 Daniele Melo Sardinha1,2*
Daniele Melo Sardinha1,2* Marcos Jessé Abrahão Silva1,2
Marcos Jessé Abrahão Silva1,2 Sebastião Kauã de Sousa Bispo3,4Alex Patrick Oliveira da Silva3Karla Valéria Batista Lima1,2Ilma Pastana Ferreira5Luana Nepomuceno Gondim Costa Lima1,2,4
Sebastião Kauã de Sousa Bispo3,4Alex Patrick Oliveira da Silva3Karla Valéria Batista Lima1,2Ilma Pastana Ferreira5Luana Nepomuceno Gondim Costa Lima1,2,4- 1Postgraduate Program in Epidemiology and Health Surveillance (PPGEVS), Evandro Chagas Institute (IEC), Ananindeua, Brazil
- 2Postgraduate Program in Parasite Biology in the Amazon (PPGBPA), State University of Pará and Evandro Chagas Institute (UEPA/IEC), Belém, Brazil
- 3University of the Amazon (UNAMA), Ananindeua, Brazil
- 4Institutional Scientific Initiation Scholarship Program (PIBIC), Evandro Chagas Institute (IEC), Ananindeua, Brazil
- 5Postgraduate Program in Nursing, Pará State University (PPGENF/UEPA), Belém, Brazil
Introduction: Vaccines have long been one of the most effective strategies for public health during epidemics and pandemics caused by infectious diseases. Vaccine hesitancy is a public health problem that hinders the control of disease transmission. It refers to the refusal or reluctance to receive vaccines for various reasons, including sex, personal beliefs, cultural factors, and a lack of confidence in vaccine safety and efficacy. The COVID-19 pandemic was controlled using vaccines, but maintaining ideal vaccination coverage is essential to continue reducing hospitalizations and deaths from COVID-19. In Brazil, vaccination coverage did not reach the targeted goal, raising concerns about the ongoing impact of COVID-19.
Objective: The study aimed to investigate the prevalence of COVID-19 vaccine hesitancy in Brazil.
Methodology: A systematic review with meta-analysis was carried out using the PubMed, Medline, LILACS, and ScienceDirect databases.
Results: In the search, 238 articles were reviewed, of which 8 were found to be eligible for analysis. The prevalence of vaccine hesitancy was 13.3%, or 0.133 (95% CI = 0.082–0.208), in Brazil. In the subgroup analysis by pandemic wave, the first pandemic wave showed a prevalence of 13.6% or 0.136 (95% CI = 0.081–0.220), while the second pandemic wave had a prevalence of 11.4% or 0.114 (95% CI = 0.029–0.358). Due to heterogeneity, meta-regression showed a significant association between vaccine hesitancy and parents of children and adolescents (Q = 95.55; df = 2; p = <0.0001), indicating that vaccine hesitancy is significantly higher in this population compared to the general population and older adults. Fake news, lack of knowledge, personal beliefs, income, being a woman, being a young male individual without comorbidities, being married with older children, being older, and being asymptomatic were the main factors influencing vaccine hesitancy.
Conclusion: In the first meta-analysis conducted in Brazil, vaccine hesitancy was more prevalent among parents of children and adolescents, and vaccine hesitancy decreased in the second pandemic wave. Public policies must be developed to address the factors that interfere with acceptance of the COVID-19 vaccine.
Introduction
Discussions about social health, including worker health and basic sanitary conditions in cities, started during the Industrial Revolution in England. At that time, the world was experiencing multiple epidemics in countries other than Brazil, resulting in thousands of hospitalizations and fatalities due to infectious diseases (1). Hygiene and basic sanitation were the first preventive measures, followed by the introduction of antibiotics and vaccines. Then, the second epidemiological transition occurred, during which infectious diseases were the main cause of illness. Over the decades, cases began to decline, leading to the eradication and elimination of many infectious diseases in several countries and giving rise to chronic diseases as the main cause of illness by the 21st century (2).
To ensure a reduction in hospitalizations and deaths from infectious diseases, vaccines emerged as the primary solution around the world. These immunobiological agents are developed to stimulate the immune response before exposure to pathogens. This development marked a historic milestone, as epidemics were controlled, leading to increased life expectancy. There is no debate about the benefits of vaccines, as we have already seen throughout history that vaccines are the best strategy (3, 4).
To date, challenges to vaccine adherence still exist, with one significant issue being vaccine hesitancy—the non-acceptance of the vaccine due to several factors, including a lack of trust, beliefs, and fake news about possible reactions or complications, such as autism and other diseases (5). Vaccine hesitancy is a public health problem worldwide, as it affects vaccination coverage and collective immunity, thereby jeopardizing the protection of individuals who have contraindications for vaccination. Strategies must be implemented to increase vaccine acceptance, with the aim of preventing epidemics and deaths in the community (6). Dialogue with the local community or through religious leaders, along with the support of health professionals, can help reduce vaccine hesitancy (7).
A pandemic caused by the coronavirus SARS-CoV-2 occurred in 2020 around the world, resulting in significant impacts on health, education, and the economy. The virus caused flu-like symptoms or severe acute respiratory syndrome, which led to millions of hospitalizations and deaths. In response, vaccines were developed in 2020 and rolled out in some countries around the world. In Brazil, the CoronaVac vaccine was administered at the beginning of 2021 to older individuals and healthcare professionals. Throughout 2021 and into 2022, the entire adult population was vaccinated with two doses, while vaccination for children in Brazil only began in 2023. The approved vaccines in Brazil included CoronaVac, Pfizer, Janssen, and AstraZeneca. In 2023, hospitalizations and deaths had already reduced, and restriction measures were being lifted (8–10).
Vaccination coverage with booster doses is still not satisfactory among adults in Brazil. COVID-19 vaccination was included in the vaccination schedule for children; however, coverage remains lower in Brazil among children and adolescents. Low vaccination coverage creates a vulnerability to a potential new COVID-19 epidemic in Brazil and around the world. The Unified Health System (SUS) has successfully distributed the vaccine throughout the country, but vaccine hesitancy remains one of the main factors that prevent ideal vaccination coverage. This hesitancy is due to false reports and denialism propagated by the Brazilian government in 2020 (11, 12).
In Brazil, no meta-analysis has been carried out on COVID-19 vaccine hesitancy. However, epidemiological and analytical studies allow the development of public policies for health promotion. This led to the following research question: “What is the prevalence of COVID-19 vaccine hesitancy in Brazil?”
Methodology
Study design
This systematic review and meta-analysis were carried out to investigate the perspectives on and measure the rate of vaccine hesitancy in Brazil. It was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines to ensure greater transparency and impartiality in the methods applied to this study (13). As this study was classified as a bibliographic review, it did not require ethical approval or committee approval.
Literature search
To conduct this meta-analysis, a guiding question was developed using the POT strategy (14) (a variation of the PICO anagram)—(P) Problem: COVID-19 vaccination rates in Brazil; (O) Outcome: high levels of vaccine hesitancy for COVID-19; and (T) Type of Study: original epidemiological studies. The objective of this approach was to quantify vaccine hesitancy and understand its determinants, thereby facilitating the development of specific interventions to reduce vaccine resistance in Brazil.
Thus, the following research question was formulated: “What is the prevalence of COVID-19 vaccine hesitancy in Brazil?” Based on this, a search was carried out in international databases for full-text, open-access articles published in Portuguese, English, or Spanish. The search included the descriptors DeCS and MeSH, along with the Boolean operator AND: “Hesitation Vaccination”; “COVID-19”; “Brazil.” The databases selected for this analysis were PubMed, Medline, LILACS, and ScienceDirect, and the time frame considered was from the beginning of the COVID-19 pandemic (March 2020) until the end of the third pandemic wave in Brazil (December 2022) (15, 16).
Data eligibility
The inclusion criteria for studies were based on original articles with case–control, cross-sectional, cohort, and descriptive epidemiological designs, and research with cross-sectional interviews. The exclusion criteria included incomplete articles, summaries, short communications, letters to the editor, case studies, case series, studies with unavailable data for extraction, and studies published in languages other than those selected for this research. Gray literature was excluded to ensure the highest level of evidence in epidemiology, considering the peer review and methodological quality of the articles published in scientific journals.
Data extraction and assessment of the methodological quality of the studies
After selection through independent and paired reading by two researchers (DMS and MJAS) and discussion of ideas with a third researcher (SKSB), the articles were organized in a Microsoft Office Excel 365 spreadsheet. Data extracted from the original documents included the article title, methodology, the database used, the pandemic wave referenced (based on epidemiological criteria for pandemic waves in Brazil), vaccine hesitancy rates, and the factors associated with the issue addressed in each study.
Then, a methodological assessment of the quality of the studies to be included was carried out through paired and independent selective assessments by two researchers (DMS and MJAS), with discussions involving a third researcher (SKSB) when needed. The assessments were based on the standardized checklists provided by the Joanna Briggs Institute (JBI), which are commonly used in systematic reviews to ensure data reliability. The JBI critical appraisal tools are instruments that are used to assess the trustworthiness, relevance, and results of published articles (17). The checklists used in your scoring form electives were as follows: Checklist for Analytical Cross-Sectional Studies, Checklist for Case–Control Studies, Checklist for Cohort Studies, Checklist for Prevalence Studies, and Checklist for Qualitative Research (18). Only studies that met more than 60% of the checklist requirements were selected, in accordance with the methodology outlined in previous literature (19).
Statistical analysis
Statistical analysis was conducted using Comprehensive Meta-Analysis v3.3 software (Biostat, Englewood, NJ, USA), with a proportion meta-analysis performed to estimate the prevalence. A random effects model was used due to the contextual discrepancies in each pandemic period and the different factors associated with possible outcomes of vaccine hesitancy, even within the same population assessed (20). A subgroup analysis was carried out according to the pandemic wave in each study. In addition, heterogeneity was assessed, a funnel plot was used to evaluate the risk of publication bias, and meta-regression was performed based on the type of population analyzed in each article (21).
Results
Study selection
A search of the selected databases yielded 238 articles: 10 from PubMed, 8 from Medline, 10 from LILACS, and 10 from ScienceDirect. After applying the filters (language, study period, availability of full texts, and studies conducted in Brazil), 36 studies remained. These studies were screened for titles related to vaccine hesitancy in Brazil. Duplicate studies were excluded (n = 12). In this context, we evaluated 16 complete articles. Furthermore, one article was excluded because it was a commentary, another was excluded for being a short communication (n = 1), and a third article was excluded since it evaluated several countries but did not include Brazil (n = 1). Then, a total of 13 studies were evaluated for data extraction and inclusion in our sample. After careful reading and analysis, five studies were excluded for not presenting the vaccine hesitancy rate, and eight studies (22–29) were eligible to be included in the sample for this systematic review (Figure 1).
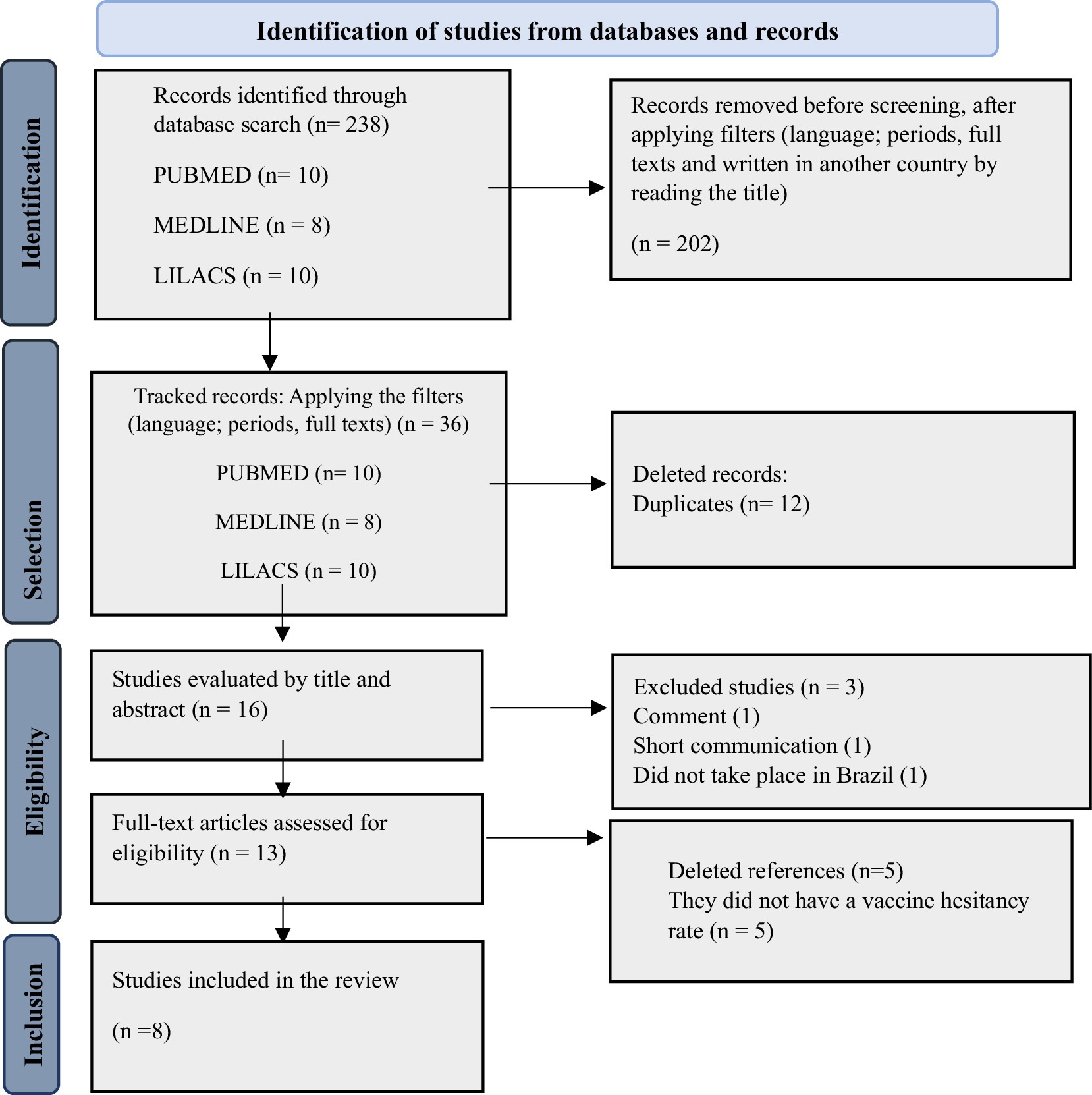
Figure 1. PRISMA flow diagram (2020) illustrating the selection of the studies included in this review. Source: authors’ own elaboration (2024).
Characterization of the included studies
A total of eight studies were included in the analysis. The studies were published in 2021 (2), 2022 (3), and 2023 (3). Seven studies were in English, and one was in Portuguese. Two (2) (23, 29) studies were related to the first pandemic wave, while the remaining six (6) (22, 24–28) focused on the second pandemic wave. The majority of the studies were sourced from the PubMed and Medline databases (n = 4; 50%). Regarding the populations studied, six studies evaluated the general population (22, 23, 25, 27–29), one study focused on older people (26), and one study examined parents of children and adolescents (24). The factors associated with vaccine hesitancy included being a woman, not being afraid of developing COVID-19, having been affected by COVID-19, political issues, belonging to a wealthier class, concerns about adverse reactions to, distrust of the vaccine, denial about the pandemic, receiving vaccine information from friends, family, and social networks, not having received the influenza vaccine, young male individuals without comorbidities, cases with older children, older people, evangelicals, and those who were asymptomatic (Table 1). Only three studies deviated from the maximum score on the JBI quality checklist. Of the six cross-sectional studies, two had a score of 87.5%, and of the two descriptive studies, one had a descriptive score of 90%.
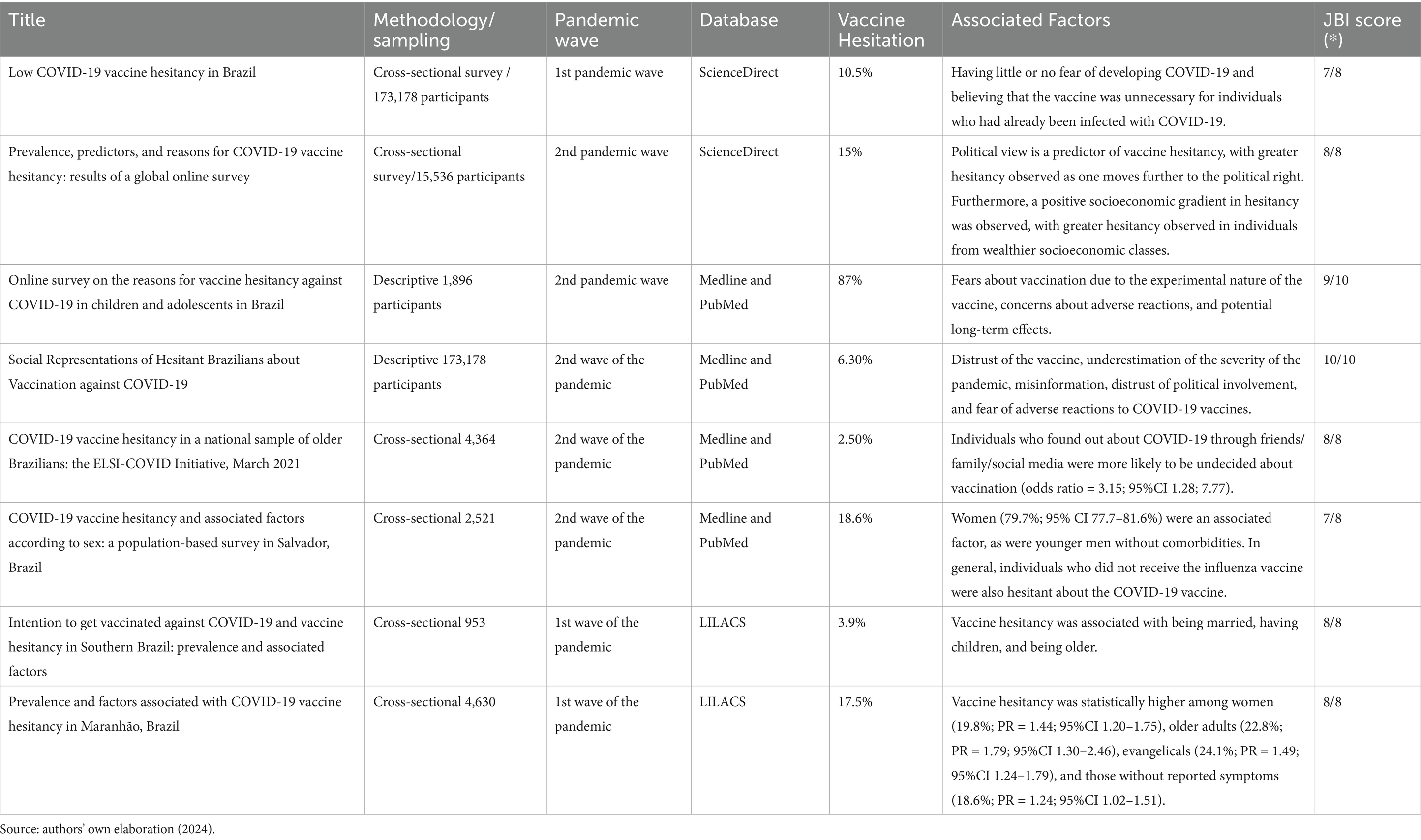
Table 1. Characteristics of the studies included in this meta-analysis.
Meta-analysis results and publication bias
In the analysis of these eight studies using a random effects model, the prevalence rate of COVID-19 vaccine hesitancy in Brazil was 13.3% or 0.133 (95% CI = 0.082–0.208). The disparities between the analyses showed statistically significant heterogeneity (Q-value = 6721.818; Df = 7; I 2 = 99.89%), with heterogeneity highlighted by the high value of I2, even within subgroups of pandemic waves (first wave = 99.55%; second wave = 99.90%). In the subgroup analysis by pandemic wave, the first pandemic wave showed a prevalence of 13.6% or 0.136 (95% CI = 0.081–0.220), while the second pandemic wave had a prevalence of 11.4% or 0.114 (95% CI = 0.029–0.358) (Figure 2). The distribution was symmetrical in the funnel plot, indicating low publication bias in the meta-analysis (Figure 3).
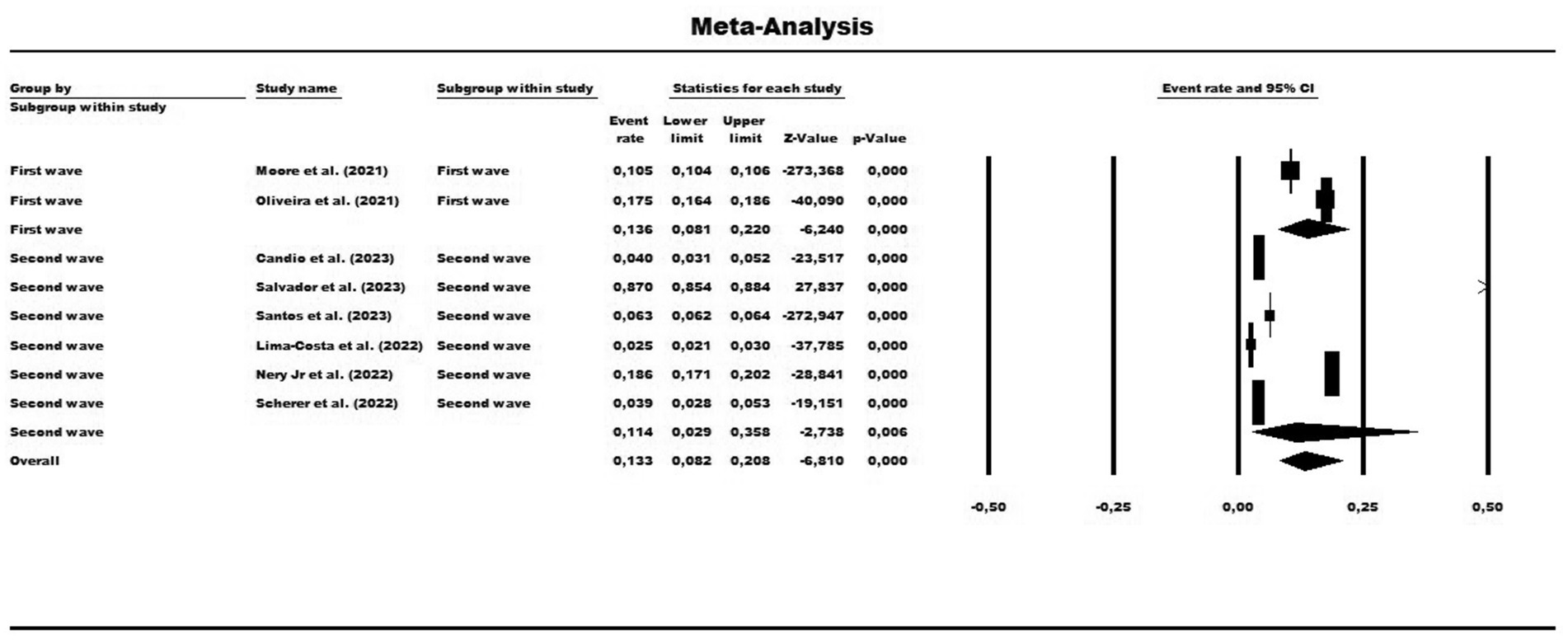
Figure 2. Forest plot showing the prevalence of COVID-19 vaccine hesitancy for the total sample, grouped by subgroups and pandemic waves. The size of each square corresponds to the weight of the related research in the meta-analysis, representing the odds ratio (OR) of each study on the map. The 95% confidence intervals (CIs) for the OR of each study are shown as horizontal lines. Numbers in bold indicate the overall OR and 95% CI, along with the total number of cases and controls.
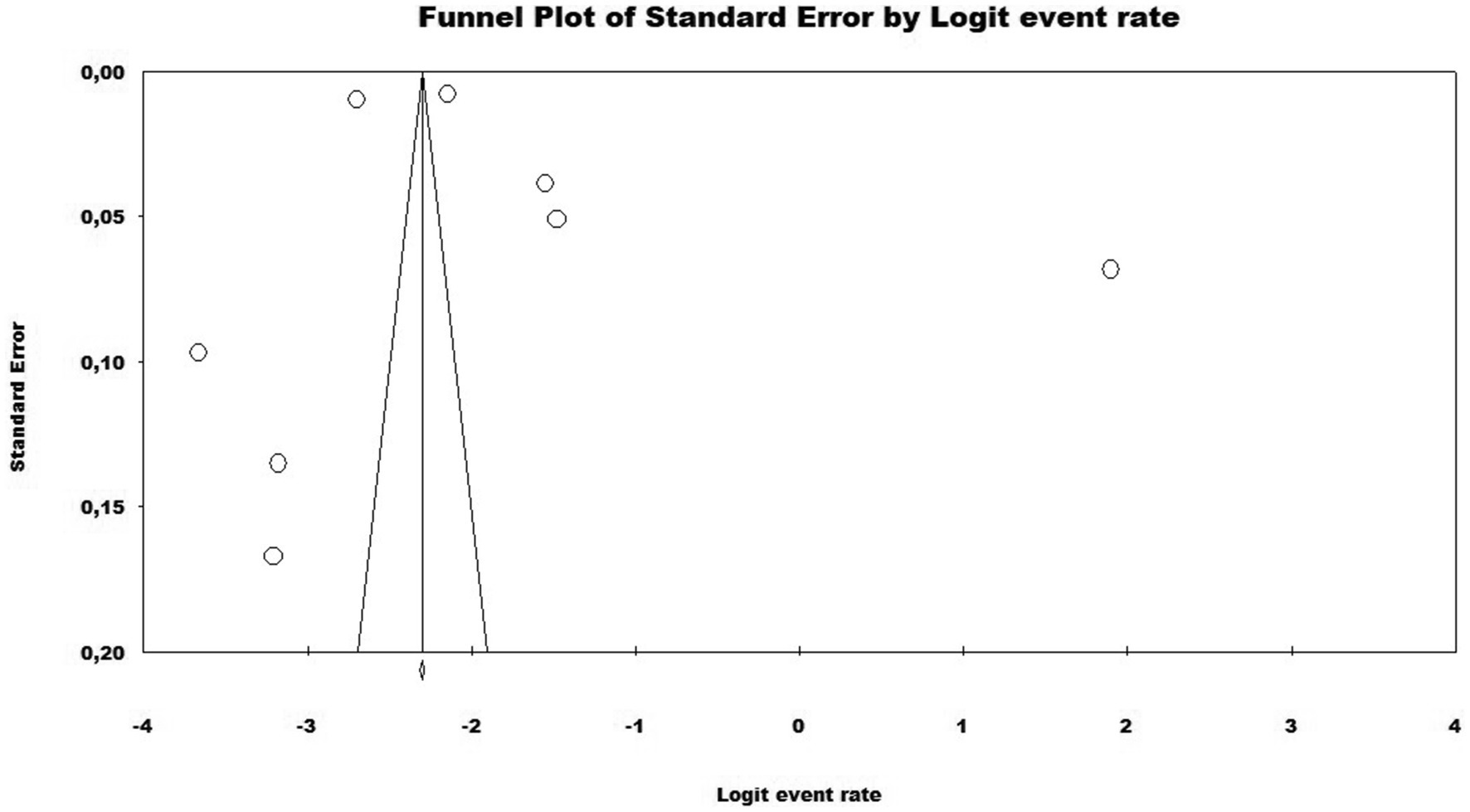
Figure 3. Funnel plot assessing publication bias in the meta-analysis of the prevalence of vaccine hesitancy regarding the SARS-CoV-2 vaccine in Brazil.
Meta-regression of the included studies through the population type covariate
Due to the high level of heterogeneity, it was necessary to search for the source of the factor that likely had the greatest weight in the concentration of divergent data. Therefore, a meta-regression was performed. The results of the meta-regression, using the type of study population as a moderator, showed a significant association between vaccine hesitancy and parents of children and adolescents (Q = 95.55; df = 2; p = <0.0001), indicating that vaccine hesitancy in this population is much higher compared to the general population and older adults (Figure 4 and Table 2).
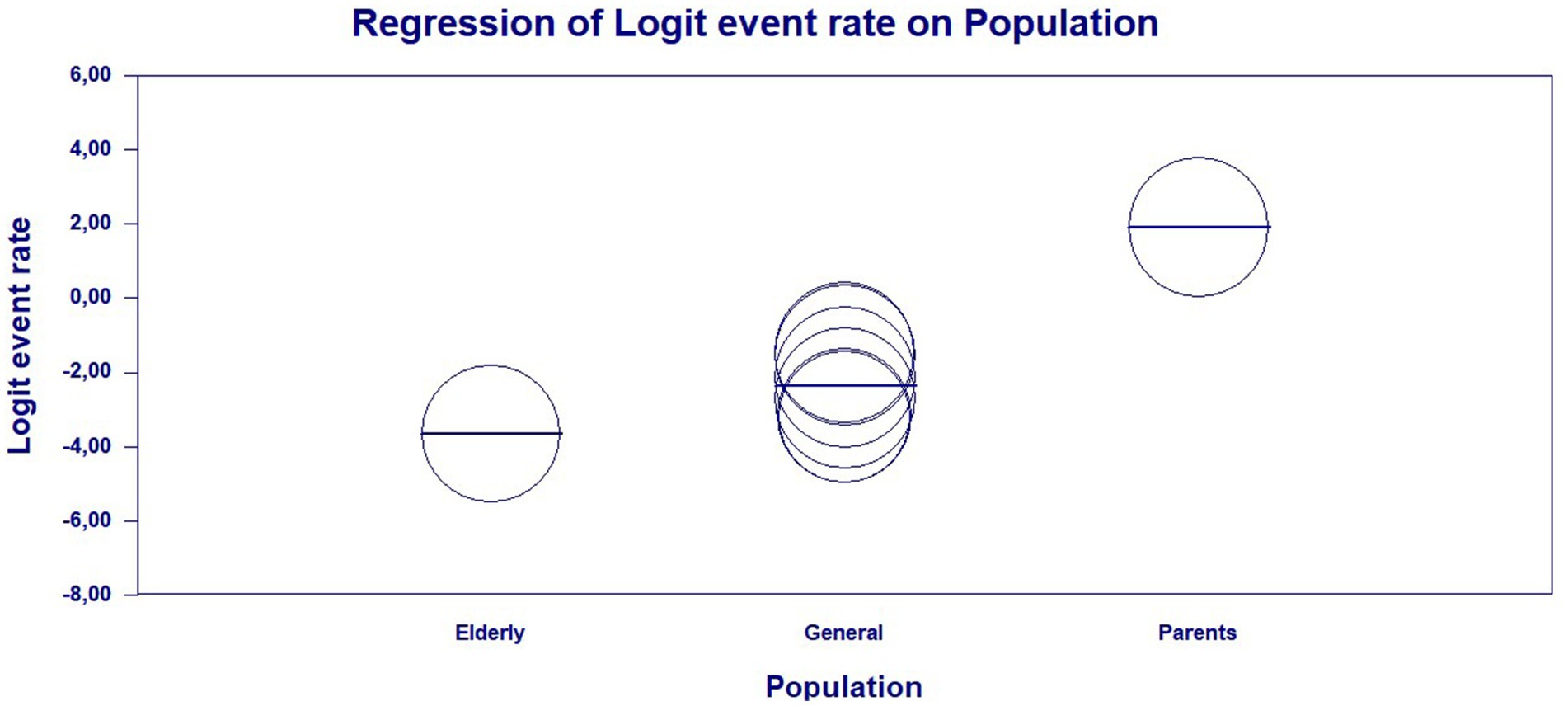
Figure 4. Scatterplot of the meta-regression of the event rate by study population type—general population, older adults, and parents of children and adolescents. Bubble size is inversely associated with study variance. The solid line reflects linear regression.
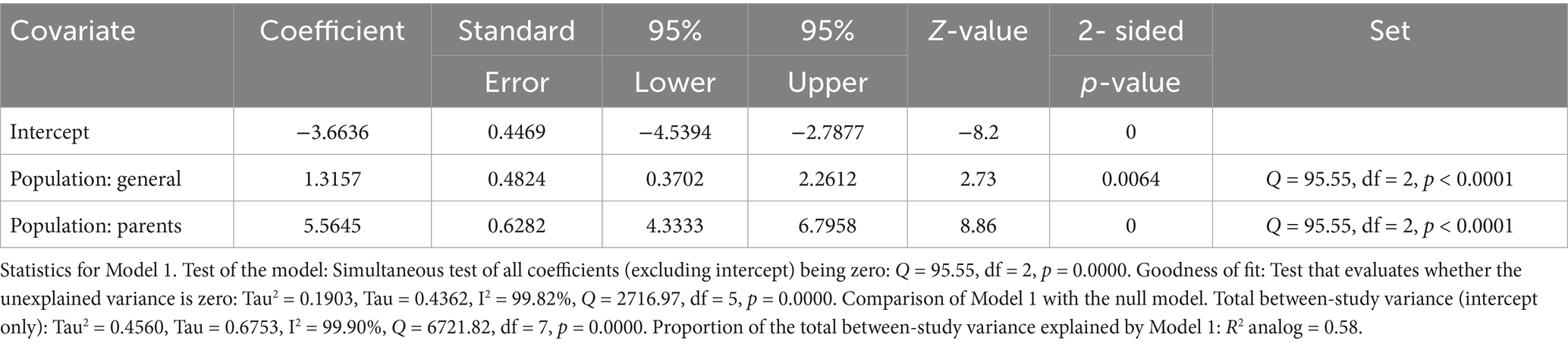
Table 2. Main results of Model 1, random effects (MM), Z-distribution, and logit event rate.
Discussion
This is the first meta-analysis to investigate the prevalence of COVID-19 vaccine hesitancy in Brazil. The limited number of available studies highlights the need for further research in this field, as vaccine hesitancy factors must be explored to guide public policies aimed at improving access and adherence to COVID-19 vaccination.
The overall prevalence of COVID-19 vaccine hesitancy in this meta-analysis was 13.3%. We analyzed vaccine hesitancy by pandemic wave and observed that in the first year of the pandemic, vaccine hesitancy was higher at 13.6%, while in the second year of the pandemic, it was 11.4%. However, meta-regression showed that the greatest difference in vaccine hesitancy was among parents of children and adolescents, compared to the general population and older adults.
Several factors affect adherence to the COVID-19 vaccine, including ethnicity, professional status, religious beliefs, political views, sex, age, education, and income (30). One study reported COVID-19 vaccine acceptance rates in various countries, with the highest rates observed in Ecuador (97.0%), Malaysia (94.3%), Indonesia (93.3%), and China (91.3%). The lowest rates were also found in Kuwait (23.6%), Jordan (28.4%), Italy (53.7%), Russia (54.9%), Poland (56.3%), the United States (56.9%), and France (58.9%) (31).
A systematic review conducted in the United States showed that the overall vaccine acceptance rate ranged from 12 to 91.4%. Factors associated with vaccine hesitancy were sex, ethnicity, age, education level, and income status. In addition, vaccine acceptance increased by 10.8% in 2020 and 7.4% in 2021. Vaccine hesitancy in the U. S. population was the highest among Black/African Americans and pregnant or breastfeeding women, while it was the lowest among men (32). Another study in the United States found that lack of confidence in the vaccine accounted for 38 and 21% of the variation in vaccine hesitancy. Sociodemographic and psychological determinants were responsible for 13 and 11% of the variation in vaccine hesitancy (33).
Another study conducted in Portugal showed that 56% of participants would wait before taking the COVID-19 vaccine, and 9% would refuse the COVID-19 vaccine. The associated factors included being younger, loss of income, not taking the flu vaccine, low confidence in the COVID-19 vaccine and the health services’ response, and doubts about the effectiveness of the vaccine (34).
Research has shown that factors such as anxiety and fear concerning one’s own health significantly influence vaccine acceptance, while fear of social and economic consequences is associated with vaccine hesitancy (35). A review highlighted several factors associated with COVID-19 vaccine hesitancy, such as concerns about vaccine effectiveness, side effects, distrust, religious beliefs, and trust in information sources (36). A study conducted in Türkiye during the first year of the pandemic found that 45.3% of participants were hesitant to receive the COVID-19 vaccine. The factors that influenced vaccine acceptance were risk perception (OR: 1.26% IC95 1.03–1.55) and age (OR: 0.94% IC95: 0.91–0.98) (37).
Potential sources of heterogeneity in Brazil may stem from various contexts. Cultural, regional, psychological, economic, religious, political, cognitive, and sex-related considerations contribute to the complex behavior surrounding vaccination decisions. COVID-19 vaccine hesitancy in Brazil is strongly influenced by the sociopolitical context of the country, characterized by a combination of misinformation, political polarization, and inequalities within the healthcare system. The context of social and regional inequalities also shapes the hesitancy, with specific religious groups, such as evangelicals, showing greater resistance, possibly due to cultural and religious convictions that affect vaccine acceptance (23, 29).
Another study conducted in Arkansas during the first year of the pandemic showed that vaccine hesitancy was higher among Black/African Americans (50.00%), individuals with a family income below US$25,000 (30.68%), those with some higher education (32.17%), those with little or no fear of COVID-19 infection (62.50%), and those with low confidence in vaccines in general (55.84%) (38). A study conducted in European countries during the second year of the pandemic highlighted that COVID-19 vaccine hesitancy was lowest in Spain, at 6.22% for women and 6.82% for men, compared to Bulgaria, where the rates of hesitancy were higher, at 64.19% for women and 59.20% for men. Men showed higher vaccine acceptance than women in the countries analyzed (39). Heterogeneity was associated with sex and groups, such as income and ethnicity.
In our meta-analysis, parents of children and adolescents showed the greatest heterogeneity among the groups, with vaccine hesitancy rates higher than those observed in other populations. This is concerning, as children and adolescents depend on their parents to get vaccinated. In Switzerland, it was no different, where an online survey study on the acceptance of the COVID-19 vaccine by country in relation to children found that the intention to vaccinate children was 58.7%. This indicates that the proportion of those unwilling to vaccinate remained high, even in the second year of the pandemic (40).
Another study in Jordan highlighted that 21.5% of parents were unsure about vaccinating their children, while 48.4% intended not to vaccinate them (41). A survey of mothers in the United Kingdom, conducted during the second year of the pandemic, showed vaccine hesitancy regarding their children in two groups: 38.4% in the first group and 25.6% in the second (42). In Qatar, a survey conducted during the first year of the pandemic showed that 29.4% of mothers were hesitant to vaccinate their children against COVID-19, while 27.5% expressed personal vaccine hesitancy. The highest hesitancy rate was associated with ethnicity, with 51.3% of Qatari mothers reporting hesitancy (43). A study in Shenzhen, China, reported a hesitancy rate of 43.37% (44). Similarly, in Saudi Arabia, 49.4% of parents did not wish to immunize their children with the COVID-19 vaccine, and 12.8% were unsure (45).
A survey of COVID-19 vaccination coverage in Norwegian children and adolescents conducted in December 2022 included 423,548 children aged 5 to 11 years, 269,830 children aged 12 to 15 years, and 120,854 children aged 16 to 17 years. Vaccine adherence in these three groups was 2.6, 73.3, and 87.3%, respectively (46). The country’s high vaccine hesitancy is responsible for low vaccination coverage among children and adolescents.
One of the reasons for the country’s general vaccine hesitancy was the association of autism spectrum disorder (ASD) with vaccination. However, this is a myth—false news shared on social media—that has contributed to low vaccination coverage worldwide. It has already been proven through extensive research that there is no association between ASD and vaccines in children and adolescents (47).
In Brazil, the “Observa Infância” project analyzed data on COVID-19 vaccination from February 2024. Vaccination coverage among children aged 3 to 4 years was 23% for two doses and only 7% for the complete vaccination schedule with three doses. In the age group of 5 to 11 years, coverage increased to 55.9% for two doses and 12.8% for completing the three-dose regimen (48). The low vaccination coverage in the fourth year of the pandemic in Brazil among children and adolescents is a public health problem. Strategies should focus on reducing vaccine hesitancy among parents. A lack of knowledge about vaccines is one of the main reasons for hesitancy, with indecision and lifestyle factors also influencing this decision (49).
The limitations of this review include high heterogeneity, possible publication bias, limited data on certain subpopulations, and potential misclassification of hesitancy levels. The main limitation of this meta-analysis is the small number of studies carried out in Brazil and the heterogeneity identified through the meta-regression. Therefore, future studies on vaccine hesitancy should be prioritized in Brazil to support public health planning and achieve an acceptable vaccination coverage of at least 95%. In addition, the COVID-19 pandemic occurred during a period of extreme political polarization in Brazil, which was accompanied by widespread circulation of fake news and contradictory information, even from health professionals and authorities. This fragmented and conflicting communication and high scientific denialism contributed to distrust of the vaccine and an increase in vaccine hesitancy (50).
Regarding the relationship between COVID-19 vaccine hesitancy and mortality/morbidity in Brazil, it was revealed that this lethality was linked to inadequate vaccination coverage, as vaccine hesitancy (27.5% nationwide) directly hindered herd immunity and permitted the spread of severe outcomes (51). Regional differences were striking, while scientific denialism and mistrust of health officials intensified transmission, and towns that voted for then-President Bolsonaro in the 2018 election experienced significantly higher mortality rates during the second wave (52, 53). In communities influenced by evangelical missionaries, conspiracy theories—such as untrue claims that vaccines cause people to change into “alligators”—became popular (54, 55). Bolsonaro’s public skepticism—including derision toward vaccines such as Sinovac and Pfizer—amplified distrust among his supporters. Structural equation modeling demonstrated that reluctance was inversely correlated with faith in governmental entities (54, 56). Due to this politicization, vaccination became a partisan issue, and people on the political left showed greater compliance (54, 57, 58).
Therefore, for future public health policies addressing Brazil’s inequalities, studies have shown that there is a need to depoliticize vaccination through cross-partisan campaigns that isolate health guidelines from political narratives, personalize community engagement to combat misinformation in religious and indigenous communities by collaborating with trusted religious leaders, prioritize regional equity by aligning genomic surveillance and vaccine access with socioeconomic vulnerability indicators, and strengthen institutional trust through transparent communication about vaccine safety and by directly countering conspiratorial beliefs. These measures must be recognized among Brazil’s sociopolitical fractures to prevent recurring mortality disparities during health crises (59, 60).
Conclusion
This is the first meta-analysis on vaccine hesitancy against COVID-19 in Brazil, and it showed that hesitancy prevalence was higher during the first year of the pandemic and decreased during the second year. The significant variation between the studies was strongly influenced by the specific population evaluated, with emphasis on the high level of vaccine hesitancy among parents of children and adolescents.
Public policies need to be developed to address the factors that interfere with the acceptance of the COVID-19 vaccine, especially among parents of children and adolescents in Brazil. Fake news, lack of knowledge, beliefs, income level, female sex, young male individuals without comorbidities, being married with older children, older age, and being asymptomatic are the main factors influencing vaccine hesitancy.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
DS: Supervision, Conceptualization, Writing – review & editing, Methodology, Software, Investigation, Writing – original draft, Formal analysis, Data curation. MS: Investigation, Writing – review & editing, Data curation, Software, Methodology, Conceptualization, Formal analysis. SB: Software, Methodology, Investigation, Writing – original draft. AS: Investigation, Writing – original draft, Methodology. KL: Visualization, Validation, Supervision, Writing – review & editing. IF: Project administration, Writing – review & editing, Visualization, Validation, Resources, Supervision. LL: Writing – review & editing, Methodology, Supervision, Visualization, Conceptualization, Resources, Funding acquisition, Validation, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by National Council for Scientific and Technological Development (CNPQ), Coordination for the Improvement of Higher Education Personnel (CAPES), Instituto Evandro Chagas (IEC) and Fundação Amazônia de Amparo a Estudos e Pesquisas (FAPESPA).
Acknowledgments
We thank the Evandro Chagas Institute (IEC) and the Post-Graduate Program in Epidemiology and Health Surveillance (PPGEVS) for their support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nunes, L d R, and Diaz, RRL. Evolução do saneamento básico na história e o debate de sua privatização no Brasil. Rev Direito Fac Guanambi. (2020) 7:e292. doi: 10.29293/rdfg.v7i02.292
2. Blacher, J, Levy, BI, Mourad, J-J, Safar, ME, and Bakris, G. From epidemiological transition to modern cardiovascular epidemiology: hypertension in the 21st century. Lancet. (2016) 388:530–2. doi: 10.1016/S0140-6736(16)00002-7
3. Wilder-Smith, A, Longini, I, Zuber, PL, Bärnighausen, T, Edmunds, WJ, Dean, N, et al. The public health value of vaccines beyond efficacy: methods, measures and outcomes. BMC Med. (2017) 15:138. doi: 10.1186/s12916-017-0911-8
4. Saadatian-Elahi, M, Horstick, O, Breiman, RF, Gessner, BD, Gubler, DJ, Louis, J, et al. Beyond efficacy: the full public health impact of vaccines. Vaccine. (2016) 34:1139–47. doi: 10.1016/j.vaccine.2016.01.021
5. Dubé, E, Laberge, C, Guay, M, Bramadat, P, Roy, R, and Bettinger, JA. Vaccine hesitancy. Hum Vaccin Immunother. (2013) 9:1763–73. doi: 10.4161/hv.24657
6. Jacobson, RM, St. Sauver, JL, and Finney Rutten, LJ. Vaccine hesitancy. Mayo Clin Proc. (2015) 90:1562–8. doi: 10.1016/j.mayocp.2015.09.006
7. Jarrett, C, Wilson, R, O’Leary, M, Eckersberger, E, and Larson, HJ. Strategies for addressing vaccine hesitancy—a systematic review. Vaccine. (2015) 33:4180–90. doi: 10.1016/j.vaccine.2015.04.040
8. Gramacho, WG, and Turgeon, M. When politics collides with public health: COVID-19 vaccine country of origin and vaccination acceptance in Brazil. Vaccine. (2021) 39:2608–12. doi: 10.1016/j.vaccine.2021.03.080
9. Ministério da Saúde. Brasil apresenta queda em casos e óbitos por COVID-19. Governo Federal. (2024). Available online at: https://www.gov.br/saude/pt-br/assuntos/noticias/2024/marco/brasil-apresenta-queda-em-casos-e-obitos-por-covid-19#:~:text (Accessed May 22, 2024).
10. Ministério da Saúde (2023). ESTRATÉGIA DE VACINAÇÃO CONTRA A COVID-19 – 2024. Ministério da Saúde, Secretaria de Vigilância em Saúde e Ambiente, Departamento de Imunização e Doenças Imunopreveníveis. Available online at: https://infoms.saude.gov.br/content/Default/Informevacinacaocovid2024_final_29dez23.pdf (Accessed May 22, 2024).
11. Galhardi, CP, Freire, NP, Fagundes, MCM, Minayo, MC d S, and Cunha, ICKO. Fake news e hesitação vacinal no contexto da pandemia da COVID-19 no Brasil. Ciênc Saúde Coletiva. (2022) 27:1849–58. doi: 10.1590/1413-81232022275.24092021
12. Silva, GM, Sousa, AARde, Almeida, SMC, Sá, ICde, Barros, FR, Sousa Filho, JES, et al. Desafios da imunização contra COVID-19 na saúde pública: das fake news à hesitação vacinal. Cienc Saude Coletiva (2023);28:739–748. doi: 10.1590/1413-81232023283.09862022
13. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
14. Santos, CM d C, Pimenta, CA d M, and Nobre, MRC. The PICO strategy for the research question construction and evidence search. Rev Latino-Am Enfermagem. (2007) 15:508–11. doi: 10.1590/s0104-11692007000300023
15. Ferrante, L, Duczmal, LH, Capanema, E, Steinmetz, WAC, Almeida, ACL, Leão, J, et al. Dynamics of COVID-19 in Amazonia: a history of government denialism and the risk of a third wave. Prev Med Rep. (2022) 26:101752. doi: 10.1016/j.pmedr.2022.101752
16. Barberia, LG, Boing, A, Gusmão, J, Miyajima, F, Abud, A, Kemp, B, et al. An assessment of the public health surveillance strategy based on molecular testing during three major pandemic waves of COVID-19 in Brazil. PLOS Glob Public Health. (2023) 3:e0002164. doi: 10.1371/journal.pgph.0002164
17. Munn, Z, Aromataris, E, Tufanaru, C, Stern, C, Porritt, K, Farrow, J, et al. The development of software to support multiple systematic review types: the Joanna Briggs institute system for the unified management, assessment and review of information (JBI SUMARI). Int J Evid Based Healthc. (2019) 17:36–43. doi: 10.1097/XEB.0000000000000152
18. Aromataris, E, and Munn, Z. JBI manual for evidence synthesis. Joanna Briggs Institute, JBI evidence implementation (2020).
19. Aromataris, E, and Munn, Z. Joanna Briggs institute reviewer’s manual, vol. 2017 The Joanna Briggs Institute (2017).
20. Cheung, MW-L, and Vijayakumar, R. A guide to conducting a meta-analysis. Neuropsychol Rev. (2016) 26:121–8. doi: 10.1007/s11065-016-9319-z
21. Tang, J-L, and Liu, JL. Misleading funnel plot for detection of bias in meta-analysis. J Clin Epidemiol. (2000) 53:477–84. doi: 10.1016/s0895-4356(99)00204-8
22. Candio, P, Violato, M, Clarke, PM, Duch, R, and Roope, LS. Prevalence, predictors and reasons for COVID-19 vaccine hesitancy: results of a global online survey. Health Policy. (2023) 137:104895. doi: 10.1016/j.healthpol.2023.104895
23. Moore, DCBC, Nehab, MF, Camacho, KG, Reis, AT, Junqueira-Marinho, M d F, Abramov, DM, et al. Low COVID-19 vaccine hesitancy in Brazil. Vaccine. (2021) 39:6262–8. doi: 10.1016/j.vaccine.2021.09.013
24. Salvador, PTCDO, Alves, KYA, Carvalho, KRSD, Nehab, MF, Camacho, KG, Reis, AT, et al. Inquérito online sobre os motivos para hesitação vacinal contra a COVID-19 em crianças e adolescentes do Brasil. Cad Saude Publica. (2023) 39:e00159122. doi: 10.1590/0102-311XPT159122
25. Santos, KCOdos, Junqueira-Marinho, M de F, Reis, AT, Camacho, KG, Nehab, MF, Abramov, DM, et al. Social representations of hesitant Brazilians about vaccination against COVID-19. Int J Environ Res Public Health (2023);20:6204. doi: 10.3390/ijerph20136204
26. Lima-Costa, MF, Macinko, J, and Mambrini, JV d M. Hesitação vacinal contra a COVID-19 em amostra nacional de idosos brasileiros: iniciativa ELSI-COVID, março de 2021. Epidemiol Serv Saude. (2022) 31:e2021469. doi: 10.1590/S1679-49742022000100020
27. Nery, N, Ticona, JPA, Cardoso, CW, Prates, APPB, Vieira, HCA, Salvador de Almeida, A, et al. COVID-19 vaccine hesitancy and associated factors according to sex: a population-based survey in Salvador, Brazil. PLoS One. (2022) 17:e0262649. doi: 10.1371/journal.pone.0262649
28. Scherer, JN, Martins, PMD, Azevedo, VA, Sperling, LE, Veronese, MV, and Renck, PGB. Intenção de se vacinar contra a COVID-19 e hesitação vacinal no Sul do Brasil: Prevalência e fatores associados. Rev Bras Psicoter. (2022) 24:61–73. doi: 10.5935/2318-0404.20220015
29. Oliveira, BLCAde, Campos, MAG, Queiroz, RC de S, Britto e Alves, MTSSde, Souza, BFde, Santos, AMdos, et al. Prevalência e fatores associados à hesitação vacinal contra a covid-19 no Maranhão, Brasil. Rev Saude Publica (2021) 55:12. doi: 10.11606/s1518-8787.2021055003417
30. Troiano, G, and Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health. (2021) 194:245–51. doi: 10.1016/j.puhe.2021.02.025
31. Sallam, M. COVID-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccine. (2021) 9:160. doi: 10.3390/vaccines9020160
32. Yasmin, F, Najeeb, H, Moeed, A, Naeem, U, Asghar, MS, Chughtai, NU, et al. COVID-19 vaccine hesitancy in the United States: a systematic review. Front Public Health. (2021) 9:770985. doi: 10.3389/fpubh.2021.770985
33. Gerretsen, P, Kim, J, Caravaggio, F, Quilty, L, Sanches, M, Wells, S, et al. Individual determinants of COVID-19 vaccine hesitancy. PLoS One. (2021) 16:e0258462. doi: 10.1371/journal.pone.0258462
34. Soares, P, Rocha, JV, Moniz, M, Gama, A, Laires, PA, Pedro, AR, et al. Factors associated with COVID-19 vaccine hesitancy. Vaccine. (2021) 9:300. doi: 10.3390/vaccines9030300
35. Bendau, A, Plag, J, Petzold, MB, and Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int Immunopharmacol. (2021) 97:107724. doi: 10.1016/j.intimp.2021.107724
36. Biswas, MR, Alzubaidi, MS, Shah, U, Abd-Alrazaq, AA, and Shah, Z. A scoping review to find out worldwide COVID-19 vaccine hesitancy and its underlying determinants. Vaccine. (2021) 9:1243. doi: 10.3390/vaccines9111243
37. İkiışık, H, Akif Sezerol, M, Taşçı, Y, and Maral, I. COVID-19 vaccine hesitancy: a community-based research in Turkey. Int J Clin Pract. (2021) 75:e14336. doi: 10.1111/ijcp.14336
38. Willis, DE, Andersen, JA, Bryant-Moore, K, Selig, JP, Long, CR, Felix, HC, et al. COVID-19 vaccine hesitancy: race/ethnicity, trust, and fear. Clin Transl Sci. (2021) 14:2200–7. doi: 10.1111/cts.13077
39. Steinert, JI, Sternberg, H, Prince, H, Fasolo, B, Galizzi, MM, Büthe, T, et al. COVID-19 vaccine hesitancy in eight European countries: prevalence, determinants, and heterogeneity. Sci Adv. (2022) 8:eabm9825. doi: 10.1126/sciadv.abm9825
40. Wagner, A, Liberatore, F, Schmelzer, S, and Dratva, J. Confident and altruistic – parents’ motives to vaccinate their children against COVID-19: a cross-sectional online survey in a Swiss vaccination Centre. Swiss Med Wkly. (2022) 152:w30156. doi: 10.4414/SMW.2022.w30156
41. Al-Qerem, W, Al Bawab, AQ, Hammad, A, Jaber, T, Khdair, SI, Kalloush, H, et al. Parents’ attitudes, knowledge and practice towards vaccinating their children against COVID-19: a cross-sectional study. Hum Vaccin Immunother. (2022) 18:2044257. doi: 10.1080/21645515.2022.2044257
42. Condie, J, Northstone, K, Major-Smith, D, and Halstead, I. Exploring associations between the big five personality traits and cognitive ability with COVID-19 vaccination hesitancy and uptake among mothers and offspring in a UK prospective cohort study. Vaccine. (2024) 42:2817–26. doi: 10.1016/j.vaccine.2024.03.018
43. Reagu, S, Mohan, S, Awwad, J, and Alabdulla, M. Maternal vaccine hesitancy towards COVID-19 immunisation of children in Qatar: a population-based cross-sectional study. Epidemiol Health. (2022) 44:e2022056. doi: 10.4178/epih.e2022056
44. Shen, X, Wu, X, Deng, Z, Liu, X, Zhu, Y, Huang, Y, et al. Analysis on vaccine hesitation and its associated factors among parents of preschool children in Songgang street, Shenzhen. Sci Rep. (2022) 12:9467. doi: 10.1038/s41598-022-12530-9
45. Khatrawi, EM, and Sayed, AA. The reasons behind COVID-19 vaccination hesitancy among the parents of children aged between 5 to 11 years old in Saudi Arabia. Int J Environ Res Public Health. (2023) 20:1345. doi: 10.3390/ijerph20021345
46. Orangzeb, S, Desalegn, A, Trinh, NTH, Zhao, J, Nordeng, H, and Lupattelli, A. COVID-19 vaccine uptake among children and adolescents in Norway: a comprehensive registry-based cohort study of over 800,000 individuals. Vaccine. (2024) 42:3420–8. doi: 10.1016/j.vaccine.2024.04.039
47. Gabis, LV, Attia, OL, Goldman, M, Barak, N, Tefera, P, Shefer, S, et al. The myth of vaccination and autism spectrum. Eur J Paediatr Neurol. (2022) 36:151–8. doi: 10.1016/j.ejpn.2021.12.011
48. Motta, I. Observa Infância: cobertura vacinal de crianças contra Covid-19 segue baixa. Fundação Oswaldo Cruz FIOCRUZ mostram que a cobertura,o esquema com três doses. (2024). Available online at: https://portal.fiocruz.br/noticia/2024/03/observa-infancia-cobertura-vacinal-de-criancas-contra-covid-19-segue-baixa#:~:text=Eles (Accessed November, 11 2024).
49. Viana, I da S, Cursino, EG, Miranda, P da S, Silva, LFda, and Machado, MED. Hesitação vacinal de pais e familiares de crianças e o controle das doenças imunopreveníveiS. Cogitare Enferm (2023);28:e84290. doi: 10.1590/ce.v28i0.84290
50. Bastos, LS, Ranzani, OT, Souza, TML, Hamacher, S, and Bozza, FA. COVID-19 hospital admissions: Brazil’s first and second waves compared. Lancet Respir Med. (2021) 9:e82–3. doi: 10.1016/S2213-2600(21)00287-3
51. Cândido-Sobrinho, SA, Júnior, F de S, Silva-Filho, JQda, Viana, VAF, and Lima, AÂM. Morbidity, mortality and immunization in severe COVID-19 among the elderly in Brazil: a five-year perspective. medRxiv (2025) 5:1–27. doi: 10.1101/2025.05.01.25326813
52. Camargo, ELS, Sousa, ÁFLde, Reis, ASdos, Fortunato, M dos R, Gouveia, I dos S, Mendes, IAC, et al. Determining factors for COVID-19 vaccine hesitancy among Brazilians: a study using structural equation modeling. Rev Bras Enferm (2024);77:e20240112. doi: 10.1590/0034-7167-2024-0112
53. Silva, KDO, Paiva, SFde, Campos, LAM, and Repeke, CEP. Hesitação à vacina no período de isolamento na pandemia COVID-19. RECIMA21 Rev Cient Multidiscip (2021);2:e27505. doi: 10.47820/recima21.v2i7.505
54. Xavier, DR, Lima E Silva, E, Lara, FA, E Silva, GRR, Oliveira, MF, Gurgel, H, et al. Involvement of political and socio-economic factors in the spatial and temporal dynamics of COVID-19 outcomes in Brazil: a population-based study. Lancet Reg Health Am. (2022) 10:100221. doi: 10.1016/j.lana.2022.100221
55. Seara-Morais, GJ, Avelino-Silva, TJ, Couto, M, and Avelino-Silva, VI. The pervasive association between political ideology and COVID-19 vaccine uptake in Brazil: an ecologic study. BMC Public Health. (2023) 23:1606. doi: 10.1186/s12889-023-16409-w
56. Paschoalotto, MAC, Cima, J, Costa, E, Valente de Almeida, S, Gomes da Costa, J, Santos, JV, et al. Politics and confidence toward the COVID-19 vaccination: a Brazilian cross-sectional study. Hum Vaccin Immunother. (2024) 20:2318139. doi: 10.1080/21645515.2024.2318139
57. Lima, EECde, Costa, LCCda, Souza, RF, Rocha, CO da E, and Ichihara, MYT. Presidential election results in 2018-2022 and its association with excess mortality during the 2020-2021 COVID-19 pandemic in Brazilian municipalities. Cad Saude Publica (2024);40:e00194723. doi: 10.1590/0102-311XEN194723
58. Paschoalotto, MAC, Costa, EPPA, Almeida, SVde, Cima, J, Costa, JGda, Santos, JV, et al. Running away from the jab: factors associated with COVID-19 vaccine hesitancy in Brazil. Rev Saude Publica (2021);55:97. doi: 10.11606/s1518-8787.2021055003903
59. Maciel, APF, Macedo, OHO, Junior, RF d S, Pereira, VG, Versiani, CMC, Mota, ÉC, et al. Strategies to reduce vaccine hesitancy in the context of the Covid-19 pandemic: scoping review. Cuadernos de Educación y Desarrollo. (2024) 16:e5362. doi: 10.55905/cuadv16n8-139
Keywords: vaccine hesitation, prevalence, public health, COVID-19, Brazil
Citation: Sardinha DM, Silva MJA, Bispo SKS, da Silva APO, Lima KVB, Ferreira IP and Lima LNGC (2025) Prevalence of COVID-19 vaccine hesitancy in Brazil: a systematic review and meta-analysis. Front. Public Health. 13:1622247. doi: 10.3389/fpubh.2025.1622247
Edited by:
Larissa Krokovsky, Brock University, CanadaReviewed by:
Shisan (Bob) Bao, The University of Sydney, AustraliaAbu-Hena Kamal, Khulna University of Engineering & Technology, Bangladesh
Copyright © 2025 Sardinha, Silva, Bispo, da Silva, Lima, Ferreira and Lima. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniele Melo Sardinha, ZGFuaWVsbGUtdmlhbm5hMjBAaG90bWFpbC5jb20=