Educ. (2020) 51:395–405. doi: 10.1080/19325037.2020.1822241
17. Walker TJ, Craig DW, Robertson MC, Szeszulski J, Fernandez ME. The relation between individual-level factors and the implementation of classroom-based physical activity approaches among elementary school teachers. Transl Behav Med. (2021) 11:745–53. doi: 10.1093/tbm/ibaa133
18. Lee RE, Szeszulski J, Lorenzo E, Arriola A, Bruening M, Estabrooks PA, et al. Sustainability via active garden education: the sustainability action plan model and process. Int J Environ Res Public Health. (2022) 19:5511. doi: 10.3390/ijerph19095511
19. Szeszulski J, Walker TJ, Robertson MC, Fernandez ME. Differences in psychosocial constructs among elementary school staff that implement physical activity programs: a step in designing implementation strategies. Transl Behav Med. (2022) 12:237–42. doi: 10.1093/tbm/ibab120
20. Fox RA, Leif ES, Moore DW, Furlonger B, Anderson A, Sharma U, et al. A systematic review of the facilitators and barriers to the sustained implementation of school-wide positive behavioral interventions and supports. Educ Treat Children. (2022) 45:105–26. doi: 10.1007/s43494-021-00056-0
21. Naylor PJ, Nettlefold L, Race D, Hoy C, Ashe MC, Wharf Higgins J, et al. Implementation of school based physical activity interventions: a systematic review. Prev Med. (2015) 72:95–115. doi: 10.1016/j.ypmed.2014.12.034
22. Shoesmith A, Hall A, Wolfenden L, Shelton RC, Powell BJ, Brown H, et al. Barriers and facilitators influencing the sustainment of health behaviour interventions in schools and childcare services: a systematic review. Implement Sci. (2021) 16:62. doi: 10.1186/s13012-021-01134-y
23. Lomsdal SA, Lyngstad IK, Lagestad PA. Teachers' perceptions of barriers related to implementation of daily physical activity in secondary school: academic pressure and the need for new competence. Teach Teach Educ. (2022) 115:103749. doi: 10.1016/j.tate.2022.103749
24. Robertson RE, Kokina AA, Moore DW. Barriers to implementing behavior intervention plans: results of a statewide survey. J Posit Behav Interv. (2020) 22:145–55. doi: 10.1177/1098300720908013
25. Forman SG, Olin SS, Hoagwood KE, Crowe M, Saka N. Evidence-based interventions in schools: developers' views of implementation barriers and facilitators. School Ment Health. (2009) 1:26–36. doi: 10.1007/s12310-008-9002-5
26. Seguin RA, Folta SC, Sehlke M, Nelson ME, Heidkamp-Young E, Fenton M, et al. The strongwomen change clubs: engaging residents to catalyze positive change in food and physical activity environments. J Environ Public Health. (2014) 2014:1–6. doi: 10.1155/2014/162403
27. Plotnikoff RC, Costigan SA, Karunamuni N, Lubans DR. Social cognitive theories used to explain physical activity behavior in adolescents: a systematic review and meta-analysis. Prev Med. (2013) 56:245–53. doi: 10.1016/j.ypmed.2013.01.013
28. Riebl SK, Estabrooks PA, Dunsmore JC, Savla J, Frisard MI, Dietrich AM, et al. A systematic literature review and meta-analysis: the theory of planned behavior's application to understand and predict nutrition-related behaviors in youth. Eat Behav. (2015) 18:160–78. doi: 10.1016/j.eatbeh.2015.05.016
29. Bosnjak M, Ajzen I, Schmidt P. The theory of planned behavior: selected recent advances and applications. Eur J Psychol. (2020) 16:352. doi: 10.5964/ejop.v16i3.3107
30. Spence JC, Lee RE. Toward a comprehensive model of physical activity. Psychol Sport Exerc. (2003) 4:7–24. doi: 10.1016/S1469-0292(02)00014-6
31. Lee RE, Cubbin C. Striding toward social justice: the ecologic milieuof physical activity. Exerc Sport Sci Rev. (2009) 37:10–7. doi: 10.1097/JES.0b013e318190eb2e
32. Ohri-Vachaspati P, DeLia D, DeWeese RS, Crespo NC, Todd M, Yedidia MJ. The relative contribution of layers of the social ecological model to childhood obesity. Public Health Nutr. (2015) 18:2055–66. doi: 10.1017/S1368980014002365
33. Purnell JQ, Lobb Dougherty N, Kryzer EK, Bajracharya S, Chaitan VL, Combs T, et al. Research to translation: the healthy schools toolkit and new approaches to the whole school, whole community, whole child model. J Sch Health. (2020) 90:948–63. doi: 10.1111/josh.12958
34. Rooney LE, Videto DM, Birch DA. Using the whole school, whole community, whole child model: implications for practice. J Sch Health. (2015) 85:817–23. doi: 10.1111/josh.12304
35. Seguin-Fowler RA, Hanson KL, Villarreal D, Rethorst CD, Ayine P, Folta SC, et al. Evaluation of a civic engagement approach to catalyze built environment change and promote healthy eating and physical activity among rural residents: a cluster (community) randomized controlled trial. BMC Public Health. (2022) 22:1674. doi: 10.1186/s12889-022-13653-4
36. Seguin RA, Eldridge G, Graham ML, Folta SC, Nelson ME, Strogatz D. Strong hearts, healthy communities: a rural community-based cardiovascular disease prevention program. BMC Public Health. (2015) 16:86. doi: 10.1186/s12889-016-2751-4
37. Seguin RA, Graham ML, Eldridge G, Nelson ME, Strogatz D, Folta SC, et al. Strong hearts for New York: a multilevel community-based randomized cardiovascular disease risk reduction intervention for rural women. Contemp Clin Trials. (2019) 82:17–24. doi: 10.1016/j.cct.2019.05.005
38. Brown AGM, Hudson LB, Chui K, Metayer N, Lebron-Torres N, Seguin RA, et al. Improving heart health among Black/African American women using civic engagement: a pilot study. BMC Public Health. (2017) 17:112. doi: 10.1186/s12889-016-3964-2
39. Sriram U, Graham ML, Folta S, Paul L, Seguin-Fowler RA. Integrating civic engagement into a lifestyle intervention for rural women – a mixed methods process evaluation. Am J Health Promot. (2023) 37:807–20. doi: 10.1177/08901171231168500
40. Seguin RA, Sriram U, Connor LM, Silver AE, Niu B, Bartholomew AN, et al. A civic engagement approach to encourage healthy eating and active living in rural towns: the HEART club pilot project. Am J Health Promot. (2018) 32:1591–601. doi: 10.1177/0890117117748122
41. Texas Essential Knowledge and Skills | Texas Education Agency (2024). Available online at: https://tea.texas.gov/academics/curriculum-standards/teks-review/texas-essential-knowledge-and-skills (accessed March 16, 2025).
42. Bodkin A, Hakimi S. Sustainable by design: a systematic review of factors for health promotion program sustainability. BMC Public Health. (2020) 20:964. doi: 10.1186/s12889-020-09091-9
43. Damschroder LJ, Reardon CM, Widerquist MAO, Lowery J. The updated consolidated framework for implementation research based on user feedback. Implement Sci. (2022) 17:75. doi: 10.1186/s13012-022-01245-0
44. Wendt J, Scheller DA, Flechtner-Mors M, Meshkovska B, Luszczynska A, Lien N, et al. Barriers and facilitators to the adoption of physical activity policies in elementary schools from the perspective of principals: an application of the consolidated framework for implementation research–a cross-sectional study. Front Public Health. (2023) 11:935292. doi: 10.3389/fpubh.2023.935292
45. Craig DW, Walker TJ, Sharma SV, Cuccaro P, Heredia NI, Pavlovic A, et al. Examining associations between school-level determinants and the implementation of physical activity opportunities. Transl Behav Med. (2024) 14:89–97. doi: 10.1093/tbm/ibad055
46. Turner L, Calvert HG, Carlson JA. Supporting teachers' implementation of classroom-based physical activity. Transl J Am Coll Sports Med. (2019) 4:165–72. doi: 10.1249/TJX.0000000000000098
47. McLoughlin GM, Sweeney R, Liechty L, Lee JA, Rosenkranz RR, Welk GJ. Evaluation of a large-scale school wellness intervention through the consolidated framework for implementation research (CFIR): implications for dissemination and sustainability. Front Health Serv. (2022) 2:881639. doi: 10.3389/frhs.2022.881639
48. Schaefers A, Xin L, Butler P, Gardner J, MacMillan Uribe AL, Rethorst CD, et al. Relationship between the inner setting of CFIR and the delivery of the healthy school recognized campus initiative: a mixed-methods analysis. Implement Sci Commun. (2024) 5:96. doi: 10.1186/s43058-024-00627-3
49. Williams M, Moser T. The art of coding and thematic exploration in qualitative research. Int Manag Rev. (2019) 15:45–55.
50. Saunders B, Sim J, Kingstone T, Baker S, Waterfield J, Bartlam B, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. (2018) 52:1893–907. doi: 10.1007/s11135-017-0574-8
51. Mohammadi S, Su TT, Papadaki A, Jalaludin MY, Dahlui M, Mohamed MNA, et al. Perceptions of eating practices and physical activity among Malaysian adolescents in secondary schools: a qualitative study with multi-stakeholders. Public Health Nutr. (2021) 24:2273–85. doi: 10.1017/S1368980020002293
52. Lee DC, O'Brien KM, McCrabb S, Wolfenden L, Tzelepis F, Barnes C, et al. Strategies for enhancing the implementation of school-based policies or practices targeting diet, physical activity, obesity, tobacco or alcohol use. Cochrane Database Syst Rev. (2024) 2024:CD011677. doi: 10.1002/14651858.CD011677.pub4
Keywords: implementation science, exercise, healthy eating, school-based intervention, physical activity
Citation: McNeely A, MacMillan Uribe A, De Mello GT, Herrero-Loza A, Ali M, Nguyen K, Olawuyi Y, Rethorst CD, Seguin-Fowler RA and Szeszulski J (2025) Educators' perceived barriers and facilitators to implementing a school-based nutrition, physical activity, and civic engagement intervention: a qualitative analysis. Front. Public Health 13:1616483. doi: 10.3389/fpubh.2025.1616483
Received: 22 April 2025; Accepted: 05 June 2025;
Published: 27 June 2025.
Edited by:
Maria Immacolata Spagnuolo, Federico II University Hospital, ItalyReviewed by:
Nurul 'Ain Azizan, University of Nottingham Malaysia Campus, MalaysiaShooka Mohammadi, University of Malaya, Malaysia
Copyright © 2025 McNeely, MacMillan Uribe, De Mello, Herrero-Loza, Ali, Nguyen, Olawuyi, Rethorst, Seguin-Fowler and Szeszulski. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jacob Szeszulski, amFjb2Iuc3plc3p1bHNraUBhZy50YW11LmVkdQ==