 Ciprian Ionuț Băcilă1,2
Ciprian Ionuț Băcilă1,2 Monica Cornea1
Monica Cornea1 Bogdan Ioan Vintilă1,2,3
Bogdan Ioan Vintilă1,2,3 Andrei Lomnasan1
Andrei Lomnasan1 Adrian Gheorghe Boicean2,3
Adrian Gheorghe Boicean2,3 Andreea Maria Grama1*Claudiu Matei2,4
Andreea Maria Grama1*Claudiu Matei2,4 Bogdan Neamtu2,5,6,7*
Bogdan Neamtu2,5,6,7*- 1Neuroscience Scientific Research Group “Dr. Gheorghe Preda” Clinical Hospital Psychiatry of Sibiu, Sibiu, Romania
- 2Faculty of Medicine, Lucian Blaga University of Sibiu, Sibiu, Romania
- 3County Clinical Emergency Hospital of Sibiu, Sibiu, Romania
- 4Medlife Polisano Hospital, Sibiu, Romania
- 5Center for Research in Mathematics and Applications, “Lucian Blaga” University of Sibiu, Sibiu, Romania
- 6Pediatric Clinical Hospital, Sibiu, Romania
- 7Whiting School of Engineering, Johns Hopkins University, Baltimore, MD, United States
Introduction: The COVID-19 pandemic significantly reshaped involuntary psychiatric hospitalizations, disrupting the balance between patient rights, public safety, and healthcare delivery. This study aims to examine the pandemic’s impact on involuntary admissions (IA) from a major psychiatric hospital in Sibiu Romania. Furthermore, it proposes a prediction model for informed consent refusal rates (ICRR).
Materials and methods: We conducted a retrospective, observational analysis of 781 involuntary admissions using records by comparing socio-demographic, clinical, and procedural variables across two periods: pre-pandemic (March 2018–February 2020) and during the pandemic (March 2020–March 2022). Variables analyzed included demographics, clinical symptoms, procedural circumstances, and hospitalization duration with Chi-Square, Cochran–Mantel–Haenszel (CMH), Breslow-Day, Cramer’s V tests and logistic regression model applied as appropriate.
Results: Psychomotor agitation, aggression, and suicidal behavior were leading reasons for involuntary admission. Confirmation rates were significantly higher among non-aggressive patients (p < 0.0001). Schizophrenia spectrum disorders were predominant diagnoses, with significantly higher confirmation rates during the pandemic (p < 0.0001). Police-initiated admissions increased significantly, while family-initiated admissions significantly declined (p < 0.001). Other consistently significant predictors included insurance status, marital status, residence type, psychotic symptoms, psychiatric comorbidities, and the source initiating the involuntary admission request (all CMH tests p ≤ 0.002). Logistic regression modeling demonstrated strong predictive performance (AUC = 0.807, accuracy = 80.7%), identifying education level, alcohol consumption, psychoactive substance use, and police involvement as significant predictors of ICRR.
Conclusion: The pandemic introduced significant procedural and management challenges to involuntary admissions at a tertiary hospital in Romania. Our predictive modeling highlights key factors influencing hospitalization outcomes, underscoring the critical need for streamlined ethical and procedural frameworks, strengthened multidisciplinary collaboration, and the integration of machine learning methodologies to enhance predictive accuracy and clinical decision-making in future public health crises.
Introduction
Declared in March 2020 by the World Health Organization, the COVID-19 pandemic led to over 776 million confirmed cases (1–3) and, within its first year, triggered significant increases in major depressive and anxiety disorders globally (4, 5). In the United Kingdom, for instance, isolation and lockdown measures drove an eight-fold rise in depression, while patients hospitalized for more than 7 days with COVID-19 showed particularly high levels of depressive and anxiety symptoms (6). Nevertheless, across Europe (Germany, Italy, Portugal) and globally (South Korea, Australia), psychiatric admissions generally declined, largely due to infection fears, stricter admission criteria, reduced bed availability, and the shift to telepsychiatry (7). Beyond these changes in admission rates, the pandemic also revealed complex ethical and legal challenges in psychiatric care despite universal rights for individuals with mental illness (8). Consequently dilemmas around patient autonomy in treatment and hospitalization (9), and stigma or discrimination delayed access until emergency IA becomes necessary (10–13). IA, while legally and ethically complex, serves as a protective intervention aimed at safeguarding both the individual and society and restoring the patient’s decision-making capacity. IA requires coordinated efforts between psychiatrists and legal professionals (14–16).
Notably, international variations in IA rates or, more specifically ICRR are shaped more by legal frameworks than clinical factors (17–20). This highlights the need for detailed socio-demographic and clinical profiling to inform public-awareness strategies and uphold compliance with European human rights standards (21, 22). In this context, the COVID-19 crisis exposed both systemic vulnerabilities and areas of resilience: while partial quarantine measures reduced emergency psychiatric admissions (23–28) acute IA increased during the first lockdown period (29, 30). In Romania, IA is governed by the Mental Health Law, which mandates a psychiatrist’s evaluation of imminent danger or potential severe deterioration after exhausting voluntary options. This is followed by judicial oversight consisting of committee review within 48 h, court confirmation, monthly reassessments, and court-authorized discharge (18, 31–33) (see Appendix A).
Although some reports exist, the impact of COVID-19 on involuntary psychiatric hospitalizations in Romania and across the Balkan region remains underexplored (7). Available data, mainly from Croatia and Romania, focus primarily on overall psychiatric admissions rather than IA cases. In Croatia, a 28% decline in total psychiatric admissions was reported at the University Hospital of Split, alongside a 20% reduction in bed capacity, with a similar decrease observed at Zagreb’s Vrapče Hospital. At our institution, “Dr Gheorghe Preda” Hospital in Sibiu, previous findings showed a drop in total hospitalizations during the pandemic, accompanied by an increased average length of stay, which altered the diversity of cases managed (34).
To address the gap in understanding ICRR in Romania and at a regional level, our study analyzes the socio-demographic, clinical, and procedural factors influencing IA by comparing the pre-pandemic and pandemic periods. We hypothesized that the COVID-19 pandemic significantly altered the socio-demographic, clinical, and procedural predictors of ICRR in Romania, and that these variables can be identified through logistic regression modeling. Potential predictors were systematically selected using comprehensive statistical methods and subsequently fed into the model. While recent studies have applied machine learning techniques such as Random Forest and XGBoost, achieving AUCs between 0.68 and 0.84 (35, 36), these approaches often entail complex implementation, extensive hyperparameter tuning, and limited interpretability. In contrast, logistic regression offers a transparent, reproducible framework suited to direct clinical application, combining robust predictive performance with mathematical clarity. Given the scarcity of ML research in involuntary psychiatric admissions, our data-driven approach aims to enhance early identification of high-risk patients and improve preparedness for future public-health crises.
Materials and methods
This is a secondary analysis in a retrospective study conducted over a period of 4 years at “Dr Gheorghe Preda” Clinical Hospital of Psychiatry from Sibiu. According to data published by the National Institute of Public Health (NIPH) (37), the hospital serves over 12,000 mentally disordered people. It is a tertiary hospital with a capacity of 453 beds and the following organizational structure: a male psychosis ward (55 beds), a female psychosis ward (63 beds), an organic mental disorders and personality disorders ward (55 beds), a gerontopsychiatry ward (50 beds), an addiction-related disorders ward (50 beds) and a chronic disorders ward (90 beds). We compared a range of factors among patients proposed for involuntary admission across two distinct timeframes: the pre-pandemic period (March 2018–February 2020) and the pandemic period (March 2020–March 2022). These factors included socio-demographic and economic characteristics, clinical and psychiatric symptoms, behavioral indicators and substance use, legal and admission circumstances, as well as restraint-related and timing variables. Our analysis focused specifically on the ICRR. The approach enabled a more nuanced understanding of the determinants influencing the confirmation of such measures and underscored the importance of identifying predictors that shape decision-making in involuntary hospitalization. Additionally, we aimed to develop and validate a machine learning model to predict the likelihood of ICRR, leveraging the comprehensive dataset derived from the examined variables.
Research design
Inclusion criteria consisted of patients proposed for IA, N = 787 (either emergency room presentation or initially voluntary admission with subsequent unfavorable outcome requiring initiation of IA measure and patients aged >18). We excluded from the study all records in electronic or physical format containing insufficient and/or inconclusive data. For individuals with multiple admissions, each IA episode was included in the statistical analysis. Every hospitalization was treated as a distinct case, accounting for the specific clinical characteristics and symptomatology present at the time of admission.
Data collection process
Data was collected from electronic records and the hospital’s IA registers in physical format, some provided by the hospital’s statistical service. Given the study’s retrospective nature and data anonymization, patients were not required to provide informed consent to participate. The socio-demographic variables considered in the analysis included age, gender, residential background, marital status, educational attainment, employment status, and insurance coverage. Clinical variables consisted of primary psychiatric diagnosis at the time of admission, presence of psychiatric comorbidities, history of relapses, time of admission (day vs. night), presence of psychotic symptoms (e.g., hallucinations or delusions noted at admission), self-aggressive behavior (including self-injurious ideation or attempts), aggressive behavior toward others, neurotoxic substance use (e.g., alcohol or psychoactive substances), and the number of hospitalization days. Additional variables analyzed comprised the application of mechanical restraint, police involvement in patient transport, the initiators of the involuntary admission (IA) request (e.g., family members, healthcare professionals, or law enforcement), whether informed consent was signed or refused by the patient during the IA committee evaluation (informed consent refusal), and time intervals associated with the various stages of the IA procedure. Psychiatric diagnoses were categorized according to DSM-5 and ICD-10 criteria (38, 39) as follows: organic mental disorders, including cognitive disorders (F00–F09); mental and behavioral disorders due to psychoactive substance use (F10–F19); schizophrenia, schizotypal, and delusional disorders (F20–F29); bipolar affective disorders (F30–F31); other affective disorders (F32–F39); personality and behavioral disorders (F60–F69); and other mental disorders (F40–F48.9, F50–F59, F70–F79, F80–F89, F90–F99).
Ethical issues of research
The study was conducted according to the ethical principles stipulated in the Declaration of Helsinki (40), having prior approval from the ethics committee (No. 5381/21.04.2023). Due to the study’s retrospective nature and the complete anonymization of the data included in the analysis, informed consent from the patients was unnecessary.
Statistical analysis
To systematically explore the factors associated with ICRR across pandemic phases, a structured multi-step statistical approach was implemented to assess both the strength and stability of associations prior to predictive modeling. Categorical variables were evaluated using chi-square tests to assess their association with ICRR across the pre-pandemic and pandemic periods, applying a significance threshold of p < 0.05. This criterion was consistently used across all statistical tests and models. Association strength was quantified using Cramér’s V, while the Cochran–Mantel–Haenszel (CMH) test assessed the stability of associations over time by controlling for study period. The Breslow–Day test was used to evaluate the homogeneity of odds ratios between the two-time frames.
Predictors were retained for multivariable modeling if they demonstrated at least a moderate association (Cramér’s V ≥ 0.20 in either period) or a significant CMH trend (α = 0.05). To address potential multicollinearity, variance inflation factors (VIF) were calculated, and only variables with VIF < 4 were included in the initial model.
A logistic regression framework was used to identify independent predictors of ICRR. Given the presence of small sample sizes and rare events in some categories, Firth’s penalized likelihood approach was applied to improve estimate stability and reduce bias. Model performance was assessed using the Area Under the Curve (AUC) from receiver operating characteristic (ROC) analysis and the Likelihood Ratio Chi-square test. Results were presented as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). All analyses were conducted in SAS Studio.
Results
During the 4-year study period, 781 people (623 patients with unique id) were admitted involuntarily out of 21,069 hospitalized in our service. In the pre-pandemic period, 24.65% of admissions were through the emergency room, and 3% were involuntary. Compared with the pre-pandemic period, during the pandemic period (March 2020–March 2022), the total number of admissions decreased significantly, but the proportion of involuntary admissions reached 5.16% of all admissions. Of the 781 cases with involuntary hospitalization included in the study, only 426 required court documentation to initiate involuntary hospitalization procedures for those who refused informed consent. In 355 cases, patients subsequently signed informed consent.
Sociodemographic and economic factors
Gender and ICRR
The distribution of gender in IA differed significantly between the pandemic and pre-pandemic periods. Males became less likely to refuse consent during the pandemic, whereas females exhibited a modest but significant increase in refusal rates (Table 1). While the proportion of male admissions decreased (65.02% [n = 277] to 61.97% [n = 220]), their consent refusal rates also reduced (51.26% [n = 142] to 46.82% [n = 103]). In contrast, female admissions increased (34.98% [n = 149] to 38.03% [n = 135]), but their likelihood of refusing consent also rose (59.73% [n = 89] to 68.15% [n = 92]). While the pre-pandemic association was weak and not statistically significant (Chi-Square p = 0.0943, Cramer’s V = 0.0811), the pandemic period showed a statistically significant association (Chi-Square p < 0.0001, Cramer’s V = 0.2081), suggesting a small to moderate effect size. The relationship between gender and refusal probability remained proportionally similar (stable, Breslow-Day test p = 0.0767), even though refusal rates shifted (CMH test p = 0.0001).
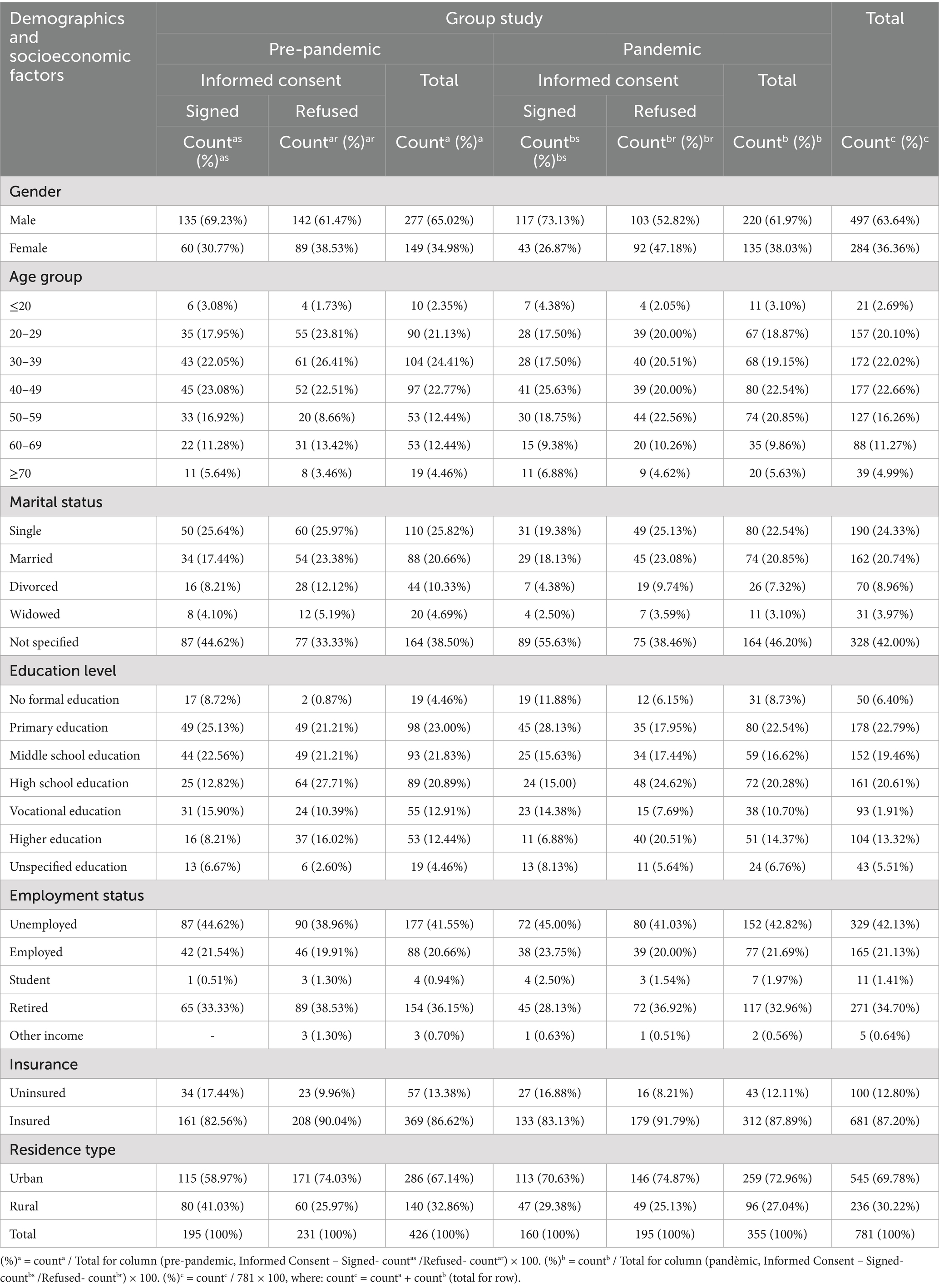
Table 1. Distribution of informed consent refusal rates (ICRR) by socio-demographic characteristics across the pre-pandemic and pandemic periods.
Age group and ICRR
The distribution of ICRR varied across age groups, with older patients being more likely to have their admission confirmed. ICRR generally decreased with age up to the 40–49 age group, with those under 20 years refusing at 40.00% (4/10) vs. 36.36% (4/11), followed by the 20–29 group at 61.11% (55/90) vs. 58.21% (39/67) and the 30–39 group at 58.65% (61/104) vs. 58.82% (40/68). Patients aged 40–49 confirmed at 53.61% (52/97) vs. 48.75% (39/80), while those aged 50–59 showed 37.74% (20/53) vs. 59.46% (44/74). Among patients 60 years and older, rates were 54.17% (39/72) vs. 52.73% (29/55). However, age was not a statistically significant predictor across periods (pre-vs pandemic), and the association remained weak and non-significant (Chi-Square p = 0.0985 vs. p = 0.5500, Cramer’s V 0.1584 vs. 0.1181). Controlling for Group Study, the CMH test (p = 0.2212) further confirmed that age did not significantly influence ICRR across study periods.
Insurance status and ICRR
Insurance status was significantly associated with ICRR, with notable differences between the pre-pandemic and pandemic periods. ICRR in insured patients increased (56.37% [208/369] to 57.37% [179/312]), while in uninsured patients decreased (40.35% [23/57] to 37.21% [16/43]). Albeit statistically significant, the association was weak to small-moderate (Chi-Square p = 0.0239 vs. p = 0.0127, Cramer’s V = 0.1095 vs. 0.1322), suggesting a slightly stronger relationship in the pandemic period. Controlling for Group_Study, the CMH test (p = 0.0008) confirmed a significant association between insurance status and ICRR across both periods, and this relationship’s strength remained stable over time (Breslow-Day, p = 0.6958).
Marital status and ICRR
Marital status was not significantly associated with ICRR before the pandemic but became significant during the pandemic. Single patients had higher ICRR in both periods (54.55% [60/110]vs. 61.25% [49/80]), and married patients had a slight decrease (61.36% [54/88] vs. 60.81% [45/74]). Divorced patients had a lower ICRR (63.64% [28/44] vs. 73.08% [19/26]), while widowed patients showed minimal change (60.00% [12/20] vs. 63.64% [7/11]). Patients with unspecified marital status had the lowest proportions in both periods, with ICRR at 46.95% (77/164) vs. 45.73% (75/164). Statistical tests showed a weak and non-significant association pre-pandemic (Chi-Square p = 0.1284, Cramer’s V = 0.1295) becoming significant with a moderate effect during the pandemic (Chi-Square p = 0.0195, Cramer’s V = 0.1817). The association across both periods was significant (CMH, p = 0.0018).
Level of education and ICRR
Education level was significantly associated with ICRR in both study periods, with higher education levels correlating with higher ICRR. No formal education had the lowest prepandemic ICRR (10.53%, 2/19), increasing to (38.71%, 12/31), followed by unspecified education (31.58%, 6/19 vs. 45.83%, 11/24). Vocational education had moderate ICRR (43.64%, 24/55 vs. 39.47%, 15/38), while primary education slightly decreased (50.00%, 49/98 vs. 43.75%, 35/80). Middle school education had a higher ICRR (52.69%, 49/93 vs. 57.63%, 34/59), whereas higher education had one of the highest ICRRs (69.81%, 37/53 pre-pandemic vs. 78.43%, 40/51 pandemic). High school graduates consistently had the highest ICRR (71.91%, 64/89 vs. 66.67%, 48/72). Statistical tests confirmed a strong association (Chi-Square p < 0.0001 vs. p = 0.0001, Cramer’s V 0.2995 vs. 0.2776), with the CMH test (p = 0.0011) confirming consistency across both periods.
Residence type and ICRR
Residence type was significantly associated with ICRR before the pandemic but weakened during the pandemic. Urban patients constituted 67.14% (286/426) pre-pandemic and 72.96% (259/355) during the pandemic, with ICRR decreasing from 59.79% (171/286) to 56.37% (146/259). Rural patients accounted for 32.86% (140/426) pre-pandemic and 27.04% (96/355) during the pandemic, with ICRR increasing from 42.86% (60/140) to 51.04% (49/96). The association was significant pre-pandemic (Chi-Square p = 0.0010, Cramer’s V = 0.1596), indicating a small-to-moderate effect size, but became non-significant during the pandemic (Chi-Square p = 0.3701, Cramer’s V = 0.0476). Statistical tests confirmed that the association remained stable over time (CMH test p = 0.0021, Breslow-Day test p = 0.1391).
Income source and ICRR
Employment status did not significantly impact ICRR in either period. Unemployed individuals comprised 41.55% (n = 177) pre-pandemic and 42.82% (n = 152) pandemic, with an ICRR of 50.85% (n = 90) vs. 52.63% (n = 80). Employed patients accounted for 20.66% (n = 88) vs. 21.69% (n = 77), with ICRR of 52.27% (n = 46) vs. 50.65% (n = 39). Retired individuals represented 36.15% (n = 154) vs. 32.96% (n = 117), refusing consent at 57.79% (n = 89) vs. 61.54% (n = 72). Students were 0.94% (n = 4) pre-pandemic and 1.97% (n = 7) pandemic, with confirmation rates of 75.00% (n = 3) vs. 42.86% (n = 3). Other income sources accounted for 0.70% (n = 3) vs. 0.56% (n = 2), refusing to consent 100% (3/3) vs. 50% (1/2).
Statistical tests indicated a weak to moderate and non-significant association (Chi-Square p = 0.2908 pre-pandemic, p = 0.4948 pandemic; Cramer’s V 0.1080 vs. 0.0977). The CMH test (p = 0.0329).
Clinical and psychiatric symptoms
Psychotic symptoms and ICRR
Psychotic symptoms at admittance strongly influenced ICRR in both periods (pre-pandemic vs. pandemic; Table 2). Patients with psychotic symptoms had higher ICRR (69.65%, 179/257 vs. 69.92%,165/236) while those without had lower ICRR (30.77%, [52/169] vs. pandemic 25.21%, [30/119]). The association was substantial and statistically significant pre-pandemic (Chi-Square p < 0.0001, Cramer’s V 0.3818) and became even stronger during the pandemic (p < 0.0001, Cramer’s V 0.4241). The relationship remained stable over time (CMH [p < 0.0001], Breslow-Day [p = 0.3851]), suggesting that psychotic symptoms remained a strong and consistent predictor of ICRR, unaffected by pandemic-related factors.
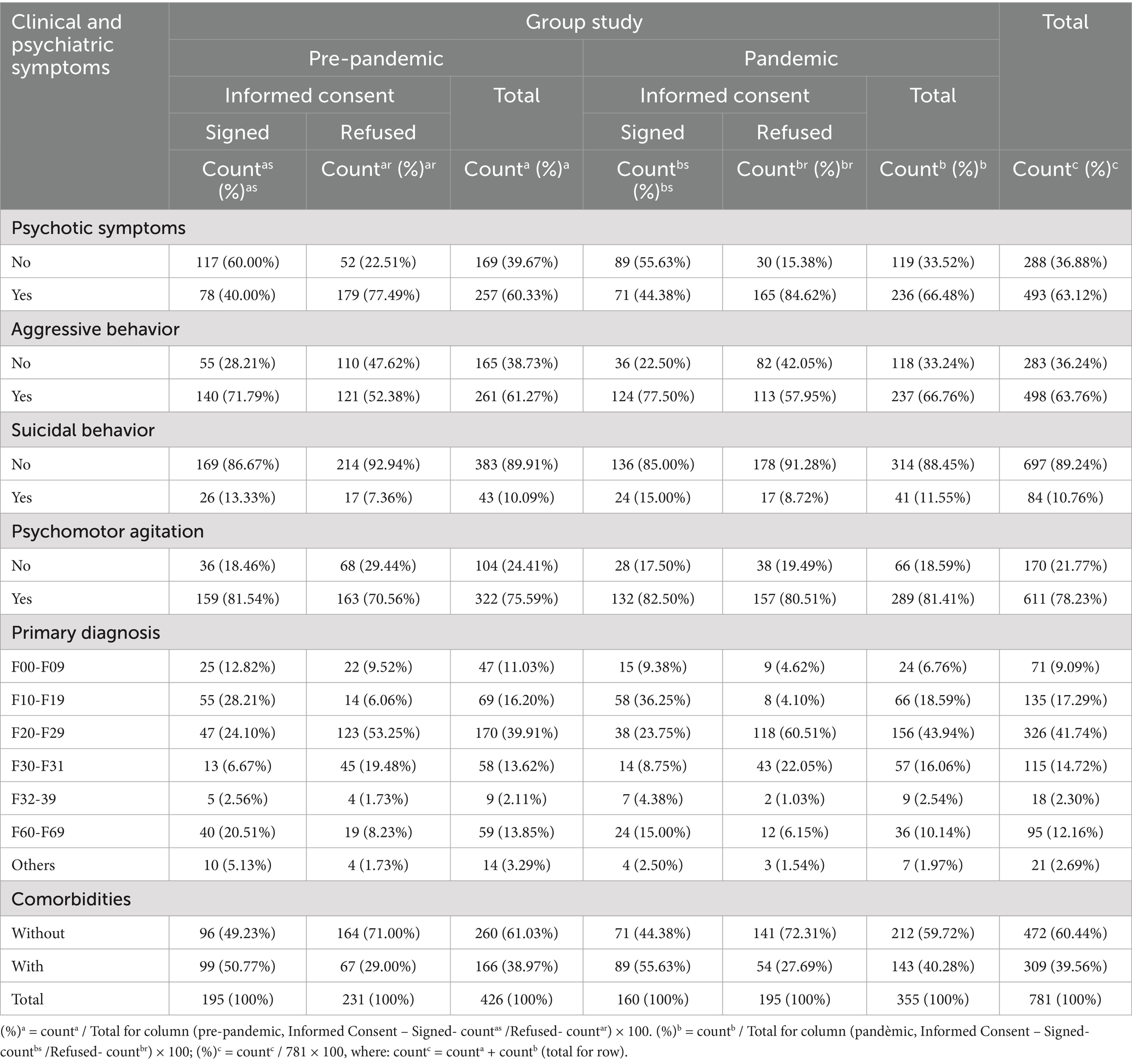
Table 2. Distribution of informed consent refusal rates (ICRR) by clinical and psychiatric factors across pre-pandemic and pandemic periods.
Aggressive behavior and ICRR
Aggressive behavior was significantly associated with ICRR across both periods. The proportion of patients exhibiting aggressive behavior increased from 61.27% (261/426) pre-pandemic to 66.76% (237/355) during the pandemic, with the ICRR slightly rising from 46.36% (121/261) to 47.68% (113/237). Non-aggressive cases decreased from 38.73% (165/426) to 33.24% (118/355), nevertheless their ICRR slightly increased too (66.67% [110/165] pre-pandemic to 69.49% [82/118] pandemic). Statistical tests confirmed a small to moderate and stable association. Chi-square tests were significant pre-pandemic (p < 0.0001, Cramer’s V = 0.1986) and during the pandemic (p < 0.0001, Cramer’s V = 0.2065). Controlling for the Study_Group, the Mantel–Haenszel test (p < 0.0001) reinforced the association. Non-aggressive individuals were likelier to have their informed consent refused despite the higher prevalence of aggression among admitted patients [Mantel–Haenszel odds ratio (0.418, 95% CI: 0.3078–0.5676)]. This relationship remained consistent over time (Breslow-Day test [p = 0.8070]).
Suicidal behavior and ICRR
Suicidal behavior showed a weak association with informed consent refusal, with slightly higher ICRR in both study periods. The majority of patients did not exhibit suicidal behavior (89.91% [383/426] vs. 88.45% [314/355]), with ICRR at 55.87% (214/383) vs. 56.69% (178/314). Before the pandemic, 10.09% (43/426) of patients exhibited suicidal behavior, increasing slightly to 11.55% (41/355) during the pandemic. Among suicidal patients, ICRR was 39.53% (17/43) vs. 41.46% (17/41). Statistical tests confirmed a weak but stable association between suicidal behavior and ICRR. Chi-square tests were significant pre-pandemic (p = 0.0414, Cramer’s V = 0.0988) but only marginally substantial during the pandemic (p = 0.0654, Cramer’s V = 0.0978). Controlling for the Study Group, suicidal behavior patients had lower odds of ICRR compared to non-suicidal patients (Mantel–Haenszel odds ratio [0.5283, 95% CI: 0.3332–0.8375], p = 0.0061). This relationship remained stable over time (Breslow-Day test [p = 0.9204]), suggesting no significant change in how suicidal behavior influenced informed consent decisions during the pandemic.
Psychomotor agitation and ICRR
Before the pandemic, 75.59% (322/426) of involuntary admissions involved patients with psychomotor agitation, increasing to 81.41% (289/355) during the pandemic, while those without agitation decreased from 24.41% (104/426) to 18.59% (66/355). Among patients without agitation, ICRR decreased from 65.38% (68/104) pre-pandemic to 57.58% (38/66) during the pandemic. In contrast, among those with agitation, ICRR increased from 50.62% (163/322) pre-pandemic to 54.33% (157/289) during the pandemic. Statistical analysis confirmed that before the pandemic, psychomotor agitation was significantly associated with ICRR (Chi-Square p = 0.0086, Cramer’s V = 0.1273), suggesting that agitation influenced refusal rates during this period. However, this association weakened and became non-significant during the pandemic (Chi-Square p = 0.6320, Cramer’s V = 0.0254), indicating that psychomotor agitation was no longer a significant factor in refusal decisions.
Primary diagnosis and ICRR
Schizophrenia spectrum disorders (F20-F29) remained the most prevalent diagnosis, increasing from 39.91% (170/426) pre-pandemic to 43.94% (156/355) pandemic, with ICRR of 72.35% (123/170) pre-pandemic vs. 75.64% (118/156) pandemic. Bipolar affective disorders (F30-F31) rose from 13.62% (58/426) to 16.06% (57/355), with ICRR at 77.59% (45/58) pre-pandemic vs. 75.44% (43/57) pandemic. Substance-related disorders (F10-F19) increased from 16.20% (69/426) to 18.59% (66/355), with ICRR decreasing from 20.29% (14/69) to 12.12% (8/66). Neurocognitive disorders (F00-F09) declined from 11.03% (47/426) to 6.76% (24/355), with ICRR of 46.81% (22/47) pre-pandemic vs. 37.50% (9/24) pandemic. Personality and behavior disorders (F60-F69) decreased from 13.55% (59/426) to 10.14% (36/355), with a slight increase in ICRR: 32.20% (19/59) pre-pandemic vs. 33.33% (12/36) pandemic. The percentage of people diagnosed with other affective disorders (F32-F39) remained relatively constant over the two periods: 2.11% (9/426) pre-pandemic vs. 2.54% (9/355) pandemic, with an ICRR of 44.44% (4/9) vs. 22.22% (2/9). The other mental disorders, which do not fall into the categories mentioned above, have decreased during the pandemic period (3.29% [14/426] vs. 1.97% [7/355]), with an increase of ICRR 28.57% (4/14) pre-pandemic vs. 42.86% (3/7). Statistical analysis confirmed a strong association between primary diagnosis and ICRR, with Chi-Square tests showing significance (p < 0.0001 pre-pandemic, Cramer’s V = 0.4908 vs. p < 0.0001 pandemic, Cramer’s V = 0.5297), and the Cochran–Mantel–Haenszel (CMH) test (p < 0.0001) reinforcing that primary diagnosis consistently influenced ICRR across both periods.
Comorbidities and ICRR
The psychiatric comorbidities significantly influenced ICRR in both periods. Before the pandemic, 38.97% (166/426) of patients had at least one comorbidity, increasing slightly to 40.28% (143/355) during the pandemic. Among patients without comorbidities, ICRR were 63.08% (164/260) pre-pandemic vs. 66.51% (141/212) pandemic, while those with comorbidities had lower ICRR [40.36% (67/166) vs. 37.76% (54/143)].
Statistical tests confirmed a stable but significant association (Chi-Square p < 0.0001 pre- vs. pandemic) with a weak-to-moderate effect (Cramer’s V −0.2224 pre-pandemic, −0.2834 pandemic). When controlling for group study, patients with comorbidities had significantly lower odds of ICRR (CMH p < 0.0001, OR = 0.3525, 95% CI: 0.2622–0.4741). The Breslow-Day test (p = 0.3928) indicated no significant shift in association over time, implying that pandemic-related factors did not alter the influence of comorbidities on IA decisions.
Behavioral factors and substance use
Alcohol consumption and ICRR
Alcohol consumers accounted for 34.51% (147/426) pre-pandemic and 34.08% (121/355) during the pandemic, with ICRR decreasing from 31.29% (46/147) to 20.66% (25/121; Table 3). Non-drinkers made up 65.49% (279/426) pre-pandemic and 65.92% (234/355) during the pandemic, with ICRR increasing from 66.31% (185/279) to 72.65% (170/234). Statistical tests confirmed a moderate-to-strong inverse relationship between alcohol consumption and ICRR, with a significant effect pre-pandemic (Chi-Square p < 0.0001, Cramer’s V = 0.3341) and a stronger effect during the pandemic (Chi-Square p < 0.0001, Cramer’s V = 0.4953). Alcohol consumers were more likely to provide informed consent compared to non-drinkers (CMH test p < 0.0001, OR = 0.1632, 95% CI: 0.1175–0.2266) and the effect of alcohol consumption on ICRR differed across periods (Breslow-Day test, p = 0.0127).
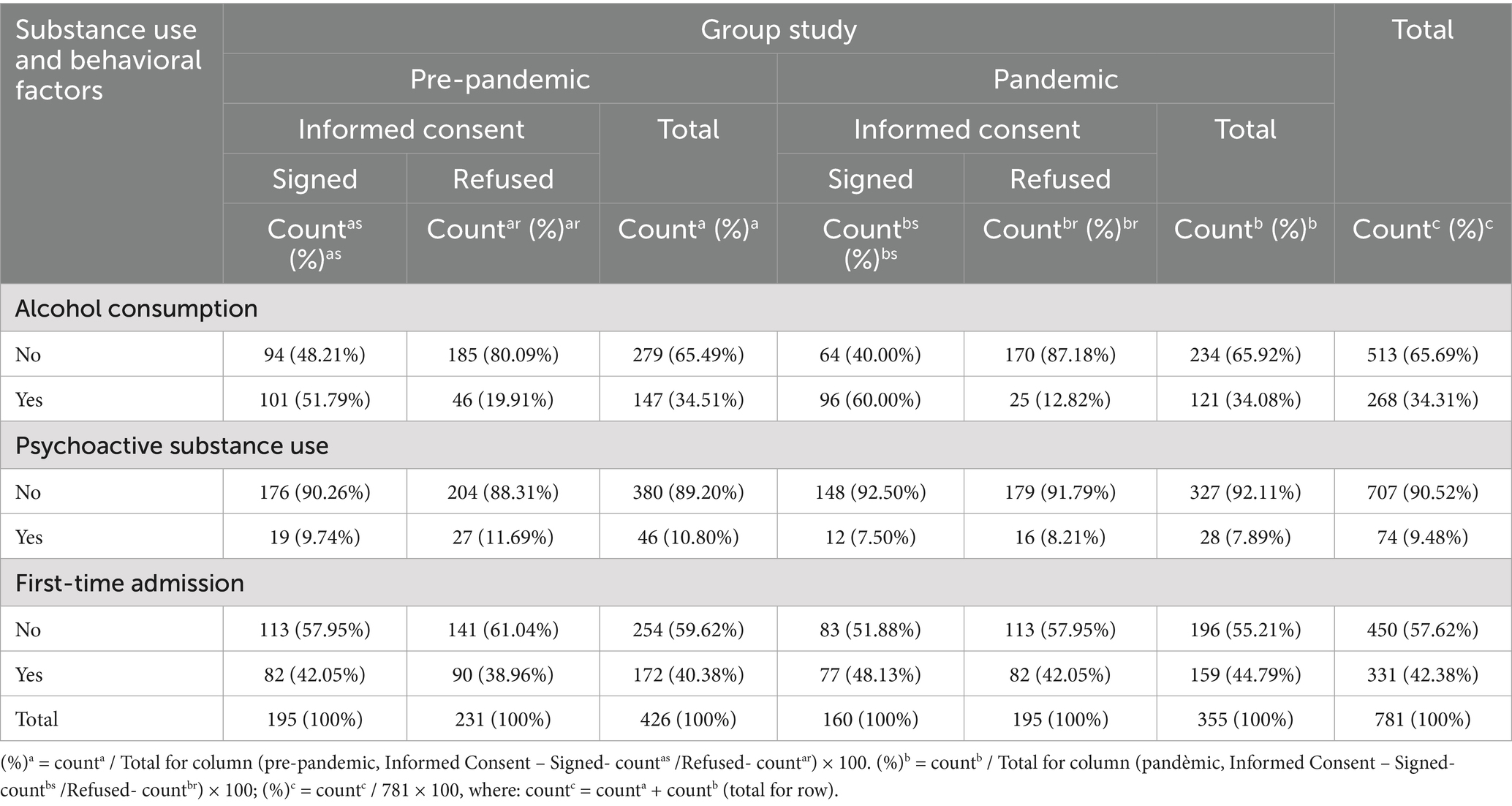
Table 3. Distribution of informed consent refusal rates (ICRR) by behavioral and substance use factors across pre-pandemic and pandemic periods.
Psychoactive substance use and ICRR
Substance users comprised 10.80% (46/426) pre-pandemic and 7.89% (28/355) during the pandemic, with ICRR slightly decreasing from 58.70% (27/46) to 57.14% (16/28). Non-users accounted for 89.20% (380/426) pre-pandemic and 92.11% (327/355) during the pandemic, with ICRR remaining stable at 53.68% (204/380) vs. 54.74% (179/327). Statistical tests confirmed no significant association between psychoactive substance use and ICRR, with non-significant Chi-Square results pre-pandemic (p = 0.5194, Cramer’s V = 0.0312) and during the pandemic (p = 0.8063, Cramer’s V = 0.0130). The CMH test (p = 0.5115) reinforced this conclusion, while the Breslow-Day test (p = 0.8344) revealed a stable relationship over time.
First-time admission and ICRR
First-time admissions accounted for 40.38% (172/426) pre-pandemic and increased slightly to 44.79% (159/355) during the pandemic, with ICRR remaining stable at 52.33% (90/172) vs. 51.57% (82/159). Previously hospitalized patients comprised 59.62% (254/426) pre-pandemic and 55.21% (196/355) during the pandemic, with ICRR at 55.51% (141/254) vs. 57.65% (113/196). Statistical analysis confirmed no significant association between first-time admission status and ICRR, with non-significant Chi-Square results pre-pandemic (p = 0.5172, Cramer’s V = 0.0314) and during the pandemic (p = 0.2522, Cramer’s V = 0.0608). This association was reinforced by the CMH test (p = 0.2109), which remained stable across both periods while the Breslow-Day test (p = 0.6879) indicated that the relationship remained stable across both periods.
Legal and admission circumstances
Police involvement and ICRR
Patients not brought in by law enforcement comprised 38.03% (162/426) pre-pandemic and 35.77% (127/355) during the pandemic, with ICRR increasing from 62.35% (101/162) to 67.72% (86/127; Table 4). Among police-referred patients, who made up 61.97% (264/426) pre-pandemic and 64.23% (228/355) during the pandemic, ICRR remained lower at 49.24% (130/264) vs. 47.81% (109/228). Statistical analysis confirmed a significant and stable inverse association between police involvement and ICRR, with a stronger effect during the pandemic (Chi-Square p = 0.0084, Cramer’s V = 0.1277 pre-pandemic; p = 0.0003, Cramer’s V = 0.1918 pandemic). Police-referred patients had significantly lower odds of ICRR compared to non-police cases (CMH test p < 0.0001, OR = 0.5149, 95% CI: 0.3818–0.6945), while the Breslow-Day test (p = 0.3401) confirmed that this association remained stable across both periods.

Table 4. Distribution of informed consent refusal rates (ICRR) by legal and admission circumstances across pre-pandemic and pandemic periods.
IA request source and ICRR
During the pandemic, the ICRR increased mainly among children-initiated referrals, rising from 48.72% (19/39) pre-pandemic to 64.44% (29/45). Spouse-initiated refusals also increased, from 53.33% (24/45) to 66.67% (14/21), while the ICRR in the cases of patients with Involuntary Admission Request by parents has increased from 63.11% (65/103) to 66.67% (52/78). In contrast, doctor-initiated ICRR significantly decreased, from 87.10% (27/31) pre-pandemic to 61.54% (24/39). Police-initiated refusals remained relatively stable, showing a slight decrease from 41.42% (70/169) to 40.97% (59/144), while sibling-initiated refusals declined from 66.67% (26/39) to 60.71% (17/28). Statistical analysis confirmed a significant association between referral source and ICRR in both periods, with Chi-Square tests yielding p < 0.0001 pre-pandemic (Cramer’s V = 0.2691) and p = 0.0015 during the pandemic (Cramer’s V = 0.2347). The CMH test (p < 0.0001) reinforced a strong association between referral source and ICRR.
Readmission and ICRR
Before the pandemic, patients hospitalized involuntarily for the first time made up 77.46% (330/426), increasing to 82.54% (293/355) during the pandemic. Among them, ICRR remained stable at 53.94% (178/330) pre-pandemic vs. 54.27% (159/293) during the pandemic. Readmitted patients accounted for 22.54% (96/426) pre-pandemic and 17.46% (62/355) during the pandemic, with ICRR showing minimal change at 55.21% (53/96) vs. 58.06% (36/62). Statistical analysis confirmed no significant association between readmission and ICRR in either period (Chi-Square p = 0.5850, Cramer’s V = 0.0290, CMH p = 0.6053). The Mantel–Haenszel odds ratio (OR = 1.0975, 95% CI: 0.7715–1.5612) indicated that hospitalization history did not influence the likelihood of ICRR. The Breslow-Day test (p = 0.7783) confirmed that this relationship remained stable.
Restraint and timing factors
Physical restraint and ICRR
The proportions of patients requiring restraint increased from 32.63% (139/426) to 36.90% (131/355) with ICRR slightly rising from 52.52% (73/139) to 54.20% (71/131; Table 5). The number of patients who did not require physical restraint decreased from 67.37% (287/426) pre-pandemic to 63.10% (224/355) during the pandemic with ICRR remaining stable at 55.05% (158/287) pre-pandemic vs. 55.36% (124/224) during the pandemic. Statistical analysis confirmed no significant association between physical restraint and ICRR in either period (pre-pandemic: Chi-Square p = 0.6225, Cramer’s V = 0.0238); pandemic: Chi-Square (p = 0.8323, Cramer’s V = 0.0112), while the Breslow-Day test (p = 0.8554) showed that the association remained stable over time.
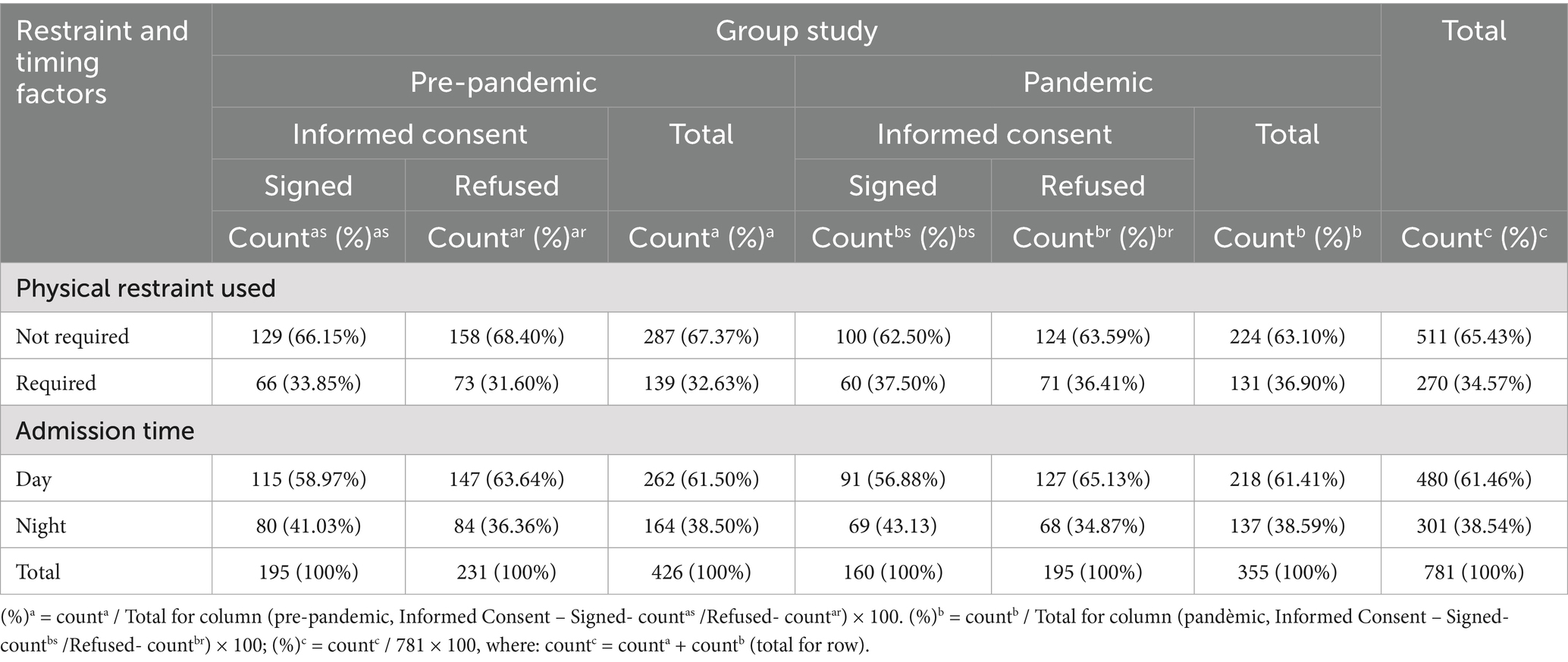
Table 5. Distribution of informed consent refusal rates (ICRR) by restraint use and admission timing across pre-pandemic and pandemic periods.
Admission time and ICRR
The proportion of daytime admissions remained consistent, with 61.50% (262/426) pre-pandemic and 61.41% (218/355) during the pandemic, ICRR increasing slightly from 56.11% (147/262) to 58.26% (127/218). Nighttime admissions also showed stability at 38.50% (164/426) pre-pandemic and 38.59% (137/355) during the pandemic with ICRR remaining nearly unchanged at 51.22% (84/164) pre-pandemic and 49.64% (68/137) during the pandemic. Statistical analysis confirmed no significant association between admission timing and ICRR in either period (pre-pandemic: Chi-Square p = 0.3245, Cramer’s V = 0.0477; pandemic: Chi-Square p = 0.1120, Cramer’s V = 0.0844). The relationship remained stable across both periods (Breslow-Day test, p = 0.6101), suggesting that external crises, such as pandemic-related stressors, did not significantly influence when patients were admitted involuntarily.
Machine learning model
The logistic regression model predicted the likelihood of ICRR = 1 based on the key sociodemographic, clinical, and behavioral factors that demonstrated statistical significance and were consistently supported across all preliminary analyses. Specifically, we retained for our final regression model education level, alcohol consumption, substance disorders, and police-initiated admissions based on Wald χ2 (p < 0.05). The model (Equation 1) showed strong predictive ability (AUC = 0.807) and statistical significance (Likelihood Ratio χ2 = 242.56, p < 0.0001), while exhibiting good calibration (Hosmer–Lemeshow χ2(8) = 12.59, p = 0.13; Figure 1).

Figure 1. The receiver operating characteristic (ROC) curve of the logistic regression model plotting sensitivity (true positive rate) against 1—specificity (false positive rate) at various threshold settings.
Education level emerged as a strong predictor of ICRR, with higher education levels associated with an increased likelihood of refusal. Compared to patients with no formal education, those with higher education were more than four times as likely to refuse consent (OR = 4.153, 95% CI: 1.748–9.862, p = 0.0013), while those with high school education were also significantly more likely to refuse (OR = 4.339, 95% CI: 1.949–9.660, p = 0.0003). Patients with middle school education (OR = 2.767, 95% CI: 1.249–6.130, p = 0.0121) and primary education (OR = 3.198, 95% CI: 1.460–7.006, p = 0.0037) also showed significantly higher refusal rates. Alcohol consumption was associated with a significantly lower likelihood of refusal, as alcohol consumers were 43% less likely to refuse consent compared to non-drinkers (OR = 0.570, 95% CI: 0.353–0.921, p = 0.0216). Similarly, patients diagnosed with substance-related disorders were 66% less likely to refuse consent (OR = 0.343, 95% CI: 0.164–0.716, p = 0.0044), suggesting that individuals with impaired cognitive insight or substance dependency may be more compliant with hospitalization decisions. Police-initiated involuntary admissions were also significantly associated with a lower likelihood of refusal, as patients brought in by law enforcement were 50% less likely to refuse consent (OR = 0.500, 95% CI: 0.294–0.851, p = 0.0106) compared to those admitted through parent-initiated referrals. This likely reflects the acute nature of crises requiring law enforcement intervention, where immediate hospitalization is deemed necessary.
Discussion
To the best of our knowledge, this study offers the first in-depth comparison of IA in Romania before and during the COVID-19 pandemic, revealing significant shifts in patient profiles and admission patterns. Consistent with international reports (24, 41), overall psychiatric admissions declined during the pandemic, while IA cases—particularly involving psychotic disorders—remained frequent or increased (28, 34, 42–44).
Demographic trends offered additional insights into the impact of the pandemic on IA. Gender-specific patterns emerged, with female patients showing increased IA and ICRR, and male patients showing decreases partially echoing previous findings (45–47). Age effects were minimal, contrasting with studies that highlight older adults as high-risk (47). Marital status became more relevant during the pandemic: single individuals had higher IA rates, reinforcing prior evidence on social support’s protective role (35, 48). Education level, notably, was associated with increased ICRR during the pandemic, especially among those with higher education. Though this contrasts with some earlier findings (21, 35), it may reflect growing autonomy or mistrust, warranting cautious interpretation and further investigation.
Geographical and behavioral factors further shaped refusal patterns. Urban–rural patterns shifted such that while urban patients had higher ICRR pre-pandemic (21), refusal rates rose among rural patients during the pandemic, possibly reflecting healthcare access barriers or changing clinical judgment. Additionally, substance and alcohol use were associated with lower refusal odds, potentially due to symptom remission post-detoxification. This diverges from literature identifying substance use as a risk factor for IA (49–51) suggesting the need for alternative, short-term containment strategies outside the IA framework.
Institutional dynamics also influenced the course of admissions. Family-initiated IA requests declined during the pandemic, while police-initiated ones increased. The relationships of dependency and control that may exist between the patient and first-degree relatives, as evidenced in studies of family abuse (52), may pose a risk for manipulation of the decision-making process, using involuntary admission as a tool of coercion. Although police involvement is commonly linked to IA in prior research (53, 54), our data show an association with reduced refusal, possibly reflecting a shift toward voluntary care once crises were managed. Meanwhile, physical restraint use and admission timing remained stable, contrary to other reports (7, 55), suggesting that these procedural elements were less affected by pandemic pressures in our setting.
Clinical presentation played a critical role in shaping IA outcomes during the pandemic. Suicidal behavior rose markedly among involuntarily admitted patients (34), aligning with broader literature on pandemic-induced psychological distress (56, 57). These findings underscore the importance of early intervention and sustained psychological support, particularly in crisis contexts (58, 59). Psychomotor agitation remained the leading reason for IA and slightly increased, often co-occurring with aggression—supporting its role as a precursor symptom (56, 60). However, aggression itself was not linked to higher confirmation rates, possibly due to the stabilizing effect of hospitalization (48, 61, 62).
Diagnostic consistency across the two periods provides additional context. Schizophrenia-spectrum disorders (F20–F29) remained the most common diagnoses, followed by substance-related (F10–F19) and bipolar disorders (F30–F31), aligning with international data (20, 63). Our findings also mirror Romanian studies showing reduced general admissions but increased IA, particularly for psychotic disorders during lockdown (28). These trends may reflect reduced outpatient access and escalating symptom severity, especially among patients with schizophrenia.
The machine learning analysis adds further nuance to these findings. Education level, substance use, and police involvement emerged as significant predictors of ICRR. Unlike prior models (35, 36) we observed a progressive increase in refusal odds with higher education. On the other hand, substance and alcohol use were linked to lower refusal odds, consistent with clinical improvement post-intoxication. Although aggressiveness and certain diagnoses like schizophrenia are established predictors in earlier studies (35, 36), their indirect influence in our model suggests the relevance of context-specific factors and the need for model refinement. The logistic regression model demonstrated robust predictive performance (AUC = 0.807), surpassing previously reported moderate outcomes (AUC = 0.68–0.72) and closely approaching results from advanced machine learning approaches (AUC = 0.84) (35, 36). These comparative insights emphasize the importance of context-specific predictor selection and the potential value of integrating comprehensive clinical, sociodemographic, behavioral, and textual electronic health records (EHR) to enhance predictive accuracy and clinical utility for involuntary psychiatric admissions. Integrated into the EHR, the model would serve as a point-of-intake decision-support tool, flagging patients at high risk of ICRR on the basis of education level, alcohol or substance use, and procedural (police involvement) factors. Targeted interventions such as extended consent discussions, early involvement of patient advocates, or tailored educational materials could then be deployed. Over time, this screening workflow may streamline triage, optimize resource allocation (e.g., assigning more time or specialist staff to high-risk cases), and ultimately reduce coercion by identifying candidates for voluntary engagement before involuntary admission becomes necessary. Prospective validation studies and careful calibration in diverse clinical settings will be essential to minimize false positives and ensure the model complements clinician judgment and patient autonomy.
Overall our findings highlight the complex, multi-layered nature of IA decisions during public health crises—shaped by individual, social, clinical, and institutional dimensions. The limited use of machine learning in this area underscores its potential to inform timely interventions and reduce unnecessary coercion in psychiatric care.
Strengths and limitations
The present study possesses distinct methodological strengths, yet it is also subject to several limitations. Data collection was conducted retrospectively over 48 months, which could affect the generalizability of the study results. Another limitation of the study is the inclusion of all presentations for an individual with multiple hospitalizations which resulted in duplication of some socio-demographic data. Although this information could reflect changes over the period analyzed (such as marital status, background, insured status, occupation, educational level or age), this was not explicitly controlled for in the analysis. Nevertheless, because the data were anonymized, it was impossible to identify readmitted individuals, assess differences in symptomatology during multiple relapses and include relevant data in this study. Significant variations between health systems and differences in legislation on involuntary admission limit the international comparison of results. Nonetheless, collaborative international studies (21, 35, 46, 64) remain essential to explore the prevalence and characteristics of nonvoluntary hospitalizations and readmissions in diverse settings and cultures, using uniform assessment instruments and standardized methodology. Despite these limitations, the large sample size and the detailed analysis of multiple sociodemographic, clinical and procedural aspects allowed a rigorous and accurate estimation of data from the study population.
Additionally, the machine learning approach employed in our study has limitations when compared to previous reports. Unlike advanced machine learning methods, such as those used by Perfalk et al. (36), our logistic regression model does not inherently account for complex interactions among variables, potentially limiting its predictive accuracy. However, employing interaction terms in logistic regression models would complicate interpretation significantly, making it challenging to translate statistical findings into actionable clinical guidelines. Moreover, the absence of detailed clinical indicators (e.g., aggressiveness scales and specific diagnostic categories) in our analysis, highlighted as significant in prior studies (35, 36) may have constrained our model’s ability to fully capture the multidimensional nature of psychiatric admissions. Nevertheless, including such detailed clinical variables would significantly increase model complexity and potentially diminish practical usability due to more complicated data collection and analysis requirements. Future studies would benefit from balancing detailed clinical information and interpretative clarity with advanced analytical techniques to enhance model performance and clinical applicability.
Furthermore, the single-center design, drawing on data from a single Romanian psychiatric hospital, limits the external validity of both the descriptive findings and the predictive model, given regional differences in admission practices, legal frameworks, and resources. Multicenter studies across diverse healthcare settings are therefore needed to corroborate and extend these results. Accordingly, the predictive algorithm, developed and tested within the same cohort, requires external validation; its robustness and generalizability must be confirmed in independent datasets before wider clinical implementation can be further recommended.
Conclusion
The COVID-19 pandemic posed significant challenges to health systems worldwide, profoundly affecting psychiatric care and involuntary admissions. In a context marked by severe restrictions, limited resources, and uncertainty, the patterns of involuntary hospitalizations shifted notably, highlighting psychotic symptoms as a key factor in ICRR. Socio-demographic factors, such as gender, education level, and marital status, along with behavioral factors like alcohol use and police involvement, significantly influenced admission outcomes. Predictive modeling further identified education level, alcohol consumption, substance-related disorders, and police-initiated referrals as significant independent predictors of consent refusal, providing valuable insights to anticipate hospitalization needs and inform clinical decision-making. These findings underscore the need for targeted psychiatric interventions and comprehensive crisis management strategies, particularly for vulnerable patient groups. Establishing a unified procedural framework through inter-institutional collaboration between medical, judicial, and law enforcement authorities is essential to address the complex medical and legal aspects of involuntary admissions, ensuring the protection of patients’ fundamental rights.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the first author, upon reasonable request. The code related to this work is available at: https://github.com/bogdanneamtu76/Inv_Admissions.git.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Clinical Hospital of Psychiatry No. 5381/21.04.2023. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because of the retrospective nature of the study.
Author contributions
CB: Investigation, Supervision, Validation, Methodology, Data curation, Conceptualization, Writing – review & editing, Resources, Writing – original draft, Project administration, Funding acquisition, Formal analysis. MC: Writing – review & editing. BV: Writing – review & editing, Formal analysis. AL: Writing – review & editing. AB: Formal analysis, Writing – review & editing. AG: Data curation, Methodology, Validation, Investigation, Conceptualization, Writing – review & editing, Resources, Formal analysis, Project administration, Writing – original draft. CM: Writing – review & editing, Formal analysis. BN: Resources, Writing – original draft, Visualization, Formal analysis, Software, Validation, Conceptualization, Data curation, Supervision, Methodology, Writing – review & editing, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Specifically, the research was financed by Lucian Blaga University of Sibiu (grant LBUS-IRG-2021-07) and by the Hasso Plattner Foundation, and carried out in collaboration with the Department of Clinical Research at the Pediatric Clinical Hospital of Sibiu.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
COVID-19, The Coronavirus disease; ICD-10, The International Classification of Diseases 10th Revision; DSM-5, The Diagnostic and Statistical Manual of Mental Disorders; CI, Confidence Interval; ICRR, informed consent refusal rate; IA, involuntary admission.
References
1. Cucinotta, D, and Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
2. World Health Organization. COVID-19 Epidemiological Update: Special Edition 174. (2024). Available online at: https://cdn.who.int/media/docs/default-source/documents/emergencies/20241224_covid-19_epi_update_special-edition.pdf?sfvrsn=b0a6ddaf_1&download=true (Accessed on 2025 Jan 2)
3. Kim, JY, Săndulescu, O, Preotescu, LL, Rivera-Martínez, NE, Dobryanska, M, Birlutiu, V, et al. A randomized clinical trial of Regdanvimab in high-risk patients with mild-to-moderate coronavirus disease 2019. Open Forum Infect Dis. (2022) 9:406. doi: 10.1093/ofid/ofac406
4. World Health Organization. Mental health and COVID-19: Early evidence of the pandemic’s impact: Scientific brief. (2022). Available online at: https://iris.who.int/bitstream/handle/10665/352189/WHO-2019-nCoV-Sci-Brief-Mental-health-2022.1-eng.pdf?sequence=1 (Accessed on 2024 Dec 12)
5. Robinson, E, Sutin, AR, Daly, M, and Jones, A. A systematic review and meta-analysis of longitudinal cohort studies comparing mental health before versus during the COVID-19 pandemic in 2020. J Affect Disord. (2022) 296:567–76. doi: 10.1016/j.jad.2021.09.098
6. Magnúsdóttir, I, Lovik, A, Unnarsdóttir, AB, McCartney, D, Ask, H, Kõiv, K, et al. Acute COVID-19 severity and mental health morbidity trajectories in patient populations of six nations: an observational study. Lancet Public Health. (2022) 7:e406–16. doi: 10.1016/S2468-2667(22)00042-1
7. Vukićević, T, Borovina Marasović, T, Botica, A, Mastelić, T, Utrobičić, T, Glavina, T, et al. Changes in the number and characteristics of tertiary hospital psychiatric admissions in South Croatia before and during the COVID-19 pandemic: a retrospective study. BMC Psychiatry. (2025) 25:17. doi: 10.1186/s12888-024-06436-1
8. Moitra, M, Owens, S, Hailemariam, M, Wilson, KS, Mensa-Kwao, A, Gonese, G, et al. Global mental health: where we are and where we are going. Curr Psychiatry Rep. (2023) 25:301–11. doi: 10.1007/s11920-023-01426-8
9. Sotelo-Monroy, GE, Villaseñor-Robledo, C, Peñaloza-Solano, G, and Tafoya-Ramos, F. Controversies between mental health and disability standards in Mexico. Rev Med Inst Mex Seguro Soc. (2023) 61:204–11.
10. Global Burden of Disease 2019 Mental Disorders Collaborators, coordinated by the Institute for Health Metrics and Evaluation. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. (2022) 9:137–50. doi: 10.1016/S2215-0366(21)00395-3
11. European Union Agency for Fundamental Rights. Involuntary Placement and Involuntary Treatment of Persons with Mental Health Problems. (2012). Available online at: https://fra.europa.eu/sites/default/files/involuntary-placement-and-involuntary-treatment-of-persons-with-mental-health-problems_en.pdf (Accessed on 2024 Dec 21)
12. Alsamiri, YA, Hussain, MA, Alsamani, OA, and Al bulayhi, AA. Promoting mental health and wellbeing as means to prevent disability: a review. Front Public Health. (2024) 12:535. doi: 10.3389/fpubh.2024.1425535
13. Kondirolli, F, and Sunder, N. Mental health effects of education. Health Econ. (2022) 31:22–39. doi: 10.1002/hec.4565
14. Stallman, HM, and Gupta, V V. Involuntary Commitment. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (2025). Available at: https://www.ncbi.nlm.nih.gov/books/NBK557377/ (Accessed July 18, 2024).
15. Tamai, S. Involuntary psychiatric admission: arbitrary deprivation of liberty or a human right? Front Psych. (2022) 13:9093. doi: 10.3389/fpsyt.2022.879093
16. Rozel, JS, Toohey, T, and Amin, P. Legal considerations in emergency psychiatry. Focus (Am Psychiatr Publ). (2023) 21:3–7. doi: 10.1176/appi.focus.20220071
17. Fiorillo, A, De Rosa, C, Del Vecchio, V, Jurjanz, L, Schnall, K, Onchev, G, et al. How to improve clinical practice on involuntary hospital admissions of psychiatric patients: suggestions from the EUNOMIA study. Eur Psychiatry. (2011) 26:201–7. doi: 10.1016/j.eurpsy.2010.01.013
18. Wasserman, D, Apter, G, Baeken, C, Bailey, S, Balazs, J, Bec, C, et al. Compulsory admissions of patients with mental disorders: state of the art on ethical and legislative aspects in 40 European countries. Eur Psychiatry. (2020) 63:e82. doi: 10.1192/j.eurpsy.2020.79
19. Jäger, M, Hotzy, F, Traber, R, Morandi, S, Schneeberger, AR, Spiess, M, et al. Kantonale Unterschiede bei der Umsetzung der fürsorgerischen Unterbringung in der Schweiz. Psychiatr Prax. (2024) 51:24–30. doi: 10.1055/a-2133-4084
20. Beysard, N, Jaquerod, X, Morandi, S, Gasser, J, and Carron, PN. Involuntary admissions to the emergency department: a retrospective observational study. Swiss Med Wkly. (2023) 153:063. doi: 10.57187/smw.2023.40063
21. Kaikoushi, K, Middleton, N, Chatzittofis, A, Bella, E, Alevizopoulos, G, and Karanikola, M. Socio-demographic and clinical characteristics of adults with psychotic symptomatology under involuntary admission and readmission for compulsory treatment in a referral psychiatric hospital in Cyprus. Front Psych. (2021) 12:602274. doi: 10.3389/fpsyt.2021.602274
22. Romanian Ombudsman – National Human Rights Institution (The People’s Advocate). Special report on monitoring the implementation of ECHR decision regarding involuntary hospitalization in psychiatric hospitals. (2024). Available online at: https://avp.ro/wp-content/uploads/2024/01/Raport-special-monitorizarea-implementarii-deciziilor-CEDO.pdf (Accessed on 2024 Nov 9)
23. Morris, NP, and Kleinman, RA. Involuntary hospitalization during the COVID-19 pandemic. American J Psychiatry Residents' J. (2020) 16:3–5. doi: 10.1176/appi.ajp-rj.2020.160102
24. Fasshauer, JM, Bollmann, A, Hohenstein, S, Mouratis, K, Hindricks, G, Meier-Hellmann, A, et al. Impact of COVID-19 pandemic on involuntary and urgent inpatient admissions for psychiatric disorders in a German-wide hospital network: inpatient psychiatric disorders during COVID-19. J Psychiatr Res. (2021) 142:140–3. doi: 10.1016/j.jpsychires.2021.07.052
25. Clerici, M, Durbano, F, Spinogatti, F, Vita, A, De Girolamo, G, and Micciolo, R. Psychiatric hospitalization rates in Italy before and during COVID-19: did they change? An analysis of register data. Ir J Psychol Med. (2020) 37:283–90. doi: 10.1017/ipm.2020.29
26. Fasshauer, JM, Bollmann, A, Hohenstein, S, Hindricks, G, Meier-Hellmann, A, Kuhlen, R, et al. Emergency hospital admissions for psychiatric disorders in a German-wide hospital network during the COVID-19 outbreak. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:1469–75. doi: 10.1007/s00127-021-02091-z
27. Jagadheesan, K, Danivas, V, Itrat, Q, Sekharan, L, and Lakra, APV. COVID-19 and psychiatric admissions: an observational study of the first six months of lockdown in Melbourne. Psychiatry Res. (2021) 300:113902. doi: 10.1016/j.psychres.2021.113902
28. Dionisie, V, Ciobanu, AM, Moisa, E, Manea, MC, and Puiu, MG. The impact of the COVID-19 pandemic on inpatient admissions for psychotic and affective disorders: the experience of a large psychiatric teaching hospital in Romania. Health. (2022) 10:570. doi: 10.3390/healthcare10081570
29. Tromans, S, Chester, V, Harrison, H, Pankhania, P, Booth, H, and Chakraborty, N. Patterns of use of secondary mental health services before and during COVID-19 lockdown: observational study. BJPsych Open. (2020) 6:e117. doi: 10.1192/bjo.2020.104
30. Carpiniello, B, Tusconi, M, Zanalda, E, and Giannantonio, M. Psychiatry during the Covid-19 pandemic: a survey on mental health departments in Italy. BMC Psychiatry. (2020) 20:593. doi: 10.1186/s12888-020-02997-z
31. Parliament of Romania. Low no. 487 of July, 2002, on mental health and the protecționism of persons with psychiatric disorders. România. (2002). Available online at: https://legislatie.just.ro/Public/DetaliiDocument/37898 (Accessed on 2024 Nov 13)
32. Government of România. (2024). Ordinance no. 18 of January 31, 2024, amending Article 55 of Law no. 487/2002. Available online at: https://sgg.gov.ro/1/wp-content/uploads/2024/01/OG-14.pdf (Accessed October 2, 2024).
33. Bergstresser, SM. Involuntary PSychIatrIc commItment in the era of covId-19. Int J Critical Diversity Stud. (2021) 4:93–108. doi: 10.13169/intecritdivestud.4.1.0092
34. Băcilă, C, Ștef, L, Bucuță, M, Anghel, CE, Neamțu, B, Boicean, A, et al. The impact of the COVID-19 pandemic on the management of mental health services for hospitalized patients in Sibiu county—central region, Romania. Health. (2023) 11:291. doi: 10.3390/healthcare11091291
35. Silva, B, Gholam, M, Golay, P, Bonsack, C, and Morandi, S. Predicting involuntary hospitalization in psychiatry: a machine learning investigation. Eur Psychiatry. (2021) 64:2220. doi: 10.1192/j.eurpsy.2021.2220
36. Perfalk, E, Damgaard, JG, Bernstorff, M, Hansen, L, Danielsen, AA, and Østergaard, SD. Predicting involuntary admission following inpatient psychiatric treatment using machine learning trained on electronic health record data. Psychol Med. (2024) 54:4348–61. doi: 10.1017/S0033291724002642
37. National Institute of Puplic Health (NIPH). National Institute of Puplic Health (NIPH). Situation analysis 2021. (2021). Available online at: https://insp.gov.ro/download/analiza-de-situatie-2021-pdf/ (Accessed on 2025 Jan 4)
38. World Health Organization. International statistical classification of diseases and related health problems, 10th revision (ICD-10). Geneva: World Health Organization (2019).
39. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, fifth edition, text revision (DSM-5-TR). Fifth, text revision. Washington, DC: American Psychiatric Association Publishing (2022).
41. Simon, J, Helter, TM, White, RG, van der Boor, C, and Łaszewska, A. Impacts of the Covid-19 lockdown and relevant vulnerabilities on capability well-being, mental health and social support: an Austrian survey study. BMC Public Health. (2021) 21:314. doi: 10.1186/s12889-021-10351-5
42. Simpson, SA, Loh, RM, Cabrera, M, Cahn, M, Gross, A, Hadley, A, et al. The impact of the COVID-19 pandemic on psychiatric emergency service volume and hospital admissions. J Acad Consultation-Liaison Psychiatry. (2021) 62:588–94. doi: 10.1016/j.jaclp.2021.05.005
43. Kalanj, K, Ćurković, M, Peček, M, Orešković, S, Orbanić, A, and Marshall, R. Impact of the COVID-19 pandemic on acute mental health admissions in Croatia. Front Public Health. (2023) 11:796. doi: 10.3389/fpubh.2023.1231796
44. Fellinger, M, Waldhör, T, Vyssoki, B, Amering, M, Leutgeb, L, Gschaider, A, et al. A country report: impact of COVID-19 lockdowns on involuntary psychiatric treatment in Austria. BJPsych Open. (2024) 10:e9. doi: 10.1192/bjo.2023.610
45. Bornheimer, LA, Li Verdugo, J, Holzworth, J, Smith, FN, and Himle, JA. Mental health provider perspectives of the COVID-19 pandemic impact on service delivery: a focus on challenges in remote engagement, suicide risk assessment, and treatment of psychosis. BMC Health Serv Res. (2022) 22:718. doi: 10.1186/s12913-022-08106-y
46. Tanner, B, Kurdyak, P, and de Oliveira, C. Adult psychiatric hospitalizations in Ontario, Canada before and during the COVID-19 pandemic. Can J Psychiatr. (2023) 68:925–32. doi: 10.1177/07067437231167386
47. Peters, SJ, Schmitz-Buhl, M, Zielasek, J, and Gouzoulis-Mayfrank, E. Involuntary psychiatric hospitalisation – differences and similarities between patients detained under the mental health act and according to the legal guardianship legislation. BMC Psychiatry. (2024) 24:892. doi: 10.1186/s12888-024-05892-z
48. Păun, RM, Pavel, AN, Matei, VP, and Tudose, C. Risk factors for involuntary admission in a Romanian patient sample. Int J Law Psychiatry. (2023) 91:101938. doi: 10.1016/j.ijlp.2023.101938
49. Gheorman, V, Dinescu, VC, Criciotoiu, O, Stanca, D, Calborean, V, Mita, A, et al. Clinical and biochemical changes induced by alcohol at the patients with mental illness. Rev Chim. (2019) 70:1406–10. doi: 10.37358/RC.19.4.7138
50. De Giorgi, F, Menculini, G, Barbi, M, Cardelli, M, Zebi, L, Amantini, K, et al. Duration of involuntary treatment in a psychiatric inpatient unit: the experience of Umbria, Central Italy. Psychiatr Danub. (2023) 35:375–82.
51. Kandsperger, S, Ecker, A, Schleicher, D, Wirth, M, Brunner, R, and Jarvers, I. Emergency-related inpatient admissions in child and adolescent psychiatry: comparison of clinical characteristics of involuntary and voluntary admissions from a survey in Bavaria, Germany. Eur Child Adolesc Psychiatry. (2024) 33:303–13. doi: 10.1007/s00787-023-02154-3
52. Buicu, GE, Gabos Grecu, M, Salcudean, A, Gabos Grecu, I, Marinescu, C, Nirestean, A, et al. Evaluation of elder physical abuse. Eur Psychiatry. (2017) 41:S583–4. doi: 10.1016/j.eurpsy.2017.01.880
53. Van Suetendael, L, Schrijvers, T, Van den Broeck, K, Michielsen, J, Dom, G, and Destoop, M. Police and judicial actors on complex mental health care needs and judicial protection measures. Tijdschr Psychiatr. (2024) 66:477–82.
54. Hustoft, K, Larsen, TK, Brønnick, K, Joa, I, Johannessen, JO, and Ruud, T. Psychiatric patients’ attitudes towards being hospitalized: a national multicentre study in Norway. BMC Psychiatry. (2022) 22:726. doi: 10.1186/s12888-022-04362-8
55. Geen, O, Gui, S, Andreychuk, S, DeBono, T, and Yousuf, H. Restraint practices in incapable wandering patients during COVID-19: ethics and best practice recommendations. Canadian Geriatrics J. (2022) 25:324–7. doi: 10.5770/cgj.25.575
56. Ambrosetti, J, Macheret, L, Folliet, A, Wullschleger, A, Amerio, A, Aguglia, A, et al. Psychiatric emergency admissions during and after COVID-19 lockdown: short-term impact and long-term implications on mental health. BMC Psychiatry. (2021) 21:465. doi: 10.1186/s12888-021-03469-8
57. Crisan, RM, Băcilă, CI, Toboltoc, PC, and Morar, S. Completed suicide linked to the COVID-19 pandemic by using the psychological autopsy method in Sibiu County, Romania: case series and literature review. Health. (2022) 10:2377. doi: 10.3390/healthcare10122377
58. Ciciurkaite, G, Marquez-Velarde, G, and Brown, RL. Stressors associated with the COVID-19 pandemic, disability, and mental health: considerations from the intermountain west. Stress Health. (2022) 38:304–17. doi: 10.1002/smi.3091
59. Vindegaard, N, and Benros, ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
60. Weltens, I, Bak, M, Verhagen, S, Vandenberk, E, Domen, P, van Amelsvoort, T, et al. Aggression on the psychiatric ward: prevalence and risk factors. A systematic review of the literature. PLoS One. (2021) 16:e0258346. doi: 10.1371/journal.pone.0258346
61. Walker, S, Mackay, E, Barnett, P, Sheridan Rains, L, Leverton, M, Dalton-Locke, C, et al. Clinical and social factors associated with increased risk for involuntary psychiatric hospitalisation: a systematic review, meta-analysis, and narrative synthesis. Lancet Psychiatry. (2019) 6:1039–53. doi: 10.1016/S2215-0366(19)30406-7
62. Karasch, O, Schmitz-Buhl, M, Mennicken, R, Zielasek, J, and Gouzoulis-Mayfrank, E. Identification of risk factors for involuntary psychiatric hospitalization: using environmental socioeconomic data and methods of machine learning to improve prediction. BMC Psychiatry. (2020) 20:401. doi: 10.1186/s12888-020-02803-w
63. Hwang, TY, Jung, G, Lee, CJ, and Kim, HY. Analysis of involuntary admissions in Korea through the admission management information system. Int J Law Psychiatry. (2020) 68:101542. doi: 10.1016/j.ijlp.2020.101542
64. Gather, J, Juckel, G, Henking, T, Efkemann, SA, Vollmann, J, and Scholten, M. Under which conditions are changes in the treatment of people under involuntary commitment justified during the COVID-19 pandemic? An ethical evaluation of current developments in Germany. Int J Law Psychiatry. (2020) 73:101615. doi: 10.1016/j.ijlp.2020.101615
65. Ministry of Health. Order no. 488 of April 15, 2016, approving the norms for the application of Las no. 487/2002 on mental health and the protecționism f personal with psychiatric disrders. 488 Romania: Official Gazette; (2016). Available online at: https://legislatie.just.ro/Public/DetaliiDocument/178134 (Accessed November 13, 2024).
Appendix A
The context of Romania
Involuntary admission is regulated in Romania by Law no. 487/2002 on mental health and the protection of persons with mental disorders (31) and Order no. 488/2016 approving the Norms for applying this law (65). Involuntary admission is required when a licensed psychiatrist finds that a person has a mental disorder and, due to it, there is an imminent danger of harm to himself or others or in case of the existence of a severe mental disorder, when his non-admission would cause a serious deterioration of his condition or the impossibility of administering appropriate treatment and only after exhausting the options of voluntary admission (31). In such cases, the patient’s mental capacity is severely impaired, preventing them from realizing the need for these therapeutic and care measures (33). In Europe, two models are used for the establishment of the involuntary admission procedure: the medical model (also practiced in Romania), with the medical procedure prevailing in the case of the measure, where the courts exercise a secondary control role, and the legal model, where the decision to restrict liberty is exclusively a matter for the judges, hence psychiatrists having a secondary role in the application of the involuntary admission procedure (18). According to the current applicable legislation, involuntary admissions can be carried out in psychiatric hospitals and psychiatric wards with adequate conditions for specialized care under specific conditions, the latter being recently introduced by Ordinance No. 18 of January 31, 2024 (32). The involuntary admission procedure begins with the request for involuntary admission, certified under the signature of the holders provided for in Article 55 of Law 487/2002. The next step is the health assessment by the psychiatrist on duty at the psychiatric hospital, who, within 24 h of the evaluation, must send the involuntary admission notification and the related documentation to the involuntary admission committee. The involuntary admissions committee, consisting of two psychiatrists and a doctor of another specialty, considers the proposal of the psychiatrist on duty within 48 h of receipt after examining the person concerned. The decision confirming involuntary admission is then sent to the management of the health facility, which is obliged to send the decision together with the medical documents to the court within 24 h. The court stage is an emergency procedure where the participation and hearing of the patient is mandatory (on-site or online). The court may order confirmation of involuntary admission, in which case the person remains in the hospital. Alternatively, it may be found that involuntary admission is unnecessary and that outpatient treatment should replace it. After the court stage, the involuntary admissions committee is required to re-examine the patient at least once every month, depending on the patient’s condition or at the request of the people entitled to do so (the head doctor, the patient’s legal or conventional representative, the public prosecutor or the patient himself). If the conditions that led to involuntary admission are no longer met, the committee will inform the management of the health unit, which will forward the proposal to terminate involuntary admission to the court, which is the last stage of the process (31).
Keywords: involuntary admission, psychiatric hospitalization, COVID-19 pandemic, risk factors, mental health crisis, logistic regression model, predictive analysis
Citation: Impact and predictive modeling of risk factors for involuntary psychiatric admissions before and during COVID-19: insights from a Romanian tertiary hospital. Front. Public Health. 13:1624219. doi: 10.3389/fpubh.2025.1624219
Edited by:
Annarita Vignapiano, Department of Mental Health, ItalyReviewed by:
Pasquale Pezzella, University of Campania Luigi Vanvitelli, ItalyMartina D’Angelo, Magna Græcia University, Italy
Copyright © 2025 Băcilă, Cornea, Vintilă, Lomnasan, Boicean, Grama, Matei and Neamtu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andreea Maria Grama, Z2FuZHJlZWFtYXJpYUB5YWhvby5jb20=; Bogdan Neamtu, Ym9nZGFuLm5lYW10dUB1bGJzaWJpdS5ybw==