 Tomasz Krawczyk
Tomasz Krawczyk Jan Piasecki
Jan Piasecki Jacqueline Galica
Jacqueline Galica Marcin Waligora
Marcin Waligora- 1Department of Bioethics and Health Psychology, Faculty of Health Sciences, Jagiellonian University Medical College, Krakow, Poland
- 2Research Ethics in Medicine Study Group (REMEDY), Jagiellonian University Medical College, Krakow, Poland
- 3Doctoral School of Medical and Health Sciences, Jagiellonian University Medical College, Krakow, Poland
- 4Division of Cancer Care and Epidemiology, Queen’s Cancer Research Institute, Kingston, ON, Canada
- 5School of Nursing, Queen’s University, Kingston, ON, Canada
Public and patient involvement and engagement (PPIE) in research is increasingly expected and often formally required by the sponsors. However, creating and sustaining conditions for meaningful PPIE can be challenging. It requires efforts of all involved parties. While much attention is given for the ethical inclusion of individuals as research participants, their collaboration with researchers and design of accessible research processes, there is a question of how research institutions can support PPIE. We argue for comprehensive changes within research institutions to facilitate meaningful PPIE practice. These changes should include institutional culture and attitudes toward the public members involved in research, to foster meaningful encounters between people with different forms of knowledge and life experience, such as professionally trained researchers and members of marginalized social groups. In this study, we propose a framework of institutional changes for PPIE, which focuses on their sociocultural and epistemic features. We explore the context of PPIE and possible risks related to disregarding public members as owners of valid knowledge. We use the order of change model as a frame and emphasize the role of third-order changes, which involve raising awareness about diverse forms of knowledge. Such changes would allow for sustaining PPIE research as knowledge space, wherein public members and researchers can respectfully share knowledge to inform scientific inquiries. Based on these conceptualizations, we outline practical examples and future directions. Better conceptualizing of institutional changes can contribute to facilitating their implementation and thereby more ethical research practice.
1 Introduction
In recent decades, the importance of involving lay people in research has become widely acknowledged within scientific communities. A variety of terms, coming from different research traditions and world regions, have been used to describe such practices (1–3). In this study, we use the term PPIE—public and patient involvement and engagement—as an umbrella term for meaningful research practices “carried out ‘with’ or ‘by’ members of the public rather than ‘to’, ‘about’, or ‘for’ them” (4). We also use the term public to collectively describe patients, their relatives and friends, research participants, and others affected by research and healthcare. As expectations for PPIE in contemporary research continue to rise, there is a growing attention to the sociocultural context of knowledge creation (5, 6). However, the primary focus is on the individuals involved and the research process (7–9). Fewer authors discuss structural and institutional issues, such as the impact of dominant scientific paradigms, institutional culture, or collective biases in academia (10–12). Thus, there is a question of how research institutions should adapt to foster PPIE.
Our main claim is that not only involved public members and individual researchers but also research institutions should change themselves to facilitate meaningful PPIE. We argue that deep institutional changes are necessary to create and sustain knowledge spaces. We define knowledge spaces in accordance with sociology of medicine as contexts wherein different forms of knowledge interact in a dialog on a possibly equal basis with the aim of enhancing understanding and foster scientific progress (13), p. 1113; (14), p. 544. The different forms of knowledge may consist of experiential knowledge, possessed by people with lived experience of the condition or circumstance under study, and professional knowledge owned by clinicians or scientists (15, 16). Knowledge spaces require the research project to become genuine collaboration between researchers and public members wherein both sides exchange their perspectives and examine existing biases. They would allow for more ethical and reliable PPIE research, contributing to, among others, broadening knowledge with the first-person experiences and empowering those in epistemically subaltern positions (17). For example, in psychology research, a team of psychotherapists can establish a participatory project with autistic people which focuses on the design of psychotherapeutic intervention for neurodivergent patients. In such project, the perspective of neurodivergent people and their experiences can be included and discussed toward increasing mutual understanding and supporting implementation of the intervention. Creating such spaces may require changes in epistemic resources of involved parties. Epistemic resources are the interpretive frameworks or cognitive schemata consisting of language, concepts, and meanings, as well as judgment rules (18), pp. 717–718. These resources guide the way how individuals approach the world and enable them to make sense of their experiences. For example, Deaf people who identify as members of Deaf culture can differently perceive both deafness and hearing and rely on spatial–visual mode of cognition; thereby, they can develop different epistemic resources than hearing majority (19). Such knowledge space would enable both Deaf people and researchers to express their knowledge, experiences, and expectations about the issue in question in an open, respectful manner. We argue that to enable and sustain such practices, comprehensive changes are necessary—changes which would also affect the epistemic resources of research institutions.
The aim of this conceptual article is to explore the epistemic and sociocultural basis for institutional change in support of meaningful PPIE, which we pursue through four specific objectives:
• To analyze the epistemic context of PPIE, including risks such as epistemic injustice (20, 21)—wrongs related to knowledge inequalities and disregarding public members as owners of valid knowledge;
• To define the conditions for knowledge spaces using the institutional order of change model (20, 22);
• To conceptualize research institutions as collective agents capable of transformation—formal social entities with a sense of group agency;
• To examine current initiatives and outline possible future theoretical and practical directions.
Through this exploration, we aim to provide a conceptual framework for analyzing changes in research institutions. We ground our analysis within the feminist, sociology of medicine, and critical disability literature, focusing our interest on the sociocultural context of creation and exploitation of knowledge. We situate our framework in health sciences research but acknowledge that it can be relevant also to other fields.
1.1 Positionality statement
We are researchers (psychologist, registered nurse, bioethicists) from Poland and Canada. We recognize our epistemic limitations in regard to underrepresented groups’ perspectives, as well as privileged positions in regard to social status and access to education and knowledge. Jointly, we have experience in research ethics, social science research, and PPIE research. Our reflection on PPIE is influenced by decolonial thought and the notion of epistemic diversity, which seeks to uncover, recognize, and position other—non-mainstream—forms of knowledge (12), p. 2513. We assume that all forms of knowledge are partial and situated within specific temporal and spatial contexts, whether it is the professional scientific knowledge or that one owned by the patients and members from marginalized communities. Our point of view is open to examination by the perspectives of members of marginalized groups, as well as researchers from other fields.
2 Sociocultural and epistemic context of PPIE
One of the broad approaches defines PPIE1 as “the active, meaningful, and collaborative interaction between patients and researchers across all stages of the research process, where research decision making is guided by patients’ contributions as partners, recognizing their specific experiences, values, and expertise” (1), p. 682.
Concerning the involved agents, interactions within PPIE entail encounters between two groups of people with different backgrounds: patients, or more broadly the members of public; and researchers2. These encounters happen in specific context—during the research process which takes place in specific research setting. Vincent et al. (23) p. 1–2 situate the relationship between researchers and members of public—working relationships—in the context of the culture of engagement in research institutions, which is shaped by the dominant (health) research paradigm context. While research decision-making in PPIE should be “guided by patients’ contributions” (1), p. 682, the rules of research processes are—by default—defined and organized by scientific rigor, researchers, and the organizational structure of research institutions (11, 23). Drawing upon the literature on collective agency (24), we propose to distinguish three kinds of agents involved in PPIE research: (i) public, (ii) researchers, and (iii) research institutions—collective agents which govern the research process (Figure 1). We understand research institutions as complex social entities, operating under rational group-level decision-making procedures (24)—universities, medical colleges, or other organizations which conduct research. The public, researchers, and research institutions may share different epistemic resources, which, are the interpretive frameworks, cognitive schemata (concepts and meanings), as well as judgment rules and cognitive procedures (18).
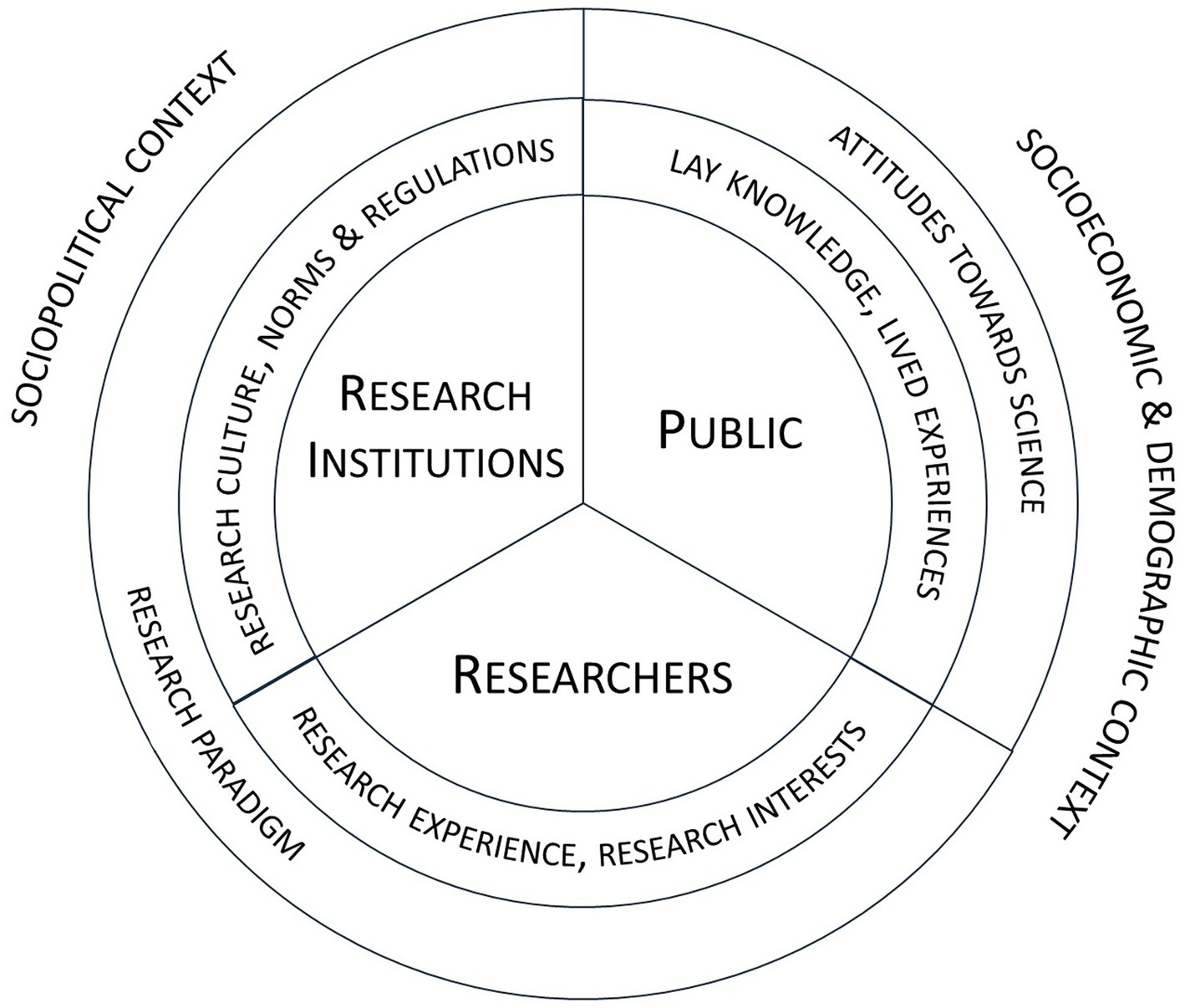
Figure 1. Overview of the agents involved in the PPIE process and the factors influencing their performance.
The public and researchers may possess not only different epistemic resources but also different values, life experiences, priorities, goals and interests, as well as have various levels of education, conceptual fluency and attitudes toward science (25). Furthermore, research institutions may vary depending their institutional, regulatory, and political contexts. They may follow different scientific paradigms, which are related to specific values, goals, and concepts (26, 27). In PPIE processes, these various backgrounds intersect which may have multiple effects. On the one hand, PPIE may have a beneficial impact on research, being a means to achieve various objectives. Harting et al. (17), pp. 11–15 reviewed the available rationale for PPIE, which they grouped into five categories. First and second, respectively, are democratic rationale and consumerist rationale, which concern the normative and economic rights of citizens to “have a voice” in research. These rationales highlight the intrinsic value of PPIE and economic interests of citizens—taxpayers. Third, a transformative rationale emphasizes the efforts to “empower marginalized groups” and express their voices through research. The last two, substantive rationale and instrumental rationale, focus on improving research quality, gathering rich contextual knowledge, as well as increasing research efficiency and applicability. PPIE and partnership approaches are also postulated as a means to achieve epistemically just healthcare and research (28).
On the other hand, PPIE takes place within hierarchical structures that may suppress perspectives that contradict mainstream scientific paradigms (6, 11). Thus, PPIE is also prone to various harms and wrongs to involved public members as epistemic agents—active contributors to and users of knowledge. For example, researchers may distrust experiential lay knowledge, question the status of public members as knowledge owners (29) or lack awareness, willingness, and resources to engage properly (9, 30). In addition, institutions which guide the research process can be opaque (31), constituting complex and demanding settings. This may lead to marginal or tokenistic engagement—symbolic or superficial processes, intended to satisfy the imposed requirements rather than foster genuine collaboration (32). Moreover, the aforementioned PPIE rationales can conflict with each other. They may differ in power and recognition regarding the context (33). For example, during joint discussions, the influence of participating institutional funders or professionals may outweigh the voice of non-profit organizations that support patient rights, which in turn may overshadow the perspectives of individual patients (34). Furthermore, different agents who argue for PPIE can share distinct (sets of) rationales. For example, research authorities may consider primarily substantive and instrumental reasons. They may emphasize research applicability and prioritize gathering extensive data on how the intervention functions across various settings. The public, however, may focus primarily on democratic or transformative rationales, placing greater value on opportunities to be heard by professionals and express their experiences of recovery. Front-line researchers may share all these rationales, stepping into a dual—researcher-activist—role (35). However, this discussion exceeds the scope of our study.
Despite its empowering character, PPIE can inadvertently result in establishing unequal and harmful relations within collaborative research initiatives (33, 34). These relations may be mutually maintained if some benefits, such as access to better healthcare, may be acquired by the public members involved in research processes (11). In addition, existing institutional structures can perpetuate power hierarchies, hindering respectful knowledge exchange and mutual learning (31, 36). Such dynamics may easily place involved people in unjustly subordinate positions toward researchers, regardless of whether they belong to marginalized groups. Unjust treatment may also arise in terms of perceived credibility of public members and their capacities to produce, process, and exploit knowledge. In what follows, we outline these risks within PPIE through the conceptual lens of epistemic injustice.
2.1 Epistemic injustice in PPIE
The concept of epistemic injustice originated from the Fricker’s work (37). Since then, it has been discussed within a range of contexts, among them healthcare and research (6, 31, 38). Epistemic injustice is defined as the wrong related to knowledge and people’s capacities as independent and active knowledge users—epistemic agents (37), p. 1. It can occur in several ways, to specific individuals, by disrupting cognitive processes or through systematic perpetuation of power differences (39). In the context of PPIE, two forms of epistemic injustice are particularly relevant: participatory epistemic injustice and epistemic trust injustice (6), pp. 315–319; see also: (40), which reflect two aspects of knowledge sharing. The first relates to whether an individual is perceived as capable and worthy of participation in knowledge generation. For example, a woman with Down syndrome from a small town may not be asked to participate in research because of a preconception that research is “too demanding” for her. The second aspect of knowledge sharing concerns whether an individual has the necessary conditions to receive knowledge and whether she perceives scientists as trustworthy. For example, an older Roma man may perceive researchers as representatives of dominant cultural group that once forbade him to use his mother tongue at school and subjected him to stigma. Consequently, he may decline participation in research out of a broader mistrust toward the dominant group. Epistemic injustice can occur at various levels. We will analyze them following the Dotson’s account (20, 21). Dotson (20, 21), (Table 1) distinguishes three kinds of epistemic injustice: testimonial, hermeneutical, and contributory injustice, structuring them within a heuristic of the institutional order of change model (22). This account allows for conceptualization of unjust epistemic practices within institutions in a gradual manner, regarding the scope of change required to oppose them. We find this approach promising for discussing the epistemic impact of research institutions on PPIE processes.
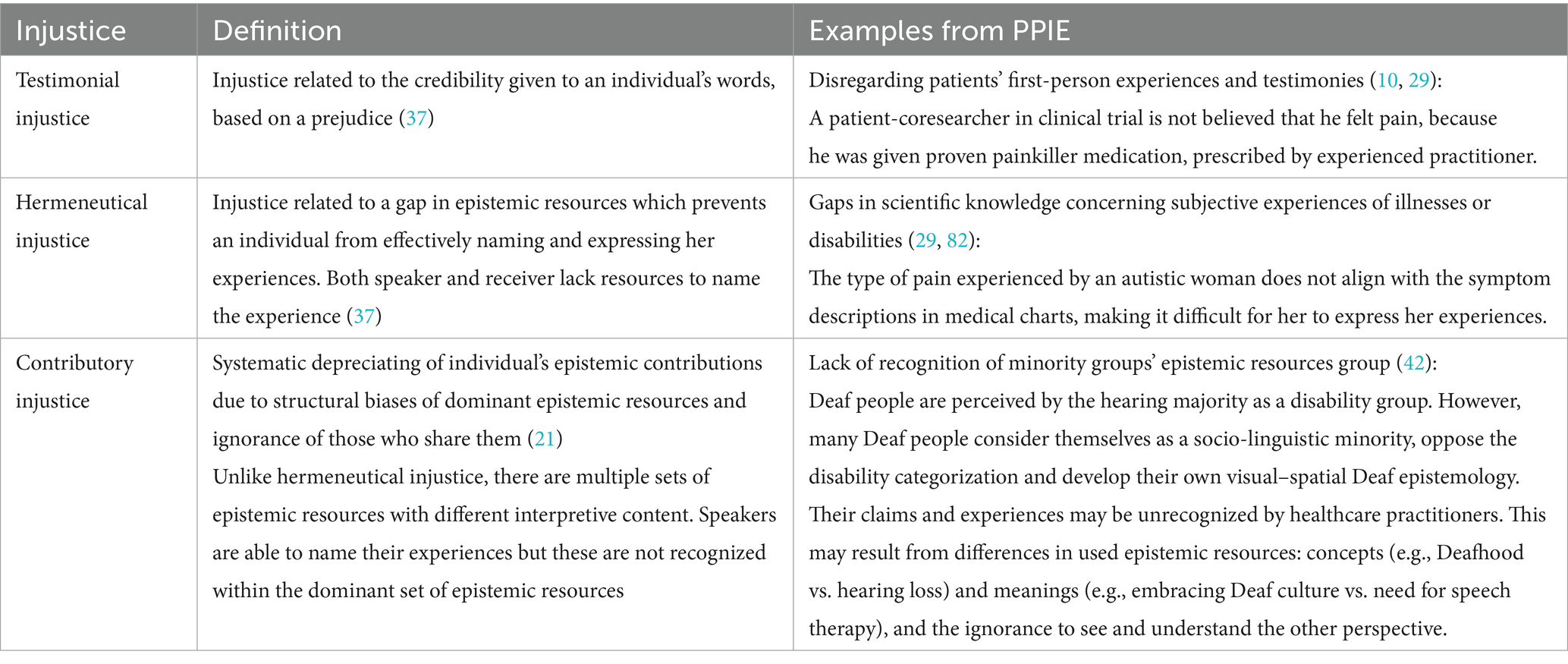
Table 1. Overview of the forms of epistemic injustice with examples from the PPIE practice.
In testimonial injustice, there is a prejudice related to the identity of an individual (speaker) which negatively influences her perception as a knower (37). Research and healthcare settings add extra layers to such prejudices. Public members may be judged not only as members of specific social group, e.g., “women or gays”, “lay people” who do not possess professional knowledge (6). Thus, their testimonies—contributions to shared knowledge—may be easily disregarded when not supported by other existing evidence. Disregarding lived testimonies in this way may lead participants to self-silencing, which can further diminish their active engagement in research processes (40).
Hermeneutical injustice, in turn, involves more complex situations where collective epistemic resources are deficient themselves—even with gaps concerning apt resources or having some resources distorted. This leaves some groups with a “significant area of [their] social experience obscured from collective understanding owing to a structural identity prejudice in the collective hermeneutical resource” (37), p. 155. PPIE is prone to such injustice. For example, evidence-based approaches have inadvertently led to the preference of generalizable data from large studies over contextualized patient’s (and also clinician’s) knowledge (41). It constrains the spectrum of “apt” terminologies in the field. Thus, patients may struggle to express themselves and meaningfully contribute to the research.
Finally, contributory injustice broadens the understanding of epistemic resources—that is there is no single, universal set of epistemic resources (21), p. 31. Each social group can possess its own set of epistemic resources, which may differ in recognition and status within social power relations. Furthermore, individuals can be (willfully) ignorant in utilizing their own set of epistemic resources, disregarding those of others (18). This perspective stresses the collective experiences of epistemic injustice in a virtue of belonging to a marginalized group (42). Such groups share similar experiences, which can articulate and interpret them, but those interpretations fall outside the mainstream set of epistemic resources, as in the example of autistic or Deaf people (see Table 1).
One of the rationales for PPIE concerns the empowerment of underrepresented groups to express their voices (17) and therefore counters epistemic injustice. However, PPIE is simultaneously prone to such injustice. The good will, commitment, and openness of public members and frontline researchers are of utmost importance in PPIE but may be insufficient to mitigate epistemic injustice and sustain favorable conditions for knowledge spaces. There is a need for structural remedies to efficiently counter the structural character of many forms of epistemic injustice, as well as their cumulative effects (43, 44). Addressing epistemic injustice at various structural and institutional levels may require differentiated approaches and tailored strategies. Here, we will use the order of change model (20–22) as a frame to outline three scopes of change within research institutions that can facilitate the establishment of knowledge spaces and related forms of epistemic justice.
3 The order of change model
The order of change model is a framework designed to portray how meaning assigned to certain experiences can be altered within organizational social structures (22). The term order reflects the idea that meaning can be changed in a gradual manner, differing in regard to the scope and depth of the change. The model distinguishes three ways—orders—of implementing changes. Dotson (21) presented these orders of change as corresponding to increasingly complex forms of changes required to counter presented three forms of epistemic injustice (see Table 2). The model uses a cognitive sciences’ concept of schemata—mental “templates, that when pressed against experience, give it form and meaning” (22), p. 484. These can be created, shared, and negotiated also within social groups, such as members of organizations, to guide collaborative actions and interpretations of the events. As such, organizational schemata are a kind of “shared epistemic resource like language [concepts and meanings] that enables goals and pursuits to be shared collectively” (20), p. 118. Schemata are generally stable and resilient to change (18); however, they can be altered when they prove insufficient for guiding how an organization engage the world. Consistent with Dotson’s approach (20, 21), we broaden the analysis from the level of organizational schemata to that of shared epistemic resources.
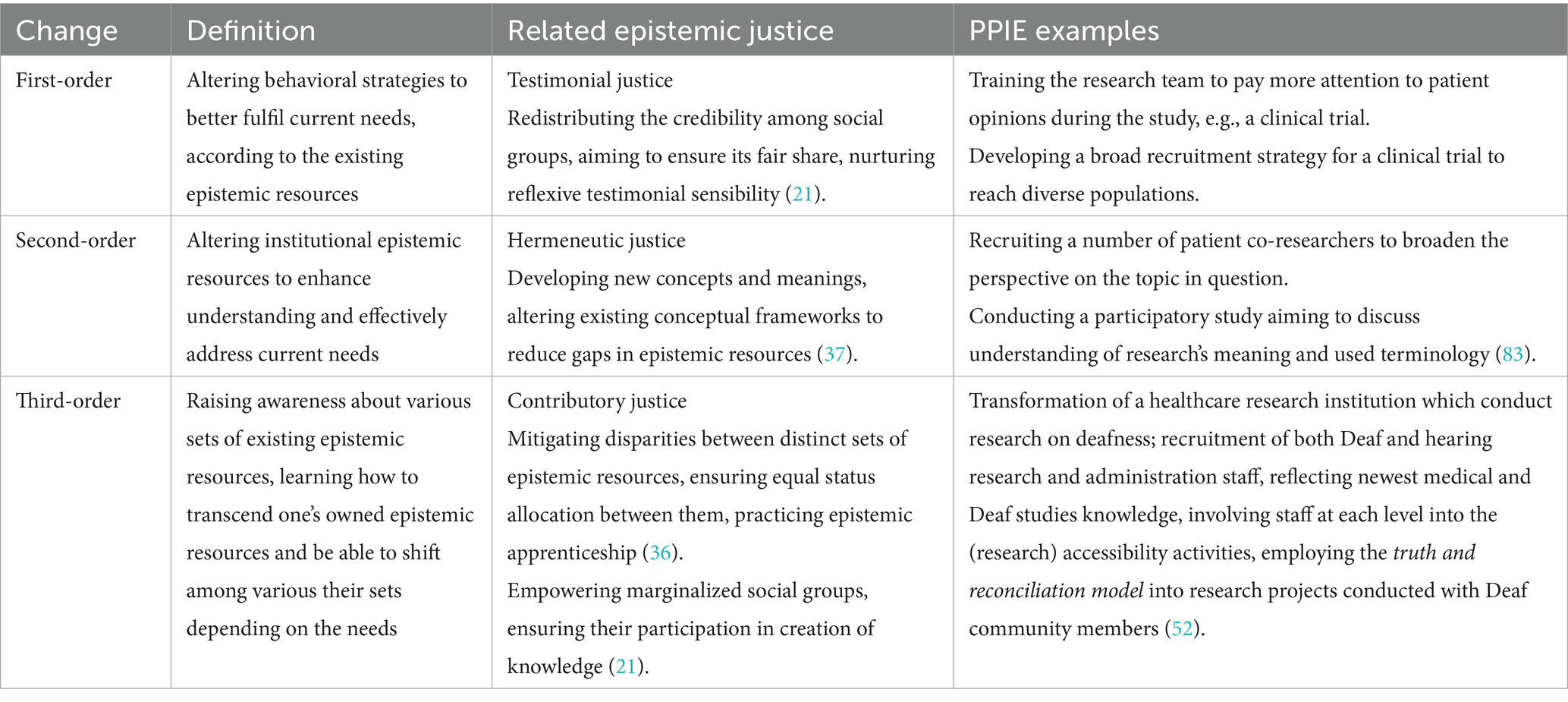
Table 2. Overview of the order of change model (22) with examples from PPIE practice and related forms of epistemic injustice.
First-order changes are (relatively) easy to introduce into the institution since they do not require going beyond existing epistemic resources. In the context of epistemic injustice, a change toward testimonial justice also does not need to question the concept of credibility given to a specific social group (21). First-order changes for PPIE may involve revising existing institutional guidelines on research conduct to enhance active participation of the public. For example, research institutions may instruct researchers to conduct research in community spaces or hire interpreters for Deaf or Latine participants (45, 46). Similarly, researchers may provide plain language summaries of publications translated into minority languages (47). First-order changes may also include modifying existing research methods, for example, adding qualitative studies to large quantitative projects and extending the spectrum of research techniques (27). Such processes do not require to directly affect institutional epistemic resources and may have little impact on how the whole institution functions. However, they can be formalized as guidelines or educational resources (48–50) and be a starting point for introducing second-order changes.
Second-order changes address insufficiencies of existing epistemic resources—hermeneutic injustice—by filling conceptual gaps, thereby enabling all individuals to express themselves more effectively (21). New terms and meanings can be incorporated into vocabularies used in research to facilitate and broaden mutual understanding between public members and researchers. This requires reshaping research culture. PPIE itself can be described as a second-order change. The public members are invited to express their perspective, name their experience which broadens knowledge about the researched issue [see substantive rationale; (17)]. It is embodied in, for example, collaborative design of research projects, data gathering, or interpretation of the results (45). Second-order changes may also increase efforts to reach participants before the study to establish relations and mitigate mistrust—an issue of utmost importance when working with marginalized groups (51, 52). Moreover, institutions may act to increase overall ethical awareness of researchers (53, 54). Various approaches are developed to facilitate the exchange of thoughts among research teams (55–57). Such processes transform epistemic resources of research institutions and alter their functioning, especially on the level of research teams. However, these changes may not be strong enough to influence the institutional structures. Researchers who introduce PPIE projects may face procedural barriers and struggle emotionally because of the institutional resistance (30). When no senior staff or authorities support the changes, there is also a risk that such PPIE projects would be perceived as partial or insincere, especially in projects with groups which have been historically oppressed in research (11, 52). Hence, there is a need for third-order changes in research institutions.
Third-order changes enable agents to recognize the plurality of schemata and move beyond their particular sets. They effect in a meta-awareness of being situated within a specific set of epistemic resources, one among the others. Thus, third-order changes result in a competence of moving between various (previously recognized) sets of epistemic resources, according to the institutional needs. Such competence can help counter contributory injustice by addressing disparities between distinct sets of epistemic resources and the unequal attribution of status among them (21). Third-order changes may provide space for those who share epistemic resources other than the mainstream ones. We argue that such changes are necessary, but also not sufficient, to ensure sustainable implementation of PPIE at research institutions and establishing them as knowledge spaces. Now, we will outline how research institutions can be conceived as collective epistemic agents—social entities with a sense of group agency, who can both obstruct and facilitate reaching epistemic justice in PPIE.
4 Research institutions as collective agents
The way social groups and organizations are formalized influences how we understand their features and the responsibilities we attribute to them (24). It also shapes the strategies needed to alter their shared epistemic resources, including the strategies required to counter epistemic injustice. Institutions are formalized, highly resilient social structures, “composed of cultural-cognitive, normative, and regulative elements that […] provide stability and meaning to social life” (58), p. 6. In addition, research and academic institutions have distinct characteristics, being “loosely coupled systems with diffused decision making, as well as goal ambiguity” (59), p. 120; (60). These features facilitate introduction of minor changes but make institutions to struggle when major, transformative changes are needed. We argue that such major changes are needed to reorientate a research institution in a new direction, such as embracing the PPIE approach.
Any major institutional change should be structurally holistic, combining both bottom-up and top-down movements (61), and impact institutional structures, processes, and actions (59). Complex activities are needed to affect research personnel at all institutional levels, as well as institutional procedures, goals, and values, ensuring that the change is sustainable (59, 61). Such changes require various resources, including financial, workforce, and time. We argue that, for changes seeking to embrace PPIE approach, among these factors the necessary—but not sufficient—condition is a change within institutional epistemic resources: raising awareness of and recognizing diverse forms of knowledge owned by various non-dominant social groups (i.e., neurodivergent people, people with chronic illnesses or ethnic minorities). The change should also interact with and be grounded in the institutional ethos (60). Fricker (61), p. 91 conceptualizes the institutional ethos as “collective motivational dispositions and evaluative attitudes within the institutional body, of which the various good or bad ends orientate the institution’s activities.” Similarly to the character of an individual, these dispositions and attitudes occur regularly and are stable within time. For example, an institution can articulate the will to respect diverse forms of knowledge in the institutional mission and formalize within decision-making procedures which motivate actions of its members. Institutions can thereby influence and shape behaviors of their members, to ensure alignment with institutional goals—a dynamic that is crucial for their proper functioning.
We may ascribe certain features to institutions—collective agents, as their structure and procedures promote some and discourage other behaviors among their members (62). We draw on a non-summative account of collective agency, according to which institutions, as formalized groups, are not reducible to the sum of their members, thus can be considered as bearers of collective agency (62), pp. 2–4. For example, an institution can exhibit a feature even if most of its members do not possess that feature individually; a research institution can remain opaque for participants, even when all its members act in a most direct manner (31). Institutional features may include shared values which constitute institutional ethos, including epistemic virtues and epistemic vices. Epistemic virtues aim at achieving epistemic goods, such as truth or understanding, for example, curiosity and humility. On the contrary, epistemic vices—“culpable failures of epistemic virtue,” like hubris, insouciance or arrogance, hinder acquisitions of the epistemic goods (61), p. 98. In PPIE, epistemic virtues and vices lay at the intersection of the pursuit of truth—gathering more accurate knowledge—and the pursuit of good—respecting public members as knowledge owners. These two aspects are deeply interconnected, as active participation of minority members may contribute to both broadening mutual knowledge and mitigating future harms, thus contributing to epistemic justice (17, 36).
Epistemic vices of research institutions can contribute to research misconduct and questionable research practices, rendering such errors institutionally grounded (63, 64). Moreover, vicious institutional ethos can conduce moral transgressions with procedural or structural factors, which can increase motivation of individual members to commit various kinds of moral transgressions (63). For example, the failure to acknowledge the neurodiversity perspective within a medical faculty may contribute to the dismissal of autistic people’s research experiences that diverge from the mainstream medical view. Moreover, it may lead to further marginalization of autistic people in healthcare by professionals who graduated in that faculty. This can limit both scientific knowledge by excluding autistic people’s perspectives and their trust in healthcare research, thereby causing social harms. Therefore, structural solutions should be implemented to foster and sustain virtuous practice at both institutional and individual levels (42, 44). Specifically, respectful PPIE research is unlikely to occur unless research institutions establish knowledge spaces that facilitate equitable dialog between researchers and the public. In this way, we consider epistemic changes as a basis for broader transformations toward epistemic justice, including redistribution of power allocations and adaptations of organizational structures and procedures.
The issue remains how to introduce such changes in practice. In her analysis of institutional changes, Boyce (59), p. 130 proposes three groups of activities to support long-lasting changes: inquiry and dialog; action learning—practical problem-solving activities; and embedding changes in the structures, systems, and cultures of the institution. These activities are consistent with our thoughts on the third-order changes in research institutions. While it is hard to find a documented large-scale example of such changes concerning both the research institution and PPIE process, we will outline directions and examples close to our understanding of third-order changes.
5 Proposed directions
Our first proposed direction is for an increased focus on PPIE within academic teaching (10, 65). It consists of two-dimensional education: about the concepts and theories of PPIE, and also by gaining living experience in learning-by-doing approach, for example, meetings with patients or supervised PPIE projects (65). It could be combined with efforts to raise ethical awareness among researchers (53, 54), as well as raising the competences of early-stage researchers (66). Integrating elements of PPIE into academic curricula may have a twofold effect on research institutions. On the one hand, it may enhance future professionals’ meta-awareness about various sets of epistemic resources within contemporary society, increasing contributory justice, as well as broaden theoretical knowledge and raise socio-cultural sensitivity. Furthermore, it may counter persistent false beliefs and unsupported claims based on existing prejudices, such as those about Black people having higher pain tolerance than white people (67) or Deaf people having more concrete minds than hearing people (68), conducing the mitigation of testimonial injustice. This change encompasses mainly first- and second-order changes, including modifications of existing teaching strategies and broadening the educational resources with new perspectives, respectively. It may contribute to future third-order changes at research institutions, if these professionals-to-be would reorient their future workplaces toward a more PPIE-oriented approach. On the other hand, the PPIE-oriented education may directly transform institutional procedures and structures. Formalized within curricula, it may serve as a demonstration of institutional commitment to PPIE, diversity, and accessibility, affecting the willingness and self-efficacy among staff (9). Thus, it may be a step toward grounding PPIE within the institutional ethos and subsequent third-order change. Thomas et al. (10) and Churcher (36) suggest also a reform of teaching conditions within academia, by reformulating teachers’ roles, learner–teacher relations, and inviting scholars with minority/lived experience background. Academic staff with diverse sociocultural background may support sustainability of institutional changes and promote academic careers among people from diverse backgrounds [e.g., scholars with lived experience (69); Deaf people at academia: (70)]. Moreover, these activities may contribute to mitigating mistrust of historically marginalized groups toward research in general and facilitate engagement processes (46). Therefore, efforts focused on academic teaching may create favorable conditions for structural changes in institutional epistemic resources, both by future generations and through formalized curricula. It is likely that professionals trained in participatory approaches would be more eager to establish knowledge spaces in their research projects and have greater awareness about the different forms of knowledge among social groups.
Further direction relates to the implementation of culturally appropriate and decolonized approaches to research. Examples of such approaches are the Indigenous Terms of Reference—the set of principles which should be followed when doing research with a specific community (71); Deaf studies—an interdisciplinary field related to Deaf community, sign languages, and deafness (72); or Kaupapa Māori research—research grounded in Māori values and customs, by Māori, for Māori and with Māori (73). Kaupapa Māori is a distinct example, as it is explicitly incorporated into New Zealand Aotearoa’s higher education, aiming also to increase share of Māori population in research enterprises (74). These approaches and movements interact with mainstream scientific paradigms and negotiate space for epistemological diversity in science. Their formalization occurs through several research teams and institutes dedicated to various underrepresented perspectives. The question remains, whether in practice they interact and coexist with mainstream paradigms or both sides function rather separately (75). However, they have already raised meta-awareness about the various sets of epistemic resources shared by, for example Māori and non-Māori people, also at the institutional level. Thus, their presence facilitates ensuring contributory justice in research and seems to fit into the scope of third-order changes at specific research institutions. Such activities allow for establishing knowledge spaces in research and ease acceptance of PPIE approaches. Another similar postulated practice is epistemic apprenticeship, coined by Churcher (36). It concerns reorienting members from marginalized groups as mentors for those who are currently in power. Churcher (36), p. 10 stresses the need to institutionalize this practice to “expose and disrupt the epistemic solipsism and arrogance of privileged subjects through challenging imaginaries that sustain unspoken and uncritical attachments to dominant ways of knowing and being.” We think, that for such enterprise to be successful, it should begin with recognizing existence of diverse sets of epistemic resources—for example, Māori and non-Māori or neurodivergent and neurotypical. Thus, it requires third-order changes at research institutions. For such changes to be sustainable, these practices should be embedded in institutional ethos, to enable research institutions to influence behaviors of their members. It would allow to treat epistemic resources of unprivileged group members with respect, not only as a supportive “tool” for mainstream ones, therefore contributing to the contributory justice.
These directions can be linked with the idea of scientific/intellectual movements (SIM) which are collective efforts to advance research projects despite the opposition from scientific community (43, 76). They may serve as a means for broadening epistemic horizons of scientific institutions through identifying existing biases and providing new perspectives (77). SIMs can transform general ideas or values (e.g., democratic science or empowerment of marginalized groups) through research projects into a form of evidence [e.g., community-based research on experiencing dementia in Deaf community; (51) or research analyzing scientists’ mental health at academia; (69)]. Such movements are by definition “bottom-up” and their impact on institutional epistemic resources may be temporary without the support of authorities and senior staff (23, 59). However, they are grounded in local experiences and knowledge. SIMs may become vehicles for highlighting local hot spots within specific institutions which should be addressed, for example, frequent instances of testimonial injustice which lead to silencing a specific social group and precluding broader recognition of its experiences. SIM, being examples of non-institutionalized movements, can function as a starting point for more robust, second- and third-order changes which affect whole institution. Let us consider a hypothetical example of a research project on Deaf people’s research experiences. The study consists of focus groups and questionnaires discussing research accessibility, Deaf people’s relations with researchers and attitudes toward healthcare research. Started by hearing researchers, research team is broadened to include Deaf community members. Outcomes of the project highlight existing injustice and imply panel discussions with the authorities of the healthcare faculty. This in turn starts accessibility initiatives for whole faculty staff, conducted by Deaf educators. Then, Deaf people are hired on research and administrative positions. A debate on inclusion of Deaf epistemology into faculty’s curricula begins—the range of teaching methods is broadened to accommodate Deaf people’s visual and spatial modes of cognition. The faculty starts to diversify teaching programs, introduce bilingual spoken-signed newsletters, and invite Deaf students to its courses. It also creates a number of mixed Deaf-hearing research teams which facilitate cooperations with local community. It results in a dialog between the recent evidence-based knowledge and contextualized experiences of local Deaf community. This simplified and idealistic vision combines bits from each proposed direction. It begins with minor first- and second-order changes and then gradually leads to a third-order change, which broadens institutional epistemic resources and increases staff awareness. Many of such practices are already introduced within Deaf studies faculties. They contribute to transforming institutional decision-making procedures and establishing research institutions as a knowledge space open to PPIE.
6 Implications and challenges
The proposed directions can serve as a practical basis for analyzing the implications, limitations, and conditions for success of the conceptual framework. We believe that it has a real-life applicability; however, empirical research is needed. Deployment of all three orders of change at research institutions is one of necessary conditions for sustaining knowledge spaces for PPIE. We gathered and contextualized within PPIE practice only some directions, which can be further developed and adapted into local contexts. An increased focus on institutional epistemic features and practical application of third-order changes would enhance our understanding of epistemic processes within institutions. Consequently, this could contribute to better theorization of research institutions and structural epistemic injustice, leading to the establishment of a learning loop.
We recognize that proposed framework may encounter certain challenges. We would like to address a few of them. First, an issue of tensions between transformative roots of PPIE, especially participatory action research, and conservative structure of scientific institutions. A bottom-up movement, grounded within the virtue of social justice can easily become a means to an end and lose its transformative goals within the institution, which is focused merely on the quality of outcomes (78, 79). We acknowledge such risks, but no approach or paradigm is free of the risk of maladaptation in practice or misinterpretation [e.g., unintended disproportions within the three components of evidence-based medicine; (41)]. Thus, efforts of all involved agents are needed to stay on the track and consider all rationales behind the process. An increased focus on the role and epistemic features of institutions is crucial to hamper such risks.
This moves us also to the issue of feasibility and practicability of such changes. Third-order changes require significant efforts. Epistemic resources, both individual and collective, are resilient to change (18); thus, it is likely to expect the will to retain status quo. Moreover, changes in epistemic resources are not a sufficient condition for sustaining knowledge spaces. Changing a research institution requires all its staff to make significant efforts—organizational, financial, and educational, to implement and sustain a third-order change (59). In addition, such changes affect power relations and implicit biases in research institutions, as well as between public members and researchers (9, 30, 36). This pertains not only to the creation of knowledge spaces for PPIE but also to the idea of PPIE in general. Researchers’ attitudes may be ambivalent, especially among senior staff (30, 80). In addition, some funders and policymakers remain reluctant toward increasing active role of the members of public in research projects (32). While PPIE is increasingly acknowledged, several questions and uncertainties remain regarding its implementation (2). These are strong arguments restricting our proposition. While we argue for changes, we are also aware that the third-order change for knowledge spaces in PPIE may be an ideal, possible to reach to a varying degree. In addition, in complex institutions, such as universities, changes may be achieved within years or decades (59). They may start with first- or second-order changes and gradually reach more endorsement. Regarding PPIE, the process has already begun.
Another issue concerns downplaying the role of individual researchers and research teams, as well as hindering bottom-up initiatives. Institutionalization may easily become formalization, thus increasing formal barriers to researchers who conduct PPIE research. However, we argue that the features of third-order changes would allow for countering such issues. We acknowledge the role of individual researchers for PPIE, as well as sometimes conflicting values between participatory research and academia (79, 81). Researchers are crucial part of this process—they realize the knowledge spaces and represent academia in often very difficult contexts. Thus, changes within institutions should be holistic, involving the staff from each level of institutional hierarchy. They should integrate bottom-up and top-down movements, with the support of deliberate consideration of institutional epistemic features. We also emphasize that we do not want to promote a unified, monolithic approach to PPIE at research institutions. We recognize that each research institution has specific features and operates in a specific context, to which it should respond with its best possible understanding (14, 56), but, without further deliberation on general (epistemic) features of academic structure, research institutions may support PPIE in an (epistemically) harmful and vicious way (64, 79). This support, as well as the introduction of third-order changes, should be fitted to local contexts to facilitate the process and mitigate the risk of epistemic harms.
7 Conclusion
Within the study, we aimed to provide a conceptual framework for analyzing sociocultural context of institutional changes supporting establishing knowledge spaces and introducing PPIE practice. Ethical research conduct, especially in the PPIE context, requires considering various forms of knowledge present in contemporary society and examine existing biases. We argue that deep third-order changes, which aim to establish institutional meta-awareness about different forms of knowledge, are necessary (but not sufficient) to facilitate ethical PPIE practice. Research institutions—as active collective agents in the process—should make efforts to sustain favorable conditions for PPIE and mitigate possible harms to involved public members.
There is a need for empirical research which will operationalize and validate our proposal. This could take the form of case studies of specific changes within research institutions. In addition, the focus on institutional features is necessary to strengthen the theoretical basis for conceptualizing and planning changes. We need interdisciplinary collaboration which would enable the analysis of epistemic, social, political, economic, and organizational aspects of institutions. Furthermore, evaluative research is necessary to assess implementation of changes in practice.
Together with ethical inclusion and accessible research processes, the focus on research institutions is crucial to improve the PPIE conduct. While deep institutional changes aiming at establishing knowledge spaces may be a long-term ideal, they seem essential for fostering epistemically just and impactful research practice.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
TK: Conceptualization, Funding acquisition, Project administration, Writing – original draft, Writing – review & editing. JP: Conceptualization, Writing – review & editing. JG: Writing – review & editing. MW: Conceptualization, Funding acquisition, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the National Science Center, Poland, under the grant 2023/49/N/HS1/01023 and the funds of Jagiellonian University Medical College under the grant N43/DBS/000306.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^Harrington et al. (1) use the term “patient engagement.” However, it matches our understanding of PPIE. For discussion of the differences in terminology, please (see 1, 3).
2. ^These groups are not mutually exclusive. For example, there may be patient-activists who conduct research or researchers who are also patients. However, being positioned as a layperson in the opaque context of (health) research institution can nevertheless be vulnerabilising, existing power differences make such distinction useful; (see 31, 82).
References
1. Harrington, RL, Hanna, ML, Oehrlein, EM, Camp, R, Wheeler, R, Cooblall, C, et al. Defining patient engagement in research: results of a systematic review and analysis: report of the ISPOR patient-centered special interest group. Value Health. (2020) 23:677–88. doi: 10.1016/j.jval.2020.01.019
2. Banner, D, Bains, M, Carroll, S, Kandola, DK, Rolfe, DE, Wong, C, et al. Patient and public engagement in integrated knowledge translation research: are we there yet? Res Involv Engagem. (2019) 5:5. doi: 10.1186/s40900-019-0139-1
3. Locock, L, and Boaz, A. Drawing straight lines along blurred boundaries: qualitative research, patient and public involvement in medical research, co-production and co-design. Evid Policy. (2019) 15:409–21. doi: 10.1332/174426419X15552999451313
4. NIHR. Briefing notes for researchers. (2021). Available online at: https://www.nihr.ac.uk/documents/briefing-notes-for-researchers-public-involvement-in-nhs-health-and-social-care-research/27371 (Accessed August 1, 2024)
5. Liabo, K, Cockcroft, EJ, Boddy, K, Farmer, L, Bortoli, S, and Britten, N. Epistemic justice in public involvement and engagement: creating conditions for impact. Health Expect. (2022) 25:1967–78. doi: 10.1111/hex.13553
6. Grasswick, H. Epistemic injustice in science In: IJ Kidd, J Medina, and G Pohlhaus, editors. The Routledge handbook of epistemic injustice. 1st ed. New York: Routledge (2017). 313323.
7. Abma, TA, and Broerse, JEW. Patient participation as dialogue: setting research agendas. Health Expect. (2010) 13:160–73. doi: 10.1111/j.1369-7625.2009.00549.x
8. Galasiński, D, Ziółkowska, J, and Elwyn, G. Epistemic justice is the basis of shared decision making. Patient Educ Couns. (2023) 111:107681. doi: 10.1016/j.pec.2023.107681
9. Schreuer, N, Shpigelman, C-N, Mor, S, Sarid, M, Kanter, AS, and Sachs, D. Academic staff members’ engagement in accessible higher education for students with disabilities. High Educ Res Dev. (2024) 43:1171–86. doi: 10.1080/07294360.2023.2292652
10. Thomas, A, Kuper, A, Chin-Yee, B, and Park, M. What is “shared” in shared decision-making? Philosophical perspectives, epistemic justice, and implications for health professions education. J Eval Clin Pract. (2020) 26:409–18. doi: 10.1111/jep.13370
11. Vincent, R, Adhikari, B, Duddy, C, Richardson, E, Wong, G, Lavery, J, et al. ‘Working relationships’ across difference - a realist review of community engagement with malaria research. Wellcome Open Res. (2022) 7:13. doi: 10.12688/wellcomeopenres.17192.1
12. Balanzó-Guzmán, A, and Ramos-Mejía, M. Towards epistemic diversity in sustainability transitions: an exploration of hybrid socio-technical systems. Sustain Sci. (2023) 18:2511–31. doi: 10.1007/s11625-023-01370-9
13. Elliott, E, and Williams, G. Developing public sociology through health impact assessment. Sociol Health Illn. (2008) 30:1101–16. doi: 10.1111/j.1467-9566.2008.01103.x
14. Gibson, A, Britten, N, and Lynch, J. Theoretical directions for an emancipatory concept of patient and public involvement. Health Interdiscip J Soc Stud Health Illness Med. (2012) 16:531–47. doi: 10.1177/1363459312438563
15. Gibson, A, Welsman, J, and Britten, N. Evaluating patient and public involvement in health research: from theoretical model to practical workshop. Health Expect. (2017) 20:826–35. doi: 10.1111/hex.12486
16. Knowles, SE, Allen, D, Donnelly, A, Flynn, J, Gallacher, K, Lewis, A, et al. More than a method: trusting relationships, productive tensions, and two-way learning as mechanisms of authentic co-production. Res Involv Engagem. (2021) 7:34. doi: 10.1186/s40900-021-00262-5
17. Harting, J, Kruithof, K, Ruijter, L, and Stronks, K. Participatory research in health promotion: a critical review and illustration of rationales. Health Promot Int. (2022) 37:ii7–ii20. doi: 10.1093/heapro/daac016
18. Pohlhaus, G. Relational knowing and epistemic injustice: toward a theory of willful hermeneutical ignorance. Hypatia. (2012) 27:715–35. doi: 10.1111/j.1527-2001.2011.01222.x
19. Cue, KR. Defining hearing culture in context of deaf culture: a grounded theory examination. Disabil Soc. (2024) 40:1–24. doi: 10.1080/09687599.2024.2369649
20. Dotson, K. Conceptualizing epistemic oppression. Soc Epistemol. (2014) 28:115–38. doi: 10.1080/02691728.2013.782585
21. Dotson, K. A cautionary tale: on limiting epistemic oppression. Front J Women Stud. (2012) 33:24. doi: 10.5250/fronjwomestud.33.1.0024
22. Bartunek, JM, and Moch, MK. First-order, second-order, and third-order change and organization development interventions: a cognitive approach. J Appl Behav Sci. (1987) 23:483–500. doi: 10.1177/002188638702300404
23. Vincent, R, Kamuya, D, Adhikari, B, Nyirenda, D, Lavery, JV, and Molyneux, S. Community engagement and the centrality of ‘working relationships’ in health research. BMJ Glob Health. (2024) 9:e015350. doi: 10.1136/bmjgh-2024-015350
24. Collins, S. Group duties: their existence and their implications for individuals. New York: Oxford University Press (2019).
25. Galica, J, Silva, A, and Robb, K. Developing an educational resource for gynecological cancer survivors and their caregivers: a methods and experience paper. Can Oncol Nurs J. (2024) 34:4–9. doi: 10.5737/236880763414
26. Emanuel, EJ, and Grady, C. Four paradigms of clinical research and research oversight. Camb Q Healthc Ethics. (2007) 16:82–96. doi: 10.1017/S0963180107070090
27. Cram, F, and Mertens, DM In: SN Hesse-Biber and RB Johnson, editors. Transformative and indigenous frameworks for multimethod and mixed methods research. New York: Oxford University Press (2015)
28. Côté, CI. A critical and systematic literature review of epistemic justice applied to healthcare: recommendations for a patient partnership approach. Med Health Care Philos. (2024) 27:455–77. doi: 10.1007/s11019-024-10210-1
29. Ho, A. Trusting experts and epistemic humility in disability. Int J Fem Approaches Bioeth. (2011) 4:102. doi: 10.2979/intjfemappbio.4.2.102
30. Boylan, A, Locock, L, Thomson, R, and Staniszewska, S. “About sixty per cent I want to do it”: health researchers’ attitudes to, and experiences of, patient and public involvement (PPI)—a qualitative interview study. Health Expect. (2019) 22:721–30. doi: 10.1111/hex.12883
31. Carel, H, and Kidd, IJ. Individual vices and institutional failings as drivers of vulnerabilisation. Soc Epistemol. (2024) 39:150–65. doi: 10.1080/02691728.2024.2400083
32. Biddle, MSY, Gibson, A, and Evans, D. Attitudes and approaches to patient and public involvement across Europe: a systematic review. Health Soc Care Community. (2021) 29:18–27. doi: 10.1111/hsc.13111
33. Schilling, I, and Gerhardus, A. Is this really empowerment? Enhancing our understanding of empowerment in patient and public involvement within clinical research. BMC Med Res Methodol. (2024) 24:205. doi: 10.1186/s12874-024-02323-1
34. O’Shea, A, Boaz, AL, and Chambers, M. A hierarchy of power: the place of patient and public involvement in healthcare service development. Front Sociol. (2019) 4:38. doi: 10.3389/fsoc.2019.00038
35. Dutta, U, Fernández, JS, Galletta, A, and Langhout, RD. Participatory action research as movement toward radical relationality, epistemic justice, and transformative intervention: a multivocal reflection In: APA handbook of research methods in psychology: Research designs: Quantitative, qualitative, neuropsychological, and biological, eds. Cooper H, Coutanche MN, McMullen LM, Panter AT, Rindskopf D, Sher KJ. vol. 2. 2nd ed. Washington: American Psychological Association (2023). 305–27.
36. Churcher, M. Designing for epistemic justice: epistemic apprenticeship as an institutional commitment. Philos Soc Crit. (2023) 51:501–26. doi: 10.1177/01914537231184493
37. Fricker, M. Epistemic injustice: Power and the ethics of knowing. New York: Oxford University Press (2007). 1208 p.
38. Carel, H, and Kidd, IJ. Epistemic injustice in healthcare: a philosophial analysis. Med Health Care Philos. (2014) 17:529–40. doi: 10.1007/s11019-014-9560-2
39. Pohlhaus, G Jr. Varietes of epistemic injustice In: IJ Kidd, J Medina, and G Pohlhaus, editors. The Routledge handbook of epistemic injustice. New York: Routledge (2017). 13–26.
40. Hookway, C. Some varieties of epistemic injustice: reflections on Fricker. Episteme. (2010) 7:151–63. doi: 10.3366/epi.2010.0005
41. Moes, F, Houwaart, E, Delnoij, D, and Horstman, K. Questions regarding ‘epistemic injustice’ in knowledge-intensive policymaking: two examples from Dutch health insurance policy. Soc Sci Med. (2020) 245:112674. doi: 10.1016/j.socscimed.2019.112674
42. McHugh, NA. Epistemic communities and institutions In: IJ Kidd, J Medina, and G Pohlhaus, editors. The Routledge handbook of epistemic injustice. 1st ed. New York: Routledge (2017). 270–8.
43. Koskinen, I, and Rolin, K. Scientific/intellectual movements remedying epistemic injustice: the case of indigenous studies. Philos Sci. (2019) 86:1052–63. doi: 10.1086/705522
44. Anderson, E. Epistemic justice as a virtue of social institutions. Soc Epistemol. (2012) 26:163–73. doi: 10.1080/02691728.2011.652211
45. Bierer, BE, White, SA, Meloney, LG, Ahmed, HR, Strauss, DH, and Clark, LT. Achieving diversity, inclusion, and equity in clinical research: guidance document. Cambridge (MA): Multi-Regional Clinical Trials, MRCT Center of Brigham and Women’s Hospital and Harvard (2021). Available online at: https://mrctcenter.org/diversity-in-clinical-research/wpcontent/uploads/sites/11/2021/09/MRCT-Center-Diversity-GuidanceDocument-Version-1.2.pdf
46. Krawczyk, T, Piasecki, J, Wasylewski, M, and Waligora, M. Ethics of research engagement with deaf people. A qualitative evidence synthesis. J Deaf Stud Deaf Educ. (2024) 29:443–55. doi: 10.1093/jdsade/enae024
47. Anderson, ML, Riker, T, Hakulin, S, Meehan, J, Gagne, K, Higgins, T, et al. Deaf ACCESS: adapting consent through community engagement and state-of-the-art simulation. J Deaf Stud Deaf Educ. (2020) 25:115–25. doi: 10.1093/DEAFED/ENZ035
48. Provincial Human Services and Justice Coordinating Committee Guidelines for enhancing the engagement of people with lived experience across the HSJCC network (2021). Available at: https://hsjcc.on.ca/wp-content/uploads/Guidelines-for-Enhancing-the-Engagement-of-People-With-Lived-Experience-Across-the-HSJCC-Network.pdf
49. WHO. WHO framework for meaningful engagement of people living with noncommunicable diseases, and mental health and neurological conditions. Geneva: WHO (2023).
50. IAP2 USA. IAP2 Core values, ethics, spectrum. (2025). Available online at: https://www.iap2usa.org/cvs (Accessed August 27, 2025)
51. Young, A, Ferguson-Coleman, E, and Keady, J. Authentic public and patient involvement with deaf sign language users: it is not just about language access. Dementia. (2018) 17:1001–10. doi: 10.1177/1471301218789567
52. Anderson, ML, Riker, T, and Wilkins, AM. Application of the truth and reconciliation model to meaningfully engage deaf sign language users in the research process. Cultur Divers Ethnic Minor Psychol. (2023) 29:15–23. doi: 10.1037/cdp0000445
53. Buedo, P, Odziemczyk, I, Perek-Białas, J, and Waligora, M. How to embed ethics into laboratory research. Account Res. (2023) 31:767–85. doi: 10.1080/08989621.2023.2165916
54. Buedo, P, Prieto, E, Perek-Białas, J, Odziemczyk-Stawarz, I, and Waligora, M. More ethics in the laboratory, please! Scientists’ perspectives on ethics in the preclinical phase. Account Res. (2024) 32:1–16. doi: 10.1080/08989621.2023.2294996
55. Timmermans, J, Blok, V, Braun, R, Wesselink, R, and Nielsen, RØ. Social labs as an inclusive methodology to implement and study social change: the case of responsible research and innovation. J Responsible Innov. (2020) 7:410–26. doi: 10.1080/23299460.2020.1787751
56. Greenhalgh, T, Hinton, L, Finlay, T, Macfarlane, A, Fahy, N, Clyde, B, et al. Frameworks for supporting patient and public involvement in research: systematic review and co-design pilot. Health Expect. (2019) 22:785–801. doi: 10.1111/hex.12888
57. Smits, D-W, van Meeteren, K, Klem, M, Alsem, M, and Ketelaar, M. Designing a tool to support patient and public involvement in research projects: the involvement matrix. Res Involv Engagem. (2020) 6:30. doi: 10.1186/s40900-020-00188-4
58. Scott, WR. Reflections: the past and future of research on institutions and institutional change. J Change Manag. (2010) 10:5–21. doi: 10.1080/14697010903549408
59. Boyce, ME. Organizational learning is essential to achieving and sustaining change in higher education. Innov High Educ. (2003) 28:119–36. doi: 10.1023/B:IHIE.0000006287.69207.00
60. Hechanova, MRM, Caringal-Go, JF, and Magsaysay, JF. Implicit change leadership, change management, and affective commitment to change. Leadersh Organ Dev J. (2018) 39:914–25. doi: 10.1108/LODJ-01-2018-0013
61. Fricker, M. Institutional epistemic vices: the case of inferential inertia In: IJ Kidd, H Battaly, and Q Cassam, editors. Vice epistemology. Abingdon, Oxon; New York, NY: Routledge (2020). 89–107.
62. Fricker, M. Can there be institutional virtues In: TS Gendler and J Hawthorne, editors. Oxford studies in epistemology. Oxford: Oxford University Press (2009). 235–52.
63. Tang, BL. Deficient epistemic virtues and prevalence of epistemic vices as precursors to transgressions in research misconduct. Res Ethics. (2024) 20:17470161231221258. doi: 10.1177/17470161231221258
64. Baird, C, and Calvard, TS. Epistemic vices in organizations: knowledge, truth, and unethical conduct. J Bus Ethics. (2019) 160:263–76. doi: 10.1007/s10551-018-3897-z
65. Karlsson, AW, and Janssens, A. Patient and public involvement and engagement (PPIE) in healthcare education and thesis work: the first step towards PPIE knowledgeable healthcare professionals. BMJ Open. (2023) 13:e067588. doi: 10.1136/bmjopen-2022-067588
66. Galica, J, Bilodeau, K, Strohschein, F, Powell, TL, Lambert, LK, and Truant, TLO. Building and sustaining a postgraduate student network: the experience of oncology nurses in Canada. Can Oncol Nurs J. (2018) 28:288–93. doi: 10.5737/23688076284288293
67. Hoffman, KM, Trawalter, S, Axt, JR, and Oliver, MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci. (2016) 113:4296–301. doi: 10.1073/pnas.1516047113
68. Marschark, M, and Wauters, L. Cognitive functioning in deaf adults and children In: The Oxford handbook of deaf studies, language, and education, vol. 1. 2nd ed. Spencer E. New York: Oxford University Press (2012). 486–99.
69. Hawke, LD, Sheikhan, NY, Jones, N, Slade, M, Soklaridis, S, Wells, S, et al. Embedding lived experience into mental health academic research organizations: critical reflections. Health Expect. (2022) 25:2299–305. doi: 10.1111/hex.13586
70. Listman, JD, and Dingus-Eason, J. How to be a deaf scientist: building navigational capital. J Divers High Educ. (2018) 11:279–94. doi: 10.1037/dhe0000049
71. Harris, R, Holmes, HM, and Mertens, DM. Research ethics in sign language communities. Sign Lang Stud. (2009) 9:104–31. doi: 10.1353/sls.0.0011
72. Gertz, G, and Boudreault, P. The SAGE Deaf Studies Encyclopedia. 3 vols. Thousand Oaks, CA: SAGE Publications, Inc. (2016). doi: 10.4135/9781483346489
73. Pihama, L, Cram, F, and Walker, S. Creating methodological space: a literature review of Kaupapa Maori research. Can J Native Educ. (2002) 26:5910.
74. Hall, M. Rethinking Māori academic development in New Zealand universities. Wellington: Open access Victoria University of Wellington (2014).
75. Koskinen, I. How institutional solutions meant to increase diversity in science fail. Synthese. (2022) 200:483. doi: 10.1007/s11229-022-03959-6
76. Frickel, S, and Gross, N. A general theory of scientific/intellectual movements. Am Sociol Rev. (2005) 70:204–32. doi: 10.1177/000312240507000202
77. Koskinen, I. Participation and objectivity. Philos Sci. (2023) 90:413–32. doi: 10.1017/psa.2022.77
78. Ives, J, Damery, S, and Redwod, S. PPI, paradoxes and Plato: who’s sailing the ship? J Med Ethics. (2013) 39:181–5. doi: 10.1136/medethics-2011-100150
79. Turcotte, PL, Holmes, D, and Murray, SJ. The shiny new object: deconstructing the patient-oriented paradigm in health sciences. J Eval Clin Pract. (2023) 29:700–8. doi: 10.1111/jep.13823
80. Thompson, J, Barber, R, Ward, PR, Boote, JD, Cooper, CL, Armitage, CJ, et al. Health researchers’ attitudes towards public involvement in health research. Health Expect. (2009) 12:209–20. doi: 10.1111/j.1369-7625.2009.00532.x
81. Mertens, DM. Transformative research: personal and societal. Int J Transform Res. (2017) 4:18–24. doi: 10.1515/ijtr-2017-0001
82. Carel, H, and Kidd, IJ. Epistemic injustice in medicine and healthcare In: IJ Kidd, J Medina, and G Pohlhaus, editors. The Routledge handbook of epistemic injustice. 1st ed. New York: Routledge (2017)
Keywords: public and patient engagement, public and patient involvement, institutional change, epistemic justice, knowledge space, research institution, research ethics
Citation: Krawczyk T, Piasecki J, Galica J and Waligora M (2025) Meaningful public involvement: changing research institutions toward epistemic justice. Front. Public Health. 13:1655189. doi: 10.3389/fpubh.2025.1655189
Edited by:
Maia Ingram, University of Arizona, United StatesReviewed by:
Francesca Moretti, University of Verona, ItalyNatalie Sampson, University of Michigan–Dearborn, United States
Copyright © 2025 Krawczyk, Piasecki, Galica and Waligora. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcin Waligora, bS53YWxpZ29yYUB1ai5lZHUucGw=
†ORCID: Tomasz Krawczyk, orcid.org.0000-0002-3093-2584
Jan Piasecki, orcid.org.0000-0003-1298-736X
Jacqueline Galica, orcid.org.0000-0002-3072-2472
Marcin Waligora, orcid.org.0000-0002-1553-1416