 LaPrincess C. Brewer1,2*†
LaPrincess C. Brewer1,2*† Mathias Lalika1†
Mathias Lalika1† Ashley N. Kyalwazi3Monica Albertie4Janice Bowie5Ashya Burgess6Lora E. Burke7Brian Buta8Lisa A. Cooper9Deidra C. Crews9Chyke A. Doubeni10Walé Elegbede11,12Jamia Erickson13
Ashley N. Kyalwazi3Monica Albertie4Janice Bowie5Ashya Burgess6Lora E. Burke7Brian Buta8Lisa A. Cooper9Deidra C. Crews9Chyke A. Doubeni10Walé Elegbede11,12Jamia Erickson13 Sarah Jenkins14Jacquelyn Johnson15Clarence Jones16Ashton Krogman1Lainey Moen1Michael Palmer17
Sarah Jenkins14Jacquelyn Johnson15Clarence Jones16Ashton Krogman1Lainey Moen1Michael Palmer17 Christi A. Patten2,18Sumedha Penheiter19Monisha W. Richard20Princess Titus21
Christi A. Patten2,18Sumedha Penheiter19Monisha W. Richard20Princess Titus21 Sueling Schardin22Stanton Shanedling23
Sueling Schardin22Stanton Shanedling23 Jeremy R. Van’t Hof24David Warner2,25Jennifer Weis2
Jeremy R. Van’t Hof24David Warner2,25Jennifer Weis2 Sharonne N. Hayes1
Sharonne N. Hayes1- 1Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, United States
- 2Center for Clinical and Translational Science, Mayo Clinic, Rochester, MN, United States
- 3San Francisco Department of Medicine, University of California, San Francisco, San Francisco, CA, United States
- 4Center for Clinical and Translational Science, Mayo Clinic, Jacksonville, FL, United States
- 5Johns Hopkins Bloomberg, School of Public Health, Baltimore, MD, United States
- 6Division of Hematology, Comprehensive Cancer Center, Mayo Clinic, Rochester, MN, United States
- 7Department of Health and Community Systems, School of Nursing, University of Pittsburgh, Pittsburgh, PA, United States
- 8Division of Geriatric Medicine and Gerontology, Center on Aging and Health, Johns Hopkins University, Baltimore, MD, United States
- 9Department of Medicine, Johns Hopkins University, School of Medicine, Baltimore, MD, United States
- 10Department of Family and Community Medicine, Wexner Medical Center, The Ohio State University, Columbus, OH, United States
- 11Strategy Management Services, Mayo Clinic, Rochester, MN, United States
- 12National Association for the Advancement of Colored People, Rochester, MN, United States
- 13Thrivent Financial, Incorporated, Rochester, MN, United States
- 14Department of Quantitative Health Sciences, Mayo Clinic, Rochester, MN, United States
- 15Christ’s Church of the Jesus Hour, Rochester, MN, United States
- 16Hue-Man Partnership, Minneapolis, MN, United States
- 17Revival Home Health and Hospice, Baltimore, MD, United States
- 18Department of Psychiatry and Psychology, Mayo Clinic College of Medicine, Rochester, MN, United States
- 19Strategy Operations, Mayo Clinic, Rochester, MN, United States
- 20The Linc, Minneapolis, MN, United States
- 21Appetite For Change, Minneapolis, MN, United States
- 22American Heart Association, Eagan, MN, United States
- 23Heart Disease and Stroke Prevention Unit, Minnesota Department of Health, Saint Paul, MN, United States
- 24Cardiovascular Division and Lillehei Heart Institute, University of Minnesota Medical School, Minneapolis, MN, United States
- 25Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, United States
The FAITH! (Fostering African-American Improvement in Total Health) Cardiovascular Health and Wellness Program is more than a decade-long community-based participatory research initiative aimed at addressing cardiovascular health disparities among African-Americans in Minnesota. Founded in 2013, the program employs a culturally tailored, community-driven approach by partnering with African-American faith communities to promote cardiovascular health through education, digital health tools, and multilevel interventions targeting the social determinants of health. Grounded in community-based participatory research principles, FAITH! prioritizes equitable academic-community partnerships, co-learning, community capacity building, and shared ownership in all aspects of research and implementation. The program’s exemplary innovations include the NIH-funded FAITH! Trial, a randomized clinical trial, testing a mobile health intervention (the FAITH! App) co-created with the African-American community, and the Techquity by FAITH! study. Techquity by FAITH! evaluates the effectiveness of a culturally relevant, community-informed mHealth intervention supported by a Digital Health Advocate network to improve overall cardiovascular health and digital health literacy. During its evolution, FAITH! has addressed emergent public health crises, including the COVID-19 pandemic, by adapting programming to provide emergency preparedness resources, health education, and vaccine outreach. Key outcomes include sustainable church-based health ministries, increased research participation, and successful translation of research into practice. The program has also contributed to research workforce development by mentoring and training diverse early-career scholars and community leaders in community-based participatory research and cardiovascular health equity research. Lessons learned highlight the transformative impact of community-based participatory research in building trust, facilitating culturally relevant dissemination, and sustaining health equity initiatives. The FAITH! model demonstrates a scalable, community-led strategy for advancing cardiovascular health in underserved populations and provides a blueprint for future initiatives aiming to reduce racial health disparities.
Introduction
In 2023, the Fostering African-American Improvement in Total Health (FAITH!) Cardiovascular Health (CVH) and Wellness Program celebrated 10 years of successful health promotion among African-Americans in Minnesota. This success was not without challenges, unexpected setbacks and new directions heralded by the unprecedented COVID-19 public health crisis. Nonetheless, the FAITH! founding director and Principal Investigator, Dr. LaPrincess Brewer, a preventive cardiologist and community activist, was guided by committed community partners to hold to the FAITH! Program’s founding mantra to “take care of your body and your spirit.” In doing so, this team aimed to tackle disparities in cardiovascular disease (CVD) through promotion of healthy lifestyle and behavior change, which has led to more than a decade of sustainability.
The FAITH! Program began in 2008 with the early success of a classroom-based chronic disease prevention program spearheaded by Dr. Brewer and peer public health students within New Friendship Baptist Church, an African-American church in East Baltimore, Maryland, near Johns Hopkins Hospital (1). Despite the church’s over 30-year history in Baltimore and location in the “backyard” of Johns Hopkins, New Friendship was never approached for health interventions development partnerships with the prestigious hospital. Dr. Brewer and her fellow public health student classmates worked closely with Rev. Dr. Michael Palmer, their New Friendship community partner, to promote CVH through nutritional education within the church community. By applying the principles of community-based participatory research (CBPR), recognizing the faith community as a unit of identity, this project demonstrates that integrating culture, community values, and health education can promote better lifestyle choices among participants and foster a sustainable “culture of health.” This initial partnership with New Friendship served as a catalyst for larger scale interventions and programming to promote ideal CVH and tackle disparities in CVD among African-Americans in the state of Minnesota.
Context
The (not so) good life in Minnesota: FAITH! origins in Minnesota
Minnesota, the “Land of 10,000 Lakes,” is home to over 5 million individuals and has been consistently recognized for being one of the healthiest states in the United States with glowing perceptions of “The Good Life” reflecting quality of life and ample economic opportunity (2). However, the disproportionate burden of CVD incidence and mortality among African-American individuals in comparison to White individuals living in Minnesota tells a much different and disheartening narrative. African-Americans aged 35–63 years in Minnesota are more than twice as likely to die from CVD than White adults of the same age, in part because of higher rates of CVD risk factors such as diabetes, obesity, and physical inactivity (3). These CVD disparities “Up South” stem from historical contexts of African-American migration from the Deep South to northern regions in optimistic pursuit of opportunities for economic upward mobility (4). Despite migration to Northern states, African-Americans continue to experience high poverty rates, chronic stress from racism and inequality, and health outcomes similar to or worse than those in the South (3, 4).
In 2012, Dr. Brewer relocated to Rochester, Minnesota, for clinical fellowship training in Cardiology at the Mayo Clinic (Mayo) flagship medical center. She quickly recognized the striking racial disparities in CVH, accentuated marginalization of African-Americans in the region, and the potential for integrating FAITH! into medically underserved and socioeconomically disenfranchised communities throughout Minnesota to address systemic health inequities. Addressing these disparities would require a CBPR approach, which is core to the FAITH! Program. This includes community-based interventions, trust-building through shared decision-making, culturally tailored approaches, and equitable, evidence-based strategies to reduce the burden of preventable diseases and improve CVH in African-American populations.
Programmatic elements: applying the CBPR principles
CBPR is a research paradigm which emphasizes community-centric strategies for culturally relevant programs to advance health equity (5). CBPR is an equitable, strength-based approach involving all stakeholders throughout the research process. Table 1 summarizes the efforts of FAITH! and its partners to operationalize CBPR principles (6).
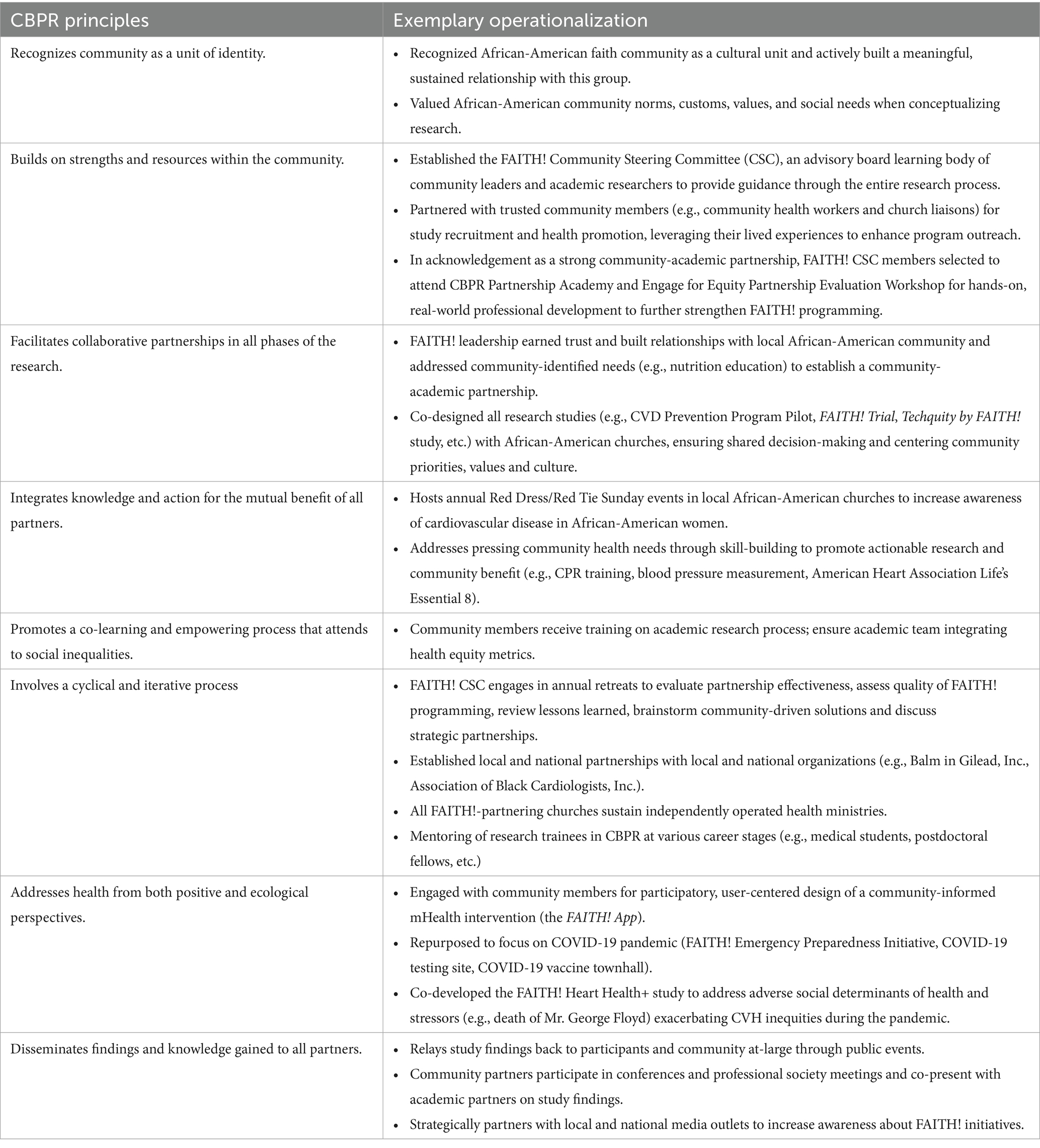
Table 1. Operationalization of the community-based participatory research (CBPR) principles by the FAITH! program.
Principle 1: Recognizing the community as a unit of identity
With a history spanning over five centuries, the “Black Church” is a sacred cultural and societal unit, serving as a haven for religious worship but also a crucible for social support, political activism, education, health/social services, cultural expression and identity (7, 8). Recognizing this crucial role of the Black Church in the lives of many African-Americans, FAITH! intentionally partnered with these institutions from its founding. At the heart of the Black Church are African-American communities which have common norms, customs, and values as well as health and social needs. This also requires an appreciation that the African-American community is not monolithic and a more nuanced understanding of geographical, social and historical contexts is warranted when conceptualizing research (9). FAITH! recognized the multifaceted, distinctive communities by integrating cultural considerations in research, including the co-design of a culturally tailored mobile health lifestyle intervention (the FAITH! App) (10–15) and a Digital Health Equity toolkit for an ongoing study to improve digital literacy among African-Americans (16).
Principle 2: Building on community strengths and resources
One of the core strategies of FAITH! in advancing health equity in African-American communities is to leverage existing community resources and strengths. The FAITH! Community Steering Committee (CSC) was established in 2017 using a rigorous, theory-informed, implementation process with the objective to better engage with the community as true collaborators and partners (17). This 20-member body is comprised of a diverse unification of academic researchers, faith leaders, community strategists, public health representatives, patient advocates, community health workers (CHWs), and other community leaders, which “steers” or guides the program’s activities to ensure that they are community-centered and actionable. Diversity in the group is a vital resource to understanding the myriad of community priorities from multiple perspectives, thus guiding both the studies and community interventions. More importantly, by representing the voices of the communities they belong to and providing valuable insights as a form of “social capital,” this committee plays a key role in building academic-community trust and fostering greater community collaboration. In addition, the CSC serves to identify existing assets (such as health and social programs) and resources (e.g., culturally congruent healthy lifestyle coaches, CHWs, venues, etc.) instrumental to facilitating team-based and implementation science (18) components within all FAITH! projects.
Furthermore, the FAITH! study recruitment efforts are primarily led by African-American community members (e.g., FAITH! Partners, CHWs, etc.), who leverage their lived experiences to promote our studies within their communities and networks. Similarly, these community partners utilize their community mobilization skills (e.g., appropriate locations, timing, activities, etc.) to inform the planning of community events to maximize engagement and participation. Acknowledging the accomplishments of our CBPR partnership, CSC co-leaders (L. B., C. J.) and a CSC member (M. W.) were invited to participate in the Engage for Equity (19) Partnership Evaluation Workshop at the University of New Mexico in January 2019, which convened prominent CBPR partnerships from across the United States for a collaborative learning experience (20, 21).
Principle 3: Facilitating collaborative and equitable partnerships
The foundational activities of FAITH! emphasized community trust-building and equitable partnership. Upon the relocation of Dr. Brewer to Mayo, she approached the Mayo Center for Clinical and Translational Science (CCaTS) to leverage existing community-engaged initiatives and partnerships between Mayo and the surrounding African-American community. At that time there were limited collaborations in place between Mayo and the surrounding African-American community and health disparities research was in its early development. Dr. Brewer initiated a series of activities with select African-American church leaders in Rochester to gauge the interest of pastors in launching FAITH! in Rochester.
First, FAITH! held “listening and transparent communication” meetings with pastors and auxiliary leaders within each church for relationship-building and to gain understanding of the needs and priorities of the African-American community in Rochester (22). The response was mixed: some community leaders were enthusiastic to build a program focused on this historically marginalized African-American population, while others expressed outright disinterest as the program was perceived as a “hit and run” research project wrought by traditional academic power structures.
Dr. Brewer stepped back from the research focus to better understand the concerns of the congregation members. It became apparent that this skepticism stemmed, in part, from limited prior interaction with Mayo, including few opportunities for sustained and meaningful engagement with the African-American community in Rochester. There was also a clear misunderstanding of the research process, particularly surrounding informed consent. Further, reasonable privacy concerns about research data collection and how this information would be used to benefit individuals and the greater good of the community were also expressed. There was a shared sentiment among community members questioning the decision to frame the project as research, as opposed to positioning it as a community-oriented initiative reflecting Mayo’s commitment to giving back. Further meetings were held with community “gatekeepers” within each church and local African-American organizations [e.g., National Association for the Advancement of Colored People (NAACP) leadership] for additional understanding of community assets.
Dr. Brewer and her team also attended church-sponsored worship services and community outreach programming. The team’s initiative of continuing to “show up” helped earn trust and allowed them to become more trustworthy to a community that was marginalized within a city centered around a medical center considered as a global “powerhouse.” With a historical context of distrust in medical research stemming from atrocities involving the federal government [e.g., Tuskegee Study of Syphilis in the Negro Male (23) sponsored by the US Public Health Service] and large medical institutions [e.g., Henrietta Lacks cell line at Johns Hopkins (24, 25)], the FAITH! team prioritized transparent and consistent communication with church congregations, highlighting how this program and its rigorous, community-centric approach would ultimately benefit the community.
In addition, several listening sessions between Mayo team leaders and church members helped foster mutual understanding and strengthen connections between the institution and surrounding African-American communities, which had historically limited engagement with Mayo’s facilities, research, and innovation (26). Notably, some participants shared that, despite living nearby for decades, they had never visited the Mayo campus and had chosen to receive care elsewhere.
To demonstrate its commitment to the community and FAITH!, Mayo partnered with FAITH! to address a community-identified need for nutrition education and healthy food preparation. FAITH! collaborated with the Mayo Dan Abraham Healthy Living Center to host a live cooking demonstration in a state-of-the-art kitchen as a means to acknowledge and respond to the community’s priorities. The culinary team prepared traditional African-American cuisine using healthier and plant-based ingredients to improve the nutritional content. This intentional approach of genuinely welcoming the community into the “ivory tower” was well received and appreciated by the community. Although somewhat of a reversal of “meeting people where they are” in the community, it was a clear display of cultural humility and trust-building.
In 2013, upon establishing a mutual understanding of shared goals and using the CBPR tenets of engagement, several churches in Rochester requested to have FAITH!’s programming as a continued part of their health ministries with a new focus on CVD prevention to address health disparities most affecting their congregations and surrounding communities (22). As an equity-first, power-sharing model, each church identified a church liaison, designated as a FAITH! Partner, to serve as a connector for the church in all research decision-making processes. This marked the official establishment of FAITH! in Rochester. Similar strategies, employing lessons from this process, were used to expand our network of church partners in the Minneapolis-St. Paul metropolitan area. This collaborative formative stage of genuine partnership laid the groundwork for all future research, community-based interventions and outreach implemented by FAITH!. The African-American faith community engaged equally to develop research questions, design studies, recruit participants, collect data, interpret results, and disseminate findings. Figure 1 illustrates a historical timeline of selected CBPR activities and milestones achieved by FAITH! since its founding, using the River of Life (27), a reflective tool that outlines the history of a CBPR partnership and highlights how the progression has influenced the current state of the partnership.
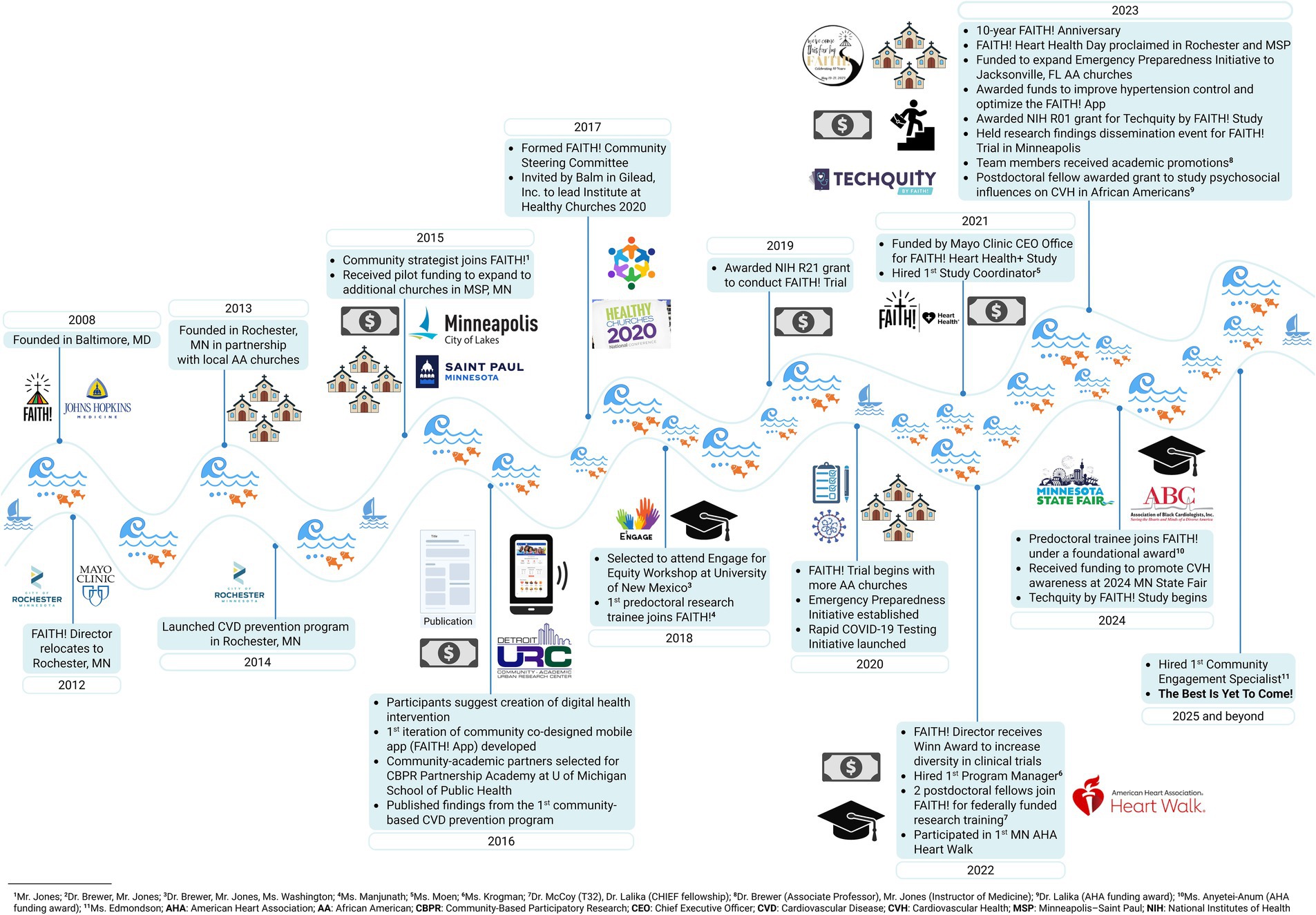
Figure 1. River of life of the FAITH! (Fostering African-American Improvement in Total Health!) program activities and milestones. A historical timeline of selected community-based participatory research activities and milestones achieved by FAITH! since its initial founding in Maryland and expansion to the FAITH! Cardiovascular Health and Wellness Program in Minnesota.
Principle 4: Integrating knowledge and action for mutual benefit
Consistent with its overarching goal of improving CVH among African-Americans as identified and mutually agreed upon by community members, FAITH!’s comprehensive suite of interventions focuses on CVH promotion and CVD prevention. For instance, the rigorously tested FAITH! App is currently being optimized into a smartphone-based application to expand dissemination to other African-American communities beyond Minnesota. In addition, insights from the FAITH! Trial (28) are being utilized to develop not only a commercially viable app but also a tool with advanced technical capabilities to address barriers to research participation among African-Americans. By enabling remote data collection, the app addresses challenges such as unreliable transportation and scheduling conflicts, thus facilitating participation in decentralized clinical trials (29).
Beyond research, FAITH! engages in initiatives to drive social change and raise awareness about community-identified challenges. Our research and dissemination events are complemented by non-research activities, including live cooking demonstrations and fitness classes, such as Zumba and Afro Karibe, to cultivate a community culture that promotes engagement in healthy behaviors. In 2018, the program collaborated with a local YMCA and church community to organize the “Walk by FAITH!” celebration series. This included a heart health fair, a health education presentation by Dr. Brewer, 2-mile walks in Rochester and Minneapolis, and a Men’s Health Symposium (30). In recognition of American Heart Month, FAITH! also hosts annual Red Dress/Red Tie Sunday events (31) within its church networks to increase awareness of CVD in African-American women.
FAITH! also leverages high-profile events to address pressing issues within the African-American community. For example, following NFL athlete, Mr. Damar Hamlin’s public cardiac arrest in 2023, FAITH!, collaborated with the local American Heart Association (AHA) affiliate to sponsor community-wide cardiopulmonary resuscitation and automated external defibrillator training at the Mayo Dan Abraham Healthy Living Center (32, 33). Additionally, FAITH! and its affiliated churches participate annually in the AHA Heart Walk to promote CVH awareness. To further engage with its community partners, FAITH! distributes a quarterly newsletter featuring resources such as internships, scholarships, podcasts, and upcoming seminars (Supplementary document 1). FAITH! also partners with national professional societies, such as the Association of Black Cardiologists, Incorporated (ABC), which has been instrumental in advancing community health advocacy (34) as well as multiple health policy changes and legislature at the federal level, such as Health Inequity and Diversity in Cardiology (35), Access to Care, and Tobacco Control (36).
Principle 5: Promoting co-learning and community empowerment
The founding and expansion of FAITH! has been driven by a bidirectional co-learning process involving academic researchers and community partners/stakeholders. Central to FAITH! is its academic-community co-led study team, which includes the FAITH! founder and principal investigator (L. B.) and a former community engagement director of a federally qualified health center (FQHC) and community strategist and leader of a grassroots organization, Hue-Man Partnership in Minneapolis, Minnesota (C. J.). They were connected in 2015 through the director of the Minnesota Department of Health CVH Unit in St. Paul, Minnesota (S. S.), acknowledging their shared passions in CVD prevention in underserved communities. Seeking avenues to nurture the partnership, the co-leaders were one of 12 academic-community dyads selected to participate in the Detroit Community-Academic Urban Research Center CBPR Partnership Academy in July 2016 (37, 38). The Academy offered a dynamic co-learning environment that integrated formal coursework, hands-on CBPR training, professional development opportunities, and real-world experience to further FAITH!’s mission. The Academy also provided the co-leaders the impetus to form the FAITH! CSC (17). Through applied practice of concepts learned, the FAITH! academic partners learned strategies to authentically and effectively identify community needs through a deeper understanding of the culture and broader social context of the African-American community. This led to studies and interventions designed to effectively address the pressing health needs of the community.
Community partners have also gained insights into complex institutional cultures and processes of academic medical centers by participating in all stages of the research process. As a result, community partners have attained research knowledge and skills by actively partnering in study design, implementation, and dissemination, while holding the research team accountable for integration of health equity metrics. As an exemplar, our community partner co-leader (C. J.) has acquired knowledge, skills, and academic productivity, resulting in successful competitive research awards as a co-investigator and co-author on manuscripts and presentations at scientific meetings (39). Further, he received academic rank as an Instructor of Medicine at Mayo Clinic, a true demonstration of recognition for his contributions to the success of FAITH! and its benefits to the community. In addition, our academic team has prioritized having training sessions with community members to improve their skills for CVH assessment and promotion [e.g., blood pressure measurement, AHA Life’s Essential 8 (40) knowledge] within their communities.
Principle 6: Cyclical and iterative process for long-term sustainability
FAITH! exemplifies the cyclical and iterative nature of CBPR through its sustained partnerships, co-developed interventions, collaborative research process, and commitment to long-term impact and sustainability (41). Through the FAITH! CSC and ongoing capacity-building efforts, the program addresses immediate health needs while empowering local African-American communities to improve long-term health outcomes. For example, through a cyclical and iterative learning process with embedded feedback mechanisms, CSC members participate in an annual retreat to: (1) evaluate partnership effectiveness in addressing health inequities (42), (2) assess FAITH! programming quality, (3) review lessons from FAITH! research advocacy and community outreach, (4) brainstorm community-driven solutions, and (5) discuss strategic partnerships to advance FAITH!’s mission.
For over 10 years, FAITH! demonstrated its commitment to sustainability through its collaborations with African-American churches in Rochester and Minneapolis-St. Paul, community-based organizations (e.g., Hue-Man Partnership, Appetite for Change), national professional societies and foundations (e.g., ABC, AHA, Robert Wood Johnson Foundation) and international faith-based organizations (e.g., The Balm In Gilead, Inc.). By leveraging academic and community resources and earning trust with African-American churches and the communities they serve, FAITH! has built a “from the ground up,” community-owned model for addressing health disparities in this population. All partnering churches now independently sustain health ministries that originated through FAITH!, with many continuing to utilize The Balm in Gilead’s Sunday Morning Health Corner (43) materials for health promotion. In Baltimore, FAITH! facilitated a post-worship service food pantry that continued to operate with sustained community support beyond the duration of the initial program (1).
FAITH! has also demonstrated sustainability through strategic funding, capacity building, and training future community-engaged researchers. Initially funded by Mayo CCaTS pilot grants, the program advanced to securing competitive federal and foundational funding from agencies, including the Centers for Disease Control and Prevention, the National Institutes of Health (NIH)/National Institute on Minority Health and Health Disparities (NIMHD), AHA and Robert Wood Johnson Foundation. One of its largest funding sources was an R01-equivalent supplement awarded in 2023 through the University of Minnesota-Mayo Clinic NIMHD P50 collaborative center grant, Center for Chronic Disease Reduction and Equity Promotion Across Minnesota (C2DREAM). The C2DREAM-funded Techquity by FAITH! study (44) aims to improve digital health literacy and CVH among African-Americans by co-designing a Digital Health Equity toolkit, training Digital Health Advocates with the ABC, and engaging them in a clinical trial to assess a community-informed mHealth intervention to address the digital divide.
To support CBPR capacity building, FAITH! actively trains researchers across career stages, including postbaccalaureate scholars, medical students, and postdoctoral fellows, through prestigious programs such as the Mayo-funded Cardiovascular Health Innovations in Equity (CHIEF) Fellowship and the NIH T32 Postdoctoral Fellowship. Trainees gain hands-on experience through integration into FAITH! activities and intensive CBPR coursework. FAITH! has also been designated as a community outreach opportunity within the Mayo graduate medical training programs (i.e., medical school, Internal Medicine residency, Cardiology fellowship programs). FAITH! trainees have secured competitive research awards (e.g., the AHA Research Supplement to Promote Diversity in Science), presented at national and international conferences, published in high-impact journals, and obtained positions within academia, government and industry (45–52).
Principle 7: Addressing health through social determinants and ecological perspectives
Health disparities in Minnesota are driven by adverse social determinants of health (SDOH) (53), such as lack of home ownership, lower education levels, and income gaps. According to the 2022 Minnesota Poverty Report, poverty rates among African-Americans were nearly three times those of White individuals (54). To address these disparities, FAITH! focuses on CVD prevention in African-Americans through innovative, tailored interventions (e.g., smartphone apps, community webinars, forums, fitness classes, and cooking demonstrations) that “meet people where they are.” FAITH! tailors its studies to better understand and address the effects of socioeconomic disenfranchisement and systemic inequities on CVH, including identifying social needs (e.g., food and housing), stressors (55), sociocultural norms (56–59), and connecting community members to resources through a personalized, web-based referral platform (60).
Originating from community-generated ideas to develop a digital CVH platform, FAITH! conducted iterative pilot studies (11, 22, 61) that informed an NIH/NIMHD-funded, randomized clinical trial, the FAITH! Trial (62). This study tested the efficacy of the community co-created FAITH! App in improving CVH behaviors and clinical factors among African-American individuals (28, 62). The intervention integrated relevant psychosocial influences on CVH and offered practical, culturally appropriate solutions to promote CVH, including social support from peers and community leaders (13, 63–65).
During the COVID-19 pandemic, SDOH inequities (e.g., limited healthcare access) contributed to high infection, hospitalization, and mortality rates among African-Americans in Minnesota (66). In response, FAITH! pivoted and repurposed its research initiatives, with funding from CCaTS and the ABC, to address urgent community needs. In 2020, FAITH! used a CBPR approach to co-design “When Disaster Strikes: Keep Calm and Be Prepared,” an emergency preparedness (EP) initiative for the African-American community in Rochester and Minneapolis-St. Paul (67–69). Informed by a SDOH-based needs assessment, the initiative included a faith-based COVID-19 EP manual, a weekly “FAITH! & COVID-19 Spread the Word!” e-newsletter (Supplementary document 2), and a culturally-tailored social marketing campaign (including the ESSENCE Wellhouse Virtual Summit; Supplementary document 3) (70, 71). Led entirely by the FAITH! CSC COVID-19 Community Task Force, this initiative reached over 100 African-American churches and an estimated 12,000 individuals (now expanded to Jacksonville, Florida churches).
FAITH! also partnered with an FQHC in St. Paul to establish a COVID-19 prevention program and drive-through SARS-CoV-2 specimen collection site in a medically underserved community, when testing sites were largely limited to more affluent areas and home-based testing was unavailable (72). In 10 weeks, over 2,000 community members, including low-income individuals and essential workers, received health education and were tested. FAITH! further studied factors influencing COVID-19 vaccine acceptance among economically marginalized patients in Minnesota (73) as well as pandemic-related, psychosocial hardships among church congregations. To address vaccine hesitancy beyond Minnesota, FAITH! and Mayo Clinic leadership at all three sites (Minnesota, Arizona, Florida) organized a virtual Town Hall to provide comprehensive education on COVID-19 vaccine options (74–76). This event featured Dr. Kizzmekia Corbett, a key NIH researcher in the Moderna vaccine development, and Dr. Pernessa Seele, an immunologist, public health activist, and CEO of The Balm In Gilead, Inc. The event was well-attended, with over 200,000 streams within its first days of airing.
Coinciding with pandemic-related health disparities was the murder of Mr. George Floyd, an African-American man, by police in Minneapolis, which contributed to widespread grief, stress, and adverse mental health challenges among African-Americans (77). Recognizing the compounded impact of the syndemic of the COVID-19 pandemic (78), the death of Floyd, and the resultant civic unrest, FAITH! initiated an ancillary study within an existing randomized clinical trial (62), the FAITH! Heart Health+ Study (79, 92). The study received financial support as part of the greater Mayo anti-racism initiatives and Chief Executive Office’s clinical trials stimulus grants to support community-engaged research. The study investigated the influence of biopsychosocial factors on CVH among African-American Minnesotans previously enrolled in the FAITH! Trial. Preliminary findings from this study show that depressive symptoms, proximity to social unrest, and high effort coping are associated with worse CVH.
Together, these initiatives underscore FAITH!’s holistic social-ecological model and multisector approach to health promotion and research that acknowledges the dynamic and complex interplay between individuals and their immediate familial, social, communal, and broader societal context. This approach has bolstered long-term resilience and preparedness in the face of adversity in the African-American community.
Principle 8: Disseminating findings and knowledge collaboratively
FAITH!’s research is community-centered, prioritizing the translation of findings to benefit the communities that the program serves. In this way, FAITH! is committed to ensuring research outcomes are effectively communicated back to the community. This is achieved through collaborative dissemination efforts, including in-person and virtual events, workshops, and seminars. Beyond publishing findings in peer-reviewed journals, the program organizes annual events to present results in accessible, lay-friendly language. Moreover, abstracts and manuscripts produced by the FAITH! team are co-authored with community partners, who actively contribute to the manuscript preparation process. Community partners also participate in national conferences and professional society meetings (e.g., AHA, American Public Health Association, Academy Health) alongside the academic team that has allowed them a venue to present study findings and engage in discussions with the global research community. Since 2015, FAITH! and Mayo have sponsored community partners to attend and present at the annual Balm in Gilead, Inc. Healthy Churches 2030 conference, including a Mayo-led workshop on enhancing representation of African-Americans in medical research which centered on the FAITH! model of community engagement (80, 81). Furthermore, FAITH! research milestones have received extensive coverage by local and national media outlets (including the oldest Black-owned newspaper in Minnesota, the Minnesota Spokesman Recorder and the Star Tribune) (82–87). This coverage has provided exceptional exposure to increase awareness about FAITH! initiatives and build a positive reputation within the community. In addition, FAITH! maintains an online presence through official social media platforms [e.g., Facebook (88) and X [formerly Twitter] (89)] and a dedicated website (90) to expand its capacity to engage with and disseminate health information to the diverse African-American community.
Discussion
Lessons learned and implications for future sustainability
In its first decade of implementation in Minnesota, FAITH! has gathered significant insights to inform its future work and long-term sustainability. In 2023, FAITH! celebrated 10 years of successful research and community engagement in Minnesota by hosting a weekend of curated events with our partnering churches, collaborators and supporters including a gala and a Sunday worship service. As a commemorative honor, May 20th was declared as FAITH! Heart Health Day in perpetuity by formal proclamations from the mayors of the cities of Rochester, Minneapolis, and St. Paul. This was truly an extraordinary moment for FAITH! and an inflection point of what is yet to come in the future. Since that time, our academic-community partner team and FAITH! collaborative network reflected on its key lessons learned as detailed below.
Building Sustainable Academic-Community Partnerships. Establishing trust requires time, cultural understanding, and academic humility. The iterative process of relationship-building emphasizes consistency and responsiveness to evolving community needs. Addressing pressing community challenges beyond health issues strengthens trust, incentivizes community participation in initiatives and fosters a shared commitment to addressing disparities. Through this partnership, FAITH! and its community partners have co-developed a mission to support actionable research aimed at improving community health, with the ultimate goal of effectively addressing CVH disparities in Minnesota, particularly within African-American communities.
Transformative Power of CBPR Principles. When applied effectively, CBPR principles enable meaningful research by enhancing trust and bridging the divide between health institutions and historically marginalized communities. For example, FAITH!’s longstanding collaboration with African-American church communities contributes to enhanced and trustworthy relationships between Mayo and the local African-American population, as evidenced by increased community engagement and institutional support for community-driven initiatives.
Community-Driven Research Contributions. Community members, when consistently engaged, actively inform every phase of the research process, from question formulation to data interpretation and dissemination of results (91). This participatory approach enhances research relevance and methodological rigor while empowering community members through their direct involvement.
Community-Informed Dissemination. Dissemination activities, such as workshops and seminars, are not merely endpoints but serve as opportunities to gather community input for refining subsequent research and interventions. For instance, feedback directly garnered from dissemination events informed the conception and development of the FAITH! App, which is now one of FAITH!’s signature interventions.
Community Enthusiasm for Research Participation. African-American communities are eager to engage in research that addresses their concerns and honor them as active collaborators in the process. Sustained engagement and transparent communication of findings are critical to fostering and maintaining this interest. For example, during FAITH! dissemination events, community members who had not previously participated in studies expressed interest in joining ongoing and future research efforts, highlighting the role of trust and perceived research value in encouraging participation.
Leveraging Community Resources. Communities possess inherent resources and expertise that can enhance research outcomes. By building trust, community members may openly share strategies to improve recruitment, identify key collaborators, and avoid missteps that could erode trust. For example, consultations with community partners shaped critical revisions to a digital health toolkit central to the ongoing Techquity by FAITH! randomized clinical trial (16).
Ownership as a Sustainability Driver. Long-term sustainability relies on fostering community ownership of research initiatives. When communities perceive research as a tool to address their health needs, their commitment drives the program’s longevity. FAITH!’s approach of addressing community-identified health priorities exemplifies this principle, creating a model that communities can sustain and expand.
Replicating Best Practices for Expansion. Lessons learned in Baltimore and Rochester were successfully adapted for expansion into Minneapolis and St. Paul, demonstrating the scalability of FAITH!’s model. For instance, the EP initiative co-developed by FAITH! with Minnesotan African-American communities during the COVID-19 pandemic now informs public health efforts in other regions of the United States (e.g., Jacksonville, Florida; Jackson, Mississippi; New Orleans, Louisiana).
Necessity of Inclusive Research Practices. Excluding community voices from research risks irrelevance, flawed methodologies, limited impact, and eroded trust. By engaging diverse community stakeholders through CBPR, FAITH! ensures that research questions and findings are relevant and actionable, thus increasing the likelihood of policy translation and systemic change.
These lessons underscore the importance of authentic partnerships, community engagement, and cultural humility in creating sustainable, impactful programs. Continuously integrating these principles positions FAITH! to expand and deepen its reach and impact on health disparities among African-Americans. Specifically, FAITH! continues to embed its interventions within existing community structures such as church-based health ministries, many of which now operate independently using tools and curricula introduced by the program. The FAITH! App is currently undergoing optimization for broader dissemination and commercialization, expanding its reach beyond Minnesota to other African-American communities across the United States. Additionally, the Digital Health Equity toolkit and Digital Health Advocate training model from the Techquity by FAITH! study are designed to be adaptable for other racial/ethnic populations and geographic contexts. By maintaining a flexible, culturally responsive framework grounded in CBPR principles, FAITH! remains well-positioned to be replicated in diverse settings, leveraging local partnerships and resources to address CVH disparities nationwide.
Implementation challenges and adaptive strategies of the FAITH! program
Despite the successes of FAITH!, several challenges emerged throughout its implementation that warrant discussion. Participant recruitment and retention were ongoing obstacles, particularly during the COVID-19 pandemic (28, 60, 62). As public health restrictions limited in-person engagement, recruitment shifted to virtual platforms (28), which reduced opportunities for direct relationship-building, a cornerstone of our community-based participatory approach. Retention was also affected by pandemic-related stressors (60), competing life demands, and digital access barriers, especially among individuals with limited technological proficiency. Integration of community feedback, while foundational to our model, required significant time and resources to ensure that input was meaningfully incorporated into intervention design and implementation. For example, virtual focus groups facilitated continued community involvement during the pandemic, but attendance variability among participants occasionally hindered consistent engagement (65). Moreover, the urgency to address emergent community needs, such as vaccine outreach and emergency preparedness, sometimes delayed research timelines and constrained the scope of real-time intervention refinements. To address these barriers, the program employed flexible enrollment strategies, provided individualized technical assistance, and engaged trusted CHWs and church liaisons to serve as digital health navigators. While these efforts helped mitigate participation challenges, they also highlighted important limitations to scaling the intervention. Moving forward, future studies should prioritize enhanced recruitment infrastructure, hybrid engagement models that combine virtual and in-person components, and directed investments in digital equity. These experiences emphasize the necessity of maintaining adaptable, multimodal engagement approaches and underscore the critical role of digital infrastructure in supporting both the sustainability and scalability of community-based interventions, particularly in the context of public health crises and ongoing structural inequities.
Conclusion
While much work remains to close racial gaps in the CVD burden for African-Americans living in Minnesota, FAITH! provides a compelling model of intentional and authentic deployment of robust, CBPR-focused approaches that are centered on community-identified needs and preferences to address health disparities. Over the last decade, FAITH! has expanded its community partners to include a network of committed churches, stakeholders, and organizations in the state of Minnesota. It has successfully designed and rigorously tested novel, community-driven interventions, establishing a solid evidence base for improving CVH and overall wellness among African-Americans. Ongoing and future efforts will remain steadfast in balancing community stewardship and scholarship as a surefire path to a lasting impact and to advance health equity.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
LCB: Writing – review & editing, Writing – original draft. ML: Writing – original draft, Writing – review & editing. AKy: Writing – review & editing, Writing – original draft. MA: Writing – review & editing. JB: Writing – review & editing. AB: Writing – review & editing. LB: Writing – review & editing. BB: Writing – review & editing. LC: Writing – review & editing. DC: Writing – review & editing. CD: Writing – review & editing. WE: Writing – review & editing. JE: Writing – review & editing. SJ: Writing – review & editing. JJ: Writing – review & editing. CJ: Writing – review & editing. AKr: Writing – review & editing. LM: Writing – review & editing. MP: Writing – review & editing. CP: Writing – review & editing. SP: Writing – review & editing. MR: Writing – review & editing. PT: Writing – review & editing. SuS: Writing – review & editing. StS: Writing – review & editing. JV: Writing – review & editing. DW: Writing – review & editing. JW: Writing – review & editing. SH: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Brewer was supported by the American Heart Association-Amos Medical Faculty Development Program (grant no. 19AMFDP35040005), NIH Building Interdisciplinary Research Careers in Women’s Health (BIRCWH) Scholar Award (grant no. K12 HD065987), American Heart Association Second Century Implementation Science Award (grant no. 23SCISA1144689), NCATS (CTSA grant no. KL2 TR002379), the Bristol-Myers Squibb Foundation, the Centers for Disease Control and Prevention (CDC, grant no. CDC-DP18-1817) and the NIH/NIMHD P50 Center for Chronic Disease Reduction and Equity Promotion Across Minnesota (C2DREAM) Program (grant no. P50MD017342) during the implementation of this work.
Acknowledgments
The authors extend their gratitude to all study participants and partnering church congregations from the Rochester and the Minneapolis–St. Paul, Minnesota metropolitan areas for their support through the years. We thank the FAITH! Community Steering Committee for their unwavering commitment to all FAITH! programming and guidance throughout the community-based participatory research process. We are grateful for the support of the Mayo Clinic Center for Clinical and Translational Science (CCaTS) and Mayo Clinic Chief Executive Office in advancing community-tailored approaches as a part of the overall mission of Mayo Clinic to provide patient-centered care and innovative research. We appreciate the contributions and support from the Mayo Clinic Clinical Research and Trials Unit, Mayo Clinic Square Sports Medicine, Mayo Clinic Dan Abraham Healthy Living Center and Mayo Clinic Heart Rhythm and Physiologic Monitoring Laboratory. Further, the community-academic partnership thanks the Mayo Clinic Media team for promoting and disseminating our work globally. We also acknowledge our local and national community partners including The Balm in Gilead, Incorporated and the Association of Black Cardiologists, Incorporated for their collaboration and commitment to advancing heart health. We are also especially grateful to our academic partners at the University of Minnesota Rasmussen Center for Cardiovascular Disease Prevention and the Johns Hopkins Center for Health Equity for their collaboration and expertise. Finally, we sincerely thank all past and present FAITH! study team members for their invaluable contributions to the growth of FAITH!.
Conflict of interest
JE was employed by company Thrivent Financial Incorporated.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1622237/full#supplementary-material
Abbreviations
ABC, Association of Black Cardiologists, Incorporated; AHA, American Heart Association; CBPR, community-based participatory research; CCaTS, Center for Clinical and Translational Science; CHW, community health workers; CSC, Community Steering Committee; CVD, cardiovascular disease; CVH, cardiovascular health; EP, emergency preparedness; FAITH, Fostering African-American Improvement in Total Health; FQHC, federally qualified health center; Mayo, Mayo Clinic; NAACP, National Association for the Advancement of Colored People; NIH, National Institutes of Health; NIMHD, National Institute on Minority Health and Health Disparities; SDOH, Social determinants of health.
References
1. Buta, B, Brewer, L, Hamlin, DL, Palmer, MW, Bowie, J, and Gielen, A. An innovative faith-based healthy eating program: from class assignment to real-world application of PRECEDE/PROCEED. Health Promot Pract. (2011) 12:867–75. doi: 10.1177/1524839910370424
2. Ehlinger, EP. Breastfeeding and Health Equity in Minnesota: A Call to Action. Minnesota Department of Health (2014). Available online at: https://mnbfc.files.wordpress.com/2013/03/bfdg-health-equity-in-mn-ehlinger.pdf
3. Van't Hof, JR, Duval, S, Luepker, RV, Jones, C, Hayes, SN, Cooper, LA, et al. Association of cardiovascular disease risk factors with sociodemographic characteristics and health beliefs among a community-based sample of African American adults in Minnesota. Mayo Clin Proc. (2022) 97:46–56. doi: 10.1016/j.mayocp.2021.08.027
4. Ferdinand, KC. Cardiovascular disparities up south: the intersection of geography, social determinants, and race. Mayo Clin Proc. (2022) 97:7–9. doi: 10.1016/j.mayocp.2021.11.008
5. Commodore-Mensah, Y, Metlock, FE, and Cooper, LA. Rethinking, reimagining, and reigniting community-engaged research to promote cardiovascular health equity. Circ Cardiovasc Qual Outcomes. (2022) 15:e009519. doi: 10.1161/CIRCOUTCOMES.122.009519
6. Israel, BA, Schulz, AJ, Parker, EA, and Becker, AB. Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health. (1998) 19:173–202.
7. Gates, HL Jr. The Black church: This is our story, this is our Song. New York: Penguin Press (2021).
8. Brewer, LC, and Williams, DR. We’ve come this far by faith: the role of the Black church in public health. Am J Public Health. (2019) 109:385–6. doi: 10.2105/AJPH.2018.304939
9. Brewer, LC, and Joseph, JJ. Not a spectator sport: improving participation of Black patients in cardiovascular clinical trials. Nat Rev Cardiol. (2024) 21:67–8. doi: 10.1038/s41569-023-00978-9
10. Brewer, LC, Jenkins, S, Lackore, K, Johnson, J, Jones, C, Cooper, LA, et al. MHealth intervention promoting cardiovascular health among African-Americans: recruitment and baseline characteristics of a pilot study. JMIR Res Protoc. (2018) 7:e31. doi: 10.2196/resprot.8842
11. Brewer, LC, Kumbamu, A, Smith, C, Jenkins, S, Jones, C, Hayes, SN, et al. A cardiovascular health and wellness mobile health intervention among church-going African Americans: formative evaluation of the FAITH! App. JMIR Form Res. (2020) 4:e21450. doi: 10.2196/21450
12. Brewer, LC, Hayes, SN, Caron, AR, Derby, DA, Breutzman, NS, Wicks, A, et al. Promoting cardiovascular health and wellness among African-Americans: community participatory approach to design an innovative mobile-health intervention. PLoS One. (2019) 14:e0218724. doi: 10.1371/journal.pone.0218724
13. Figueroa, CA, Murayama, H, Amorim, PC, White, A, Quiterio, A, Luo, T, et al. Applying the digital health social justice guide. Front Digit Health. (2022) 4:807886. doi: 10.3389/fdgth.2022.807886
14. Rowland, S, Brewer, LC, and Rosas, LG. Digital health equity - a call to action for clinical and translational scientists. J Clin Transl Sci. (2024) 8:e145. doi: 10.1017/cts.2024.564
15. Powell-Wiley, TM, Brewer, LC, Burke, LE, Hernandez, R, Landsbaugh Kaar, J, Kepper, M, et al. Role of Technology in Promoting Heart Healthy Behavior Change to increase equity in optimal cardiovascular health: a scientific statement from the American Heart Association. Circulation. (2025) 151:e972–85. doi: 10.1161/CIR.0000000000001314
16. National Institutes of Health. RePORTER: Techquity by FAITH!: A cluster randomized controlled trial to assess the efficacy of a community-informed, cardiovascular health promotion mobile hlth intervention with digital health advocate support. (2023). Available online at: https://reporter.nih.gov/search/tMNPJ0EPsU6g3aolWXoDKw/project-details/10891016 (Accessed March 10, 2025).
17. Manjunath, C, Ifelayo, O, Jones, C, Washington, M, Shanedling, S, Williams, J, et al. Addressing cardiovascular health disparities in Minnesota: establishment of a community steering committee by FAITH! (fostering African-American improvement in Total health). Int J Environ Res Public Health. (2019) 16:4144. doi: 10.3390/ijerph16214144
18. Moise, N, Cené, CW, Tabak, RG, Young, DR, Mills, KT, Essien, UR, et al. Leveraging implementation science for cardiovascular health equity: a scientific statement from the American Heart Association. Circulation. (2022) 146:e260–78. doi: 10.1161/CIR.0000000000001096
19. Engage for Equity. Combining knowledge and action for social change. Available online at: https://engageforequity.org/ (Accessed April 4, 2025).
20. Parker, M, Wallerstein, N, Duran, B, Magarati, M, Burgess, E, Sanchez-Youngman, S, et al. Engage for equity: development of community-based participatory research tools. Health Educ Behav. (2020) 47:359–71. doi: 10.1177/1090198120921188
21. Sánchez, V, Sanchez-Youngman, S, Dickson, E, Burgess, E, Haozous, E, Trickett, E, et al. CBPR implementation framework for community-academic partnerships. Am J Community Psychol. (2021) 67:284–96. doi: 10.1002/ajcp.12506
22. Brewer, LC, Balls-Berry, JE, Dean, P, Lackore, K, Jenkins, S, and Hayes, SN. Fostering African-American improvement in total health (FAITH!): an application of the American Heart Association's life's simple 7 among Midwestern African-Americans. J Racial Ethn Health Disparities. (2017) 4:269–81. doi: 10.1007/s40615-016-0226-z
23. U.S. Centers for Disease Control and Prevention. The U.S. Public Health Service untreated syphilis study at Tuskegee (2024) Available online at: https://www.cdc.gov/tuskegee/about/index.html (Accessed March 10, 2025).
24. Beskow, LM. Lessons from HeLa cells: the ethics and policy of biospecimens. Annu Rev Genomics Hum Genet. (2016) 17:395–417. doi: 10.1146/annurev-genom-083115-022536
25. Skloot, R. The immortal life of Henrietta lacks. 1st ed. New York: Crown Publishing Group (2010).
26. Brewer, LC, Morrison, EJ, Balls-Berry, JE, Dean, P, Lackore, K, Jenkins, S, et al. Preventing cardiovascular disease: participant perspectives of the FAITH! Program. J Health Psychol. (2017) 24:1359105317695878. doi: 10.1177/1359105317695878
27. Sanchez-Youngman, S, and Wallerstein, N. Partnership river of life: creating a historical time line In: N Wallerstein, B Duran, JG Oetzel, and M Minkler, editors. Community-based participatory research for health: Advancing social and health equity. 3rd ed. San Francisco, CA: Jossey-Bass (2018). 363–7.
28. Brewer, LC, Jenkins, S, Hayes, SN, Kumbamu, A, Jones, C, Burke, LE, et al. Community-based, cluster-randomized pilot trial of a cardiovascular mobile health intervention: preliminary findings of the FAITH! Trial. Circulation. (2022) 146:175–90. doi: 10.1161/CIRCULATIONAHA.122.059046
29. Harmon, DM, Noseworthy, PA, and Yao, X. The digitization and decentralization of clinical trials. Mayo Clin Proc. (2023) 98:1568–78. doi: 10.1016/j.mayocp.2022.10.001
30. Harmon, S. Black cardiologist celebrates 10 years of stronger hearts and communities. Minnesota: Minnesota spokesman-recorder; (2018). Available online at: https://spokesman-recorder.com/2018/06/22/black-cardiologist-celebrates-10-years-of-stronger-hearts-and-communities/ (Accessed April 30, 2025).
31. KIMT3. Red Dress Red Tie event raises awareness for heart health. (2025). Available online at: https://www.kimt.com/video/red-dress-red-tie-event-raises-awareness-for-heart-health/video_3ff25fd8-8f1a-5759-959b-6966e60ca64e.html (Accessed April 30, 2025).
32. Tollefson, T. (2023). Mayo Clinic hosts public CPR training: KAALTV. Available online at: https://www.kaaltv.com/news/mayo-clinic-hosts-public-cpr-training/.
33. Prondzinski, O. Disparities in CPR, expert weighs in on why the black community needs more training (2023). Available online at: https://www.kttc.com/2023/08/19/disparities-cpr-expert-weighs-why-black-community-needs-more-training/ (Accessed April 30, 2025).
34. Bess, C, Ferdinand, D, Underwood, P, Ivy, D, Albert, MA, Onwuanyi, A, et al. Promoting cardiovascular health equity: Association of Black Cardiologists Practical Model for community-engaged partnerships. J Am Coll Cardiol. (2024) 83:632–6. doi: 10.1016/j.jacc.2023.11.025
35. Kuehn, BM. Association of Black Cardiologists Calls for urgent effort to address health inequity and diversity in cardiology. Circulation. (2020) 142:1106–7. doi: 10.1161/CIRCULATIONAHA.120.050130
36. The Association of Black Cardiologists (ABC). Advocacy. Available online at: https://abcardio.org/advocacy/ (Accessed December 18, 2024).
37. Coombe, CM, Schulz, AJ, Guluma, L, Allen, AJ 3rd, Gray, C, Brakefield-Caldwell, W, et al. Enhancing capacity of community-academic partnerships to achieve health equity: results from the CBPR partnership academy. Health Promot Pract. (2020) 21:552–63. doi: 10.1177/1524839918818830
38. The Detroit Community-Academic Urban Research Center. Detroit urban research center CBPR partnership academy. Available online at: https://www.detroiturc.org/cbpr-partnership-academy.html (Accessed April 4, 2025).
39. Reopell, L, Nolan, TS, Gray, DM, 2nd,, Williams, A, Brewer, LC, et al. Community engagement and clinical trial diversity: navigating barriers and co-designing solutions-a report from the "health equity through diversity" seminar series. PLoS One. (2023) 18:e0281940. doi: 10.1371/journal.pone.0281940
40. Lloyd-Jones, DM, Allen, NB, Anderson, CAM, Black, T, Brewer, LC, Foraker, RE, et al. Life's essential 8: updating and enhancing the American Heart Association's construct of cardiovascular health: a presidential advisory from the American Heart Association. Circulation. (2022) 146:e18–43. doi: 10.1161/CIR.0000000000001078
41. Breathett, K, and Manning, KD. Catalyzing restructure of a broken health care system. Circ Cardiovasc Qual Outcomes. (2024) 17:e010009. doi: 10.1161/CIRCOUTCOMES.123.010009
42. Ward, M, Schulz, AJ, Israel, BA, Rice, K, Martenies, SE, and Markarian, E. A conceptual framework for evaluating health equity promotion within community-based participatory research partnerships. Eval Program Plann. (2018) 70:25–34. doi: 10.1016/j.evalprogplan.2018.04.014
43. Balm In Gilead. Sunday morning health corner. Available online at: https://www.balmingilead.org/smhc/ (Accessed April 7, 2025).
44. Center for Chronic Disease Reduction and Equity Promotion Across Minnesota. Project 5: Techquity by FAITH!. (2023) Available online at: https://www.mnc2dream.org/projects/project5 (Accessed April 7, 2025).
45. Center for Chronic Disease Reduction and Equity Promotion Across Minnesota. Congratulations Mathias Lalika, MD, MPH. (2024). Available online at: https://www.mnc2dream.org/news/congratulations-dr-mathias-lalika-md-mph (Accessed April 7, 2025).
46. American College of Physicians. (2022). MN-ACP Abstract Award: Medical Student Research/QI. Available online at: https://www.acponline.org/about-acp/chapters-regions/united-states/minnesota-chapter/news-meetings/minnesota-governors-newsletter-may-2022 (Accessed April 30, 2025).
47. Tadese, K, Jenkins, S, Aycock, D, Jones, C, Hayes, SN, Burke, LE, et al. Factors facilitating academic-community research partnerships with African American churches: recruitment process for a community-based, cluster randomized controlled trial during the COVID-19 pandemic. Health Promot Pract. (2022) 25:15248399221118394. doi: 10.1177/15248399221118394
48. Kyalwazi, AN, Loccoh, EC, Brewer, LC, Ofili, EO, Xu, J, Song, Y, et al. Disparities in cardiovascular mortality between Black and White adults in the United States, 1999 to 2019. Circulation. (2022) 146:211–28. doi: 10.1161/CIRCULATIONAHA.122.060199
49. Harmon, DM, Adedinsewo, D, Van't Hof, JR, Johnson, M, Hayes, SN, Lopez-Jimenez, F, et al. Community-based participatory research application of an artificial intelligence-enhanced electrocardiogram for cardiovascular disease screening: a FAITH! Trial ancillary study. Am J Prev Cardiol. (2022) 12:100431. doi: 10.1016/j.ajpc.2022.100431
50. Thomas, VE, Metlock, FE, Hines, AL, Commodore-Mensah, Y, and Brewer, LC. Community-based interventions to address disparities in cardiometabolic diseases among minoritized racial and ethnic groups. Curr Atheroscler Rep. (2023) 25:467–77. doi: 10.1007/s11883-023-01119-w
51. Haynes, N, Kaur, A, Swain, J, Joseph, JJ, and Brewer, LC. Community-based participatory research to improve cardiovascular health among US racial and ethnic minority groups. Curr Epidemiol Rep. (2022) 9:212–21. doi: 10.1007/s40471-022-00298-5
52. Doran, C. (2023) Science Saturday: Can AI-enhanced heart screening address health disparities? Available online at: https://newsnetwork.mayoclinic.org/discussion/science-saturday-can-ai-enhanced-heart-screening-address-health-disparities/ (Accessed April 30, 2025).
53. Powell-Wiley, TM, Baumer, Y, Baah, FO, Baez, AS, Farmer, N, Mahlobo, CT, et al. Social determinants of cardiovascular disease. Circ Res. (2022) 130:782–99. doi: 10.1161/CIRCRESAHA.121.319811
54. Minnesota Department of Employment and Economic Development. Minnesota Disparities by Race Report: Minnesota Economic Disparities by Race and Origin (2022) Available online at: https://mn.gov/deed/assets/24-02MN_tcm1045-435939.pdf
55. Brewer, LC, Redmond, N, Slusser, JP, Scott, CG, Chamberlain, AM, Djousse, L, et al. Stress and achievement of cardiovascular health metrics: the American Heart Association life's simple 7 in blacks of the Jackson heart study. J Am Heart Assoc. (2018) 7:e008855. doi: 10.1161/JAHA.118.008855
56. Kyalwazi, AN, Woods-Giscombe, CL, Johnson, MP, Jones, C, Hayes, SN, Cooper, LA, et al. Associations between the superwoman Schema, stress, and cardiovascular health among African-American women. Ann Behav Med. (2024) 58:863–8. doi: 10.1093/abm/kaae047
57. Cyriac, J, Jenkins, S, Patten, CA, Hayes, SN, Jones, C, Cooper, LA, et al. Improvements in diet and physical activity-related psychosocial factors among African Americans using a Mobile health lifestyle intervention to promote cardiovascular health: the FAITH! (fostering African American improvement in Total health) app pilot study. JMIR Mhealth Uhealth. (2021) 9:e28024. doi: 10.2196/28024
58. Brewer, LC, Bowie, J, Slusser, JP, Scott, CG, Cooper, LA, Hayes, SN, et al. Religiosity/spirituality and cardiovascular health: the American Heart Association life's simple 7 in African Americans of the Jackson heart study. J Am Heart Assoc. (2022) 11:e024974. doi: 10.1161/JAHA.121.024974
59. Manjunath, C, Jenkins, SM, Phelan, S, Breitkopf, CR, Hayes, SN, Cooper, LA, et al. Association of body image dissatisfaction, behavioral responses for healthy eating, and cardiovascular health in African-American women with overweight or obesity: a preliminary study. Am J Prev Cardiol. (2021) 8:100254. doi: 10.1016/j.ajpc.2021.100254
60. Brewer, LC, Jones, C, Slusser, JP, Pasha, M, Lalika, M, Chacon, M, et al. Mhealth intervention for promoting hypertension self-management among African American patients receiving care at a community health center: formative evaluation of the FAITH! Hypertension app. JMIR Form Res. (2023) 7:e45061. doi: 10.2196/45061
61. Brewer, LC, Hayes, SN, Jenkins, SM, Lackore, KA, Breitkopf, CR, Cooper, LA, et al. Improving cardiovascular health among African-Americans through Mobile health: the FAITH! App pilot study. J Gen Intern Med. (2019) 34:1376–8. doi: 10.1007/s11606-019-04936-5
62. Brewer, LC, Jenkins, S, Hayes, SN, Kumbamu, A, Jones, C, Burke, LE, et al. Community-based, cluster-randomized pilot trial of a cardiovascular mHealth intervention: rationale, design, and baseline findings of the FAITH! Trial. Am Heart J. (2022) 247:1–14. doi: 10.1016/j.ahj.2022.01.009
63. Brewer, LC, Fortuna, KL, Jones, C, Walker, R, Hayes, SN, Patten, CA, et al. Back to the future: achieving health equity through health informatics and digital health. JMIR Mhealth Uhealth. (2020) 8:e14512. doi: 10.2196/14512
64. Lalika, M, Jenkins, S, Hayes, SN, Jones, C, Burke, LE, Cooper, LA, et al. Efficacy of a culturally tailored mobile health lifestyle intervention on cardiovascular health among African Americans with preexisting risk factors: the FAITH! Trial. Digit Health. (2024) 10:20552076241295305. doi: 10.1177/20552076241295305
65. Brewer, LC, Cyriac, J, Kumbamu, A, Burke, LE, Jenkins, S, Hayes, SN, et al. Sign of the times: community engagement to refine a cardiovascular mHealth intervention through a virtual focus group series during the COVID-19 pandemic. Digit Health. (2022) 8:20552076221110537. doi: 10.1177/20552076221110537
66. Minnesota Department of Health. Case & Variant Data: COVID-19 Situation Update. Available online at: https://www.health.mn.gov/diseases/coronavirus/stats/case.html (Accessed December 18, 2024).
67. Brewer, LC, Asiedu, GB, Jones, C, Richard, M, Erickson, J, Weis, J, et al. Emergency preparedness and risk communication among African American churches: leveraging a community-based participatory research partnership COVID-19 initiative. Prev Chronic Dis. (2020) 17:E158. doi: 10.5888/pcd17.200408
68. Lalika, M, Salinas, M, Asiedu, GB, Jones, C, Richard, M, Erickson, J, et al. Perspectives of African American church leaders in response to COVID-19 emergency preparedness and risk communication efforts within a community engaged research partnership: COVID-19 emergency risk communication. Disaster Med Public Health Prep. (2023) 17:e532. doi: 10.1017/dmp.2023.182
69. Powell, B. Black churches become important centers for community COVID-19 information. (2020) Available online at: https://kstp.com/health-medical/coronavirus/black-churches-become-important-centers-for-community-covid-19-information/ (Accessed April 30, 2025).
70. Minnesota Spokesman-Recorder. Mayo’s Dr. LaPrincess Brewer to appear on essence COVID-19 summit to address health disparities. (2020) Available online at: https://spokesman-recorder.com/2020/05/06/mayos-dr-laprincess-brewer-to-appear-on-essence-covid-19-summit-to-address-health-disparities/ (Accessed April 30, 2025).
71. FAITH!. 10 Commandments for a Healthy Heart During the COVID-19 Pandemic. (2020) Available online at: https://abcardio.org/wp-content/uploads/2021/04/10-Commandments-for-Healthy-Heart-During-COVID-19-DRBREWER-11-18-2020.pdf] (Accessed April 30, 2025).
72. Brewer, LC, Woods, C, Patel, A, Weis, J, Jones, C, Abbenyi, A, et al. Establishing a SARS-CoV-2 (COVID-19) drive-through collection site: a community-based participatory research partnership with a federally qualified health center. Am J Public Health. (2021) 111:658–62. doi: 10.2105/AJPH.2020.306097
73. Lalika, M, Woods, C, Patel, A, Scott, C, Lee, A, Weis, J, et al. Factors associated with COVID-19 vaccine acceptance among patients receiving Care at a Federally Qualified Health Center. J Prim Care Community Health. (2023) 14:21501319231181881. doi: 10.1177/21501319231181881
74. Mayo Foundation for Medical Education and Research. (Mis)trust in the COVID-19 Vaccine in the African American Community. (2021) Available online at: https://content.govdelivery.com/attachments/MNMDH/2021/08/27/file_attachments/1917692/Mayo%20Clinic%20%28Mis%29trust%20in%20the%20COVID-19%20Vaccine%20in%20the%20African%20American%20Community%20%28FLYER%29.pdf] (Accessed April 30, 2025).
75. American Caregiver Association. Virtual public forum: (Mis)trust in the COVID-19 vaccine in the African American community. (2021) Available online at: https://americancaregiverassociation.org/virtual-public-forum-mistrust-in-the-covid-19-vaccine-in-the-african-american-community/ (Accessed April 30, 2025).
76. Minnesota Spokesman-Recorder. Mayo Clinic hosts webinar on COVID, Black community, and vaccinations. (2021) Available online at: https://spokesman-recorder.com/2021/08/25/mayo-clinic-hosts-webinar-on-covid-black-community-and-vaccinations/ (Accessed April 30, 2025).
77. Santaularia, NJ, Larson, R, Robertson, CE, and Uggen, C. The mental health consequences of George Floyd's murder in Minneapolis in Black, Latine, and White communities. Am J Epidemiol. (2024). 194, 1900–1908. doi: 10.1093/aje/kwae359
78. Bulled, N, and Singer, M. Conceptualizing COVID-19 syndemics: a scoping review. J Multimorb Comorb. (2024) 14:26335565241249835. doi: 10.1177/26335565241249835
79. Lalika, M, McCoy, CR, Jones, C, Bancos, I, Cooper, LA, Hayes, SN, et al. Rationale, design, and participant characteristics of the FAITH! Heart health+ study: an exploration of the influence of the social determinants of health, stress, and structural racism on African American cardiovascular health. Contemp Clin Trials. (2024) 143:107600. doi: 10.1016/j.cct.2024.107600
80. Brewer, LC, Pasha, M, Seele, P, Penheiter, S, White, R, Willis, F, et al. Overcoming historical barriers: enhancing positive perceptions of medical research among African Americans through a conference-based workshop. J Gen Intern Med. (2021) 36:2547–54. doi: 10.1007/s11606-021-06736-2
81. Pullins, CT, Seele, PC, White, RO, Willis, FB, Poole, K, Albertie, ML, et al. Health behaviors and preventive healthcare utilization among African-American attendees at a faith-based public health conference: healthy churches 2020. J Relig Health. (2018) 57:2538–51. doi: 10.1007/s10943-018-0667-2
82. Kiene, T. (2024) Techquity by FAITH! study: Bridging the digital health divide. Available online at: http://spokesman-recorder.com/2024/02/26/bridging-the-racial-gap-in-healthcare-a-new-study-investigates-digital-access/ (Accessed April 7, 2025).
83. Berg, E. (2024) Rochester Celebrates FAITH! Heart Health Day. Available online at: https://www.kimt.com/news/rochester-celebrates-faith-heart-health-day/article_659351ce-16fd-11ef-85e4-63aa4de936e4.html (Accessed April 7, 2025).
84. Min, E. (2025) ‘Red Dress & Red Tie Sunday’: Mayo Clinic cardiologist shares importance of heart health. Available online at: https://www.kttc.com/2025/02/09/red-dress-red-tie-sunday-mayo-clinic-cardiologist-shares-importance-heart-health/ (Accessed April 7, 2025).
85. Eldred, SM. Mayo study shows better health outcomes for religiously active Black Minnesotans. (2022) Available online at: https://www.startribune.com/mayo-study-shows-better-health-outcomes-for-religiously-active-black-minnesotans/600209850 (Accessed April 30, 2025).
86. Cardionerds. 131. Narratives in Cardiology: Health Equity, Community Based Participatory Research, & Underrepresented Minority Women Physician-Scientists with Dr. LaPrincess Brewer. (2021) Available online at: https://www.cardionerds.com/131-health-equity-community-based-participatory-research-underrepresented-minority-women-physician-scientists-with-dr-laprincess-brewer/] (Accessed April 30, 2025).
87. FITsOnTheGO. Dr. LaPrincess Brewer and Dr. Tasha Phillips-Wilson on FAITH Trial/Community Health. (2024) Available online at: https://www.youtube.com/watch?v=bmE12OBbXQc (Accessed April 30, 2025).
88. FAITH!. FAITH cardiovascular health & wellness program. Available online at: https://www.facebook.com/FAITH4Heart/ (Accessed April 30, 2025).
89. FAITH!. FAITH! Cardiovascular health & wellness program. Available online at: https://x.com/FAITH4Heart (Accessed April 30, 2025).
90. FAITH!. FAITH! Cardiovascular Health & Wellness Program. Available online at: FAITH4Heart.com (Accessed April 30, 2025).
91. Mackenzie, IS, Brewer, LC, and Zhavoronkov, A. Clinical trials reimagined: integrating community engagement and artificial intelligence. Fortschr Med. (2025) 6:100743. doi: 10.1016/j.medj.2025.100743
92. Ortiz, R, Joseph, J, Johnson, MP, Moen, L, Lalika, M, Jones, C, et al. A community-engaged approach for assessment of cortisol dynamic range and multi-level chronic stress in African Americans: the FAITH! heart health+ ancillary study. J Particip Med. 69604 (forthcoming/in press). doi: 10.2196/69604
Keywords: cardiovascular health, community-based participatory research, health disparities, health equity, social determinants of health
Citation: Brewer LC, Lalika M, Kyalwazi AN, Albertie M, Bowie J, Burgess A, Burke LE, Buta B, Cooper LA, Crews DC, Doubeni CA, Elegbede W, Erickson J, Jenkins S, Johnson J, Jones C, Krogman A, Moen L, Palmer M, Patten CA, Penheiter S, Richard MW, Titus P, Schardin S, Shanedling S, Van’t Hof JR, Warner D, Weis J and Hayes SN (2025) Community-based participatory design of a decade: the FAITH! Cardiovascular Health and Wellness Program. Front. Public Health. 13:1622237. doi: 10.3389/fpubh.2025.1622237
Edited by:
Buket Akinci, Biruni University, TürkiyeReviewed by:
Laura Hayman, University of Massachusetts Boston, United StatesŞafak Yiğit, Istanbul Galata University, Türkiye
Copyright © 2025 Brewer, Lalika, Kyalwazi, Albertie, Bowie, Burgess, Burke, Buta, Cooper, Crews, Doubeni, Elegbede, Erickson, Jenkins, Johnson, Jones, Krogman, Moen, Palmer, Patten, Penheiter, Richard, Titus, Schardin, Shanedling, Van’t Hof, Warner, Weis and Hayes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: LaPrincess C. Brewer, YnJld2VyLmxhcHJpbmNlc3NAbWF5by5lZHU=
†These authors have contributed equally to this work and share first authorship