 Lin Lan
Lin Lan Xiaoli Chen
Xiaoli Chen Hao Zhang
Hao Zhang LuYing Zhong1,2,3
LuYing Zhong1,2,3- 1Emergency Department of West China Hospital, Sichuan University, Chengdu, China
- 2West China School of Nursing, Sichuan University, Chengdu, China
- 3Institute of Disaster Medicine, Sichuan University, Chengdu, China
- 4Nursing Department of West China Hospital, Sichuan University, Chengdu, China
Objective: This study aims to explore the heterogeneity of burnout among emergency department nurses, identify the factors influencing burnout in different subtypes of emergency nurses, and provide targeted strategies and measures to reduce burnout in emergency department nurses.
Methods: A cross-sectional survey was conducted from December 26, 2023, to January 18, 2024, involving 1,555 emergency nurses from 30 tertiary hospitals in China. The survey was distributed via an online questionnaire platform, which included general demographic information and the Maslach Burnout Inventory (MBI). The collected data were analyzed using latent profile analysis, Kruskal–Wallis H test, and multiple logistic regression.
Results: A total of 1,555 questionnaires were sent out in this survey, and finally 1,540 were included for data analysis. The average burnout score among emergency nurses was (4.77 ± 6.16). Occupational burnout could be categorized into three subtypes: low burnout-low professional efficacy (C1), low burnout-high professional efficacy (C2), and high burnout-low professional efficacy (C3). The proportions of these subtypes were 41%, 32.3%, and 26.7%, respectively. Significant differences in the latent categories of burnout were observed for age (χ2 = 31.749, P < 0.001), education level (χ2 = 6.778, P = 0.034), professional title (χ2 = 21.928, P < 0.001), years of work (χ2 = 29.269, P < 0.001), weekly working hours (χ2 = 52.493, P < 0.001), number of night shifts (χ2 = 34.685, P < 0.001), and monthly income (χ2 = 18.994, P < 0.001).
Conclusion: Occupational burnout is prevalent among emergency nurses, with significant heterogeneity in burnout types. Burnout is associated with age, education level, professional title, number of night shifts, weekly working hours, and monthly income. The heterogeneity of burnout subtypes and their influencing factors provides a basis for future personalized interventions.
1 Introduction
With the continuous development of the global healthcare industry and the increasing demand for emergency medical services, emergency nursing is facing unprecedented challenges. Emergency nurses are required to manage high work pressure, heavy tasks, and complex clinical situations (1, 2), while also handling emotional burdens, long shift hours, and sudden patient needs (3). These factors together contribute to the growing prevalence of burnout among emergency nurses (4). Occupational burnout, a common syndrome among professionals, is recognized by the World Health Organization (WHO) as a work-related chronic stress issue in its International Classification of Diseases (5). Burnout affects nurses' physical and mental health (6) and their quality of work life (7), leading to an increased intention to leave the profession (8). Several international studies have shown that nurse burnout is associated with higher patient mortality, infection rates, length of hospital stays, and failure in resuscitation efforts (9, 10). A cross-national study involving six countries found that the higher the nurse burnout, the lower the nursing quality score (11). Therefore, understanding the causes and mechanisms of occupational burnout in emergency nurses has become an important research topic in emergency nursing. Burnout primarily manifests in three core dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment (12). Emotional exhaustion represents the individual stress dimension of burnout, indicating a state of physical and emotional fatigue resulting from prolonged overuse of emotional resources; it is the most basic and central feature of burnout. Depersonalization represents the interpersonal dimension of burnout, referring to the negative, indifferent, and detached responses individuals show toward work, particularly in relation to their service recipients. Reduced personal accomplishment represents the self-evaluation dimension, indicating a sense of worthlessness, helplessness, and lack of accomplishment in one's work. Although many studies have explored the factors and impacts of burnout (13), there remains a lack of research specifically targeting emergency nurses, especially systematic analyses of the latent factors and characteristics of burnout at different levels. Latent Profile Analysis (LPA) offers significant advantages in identifying latent subgroups within data, handling multidimensional data, avoiding arbitrary classifications, and enhancing classification accuracy. This study aims to conduct a multidimensional latent profile analysis (14) of occupational burnout among emergency nurses, using a quantitative survey to comprehensively explore the latent dimensions and influencing factors of burnout in this group.
2 Methods
2.1 Study design and participants
This study is part of a cross-sectional survey involving 1,540 emergency nurses in China, focusing on their health status, work-related characteristics, and family dynamics. The survey assessed multiple factors, including somatic symptoms, sleep quality, workplace violence, occupational burnout, work environment, work-family role conflict, and occupational stress among emergency nurses. To date, three articles have been published using this dataset, examining: (a) Gender differences in burnout and work-family conflict among emergency nurses (15); (b) The association between effort-reward imbalance and health outcomes in emergency nurses (16); (c) The relationship between workplace violence and occupational health in emergency nurses (17). This study primarily investigates the latent profile features of occupational burnout in emergency nurses. This research was conducted in accordance with the STROBE guidelines.
2.2 Measures
A basic demographic survey designed by the research team was used to collect general sociological information from the 1,555 emergency nurses, including demographic details (gender, age, education level, marital status, childbearing status), lifestyle habits (smoking, alcohol consumption), and work-related characteristics (years of work, weekly working hours, frequency of night shifts, monthly income, etc.).
2.2.1 Occupational burnout survey
The Maslach Burnout Inventory-General Survey (MBI-GS), developed by Maslach et al. (18) and revised by Wei et al. (19), was used to assess the occupational burnout status of the participants. This scale is widely applicable to various occupational groups and has been cross-culturally adapted and validated by domestic scholars, demonstrating good reliability and validity. The scale consists of 16 items, each rated on a 7-point Likert scale (0–6). The questionnaire includes three dimensions: emotional exhaustion, depersonalization, and reduced personal accomplishment. The first two dimensions are scored positively, where higher scores indicate greater burnout; the third dimension is scored reversely, with lower scores indicating greater burnout. The comprehensive burnout score is calculated as follows: Comprehensive burnout score = [0.4 × emotional exhaustion score + 0.3 × depersonalization score + 0.3 × (6 – personal accomplishment score)]. A comprehensive burnout score <1.5 is classified as no burnout, a score between 1.5 and <3.5 as suspected burnout, and a score ≥3.5 as burnout. In this study, the Cronbach's α coefficients for the three dimensions and the overall questionnaire were 0.914, 0.814, 0.899, and 0.860, respectively.
2.3 Data collection
An electronic version of the survey was created using the “Wenjuanxing” platform, which included an informed consent form and a link to the questionnaire. Through the Emergency Nursing Specialty Committee of the Chinese Nursing Association, the head nurses of the emergency departments in the participating hospitals were contacted to discuss the research objectives, significance, and procedures. After obtaining consent, the head nurses distributed the survey QR code link to eligible emergency department nurses via WeChat and explained the purpose of the study. Participation was voluntary and anonymous. Each IP address was limited to one response to avoid duplicate submissions. After the questionnaires were collected, they were promptly reviewed, and invalid questionnaires (e.g., those with identical answers, clear patterns, or contradictions) were excluded.
2.4 Statistical analysis
Latent profile analysis was performed using Mplus 8.3 software, with the 16-item burnout scores as observed indicators. Profiles were selected from 1 to 5 for analysis. Statistical analysis was conducted using SPSS 25.0. Continuous data were expressed as mean ± standard deviation, while categorical or ordinal data were presented as frequencies, percentages, or proportions. The three latent profiles were treated as dependent variables. One-way ANOVA was used for comparing continuous variables between groups, while categorical variables were analyzed using chi-square tests. Variables showing significant differences were further analyzed using logistic regression, with P < 0.05 considered statistically significant.
3 Results
3.1 Characteristics of participants
A total of 1,540 emergency nurses from 30 hospitals participated in the survey, with an average age of 32.23 ± 6.80 years, and 78.6% were female. The emergency nurses exhibited significant levels of burnout, with an average burnout score of (4.77 ± 6.16). Descriptive analysis of the demographic information, lifestyle habits, and work characteristics of the 1,540 emergency nurses is shown in Table 1.
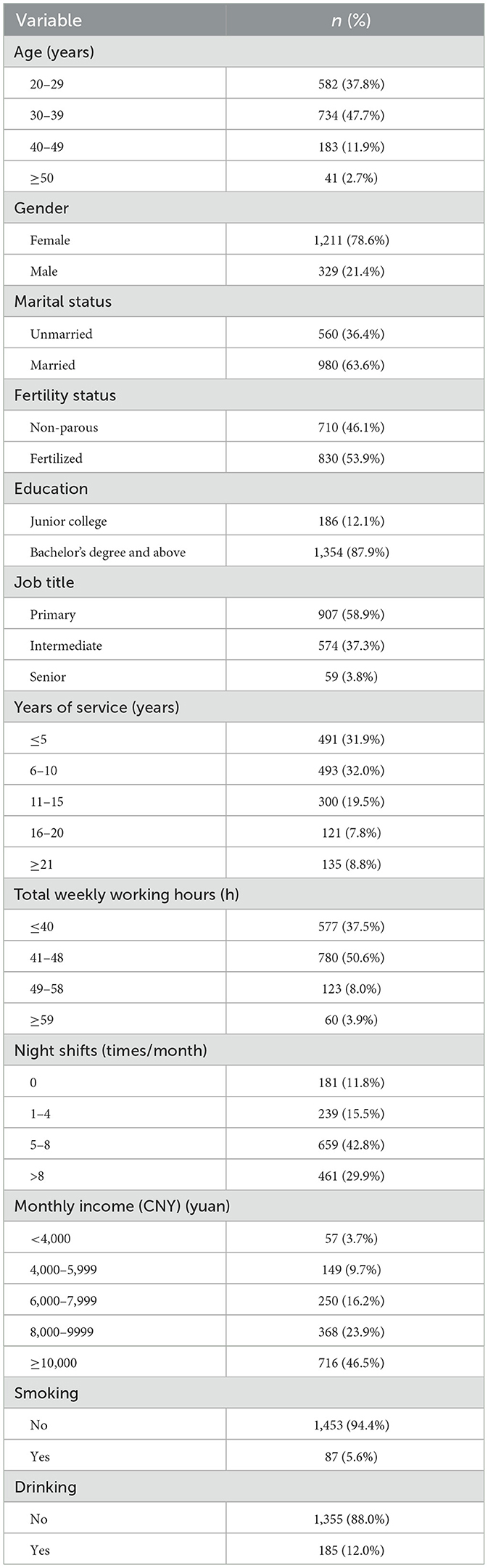
Table 1. Demographic characteristics of emergency nurses.
3.2 Descriptive analysis of occupational burnout survey results
The occupational burnout score for emergency nurses was 4.77 ± 6.16. According to the comprehensive burnout score from the burnout scale, a score ≥3.5 is classified as occupational burnout, indicating that emergency nurses generally experience occupational burnout. Emergency nurses scored higher on the first two dimensions and lower on the personal accomplishment dimension, suggesting a higher level of burnout. The average scores for the emotional exhaustion dimension were 11.3 ± 7.76, depersonalization were 8.61 ± 7.58, and personal accomplishment were 13.79 ± 10.04, as shown in Table 2.

Table 2. Descriptive analysis of occupational burnout.
3.3 Latent profile analysis of occupational burnout in emergency nurses
Latent profile analysis was performed using the 16 items of the burnout scale. The number of categories was gradually increased from the initial model, fitting latent profile models for 1–5 categories. The fit indices for each category model are shown in Table 3. The model with one category (zero model) had the worst fit, but as the number of categories increased, the AIC, BIC, and aBIC values consistently decreased. The pLMR and pBLRT indices indicated that the 2-category, 3-category, 4-category, and 5-category models fit well. The reduction in aBIC values became smaller after the 3-category model, suggesting that model improvement slowed down after the third category. Considering all fit indices and clinical relevance, the 3-category model was considered the optimal model.
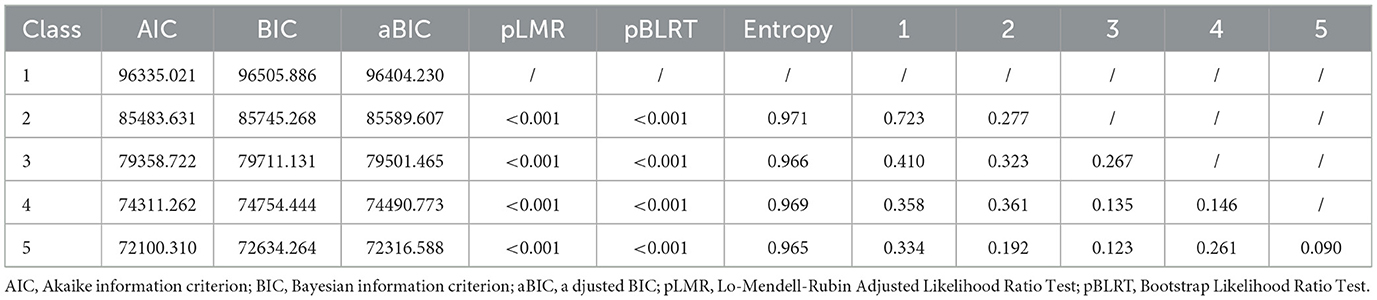
Table 3. Fit indices of the latent profile model for occupational burnout.
3.4 Determining the latent categories of occupational burnout in emergency nurses based on the three-category model
A latent profile graph of emergency nurses' occupational burnout was created using standardized Z-scores for emotional exhaustion, depersonalization, and reduced personal accomplishment across the three categories, as shown in Figure 1.
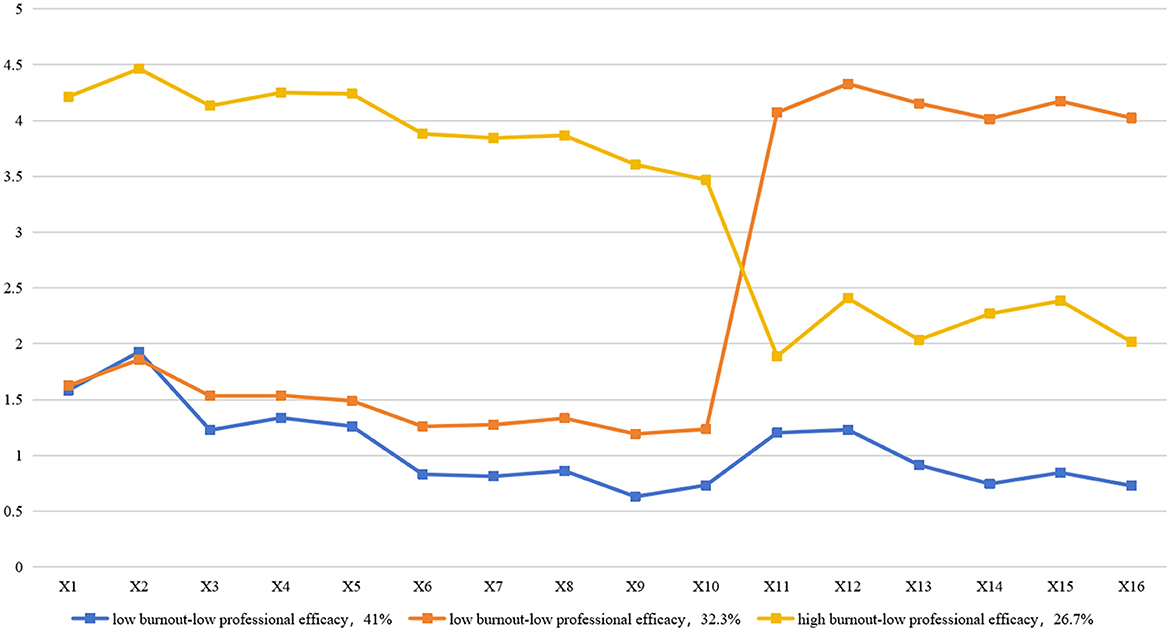
Figure 1. Potential profiles of occupational burnout.
Category C1, which accounted for the highest proportion (41%, 631 nurses), had a burnout profile characterized by low emotional exhaustion, low depersonalization, and low professional efficacy. Category C2, which made up 32.3% (497 nurses), had a burnout profile characterized by low emotional exhaustion, low depersonalization, and high professional efficacy. Category C3, which represented 26.7% (412 nurses), had a burnout profile characterized by high emotional exhaustion, high depersonalization, and low professional efficacy.
These categories were named “low burnout-low professional efficacy,” “low burnout-high professional efficacy,” and “high burnout-low professional efficacy” based on their score characteristics.
3.5 Analysis of factors influencing latent profiles
3.5.1 Univariate analysis of demographic variables
The results of the univariate analysis showed that there were significant differences between the latent categories of nurses in terms of age (χ2 = 31.749, P < 0.001), education level (χ2 = 6.778, P = 0.034), job title (χ2 = 21.928, P < 0.001), years of work experience (χ2 = 29.269, P < 0.001), weekly working hours (χ2 = 52.493, P < 0.001), frequency of night shifts (χ2 = 34.685, P < 0.001), and monthly income (χ2 = 18.994, P < 0.001), as shown in Table 4.
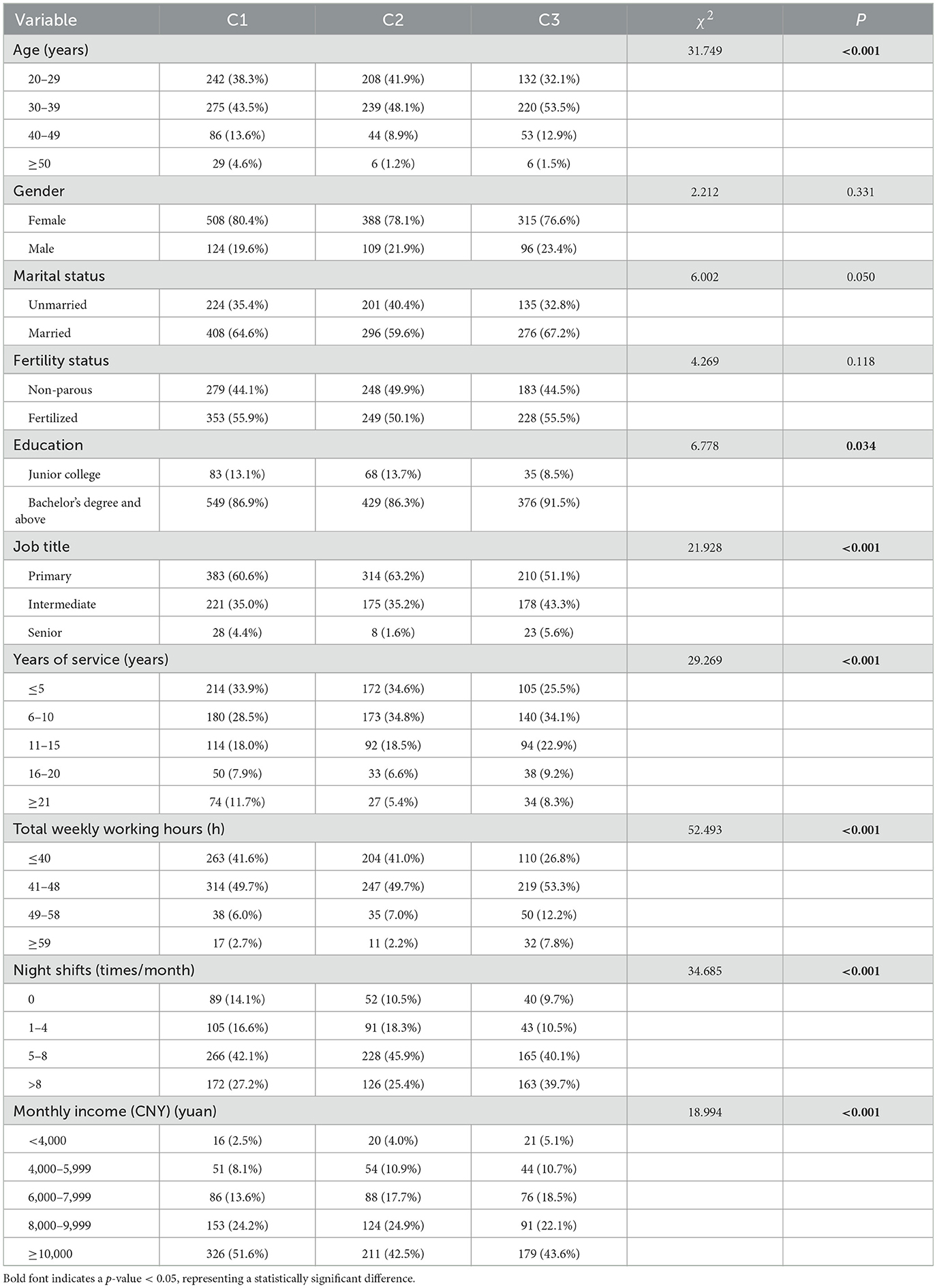
Table 4. Single-factor analysis of the profile types of occupational burnout.
3.5.2 Multivariate logistic regression analysis
Multivariate logistic regression was performed to analyze the factors influencing the latent burnout profiles. Table 5 shows that, compared with the “low burnout-low professional efficacy” (C1) nurses, those aged 20–29 years (p = 0.030) and with a monthly income ≥10,000 RMB compared to those earning <4,000 RMB (p = 0.049, 4,000–5,999 RMB p = 0.019, 6,000–7,999 RMB p = 0.021) were more likely to experience “low burnout-high professional efficacy” (C2). Compared with C3 (“high burnout-low professional efficacy”), those aged 20–29 years (p = 0.009), 30–39 years (p = 0.012), and 40–49 years (p = 0.031) were more likely to belong to the C3 burnout category than those aged ≥50 years. Monthly income (p < 0.05) also played a role, with lower income (<4,000 RMB) associated with higher likelihood of C1 burnout. Primary job titles were more likely to be associated with C1 (p = 0.034), while fewer night shifts (0 times p = 0.008, 1–4 times p = 0.001) were more likely to lead to C1 burnout. Longer weekly working hours (>59 h) increased the likelihood of C3 burnout.
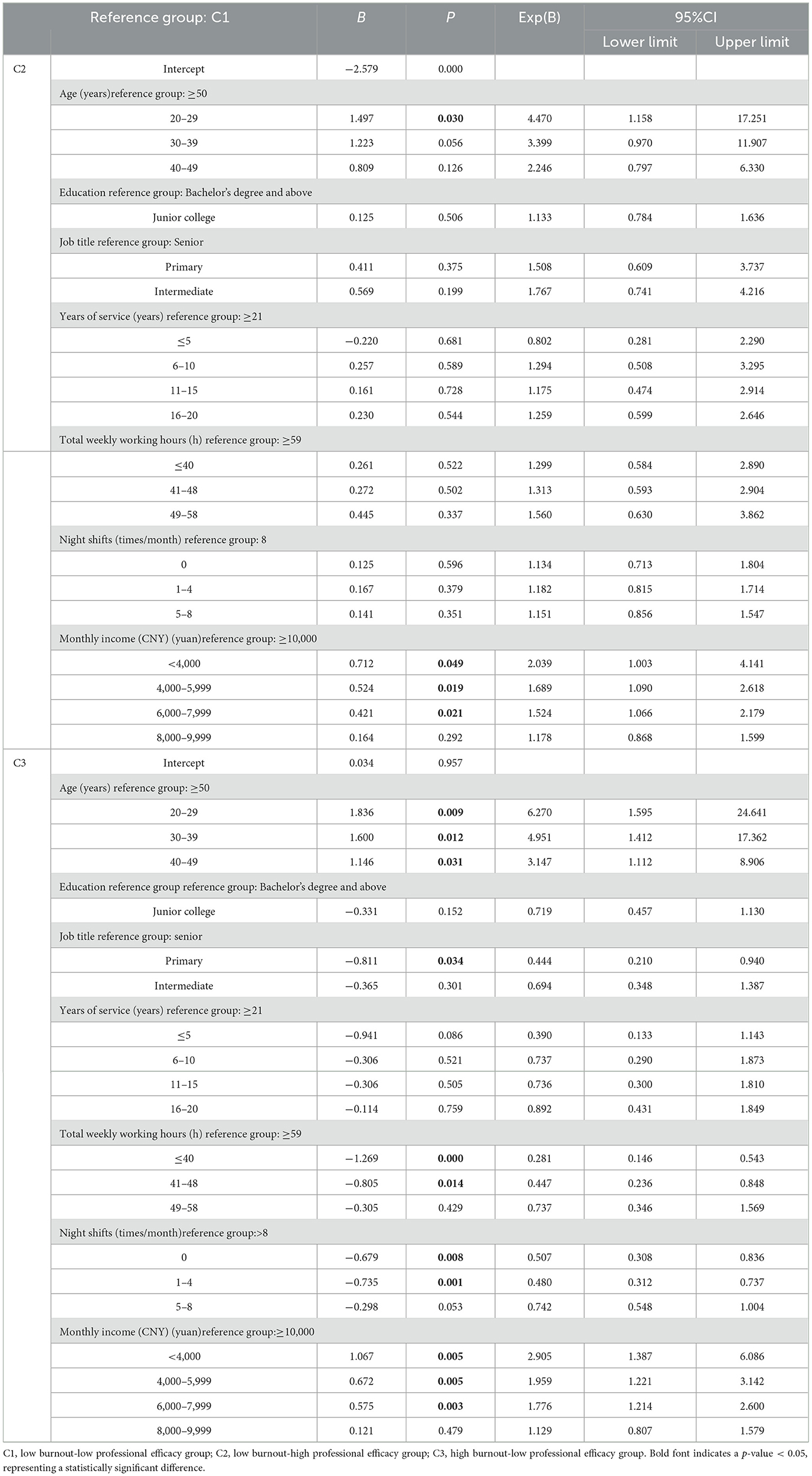
Table 5. Multivariate regression results of the profile types of occupational burnout.
4 Discussion
4.1 Profile characteristics of occupational burnout in emergency nurses
Emergency nurses generally experience occupational burnout, consistent with studies by other researchers (20, 21). The occupational burnout of emergency nurses is categorized into three types. The “low burnout—low professional efficacy” group (C1) accounts for 41%, which is the largest group. This group has low scores in emotional exhaustion and depersonalization, indicating that these nurses experience less psychological fatigue and energy depletion, maintain a high level of responsibility toward patients, and do not show indifference or negative attitudes. However, their professional efficacy score is low, suggesting a lack of confidence in their professional abilities and potentially low self-efficacy. The “low burnout—high professional efficacy” group (C2) accounts for 32.3%, indicating that some emergency nurses, despite facing pressure, still maintain high confidence in their professional abilities. Their emotional exhaustion and depersonalization scores are low, showing relatively light psychological burdens and fatigue, while their professional efficacy score is high, demonstrating full recognition of their professional value and abilities. The “high burnout—low professional efficacy” group (C3) is the smallest at 26.7%, and this group requires special attention. It exhibits the most prominent burnout characteristics, with high scores in emotional exhaustion and depersonalization, indicating that these nurses have long endured high levels of work pressure and their psychological energy is depleted. They may display negative attitudes toward work and patients, and their low professional efficacy score suggests a lack of self-confidence, potentially doubting their professional abilities.
4.2 Factors influencing occupational burnout in emergency nurses
4.2.1 Demographic characteristics
Age: There is a strong relationship between the age of emergency nurses and occupational burnout (22). When comparing C1 (“low burnout—low professional efficacy”) with C2 (“low burnout—high professional efficacy”), nurses aged 20–29 are more likely to belong to the C2 burnout group, as younger nurses are more likely to exhibit low burnout but high professional efficacy. This may be because younger nurses, who are new to the workforce, experience some adjustment stress but perform well in basic clinical tasks, leading to high professional efficacy (23). When comparing C1 (“low burnout—low professional efficacy”) with C3 (“high burnout—low professional efficacy”), nurses younger than 39 are more likely to experience C3 burnout, with the likelihood of C3 decreasing with age. Middle-aged nurses tend to be more mature in terms of skills, experience, and career adaptation. However, they may face accumulated work pressure, family responsibilities, and career development bottlenecks, which increase emotional exhaustion while still maintaining some level of professional efficacy. As age increases (24), psychological resilience and professional skills improve, and older nurses tend to handle work pressure and emotional fluctuations better. When disregarding professional efficacy, nurses' occupational burnout demonstrates an inverted U-shaped trajectory across the lifespan: it progressively increases with age, peaks during middle adulthood, and subsequently declines thereafter. This phenomenon occurs because middle-aged nurses face triple challenges—career plateau, family caregiving burdens, and declining physical stamina—leading to peak burnout levels, while senior nurses demonstrate gradual burnout reduction through mature adaptation strategies and work adjustments, ultimately forming the characteristic inverted U-shaped curve. A comparison between Group C1 and Group C3 revealed that younger nurses are more prone to type C3 job burnout. Since the number of nurses aged 20–29 far exceeds those over 40, a larger proportion of emergency nurses fall into the C3 category of burnout, characterized by high burnout and low efficacy. Nursing administrators should take measures to enhance nurses' efficacy and reduce job burnout based on the factors influencing it. Education: Multiple studies have shown that education level is a factor influencing nurse burnout (25, 26). Nurses with higher education may have higher career expectations while facing more professional challenges. Higher education is often associated with greater work burden and pressure, such as taking on more management responsibilities or engaging in academic research. Furthermore, highly educated nurses may have higher expectations for their career development, and failure to meet these expectations may lead to disappointment and burnout.
4.2.2 Work characteristics
Professional Title: Nurses with lower professional titles tend to have less experience (27) and face higher technical demands, leading to greater stress. However, because they still have high expectations for their career, they may try harder to adapt and reduce some of the burnout. Nurses with a lower professional title are more likely to belong to the C1 burnout group, suggesting that the higher the professional title, the less likely a nurse is to experience high burnout (28). Senior nurses typically have more clinical experience and professional accumulation, and are more involved in management work, with less direct involvement in high-intensity clinical tasks. They have higher decision-making power and autonomy, allowing them to better control their work pace and reduce burnout. Nurses with higher professional titles may have relatively higher incomes in the hospital, receive greater recognition from colleagues and superiors, and experience a stronger sense of personal achievement, leading to a significant reduction in job burnout. However, senior nurses, who have been in high-load, high-responsibility positions for extended periods, may experience both psychological and physical fatigue. Years of Work Experience: Work experience is usually correlated with a nurse's age. Nurses with shorter work experience (1–5 years) are still in the career adjustment phase and are more likely to experience high burnout, with clear emotional exhaustion, a lack of experience and skills, and low self-confidence, making them more susceptible to work-related stress. Nurses with medium work experience (6–15 years) often handle a large volume of clinical tasks but are in a stable period of their careers, having accumulated rich experience, which enhances their adaptability and alleviates burnout, though they may face career development bottlenecks. Nurses with long work experience (≥16 years) may experience burnout due to the repetitive nature of their work or health issues, while also lacking motivation for further career development (29). Work Hours: Nurses with shorter weekly working hours ( ≤ 40 h) are less likely to experience C3 burnout and tend to have lower burnout levels. Conversely, longer work hours increase the likelihood of high burnout. Work hours (30) are an important factor influencing burnout. Emergency nurses, who work at a fast pace and have heavy workloads, are more likely to experience burnout due to prolonged periods of high-intensity and high-pressure work, leading to both physical fatigue and psychological stress. Night Shifts: Nurses working more than eight night shifts per month are more likely to experience C3 burnout. Frequent night shifts disrupt the nurse's circadian rhythm, which may lead to sleep disorders, emotional instability, and reduced work efficiency, all of which are important contributors to burnout (31, 32). Emergency nurses must work 24-h shifts to ensure timely patient care, and night shifts are often accompanied by emergencies and urgent tasks, increasing the physical and psychological demands placed on nurses. Income Level: When comparing C1 with C2, higher income levels (≥10,000 yuan) are associated with the C2 burnout group, while lower incomes (e.g., <4,000 yuan) increase the likelihood of belonging to C1. This suggests that higher income is linked to low burnout and high professional efficacy. A higher income (21) gives nurses a sense of fair compensation and work recognition, enhancing their professional identity and motivation. Conversely, lower income may make nurses feel undervalued, contributing to burnout. Nurses with low incomes may also experience financial stress, which further exacerbates burnout risks. Low salary, high work pressure, and limited career advancement opportunities can add to nurses' psychological burdens.
4.3 Limitation
While the latent profile analysis identified three distinct burnout subtypes among ED nurses, several limitations should be noted. First, sample constraints, participants were recruited solely from China EDs, limiting generalizability to other countries or healthcare systems. Second, cross-sectional nature, the static classification cannot capture dynamic transitions between subtypes. Longitudinal validation is warranted. Variable selection: Profiles were constructed based on emotional exhaustion, cynicism, professional efficacy, while potentially influential factors (e.g., organizational support, personality traits) were unaccounted for. Third, methodological considerations: LPA results are sensitive to indicator selection and fit criteria (e.g., BIC/ABIC). Replication with alternative methods is recommended. Lastly, Clinical applicability: Translating statistical subtypes into actionable clinical identification remains challenging.
5 Conclusion
This study identified three latent profile types of occupational burnout in emergency nurses: “low burnout-low professional efficacy,” “low burnout-high professional efficacy,” and “high burnout-low professional efficacy.” Significant correlations were found between these burnout types and factors such as age, education, job title, night shift frequency, working hours, and monthly income. The findings provide a scientific basis for reducing burnout in emergency nurses, including strategies like optimizing shift schedules (33), improving work environments, offering mindfulness training (34, 35), and providing better technical and medical support.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics Review Committee of West China Hospital, Sichuan University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LL: Writing – original draft, Supervision, Formal analysis, Writing – review & editing, Data curation, Validation. XC: Investigation, Methodology, Supervision, Writing – review & editing. HZ: Writing – review & editing, Data curation, Project administration, Formal analysis, Investigation. LZ: Software, Writing – review & editing, Investigation, Data curation, Project administration. LY: Validation, Writing – review & editing, Project administration, Writing – original draft, Resources, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to thank all the participants of this project and the investigators for collecting the data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ilić IM, Arandjelović MŽ, Jovanović JM, Nešić MM. Relationships of work-related psychosocial risks, stress, individual factors and burnout - questionnaire survey among emergency physicians and nurses. Med Pr. (2017) 68:167–78. doi: 10.13075/mp.5893.00516
2. Rozo JA, Olson DM, Thu HS, Stutzman SE. situational factors associated with burnout among emergency department nurses. Workplace Health Saf . (2017) 65:262–5. doi: 10.1177/2165079917705669
3. Power H, Skene I, Murray E. The positives, the challenges and the impact; an exploration of early career nurses experiences in the Emergency Department. Int Emerg Nurs. (2022) 64:101196. doi: 10.1016/j.ienj.2022.101196
4. Adriaenssens J, De Gucht V, Maes S. Determinants and prevalence of burnout in emergency nurses: a systematic review of 25 years of research. Int J Nurs Stud. (2015) 52:649–61. doi: 10.1016/j.ijnurstu.2014.11.004
5. World Health Organization. International Statistical Classification of Diseases and Related Health Problems (ICD). Geneva: World Health Organization (2019). Available online at: https://icd.who.int/
6. Hall LH, Johnson J, Watt I, Tsipa A, O'Connor DB. Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS ONE. (2016) 11:e0159015. doi: 10.1371/journal.pone.0159015
7. Wang QQ, Lv WJ, Qian RL, Zhang YH. Job burnout and quality of working life among Chinese nurses: a cross-sectional study. J Nurs Manag. (2019) 27:1835–44. doi: 10.1111/jonm.12884
8. Ma Y, Chen F, Xing D, Meng Q, Zhang Y. Study on the associated factors of turnover intention among emergency nurses in China and the relationship between major factors. Int Emerg Nurs. (2022) 60:101106. doi: 10.1016/j.ienj.2021.101106
9. Schlak AE, Aiken LH, Chittams J, Poghosyan L, McHugh M. Leveraging the work environment to minimize the negative impact of nurse burnout on patient outcomes. Int J Environ Res Public Health. (2021) 18:610. doi: 10.3390/ijerph18020610
10. Cimiotti JP, Aiken LH, Sloane DM, Wu ES. Nurse staffing, burnout, and health care-associated infection. Am J Infect Control. (2012) 40:486–90. doi: 10.1016/j.ajic.2012.02.029
11. Poghosyan L, Clarke SP, Finlayson M, Aiken LH. Nurse burnout and quality of care: cross-national investigation in six countries. Res Nurs Health. (2010) 33:288–98. doi: 10.1002/nur.20383
12. Maslach C. and Leiter MP, Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. (2016) 15:103–11. doi: 10.1002/wps.20311
13. Nyarko BA, Yin Z, Chai X, Yue L. Nurses' alarm fatigue, influencing factors, and its relationship with burnout in the critical care units: a cross-sectional study. Aust Crit Care. (2024) 37:273–80. doi: 10.1016/j.aucc.2023.06.010
14. Qiu HZ Latent class Model: Principles and Techniques. Beijing: Educational Science Publishing House (2008).
15. Diao D, Chen X, Zhong L, Zhang H, Zhang J. Sex differences in burnout and work-family conflict among Chinese emergency nurses: a cross-sectional study. Front Public Health. (2024) 12:1492662. doi: 10.3389/fpubh.2024.1492662
16. Tong L, Zhu L, Zhang H, Zhong L, Diao D, Chen X, et al. Effort-reward imbalance and health outcomes in emergency nurses: the mediating role of work-family conflict and intrinsic effort. Front Public Health. (2024) 12:1515593. doi: 10.3389/fpubh.2024.1515593
17. Zhang H, Zhou J, Zhong L, Zhu L, Chen X. Relationship between workplace violence and occupational health in emergency nurses: the mediating role of dyssomnia. Nurs Crit Care. (2025) 30:e70008. doi: 10.1111/nicc.70008
18. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. (2001) 52:397–422. doi: 10.1146/annurev.psych.52.1.397
19. Zhu W, Lou XP, Wang ZM. To evaluate the reliability and validity of Maslash Burnout Inventory generic version in nurses. Chin Behav Med Sci. (2007) 16:849–51. doi: 10.3760/cma.j.issn.1674-6554.2007.09.031
20. Moscu CA, Marina V, Dragomir L, Anghele AD, Anghele M. The impact of burnout syndrome on job satisfaction among emergency department nurses of emergency clinical county hospital “Sfântul Apostol Andrei” of Galati, Romania. Medicina. (2022) 58:1516. doi: 10.3390/medicina58111516
21. Munn LT, O'Connell N, Huffman C, McDonald S, Gibbs M, Miller C, et al. Job-related factors associated with burnout and work engagement in emergency nurses: evidence to inform systems-focused interventions. J Emerg Nurs. (2024) 51249–60. doi: 10.1016/j.jen.2024.10.007
22. Udho S, Kabunga A. Burnout and associated factors among hospital-based nurses in Northern Uganda. Biomed Res Int. (2022) 24:8231564. doi: 10.1155/2022/8231564
23. Almezieny T, Alashaikh A, Alnasser R, Dammas S, Alsubaie N, Alhusaini Y, et al. Prevalence and impact of burnout in Emergency Department nurses; a multicenter study in Riyadh, Saudi Arabia. Med Sci. (2024) 28:1–12. doi: 10.54905/disssi.v28i145.e14ms3304
24. Yu X, Qu H, Ni Y, Tang X, Zhou H. Comparative study of job burnout in Shanghai-based nurses against Maslach norm and Hangzhou norm. Int Nurs Rev. (2025) 72:e12952. doi: 10.1111/inr.12952
25. Xie J, Li J, Wang S, Li L, Wang K, Duan Y, et al. Job burnout and its influencing factors among newly graduated nurses: a cross-sectional study. J Clin Nurs. (2021) 30:508–17. doi: 10.1111/jocn.15567
26. Zhang XM, Liu Y, Xu Y. Investigation and analysis of job burnout of nurses in emergency department. Gen Pract Nurs. (2011) 9:1023–4. doi: 10.3969/j.issn.1674-4748.2011.011.060
27. You JH, Dong HM. Investigation on burnout and work engagement of emergency nurses in 8 secondary hospitals in Ningbo. Hosp Stat China. (2017) 24:144–7. doi: 10.3969/j.issn.1006-5253.2017.02.023
28. Chen LH. Investigation and analysis of job burnout of nurses in emergency department. Int J Nurs. (2013) 32:561–3. doi: 10.3760/cma.j.issn.1673-4351.2013.03.062
29. Liu C. Relationship between life style and job burnout of nurses in emergency department in Luohe city. J Xinxiang Med Coll. (2013) 285–7.
30. Cochran KL, Doo K, Squires A, Shah T, Rinne S, Mealer M. addressing burnout syndrome from a critical care specialty organization perspective. AACN Adv Crit Care. (2020) 31:158–66. doi: 10.4037/aacnacc2020579
31. Bagheri Hosseinabadi M, Ebrahimi MH, Khanjani N, Biganeh J, Mohammadi S, Abdolahfard M. The effects of amplitude and stability of circadian rhythm and occupational stress on burnout syndrome and job dissatisfaction among irregular shift working nurses. J Clin Nurs. (2019) 28:1868–78. doi: 10.1111/jocn.14778
32. Li L, Wang X, Zhou J, Liu M, Wang S, Zhou Y, et al. Factors associated with chronotype, job burnout, and perceived stress among nurses in Chinese tertiary hospitals: a multicenter cross-sectional study. Chronobiol Int. (2024) 41:1058–67. doi: 10.1080/07420528.2024.2373224
33. Zhou W, He G, Wang H, He Y, Yuan Q, Liu D. Job dissatisfaction and burnout of nurses in Hunan, China: a cross-sectional survey. Nurs Health Sci. (2015) 17:444–50. doi: 10.1111/nhs.12213
34. Sun Y, Lin MD, Liu CM, LU Y, Liu T, Zhao N. To explore the effects of mindfulness-based stress reduction training on job burnout and quality of life of nurses in emergency department. Nurs Res. (2023) 37:3007–11. doi: 10.12102/j.issn.1009-6493.2023.16.028
Keywords: emergency department nurses, burnout, latent profile analysis, influencing factor, cross-sectional study
Citation: Lan L, Chen X, Zhang H, Zhong L and Ye L (2025) Characterizing potential subtypes and influencing factors of burnout in emergency department nurses by latent profile analysis. Front. Public Health 13:1654398. doi: 10.3389/fpubh.2025.1654398
Received: 26 June 2025; Accepted: 29 August 2025;
Published: 25 September 2025.
Edited by:
Hubertus Himmerich, King's College London, United KingdomReviewed by:
Sinan Yilmaz, Atatürk University, TürkiyeSisca Mayang Phuspa, Universitas Darussalam Gontor, Indonesia
Natalia Budzyńska, Medical University of Gdansk, Poland
Copyright © 2025 Lan, Chen, Zhang, Zhong and Ye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lei Ye, eWVsZWkxMTE3QDEyNi5jb20=