 John Marwa Gikaro1,2
John Marwa Gikaro1,2 George Claud Goi1†
George Claud Goi1† Farida Hassan Taamala1†
Farida Hassan Taamala1† Hussein Hamisi Hamadi1†
Hussein Hamisi Hamadi1† Jenifa Charles Welema1†
Jenifa Charles Welema1† Zakia Mussa Minduva1†
Zakia Mussa Minduva1† Elia Asanterabi Swai1,2,3,4*
Elia Asanterabi Swai1,2,3,4*- 1Department of Physiotherapy, School of Rehabilitation Medicine, KCMC University, Moshi, Tanzania
- 2Department of Physiotherapy, Kilimanjaro College of Health and Allied Sciences, Moshi, Tanzania
- 3Department of Epidemiology and Global Health, Umeå University, Umeå, Sweden
- 4Department of Community Medicine and Rehabilitation, Umeå University, Umeå, Sweden
Background: Musculoskeletal disorders (MSDs) are among the top conditions that affect the working population including teachers. Historically, Kilimanjaro region including Moshi municipal, has been a pioneer in education development in Tanzania. Moshi municipality represent a diverse setting of primary and secondary education; however, no study has yet examined MSDs among teachers in this setting.
Objective: The aim of this study was to investigate the prevalence of MSDs among primary and secondary school teachers, and identify the associated factors.
Methodology: A cross-sectional study was conducted among 205 primary and secondary school teachers in Moshi Municipal, Northern Tanzania. Data was collected using a structured questionnaire that incorporated the Standardized Nordic Musculoskeletal Questionnaire (SNMQ). Logistic regression model was used to estimate the factors associated with MSDs.
Results: The 12-month and 7-day prevalence of MSDs in one or more body sites was 61.5% and 44.4%, respectively. Twelve-month prevalence was higher in the lower back (44.4%), followed by the neck (31.2%), upper back (26.8%), and shoulders (18.5%). Seven-day prevalence was higher in the lower back (29.8%), followed by the neck (16.1%), ankles/feet (12.2%), and upper back (9.8%). Predictors of MSDs at different body parts were the age, gender, BMI, working duration, number of working hours, number of classes, and number of students in class.
Conclusion: Occupational factors significantly contribute to MSDs among teachers. Complying to recommended workload for teachers may help to prevent MSDs in teaching profession.
Introduction
Musculoskeletal disorders (MSDs) are among the commonest conditions in the working population that is engaged in jobs that involve repetitive tasks, prolonged static or awkward postures, and manual handling (1). MSDs affect body structures such as muscles, tendons, ligaments, fascia, nerves and joints depending on their involvement with job tasks (2); for instance, a fault to a muscle or tendon may transpire because of overuse, or prolonged awkward posture. MSDs occur in highly mobile body parts such as the neck and back, weight bearing joints such as hips and knees, and major muscle groups such as paraspinals and shoulder stabilizers that maintain body posture during working (3).
The teaching profession, especially in lower levels, involves physical and psychological demands that make teachers highly vulnerable to MSDs (4). Teachers are required to maintain prolonged static postures such as standing or sitting during preparation of lessons, lecturing, or marking assignments (5, 6). Similarly, teachers are exposed to repetitive tasks such as writing on boards, grading papers, and when using assistive teaching equipment (7, 8). Low teacher-to-student ratio increases the workloads that have both physical and psychological demands. In general, prolonged postures lead to fatigue; repetitive tasks lead to microinjuries; poorly designed furniture at work, particularly in low resourced areas, lead to strain; and high workloads pose a significant risk for teachers to develop MSDs at work (4, 6, 9). Additionally, psychosocial work stressors of the profession exacerbate tension in major muscle involved in maintaining posture, which can increase the risk of developing MSDs (10). Treating teachers with MSDs has been proven to increase healthcare costs (4). MSDs can negatively influence active engagement in teaching tasks leading to decreased productivity (11). Moreover, absenteeism caused by MSDs is likely to interfere with the students’ learning environment potentially leading to reduced academic performance (12). Research shows that MSDs are among the top occupational hazards in teaching profession across the globe (13). In recent years, highest prevalence of MSDs among teachers have been recorded in Brazil (6), Chile (14), Taiwan (15), Saudi Arabia (16), Pakistan (17), Nigeria (18), and Cameroon (19). While, lower records have been reported in Turkey (20), Iran (21), and Sweden (22). Additionally, in Chile, the prevalence of MSDs among teachers in urban public school was slightly higher than that of teachers from rural areas (23). Tanzania, like many developing countries, faces unique challenges in its education, especially overcrowded classrooms, and poor infrastructure. However, there is limited scrutiny of potential contextual factors unique to teaching profession in Tanzania. As a result, little is known regarding the magnitude of the MSDs among teachers, associated factors, and intervention that aligns with the national health system.
Kilimanjaro region is one of the regions with highest number of primary and secondary schools in Tanzania. Moshi municipal alone, the administrative and economic capital of Kilimanjaro region, has a total of 80 primary and secondary schools. The introduction of the free primary and secondary education system has improved the number of pupils attending school; however, the teacher–student ratio and other occupational factors could influence teachers experience on MSDs, especially in a setting with diverse education settings like Moshi municipality. Studying teachers in Moshi municipality gives a reflection of teachers in the region, that may represent majority in the country. Our study aimed at exploring the prevalence and factors associated with MSDs among primary and secondary school teachers in Northern Tanzania. We believe that the insights obtained from this study could be useful in setting baseline prevention and intervention strategies for MSDs among primary and secondary teachers in the country.
Materials and methods
Study design and participants
This cross-sectional study was conducted from June to July 2024 in 14 public primary and secondary schools in Moshi Municipal, Kilimanjaro region, Tanzania. Teachers in respective schools who met inclusion criteria were included in the study. We included teachers from public schools. Exclusion criteria were working experience of less than 1 year, recent surgeries/trauma, and systemic conditions, for example systemic lupus erythromatosus and Rheumatoid arthritis, for they directly affect musculoskeletal system. Multi-stage sampling technique was used to obtain study participants. Researchers identified the 21 wards in Moshi Municipality, with a total of 80 schools (52 primary and 28 secondary schools). In the initial stage, 10 out of 21 wards were selected using simple random technique. All 31 schools from the 10 wards were listed using numerals 1–31. We included schools that happened to be assigned even numbers. Generally, 14 public schools (eight primary and six secondary schools) were systematically selected. Finally, simple random sampling was used to select participants from the selected schools. The total number of teachers in Moshi municipal at the time of data collection was 567. Cochran’s formula for finite population (24) was used to estimate sample size. The estimated sample size was 230, however, 205 teachers who were present during the time of data collection, and willing to participate in the study were recruited.
Data collection
Data were collected using a self-reported structured questionnaire that incorporated the Standardized Nordic Musculoskeletal Questionnaire (SNMQ). The questionnaire had three parts: Part A regarding demographic characteristics, Part B inquiring about occupational factors, and Part C with information of body parts with MSDs according to SNMQ (25). Pilot study was done to validate the questionnaire prior to actual data collection. Ten teachers, five from primary school and five from secondary school, were conveniently recruited to participate in the pilot study. They were instructed to complete the questionnaire and provide feedback that was used to improve its clarity and validity. Data gathered during piloting was not included in final analysis. Participants were asked to fill in all relevant parts of the questionnaire and collect as soon as they finished. All participants provided written consent, and they were free to withdraw from the study any time they felt like so. All procedures were conducted according to the Helsinki Declaration. Permission to conduct this study was ratified by the College Research Ethics Review Committee (No. UG.132/2024), and Moshi Municipal Council (Ref. No. MMC/A.40/13/1VOL.33/332).
Musculoskeletal disorders
The SNMQ was used for evaluating MSDs among teachers. The questionnaire provides information about pain prevalence in 12 body areas, that is, the neck, shoulders, elbows/forearms, wrists/hands, upper back, lower back, hips/thighs, knees, and feet/ankles. The tool inquires information about pain/discomfort/ache in any of the areas for the past 12 months, and 7 days. Also, the tool help to investigate whether there were limitations caused by the MSDs at home or work.
Data analysis
Collected data were entered in Microsoft Excel. Data cleaning was done to check for errors during data entry. Data was then imported to R software for Windows (version 4.4.1) for further management and analysis. Findings for descriptive statistics were presented using frequencies, percentages, and chi-square test. Shapiro–Wilk normality test was used to determine the distribution of continuous variables. Continuous variables that were normally distributed were processed using means with respective standard deviations (M ± SD), non-normally distributed variables were presented using medians and respective interquartile ranges (IQR). Sociodemographic, anthropometric, and occupational factors among teachers were compared by gender. Prevalence of MSDs were presented as frequency and percentage according to presence in the previous 12 months and 7 days. To account for participants with MSDs in multiple body sites, grouping was done into percentile 50 according to the previous 12 months and 7 days, where in both cases p50 was 2. MSDs were compared with sociodemographic and occupational variables among teachers with MSDs in two painful regions or less (≤p50) or more than two painful regions (>p50). Physical activity level was classified according to recommendations of the World Health Organization: adequate, if the participant engaged in moderate-intensity physical activity for at least 150 min per week, and inadequate, if the time for moderate-intensity physical activity was less than 150 min in a week. Categorical variables were compared using the chi-squared and Fisher exact tests for the association. Backward elimination method, with p-value set at 0.05, was used to select the predictor factors that were suitable to fit the model. Logistic regression models were conducted to analyze the association between the MSDs (≤p50 and >p50) and selected factors with reference to absence of MSDs (no MSDs). The statistical significance was set at p < 0.05 (95% confidence interval). Finally, the Hosmer–Lemeshow test was used to evaluate the models’ goodness of fit, where values above 0.05 indicated that the model fit the data.
Results
Demographic characteristics
Shapiro test showed that data for BMI and age were not normally distributed (p < 0.05). Majority of participants were females (62%), and aged less than 40 years (50.2%) with median age of 39 years. The proportion of MSDs was high in females (66.1%) than in males (50%). For the past 12 month, 61.5% of the participants had MSDs in one or more body site, females leading. Similarly, over the past 7 days, 44.4% of participants had MSDs in one or more body sites. The proportion of females with limitations resulting from MSDs was nearly twice as males. The proportion of females who were obese was over two times higher (37%) than males (17.9%). Female teachers with certificate level of education were over four times (14.2%) compared to males (3.8%). The detailed participant characteristics is given in Table 1.
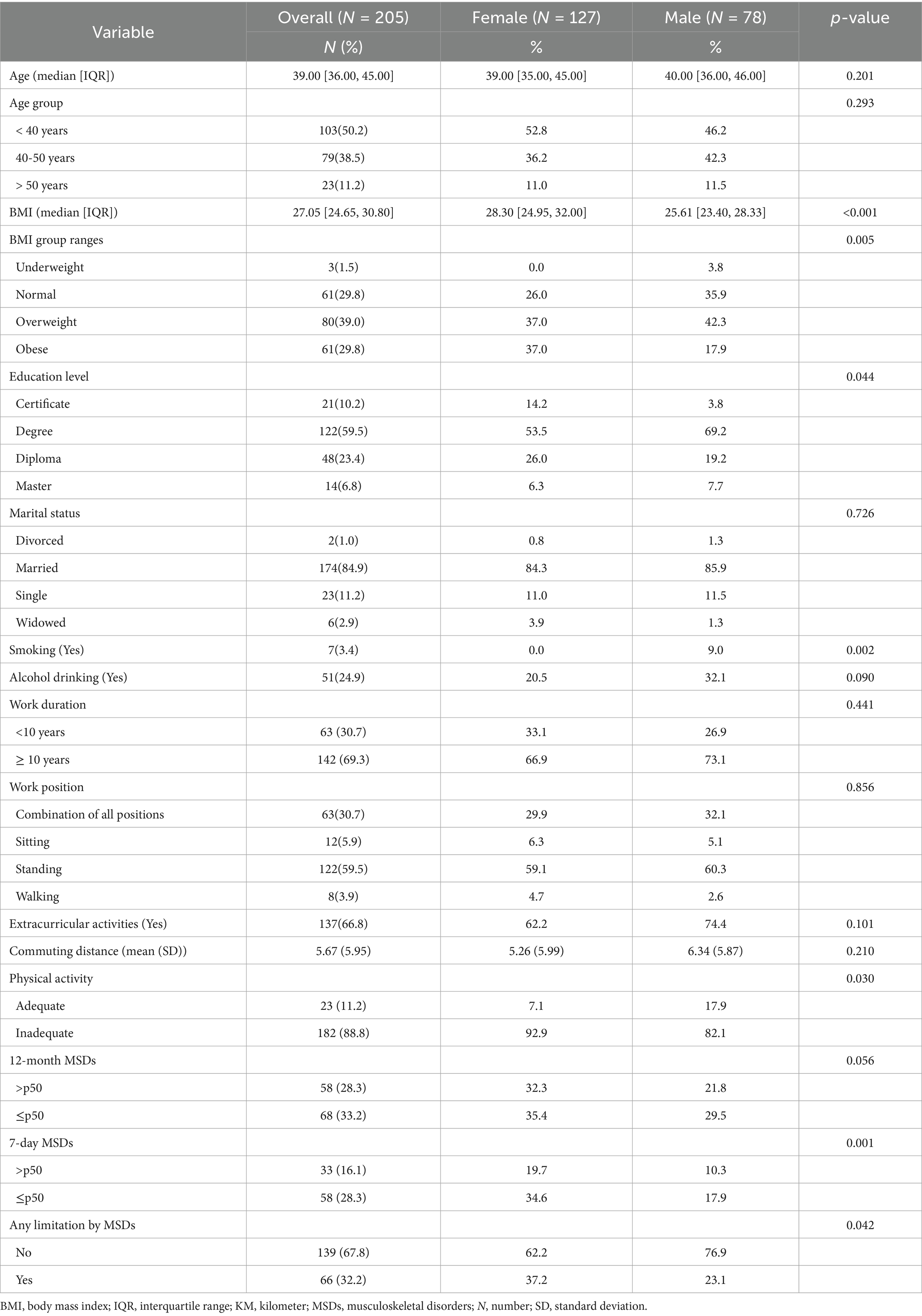
Table 1. Demographic characteristics stratified by gender.
Prevalence of MSDs
For the past 12 months, MSDs were higher in the lower back (44.4%), followed by the neck (31.2%), upper back (26.8), and shoulders (18.5). Nearly three-quarters of participants with MSDs at the lower back (72.7%) presented with activity limitation at home or work. Correspondingly, more than half of participants with MSDs at neck (56.1%), and upper back (51.5%) were limited from normal work. For the past 7 days, MSDs were higher in the lower back (29.8%), followed by the neck (16.1%), ankles/feet (12.2%), upper back (9.8%), shoulders (9.8%), and knees (8.8%). Over half (53%) of participants with MSDs at the lower back were limited from normal work at home or away from home, while over a quarter of participants with MSDs at the ankle/feet (25.8%), and neck (28.8%) were limited from normal work. Prevalence of MSDs at each body site is provided in Table 2.
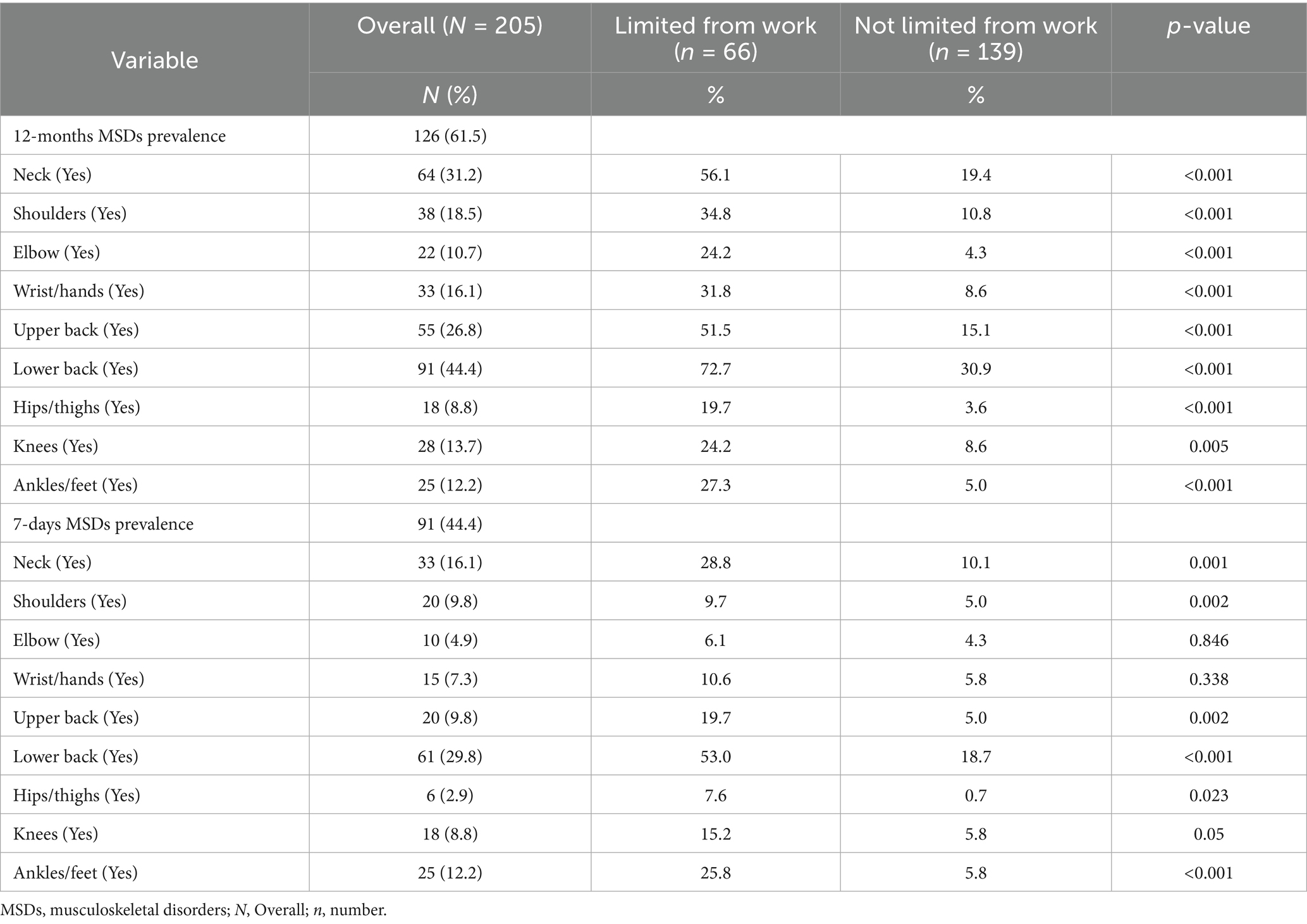
Table 2. Prevalence of MSDs in the past 12-months, and 7-days stratified by limitation from work.
Association between presence of MSDs and occupational factors
The logistic regression model for 12-month MSDs prevalence showed that there was a significant positive association between presence of MSDs in two or less body sites (≤p50) and BMI (OR = 1.14, p = 0.001), and number of working hours per day (OR = 1.175, p = 0.008). Additionally, MSDs in more than two body sites (>p50) was positively and significantly associated with BMI (OR = 1.19, p < 0.001), and number of classes (OR = 1.48, p = 0.047). Details of variables selected by backward elimination for the model, and odds ratios with respective 95% confidence intervals are shown in Table 3.
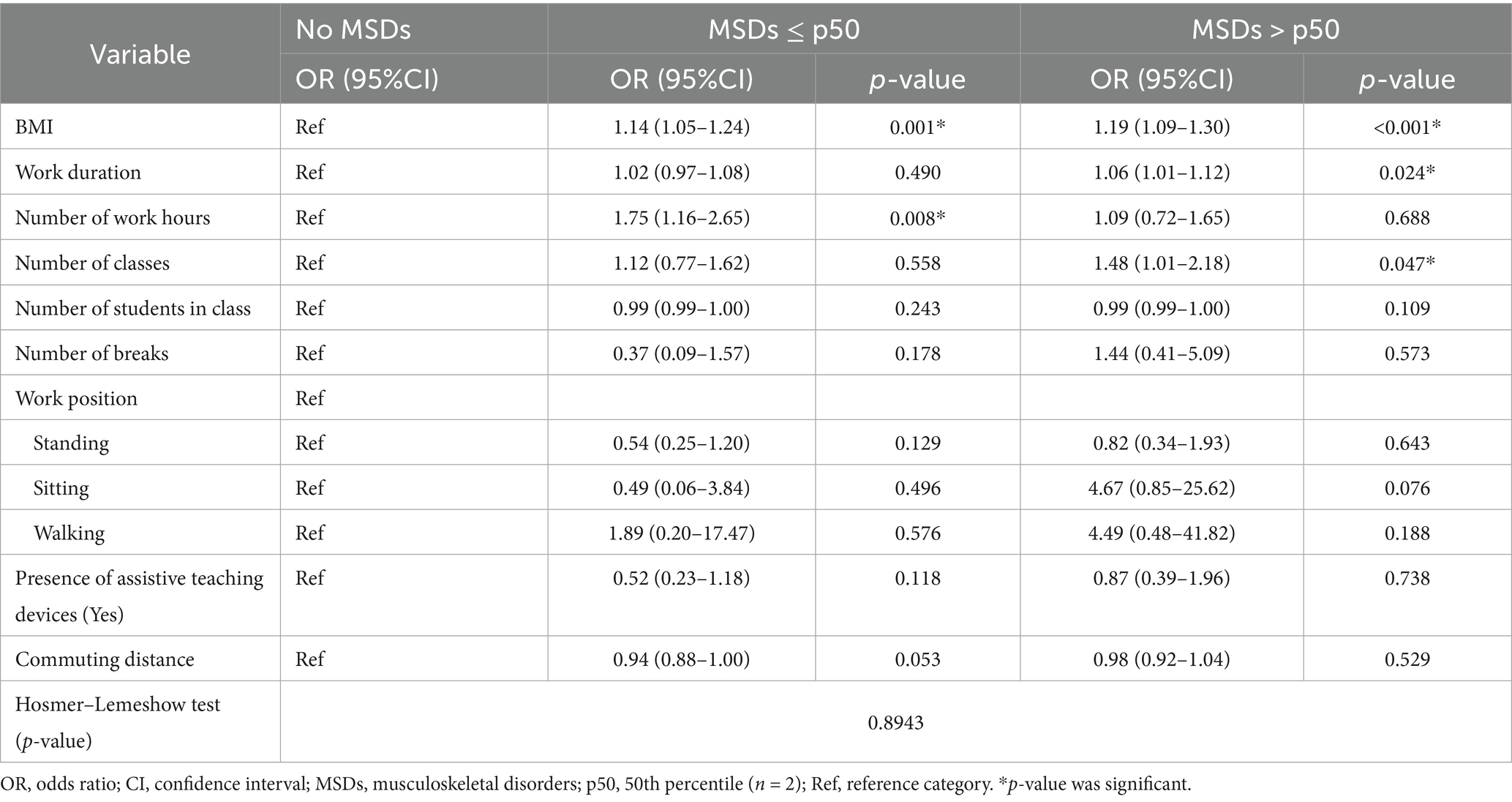
Table 3. Factors associated with 12-month MSDs prevalence.
The 7-day MSDs prevalence regression model revealed that there was a significant positive association between MSDs at two or less body sites (≤p50) and female gender (OR = 2.87, p = 0.008), and number of students in class (OR = 1.01, p = 0.023). On the other hand, MSDs at more than two body sites (>p50) was positively and significantly associated with age (OR = 1.08, p = 0.009), and BMI (OR = 1.12, p = 0.013). Variables retained during backward stepwise elimination method, odds ratios and respective 95% confidence intervals are shown in Table 4.
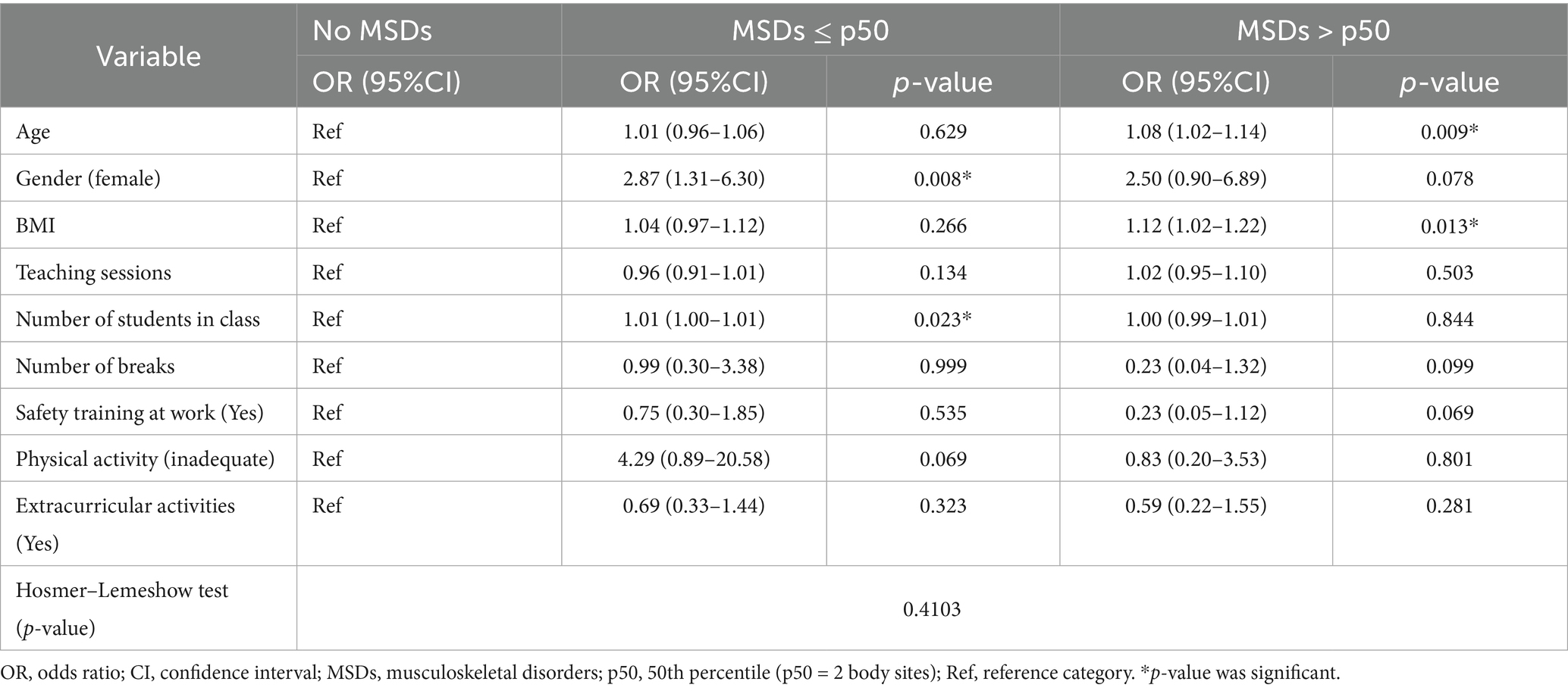
Table 4. Factors associated with 7-day MSDs prevalence.
Association between MSDs in individual body site and occupational factors
Regression analysis for MSDs in specific body was done for all body sites, however, the Hosmer–Lemeshow test only supported the models for the neck (p = 0.090) and low back pain (p = 0.516). The neck model showed that there was a significant positive association between neck MSDs and age (OR = 1.02, p = 0.016), working hours (OR = 1.07, p = 0.037), and number of classes (OR = 1.07, p = 0.039). Interestingly, there was a significant negative association between neck MSDs and number of students in a class (OR = 0.99, p = 0.043). For MSDs at the lower back, there was a significant positive association between low back MSDs and BMI (OR = 1.03, p < 0.001). Supplementary Table S1 provides the details of the variables selected for each body site model using backward elimination method, and corresponding odds rations with their respective 95% confidence intervals.
Discussion
Work-related musculoskeletal disorders (WMSDs) lead to pain, functional dependency, and decreased quality of life, imposing a substantial burden on workers in different fields (26). Direct consequences of WMSDs include absenteeism, reduced productivity, increased healthcare costs, psychological distress, and early retirement (27). Our findings showed that over half of the study participants had MSDs at one or more body sites, females being more affected compared to males. Multiple administrative, ergonomic and lifestyle factors significantly influenced MSDs among teachers.
In the current study, the 12-month prevalence of MSDs among primary and secondary school teachers was 61.5%. This finding is comparable with the findings reported by Durmus and Ilhanli (60.3%) in Turkey (28). Despite the differences in geographical and socioeconomic settings, both studies involved primary school teachers, who are likely to have higher workloads, and whose teaching activities involve multiple repetitive tasks, and static working positions. On the contrary, other studies had demonstrated higher prevalence of MSDs among teachers elsewhere. For example, Kraemer et al. (6) reported that all participants experiences MSDs at one or more body sites, while Cheng et al. (15), and Althomali (16) both found prevalence of over 90%. This large difference noted here could be because the participants were from public schools that usually train more students that could be beyond recommended teacher-to-student ratio, thus subjecting teachers to heavy workload. Also, other teachers were from elementary level where they have to individualize teaching activities based on the need of each student, an overwhelming duty that is likely to cause over exhaustion. On the other hand, the prevalence of less than 50% was reported by Alias et al. (29) and Karakaya et al. (20) in Malaysia and Turkey, respectively. Perhaps significant difference in improved infrastructure, working conditions, and education and health systems compared to Tanzania could be the reason for reduced prevalence. In addition, we found that the proportion of MSDs was high in females than in males. This finding is supported by previous studies that showed that MSDs were significantly higher in female gender than in men (30–32). Perhaps this is because, physiologically, women are more at risk of low muscle mass, early degeneration that may contribute to MSDs.
We found that the most affected part both for the past 7 days and 12 months was the lower back followed by the neck. On the contrary, in Malaysia it was found that the most affected body parts for the past 7 days and 12 months were the feet and knees (29). Also, in Cameroon, the 12-month and seven-day prevalence was higher in the neck followed by the lower back and shoulders (19). Additionally, Ojukwu et al. (18) reported that shoulder and neck had the highest prevalence. The differences observed could perhaps be because of the setup of working environment. For instance, teachers who are subjected to standing for longer periods during teaching, and have many class sessions per week are likely to complain of discomfort at their feet and knees. Likewise, teachers working in prolonged sitting position are at greater risks of developing back and neck pain. Teachers repeatedly writing on the boards, particularly overhead, have higher chances of perceiving ache at the shoulders and neck. Even though teachers all over the world are engaged in nearly similar teaching activities, specific body part may develop MSDs depending on nature of facilities at work, infrastructures, ergonomics knowledge and other lifestyle factors (5).
The current study shows that there was a significant positive association between 12-month prevalence of MSDs and working hours in a day. A similar finding was reported in Taiwan, showing that teachers working for more than recommended duration per week were at higher risks of developing MSDs (15). The probable reason could be because long hours of working expose teachers to exhaustion, prolonged static and awkward positions, or repetitive tasks that are directly associated with MSDs. Also, we found significant positive associations between MSDs in the last 12 months and work duration and number of classes. This observation corresponds to a study by Fahmy et al. (7) that also found that the number of students per classroom and the number of classes per week were positively associated with WMSDs among teachers. The similarity of this finding could be because most teachers across the globe tend to have more workloads. Besides, high number of class sessions and weekly teaching hours increase both physical and mental demands of the job leading to greater risks for MSDs. In addition, we found a strong positive association between multisite MSDs and BMI for the past 12 months. A finding similar to a previous study (33) that showed a significant relationship between BMI and musculoskeletal symptoms in the working population. This relationship could perhaps be due to the fact that high BMI may subject the more mechanical stress to the joints and spine leading to discomfort, ache or pain.
Our study also found that, in addition to BMI, MSDs over the last 7 days was positively associated with age, gender, and number of students. In the current study, age was significantly associated with MSDs at more than two body sites. This finding corresponds to finding from a survival analysis study which showed that biological aging contributed to multiple MSDs that may affect multiple body sites (34). Consequently, a recent study from Nigeria has shown signification difference between males and females for MSDs in favor of males (35). This could be supported by biological factors like lower muscle mass and fluctuations of hormones that influence bone resorption. Also, research shows that high number of students is likely to increase workload for teachers posing a major risk for MSDs (36). This finding from previous study supports our findings that showed that neck pain was positively associated with working hours and number of classes. This conforms to a previous report that awkward postures of the neck and repetitive neck movements are likely increase the risks of MSDs (37).
This study has provided insights on the extent of musculoskeletal disorders among primary and secondary school teachers in a low-resourced country. It was discovered that having MSDs at any part of the body result to difficulties in carrying out normal duties at work. Understanding the magnitude of the MSDs and their associated factors in teaching profession is important in planning respective preventive interventions. The key strengths of our study include the use of multi-stage sampling technique that ensured that every teacher in the municipality had a chance to participate in the study, thus reducing bias. Also, we recruited a relatively representable sample accordingly. However, our study had several limitations: this study being a descriptive cross-sectional study, it could not ascertain the causational relationship as MSDs could be caused by other confounders that were not measured. Nevertheless, the analysis involved fitting regression model that considered both crude and adjusted odds ratios to estimate the associations. Further, the use of a questionnaire that required information from the past 12 months could influence responses to recall bias, however, all participants were given enough time to fill the questionnaire truthfully and correctly as possibly they could. Moreover, gathering data from only teachers who were present on the day of data collection could have subjected out study to selection bias. Also, considering the multifactorial causes of MSDs, such as poor sleep quality and stress, which were not evaluated in this study, affects our impression on the factors observed to influence MSDs. Finally, collecting data from one municipal council may not be generalized across the nation, nonetheless, most municipalities have nearly the same socioeconomic characteristics.
Conclusion
Over 50 % of primary and secondary school teachers in Moshi municipal reported having MSDs at one or more body sites. The most commonly affected areas were the neck, lower and upper back. Occupational factors such as long working hours, high number of classes, number of students in class, and duration of work increased the risk of MSDs among teachers. Additionally, BMI, gender and age were positively associated with MSDs at various body parts. Adhering to recommended classes per week, teacher-pupil ratio, and working hours may help to prevent the MSDs among teachers. Also, active living could be an essential strategy of preventing MSDs among teachers as it plays crucial part in weight management.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by College Research Ethics Review Committee (No. UG.132/2024), and Moshi Municipal Council (Ref. No. MMC/A.40/13/1VOL.33/332). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JG: Project administration, Writing – review & editing, Supervision, Writing – original draft, Formal analysis, Conceptualization. GG: Writing – original draft, Writing – review & editing, Data curation. FT: Data curation, Writing – original draft, Writing – review & editing. HH: Writing – review & editing, Writing – original draft, Data curation. JW: Data curation, Writing – review & editing, Writing – original draft. ZM: Data curation, Writing – review & editing, Writing – original draft. ES: Formal analysis, Writing – review & editing, Supervision, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1654131/full#supplementary-material
References
1. Soares, CO, Pereira, BF, Pereira Gomes, MV, Marcondes, LP, De Campos Gomes, F, and De Melo-Neto, JS. Preventive factors against work-related musculoskeletal disorders: narrative review. Rev Bras Med Trab. (2019) 17:415–30. doi: 10.5327/Z1679443520190360
2. World Health Organization. Musculoskeletal health (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (Accessed October 2, 2025)
3. National Academies of Sciences Engineering and Medicine. Musculoskeletal Disorders. Selected health conditions and likelihood of improvement with treatment. Washington, D.C.: National Academies Press (2020).
4. Tahernejad, S, Hejazi, A, Rezaei, E, Makki, F, Sahebi, A, and Zangiabadi, Z. Musculoskeletal disorders among teachers: a systematic review and meta-analysis. Front Public Health. (2024) 12:1399552. doi: 10.3389/fpubh.2024.1399552
5. Ramírez-García, CO, Lluguay-Quispillo, DJ, Inga-Lafebre, JD, Cuenca-Lozano, MF, Ojeda-Zambrano, RM, and Cárdenas-Baque, CC. Musculoskeletal disorders in primary school teachers. Sustainability. (2023) 15:1–17.
6. Kraemer, K, Moreira, MF, and Guimarães, B. Musculoskeletal pain and ergonomic risks in teachers of a federal institution. Rev Bras Med Trab. (2020) 18:343–51. doi: 10.47626/1679-4435-2020-608
7. Fahmy, VF, Momen, MAMT, Mostafa, NS, and Elawady, MY. Prevalence, risk factors and quality of life impact of work-related musculoskeletal disorders among school teachers in Cairo. Egypt BMC Public Health. (2022) 22:1–17. doi: 10.1186/s12889-022-14712-6
8. Rahim, AAA, Jeffree, MS, Daud, DMA, Pang, N, and Sazali, MF. Factors associated with musculoskeletal disorders among regular and special education teachers: a narrative review. Int J Environ Res Public Health. (2022) 19:1–10. doi: 10.3390/ijerph191811704
9. Bolarinwa, MA, and Kumapayi, AO. Ergonomic risk assessment of Nigerian teaching personnel: cases of a secondary school and a tertiary institution in Ibadan, Nigeria. Eur J Med Health Sci. (2023) 5:56–62. doi: 10.24018/ejmed.2023.5.4.1865
10. Vargas-Prada, S, and Coggon, D. Psychological and psychosocial determinants of musculoskeletal pain and associated disability. Best Pract Res Clin Rheumatol. (2015) 29:374–90. doi: 10.1016/j.berh.2015.03.003
11. Cappella, E, Kim, HY, Neal, JW, and Jackson, DR. Classroom peer relationships and behavioral engagement in elementary school: the role of social network equity. Am J Community Psychol. (2013) 52:367–79. doi: 10.1007/s10464-013-9603-5
12. Julius, A, and Dorothy, N. The impact of teachers’ absenteeism on students’ academic performance in Uganda. A case study of Busiro-Sub County Wakiso District. Metropolitan J Soc Educ Res. (2024) 3:435–45. doi: 10.37284/eajes.5.2.679
13. Erick, P, Tumoyagae, T, and Masupe, T. Musculoskeletal disorders in the teaching profession In: Ergonomics-New Insights (2022). 1–20.
14. Vega-Fernández, G, Gonzalez-Torres, C, Solis-Soto, M, and Lizana, PA. Musculoskeletal disorders and quality of life for Chilean teachers during the COVID-19 pandemic at the academic year-end. Front Public Health. (2024) 12:1277578. doi: 10.3389/fpubh.2024.1277578
15. Cheng, KHY, Cheng, CY, and Ju, YY. Work-related musculoskeletal disorders and ergonomic risk factors in early intervention educators. Appl Ergon. (2013) 44:134–41. doi: 10.1016/j.apergo.2012.06.004
16. Althomali, OW. Long-term prevalence and risk factors of musculoskeletal disorders among the schoolteachers in Hail, Saudi Arabia: a cross-sectional study. BioMed Res Int. (2022) 2022:1–7. doi: 10.1155/2022/3610196
17. Chand, RK, Roomi, MA, Begum, S, and Mudassar, A. Prevalence of musculoskeletal disorders, associated risk factors and coping strategies among secondary school teachers in Fiji. Rawal Med J. (2020) 45:377–81.
18. Ojukwu, CP, Anyanwu, GE, Eze, B, Chukwu, SC, Onuchukwu, CL, and Anekwu, EM. Prevalence, pattern and correlates of work-related musculoskeletal disorders among school teachers in Enugu, Nigeria. Int J Occup Saf Ergon. (2021) 27:267–77. doi: 10.1080/10803548.2018.1495899
19. Ndongo, JM, Lele, ECB, Guessogo, WR, Meche, LP, Ayina, CNA, Guyot, J, et al. Musculoskeletal disorders among secondary school teachers in Douala, Cameroon: the effect of the practice of physical activities. Front Rehabil Sci. (2022) 3:1–8. doi: 10.3389/fresc.2022.1023740
20. Karakaya, İÇ, Karakaya, MG, Tunç, E, and Kıhtır, M. Musculoskeletal problems and quality of life of elementary school teachers. Int J Occup Saf Ergon. (2015) 21:344–50. doi: 10.1080/10803548.2015.1035921
21. Mohseni Bandpei, MA, Ehsani, F, Behtash, H, and Ghanipour, M. Occupational low back pain in primary and high school teachers: prevalence and associated factors. J Manip Physiol Ther. (2014) 37:702–8. doi: 10.1016/j.jmpt.2014.09.006
22. Arvidsson, I, Simonsen, JG, Lindegård-Andersson, A, Björk, J, and Nordander, C. The impact of occupational and personal factors on musculoskeletal pain - a cohort study of female nurses, sonographers and teachers. BMC Musculoskelet Disord. (2020) 21:1–8. doi: 10.1186/s12891-020-03640-4
23. Vega-Fernández, G, Lera, L, Leyton, B, Cortés, P, and Lizana, PA. Musculoskeletal disorders associated with quality of life and body composition in urban and rural public school teachers. Front Public Health. (2021) 9:607318. doi: 10.3389/fpubh.2021.607318
24. Uakarn, C, Chaokromthong, K, and Sintao, N. Sample size estimation using Yamane and Cochran and Krejcie and Morgan and Green formulas and Cohen statistical power analysis by Gpower and comparisons. APHEIT Int J. (2021) 10:76–88.
25. Kuorinka, I, Jonsson, B, Kilbom, A, Vinterberg, H, Biering-S6rensen, F, Andersson, G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. (1987) 18:233–7. doi: 10.1016/0003-6870(87)90010-x
26. Alhashim, AAA, Alyousof, AA, Aldawsari, MR, Alghannam, AA, Alsayed, MA, Alawadh, RA, et al. Work-related musculoskeletal disorders and their impact on quality of life: a comprehensive review. Saudi J Med Pharm Sci. (2025) 11:360–77. doi: 10.36348/sjmps.2025.v11i05.002
27. Dimitriou, C, Alegakis, A, Karageorgiou, I, Mantadaki, AE, and Symvoulakis, EK. Original paper stress and prevalence of musculoskeletal disorders among the nursing personnel of a tertiary hospital unit in Greece: a cross-sectional study. Curr Health Sci J. (2023) 49:45–53. doi: 10.12865/CHSJ.49.01.45
28. Durmus, D, and Ilhanli, I. Are there work-related musculoskeletal problems among teachers in Samsun, Turkey? J Back Musculoskelet Rehabil. (2012) 25:5–12. doi: 10.3233/BMR-2012-0304
29. Alias, AN, Karuppiah, K, How, V, and Perumal, V. Prevalence of musculoskeletal disorders (MSDs) among primary school female teachers in Terengganu. Malaysia Int J Ind Ergon. (2020) 77:1–8. doi: 10.1016/j.ergon.2020.102957
30. Cavallari, JM, Ahuja, M, Dugan, AG, Meyer, JD, Simcox, N, Wakai, S, et al. Differences in the prevalence of musculoskeletal symptoms among female and male custodians. Am J Ind Med. (2016) 59:841–52. doi: 10.1002/ajim.22626
31. Wijnhoven, HAH, De Vet, HCW, Susan, H, and Picavet, J. Prevalence of musculoskeletal disorders is systematically higher in women than in men. Clin J Pain. (2006) 22:717–24. doi: 10.1097/01.ajp.0000210912.95664.53
32. Rungruangbaiyok, C, Vongvaivanichakul, P, Lektip, C, Sutara, W, Jumpathong, P, Miyake, E, et al. Prevalence and associated factors of musculoskeletal disorders among older patients treated at Walailak university physical therapy Clinic in Thailand: a retrospective study. Int J Environ Res Public Health. (2024) 21:1253. doi: 10.3390/ijerph21091253
33. Viester, L, Verhagen, EA, Hengel, KMO, Koppes, LL, Van Der Beek, AJ, and Bongers, PM. The relation between body mass index and musculoskeletal symptoms in the working population. BMC Musculoskelet Disord. (2013) 14:238. doi: 10.1186/1471-2474-14-238
34. Wei, W, Qi, X, Cheng, B, Zhang, N, Zhao, Y, Qin, X, et al. A prospective study of associations between accelerated biological aging and twenty musculoskeletal disorders. Commun Med. (2024) 4:266. doi: 10.1038/s43856-024-00706-5
35. Afolabi, JO, Abel, PT, and Oyeyemi, AL. Prevalence of musculoskeletal disorders and associated risk factors among undergraduates of a private university in Nigeria. Work. (2025) 82:154–64. doi: 10.1177/10519815251341142
36. Furuta, DT, Tebar, WR, Beretta, VS, Tebar, FG, de Carvalho, AC, Leoci, IC, et al. Analysis of the association between high workload and musculoskeletal pain in public school teachers according to physical activity level. Work. (2024) 78:111–7. doi: 10.3233/WOR-230474
Keywords: work-related musculoskeletal disorders, occupational health, teachers, Tanzania, Moshi municipality
Citation: Gikaro JM, Goi GC, Taamala FH, Hamadi HH, Welema JC, Minduva ZM and Swai EA (2025) Prevalence and factors associated with musculoskeletal disorders among primary and secondary school teachers. Front. Public Health. 13:1654131. doi: 10.3389/fpubh.2025.1654131
Edited by:
Pablo A. Lizana, Pontificia Universidad Católica de Valparaíso, ChileReviewed by:
Jerson Mekoulou, University of Douala, CameroonVishnu B. Menon, Amrita Vishwa Vidyapeetham University, India
Copyright © 2025 Gikaro, Goi, Taamala, Hamadi, Welema, Minduva and Swai. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elia Asanterabi Swai, ZWxpYS5zd2FpQHVtdS5zZQ==
†These authors have contributed equally to this work