 Shanyu Zhou
Shanyu Zhou Huiqing Chen
Huiqing Chen Min Yang
Min Yang- Guangdong Province Hospital for Occupational Disease Prevention and Treatment, Guangzhou, Guangdong, China
Background: Essential service workers are exposed to significant occupational health risks. Low occupational health literacy (OHL) has been linked to increased risks of occupational injuries and work-related illnesses. However, limited evidence exists regarding the OHL of essential service workers and the impact of enterprise characteristics on OHL. This study aimed to examine the associations between enterprise characteristics and OHL among essential service workers in Guangdong Province, China.
Study design: Cross-sectional study.
Methods: A cross-sectional survey was conducted among 2,640 essential service workers from the environmental sanitation (n = 880), transportation (n = 880), and express and food delivery industries (n = 880), using multi-stage cluster random sampling. OHL was assessed using the National Occupational Health Literacy Monitoring Questionnaire, which measures four dimensions: knowledge of occupational health laws, knowledge of occupational health protection, skills of occupational health protection, and healthy work patterns and behaviors. Multivariable logistic regression was used to examine associations between enterprise characteristics (scale, ownership, industry) and OHL, with stratified analyses by monthly income.
Results: The overall OHL level among essential service workers was 52.8%. Working in small and micro enterprises (adjusted OR = 1.42, 95% CI: 1.17–1.72) and private enterprises (adjusted OR = 1.28, 95% CI: 1.05–1.55) was associated with higher OHL, while employment in the express and food delivery industry was associated with lower OHL (adjusted OR = 0.64, 95% CI: 0.49–0.82). Monthly income significantly moderated these associations, with stronger effects observed in higher-income groups.
Conclusion: Enterprise characteristics significantly influence OHL among essential service workers. Targeted OHL promotion strategies should be developed based on enterprise characteristics, with particular attention to large, state-owned enterprises and express and food delivery workers.
Introduction
Occupational health literacy (OHL) refers to workers’ consciousness and capacity to access fundamental occupational health knowledge, implement healthy work and lifestyle practices, mitigate risks of occupational diseases and work-related illnesses, and maintain and promote their personal health status (1). The World Health Organization recognizes health literacy as a critical determinant of health (2). In the workplace, adequate OHL empowers workers to make health-appropriate decisions, comply with safety protocols and actively participate in health promotion activities (3, 4). Conversely, research has demonstrated that low OHL levels are associated with increased occupational injuries, reduced work ability, and a higher prevalence of work-related illnesses (5–8), highlighting the need to address OHL as a public health priority. Moreover, OHL can be improved through interpersonal support and organizational initiatives that promote healthy behaviors and take a comprehensive approach to employee health (9, 10).
Despite the recognized importance of OHL for worker health and safety, existing research has largely concentrated on traditional industries, with less attention paid to occupational groups that are essential to urban functioning. In China, essential service workers—including environmental sanitation workers, transportation drivers, and express and food delivery personnel—not only constitute a significant proportion of the workforce, but also play a fundamental role in maintaining urban operations (11). These workers are routinely exposed to various occupational hazards, including adverse weather conditions, irregular work hours, high physical demands, traffic accidents, and psychosocial stress (12). However, despite their occupational vulnerability, limited surveillance data exist regarding their OHL levels and associated factors. China has experienced a significant structural transformation in its labor force, with a marked shift toward the tertiary sector. As China’s largest employment hub, Guangdong Province encompasses approximately one-tenth of the nation’s workforce. By 2021, the tertiary industry employed 37.54 million workers, accounting for 53.1% of the province’s total workforce—a 4.5% increase from 2017 (13, 14). This transformation is particularly manifested in the rapid growth of platform-based essential services, where workers face unique occupational health challenges.
Research suggests that enhancing health literacy requires consideration of both individual factors and organizational influences. In the workplace context, this interplay between individual and organizational factors becomes especially critical for OHL (15). Given the unique occupational context of essential service workers, it is important to further explore the determinants that may influence their OHL, particularly those related to the organizational and structural environment in which they work. Among these, enterprise characteristics—such as enterprise scale, ownership, and industry—may play a significant role by shaping organizational health policies, access to occupational health services, training opportunities, and workplace health culture (16–18). However, empirical evidence examining the relationship between enterprise characteristics and OHL remains limited. Existing studies have primarily focused on traditional manufacturing sectors, while essential service industries have received insufficient attention (19). Understanding how enterprise characteristics affect OHL is crucial for developing targeted interventions and improving occupational health protection systems.
Therefore, this study aimed to assess OHL levels among essential service workers in Guangdong, analyze the associations between enterprise characteristics and OHL, and explore the potential moderating effect of workers’ income levels in these relationships. The findings will contribute to the evidence base for the development of targeted occupational health interventions in the essential service sector.
Methods
Study design and sampling
This cross-sectional study was conducted as part of the Guangdong Province Key Population Occupational Health Literacy Surveillance Project in 2022. According to the project protocol, each selected district required a minimum of 220 participants from each industry. With four districts and three industries involved, this determined the total target sample size of 2,640 participants.
A multistage stratified random sampling method was employed. Initially, four cities were randomly selected from Guangdong Province, followed by the selection of one district within each city: Baiyun district in Guangzhou, Xiangzhou district in Zhuhai, Dianbai district in Maoming, and the municipal district of Dongguan. Within each selected district, enterprises from three targeted industries—environmental sanitation, transportation, and express and food delivery—were randomly sampled. Specifically, 1–3 sanitation institutions, 2–3 transportation companies (including taxi, public transportation, freight, and ride-hailing platform companies), and 1–3 express or food delivery companies were selected in each district. Eligible sanitation workers, drivers, couriers, and food delivery workers from these enterprises who voluntarily agreed to participate were recruited for the survey.
A total of 42 enterprises were selected: 12 from the environmental sanitation industry, 17 from the transportation industry, and 13 from the express and food delivery industry. The questionnaires underwent real-time review, and data collection stopped automatically when 220 valid responses were reached for each industry in each district. A total of 2,787 questionnaires were collected. After quality review, 147 questionnaires were excluded (21 due to duplicated answers and 126 due to completion time less than 3 min), resulting in 2,640 valid questionnaires, with 880 individuals from each industry (Figure 1).
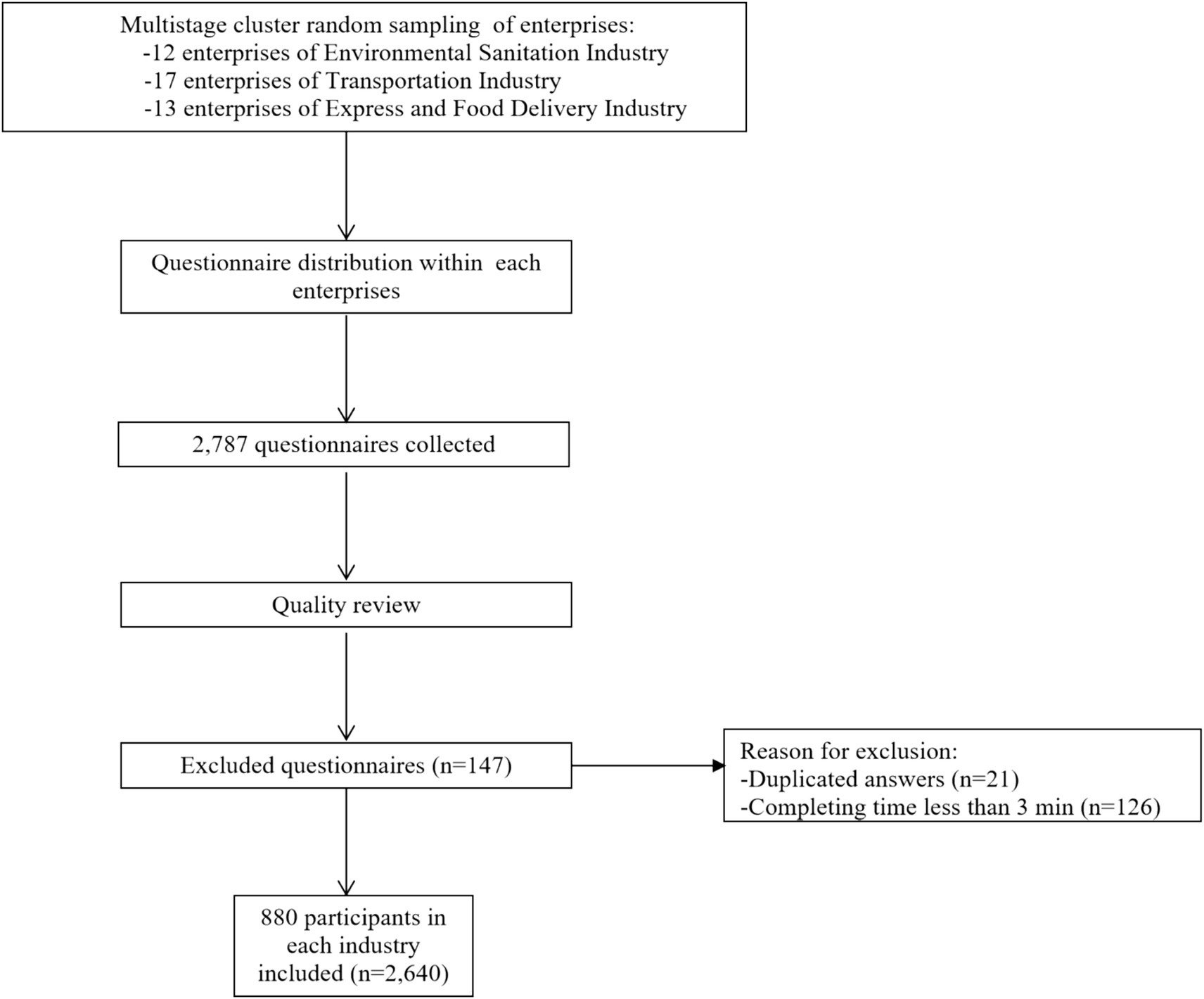
Figure 1. Flow chart of sample selection.
Questionnaire and data collection
The OHL was assessed using the National Occupational Health Literacy Monitoring Questionnaire, which was developed by the National Institute for Occupational Health and Poison Control and validated in previous studies (20). The questionnaire consisted of two sections: (1) basic demographic and occupational information, including sex, age, ethnic group, marital status, household registration status (hukou type), enterprise scale, ownership, industry, educational level, monthly income, working years and so on. (2) An OHL assessment with 41 items across four dimensions: knowledge of occupational health laws (11 items), knowledge of occupational health protection (14 items), skills of occupational health protection (4 items), and healthy work patterns and behaviors (12 items). The questionnaire was administered through the National Occupational Health Literacy Monitoring Survey Information System1. To ensure data quality and prevent potential online data collection bias, the system generated unique QR codes for questionnaire access, preventing duplicate submissions (21). Participants completed the survey anonymously by scanning these QR codes with smartphones under supervised conditions. A comprehensive data quality assurance mechanism was incorporated, including mandatory response fields to ensure data completeness, automated logical consistency checks, and backend data verification with real-time completion status tracking. Trained research staff conducted on-site supervision during questionnaire completion, providing clarification on items when necessary while avoiding response influence.
Measures
Dependent variables
According to the ‘Standards for Calculating Occupational Health Literacy Levels among Key Populations (2022), both overall and dimension-specific OHL levels were assessed (22). The scoring system assigned different weights to questionnaire items: in the Basic Skills of Occupational Health Protection dimension, one multiple-choice item carried 4 points, while three single-choice items were assigned 3 points each. Items in all other dimensions were valued at 1 point apiece, yielding a maximum total score of 50. Due to skip patterns in some multiple-choice questions, the number of items answered varied among respondents, resulting in different possible total scores for each respondent. Adequate OHL was defined as achieving ≥80% of the total possible score. The same criterion was applied to each dimension. The overall OHL level was determined as the proportion of participants who met the criterion for adequate OHL, and the same method was used to calculate dimension-specific OHL levels.
Independent variables
Enterprise characteristics included scale, ownership and industry. Scale was classified based on the total number of employees in accordance with the official standards of the National Bureau of Statistics of China (23). Specifically, enterprises with 1,000 or more employees were defined as large enterprises, and those with 300–999 employees were classified as medium enterprises. In line with the statistical standards, enterprises with 20–299 employees are considered small enterprises, and those with fewer than 20 employees are considered micro enterprises. However, in this study, due to the relatively small number of micro enterprises (n = 116), small and micro enterprises were combined into a single category (enterprises with fewer than 300 employees) for the purposes of analysis. Ownership was classified into three categories: state-owned enterprises, private enterprises, and foreign/Hong Kong-Macao-Taiwan (HKMT)-funded enterprises, based on the registration types specified by the Administration for Industry and Commerce (24). Industry was divided into three categories according to the main business activities of the enterprises: environmental sanitation, transportation, express and food delivery.
Covariates
Potential confounders included sex (male and female), age (<30, 30–39, 40–49, and ≥50 years), ethnicity (Han, others), marital status (married, unmarried, others), hukou type (agricultural, Non-agricultural), education level (primary education or below, lower secondary education, upper secondary education, tertiary education), monthly income (<3,000, 3,000–4,999, 5,000–6,999, and ≥7,000 CNY), and working years (<2, 2–<4, 4–<6, and ≥6 years).
Statistical analysis
Descriptive statistics were used to summarize all variables, with categorical variables expressed as frequencies and percentages. The distribution of overall OHL and its dimensions across enterprise characteristics was summarized. Chi-square tests were used to examine differences in OHL and its dimensions among enterprise characteristics. Logistic regression models were employed to assess associations between enterprise characteristics and OHL, as well as its four dimensions, with both crude and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) reported. Adjusted models included sex, age, working years, ethnic group, marital status, hukou type, education level, monthly income, and other enterprise characteristics. Stratified analyses by monthly income and interaction analyses between enterprise characteristics and monthly income were also conducted. All analyses were performed using R software (version 4.4.2), with a two-sided p-value <0.05 considered statistically significant.
Results
Participant characteristics
A total of 2,640 participants were included in this study. Males predominated (70.8%), with most participants aged between 30–39 years (29.9%) and 40–49 years (29.1%). Most participants worked in small and micro enterprises (57.4%), under private ownership (53.7%), and were equally distributed across three industries: environmental sanitation, transportation, and express and food delivery services (33.3% each). The demographic and occupational characteristics of participants are detailed in Table 1.
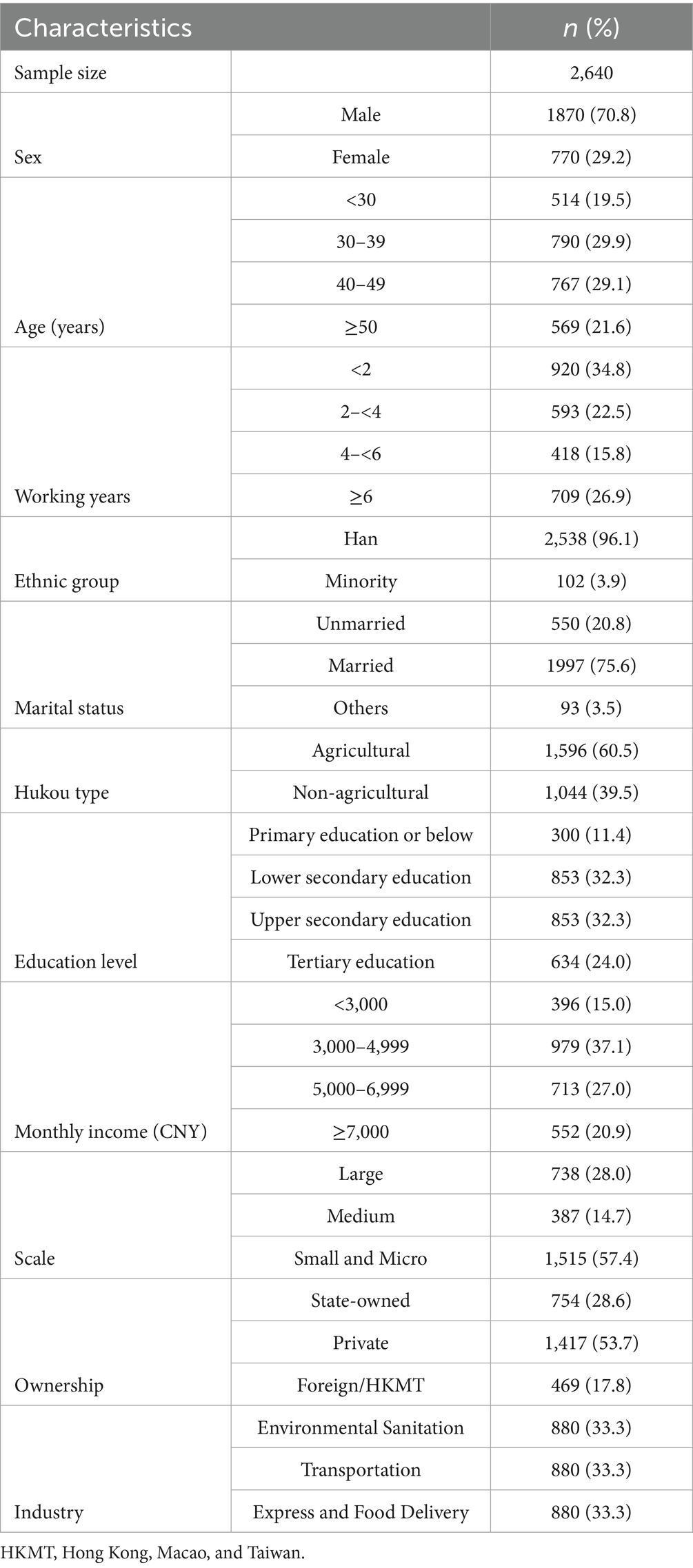
Table 1. The demographic and occupational characteristics of participants.
OHL levels by enterprise characteristics
The overall OHL level among essential service workers was 52.8%, with the knowledge of occupational health protection dimension showing the highest level (77.6%) and skills of occupational health protection dimension showing the lowest (44.5%). As presented in Table 2, analysis across industries revealed no significant differences in overall OHL levels (χ2 = 0.149, p = 0.928), with levels of 53.3, 52.4, and 52.7% observed in environmental sanitation, transportation, and express and food delivery industries, respectively. However, significant differences were observed in the healthy work patterns and behaviors dimension (p < 0.001), where environmental sanitation workers having the highest level (64.2%) and express and food delivery workers the lowest (53.6%). In terms of enterprise characteristics, small and micro enterprises showed significantly higher OHL levels (56.9%) compared to large enterprises (47.0%) (χ2 = 23.981, p < 0.001). Furthermore, significant variations were found across ownership types (χ2 = 46.943, p < 0.001), with foreign/HKMT-funded enterprises showing the highest OHL level (60.1%), followed by private enterprises (55.8%), while state-owned enterprises demonstrated the lowest level (42.6%).
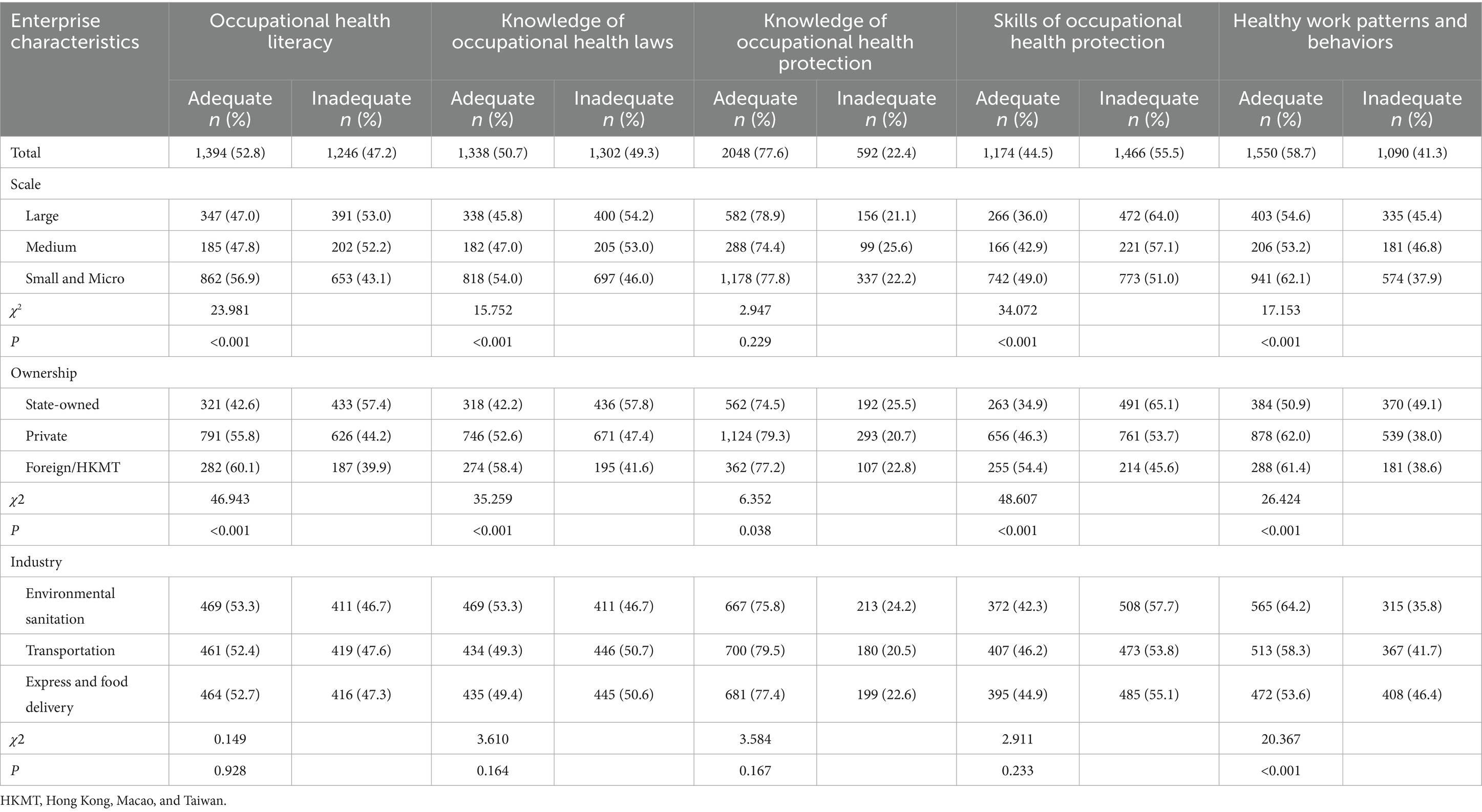
Table 2. Distribution of occupational health literacy and its dimensions by enterprise characteristics.
Associations between enterprise characteristics and OHL
Logistic regression analyses revealed significant associations between enterprise characteristics and OHL dimensions (Table 3). In terms of enterprise scale, small and micro enterprises showed positive associations compared to large enterprises, with crude OR of 1.49 (95%CI:1.25–1.78, p < 0.05) for overall OHL, which remained significant after adjusting for demographic and other enterprise characteristics (adjusted OR = 1.42, 95%CI: 1.17–1.72, p < 0.05). This pattern was particularly in Skills of Occupational Health Protection (adjusted OR = 1.56, 95%CI: 1.28–1.90, p < 0.05). Regarding ownership, private enterprises demonstrated positive association with overall OHL compared to state-owned enterprises (adjusted OR = 1.28, 95%CI: 1.05–1.55, p < 0.05), while foreign/HKMT enterprises showed negative association in Healthy Work Patterns and Behaviors dimension (adjusted OR = 0.83, 95%CI: 0.72–0.95, p < 0.05). For industries, compared to environmental sanitation industry, express and food delivery industry showed significant negative associations in both Healthy Work Patterns and Behaviors dimension (adjusted OR = 0.53, 95%CI: 0.41–0.68, p < 0.05) and overall OHL (adjusted OR = 0.64, 95%CI: 0.49–0.82, p < 0.05). Transportation sector also demonstrated negative association in Healthy Work Patterns and Behaviors dimension (adjusted OR = 0.68, 95%CI: 0.54–0.86, p < 0.05).
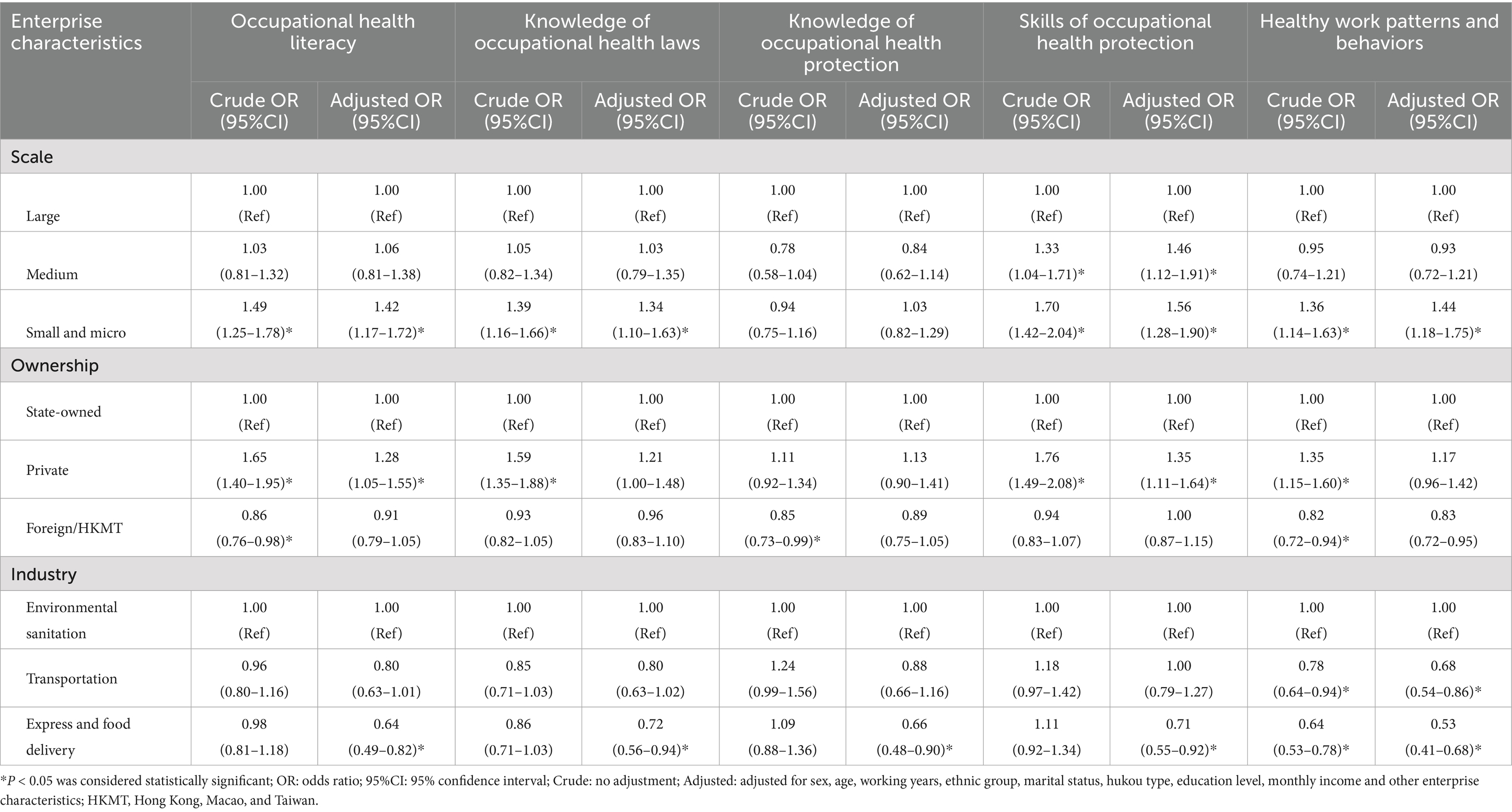
Table 3. Association between enterprise characteristics and different dimensions of occupational health literacy.
Stratified analyses
Stratified analyses revealed significant interactions between monthly income levels and enterprise characteristics in relation to OHL and its dimensions (all Pfor interaction<0.05, Figure 2). The association between small/micro enterprises and OHL was markedly stronger in the high-income subgroup (≥7,000 CNY) with an adjusted OR of 4.67 (95% CI: 2.92–7.65) compared to other income subgroups. The relationship between ownership and OHL, particularly knowledge of occupational health laws, was significantly positive only in private enterprises within the low-income subgroup (<3,000 CNY). The negative association between industry and OHL was only statistically significant only in higher income subgroups, suggesting that industry-specific factors predominantly influence OHL among higher-income workers.
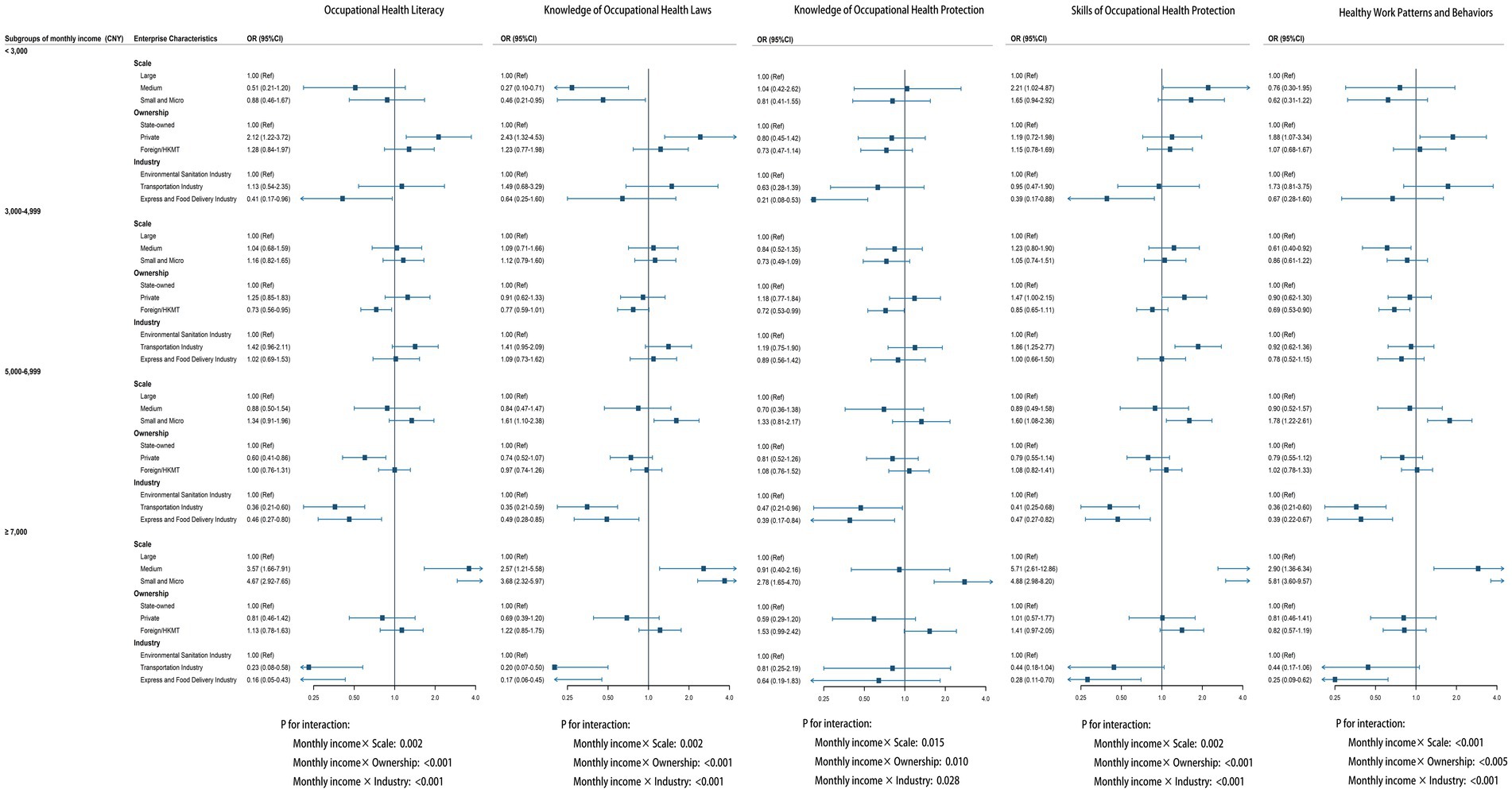
Figure 2. Associations between enterprise characteristics and occupational health dimensions stratified by monthly income. OR: odds ratio; 95%CI: 95% confidence interval; Adjusted for sex, age, working years, ethnic group, marital status, hukou type, education level, monthly income and other enterprise characteristics; HKMT: Hong Kong, Macao, and Taiwan; Pfor interaction were calculated between monthly income and enterprise scale, ownership, and industry, respectively.
Discussion
This surveillance study provides important insights into OHL among essential service workers in Guangdong Province, China. Our findings revealed a relatively low overall OHL level of 52.8%, significant associations between enterprise characteristics (scale, ownership, and industry) and OHL levels, as well as notable moderating effects of workers’ monthly income on these relationships. These results highlight the complex interplay between enterprise characteristics and monthly income in shaping OHL among essential service workers, emphasizing the importance of considering both enterprise factors and income levels in OHL surveillance and the development of targeted interventions.
Inadequate health literacy is a universal problem both in the general and working populations, and it may be restricting the workers understanding of occupational health and safety training (25). The overall OHL level of 52.8% among essential service workers in this study is higher than the tertiary industry national average (48.9%), but lower than that of secondary industry workers (56.5%) (26). Unlike workers in more regulated industries, essential service workers often have limited access to occupational health resources, training opportunities, and organizational support systems, which may further exacerbate their vulnerability to occupational risks. While unadjusted analysis showed similar OHL levels across environmental sanitation (53.3%), transportation (52.4%), and express and food delivery industries (52.7%), multivariate analysis revealed significant differences after controlling for confounding factors. Environmental sanitation workers demonstrated the highest level in healthy work patterns and behaviors (64.2%) and knowledge of occupational health protection (75.8%). This strong performance could be attributed to the standardization of sanitation work and implementation of comprehensive occupational health management systems in recent years. Our findings show similar patterns with previous research, where approximately 70.7% of sanitation workers showed moderate levels of knowledge in preventing occupational health risks, and 70.1% reported regular use of personal protective equipment during work (27). These results suggest that sanitation workers generally maintain relatively good levels of occupational health knowledge and protective behaviors. Transportation workers showed moderate levels of occupational health literacy (52.4%) and knowledge of occupational health protection (79.5%), yet their healthy work behaviors (58.3%) were lower than environmental sanitation workers. This gap between knowledge and behavior deserves attention. Transportation workers typically receive safety training and daily health education, which may explain their moderate knowledge levels. However, a study has shown that these workers, particularly online ride-hailing drivers, are characterized by working long hours with few breaks (28). Such intensive work patterns may contribute to fatigue and reduced adherence to healthy work practices despite having adequate health knowledge. Notably, express and food delivery workers demonstrated significantly lower OHL levels in the adjusted models. This finding aligns with previous research highlighting the precarious working conditions in the rapidly expanding gig economy (29). Unlike workers in more traditional sectors, express and food delivery personnel often operate as independent contractors rather than formal employees, which may limit their access to systematic occupational health training and organizational support systems (30). Additionally, express and food delivery workers usually operate under intense time pressures, and irregular work schedules, which may limit their opportunities to engage in health-promoting activities and access occupational health resources (31, 32). The relatively lower OHL compared to secondary industry may be attributable to inadequate health training and weaker protection systems, highlighting the need for targeted interventions in these essential service sectors.
Further analysis revealed that enterprise scale was also significantly associated with OHL. Specifically, our study found that workers from small and micro enterprises had higher OHL levels compared to those from large enterprises, which contrasts with previous research suggesting that smaller enterprises usually have limited resources for occupational health services and training (19). One possible explanation for this discrepancy might be the implementation of the “Occupational Health Support Initiative for Small, Medium and Micro-sized Enterprises” in recent years, which has promoted the standardization of occupational health management and increased workers’ awareness of occupational health protection. This initiative may have significantly improved the accessibility and effectiveness of occupational health education and training within smaller enterprises (33). Moreover, smaller enterprises might have closer interpersonal relationships and communication channels between management and employees, facilitating more effective dissemination of occupational health information and greater responsiveness to health concerns (34). This trend was particularly evident among workers with a monthly income ≥7,000 CNY, possibly because higher-income employees tend to have greater health awareness and are more likely to benefit from occupational health initiatives implemented in small and micro enterprises (35).
Our results regarding enterprise ownership and OHL present a contrast to existing literature. We found that workers in private enterprises had significantly higher overall OHL compared to those in state-owned enterprises, whereas previous studies typically reported better occupational health practices and resources in state-owned enterprises due to their greater regulatory oversight and resource availability (26). This unexpected finding may reflect evolving management practices in China’s private sector, where competitive market pressures increasingly incentivize enterprises to prioritize employee health as a critical factor for productivity and corporate reputation (36, 37). Interestingly, our stratified analysis indicated that this positive association between private ownership and OHL was particularly pronounced among low-income workers. Private enterprises might adopt more targeted and flexible health promotion strategies tailored to lower-income workers, who are often at greater occupational risk and have limited access to external health resources.
A key strength of this study is its focus on essential service workers—a population often overlooked in occupational health research—as well as its comprehensive examination of the influence of enterprise characteristics on occupational health literacy. Several limitations should be acknowledged. First, due to the cross-sectional nature of the data, the temporal sequence between enterprise characteristics and OHL cannot be established, and thus, causality cannot be inferred from the observed associations. Second, although participants were recruited from several key industries, the sample size was relatively small compared to the total population of essential service workers in Guangdong Province. However, using G*Power 3.1.9.7, a post-hoc power analysis revealed that our sample size of 2,640 participants provided adequate statistical power (85.05%) to detect an odds ratio of 1.28 (α = 0.05, two-tailed), suggesting our study was sufficiently powered to detect the hypothesized effects. Nevertheless, the relatively small sample size may still limit the representativeness of our findings, thereby restricting the generalizability of our conclusions to all essential service workers in the region. Finally, while our study examined several key enterprise characteristics, other potentially important organizational factors—such as leadership commitment to health, workplace social support, and specific occupational health management practices—were not assessed. These factors may mediate or moderate the relationships between enterprise characteristics and OHL and warrant investigation in future studies. To address these limitations, future research should consider recruiting larger and more representative samples across different geographic regions and occupational groups, thereby enhancing the external validity of the findings. Moreover, adopting longitudinal study designs would allow for a better understanding of the causal relationships between enterprise characteristics and OHL over time. In addition, mixed-methods approaches—combining quantitative surveys with in-depth qualitative interviews—could provide deeper insights into workers’ lived experiences and the organizational cultures that facilitate or hinder improvements in occupational health literacy (38). Furthermore, intervention trials are warranted to evaluate the effectiveness of innovative strategies, such as mobile-based learning, gamification, or AI-driven personalized health promotion, in diverse enterprise settings (39–41). Such studies would not only help identify best practices for promoting OHL among essential service workers, but also inform the development of scalable and sustainable interventions tailored to the unique needs of different worker populations.
Importantly, our findings underscore the need for differentiated policy approaches across various enterprise types to enhance occupational health literacy. For the express and food delivery sector, where OHL levels are significantly lower, policymakers should prioritize the establishment of mandatory occupational health training programs and standardized health protection protocols, particularly focusing on platform companies’ responsibilities toward gig workers (42, 43). The successful standardized occupational health management systems in the environmental sanitation sector could serve as a model for other industries, while the transportation sector requires specific policies to bridge the gap between knowledge and behavioral practices, such as strengthening work hours regulation. The demonstrated success of the “Occupational Health Support Initiative for Small, Medium and Micro-sized Enterprises” suggests the value of continuing and expanding such targeted support programs, while large enterprises should be encouraged to adopt more personalized and interactive approaches to health education (44). Given the positive outcomes observed in private enterprises, particularly among lower-income workers, policymakers should promote the sharing of best practices across ownership types, encouraging state-owned enterprises to incorporate more flexible and targeted approaches to health promotion. These targeted policy interventions, tailored to specific enterprise characteristics, could significantly improve occupational health literacy and ultimately enhance worker well-being across essential service sectors.
Conclusion
This surveillance study identified that enterprise characteristics are significantly associated with OHL among essential service workers in Guangdong Province, China. Employment in small/micro enterprises and private enterprises was associated with higher OHL levels, while working in the express and food delivery industry was associated with lower OHL levels. These findings highlight the need to consider enterprise characteristics in occupational health surveillance and when developing targeted interventions to improve OHL. Future longitudinal studies are needed to clarify the causal mechanisms of these associations and to evaluate the effectiveness of enterprise-targeted OHL interventions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Medical Ethics Committee of Guangdong Province Hospital for Occupational Disease Prevention and Treatment. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent was obtained from each participant.
Author contributions
SZ: Formal analysis, Funding acquisition, Methodology, Software, Writing – original draft, Writing – review & editing. HC: Data curation, Investigation, Writing – review & editing. JW: Investigation, Writing – review & editing. BX: Investigation, Writing – review & editing. XY: Investigation, Writing – review & editing. MH: Data curation, Writing – review & editing. MY: Conceptualization, Funding acquisition, Investigation, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Medical Scientific Research Foundation of Guangdong Province of China (A2024311) and Guangzhou Innovative Environment Plan Project (2060702).
Acknowledgments
We would like to express our sincere gratitude to all staff members and workers who contributed to the data collection process.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. National Institute for Occupational Health and Poison Control. Occupational Health Literacy for Chinese Workers – Basic Knowledge and Skills (2022 Edition) [Internet]. (2022). Available online at: https://niohp.chinacdc.cn/sndt/202203/t20220307_257538.htm (Accessed April 8, 2025).
2. World Health Organization. Shanghai declaration on promoting health in the 2030 agenda for sustainable development. Health Promot Int. (2017) 32:7–8. doi: 10.1093/heapro/daw103
3. Friedrich, J, Münch, AK, Thiel, A, Voelter-Mahlknecht, S, and Sudeck, G. Occupational health literacy scale (OHLS): development and validation of a domain-specific measuring instrument. Health Promot Int. (2023) 38:daac182. doi: 10.1093/heapro/daac182
4. Franke, F, Felfe, J, and Pundt, A. The impact of health-oriented leadership on follower health: development and test of a new instrument measuring health-promoting leadership. German J Hum Resour Manag. (2014) 28:139–61. doi: 10.1177/239700221402800108
5. Rauscher, KJ, and Myers, DJ. Occupational health literacy and work-related injury among U.S. adolescents. Int J Inj Control Saf Promot. (2014) 21:81–9. doi: 10.1080/17457300.2013.792288
6. Friedrich, J, Rupp, M, Feng, YS, and Sudeck, G. Occupational health literacy and work ability: a moderation analysis including interpersonal and organizational factors in healthy organizations. Front Public Health. (2024) 12:1243138. doi: 10.3389/fpubh.2024.1243138
7. Mõttus, R, Johnson, W, Murray, C, Wolf, MS, Starr, JM, and Deary, IJ. Towards understanding the links between health literacy and physical health. Health Psychol. (2014) 33:164–73. doi: 10.1037/a0031439
8. Suthakorn, W, Songkham, W, Tantranont, K, Srisuphan, W, Sakarinkhul, P, and Dhatsuwan, J. Scale development and validation to measure occupational health literacy among Thai informal workers. Saf Health Work. (2020) 11:526–32. doi: 10.1016/j.shaw.2020.06.003
9. Nutbeam, D. The evolving concept of health literacy. Soc Sci Med. (2008) 67:2072–8. doi: 10.1016/j.socscimed.2008.09.050
10. Tuomi, K, Vanhala, S, Nykyri, E, and Janhonen, M. Organizational practices, work demands and the well-being of employees: a follow-up study in the metal industry and retail trade. Occup Med. (2004) 54:115–21. doi: 10.1093/occmed/kqh005
11. World Bank W ILO WaterAid. Health, safety and dignity of sanitation workers. Washington, DC: World Bank (2019).
12. Wang, MH, Chen, YL, and Chiou, WK. Using the OVAKO working posture analysis system in cleaning occupations. Work. (2019) 64:613–21. doi: 10.3233/WOR-193022
13. National Bureau of Statistics of China. China statistical yearbook 2022 [Internet]. Available online at: https://www.stats.gov.cn/sj/ndsj/2022/indexch.htm (Accessed April 13, 2025).
14. Guangdong Statistics Bureau, Guangdong investigation team of the National Bureau of Statistics. Guangdong statistical yearbook 2022 [Internet]. Available online at: http://tjnj.gdstats.gov.cn:8080/tjnj/2022/
15. Lindert, L, Choi, KE, Pfaff, H, and Zeike, S. Health literacy at work – individual and organizational health literacy, health supporting leadership and employee wellbeing. BMC Health Serv Res. (2023) 23:736. doi: 10.1186/s12913-023-09766-0
16. Jakobsen, ME, Kjærgaard, A, Rudolf, EM, Palmqvist, J, and Ajslev, JZN. Enterprise characteristics were associated with adherence to a dialog-based inspection practice aimed at improving occupational safety and health in Denmark. Saf Health Work. (in press) (2025). doi: 10.1016/j.shaw.2025.05.002
17. Payne, J, Cluff, L, Lang, J, Matson-Koffman, D, and Morgan-Lopez, A. Elements of a workplace culture of health, perceived organizational support for health, and lifestyle risk. Am J Health Promot. (2018) 32:1555–67. doi: 10.1177/0890117118758235
18. Fabius, R, and Phares, S. Companies that promote a culture of health, safety, and wellbeing outperform in the marketplace. J Occup Environ Med. (2021) 63:456–61. doi: 10.1097/JOM.0000000000002153
19. Wang, J, Li, S, Sun, Y, and Sun, X. Occupational health literacy level and its influencing factors among key populations of secondary industry in China. Industr Health Occupat Dis. (2024) 50:97–102. doi: 10.13692/j.cnki.gywsyzyb.2024.02.001
20. Health literacy monitoring and statistical survey system for Chinese residents and key populations [Internet]. National Bureau of Statistics. (2022). Available online at: https://www.stats.gov.cn/fw/bmdcxmsp/bmzd/202302/t20230215_1907197.html (Accessed April 12, 2025).
21. Li, S, Sun, Y, and Sun, X. Introduction of the national technical plan for monitoring occupational health literacy of key population groups in 2022. China Occupat Med. (2023) 50:189–93. doi: 10.20001/j.issn.2095-2619.20230414
22. National Institute of Occupational Health and Poison Control, Chinese Center for Disease Control and Prevention. Notice on the Issuance of “Standards for calculating occupational health literacy levels among key populations (2022)”. Beijing: Chinese Center for Disease Control and Prevention. Report No.: NIOHP Letter [2023] No. 5. [Official correspondence] (2023).
23. National Bureau of Statistics of China. Standards for the classification of large, medium, small, and Micro-sized Enterprises in Statistics (2017). Available online at: https://www.stats.gov.cn/xxgk/tjbz/gjtjbz/202008/t20200811_1782335.html (Accessed April 13, 2025).
24. National Bureau of Statistics of China, State Administration for Industry and Commerce of the People’s Republic of China. Regulations on the classification of Enterprise registration types [Internet]. Available online at: https://www.gov.cn/zwgk/2011-11/17/content_1995548.htm (Accessed April 13, 2025).
25. Güner, MD, and Ekmekci, PE. Health literacy level of casting factory workers and its relationship with occupational health and safety training. Workplace Health Saf. (2019) 67:452–60. doi: 10.1177/2165079919843306
26. Sun, Y, Sun, X, Wan, X, Yu, S, and Li, S. Occupational health literacy level and its influencing factors among key populations in China in 2022. China Occupat Med. (2023) 50:241–7. doi: 10.20001/j.issn.2095-2619.20230601
27. Khatri, S, Shah, GK, Bhandari, P, Koirala, S, Neupane, K, Bhattarai, N, et al. Musculoskeletal disorders and other occupational health outcomes among sanitation workers in Nepal: a community based cross-sectional survey exploring the risk factors, knowledge, and practices. BMC Public Health. (2025) 25:1–14. doi: 10.1186/s12889-025-22282-6
28. Tang, W, Chen, J, Wang, S, Jiang, X, Lu, Y, Wu, S, et al. Debt, sleep deprivation and psychological distress among online ride-hailing drivers: evidence from China. Gen Psychiatr. (2024) 37:e101332. doi: 10.1136/gpsych-2023-101332
29. Anwar, MA, and Graham, M. Between a rock and a hard place: freedom, flexibility, precarity and vulnerability in the gig economy in Africa. Compet Change. (2020) 25:237–58. doi: 10.1177/1024529420914473
30. Bajwa, U, Gastaldo, D, Di Ruggiero, E, and Knorr, L. The health of workers in the global gig economy. Glob Health. (2018) 14:124. doi: 10.1186/s12992-018-0444-8
31. Mbare, B. Psychosocial work environment and mental wellbeing of food delivery platform workers in Helsinki, Finland: a qualitative study. Int J Qual Stud Health Well-being. (2023) 18:2173336. doi: 10.1080/17482631.2023.2173336
32. Liu, B, Guo, Y, and Fu, Y. The impact of occupational stigma on gig workers’ workplace well-being: a cross-sectional study based on the platform-based food-delivery sector in China. J Occup Environ Med. (2022) 64:e527–34. doi: 10.1097/JOM.0000000000002604
33. Vinberg, S, Torsdatter Markussen, L, and Landstad, BJ. Cooperation between occupational health services and small-scale Enterprises in Norway and Sweden: a provider perspective. Workplace Health Saf. (2017) 65:355–64. doi: 10.1177/2165079916668527
34. Wang, Q, Mei, Q, Liu, S, and Zhang, J. Analysis of managing safety in small enterprises: dual-effects of employee prosocial safety behavior and government inspection. Biomed Res Int. (2018) 2018:1–12. doi: 10.1155/2018/6482507
35. Chen, W, Ren, H, Wang, N, Xiong, Y, and Xu, F. The relationship between socioeconomic position and health literacy among urban and rural adults in regional China. BMC Public Health. (2021) 21:527. doi: 10.1186/s12889-021-10600-7
36. Chen, Z. The influence mechanism of Occupational Health risk attribution on work performance: the chain mediating effect of Positive Emotion and work engagement [internet] [master thesis]. China University of Mining and Technology; (2021)
37. Sato, Y, Iwakiri, K, Matsuo, T, and Sasaki, T. Impact of health literacy on health practices in the working life of young Japanese nurses and care workers. Ind Health. (2021) 59:171–9. doi: 10.2486/indhealth.2020-0218
38. Zipfel, N, de Wit, M, Snippen, NC, Bosma, AR, Hulshof, CTJ, de Boer, AGEM, et al. Improving person-centered occupational health care for workers with chronic health conditions: a feasibility study. BMC Med Educ. (2023) 23:224. doi: 10.1186/s12909-023-04141-3
39. Shah, IA, and Mishra, S. Artificial intelligence in advancing occupational health and safety: an encapsulation of developments. J Occup Health. (2024) 66:17. doi: 10.1093/joccuh/uiad017
40. Ebert, DD, Heber, E, Berking, M, Riper, H, Cuijpers, P, Funk, B, et al. Self-guided internet-based and mobile-based stress management for employees: results of a randomised controlled trial. Occup Environ Med. (2016) 73:315–23. doi: 10.1136/oemed-2015-103269
41. Zhang, C, van Gorp, P, Derksen, M, Nuijten, R, Ijsselsteijn, WA, Zanutto, A, et al. Promoting occupational health through gamification and e-coaching: a 5-month user engagement study. Int J Environ Res Public Health. (2021) 18:2823. doi: 10.3390/ijerph18062823
42. Dong, J, Zhang, G, and Wu, L. Life against algorithmic management: a study on burnout and its influencing factors among food delivery riders. Front Public Health. (2025) 13:1531541. doi: 10.3389/fpubh.2025.1531541
43. Nilsen, M, and Kongsvik, T. Health, safety, and well-being in platform-mediated work – a job demands and resources perspective. Saf Sci. (2023) 163:106130
Keywords: occupational health literacy, essential service workers, enterprise characteristics, cross-sectional study, tertiary industry
Citation: Zhou S, Chen H, Wu J, Xia B, Yu X, Huang M and Yang M (2025) Enterprise characteristics and occupational health literacy among essential service workers in Guangdong Province, China: a cross-sectional study. Front. Public Health. 13:1632185. doi: 10.3389/fpubh.2025.1632185
Edited by:
Hana Brborović, University of Zagreb, CroatiaReviewed by:
Yuke Tien Fong, Singapore General Hospital, SingaporeLa Ode Reskiaddin, University of Jambi, Indonesia
Copyright © 2025 Zhou, Chen, Wu, Xia, Yu, Huang and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Yang, MTM2OTk3MDQxMjFAMTYzLmNvbQ==