 Jieun Shin1
Jieun Shin1 Seunghui Baek2*
Seunghui Baek2*- 1Department of Biomedical Informatics, College of Medicine, Konyang University, Daejeon, Republic of Korea
- 2Department of Health and Exercise Management, Sungshin Women’s University, Seoul, Republic of Korea
Background: This study aimed to identify the determinants of self-reported health literacy among older adults aged 65 years and above in South Korea.
Methods: Data were obtained from the 2021 Korean Health Panel Survey, including 4,220 participants aged 65 and above. Statistical analyses such as t-tests, ANOVA, and logistic regression were conducted to examine the effects of personal characteristics and health behaviors on self-reported health literacy.
Results: The analysis revealed that men, younger participants, those with spouses, higher education levels, and individuals engaging in positive health behaviors-including non-smoking, non-drinking, and regular exercise-had significantly higher levels of self-reported health literacy.
Conclusion: These findings suggest the importance of developing targeted strategies to improve health literacy among older adults, particularly focusing on personal characteristics and health behaviors that are associated with higher health literacy.
1 Introduction
Health literacy refers to the capacity to access, understand, evaluate, and utilize health-related information to make informed healthcare decisions and maintain overall well-being (1). It plays a pivotal role in promoting effective communication between healthcare providers and patients, supporting adherence to medical recommendations, and empowering individuals to manage chronic conditions successfully.
The adoption and maintenance of healthy lifestyles represent critical determinants of health outcomes, particularly for older adults, who often face challenges navigating complex healthcare systems and medical information. These practices are vital for extending healthspan and enhancing quality of life (1, 2). As individuals age, the ability to interact effectively with the healthcare system becomes increasingly difficult due to cognitive decline, sensory impairments, and the intricacy of medical terminology.
South Korea is among the fastest-aging nations globally, with the proportion of older adults projected to exceed 20% of the total population by 2025 (3). Aging is accompanied by rising rates of chronic illnesses, increased barriers to healthcare access, and escalating medical expenses—factors that collectively underscore the growing importance of health literacy (4). In particular, older adults’ levels of health literacy directly influence their capacity to seek, understand, and use health-related information. Empirical evidence suggests that inadequate health literacy is linked to adverse health outcomes (5, 6).
Health behaviors function as key mediating mechanisms in the relationship between health literacy and health outcomes. Higher health literacy is associated with a greater likelihood of engaging in positive health behaviors, including preventive screenings, regular physical activity, and a nutritious diet. Such behaviors, in turn, contribute to better health outcomes (2, 5).
However, the relationships among health literacy, health behaviors, and health outcomes are unlikely to follow a simple linear pathway. As suggested by previous studies, these variables are influenced by a complex interplay of factors such as social support, access to healthcare, psychological traits, and sociocultural or environmental contexts (2, 7). While health literacy may influence health outcomes through its effect on health behaviors, this pathway is often moderated or mediated by variables such as socioeconomic status, family and community networks, and the complexity of the healthcare system.
Accordingly, this study recognizes the multilayered interactions between health literacy, health behaviors, and health outcomes, and aims to provide a comprehensive analysis of key sociodemographic and behavioral determinants.
Previous research has highlighted that demographic variables such as age, gender, educational attainment, income, and cultural context significantly affect health literacy (5, 7). Given the rapid growth of the older population, disaggregated analysis by age group has become increasingly essential. Studies have also confirmed notable gender-based differences in health behavior, underscoring the necessity of a nuanced analysis of health literacy by both gender and age within the older adults (8).
In addition, behavioral elements such as lifestyle practices, healthcare service utilization, and active health information-seeking behavior have been found to significantly influence health literacy (9). Nonetheless, existing research has largely focused on general determinants of health literacy, with a marked paucity of comprehensive studies centered on older adults in Korea. Therefore, this study aims to examine the levels of health literacy and its associated sociodemographic and behavioral factors among older adults in Korea, using nationally representative data. By doing so, it seeks to lay the groundwork for developing targeted strategies and policies to improve health literacy in this growing population segment.
2 Methods
2.1 Study design
This study utilized data from the 2021 Korean Health Panel Survey,1 targeting individuals aged 65 years and older. Of the total 4,480 eligible older adults, 260 individuals who did not complete the self-reported health literacy questionnaire were excluded. Additionally, 310 individuals who failed to respond to at least one health behavior question—specifically regarding smoking, alcohol consumption, or physical activity—were also excluded. As a result, a final analytic sample of 3,910 participants was included in the study (Figure 1).
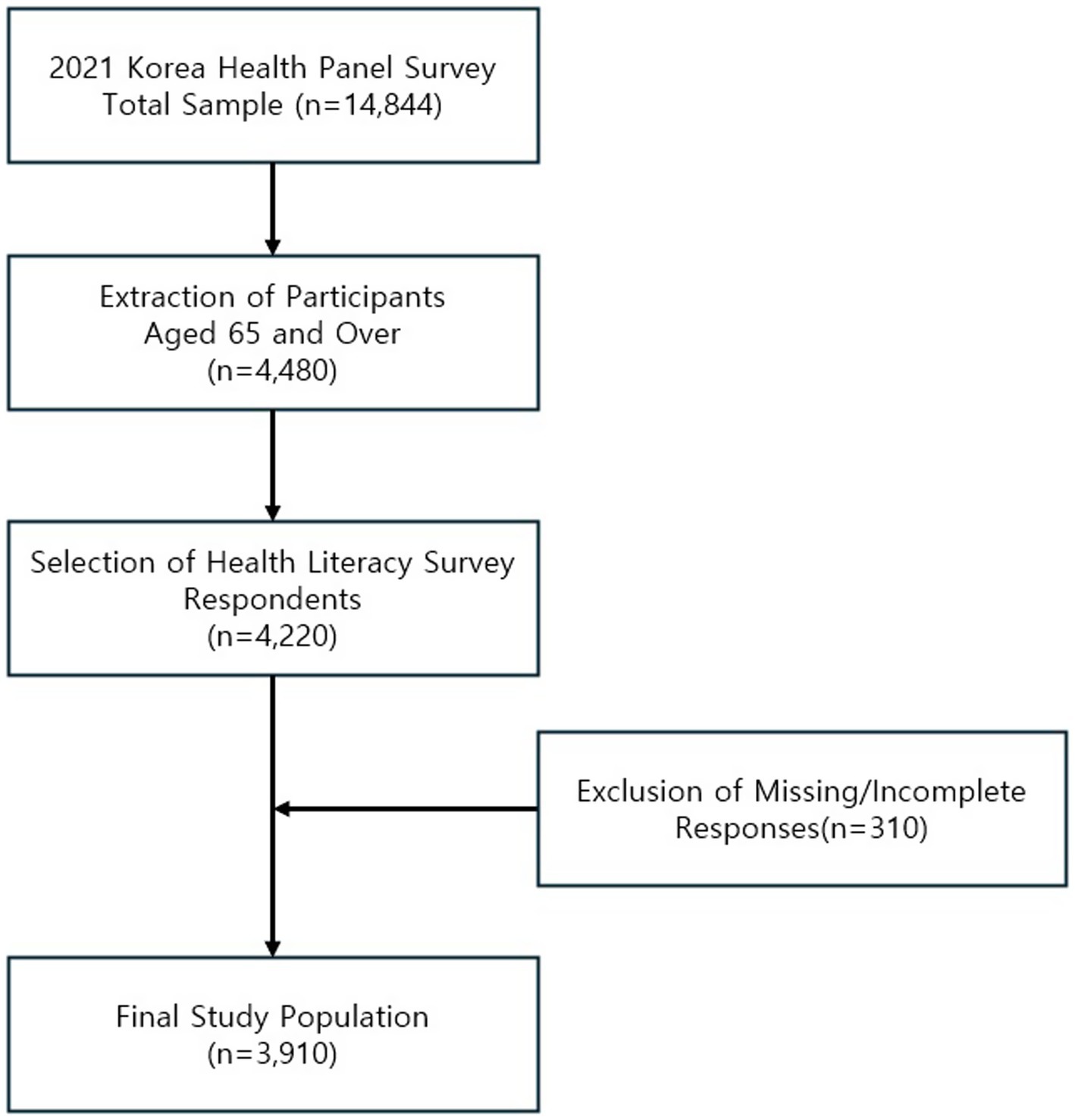
Figure 1. Flowchart of participant selection from the 2021 Korea Health Panel Survey.
2.2 Self-reported health literacy
The Korean version of the HLS-EU-Q16 used in this study was culturally adapted and psychometrically validated for older Korean adults by Chun and Lee (10), through a rigorous process of back-translation and expert review. The validation study reported high internal consistency (Cronbach’s α = 0.89), strong item-total correlations (all > 0.40), and a unidimensional factor structure, supporting the construct validity of the tool.
This version was also adopted in the 2021 Korea Health Panel Survey, confirming its applicability in large-scale population-based studies in Korea.
We utilized the Korean version of the HLS-EU-Q16, a 16-item short form of the original HLS-EU-Q47, which was developed for the European Health Literacy Survey to facilitate cross-national comparisons of health literacy levels across European countries (1, 11). For each item, responses were scored as 0 for “very difficult” or “difficult,” and as 1 for “easy” or “very easy.” The total score ranged from 0 to 16, with a cutoff value of 12 commonly used to distinguish levels of health literacy. Scores above 12 were categorized as “adequate” or “high self-reported health literacy,” while scores of 12 or below were categorized as “inadequate” or “low self-reported health literacy” (12).
In this study, participants were classified into high and low health literacy groups based on this 12-point threshold.
2.3 General & health-related characteristics
General characteristics included age group (65–69, 70–79, and 80+) and gender (male, female). Health-related characteristics comprised marital status, educational attainment, and economic activity status. Marital status was categorized as “yes” for participants who were currently married and “no” for all others. Educational attainment was grouped into three categories: middle school or less, high school, and college or higher. Economic activity status was defined as “yes” for individuals currently engaged in any form of economic activity and “no” otherwise.
Additional health-related characteristics included smoking, alcohol consumption, and physical activity. Smoking status was coded as “yes” for current smokers (daily or occasional) and “no” for former smokers or those who had never smoked. Alcohol consumption was classified as “no” for individuals who reported never having consumed alcohol in their lifetime or who had not consumed any alcohol in the past year; all other responses were coded as “yes.” Physical activity was assessed based on regular participation in sports or exercise. Participants who reported such activity were categorized as “yes,” and those who did not were categorized as “no.”
2.4 Statistics analysis
To analyze differences in self-reported health literacy (HL) levels according to personal characteristics and health behaviors, chi-square tests were performed using IBM SPSS Statistics 25.0. To identify factors associated with HL levels (0 = low, 1 = high), logistic regression analyses stratified by age group (65–69, 70–79, and 80+) and gender (male, female) were conducted. Marital status, educational attainment, and economic activity were included as common covariates. Health behaviors—specifically smoking, alcohol consumption, and physical activity—were entered into the model using the forward selection method. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for each variable. A p-value of <0.05 was considered statistically significant.
To visualize the distribution of health behavior practices among participants, Sankey diagrams were generated based on the number of healthy behaviors practiced (ranging from 0 to 3), stratified by gender and age group. Health behaviors were defined by three domains: smoking, alcohol consumption, and physical activity. A score of 1 was assigned to each behavior if a participant practiced a healthy behavior (e.g., non-smoking, moderate drinking, or regular physical activity), and 0 otherwise. The total health behavior score was then summed and classified into four categories: 0 (none practiced) to 3 (all practiced).
The visualizations were developed in the Python-based Google Colaboratory environment using the go. Sankey () function from the Plotly library. These Sankey diagrams were used to intuitively depict the flow from the number of healthy behaviors practiced to the level of self-reported HL (high vs. low) across different age and gender subgroups, enabling visual comparisons of patterns in HL and health behavior engagement among older adults.
3 Result
3.1 Descriptive statistics
When examining respondents’ awareness of the various dimensions of self-reported health literacy (HL) by survey item, the results revealed notable differences across domains (Table 1).
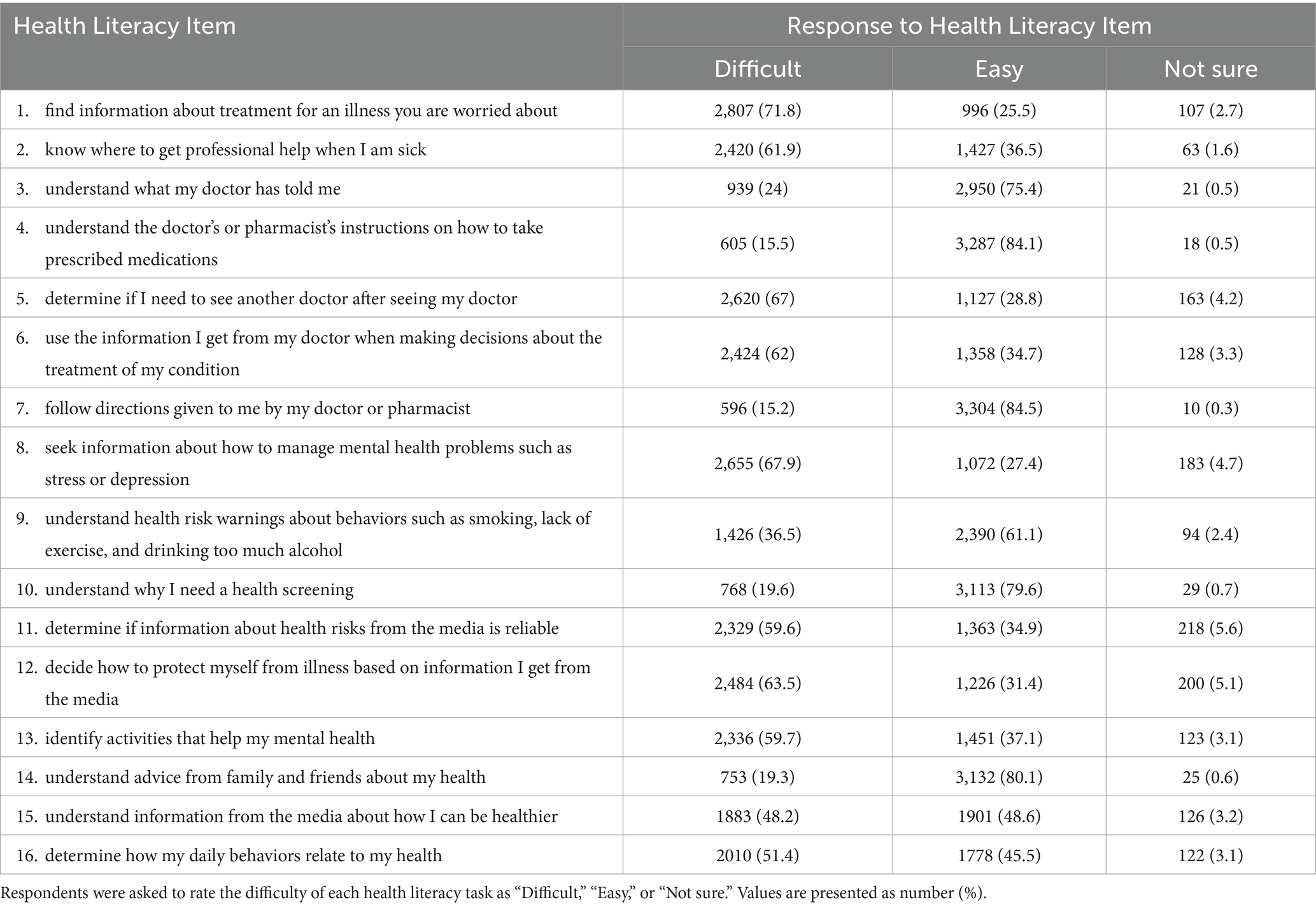
Table 1. Response rates by health literacy item.
Older adults reported greater difficulty in tasks related to information-seeking and evaluation—particularly in finding information about treatment (71.8%), managing mental health problems (67.9%), deciding whether to seek a second opinion (67.0%), and determining the reliability of media-based health information (59.6%). In contrast, HL was relatively high in domains involving direct communication with healthcare providers, such as understanding medication instructions (84.1%), following directions from doctors or pharmacists (84.5%), and understanding advice from family and friends (80.1%).
Sociodemographic and health behavior variables were analyzed across age and gender groups, and all variables demonstrated statistically significant differences (p < 0.001) (Table 2). Men were more likely to be married and economically active, while women tended to have lower educational attainment but reported more favorable health behaviors, such as lower rates of smoking and alcohol consumption. Engagement in healthy behaviors declined with age in both genders.
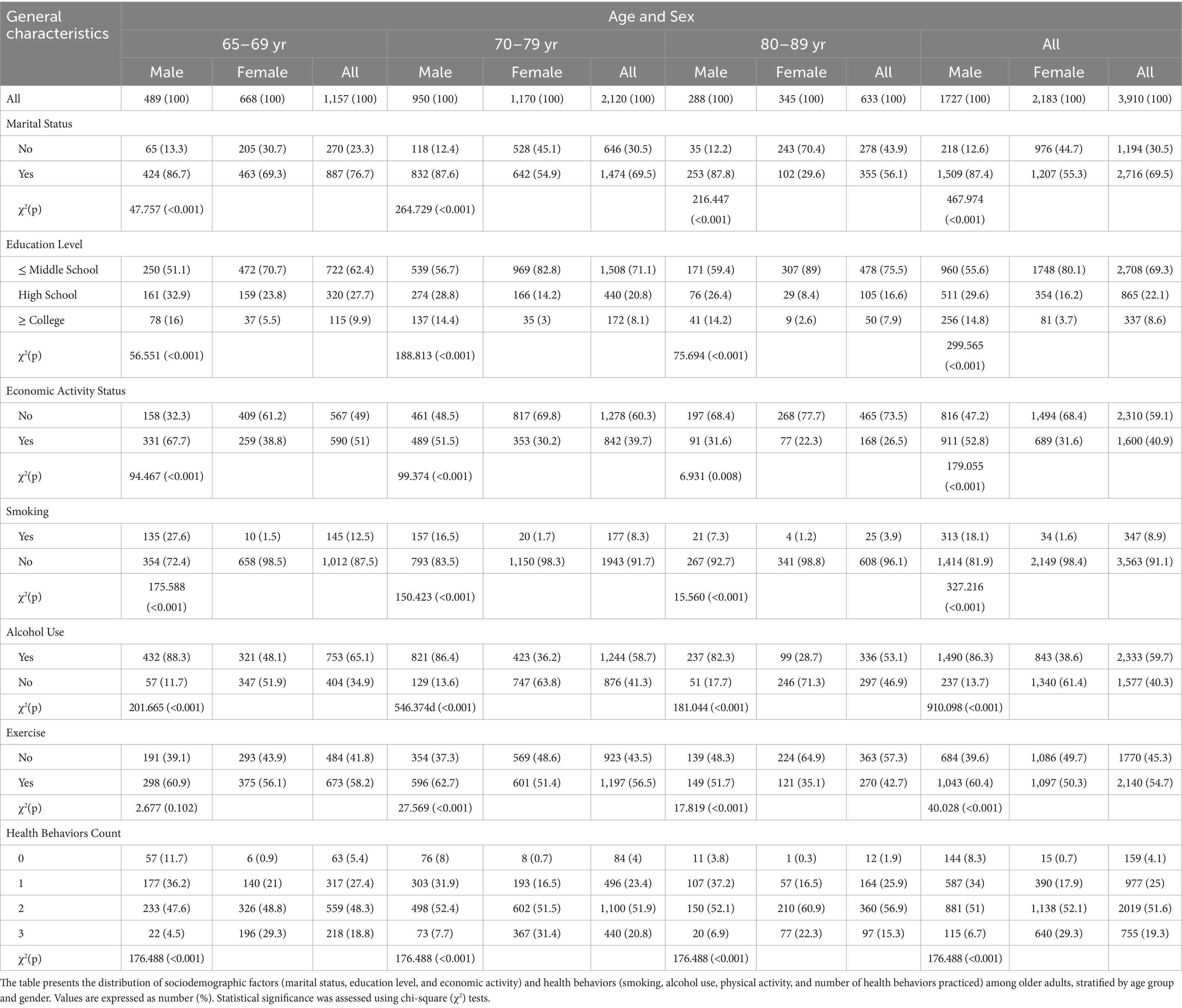
Table 2. Results of the distribution of general characteristics and health behaviors by gender and age of subjects.
An analysis of sociodemographic characteristics and health behaviors by age and gender revealed statistically significant differences across all variables (p < 0.001, Table 2).
In terms of marital status, men were consistently more likely to be married than women across all age groups. Among those aged 65–69, 86.7% of men were married compared to 69.3% of women. This pattern persisted in the 70–79 age group (men: 87.6%, women: 54.9%) and was even more pronounced in the 80–89 age group (men: 87.8%, women: 29.6%). Educational attainment also showed marked gender and age differences. Women had a lower proportion of higher education (college or above) across all age groups. Notably, among women aged 80–89, 89% had completed only middle school or less, compared to 59.4% of men in the same age group. Overall, 80.1% of women and 55.1% of men had an education level of middle school or less. Economic activity was significantly higher among men. In the 65–69 age group, 67.7% of men were economically active, compared to just 38.8% of women. Similar patterns were observed in the 70–79 (men: 54.5%, women: 30.2%) and 80–89 (men: 31.6%, women: 22.3%) age groups. Smoking and alcohol consumption were also substantially higher in men. The overall current smoking rate was 18.2% among men and only 1.6% among women. Similarly, 86.3% of men reported current alcohol consumption, compared to 38.6% of women. Engagement in regular physical activity was generally higher in men. In the 65–69 age group, 60.9% of men and 56.1% of women reported engaging in regular exercise. This trend continued in the 70–79 group (men: 62.7%, women: 51.4%) and the 80–89 group (men: 51.7%, women: 35.1%). Regarding the number of healthy behaviors practiced (based on a 0–3 score for non-smoking, non-drinking, and regular exercise), there were clear gender differences. A higher proportion of women reported practicing all three healthy behaviors compared to men. Specifically, among those aged 65–69, 29.3% of women versus only 4.5% of men practiced all three. This trend continued in the 70–79 group (women: 31.4%, men: 7.7%) and the 80–89 group (women: 22.3%, men: 6.9%).
3.2 Self- reported HL levels among older adults
Chi-square analyses revealed significant associations between HL levels and health behaviors in several subgroups (Table 3). For men aged 65–69, the proportion of HL-high individuals was higher among non-drinkers (57.9%) compared to drinkers (36.3%), and among those who exercised (43.0%) compared to those who did not (32.5%). Similar patterns were observed in men aged 70–79 and 80+, where exercise was significantly associated with higher HL. Among women, exercise was significantly linked to HL across all age groups except for those aged 80 and above. Smoking and drinking were generally not significantly associated with HL in women.
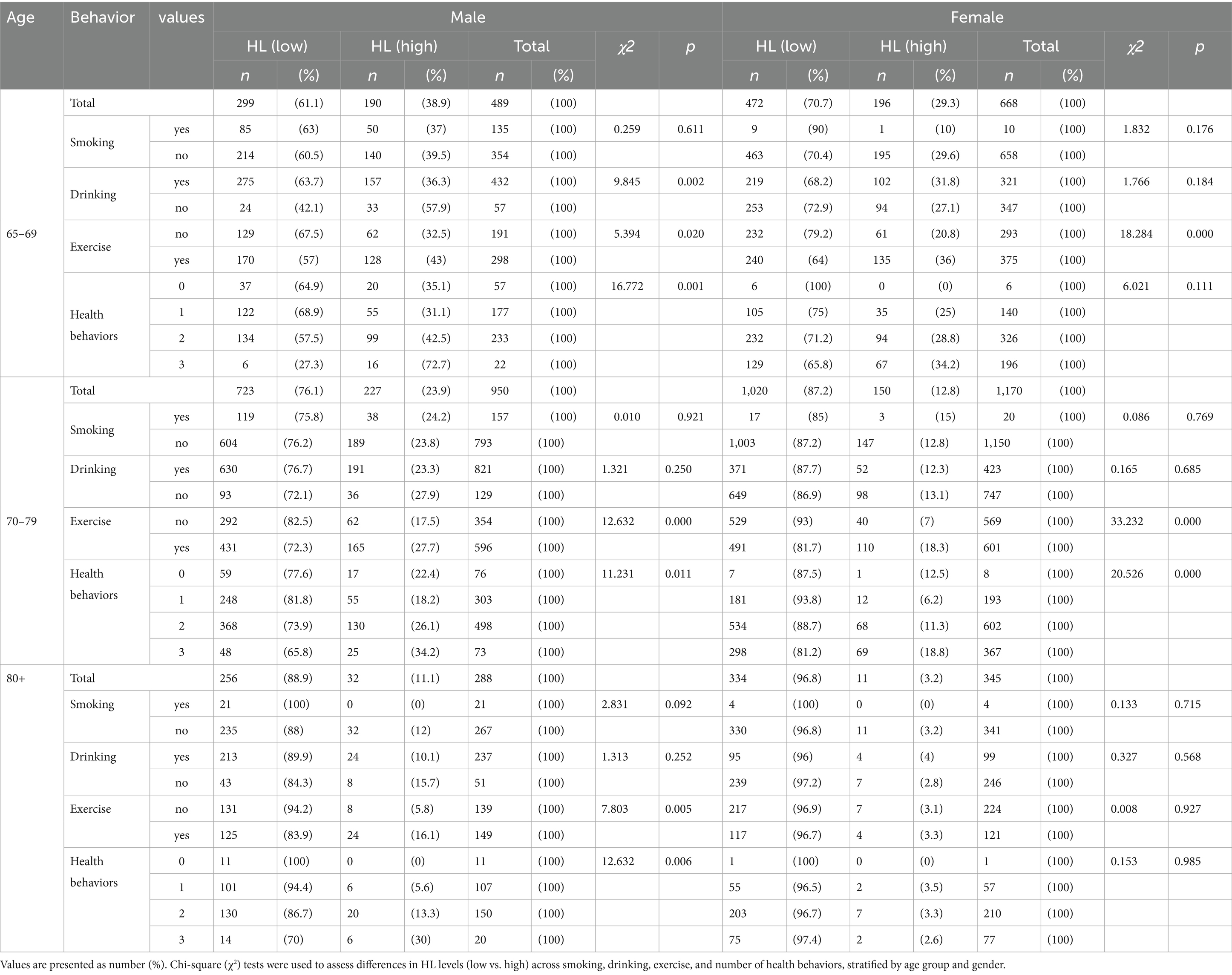
Table 3. Distribution of self-reported HL levels among older adults.
In both men and women, a consistent trend emerged: individuals who practiced more healthy behaviors (non-smoking, non-drinking, and regular exercise) were more likely to report high HL. This relationship was especially clear among those who practiced all three behaviors, with HL-high rates peaking in these groups, although the pattern was less evident in women aged 80 and above.
3.3 Key predictors of self-reported health literacy (HL)
Logistic regression analyses stratified by age and gender (Table 4; Figure 2) revealed that educational attainment and regular physical activity were consistent predictors of higher self-reported health literacy (HL) across all age and gender groups.
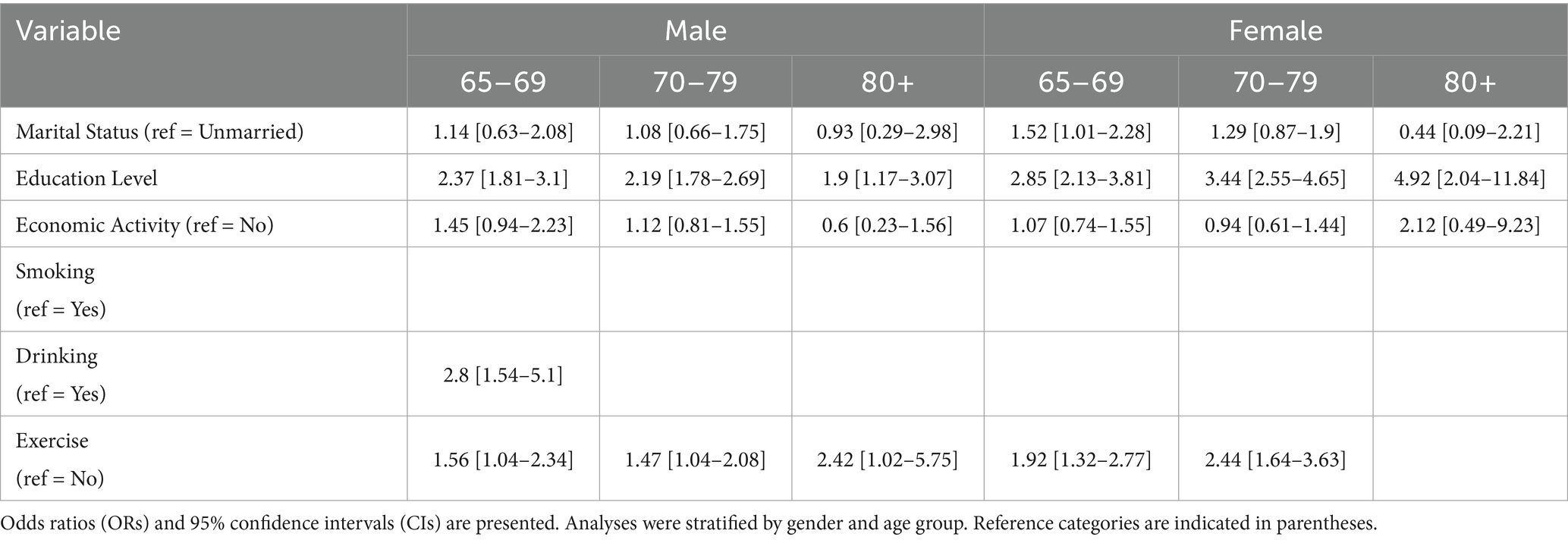
Table 4. Predictors of self-reported health literacy by age and gender.
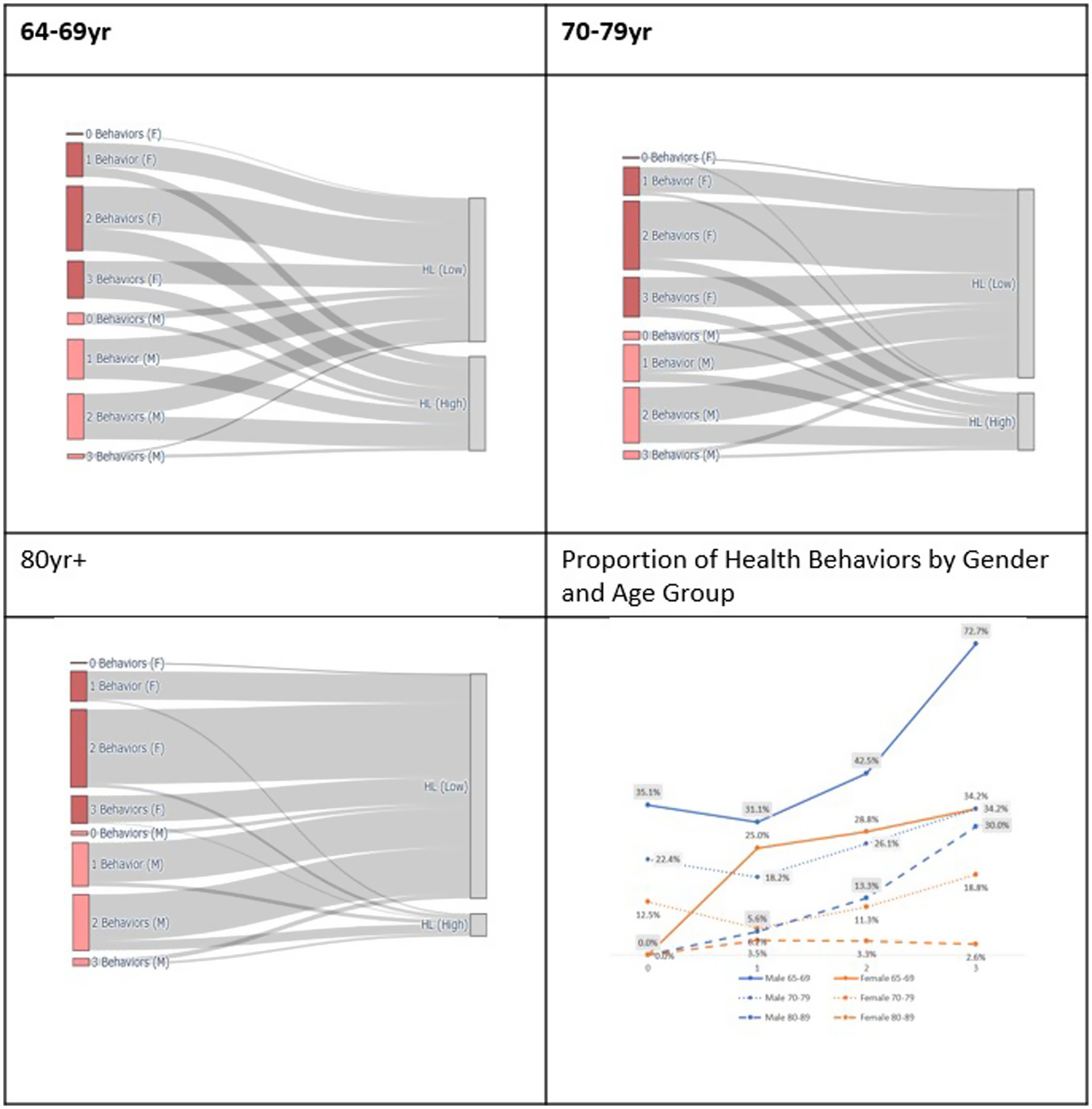
Figure 2. Distribution of health behaviors and health literacy levels by gender and age group.
Among men aged 65–69, those with higher educational attainment were more than twice as likely to report high HL compared to those with lower education (OR = 2.37, 95% CI: 1.81–3.10). In this group, regular physical activity (OR = 1.56, 95% CI: 1.04–2.34) and abstaining from alcohol (OR = 2.80, 95% CI: 1.54–5.11) were also significantly associated with higher HL.
In women aged 65–69, higher educational attainment was also significantly associated with higher HL (OR = 2.85, 95% CI: 2.13–3.81). Additionally, being married (OR = 1.52, 95% CI: 1.01–2.28) and engaging in regular physical activity (OR = 1.92, 95% CI: 1.32–2.77) were positively associated with HL.
In the 70–79 age group, education remained a significant predictor of HL in both men (OR = 2.19, 95% CI: 1.78–2.69) and women (OR = 3.44, 95% CI: 2.55–4.65). Among women, regular physical activity also showed a significant positive association with HL (OR = 2.44, 95% CI: 1.64–3.63). However, this relationship was not observed in men within the same age group.
Among adults aged 80 and older, the relationship between educational attainment and HL was most pronounced in women (OR = 4.92, 95% CI: 2.04–11.84), indicating that highly educated older women were nearly five times more likely to report high HL compared to those with lower education.
In contrast, economic activity, smoking, and marital status (in some age groups) did not show consistent or significant associations with HL across most subgroups.
4 Discussion
This study contributes to the growing body of evidence on health literacy (HL) by examining how sociodemographic and behavioral factors influence HL among older adults in Korea. To our knowledge, this is one of the first studies to examine predictors of health literacy among older Korean adults using a nationally representative dataset and a validated tool suitable for international comparisons.
Previous research has established that HL is closely related to demographic characteristics and health-related behaviors (5, 7). The present findings are consistent with and complement these studies by highlighting specific behavioral patterns and subgroup differences. The present findings are consistent with and complement these studies by highlighting specific behavioral patterns and subgroup differences.” In the Korean context, previous research has also identified education, income, and social engagement as significant determinants of HL among older adults (13). Additionally, Jeong and Kim (14) found that over 60% of Korean adults reported inadequate health literacy, which was strongly associated with barriers to health information access such as low education, older age, and digital limitations.
These findings support the relevance of our behavioral variables and affirm the study’s contribution to the national discourse on health literacy determinants.
Notably, regular physical activity was positively associated with HL, aligning with prior studies that suggest health-promoting behaviors enhance both cognitive function and HL (15). Recent research has demonstrated that physical activity improves cognitive capacity, which in turn supports the development of HL (16, 17). This may help explain the positive association between exercise and HL observed in this study. Furthermore, it is plausible that individuals who engage in regular exercise are also more proactive in seeking and processing health information.
Gender differences in HL were also observed, with men reporting higher HL levels than women. This may reflect underlying sociocultural influences or differences in health information–seeking behavior. For example, men are more likely to actively search for health information via digital platforms, whereas women often rely on interpersonal sources such as family or healthcare providers. These behavioral differences can contribute to gender gaps in HL and should be considered when designing targeted interventions, especially in digital health literacy education (18).
While this study did not directly assess digital health literacy, prior research has highlighted its relevance for older adults. For instance, Hwang et al. found that age, gender, education level, and chronic illness significantly affect digital HL among older adults living alone in Korea (19). Such findings suggest that digital access and competency may indirectly influence general HL levels, especially among those with limited exposure to digital health resources. Although this study did not measure digital HL, the absence of significant associations among women aged 80 and older may reflect underlying digital disparities in this group. Future research is needed to clarify the intersection between traditional and digital HL in older populations, particularly those facing technological barriers.
While this study did not directly assess functional ability, previous research has shown that low HL is associated with a greater risk of impairment in activities of daily living (ADLs) among older adults with chronic conditions (20). This suggests that HL may influence not only information processing but also the capacity to perform daily health-related tasks, which should be explored in future research.
Although this study did not examine the relationship between HL and the use of dietary supplements, previous research has shown that older adults with low HL may struggle to understand relevant product information. For instance, Ko et al. reported that individuals with higher HL were better equipped to interpret and apply information about dietary (21). This highlights the importance of improving health communication strategies, particularly among older populations.
Taken together, the findings suggest that HL is influenced by a range of demographic and behavioral factors, and that digital HL, in particular, plays a critical role in maintaining functional health and independent living. Furthermore, the relationship between HL and health behaviors may be bidirectional. Older adults with higher HL are more likely to recognize and modify risky behaviors, such as smoking and alcohol consumption, and are also more inclined to adopt and sustain healthy lifestyles—thereby reinforcing a positive cycle between HL and health behavior (22).
To improve HL among older adults, there is a need for tailored education programs and innovative methods of health information delivery. Digital platforms, in particular, should be leveraged to address the needs of digitally underserved populations. Future research should examine the relationship between traditional and digital HL and develop customized interventions to bridge these gaps.
While previous studies such as Jeong and Kim have emphasized the impact of access barriers on health literacy, they did not explore how specific health behaviors interact with literacy levels (14). Despite the growing body of research on health literacy, few studies have examined its relationship with specific behavioral factors among older Korean adults using nationally representative data.
This study adds to the literature by highlighting age- and gender-specific predictors of HL and by using a validated instrument applied in a large-scale national survey.
Finally, this study used a self-reported measure of HL, which may be subject to response bias. In addition, the generalizability of findings may be limited due to sample characteristics. These limitations should be addressed in future studies employing more diverse measurement tools and representative samples.
5 Conclusion
This study investigated key sociodemographic and behavioral determinants of health literacy (HL) among older adults in Korea, using nationally representative data and a validated international tool. Higher HL levels were associated with being male, younger in age, having higher educational attainment, being married, and engaging in regular exercise. These findings offer novel insights into subgroup-specific disparities in HL and reinforce the need for targeted policy interventions.
To improve HL in this population, it is essential to promote physical activity and support the rebuilding of social networks and participation in economic activities—particularly among older women. Tailored HL strategies that consider gender- and age-specific characteristics are crucial.
Future research should focus on developing and evaluating integrated interventions that incorporate digital health literacy, which will be instrumental in informing national policies and designing effective programs to enhance HL among older adults in South Korea.
However, as this study employed a cross-sectional design, causal relationships between health literacy and the associated factors cannot be confirmed. Future studies using longitudinal designs are needed to validate these associations over time.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
This study was approved by the Konyang University Institutional Review Board (Approval number: KYU2025-05-003). Written informed consent from the [patients/participants OR patients/participants legal guardian/next of kin] was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
JS: Project administration, Formal analysis, Methodology, Investigation, Writing – review & editing, Writing – original draft, Data curation, Visualization, Conceptualization. SB: Writing – original draft, Supervision, Methodology, Writing – review & editing, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2024S1A5A8026723).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Sørensen, K, Van Den Broucke, S, Fullam, J, Doyle, G, Pelikan, J, Slonska, Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. (2012) 12:80. doi: 10.1186/1471-2458-12-80
2. Nutbeam, D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. (2000) 15:259–67. doi: 10.1093/heapro/15.3.259
4. OECD. (2025). Ageing and health: Key statistics. Available online at:https://www.oecd.org/health/ageing/
5. Berkman, ND, Sheridan, SL, Donahue, KE, Halpern, DJ, and Crotty, K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. (2011) 155:97–107. doi: 10.7326/0003-4819-155-2-201107190-00005
6. WHO. (2013). Health literacy: The solid facts. Available online at:https://www.euro.who.int/en/publications/abstracts/health-literacy.-the-solid-facts
7. Paasche-Orlow, MK, and Wolf, MS. The causal pathways linking health literacy to health outcomes. Am J Health Behav. (2007) 31:19–26.
8. Lee, KE, Yom, YH, Kim, SS, and Han, JH. Gender differences in oral health literacy related factors among elderly people. J Korean Acad Community Health Nurs. (2014) 25:54. doi: 10.12799/jkachn.2014.25.1.54
9. Von Wagner, C, Steptoe, A, Wolf, MS, and Wardle, J. Health literacy and health actions: a review and a framework from Health Psychology. Health Educ Behav. (2009) 36:860–77. doi: 10.1177/1090198108322819
10. Chun, H, and Lee, JY. Factors associated with health literacy among older adults: results of the HLS-EU-Q16 measure. KJHEP. (2020) 37:1–13. doi: 10.14367/kjhep.2020.37.1.1
11. Pelikan, JM, and Ganahl, K. Measuring health literacy in general populations: primary findings from the HLS-EU consortium’s health literacy assessment effort. In: A. H. Schulz, J. Mantas, B. Blobel, editors. Studies in health technology and informatics [internet]. Amsterdam, Netherlands: IOS Press (2017) p. 34–59.
12. Sun, S, Lu, J, Wang, Y, Wang, Y, Wu, L, Zhu, S, et al. Gender differences in factors associated with the health literacy of hospitalized older patients with chronic diseases: a cross-sectional study. Front Public Health. (2022) 10:944103. doi: 10.3389/fpubh.2022.944103
13. Kim, J, Jeon, SW, Byun, H, and Yi, E. Exploring E-health literacy and technology-use anxiety among older adults in Korea. Healthcare. (2023) 11:1556. doi: 10.3390/healthcare11111556
14. Jeong, SH, and Kim, HK. Health literacy and barriers to health information seeking: a nationwide survey in South Korea. Patient Educ Couns. (2016) 99:1880–7. doi: 10.1016/j.pec.2016.06.015
15. Zhang, X, Li, Z, Liu, Y, and Gai, Z. Great expectations: induced pluripotent stem cell technologies in neurodevelopmental impairments. Int J Med Sci. (2021) 18:459–73. doi: 10.7150/ijms.51842
16. Soreya, B, and Nora, A. Physical activity and its prophylactic effects on cognition and dementia. EJMHR. (2023) 1:79–86. doi: 10.59324/ejmhr.2023.1(3).15
17. Abdalkareem Jasim, S, Singh, M, Baqir Al-Dhalimy, AM, Zwamel, AH, Jawad, IA, and Shalaby, NS. The impact of chronic exercise on cognitive function: an overview of reviews. IJPS. (2024) 19:463–472. doi: 10.18502/ijps.v19i4.16561
18. Ireland, S, and Smith, JA. Health literacy across the life course: understanding equity and the influence of culture and gender. R Midford, G Nutton, B Hyndman, and S Silburn, editors. Health and education interdependence [Internet]. Singapore: Springer Singapore; (2020)
19. Hwang, M, Kim, G, Lee, S, and Park, YH. Digital health literacy and associated factors among older adults living alone in South Korea: a cross-sectional study. Res Community Public Health Nurs. (2024) 35:389. doi: 10.12799/rcphn.2024.00766
20. Choi, HG. Association between health literacy and disability in activities of daily living among older adults with multimorbidity: findings from the Korean health panel survey in 2021. J Korean Acad Fundam Nurs. (2024) 31:506–14. doi: 10.7739/jkafn.2024.31.4.506
21. Ko, Y, Kim, HJ, and Lee, SM. Health literacy, label comprehension, and consumer perceptions of quasi-drug information among Korean adults: a cross-sectional study. RMHP. (2025) 18:173–83. doi: 10.2147/RMHP.S502368
Keywords: health literacy, older adult, health behavior, logistic regression, South Korea
Citation: Shin J and Baek S (2025) Determinants of self-reported health literacy among older adults in South Korea: a cross-sectional study. Front. Public Health. 13:1628245. doi: 10.3389/fpubh.2025.1628245
Edited by:
Wei Luan, Shuguang Hospital Affiliated to Shanghai University of TCM, ChinaReviewed by:
Enver Envi Roshi, University of Medicine, AlbaniaPhuong Thi Anh Nguyen, Hue University, Vietnam
Copyright © 2025 Shin and Baek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Seunghui Baek, c2gxMDBAc3VuZ3NoaW4uYWMua3I=