 Kuba Sękowski1
Kuba Sękowski1 Agnieszka Mazurek1
Agnieszka Mazurek1 Zuzanna Grześczyk-Nojszewska1
Zuzanna Grześczyk-Nojszewska1 Mateusz Jankowski1Agnieszka Kamińska2Agata Olearczyk3
Mateusz Jankowski1Agnieszka Kamińska2Agata Olearczyk3 Andrzej Silczuk4*
Andrzej Silczuk4* Justyna Grudziąż-Sękowska1
Justyna Grudziąż-Sękowska1- 1School of Public Health, Centre of Postgraduate Medical Education, Warsaw, Poland
- 2Ophthalmology Department, Faculty of Medicine, Collegium Medicum, Cardinal Stefan Wyszyński University in Warsaw, Warsaw, Poland
- 3Health Innovation Unit, SGH Warsaw School of Economics, Warsaw, Poland
- 4Department of Environmental Psychiatry, Faculty of Life Sciences, Medical University of Warsaw, Warsaw, Poland
Introduction: Obesity is a growing public health problem. This study aimed to assess public awareness of obesity causes, complications, and treatment methods in a representative sample of adults in Poland.
Methods: A cross-sectional study was conducted in May 2025 among a representative sample of 1,088 Polish adults using a computer-assisted web interview (CAWI). The structured questionnaire assessed attitudes toward obesity with 10 different questions.
Results: Most respondents (84.8%) correctly identified obesity as a disease. Lifestyle factors—lack of physical activity (82.4%) and unhealthy diet (73.9%)—were the most frequently reported causes. Complications such as type 2 diabetes (81.1%) and hypertension (79.2%) were well recognized, but awareness of conditions like polycystic ovary syndrome (17.3%) and asthma (24.7%) was limited. Increased physical activity (86.9%) and diet (86.7%) were widely acknowledged as treatment methods, while fewer participants recognized pharmacotherapy (34.9%) or bariatric surgery (51.6%). Gender, education, and self-reported economic status significantly (p < 0.05) influenced awareness patterns. In multivariable analysis, female gender was associated with higher recognition of obesity as a disease (aOR: 1.62; 95%CI: 1.15–2.27; p = 0.005), while adults aged 30–39 showed lower recognition (aOR: 0.59; 95%CI: 0.37–0.96; p = 0.04).
Conclusions: There is an urgent need for tailored public health education in Poland that emphasizes the multifactorial nature of obesity, addresses knowledge gaps in treatment options, and reduces social stigma. Strategic interventions must consider demographic and socioeconomic differences to improve population-level obesity literacy and outcomes.
1 Introduction
Obesity is a chronic complex disease characterized by excessive adiposity, which can impair health (1). In the majority of cases, it is considered to be multifactorial (2); however, the etiology is still at least partially unknown (3). Among its causes are obesogenic environments, high-calorie intake, psychological factors, inadequate physical activity, genetic variants, and diseases that affect the endocrine system. As a surrogate marker, BMI is used as a measure of adiposity (1).
From a public health perspective, obesity is now a pandemic and a global public health problem. The prevalence of obesity worldwide has nearly tripled since 1975 (4). In 2022, 12.5% of the world's population, or 890 million people, were obese (5). The prevalence of obesity is highest in the United States and lowest in Sub-Saharan Africa and Southeast Asia (4).
Obesity is also linked to socioeconomic status: in low-income countries, obesity is associated with higher socioeconomic status, while in highly developed countries; it typically correlates with lower socioeconomic status (6). This association is stronger for women than for men (6).
Until recently, obesity therapy included mostly attempts to reduce body weight through diet and physical activity and bariatric surgery. In recent years, the introduction of new drugs to the pharmaceutical market and the expansion of indications for existing drugs to other diseases have significantly increased the role of pharmacotherapy in treating obesity (7, 8). For many patients who did not have the opportunity or were afraid of surgical treatment, it opened up access to therapies that can radically improve their quality of life and functioning in society. In public opinion, this sudden increase in the popularity of treatment is sometimes even referred to as a “fashion” for treating obesity, often perceived very negatively (9).
Efforts are being made worldwide to reduce the incidence of obesity through educational activities, preventive measures, health programs, and appropriate legislative changes. Educational and preventive activities most often include educational classes in schools, cooking workshops, sports classes, and dietary consultations (10, 11). Legislative changes are mainly aimed at reducing demand and limiting the availability of high-calorie, high-sugar, high-fat, and highly processed foods. This is achieved by imposing additional taxes or fees on these products and increasing their prices, which is intended to translate into reduced demand while discouraging corporations from producing them (12).
Obesity prevention is also a key goal of health policies at the international level, including those of the European Union and the WHO, as well as in their plans and recommendations. The EU4 Health Program (13) provides member states with funding for health initiatives and the improvement of healthcare systems, with the overarching goal of reducing cancer incidence. One of the key elements of the program is Europe's Beating Cancer Plan (14), which promotes the reduction of cancer risk factors, with a particular emphasis on obesity and low physical activity. Improving diet and increasing physical activity are among the actions recommended in the program to be implemented from 2021 to 2025.
In 2022, the WHO adopted the Acceleration Plan to Stop Obesity (12), which sets ambitious goals for member states in obesity prevention by indicating specific tasks to be achieved by 2025 and 2030. These goals are essential for the WHO's planned 30% reduction in premature deaths caused by non-communicable diseases by 2030 (15). The objectives include reducing the incidence of obesity among children, adolescents, and adults; decreasing the level of physical inactivity; promoting breastfeeding; increasing the availability of nutrition professionals; and introducing national regulations on advertising food and beverages to children.
Since it has been demonstrated that inequalities in income and educational levels among family members have a significant impact on the risk of overweight and obesity in young children (16, 17), this perspective must also be reflected in the planning of health policies. Such actions are possible, among others, by providing access to free, healthy food in schools and kindergartens, sports activities for seniors or promoting breastfeeding (18).
In the context of Poland, based on data from the Central Statistical Office from 2019 (19) for the population over 15 years of age, approximately 19.5% of men and 17.6% of women have obesity, and 45.6% of men and 31.3% of women are overweight. Over the last 15 years, there has been a consistent increase in the incidence of excess body weight. Obesity in Poland is most common among people over 50 years of age. Obesity and overweight as health problems in Poland began to intensify during the transformation of the political system as a result of dynamic socioeconomic changes and the resulting rapid adaptation to the Western lifestyle. Currently, the most disturbing trend in Poland is the rate of growth of obesity and overweight, especially in the youngest age groups (20).
Evaluating the public knowledge about obesity is an essential element in planning and implementing public policies and public health interventions. Observing changing paradigms about obesity (7, 21) allows, above all, more effective interventions to reduce the incidence and increase the availability and willingness to undertake treatment. Classifying and understanding obesity as a disease entity is necessary to reduce stigmatization and discrimination (2, 22) of people living with obesity and to improve their physical and mental health.
This study aimed to public awareness of obesity causes, complications, and treatment methods in a representative sample of adults in Poland.
2 Material and methods
2.1 Study design and population
This cross-sectional study was conducted in Poland between May 23 and May 26, 2025. A representative sample of the adult population was surveyed using a computer-assisted web interview (CAWI) questionnaire. The survey was administered by the Nationwide Research Panel Ariadna (23), a private research panel provider.
Participants were recruited from a panel of over 100,000 registered individuals. Quota sampling was employed to ensure stratification of the sample by age, sex, and place of residence, based on the demographic characteristics of the general population reported by Statistics Poland (24). Panelists who refused to participate were replaced with individuals from the corresponding stratum to ensure the minimum sample size of 1,000 respondents was met. Only complete responses were collected.
Participation in the survey was voluntary, and all responses were anonymous. Informed consent was obtained from each participant before administering the survey. The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The study protocol was approved by the Ethics Committee at the Center of Postgraduate Medical Education on May 14, 2025 (decision no. 41/2025).
2.2 Measures
The study questionnaire was prepared based on the literature review (3–10). All participants were required to complete a ten-item questionnaire and provide information regarding their height, weight, marital status, household size, number of children, education level, occupational status, and economic status. Height and weight data were used to compute Body Mass Index (BMI) and group respondents into four BMI categories (underweight: < 18.5, healthy weight: ≥18.5 to < 25, overweight: ≥25 to < 30, obesity ≥30) (25). The questionnaire was designed by the authors following a literature review (2–7). Four questions assessed the respondents' knowledge of obesity as a medical condition, and six questions examined their social perception of obesity. Only the questions regarding knowledge were explored in this publication. The remaining questions will be addressed in a subsequent publication.
One question assessed the respondents' recognition of obesity as a disease, with responses recorded on a five-point Likert scale ranging from “definitely yes” to “definitely no.” Responses of “definitely yes” and “rather yes” were aggregated to represent a “yes” response. Three check-all-that-apply questions, each with seven choices, assessed the respondents' knowledge about the causes, complications, and treatment and management of obesity.
A pilot study with 15 adults (general population, non-medical workers) was conducted to verify the questions used in the questionnaire. The study questionnaire was filled out 7 days apart. After this procedure, responses provided twice by the same group of respondents were analyzed, including content validation or stylistic check. One question was removed, two questions were modified, and four multiple-choice answers were revised.
2.3 Statistical analysis
Data analysis was conducted using IBM SPSS v.29 (Armonk, NY, United States). Categorical variables were presented in tables using raw counts and proportions. The associations between the demographic and socioeconomic characteristics of the respondents and their responses were evaluated using the chi-square test of independence. Logistic regression was used to explore the relationship between 10 demographic and socioeconomic independent variables and the recognition of obesity as a disease. Only the variables demonstrating a statistically significant relationship with the outcome in univariable regression were included in the multivariable regression model. The strength of the relationship was quantified using odds ratios (OR) and 95% confidence intervals (95% CI). The p-value of less than 0.05 defines statistical significance.
3 Results
One thousand eighty-eight adults participated in the study. Of those, 54.0% were female. In terms of age distribution, 30.1% were aged 60 years or older, 19.8% were aged 30 to 39, and 19.4% were aged 40 to 49. Over half of the study population was overweight (37.9%) or obese (20.2%). A total of 39.2% of participants were classified as having a healthy weight. A comprehensive summary of the study population's characteristics is presented in Table 1.
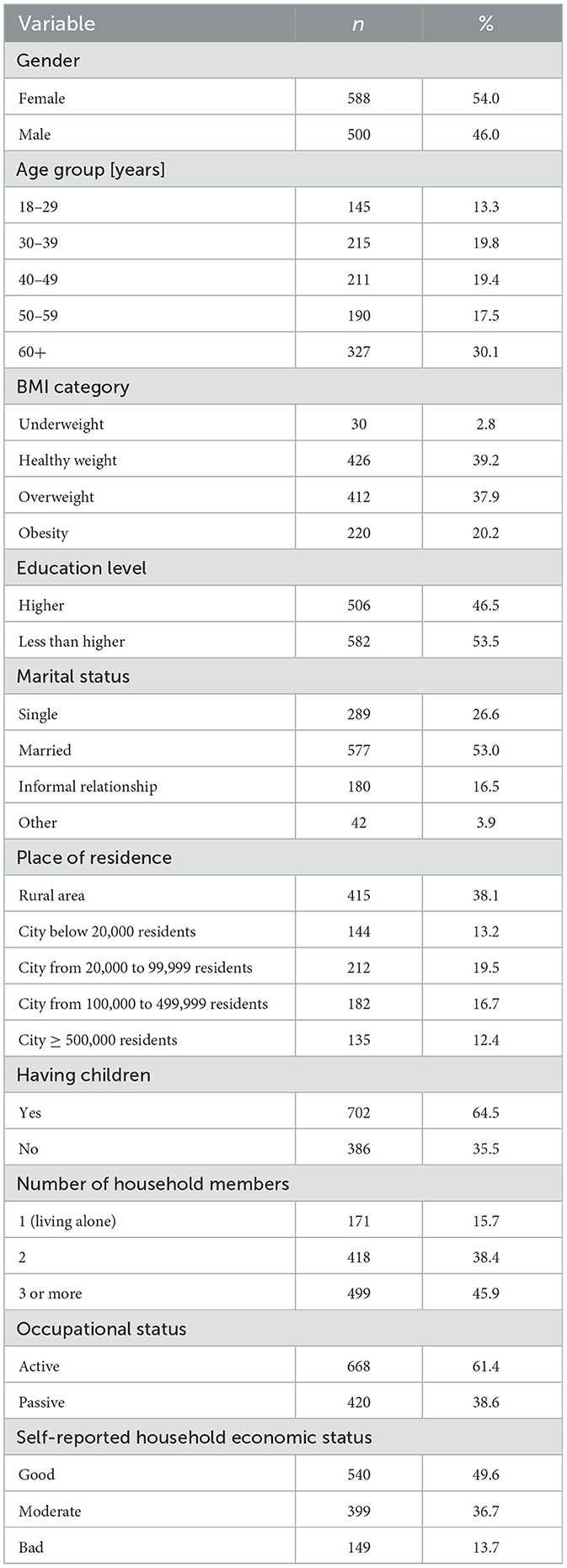
Table 1. Characteristics of the study population (n = 1,088).
3.1 Public knowledge of obesity
The majority of the study participants (“definitely yes”: 42.6% and “rather yes”: 42.2%) correctly identified obesity as a disease (Table 2). The most frequently selected causes of obesity were a lack of physical activity (82.4%), an unbalanced diet (73.9%), hormonal disorders (69.0%), and a genetic predisposition (66.2%) (Table 2). Type 2 diabetes was the most commonly recognized complication of obesity (81.1%). Additionally, 79.2% of respondents were aware that hypertension could result from obesity, and 73.5% understood that heart failure might also be a consequence. Notably, only 24.7% of respondents indicated asthma as a potential complication of obesity, and just 17.3% recognized polycystic ovary syndrome (PCOS) as a possible complication (Table 2). The two most identified methods for managing obesity were increased physical activity (86.9%) and a healthy diet (86.7%). Less than half of the respondents recognized that obesity management could involve psychological or psycho-dietetic interventions (43.1%), and even fewer (36.1%) were aware that regular sleep could be a management strategy. Furthermore, 51.6% of respondents knew that obesity could be treated surgically, while only 34.9% recognized pharmacotherapy as a treatment option (Table 2).

Table 2. Public knowledge of obesity in a representative sample of adults in Poland (n = 1,088).
3.2 Socioeconomic differences in public awareness of causes of obesity
Women, compared to men, more often indicated (p < 0.05) a poorly balanced diet, lack of physical activity, mental disorders or experiencing difficult emotions, lack of time for preparing nutritious meals or physical activity, and hormonal disorders as potential causes of obesity (Table 3). Among the respondents aged 60 and older, lack of physical activity and genetic predisposition were noted as causes of obesity more frequently than in other age groups. However, this age group was the least likely (p < 0.001) to recognize the link between obesity and mental disorders or experience difficult emotions, and lack of time for preparing nutritious meals and engaging in physical activity. In contrast, awareness of these associations was highest (p < 0.001) among the youngest respondents, aged 18 to 29 (Table 3). Awareness of the connection between genetic predisposition and obesity increased with higher BMI categories. Those classified as underweight showed the least awareness, while individuals with obesity showed the highest level of awareness (p = 0.01; Table 3).
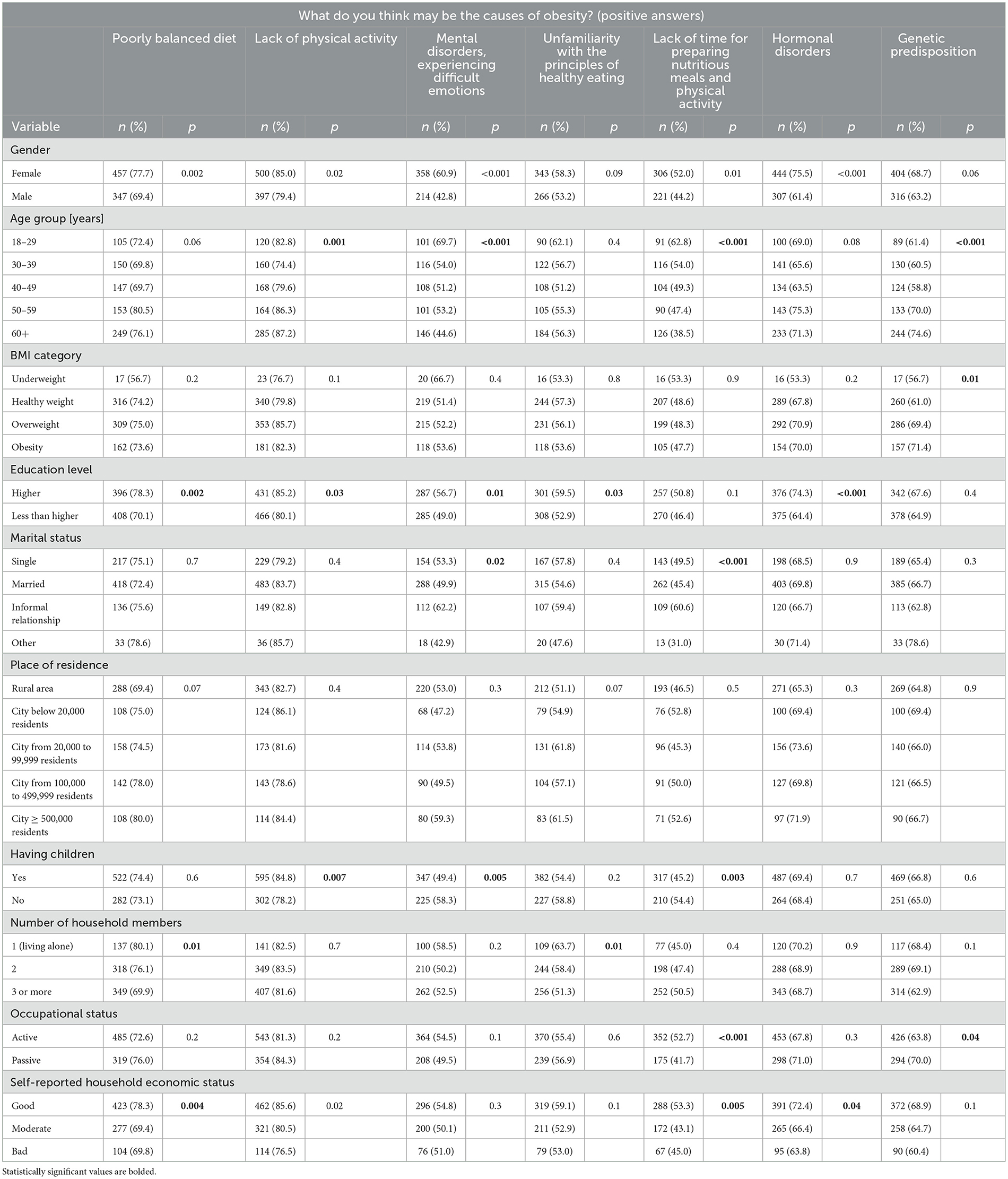
Table 3. Socioeconomic differences in public awareness of causes of obesity in a representative sample of adults in Poland (n = 1,088).
Respondents with higher education were more likely (p < 0.05) than those with less than higher education to recognize a poorly balanced diet, lack of physical activity, mental disorders or experiencing difficult emotions, hormonal disorders, and unfamiliarity with healthy eating principles as factors contributing to obesity (Table 3). Individuals in informal relationships were more likely (p < 0.05) than married and single individuals to attribute obesity to mental disorders or experiencing difficult emotions, and a lack of time for preparing nutritious meals or physical activity as the causes of obesity (Table 3). The same pattern was observed in respondents without children, who were more likely (p < 0.05) to recognize these connections than respondents with children. However, the respondents with children identified a lack of physical activity as a contributing factor to obesity more often (p = 0.007; Table 3). As household size increased, the ability to identify a poorly balanced diet and unfamiliarity with healthy eating principles as causes of obesity decreased (p = 0.01). Specifically, individuals living alone showed the highest awareness of these dietary factors, while those in households of three members or more recognized them the least (Table 3). Occupationally active respondents were less aware (p = 0.04) that genetic predisposition could play a role in the development of obesity than occupationally passive respondents. However, they were more likely (p < 0.001) to associate a lack of time for preparing nutritious meals or physical activity with obesity (Table 3). Respondents with good self-reported household economic status more often (p < 0.05) than those with moderate and bad status indicated a poorly balanced diet, lack of physical activity, lack of time for preparing nutritious meals or physical activity, as well as hormonal disorders as possible causes of obesity (Table 3). There were no significant differences in awareness of causes of obesity by place of residence (Table 3).
3.3 Socioeconomic differences in public awareness of complications of obesity
Women were more likely than men (p < 0.05) to accurately identify nearly all health consequences of obesity, including type 2 diabetes, heart failure, asthma, sleep apnea, and PCOS (Table 4). Among respondents aged 18 to 29, PCOS was recognized more frequently (p < 0.001) compared to other age groups. In contrast, respondents aged 50 to 59 were more likely (p < 0.05) to identify sleep apnea and osteoarthritis than those in different age groups (Table 4). The only significant difference (p < 0.001) in responses by BMI category was for PCOS, with underweight and healthy weight individuals demonstrating greater awareness than the individuals with overweight and obesity (Table 4).
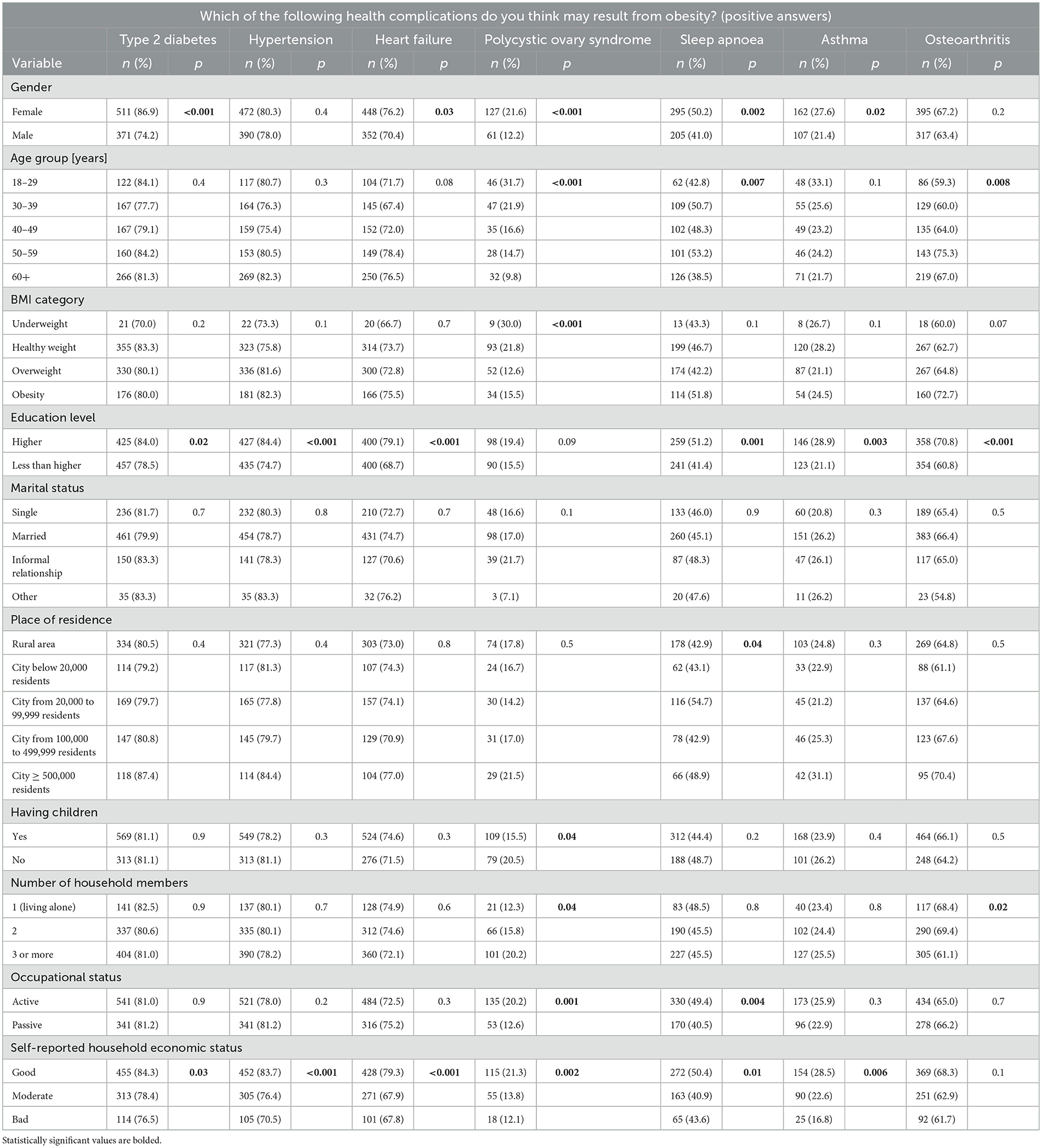
Table 4. Socioeconomic differences in public awareness of health complications associated with obesity in a representative sample of adults in Poland (n = 1,088).
Respondents with higher education showed significantly more awareness (p < 0.05) of type 2 diabetes, hypertension, heart failure, asthma, sleep apnea, and osteoarthritis as possible complications of obesity than those with less than higher education (Table 4). Additionally, there were notable differences in the correct identification of sleep apnea based on place of residence (p = 0.04) and in the recognition of PCOS among individuals with and without children (p = 0.04), with childless individuals showing greater awareness (Table 4). In terms of household size, respondents living with one other person were the most aware (p = 0.02) of the possibility that obesity can cause osteoarthritis. In contrast, respondents in households of three or more members were more likely (p = 0.04) to identify a link between PCOS and obesity compared to individuals in smaller households (Table 4). Respondents with an active occupational status were more aware (p < 0.05) than those with a passive status that obesity could result in PCOS and sleep apnea (Table 4). Significant differences (p < 0.05) were observed in all reported consequences of obesity, except for osteoarthritis, when considering self-reported economic status. Respondents with good financial status demonstrated the most awareness (Table 4). There were no significant differences in the understanding of possible complications of obesity by marital status (Table 4).
3.4 Socioeconomic differences in public awareness of obesity treatment and management
Consistent with findings regarding the causes and consequences of obesity, women also outperformed men (p < 0.05) in correctly identifying the methods available for the treatment and management of obesity, such as increased physical activity, regular sleep, pharmacotherapy, surgical operations, visits to a psychologist or psycho-dietitian, and visits to a dietitian (Table 5). There were also significant differences (p < 0.05) in awareness of those methods across age groups. Specifically, respondents aged 18 to 29 were the most likely to select regular sleep, and a visit to a psychologist or psycho-dietitian as possible treatment and management options. Respondents aged 30 to 39 were the most aware of the possibility of utilizing pharmacotherapy in the treatment of obesity, while those aged 50 to 59 indicated increased physical activity and surgical operations more often than those in other age groups (Table 5). Underweight individuals showed the highest level of awareness (p < 0.05) regarding the utility of visits to a psychologist or psycho-dietitian for obesity management. Conversely, individuals with obesity had the least awareness of this option. However, obese individuals, along with individuals with a healthy weight, were more likely to recognize a visit to a dietitian as a management method compared to underweight and overweight respondents (Table 5).
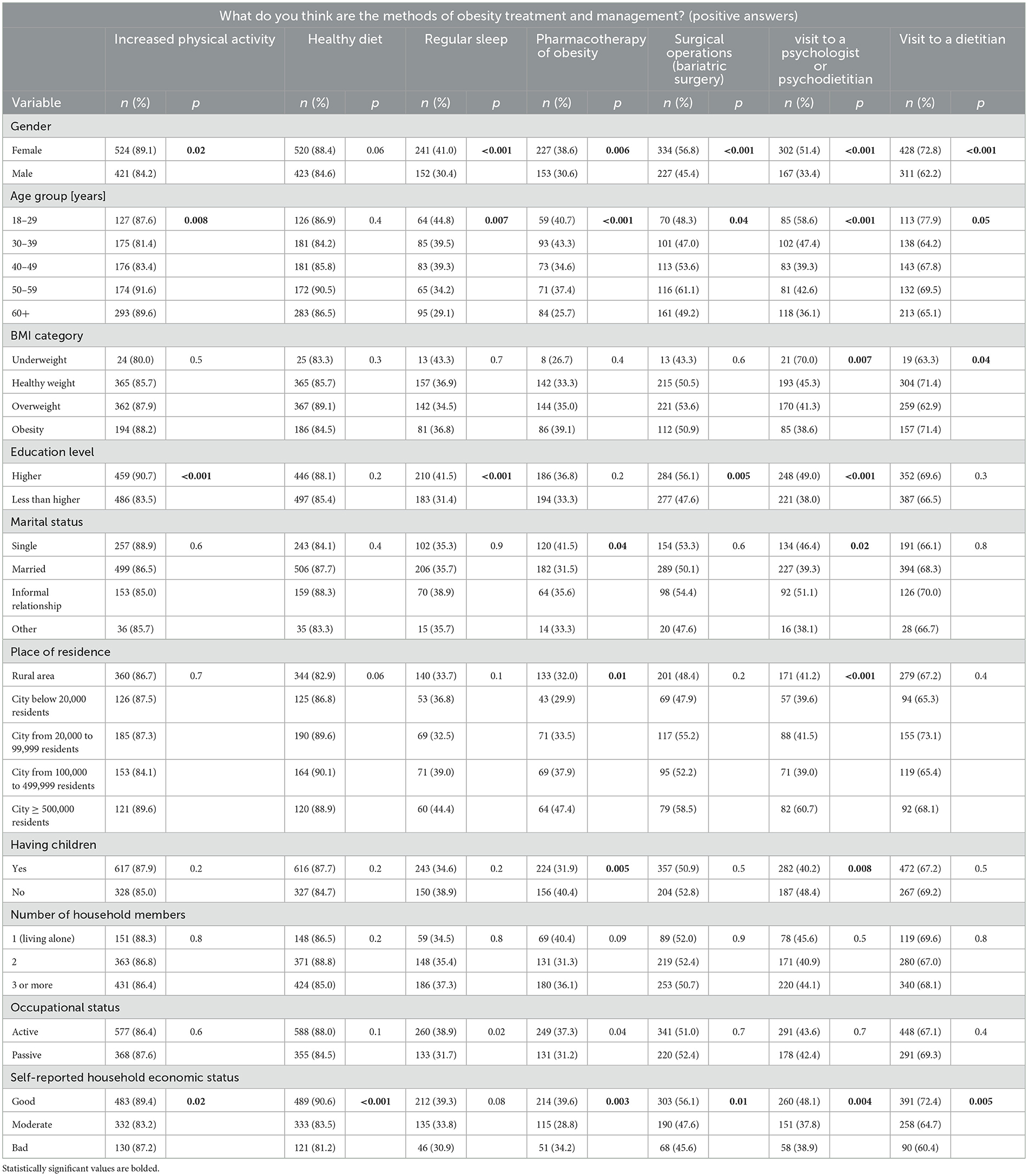
Table 5. Socioeconomic differences in public awareness of obesity treatment and management methods among a representative sample of adults in Poland (n = 1,088).
Respondents with higher education were more likely than those with lower education (p < 0.05) to correctly identify increased physical activity, regular sleep, surgical operations, and visits to a psychologist or psychotherapist as valid treatment and management methods (Table 5). Awareness of the use of pharmacotherapy and visits to a psychologist or psycho-dietitian in the treatment of obesity differed significantly (p < 0.05) according to marital status, having children, and place of residence. Respondents without children or those living in large cities were more aware of these treatment options. Single individuals showed greater awareness of pharmacotherapy, while respondents in informal relationships were more likely to recognize visits to a psychologist or psycho-dietitian as possible obesity management approaches (Table 5). Occupationally active respondents were more likely (p < 0.05) than those with a passive status to indicate pharmacotherapy and regular sleep as possible obesity treatment and management modalities (Table 5). There were significant differences (p < 0.05) in awareness of all treatment and management methods, except regular sleep, based on economic status. Respondents who reported their financial status as good consistently demonstrated greater awareness than those who identified their status as moderate or poor (Table 5). There were no significant differences in awareness of treatment and management methods by household size.
3.5 Socioeconomic factors associated with public awareness of obesity as a disease
In the multivariable logistic regression model (Table 6), only the female gender (aOR: 1.62; 95%CI: 1.15–2.27; p = 0.005) was associated with higher odds of recognizing obesity as a disease. Age 30 to 39 (aOR: 0.59; 95%CI: 0.37–0.96; p = 0.04) was associated with lower odds of recognizing obesity as a disease (Table 6).
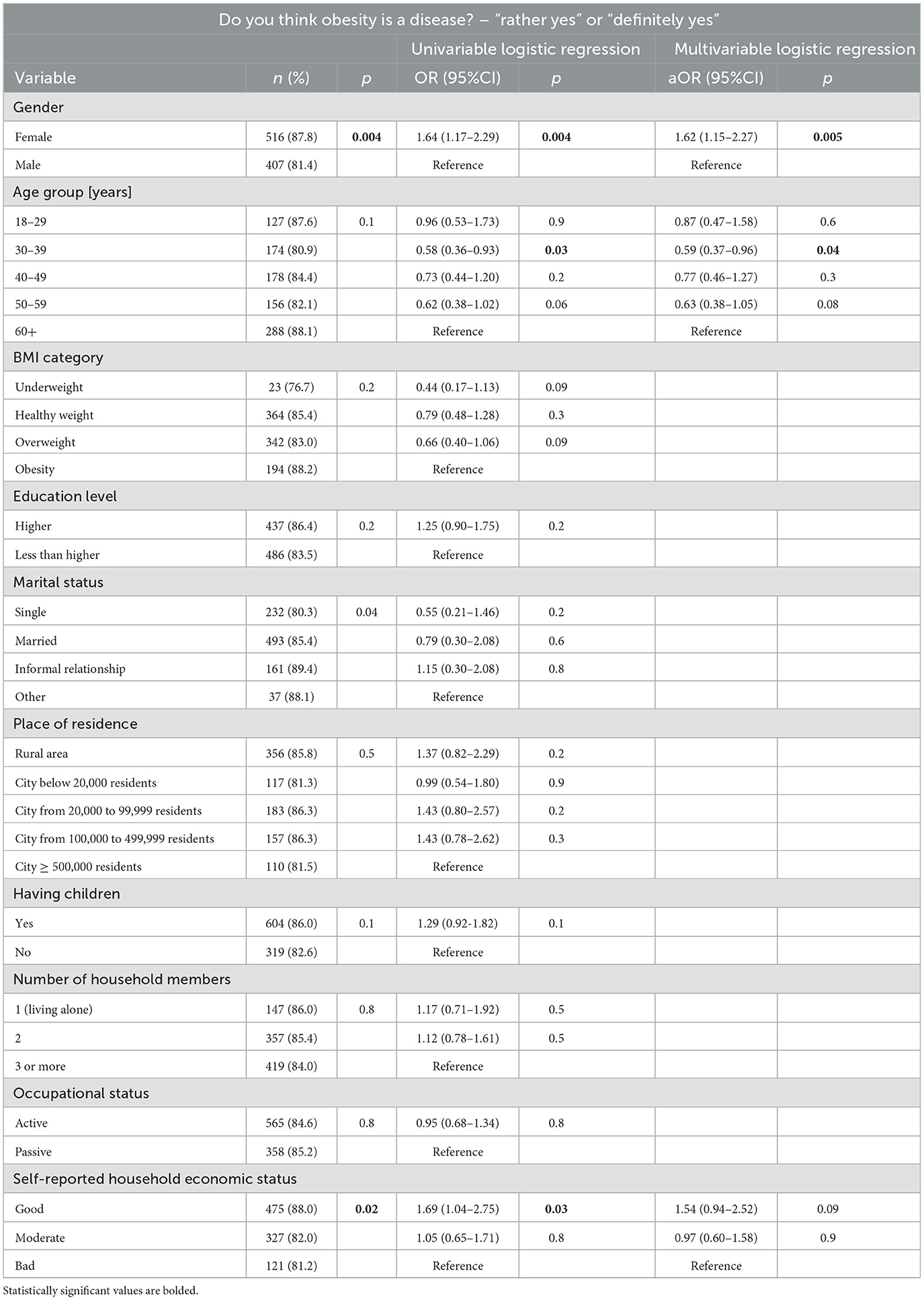
Table 6. Factors associated with public awareness of obesity as a disease in a representative sample of adults in Poland (n = 1,114).
4 Discussion
Recognition of overweight and obesity as a chronic disease remains a contested issue across populations, with significant disparities observed based on gender and age. In the Polish adult population surveyed in this study, 84.8% of respondents acknowledged obesity as a disease, aligning with global trends toward medicalizing obesity. This finding mirrors the shift in clinical and public health narratives as endorsed by the World Health Organization, and reflected in recent definitions by Rubino et al. (2), which classify obesity as a multifactorial, chronic disease affecting physiological, psychological, and metabolic systems. However, not all groups within the study demonstrated equal recognition. Women were significantly more likely than men to perceive obesity as a disease (87.8% vs. 81.4%), while individuals aged 30–39 were the least likely to hold this view (aOR: 0.59; p = 0.04), suggesting lingering resistance among younger adults to framing obesity within a medical paradigm.
Public awareness of the causes of obesity was relatively high, particularly regarding lifestyle-related factors. The most frequently cited causes included lack of physical activity (82.4%) and a poorly balanced diet (73.9%). Yet, there were substantial gaps in the understanding of more complex or less visible determinants such as mental health challenges (52.6%), hormonal disorders (69.0%), and genetic predisposition (66.2%). These trends are consistent with other European data (16) and global findings (26), which point to a bias toward behavioral explanations at the expense of biological and psychosocial ones. This incomplete picture undermines the holistic conceptualization necessary for effective interventions. Notably, younger individuals (aged 18–29) were more aware of psychosocial determinants, whereas the older adult (60+) emphasized genetic and physical activity factors but under-recognized emotional and time-related contributors. This suggests generational shifts in perception, perhaps influenced by newer public discourse on mental health and chronic stress. Similarly, those with higher education levels demonstrated greater recognition of multifactorial causes, reinforcing findings from Autret and Bekelman, who documented a strong correlation between education and obesity literacy (6).
When it comes to awareness of complications, most respondents accurately identified type 2 diabetes (81.1%), hypertension (79.2%), and heart failure (73.5%) as consequences of obesity. However, awareness was significantly lower for conditions like sleep apnea (46.0%), osteoarthritis (65.4%), asthma (24.7%), and PCOS (17.3%)—a finding that aligns with prior reports highlighting the public's limited understanding of obesity's less “visible” or sex-specific health outcomes (27). In particular, women consistently showed higher awareness than men across nearly all complications, and education level again emerged as a critical determinant: respondents with higher education recognized six out of seven complications more frequently than their counterparts. These disparities echo findings from other studies, which emphasize the role of disease conceptualization in clinical understanding and stigma reduction (22, 28).
Awareness of treatment options for obesity varied widely. While lifestyle changes such as physical activity (86.9%) and dietary improvements (86.7%) were commonly identified, only 51.6% acknowledged bariatric surgery, and just 34.9% recognized pharmacotherapy as viable treatments. This is particularly concerning in light of the rapid advancements and increased availability of anti-obesity medications, as highlighted by Müller et al. (8) and Berning et al. (29). Despite the evolving pharmacological landscape, a lack of public education persists, potentially hindered by negative social narratives surrounding medicalized treatment, frequently dismissed as a “fashion” or shortcut (30). Again, women, those with higher education, and individuals from households with better self-reported economic status demonstrated higher levels of awareness across all treatment modalities. Urban respondents and those without children were also more informed about psychological and pharmacological interventions, underscoring access and exposure as likely factors. Low awareness of obesity as a disease and its treatment methods may lead to inadequate obesity management.
The social and economic gradient in obesity awareness was clearly evidenced in the study's findings. Respondents with a good economic status were consistently more knowledgeable about the causes, complications, and treatment methods. Conversely, those with moderate or poor financial conditions scored lower across nearly all indicators. This aligns with broader global evidence indicating that socioeconomic status significantly influences both risk exposure and health literacy (16, 27). Particularly striking is the disconnect in pharmacotherapy awareness between high and low socio-economic groups—a gap that may exacerbate health inequalities as novel treatments become more widespread but remain underutilized in lower-income populations. Furthermore, the place of residence was less influential than expected, suggesting that economic status and education may be more potent drivers of awareness than urban vs. rural divides.
Further studies should focus more deeply on gender stereotypes, educational barriers, and access to healthcare as potential reasons for observed differences in public perception of obesity among adults in Poland. Moreover, studies in high-risk populations are also needed.
Considering these findings, it is crucial to reiterate that the costs of obesity are substantial and have a wide economic impact. In 2019, the impact of overweight and obesity was estimated at 2.19% of GDP globally and projected to grow to 3.29% of GDP by 2060, resulting in 5 million deaths (31). Direct costs of the treatment of obesity (including many comorbidities resulting from the disease in question) rise with increasing BMI (32, 33), reaching 0.7% to 17.8% of the total expenditure on healthcare systems, depending on the country (34). Between 2020 and 2050, the OECD countries were predicted to spend on average 8.4% of their total health budgets on the consequences of obesity (35). Moreover, the indirect costs are much higher and can reach even 80% of societal costs (36).
Therefore, investment in prevention is critical and should involve strong education as a primary intervention. Actions should be taken starting from the youngest age, since the costs of overweight and obesity among children are also rising (37).
4.1 Practical implications
The findings underscore the pressing need for multidimensional educational interventions aimed at enhancing public literacy around obesity, particularly its recognition as a chronic disease and awareness of its less visible complications and evidence-based treatment options. Given the persistent knowledge gaps among certain demographic groups—especially men, individuals with lower educational attainment, and those in poorer economic conditions—targeted campaigns are essential to promote informed decision-making and reduce stigma. Policymakers should prioritize integrating obesity education into national health strategies, with a specific focus on the younger adult population and the socioeconomically disadvantaged, ensuring access to accurate information on modern therapeutic modalities such as pharmacotherapy and psycho-dietetic support. This approach can strengthen population-level prevention efforts and improve the uptake of effective, individualized obesity treatments. New subject “health education” that will be introduced in school in Poland starting from September 2025 should pay particular attention to building awareness on overweight and obesity among school-aged children and adolescents.
4.2 Limitations
This study has several limitations. Firstly, it included only adults who were pre-registered with the research panel and had Internet access, which could restrict the generalizability of the findings to the general population. Additionally, the CAWI methodology is prone to response bias. All data, including anthropometrics, education, and economic status, were self-reported by the study participants and not independently verified by the authors. However, self-reported anthropometrics data are strongly correlated with actual measurements. Furthermore, the study questionnaire was specifically developed by the authors for this study and was therefore not formally validated. Lastly, the study focused solely on the seven most common causes, complications, and treatment and management strategies of obesity, limiting its scope.
5 Conclusions
This study reveals that while the majority of Polish adults recognize obesity as a chronic disease, considerable disparities persist in their awareness of its causes, complications, and treatment methods. Lifestyle-related factors, such as physical inactivity and poor diet, are widely understood; however, knowledge about psychosocial and medical contributors remains insufficient. Similarly, the understanding of obesity-related complications and treatment options, especially pharmacological and psychological interventions, is unevenly distributed across demographic and socioeconomic groups. These findings underscore the urgent need for targeted educational campaigns and health policy interventions that aim to enhance obesity literacy, reduce stigma, and improve access to diverse treatment modalities. Future public health strategies should prioritize comprehensive, equitable approaches that consider the nuanced determinants of health knowledge and behaviors within the population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee at the Centre of Postgraduate Medical Education on May 14, 2025 (decision no. 41/2025). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KS: Conceptualization, Visualization, Project administration, Methodology, Formal analysis, Writing – review & editing, Investigation, Data curation, Writing – original draft. AM: Formal analysis, Methodology, Writing – review & editing, Conceptualization, Writing – original draft. ZG-N: Conceptualization, Methodology, Writing – review & editing, Writing – original draft. MJ: Investigation, Supervision, Writing – review & editing, Methodology, Conceptualization, Writing – original draft, Data curation, Formal analysis. AK: Conceptualization, Writing – review & editing, Formal analysis. AO: Formal analysis, Investigation, Writing – review & editing, Writing – original draft, Conceptualization. AS: Investigation, Writing – review & editing, Formal analysis. JG-S: Methodology, Data curation, Investigation, Writing – review & editing, Visualization, Conceptualization, Formal analysis, Writing – original draft, Project administration.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. ICD-11 for Mortality and Morbidity Statistics (2024). Available online at: https://icd.who.int/browse/2024-01/mms/en#149403041 (Accessed June 30, 2025).
2. Rubino F, Cummings DE, Eckel RH, Cohen RV, Wilding JPH, Brown WA, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. (2025) 13:221–62. doi: 10.1016/S2213-8587(24)00316-4
3. Hanson P, Weickert MO, Barber TM. Obesity: novel and unusual predisposing factors. Ther Adv Endocrinol Metab. (2020) 11:2042018820922018. doi: 10.1177/2042018820922018
4. Bak-Sosnowska M, Białkowska M, Bogdański P, Chomiuk T, Gałazka-Sobotka M, Holecki M, et al. Clinical recommendations for the management of patients with obesity 2022 – position of the polish society for the treatment of obesity. Med Prakt Spec Educ. (2022) 1–87.
5. World Health Organization. One in eight people are now living with obesity. (2024). Available online at: https://www.who.int/news/item/01-03-2024-one-in-eight-people-are-now-living-with-obesity (Accessed June 30, 2025).
6. Autret K, Bekelman TA. Socioeconomic status and obesity. J Endocrine Soc. (2024) 8:bvae176. doi: 10.1210/jendso/bvae176
7. Luli M, Yeo G, Farrell E, Ogden J, Parretti H, Frew E, et al. The implications of defining obesity as a disease: a report from the Association for the Study of Obesity 2021 annual conference. eClinicalMedicine. (2023) 58:101962. doi: 10.1016/j.eclinm.2023.101962
8. Müller TD, Blüher M, Tschöp MH, DiMarchi RD. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov. (2022) 21:201–23. doi: 10.1038/s41573-021-00337-8
9. Podolsky MI, Raquib R, Hempstead K, Stokes AC. Trends in obesity care among US Adults, 2010–2021. Med Care. (2025) 63:234–40. doi: 10.1097/MLR.0000000000002113
10. Callaghan T, Motta M, Stein M, Goidel K. The prevalence and consequences of support for off-label Ozempic prescriptions. Health Econ Policy Law. (2025) 1–14. doi: 10.1017/S1744133124000306
11. WHO Regional Office for Europe. A focus on adolescent physical activity, eating behaviours, weight status and body image in Europe, central Asia and Canada. Health Behaviour in School-aged Children international report from the 2021/2022 survey (2024). Available online at: https://www.who.int/europe/publications/i/item/9789289061056 (Accessed June 30, 2025).
12. World Health Organization. WHO acceleration plan to stop obesity (2023). Available online at: https://www.who.int/publications/i/item/9789240075634 (Accessed June 30, 2025)
13. European Commission. EU4Health programme 2021–2027 – a vision for a healthier European Union. (2024). Available online at: https://health.ec.europa.eu/funding/eu4health-programme-2021-2027-vision-healthier-european-union_en#work-programmes (Accessed June 30, 2025).
14. European Commission. Review of Europe's Beating Cancer Plan (2024). Available online at: https://health.ec.europa.eu/publications/review-europes-beating-cancer-plan_en (Accessed June 30, 2025).
15. World Health Organization. Noncommunicable diseases: Fact sheet (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (Accessed June 30, 2025).
16. WHO Regional Office for Europe. WHO European Regional Obesity Report 2022. Copenhagen. (2022). Available online at: https://iris.who.int/bitstream/handle/10665/353747/9789289057738-eng.pdf?sequence=1 (Accessed June 30, 2025).
17. Liang R. Poverty and childhood obesity: current evidence and future directions. Curr Obes Rep. (2025) 14:1–12. doi: 10.1007/s13679-025-00627-x
18. Sun J, Han J, Jiang X, Ying Y, Li S. Association between breastfeeding duration and BMI, 2009–2018: evidence from NHANES. Front Nutr. (2024) 11:1463089. doi: 10.3389/fnut.2024.1463089
19. Central Statistical Office in Poland. Percentage of people over 15 years of age by body mass index (BMI) (2019). Available online at: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/odsetek-osob-w-wieku-powyzej-15-lat-wedlug-indeksu-masy-ciala-bmi,23,1.html (Accessed June 30, 2025).
20. Kułaga Z, Grajda A, Gurzkowska B, Wojtyło MA, Góźdź M, Litwin MS. The prevalence of overweight and obesity among Polish school- aged children and adolescents. Przegl Epidemiol. (2016) 70:641–51.
21. Brand-Miller J. Challenging the dogma. Int J Obes. (2020) 44:1631–2. doi: 10.1038/s41366-020-0601-z
22. Rathbone JA, Cruwys T, Jetten J, Banas K, Smyth L, Murray K. How conceptualizing obesity as a disease affects beliefs about weight, and associated weight stigma and clinical decision-making in health care. Br J Health Psychol. (2023) 28:291–305. doi: 10.1111/bjhp.12625
23. Nationwide Research Panel Ariadna. Available online at: https://panelariadna.com/ (Accessed June 30, 2025).
24. Główny Urzad Statystyczny (GUS). Demographic Yearbook of Poland 2024 (2024). Available online at: https://stat.gov.pl/en/topics/statistical-yearbooks/statistical-yearbooks/demographic-yearbook-of-poland-2024,3,18.html (Accessed June 30, 2025).
25. Centers for Disease Control and Prevention (CDC). Adult BMI Categories (2024). Available online at: https://www.cdc.gov/bmi/adult-calculator/bmi-categories.html (Accessed June 30, 2025).
26. International Agency for Research on Cancer. Energy balance and obesity: Report of a working group. Lyon: World Health Organization, International Agency for Research on Cancer (2017). Available online at: https://www.iarc.who.int/wp-content/uploads/2018/07/pr253_E.pdf (Accessed June 30, 2025).
27. Kapoor N, Arora S, Kalra S. Gender disparities in people living with obesity - an unchartered territory. J Midlife Health. (2021) 12:103–7. doi: 10.4103/jmh.jmh_48_21
28. Rook ED, Holmes KJ. How language shapes anti-fat bias: comparing the effects of disease and fat-rights framing. Front Commun. (2023) 8:1284074. doi: 10.3389/fcomm.2023.1284074
29. Berning P, Adhikari R, Schroer AE, Jelwan YA, Razavi AC, Blaha MJ, et al. Longitudinal analysis of obesity drug use and public awareness. JAMA Netw Open. (2025) 8:e2457232. doi: 10.1001/jamanetworkopen.2024.57232
30. Makris N, Gkintoni A, Goulas A. Social pharmacology as an underappreciated field in medical education: a single medical school's experience. Med Educ Online. (2021) 26:1–5. doi: 10.3389/fphar.2021.714707
31. Andersson E, Eliasson B, Carlsson KS. Current and future costs of obesity in Sweden. Health Policy. (2022) 126:558–64. doi: 10.1016/j.healthpol.2022.03.010
32. Atella V, Kopinska J, Medea G, Belotti F, Piano Mortari A, Kopinska J, et al. Outpatient healthcare costs associated with overweight and obesity in Italy. BMC Health Serv Res. (2023) 23:619. doi: 10.1186/s12913-023-09576-4
33. Cawley J, Biener A, Meyerhoefer C, Ding Y, Zvenyach T, Smolarz BG, et al. Direct medical costs of obesity in the United States and the most populous states. J Manag Care Spec Pharm. (2021) 27:354–66. doi: 10.18553/jmcp.2021.20410
34. Chew NWS, Ng CH, Tan DJH, Lim WH, Tan B, Lim XY, et al. The global burden of metabolic disease: data from 2000 to 2019. Cell Metab. (2023) 35:414–28.e3. doi: 10.1016/j.cmet.2023.02.003
35. Ling J, Chen S, Zahry NR, Kao TA. Economic burden of childhood overweight and obesity: a systematic review and meta-analysis. Obes Rev. (2023) 24:e13535. doi: 10.1111/obr.13535
36. Nagi MA, Alqarni SSM, Alzahrani SH, Alqarni MA, Alzahrani AM, et al. Economic costs of obesity: a systematic review. Int J Obes. (2024) 48:33–43. doi: 10.1038/s41366-023-01398-y
Keywords: obesity, health literacy, disease awareness, socioeconomic factors, health knowledge, attitudes, diet, lifestyle
Citation: Sękowski K, Mazurek A, Grześczyk-Nojszewska Z, Jankowski M, Kamińska A, Olearczyk A, Silczuk A and Grudziąż-Sękowska J (2025) Public awareness of obesity causes, complications, and treatment methods in a representative sample of adults in Poland. Front. Public Health 13:1656877. doi: 10.3389/fpubh.2025.1656877
Received: 17 July 2025; Accepted: 29 August 2025;
Published: 18 September 2025.
Edited by:
Fatemeh Mohammadi-Nasrabadi, National Nutrition and Food Technology Research Institute, IranReviewed by:
Nasser M. Alorfi, Umm Al Qura University, Saudi ArabiaMaciej Białorudzki, University of Zielona Góra, Poland
Copyright © 2025 Sękowski, Mazurek, Grześczyk-Nojszewska, Jankowski, Kamińska, Olearczyk, Silczuk and Grudziąż-Sękowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrzej Silczuk, YW5kcnplai5zaWxjenVrQHd1bS5lZHUucGw=