 Mingrui Zhang
Mingrui Zhang Hongxu Zhu
Hongxu Zhu Yi Xu1,2*
Yi Xu1,2* Kaihan Yang
Kaihan Yang- 1School of Basic Medical Sciences, Chengdu University, Chengdu, China
- 2School of Nursing, Chengdu University, Chengdu, China
Background: Individuals infected with HIV experience significant stigma, and since this stigma can severely impact their quality of life, it is essential to implement interventions aimed at reducing the stigma faced by this population.
Objective: To summarize and analyze the core components and effectiveness of interventions targeting stigma among people living with HIV. Methods A scoping review methodology was employed to search the PubMed, Web of Science, Embase, Cochrane, and Scopus databases from their inception dates up to March 14, 2025. The included studies were categorized and analyzed.
Results: A total of 39 articles were included in this review. Interventions addressing HIV-related stigma were conducted among various populations including pregnant women, older adults, adolescents, and sexual minority groups. Intervention contents included cognitive behavioral therapy, motivational interviewing, information-motivation-behavioral skills intervention, among others. There was significant variation in the frequency and duration of stigma interventions. Outcome measures used across studies included internalized stigma, externalized HIV Stigma, enacted stigma.
Conclusion: The findings indicate that most interventions demonstrate varying degrees of effectiveness in reducing HIV-related stigma, with CBT-based approaches potentially being more effective, although standardization and longer follow-up periods are required. However, the differences in effectiveness across different populations, intervention content, implementation forms, and follow-up durations suggest that current stigma reduction strategies for AIDS still have room for optimization.
1 Introduction
According to the Joint United Nations Programme on HIV/AIDS, by the end of 2023, there were approximately 39.9 million people worldwide living with HIV infection/AIDS, among whom 1.3 million were newly diagnosed cases in that year, and 30.7 million individuals were receiving antiviral treatment (1). With continuous advancements and effective implementation of antiretroviral therapy, the prognosis for people living with HIV has improved significantly, and their life expectancy has increased. In 2016, LAZARUS et al. proposed a new goal: ensuring that 90% of those achieving viral suppression attain good quality of life (2). This objective highlights that as survival duration extends for people living with HIV, improving their quality of life has become a key issue in global AIDS prevention and control efforts. Quality of life is a multidimensional concept encompassing physical health, psychological well-being, social relationships, and environmental adaptation. Among these dimensions, stigma stands out as one of the most significant factors affecting the quality of life of people living with HIV.
The word “stigma” originated from ancient Greece, referring to the mark left by a hot iron on prisoners, as well as to a stain or blemish identified by moral standards as abnormal or bad. Goffman pointed out that shame is a notable, marked difference (3), which makes various forms of discrimination possible, ultimately depriving individuals/groups of full social acceptance, reducing personal opportunities (4), and intensifying social inequality. In people living with HIV, HIV-related stigma mainly includes enacted stigma, anticipated stigma, and internalized stigma (5). Enacted stigma refers to actual experiences of prejudice, discrimination, and exclusion described by stigmatized individuals (6); anticipated stigma involves expectations of prejudicial reactions from others upon learning of someone’s HIV status (7); internalized stigma occurs when members of stigmatized groups accept negative societal beliefs and feelings about themselves and experience social devaluation associated with their stigmatized status (8). Stigma not only harms the mental health of people living with HIV but may also hinder disease prevention and treatment as well as social integration. At the psychological level, stigma easily leads to depression, anxiety, or self-denial among infected individuals, and even refusal of testing or delayed treatment due to fear of discrimination, seriously affecting adherence to antiviral therapy (9). Regarding social relationships, infected individuals may experience intensified loneliness and financial hardship due to family rejection, workplace discrimination, or social isolation. Furthermore, avoidance of treatment can further affect their management of personal health, creating a vicious cycle. Particularly for women, sexual minorities, drug users, and other vulnerable populations, multiple stigmas are more likely to add to the low quality of their life (10).
To alleviate stigma among people living with HIV and improve their quality of life, it is urgent to explore effective intervention measures. Existing reviews have addressed some aspects of HIV-related stigma; however, limitations remain. First, although various statistical methods have been included in previous studies, the methodological quality of these studies varies (11); second, the study locations were limited to specific regions, lacking generalizability (12); third, the populations studied were restricted to specific subgroups, limiting the transferability of findings (13). Therefore, it remains unclear whether the reported stigma-reduction interventions can be extended to other HIV populations and yield similar effects. Although several reviews have summarized interventions to combat HIV stigma and identified significant heterogeneity in interventions, controls, and outcomes (14), few reviews specifically focus on randomized controlled trials—the most robust form of evidence.
Given the current fragmented evidence and the lack of a comprehensive focus on rigorously evaluated trials, we conducted a scoping review of randomized controlled trials targeting HIV-related stigma, systematically organizing RCT-based interventions for HIV-related stigma worldwide. The aim is to address issues such as interventions to reduce stigma among HIV-infected individuals, their effectiveness, and recommendations for future research.
2 Define the scope of the review objectives
This scoping review aims to determine the scope and content of existing literature regarding stigma among people living with HIV, and to provide guiding recommendations for future research and practice. Specifically, this review aims to present a conceptual mapping of the content, format, indicators, stigma assessment tools, and outcomes of interventions addressing HIV-related stigma.
3 Inclusion criteria
The detailed eligibility criteria for the study were determined using the PICOS framework:
(1) Participants: Participants included in the study must be individuals infected with HIV, without restrictions on race, age, nationality, etc.;
(2) Intervention: The experimental group received any intervention that can reduce HIV-related stigma;
(3) Control: The control group received standard treatment or care, routine education, or is placed on a waiting list;
(4) Outcomes: The study outcomes must include HIV-related stigma, encompassing internalized HIV stigma, externalized HIV stigma, anticipated HIV stigma, and enacted HIV stigma;
(5) Design: The study must be a randomized controlled trial (RCT).
4 Methods
This study was initially designed as a meta-analysis and registered in PROSPERO with the identifier CRD420250611522. However, due to significant heterogeneity among the interventions and study designs included in this review, a scoping review design was deemed more appropriate. The methods of this scoping review deviated somewhat from the original PROSPERO registration. This report follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist and explanation (15), and is registered in OSF with the DOI https://doi.org/10.17605/OSF.IO/KT9XR.
4.1 Search strategy
A comprehensive search was conducted across five databases, including PubMed, Web of Science, Embase, Cochrane, and Scopus, from the establishment of the databases until March 14, 2025, using various search strategies. For example, in PubMed, a combination of Medical Subject Headings (MeSH) terms and text words were applied for the following concepts: ① HIV ② stigma ③ RCT. Grey literature, such as conference abstracts and government reports, was excluded. Additionally, reference lists of selected articles were examined to identify any additional articles or studies not captured through the database searches. Detailed information on all search strategies used can be found in the Supplementary materials.
4.2 Study selection
All search results were imported into the reference management program Endnote X9, and duplicates were removed. Two researchers (ZMR and ZHX) independently screened the titles and abstracts of the studies according to the inclusion criteria. We read the full texts of potentially relevant studies to select eligible articles and provided detailed reasons for exclusion. The specific screening process is shown in Figure 1. Any discrepancies during the selection process were resolved through discussion between the two researchers or consultation with a third researcher (XY).
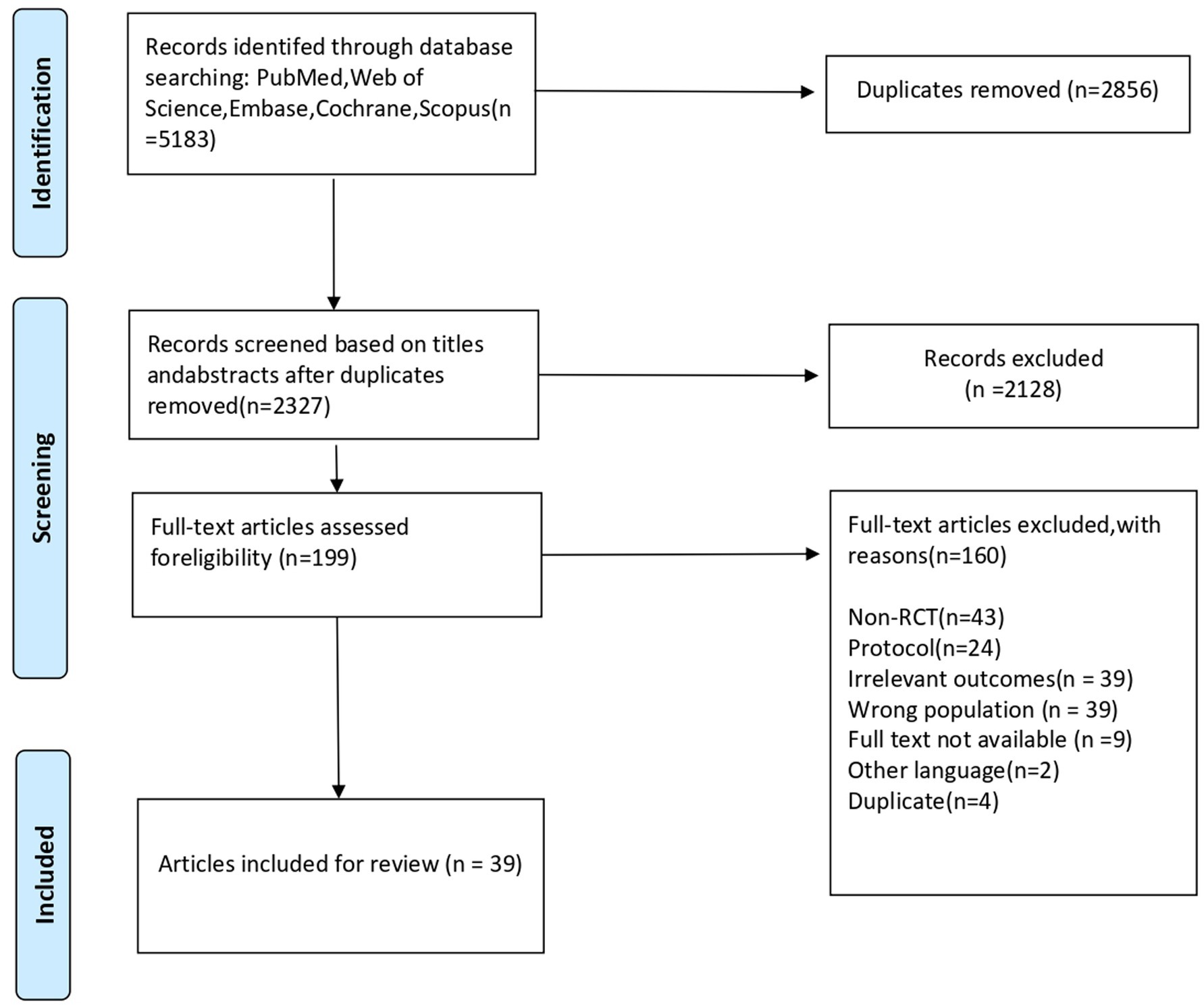
Figure 1. PRISMA 2009 flow diagram. From: Moher et al. (64). For more information, visit www.prisma-statement.org.
4.3 Data extraction
Two researchers (ZMR and ZHX) independently extracted and recorded the data into a predesigned form. Any discrepancies were resolved through discussion or by involving a third researcher (XY). The extracted data were entered into an Excel spreadsheet for analysis. The data extraction table included the following categories: (1) general study information: first author, year, and country; (2) study type, methodology, and sample size; (3) study participants; (4) intervention content in the intervention and control groups; (5) intervention implementers, intervention format (online or offline); (6) intervention dose (frequency of interventions, duration per session, total duration of intervention, and follow-up period); (7) specific intervention content; (8) outcome measures; (9) measurement tools; (10) main outcome results of the intervention.
4.4 Data synthesis and analysis
The translation was conducted by two reviewers (ZMR and ZHX) after reaching a consensus through discussion. Comprehensive data from various sources led to several key observations: (1) general information of the included studies; (2) intervention content; (3) intervention format; (4) intervention implementer; (5) measures for the control group; (6) number, frequency, and duration of interventions; (7) outcome indicators and measurement tools; (8) follow-up period; (9) intervention effectiveness.
4.5 Critical evaluation
The objective of this study was to determine the scope of all available literature regarding interventions for HIV-related stigma; therefore, to consider the full body of available evidence, articles included in this scoping review were not subjected to formal critical appraisal (16).
5 Result
Systematic literature search identified 5,183 references on March 14, 2025. Thirty-nine studies were considered to meet the inclusion criteria. The characteristics of the included literature are shown in Table 1.

Table 1. Characteristics of included studies.
5.1 General information of the included studies
All 39 included studies were published between 2003 and 2024, with 24 (62%) originating from the United States, 2 (5%) from South Africa, 1 (3%) from China, 1 (3%) from Indonesia, 1 (3%) from Belgium, 1 (3%) from Nepal, 1 (3%) from Kenya, 1 (3%) from Uganda, 1 (3%) from South Korea, 1 (3%) from Zimbabwe, 1 (3%) from Pakistan, 1 (3%) from India, 1 (3%) from Canada, 1 (3%) from Zambia, 1 (3%) from Sweden. All 39 studies were randomized controlled trials. The sample sizes ranged from 22 to 1799 across the studies, totaling 9,058.
Nationalities of the study samples: 10 studies (26%) were from the United States, 4 studies (10%) from South Africa, 4 studies (10%) from Kenya, 2 studies (5%) from Tanzania, 2 studies (5%) from India, 2 studies (5%) from Thailand, 2 studies (5%) from Zambia, 2 studies (5%) from Uganda, 1 study (3%) from Indonesia, 1 study (3%) from Ethiopia, 1 study (3%) from Australia, 1 study (3%) from Nepal, 1 study (3%) from Russia, 1 study (3%) from the Dominican Republic, 1 study (3%) from South Korea, 1 study (3%) from Zimbabwe, 1 study (3%) from Pakistan, and 1 study (3%) from Vietnam.
All samples included in the studies were individuals infected with HIV: 10 studies (26%) involved female HIV-infected populations, among which 2 studies (5%) focused on perinatal women, 2 studies (5%) on mothers, and 1 study on married and widowed women; 2 studies (5%) involved Black women; 8 studies (21%) involved adolescents; 4 studies (10%) targeted sexual minority groups; 1 study (3%) involved older adult(s); 1 study (3%) involved drug users; 1 study (3%) involved men who consumed alcohol; 1 study (3%) involved HIV patients who had recently initiated HIV care; 1 study (3%) involved HIV patients not receiving ART; 1 study (3%) involved HIV patients with depression.
5.2 Intervention contents for reducing stigma among people living with HIV
The 22 studies included in this paper explicitly reported the methods/theories upon which HIV-related stigma reduction interventions were based, with five studies employing two or more methods/theories. The most frequently used method was Cognitive Behavioral Therapy (n = 7) (13, 17–22), followed by Motivational Interviewing (n = 4) (17, 20, 23–25), Information-Motivation-Behavioral Skills (IMB) intervention (n = 3) (26–28), and Acceptance and Commitment Therapy (n = 2) (5, 29).
5.3 Intervention formats for reducing stigma among people living with HIV
The intervention measures in different studies can be categorized into online and offline approaches, with some studies employing a combination of both (30). Offline interventions are primarily conducted through face-to-face interactions, including counseling (23, 24, 31–35), education (5, 13, 17, 18, 20–22, 25, 26, 29, 32, 33, 36–42), and discussion sessions (13, 17, 18, 21, 24, 26, 28, 30, 37, 38, 43–45). Additional offline strategies include follow-up monitoring of participants to improve adherence (30, 34, 35, 42, 46), educating network members after offline recruitment (27), and providing economic support for participants to purchase agricultural supplies (43). Online interventions are mainly implemented via platforms such as telephone calls, text messages, and social media software. These include delivering educational courses through online platforms (19), posting relevant information or engaging in communication via social media (30, 47–50), and using electronic devices to watch specially produced videos (51, 52).
5.4 Implementers of interventions to reduce stigma among people living with HIV
Because online interventions are delivered through electronic devices, only offline interventions involve implementers. Implementers can be broadly categorized into healthcare workers and non-healthcare workers. Healthcare workers include physicians, nurses (28, 31, 42), psychiatrists (19), national trainers with a graduate degree in public health (38), and staff members of health organizations (24, 30, 44, 45); non-healthcare workers include psychologists (5, 23), community support workers (32, 37), researchers (18), patients (20), family members, peers within research advisory groups and social support systems (13, 20, 21, 23, 25, 26, 29, 33, 34, 36, 40, 46), and other individuals living with HIV (17, 53).
5.5 Control group interventions in research on reducing stigma among people living with HIV
All studies included in this review were RCTs and had control groups. Compared with the intervention groups, participants in the control groups engaged in various activities, including receiving standard HIV treatment and care (5, 13, 17, 20–26, 28–35, 37–40, 42–46, 50–53); being assigned to a waitlist and later receiving the same intervention as the experimental group (18); recruiting network members offline without providing education; receiving usual care plus a booklet containing standard information (25, 49); receiving general HIV information via software (47); receiving general health education (23) and self-management education (21); and one study did not report the intervention details for the control group (19).
5.6 Number of interventions, frequency, and duration
Among the 39 included studies, the number of interventions ranged from 1 to 36. The highest intervention frequency was eight times per week, and the duration of each intervention session ranged from 1 min to 2 h. The total duration of the interventions ranged from 3 weeks to 18 months, with 16 studies not reporting the intervention duration.
5.7 Outcome measures and assessment tools
The primary outcome measure was HIV-related stigma, including total stigma, internalized stigma, anticipated stigma, enacted stigma, and external stigma. The range of outcome measurement tools used in the included studies was broad, including the HIV Stigma Scale (HSS)(36, 43, 50); a 14-item subscale of the HSS (48); a modified 16-item scale derived from the HSS (35, 42); a 12-item scale adapted or simplified from the HSS (23, 30); a 10-item scale adapted or simplified from the HSS (17, 20, 24, 31, 46, 50); a 9-item scale from the HSS (21); a modified 7-item scale based on the HSS (26); an 8-item scale adapted from the HSS (33); a 5-item scale adapted from the HSS (51); the Internalized AIDS-Related Stigma Scale (IA-RSS) (13, 40, 51, 53); a 9-item version of the IA-RSS (43); a 7-item version of the IA-RSS (5); a 6-item version of the IA-RSS (29, 49); a modified 5-item version of the IA-RSS (51); a 3-item version of the IA-RSS (44); the 33-item HIV/AIDS Stigma Instrument—Patient Version (HASI-P) (36); a modified 28-item version of the HASI-P (45); a 5-item version of the HASI-P (32); the 28-item Internalized HIV Stigma Scale (IHSS) (52); a questionnaire developed by the Global Stigma and Discrimination Indicators Working Group (GSDIWG) and the Strive Research Consortium to assess HIV stigma in the general population (47); the 23-item HIV Stigma Scale developed by Genberg et al. (38); a modification of the Westbrook LE Pediatric Epilepsy-Related Stigma Scale (37); Serithi’s 16-item Internalized Stigma Scale (18); the six-item internalized stigma subscale from the Mechanisms of HIV Stigma Scale (19); the Demi HIV Stigma Scale (28); the HIV Stigma Scale developed by Earnshaw et al. (25); one study measured HIV stigma using a modified TRIP project-based scale (27); and one study did not specify the name of the questionnaire (34).
5.8 Follow-up time
Among the 39 included studies, the follow-up time ranged from 3 weeks to 36 months, with the most common follow-up period being 6 months (n = 10). One study conducted assessments immediately after the intervention; one study conducted follow-up at 12 months postpartum; and another study followed up participants 80 to 120 days after the last intervention. All included studies reported changes after the intervention in their follow-up assessments.
5.9 Intervention effect
59% (23/39) of the studies reported significant changes in stigma after the intervention, indicating the effectiveness of the interventions in reducing HIV-related stigma. Two studies reported a significant decrease in stigma after the intervention, but there was no significant difference compared with the control group (36, 47). 28% (11/39) of the studies reported that the intervention had no effect on reducing HIV stigma. One study reported that both the intervention and control groups experienced reduced internalized stigma, but the intervention group showed increased externalized stigma (17). One study reported that the average total stigma score in the intervention group was lower than that in the control group; both groups demonstrated decreased total stigma scores compared with baseline, but the intervention group exhibited increased externalized stigma compared with baseline (20). Additionally, one study using a multilevel intervention achieved different outcomes by modifying the sequence of interventions (35).
6 Discussion
Through a scoping review of 39 randomized controlled trials, it was found that although there were significant differences between populations and outcomes, most interventions showed effectiveness in reducing HIV related stigma, particularly those based on cognitive behavioral therapy.
6.1 Principal findings
The 39 randomized controlled trials (RCTs) included in this article show that, although overall 59% (23/39) of the studies demonstrated that interventions effectively reduced stigma among people living with HIV, there was substantial variation in intervention effectiveness across different studies.
6.1.1 Standardize intervention content to promote the application and dissemination of interventions
Currently, there is no unified standard for specific intervention programs targeting HIV-related stigma, and the content of interventions varies. In teams conducting HIV stigma interventions, some are composed of healthcare workers while others consist of individuals from social networks, aiming to provide more comprehensive and long-term support to patients in order to enhance the effectiveness of interventions. This study found that research employing cognitive behavioral therapy (CBT) yielded relatively positive outcomes, showing significant effects in reducing stigma. CBT is a structured, problem-oriented approach that uses cognitive and behavioral techniques to challenge dysfunctional beliefs (54). CBT helps individuals reduce negative self thoughts, accept themselves, and ultimately lower internal shame through the deconstruction and reconstruction of cognition and behavior. Research indicates that CBT has largely helped address various mental health issues among people living with HIV/AIDS. These findings suggest that combining antiretroviral therapy (ART) with psychological interventions (CBT) is a better treatment option for people living with HIV/AIDS than standard treatment alone (13, 17, 19). Meanwhile, interventions based on Motivational Interviewing (MI) and Acceptance and Commitment Therapy (ACT) have not demonstrated as consistent an effect as CBT. In some studies, MI intervention has effectively reduced HIV related stigma by empowering individuals and helping them build a strong inner world (23); ACT intervention helps HIV infected individuals accept their inner thoughts, coexist peacefully with pain, establish a more stable and objective self-awareness foundation, guide individuals to shift their perception of stigma towards a meaningful life (5), and thus reduce HIV related stigma. However, these two theories have shown different intervention effects in different studies. Through comparison, it is found that the reason for the different intervention results is likely due to the specificity of the study population. Due to the special psychological conditions of HIV positive drug users and HIV positive men who have sex with men in some studies, the intervention effects of MI and ACT are affected (5, 23), ultimately leading to no significant change in the stigma of HIV infected individuals. In comparison, studies with unclear theoretical foundations or overly broad intervention contents were less effective, indicating that a scientific theoretical basis is crucial in interventions aimed at reducing HIV-related stigma (40, 51). Therefore, during the development of intervention programs, strict adherence to or reference of scientific theories or evidence is necessary to formulate rigorous, standardized, and clearly defined intervention plans, thereby advancing the implementation of interventions targeting HIV-related stigma and promoting patient well-being.
6.1.2 Adjust the design of intervention formats to promote diverse applications of intervention forms
In terms of intervention formats, they are mainly divided into online and offline categories. Face-to-face offline interventions (especially group discussions and support groups) have demonstrated significant advantages in improving enacted stigma and internalized stigma. In-person interactions help break the sense of isolation and provide emotional support. Moreover, offline interventions can adjust content and methods promptly according to participants’ facial expressions and body language, facilitating smooth implementation of the intervention (55). Additionally, these interventions can strengthen individuals’ connections with society and reduce sensitivity to external negative evaluations (56). However, loss to follow-up may occur due to issues such as distance and privacy concerns. Conversely, although online interventions (e.g., app notifications, app-based courses) are convenient and offer better privacy, they largely rely on self-directed learning, which demands higher levels of personal initiative. This often significantly increases the likelihood of incomplete interventions and therefore shows limited effectiveness in reducing deep-seated stigma (57). Particularly for online interventions lacking real-time feedback mechanisms, researchers cannot confirm whether participants genuinely adhere strictly to the planned intervention, making reduced engagement more likely to compromise intervention effectiveness. It may also lead to increased loss to follow-up, affecting the accuracy of research outcomes (58). Therefore, in future studies, researchers should attempt to combine both online and offline intervention formats scientifically, integrating the strengths of each approach. It is essential to ensure smooth implementation of the intervention while simultaneously reducing attrition rates during post-intervention follow-ups, thus guaranteeing effective intervention delivery.
6.1.3 Optimize classification of research subjects to promote flexible application of interventions
The manifestations and degrees of stigma vary significantly across different populations. In known RCT studies, interventions among female HIV-infected individuals generally showed better effectiveness, possibly because this population bears a heavier burden of stigma, pays more attention to health issues, actively seeks services, and women are more likely to engage in interventions through family or community relationships. Additionally, programs such as prevention of mother-to-child transmission (PMTCT) often integrate psychological support, enhancing the accessibility of interventions (59, 60). However, the effectiveness of interventions targeting sexual minority groups and drug users is less ideal. Sexual minority groups and drug users may suffer from comorbid mental or psychological disorders, leading to lower acceptance of psychological interventions. Furthermore, these two groups might experience other types of stigma simultaneously, resulting in varying levels of resistance toward interventions and affecting intervention continuity (61, 62). In some studies focusing on adolescent HIV-infected individuals, the psychological development during adolescence is at a unique stage characterized by identity exploration. Their unstable self-esteem and high sensitivity to privacy limit the effectiveness of interventions (63). Therefore, future intervention designs should be based on the characteristics of target populations, conducting more detailed needs analyses according to sources of stigma and personalizing intervention content adjustments, so that intervention strategies can achieve maximum effectiveness for corresponding populations.
6.1.4 Improve the intervention evaluation system, and promote continuous improvement of intervention protocols
Evaluating the effectiveness of stigma interventions helps intervention implementers objectively understand the strengths and weaknesses of these interventions. Over 20 different versions of stigma measurement tools have been used in included studies, most of which were the HIV Stigma Scale (HSS) or its adapted versions. Although these tools have demonstrated reliability and validity to some extent, differences in scale structure, number of items, and scoring methods have led to discrepancies in defining and capturing the concept of “stigma” across studies. For example, some scales focus primarily on internalized stigma while neglecting enacted stigma and externalized stigma, resulting in incomplete evaluation of intervention effects (5). Some scales were adapted for specific regions and therefore lack generalizability (50). Therefore, differences in selected measurement tools may partially obscure the true effectiveness of the interventions. Additionally, previous studies have lacked long-term follow-up investigations, leading to insufficient evaluation of the long-term efficacy of HIV-related stigma interventions. Thus, future research should not only improve the evaluation system for stigma interventions and conduct multidimensional assessments of their effects, but also require researchers to refine intervention protocols based on findings from prior studies and continue conducting multi-center, large-sample, and long-term studies, in order to enhance the effectiveness of stigma interventions among people living with HIV and provide references for stigma interventions among patients with other diseases.
6.2 Limitation
Although this study is based on randomized controlled trials (RCTs) and systematically reviews stigma interventions among people living with HIV globally, it still has certain limitations. First, the included studies show significant heterogeneity in intervention content, theoretical basis, implementation methods, intervention frequency, and follow-up duration, making quantitative synthesis analysis impossible; therefore, only descriptive summaries were conducted, which somewhat limits the precision and generalizability of the findings. Second, although most studies used scales developed from the HIV Stigma Scale (HSS), differences exist across versions in structural design, dimension categorization, and measurement focus, potentially affecting comparability of results across studies. Additionally, this review did not search for grey literature such as conference proceedings, thus carrying a risk of publication bias that might overestimate intervention effects. This study did not conduct a formal methodological quality or bias risk assessment on the included studies. This means that although we systematically report the findings and trends of existing research, we cannot determine whether these findings stem from methodological rigor. The majority of included literature was published in English, and coverage of specific populations such as adolescents, older adult(s), transgender people, and drug users was insufficient, limiting the general applicability of the conclusions.
6.3 Recommendations for future research and clinical practice
In response to the limitations revealed in this study, future research on HIV-related stigma interventions can be improved and deepened in the following directions. First, standardized measurement tools that have undergone cross-cultural validation should be adopted as much as possible to ensure comparability of intervention effects and accurate interpretation of results. Second, greater emphasis should be placed on the rigorous application of theoretical models during intervention design, strengthening the integration of theory and practice to enhance the targeting and scientific rigor of interventions. Furthermore, future studies should conduct detailed needs assessments based on the specific characteristics of target populations (e.g., age, gender, social identity) to develop more personalized intervention approaches. At the same time, hybrid models combining online and offline components should be further explored to balance confidentiality, accessibility, and interactivity of interventions. Finally, increased attention should be given to populations that are currently underrepresented in research, such as older adults, transgender individuals, and drug users, thereby expanding the applicability of interventions and truly achieving widespread and precise reduction of HIV-related stigma.
7 Conclusion
This study, based on the method of scoping review, systematically summarized 39 randomized controlled trials (RCTs) worldwide, and analyzed the content, format, theoretical basis, and effectiveness of interventions targeting HIV-related stigma among people living with HIV. Overall, most interventions were somewhat effective in reducing HIV-related stigma to a certain extent. However, the variability in intervention effects across different populations, intervention formats, and follow-up periods indicates that there is still room for improvement in HIV stigma reduction interventions.
By comparing the intervention measures included in this study, it is found that cognitive-behavioral therapy based intervention measures should be considered a promising model. Moreover, researchers should choose theories that are suitable for different populations and intervene based on them. Adopting standardized measurement tools to standardize the measurement of stigma related to HIV infected individuals; the trial period should be expanded and the follow-up observation period extended to evaluate the sustained effectiveness of the intervention. At the same time, attention should be paid to populations that are currently under covered by research, such as adolescents, the older adult(s), and transgender individuals, and a mixed online and offline intervention model should be explored to adapt intervention measures to more diverse environments and populations, and to improve the universality and accessibility of interventions. Only by continuously optimizing intervention strategies and addressing the limitations of current research can more effective intervention measures be developed to reduce the stigma faced by HIV infected individuals.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MZ: Visualization, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft, Writing – review & editing. HZ: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Writing – original draft, Writing – review & editing. YX: Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. XL: Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. KY: Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. BN: Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. XW: Data curation, Writing – original draft, Software, Investigation, Conceptualization, Methodology.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1655870/full#supplementary-material
References
1. Garratt, A, Muraleetharan, A, Fairhead, C, and Hill, A. Effects of test-and-treat versus PrEP on elimination of HIV transmission: analysis of 24 HIV prevention trials. AIDS (London, England). (2025) 39:1470–75. doi: 10.1097/QAD.000000000000004232
2. Lazarus, JV, Safreed-Harmon, K, Barton, SE, Costagliola, D, Dedes, N, del Amo Valero, J, et al. Beyond viral suppression of HIV – the new quality of life frontier. BMC Med. (2016) 14:94. doi: 10.1186/s12916-016-0640-4
3. Wu, JZZ, Zayts-Spence, O, and Fortune, Z. Conceptualizing mental health stigma in organizational settings: a sociolinguistic perspective. BMC Psychol. (2024) 12:713. doi: 10.1186/s40359-024-02127-4
4. Judgeo, N, and Moalusi, KP. My secret: the social meaning of HIV/AIDS stigma. SAHARA-J J Soc Aspects HIV/AIDS. (2014) 11:76–83. doi: 10.1080/17290376.2014.932302
5. Luoma, JB, Rossi, SL, Sereda, Y, Pavlov, N, Toussova, O, Vetrova, M, et al. An acceptance-based, intersectional stigma coping intervention for people with HIV who inject drugs—a randomized clinical trial. Lancet Regl Health Europe. (2023) 28:100611. doi: 10.1016/j.lanepe.2023.100611
6. Yendewa, GA, Kpaka, RA, Sellu, E, Yendewa, SA, Massaquoi, SPE, Cummings, PE, et al. Perceived and enacted HIV-related stigma in eastern and southern Sierra Leone: a psychometric study of an HIV stigma scale. medRxiv. (2023). doi: 10.1101/2023.07.07.23292152
7. Quinn, DM, and Chaudoir, SR. Living with a concealable stigmatized identity: the impact of anticipated stigma, centrality, salience, and cultural stigma on psychological distress and health. J Pers Soc Psychol. (2009) 97:634–51. doi: 10.1037/a0015815
8. Rao, D, Desmond, M, Andrasik, M, Rasberry, T, Lambert, N, Cohn, SE, et al. Feasibility, acceptability, and preliminary efficacy of the Unity workshop: an internalized stigma reduction intervention for African American women living with HIV. AIDS Patient Care STDs. (2012) 26:614–20. doi: 10.1089/apc.2012.0106
9. Mahajan, AP, Sayles, JN, Patel, VA, Remien, RH, Sawires, SR, Ortiz, DJ, et al. Stigma in the HIV/AIDS epidemic: a review of the literature and recommendations for the way forward. AIDS (London, England). (2008) 22:S67–79. doi: 10.1097/01.aids.0000327438.13291.62
10. Logie, CH, Wang, Y, Lacombe-Duncan, A, Wagner, AC, Kaida, A, Conway, T, et al. HIV-related stigma, racial discrimination, and gender discrimination: pathways to physical and mental health-related quality of life among a national cohort of women living with HIV. Prev Med. (2018) 107:36–44. doi: 10.1016/j.ypmed.2017.12.018
11. Codjoe, L, Barber, S, Ahuja, S, Thornicroft, G, Henderson, C, Lempp, H, et al. Evidence for interventions to promote mental health and reduce stigma in Black faith communities: systematic review. Soc Psychiatry Psychiatr Epidemiol. (2021) 56:895–911. doi: 10.1007/s00127-021-02068-y
12. Kaur, A, Kallakuri, S, Kohrt, BA, Heim, E, Gronholm, PC, Thornicroft, G, et al. Systematic review of interventions to reduce mental health stigma in India. Asian J Psychiatr. (2021) 55:102466. doi: 10.1016/j.ajp.2020.102466
13. Bogart, LM, Barreras, JL, Gonzalez, A, Klein, DJ, Marsh, T, Agniel, D, et al. Pilot randomized controlled trial of an intervention to improve coping with intersectional stigma and medication adherence among HIV-positive Latinx sexual minority men. AIDS Behav. (2020) 25:1647–60. doi: 10.1007/s10461-020-03081-z
14. Vaishnav, M, Javed, A, Gupta, S, Kumar, V, Vaishnav, P, Kumar, A, et al. Stigma towards mental illness in Asian nations and low-and-middle-income countries, and comparison with high-income countries: a literature review and practice implications. Indian J Psychiatry. (2023) 65:995–1011. doi: 10.4103/indianjpsychiatry.indianjpsychiatry_667_23
15. Tricco, AC, Lillie, E, Zarin, W, O’Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
16. Munn, Z, Peters, MDJ, Stern, C, Tufanaru, C, McArthur, A, and Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18:143. doi: 10.1186/s12874-018-0611-x
17. Dow, DE, Mmbaga, BT, Gallis, JA, Turner, EL, Gandhi, M, Cunningham, CK, et al. A group-based mental health intervention for young people living with HIV in Tanzania: results of a pilot individually randomized group treatment trial. BMC Public Health. (2020) 20:1358. doi: 10.1186/s12889-020-09380-3
18. Tshabalala, J, and Visser, M. Developing a cognitive behavioural therapy model to assist women to deal with HIV and stigma.pdf. S Afr J Psychol. (2011) 47:17–28. doi: 10.1177/008124631104100103
19. Walsh, JL, Quinn, KG, Hirshfield, S, John, SA, Algiers, O, Al-Shalby, K, et al. Acceptability, feasibility, and preliminary impact of 4 remotely-delivered interventions for rural older adults living with HIV. AIDS Behav. (2024) 28:1401–14. doi: 10.1007/s10461-023-04227-5
20. Mkumba, L. Evaluating the long-term outcomes of a mental health intervention in Tanzanian youth living with HIV [master’s thesis]. Durham (NC): Duke University (2020).
21. Nabunya, P, Ssewamala, FM, Kizito, S, Mugisha, J, Brathwaite, R, Neilands, TB, et al. Preliminary impact of group-based interventions on stigma, mental health, and treatment adherence among adolescents living with human immunodeficiency virus in Uganda. J Pediatr. (2024) 269:113983. doi: 10.1016/j.jpeds.2024.113983
22. Abbas, Q, Nisa, M, Khan, MU, Anwar, N, Aljhani, S, Ramzan, Z, et al. Brief cognitive behavior therapy for stigmatization, depression, quality of life, social support and adherence to treatment among patients with HIV/AIDS: a randomized control trial. BMC Psychiatry. (2023) 23:539. doi: 10.1186/s12888-023-05013-2
23. Rongkavilit, C, Wang, B, Naar-King, S, Bunupuradah, T, Parsons, JT, Panthong, A, et al. Motivational interviewing targeting risky sex in HIV-positive young Thai men who have sex with men. Arch Sex Behav. (2015) 44:329–40. doi: 10.1007/s10508-014-0274-6
24. Budhwani, H, Robles, G, Starks, TJ, MacDonell, KK, Dinaj, V, and Naar, S. Healthy choices intervention is associated with reductions in stigma among youth living with HIV in the United States (ATN 129). AIDS Behav. (2021) 25:1094–102. doi: 10.1007/s10461-020-03071-1
25. Hickey, MD, Ouma, GB, Mattah, B, Pederson, B, DesLauriers, NR, Mohamed, P, et al. The kanyakla study: randomized controlled trial of a microclinic social network intervention for promoting engagement and retention in HIV care in rural western Kenya. PLoS One. (2021) 16:e0255945. doi: 10.1371/journal.pone.0255945
26. Yigit, I, Modi, RA, Weiser, SD, Johnson, MO, Mugavero, MJ, Turan, JM, et al. Effects of an intervention on internalized HIV-related stigma for individuals newly entering HIV care. AIDS (London, England). (2020) 34:S73–s82. doi: 10.1097/QAD.0000000000002566
27. Williams, LD, van Heerden, A, Friedman, SR, Chibi, B, Rodriguez, WA, and Memela, P. Changes in stigma and social support among participants in a randomized trial of a novel expanded social network-based HIV testing intervention in KwaZulu-Natal, South Africa. AIDS Behav. (2024) 28:2619–29. doi: 10.1007/s10461-024-04379-y
28. Miles, MS, Holditch-Davis, D, Eron, J, Black, BP, Pedersen, C, and Harris, DA. An HIV self-care symptom management intervention for African American mothers. Nurs Res. (2003) 52:350–60. doi: 10.1097/00006199-200311000-00002
29. Musanje, K, Kasujja, R, Camlin, CS, Hooper, N, Hope-Bell, J, Sinclair, DL, et al. Effectiveness of a mindfulness and acceptance-based intervention for improving the mental health of adolescents with HIV in Uganda: an open-label trial. PLoS One. (2024) 19:e0301988. doi: 10.1371/journal.pone.0301988
30. Graff, NR, Hong, C, Guthrie, B, Micheni, M, Chirro, O, Wahome, E, et al. The effect of the Shikamana peer-and-provider intervention on depressive symptoms, alcohol use, and other drug use among gay, bisexual, and other men who have sex with men in Kenya. AIDS Behav. (2023) 27:3053–63. doi: 10.1007/s10461-023-04027-x
31. Nyamathi, A, Ekstrand, M, Salem, BE, Sinha, S, Ganguly, KK, and Leake, B. Impact of Asha intervention on stigma among rural Indian women with AIDS. West J Nurs Res. (2013) 35:867–83. doi: 10.1177/0193945913482050
32. Lifson, AR, Hailemichael, A, Workneh, S, MacLehose, RF, Horvath, KJ, Hilk, R, et al. Impact of community support workers in rural Ethiopia on emotional and psychosocial health of persons living with HIV: results of a three-year randomized community trial. AIDS Behav. (2023) 27:2834–43. doi: 10.1007/s10461-023-04007-1
33. Derose, KP, Palar, K, Then-Paulino, A, Han, B, Armenta, G, Celeste-Villalvir, A, et al. Changes in HIV internalized and experienced stigmas and social support after an urban gardens and peer nutritional counseling intervention among people with HIV and food insecurity in the Dominican Republic. J Acquir Immune Defic Syndr. (2024) 97:55–62. doi: 10.1097/QAI.0000000000003462
34. Willis, N, Milanzi, A, Mawodzeke, M, Dziwa, C, Armstrong, A, Yekeye, I, et al. Effectiveness of community adolescent treatment supporters (CATS) interventions in improving linkage and retention in care, adherence to ART and psychosocial well-being: a randomised trial among adolescents living with HIV in rural Zimbabwe. BMC Public Health. (2019) 19:117. doi: 10.1186/s12889-019-6447-4
35. Singh, RJ, Sarna, A, Schensul, JJ, Mahapatra, B, Ha, T, and Schensul, SL. A multilevel intervention to reduce stigma among alcohol consuming men living with HIV receiving antiretroviral therapy: findings from a randomized control trial in India. AIDS (London, England). (2020) 34:S83–s92. doi: 10.1097/QAD.000000000000002604
36. Psaros, C, Stanton, AM, Raggio, GA, Mosery, N, Goodman, GR, Briggs, ES, et al. Optimizing PMTCT adherence by treating depression in perinatal women with HIV in South Africa: a pilot randomized controlled trial. Int J Behav Med. (2023) 30:62–76. doi: 10.1007/s12529-022-10071-z
37. Nestadt, DF, Saisaengjan, C, McKay, MM, Bunupuradah, T, Pardo, G, Lakhonpon, S, et al. CHAMP+ Thailand: pilot randomized control trial of a family-based psychosocial intervention for perinatally HIV-infected early adolescents. AIDS Patient Care STDs. (2019) 33:227–36. doi: 10.1089/apc.2019.0021
38. Bhatta, DN, and Liabsuetrakul, T. Efficacy of a social self-value empowerment intervention to improve quality of life of HIV infected people receiving antiretroviral treatment in Nepal: a randomized controlled trial. AIDS Behav. (2017) 21:1620–31. doi: 10.1007/s10461-016-1546-z
39. Peltzer, K, Babayigit, S, Rodriguez, VJ, Jean, J, Sifunda, S, and Jones, DL. Effect of a multicomponent behavioural PMTCT cluster randomised controlled trial on HIV stigma reduction among perinatal HIV positive women in Mpumalanga province, South Africa. SAHARA J J Soc Aspects HIV/AIDS Res Alliance. (2018) 15:80–8. doi: 10.1080/17290376.2018.1510787
40. Bogart, LM, Mutchler, MG, Goggin, K, Ghosh-Dastidar, M, Klein, DJ, Saya, U, et al. Randomized controlled trial of rise, a community-based culturally congruent counseling intervention to support antiretroviral therapy adherence among Black/African American adults living with HIV. AIDS Behav. (2023) 27:1573–86. doi: 10.1007/s10461-022-03921-0
41. Echenique, M, Illa, L, Saint-Jean, G, Avellaneda, VB, Sanchez-Martinez, M, and Eisdorfer, C. Impact of a secondary prevention intervention among HIV-positive older women. AIDS Care. (2013) 25:443–6. doi: 10.1080/09540121.2012.712666
42. Kaai, S, Bullock, S, Sarna, A, Chersich, M, Luchters, S, Geibel, S, et al. Perceived stigma among patients receiving antiretroviral treatment: a prospective randomised trial comparing an m-DOT strategy with standard-of-care in Kenya. SAHARA J:J Soc Aspects HIV/AIDS Res Alliance. (2010) 7:62–70. doi: 10.1080/17290376.2010.9724958
43. Odhiambo, JA, Weiser, SD, Frongillo, EA, Burger, RL, Weke, E, Wekesa, P, et al. Comparing the effect of a multisectoral agricultural intervention on HIV-related health outcomes between widowed and married women. Soc Sci Med. (2023) 330:116031. doi: 10.1016/j.socscimed.2023.116031
44. Denison, JA, Burke, VM, Miti, S, Nonyane, BAS, Frimpong, C, Merrill, KG, et al. Project YES! Youth engaging for success: a randomized controlled trial assessing the impact of a clinic-based peer mentoring program on viral suppression, adherence and internalized stigma among HIV-positive youth (15-24 years) in Ndola, Zambia. PLoS One. (2020) 15:e0230703. doi: 10.1371/journal.pone.0230703
45. Phiri, SC, Mudhune, S, Prust, ML, Haimbe, P, Shakwelele, H, Chisenga, T, et al. Impact of the Umoyo mother-infant pair model on HIV-positive mothers’ social support, perceived stigma and 12-month retention of their HIV-exposed infants in PMTCT care: evidence from a cluster randomized controlled trial in Zambia. Trials. (2019) 20:505. doi: 10.1186/s13063-019-3617-8
46. Masquillier, C, Wouters, E, Mortelmans, D, and le Roux Booysen, F. The impact of community support initiatives on the stigma experienced by people living with HIV/AIDS in South Africa. AIDS Behav. (2015) 19:214–26. doi: 10.1007/s10461-014-0865-1
47. Madona, A, Azizah, AN, Nur Khasanah, DJ, Seviani, KF, Aji, DP, and Arifah, I. Effectiveness of Pandang Dengar orang Dengan HIV campaign in reducing HIV stigma among youth in Pati regency, Indonesia. Althea Med J. (2024) 11:3188. doi: 10.15850/amj.v11n2.3188
48. Zhu, M, Cai, W, Li, L, Guo, Y, Monroe-Wise, A, Li, Y, et al. Mediators of intervention effects on depressive symptoms among people living with HIV: secondary analysis of a Mobile health randomized controlled trial using latent growth curve modeling. JMIR Mhealth Uhealth. (2019) 7:e15489. doi: 10.2196/15489
49. Shim, MS, Kim, S, Choi, M, Choi, JY, Park, CG, and Kim, GS. Developing an app-based self-management program for people living with HIV: a randomized controlled pilot study during the COVID-19 pandemic. Sci Rep. (2022) 12:19401. doi: 10.1038/s41598-022-19238-w
50. Rhodes, SD, Tanner, AE, Mann-Jackson, L, Alonzo, J, Song, EY, Smart, BD, et al. Outcomes from a randomized trial of a bilingual mHealth social media intervention to increase care engagement among young gay, bisexual, and other men who have sex with men and transgender women with HIV. Health Educ Behav. (2022) 49:975–84. doi: 10.1177/10901981221125400
51. Bryant, JV, Carcioppolo, N, Lun, D, and Potter, J. Entertainment-education to reduce internalized stigma, increase intimate partner status disclosure intentions, and increase antiretroviral medical adherence intentions: a randomized controlled trial targeting black women living with HIV in the southern U.S. Soc Sci Med. (2023) 327:115945. doi: 10.1016/j.socscimed.2023.115945
52. Barroso, J, Relf, MV, Williams, MS, Arscott, J, Moore, ED, Caiola, C, et al. A randomized controlled trial of the efficacy of a stigma reduction intervention for HIV-infected women in the deep south. AIDS Patient Care STDs. (2014) 28:489–98. doi: 10.1089/apc.2014.0014
53. Van Tam, V, Larsson, M, Pharris, A, Diedrichs, B, Nguyen, HP, Nguyen, CT, et al. Peer support and improved quality of life among persons living with HIV on antiretroviral treatment: a randomised controlled trial from North-Eastern Vietnam. Health Qual Life Outcomes. (2012) 10:53. doi: 10.1186/1477-7525-10-53
54. Qin, K, Zeng, J, Liu, L, and Cai, Y. Effects of cognitive behavioral therapy on improving depressive symptoms and increasing adherence to antiretroviral medication in people with HIV. Front Psychol. (2022) 13:990994. doi: 10.3389/fpsyt.2022.990994
55. Akre, C, Polvinen, J, Ullrich, NJ, and Rich, M. Children’s at home: pilot study assessing dedicated social Media for Parents of adolescents with Neurofibromatosis type 1. J Genet Couns. (2018) 27:505–17. doi: 10.1007/s10897-018-0213-0
56. Molino, ATC, Kriegshauser, KD, and McNamara Thornblade, D. Transitioning from in-person to telehealth cognitive-behavioral therapy for social anxiety disorder during the COVID-19 pandemic: a case study in flexibility in an adverse context. Clin Case Stud. (2022) 21:273–90. doi: 10.1177/15346501211073595
57. Bauermeister, JA, Muessig, KE, LeGrand, S, Flores, DD, Choi, SK, Dong, W, et al. HIV and sexuality stigma reduction through engagement in online forums: results from the HealthMPowerment intervention. AIDS Behav. (2019) 23:742–52. doi: 10.1007/s10461-018-2256-5
58. López-Del-Hoyo, Y, Fernández-Martínez, S, Pérez-Aranda, A, Barceló-Soler, A, Bani, M, Russo, S, et al. Effects of eHealth interventions on stress reduction and mental health promotion in healthcare professionals: a systematic review. J Clin Nurs. (2023) 32:5514–33. doi: 10.1111/jocn.16634
59. Ruegsegger, LM, Stockton, M, Go, VF, Piscalko, H, Davis, D, Hoffman, IF, et al. Stigma, social support, and sexual behavior among female sex Workers at Risk for HIV in Malawi. AIDS Educ Prev. (2021) 33:290–302. doi: 10.1521/aeap.2021.33.4.290
60. Jaspal, R. Stigma and HIV concealment motivation among gay men living with HIV in Finland. J Homosex. (2022) 69:699–715. doi: 10.1080/00918369.2020.1851958
61. Miller, SS, Mantell, JE, Parmley, LE, Musuka, G, Chingombe, I, Mapingure, M, et al. Stigma, social cohesion, and HIV risk among sexual and gender minorities in two cities in Zimbabwe. AIDS Behav. (2022) 26:2994–3007. doi: 10.1007/s10461-022-03622-8
62. Korolenko, TP, Ovchinnikov, AA, Sultanova, AN, Chukhrova, MG, and Sycheva, TY. Dynamics of personality characteristics in the process of psychocorrective intervention in drug addicts. Zh Nevrol Psikhiatr Im S S Korsakova. (2021) 121:53–8. doi: 10.17116/jnevro202112101153
63. Gillette, E, Naanyu, V, Nyandiko, W, Chory, A, Scanlon, M, Aluoch, J, et al. HIV-related stigma shapes research participation for youth living with HIV in Kenya. J Int Assoc Provid AIDS Care. (2023) 22:23259582231170732. doi: 10.1177/23259582231170732
Keywords: HIV, AIDS, stigma, intervention, RCT, scoping review
Citation: Zhang M, Zhu H, Xu Y, Li X, Yang K, Niu B and Wang X (2025) Intervention measures for stigma in HIV patients: a scoping review of randomized controlled trials. Front. Public Health. 13:1655870. doi: 10.3389/fpubh.2025.1655870
Edited by:
Wulf Rössler, Charité University Medicine Berlin, GermanyReviewed by:
Timothy N. Crawford, Wright State University, United StatesZelalem G. Dessie, Bahir Dar University, Ethiopia
Copyright © 2025 Zhang, Zhu, Xu, Li, Yang, Niu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi Xu, Y2RkeHh5MjAyNEAxNjMuY29t
†These authors have contributed equally to this work and share first authorship