 Camille Favola1*
Camille Favola1* Fabienne d'Arripe-Longueville1
Fabienne d'Arripe-Longueville1 Lou-Anne Piroird1
Lou-Anne Piroird1 Meggy Hayotte1
Meggy Hayotte1 Stéphanie Mériaux-Scoffier1,2,3
Stéphanie Mériaux-Scoffier1,2,3- 1Université Côte-d'Azur, LAMHESS (UPR 6312), Nice, France
- 2Institut Universitaire de France, Nice, France
- 3Centre de Recherche de l'Institut Universitaire en Santé Mentale de Montréal, Université du Québec à Trois-Rivières, Montréal, QC, Canada
Introduction: Due to the trauma they have experienced, women who are survivors of violence struggle to engage in regular physical activity despite its numerous benefits. Identifying the factors that facilitate or hinder engagement in physical activity within this population is therefore essential. However, no valid tool currently exists specifically for this purpose. This study, based on the concept of decisional balance drawn from the transtheoretical model of behavior change, aimed to develop and validate the Decisional Balance Scale for Physical Activity in Female Survivors of Violence (DBSPA-FSV).
Methods: Three hundred one volunteers participated in three complementary steps which followed established validation procedures. In step 1, a preliminary version of the items was developed based on the existing literature. In step 2, the dimensionality and convergent validity of the scale were examined. In step 3, the reliability of the scale was tested.
Results: In step 1, a preliminary version of 32 items was developed. The scale was refined to 22 items, grouped into two factors (facilitators and barriers) and six sub-dimensions (physical, psychological, and socio-environmental). In step 2, bi-factor confirmatory models with a global construct and six or two correlated factors demonstrated satisfactory fit indexes. Convergent validity was confirmed by significant correlations between DBSPA- FSV constructs and the concept of self-determined motivation in the expected directions. In step 3, the internal and test-retest reliability of the scale were confirmed.
Discussion: The DBSPA-FSV scale exhibits satisfactory psychometric properties and will contribute to research on the engagement in physical activity of women survivors of violence.
1 Introduction
Violence against women exists along a continuum, spanning psychological abuse, physical aggression, and sexual violence (1). It represents a critical global public health concern. According to the United Nations, violence against women includes all forms of gender-based violence that cause physical, sexual, or psychological harm or suffering, encompassing threats, coercion, or arbitrary deprivation of liberty, whether occurring in public or private settings (2). This is the definition of violence used in this study. Globally, ~736 million women—nearly one in three—have experienced physical and/or sexual violence by an intimate partner, non-partner, or both, at least once in their lifetime (3). Despite this staggering prevalence, underreporting remains widespread. A 2021 World Health Organization report revealed that fewer than 40% of women who experience violence seek any form of support, and of those, <10% contact the police (4). Silence among survivors is often driven by fear, stigma, and a deep-seated mistrust in judicial systems (4). In some national studies, fewer than one in 10 rape complaints lead to a conviction. These statistics highlight a disturbing reality: official reports capture only a fraction of the true extent of gender-based violence (5).
Violence can have profound and sometimes delayed effects on physical and mental health, particularly in the form of psychological trauma. Childhood violence, in particular, has been shown to lead to long-term consequences that may persist regardless of any violence experienced in adulthood (6). The more physical violence individuals endure, the more their quality of life deteriorates, affecting both their health and social relationships (7). These effects extend beyond childhood, as survivors of sexual violence frequently report physical symptoms such as migraines, fatigue, eating disorders, and various forms of chronic pain (7). The long-term psychological and physical consequences of violence (particularly when experienced in childhood) highlight the need for holistic responses. Non-pharmacological approaches such as physical activity (PA) have emerged as promising avenues for support and recovery. Several studies have highlighted the positive impact of PA on the physical and mental health of survivors. A meta-analysis showed that PA programs significantly reduce post-traumatic stress disorder (PTSD) symptoms compared to control groups (8). Other authors have found that PA not only alleviates PTSD symptoms but is especially effective for individuals resistant to conventional treatments, reducing anxiety, depression, sleep disorders, and cardiovascular problems often linked to PTSD (9). Moro (10) demonstrated that PA reduces the risk factors for developing metabolic diseases, which are exacerbated by a sedentary lifestyle, and advocated for its use as a first-line treatment. Participation in PA programs can reduce the risk of chronic diseases, lower mortality, and improve mental health, especially among individuals with PTSD, as confirmed by a systematic review (11). The World Health Organization has also emphasized the broad health consequences of violence, including chronic pain and general health deterioration. In this context, tailored physical activity could offer a meaningful avenue for improving both physical and mental wellbeing (12). More specifically, high-intensity exercises appeared to be more effective in reducing PTSD symptoms than moderate-intensity exercises (13). Furthermore, Basile et al. (14) confirmed that PA effectively combats mild to moderate depression, alleviates major depression symptoms, and lowers mortality rates. Despite these benefits, women who have experienced violence often face significant barriers to engaging in PA, leading to increased sedentary behaviors (15, 16). Understanding and addressing these barriers is crucial to promoting PA engagement in this population.
Several studies have highlighted the positive impact of physical activity (PA) on the physical health of survivors (17). Psychological trauma—defined as “exposure to actual or threatened death, serious injury, or sexual violence” (DSM-5-TR) (18) can lead to post-traumatic stress disorder (PTSD), one of the most recognized and debilitating manifestations of trauma. PTSD symptoms are grouped into five main clusters: intrusive memories and flashbacks, avoidance behaviors, negative alterations in cognition and mood, heightened arousal and reactivity (including sleep disturbances and irritability), and dissociative symptoms such as depersonalization or derealization. Given the complexity and persistence of these symptoms, PTSD represents a major public health concern, affecting ~5%−12% of the general population, with significantly higher prevalence among survivors of violence (19). In this context, physical activity has emerged as a promising complementary intervention. The beneficial effects of physical activity (PA) on mental health are supported by several mechanisms. Neurobiologically, PA helps reduce stress reactivity, improve mood regulation, and enhance sleep quality (8). Psychosocially, it contributes to strengthening perceived self-efficacy, reducing feelings of isolation, and providing a constructive outlet for stress management (17). A meta-analysis has shown that PA programs significantly reduce PTSD symptoms compared to control groups (8). Similarly, other studies have found that PA is particularly effective for individuals resistant to conventional treatments. Research has demonstrated that PA contributes to reducing anxiety, depression, sleep disturbances, and cardiovascular issues often associated with PTSD (9). Physical activity (PA) reduces risk factors for metabolic diseases linked to sedentary lifestyles and is recognized as a first-line intervention and potential alternative to medication (10). Evidence also shows that PA lowers mortality rates, decreases the risk of chronic conditions, and enhances mental health (11). The World Health Organization emphasizes the wide-ranging health consequences of violence, including chronic pain and general health decline, highlighting the value of tailored PA for improving both physical and psychological outcomes. High-intensity exercise appears particularly effective in reducing PTSD symptoms, and PA more broadly has been shown to alleviate depression and lower mortality risk (14). Yet, women who have experienced violence often face significant barriers to engaging in PA, resulting in greater sedentary behavior (15, 16). Addressing these barriers is crucial to promoting recovery in this vulnerable population.
Barriers to engaging in PA can be psychological, social, environmental, or physical. Among these, psychological barriers play a significant role in limiting PA participation of women survivors of violence. These include: (a) fear, often stemming from past experiences (19); (b) psychological trauma, which can negatively affect their ability to engage in new or demanding activities (20); (c) loss of self-confidence and social withdrawal, which is an obstacle to their participation in group activities (19). Some survivors also experience physiological arousal during exercise—such as increased heart rate or breathing—as reminiscent of traumatic experiences, which they perceive as threatening or overwhelming. This form of hyperawareness of bodily sensations can lead to avoidance of physical activity altogether, particularly among survivors of sexual violence (21). Social and physical environments can also be seen as major obstacles: social isolation, which reduces opportunities to participate in structured or group activities, and environments perceived as a threat to their physical and emotional wellbeing (15). Finally, some women perceive PA as a threat to their physical integrity and consider it dangerous, which reinforces their reluctance to participate (15). To overcome these obstacles, it is essential to put in place supportive conditions or strategies tailored to the needs of women who have experienced violence, in order to encourage their engagement in physical activity. These women must feel comfortable in their social environment and establish meaningful connections with other participants (20). Intervention teams should foster a culture of trust, respect, and confidentiality to ensure a safe space for participants (17). In this perspective, recent studies highlight the importance of encouraging these women to exercise and improve their overall wellbeing by offering interventions that take into account the trauma they have experienced (17). Additionally, studies point out that it is essential for them to experience the benefits of exercise, both physically and psychologically, to maintain their engagement in PA (22). Specific PA programs for women survivors of violence are therefore highly justified. However, no existing study has provided a theoretical framework to explain behavior change or offered a validated tool to quantitatively measure PA engagement within this specific population (16). It is therefore essential to develop decision balance questionnaires based on strong theoretical foundations and tailored to the unique needs of this population to measure what encourages or hinders their participation in PA. Decision balance questionnaires, which assess the perceived pros and cons of engaging in a behavior such as physical activity, provide insight into the motivational processes underlying behavior change (23).
One particularly useful framework for explaining health behavior change, including physical activity (PA), is the Transtheoretical Model of Behavior Change (24, 25). This model is especially relevant in this context as it conceptualizes the change not as a single event but as a dynamic, staged process. This perspective is particularly appropriate for survivors of violence, whose engagement in PA may be shaped by fluctuating psychological readiness as well as unique barriers and facilitators. Unlike other models that focus on static determinants of behavior, the model highlights individual readiness to change and supports the tailoring of interventions to specific needs. The model comprises five stages—precontemplation, contemplation, preparation, action, and maintenance—with progression occurring in a non-linear manner depending on personal experiences. Two central mechanisms underpinning the model are self-efficacy, which reflects an individual's confidence in their capacity to achieve change, and decisional balance, which involves weighing the perceived benefits and drawbacks of adopting a behavior.
The concept of decisional balance, introduced in 1977 by Janis and Mann (23) and later integrated into the Transtheoretical Model of Behavior Change (24, 25), refers to an individual's cognitive evaluation of the perceived benefits (pros) and perceived costs (cons) of adopting a specific behavior. This framework helps to understand the motivational processes that influence behavior change and resistance. In the context of physical activity (PA), decisional balance provides a structured way to assess the facilitators and barriers that individuals weigh when deciding whether to engage in PA. In 1992, Marcus et al. (26) developed an English-language version of the decisional balance scale for physical activity (PA), which evaluates these facilitators and barriers. Eeckhout et al. (27) later translated this scale into French for use in the general population. However this version does not account for the psychological dimensions specific to women who have experienced violence (e.g., no emphasis on trust, security and confidentiality was needed) (27). Other decisional balance tools have been developed for specific contexts, such as the workplace (28) or for populations with particular health conditions like cystic fibrosis (29) or arthritis (30). However, these tools were designed for specific groups with different facilitators and barriers with respect to PA than those perceived by women survivors of violence. For example, the decisional balance developed (29) in the context of cystic fibrosis includes items related to this genetic disease that affects the respiratory system (e.g., “good physical condition supports transplant success”). Such items are not applicable to our population. As a result, existing decisional balance tools are either too generic and do not take into account the unique needs of women survivors of violence, or, on the contrary, are too specific and therefore not applicable in the specific context of violence. In short, no tool is currently available to measure the facilitators and barriers for engaging in PA perceived by women survivor of violence, considering the psychological and physical trauma they have experienced.
The aim of this study was to develop and validate a Decisional Balance Scale for Physical Activity in Female Survivors of Violence (DBSPA-FSV) in a French sample. Three complementary steps were followed in accordance with recommendations for scale development and validation (31, 32). The items were developed by consensus by a group of experts, were based on the literature to ensure the validity of the scale content, and were subjected to additional analyses to check clarity (Step 1). Dimensionality and convergent validity of the DBSPA-FSV were examined through confirmatory factor analyses (CFA) and Pearson's correlations (Step 2). The convergent validity will be examined by investigating relationship between DBSPA-FSV with self-determination. Previous research indicates that individuals in early stages of readiness tend to be less self-determined in their physical activity behavior than those in more advanced stages (33). In the specific context of survivors of violence, a correlation between perceived barriers and lower motivation has also been reported (17). Specifically, we hypothesized that higher perceived facilitators (vs. barriers) will be associated with more self-determined forms of motivation. Finally, reliability of the scale was examined by measuring its internal consistency and its consistency across time (Step 3). For all steps, the protocol was approved by the local ethics committee for non-interventional research (authorization no. 2023-104) of University XXX. All participants were adults and individuals under 18 were excluded. Informed consent was obtained online via an information page and a checkbox before accessing the questionnaire. The questionnaires were administered online using LimeSurvey software version 3.17.3+ (LimeSurvey, CE), which guaranteed free participation, anonymity and confidentiality of the answers, and removed any possibility of missing data. No incentive for participation was provided. Statistical analyses were carried out using IBM SPSS and AMOS version 27 software (IBM Corp.). Finally, the study was open to all women, and no mention of violence was made in the recruitment materials. Whether women had experienced violence or not was assessed through self-report as part of the questionnaire, and all participants—both survivors and non-exposed women—were included in the analyses. This strategy preserved participant anonymity, avoided direct solicitation, and ensured a non-discriminatory recruitment process.
2 Step 1: development of a preliminary version of the decisional balance scale for physical activity in female survivors of violence (DBSPA-FSV scale)
The aim of this step of the study was to develop a preliminary version of the scale, by defining items that reflect the barriers and facilitators for engaging in PA specific to female survivors of violence based on the existing literature.
2.1 Method
2.1.1 Development of the DBSPA-FSV scale
A committee of seven experts was set up, including: (a) four researchers and a master's degree student specialized in the fields of sport science, health psychology, and sport psychology, and (b) two representatives of associations working notably with survivors of violence. This committee developed items based on existing scales of decisional balance (28–30), on the studies by Pebole et al. (7, 15, 17) on the PA participation of women survivors of violence, and on a qualitative study of the barriers and facilitators for engaging in PA reported by women survivors of violence (22). Physical, psychological, social and environmental barriers and facilitators were identified. The committee created items for the following six subscales: (a) physical barriers, (b) psychological barriers, (c) socio-environmental barriers, (d) physical facilitators, (e) psychological facilitators, and (f) socio-environmental facilitators. These subscales could be grouped into two general subscales of barriers or facilitators. In line with the usual recommendations to have at least three items per factor to avoid estimation problems (29), the committee initially chose to develop four items per dimension. Item wording guidelines (34) and the principle of over-inclusiveness (31) were closely followed. Initially, the scale included 32 items (16 for facilitators and 16 for barriers). After several meetings, the experts' committee decided to remove eleven items (five facilitators and six barriers) which were redundant, lacked clarity or were ambiguous. At the end of this item development process, a 22-item scale was obtained, which included 11 facilitators and 11 barriers.
2.1.2 Participants and procedure
Two analyses were conducted to assess the clarity of the scale. In the first step, a sample of 20 women aged 18–72 years (Mage = 32.05; SD = 15.16) from the south of France, with educational levels ranging from middle school diploma to PhD, rated the clarity of the 22-item DBSPA-FSV using a six-point Likert scale (one = not clear at all to six = completely clear). Participants were also invited to suggest alternative wording for any items they found unclear. Items with an average rating below 4.50 were revised accordingly. In the second step, a separate sample of 25 women (Mage = 38.96; SD = 17.87) evaluated the clarity of the revised version of the 22-item DBSPA-FSV (see Table 1). The two subsamples were recruited independently: the first group through convenience sampling within the researchers' networks, without criteria related to exposure to violence to ensure anonymity and avoid distress; and the second group from a larger pool of participants in the main survey. Both subsamples were independent and did not overlap with the main sample described in Section 3.1.1.

Table 1. The 22-item version of the decisional balance scale for physical activity in female survivors of violence (DBSPA-FSV).
2.2 Results and discussion
An initial clarity analysis revealed rather satisfactory scores, with all items scoring at least 4.15/6 (M = 5.32; SD = 0.39). In response to the participants' recommendations, the items rated below 4.5 were rephrased as follows: (a) “I go to the place where I exercise accompanied” was replaced by “I go to the place where I exercise with someone I trust”; (b) “those close to me support me in my practice” were reworded as follows: “I have someone (a partner, a friend, other) who encourages/motivates me to exercise”; and (c) “I've changed my living environment” was replaced by “I live in a reassuring environment.”
The second clarity analysis resulted in a score of at least 4.48/6 for all items (M = 5.41, SD = 0.27). Therefore, the clarity of all items was considered satisfactory.
3 Step 2: dimensionality and convergent validity of the DBSPA-FSV
The second step of the study was to analyze the dimensionality of the DBSPA-FSV using a confirmatory factor analysis (CFA), and to examine its convergent validity by investigating its correlations with theoretically related constructs such as the different types of motivation for engaging in PA (35).
3.1 Method
3.1.1 Participants and procedure
A total sample of 301 women (Mage = 19.76; SD = 5.80) survivors of violence (n = 136) and women not exposed to violence (n = 165), took part in the study. This sample was not limited to students but included participants with varied socio-demographic and educational profiles. All participants were included in the analyses. As a reminder, violence in this study is defined as any behavior along the continuum of violence, including psychological abuse, physical aggression, and sexual violence (36). Participants were recruited through social media and within university settings, via online posts and posters displayed in student-accessible areas. Additionally, brief presentations were made in large lecture halls to inform students about the study and reach a broader audience. Participants were asked to provide general information (e.g., demographic data), to complete the DBSPA-FSV scale, and take a survey that assesses the different types of motivation for engaging in PA. Participants' characteristics are presented in Table 2.
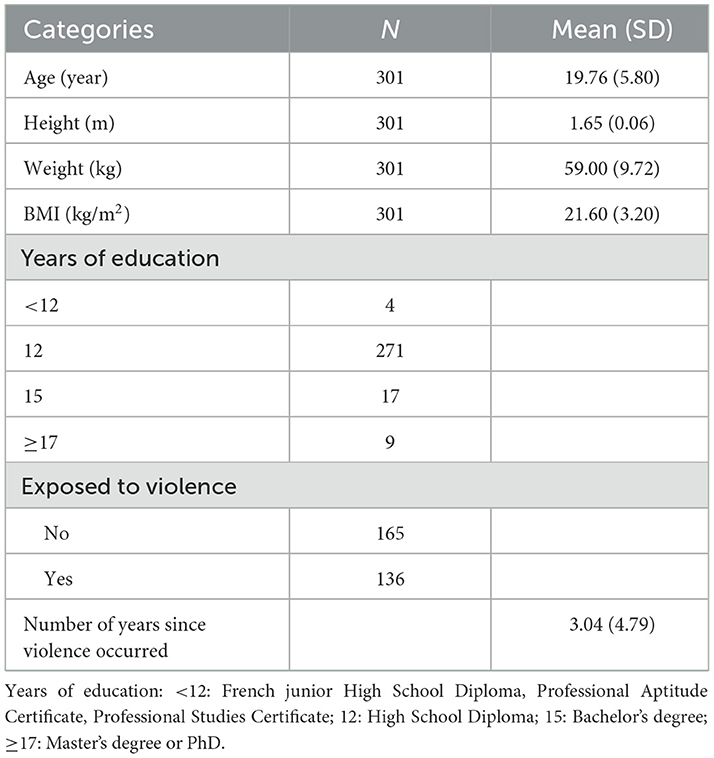
Table 2. Characteristics of the participants involved in checking the dimensionality and the convergent validity of the DBSPA-FSV scale (N = 301).
3.1.2 Measures
3.1.2.1 Demographic data
Information about gender, age, height, weight, highest degree and marital status were gathered. In addition, the presence or absence of violence experienced was measured (“Have you experienced violence in your life?”) after a description of the continuum of violence. In the event of violence, respondents were asked to provide the number of years since violence occurred.
3.1.2.2 DBSPA-FSV scale
The 22-item scale developed in the previous step was used. Each item was rated on a six-point Likert scale (strongly disagree: one, to strongly agree: six).
3.1.2.3 Motivation for physical activity (EMAPS)
Motivation for engaging in PA was assessed using the scale of motivation toward PA in a health context (37). This questionnaire includes 18 items rated on a Likert scale ranging from 1 to 7 (does not apply to me at all: 1, to perfectly applies to me: 7). The 18 items are classified into six types of motivation along a continuum (i.e., amotivation: lack of intention to act; external regulation: behavior driven by external rewards or pressures; introjected regulation: behavior motivated by internal pressures such as guilt; identified regulation: behavior recognized as personally important; integrated regulation: behavior fully aligned with one's values, all representing forms of extrinsic motivation; and intrinsic motivation: behavior undertaken for inherent enjoyment and interest). These can be grouped into self-determined forms (identified, integrated, and intrinsic) and non-self-determined forms (external, introjected, and amotivation). This classification makes it possible to distinguish motivations reflecting autonomous engagement in PA from those driven by external or internal pressures. Cronbach's alphas were above 0.79 and therefore considered fairly high (38).
3.1.3 Data analysis
3.1.3.1 Confirmatory factor analysis
As the development of the DBSPA-FSV scale was based on the literature, the number of factors were defined a priori and two series of hypothesized models were defined according to the methodology of Myers et al. (39). First a unidimensional model, representing a global view of the decisional factors (barriers and facilitators) for engaging in PA was tested. Then, a first series of models were examined: (a) a two-factor correlated model (barriers; facilitators); and (b) a bi-factor model with a general factor (decisional balance) and two correlated factors (barriers; facilitators). A second series of models were then tested: (a) a six-factor model correlated with each level of PA barriers and facilitators; and (b) a bi-factor model with a general factor (decisional balance) and six correlated factors (each level of barriers and facilitators). The following indexes and their criteria were reported and evaluated (31): (a) Chi-square value (χ2) and Chi-square statistic divided by degrees of freedom (df), with values below 3.00 considered acceptable; (b) root-mean-square error of approximation (RMSEA), for which values close to or below 0.08 were considered acceptable; (c) comparative fit index (CFI) and Tucker-Lewis index (TLI), for which values close to or above 0.90 were considered acceptable; and (d) the Akaike Information Criterion (AIC) and expected cross validation index (ECVI), in which lower values were considered better.
3.1.3.2 Convergent validity
Bivariate Pearson correlations were used. Correlations were interpreted following Cohen's guidelines (40): (a) < 0.10: trivial; (b) 0.10–0.30: small; (c) 0.30–0.50: moderate; (d) 0.50–0.70: large; (e) 0.70–0.90: very large, and (f) >0.90: almost perfect. We computed Pearson correlations for the eight factors of the DBSPA-FSV scale (i.e., global factor of barriers, physical barriers, psychological barriers, socio-environmental barriers, global factor of facilitators, physical facilitators, psychological facilitators, socio-environmental facilitators) and the six types of motivation for PA. Therefore, we expected positive correlations between facilitators and self-determined forms of motivation for PA, and negative correlations between facilitators and non-self-determined forms of motivation for PA. Conversely, we expected negative correlations between barriers and self-determined forms of motivation for PA, and positive correlations between barriers and non-self-determined forms of motivation for engaging in PA.
3.2 Results
Skewness and kurtosis were assessed for the eight dimensions of the DBSPA-FSV, and the six types of motivation for PA. Skewness ranged from −1.69 to 1.61, and kurtosis ranged from – 0.98 to 4.26. Therefore, the normality of data was assumed (33). Subsequent factor analyses employed robust estimators that tolerate moderate departures from normality.
3.2.1 Confirmatory factor analysis
Two series of models were tested with the 22-item version of the DBSPA-FSV scale (N = 301). We examined five models: (a) a unidimensional model; (b) a two-factor correlated model; (c) a bi-factor model with a general factor and two correlated factors; (d) a six-factor correlated model; and (e) a bi-factor model with a general factor and six correlated factors. Fit indexes of the tested models are presented in Table 3. The unidimensional model did not present satisfactory fit indexes. The two-factor and the six-factor models presented better fit indexes but still not sufficient to be acceptable. The bi-factor models had the best fit indexes but still did not achieve sufficient fit indexes. Therefore, the modification indexes identified by AMOS were examined, and correlations between the errors of the items PsyB2 and PsyB4, and between the errors of the items SEB1 and SEB4 were added to the models. This addition of correlations between errors, recommended by Byrne (41) was applied to the five models and resulted in acceptable fit indexes for the bi-factor models (see Table 3, and Figures 1, 2). Since the choice of model was based on theoretical reasoning, we chose to keep the two bifactorial models because they presented satisfactory to good indexes, provided the best goodness-of-fit indexes as well as the lowest ECVI and AIC indexes, and they were complementary. This complementarity lies in the fact that various dimensions of the scale can be explored according to the six barriers and facilitators at each level (physical, psychological, and socio-environmental) but also according to the two global dimensions (barriers and facilitators).
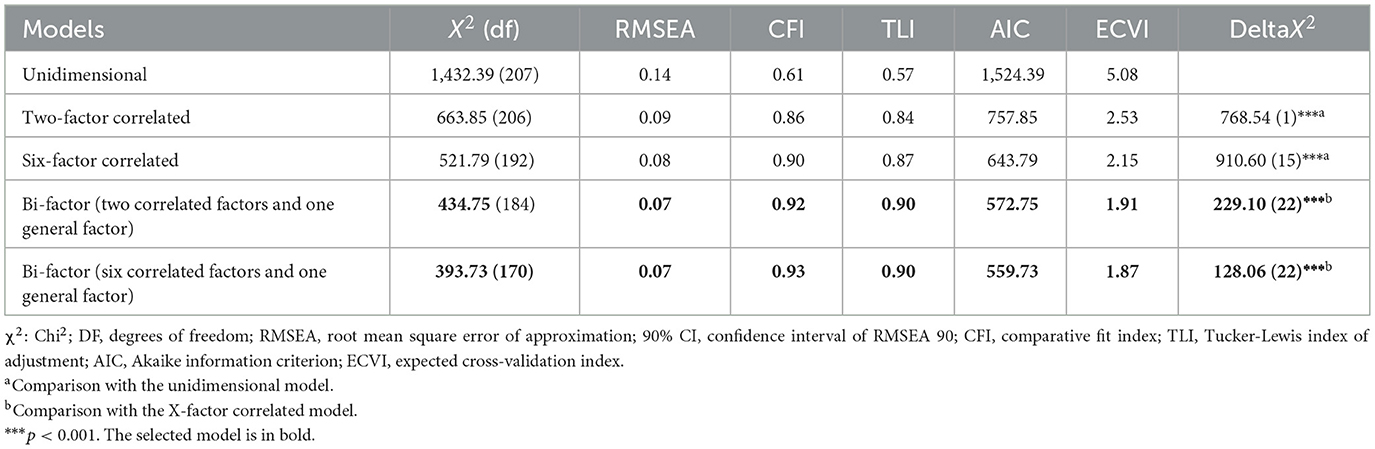
Table 3. Fit indexes of the different models examined by the confirmatory factor analysis (N = 301).
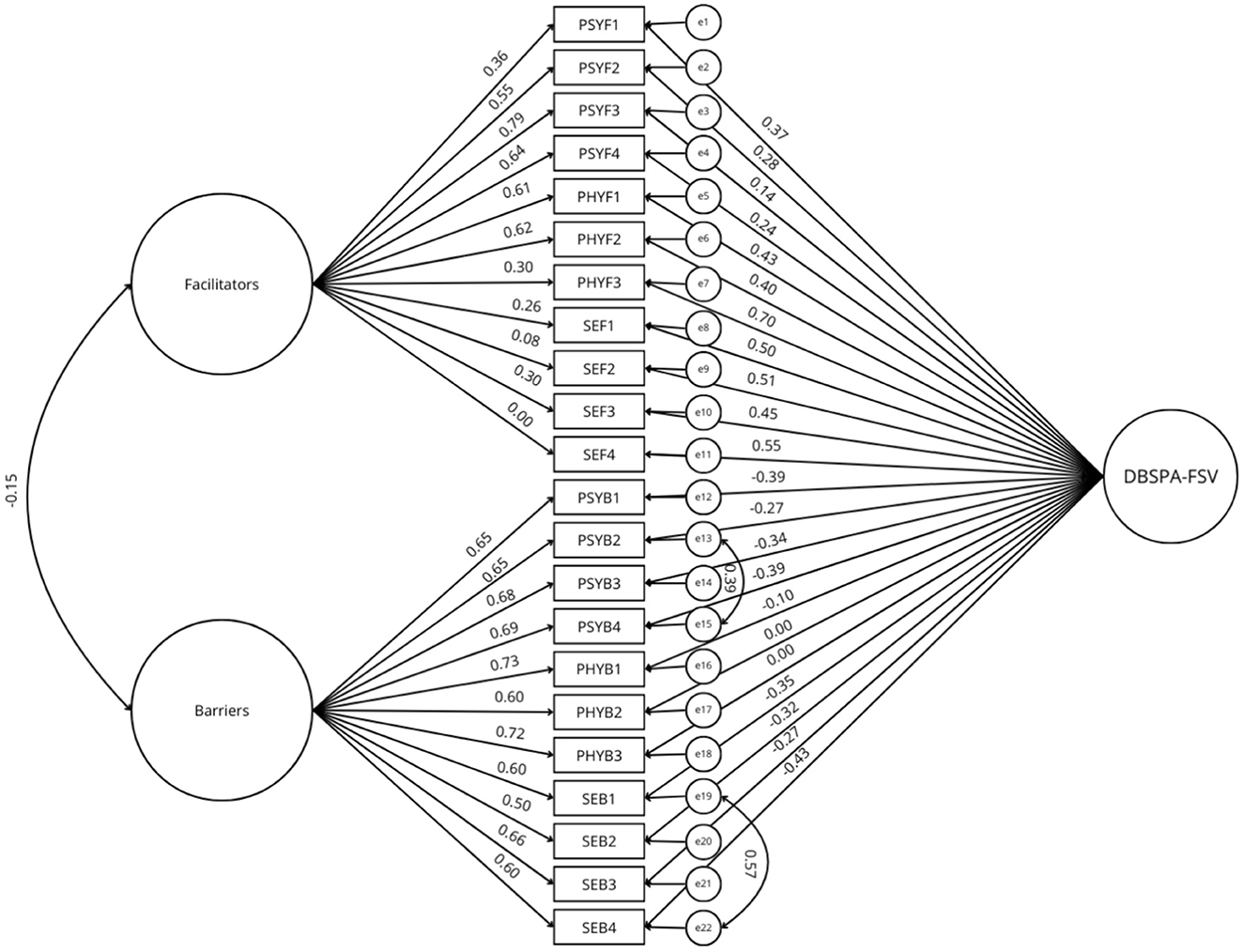
Figure 1. Estimation coefficients and standardized measurement errors of the bi-factor model with one general factor and two correlated factors. PSYF, psychological facilitator; PHYF, physical facilitator; SEF, socio-environmental facilitator; PSYB, psychological barrier; PHYB, physical barrier; SEB, socio-environmental barrier; DBSPA-FSV, decisional balance scale for physical activity in female survivors of violence.
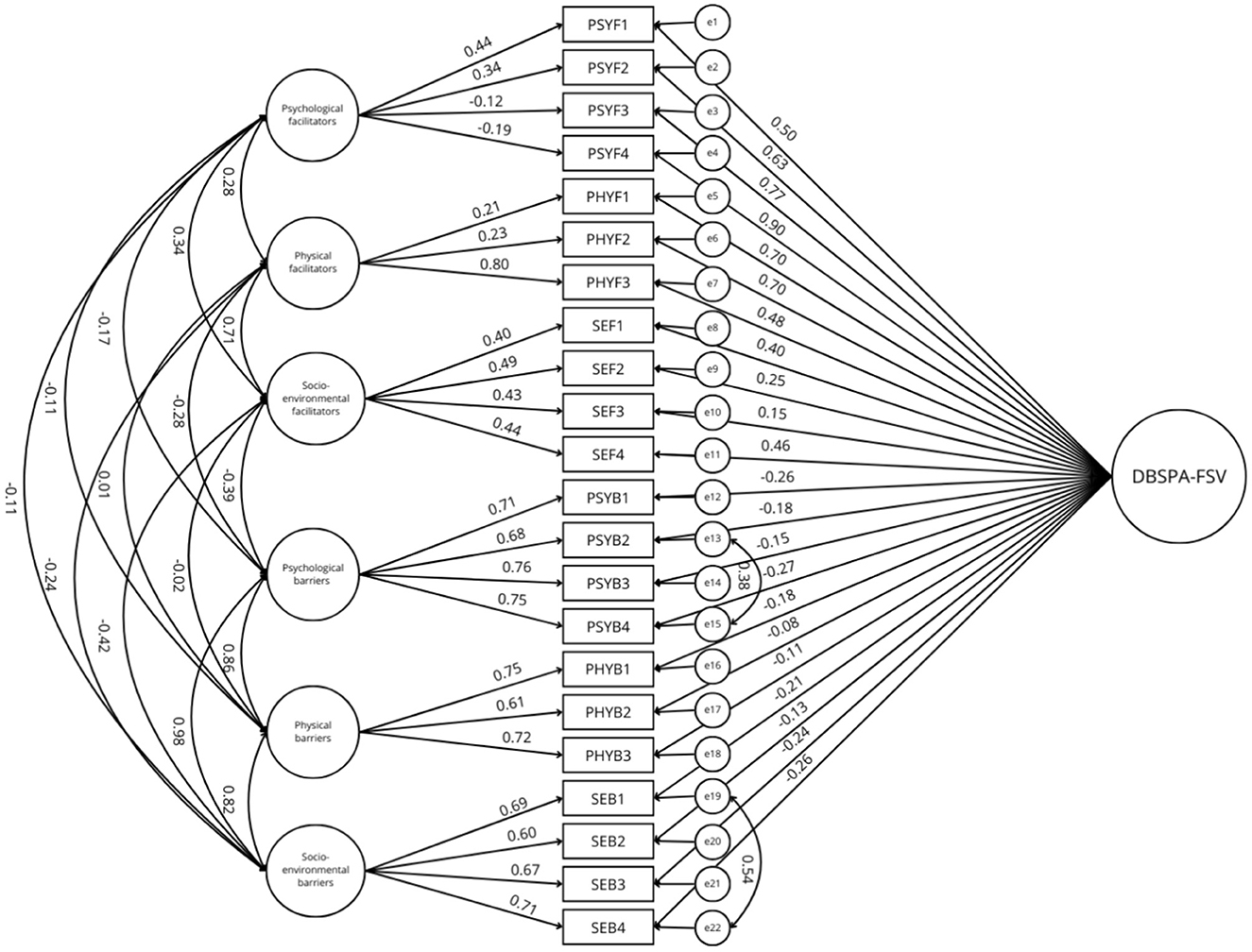
Figure 2. Estimation coefficients and standardized measurement errors of the bi-factor model with one general factor and six correlated factors. PSYF, psychological facilitator; PHYF, physical facilitator; SEF, socio-environmental facilitator; PSYB, psychological barrier; PHYB, physical barrier; SEB, socio-environmental barrier; DBSPA-FSV, decisional balance scale for physical activity in female survivors of violence.
3.2.2 Convergent validity
Pearson's correlations between the barriers and facilitators for engaging in PA and the different types of motivation for PA are presented in Table 4. The general and specific dimensions of facilitators were positively correlated with intrinsic, integrated, identified, and introjected types of motivations for PA (p < 0.01). They also were negatively correlated with amotivation (p < 0.01). Only psychological barriers showed a small significant correlation with external regulation of motivation for PA (p < 0.05). The general and specific dimensions of barriers were negatively correlated with intrinsic, integrated, identified, and introjected regulations of motivation for PA (p < 0.05), except physical barriers which showed no correlation with identified and introjected regulations of motivation for PA. All barriers were also positively correlated with amotivation and external regulation of motivation (p < 0.05).
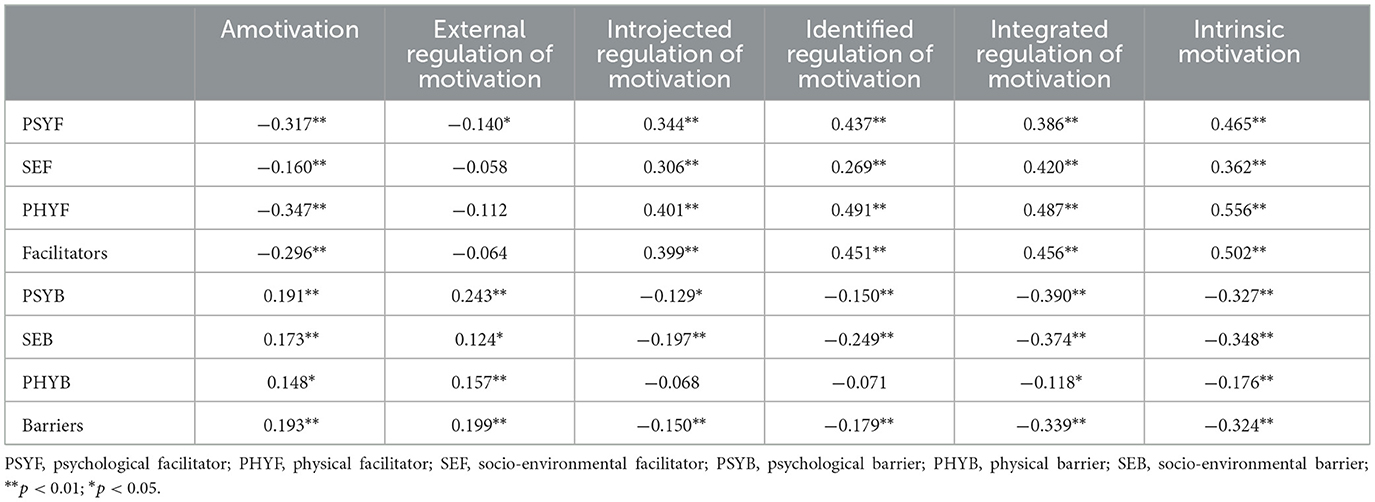
Table 4. Convergent validity results based on Pearson correlations (N = 301).
3.3 Discussion
The confirmatory factor analysis (CFA) showed that the bifactor models with six correlated factors and with two correlated factors both presented the best fit indexes. Thus, these two models are statistically valid. They allow us to examine both an overall decisional balance score, and a simplified two-factor structure (barriers and facilitators) or a more detailed six-factor structure (physical, psychological, and socio-environmental facilitators; physical, psychological, and socio-environmental barriers). These two models provide a comprehensive understanding of the decision balance for each individual. In accordance with the French version of the decisional balance for PA in the general population (27), the DBSPA-FSV can be used to calculate an overall decision balance score based on barrier and facilitator scores but also to identify the scores for each type of barrier and facilitator (physical, psychological, and socio-environmental). Convergent validity was confirmed by relationships between the DBSPA-FSV constructs and the different types of motivations for PA (35) in the expected directions.
4 Step 3: reliability of the DBSPA-FSV
The purpose of the third step of the study was to examine the reliability of the 22-item DBSPA-FSV scale. The term “reliability” refers to the consistency or repeatability of measurements (38). The internal consistency of the DBSPA-FSV scale and its temporal stability over a 2-week interval were examined.
4.1 Method
4.1.1 Participants and procedure
Participants were 59 female students (Mage = 23.00 years, SD = 10.38) of a sport science University of the South of France. Their sociodemographic characteristics are presented in Table 5. Volunteer participants from the main sample (N = 301) were asked to complete the 22-item version of the DBSPA-FSV scale on a second occasion within a 2-week interval.
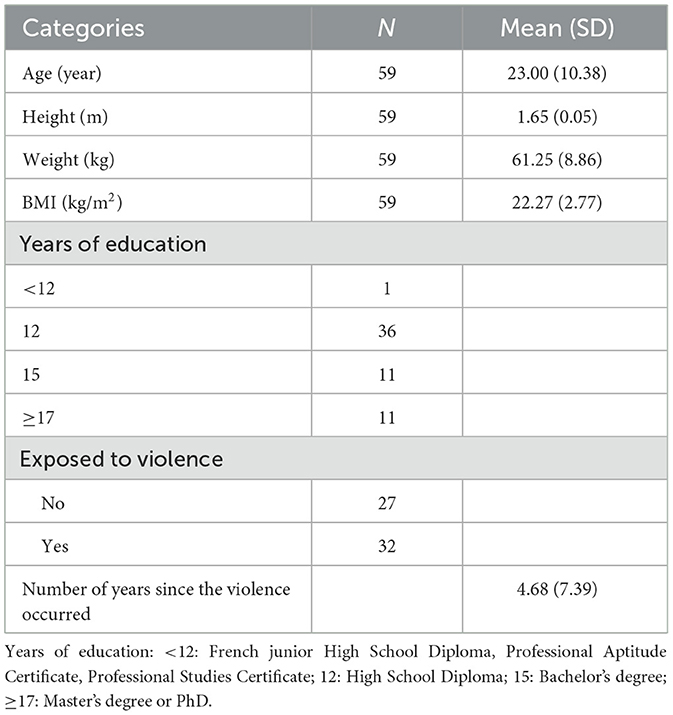
Table 5. Characteristics of the participants involved in checking the reliability of the DBSPA-FSV scale (N = 59).
4.1.2 Data analyses
Internal consistency was assessed using Cronbach's alpha coefficients (42) calculated for each dimension of the scale. In line with Aldridge et al. (43), we used the intra-class correlation coefficient (ICC) to assess the test-retest reliability. Values < 0.50 were expected to indicate poor reliability, values between 0.50 and 0.75 moderate reliability, values between 0.75 and 0.90 good reliability, and values >0.90 excellent reliability (40).
4.2 Results
Skewness and kurtosis were assessed for the eight dimensions of the DBSPA-FSV at the two-time measurements. Skewness ranged from −1.48 to 0.61, and kurtosis ranged from −1.44 to 3.49. Therefore, the normality of data was assumed (33).
4.2.1 Internal consistency
Cronbach's alphas for each subscale were calculated (see Table 6). For both time measurements, Cronbach's alphas ranged from 0.60 to 0.89. All constructs were above 0.70, except socio-environmental facilitators (αT1 = 0.66; αT2 = 0.62) and physical barriers (αT1 = 0.66; αT2 = 0.60).
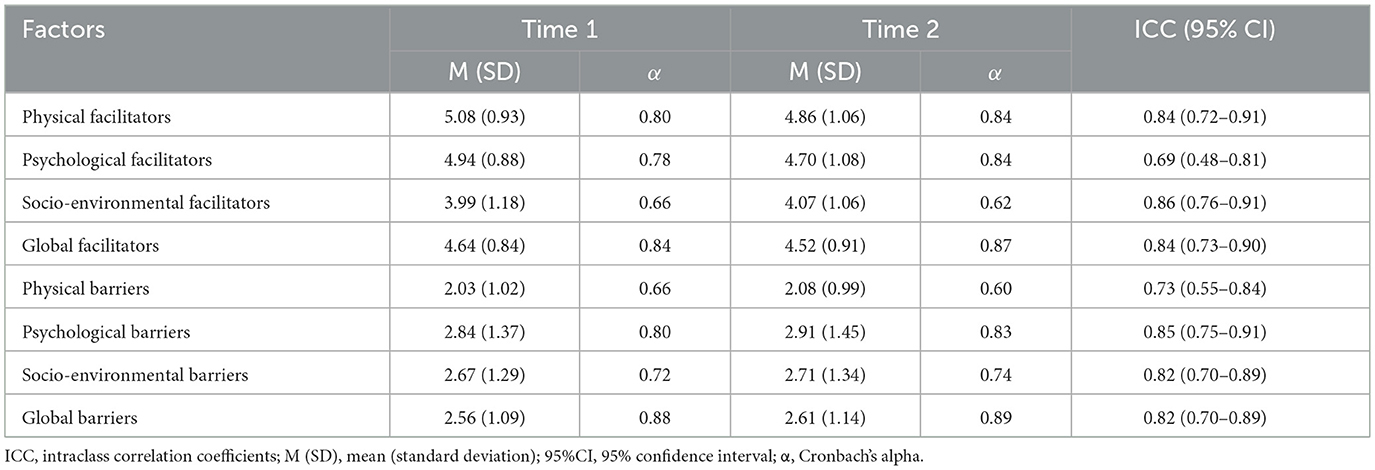
Table 6. Intraclass correlation coefficients (N = 59).
4.2.2 Test-retest reliability
The ICC results are presented in Table 6. Physical facilitators, socio-environmental facilitators, global facilitators, psychological barriers, socio-environmental barriers, and global barriers presented good reliability (43). Psychological facilitators and physical barriers presented moderate reliability (43).
4.3 Discussion
Internal consistency was demonstrated for all subscales (see Table 6), although the socio-environmental facilitators and physical barriers showed only marginally acceptable internal consistency (38). Therefore, the internal consistency was attested. The ICC of the DBSPA-FSV dimensions were moderate to good (44). Therefore, the test-retest reliability was attested.
Internal consistency was demonstrated for all subscales (see Table 6), although the socio-environmental facilitators and physical barriers showed only marginally acceptable internal consistency (38) and therefore should be subject to refinement in future studies. Thus, internal consistency was attested. The ICC of the DBSPA-FSV dimensions ranged from moderate to good (44). Therefore, test-retest reliability was attested.
5 General discussion
This study aimed to develop and validate a DBSPA-FSV scale that measures the barriers and facilitators for engaging in PA specific to female survivors of violence. The resulting 22-item scale comprises two subfactors (facilitators and barriers) each encompassing three dimensions: physical, psychological, and socio-environmental. This scale demonstrated satisfactory psychometric properties and represents a key step forward in understanding the psychological factors influencing PA engagement among this population. Existing decisional balance tools are either too generic, failing to capture the specific psychological needs of women exposed to violence—such as the need for safety, trust, and confidentiality—or are too narrowly tailored to other populations (e.g., workplace settings or chronic illnesses), making them unsuitable to this context. Developing a decisional balance scale specifically adapted to women exposed to violence was therefore essential to fill this gap and to support the design of trauma-informed PA interventions.
First, the clarity of all scale items was evaluated to ensure accurate comprehension. Then, an analysis of the dimensional structure was conducted, which led to the selection of two models. The results showed that the bifactor models—with a general factor and either two correlated factors or six correlated factors—presented good fit indices. These validated models offer robust frameworks for understanding both the general and specific dimensions of the barriers and facilitators to engaging in physical activity encountered by women exposed to violence. The validated bifactor models thus provide a comprehensive tool for assessing decisional balance, taking into account both the overall structure and its specific components. As expected, the scale correlated in the anticipated directions with different types of motivation for physical activity (i.e., intrinsic motivation, extrinsic motivation by integrated regulation, identified regulation, introjected regulation, external regulation, and amotivation), demonstrating good convergent validity. These associations support the theoretical coherence of the instrument and open avenues for future research, particularly regarding how different forms of violence may distinctly influence motivational processes related to physical activity. Finally, each of the scale's dimensions showed acceptable internal consistency, as indicated by Cronbach's alpha coefficients. Temporal reliability was also satisfactory across the eight dimensions. Altogether, the validation phases demonstrated the solid psychometric properties of the DBSPA-FSV scale.
This study presents several notable strengths, including the development of an original tool specifically tailored to women exposed to violence, addressing a gap in existing measures of decisional balance for physical activity. The scale is grounded in a solid theoretical framework and was developed through a rigorous, multi-phase psychometric validation process, ensuring both conceptual relevance and methodological robustness. In addition to the strengths of this study, certain limitations must be acknowledged. First, we did not collect data on participants' race or ethnicity, which limits the ability to explore potential interactions between cultural or racial factors and PA engagement. Socioeconomic status was assessed only through the highest educational degree obtained, which provides a partial indicator. Future studies should include more comprehensive measures of socioeconomic and ethnocultural background. Additionally, the type of violence experienced (e.g., psychological, physical, or sexual), the age at which it occurred (e.g., childhood or adulthood), and the duration or frequency of the exposure (e.g., repeated vs. isolated incidents) were not assessed. This lack of contextual factors limits the exploration of potential distinctions. Prior research suggests that such variables can significantly shape psychological outcomes and behavioral responses (45). Future studies should address these questions to allow for a more nuanced understanding of how the nature and timing of violence influence decisional processes related to physical activity. Although this validation highlighted the good psychometric properties of the tool, it is important to emphasize the heterogeneity of behaviors on the continuum of violence experienced by the participants (36). Future studies would be necessary to explore in greater depth differences on the continuum of violence. Temporal stability was attested. However, responses to the barriers and facilitators could evolve over time or vary depending on the severity and recurrence of trauma.
Therefore, a study of their evolution over time would provide valuable insights. Longitudinal studies could assess how interventions targeting specific barriers and facilitators impact PA engagement and overall wellbeing. Furthermore, future research should explore the role of introjected forms of motivation in sustaining long-term PA engagement, given their positive correlations with facilitators despite being extrinsic in nature. Finally, validation of this tool will also allow us to carry out more quantitative studies to examine the psychological correlates of the decisional balance for PA, and to define intervention strategies tailored to survivor profiles.
This scale offers many practical applications. Health and sport professionals can leverage it to design targeted intervention strategies and customize programs to address psychological, physical, and socio-environmental barriers. International validation of the tool in the future could facilitate broader research on PA engagement across diverse cultural contexts, thereby enhancing its overall usefulness. In sum, the DBSPA-FSV scale is a valuable instrument for advancing both theoretical research and applied practices. By contributing to a nuanced understanding of the decisional balance for PA in female survivors of violence, whether through a global index, two broad dimensions (barriers and facilitators), or six specific sub-dimensions, this tool paves the way for the development of innovative strategies to improve their physical and psychological health.
The present research highlights the value of the DBSPA-FSV scale as a novel and psychometrically sound tool to assess the barriers and facilitators for engaging in PA perceived by female survivors of violence. Beyond bridging a critical gap in sport and exercise psychology, this scale has also a broader relevance for public health, trauma-informed care, mental health interventions, and health behavior change research. By capturing the psychological, physical, and socio-environmental factors that influence physical activity engagement in this vulnerable population, the DBSPA-FSV can support the development of targeted, interdisciplinary interventions aimed at promoting physical activity and improving overall wellbeing.
6 Conclusion
The DBSPA-FSV scale is a robust and innovative tool for assessing the barriers and facilitators for engaging in PA specific to female survivors of violence. It enriches the sport psychology literature while offering practical value for health and sports professionals. The scale's validation in French-speaking contexts provides a foundation for further international adaptation and application. By providing a deeper understanding of the unique challenges faced by women survivors of violence, the DBSPA-FSV scale could contribute to the development of tailored and impactful interventions for survivors of violence and support them in their journey toward greater PA engagement, improved wellbeing, and better quality of life. Beyond bridging a critical gap in sport and exercise psychology, this scale also has broader relevance for public health, trauma-informed care, mental health interventions, and health behavior change research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The protocol was approved by the Local Ethics Committee for non-interventional research (authorization no. 2023-104). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
CF: Investigation, Writing – review & editing, Writing – original draft, Data curation, Formal analysis, Methodology. Fd'A-L: Conceptualization, Writing – review & editing, Supervision, Methodology, Writing – original draft. L-AP: Formal analysis, Data curation, Writing – original draft. MH: Writing – review & editing, Writing – original draft, Supervision, Data curation, Formal analysis, Methodology. SM-S: Formal analysis, Writing – original draft, Conceptualization, Methodology, Writing – review & editing, Supervision.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project received a PhD grant from the Région Sud Provence-Alpes Côte d'Azur, and support from the Azur Sport Santé association and the Fédération Française d'Éducation Physique et de Gymnastique Volontaire. Additionally, the project was awarded a research grant from the Groupe Pasteur Mutualité and Villa M. This work was supported by the French government, through the UCAJEDI Investments in the Future project managed by the National Research Agency (ANR) under reference number ANR-15-IDEX-01. Finally, this project was awarded a research grant from the Comité National Olympique et Sportif Français.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Violence Against Women Prevalence Estimates, 2018: Global, Regional and National Prevalence Estimates for Intimate Partner Violence Against Women and Global and Regional Prevalence Estimates for Non-Partner Sexual Violence Against Women [Internet]. Geneva: World Health Organization (2021). Available online at: https://www.who.int/publications/i/item/9789240022256 (Accessed October 14, 2025).
2. United Nations Human Rights Office of the High Commissioner. Declaration on the Elimination of Violence against Women [Internet]. Geneva: United Nations (1993). Available online at: https://www.ohchr.org/en/instruments-mechanisms/instruments/declaration-elimination-violence-against-women (Accessed October 14, 2025).
3. UN Women. Facts and Figures: Ending Violence Against Women [Internet]. New York, NY: United Nations Entity for Gender Equality and the Empowerment of Women (2023). Available online at: https://www.unwomen.org/en/articles/facts-and-figures/facts-and-figures-ending-violence-against-women (Accessed October 14, 2025).
4. World Health Organization. Violence Against Women [Internet]. Geneva: World Health Organization (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (Accessed October 14, 2025).
5. Haut Conseil à l'Égalité entre les femmes et les hommes. Avis sur la définition du viol et des autres agressions sexuelles en droit français [Opinion on the Definition of Rape and Other Sexual Assaults in French Law]. Paris: HCE (2016). Available online at: https://www.haut-conseil-egalite.gouv.fr/IMG/pdf/hce_avis_viol_2016_10_05.pdf (Accessed October 14, 2025).
6. Bouchard EM, Tourigny M, Joly J, Hébert M, Cyr M. Les conséquences à long terme de la violence sexuelle, physique et psychologique vécue pendant l'enfance [Long-term consequences of sexual, physical, and psychological violence experienced during childhood]. Rev Epidemiol Sante Publique. (2008) 56:333–44. French. doi: 10.1016/j.respe.2008.06.260
7. Pebole M, Gobin RL, Hall KS. Trauma-informed exercise for women survivors of sexual violence. Transl Behav Med. (2021) 11:686–91. doi: 10.1093/tbm/ibaa043
8. Rosenbaum S, Vancampfort D, Steel Z, Newby J, Ward PB, Stubbs B. Physical activity in the treatment of post-traumatic stress disorder: a systematic review and meta-analysis. Psychiatry Res. (2015) 230:130–6. doi: 10.1016/j.psychres.2015.10.017
9. Oppizzi LM, Umberger R. The effect of physical activity on PTSD. Issues Ment Health Nurs. (2018) 39:179–87. doi: 10.1080/01612840.2017.1391903
10. Moro C. Prévention des maladies métaboliques par l'activité physique: des preuves aux mécanismes [Prevention of metabolic diseases through physical activity: from evidence to mechanisms]. Médecine Mal Métaboliques. (2019) 13:617–21. French. doi: 10.1016/S1957-2557(19)30186-5
11. Wright S, Chiocchia V, Elugbadebo O, Simple O, Furukawa TA, Friedrich C, et al. The therapeutic potential of exercise in post-traumatic stress disorder and its underlying mechanisms: a living systematic review of human and non-human studies. Wellcome Open Res. (2025) 9:720. doi: 10.12688/wellcomeopenres.23033.2
12. World Health Organization. Injuries and Violence [Internet]. Geneva: World Health Organization (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence (Accessed October 14, 2025).
13. Greene DR, Holland-Winkler AM, Petruzzello SJ. Enjoyment and affective responses to moderate- and high-intensity exercise: a randomized controlled trial in individuals with subsyndromal PTSD. Sports. (2024) 12:138. doi: 10.3390/sports12050138
14. Basile KC, Chen J, Black MC, Saltzman LE. Prevalence and characteristics of sexual violence victimization among U.S. adults, 2001–2003. Violence Vict. (2007) 22:437–51. doi: 10.1891/088667007781553955
15. Pebole M, Hall K, Petruzzello S, Alston R, Gobin R. Exercise preferences among women survivors of sexual violence by PTSD and physical activity level: implications and recommendations for trauma-informed practice. Ment Health Phys Act. (2022) 23:1–9. doi: 10.1016/j.mhpa.2022.100470
16. Wheatley L, Mastrogiovanni C, Pebole M, McKeon G, Rosenbaum S, Rees S, et al. Physical activity levels and sedentary behavior in people who have experienced gender-based violence: a systematic review. Ment Health Phys Act. (2024) 26:100596. doi: 10.1016/j.mhpa.2024.100596
17. Pebole MM, Singleton CR, Hall KS, Petruzzello SJ, Alston R, Gobin RL. Perceived barriers and benefits of exercise among women survivors of sexual violence by physical activity level and posttraumatic stress disorder status. Violence Against Women. (2024) 30:3726–50. doi: 10.1177/10778012231182412
18. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR. 5th ed., text rev. Washington (DC): American Psychiatric Publishing (2022). doi: 10.1176/appi.books.9780890425787
19. Inserm. Troubles Stress Post-traumatique. Paris: Inserm (2020). Available online at: https://www.inserm.fr/dossier/troubles-stress-post-traumatique/ (Accessed October 14, 2025).
20. Thomas J-L. Les conséquences des violences sexuelles sur la santé physique: revue de la littérature [The consequences of sexual violence on physical health: a literature review]. Rev Français Dommage Corporel. (2015) 3:253–69. French.
21. Smith-Marek EN, Baptist J, Lasley C, Cless JD. I don't like being that hyperaware of my body: women survivors of sexual violence and their experience of exercise. Qual Health Res. (2018) 28:1692–707. doi: 10.1177/1049732318786482
22. Favola C, d'Arripe-Longueville F, Mériaux-Scoffier S. Barriers and facilitators to physical activity among women victims of violence: a qualitative study based on the transtheoretical model of behavior change. Women Sport Phys Act. (Under Review).
23. Janis IL, Mann L. Decision-Making: A Psychological Analysis of Conflict, Choice and Commitment. New York: Free Press (1977).
24. Prochaska JO, DiClemente CC. Transtheoretical therapy: toward a more integrative model of change. Psychother Theor Res Pract. (1982) 19:276–88. doi: 10.1037/h0088437
25. Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: applications to addictive behaviors. Am Psychol. (1992) 47:1102–14. doi: 10.1037/0003-066X.47.9.1102
26. Marcus BH, Rakowski W, Rossi JS. Assessing motivational readiness and decision making for exercise. Health Psychol. (1992) 11:257–61. doi: 10.1037/0278-6133.11.4.257
27. Eeckhout C, Francaux M, Heeren A, Philippot P. Mesure de la balance décisionnelle en vue de pratiquer une activité physique régulière (BDAP): adaptation et validation francophone de l'échelle Decisional Balance for Exercise [Measuring decisional balance for engaging in regular physical activity: adaptation and French validation of the decisional balance for exercise scale]. Rev Eur Psychol Appl. (2013) 63:185–91. French. doi: 10.1016/j.erap.2013.01.001
28. d'Arripe-Longueville F, Hayotte M, Planchard JH, Steiner DD, Corrion K. Development and validation of the workplace decisional balance scale for exercise (WDBex) in a French sample. J Occup Environ Med. (2021) 63:E715–23. doi: 10.1097/JOM.0000000000002349
29. Filleul V, Ladune R, Gruet M, Falzon C, Fuchs A, Mély L, et al. Development and validation of the Cystic Fibrosis Decisional Balance for Physical Activity scale (CF-DB-PA). BMC Pulm Med. (2021) 21:121. doi: 10.1186/s12890-021-01471-0
30. Davergne T, Moe RH, Fautrel B, Gossec L. Development and initial validation of a questionnaire to assess facilitators and barriers to physical activity for patients with rheumatoid arthritis, axial spondyloarthritis and/or psoriatic arthritis. Rheumatol Int. (2020) 40:2085–95. doi: 10.1007/s00296-020-04692-4
31. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. (2018) 6:149. doi: 10.3389/fpubh.2018.00149
32. Vallerand RJ. Vers une méthodologie de validation trans-culturelle de questionnaires psychologiques: implications pour la recherche en langue française [Toward a methodology for cross-cultural validation of psychological questionnaires: implications for research in the French language]. Can Psychol. (1989) 30:662–80. French. doi: 10.1037/h0079856
33. Daley AJ, Duda JL. Self-determination, stage of readiness to change for exercise, and frequency of physical activity in young people. Eur J Sport Sci. (2006) 6:231–43. doi: 10.1080/17461390601012637
34. Lin SH, Hsieh PJ. Book review: Kline RB. Principles and practice of structural equation modeling (2nd ed). Res Soc Work Pract. (2010) 20:126–8. doi: 10.1177/1049731509336986
35. Deci EL, Ryan RM, editors. Self-determination research: reflections and future directions. In: Handbook of Self-Determination Research. University of Rochester Press (2002). p. 431–41.
36. Kelly L, Traduit de l'anglais par Tillous M. Le continuum de la violence sexuelle [The Continuum of Sexual Violence]. Cahiers du Genre. (2019) 66:17–36. doi: 10.3917/cdge.066.0017
37. Boiché J, Gourlan M, Trouilloud D, Sarrazin P. Development and validation of the “Echelle de Motivation envers l'Activité Physique en contexte de Santé”: a motivation scale towards health-oriented physical activity in French. J Health Psychol. (2019) 24:386–96. French. doi: 10.1177/1359105316676626
38. Taber KS. The use of Cronbach's alpha when developing and reporting research instruments in science education. Res Sci Educ. (2018) 48:1273–96. doi: 10.1007/s11165-016-9602-2
39. Myers ND, Martin JJ, Ntoumanis N, Celimli S, Bartholomew KJ. Exploratory bifactor analysis in sport, exercise, and performance psychology: a substantive-methodological synergy. Sport Exerc Perform Psychol. (2014) 3:258–72. doi: 10.1037/spy0000015
41. Byrne BM. Structural Equation Modeling with Amos: Basic Concepts, Applications, and Programming. 3rd ed. Routledge (2016). doi: 10.4324/9781315757421
42. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. (1951) 16:297–334. doi: 10.1007/BF02310555
43. Aldridge VK, Dovey TM, Wade A. Assessing test-retest reliability of psychological measures: persistent methodological problems. Eur Psychol. (2017) 22:207–18. doi: 10.1027/1016-9040/a000298
44. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
Keywords: psychometric validation, transtheoretical model, behavior change, facilitators and barriers, self-determined motivation, physical activity engagement, women's health
Citation: Favola C, d'Arripe-Longueville F, Piroird L-A, Hayotte M and Mériaux-Scoffier S (2025) Development and validation of the Decisional Balance Scale for Physical Activity in Female Survivors of Violence (DBSPA-FSV). Front. Public Health 13:1638237. doi: 10.3389/fpubh.2025.1638237
Received: 30 May 2025; Accepted: 07 October 2025;
Published: 28 October 2025.
Edited by:
Estela Capelas Barbosa, University of Bristol, United KingdomReviewed by:
Bangbang Syamsudar, STKIP Pasundan, IndonesiaTsun-Feng Chiang, National Chiayi University, Taiwan
Hannah Hammond, University of Birmingham, United Kingdom
Kaley Davis, Marquette University, United States
Copyright © 2025 Favola, d'Arripe-Longueville, Piroird, Hayotte and Mériaux-Scoffier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camille Favola, Y2FtaWxsZS5mYXZvbGFAdW5pdi1jb3RlZGF6dXIuZnI=