 Bogusława Serzysko1*†
Bogusława Serzysko1*† Renata Mroczkowska2†
Renata Mroczkowska2† Jolanta Kamińska3†Beata Podsiadło4Grzegorz Żarczyński5Anna Krajza6
Jolanta Kamińska3†Beata Podsiadło4Grzegorz Żarczyński5Anna Krajza6- 1Department of Healthcare, Higher School of Applied Sciences in Ruda Śląska, Ruda Śląska, Poland
- 2Institute of Health Sciences, University of Opole, Opole, Poland
- 3Faculty of Medicine and Health Sciences, Academy of Applied Sciences in Nowy Sącz, Nowy Sącz, Poland
- 4Silesian Medical University in Katowice Faculty of Health Sciences in Katowice, Katowice, Poland
- 5College of Health Sciences in Bydgoszcz, Bydgoszcz, Poland
- 6Maria Sklodowska-Curie National Institute of Oncology, National Research Institute Gliwice, Gliwice, Poland
Introduction: The nursing profession involves substantial emotional and organizational demands, which may negatively affect nurses’ mental health and overall satisfaction with life and work.
Objective: To assess the levels of anxiety, depression, and irritability/anger symptoms in nurses and examine their associations with life and job satisfaction. In this study, the HADS-M subscale assessing irritability/anger was used. It captures symptoms of irritability and anger but does not measure aggression or anger expression as behavioral constructs.
Methods: A cross-sectional online survey was conducted among 538 registered nurses in Poland. Validated instruments were applied: HADS-M (for anxiety, depression, and irritability/anger symptoms), SWLS (life satisfaction), and SSP (job satisfaction). Statistical analyses included descriptive statistics, Spearman’s rank-order correlations, internal consistency (Cronbach’s alpha), and multiple linear regression (two-tailed, α = 0.05).
Results: A high prevalence of psychological symptoms was observed. All symptom domains were significantly and negatively correlated with life and job satisfaction (p < 0.001). Multiple regression analyses indicated that depressive symptoms were the strongest predictors of both life satisfaction (β = −0.429) and job satisfaction (β = −0.315), followed by irritability/anger symptoms. All models were statistically significant (p < 0.001).
Conclusion: Anxiety, depression, and irritability/irritability/anger symptoms significantly reduce nurses’ satisfaction with life and work. Depressive symptoms exerted the most profound impact. These findings emphasize the urgent need for targeted mental health support programs and preventive strategies to enhance nurses’ well-being and professional performance.
1 Introduction
Nurses play a pivotal role not only in providing direct patient care but also in shaping standards of care and advancing the professional development of nursing as a discipline (1, 2). They constitute the largest professional group in the Polish healthcare system. According to data from the Supreme Chamber of Nurses and Midwives, by 2022, 36% of actively employed nurses were aged 51–60, and nearly one-third were eligible for retirement. The average age of a nurse in Poland was 54 years and is projected to increase to 58 years by 2030 (3).
The majority of nurses work in rotating shifts, which disrupt circadian rhythms and adversely affect both mental and physical functioning (4). Nursing is considered a profession with a high risk of exposure to occupational stressors. In addition to shift work, the most frequently cited burdens include exposure to death and dying, emotional and physical overload, staff shortages, workplace bullying, and professional burnout (5, 6). The cumulative effect of these factors may result in decreased quality of life and reduced job satisfaction.
Subjective quality of life is a key component of psychological well-being (7, 8). Research indicates that chronic stress, emotional exhaustion, and negative affective states-frequently experienced by nurse-may diminish the quality of care, professional performance, and job satisfaction (9). Emotional responses such as anxiety, worry, and irritability are natural elements of daily functioning; however, prolonged stress exposure can result in psychophysiological dysfunctions, including sleep disturbances, somatic complaints, cardiovascular issues, or substance abuse (10–20). Shift work further impairs the gastrointestinal, hormonal, and cardiovascular systems (21–23). Accordingly, the World Health Organization recognizes nursing as one of the most demanding and stressful professions (24).
Studies conducted by researchers such as Zheng et al. (25), Desouky and Allama (26), Niedhammer et al. (27), and Nakada et al. (28) confirm high prevalence of depressive symptoms among nurses. Zheng et al. (25) additionally demonstrated that these symptoms are often intensified in this professional group. Studies conducted among nurses in Iran also confirm the frequent occurrence of anxiety and depressive disorders (29, 30). Abadi et al. (31) examined the influence of personality and occupational factors on the prevalence of anxiety and depression. Both physical and mental health in nurses are closely linked to the quality of their professional performance—particularly in relation to patient care, job satisfaction, and efficacy.
In recent years, growing attention has been paid to anger symptoms and irritability as important indicators of psychological strain among nurses. Although not always manifesting as overt aggression, these symptoms are often referred to in the literature as irritability (internalized anger) and may reflect difficulties in emotional regulation. Studies indicate that trait anger and modes of anger expression—particularly emotional suppression—are associated with lower job satisfaction and greater risk of burnout. Additionally, nurses frequently experience aggression in the workplace, both from patients and colleagues, which significantly compromises their psychological well-being. Such experiences may lead to chronic overload, reduced engagement, and lower job satisfaction (32–38).
Today’s nursing work environment also involves a risk of direct emotional aggression from patients or their families. Such encounters may result in chronic stress, anxiety, emotional tension, and overall deterioration in well-being. In severe cases, they may lead to post-traumatic stress disorder (PTSD) (38). In the face of such threats, job motivation, satisfaction, and care quality may deteriorate, while the risk of medical errors and adverse events increases (20).
To better understand these associations, this study adopted the Job Demands-Resources (JD-R) model, which posits that occupational well-being depends on the balance between job demands (e.g., workload, emotional pressure) and resources (e.g., support, autonomy, recognition) (39, 40). When demands outweigh resources, the risk of burnout and emotional dysregulation increases. This approach is complemented by the Job Demand—Control model (41), which emphasizes that the greatest risk of occupational stress occurs when high workload is accompanied by low decision latitude (42). Siegrist’s effort–reward imbalance model (43) further suggests that insufficient rewards—both financial and emotional—in the context of high employee effort contribute to chronic stress and depressive symptoms (44). On the individual level, the theory of emotional self-regulation (Baumeister and Heatherton) (45) proposes that chronic stress weakens the ability to control emotions, which may lead to irritability and a decline in quality of life (46).
Recently, increased scholarly attention has been devoted to anger symptoms-often labeled “irritability” or “nervousness” in the literature. Although these symptoms are not unequivocally classified as clinical aggression, they constitute important indicators of emotional overload and affect regulation difficulties. Studies have shown that trait anger and its expression patterns, such as emotional suppression, are significantly associated with reduced job satisfaction and an increased risk of burnout among nurses (47–49). Furthermore, exposure to workplace violence—both verbal and physical—from patients, their families, or coworkers—can impair psychological well-being and lead to burnout symptoms, reduced engagement, and lower job satisfaction (33–35).
Despite numerous studies confirming the high level of emotional strain among nurses, there is still a lack of comprehensive analyses that simultaneously assess the relationship between the severity of negative emotions—such as anxiety, depression, and anger symptoms—and quality of life, both professionally and personally, in this occupational group. This is particularly true for studies that incorporate a broad range of psychosocial and organizational variables in the context of the Polish healthcare system.
International studies by Liu et al. (33) and Kim et al. (47) confirm the associations between symptoms of anxiety, depression, and anger symptoms and professional burnout and quality of life among nurses, but most often focus on a single variable or individual risk factor. Similarly, researchers such as Zheng et al. (48), Niedhammer et al. (49), and Nakada et al. (50) report a high prevalence of depressive and anxiety symptoms in this occupational group, highlighting the global nature of the problem. However, in Poland, there is still a lack of studies addressing the co-occurrence of multiple negative emotions and their cumulative impact on nurses’ well-being—both at work and beyond. Previous analyses, such as those by Uchmanowicz et al. (51) and Talarowska and Gałecki (52), have rarely explored the relationship between the full spectrum of negative emotional states and quality of life in the specific context of a healthcare system characterized by chronic staffing shortages, work overload, low salaries, and organizational changes.
To avoid conceptual ambiguity, it is necessary to clarify the main constructs examined in this study. Job satisfaction can be understood as the individual’s evaluation of their professional duties, reflecting the extent to which these activities are perceived as meaningful, rewarding, and consistent with personal values (53). Life satisfaction, in turn, represents a broader perspective, referring to the overall cognitive judgment of the quality of one’s life as a whole (54).
In contrast to these cognitive appraisals, the study focuses on emotional symptoms. Symptoms of anxiety are conceptualized as persistent tension, worry, or apprehension that interfere with daily functioning. Symptoms of depression do not necessarily indicate a clinical disorder but rather reflect mood-related difficulties, including sadness, loss of interest, or reduced motivation. Anger is conceptualized as a natural, immediate emotional reaction to frustration or provocation; in the present study we operationalize this affect as “anger symptoms” using the HADS-M irritability/anger subscale. Unlike aggression, which refers to behavioral manifestations, anger symptoms may serve an adaptive function if adequately regulated (10, 45).
It is also important to distinguish between mood-related phenomena (such as symptoms of anxiety and depression), which are generally more enduring and pervasive, and emotions like anger, which are typically shorter in duration and arise in response to specific stimuli (10). This distinction underscores the complex and multidimensional nature of psychological functioning considered in the present research. For clarity, in this manuscript we treat anxiety and depressive symptoms as mood phenomena (longer-lasting, pervasive), whereas anger is treated as an emotion (short-lived, stimulus-bound); we assess anger symptoms using the HADS-M anger subscale and do not assess aggressive behavior. Throughout this manuscript, the term “depression” refers exclusively to “symptoms of depression” as measured by the HADS-M; we do not infer clinical diagnoses.
The aim of this study was to evaluate the associations between the intensity of anxiety, depressive, and irritability/anger symptoms (operationalized via the HADS-M irritability/anger subscale) and levels of life and job satisfaction among nurses. The study also considered occupational factors such as years of experience, duration of employment at the current facility, shift work schedule, average monthly working hours, and number of jobs held. While stress and occupational burnout are addressed in the theoretical framework of this study, they were not directly measured and are discussed in the limitations section.
2 Materials and methods
2.1 Study design and setting
This was a cross-sectional study conducted using a diagnostic survey method. Data were collected via an anonymous online questionnaire distributed through the Google Forms platform between June 2023 and February 2024.
Given the specific characteristics of nursing work and the difficulty of conducting on-site research in clinical settings, a remote data-collection approach was adopted. Recruitment relied on purposive sampling via closed professional groups and thematic forums on social media, enabling access to nurses employed across multiple regions of Poland and in diverse healthcare facilities (hospitals, outpatient clinics, long-term care institutions, and other medical settings). Geographic quotas were not applied and province/voivodeship was not recorded; therefore, the study does not claim nationwide representativeness. This stance is consistent with the size and structure of the national nursing workforce reported by the Supreme Chamber of Nurses and Midwives (NIPiP) in 2022 (3), against which our convenience sample should not be viewed as representative.
Participation was entirely voluntary; no directly identifiable information was collected; and all data were stored securely with access limited to the research team. This strategy prioritized feasibility and confidentiality for a hard-to-reach workforce while acknowledging the non-probability nature of the sample.
Although not designed for population inference, the sample provided adequate statistical power for within-sample associations. A post-hoc power analysis in G*Power 3.1 for a two-tailed correlation test (Spearman), with α = 0.05, assumed medium effect (ρ = 0.30), and N = 538 yielded power 1–β ≈ 0.999, indicating very high sensitivity to detect the hypothesized relationships.
2.2 Participants
The study targeted actively employed registered nurses in Poland. Inclusion criteria were: current employment as a nurse in Poland, age ≥ 18 years, ability to complete an online Polish-language survey, and informed, voluntary consent with acknowledgment of the study’s purpose, anonymity, and data-processing procedures.
Exclusion criteria were: not currently employed as a nurse, nursing students/interns, midwives or other healthcare professionals working in non-nursing roles, lack of consent, and duplicate or incomplete questionnaires (removed prior to analysis).
Participants were recruited via purposive sampling through closed professional groups and thematic forums on social media. Respondents completed the questionnaire independently in a web browser. No geographic quotas were used and province/voivodeship was not recorded; therefore, we do not claim nationwide representativeness.
A total of 550 forms were submitted. After eligibility screening and data-quality checks, 538 fully completed questionnaires were retained for the final analysis. The sample encompassed nurses with diverse demographic and professional profiles, including variation in age, years of experience, employment setting (e.g., outpatient care, medical/surgical wards, ICU/ED, long-term care), work schedules, and educational levels.
2.3 Population characteristics
The final sample comprised 538 nurses. The majority were women (96.65%, n = 520), while men accounted for 3.35% (n = 18). The largest age group was 51–60 years (40.15%, n = 216), followed by 41–50 years (31.78%, n = 171). The youngest participants, aged 22–30, represented 9.29% (n = 50), and those over 60 years accounted for 6.32% (n = 34).
Most participants lived in urban areas (76.77%, n = 413), while 23.23% (n = 125) resided in rural areas. In terms of education, the most frequent qualification was a bachelor’s degree in nursing (39.41%, n = 212), followed by a master’s degree (33.83%, n = 182) and secondary medical education (26.77%, n = 144). Regarding marital status, most respondents were married (67.47%, n = 363). Others were single (10.22%), divorced (10.22%), widowed (5.02%), or in informal relationships (7.06%). In terms of work experience, the most common ranges were 31–40 years (33.64%, n = 181) and 21–30 years (29.37%, n = 158). A small proportion (3.16%) reported less than one year of total work experience. At their current workplace, most participants had worked for less than 5 years (25.46%), followed by 10–20 years (22.68%) and 5–9 years (12.45%). A minority (3.16%) had been employed at the same institution for over 40 years.
Participants were employed in a variety of healthcare settings. The most frequent workplaces were outpatient care facilities (38.29%), medical wards (36.25%), and surgical units (18.77%). A total of 10.59% were employed in intensive care units and emergency departments (ICU/ED), and 12.83% worked in long-term care.
Most respondents were employed on a permanent contract (94.98%). Approximately half (50.74%) worked 168–250 h per month, while 45.72% worked fewer than 168 h. A shift-work system reported by 72.49% of participants. The majority (63.38%) were employed in a single workplace, while 31.60% worked in two facilities simultaneously. Descriptive characteristics of the sample (sex, age, place of residence, education, marital status, job tenure, tenure at the current workplace, and place of work) are presented in Table 1.
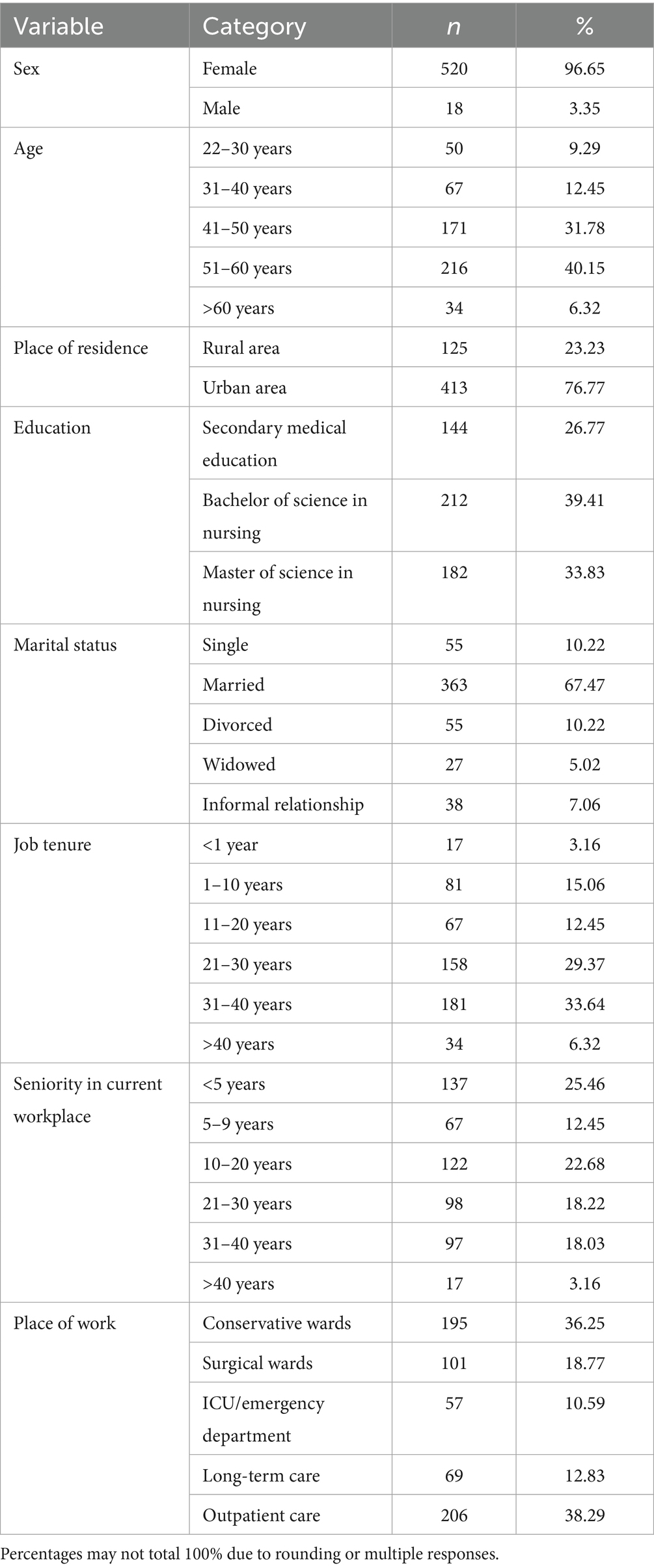
Table 1. Sociodemographic and professional characteristics of the respondents (n = 538).
3 Measures and instruments
The study used a self-developed questionnaire and three standardized tools: the Hospital Anxiety and Depression Scale—Modified (HADS-M) by Zigmond and Snaith (55), the Job Satisfaction Scale (SSP) by Zalewska (53), and the Satisfaction with Life Scale (SWLS) by Diener et al. (54).
The original questionnaire included 34 items. Section I (items 1–12) addressed sociodemographic and occupational variables. Section II (items 13–22) explored emotional responses related to professional duties. Section III (items 23–34) focused on perceived occupational stress and its effects on personal and professional life.
The HADS-M consists of 16 items that assess three emotional domains: anxiety, depression, and irritability/anger. It is a modified version of the original HADS by Zigmond and Snaith (55). The Polish adaptation was developed by Majkowicz (56). The irritability/anger subscale was added based on an unpublished version used in clinical research. Although HADS-M was originally designed for somatic patients, it has also been applied in population studies, including research among nurses, despite lacking formal validation in this professional group (57) and aggressive behaviors were not assessed. Each subscale uses a 4-point Likert scale (0–3). Scores range from 0–21 for anxiety and depression, and 0–6 for anger. Interpretation thresholds: 0–7 = normal, 8–10 = borderline, ≥11 = possible disorder (58). In this study, Cronbach’s alpha values were: anxiety −0.84, depression −0.863, anger −0.81, confirming good internal consistency.
Job Satisfaction Scale (SSP). This instrument evaluates the cognitive aspect of general job satisfaction and includes five items rated on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). A higher score indicates greater job satisfaction. In this study, Cronbach’s alpha was 0.89, consistent with the original validation (53).
Satisfaction with Life Scale (SWLS). This tool assesses global life satisfaction using five items scored on a 7-point Likert scale. Total scores range from 5 to 35, with higher scores indicating greater life satisfaction. The Polish adaptation was developed by Juczyński (59). Reliability coefficients were: original version −0.87 (54), Polish adaptation −0.72 (59), current study −0.89.
3.1 Statistical analysis
Data collected from 538 nurses employed in various healthcare facilities were subjected to descriptive and inferential analyses using Statistica v.13.0 (TIBCO Software Inc., 2017) and Microsoft Excel. Categorical variables are presented as n (%) and scale scores as mean (SD) or median (IQR), as appropriate. Because summed scale scores can deviate from normality, associations were examined with Spearman’s rank-order correlation (ρ). To identify independent predictors of depressive symptoms, anxiety, and irritability/anger symptoms, separate multiple linear regression models were fitted for each dependent variable with SWLS and SSP total scores as predictors. Model assumptions (linearity, normality and homoscedasticity of residuals) were checked via residual diagnostics; multicollinearity was assessed with VIF; influential observations were screened using Cook’s distance. Where heteroscedasticity was detected, heteroscedasticity-robust standard errors (HC3) were used. Standardized coefficients (β) with 95% confidence intervals were reported. Internal consistency was evaluated with Cronbach’s alpha. All tests were two-tailed with α = 0.05. Post hoc power analysis (G*Power 3.1) for a two-tailed correlation (α = 0.05; n = 538) indicated power > 0.999 to detect a medium effect (ρ = 0.30); the minimum detectable correlation at 80% power was |ρ| ≈ 0.12 (≈0.14 for 90% and ≈0.155 for 95%).
3.2 Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki (1975, revised in 2013) (60). All participants gave informed consent, and anonymity was maintained throughout the research. Participants were informed of the study’s purpose and their right to withdraw at any time without consequences. According to Polish regulations and institutional guidelines, anonymous non-interventional survey-based studies that do not involve sensitive personal data or direct health interventions do not require ethics committee approval. These studies are not classified as medical experiments under Article 21 of the Polish Act of December 5, 1996, on the professions of physician and dentist (Dz.U.2019.537 j.t.). Contact details were provided for participants in case of additional questions or concerns.
4 Results
A total of 538 nurses employed in various healthcare settings participated in the study. The results are presented in the following order: general psychological symptoms and work-related stress, scale assessments, correlation analyses, and regression modeling. All statistical analyses were performed using Statistica v.13.0 (77) and Microsoft Excel.
4.1 Psychological symptoms and emotional states related to work
A large proportion of respondents reported feeling emotionally exhausted due to work (86.25%) and physically fatigued (52.97%). Additionally, 36.80% of participants declared feeling tired upon waking, triggered by the mere thought of going to work.
Work-related anxiety was most frequently reported several times per month (39.96%), several times per week (28.07%), or daily (12.45%). A total of 19.52% of respondents reported no such emotions. Regarding irritability/anger symptoms, 44.61% experienced them several times per month, 31.23% several times per week, and 11.34% daily. No such experiences were reported by 12.83% of participants.
Work satisfaction was experienced several times a month by 41.45% of nurses, several times a week by 27.32%, and daily by 16.73%. A lack of job satisfaction was reported by 14.50% of respondents.
Work errors caused by excessive workload occurred most frequently several times per year (55.58%), less often several times a month (9.85%), once a week (1.86%), or daily (0.74%). A total of 31.97% declared never making such errors. 15.43% reported having taken sick leave due to psychological overload, while 84.57% had not used this form of absence.
4.2 Work-related stress and its sources
Workplace stress was common among respondents. Daily stress was reported by 32.90% of participants, several times per week by 32.16%, and several times per month by 32.71%.
The most frequently reported sources of occupational stress included time pressure and work urgency (72.86%) and staff shortages (71.00%). Other reported causes included responsibility for patient health and life (51.86%), lack of supervisor support (44.98%), low pay (42.75%), and poor work organization (37.73%). Additional stressors were contact with patient death (29.74%), lack of breaks (28.25%), fear of infection (28.25%), shift work (26.39%), exposure to harmful factors (25.65%), and limited opportunities for professional development (10.04%). Detailed data are presented in Table 2.
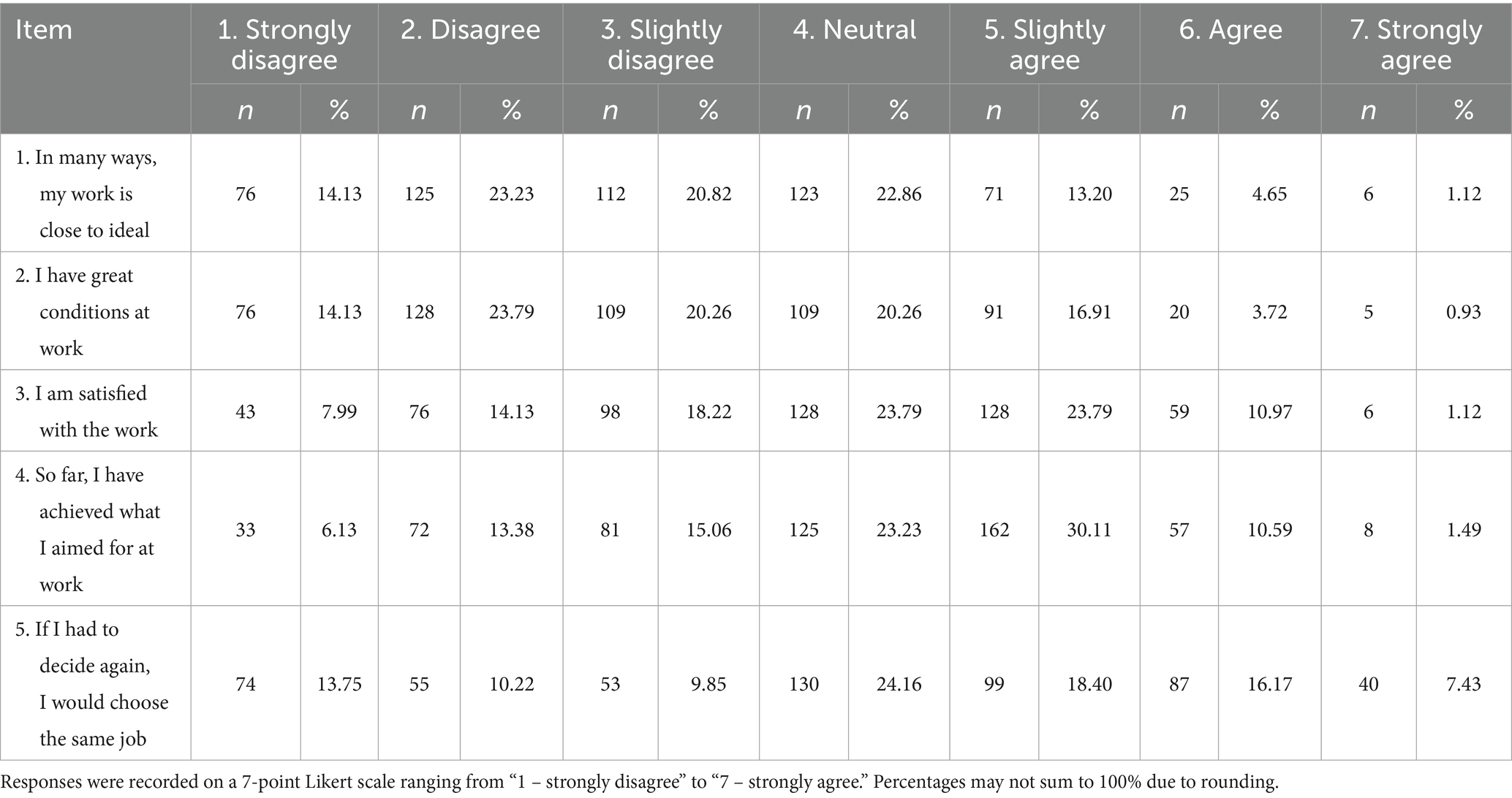
Table 2. Distribution of responses to the job satisfaction scale (SSP) (n = 538).
4.3 HADS-M, SSP, and SWLS scale results
According to the HADS-M scale results, 46.65% of respondents occasionally experienced tension and irritability, while 49.07% reported symptoms of depression. Internal anxiety was declared by 44.80% of participants. Sad thoughts occurred in 39.22% of respondents, while 46.10% reported feeling cheerful and positive at times. Conversely, 42.57% stated they sometimes felt irritated and angry; anger symptoms were reported rarely (34.76%) or sometimes (32.53%). Detailed HADS-M results are presented in Tables 3, 4.
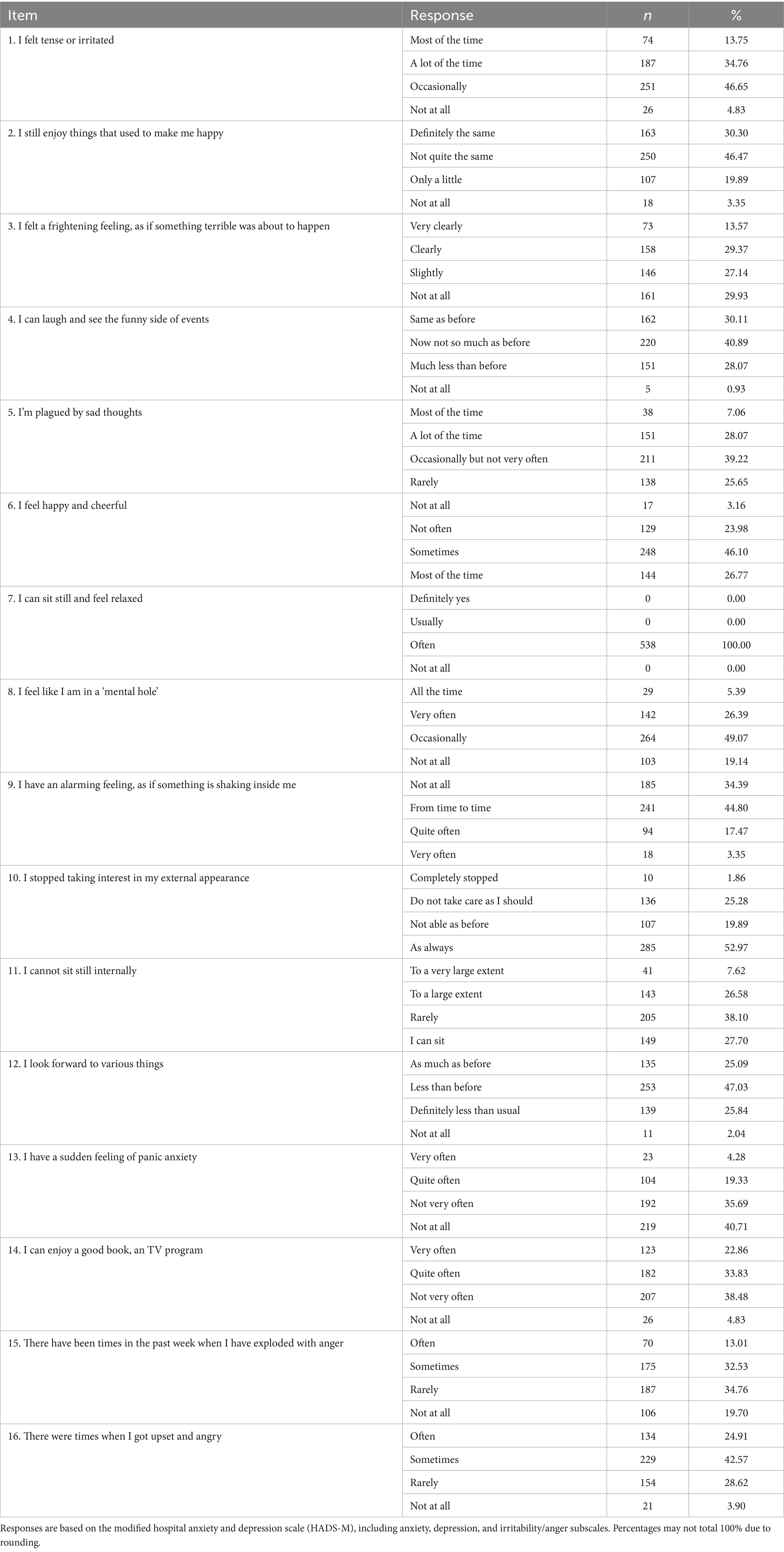
Table 3. Distribution of responses to the HADS-M irritability/anger symptoms subscale (n = 538).
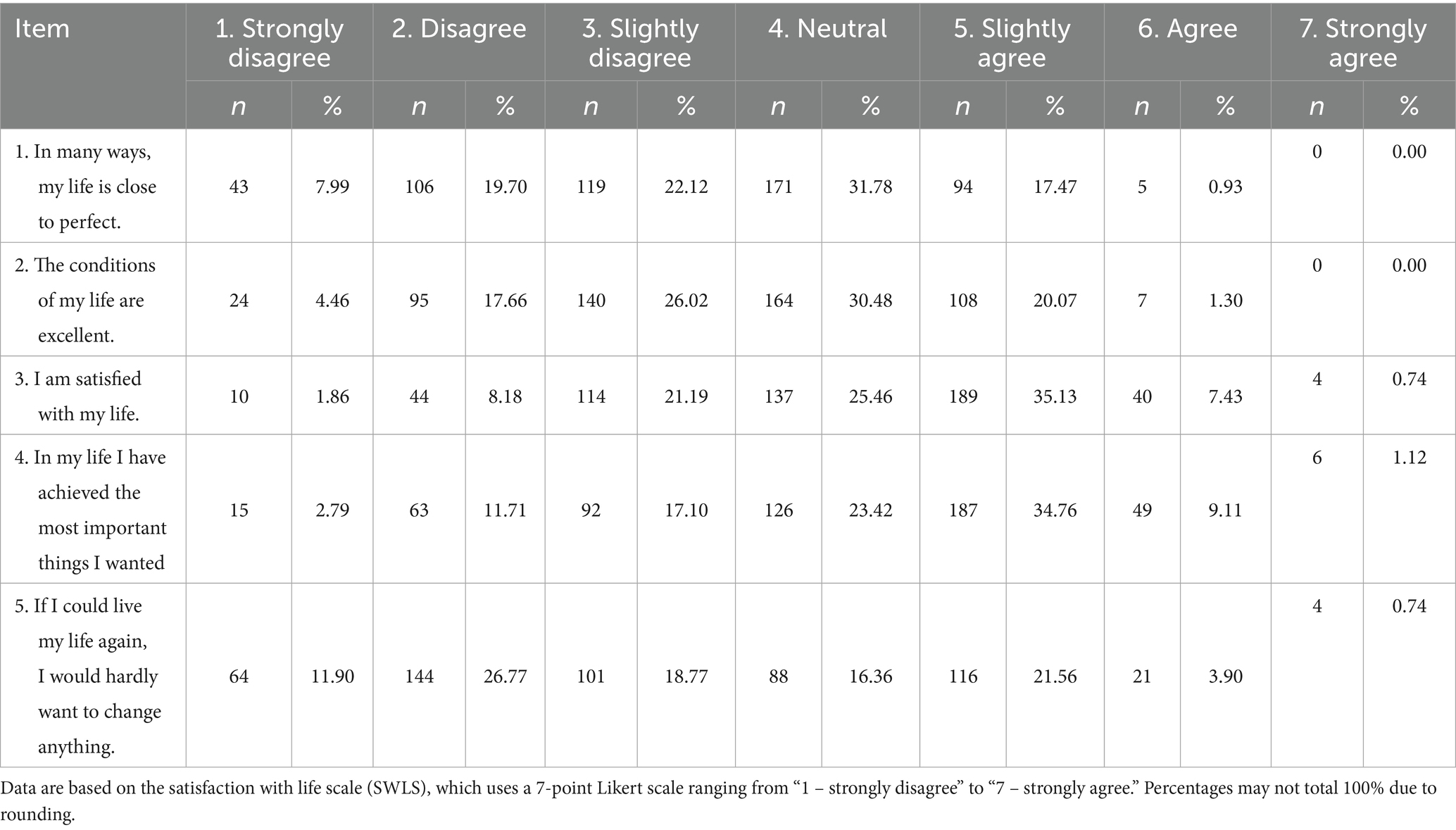
Table 4. Distribution of responses to the satisfaction with life scale (SWLS) (n = 538).
The Job Satisfaction Scale (SSP) results revealed notable variation. For example, the statement “In many ways my job is close to ideal” received disagreement from 23.23% of participants, a neutral response from 22.86%, and partial disagreement from 20.82%. The full distribution of responses is provided in Table 5.
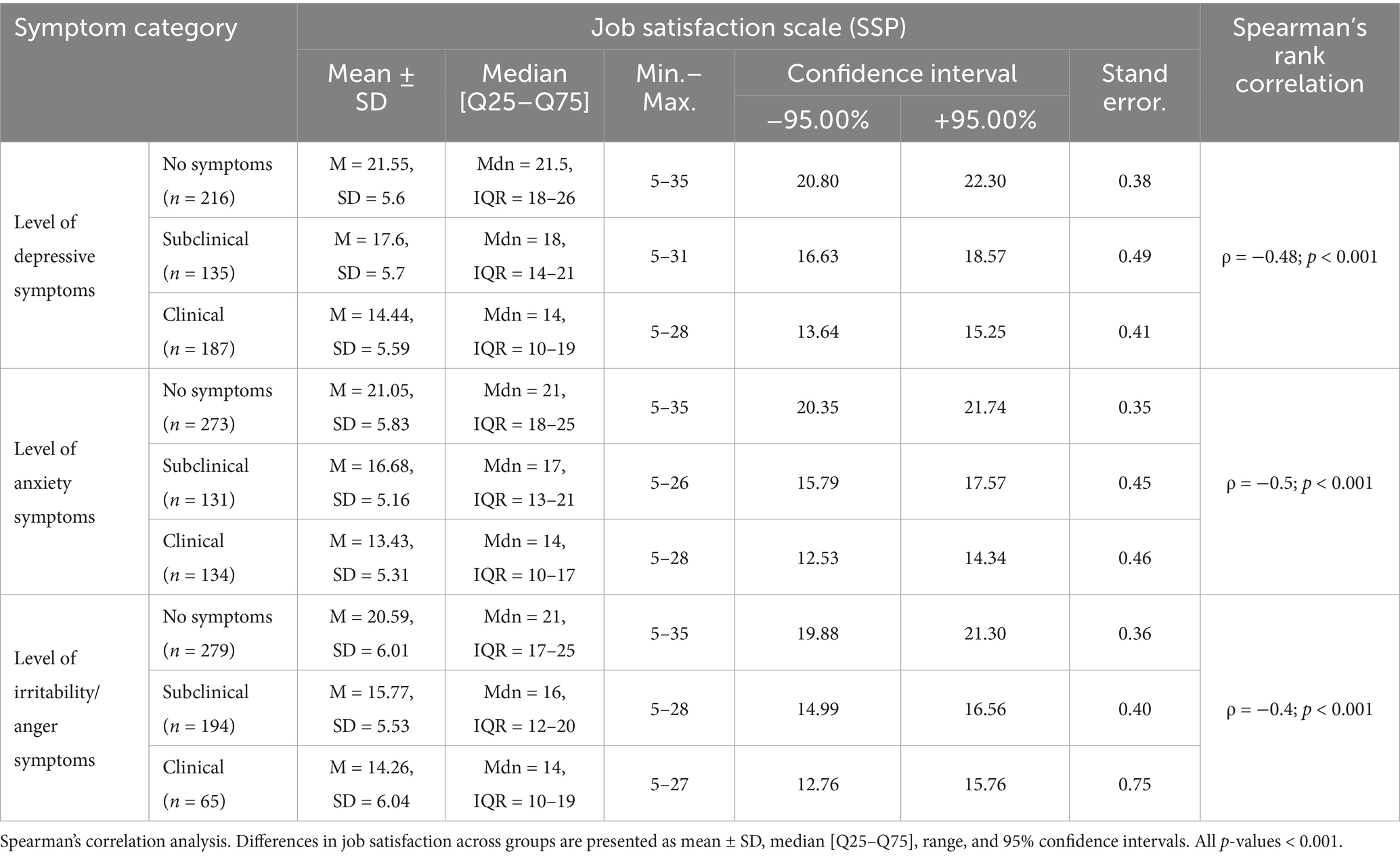
Table 5. Relationship between levels of depression, anxiety and irritability/anger symptoms and job satisfaction (n = 538).
For the Satisfaction with Life Scale (SWLS), most respondents selected neutral answers to the statements “My life is close to ideal” (31.78%) and “The conditions of my life are excellent” (30.48%). Detailed results are presented in Table 6.
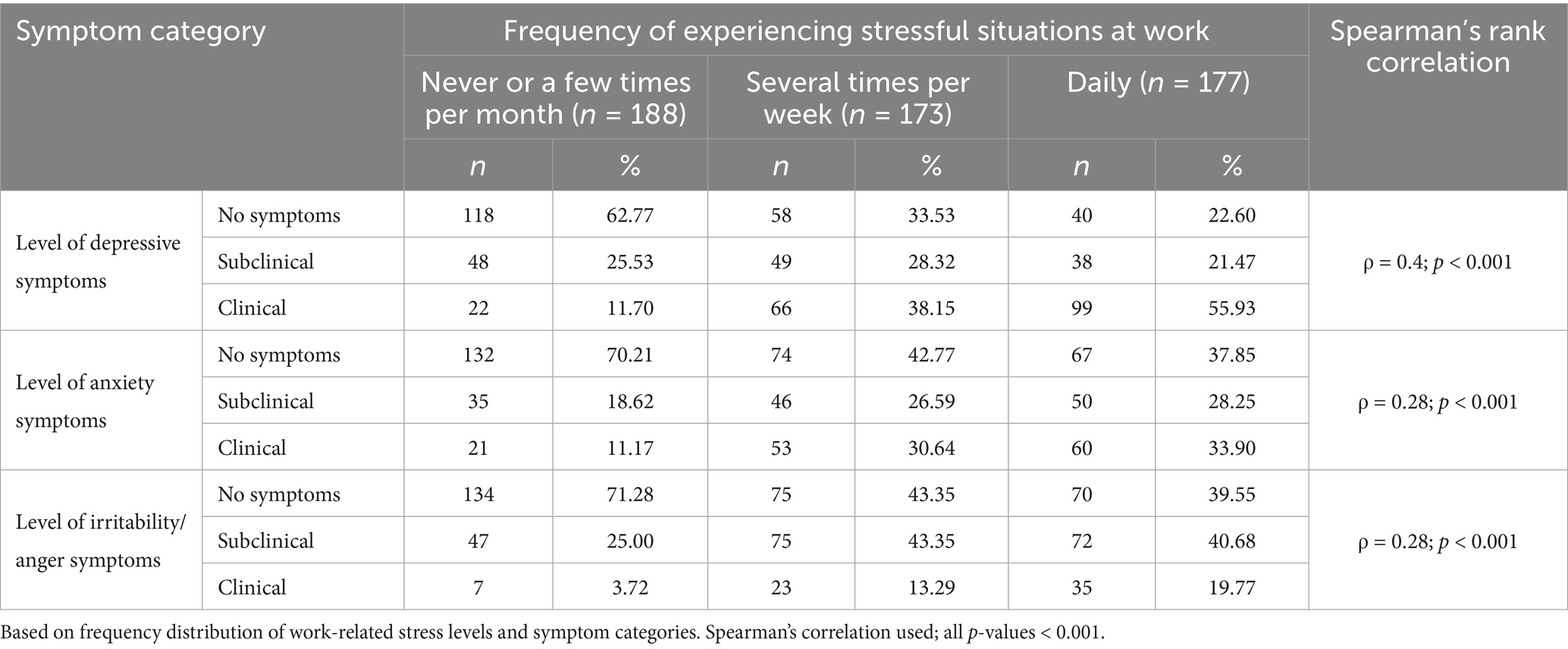
Table 6. Relationship between frequency of experiencing work-related stress and levels of depression, anxiety and irritability/anger symptoms (n = 538).
4.4 Correlations between variables
Spearman’s rank-order correlation analyses showed statistically significant negative associations between life satisfaction and symptoms of depression (ρ = −0.56; p < 0.001), anxiety (ρ = −0.55; p < 0.001), and (ρ = −0.38; p < 0.001). Similar correlations were found between job satisfaction and these symptoms: depression (ρ = −0.48), anxiety (ρ = −0.50), and (ρ = −0.40), all significant at p < 0.001. Results are summarized in Table 7.
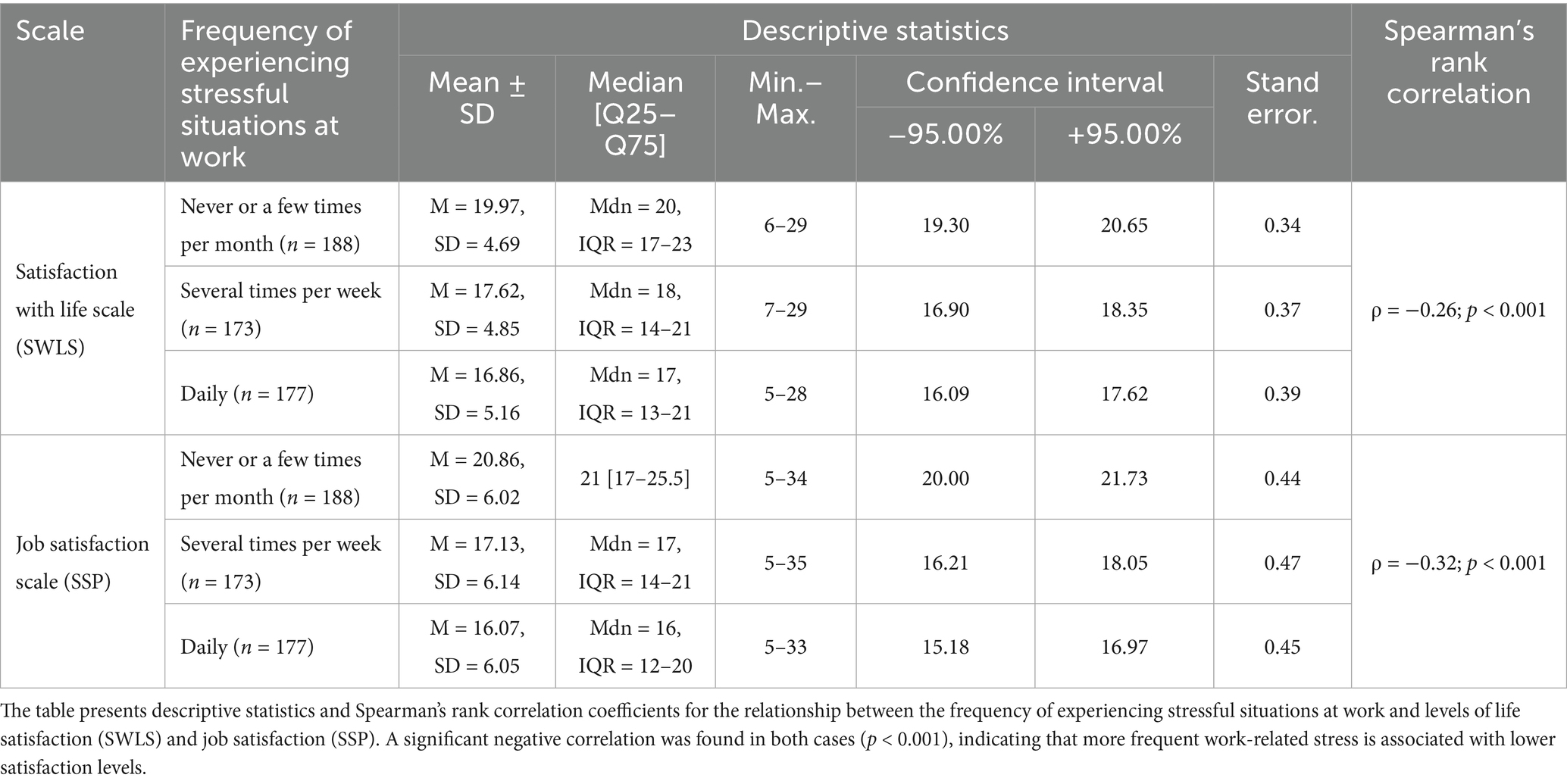
Table 7. Relationship between frequency of experiencing work-related stress and levels of life and job satisfaction (n = 538).
4.5 Predictors of psychological functioning—regression analysis
Multiple linear regression models were constructed to identify predictors of depression, anxiety, and symptoms. Total scores from the SWLS and SSP were included as independent variables in each model. All three models reached statistical significance (p < 0.001). The highest explanatory power was observed in the depression model (R2 = 0.452), followed by anxiety (R2 = 0.324) and (R2 = 0.237). Regression results are summarized in Table 8.
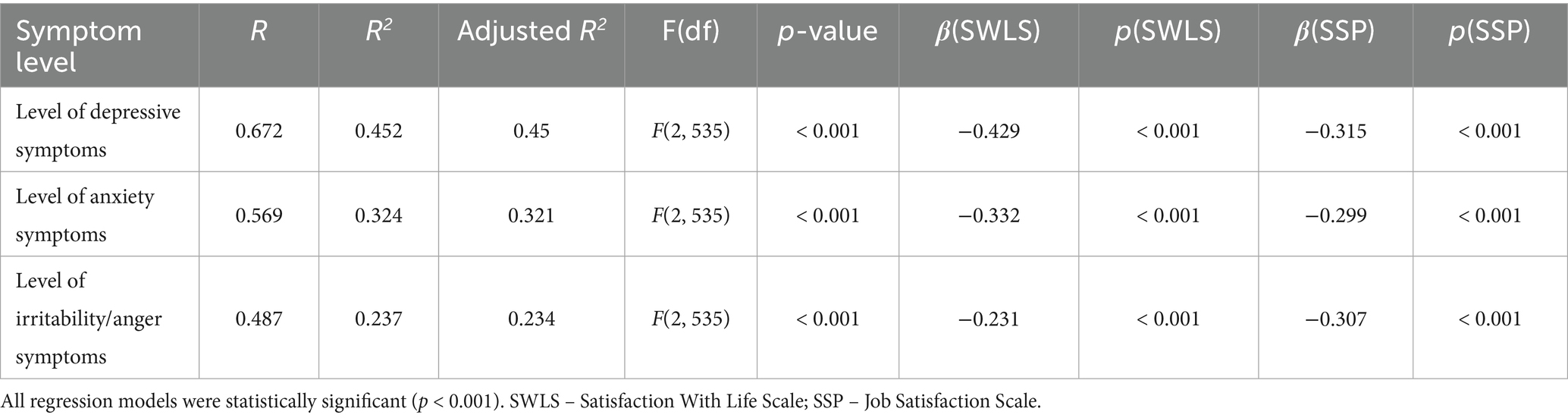
Table 8. Multiple regression models predicting depression, anxiety, and irritability/anger symptoms (n = 538).
4.6 Reliability of measurement instruments
Internal consistency of the applied scales was assessed using Cronbach’s alpha. The HADS subscales yielded the following values: HADS-Anxiety (α = 0.868; after removing item 7), HADS-Depression (α = 0.863), and HADS-Anger subscale (α = 0.813). The Satisfaction with Life Scale (SWLS) reached α = 0.86, and the Job Satisfaction Scale (SSP) α = 0.89. These values indicate high psychometric reliability. Reliability coefficients are presented in Table 9.
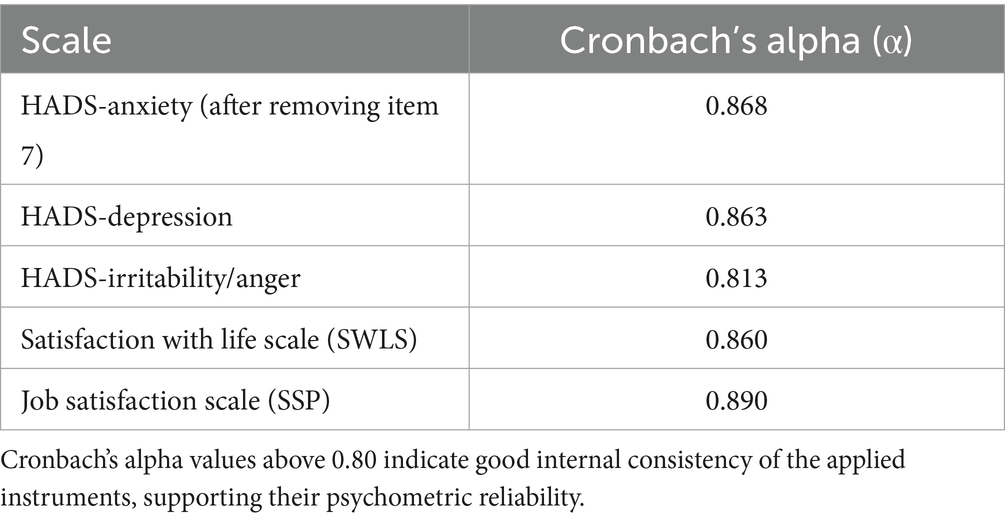
Table 9. Internal consistency (Cronbach’s alpha) of the applied scales.
4.7 Ethical considerations
All participants provided informed consent. According to national regulations and institutional policies, ethical approval was not required for this type of non-interventional, anonymous online survey.
5 Discussion
The findings of this study allow for a multidimensional analysis of the severity of depression, anxiety, and irritability/anger symptoms among nurses, as well as their relationship with job and life satisfaction. The nursing profession is associated with substantial physical and mental burdens. Occupational stress—resulting from interactions with patients and their families, staffing shortages, shift work, and interpersonal dynamics—is a constant element of nurses’ professional reality. These factors promote the development of intensified anxiety and depressive symptoms, driven by prolonged emotional strain, a sense of helplessness, and exposure to death and suffering.
A high prevalence of anxiety among nurses has been confirmed in previous studies. For instance, Sharif et al. (61) reported that 89.7% of respondents experienced anxiety, with 73% describing it as moderate or severe. These data are consistent with the current findings, where 12.45% of nurses experienced anxiety daily, 28.07% several times per week, and 39.96% several times per month. Similarly, Huang et al. (11) indicated that longer work experience may increase the risk of anxiety disorders, while Maharaj et al. (62) reported symptoms in 41.2% of nurses.
Depression, one of the most common mental disorders, also affects nursing personnel. Constant exposure to illness, death, and clinical responsibility may lead to chronic mood deterioration. In this study, 6% of participants reported experiencing depressive symptoms daily, 26.39% very frequently, and nearly half (49.07%) declared sporadic symptoms. Anxiety and depression are currently among the most frequently diagnosed mental health conditions (63). According to the World Health Organization, nurses are particularly vulnerable to the negative effects of occupational stress (24). This is supported by Angermeyer et al. (64), who found a high prevalence of anxiety, depression, and fatigue among nurses. Wang et al. (65) also emphasized that workplace-related factors significantly influence the development of psychopathological symptoms.
International studies have reported that the prevalence of anxiety and depressive symptoms among nurses ranges from 11 to 80%, depending on the country and methodology (62). In our study, 34.76% met the HADS-M clinical cut-off for depressive symptoms and 24.91% met the clinical cut-off for anxiety symptoms, which is consistent with the mid-to-upper range of prior estimates.
Shift work, performed by 72.49% of participants, has been identified as a factor that disrupts circadian rhythms and burdens mental health. Several studies [e.g., Maharaj et al. (62), Cheung et al. (66), Sharif et al. (61), and Motta de Vasconcelos et al. (67)] have demonstrated a relationship between shift work and depression. Additionally, a lack of social support and emotional connections can increase the risk of mood disorders (65, 67).
In light of the above findings, implementing preventive programs and psychological interventions in the workplace appears justified. Literature suggests that mindfulness-based interventions may help enhance psychological resilience and reduce stress (68).
Irritability/anger symptoms, frustration, and emotional aggression—both internalized and externally expressed—also warrant attention. Only 12.83% of respondents in this study reported an absence of such emotions. The most commonly reported frequency of anger was several times per month (44.61%).
These findings are consistent with those of Wyderka and Niedzielska (69), who found that 40% of nurses had difficulties with emotional regulation. Cheung et al. (66) noted that nurses are more likely to experience emotional aggression than other professional groups. Mosiołek et al. (70) reported that 66.7% of respondents had experienced verbal aggression and 50% had experienced physical aggression from patients.
The impact of emotional overload on nurses’ mental health is therefore significant. In terms of occupational satisfaction, only 5.57% of participants described their job as fully satisfying, while more than half (58.18%) reported varying degrees of dissatisfaction.
Nonetheless, 44.61% of respondents indicated they would choose the nursing profession again. In a study by Ostrowicka et al. (71), only 5% of participants reported a complete lack of job satisfaction. Factors influencing satisfaction included workplace relationships, employment stability, and working conditions.
Kunecka (72) and Gawęda et al. (73) have emphasized that a positive team atmosphere and a sense of meaning in work enhance job satisfaction. Lubrańska (74) found a strong correlation between job satisfaction and life satisfaction. Siemiginowska et al. (75) and Mroczkowska et al. (76) highlighted that shift work intensifies work–life conflict, although it does not always directly reduce overall satisfaction.
In summary, our findings confirm that nurses’ psychological well-being is strongly influenced by working conditions, interpersonal relationships, and workplace organization. Therefore, healthcare facility administrators should implement comprehensive strategies to promote the mental health of nursing personnel. Particular emphasis should be placed on improving the work environment, reducing occupational stressors, and preventing workplace phenomena such as bullying. Proper interventions may help reduce symptoms of anxiety and depression, and anger symptoms, thereby enhancing occupational well-being.
5.1 Limitations of the study
Despite the statistically significant findings, this study has several limitations that must be considered when interpreting and generalizing the results.
First, the use of purposive sampling and an online survey format may have influenced the sample structure. The study primarily included individuals active on social media, potentially excluding participants less familiar with digital technologies. It is also possible that the sample was overrepresented by individuals more motivated to share emotional experiences, as evidenced by a higher proportion of older respondents with longer work experience.
Second, the cross-sectional design of the study does not allow for causal inferences. The results reflect co-occurring variables at a single point in time, without the possibility of assessing their temporal dynamics. Moreover, although standardized and validated self-report tools were used, there remains a risk of subjectivity, anchoring bias, or socially desirable responses.
It is also important to note that the study focused exclusively on nurses working in Poland. Thus, caution should be exercised when attempting to generalize these findings to other professional or international populations that may operate under different systemic conditions. We did not collect province/voivodeship, formal specialty status, or job grade (e.g., ward/charge vs. staff), which limits geographic and professional subgroup analyses.
Nevertheless, this study provides a valuable contribution to understanding the mental health, well-being, and working conditions of nurses, and underscores the need for further research in this field.
6 Conclusion
Nurses experience considerable psychological burden, which contributes to the intensification of depressive, anxiety, and irritability/anger symptoms, as well as a reduction in life and job satisfaction. The most significant factors negatively affecting their well-being include shift work, excessive workload, lack of organizational support, and frequent exposure to stressful situations.
The results revealed statistically significant associations: the more intense the emotional symptoms, the lower the levels of life and job satisfaction. This highlights the critical role of working conditions and interpersonal relationships in maintaining the mental health of this professional group.
The findings emphasize the need to implement strategies that support the mental health of nursing personnel. These include emotional aggression prevention, the development of psychoeducational programs, and organizational changes aimed at reducing occupational stress. Ensuring the psychological well-being of nursing teams may not only improve the quality of patient care but also enhance the overall functioning of the healthcare system.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The study was conducted strictly in accordance with the 1975 Declaration of Helsinki (revised in 2013) (33). Informed consent was obtained from all participants, and their anonymity was assured throughout the study. Participants were informed about the purpose of the study and were assured that they could withdraw from participation at any stage, without any consequences. It is worth noting that according to local regulations and institutional guidelines, non-interventional survey-based research that does not involve sensitive personal data or direct health interventions usually does not require approval from a bioethics committee. This type of research does not meet the definition of a medical experiment under Article 21 of the Law on the Profession of Physician and Dentist of December 5, 1996 (Journal of Laws 2019.537) and does not require the opinion of the Bioethics Committee. Nevertheless, in case of any doubts or the need for additional information, participants have been provided with contact information for further inquiries. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
BS: Conceptualization, Writing – review & editing, Methodology, Project administration. RM: Writing – review & editing, Methodology, Conceptualization. JK: Writing – original draft, Methodology, Conceptualization. BP: Formal analysis, Writing – review & editing. GŻ: Writing – review & editing. AK: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We thank the nurses who participated in the survey and the moderators of professional social-media groups who assisted with study dissemination.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Needleman, J, Liu, J, Shang, J, Larson, EL, and Stone, PW. Association of registered nurse and nursing support staffing with inpatient hospital mortality. BMJ Qual Saf. (2020) 29:10–8. doi: 10.1136/bmjqs-2018-009219
2. Twigg, DE, Whitehead, L, Doleman, G, and El-Zaemey, S. The impact of nurse staffing methodologies on nurse and patient outcomes: a systematic review. J Adv Nurs. (2021) 77:4599–611. doi: 10.1111/jan.14909
3. Naczelna Izba Pielęgniarek i Położnych. Pielęgniarka i położna – zawody deficytowe w polskim systemie ochrony zdrowia. (2022). Warszawa: NIPiP. Available online at: https://nipip.pl/wp-content/uploads/2022/06 (Accessed September 8, 2025).
4. Peplonska, B, Bukowska, A, and Sobala, W. Association of rotating night shift work with BMI and abdominal obesity among nurses and midwives. PLoS One. (2015) 10:e0133761. doi: 10.1371/journal.pone.0133761
5. Berthelsen, M, Pallesen, S, Magerøy, N, Tyssen, R, Bjorvatn, B, Moen, BE, et al. Effects of psychological and social factors in shiftwork on symptoms of anxiety and depression in nurses. J Occup Environ Med. (2015) 57:1127–37. doi: 10.1097/JOM.0000000000000532
6. Kim, JM, and Vasuki, R. The relationship between sleep disorders, job satisfaction, practicing health promoting behavior, quality of life and turnover intention of shift nurses and non-shift nurses. Int J Adv Smart Converg. (2019) 8:58–67. doi: 10.7236/IJASC.2019.8.4.58
7. The WHOQOL Group. The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. (1995) 41:1403–9. doi: 10.1016/0277-9536(95)00112-K
8. Naz, S, Hashmi, AM, and Asif, A. Burnout and quality of life in nurses of a tertiary care hospital in Pakistan. J Pak Med Assoc. (2016) 66:532–6.
9. Li, X, Jiang, T, Sun, J, Shi, L, and Li, J. The relationship between occupational stress, job burnout and quality of life among surgical nurses in Xinjiang. China BMC Nurs. (2021) 20:181. doi: 10.1186/s12912-021-00703-2
10. Dąbrowski, A. Czym są emocje? Prezentacja wieloskładnikowej teorii emocji. Analiza i Egzystencja. (2014) 27:123–46. Available at: https://bazhum.muzhp.pl/media/texts/analiza-i-egzystencja/2014-tom-27/analiza_i_egzystencja-r2014-t27-s123-146.pdf
11. Huang, LC, Wu, MP, Ho, CH, and Wang, JJ. Risks of treated anxiety, depression, and insomnia among nurses: a nationwide longitudinal cohort study. PLoS One. (2018) 13:e0204224. doi: 10.1371/journal.pone.0204224
12. Tsai, K, Lee, TY, and Chung, MH. Insomnia in female nurses: a nationwide retrospective study. Int J Occup Saf Ergon. (2017) 23:127–32. doi: 10.1080/10803548.2016.1248604
13. Portela, LF, Luna, CK, Rotenberg, L, Silva-Costa, A, Toivanen, S, Araujo, T, et al. Job strain and self-reported insomnia symptoms among nurses: what about the influence of emotional demands and social support? Biomed Res Int. (2015) 2015:820610. doi: 10.1155/2015/820610
14. Yazdanshenas Ghazwin, M, Kavian, M, Ahmadloo, M, Jarchi, A, Golchin Javadi, S, Latifi, S, et al. The association between life satisfaction and the extent of depression, anxiety and stress among Iranian nurses: a multicenter survey. Iran J Psychiatry. (2016) 11:120–7.
15. Li, S, Li, L, Zhu, X, Wang, Y, Zhang, J, Zhao, L, et al. Comparison of characteristics of anxiety sensitivity across career stages and its relationship with nursing stress among female nurses in Hunan. China BMJ Open. (2016) 6:e010829. doi: 10.1136/bmjopen-2015-010829
16. Karanikola, MN, Giannakopoulou, M, Kalafati, M, Kaite, CP, Patiraki, E, Mpouzika, M, et al. Anxiety symptoms and quality of interaction among oncology nurses: a correlational, cross-sectional study. Rev Esc Enferm USP. (2016) 50:800–7. doi: 10.1590/s0080-623420160000600013
17. Lin, TC, Lin, HS, Cheng, SF, Wu, LM, and Ou-Yang, MC. Work stress, occupational burnout and depression levels: a clinical study of paediatric intensive care unit nurses in Taiwan. J Clin Nurs. (2016) 25:1120–30. doi: 10.1111/jocn.13119
18. Wang, SM, Lai, CY, Chang, YY, Huang, CY, Zauszniewski, JA, and Yu, CY. The relationships among work stress, resourcefulness, and depression level in psychiatric nurses. Arch Psychiatr Nurs. (2015) 29:64–70. doi: 10.1016/j.apnu.2014.10.002
19. Cheung, T, and Yip, PS. Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int J Environ Res Public Health. (2015) 12:11072–100. doi: 10.3390/ijerph120911072
20. Witczak, I. Zdarzenia niepożądane oraz błędy medyczne występujące w procesach diagnostyczno-terapeutycznych usług zdrowotnych. (2022). Wrocław: Uniwersytet Medyczny. Available online at: https://ppm.umw.edu.pl (Accessed September 8, 2025).
21. Najder, A, and Potocka, A. Psychospołeczne zagrożenia zawodowe i ich związek ze zdrowiem oraz funkcjonowaniem zawodowym pracowników ochrony zdrowia. Pielęgniarstwo Polskie. (2015) 3:313–20. doi: 10.20883/issn.0860-8466
22. Serzysko, B, Podsiadło, B, and Kazimierczak, M. Praca zmianowa a patologie przewodu pokarmowego u pielęgniarek In: Współczesne pielęgniarstwo specjalistyczne. Bytom: Wiedza (2014). 339–47.
23. Serzysko, B, Mroczkowska, R, Ptaszek, G, and Podsiadło, B. Praca zmianowa jako czynnik ryzyka chorób układu krążenia w grupie zawodowej pielęgniarek In: R Mroczkowska and E Molka, editors. Współczesne pielęgniarstwo specjalistyczne, vol. I. Bytom: Wiedza (2014). 179–88.
24. World Health Organization. State of the world’s nursing 2020: Investing in education, jobs and leadership. (2020). Geneva: WHO. Available online at: https://www.who.int/publications/i/item/9789240003279 (Accessed September 8, 2025).
25. Zheng, G, Lyu, X, Pan, L, and Chen, A. The role conflict-burnout-depression link among Chinese female health care and social service providers: the moderating effect of marriage and motherhood. BMC Public Health. (2022) 22:1–13. doi: 10.1186/s12889-022-12641-y
26. Desouky, D, and Allam, H. Occupational stress, anxiety and depression among Egyptian teachers. J Epidemiol Glob Health. (2017) 7:191–8. doi: 10.1016/j.jegh.2017.06.002
27. Niedhammer, I, Malard, L, and Chastang, J-F. Occupational factors and subsequent major depressive and generalized anxiety disorders in the prospective French national SIP study. BMC Public Health. (2015) 15:200. doi: 10.1186/s12889-015-1559-y
28. Nakada, A, Iwasaki, S, Kanchika, M, Nakao, T, Deguchi, Y, Konishi, A, et al. Relationship between depressive symptoms and perceived individual-level occupational stress among Japanese schoolteachers. Ind Health. (2016) 54:396–402. doi: 10.2486/indhealth.2015-0195
29. Fereidouni, Z, Dehghan, A, and Najafi, KM. The prevalence of depression among nurses in Iran: a systematic review and meta-analysis. Int J Med Rev. (2018) 5:163–7. doi: 10.29252/IJMR-050407
30. Hemmati, F, Sarokhani, M, Abdan, Z, Sarokhani, D, Dehkordi, AH, and Fakhri, M. The prevalence of depression, anxiety and stress in nurses working in Iranian hospitals: a systematic review and meta-analysis. Prz Epidemiol. (2021) 75:254–62. doi: 10.32394/pe.75.24
31. Abadi, MBH, Taban, E, Khanjani, N, Konjin, ZN, Khajehnasiri, F, and Samaei, SE. Relationships between job satisfaction and job demand, job control, social support, and depression in Iranian nurses. J Nurs Res. (2021) 29:e143. doi: 10.1097/jnr.0000000000000410
32. Karanikola, MN, Giannakopoulou, M, Mpouzika, M, Kaite, CP, Tsiaousis, GZ, Papathanassoglou, ED, et al. Dysfunctional psychological responses among intensive care unit nurses: a systematic review. Rev Esc Enferm USP. (2015) 49:847–57. doi: 10.1590/S0080-623420150000500020
33. Liu, Y, Aungsuroch, Y, and Yunibhand, J. Job satisfaction in nursing: a concept analysis study. Int Nurs Rev. (2016) 63:84–91. doi: 10.1111/inr.12215
34. Khan, MN, Hamid, S, Hayat, K, Asif, A, Bilal, M, Hameed, MA, et al. Workplace violence and its associated factors among nurses: a cross-sectional study in public hospitals of Punjab. Pakistan BMJ Open. (2022) 12:e052333. doi: 10.1136/bmjopen-2021-052333
35. Al-Ghabeesh, SH, and Qattom, H. Workplace violence against nurses in Jordan. Int Nurs Rev. (2019) 66:151–3. doi: 10.1111/inr.12524
36. Torkaman, M, Afshari-Saleh, L, Rezapour-Nasrabad, R, and Karami, A. Association between anger and job burnout among Iranian nurses: the mediating effect of emotional regulation. J Nurs Manag. (2020) 28:797–803. doi: 10.1111/jonm.12993
37. Lee, YW, Kim, JH, and Lee, SH. Anger expression and its relationship with job stress and burnout among Korean nurses: a cross-sectional study. J Psychiatr Ment Health Nurs. (2019) 26:187–95. doi: 10.1111/jpm.12534
38. Krajewska-Kułak, E, Kułak-Bejda, A, Łukaszuk, C, and Kowalczuk, K. Komunikowanie się z pacjentem agresywnym, roszczeniowym i jego rodziną In: K–K E, A Guzowski, and G Bejda, editors. Kontekst “Inności” w komunikacji interpersonalnej. Białystok: Uniwersytet Medyczny w Białymstoku (2019). 385–95.
39. Demerouti, E, Bakker, AB, Nachreiner, F, and Schaufeli, WB. The job demands-resources model of burnout. J Appl Psychol. (2001) 86:499–512. doi: 10.1037/0021-9010.86.3.499
40. Schaufeli, WB, and Taris, TW. Burnout and work engagement: ten years later. Annu Rev Organ Psychol Organ Behav. (2021) 8:1–25. doi: 10.1111/j.1464-0597.2007.00285.x
41. Karasek, RA. Job demands, job decision latitude, and mental strain: implications for job redesign. Adm Sci Q. (1979) 24:285–308. doi: 10.2307/2392498
42. Negussie, N, and Kaur, G. The Effect of Job Demand–Control–Social Support Model on Nurses’ Job Satisfaction in Specialized Teaching Hospitals, Ethiopia. Ethiop J Health Sci. (2016) 26:311–20. doi: 10.4314/ejhs.v26i4.3
43. Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. (1996) 1:27–41. doi: 10.1037/1076-8998.1.1.27
44. Zhang, X, Zhang, L, Xue, B, Li, Y, Yan, M, Luo, H, et al. Effort–reward imbalance and well-being among psychiatric nurses: the mediating role of burnout and decent work. BMC Nurs. (2024) 23:635. doi: 10.1186/s12912-024-02301-4
45. Baumeister, RF, and Heatherton, TF. Self-regulation failure: an overview. Psychol Inq. (1996) 7:1–15. doi: 10.1207/s15327965pli0701_1
46. Lewczuk, K, Wizła, M, Oleksy, T, and Wyczesany, M. Emotion regulation, effort and fatigue: complex issues worth investigating. Front Psychol. (2022) 13:742557. doi: 10.3389/fpsyg.2022.742557
47. Kim, Y, Lee, E, and Lee, H. Association between anger expression and burnout among nurses during the COVID-19 pandemic: mediating effects of resilience and social support. J Nurs Manag. (2022) 30:724–32. doi: 10.1111/jonm.13544
48. Zheng, R, Zhou, Y, Fu, Y, and He, S. Network analysis of anxiety and depressive symptoms among nurses during the COVID-19 pandemic. J Affect Disord. (2021) 282:33–8. doi: 10.1016/j.jad.2020.12.126
49. Niedhammer, I, Chastang, J-F, David, S, and Kelleher, C. Working conditions and depression in the French national working population: results from the SUMER survey. Int Arch Occup Environ Health. (2021) 94:117–26. doi: 10.1007/s00420-020-01572-2
50. Nakata, A, Irie, M, and Takahashi, M. Work hours, sleep sufficiency, and prevalence of depression among full-time employees. J Clin Psychiatry. (2011) 72:605–14. doi: 10.4088/JCP.10m06397gry
51. Uchmanowicz, I, Rosińczuk, J, Jankowska-Polańska, B, Karniej, P, Lisiak, M, Chudiak, A, et al. Wpływ stresu zawodowego na jakość życia i funkcjonowanie psychiczne pielęgniarek In: I Uchmanowicz, J Rosińczuk, and B Jankowska-Polańska, editors. Badania naukowe w pielęgniarstwie i położnictwie. Wrocław: Continuo (2017). 26–34.
52. Talarowska, M, and Gałecki, P. Zaburzenia afektywne jako efekt przewlekłego stresu zawodowego – przegląd literatury. Farmakoter Psychiatr Neurol. (2018) 34:89–96.
53. Zalewska, AM. Skala satysfakcji z pracy – miara poznawczego aspektu ogólnej satysfakcji z pracy. Acta Univ Lodziensis Folia Psychol. (2003) 7:49–61. Available at: https://bazhum.muzhp.pl/media/texts/acta-universitatis-lodziensis-folia-psychologica/2003-tom-7/acta
54. Diener, E, Emmons, RA, Larsen, RJ, and Griffin, S. The satisfaction with life scale. J Pers Assess. (1985) 49:71–5. doi: 10.1207/s15327752jpa4901_13
55. Zigmond, AS, and Snaith, RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
56. Majkowicz, M.. Praktyczna ocena efektywności opieki paliatywnej—wybrane techniki badawcze. In: K Walden-Gałuszkode and M Majkowicz, editors. Ocena jakości opieki paliatywnej w teorii i praktyce. (2000). Gdańsk: Akademia Medyczna; 21–42.
57. Podwalski, P, Szczygieł, K, Tyburski, E, Samochowiec, A, and Samochowiec, J. Concerns, attitudes and comparison of the COVID-19 epidemic impact on the mental state of medical and nonmedical employees. Psychiatr Pol. (2022) 56:277–88. doi: 10.12740/PP/127006
58. Kozieł, P, Lomper, K, Uchmanowicz, B, and Polański, J. Związek akceptacji choroby oraz lęku i depresji z oceną jakości życia pacjentek z chorobą nowotworową gruczołu piersiowego. Medycyna Paliatywna w Praktyce. (2016) 10:28–36.
59. Juczyński, Z. Narzędzia pomiaru w promocji i psychologii zdrowia. Skala Satysfakcji z Życia. (2001). Warszawa: Pracownia Testów Psychologicznych PTP; 134–138.
60. World Medical Association. WMA declaration of Helsinki—ethical principles for medical research involving human subjects. (2013). Available online at: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (Accessed Sep 8, 2025).
61. Sharif, A, Fallahi Khoshknab, M, Mohammadi, S, Zeraati, M, Jamshidi, Z, Aghabeygi-Arani, M, et al. Depression, anxiety, and stress among Iranian nurses in COVID-19 care wards. BMC Psychol. (2022) 10:205. doi: 10.1186/s40359-022-00911-8
62. Maharaj, S, Lees, T, and Lal, S. Prevalence and risk factors of depression, anxiety, and stress in a cohort of Australian nurses. Int J Environ Res Public Health. (2018) 16:61. doi: 10.3390/ijerph16010061
63. Knudsen, AK, Harvey, SB, Mykletun, A, and Øverland, S. Common mental disorders and long-term sickness absence in a general working population: the Hordaland health study. Acta Psychiatr Scand. (2013) 127:287–97. doi: 10.1111/j.1600-0447.2012.01902.x
64. Angermeyer, MC, Bull, N, Bernert, S, Dietrich, S, and Kopf, A. Burnout of caregivers: a comparison between partners of psychiatric patients and nurses. Arch Psychiatr Nurs. (2006) 20:158–65. doi: 10.1016/j.apnu.2005.12.004
65. Wang, J, Schmitz, N, Smailes, E, Sareen, J, and Patten, S. Workplace characteristics, depression, and health-related presenteeism in a general population sample. J Occup Environ Med. (2010) 52:836–42. doi: 10.1097/JOM.0b013e3181ed3d80
66. Cheung, T, Wong, SY, Wong, KY, Law, LY, Ng, K, Tong, MT, et al. Depression, anxiety and symptoms of stress among Hong Kong nurses: a cross-sectional study. Int J Environ Res Public Health. (2016) 13:779. doi: 10.3390/ijerph13080779
67. Motta de Vasconcelos, E, De Martino, MMF, and de Souza França, SP. Burnout and depressive symptoms in intensive care nurses: relationship analysis. Rev Bras Enferm. (2018) 71:135–41. doi: 10.1590/0034-7167-2016-0019
68. Bae, HJ, Chang, HK, and Eun, Y. The mediating effect of mindfulness in the relationship between self-esteem and burnout among clinical nurses. Korean J Stress Res. (2018) 26:243–9. doi: 10.17547/kjsr.2018.26.3.243
69. Wyderka, IM, and Niedzielska, T. Ergonomia pracy w pielęgniarstwie. Pielęgniarstwo Polskie. (2016) 2:165–9. doi: 10.20883/pielpol.2016.5
70. Mosiołek, A, Gierus, J, Margański, M, Margańska, K, and Szulc, A. Konsekwencje zachowań agresywnych ze strony pacjentów z zaburzeniami psychicznymi dla personelu medycznego. Psychiatria. (2020) 17:23–8. doi: 10.5603/PSYCH.2020.0004
71. Ostrowicka, M, Walewska-Zielecka, B, and Olejniczak, D. Czynniki motywujące i satysfakcja z pracy pielęgniarek w wybranych placówkach publicznej i prywatnej służby zdrowia. Zdrowie Publiczne i Zarządzanie. (2013) 11:191–209. doi: 10.4467/20842627OZ.14.017.1627
72. Kunecka, D. Determinanty satysfakcji zawodowej kadry pielęgniarskiej w Polsce. Zdrowie Publiczne i Zarządzanie. (2018) 14:26–31. doi: 10.4467/20842627OZ.16.004.5566
73. Gawęda, A, Śnieżek, A, and Serzysko, B. Satysfakcja z pracy w opinii badanych pielęgniarek. Pielęgniarstwo i Zdrowie Publiczne. (2018) 8:269–76. doi: 10.17219/pzp/91608
74. Lubrańska, A. Klimat organizacyjny a konflikty ról w perspektywie równowagi praca–życie. Zarządzanie Zasobami Ludzkimi. (2021) 140:65–80. doi: 10.5604/01.3001.0015.0599
75. Siemiginowska, P, Iskra-Golec, I, and Wątroba, J. Relacja praca/rodzina, zadowolenie z pracy i życia oraz zdrowie u pielęgniarek zmianowych i dziennych. Stud Psychol. (2014) VII:138–52. Available at: https://studia-psychologica.uken.krakow.pl/article/view/5607
76. Mroczkowska, R, Piejko, W, and Serzysko, B. Aggressive behavior in the workplace – experiences of young nurses: preliminary study. Med Pr Work Health Saf. (2025) 76:87–99. doi: 10.13075/mp.5893.01538
77. TIBCO Software Inc. Statistica (data analysis software system). Version 13. 2017. Available at: http://statistica.io.
Keywords: nurses, job satisfaction, life satisfaction, anxiety symptoms, depression symptoms, irritability/anger symptoms, mental health, occupational stress
Citation: Serzysko B, Mroczkowska R, Kamińska J, Podsiadło B, Żarczyński G and Krajza A (2025) The relationship of job and life satisfaction with symptoms of anxiety, depression, and irritability/anger in nurses. Front. Public Health. 13:1617148. doi: 10.3389/fpubh.2025.1617148
Edited by:
Federica Vallone, University of Naples Federico II, ItalyReviewed by:
Lambert Zixin Li, National University of Singapore, SingaporeMaria Francesca Cattaneo Della Volta, University of Naples Federico II, Italy
Hadi Khoshab, Bam University of Medical Sciences and Health Services, Iran
Copyright © 2025 Serzysko, Mroczkowska, Kamińska, Podsiadło, Żarczyński and Krajza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bogusława Serzysko, Ym9ndXNpYS5zZXJ6eXNrb0Bwb2N6dGEuZm0=
†ORCID: Bogusława Serzysko, https://orcid.org/0000-0003-0005-4714
Renata Mroczkowska, https://orcid.org/0000-0003-1535-0057
Jolanta Kamińska, https://orcid.org/0000-0002-1297-3454