 Juan Martín Hernández1Ignacio Barbero Navarro2
Juan Martín Hernández1Ignacio Barbero Navarro2 Diego Rodríguez Menacho2Paloma Villalva Hernández1,2Jose María Barrera Mora2
Diego Rodríguez Menacho2Paloma Villalva Hernández1,2Jose María Barrera Mora2 David Ribas-Pérez2*Antonio Castaño Séiquer2
David Ribas-Pérez2*Antonio Castaño Séiquer2- 1Servicio Andaluz de Salud, Spain
- 2Department of Stomatology, Universidad de Sevilla, Sevilla, Spain
Background: Health equity, particularly in oral health, remains a challenge for socially excluded populations such as migrants. This study investigates the oral health status and associated social determinants of health among adult immigrants residing at the Temporary Stay Center for Immigrants (CETI) in Melilla, Spain.
Methods: A cross-sectional study was conducted in March 2024 involving 128 adult CETI residents. Data collection included standardized oral examinations following WHO guidelines and structured questionnaires assessing sociodemographic variables, health habits, and dental care history. Statistical analyses were performed using SPSS 29.0, with significance set at p < 0.05.
Results: The sample was predominantly Latin American (80.5%) and male (67.2%), with a mean age of 34.85 years. While most participants reported good oral hygiene habits, 67.2% were partially edentulous, and the mean Decayed, Missing, Filled, Teeth (DMFT) index was 9.73—higher than national averages. Only 9.4% used dental prostheses. Significant differences were observed between Latin American and African subgroups regarding age distribution, oral hygiene habits, and access to dental care.
Conclusion: Migrant populations at CETI face substantial oral health challenges and disparities linked to origin, education, and access to care. Ongoing epidemiological monitoring is essential to inform tailored, equity-oriented public health interventions that address the dynamic needs of these populations.
1 Introduction
One of our main responsibilities as healthcare professionals is to ensure equity in access to healthcare services and treatments aimed at improving patients’ overall health. But what exactly is health equity according to the World Health Organization (WHO)? It is defined as:
“The absence of unfair and avoidable or remediable differences in health among population groups defined socially, economically, demographically or geographically” (1).
As indicated by this definition, key drivers of health equity include social, economic, demographic, and geographic conditions. These factors tend to have a greater impact on disadvantaged groups, highlighting the importance of focusing research efforts on these populations to effectively address and reduce health inequities in comparison to the broader population.
Health inequalities are significantly shaped by what the WHO calls the social determinants of health (SDH). These are non-medical factors that influence health outcomes—broadly encompassing the conditions in which people are born, grow, live, work, and age. These conditions are shaped by the distribution of money, power, and resources at global, national, and local levels, including political systems, social norms, and economic policies. Health follows a social gradient—those with lower socioeconomic status generally experience worse health outcomes (2). Migrant populations are particularly vulnerable, as they are often exposed to multiple risk factors simultaneously.
It is incorrect to assume that social exclusion only occurs in developing countries. Even in high-income nations, there are socially excluded groups. For instance, Harvard University in the United States has implemented social dentistry programs aimed at low-income families, homeless individuals (3, 4), Spanish-speaking minorities (5, 6), and people with disabilities (7). In Spain, similar initiatives are conducted by the Universities of Valencia and Seville, which have developed specific programs for vulnerable populations (8, 9).
Building on this, it is important to recognize that these same social dynamics influence not only general health but also oral health, which is the specific focus of our work. Scientific evidence reveals a strong correlation between social inequalities and poor oral health, making oral health a valuable indicator of how social disadvantages impact overall well-being (2, 8–11).
Moreover, oral health plays a crucial role in daily functioning, nutrition, speech, and self-esteem. It can also serve as a gateway for detecting systemic diseases and chronic conditions. As such, poor oral health reflects and exacerbates broader health inequalities, underlining the need for targeted interventions in disadvantaged communities.
Achieving equity in oral health requires more than knowledge of social inequalities—it also demands an understanding of individuals’ life histories and societal contexts. In the case of migrants, this includes both their country of origin and the host society in which they aim to integrate.
In recent years, numerous preventive social dentistry programs have been developed for marginalized groups, aligned with the WHO’s holistic definition of health as a state of complete biological and psychological well-being influenced by sociocultural determinants (2).
Before implementing preventive actions aimed at immigrants and refugees, it is essential to assess their current health status and determine the level of intervention needed to improve it. With an initial epidemiological survey that would provide a deeper understanding of the target population, not only in terms of objective oral health status but also regarding relevant social, personal, and geographic determinants.
Migration is an increasingly important global issue that is significantly influencing the course of the 21st century. Migrants often face vulnerable and unstable circumstances as they seek improved living conditions in countries with unfamiliar cultures, languages, and social structures—many entering via irregular routes. Consequently, migration presents complex challenges related to personal well-being, humanitarian concerns, and social exclusion (12). The magnitude of this issue is underscored by growing global economic disparities and ongoing conflicts. The emotional and psychological toll of extreme migration experiences has even led to the identification of the so-called “Ulysses Syndrome,” a stress-related condition affecting many migrants (13).
Epidemiological studies serve as the primary source of information on disease distribution, health determinants, and risk factors within populations, and are vital for the design of effective preventive and therapeutic programs (14).
Each migrant population is unique and must be studied accordingly. Individual backgrounds, personal histories, and identified SDH factors (3) should be taken into account. It is crucial to understand how each specific population arrives in the host country, where they come from, what language they speak, their education level, and other contextual elements that affect their physical and psychological health, integration capacity, and access to healthcare systems. Facilitating access to healthcare services is now recognized as one of the most important factors in improving the health of migrant populations (15, 16).
It is also necessary to evaluate the host country’s healthcare system—its strengths, limitations, and ability to integrate marginalized populations—to provide the best possible support to incoming migrants (17–19).
In our case, the immigrant population under study is housed at the Temporary Stay Center for Immigrants (CETI) in the Autonomous City of Melilla, Spain. Unlike other autonomous regions in Spain, Melilla does not conduct regular epidemiological surveys on oral health—an important tool for shaping public health policy. These surveys are key to achieving national oral health goals set by the General Council of Dentists of Spain for (18), as well as global objectives outlined by the WHO (2).
Acknowledging this data gap, we have conducted several epidemiological studies in Melilla—some focused on local health conditions (20) and most targeting the immigrant population at CETI (21–23).
Our ongoing research has revealed that the CETI migrant population is highly dynamic. While it was once composed mainly of sub-Saharan and North African migrants (as one might expect due to Melilla’s geographical location), the current population is predominantly Latin American. These groups differ significantly in language, health habits, and needs. Understanding such shifts requires knowledge of local and national political and migration policies, which we will discuss later in this work. Shifts in migratory flows in recent years, along with the relocation of existing migrant populations to other regions of Spain or Europe, may account for the observed changes in predominant nationalities (24).
This variability underscores the necessity of conducting this cross-sectional epidemiological study, which aims to inform and improve public health interventions tailored to the changing needs of CETI’s population. Well-targeted oral health education programs have been shown to be particularly effective for refugees (16).
The main objective of this study was to assess the oral health status of socially excluded adult immigrants living at the CETI in Melilla, and to provide data that will help policymakers develop informed, effective public health strategies.
2 Materials and methods
2.1 Study design
This study employed a cross-sectional design. Data were collected through a survey administered to 128 adult residents at the Temporary Stay Center for Immigrants (CETI) during the last week of March 2024. The methodology included a standardized oral cavity examination in accordance with World Health Organization (WHO) guidelines. Additionally, a structured questionnaire focusing on oral health was used. This questionnaire is validated by the WHO and included in the manual Oral health surveys: Basic methods (25). Specifically, Annexes 1 and 7 of the manual were utilized as we can see as an Supplementary Table 1.
2.2 Population characteristics
2.2.1 Gender
The study sample included 128 individuals, of whom 86 (67.2%) were men and 42 (32.8%) were women. Despite the numerical difference, the gender differences—even when analyzed by age groups—were not statistically significant. The Chi-square test for gender distribution between the two ethnic groups evaluated also showed no significant difference.
2.2.2 Age
Participants ranged in age from 18 to 66 years, with a mean age of 34.85 years. For statistical purposes, age was grouped into three categories: Young Adult (18–29 years; n = 47, 36.7%), Adult (30–50 years; n = 68, 53.1%), and Older Adult (51–66 years; n = 13, 10.2%).
2.2.3 Origin
Subjects came from diverse countries: Chile (n = 1), Colombia (n = 55), Cuba (n = 1), Honduras (n = 2), Mali (n = 4), Morocco (n = 23), Peru (n = 7), an unspecified country (n = 1), and Venezuela (n = 34). Almost 43% of the sample came from Colombia. To simplify data analysis, they were grouped into two broader categories: Latin Americans (n = 103, 80.5%) and Africans (n = 25, 19.5%).
2.2.4 Educational level
Participants reported a wide variety of previous occupations and education levels. For analysis, they were grouped as follows: Students (n = 13, 10.2%), Elemental Formation (n = 71, 55.5%), Vocational Training (n = 13, 10.2%), and Higher Education (n = 13, 10.2%) (Figure 1).
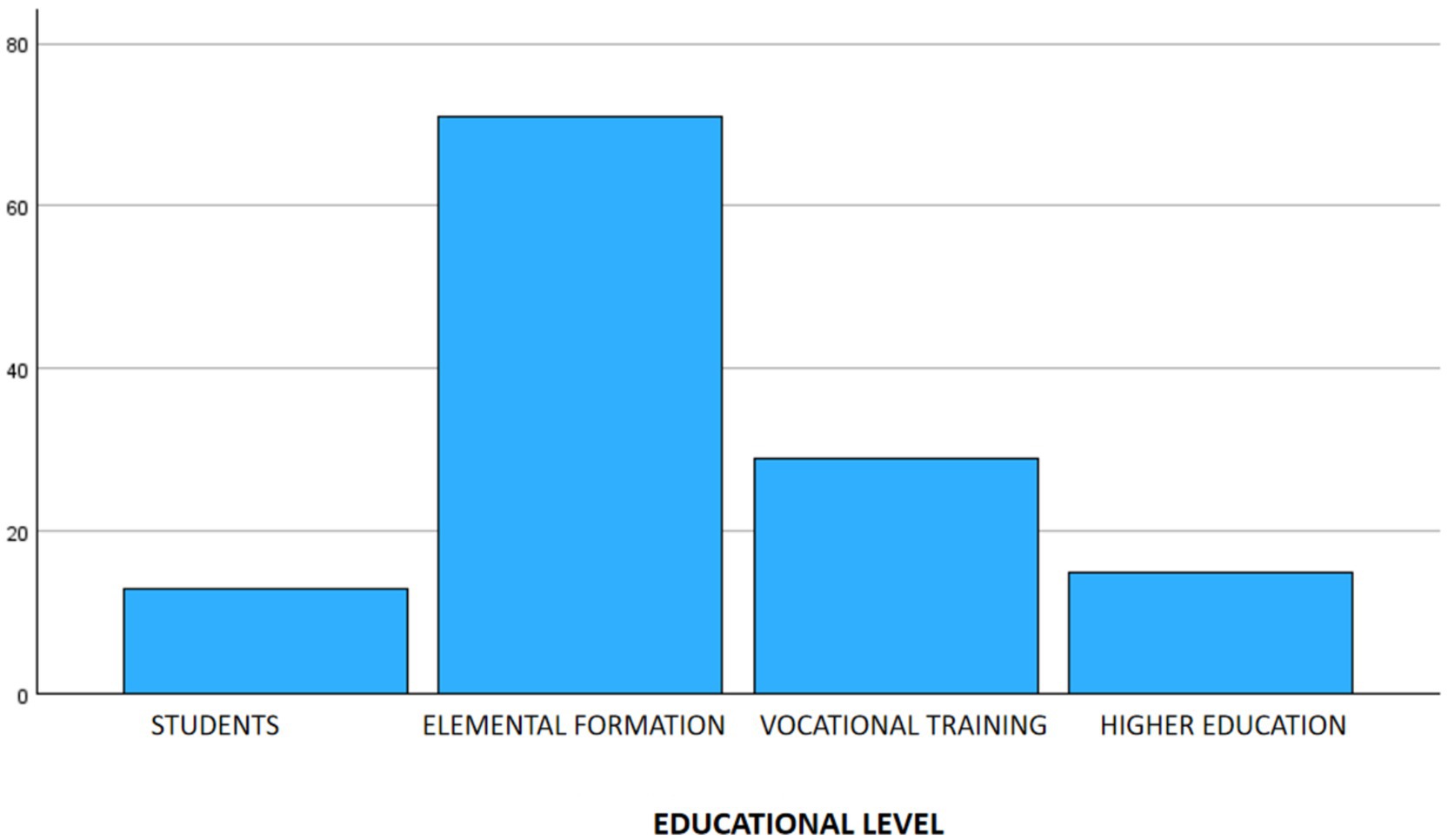
Figure 1. Distribution of the sample by educational level.
2.3 Statistical analysis
Quantitative variables were analyzed using the Student’s t-test, while qualitative variables were examined using the Chi-square test. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 29.0 (Statistical Package for Social Sciences, Chicago, IL, USA).
2.4 Ethical considerations of the study
This research involving human participants was conducted in accordance with the ethical standards of the institutional and/or national research committee, and with the 1964 Helsinki Declaration and its later amendments. Ethical approval was obtained from the Odontologia Social Foundation ethics committee (n° 04/24) approved in January 2024.
3 Results
3.1 Habits
3.1.1 Sugar-sweetened beverage consumption
Eighty-five respondents (67.2%) consumed sugary drinks, while 42 (33.6%) did not. Among the 85 consumers, 69 drank one glass per day (80.2%), 7 drank two (8.1%), and 10 drank more than two (11.6%).
3.1.2 Sugary food consumption
Eighty-two participants (64.1%) reported consuming sugary foods. However, this may be underreported due to the regular snack provided at the center.
3.1.3 Toothbrushing frequency
Average of 2.88 times/day. Distribution: never (1.6%), once/day (11.7%), twice/day (36.7%), three times/day (50%). Gingival bleeding: 59.4% reported no bleeding; 40.6% reported bleeding during brushing.
3.1.4 Smoking
26.6% of respondents smoked. Among them, 52.9% smoked <5 cigarettes/day, 14.7% smoked 5–10 cigarretes, and 32.4% smoked >10 cigarretes (Figure 2).
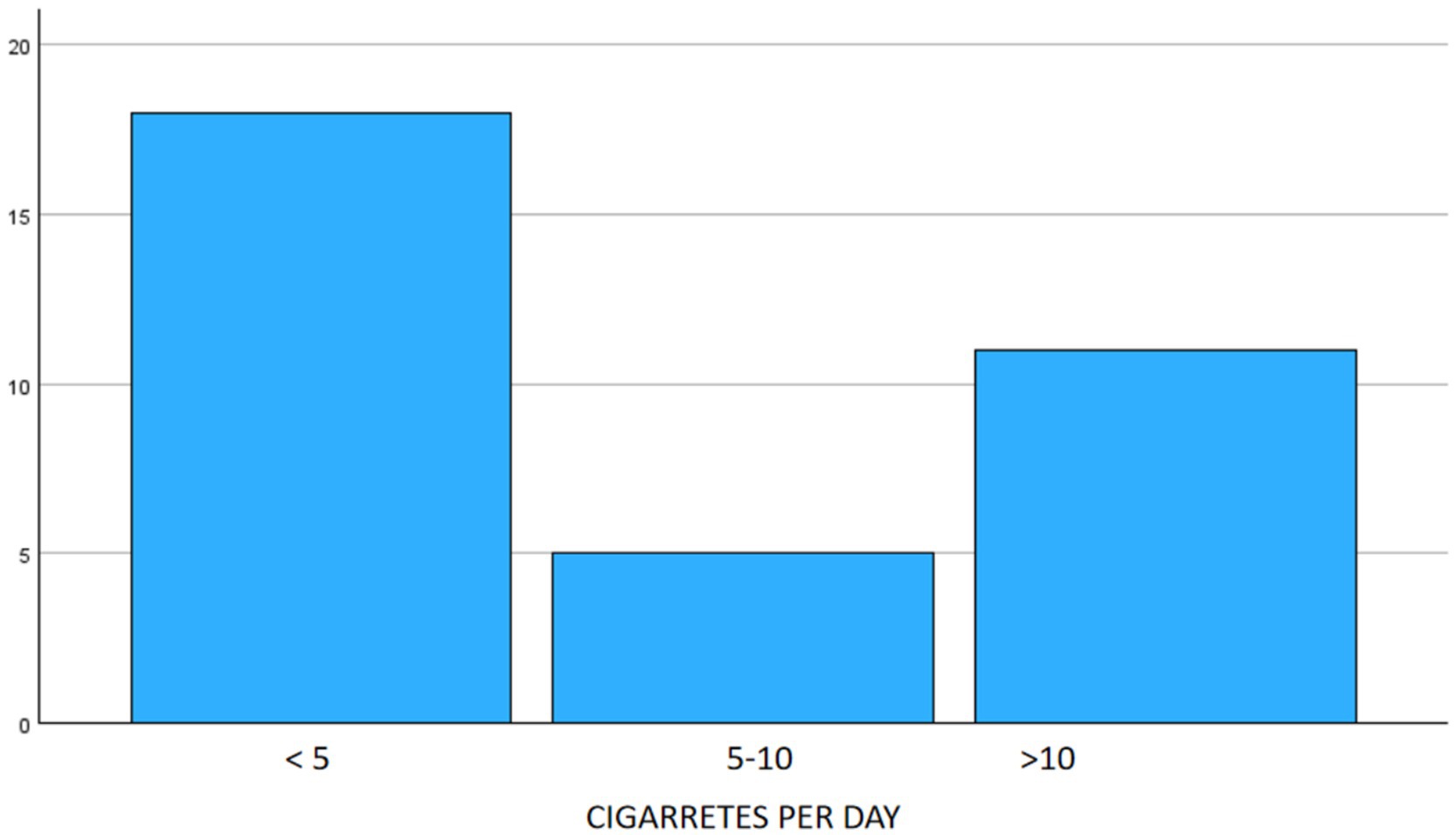
Figure 2. Smoking habits in the sample.
3.2 Dental visits
Last dental visit distribution: <6 months (28.1%), 6 months–1 year (31.3%), 1–2 years (11.7%), 2–5 years (14.1%), >5 years (8.5%), never (6.3%) (Table 1).
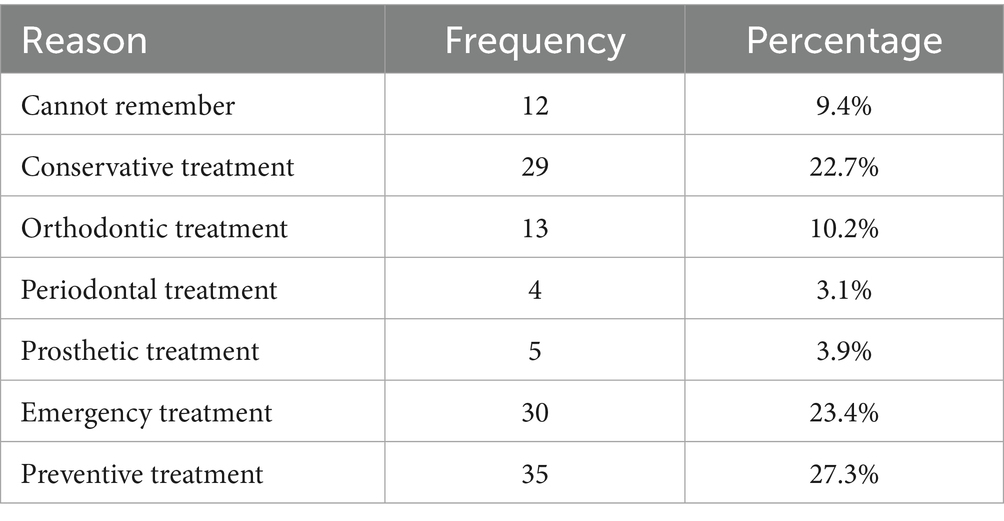
Table 1. Reason for last dental visit.
3.3 General oral condition
Dentition status: 32.9% fully dentate, 67.2% partially edentulous, 0% completely edentulous.
Use of dental prostheses: Only 9.4% wore partial dentures.
Mean values:
• Total teeth: 27.84.
• Healthy teeth: 24.15.
• Teeth with caries: 3.54.
• Filled teeth: 3.18.
• Missing teeth: 3.01.
• Missing due to caries: 1.57.
• Non-erupted: 1.14.
• Sealed: 0.12.
Tooth opacities: 90% had none. Others had diffuse or demarcated opacities, or hypoplasia.
Fluorosis: Absent in 97.7%.
Erosion: 91.4% had none. Minimal cases showed enamel, dentin, or pulp involvement.
Dental trauma: 93% had none. Minor cases of treated or untreated trauma observed.
DMFT Index: Mean value was 9.73 (range: 0–27).
3.4 Cross-tabulation of variables
As previously mentioned, in the analytical phase of the study, variables were cross-tabulated according to their qualitative and/or quantitative nature, and the corresponding statistical analyses were performed. A p-value of < 0.05 was considered statistically significant.
In this context, the chi-square test applied to qualitative variables revealed statistically significant associations between:
• Nationality and prosthesis-wearing status (p = 0.001).
• Nationality and smoking habits (p = 0.0042).
• Nationality and oral hygiene habits (p = 0.002).
• Gender and smoking habits (p = 0.009).
When comparing origin with age groups, statistically significant differences were observed (Chi-square, p < 0.001). Latin American immigrants tended to be older, with greater representation in the 30–50 and 51–66 age groups, while African immigrants were mostly within the 18–30 age group and had no representation among older adults (see Figure 3).
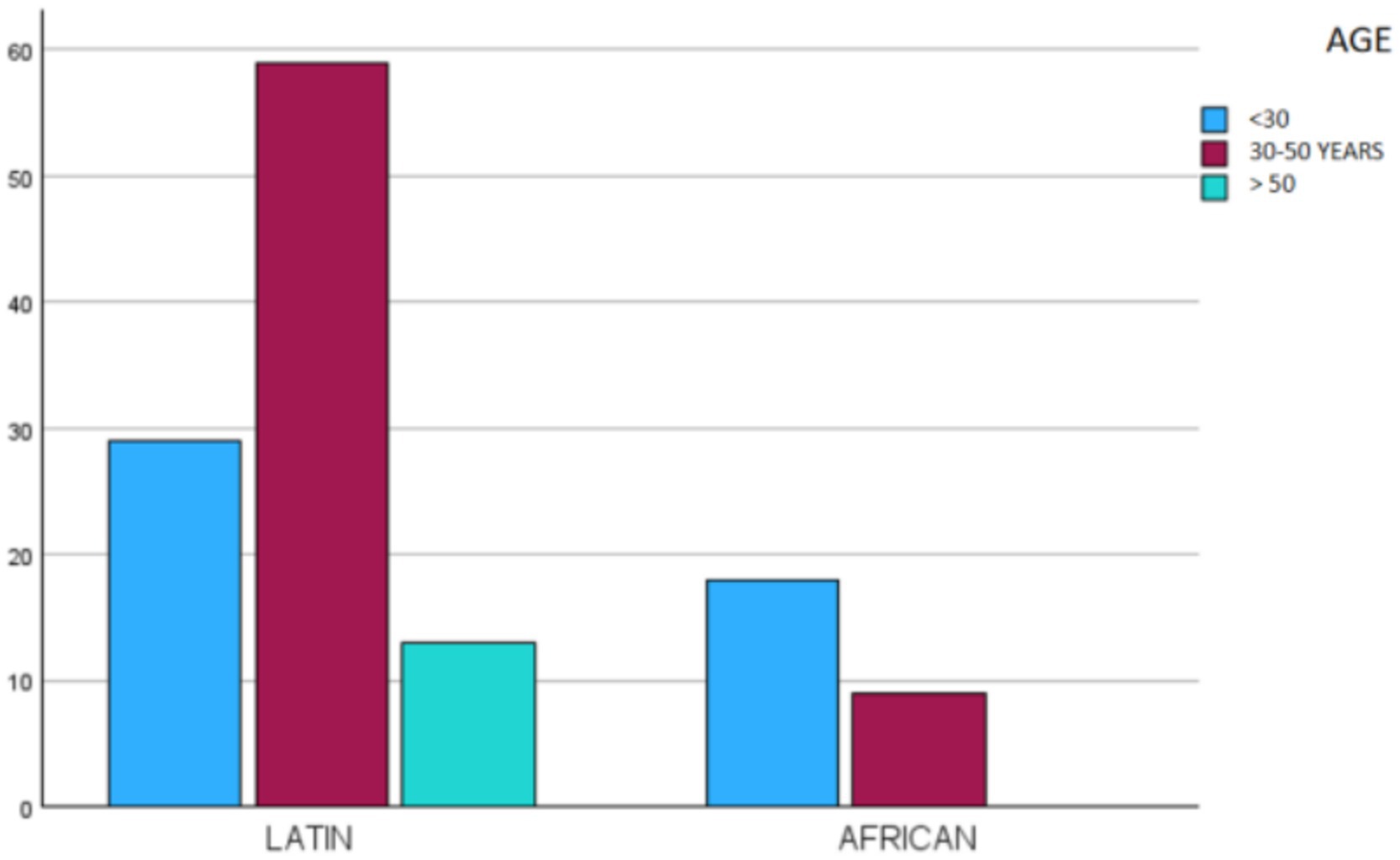
Figure 3. Distribution of the sample by age and place of origin.
4 Discussion
Migration is one of the most defining phenomena of our century. Population movements driven by inequalities between countries—and more recently, by political persecution or armed conflicts—have given rise to groups in extreme need and pockets of poverty and marginalization that receiving countries must manage and address. This study can only be understood within such a current and socially, economically, and culturally significant context as that of migration (12).
If we aim to design effective intervention strategies to improve the overall health—and, specifically, the oral health—of these populations, we must first understand their changing nature. For this reason, ongoing epidemiological studies such as this one are necessary and will continue to be essential. International migration patterns have shifted considerably in recent years, leading to a deeper understanding of the diversity among migrants—previously regarded as a fixed pattern tied to particular ethnic groups (21).
Focusing on our immigrant population at the CETI in Melilla, one of the first striking findings was the origin of the participants. Given the geographical location of the center, it would be expected that most of its users would be of African origin. However, of the 128 individuals surveyed, 103 (80.5%) were Latin American and only 25 (19.5%) were African. To understand this phenomenon, we must consider the history of the CETI, which, since its founding in 1999, has predominantly hosted African migrants.
Traditionally, refugees came from Algeria, Morocco, Mali, Guinea, Cameroon, Nigeria, Chad, Angola, Gabon, the Democratic Republic of the Congo, Niger, Zimbabwe, Ivory Coast, and many other sub-Saharan countries (25). In 2011, the Syrian civil war brought a large influx of Syrian refugees to the center (26). More recently, Latin American migrants have discovered that entering the CETI can help accelerate the bureaucratic process required to obtain residency in Spain. For this reason, many Latin American migrants already residing in the country in irregular situations are now arriving en masse, which explains the large number of Colombian and Venezuelan individuals among those surveyed (27).
The sex and age distributions found in our sample are consistent with the findings of other authors, with a higher proportion of young or middle-aged men and fewer women or older adult individuals (28). However, there was a statistically significant difference (Chi-square, p < 0.05) in the ages of migrants when comparing Latin Americans with Africans: the 30–50 age group was most frequent among Latin Americans, while the 18–29 age group was most frequent among Africans. Notably, there were no individuals over 50 among the African participants. This may be explained by the fact that many Latin Americans already have relatives established in Spain, which means that many respondents may be arriving to reunite with their families. Since almost all African migrants come from sub-Saharan countries, they must cross the entire Sahara Desert under harsh conditions to reach Melilla. This results in a migration composed of young people, which is why there are no individuals over the age of 50 of African origin in our sample (29).
One of the key issues to address is socio-health inclusion. Migration can lead individuals to lose access to even the most basic health care. In many cases, the harsh living conditions they are forced to endure significantly worsen their health status—including oral health—thereby hindering their integration into the host community. Temporary stay centers, such as the CETI, which provide individualized socio-health care, aim to reduce these disparities. As a result, migrants’ integration into receiving communities is improved, and potential rejection on health-related grounds is minimized (21).
With respect to oral health and associated behaviors, the data obtained in this study deviate from those of earlier research (25, 28, 29). Regarding diet, it is clear that sugar consumption is high. As explained in the results section, many participants may not be fully aware of their own consumption, introducing a bias in the survey results. Nonetheless, no significant differences were observed based on origin or gender.
The good oral hygiene reported by the participants is noteworthy, with an average brushing frequency of 2.35 times per day. This differs from previous reports by other authors (28, 30) and may be attributed to the origin of the surveyed populations. When comparing Latin Americans and Africans, statistically significant differences were found (Chi-square, p < 0.001) in favor of Latin Americans, who accounted for 80.9% of those brushing twice daily and 89.1% of those brushing three times daily. Notably, none of the Latin American respondents reported not brushing at all.
Another striking finding is that while 40.6% of participants reported gingival bleeding during brushing, only 3.1% reported having visited a dentist for periodontal treatment, and only 22% had sought restorative treatment. This is noteworthy considering the high prevalence of both pathologies according to the literature (15, 30). Gingival bleeding should be a clear indication for seeking dental care, as it may signal the presence of gingivitis or periodontitis—conditions that, if left untreated, can lead to tooth loss. Such a low rate (3.1%) of periodontal treatment suggests a lack of awareness, limited access, or low prioritization of oral health. The fact that only 22% of individuals had received restorative treatment further implies that many cases of dental caries are likely going untreated, thereby exacerbating long-term oral health issues. These findings may reflect a normalization of oral discomfort and a tendency to seek care only in acute or critical situations, while ignoring symptoms that should prompt preventive or early intervention.
The prevalence of smoking was not particularly high, with only 33% of participants reporting the habit, and among these, 53% smoked fewer than five cigarettes per day. However, there was a statistically significant difference between men and women, with a higher proportion of male smokers (Chi-square, p < 0.01).
Similarly surprising was the level of dental care received: nearly 60% of the surveyed individuals had visited the dentist within the last year, despite their status as migrants. Only 6.3% reported never having visited a dentist, and these were almost entirely of African origin. Differences in the time since the last dental visit were statistically significant between Latin Americans and Africans (Chi-square, p < 0.001), but not between men and women. Perhaps the lack of health awareness in this African population is the cause of this significant difference.
Another point of interest is the discrepancy between the need for prosthetic treatment and actual prosthesis use. Despite good hygiene habits and the relatively high number of teeth retained, 67% of the participants were partially edentulous, while only 9.4% used prosthetic devices.
Other dental health indicators—such as fluorosis, enamel opacities, erosion, or trauma—did not represent significant health problems due to their low prevalence.
The mean DMFT index (Decayed, Missing, and Filled Teeth) was 9.73, with values ranging from 0 to 27. This figure is considerably higher than that reported in the general population of the host country (19, 31). As this index explores the individuals’ history of dental caries, it is evident that the number of caries (treated or untreated) among the immigrant population is significantly higher than that of the host country’s population.
All of these epidemiological data—and those that may be gathered in future studies of immigrant populations—are essential for understanding these constantly evolving groups. They must be analyzed with the aim of reducing the health inequities, particularly in oral health, that these migrant populations face (10). This knowledge should also be complemented by a comprehensive understanding of the host country’s healthcare system and how to facilitate access to it for migrants, thereby promoting better integration and health outcomes (10).
5 Conclusion
This study reveals that the migrant population at the CETI in Melilla faces significant oral health challenges, including high rates of caries, tooth loss, and low use of dental prostheses, with notable differences by geographic origin. Despite generally adequate oral hygiene habits, poor oral health highlights gaps in access to preventive and therapeutic dental services.
Strengths include the use of standardized WHO methods and consideration of social determinants, allowing comprehensive analysis. Limitations involve a small sample size, cross-sectional design, and potential self-report bias. Health programs should focus on equity-based public health interventions, oral health education, improved access to dental care, and tailored treatments. Temporary centers can be key sites for preventive programs to reduce inequalities and support social integration.
Future research should include longitudinal studies to monitor oral health trends and qualitative studies on cultural, economic, and structural barriers. Intersectoral collaboration is essential for effective, sustainable strategies addressing the diverse needs of Melilla’s migrant population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Odontologia Social Foundation Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JM: Methodology, Conceptualization, Writing – original draft. IB: Writing – review & editing, Data curation, Conceptualization. DR: Writing – review & editing, Methodology, Investigation. PV: Methodology, Writing – review & editing, Investigation. JB: Investigation, Writing – review & editing, Software, Formal analysis, Methodology. DR-P: Data curation, Conceptualization, Writing – original draft, Writing – review & editing. AC: Writing – review & editing, Visualization, Resources.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1641311/full#supplementary-material
References
1. World Health Organization. Constitution of the World Health Organization [internet]. (1948). Available online at: http://www.who.int/gb/bd/PDF/bd46/s-bd46_p2.pdf (Accessed 14 October, 2007).
2. World Health Organization. Educación para la salud: manual sobre educación sanitaria en atención primaria de salud. Ginebra: Organización Mundial de la Salud (1989).
3. Swann, BJ, and Obadan, EM. Programas de Odontología Social de la Universidad de Harvard (EEUU) In: Odontología preventiva y comunitaria: la odontología social: un deber, una necesidad, un reto (2012). 771–84.
4. O’Connell, JJ, Oppenheimer, SC, Judge, CM, Taube, RL, Blanchfield, BB, Swain, SE, et al. The Boston health care for the homeless program: a public health framework. Am J Public Health. (2010) 100:1400–8. doi: 10.2105/AJPH.2009.173609
5. Sentell, T, Shumway, M, and Snowden, L. Access to mental health treatment by English language proficiency and race/ethnicity. J Gen Intern Med. (2007) 22:289–93. doi: 10.1007/s11606-007-0345-7
6. Fiscella, K, and Sanders, MR. Racial and ethnic disparities in the quality of health care. 37, Annual Review of Public Health. Annual Reviews Inc.; (2016). p. 375–394. doi: 10.1146/annurev-publhealth-032315-021439
7. Nelson, LP, Getzin, A, Graham, D, Zhou, J, Wagle, EM, McQuiston, J, et al. Unmet dental needs and barriers to care for children with significant special health care needs. Pediatr Dent. (2011) 33:29–36.
8. Castaño-Seiquer, A. Odontología Social: Un Proyecto Iberoamericano Para El Mundo. Diputacion Huelvade, editor. Huelva: Diputación Provincial de Huelva. Servicio de Publicaciones; (2017).
9. Castaño Seiquer, A, and Ribas Pérez, D. Odontología preventiva. Conceptualización y generalidades In: Odontología preventiva y comunitaria: la odontología social: un deber, una necesidad, un reto, Editor “Fundacion Odontologia Social”. Seville. Spain (2012). 31–7.
10. Narvai, PC, Castaño Seiquer, A, and Doldan Lema, J. “Los desafíos de la odontología.” Manual de introducción a la odontología. Madrid, Spain: Ripano; (2005). p. 277–280.
11. Northridge, ME, Kumar, A, and Kaur, R. Disparities in access to oral health care. Annu Rev Public Health. (2020) 41:513–35. doi: 10.1146/annurev-publhealth-040119-094318
12. Dziedzic, A, Riad, A, Tanasiewicz, M, and Attia, S. The increasing population movements in the 21st century: a call for the E-register of health-related data integrating health Care Systems in Europe. Int J Environ Res Public Health. (2022) 19:3720. doi: 10.3390/ijerph192113720
13. Achotegui, J. Emigrar hoy en situaciones extremas. El síndrome de Ulises. Aloma: Revista De Psicologia, Ciències De l’Educació I De l’Esport. (2012) 30:79–86.
14. Celentano, DD, and Szklo, M. Gordis epidemiology. Amsterdam, The Netherlands: Elsevier Health Sciences (2018).
15. Pabbla, A, Duijster, D, Grasveld, A, Sekundo, C, Agyemang, C, and van der Heijden, G. Oral health status, oral health behaviours and oral health care utilisation among migrants residing in Europe: a systematic review. J Immigr Minor Health. (2021) 23:373–88. doi: 10.1007/s10903-020-01056-9
16. Muller, R, Bilich, L, and Jones, M. Impact of an oral health education program on the oral health literacy of refugees. J Immigr Minor Health. (2024) 26:699–710. doi: 10.1007/s10903-024-01594-6
17. Fernández, G, Comité, M, De La, T, and Foessa, F. Conclusiones principales del VII Informe sobre exclusión y desarrollo social en España 2014. Almogaren. (2015) 56:49–70.
18. Bravo Pérez, M, Almerich Silla, J, Canorea Díaz, E, Casals Peidró, E, Cortés Martinicorena, F, Expósito Delgado, A, et al. Encuesta de salud oral en españa 2020. ROCE. (2020) 25:12–69.
19. De Sanidad M. Informe Anual del Sistema Nacional de Salud 2023 Informes, Estudios E Investigación, Madrid, Spain (2024).
20. Hernandez-Donadeu, M, Ribas-Pérez, D, Rodriguez Menacho, D, Villalva Hernandez-Franch, P, Barbero Navarro, I, and Castaño-Séiquer, A. Epidemiological study of oral health among children and adolescent schoolchildren in Melilla (Spain). Healthcare (Switzerland). (2023) 11:2086. doi: 10.3390/healthcare11142086
21. Martín-Cano, MdC, Sampedro-Palacios, CB, Ricoy-Cano, AJ, and De La Fuente-Robles, YM. Superdiversity and disability: social changes for the cohesion of migrations in Europe. Int J Environ Res Public Health. (2020) 17:6460. doi: 10.3390/ijerph17186460
22. Ribas-Pérez, D, Sevillano Garcés, D, Rodriguez Menacho, D, Hernandez-Franch, PV, Barbero Navarro, I, and Castaño Séiquer, A. Cross-sectional study on oral health-related quality of life using OHIP-14 in migrants children in Melilla (Spain). Children. (2023) 10:1168. doi: 10.3390/children10071168
23. Kizi, G, Raquel Barata, A, Ventura, I, Flores-Fraile, J, Ribas-Perez, D, and Castaño-Seiquer, A. Oral health in migrants children in Melilla, Spain. Children. (2023) 10:888. doi: 10.3390/children10050888
24. Ferreira-Alfaya, FJ. Inequalities in health literacy between European population and newly arrived male sub-Saharan migrants in Europe. Health Promot Int. (2024) 39:129. doi: 10.1093/heapro/daae129
25. Riatto, SG, Montero, J, Pérez, DR, Castaño-Séiquer, A, and Dib, A. Oral health status of Syrian children in the refugee center of Melilla, Spain. Int J Dent. (2018) 2018:2637508. doi: 10.1155/2018/2637508
26. World Health Organization. Oral health surveys basic methods. 5th ed (2013). Geneva, Switzwerland: WHO.
27. Luque Revuelto, RM, and Moreno Muñoz, D. Nuevas dinámicas migratorias en la Colombia del posconflicto: entre el desplazamiento forzado, la inmigración venezolana y la COVID-19. Revista de Geografía Norte Grande. (2024) 88:1–24. doi: 10.4067/S0718-34022024000200114
28. Lauritano, D, Moreo, G, Carinci, F, Campanella, V, Della Vella, F, and Petruzzi, M. Oral health status among migrants from middle-and low-income countries to Europe: a systematic review. Int J Environ Res Public Health. (2021) 18:12203. doi: 10.3390/ijerph182212203
29. Salas-Coronas, J, Cabezas-Fernández, MT, Lozano-Serrano, AB, Soriano-Pérez, MJ, Vázquez-Villegas, J, and Cuenca-Gómez, JÁ. Newly arrived African migrants to Spain: epidemiology and burden of disease. Am J Trop Med Hyg. (2018) 98:319–25. doi: 10.4269/ajtmh.17-0604
30. Rad, SAB, Oliveira, ME, Maklennan, A, Castiglia, P, and Campus, G. Higher prevalence of dental caries and periodontal problems among refugees: a scoping review. J Glob Health. (2023) 13:04111. doi: 10.7189/jogh.13.04111
Keywords: oral health, health inequities, migrant populations, epidemiology, Melilla, Spain
Citation: Martín Hernández J, Barbero Navarro I, Rodríguez Menacho D, Villalva Hernández P, Barrera Mora JM, Ribas-Pérez D and Castaño Séiquer A (2025) Social determinants of oral health in migrants at the Spanish border. Front. Public Health. 13:1641311. doi: 10.3389/fpubh.2025.1641311
Edited by:
Allison Squires, New York University, United StatesReviewed by:
Cristina Belén Sampedro Palacios, University of Jaén, SpainDaniel Granada, Federal University of Santa Catarina, Brazil
Beatriz Costas-Rodriguez, Carlos Albizu University, Puerto Rico
Copyright © 2025 Martín Hernández, Barbero Navarro, Rodríguez Menacho, Villalva Hernández, Barrera Mora, Ribas-Pérez and Castaño Séiquer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Ribas-Pérez, ZHJpYmFzQHVzLmVz