 Xuesong Yang
Xuesong Yang Yuyan Ling2
Yuyan Ling2- 1Institute of Safety Production Theory and Standards, China Academy of Safety Sciences and Technology, Beijing, China
- 2School of Emergency Management and Safety Engineering, China University of Mining and Technology-Beijing, Beijing, China
Background: China has the largest construction workforce in the world but faces severe occupational health challenges. Coping behaviors related to occupational health risks (CBOHR) are key to mitigating these hazards but remain understudied.
Materials and methods: A cross-sectional survey of 484 construction workers was conducted to assess Capability, Opportunity, Motivation, and Behavior using the COM-B model. Structural equation modeling (SEM) was employed to test mediating pathways, and association-rule mining (ARM) was used to identify determinants of high- and low-level CBOHR.
Results: The results showed that the COM-B framework—comprising three modules (Capability, Opportunity, and Motivation) with 15 behavior change domains, and a Behavior module with eight specific CBOHRs—demonstrated satisfactory fit, reliability, and validity. Bootstrapping confirmed that Motivation fully mediates the relationship between Capability and Behavior and partially mediates the relationship between Opportunity and Behavior. ARM further identified key domains associated with high and low levels of CBOHR.
Conclusion: Strongly correlated item sets identified through association rule analysis revealed domains strongly linked to both high (and low) levels of each CBOHR. This study is the first to integrate the COM-B model with data mining in the context of occupational health, highlighting “motivation–values–policy” as actionable levers for CBOHR interventions. The findings provide preliminary evidence to support the development of scalable worker health programs.
1 Introduction
Work-related health risks faced by workers in the construction industry stem from a wide range of occupational hazards, such as noise, dust, heat, musculoskeletal disorders (MSDs), and work stress (1–4). The large scale of the construction industry presents many obstacles to the prevention of health damage in this sector, especially in developing economies such as China, where rapid urbanization and infrastructure development have led to a huge number of construction projects (5). However, currently, the temporary nature of construction projects and the large number of migrant workers make it inevitable that immediate safety concerns take precedence over long-term health concerns, due to cost constraints and limited access to medical services (6).
Unlike the control of unsafe behaviors, where managers' accomplishments can be assessed based on certain indicators, such as the frequency of accidents and incidents (5, 7). Health-risking behaviors occur often in the workplace and may go unnoticed by both employees and supervisors. There are no explicit documents to police or monitor workers' self-protective health measures in China's construction sector. For instance, OHS supervisors are unlikely to notice if a worker does not wear a mask or fails to take precautions to protect physical health at work. On the other hand, a worker who does not wear a helmet at work may receive a warning or even a penalty (8). That is, chronic health problems do not lead to disputes over rights and responsibilities between the organization and the individual and may not affect the direct interests of the company. Despite everyone agreeing to further protect workers' health, few companies take this step, especially for frontline workers.
Various factors contribute to work-related ill health, such as unavoidable occupational hazards, organizational management issues, government regulations, and personal lifestyles, in which individual self-management of occupational health is easily overlooked. The competence of workers to adopt efficient risk-coping behaviors when confronted with occupational health hazards can be interpreted as worker health self-management. Notably, when construction workers are faced with occupational health risk challenges, they often do not choose to take proactive action in coping (9, 10). Coping behaviors related to occupational health risk (CBOHR) are complex, with changing risk scenarios, yet integrated behavior change theories have often been overlooked in behavior change efforts. For interventions of risk-coping behavior change, construction workers remain an understudied occupational group who address health damage from occupational health hazards through self-response.
There is currently a knowledge gap in how more complex factors of behavior change determine effective coping when construction workers are faced with occupational health risk situations. The Theoretical Domains Framework (TDF) was considered to systematically determine barriers and facilitators of CBOHR. It explained the factors on health-related behavior change (11, 12). In addition, for data mining of the behavior change model, association rules appear to be a useful tool for problem-solving. Data mining approaches using association rules have been utilized to identify crucial influencing elements by discovering valuable associations concerning the outcome variables (13, 14). This technique can assist researchers in more precisely identifying the critical elements that lead to high-level or low-level coping behaviors. This enables a deeper understanding of the factors that facilitate or impede coping behavior change. To address the dilemma of occupational health management for construction workers, classical statistical modeling coupled with association rule data mining may offer a guide for worker health behavior interventions.
The goals of this study are to address the present gap in CBOHR among construction workers. (1) A literature review was conducted to identify potential determinants of CBOHR for construction workers from domains connected to behavior change and to formulate hypotheses. (2) Measurement tools for CBOHR-related constructs were developed for this study based on the scientific scale development methods. (3) Establishing a model for CBOHR and using quantitative analysis to identify predictors of target behaviors and effect pathways among modules. (4) Based on the association rule approach, strong associations between high-level behaviors and low-level behaviors were extracted to further understand the essential factors of CBOHR. The method this paper employed was coupling the hypothesis-testing” paradigm with the association rule technique to accurately identify determinants and mechanisms of CBOHR, which can help managers and practitioners to develop more scientific intervention strategies.
2 Literature review
2.1 Coping with occupational health risk
2.1.1 Occupational health risk
Health risk represents the process by which exposure to risk factors leads to disease burden, ultimately enabling the identification of convincing causal relationships between risk–outcome pairs–that is, the derivation of risk factors from their attributable health consequences (15). Occupational health risk assessment and occupational health risk management are the two main components of the scientific field of occupational health risks (16). The former focuses more on quantitative or qualitative calculations of objective health risks from exposure to hazards using deterministic or uncertainty analysis (17–19). Risk management is the adoption of a series of control measures in response to the existence of risks, which may be from organizational and individual behaviors (20, 21). Health-risk factors were divided into five main categories through reviewing published global studies on occupational health management of construction workers, namely, physical hazards, chemical hazards, behavioral hazards, psychological hazards, and biological hazards, which accounted for approximately 51.4%, 19.5%, 15.4%, 12.0%, and 1.7% of research attention, respectively (22). Through epidemiological surveys, construction workers had a significantly higher risk of work-related diseases, especially respiratory, skin, and musculoskeletal diseases, than workers in other industries (23). In addition, the incidence of work-related substance abuse, sleep disorders, psychiatric disorders, and mania had risen significantly for young construction workers (24). Studies on health risks of construction workers are mainly based on epidemiological surveys and psychometric paradigms (i.e., validated questionnaire-based measurement), with epidemiological surveys mainly including physiological functional data by cohort, controlled as well as cross-sectional studies (25–29); questionnaires, scales, and interviews involved in psychometric paradigms are commonly used (10, 30, 31). The last decade has seen the rise of approaches combining subjective psychometric paradigms with intervention trials, simulation experiments, and data mining techniques (14, 32–34). Since health risks are inherently uncertain, future research should focus on improving the accuracy of data collection and analysis, and more fine-grained metrics for risk should be developed to streamline the knowledge structure of occupational health management.
2.1.2 Coping with risks
People evaluate the risk when they become aware of a threat or danger, and they respond by adopting specific activities or procedures to cope with the risk scenario (16, 35). Coping was defined as “changing cognitive and behavioral efforts to manage specific external and/or internal needs” and was guided by two core concepts, approach and avoidance, in the context of stressors, for example, that are oriented either toward or away from threat (36–38). Adopting a response is usually done in a dynamic change of risk perception; however, because the generation of coping tendencies is intra-individual and subjective, there have not been many studies specifically on how construction workers cope with occupational health risks (9). Risk perception is a highly individualized aspect of risk management that frequently serves as a crucial connection to risk management programs. Risk perception is a mental construct, often shaped by cognitive biases, that plays a critical role in shaping responses to risk and serves as a crucial connection to effective risk management programs (39). The field of health risk coping primarily focuses on coping tendencies or competencies related to intra-individual characteristics and external stimuli, with an emphasis on explaining the mechanisms that generate coping responses to health challenges through a psychological paradigm (40–42). The scale of COPE that was developed in 1989 separated 13 conceptually distinct subscales, which were further divided into problem-focused coping and emotion-focused coping (43). COPE is still a useful tool for researching how people respond to health challenges and issues, particularly how the public and medical professionals cope with health risks during the COVID-19 pandemic (44, 45). Coping skills are usually related to personality, experience (or knowledge), and social and environmental influences (46). For construction workers‘ risk-coping competence, occupational safety was given more importance, indicating that research should focus more on coping with occupational health risks. The exploration of the mechanisms of the construction workers' health risk coping model should be facilitated based on conventional coping-related theories and research information in other fields of health risk.
2.1.3 Coping behavior of health risk
The majority of research on construction worker health management focused on risk factors and health intervention strategies from an organizational perspective (47–49). Such studies have regarded these responses as health-protective behaviors. The purpose of health-protective behaviors is to achieve desirable health outcomes. In the studies of health behavior, it was classified as preventive health behaviors (actions taken to avoid illness or injury) and sick-role behaviors (actions taken after diagnosis of a medical problem to restore good health or to prevent further disease progress) (50), or as frequent and infrequent behavior (51). Based on the frequency of behavior implementation, health behaviors are further classified more broadly: frequent preventive behaviors, for example, lifestyle; infrequent preventive behaviors, including disease screening and health assessment; and disease management behaviors, including prevention and control of disease progression (52). Protective motivation (intention) (53), health literacy (54), personality attributes [responsibility (55), optimism (56), and so on], and self-efficacy (57), to varying degrees, play a distinct role in preventative health-protective behaviors when faced with high health risks. In terms of occupational health protective behaviors, they should be considered as preventative health-protective behaviors (both frequent and infrequent prevention) mainly aiming at preventing the incidence of occupation-related ill health and increasing the wellbeing of workers. Further research is necessary to determine, in occupational health settings, the person variables that make behavior occur or change.
The viewpoint of our research is that health-protective behavior is more appropriately called the coping behavior of occupational health risk (CBOHR) in occupational health. This highlights the specific health effects of occupational hazards in the workplace and emphasizes the countermeasures taken to prevent these damages. Many health-protective behaviors are appropriately used for daily health maintenance or health promotion. In the workplace environment of construction workers, however, health damage caused by occupational hazards must be different from that in daily life. Taking measures to cope with the risks brought by occupational hazards and thereby protecting their own health from damage is considered a key component of workers' competence for occupational health self-management.
2.2 COM-B model of behavior change
2.2.1 Theoretical domains framework
In order to clarify the theoretical understanding of behavioral change processes, 61 experts from the fields of psychological theory, health services research, and health psychology developed a consensus set of key theoretical constructs (Theoretical Domains Framework, TDF), consisting of 12 domains, which was published in 2005 (12). A group of behavioral scientists who were unaware of the original framework domains then assessed the validity of the domain framework through an empirical base and reordered the 112 unique theoretical constructs, resulting in a 14-domain framework (11). The TDF, which was a framework rather than a theory, was created through expert consensus categorization and compilation of 128 component constructs from 33 theories pertinent to behavior-related implementation issues. Its purpose was to assist users in identifying the critical factors influencing behavior change. Over 800 peer-reviewed articles employing this framework have been published in Web of Knowledge in the past decade since its initial design was made available (58). The description of the domains and theoretical constructs in the TDF is shown in Supplementary Table S1.
The framework was developed to make the many behavior change theories more comprehensible to the interdisciplinary audiences involved in implementation and can be used to understand the barriers and facilitators of behavior change in a range of settings, facilitating the development of behavior change techniques and the design of interventions (59). The initial application of the TDF was to qualitatively and quantitatively analyze the behavior change among healthcare practitioners, which has been widely used in the clinical field. Thus, more research is needed on healthcare practitioner-specific barriers and facilitators of behavior. As TDF research is growing, more researchers are attempting to apply it across a wide range of behavioral interventions, such as occupational safety behavior change (60, 61), physical activity (62), and safety behaviors related to patients (63). Designing questionnaires based on TDF may be a quicker option to pinpoint the key factors of behavior change in a larger sample (64).
2.2.2 COM model
Construction workers are confronted with a multitude of work-related health issues, and their coping behaviors may exhibit overlapping and transformative characteristics. Consequently, health risk-coping behaviors have not received adequate scholarly attention. Furthermore, the lack of authoritative measurement tools and behavioral capture methodologies has posed a series of obstacles to conducting in-depth scientific research on health interventions for construction workers. Behavior change theories can explain coping behavior and interventions based on theories that aim to promote work-related health and wellbeing (40, 65, 66). Behavior change interventions aim to target the prevalence or incidence of particular behaviors in specified populations. A large number of studies rely on specific theories; however, a more integrative cross-theoretical approach should be employed to explore a wider array of constructs as potential behavioral determinants, thereby increasing the likelihood of a successful intervention. The determinations of behavior change were summarized and reorganized in the TDF, but without further theorizing their interactions, leading to the proposal of a new behavior change model framework (termed the “COM system”) containing three key modules: Capability, Opportunity, and Motivation (67). A theoretical model of behavior change was formed by mapping the TDF domains to the COM-B system. The three fundamental conditions of Capability (ability), Motivation, and Opportunity that affect behavior were frequently included in the study of behavioral effects as a global model, derived from the integration of multiple behavioral theories (68–70). The COM-B model has the advantage of mapping the domains in the TDF in its system and serving as the theoretical core of a behavioral intervention pattern that takes into account comprehensiveness, coherence, and a clear link to an overarching behavioral model (67).
After a decade of growth, the COM-B model framework is currently the foundation for an increasing amount of behavior change research, which continues to develop its potential in many fields.
An increasing body of research has explored healthcare practitioner-specific barriers and facilitators of behavior change across a wide range of clinical situations, such as protective behaviors for oral and dental health (71, 72), management of patient health behaviors (73, 74), and medication use or treatment decision-making (75, 76), and often identifying validated variables as key explanatory factors. Additionally, in some practices of public health, researchers are interested in investigating the efficacy of behavior change intervention models. Examples of these areas of practice include specific behavior interventions for children or adolescents (77, 78), physical activity and exercise (79, 80), family health care behaviors (81, 82), control of unhealthy lifestyle behaviors (such as smoking cessation, weight management, and d substance abuse) (83–86), and behavior of environmental protection (87, 88). Numerous studies have applied the COM-B model to workplace health-promoting behaviors. For instance, interventions targeting sedentary behavior among office workers (89, 90) demonstrated that the COM-B model predicted sitting behavior more effectively, albeit marginally, than competing single models in terms of variance explained (91). The COM-B model also appeared beneficial for understanding occupational safety behaviors, such as explaining the low rate of helmet use among farmers operating machinery (92) and ways to improve the appropriate use of personal protection equipment (PPE) by ward staff during the COVID-19 pandemic (93). Many studies used this model to demonstrate that capability and opportunity are associated with target behaviors through the mediating effect of motivation, and they are also directly associated with behavior to some extent.
The COM-B model framework has proven its excellent performance in many fields (non-clinical medicine), and its applications are likely to become more widespread in the future. It has seldom been taken into account in the current field of behavior change of occupational health, and it is necessary to introduce this integrated model for construction workers. The constructs in the COM-B model that facilitate and hinder these behaviors must therefore be used to identify the important factors underlying CBOHR. However, existing COM-B research has yet to disentangle the differential impacts of “capability–motivation” vs. “opportunity–motivation” on low-resource workers.
2.3 Association rule mining
Association rule analysis, originally proposed by Agrawal, yielded notable findings from market basket data and has since become a classic example in data mining (94). The primary concept behind this approach was to use an effective algorithm to mine the association rules between sets of items in a large basket of data (items bought by a customer over a period of time in a supermarket) to form the antecedent (X) and infer the consequent (Y), typically expressed as “X → Y.” The most important parameters in the algorithm included Support, Confidence, and Lift, and the results that satisfy these parameters at the same time are considered valuable rules (95).
In the research field of occupational health and safety, association rule mining (ARM) methods were acceptable and provided powerful scientific data to support safety or health improvement. The analysis of the connections between illness absence and lifestyle, as well as medical outcomes among 6,010 employees of a Japanese telecommunication company, was conducted using ARM, and the findings provided valuable guidance for avoiding sickness absence at work (96). The investigation of variables affecting retired athletes' levels of life satisfaction and loneliness by transforming questionnaire data into binary attributes and using a tree-based frequent item set mining method to discover association rules demonstrated greater validity (97). ARM was used to explore the relationship between healthcare workers' level of awareness, preparedness to manage suspected patients, and case-management training received, using multicenter and cross-sectional data in 59 countries during the COVID-19 pandemic, providing proof in favor of increased training opportunities (98). Female homeworkers' health concerns were frequently disregarded, even though they confront major health and safety challenges, while ARM can assist managers to discover factors that impact female homeworkers' exposure to occupational ill health (99). ARM has also become a popular approach in the field of occupational safety research, particularly in the prevention of workplace accidents and incidents. ARM techniques were used to discover cause-and-effect patterns of steel plant accidents from accident investigation data (100) and to explore correlations among human factor events in nuclear power plants, improving a weight association rule based on statistics (101). Cross-sectional data from questionnaires or interviews, as well as injury and incident data recorded, were utilized in research on construction accident prevention to extract novel insight into construction occupational safety using ARM techniques (102–105). There was a clear connection between construction accident prevention and unsafe behaviors, with various unsafe behavior categories frequently being associated with various accident outcomes (106). The mechanisms influencing construction workers' unsafe behaviors were complex and multifactorial, and the correlations among the characteristics of unsafe behaviors had been studied based on ARM (107). ARM through questionnaire data was a new attempt in occupational health and safety in the construction industry, which seems to explain cause-and-effect patterns well (14).
2.4 Research hypothesis
In this study, we initially conducted the design and testing of the Capability, Opportunity, Motivation, and Behavior (target behaviors) as subscales separately. Next, these four modules were integrated into the COM-B model for the quantitative analysis of the roles of Capability, Motivation, and Opportunity in influencing construction workers' risk-coping behaviors.
Although the TDF/COM-B framework has been validated in the fields of healthcare and lifestyle, its applicability in the occupational health context of construction workers still faces two major gaps: (i) high onsite mobility and cultural heterogeneity, which may undermine the effect of social norms; and (ii) cross-sectional evidence that focuses solely on safety behaviors, without examining the dynamic mechanisms of health risk management. Therefore, this study proposes hypotheses H1–H5 to validate the convergent and predictive validity of the COM-B framework in this context.
Hypothesis 1 (H1). Capability is positively and directly associated with coping behavior.
Hypothesis 2 (H2). Opportunity is positively and directly associated with coping behavior.
Hypothesis 3 (H3). Motivation is positively and directly associated with coping behavior.
Hypothesis 4 (H4). Capability is positively indirectly associated with coping behavior through motivation as a mediator.
Hypothesis 5 (H5). Opportunity is positively and indirectly associated with coping behavior through motivation as a mediator.
3 Materials and methods
3.1 Design of the scale
3.1.1 Generation of items
The items in the Capability and Motivation were referenced to the dimensions mapping under the theoretical domain framework of behavior change to the COM-B model. This is an exploratory study about occupational health-related behaviors of construction workers attempting to make a clear behavior change mechanism through the COM-B model. Morgan introduced the TDF to the measurement of occupational safety behaviors and developed a safety behavior change questionnaire that was valuable to our study (60). Safety and health behaviors at work share overlapping and similar characteristics, linked together through occupational risk (108). Therefore, we adopted Morgan's process for obtaining research evidence on safety behavior change mechanisms based on the TDF. Through publications based on TDF-related questionnaires or interviews, on-site surveys of projects under construction by our research team, and the status of occupational health management of construction workers, we designed the initial items within domains in TDF. And then they were mapped to modules, respectively (Supplementary Table S2).
3.1.1.1 Capability
In the “COM-B” system, Capability was seen as an essential factor of behavior generation. It was defined as “an individual's psychological and physical capacity to engage in the activity concerned”. For occupational health behavior of construction workers, capacity encompasses knowledge, skills, and behavioral habits. Physical capacity is a requirement for a construction worker to be able to get the job, so there is not much physical capacity to consider in occupational health behaviors. We merged knowledge and skills into one construct because construction workers' knowledge and skills regarding occupational health protection are not easily distinguishable. Therefore, under the Capability module, we divided into three latent variables as domains, consisting of four constructs of TDF: “behavioral regulation,” “memory, attention and decision processes,” and “knowledge and skills.” Under each domain, we designed four related preliminary items. The flowchart of subscale development of Capability is shown in Figure 1. Figure 1 delineates a seven-step, empirically validated procedure for constructing the COM-B-based scale, representing a mature scale-development workflow.

Figure 1. Flowchart for developing the COM-B-based scale.
3.1.1.2 Motivation
Motivation was considered to be composed of habitual processes, emotional responding, and analytical decision-making, which mainly reflect the direct energy for behavior at the level of individual thought. Motivation has been mentioned in many behavioral theories, and the COM-B model incorporates constructs from relevant behavior change theories. We used seven domains as latent variables, i.e., “emotion,” “social/professional role and identity,” “beliefs about capabilities,” “beliefs about consequences,” “intentions,” “reinforcement,” and “optimism.” The domain called Goals was not well-suited for construction workers' health behaviors in occupational activities, because there are few specific goals for health promotion. Four initial items were designed for each domain. The flowchart of subscale development of Motivation is shown in Figure 1.
3.1.1.3 Opportunity
Unlike Capability and Motivation, which were intrinsic drivers of behavior change, Opportunity acted as an external force for the individual to influence behavior. Opportunity included physical and social factors afforded by environment and culture, respectively, and was defined as “factors that lie outside the individual that make the behavior possible or prompt it”. In the COM-B model, the module of Opportunity was composed of two domains, “Environmental context and resources” and “Social influence”. We embedded the occupational health culture scale (OHCS) that had already completed in a published study into Opportunity (this scale contains environmental components), including the five domains of “values” (3 items), “leadership support” (5 items), “policies and norms” (5 items), “physical environment” (4 items), and “employee involvement” (4 items) (109). Culture exists as an external factor, but it has to be reflected through the subjective psychological feelings of individuals so that the authenticity and accuracy of the measurement can be ensured. Therefore, we employed OHCS instead of the Opportunity subscale to complete the measurement (the integrated theoretical COM model framework shown as Figure 2).

Figure 2. Integrated COM model framework.
3.1.1.4 Target behavior
Target behavior was regarded as the dependent variable in this study. The module of behavior was not developed as a subscale because there was no consensus research on the domain delineation of health behaviors among construction workers. Experienced measurement methods used to assess risk-coping behaviors in occupational health for construction workers have rarely been explored. Therefore, many studies have exemplified protective behaviors in occupational health that are unique to construction workers or frequently engaged during their operations. We mainly cited the risk coping behaviors of occupational health for construction workers, summarized by Liu et al. (9). To more scientifically measure the level of construction workers' behaviors, we synthesized eight specific behaviors based on publications, on-site research, and interviews with experienced construction workers. Identifying the target behaviors was a key step in the TDF approach and the outcome variable studied in the COM-B model, which provided a basis for exploring the determinants that facilitate and impede the occurrence of the behaviors. After forming these target behaviors, we conducted a stakeholder consultation, which was similar to some of the methods used to develop questionnaires based on TDF. In order to support the improvement of these items of behavior, comments of experts were adopted (60, 110). The types of eight target behaviors are as follows: medical insurance (Behavior 1, BEH-1), usage of protective equipment (Behavior 2, BEH-2), maintaining ventilation (Behavior 3, BEH-3), physical examination (Behavior 4, BEH-4), avoiding rest and eating in the workplace (Behavior 5, BEH-5), good interpersonal/social relationship (Behavior 6, BEH-6), avoiding musculoskeletal disorders (Behavior 7, BEH-7), and avoiding cold-related or heat-related illness (Behavior 8, BEH-8) (9).
3.1.2 Optimization of items
We have established a fifteen-member group of experts in the fields of health promotion, occupational disease prevention, behavioral science, OHS management, and scale development, including researchers from scientific institutions, OHS managers, industrial hygiene engineers, and occupational health physicians. We convened a panel of experts to refine the scale. For example, frontline field experts believed that the concept of “resources available on the site” might be unclear to construction workers. Therefore, the questionnaire should rephrase the description of these resources to ensure clarity. Formal written language was used in the publication; however, in the questionnaire, some colloquial adaptations could be made appropriately to align with the Chinese language habits while ensuring that the meaning remains intact. As a result, replacing the phrase “I can use some equipment or resources to cope with occupational health risks” with “I can cope with occupational health risks in some ways” would help workers make more accurate choices.
Moreover, at the pre-testing phase, we used the cognitive interview method, which was also adopted and recommended in questionnaire development (111, 112). Fifteen construction workers with over 100 years of experience on construction sites were selected to discuss the design of the items with our researchers. A report of our design and measurement purpose was given to them, allowing them to assess the content validity and reliability of the questionnaire. We obtained the interviewees' feelings about answering the questions and their suggestions for the items.
3.2 Sample
In 2021, our research team launched a project called “Standardization of Occupational Health Management in Construction Projects“ with a regional company of a large real estate group in China. At two of the company's construction projects (large residential projects) in southwestern China in May 2021, researchers of this study administered the COM-B questionnaire to a random sample of 450 workers, receiving 409 valid questionnaires. In September 2021, questionnaires were distributed to 79 female construction employees, and 75 valid responses were collected. Participants were included based on the following criteria: able to understand and complete the questionnaire; aged between 18 and 70 years; in good physical condition; and with no history of occupational disease. All workers signed the consent form and completed the study instruments in writing. There were no ethical issues in this survey, and each respondent signed a privacy agreement (the demographic results were presented in Supplementary Table S3).
3.3 Data analysis
3.3.1 Statistical analysis
Two subscales, Capability and Motivation, were used for exploratory and confirmatory factor analysis, respectively. We divided the sample (n=484) into two parts, with the first half (sample 1) used for exploratory factor analysis (EFA) and the second half (sample 2) used for confirmatory factor analysis (CFA). Before conducting exploratory factor analysis, we analyzed the sample for inter-item and total item correlations, requiring that the total item correlation for each item not be < 0.5.
In the exploratory factor analysis, this study used principal component factor analysis with the varimax rotation eigenvalue criterion > 1.0 to detect the latent variables. Before identifying the latent variables, we verified the feasibility of factor analysis by using the Kaiser-Meyer-Olkin (KMO) test and Bartlett's sphericity test. Typically, factor analysis is more suitable when the KMO value exceeds 0.8 and the Bartlett's sphericity test p < 0.01. And then, items are determined to be retained or removed through factor loadings and cross-loading. In general, the factor loadings should be >0.5 and only in one of the domains (items with cross-loadings >0.5 should be eliminated or modified).
After completing the exploratory factor analysis, we validated the fit results for the domain (factor structure). The confirmation factor analysis of this paper was similar to Morgan's approach, which developed a safety behavior change questionnaire based on the TDF, presenting the CFA in more detail in their study (60). In this process, the exclusion of unsuitable items was made by the modification index (M.I.). The absolute fit index contains chi-squared/degree of freedom (χ2/df), goodness-of-fit index (GFI), adjusted for the model's degrees of freedom (AGFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). The relative fit index contains the normal fit index (NFI), the Tucker-Lewis Index (TLI), and the comparative fit index (CFI). Both IBM SPSS 24.0 and IBM AMOS 25.0 were used to complete the exploratory factor and validation factor analysis. In addition, the convergent validity was expressed by the average variance extracted (AVE), and an AVE >0.5 indicates acceptable convergence. The Cronbach's alpha coefficient is usually used to characterize internal consistency of the scale items, with a value between 0 and 1, and the larger the value, the higher the reliability, with 0.70 being an acceptable threshold. The composite reliability (CR) value >0.7 represents an appropriate construct reliability.
3.3.2 Model analysis
The next process was to construct the COM-B overall model and analyze the fit by structural equation modeling (SEM) based on a hypothetical model framework. According to the previous hypothesis, Capability, Opportunity, and Motivation have an effect on CBOHR, and Motivation, meanwhile, acts as a mediator. We performed a structural equation modeling analysis using the maximum likelihood estimation in IBM AMOS 25.0 to observe the influence of the components on the target behavior. Then, the mediating effects analysis was conducted using a bootstrapping approach in Amos software. Indirect effects were assessed using n = 5,000 bootstrap re-samples. They were tested for significance after correcting for 95% bias, and the confidence interval (bias-corrected 95% CI and percentile 95% CI) did not include zero.
3.3.3 Association rule analysis
3.3.3.1 Data preprocessing
To investigate an association between diverse CBOHR and domains of behavior changes, the Association Rule Mining (ARM) technique was used to explore the co-occurrence relationship. Data preprocessing was performed to transform the data into a scale and descriptive statistics suitable for ARM. We transformed the quantitative scores of the scales into “High (H),” “Middle (M),” and “Low (L)” qualitative categorizations, respectively. Tercile splits were not considered in this work because, according to our sample normality tests (kurtosis and skewness), the mean scores are clustered around 3, which could result in a very small sample being included in the association analysis (113). Therefore, domains were classified into three degrees: average score < 3 As “low,” 3 ≤ average score < 4 as “medium,” and average score ≥ 4 as “high.” According to the five-point Likert scale we employed, scores of 1 and 2 were negative responses. Although a score of 3 was a positive response, it was usually considered to be close to a neutral response and did not accurately capture the mental attitude of the respondent. Scores of 4 and 5 can be considered as positive responses with a strong attitude.
3.3.3.2 Parameter and rule setting
The significance of association rules is to discover useful rules above the threshold of a set parameter. Setting reasonable parameters is essential for discovering valuable rules. The Apriori algorithm is an optimized classical algorithm that has been widely used and aims to construct frequent item sets using an iterative method on horizontal search. It was found that a minimum support of 5% has high data mining efficiency (94). Similar findings were obtained in the study of Li et al. (14), and their work transformed the questionnaire data into qualitative categories labeled “high” and “low” as well. The minimum parameters were set according to the research expectation and the scale of the data. When the rules satisfy the requirements of minimum Support, Confidence, and Lift (shown in Equations 1–3) at the same time, the strong rules are considered available. Strong rules will be filtered out, and occurrence patterns within strong rules will be analyzed.
4 Results
4.1 Factor analysis for subscales
4.1.1 Subscale of capability
In the subscale of Capability, the first exploratory factor analysis yielded four latent variables with eigenvalues greater than one, accounting for 73.18% of the total variance. The KMO test for sampling adequacy was 0.886, and the Bartlett test for sphericity was highly significant (p < 0.001). By observing the inter-item and item-total correlations of 12 items, we eliminated items with correlation coefficients < 0.5. Two items (KS3 and DM1) were eliminated because their modified item-total correlations were 0.199 and 0.105, respectively.
Following varimax rotation, the component matrix of the factor structure revealed that KS-3 and DM-1 loaded onto a newly extracted factor. Within this factor, KS-3 had a factor loading of −0.534 and demonstrated a cross-loading of >0.5 (specifically, 0.607) with the “Behavioral regulation” dimension. In contrast, DM-1 had a strong factor loading of 0.817; however, its content showed no substantive conceptual alignment with KS-3. This suggests that DM-1 does not satisfy the theoretical or conceptual criteria necessary to be grouped with KS-3 under the same latent construct, as shown in Supplementary Table S4.
Confirmatory factor analysis was employed to assess the degree of fit between the observed data and the conceptual model. We modified the three-factor model according to the modification index (M.I.) values. BR3 had the highest M.I., and considering that each domain maintained the same number of items, BR3 was removed. The results indicated a good model fit for the latent variable of Capabilities. Model fit indices before and after modifications are shown in Supplementary Table S5.
For modified models, the Cronbach alpha coefficient and CR of each factor exceeded the threshold of 0.70, and the corrected item-to-total correlations were all >0.5, meaning good internal consistency reliability (Table 1). The square root of AVE exceeds the domain correlation, and therefore, the domains presented convergent and discriminant validity, as shown in Table 2.

Table 1. Factor loading results for the subscale of capability.

Table 2. Correlations between factor structures for the subscale of capability.
4.1.2 Subscale of motivation
There were nine latent variables with eigenvalues greater than one in the exploration factor analysis, and their total variance was 70.98%. The KMO test for sampling adequacy was 0.868, and the Bartlett test for sphericity was highly significant (p < 0.001). Item-total, factor loadings, and cross-loadings were likewise used to determine whether the existence of items was appropriate to the scale. In this process, seven items were removed, which were from seven domains. Factor loadings of OP2 and EM3 were < 0.5. INT3 and BCA2 formed a new latent variable, whereas these two items had poor relevance in regard to item content. BCO3 and SR4 formed an uncorrelated latent variable, with a factor of < 0.5 for BCO3; therefore, this latent variable was excluded. Given that a latent variable should involve no less than three items, and the factor loadings are < 0.5 for BCO3, a latent variable formed by BCO3 and SR4 was excluded. While REI3 had acceptable loading factors, the item-total correlation was 0.306, which was also a judgment for item elimination.
The next work confirmed the seven-factor model of Motivation using AMOS 25.0 and put the calculation in Supplementary Table S5. We did not make any modifications to this model because its fit was adequate. Reliability tests on the subscale of Motivation obtained internal consistency reliability, as shown in Table 3. The results of convergent and discriminant validity were calculated as shown in Table 4. These results demonstrated that the subscales of Motivation have reasonable reliability and validity.
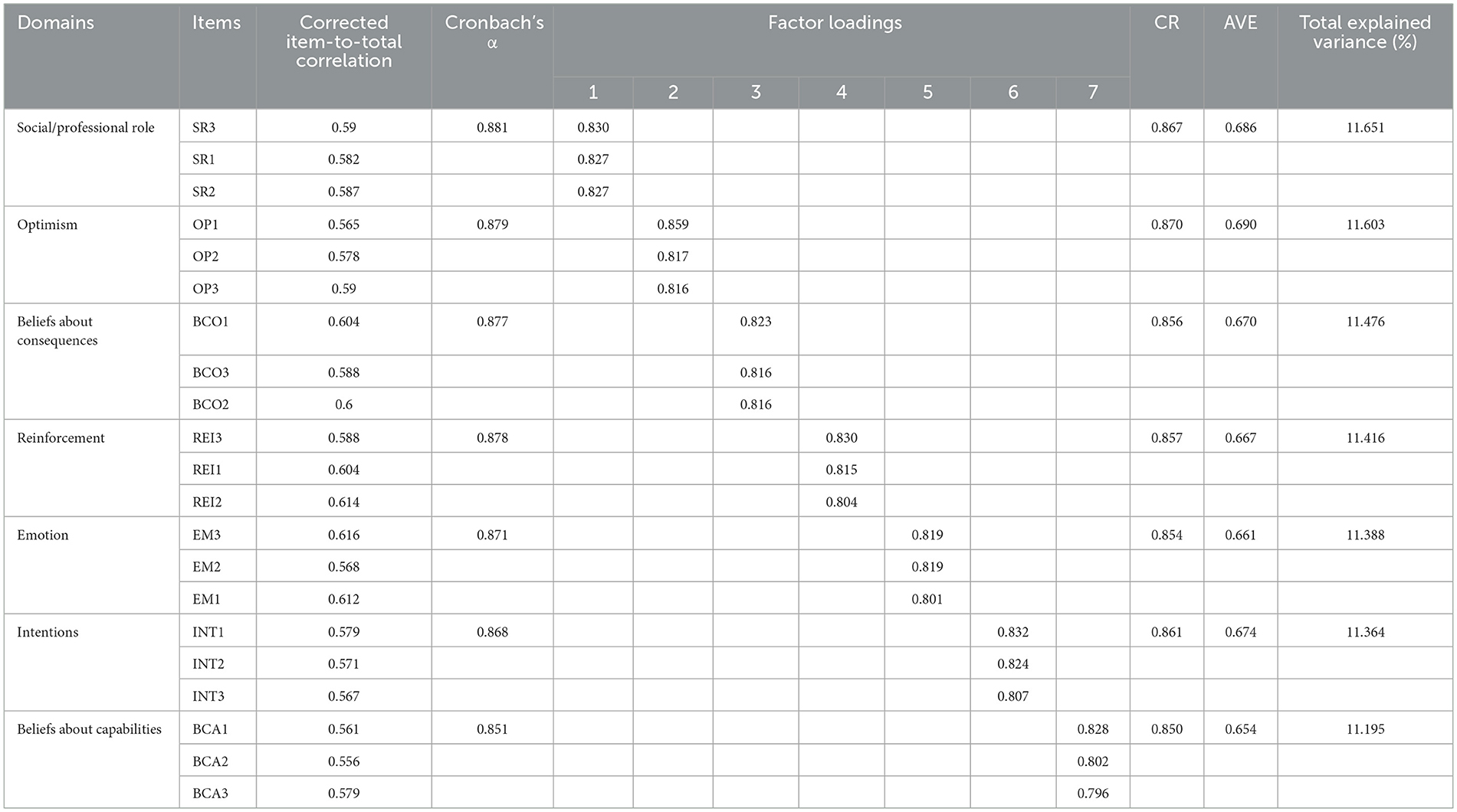
Table 3. Factor loading results for the subscale of motivation.

Table 4. Correlations between factor structures for the subscale of motivation.
4.2 Confirmation factor analysis of the model
Through hierarchical confirmation factor analysis and items removed by statistically unreliable indicators, Capability and Motivation as second-order factor models (latent variables) had been shown to have good reliability and validity. We had developed the subscale of Opportunity in the previous study, so this module was only tested with a factor model, and the reasonable fit results are shown in Supplementary Table S1. The results of the global COM-B model indicated that the fit was acceptable: χ2/df = 1.196, GFI = 0.885, AGFI = 0.874, NFI = 0.908, TLI = 0.983, CFI = 0.949, RMSEA = 0.00, and SRMR = 0.035. The results of the factor loadings, AVE, and CR calculations for the second-order latent variables are shown in Table 5. Only the second-order latent variables of the Motivation subscale had an AVE value close to the acceptable threshold (AVE = 0.482), while all other second-order latent variables exhibited AVE values within a broader acceptable range. It might be because Motivation encompasses a relatively large range of constructs containing seven domains. Moreover, the influence of Motivation was very complex, and it is reasonable that there are some biases in respondents' understanding and reflection of motivation.

Table 5. CR and AVE values for second-order latent variables.
The validation results of the structural equation model designed according to the COM-B model framework are shown in Figure 3. Capability, as a second-order latent variable, had little direct effect on Behavior (β = −0.04, P = 0.378) and was not statistically significant. Therefore, hypothesis 1 was not valid. The direct effect of Opportunity as a second-order latent variable on Behavior was positive and statistically reliable (β= 0.26, p < 0.001), and hypothesis 2 was supported. Motivation had the most significant direct positive effect on Behavior (β= 0.41, p < 0.001), as the strongest indicator in the COM construct, and thus hypothesis 3 was also supported. Within the inner COM model, the direct positive effect of both Capability and Opportunity on motivation was 0.21 (p < 0.001) and 0.18 (p < 0.001), respectively. For the test of mediating effects of Motivation (hypotheses 4 and 5), n = 5,000 bootstrap replicate sampling results can be inferred by bias-corrected 95% CI and percentile 95% CI results (Table 6). It was statistically significant that Motivation was a mediator of both the paths for Capability to Behavior and Opportunity to Behavior, respectively. Notably, Motivation fully mediated the relationship between Capability and Behavior, as the direct effect of Capability on Behavior was not statistically significant. In addition, Motivation served as a partial mediator in the pathway from Opportunity to Behavior. These findings support Hypotheses 4 and 5.

Figure 3. Confirmation factor analysis and path coefficients of the COM-B model.

Table 6. Mediating effect test of motivation.
4.3 Association rules from data mining
This study positioned ARM as an exploratory data description tool for identifying co-occurrence patterns among variables, rather than for causal inference or hypothesis testing. A preprocessed dataset was conducted using Apriori ARM, according to the set parameters (minimum Confidence was 50%, minimum Support was 5%, Lift > 2) (14). A total of 123,324 association rule results were obtained by this set of parameters. These rules are categorized into eight specific CBOHR into “BEH-1 = H (High)” to “BEH-8 = H” and “BEH-1 = L(Low)” to “BEH-8 = Low”, for a total of 16 partitions. Items containing M (Middle) in each behavior partition were eliminated because we expected to get high-scoring domains associated with high-scoring behaviors and low-scoring domains associated with low-scoring behaviors. Middle-scoring domains and behaviors were excluded since the effect of these on behavior was insignificant. For BEH-2 = L, BEH-3 = L, and BEH-6 = L, we retained the domain with the highest score (M) because these domains had too few rules (13, 7, and 9 rules, respectively). Furthermore, for the domain of values inside Opportunities, the scores were only M and H, and therefore, we regarded M as L in this domain. After eliminating the middle-scoring domains, the final 3,028 rules remained. Their Support and Confidence distributions were shown in Figure 4. In each behavioral partition, the Support was mostly distributed in the interval of 5%−10%, and the Confidence distribution was concentrated in the interval of 50%−70%. The rules within the high-scoring behavioral partition were well above those within the low-scoring ones.
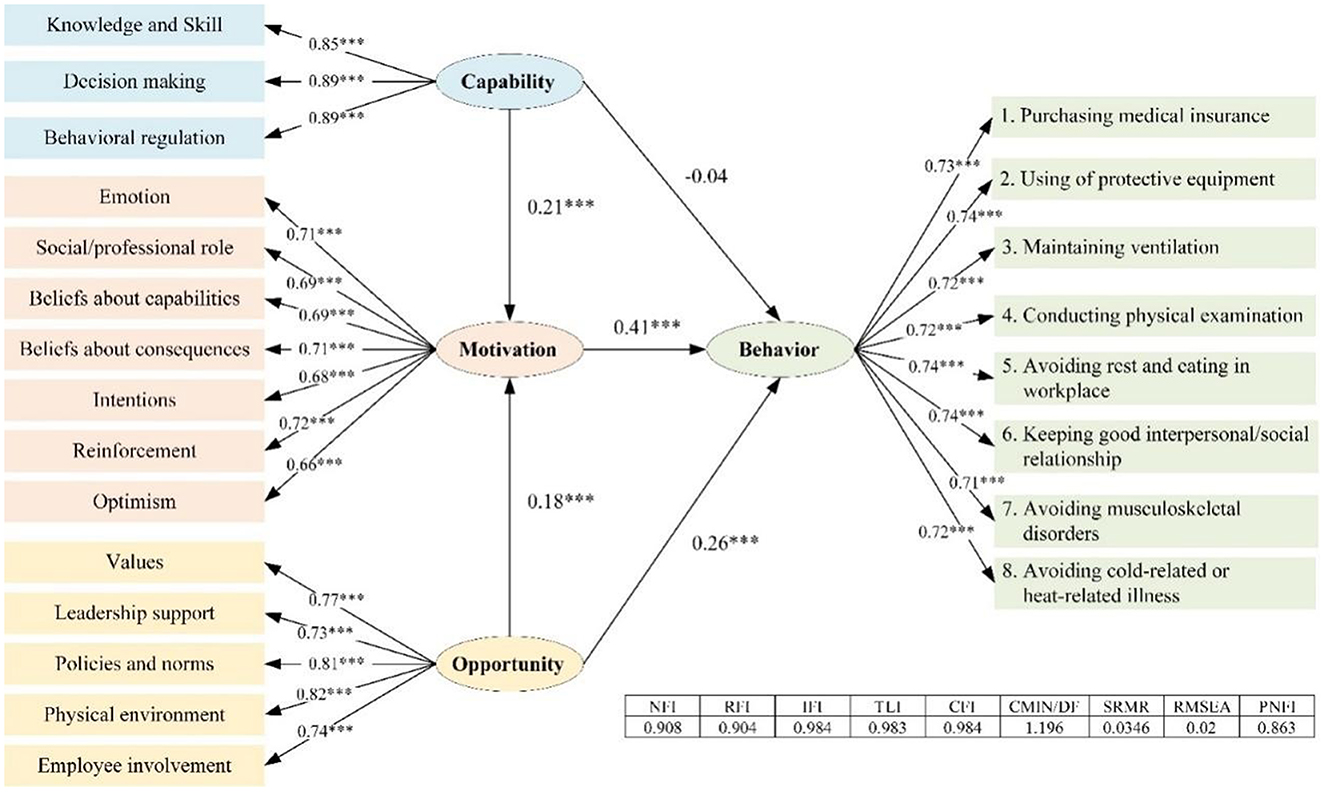
Figure 4. Support and Confidence distribution of association rule analysis results for behavior. ***P < 0.001.
Next, we performed further rule extraction based on the Lift. Lift, an essential indicator in association rules, represents the concurrence frequency and relevance of domains (shown in Equation 3). According to Lift, the rules distributed in the 16 behavioral partitions were ranked, and we defined the top ten of Lift in each partition as strongly associated rules.
Figure 5 showed the strong association domains for each behavioral partition when the BEH = H were available. In partitions with BEH = H, the strongly associated sets had at least three domains. Interestingly, the set of strongly correlated domains for each partition with BEH = H almost always contains VAL (Values) and PN (Policies and norms), which came from the Opportunity. In Motivation, the occurrence in the strongly associated sets varied in different Behavior partitions, and Supplementary Table S6 showed the frequency distribution of domains in the strong associated rules with BEH = High. For high-scoring behavioral partitions, the strongly correlated domains in Opportunity were PN and VAL. In addition, the strongly correlated domains from Motivation had significant differences. For example, for BEH-1=H, the strongly correlated domains in the Motivation were SR, REI, OP, and INT, while those for BEH-2=H were SR, BCO, and EM (domains appeared at least five times in 10 strong correlation rules). This can, at the same time, explain to some extent part of the reason for the low AVE of Motivation in the confirmation factor analysis of the COM-B model, which, of course, cannot be perceived as statistical validation. Also, the extent to which different domains in Motivation played an influential and mediating role may be at different levels for each CBOHR.
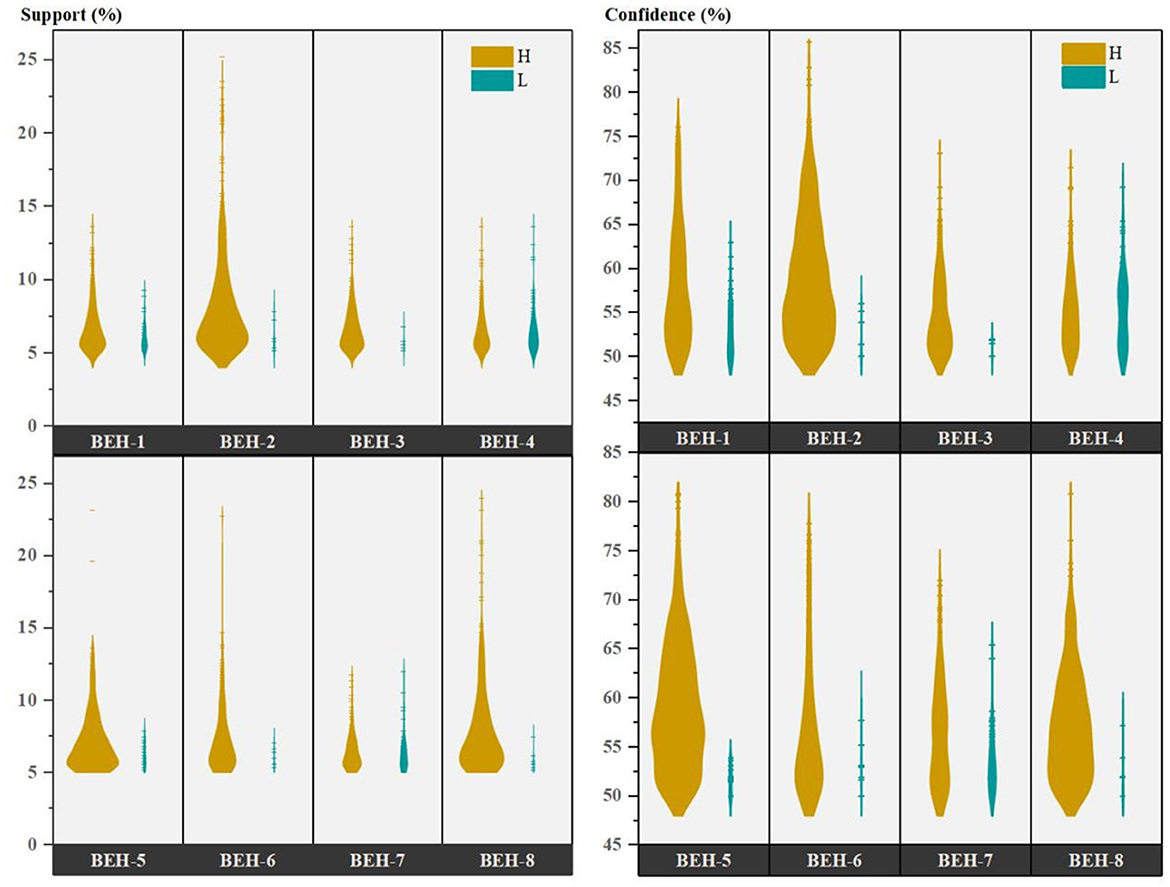
Figure 5. Strong association rule filtered from behavior = high.
For low-scoring behaviors, the strong association domains for each behavioral partition exhibited distinct association characteristics compared to high-scoring ones (Figure 6). Supplementary Table S7 presents the frequency distribution of domains in strong association rules about BEH=L. The domains in Capability demonstrated a strong association with l BEH = L, which was not found in the strong association rules for BEH = H. It illustrated that low levels of CBOHR have a strong correlation with respondents' low Capability level. The sets appearing in Opportunity, other than VAL and PN, have PE as another frequent domain, indicating that BEH = L had a strong correlation with PE = L. The domains in Motivation appeared significantly less frequently than those where the behavior partition was high. This might be related to the fact that far fewer association rules that were above the required parameter threshold yielded in the low-scoring behavior partitions than in the high-scoring behavior partitions.

Figure 6. Strong association rule filtered from behavior = low. For BEH-2=L, BEH-3=L, and BEH-6=L, we retained the domain with its score was M because there were too few rules inside these domains, which were 13, 7, 9 rules respectively.
The analysis of these association results can inform interventions aimed at changing CBOHR. Traditional structural equation modeling (SEM) has been effective in identifying and predicting the effects of dependent variables (behaviors) and explaining the variance accounted for by latent variables. Quantitative analysis within SEM can reveal the path coefficients between second-order latent variables (modules). However, evaluating the relationship between first-order latent variables (domains) and outcome variables becomes challenging, particularly in complex global models. ARM provides a complementary approach, combining semi-quantitative and semi-qualitative methods to enhance or support statistical interpretation. Moreover, ARM can help identify the determinants of target behavior change from a qualitative perspective, enabling more precise identification of crucial elements for behavior intervention.
5 Discussion
5.1 Mediating effect for motivation
5.1.1 Mediating effect of capability on behavior
As shown in the results of the hypothesis test, there was no statistically significant direct effect from Capability to Behavior. Capability refers to the process of identifying and comprehending exposed occupational hazards through knowledge, skills, memory, and behavior management habits, all of which are encompassed within the Capability component. These elements are essential for managing occupational health risks in the workplace. Risk information is then processed during the cognitive risk phase, which involves both Capability and Motivation, as these factors directly influence the formation of risk-coping decisions. Therefore, we can assume that the individual chain evolution process for information processing of occupational health risk and coping implementation follows the following pattern: “identifying → cognizing → deciding → coping” (Figure 7).

Figure 7. Individual chain evolution process for information processing of occupational health risk.
In the sets of strongly correlated items where BEH=H (high behavior level), no domains from Capability appeared frequently. However, in the sets of strongly associated items, BEH, L, DM, KS, and BR appeared with varying degrees of frequency. For example, in the CBOHR partition related to “purchasing health insurance”(BEH-1), “KS = L” was strongly correlated with low-scoring behavior, suggesting that limited knowledge and skills (KS) may serve as a barrier to BEH-1. Within the Motivation category, SR and REI showed the strongest associations with BEH-1. For insurance-related activities and healthcare services, it is important to educate workers and provide clear guidance on how to maximize available healthcare resources at minimal cost. Interventions targeting OP and INT should be effectively combined with enhancements to KS, such as through clear communication about the availability and importance of health insurance services. Ensuring that workers are aware of the benefits—and have access to and confidence in using them—is essential for improving uptake and behavioral outcomes.
5.1.2 Mediating effect of opportunity to behavior
The main concepts of Opportunity were social influence and environmental resources. Opportunity may not be involved at the beginning of the individual chain evolution process for information processing of occupational health risk and coping implementation, because there was no relevant evidence for the relationship between Opportunity and Capability in this research. The results of the structural equation modeling research, however, demonstrated that Opportunity may affect cognition, decision, and coping at the same time (Figure 7). In the health promotion (health protective behavior enhancement) model framework, interpersonal (social) influences as well as environmental influences were parallel with specific behavioral cognitions (Motivation), on the premise that personal factors were being considered at the forefront (114). Among the results of the association analysis, the strong association sets for BEH = H, PN, and VAL were the most remarkable Opportunity-based domains. They served as the strongest association domains of excellent CBOHR performance, but the engagement domains from Motivation were different for different types of behaviors. As a result, fostering positive values among construction workers was crucial to the success of CBOHR, and it was important to communicate the health concept of companies to employees. Moreover, PN was a key factor in promoting workers' CBOHR, especially for behaviors like the usage of protective equipment (BEH-2). BCO appeared in high frequency in the sets of strongly correlated partitions for BEH-2 = H and BEH-2 = L, indicating that the belief about consequence was critical in Motivation. To overcome the barriers to the usage of protective equipment by construction workers, it was important to reinforce their clear understanding of the effects of the equipment and let them know that adopting these measures can help them prevent negative health outcomes.
5.2 The significance of this research
5.2.1 Contribution of the data results to objectives
Programs that promote worker health require sustained investment and long-term commitment. From the perspective of benefits, employers often do not have a positive attitude toward such initiatives, as substantial efforts cannot be immediately rewarded, and minimal efforts cannot be penalized (115). From the point of view of responsibility, factors such as high employee mobility and the cumulative nature of health damage over time make it difficult to hold employers accountable for work-related ill health, particularly in the construction sector, where workers frequently change employers. This reduces financial incentive for employers to invest in preventive health measures (116). From the viewpoint of performance, there were many determinants of worker health promotion, in addition to the fact that the desired effects may not occur in the short term and a lack of methods to make a measurable link between beneficial measures and performance (117). From the perspective of ownership, there were almost no medical personnel dedicated to managing workers' health on construction sites, and the involvement of managers was limited to superficial approaches. Staff felt it was more appropriate to hand over health management to health professionals (115).
Failure of adequate emphasis on occupational health management or epidemiological information management was seen as a barrier to OHS success (118). Therefore, an excellent OHS management system involves the adoption of preventive measures to reduce work-related risks by proactive action to improve workers' health, safety, and satisfaction. In China, it is extremely clear that the process for managing occupational health has gaps and that managers lack occupational health knowledge. Additionally, it is believed that the solution to this problem lies in the necessity for employees to develop a personal sense of accountability for health-related concerns. Especially at this stage of development, as seen in China, it is crucial to strengthen employees‘ own occupational health management to achieve maximum health risk reduction with the least amount of financial expenditure. Of course, employers and the government must continue to strengthen their functions and responsibilities while also improving the level of occupational health self-management among workers as a supporting role. This research can help behavior change practitioners understand the domains in which to implement interventions and build continuous intervention programs when they are aware that workers are lacking in a certain CBOHR habit. Furthermore, the research can provide evidentiary support for targeted intervention domains that correlate to distinct levels of behavior because overcoming behavioral difficulties is a sustained and phased process.
5.2.2 Innovativeness of the method
Quantitative research by questionnaire can efficiently measure barriers and facilitators to the presence of CBOHR in construction workers and design applicable intervention programs through the theoretical domain framework of behavior change. Adopting a psychometric paradigm based on psychophysical scaling and multivariate analysis techniques can produce representations of individuals‘ internal attitudes on the effects of target behaviors. This approach is more likely to be adopted by managers and supervisors responsible for improving workers' health behavior on construction projects.
SEM can systematically identify facilitators and barriers; however, the results did not clearly highlight the most influential indicators within the COM constructs. In complicated models involving numerous variables, conventional statistical methods, such as correlation analysis, linear regression analysis, and SEM, may produce unstable or ambiguous conclusions, as they operate within a “hypothesis-testing” paradigm focused on confirming predefined effects among modules. As a result, findings from these statistical methods may not fully capture the intricacies of psychological and organizational management challenges. Data mining techniques, which are well-suited to analyzing large datasets with numerous variables, might provide a potential solution. By qualitatively processing questionnaire data, ARM could infer relationships between factors that are difficult to quantify or impossible to describe. This study innovatively combines the commonly used SEM with ARM techniques, which proved more effective in identifying key factors and mechanisms underlying CBOHR. The combination of quantitative and qualitative analyses may be more effective in assisting managers, practitioners, and researchers in designing CBOHR intervention plans that are scientifically grounded and more responsive to workers' evolving needs.
5.3 Limitation
There is currently no applicable scale for assessing the Capability, Motivation, and Behavior modules in the context of construction worker health. Therefore, we followed a conventional method by splitting the sample data into two parts for exploratory and confirmatory factor analyses, respectively. Measurement bias might exist in preliminary scales that had not undergone multi-case or large-sample validation. However, the scale's measuring function was partially supported by validity assessments conducted by occupational safety and health experts in the construction field. In addition, a sizable number of construction workers and related occupational health managers in the field participated in this research. The satisfactory reliability and validity results further support the scale's performance. The next step involves undertaking a larger range of research to confirm the scale's generalizability. This will also improve the questionnaire, equipping decision-makers in the construction industry with the necessary resources to gather more comprehensive research evidence for intervention adoption. The goal of this research was to provide decision-makers in occupational health improvement in the construction industry with the tools that obtain more comprehensive research evidence on intervention implementation.
This study did not validate the interaction between Capability and Opportunity. Similar to most studies that apply the unified framework of Capability, Opportunity, and Motivation, we treated the domains of Capability and Opportunity as parallel initial variables. Personal factors such as knowledge, memory, and experience can be transmitted to each other through interpersonal influences, which may exist within the group. However, one of our previous studies showed that, just like Chinese occupational groups such as miners and construction workers with high mobility, interpersonal influences among colleagues were not demonstrated. This did not confirm whether other domains of Opportunity (or culture) had an impact on the individual's ability. Therefore, this unexplored area may be worth exploring.
Occupational health risk factors regarding construction workers are numerous and may overlap with safety risk factors, making coping behaviors sometimes ambiguous or sometimes singular. The eight behaviors we screened may not provide complete coverage of construction workers' CBOHR in the workplace and thus are not considered representative. The purpose of this study was to investigate the mechanisms influencing CBOHR change in construction workers using the COM-B model combined with ARM. Considering the types of projects that may be necessary for subsequent project-based CBOHR studies, this paper aims to provide both theoretical and evidential support for intervention implementation.
6 Conclusion
This study empirically validates the COM-B framework within the occupational health context of Chinese construction workers for the first time. These findings extend the generalizability of COM-B beyond clinical and lifestyle settings, establishing a psychometrically robust instrument for assessing construction-specific capability, opportunity, and motivation.
The integration of COM-B with ARMRM demonstrates a transferable workflow: practitioners can rapidly identify culture-specific levers (values and policy norms) and design low-resource interventions without the need for longitudinal data. This proof-of-concept positions the framework as a ready-to-use toolkit for industry stakeholders seeking to reduce the occupational disease burden across diverse construction settings.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Author contributions
XY: Methodology, Conceptualization, Investigation, Writing – original draft. YLin: Investigation, Software, Data curation, Writing – original draft. LW: Writing – review & editing, Data curation, Validation. YLi: Investigation, Writing – review & editing. MZ: Supervision, Funding acquisition, Writing – review & editing, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by grant [No. 2025JBKY18] Basic Scientific Research Program of the China Academy of Safety Science and Technology and by grant [No. 52074302] from the National Natural Science Foundation of China and by grant [No. 2024EMST121201] from the Key Science and Technology Program of Ministry of Emergency Management of the People's Republic of China.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1643332/full#supplementary-material
References
1. Chong D, Chen L, Peng Y, Yu A. Occupational noise-related perception and personal protection behavior among Chinese construction workers. Saf Sci. (2022) 147:105629. doi: 10.1016/j.ssci.2021.105629
2. Jonsson E, Järvholm B, Andersson M. Silica dust and sarcoidosis in Swedish construction workers. Occup Med. (2019) 69:482–6. doi: 10.1093/occmed/kqz118
3. Minna S, Mika N. Relationship between construction workers' musculoskeletal disorders and occupational health service activities. Work. (2012) 41:3753–6. doi: 10.3233/WOR-2012-0676-3753
4. Wu X, Li Y, Yao Y, Luo X, He X, Yin W. Development of construction workers job stress scale to study and the relationship between job stress and safety behavior: an empirical study in Beijing. Int J Environ Res Public Health. (2018) 15:2409. doi: 10.3390/ijerph15112409
5. Qi H, Zhou Z, Li N, Zhang C. Construction safety performance evaluation based on data envelopment analysis (DEA) from a hybrid perspective of cross-sectional and longitudinal. Saf Sci. (2022) 146:105532. doi: 10.1016/j.ssci.2021.105532
6. Jones W, Gibb A, Haslam R, Armstrong J. Raising the bar for occupational health management in construction. Proc Inst Civil Eng-Civil Eng. (2019) 172:183–90. doi: 10.1680/jcien.19.00029
7. Zhou Z, Goh YM, Li Q. Overview and analysis of safety management studies in the construction industry. Saf Sci. (2015) 72:337–50. doi: 10.1016/j.ssci.2014.10.006
8. Dong S, Li H, Yin Q. Building information modeling in combination with real time location systems and sensors for safety performance enhancement. Saf Sci. (2018) 102:226–37. doi: 10.1016/j.ssci.2017.10.011
9. Liu H, Li J, Li H, Li H, Mao P, Yuan J. Risk perception and coping behavior of construction workers on occupational health risks-a case study of Nanjing, China. Int J Environ Res Public Health. (2021) 18:7040. doi: 10.3390/ijerph18137040
10. Wong TKM, Man SS, Chan AHS. Critical factors for the use or non-use of personal protective equipment amongst construction workers. Saf Sci. (2020) 126:104663. doi: 10.1016/j.ssci.2020.104663
11. Cane J, O'Connor D, Michie S. Validation of the theoretical domains framework for use in behavior change and implementation research. Implement Sci. (2012) 7:1–17. doi: 10.1186/1748-5908-7-37
12. Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. (2005) 14:26–33. doi: 10.1136/qshc.2004.011155
13. Choudhary P, Gupta A, Velaga NR. Perceived risk vs actual driving performance during distracted driving: A comparative analysis of phone use and other secondary distractions. Transp Res Pt F-Traffic Psychol Behav. (2022) 86:296–315. doi: 10.1016/j.trf.2022.03.001
14. Li X, Fei Y, Rizzuto TE, Yang F. What are the occupational hazards of construction project managers: a data mining analysis in China. Saf Sci. (2021) 134:105088. doi: 10.1016/j.ssci.2020.105088
15. GBD 2017 Risk Factor Collaborators. Global regional and national comparative risk assessment of 84 behavioral environmental and occupational and metabolic risks or clusters of risks for 195 countries and territories 1990–2017: a systematic analysis for the Global Burden of Disease Study (2017). Lancet. (2018) 392:1923–4. doi: 10.1016/S0140-6736(18)32225-6
16. Aven T. Risk assessment and risk management: review of recent advances on their foundation. Eur J Oper Res. (2016) 253:1–13. doi: 10.1016/j.ejor.2015.12.023
17. Tong R, Cheng M, Zhang L, Liu M, Yang X, Li X, et al. The construction dust-induced occupational health risk using Monte-Carlo simulation. J Clean Prod. (2018) 184:598–608. doi: 10.1016/j.jclepro.2018.02.286
18. Tong R, Zhang B, Yang X, Cao L. Health risk assessment of chefs intake of cooking fumes: focusing on Sichuan cuisine in China. Hum Ecol Risk Assess. (2019) 27:162–90. doi: 10.1080/10807039.2019.1698282
19. Zhou L, Tian F, Zou H, Yuan W, Hao M, Zhang M. Research progress in occupational health risk assessment methods in China. Biomed Environ Sci. (2017) 30:616–22. doi: 10.3967/bes2017.082
20. Li X, Fang Z, Shen C. Research on the process of occupational health management and its impact on occupational health performance in construction enterprises. In: ICCREM 2016: BIM Application and Off-Site Construction. Reston, VA: American Society of Civil Engineers (2017). p. 1318–1325.
21. Sousa V, Almeida NM, Dias LA. Risk-based management of occupational safety and health in the construction industry - Part 1: Background knowledge. Saf Sci. (2014) 66:75–86. doi: 10.1016/j.ssci.2014.02.008
22. Liang H, Shi X. Exploring the structure and emerging trends of construction health management: a bibliometric review and content analysis. Eng Constr Archit Manag. (2021) 29:1861–89. doi: 10.1108/ECAM-01-2021-0080
23. Stocks SJ, Turner S, McNamee R, Carder M, Hussey L, Agius RM. Occupation and work-related ill-health in UK construction workers. Occup Med. (2011) 61:407–15. doi: 10.1093/occmed/kqr075
24. Frimpong S, Bemah Antwi A, Yosia Sunindijo R, Changxin Wang C, Ampratwum G, Dansoh A, et al. Health status of young construction workers in the Global South: The case of Ghana. Saf Sci. (2022) 148:105673. doi: 10.1016/j.ssci.2022.105673
25. Faber A, Stroyer J, Hjortskov N, Schibye B. Changes in physical performance among construction workers during extended workweeks with 12-hour workdays. Int Arch Occup Environ Health. (2010) 83:1–8. doi: 10.1007/s00420-009-0471-0
26. Seixas NS, Neitzel R, Stover B, Sheppard L, Feeney P, Mills D, et al. 10-Year prospective study of noise exposure and hearing damage among construction workers. Occup Environ Med. (2012) 69:643–50. doi: 10.1136/oemed-2011-100578
27. Toren K, Jarvholm B. Effect of occupational exposure to vapors, gases, dusts, and fumes on COPD mortality risk among Swedish construction workers: a longitudinal cohort study. Chest. (2014) 145:992–7. doi: 10.1378/chest.13-1429
28. Claessen H, Arndt V, Drath C, Brenner H. Smoking habits and occupational disability: A cohort study of 14,483 construction workers. Occup Environ Med. (2010) 67:84–90. doi: 10.1136/oem.2009.046318
29. Claessen H, Brenner H, Drath C, Arndt V. Serum uric acid and risk of occupational disability: Findings from a cohort study of male construction workers in Germany. Arthritis Care Res. (2010) 62:1278–86. doi: 10.1002/acr.20204
30. Man SS, Chan AHS, Alabdulkarim S. Quantification of risk perception: Development and validation of the construction worker risk perception (CoWoRP) scale. J Saf Res. (2019) 71:25–39. doi: 10.1016/j.jsr.2019.09.009
31. Peng L, Chan AHS. Adjusting work conditions to meet the declined health and functional capacity of older construction workers in Hong Kong. Saf Sci. (2020) 127:104711. doi: 10.1016/j.ssci.2020.104711
32. Fang D, Jiang Z, Zhang M, Wang H. An experimental method to study the effect of fatigue on construction workers' safety performance. Saf Sci. (2015) 73:80–91. doi: 10.1016/j.ssci.2014.11.019
33. Yang Y, Chan AP. Perceptual strain index for heat strain assessment in an experimental study: an application to construction workers. J Therm Biol. (2015) 48:21–7. doi: 10.1016/j.jtherbio.2014.12.007
34. Zhao Y, Yi W, Chan APC, Wong DP. Impacts of cooling intervention on the heat strain attenuation of construction workers. Int J Biometeorol. (2018) 62:1625–34. doi: 10.1007/s00484-018-1562-y
35. Ganster DC, Rosen CC. Work stress and employee health. J Manag. (2013) 39:1085–122. doi: 10.1177/0149206313475815
36. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. Berlin: Springer Publishing Company. (1984).
37. Nes LS, Segerstrom SC. Dispositional optimism and coping: a meta-analytic review. Pers Soc Psychol Rev. (2006) 10:235–51. doi: 10.1207/s15327957pspr1003_3
38. Roth S, Cohen LJ. Approach, avoidance, and coping with stress. Am Psychol. (1986) 41:813–9. doi: 10.1037//0003-066X.41.7.813
40. Chang YT, Tsai FJ, Yeh CY, Chen RY. From cognition to behavior: Associations of workplace health culture and workplace health promotion performance with personal healthy lifestyles. Front Public Health. (2021) 9:745846. doi: 10.3389/fpubh.2021.745846
41. Robinson MD, Irvin RL, Persich MR. Ego effectiveness: a novel individual difference approach to health behavior and coping. J Health Psychol. (2021) 27:1679–96. doi: 10.1177/13591053211001412
42. Robinson MD, Persich MR, Krishnakumar S. What would you do? A new approach to health competence based on situational judgment. J Pers. (2019) 88:676–88. doi: 10.1111/jopy.12518
43. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. (1989) 56:267–83. doi: 10.1037//0022-3514.56.2.267
44. Bashirian S, Jenabi E, Khazaei S, Barati M, Karimi-Shahanjarini A, Zareian S, et al. Factors associated with preventive behaviors of COVID-19 among hospital staff in Iran in 2020: an application of the Protection Motivation Theory. J Hosp Infect. (2020) 105:430–3. doi: 10.1016/j.jhin.2020.04.035
45. Savitsky B, Findling Y, Ereli A, Hendel T. Anxiety and coping strategies among nursing students during the covid-19 pandemic. Nurse Educ Pract. (2020) 46:102809. doi: 10.1016/j.nepr.2020.102809
46. Ma H, Wu Z, Chang P. Social impacts on hazard perception of construction workers: a system dynamics model analysis. Saf Sci. (2021) 138:105240. doi: 10.1016/j.ssci.2021.105240
47. Lingard H, Turner M. Improving the health of male, blue collar construction workers: a social ecological perspective. Constr Manag Econ. (2015) 33:18–34. doi: 10.1080/01446193.2014.997259
48. Lewkowski K, Li IW, Fritschi L, Williams W, Heyworth JS. A systematic review of full-shift, noise exposure levels among construction workers: are we improving? Ann Work Expo Health. (2018) 62:771–82. doi: 10.1093/annweh/wxy051
49. van Deurssen EH, Pronk A, Meijster T, Tielemans E, Heederik D, Hengel KMO. Process evaluation of an intervention program to reduce occupational quartz exposure among Dutch construction workers. J Occup Environ Med. (2015) 57:428–35. doi: 10.1097/JOM.0000000000000382
50. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. (1984) 11:1–47. doi: 10.1177/109019818401100101
51. Ouellette JA, Wood W. Habit and intention in everyday life: the multiple Processes by Which Past Behavior Predicts Future Behavior. Psychol Bull. (1998) 124:54–74. doi: 10.1037//0033-2909.124.1.54
52. Sheeran P, Maki A, Montanaro E, Avishai-Yitshak A, Bryan A, Klein WMP, et al. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: a meta-analysis. Health Psychol. (2016) 35:1178–88. doi: 10.1037/hea0000387
53. Webb TL, Sheeran P. Does changing behavioral intentions engender behavior change: a meta-analysis of experimental evidence. Psychol Bull. (2006) 132:249–68. doi: 10.1037/0033-2909.132.2.249
54. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. (2012) 12:1–13. doi: 10.1186/1471-2458-12-80
55. Roberts BW, Walton KE, Bogg T. Conscientiousness and health across the life course. Rev Gen Psychol. (2005) 9:156–68. doi: 10.1037/1089-2680.9.2.156
56. Carver CS, Scheier MF, Segerstrom SC. Optimism. Clin Psychol Rev. (2010) 30:879–89. doi: 10.1016/j.cpr.2010.01.006
57. Smith MS, Wallston KA, Smith CA. The development and validation of the perceived health competence scale. Health Educ Res. (1995) 10:51–64. doi: 10.1093/her/10.1.51
58. Atkins L, Francis J, Islam R, O'Connor D, Patey A, Ivers N, et al. A guide to using the Theoretical Domains Framework of behavior change to investigate implementation problems. Implement Sci. (2017) 12:1–18. doi: 10.1186/s13012-017-0605-9
59. Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: Mapping theoretically derived behavioral determinants to behavior change techniques. Appl Psychol-Int Rev. (2008) 57:660–80. doi: 10.1111/j.1464-0597.2008.00341.x
60. Morgan JI, Curcuruto M, Steer M, Bazzoli A. Implementing the theoretical domains framework in occupational safety: Development of the safety behavior change questionnaire. Saf Sci. (2021) 136:105135. doi: 10.1016/j.ssci.2020.105135
61. Smith KG, Paudyal V, Quinn F, Klein S, Stewart D. Offshore workers and health behavior change: an exploration using the Theoretical Domains Framework. Int Marit Health. (2018) 69:248–56. doi: 10.5603/IMH.2018.0040
62. Taylor N, Lawton R, Conner M. Development and initial validation of the determinants of physical activity questionnaire. Int J Behav Nutr Phys Act. (2013) 10:74–84. doi: 10.1186/1479-5868-10-74
63. Taylor N, Parveen S, Robins V, Slater B, Lawton R. Development and initial validation of the influences on patient safety behaviors questionnaire. Implement Sci. (2013) 8:1–8. doi: 10.1186/1748-5908-8-81
64. Taylor N, Parveen S, Robins V, Slater B, Lawton R. Discriminant content validity of a theoretical domains framework questionnaire for use in implementation research. Implement Sci. (2013) 9:1–16. doi: 10.1186/1748-5908-9-11
65. Liu Q, Chen W, Qi R, Geng Y, Liu Y, Zhou Y, et al. The utility of health belief model to explain self-protective behavior against pneumoconiosis in Chinese underground coal miners: a cross-sectional study. BMJ Open. (2019) 9:e026772. doi: 10.1136/bmjopen-2018-026772
66. Ronis DL, Hong O, Lusk SL. Comparison of the original and revised structures of the Health Promotion Model in predicting construction workers' use of hearing protection. Res Nurs Health. (2006) 29:3–17. doi: 10.1002/nur.20111
67. Michie S, Stralen MM, West R. The behavior change wheel: a new method for characterising and designing behavior change interventions. Implement Sci. (2011) 6:42. doi: 10.1186/1748-5908-6-42
68. Bigné E, Hernández B, Ruiz C, Andreu L. How motivation, opportunity and ability can drive online airline ticket purchases. J Air Transp Manag. (2010) 16:346–9. doi: 10.1016/j.jairtraman.2010.05.004
69. Li D, Xu X, Chen C, Menassa C. Understanding energy-saving behaviors in the American workplace: a unified theory of motivation, opportunity, and ability. Energy Res Soc Sci. (2019) 51:198–209. doi: 10.1016/j.erss.2019.01.020
70. Willmott T, Parkinson J. Motivation, opportunity, and ability: understanding new habits and changes adopted for weight management. Int J Consum Stud. (2017) 41:291–8. doi: 10.1111/ijcs.12340
71. Abreu-Placeres N, Newton JT, Pitts N, Garrido LE, Ekstrand KR, Avila V, et al. Understanding dentists' caries management: the COM-B ICCMS questionnaire. Community Dent Oral Epidemiol. (2018) 46:545–54. doi: 10.1111/cdoe.12388
72. Buchanan H, Newton JT, Baker SR, Asimakopoulou K. Adopting the COM-B model and TDF framework in oral and dental research: a narrative review. Community Dent Oral Epidemiol. (2021) 49:385–93. doi: 10.1111/cdoe.12677
73. Clark E, Wood F, Wood S. Barriers and facilitators to the use of personal information documents in health and social care settings for people living with dementia: A thematic synthesis and mapping to the COM-B framework. Health Expect. (2022) 25:1215–31. doi: 10.1111/hex.13497
74. Silveira SL, Riemann-Lorenz K, Heesen C, Motl RW. Current and long-term physical activity among adults with multiple sclerosis in the United States: COM-B variables as Explanatory Factors. Int J Behav Med. (2021) 28:561–74. doi: 10.1007/s12529-020-09946-w
75. Barker F, Atkins L, de Lusignan S. Applying the COM-B behavior model and behavior change wheel to develop an intervention to improve hearing-aid use in adult auditory rehabilitation. Int J Audiol. (2016) 55:90–8. doi: 10.3109/14992027.2015.1120894
76. Duan Z, Liu C, Han M, Wang D, Zhang X, Liu C. Understanding consumer behavior patterns in antibiotic usage for upper respiratory tract infections: A study protocol based on the COM-B framework. Res Social Adm Pharm. (2021) 17:978–85. doi: 10.1016/j.sapharm.2020.07.033
77. Khalilollahi A, Kasraian D, Kemperman ADAM, van Wesemael P. Application of the COM-B model to the correlates of children's outdoor playing and the potential role of digital interventions: a systematic literature review. Children's Geograph. (2022) 21:442–58. doi: 10.1080/14733285.2022.2075692
78. Law J, Dornstauder M, Charlton J, Greaux M. Tele-practice for children and young people with communication disabilities: employing the COM-B model to review the intervention literature and inform guidance for practitioners. Int J Lang Commun Disord. (2021) 56:415–34. doi: 10.1111/1460-6984.12592
79. Bentley MR, Mitchell N, Sutton L, Backhouse SH. Sports nutritionists' perspectives on enablers and barriers to nutritional adherence in high performance sport: a qualitative analysis informed by the COM-B model and theoretical domains framework. J Sports Sci. (2019) 37:2075–85. doi: 10.1080/02640414.2019.1620989
80. Howlett N, Schulz J, Trivedi D, Troop N, Chater A. A prospective study exploring the construct and predictive validity of the COM-B model for physical activity. J Health Psychol. (2019) 24:1378–91. doi: 10.1177/1359105317739098
81. Curtis K, Atkins L, Brown K. Big hearts, small hands: a focus group study exploring parental food portion behaviors. BMC Public Health. (2017) 17:716. doi: 10.1186/s12889-017-4711-z
82. Woodland L, Hodson A, Webster RK, Amlôt R, Smith LE, Rubin J. A qualitative study evaluating the factors affecting families' adherence to the first COVID-19 lockdown in England using the COM-B model and TDF. Int J Environ Res Public Health. (2022) 19:7305. doi: 10.3390/ijerph19127305
83. Coupe N, Cotterill S, Peters S. Enhancing community weight loss groups in a low socioeconomic status area: application of the COM-B model and Behavior Change Wheel. Health Expect. (2021) 2021:1–13. doi: 10.1111/hex.13325
84. Kwah KL, Fulton EA, Brown KE. Accessing national health service stop smoking services in the UK: a COM-B analysis of barriers and facilitators perceived by smokers, ex-smokers and stop smoking advisors. Public Health. (2019) 171:123–30. doi: 10.1016/j.puhe.2019.03.012
85. Mazloomy Mahmoodabad SS, Zareei Mahmoodabadi H, Mazhari Majd H, Miri MR. Analysis of capability, motivation and opportunity to prevent substance abuse in sensation seeking students on the outskirts of a city in Eastern Iran: a qualitative study. BMC Psychol. (2022) 10:37. doi: 10.1186/s40359-022-00748-1
86. Vasiliou VS, Dockray S, Dick S, Davoren MP, Heavin C, Linehan C, et al. Reducing drug-use harms among higher education students: MyUSE contextual-behavior change digital intervention development using the Behavior Change Wheel. Harm Reduct J. (2021) 18:1–23. doi: 10.1186/s12954-021-00491-7
87. Allison AL, Lorencatto F, Michie S, Miodownik M. Barriers and enablers to food waste recycling: a mixed methods study amongst UK citizens. Int J Environ Res Public Health. (2022) 19:2729. doi: 10.3390/ijerph19052729
88. Perros T, Allison AL, Tomei J, Parikh P. Behavioral factors that drive stacking with traditional cooking fuels using the COM-B model. Nat Energy. (2022) 7:886–98. doi: 10.1038/s41560-022-01074-x
89. Ojo SO, Bailey DP, Hewson DJ, Chater AM. Perceived barriers and facilitators to breaking up sitting time among desk-based office workers: A qualitative investigation using the TDF and COM-B. Int J Environ Res Public Health. (2019) 16:2903. doi: 10.3390/ijerph16162903
90. Munir F, Biddle SJH, Davies MJ, Dunstan D, Esliger D, Gray LJ, et al. Stand more at work (SMArT Work): using the behavior change wheel to develop an intervention to reduce sitting time in the workplace. BMC Public Health. (2018) 18:319. doi: 10.1186/s12889-018-5187-1
91. Howlett N, Schulz J, Trivedi D, Troop N, Chater A. Determinants of weekly sitting time: construct validation of an initial COM-B model and comparison of its predictive validity with the Theory of Planned Behavior. Psychol Health. (2021) 36:96–114. doi: 10.1080/08870446.2020.1763994
92. Irwin A, Mihulkova J, Berkeley S, Tone LR. ‘No-one else wears one:' Exploring farmer attitudes towards All-Terrain Vehicle helmets using the COM-B model. J Safety Res. (2022) 81:123–33. doi: 10.1016/j.jsr.2022.02.004
93. Castro-Sanchez E, Alexander CM, Atchison C, Patel D, Leung W, Calamita ME, et al. Evaluation of a personal protective equipment support programme for staff during the COVID-19 pandemic in London. J Hosp Infect. (2021) 109:68–77. doi: 10.1016/j.jhin.2020.12.004
94. Agrawal R, Imielinski T, Swami A. Mining association rules between sets of bibitems in large databases. ACM SIGMOD Record. (1993) 22:207–16. doi: 10.1145/170036.170072
95. Huang, L., Chen, H., and wang, X., Chen, G. A fast algorithm for mining association rules. J Comput Sci Technol. (2000) 15:619–24. doi: 10.1007/BF02948845
96. Sugimori H, Iida Y, Suka M, Ichimura T, Yoshida K. Data mining for seeking relationships between sickness absence and Japanese worker's profile. Knowl-Based Intellig Inform Eng Syst. (2003) 2774:410–16. doi: 10.1007/978-3-540-45226-3_56
97. Meng Q, Sha J. Tree-based frequent bibitemsets mining for analysis of life-satisfaction and loneliness of retired athletes. Cluster Comput. (2017) 20:3327–35. doi: 10.1007/s10586-017-1080-4
98. Huy NT, Chico RM, Huan VT, Shaikhkhalil HW, Uyen VNT, Qarawi ATA, et al. Awareness and preparedness of healthcare workers against the first wave of the COVID-19 pandemic: a cross-sectional survey across 57 countries. PLoS ONE. (2021) 16:e0258348. doi: 10.1371/journal.pone.0258348
99. Yasir M, Ashraf A, Chaudhry MU, Hassan F, Lee J, Jasiński M, et al. D-GENE-Based discovery of frequent occupational diseases among female home-based workers. Electronics. (2021) 10:1230. doi: 10.3390/electronics10111230
100. Verma A, Khan SD, Maiti J, Krishna OB. Identifying patterns of safety related incidents in a steel plant using association rule mining of incident investigation reports. Saf Sci. (2014) 70:89–98. doi: 10.1016/j.ssci.2014.05.007
101. Jiang J, Zhang L, Wang Y, Zhang K, Yang D, He W. Association rules analysis of human factor events based on statistics method in digital nuclear power plant. Saf Sci. (2011) 49:946–50. doi: 10.1016/j.ssci.2011.02.010
102. Liao C, Perng Y. Data mining for occupational injuries in the Taiwan construction industry. Saf Sci. (2008) 46:1091–102. doi: 10.1016/j.ssci.2007.04.007
103. Shin D, Park Y, Seo J, Lee D. Association rules mined from construction accident data. KSCE J Civ Eng. (2018) 22:1027–39. doi: 10.1007/s12205-017-0537-6
104. Trillo Cabello A, Martínez-Rojas M, Carrillo-Castrillo JA, Rubio-Romero JC. Occupational accident analysis according to professionals of different construction phases using association rules. Saf Sci. (2021) 144:105457. doi: 10.1016/j.ssci.2021.105457
105. Xu X, Zou PXW. Discovery of new safety knowledge from mining large injury dataset in construction. Saf Sci. (2021) 144:105481. doi: 10.1016/j.ssci.2021.105481
106. Wang H, Chen J, Arifai AM, Gheisari M. Exploring empirical rules for construction accident prevention based on unsafe behaviors. Sustainability. (2022) 14:4058. doi: 10.3390/su14074058
107. Guo S, Zhang P, Ding L. Time-statistical laws of workers' unsafe behavior in the construction industry: a case study. Physica A. (2019) 515:419–29. doi: 10.1016/j.physa.2018.09.091
108. La Fata CM, Giallanza A, Micale R, La Scalia G. Ranking of occupational health and safety risks by a multi-criteria perspective: Inclusion of human factors and application of VIKOR. Saf Sci. (2021) 138:105234. doi: 10.1016/j.ssci.2021.105234
109. Yang X, Zhao X, Wang Y, Tong R. Development of occupational health culture scale: a study based on miners and construction workers. Front Public Health. (2022) 10:992515. doi: 10.3389/fpubh.2022.992515
110. Lawton R, Heyhoe J, Louch G, Ingleson E, Glidewell L, Willis TA, et al. Using the Theoretical Domains Framework (TDF) to understand adherence to multiple evidence-based indicators in primary care: a qualitative study. Implement Sci. (2016) 11:113. doi: 10.1186/s13012-016-0479-2
111. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quinonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. (2018) 6:149. doi: 10.3389/fpubh.2018.00149
112. Singh A, Ali A. Psychosocial inventory for caregivers (PIC) of persons with mental illness: content validity and cognitive interviewing process. Asian J Psychiatr. (2022) 70:103020. doi: 10.1016/j.ajp.2022.103020
113. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. (2001) 52:397–422. doi: 10.1146/annurev.psych.52.1.397
114. Pender NJ, Murdaugh CL, Parsons MA. Health Promotion in Nursing (7th Edition). Boston: Pearson Education. (2014).
115. Jones W, Gibb A, Haslam R, Dainty A. Work-related ill-health in construction: The importance of scope, ownership and understanding. Saf Sci. (2019) 120:538–50. doi: 10.1016/j.ssci.2019.07.038
116. Los FS, de Boer A, van der Molen HF, Hulshof CTJ. The implementation of workers' health surveillance by occupational physicians: a survey study. J Occup Environ Med. (2019) 61:e497–502. doi: 10.1097/JOM.0000000000001740
117. Oude Hengel KM, Blatter BM, van der Molen HF, Bongers PM, van der Beek AJ. The effectiveness of a construction worksite prevention program on work ability, health, and sick leave: results from a cluster randomized controlled trial. Scand J Work Environ Health. (2013) 39:456–67. doi: 10.5271/sjweh.3361
Keywords: behavior change technique, COM-B model, association rule analysis, coping behavior, occupational health risk, construction worker
Citation: Yang X, Ling Y, Wang L, Li Y and Zeng M (2025) Coping behavior toward occupational health risks among construction workers: determinant identification using the COM-B model and data mining analysis. Front. Public Health 13:1643332. doi: 10.3389/fpubh.2025.1643332
Received: 08 June 2025; Accepted: 01 August 2025;
Published: 12 September 2025.
Edited by:
K. S. Anandh, SRM Institute of Science and Technology, IndiaReviewed by:
Senthamizh Sankar S., Indian Institute of Technology Madras, IndiaRahul Deb Bera, Institute of Management Study, British Indian Ocean Territory
Copyright © 2025 Yang, Ling, Wang, Li and Zeng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mingrong Zeng, amVmb3gyMTJAMTYzLmNvbQ==