 Helena Manger
Helena Manger Katja Beck-Doßler2
Katja Beck-Doßler2 Olaf Hoos
Olaf Hoos Andrea Szczesny
Andrea Szczesny- 1Department of Business Management, University of Würzburg, Würzburg, Germany
- 2Conflict Management Service, University of Würzburg, Würzburg, Germany
- 3Center for Sports and Physical Education, University of Würzburg, Würzburg, Germany
- 4Healthy University Office, University of Würzburg, Würzburg, Germany
Background: Sedentary work environments contribute to low physical activity (PA) levels, which are associated with adverse health and productivity outcomes. Workplace interventions such as step challenges offer a promising strategy to promote PA.
Aim: This study investigates the effects of a six-week, team-based step contest conducted at a German university and examines personal and work-related factors including the role of leaders influencing PA.
Methods: A one-group pre-post design was used to assess daily step counts of 331 participants across 44 self-formed teams during baseline, intervention and follow-up periods. Step data were collected via a mobile app, and a survey captured various demographic, work-related and intervention-related factors.
Results: The step challenge significantly increased daily step counts by 1,700 on average compared to baseline. However, this increase was not sustained during follow-up. Males and older participants exhibited greater improvements. Notable, individuals in leadership positions showed a relatively greater increase in step counts during the intervention. However, the presence of a leader within a team did not significantly impact team colleagues’ performance. Other work-related factors such as work location and commute mode correlated with participants’ step counts but did not impact the step challenge’s effectiveness.
Conclusion: Our findings suggest that team-based workplace interventions can effectively boost short-term PA but sustaining these improvements remains challenging and requires ongoing actions. Further, it is essential to take personal and work-related factors including the role of leaders into account to develop targeted strategies that enhance PA. Tailored strategies and organizational support are needed to promote long-term engagement. These insights may inform future workplace health initiatives aiming for sustainable impact.
1 Introduction
The decline in physical activity (PA) and the rise of sedentary work are strongly related to desk-based occupations as many employees spend most work hours sitting (1–4). Low activity levels contribute to decreased productivity, higher absenteeism, and increased healthcare costs (4, 5). Hence, the World Health Organization (WHO) recommends reducing sedentary behavior and increasing PA (6) to significantly counteract the risk for cardiovascular disease, diabetes, obesity, and mental health disorders (2, 7–11).
To address these challenges, workplace interventions have gained attention. Organizations increasingly adopt workplace health initiatives to promote PA and thereby aim to increase productivity, job satisfaction, and reduce absenteeism (12–16).
In this context step challenges, particularly those incorporating feedback and social comparison, have shown high potential (17–24). Team incentives may further enhance engagement (14, 25–29). Previous research on step challenges has shown that both financial incentives (26, 30) as well as non-monetary rewards increase PA in short-term but long-term sustainability is uncertain (31, 32). Outbalancing incentive-removal post-intervention on the one hand and increased awareness of PA benefits and habit formation on the other seem to be decisive for sustained improvements. Further, randomized controlled trials indicate that intervention success strongly depends on design and participant characteristics (33–35). Within the specific setting of higher education, a “healthy university concept” (36) includes PA promotion. Setting-specific team-based competitions with incentives have shown very promising increases of up to 4,800 steps per day (30). Besides, the ARK project in Norway demonstrated the effectiveness of holistic health promotion programs in higher education (36), and a systematic review of 17 studies found positive health outcomes in PA, weight management, and nutrition (37). However, diverse employee demographics and organizational structures present unique challenges for workplace interventions (38, 39) with time constraints, workplace cultures, and the complexity of integrating such programs into daily routines representing typical barriers (40). Besides, gender and age differences may influence changes in PA behavior. Men tend to be more motivated by competition, whereas women prioritize fitness and appearance (41, 42), and gender specific differences in motivation for PA diminish with age (43). Younger individuals are motivated by health and goalsetting (44). Also, factors like lifestyle, education and job characteristics influence activity levels (40, 45). Additionally, in the context of workplace PA interventions, leadership may influence behavior changes (16, 46, 47). Leaders shape organizational culture and often serve as role models (15, 48–50). Notably, participation in health interventions may also contribute to improvements of leadership (15, 51).
However, few studies have explored the role of leadership in the context of workplace PA interventions involving self-formed teams without designated intervention leaders. This gap is especially relevant in higher education institutions, where leadership structures differ significantly from those in the private sector. At universities, leadership is often distributed and exercised through indirect forms such as mentorship, coordination, and project management rather than through formal, hierarchical authority (52, 53). Understanding these unique leadership dynamics is critical for evaluating PA promotion interventions in academic environments. Additionally, recognizing personal and work-related factors seems crucial for designing effective workplace interventions for PA promotion. Therefore, this study examines the effectiveness of a six-week team step challenge using a gamified mobile app in increasing daily step counts among employees at a German university. Further this study explores individual, work-related, and team-related influencing factors. A particular focus is placed on the role of leadership, examining whether individuals in leadership roles show different outcomes, and whether their presence influences team performance.
We hypothesize that a non-monetary, team-based step contest will increase daily step counts compared to baseline levels, but we expect step counts to decline post-intervention. In addition, we examine how intervention effects relate to individual characteristics, and workplace dynamics. In addition, we expect individuals with leadership responsibilities to demonstrate greater engagement, and explore whether their presence affects overall team outcomes.
2 Methods
2.1 Study design and participants
This manuscript follows the Template for Intervention Description and Replication (TIDieR) checklist to ensure clear and replicable reporting of the intervention (54).
The intervention was a team-based step challenge, named “Team-Heroes,” in a German university. The goal of the intervention was to promote PA and foster team spirit among university employees.
Participants used a mobile app, which tracked steps via smart devices (55). Participant recruitment was done via university website and email. 331 individuals self-selected into 44 teams of 3–15 members. A survey with 15 items on participants’ demographics, lifestyle habits, job-related characteristics, and motives towards participation was conducted electronically as part of the registration along with participants consent for anonymous data collection and analysis.1 Of particular interest is the answer to the question of whether a person has personal responsibilities at work, indicating leadership roles. In addition, to better understand the leadership landscape, data from the university’s human resources (HR) system was collected. Step data were collected during a baseline period, a intervention period, and a follow-up period. The step-challenge app automatically synchronized step counts detected by the accelerometer of participants’ smart devices. During the intervention, participants received feedback on team step count and ranking as well as a map with a virtual journey via the app. No feedback was provided during baseline and follow-up phases. Members of the winner team received culture vouchers at the end of the intervention—gift certificates redeemable at local cultural institutions such as theaters or museums—and certificates of achievement, which were personalized documents listing the team’s name and final ranking, awarded to each team member. These prizes were not announced prior to the challenge.
The intervention was organized and coordinated by the university’s healthy workplace initiative team. The step challenge was delivered digitally through the mobile app and took place remotely. No specific physical infrastructure was required beyond access to a smartphone or wearable device. Data collection took place over a 12-week period from late August to mid-November 2023. The intervention lasted 6 weeks. The baseline and follow-up periods each lasted 3 weeks.
Teams were self-formed based on social or work relationships. The app features and challenge structure were standardized across all participants.
No modifications were made to the intervention during the study period. The intervention was delivered as planned.
All measures were taken to ensure participant confidentiality, anonymity, and privacy. The study was conducted in accordance with the declaration of Helsinki and was approved by the institutional review board (approval number: EV2025/1-0302).
2.2 Primary outcome and data treatment
We chose a one-group pre-post design. Participants’ daily steps served as primary outcome. Participants with no valid step data were excluded. To ensure data quality, extreme values (<1,000 or >35,000 steps/day) were treated as missing values (26, 45, 56), based on the distribution of our dataset, where the 5th percentile was 950 steps and the 99th percentile was 34,079 steps. Values outside this range were rare and potentially affected by device errors or manipulation. An individual-centered imputation method for missing step counts by using the average of individual’s weekday or weekend data (56) was applied separately to each phase (baseline, intervention, follow-up). For individuals who had no data available from any weekday or weekend within a specific period, we substituted the missing steps with the overall weekday or weekend average. With these procedures we obtained a balanced dataset of 27,804 observations from 331 participants in total. For variables related to participants’ self-reported characteristics, a worst-case scenario approach was applied (14). Every missing data point was treated as such and not imputed. Responses marked as “other” were treated as missing.
2.3 Statistical analysis
Besides descriptive statistics (mean ± standard deviations), one-way mixed analysis of variance (ANOVA) with repeated measures was conducted to assess changes in step counts across study periods (baseline, intervention, follow-up). Post hoc pairwise comparisons with Bonferroni correction were applied. Additionally, two-way ANOVA with repeated measures was used to examine differences in step counts and intervention effectiveness based on personal and work-related factors. Participants’ mean daily step counts served as dependent variable. If Levene’s test indicated a violation of the assumption of homogeneity of variances, the dependent variable was logarithmized. Pearson pairwise correlation analysis was performed to explore relationships between participants’ characteristics. Analysis was conducted using Stata Version 17.0.
3 Results
Figure 1 visualizes dynamics of daily step counts throughout the study. Average daily step counts increased from 8,955 steps/day at baseline to 10,653 during the intervention, declining to 8,514 in follow-up (see Table 1). A one-way ANOVA using the logarithm of the step variable identified a significant main effect of the intervention [F (2, 660) = 42.15, p < 0.01, = 0.11]. Post hoc pairwise comparisons revealed that step counts were significantly higher during the intervention compared to baseline (p < 0.01) and follow-up (p < 0.01). The difference between baseline and follow-up was not statistically significant. A post-hoc one-way ANOVA showed a significant main effect of treatment weeks on step counts (F (5, 1,650) = 17.44, p < 0.01, = 0.05). Post hoc comparisons indicated a significant decline in step counts from the first to the later weeks of the intervention.
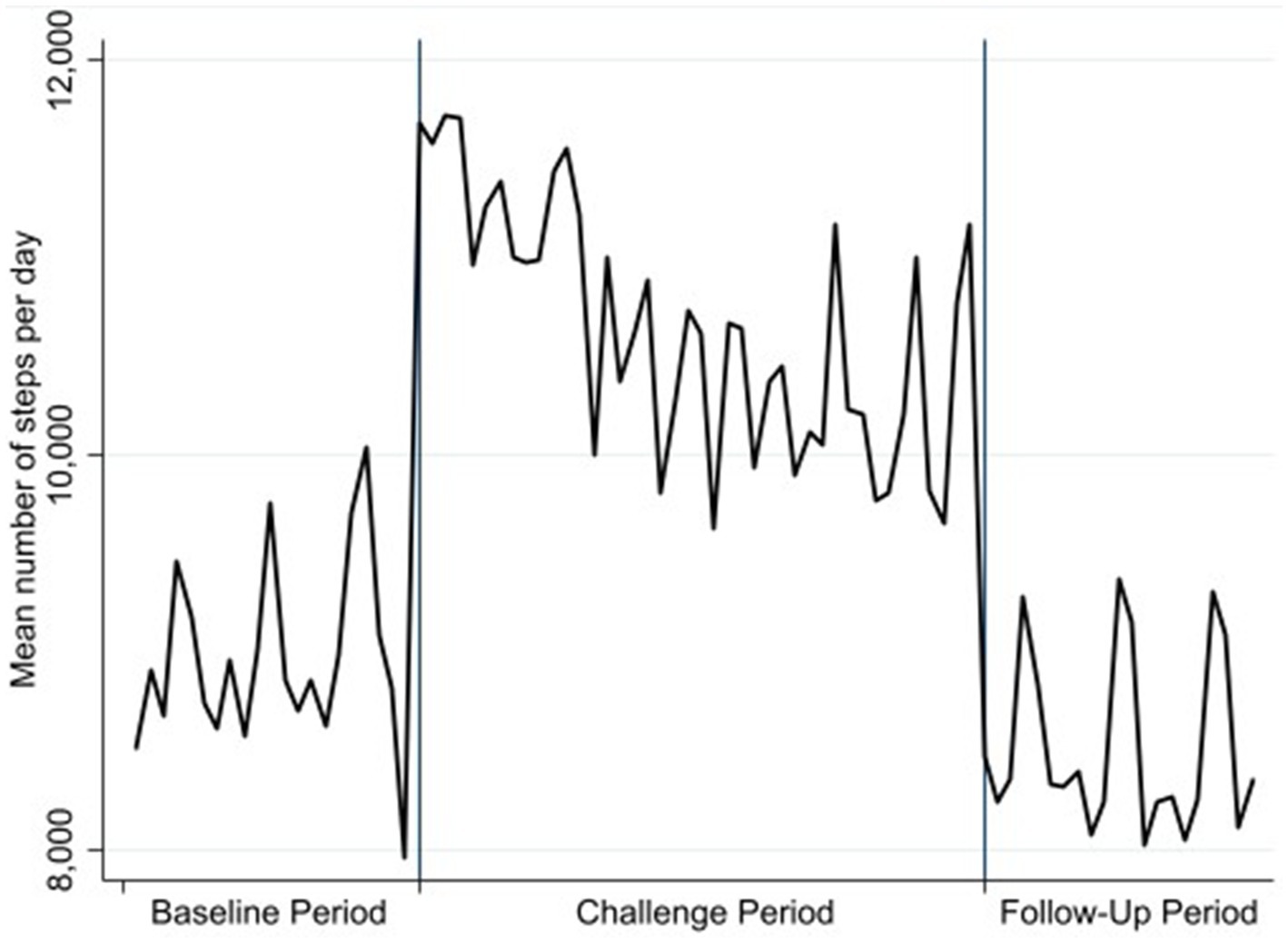
Figure 1. Average daily step counts.
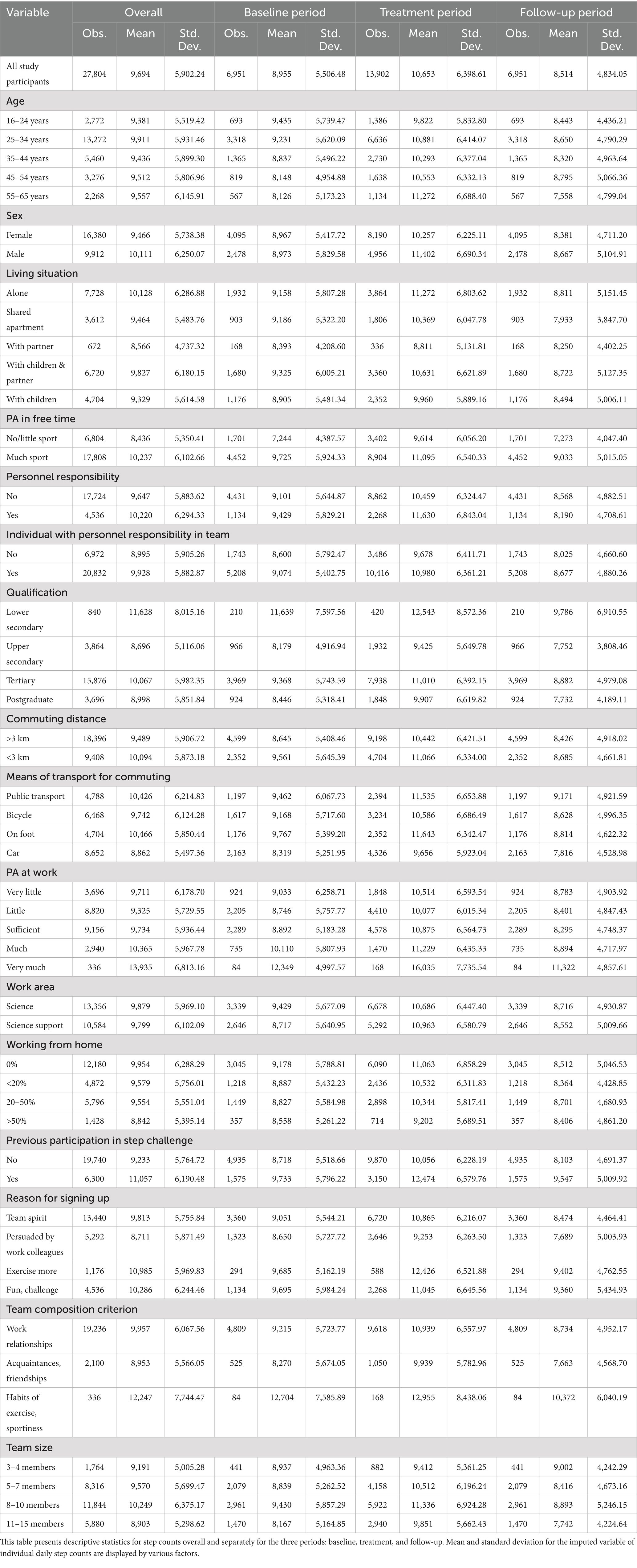
Table 1. Summary statistics.
The mean age was 35.07 (±11.04) years. ANOVA results indicated no significant main effect of age on step counts (see Table 2), but older participants (55–65 years) exhibited the largest relative increase in daily step counts. Among participants, 62% were female (see Table 3). Baseline step counts were comparable between males and females, though males exhibited a greater increase during the intervention (see Tables 1, 2).
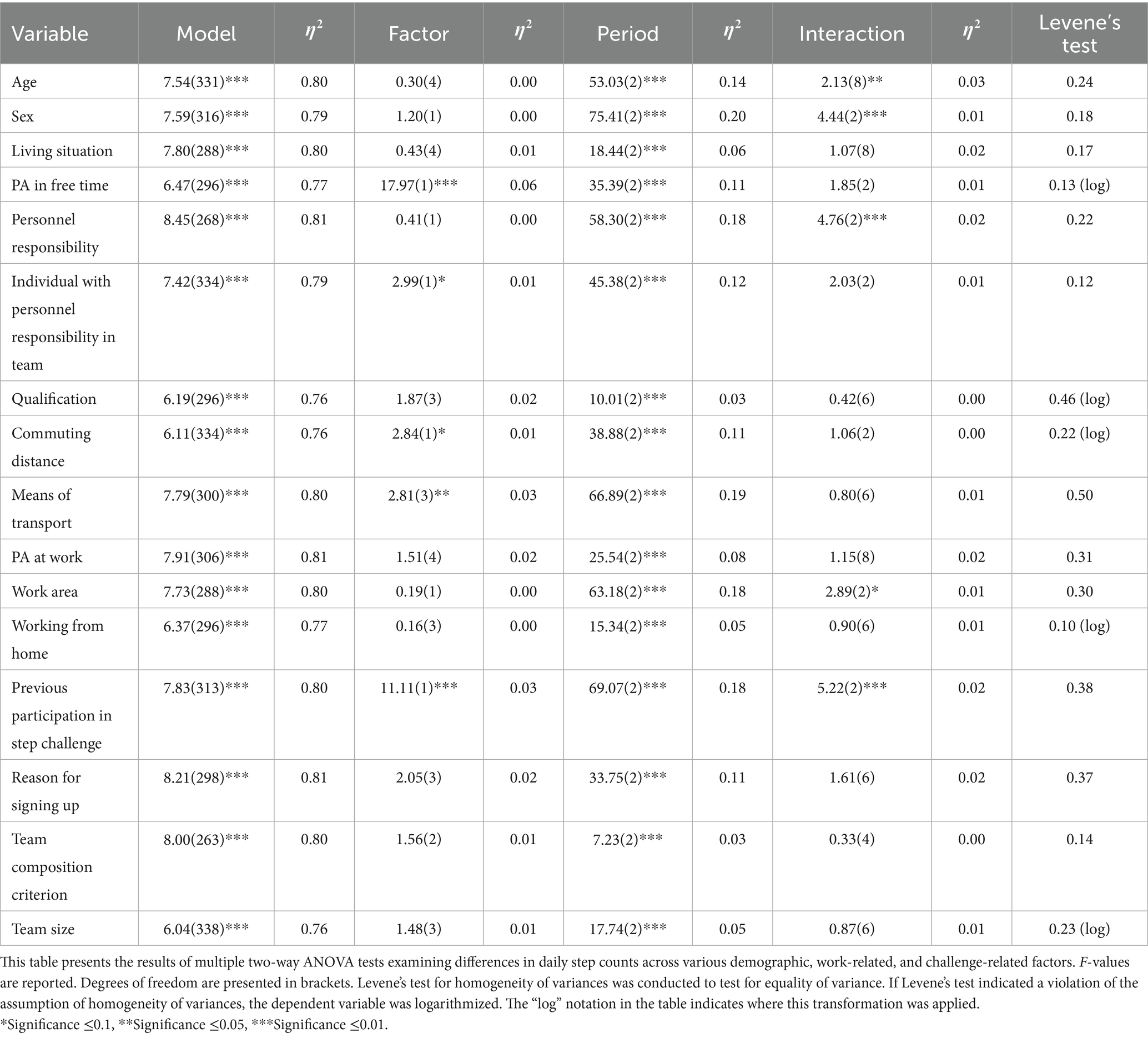
Table 2. Two-way ANOVA results.
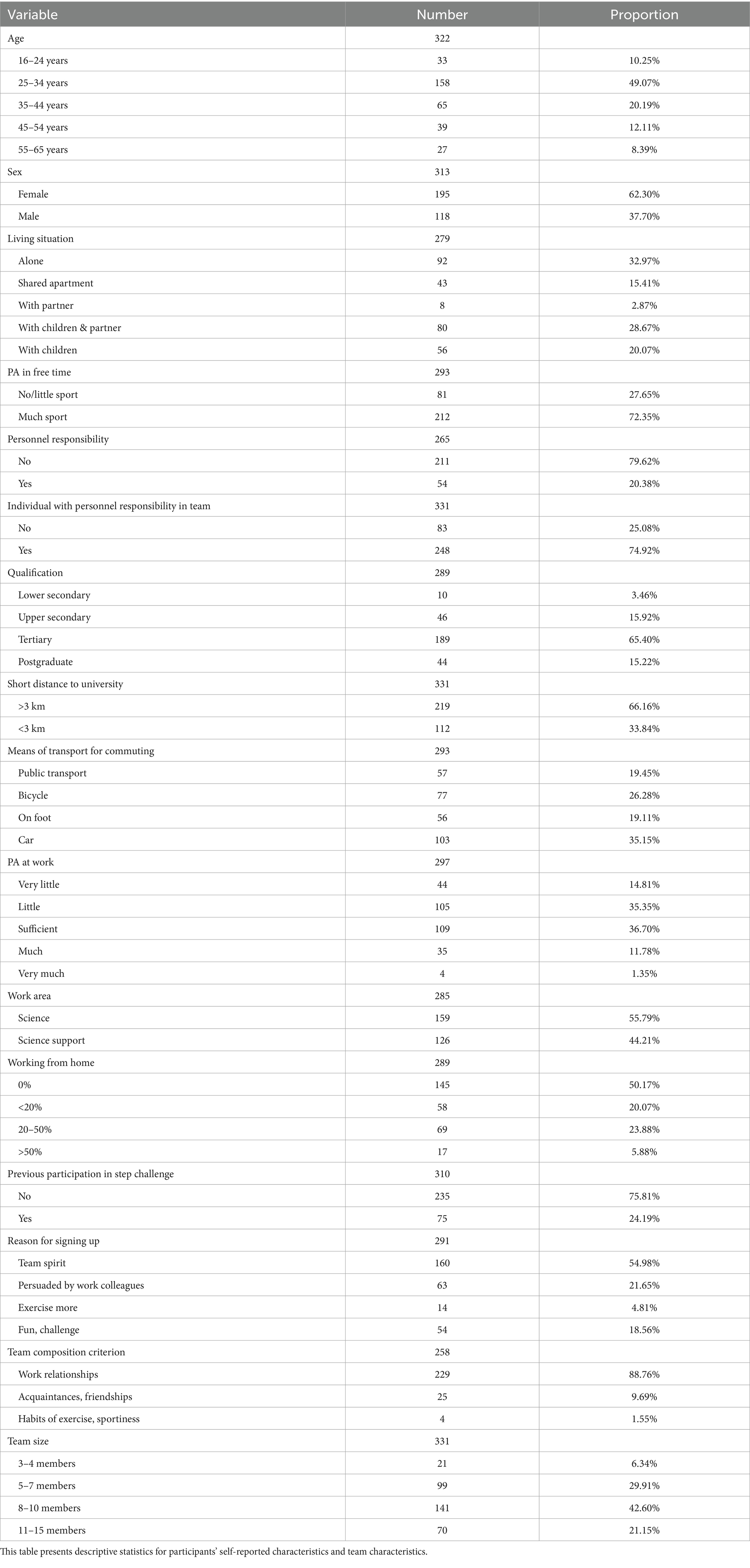
Table 3. Participants’ characteristics.
More than 72% of participants reported engaging in PA multiple times per week during their free time (see Table 3). Descriptive statistics indicated that active participants walked more across all periods (see Table 1). A significant main effect of PA in free time on step counts was observed, though no significant interaction effect with the intervention was found (see Table 2).
A key focus of this study was the role of leadership. Data from the university’s HR system indicated that in May 2025, 423 individuals in scientific positions held officially designated leadership roles, collectively responsible for 3,846 employees (excluding student assistants). In scientific support, 62 leadership positions were identified, overseeing 871 employees. Leadership roles cover a wide range of functions. In the scientific domain, these include professorial leadership, research group leaders, spokespersons of major research projects, deans, and central facility directors. In scientific-support, leadership roles encompass department and unit heads, project managers, heads of technical and administrative services, and coordinators of specialized services such as family support or equal opportunity offices. Among study participants, approximately 20% reported having personnel responsibilities at work (22.79% among scientific staff, 19.13% among science support staff) (see Table 3). While this factor did not exhibit a significant main effect on mean daily step counts, a significant interaction effect with the intervention was identified (see Table 2). Individuals in leadership roles demonstrated a significantly greater increase in daily step counts. 75% of participants were in teams with at least one member holding personnel responsibilities (see Table 3), yet the presence of such individuals within a team did not significantly influence the challenge’s effectiveness in increasing daily step counts (see Table 2). 37% of participants were in teams with one leader, 23% with two, 8% with three, and 7% with four leaders. The maximum proportion of team members with leadership roles was 50%.
Results suggested a trend, with participants living closer to the university walking more across all three periods (see Tables 1, 2). However, the ANOVA results revealed no significant interaction effect of commuting distance with the intervention (see Table 2). Similarly, means of transport for commuting had a significant main effect on step counts, but we found no significant interaction effect with the intervention (see Table 2). Bonferroni-adjusted pairwise comparisons revealed significantly lower step counts for car users compared to public transport users and those walking.
PA at work did not significantly affect steps, nor was there a significant interaction effect with the intervention (see Table 2). However, descriptive statistics suggested that individuals with higher PA tended to have higher step counts (see Table 1).
Participants were nearly evenly split between science staff and science support roles (see Table 3). While both groups had similar baseline step counts, science support staff showed a greater increase in daily steps during the intervention (see Tables 1, 2). In contrast, simple main effects analysis did not indicate a significant impact of work area on step counts.
First-time step challenge participants, who comprised the majority (76%) of the sample (see Table 3), walked significantly less in all periods compared to others, and the intervention was more effective among those with prior challenge experience (see Table 2). Additionally, prior participation was positively correlated with working in science support roles (p < 0.01) and negatively correlated with joining the challenge due to persuasion by colleagues (p < 0.01). There is a trend suggesting that those in leadership positions may be slightly more likely to have participated before (p = 0.09) (see Table 2).
The reason for signing up and team composition criteria did not significantly influence steps, nor did it impact intervention effectiveness (see Table 2). However, descriptive statistics indicated that those who reported to form teams due to exercise habits showed higher step counts across all periods (see Table 1).
Team size ranged from 3 to 15 members. ANOVA results did not show a significant relationship of team size to step counts (see Table 2). Descriptive statistics indicated that smaller teams showed the smallest increase in daily steps while teams with 8–10 members showed the largest increase in daily steps (see Table 1). However, all groups experienced a decline in steps during the follow-up period.
4 Discussion
Our study provides interesting insights into step count trends during a step challenge intervention. Participants walked more than double the average German population (57), reaching approximately 10,700 steps/day during the intervention. Even pre-intervention, participants were already quite active, averaging around 9,000 steps/day, consistent with research showing that workplace interventions often attract physically active individuals (34). Indeed, the majority of participants reported engaging in sports multiple times per week. While research suggests that less active individuals benefit more from PA promotion programs (34, 35), such interventions often fail to engage this group. Our findings highlight this participation bias and underscore the need for targeted strategies to attract less active employees.
The challenge led to an increase of about 1,700 steps/day, demonstrating its effectiveness in promoting activity. This rise aligns with previous workplace PA interventions (18, 21, 24) including team-based interventions (14, 19, 20, 25, 26, 29), though it is lower than the 4,799-step increase observed in a team competition with financial incentives (30). This smaller effect may be due to a higher baseline (8,955 vs. 5,959 steps/day), the absence of a daily step goal, or the lack of monetary rewards. Nonetheless, our findings confirm that team-based challenges can still drive meaningful behavior change. Notably, our step increase surpasses the modest effects reported in some studies (18–20).
Participants showed strong initial engagement, likely driven by novelty, followed by a gradual decline, suggesting potential fatigue or being incompatible with daily duties over longer terms. This pattern underscores the importance of monitoring and addressing factors that may contribute to decreasing activity over time. After the challenge, step counts dropped, indicating that while short-term interventions effectively boost activity, maintaining long-term habits may require additional strategies. Step counts were even lower than before the challenge, though not statistically significant, possibly due to recovery after an intense final push or a return to typical activity levels if participants had increased their steps during the baseline period in preparation for the challenge.
By utilizing the multi-campus higher education environment, marked by a diverse range of stakeholder roles and operational goals (38, 39), our study captures the influence of team-based competitions on PA within a heterogeneous organizational context. This context provides additional insights into variations in activity levels and the effectiveness of workplace interventions.
Sociodemographic differences were evident. Our results suggest that female work forces are more likely to participate in team-based step contests. However, males exhibited a greater step increase, likely due to their higher competitiveness (41–43, 58, 59). Age influenced the effectiveness of the intervention with older participants showing the highest relative step increase. This aligns with research showing that older adults are more driven by extrinsic motivation in PA (27, 41), while younger individuals may respond better to goal setting (44). Our study did not include a daily step goal, which has been a key motivator in other studies (34). Further, our findings do not indicate that family responsibilities hinder PA aligning with prior research (19, 60). In general, higher self-reported PA in free time positively correlated with daily step counts aligning with prior research (19, 45). However, while previous research suggests that less active individuals benefit more from such interventions (24, 34, 35, 61), our study does not support this for the university setting.
In addition, work-related characteristics played a substantial role. Our analysis confirms results of previous research showing a link between commuting and PA (42, 60), with car users walking less. Besides, working from home showed a trend of lower steps, possibly due to reduced incidental movement (3) but the results were not significant. As suggested by prior research, we found differences between academics and science-supportive employees (40). Participants in academic or scientific roles exhibited a lower step count increase compared to science support staff. Science support staff were also more likely to have participated in a previous step challenge, as indicated by the positive correlation with prior participation, suggesting a higher initial engagement with PA initiatives.
Additionally, leadership may play an important role in shaping behavior within workplace PA interventions (16, 46, 47). In the university context, personnel responsibility typically involves supervisory duties over staff or students. This includes tasks such as delegating work, monitoring performance, approving leave, and supporting professional development. Individuals with personnel responsibilities are often accountable for team outcomes and contribute to the functioning of academic or administrative structures. Leadership at universities is more complex than formal supervisory roles alone. It is shaped by relational dynamics, trust, and informal negotiations of influence and responsibility (52, 53). The diversity of leadership roles reflects the distributed and non-hierarchical nature of leadership in higher education. This complexity extends across both scientific and scientific-support domains, including positions such as deans, research group leaders, department heads, technical managers, and coordinators of institutional services. Such a nuanced leadership structure is particularly relevant when evaluating participation in university-wide initiatives like team-based health promotion programs. In these contexts, the presence and engagement of individuals in leadership roles may influence participation and outcomes through role modeling, team motivation, or cultural signaling (15, 16, 46, 48–50).
Data from the university’s HR system shows that approximately 9% of employees hold formal leadership roles—9.91% in scientific positions and 6.65% in scientific-support roles. In contrast, 20% of study participants reported having personnel responsibilities, suggesting that individuals in leadership roles may be more inclined to engage in such health initiatives. Among scientific staff in the study, the figure was even higher (22.79%), aligning with institutional trends. This overrepresentation suggests that workplace PA interventions may appeal especially to individuals with leadership responsibilities.
It is also possible that the discrepancy between reported and formal leadership roles reflects the unique leadership culture in universities. Given the distributed and often informal nature of academic leadership (52, 53), individuals may perceive themselves as having personnel responsibility even in the absence of formal supervisory roles. Such perceptions can still influence engagement in workplace health initiatives, as informal leadership may foster a sense of responsibility, role modeling, or team cohesion.
Taken together, these findings suggest that workplace PA interventions may particularly appeal to individuals who see themselves in leadership roles—whether formally recognized or not. Survey results support this trend, showing that participants in leadership roles were more likely to have taken part in previous step challenges.
During the intervention, these individuals also showed greater increases in step count—possibly reflecting a desire to serve as role models or to support team cohesion (48, 49). Leaders may also be more accustomed to setting and pursuing goals, making them particularly responsive to structured, gamified health programs (62, 63). Another possible explanation is that individuals in leadership roles may have experienced increased pressure to perform due to their visibility within the team. This perceived accountability could have driven them to increase their activity levels, independent of intrinsic motivation or role modeling intentions.
Despite these findings, our results indicate that the mere presence of a leader in a team did not significantly affect other team members’ outcomes. This could be because the step challenge primarily relied on individual motivation rather than leadership-driven encouragement (46). Leaders may have focused on their own performance rather than actively fostering participation within their teams. Lack of leadership support may hinder PA promotion (16, 46, 47). Research highlights that there is a need to equip leaders with knowledge to foster participation and engagement (64). To leverage leadership more effectively in workplace PA interventions, organizations should implement strategies that actively involve leaders in promoting engagement within their teams. These insights highlight the importance of understanding how leaders’ PA behaviors may influence the effectiveness of workplace PA promotion interventions as pointed out in prior research (15, 38, 47).
Although some teams included multiple individuals with leadership responsibilities, there were no teams composed exclusively of leaders. The maximum proportion of leadership roles within a team was 50%, suggesting that leaders did not form separate, leader-only teams but were instead integrated into mixed-role groups. It is also plausible that some teams included multiple leadership levels (e.g., institute heads, professors, and research group leaders).
Further, participants with prior experience in step challenges had higher baseline step counts and demonstrated a greater increase in activity levels, highlighting a potential predisposition toward competition or intervention-driven PA – an observation that aligns with previous research (25).
Team composition might also play a role. Participants that joined teams based on shared exercise habits showed on average higher step counts across all three study periods. Team size ranged from 3 to 15 members, similar to earlier studies (19, 26). Teams with moderate size exhibited higher step counts.
Despite these insights, limitations must be acknowledged. Self-selection may have introduced bias and the reliance on participants’ step-tracking devices and self-reported data could affect the accuracy of the obtained data. Additionally, other forms of PA (e.g., cycling, swimming, yoga, aerobics) were not captured, as the app only recorded walking—i.e., step-based movement detected by smart devices. The predominantly female, office-based sample and short follow-up period also limit generalizability and long-term conclusions. Furthermore, it is unclear whether the teams in the study were strictly work teams, and whether the individuals reporting to have personnel responsibilities were formal, work-related leaders of their team colleagues. Finally, while we excluded extreme step values (<1,000 or >35,000 steps/day) to reduce potential measurement error, this decision may have led to the omission of valid but rare activity patterns. However, a robustness check including these values yielded comparable results, suggesting limited impact on the overall findings. A key limitation of this study is the absence of a control group, which restricts our ability to attribute the observed increase in step count solely to the intervention. The challenge took place in autumn 2023, with the baseline phase occurring during the semester break and the follow-up during the academic semester. External factors such as seasonal weather changes, academic workload fluctuations, and working-from-home patterns may have influenced participants’ activity levels regardless of the intervention. Future studies should consider including a control group to better isolate the effects of the intervention.
5 Conclusion
This study highlights the potential of a six-week team-based step challenge on university employees’ PA with an average increase of almost 20% in daily step count. However, the effectively boosted short-term activity was not maintained post-challenge. Further, step count increase was modulated by personal, work-related and team composition factors. Most beneficial outcomes might be achieved for male and older individuals, for leaders and science support staff, for those with prior experience and already active subjects, while several other groups in the higher educational setting may not be attracted in a similar way.
This strengthens the notion that both diverse employee demographics and organizational structures as well as the complexity of integrating PA enhancing interventions into daily routines represent typical barriers for the higher educational setting (38, 40).
A particularly notable insight from our study is the role of leadership on PA changes. Leaders demonstrated higher increases in step counts, likely due to strong goal orientation or a desire to lead by example. However, their presence alone did not significantly trigger team-wide activity levels, suggesting that leadership alone is not sufficient to drive collective behavior change. Actively involving and equipping leaders to support and motivate their teams might enhance the effectiveness of future programs.
Future research should therefore explore how different leadership styles influence participation and engagement in workplace PA programs. Interventions that actively involve and equip leaders to support and motivate their teams may enhance the overall impact of such programs. Additionally, strategies are needed to reach the less active individuals and more sedentary groups, as well as ways to keep them engaged and motivated throughout the challenge. A more diverse participant pool would additionally enlighten our understanding of how different demographic groups engage in PA challenges. Additionally, given the rising prevalence of remote work, developing tailored interventions for this population is increasingly important. Research is also needed to identify ways to sustain PA gains.
For institutions, these results suggest that short-term, low-cost digital interventions can be effective in initiating PA improvements. However, for long-term impact, such programs should be embedded into broader workplace health promotion strategies. This includes leadership training to support team motivation, personalized approaches for different employee groups, and support for integrating PA into daily routines.
Overall, our findings highlight the complexity of influencing factors on PA behavior and emphasize the need for personalized, sustainable interventions to promote long-term activity across diverse populations and how this is related to leadership support.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Julius-Maximilians-University of Würzburg Faculty of Human Sciences Ethics Committee for the Master of Science Exercise Science & Training. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
HM: Visualization, Project administration, Formal analysis, Resources, Data curation, Writing – review & editing, Methodology, Conceptualization, Software, Writing – original draft, Investigation. KB-D: Resources, Writing – review & editing, Project administration. OH: Data curation, Project administration, Methodology, Conceptualization, Supervision, Writing – review & editing, Investigation. AR: Writing – review & editing, Project administration, Visualization, Validation, Methodology, Conceptualization. AS: Conceptualization, Writing – review & editing, Methodology, Investigation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to thank all the participants of this intervention.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that Gen AI was used in the creation of this manuscript. Generative AI tools (e.g., ChatGPT by OpenAI) were used during the preparation of this manuscript to support language editing, improve clarity, and check for consistency in phrasing. All intellectual content, analysis, and interpretations presented in the paper are the sole work of the authors.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^Examples of survey questions (originally in German) include: “Do you have personnel responsibility at work?” (Yes/No), “How do you usually commute from home to workplace?” (On foot/By bike/By public transport/By car), and “On how many days per week do you regularly engage in physical activity in your free time for at least 30 min?” (No regular activity/1 day/2–3 days/4–5 days/6–7 days).
References
1. Ryde, GC, Brown, HE, Gilson, ND, and Brown, WJ. Are we chained to our desks? Describing desk-based sitting using a novel measure of occupational sitting. J Phys Act Health. (2014) 11:1318–23. doi: 10.1123/jpah.2012-0480
2. Chau, JY, van der Ploeg, HP, Merom, D, Chey, T, and Bauman, AE. Cross-sectional associations between occupational and leisure-time sitting, physical activity, and obesity in working adults. Prev Med. (2012) 54:195–200. doi: 10.1016/j.ypmed.2011.12.020
3. Chaudhary, N, Jones, M, Rice, SP, Zeigen, L, and Thosar, SS. Transitioning to working from home due to the COVID-19 pandemic significantly increased sedentary behavior and decreased physical activity: a meta-analysis. Int J Environ Res Public Health. (2024) 21:851. doi: 10.3390/ijerph21070851
4. Ng, SW, and Popkin, BM. Time use and physical activity: a shift away from movement across the globe. Obes Rev. (2012) 13:659–80. doi: 10.1111/j.1467-789X.2011.00982.x
5. Pronk, NP, Martinson, B, Kessler, RC, Beck, AL, Simon, GE, and Wang, P. The association between work performance and physical activity, cardiorespiratory fitness, and obesity. J Occup Environ Med. (2004) 46:19–25. doi: 10.1097/01.jom.0000105910.69449.b7
6. World Health Organization. WHO guidelines on physical activity and sedentary behaviour. Geneva: World Health Organization (2020).
7. Ao, Z, He, H, Shi, H, and Liu, H. Step count and multiple health outcomes: an umbrella review. J Evid Based Med. (2024) 17:278–95. doi: 10.1111/jebm.12596
8. Blair, SN, and Morris, JN. Healthy hearts-and the universal benefits of being physically active: physical activity and health. Ann Epidemiol. (2009) 19:253–6. doi: 10.1016/j.annepidem.2009.01.019
9. Singh, B, Olds, T, Curtis, R, Dumuid, D, Virgara, R, Watson, A, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. (2023) 57:1203–9. doi: 10.1136/bjsports-2022-106195
10. Pedersen, BK, and Saltin, B. Exercise as medicine—evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. (2015) 25:1–72. doi: 10.1111/sms.12581
11. Sheng, M, Yang, J, Bao, M, Chen, T, Cai, R, Zhang, N, et al. The relationships between step count and all-cause mortality and cardiovascular events: a dose-response meta-analysis. J Sport Health Sci. (2021) 10:620–8. doi: 10.1016/j.jshs.2021.09.004
12. Bernacki, EJ, and Baun, WB. The relationship of job performance to exercise adherence in a corporate fitness program. J Occup Med. (1984) 26:529–31.
13. Robison, JI, Rogers, MA, Carlson, JJ, Mavis, BE, Stachnik, T, Stoffelmayr, B, et al. Effects of a 6-month incentive-based exercise program on adherence and work capacity. Med Sci Sports Exerc. (1992) 24:85–93. doi: 10.1249/00005768-199201000-00015
14. Ryde, GC, Tomaz, SA, Sandison, K, Greenwood, C, and Kelly, P. Measuring productivity, perceived stress and work engagement of a nationally delivered workplace step count challenge. Int J Environ Res Public Health. (2022) 19:19. doi: 10.3390/ijerph19031843
15. Santos, IL, and Miragaia, D. Physical activity in the workplace: a cost or a benefit for organizations? A systematic review. Int J Workplace Health Manag. (2023) 16:108–35. doi: 10.1108/IJWHM-04-2021-0076
16. Halling Ullberg, O, Toivanen, S, Tillander, A, and Bälter, K. Workplace health promotion to facilitate physical activity among office workers in Sweden. Front Public Health. (2023) 11:1175977. doi: 10.3389/fpubh.2023.1175977
17. Patel, MS, Volpp, KG, Rosin, R, Bellamy, SL, Small, DS, Fletcher, MA, et al. A randomized trial of social comparison feedback and financial incentives to increase physical activity. Am J Health Promot. (2016) 30:416–24. doi: 10.1177/0890117116658195
18. Poirier, J, Bennett, WL, Jerome, GJ, Shah, NG, Lazo, M, Yeh, H-C, et al. Effectiveness of an activity tracker- and internet-based adaptive walking program for adults: a randomized controlled trial. J Med Internet Res. (2016) 18:e34. doi: 10.2196/jmir.5295
19. Johannesson, M, Östling, R, and Ranehill, E. The effect of competition on physical activity: a randomized trial. BE J Econ Anal Policy. (2010) 10:10. doi: 10.2202/1935-1682.2555
20. Wang, J, Fang, Y, Frank, E, Walton, MA, Burmeister, M, Tewari, A, et al. Effectiveness of gamified team competition as mHealth intervention for medical interns: a cluster micro-randomized trial. NPJ Digit Med. (2023) 6:4. doi: 10.1038/s41746-022-00746-y
21. Abraham, C, and Graham-Rowe, E. Are worksite interventions effective in increasing physical activity? A systematic review and meta-analysis. Health Psychol Rev. (2009) 3:108–44. doi: 10.1080/17437190903151096
22. Adams, MA, Hurley, JC, Todd, M, Bhuiyan, N, Jarrett, CL, Tucker, WJ, et al. Adaptive goal setting and financial incentives: a 2 × 2 factorial randomized controlled trial to increase adults’ physical activity. BMC Public Health. (2017) 17:286. doi: 10.1186/s12889-017-4197-8
23. Schembre, SM, Liao, Y, Robertson, MC, Dunton, GF, Kerr, J, Haffey, ME, et al. Just-in-time feedback in diet and physical activity interventions: systematic review and practical design framework. J Med Internet Res. (2018) 20:e106. doi: 10.2196/jmir.8701
24. Brett, CE, and Pires-Yfantouda, R. Enhancing participation in a national pedometer-based workplace intervention amongst staff at a Scottish university. Int J Health Promot Educ. (2017) 55:215–28. doi: 10.1080/14635240.2017.1329632
25. Tullar, JM, Walker, TJ, Page, TF, Taylor, WC, Roman, R, and Amick, BC. Evaluation of a worksite-based small group team challenge to increase physical activity. Am J Health Promot. (2019) 33:259–66. doi: 10.1177/0890117118784229
26. Patel, MS, Asch, DA, Rosin, R, Small, DS, Bellamy, SL, Eberbach, K, et al. Individual versus team-based financial incentives to increase physical activity: a randomized, controlled trial. J Gen Intern Med. (2016) 31:746–54. doi: 10.1007/s11606-016-3627-0
27. Kassavou, A, Turner, A, and French, DP. Do interventions to promote walking in groups increase physical activity? A meta-analysis. Int J Behav Nutr Phys Act. (2013) 10:18. doi: 10.1186/1479-5868-10-18
28. Estabrooks, PA, Harden, SM, and Burke, SM. Group dynamics in physical activity promotion: what works? Soc Personal Psychol Compass. (2012) 6:18–40. doi: 10.1111/j.1751-9004.2011.00409.x
29. Pearson, E, Prapavessis, H, Higgins, C, Petrella, R, White, L, and Mitchell, M. Adding team-based financial incentives to the carrot rewards physical activity app increases daily step count on a population scale: a 24-week matched case control study. Int J Behav Nutr Phys Act. (2020) 17:139. doi: 10.1186/s12966-020-01043-1
30. Safi, A, Deb, S, Kelly, A, Cole, M, Walker, N, and Zariwala, MG. Incentivised physical activity intervention promoting daily steps among university employees in the workplace through a team-based competition. Front Public Health. (2024) 11:1121936. doi: 10.3389/fpubh.2023.1121936
31. Freak-Poli, RL, Cumpston, M, Albarqouni, L, Clemes, SA, and Peeters, A. Workplace pedometer interventions for increasing physical activity. Cochrane Database Syst Rev. (2020) 7:CD009209. doi: 10.1002/14651858.CD009209.pub3
32. Lock, M, Post, D, Dollman, J, and Parfitt, G. Efficacy of theory-informed workplace physical activity interventions: a systematic literature review with meta-analyses. Health Psychol Rev. (2021) 15:483–507. doi: 10.1080/17437199.2020.1718528
33. To, QG, Chen, TT, Magnussen, CG, and To, KG. Workplace physical activity interventions: a systematic review. Am J Health Promot. (2013) 27:e113–23. doi: 10.4278/ajhp.120425-LIT-222
34. Bravata, DM, Smith-Spangler, C, Sundaram, V, Gienger, AL, Lin, N, Lewis, R, et al. Using pedometers to increase physical activity and improve health: a systematic review. JAMA. (2007) 298:2296–304. doi: 10.1001/jama.298.19.2296
35. Mason, MR, Ickes, MJ, Campbell, MS, and Bollinger, LM. An incentivized, workplace physical activity intervention preferentially increases daily steps in inactive employees. Am J Health Promot. (2018) 32:638–45. doi: 10.1177/0890117117723803
36. Innstrand, ST, and Christensen, M. Healthy universities. The development and implementation of a holistic health promotion intervention programme especially adapted for staff working in the higher educational sector: the ARK study. Glob Health Promot. (2020) 27:68–76. doi: 10.1177/1757975918786877
37. Plotnikoff, R, Collins, CE, Williams, R, Germov, J, and Callister, R. Effectiveness of interventions targeting health behaviors in university and college staff: a systematic review. Am J Health Promot. (2015) 29:e169–87. doi: 10.4278/ajhp.130619-LIT-313
38. Newton, J, Dooris, M, and Wills, J. Healthy universities: an example of a whole-system health-promoting setting. Glob Health Promot. (2015) 23:57–65. doi: 10.1177/1757975915601037
39. Boland, T, and Fowler, A. A systems perspective of performance management in public sector organisations. Int J Public Sect Manag. (2000) 13:417–46. doi: 10.1108/09513550010350832
40. Gilson, N, McKenna, J, and Cooke, C. Experiences of route and task-based walking in a university community: qualitative perspectives in a randomized control trial. J Phys Act Health. (2008) 5:S176–82. doi: 10.1123/jpah.5.s1.s176
41. Molanorouzi, K, Khoo, S, and Morris, T. Motives for adult participation in physical activity: type of activity, age, and gender. BMC Public Health. (2015) 15:15. doi: 10.1186/s12889-015-1429-7
42. Vašíčková, J, Hřebíčková, H, and Groffik, D. Gender, age and body mass differences influencing the motivation for physical activity among polish youths. J Sports Sci. (2014) 2:1–12.
43. Ortega Martínez, LM, Araya Vargas, GA, Smith Castro, V, and Hernández Campos, M. Influencia Del Sexo En La Motivación Para La Actividad Física Y Deporte: un Meta-Análisis. [Influence of sex on motivation for physical activity and sport: a meta-analysis]. Retos. (2024) 55:1081–93. doi: 10.47197/retos.v55.103811
44. Capel, T, Schnittert, JF, Snow, S, and Vyas, D. Exploring motivations of young adults to participate in physical activities. CHI'15 (2015):1409–1414
45. Bassett, DR, Wyatt, HR, Thompson, H, Peters, JC, and Hill, JO. Pedometer-measured physical activity and health behaviors in U.S. adults. Med Sci Sports Exerc. (2010) 42:1819–25. doi: 10.1249/MSS.0b013e3181dc2e54
46. Hoert, J, Herd, AM, and Hambrick, M. The role of leadership support for health promotion in employee wellness program participation, perceived job stress, and health behaviors. Am J Health Promot. (2018) 32:1054–61. doi: 10.1177/0890117116677798
47. Weinstein, M, and Cheddie, K. Adoption and implementation barriers for worksite health programs in the United States. Int J Environ Res Public Health. (2021) 18:18. doi: 10.3390/ijerph182212030
48. Yao, L, Li, P, and Wildy, H. Health-promoting leadership: concept, measurement, and research framework. Front Psychol. (2021) 12:12. doi: 10.3389/fpsyg.2021.602333
49. Turgut, S, Schlachter, S, Michel, A, and Sonntag, K. Antecedents of health-promoting leadership and workload as moderator. J Leadersh Organ Stud. (2020) 27:203–14. doi: 10.1177/1548051819848988
50. Schaufeli, W. Engaging leadership: how to promote work engagement? Front Psychol. (2021) 12:754556. doi: 10.3389/fpsyg.2021.754556
51. Burton, JP, Hoobler, JM, and Scheuer, ML. Supervisor workplace stress and abusive supervision: the buffering effect of exercise. J Bus Psychol. (2012) 27:271–9. doi: 10.1007/s10869-011-9255-0
52. Middlehurst, R, Goreham, H, and Woodfield, S. Why research leadership in higher education? Exploring contributions from the UK’S leadership foundation for higher education. Leadership. (2009) 5:311–29. doi: 10.1177/1742715009337763
53. Branson, CM, Franken, M, and Penney, D. Middle leadership in higher education. Educ Manag Adm Leadersh. (2016) 44:128–45. doi: 10.1177/1741143214558575
54. Hoffmann, TC, Glasziou, PP, Boutron, I, Milne, R, Perera, R, Moher, D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. (2014) 348:g1687. doi: 10.1136/bmj.g1687
55. Instingo. Gauting (2025). Available online at: https://www.instingo.de/en/ (accessed March 03, 2025)
56. Kang, M, Zhu, W, Tudor-Locke, C, and Ainsworth, B. Experimental determination of effectiveness of an individual information-centered approach in recovering step-count missing data. Meas Phys Educ Exerc Sci. (2005) 9:233–50. doi: 10.1207/s15327841mpee0904_3
57. Althoff, T, Sosič, R, Hicks, JL, King, AC, Delp, SL, and Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature. (2017) 547:336–9. doi: 10.1038/nature23018
58. Lier, LM, and Breuer, C. The motivating power of gamification: does the inclusion of game elements increase the effectiveness of worksite health promotion programs? Int J Workplace Health Manag. (2020) 13:1–15. doi: 10.1108/IJWHM-04-2019-0055
59. Gupta, ND, Poulsen, A, and Villeval, MC. Male and female competitive behavior–experimental evidence. IZA Discussion Paper No. 1833. (2005). doi: 10.23668/psycharchives.8969
60. Terzano, K, and Morckel, VC. Walk or bike to a healthier life: commuting behavior and recreational physical activity. Environ Behav. (2011) 43:488–500. doi: 10.1177/0013916510366644
61. Puig-Ribera, A, McKenna, J, Gilson, N, and Brown, WJ. Change in work day step counts, wellbeing and job performance in Catalan university employees: a randomised controlled trial. Promot Educ. (2008) 15:11–6. doi: 10.1177/1025382308097693
62. Locke, EA, Latham, GP, and Erez, M. The determinants of goal commitment. Acad Manag Rev. (1988) 13:23–39. doi: 10.2307/258352
63. Latham, GP, and Locke, EA. New developments in and directions for goal-setting research. Eur Psychol. (2007) 12:290–300. doi: 10.1027/1016-9040.12.4.290
Keywords: health promotion, occupational health, exercise, walking, leadership, workplace intervention, team-based challenge
Citation: Manger H, Beck-Doßler K, Hoos O, Reusch A and Szczesny A (2025) Do leaders walk the extra mile? The contribution of personal and work-related factors on daily step count increase in a university team step challenge. Front. Public Health. 13:1648761. doi: 10.3389/fpubh.2025.1648761
Edited by:
Jenna L. Scisco, Eastern Connecticut State University, United StatesReviewed by:
Carrie Bulger, Quinnipiac University, United StatesMurali Krishnan, National Institute of Epidemiology (ICMR), India
Copyright © 2025 Manger, Beck-Doßler, Hoos, Reusch and Szczesny. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helena Manger, aGVsZW5hLm1hbmdlckB1bmktd3VlcnpidXJnLmRl
†ORCID: Helena Manger, https://orcid.org/0009-0003-6333-6222