 Esteban Ortiz-Prado1*
Esteban Ortiz-Prado1* Enrique Terán2
Enrique Terán2 Karla Alejandra Cuenca1Julia Saa Echeverria1Martín Gallardo1María Paz Cadena1Mateo Barriga1
Karla Alejandra Cuenca1Julia Saa Echeverria1Martín Gallardo1María Paz Cadena1Mateo Barriga1 Jorge Vasconez-Gonzalez1
Jorge Vasconez-Gonzalez1 Juan S. Izquierdo-Condoy1
Juan S. Izquierdo-Condoy1- 1One Health Research Group, Faculty of Health Science, Universidad de Las Americas, Quito, Ecuador
- 2Colegio de Ciencias de la Salud, Universidad San Francisco de Quito USFQ, Quito, Ecuador
Background: In Latin America, public health proposals by presidential candidates often lack methodological rigor, limiting their feasibility and impact. Evidence-based planning aligned with national health priorities and disease burden is essential to address critical issues such as chronic diseases, mental health, and healthcare access.
Objective: This study evaluates the methodological robustness of public health policy proposals from 16 Ecuadorian presidential candidates for the 2025–2029 elections. The assessment focuses on key health variables, analyzing the presence of SMART objectives, epidemiological evidence, and alignment with local and global health priorities.
Methods: A systematic evaluation framework was applied to analyze the health components of each candidate’s plan. The study used internationally recognized policy evaluation models, including the CDC’s Six-Step Policy Evaluation Framework and the UK Magenta Book Guidelines. Health variables were weighted based on national priorities, with percentage scores assigned according to alignment with GBD 2021 Ecuador data. Each proposal was assessed for inclusion or omission of these variables, allowing for a comparative ranking of methodological rigor.
Results: The analysis of public health proposals from Ecuadorian presidential candidates revealed significant methodological deficiencies. A total of 81% of proposals lacked SMART objectives, limiting their ability to establish measurable goals. 76% failed to integrate key health determinants such as environmental health, intersectoral collaboration, and research funding. 92% did not include a defined financial strategy, raising concerns about feasibility. Only one candidate (Noboa/Pinto) scored above 50% compliance with the GBD Ecuador 2021 priorities. Mental health and infectious disease prevention were the most frequently addressed topics, while air pollution, food safety, and post-market drug surveillance were largely overlooked. Chronic disease care, environmental sanitation, and vaccine production were among the most underrepresented health priorities.
Conclusion: Public health proposals from Ecuadorian presidential candidates (2025–2029) showed major methodological gaps, with 81% lacking SMART objectives and 92% lacking financial plans. Key areas such as neonatal care and non-communicable disease prevention were often omitted. A more systematic, evidence-based approach is needed, supported by collaboration between policymakers, researchers, and international health agencies.
1 Introduction
Public health policies proposed by government candidates play a critical role in shaping national healthcare strategies. However, in many Latin American countries, including Ecuador, these proposals often lack methodological rigor, failing to address key public health determinants effectively. The absence of evidence-based planning, limited integration of epidemiological data, and poor financial structuring weaken the feasibility of these health initiatives (1).
Since 2007, Ecuador began the process of transforming its health sector toward universal and free access to healthcare (2). In 2008, the Constitution of Ecuador recognized the right to health with a systemic approach. That same year, the Constitution also established the State as the guarantor of the right to health through the formulation of policies, plans, and programs (3). Between 2007 and 2016, a total of USD 16.208 billion was invested in health. In 2017, the investment amounted to USD 306 million, which was reduced in subsequent years to USD 201 million in 2018 and USD 110 million in 2019 (3, 4). Later, due to the COVID-19 pandemic and the resulting additional costs, the government invested USD 897 million, of which USD 363 million were allocated to the National Vaccination Plan (5). By 2023, national health spending increased by 2.9%, reaching USD 7.773 billion. According to the 2024 Accountability Report, the most significant actions included investments in medicines, infrastructure, and medical equipment, with a total budget execution of USD 2.742 billion (6, 7).
Currently, the healthcare system faces multiple structural challenges, including persistent shortages of essential medications, which compromise equitable access to treatment (8, 9). These deficiencies are compounded by a lack of medical supplies and substandard working conditions for primary care professionals, all of which negatively impact the quality and continuity of healthcare services (10, 11). Institutional fragility further exacerbates the situation, driven in large part by the frequent turnover of health authorities, which disrupts governance and undermines strategic continuity. This issue is particularly evident within the Ministry of Public Health, where leadership positions have often been assigned to individuals with limited expertise in health policy and management. Notably, between 2023 and 2025, five different health ministers have held office (8, 12, 13). Another pressing issue and priority is the government’s debt to dialysis service providers, which amounts to 250 million USD dólares (14, 15). As a result, these providers lack the necessary medical supplies, which has even led to the death of several patients (16).
In Ecuador, past healthcare reforms have faced challenges in execution due to weak institutional structures, insufficient and irregular resource distribution, leading to unequal access to medical services, especially in rural areas (17). Additionally, the lack of interdisciplinary cooperation and the prioritization of short-term political interests have obstructed long-term advancements in public health. For example, the severe health, social, and economic consequences of the pandemic may persist for decades, due to deficiencies in the poorly functioning healthcare system, worsening social disparities. In the absence of comprehensive and forward-thinking policies, nations may experience extended recovery times, deteriorating public health conditions, and greater financial strain on vulnerable communities (18). To overcome these obstacles, it is crucial to implement evidence-based strategies to improve the efficiency and durability of health policies. It is also important to highlight that good governance enables the delivery of health services in an equitable and sustainable manner. High-quality governance in health policy formulation is a key factor in shaping the improvement of health systems, their functioning, legitimacy, and outcomes (19, 20).
The use of research evidence in public health policymaking is often inconsistent due to barriers such as restricted access to relevant studies, political and ideological influences, and the lack of systematic reviews tailored to local contexts (21, 22). Decision-makers frequently rely on anecdotal evidence or public sentiment rather than robust scientific data, which can result in policies that are misaligned with actual healthcare needs (23). Moreover, the limited application of knowledge translation strategies further impedes the implementation of research-informed policies (24).
Given these methodological deficiencies, there is an urgent need for evidence-based public health proposals. Integrating multidisciplinary evidence, fostering knowledge translation, and utilizing rapid review methodologies can strengthen public health planning (25). Furthermore, aligning policy proposals with national disease burden data, such as the Global Burden of Disease (GBD) study, ensures that healthcare priorities reflect the most pressing population health concerns (26).
This study assesses the methodological robustness of Ecuadorian presidential candidates (Figure 1) public health policy proposals for the 2025–2029 elections. This study applies internationally recognized policy evaluation frameworks—the CDC’s Six-Step Policy Evaluation Framework and the UK Magenta Book Guidelines—not as rigid protocols, but as methodological guides to assess structure, feasibility, and use of evidence in health policy proposals (27, 28). These frameworks helped inform the analysis of SMART objectives, integration of epidemiological data, financial planning, and clarity of implementation strategies. The findings highlight critical gaps and emphasize the importance of structured, evidence-based policymaking to improve health outcomes in Ecuador.
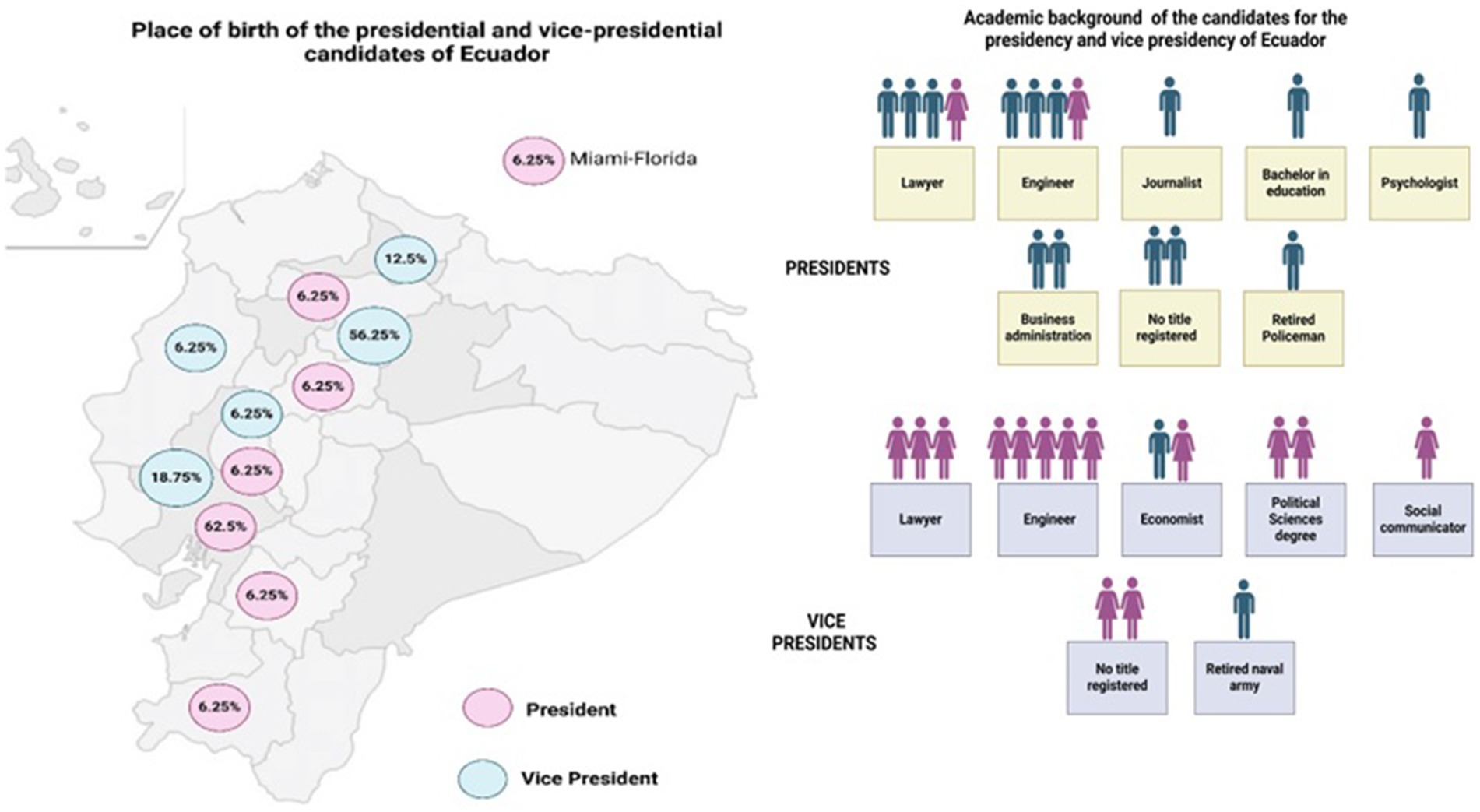
Figure 1. Characteristics of the candidates for the presidency and vice presidency of Ecuador (Created with BioRender.com).
2 Materials and methods
2.1 Study design
This study is a qualitative policy analysis assessing the methodological rigor of public health proposals from 16 Ecuadorian presidential candidates for the 2025–2029 election cycle. The study evaluates how well these proposals align with national health priorities and evidence-based policymaking principles. The analysis focuses on the inclusion of structured planning, epidemiological data, financial feasibility, and intersectoral health approaches.
2.2 Sample and setting
This study analyzed the official public policy proposals of all 16 presidential binomials registered for the 2025 Ecuadorian national elections. Documents were collected between August and October 2024 from official candidate websites, political party platforms, and publicly accessible campaign materials, including manifestos and downloadable plans. Only proposals that explicitly included public health policy components were eligible for analysis. Materials lacking clear health-related content were excluded.
Ecuador, a country of over 17 million people, presents a complex public health landscape with disparities in access, disease burden, and healthcare infrastructure. Therefore, evaluating presidential candidates’ health policies is crucial to understanding their potential impact on national healthcare outcomes.
2.3 Data collection and analysis
Data collection followed a deductive qualitative content analysis framework. Two independent reviewers screened each full-length government plan for health-related content. Explicit policy measures were extracted verbatim and categorized using a structured matrix based on a predefined list of 30 public health policy variables. These variables were selected through a systematic process grounded in Ecuador’s epidemiological profile, as reported in the Global Burden of Disease (GBD) 2021 study. Additional data sources included national hospital admission and mortality records from the Instituto Nacional de Estadística y Censos (INEC, 2023), and regional health priorities outlined by the World Health Organization (WHO) and the Pan American Health Organization (PAHO) (5, 29–31).
The 30 variables were organized into seven thematic domains to ensure comprehensive and non-overlapping coverage of key public health priorities. These domains included health equity, access to healthcare, mental health, infectious disease control, environmental health, chronic disease care, and pharmaceutical and regulatory policy, such as vaccine production and drug surveillance. Only specific and actionable proposals aligned with these predefined variables were included in the analysis. Vague or aspirational statements—for instance, general mentions of “improving health”—were excluded unless they clearly met the established criteria. Each reviewer independently coded the material, and discrepancies were resolved through consensus discussions.
2.4 Scoring and weighting system
Each candidate’s proposal was systematically evaluated using a binary scoring system. For each of the 30 predefined public health policy variables, a score of 1 was assigned when the proposal included a clear, specific, and actionable measure; a score of 0 was assigned when the variable was absent or vaguely addressed. This allowed for a standardized and replicable comparison across all proposals. The weighting of each topic was determined based on its relative impact on Ecuador’s health burden.
To account for the relative importance of each variable, weights were assigned based on their estimated contribution to Ecuador’s national health burden, as reported in the GBD 2021 study. Higher-weighted variables included healthcare access (7%), mental health (6%), infectious diseases (6%), chronic disease care (6%), and health equity (5%). Moderate-weighted variables such as environmental health, food safety, epidemic preparedness, and vaccine production were assigned weights ranging from 2 to 5%, reflecting their intermediate impact on public health outcomes.
The final score for each candidate was calculated by summing the weighted scores across all variables, expressed as a percentage of the maximum possible score (100%). This allowed for a comparative ranking of methodological rigor among all 16 proposals.
2.5 Statistical analysis
Descriptive statistics were used to summarize the frequency and distribution of public health policy measures across the 16 candidate proposals. Comparative ranking analysis was conducted based on the total weighted scores, enabling the identification of gaps in coverage and methodological inconsistencies. Inter-rater reliability was assessed using Cohen’s kappa statistic, which yielded a value of 0.85, indicating strong agreement between the two independent members of the research team. Any discrepancies in variable classification were resolved through consensus discussions.
2.6 Ethical considerations
This study received approval from the local Institutional Review Board (IRB), the Comité de Ética de Investigación en Seres Humanos de la Universidad de Las Américas (CEISH-UDLA), with exemption letter number 2023-EXC-008. CEISH-UDLA determined that the project is exempt from further ethical evaluation, in accordance with current legal regulations. The study relied exclusively on publicly available, non-identifiable government data, without involving human participants.
3 Results
3.1 General results
The analysis of the public health proposals from the 16 Ecuadorian presidential candidates showed significant differences in their comprehensiveness and alignment with national health priorities. As per the Ecuadorian electoral law, named Democracy code, in its article 3, the state warranties the equal participation of women and men [9a—Consejo Nacional Electoral. Reglamento para la democracia interna de las organizaciones políticas. Quito. 2022 (32)]. Despite of that, the vast majority of the presidential candidates were males (87.5%), and therefore the same number of vice-presidential candidates were females.
Regarding the academic profile of the presidential candidates, there were equal number of lawyers (n = 4) than those with an engineering diploma. However, there were still two candidates with no title, and one retired policeman. Similarly, for the vice-presidency, there were more candidates with an engineering diploma (n = 5), although it was in marketing, business management, or information technology; followed by lawyers (n = 4). There were also two candidates with no registered title and one retired army candidate (Figure 1).
The total scores for each candidate ranged from 53 to 98%, based on the number of addressed variables weighted according to their health burden. Escala/Terán achieved the highest score at 98%, covering nearly all evaluated variables. Tillería/Rosero had the lowest score at 53%, addressing the fewest health-related concerns.
Access to healthcare was present in 14 proposals, while mental health and infectious disease control were included 13 and 9 proposals, respectively. Tobacco control was presented only in 1 proposal, and post-market drug surveillance and counterfeit medicine control were included in the 2 and 5 proposals, respectively. Vaccine production appeared in only in 3 proposals, and chronic disease care was inconsistently addressed.
In Table 1 are summarized the concrete public health proposal declared in the official governmental plans of the binomial candidates.
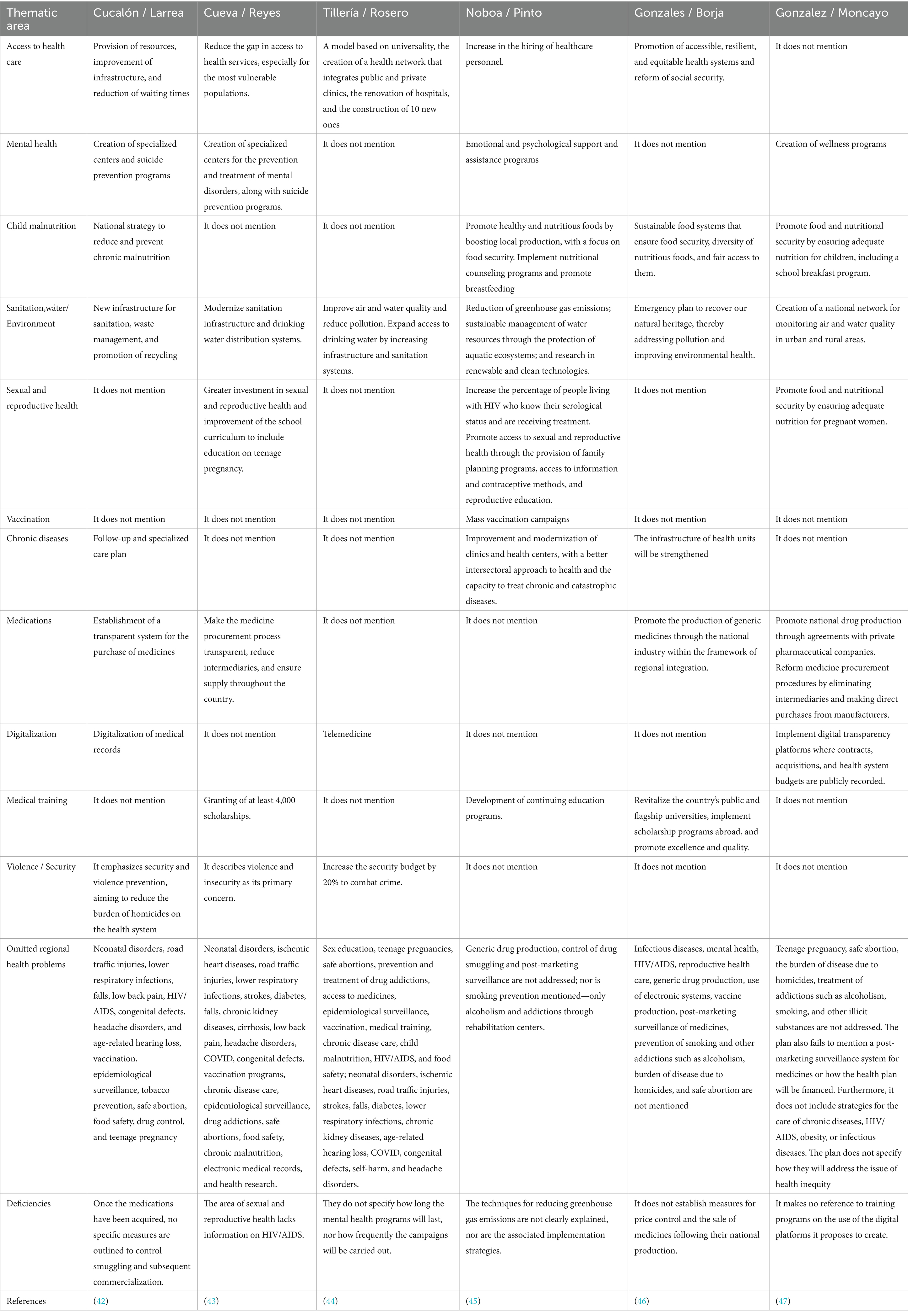
Table 1. Public health proposal declared in the official governmental plans of the binomial candidates.
3.2 Alignment with local and global health priorities
Among the leading causes of morbidity and mortality in Ecuador, neonatal disorders, ischemic heart disease, and interpersonal violence were the least addressed. Only Noboa/Pinto and Inza/Molina included neonatal care interventions, while preventive strategies for cardiovascular diseases were largely absent (Figure 2). Interpersonal violence was covered in 14 proposals, and road injuries were included in five. Lower respiratory infections and stroke were not mentioned in any proposals.
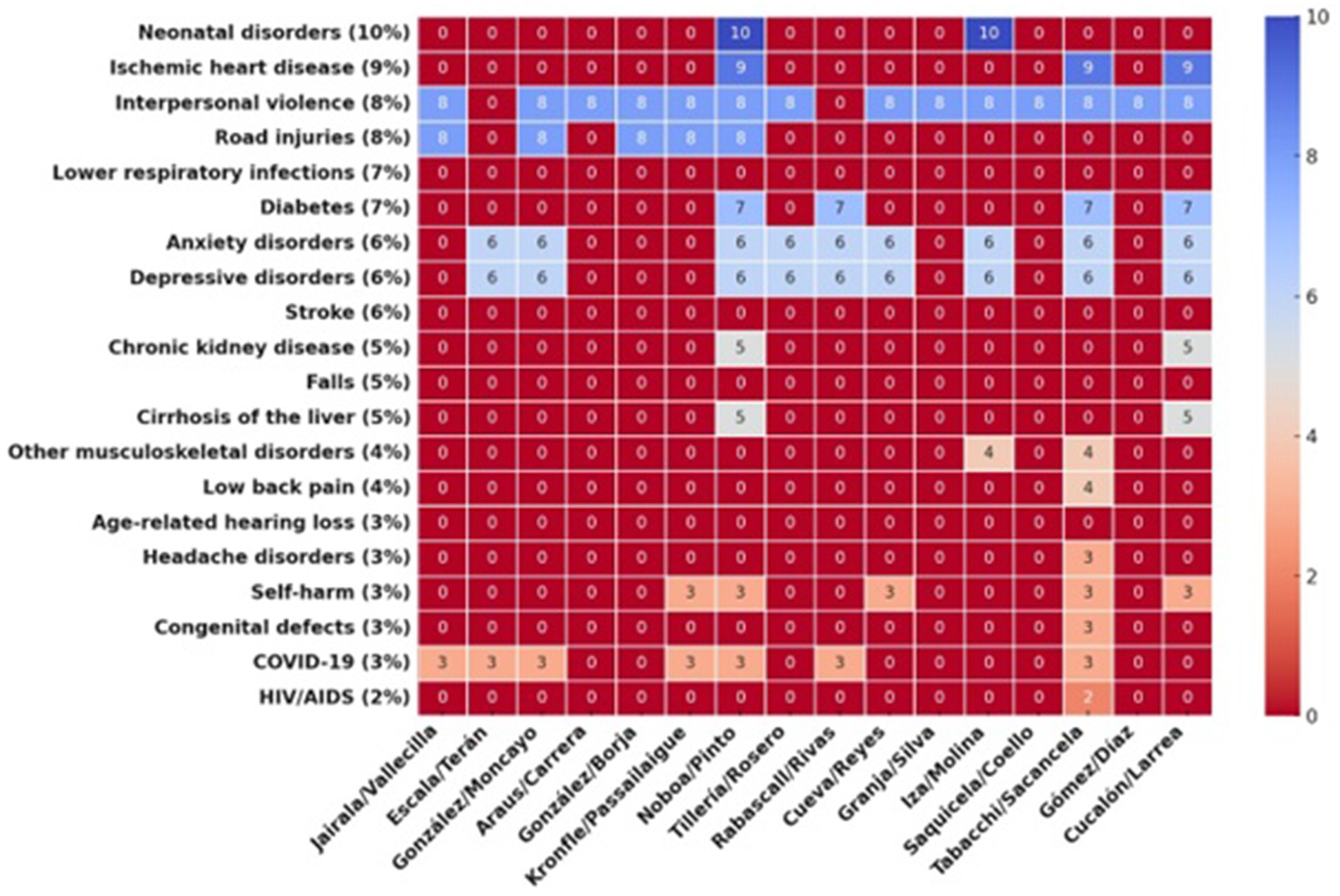
Figure 2. Heatmap displaying the burden of disease distribution across different candidates. The color scale transitions from red (indicating lower values or absence) to deep blue (representing higher values and greater burden). Candidate names are bold and right (Created with Prisma chart).
Non-communicable diseases such as diabetes, anxiety disorders, and depressive disorders were included 4, 9 and 9 proposals, respectively. Mental health was a frequently addressed topic included in 13 proposals, and COVID-19 appeared in 7 proposals. HIV/AIDS prevention and treatment were included in only one proposal.
3.3 Addressing local health needs
Healthcare workforce development was addressed in most proposals, while funding for health research and postgraduate training was included in fewer than half. Environmental and food safety policies were inconsistently covered, and air pollution was included in fewer than half of the proposals. Pharmaceutical policy planning varied, with fewer than half of the proposals including access to essential medicines. Vaccine production was mentioned in only a few proposals (Figure 3). Healthcare financing was covered in most proposals, but few included clear strategies for budget allocation.
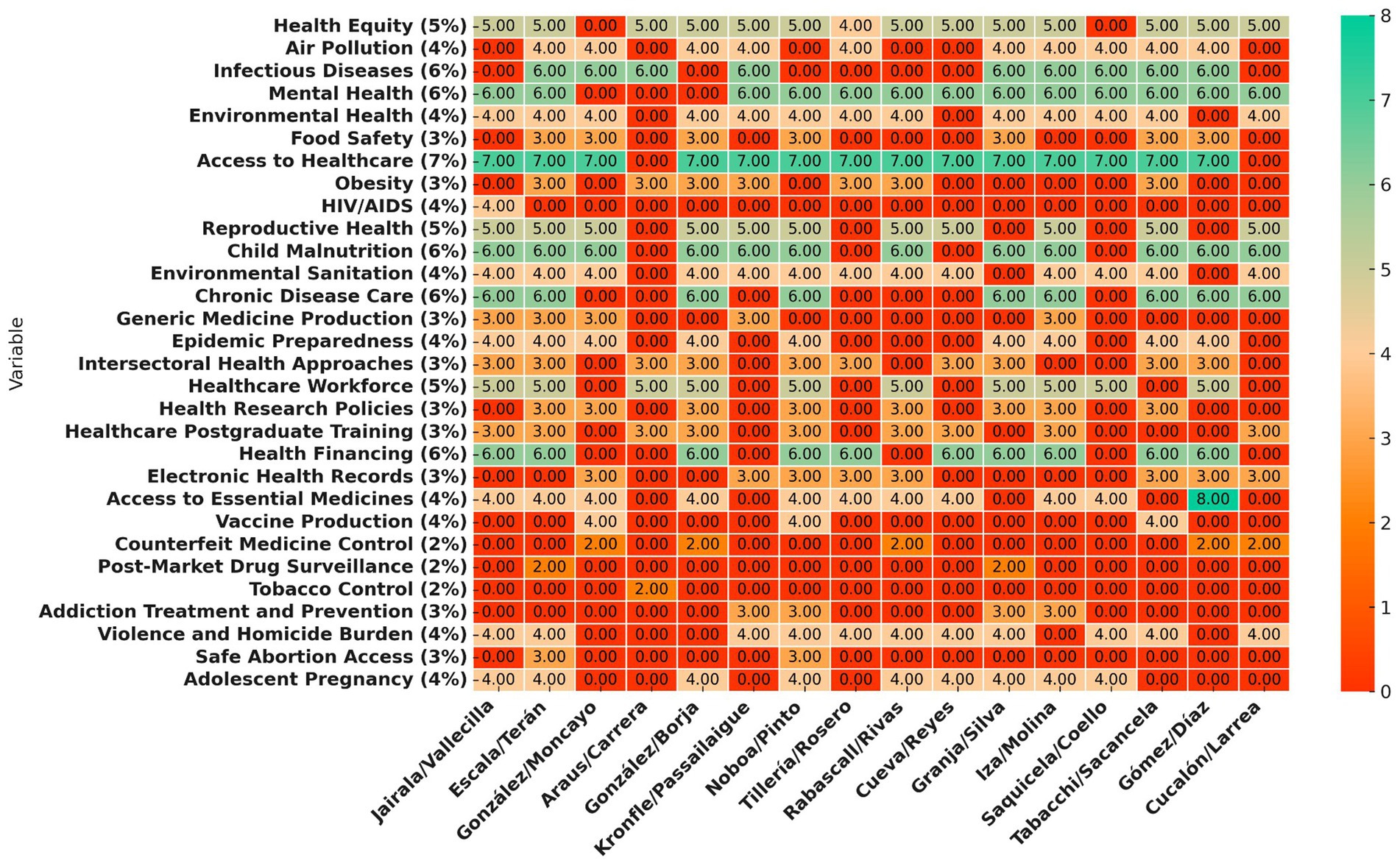
Figure 3. Heatmap displaying the distribution of variables across different candidates. The color scale transitions from red-orange for lower values to turquoise-green for higher values, with dark orange representing zero values. Candidate names are bold and right (Created with Prisma chart).
3.4 Overall assessment
Candidates with higher methodological scores used structured frameworks, epidemiological data, and evidence-based interventions. Those with lower scores relied on general statements without clear implementation plans or measurable objectives. Coverage discrepancies indicated a lack of a standardized, evidence-based approach to public health policymaking (Figure 4).
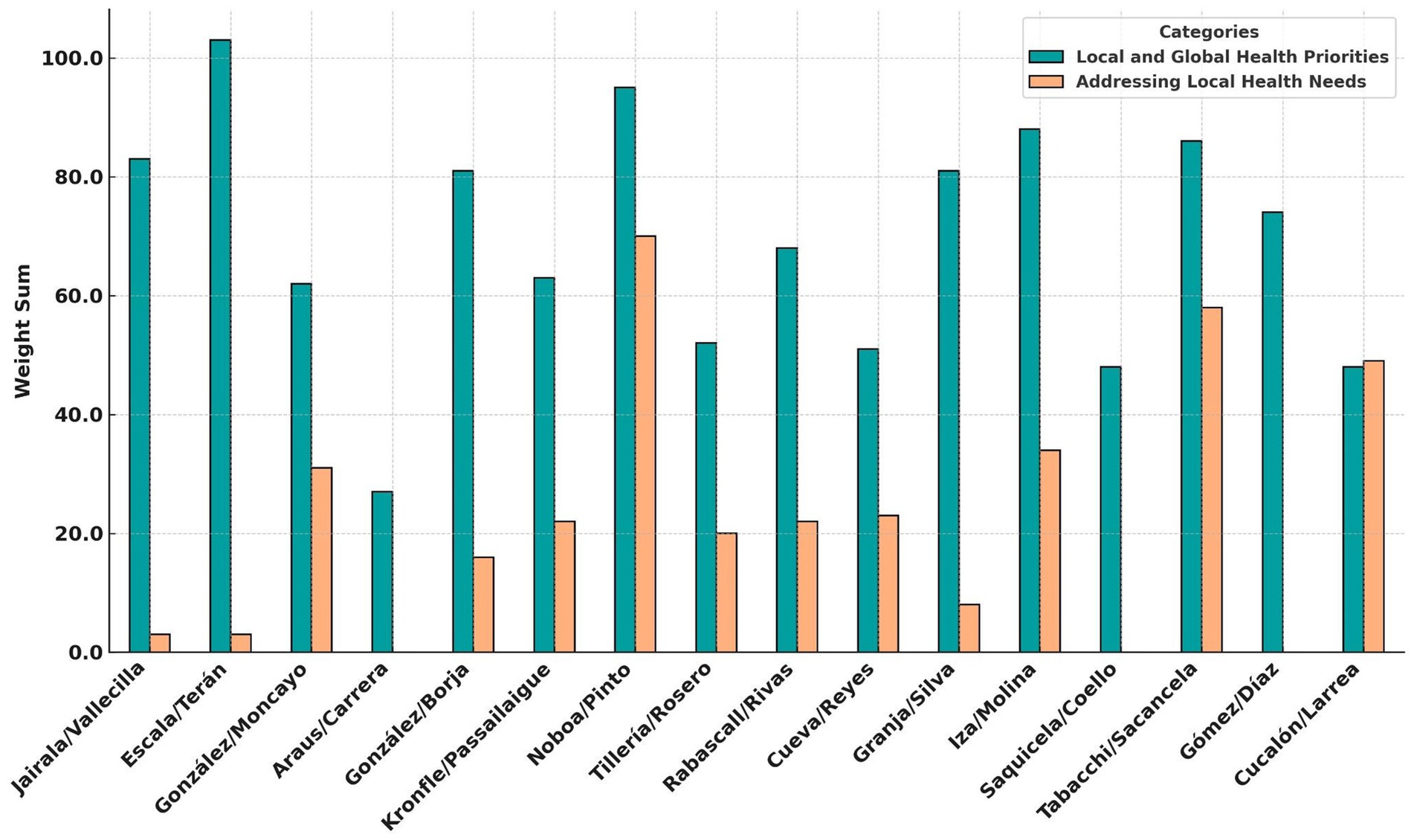
Figure 4. Comparison of local and global health priorities vs. addressing local health needs among presidential candidates. The turquoise bars represent the weight sum for prioritization of local and global health issues, while the peach bars represent the weight (Created with Prisma chart).
Each of the methodological criteria defined in the study—structured planning, epidemiological data, financial feasibility, and intersectoral approaches—was used as part of the evaluation matrix. These dimensions were assessed comparatively across proposals, and their influence is reflected in the scoring system and visualized in Figure 4.
The findings showed that many proposals lacked alignment with Ecuador’s health burdens. Key areas such as tobacco control, vaccine production, and chronic disease management were frequently omitted, highlighting the need for more comprehensive and data-driven public health policies.
4 Discussion
The analysis of public health proposals from candidates in Ecuador’s 2025 presidential election reveals substantial methodological deficiencies that compromise both the feasibility and effectiveness of the proposed policies. A central issue is the limited use of research-based evidence in the decision-making process. Many proposals lack references to epidemiological data, systematic reviews, or burden-of-disease assessments, thereby weakening their scientific foundation. This reflects a broader trend in global public health policymaking, where decision-makers often face barriers in accessing and applying research evidence within policy frameworks. The persistent disconnect between academic researchers and political actors—as well as the perception of scientific evidence as bureaucratic or impractical—contributes to the absence of structured, data-driven strategies in many political health proposals.
Our analysis shows that a multidisciplinary approach to the development of these proposals was largely absent in most candidate plans. Effective evidence-based decision-making requires the integration of multiple scientific disciplines, including epidemiology, environmental health, and behavioral sciences (33, 34). However, many proposals failed to incorporate cross-sectoral perspectives, instead emphasizing isolated policy measures that overlook broader social determinants of health. The absence of systematic reviews and meta-analyses adapted to Ecuador’s health priorities further exacerbates these methodological shortcomings. This pattern reflects challenges common to other low- and middle-income countries, where local health research infrastructures are often underfunded and underutilized.
The lack of robust evidence-based policymaking underscores the urgent need for structured frameworks that ensure policy proposals are grounded in empirical data. A major limitation is the frequent reliance on broad, generic statements that lack clear implementation pathways or measurable objectives. This is particularly evident in the absence of SMART (Specific, Measurable, Achievable, Relevant, and Time-bound) criteria in most proposals, making it difficult to assess policy effectiveness over time. Moreover, the widespread lack of financial planning further calls into question the feasibility of these proposals, as policies without defined budgets are unlikely to be implemented effectively.
Improving public health policymaking in Ecuador will require better integration of governance principles, scientific evidence, and strategic communication (23, 35). Effective health proposals must incorporate not only epidemiological data but also address key governance challenges, such as intersectoral coordination and regulatory enforcement (36). Internationally, knowledge translation strategies have been developed to bridge the gap between research and policy. In the Ecuadorian context, this could include institutional mechanisms that facilitate collaboration between public health researchers and policymakers, ensuring that proposals are informed by high-quality data and systematic evaluations.
Our findings also indicate that most candidate proposals fail to align with Ecuador’s current disease burden or global health priorities. Although mental health and infectious diseases were frequently mentioned, critical areas such as neonatal disorders, ischemic heart disease, and stroke prevention were largely neglected. This misalignment suggests that policy planning is not sufficiently informed by the country’s epidemiological profile. Particularly concerning is the limited focus on chronic disease management, despite the growing impact of non-communicable diseases in Ecuador.
In addition, vaccine production, pharmaceutical regulation, and health system resilience received minimal attention, despite their importance in ensuring national health security. Local vaccine production offers multiple benefits, including a stable supply, reduced dependence on imports, and increased readiness in the face of global shortages. However, Ecuador has experienced a notable decline in vaccination coverage since the discontinuation of domestic vaccine manufacturing, especially for BCG and DTP vaccines (37). The omission of tobacco and e-cigarette control policies, as well as post-market drug surveillance, further reflects a broader neglect of long-term regulatory and preventive health measures (38). This pattern suggests a tendency to prioritize short-term political gains over evidence-based, sustainable health strategies.
To enhance the methodological rigor of public health proposals, it is essential to strengthen the integration of scientific evidence into policy development. Future proposals should incorporate systematic reviews, use current epidemiological data, and include detailed financial planning to ensure feasibility. The development of a standardized framework for evaluating health policy proposals could also improve consistency and alignment with national priorities (39–41). Tools such as rapid review methodologies and Delphi consensus techniques—already applied successfully in other countries—may serve as useful models for improving the design and evaluation of evidence-based public health policies in Ecuador.
The findings highlight the need for a shift in the political approach to health policymaking, moving from broad, aspirational goals to structured, evidence-based strategies that are actionable and measurable. Addressing these gaps will require increased collaboration between policymakers, public health researchers, and regulatory institutions to ensure that future proposals align with Ecuador’s pressing health needs while adhering to global best practices.
5 Limitations
This study has several limitations that should be considered when interpreting its findings. First, the analysis relied exclusively on publicly available government plans, which may not fully reflect the entire scope of each candidate’s health policy agenda. Some candidates may have had additional, unpublished proposals or internal strategies not captured in this review. Moreover, the absence of direct communication with candidates or their policy teams limits our understanding of the rationale behind specific policy choices, contextual constraints, or implementation considerations. Importantly, the policy proposals analyzed reflect pre-electoral declarations that are subject to change once candidates are elected and must develop official government plans. Therefore, the dynamic nature of political program refinement was not captured in this cross-sectional study.
Second, the level of detail and clarity varied significantly across the proposals. While some candidates provided structured frameworks with measurable objectives, others included only broad or aspirational statements. This variation may have influenced the scoring process, as more detailed proposals were more likely to explicitly address the predefined variables. Although a binary scoring system was applied uniformly, the inherent asymmetry in proposal quality introduces potential bias.
Third, the assignment of weights to the 30 public health variables was based on expert judgment informed by epidemiological data from the GBD 2021 study and national statistics. However, the process did not involve a formal consensus method such as a Delphi panel and therefore introduces a degree of subjectivity. While grounded in evidence and public health expertise, the prioritization scheme may not fully reflect the political, economic, or institutional constraints affecting policy feasibility in Ecuador.
Fourth, although the study emphasizes the use of scientific evidence in policy formulation, we recognize that other factors—such as governance capacity, political will, stakeholder influence, and budget availability—may exert greater relative weight in determining policy effectiveness. The mere presence of evidence-informed content does not ensure implementation success. Future research should explore these political and institutional determinants in greater depth.
Finally, the study employed a cross-sectional design that captures the content of the proposals at a single point in time. As such, it does not assess how these policies may evolve, be revised, or ultimately be implemented if the candidates are elected. The absence of a longitudinal component limits the ability to examine real-world impact or policy sustainability.
Despite these limitations, this study provides a structured evaluation of the methodological rigor of health proposals and highlights critical gaps in evidence-based policymaking. Addressing these challenges will require greater transparency in policy formulation, stronger integration of scientific evidence, and improved mechanisms to assess the long-term impact of proposed health interventions.
6 Conclusion
This evaluation of public health proposals from Ecuadorian presidential candidates reveals substantial methodological shortcomings. Many plans lacked structured, evidence-based approaches, with limited use of standardized frameworks, few SMART objectives, and insufficient financial planning—factors that collectively undermine the feasibility and effectiveness of the proposed interventions. Although frequently discussed issues such as healthcare access and mental health were commonly addressed, several critical areas—such as neonatal care, ischemic heart disease, and stroke prevention—were largely neglected. These omissions point to a lack of alignment with both national health needs and global disease burden priorities.
Candidates who achieved higher methodological scores were those whose proposals incorporated epidemiological data, structured planning, and clear financial strategies. In contrast, candidates with lower scores often relied on general, non-specific statements that lacked measurable goals or defined implementation pathways. The overall inconsistency across proposals underscores the urgent need for a more systematic, evidence-informed approach to public health policymaking in Ecuador.
To enhance the quality and impact of future proposals, it is essential to strengthen the integration of scientific evidence into political health agendas. Policymaking should be aligned with Ecuador’s current epidemiological profile and give priority to underrepresented areas such as chronic disease management, environmental health, and vaccine production. Moreover, the tendency to favor politically expedient or short-term solutions over long-term, evidence-based strategies must be addressed to ensure sustainable improvements in population health.
Improving public health policy in Ecuador will require stronger collaboration among policymakers, public health researchers, and international organizations. This includes the development of institutional mechanisms to evaluate policy proposals based on official data sources—such as those from the INEC or the Ministry of Public Health—and to ensure that political plans are grounded in scientific rigor and national health priorities.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
This study received approval from the local Institutional Review Board (IRB), the Comité de Ética de Investigación en Seres Humanos de la Universidad de Las Américas (CEISH-UDLA), with exemption letter number 2023-EXC-008. CEISH-UDLA determined that the project is exempt from further ethical evaluation, in accordance with current legal regulations. Written informed consent to participate in this study was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
EO-P: Conceptualization, Methodology, Resources, Software, Validation, Formal analysis, Visualization, Funding acquisition, Writing – original draft, Writing – review & editing. ET: Validation, Writing – review & editing. KC: Resources, Writing – original draft. JE: Resources, Writing – original draft. MG: Resources, Writing – original draft, Writing – review & editing. MC: Resources, Writing – original draft. MB: Resources, Writing – original draft. JV-G: Methodology, Resources, Formal analysis, Writing – original draft, Visualization, Writing – review & editing. JI-C: Methodology, Software, Formal analysis, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was partially funded by Universidad de Las Américas (UDLA) under Grant EOP.18.10.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kneale, D, Rojas-García, A, Raine, R, and Thomas, J. The use of evidence in English local public health decision-making: a systematic scoping review. Implement Sci. (2017) 12:53. doi: 10.1186/s13012-017-0577-9
2. Campos, C. Evolución del sistema de salud de Ecuador: Buenas prácticas y desafíos en su construcción en la última década 2005-2014. An Fac Med. (2017) 78:452–60. doi: 10.15381/anales.v78i4.14270
3. Espinosa, V, Acuña, C, de la Torre, D, and Tambini, G. La reforma en salud del Ecuador. Rev Panam Salud Publica. (2017) 41:e96. doi: 10.26633/RPSP.2017.96
4. Baez, J. (2021). La inversión en salud se redujó un 36% en 2019 – Rebelion. Available online at: https://rebelion.org/la-inversion-en-salud-se-redujo-un-36-en-2019/ (Accessed August 3, 2025).
5. INEC. (2023). Camas y Egresos Hospitalarios 2023. Instituto Nacional de Estadística y Censos. Available online at: https://www.ecuadorencifras.gob.ec/camas-y-egresos-hospitalarios-2023/ (Accessed August 2, 2025).
6. INEC (2024). Cuentas Satélites de Salud (CSS) Serie 2007-2023. Available online at: https://www.ecuadorencifras.gob.ec/documentos/web-inec/Estadisticas_Economicas/Cuentas_Satelite/Salud/2023/PPT_Cuentas_Satelite_Salud_2023.pdf (Accessed August 3, 2025).
7. Ministerios de Salud Pública. (2025). Inversión en medicamentos, infraestructura y equipamiento sanitario fueron las acciones más relevantes durante la Rendición de Cuentas 2024 – Ministerio de Salud Pública. Available online at: https://www.salud.gob.ec/inversion-en-medicamentos-infraestructura-y-equipamiento-sanitario-fueron-las-acciones-mas-relevantes-durante-la-rendicion-de-cuentas-2024/ (Accessed August 3, 2025).
8. Witt, GFV, Ronquillo, MCJ, Bravo, EMG, and Rodríguez, P. de las MW. Desafíos y problemas de la salud pública en Ecuador. RECIAMUC. (2023) 7:10–21. doi: 10.26820/reciamuc/7.(2).abril.2023.10-21
9. Primicias. (2025). Pacientes piden la emergencia del sistema de salud en Ecuador por falta de medicamentos. Primicias. Available online at: https://www.primicias.ec/sociedad/pacientes-enfermedades-catastroficas-emergencia-sistema-salud-ecuador-iess-msp-99747/ (Accessed August 3, 2025).
10. Ortiz-Prado, E, Merlo-Chaves, LF, Vasconez-Gonzalez, J, Suarez-Sangucho, IA, and Izquierdo-Condoy, JS. Ensuring safety and security for Ecuador’s rural health doctors: a call to action. Front Public Health. (2025) 13:1607070. doi: 10.3389/fpubh.2025.1607070
11. Izquierdo-Condoy, JS, Morales-Lapo, E, Hidalgo, M, Tello-De-la-Torre, A, Ruiz-Sosa, C, Guerrero-Castillo, GS, et al. Job satisfaction and self-perceptions among Ecuadorian medical doctors during their compulsory rural community social service: a countrywide cross-sectional analysis. J Prim Care Community Health. (2023) 14:21501319231179936. doi: 10.1177/21501319231179936
12. El Universo. (2025). Cinco ministros de Salud ha tenido Daniel Noboa desde que asumió el poder en 2023, tres en los últimos dos meses. El Universo. Available online at: https://www.eluniverso.com/noticias/politica/cinco-ministros-salud-gobierno-daniel-noboa-asumio-presidencia-nota/ (Accessed August 3, 2025).
13. Ortiz-Prado, E, Suárez Sangucho, IA, Cañizares Fuentes, WR, Vasconez-Gonzalez, J, and Izquierdo-Condoy, JS. The imperative of public health expertise in Ecuadorian health leadership: a call for competency-based appointments. Int J Public Health. (2025) 69:1607894. doi: 10.3389/ijph.2024.1607894
14. Vásconez, L. (2025). ¿Cuánto debe el Ministerio de Salud a las clínicas de diálisis en Ecuador? El Comercio Available online at: https://www.elcomercio.com/actualidad/negocios/cuanto-deben-ministerio-salud-clinicas-dialisis-ecuador.html (Accessed May 3, 2025).
15. PRIMICIAS. (2024). Nueva protesta por falta de pagos a clínicas de diálisis en Ecuador, alrededor de 1.000 pacientes han fallecido. Primicias. Available online at: https://www.primicias.ec/sociedad/protesta-quito-pacientes-clinicas-dialisis-deuda-ministerio-finanzas-81314/ (Accessed May 3, 2025).
16. Redacción. (2024). Mil personas fallecidas por falta de atención renal. ¿Cómo es posible?. Radio Pichincha. Available online at: https://www.www.radiopichincha.com/mil-personas-fallecidas-por-falta-de-atencion-renal/ (Accessed August 2, 2025).
17. Yakhkind, A, Lang, AE, Brophy, G, Tesoro, E, Levasseur-Franklin, KE, and Maldonado, N. Substandard and falsified medications: a barrier to Global Health equity exemplified in Ecuador. Neurocrit Care. (2023) 38:1–6. doi: 10.1007/s12028-022-01658-1
18. The Lancet Public Health. Public health must be a priority in the 2020 US election. Lancet Public Health. (2020) 5:e512. doi: 10.1016/S2468-2667(20)30214-0
19. Hamra, R, Siddiqi, S, Carmel, E, and Ammar, W. Assessing the governance of the health policy-making process using a new governance tool: the case of Lebanon. Health Res Policy Syst. (2020) 18:66. doi: 10.1186/s12961-020-00557-1
20. Harbi, N, Alabaad, A, Alazwari, M, Alaqidi, I, Alasmri, D, Alturaiki, A, et al. Critical analysis of healthcare policy, governance, and public health strategies. J Ecohumanism. (2024) 3:85149–59. doi: 10.62754/joe.v3i8.5191
21. McMichael, C, Waters, E, and Volmink, J. Evidence-based public health: what does it offer developing countries? J Public Health (Oxf). (2005) 27:215–21. doi: 10.1093/pubmed/fdi024
22. Orton, L, Lloyd-Williams, F, Taylor-Robinson, D, O’Flaherty, M, and Capewell, S. The use of research evidence in public health decision making processes: systematic review. PLoS One. (2011) 6:e21704. doi: 10.1371/journal.pone.0021704
23. Cairney, P, and Oliver, K. Evidence-based policymaking is not like evidence-based medicine, so how far should you go to bridge the divide between evidence and policy? Health Res Policy Syst. (2017) 15:35. doi: 10.1186/s12961-017-0192-x
24. Armstrong, R, Waters, E, Dobbins, M, Anderson, L, Moore, L, Petticrew, M, et al. Knowledge translation strategies to improve the use of evidence in public health decision making in local government: intervention design and implementation plan. Implement Sci. (2013) 8:121. doi: 10.1186/1748-5908-8-121
25. Bambra, C, Bellis, M, Greatley, A, Greengross, S, Wood, S, Lincoln, P, et al. Reducing health inequalities in priority public health conditions: using rapid review to develop proposals for evidence-based policy. J Public Health (Oxf). (2010) 32:496–505. doi: 10.1093/pubmed/fdq028
26. Bae, J-M. Suggestions for the promotion of evidence-based public health in South Korea. Epidemiol Health. (2017) 39:e2017030. doi: 10.4178/epih.e2017030
27. Centers for Disease Control and Prevention. (2024). CDC Program Evaluation Framework Action Guide. CDC Approach to Program Evaluation. Available online at: https://www.cdc.gov/evaluation/php/evaluation-framework-action-guide/index.html [Accessed August 5, 2025]
28. HM Treasury. (2020). The Magenta book: central government guidance on evaluation. GOVUK. Available online at: https://www.gov.uk/government/publications/the-magenta-book (Accessed August 5, 2025).
29. Ward, ZJ, and Goldie, SJ. Global burden of disease study 2021 estimates: implications for health policy and research. Lancet. (2024) 403:1958–9. doi: 10.1016/S0140-6736(24)00812-2
30. PAHO (2020). Strategic plan of the Pan American health organization 2020-2025: equity at the heart of health Available online at: https://iris.paho.org/handle/10665.2/52473 (Accessed August 3, 2025).
31. WHO. (2025). Region of the Americas. World Health Organization. Available online at: https://www.who.int/about/accountability/results/who-results-report-2024-2025/region-AMRO (Accessed August 2, 2025).
32. Consejo Nacional Electoral. (2022). Reglamento para la democracia interna de las organizaciones políticas. Available online at: https://www.cne.gob.ec/wp-content/uploads/2020/06/CODIFICACION_DEL_REGLAMENTO_DE_DEMOCRACIA_INTERNA.pdf (Accessed August 5, 2025).
33. Brownson, RC, Fielding, JE, and Green, LW. Building capacity for evidence-based public health: reconciling the pulls of practice and the push of research. Annu Rev Public Health. (2018) 39:27–53. doi: 10.1146/annurev-publhealth-040617-014746
34. Chambers, L, Ehrlich, A, Picard, L, and Edwards, P. The art and science of evidence-based decision-making … Epidemiology can help! Can J Public Health. (2002) 93:I1–8.
35. Young, I, Gropp, K, Pintar, K, Waddell, L, Marshall, B, Thomas, K, et al. Experiences and attitudes towards evidence-informed policy-making among research and policy stakeholders in the Canadian Agri-food public health sector. Zoonoses Public Health. (2014) 61:581–9. doi: 10.1111/zph.12108
36. Bennett, G, and Jessani, N. (2011). The knowledge translation toolkit. Bridging the “know-do” gap: a resource for researchers.
37. Ortiz-Prado, E, Villacreses-Brito, LC, Vasconez-Gonzalez, J, Jacome, CA, Arias-Intriago, M, and Izquierdo-Condoy, JS. Assessing immunization coverage and the negative impact of local vaccine production cessation in Ecuador. Vaccine. (2025) 13:348. doi: 10.3390/vaccines13040348
38. Izquierdo-Condoy, JS, and Ortiz-Prado, E. Urgent action needed: addressing the regulatory gap in e-cigarette trade and usage. J Public Health Policy. (2024) 45:582–7. doi: 10.1057/s41271-024-00505-1
39. Bradt, DA. Evidence-based decision-making (part 1): origins and evolution in the health sciences. Prehosp Disaster Med. (2009) 24:298–305. doi: 10.1017/S1049023X00007019
40. Minjina, B. The use of the evidence from the behavioral sciences in the organizational decision-making process. Manag Dyn Knowl Econ. (2015) 3:381–408.
41. Spring, B. Health decision making: lynchpin of evidence-based practice. Med Decis Mak. (2008) 28:866–74. doi: 10.1177/0272989X08326146
42. Cucalón, H, Larrea, C, and González, I (2024). Plan de trabajo Construye – Consejo Nacional Electoral – CNE Ecuador. Available online at: https://www.cne.gob.ec/download/plan-de-trabajo-construye/ (Accessed February 12, 2025).
43. Cueva, J, and Reyes, C (2024). Plan de trabajo Amigo – Consejo Nacional Electoral – CNE Ecuador. Available online at: https://www.cne.gob.ec/download/plan-de-trabajo-amigo/ (Accessed February 12, 2025).
44. Tilleria, L, and Rosero, K (2024). Plan de trabajo Avanza – Consejo Nacional Electoral – CNE Ecuador. Available online at: https://www.cne.gob.ec/download/avanza/ (Accessed February 12, 2025).
45. Acción Democrática Nacional. (2024). Plan de trabajo ADN – Consejo Nacional Electoral – CNE Ecuador. Available online at: https://www.cne.gob.ec/download/plan-de-trabajo-adn/ (Accessed February 12, 2025).
46. Alianza Revolución Ciudadana (2024). RETO LISTAS 5-33. Plan de TRABAJO del BINOMIO PRESIDENCIAL de la ALIANZA REVOLUCIÓN CIUDADANA - RETO LISTAS 5-33, 2025-2029. Available online at: https://ecuadorchequea.com/wp-content/uploads/2025/01/REVOLUCION-CIUDADANA-RETO-Plan-de-trabajo.pdf (Accessed August 3, 2025).
47. Partido Sociedad Patriótica (2024). PLAN DE GOBIERNO ECUADOR SOSTENIBLE 2025-2029. Available online at: https://ecuador-decide.org/wp-content/uploads/2025/01/PSP3_Andrea-Gonzalez-1.pdf (Accessed August 3, 2025).
Keywords: public health policy, Ecuador, evidence-based policymaking, health equity, political proposals
Citation: Ortiz-Prado E, Terán E, Cuenca KA, Echeverria JS, Gallardo M, Cadena MP, Barriga M, Vasconez-Gonzalez J and Izquierdo-Condoy JS (2025) Ecuador’s 2025 presidential election and the disconnection between public health and the political agendas. Front. Public Health. 13:1628203. doi: 10.3389/fpubh.2025.1628203
Edited by:
Josefina Amanda Suyo Vega, Cesar Vallejo University, PeruReviewed by:
Gabriel Jaime Otálvaro-Castro, Universidad de Antioquia, ColombiaVictor Becerril-Montekio, Instituto Nacional de Salud Pública, Mexico
Copyright © 2025 Ortiz-Prado, Terán, Cuenca, Echeverria, Gallardo, Cadena, Barriga, Vasconez-Gonzalez and Izquierdo-Condoy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Esteban Ortiz-Prado, ZS5vcnRpenByYWRvQGdtYWlsLmNvbQ==