 Stinne Glasdam1*†
Stinne Glasdam1*† Hongxuan Xu2†
Hongxuan Xu2† Ruth-Ellen Slåtsveen3†
Ruth-Ellen Slåtsveen3† Christie Stilwell4†Gitte Wind5†
Christie Stilwell4†Gitte Wind5† Ragnhild Julante Andersen Gulestø6†
Ragnhild Julante Andersen Gulestø6† Pier-Luc Turcotte7†
Pier-Luc Turcotte7†- 1Department of Health Sciences, Lund University, Lund, Sweden
- 2Department of Care Science, Malmo universitet, Malmö, Sweden
- 3Centre for Development of Institutional and Home Care Services in Oslo Kommune, Oslo, Norway
- 4Faculty of Health, Dalhousie University, Halifax, NS, Canada
- 5Department of Nursing and Nutrition, Kobenhavns Professionshojskole, Copenhagen, Denmark
- 6Department of Health Sciences, VID Vitenskapelige Hogskole, Oslo, Norway
- 7University of Ottawa, Ottawa, ON, Canada
Background: Ageing-in-place policies have increasingly shifted elder care responsibilities onto family members. Among older cohabiting couples, one’s partner’s illness significantly impacts the other’s daily life and well-being.
Aim: To explore the responsibilities and strategies of caregiving partners in older cohabiting couples from the perspectives of cohabiting caregivers.
Methods: A qualitative systematic literature review was conducted across seven databases, following PRISMA guidelines and registered in PROSPERO (CRD42025632103). Sixty-five studies were included based on predefined inclusion and exclusion criteria using Covidence. Quality was assessed using the Critical Appraisal Skills Programme (CASP) checklist for qualitative studies. Data were synthesised through descriptive numerical summaries and thematic analysis.
Results: The studies, conducted in 20 countries, primarily used individual interviews for data collection. Three overarching themes emerged: (1) strategies directed towards the partner, (2) strategies to maintain personal identity and space, and (3) strategies for navigating formal care systems. Cohabiting caregivers often assumed daily responsibilities despite emotional and physical strain. They relied on both informal and formal support to care for their partner and preserve time for themselves. However, formal care involvement led to issues such as broken agreements and inadequate services.
Conclusion: Older cohabiting caregivers constantly balance and adapt their caregiving roles in relation to their partner, themselves, and formal care providers. This shift in responsibility results in an often invisible, morally-driven labour that remains under-recognised in Ageing-in-place policies. The study highlights the need for policy frameworks and interventions that acknowledge caregivers’ moral labour, enhance the quality of formal care, and support caregiver autonomy.
Clinical trial registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42025632103, identifier (CRD42025632103).
Introduction
Healthcare services are continuously evolving due to advancements in knowledge, changes in the population’s health conditions, and demographic shifts, creating a substantial and continuous influence on global population dynamics (1). As part of this evolving landscape, there is a shift away from institutional care as the conventional standard for older adults and contemporary trends indicate a growing preference for and acknowledgement of older adults’ preference for living at home into advanced age, also called ‘Ageing-in-place’ (1–3). In many western countries, governments have outlined Ageing-in-place policies that shift the responsibility of elder care from health professionals to family members (4–6). Ageing-in-place is generally presented as beneficial for the well-being and autonomy of older adults, given that remaining in familiar surroundings can improve quality of life and foster a sense of security and dignity (7–9). However, it can carry implicit expectations about life at home in old age (10, 11) that shape societal perceptions as to what a ‘good’ life means in old age (12, 13). Hence, concerns have arisen regarding the impact of discourses on successful, active, and healthy ageing on older adults (14), which often impose expectations on how older adults should lead their lives (11, 14) and overlook the fact that old age is not a homogeneous experience (15, 16).
Ageing-in-place policies also have complex implications, particularly as they increasingly rely on partners and other family members to provide necessary support (4, 17, 18, 126). Partners often serve as the primary source of care in later life (19, 20). The interaction between older couples and their environments influences how they experience and adjust to old age at home, creating a dynamic that is personal, social, and physical (21, 22). For instance, research highlights that couples often frame their frailty and health issues differently, depending on their collective outlook and shared memories, as they prepare for future possibilities, including end-of-life (23, 24). While many partners willingly assume caregiving responsibilities, it cannot be assumed that they are all enabled or willing to do so (25). In couples with low quality relationships, partners may not want to provide care (26). In addition, traditional gendered expectations significantly affect caregiving, where providing care for a partner is viewed as a feminine role for the wives rather than husbands (19, 27, 28). However, this is not always the case, as a study from the Netherlands found no gendered differences in the likelihood of older adults to receive care from their partner, rather it was influenced more by other factors such as the partner’s ability to provide care or relationship quality (29).
Frailty in one partner often leads to transformation in the partners’ relationship, where caring becomes integral to everyday life and is influenced by their unique life courses and histories together (30). Older couples frequently adapt to challenges through shared routines and mutual support, relying on long-standing companionship to help maintain each other’s wellbeing (27). Rather than restricting fulfilment, this shift in roles can deepen connection and purpose between partners, challenging assumptions about loss of independence (30–32). Partner caregiving often entails a dual role, as caregivers must also manage their own age-related health challenges (19, 33). This underscores the diverse ageing experiences, with the past and future continuing to shape partners’ care roles (23, 34). While caregiving can be deeply meaningful, it presents distinctive physical, emotional, and social strains, especially as both partners experience the ageing process individually and together. Many older adults depend on their partners for support, whether by choice or financial necessity, creating a unique caregiving dynamic where both partners may confront similar physical or cognitive limitations (22, 27, 28), though to varying extents as one is able to fully or partially care for the other at home.
Recent literature reviews characterise informal caregiving for frail or ill older adults, such as those living with dementia, multimorbidity, or undergoing cancer treatment, as a demanding and often burdensome job (18, 27, 35–39). Caregivers manage daily activities, face a gradual erosion of reciprocity in their relationships, and risk social isolation. At the same time, they are often required to provide instrumental, preventive, and emotional care, frequently at the expense of their own well-being and personal routines. While some studies highlight positive aspects, such as personal growth, enhanced relational closeness, and family cohesion, the literature remains fragmented, particularly regarding how cohabiting partner caregivers understand and manage their responsibilities and sustain caregiving in everyday life. This reveals a significant knowledge gap concerning the everyday practices and strategies of cohabiting caregivers navigating these complex roles. Through a review of the existing literature, this study aims to explore the responsibilities and strategies of the caregiving partners in older couples living at home, from the perspectives of cohabiting older adults.
Method
This study carried out a qualitative systematic review to synthesise insights from qualitative studies, following a method adapted from Bettany-Saltikov and McSherry (40). It is conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (41), and the review protocol is registered with PROSPERO (registration number CRD42025632103).
Identifying the research questions
This review aimed to answer the following three research questions:
(1) What are the well-being and health conditions of cohabiting older adults living at home?
(2) What responsibilities did cohabiting caregivers have for their partner and themselves in daily life?
(3) What strategies did cohabiting caregivers use to make daily life work for themselves and their partner?
Inclusion and exclusion criteria
The inclusion criteria were: (1) Studies about responsibilities and strategies of the caregiving partners in older couples living at home, (2) Perspectives of older cohabiting caregivers and care receivers at home, age 60 + years old, (3) Qualitative studies or qualitative sub-studies in mixed method studies, (4) Published in English, French, or Scandinavian languages, and (5) Published between 1 January 2015–28 January 2025 to align with the latest evidence related to the study’s aim. The review excluded: (1) Systematic literature reviews, (2) Intervention studies, (3) Editorials/commentaries, (4) Dissertations/theses, and (5) Guidelines/recommendations. Old age is defined differently across academic traditions and countries, with thresholds ranging from 50 to 70 years. For this study, we included studies involving adults aged 60 and older, as our preliminary literature search identified this age range as the most used definition.
Searching, selecting, appraising, and extracting relevant data
A search was performed in the PubMed, EMBASE, CINAHL Complete, Eric, SocINDEX, and PsycInfo databases with support from an experienced librarian (Last search: 28 January 2025). Inclusion and exclusion criteria were defined according to the Population, Exposure, and Outcome (PEO) model. The PEO model was selected because it offers a structured approach to framing research questions and organising data, which aligns effectively with qualitative methodologies (40, 42). The search strategy followed the building block approach structured around the PEO model (Table 1).
Table 1. Populations, exposures, and outcomes (PEO).
Search terms within each block were tailored to suit the specific requirements of each database. Details of the search strategies are provided in Table 2.
Table 2. Search strategies.
The initial search yielded 9,404 publications, which were imported into Covidence software for screening. Two authors (SG and HX) jointly conducted the title and abstract selection process, and three authors (SG, HX and RJAG) the full text screening. To identify additional relevant studies beyond those retrieved using the current search strings, a citation pearl search was conducted in the Web of Science database (Last search: 5 March 2025). This process involved two approaches: (1) examining the reference lists of the included articles to identify further relevant publications, and (2) exploring newer publications that cited the included articles to assess their relevance for inclusion in the current literature review. For any disagreements during screening, full-text review, or pearl search, discussions were held with the co-authors until consensus was achieved. If the two authors (SG and HX) disagreed or were in doubt about a publication’s relevance in the initial screening process, the publication was included in the full-text screening. In cases of disagreement during full-text screening, a third author (RJAG) read the articles and a consensus decision was reached. No disagreements remained regarding final inclusion or exclusion, as discussions mainly concerned articles that addressed the study’s aim only partially in their results. Finally, the third author (RJAG) read and assessed all included publications and supported their inclusion. A PRISMA flow diagram (Figure 1) details the study selection process, with the 65 included publications.
Figure 1. PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. Source: Page et al. (41). This work is licensed under CC BY 4.0. To view a copy of this license, visit https://creativecommons.org/licenses/by/4.0/.
The quality of the included publications was evaluated using the Critical Appraisal Skills Program (CASP) qualitative study checklist (43), ensuring the review’s findings were based on credible, high-quality evidence and reflecting a commitment to methodological rigor. Its use was supported by the Cochrane Qualitative and Implementation Methods Group (44). This checklist comprised 10 questions that assess various aspects of the studies, such as their aims, methodology, design, recruitment strategies, data collection, data analysis, findings, and overall research significance, as detailed in Table 3. The quality appraisal aimed to ensure the robustness of the evidence in addressing our research question.
Table 3. Qualitative study appraisal.*
Analytical strategy
The data analysis strategy comprised a descriptive numerical summary analysis, titled ‘Characteristics of the Studies,’ and a reflexive thematic analysis, inspired by Braun and Clarke’s (45) approach. Initially, the publications were read multiple times to ensure thorough familiarisation with the material (45). The following data were extracted by all the authors: (1) Authors, (2) Location, (3) Journal, (4) Study period, (5) Study design, (6) Sample size, (7) Target group and context, (8) Theory/concepts, (9) Results, and (10) Limitations. The focus of data extraction was on the qualitative findings pertinent to the review’s aim and research questions (40). The included studies span a range of contexts and countries, each with distinct cultural and healthcare system characteristics. To manage this diversity, we focused on extracting data relevant across various settings while acknowledging contextual differences. This process was guided by the study’s aim and research questions, and did not require standardized data extraction forms. SG, HX and RJAG verified the extracted data for accuracy and ensured that all relevant results were extracted, and discussed with each other, if they were in doubt. A selection of the extracted data is presented in Table 4.

Table 4. Study characteristics.
The result sections of the publications were initially coded and then reorganised to align with the review’s research questions (45). From these codes, preliminary themes were developed by examining patterns of similarity and difference. Codes with similar meanings were clustered together to form overarching themes. The themes were reviewed and refined through a collaborative process among the authors. This involved multiple iterations, where the themes were revisited alongside the empirical data and research questions to ensure that the themes accurately reflected the data (45). In the final stage, each main theme and its sub-themes were clearly defined, refined, and named. They were thoroughly reviewed to ensure they were both succinct and sufficiently descriptive (45). The resulting themes and subthemes are presented in Figure 2.
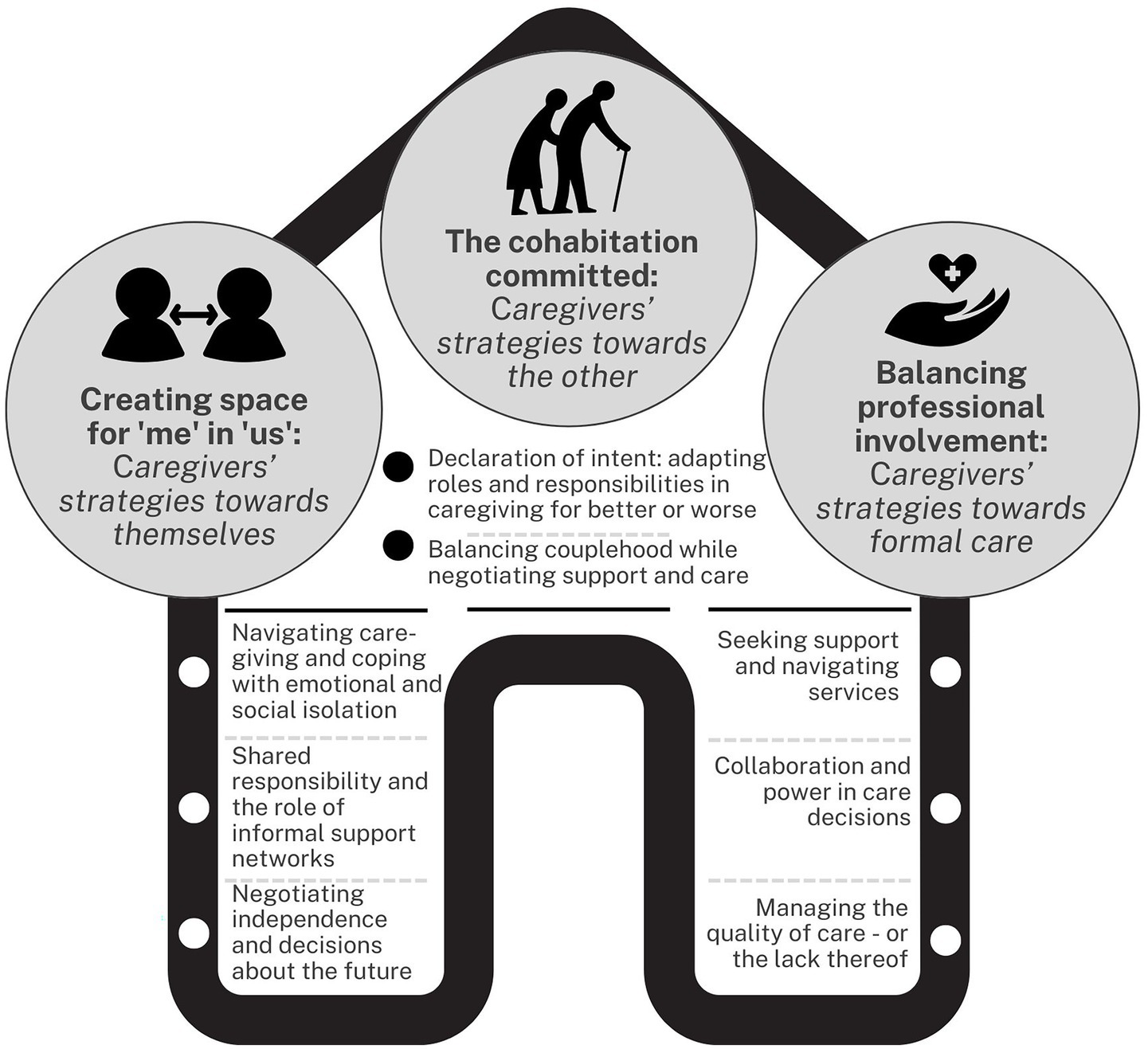
Figure 2. Themes and subthemes.
Results
Characteristics of the studies
The studies were conducted in Sweden (n = 12), United Kingdom (n = 12), Norway (n = 7), China (n = 6), United States of America (n = 5), Canada (n = 4), Australia (n = 3), Finland (n = 3), Iceland (n = 2), Netherlands (n = 2), New Zealand (n = 2), Brazil (n = 1), Iran (n = 1), Ireland (n = 1), Israel (n = 1), Italy (n = 1), Japan (n = 1), Germany (n = 1), Switzerland (n = 1), and Taiwan (n = 1). Almost all studies were conducted in one country, and two studies were conducted in two countries. A total of 1,103 participants took part in the included studies, distributed as 682 cohabiting caregiver partners, 164 older care receiving adults, 175 other relatives, 66 healthcare professionals and 16 stakeholders. All studies used qualitative methods, where most studies (n = 50) used individual interviews, eight studies used focus group interviews, and one study used video recordings. Six studies used both observations and interviews. Ten different analytical methods were used where 26 studies conducted thematic analysis, 12 used content analysis, 11 applied a phenomenological analysis, five used a grounded theory analysis, four applied a hermeneutic phenomenological analysis, two used a hermeneutic analysis, and five used other analytical methods, see Table 4.
The older care receivers were described as living with dementia (n = 31), chronic diseases (n = 14), disabilities (n = 6), and other mixed medical diagnosis (n = 14). Twenty-seven studies focused primarily on older partner caregivers. Ten studies included both the cohabiting caregiver and the care receiver. Nineteen studies included other family members as well as the older partner caregiver and/or the care receivers. Other eight studies also included healthcare personnel. The articles were published in journals with a specific focus on health(care) science (n = 17), dementia (n = 10), gerontology/geriatrics (n = 15), nursing (n = 8), psychiatry or mental health (n = 3), and others (n = 11). The impact factor of the journals ranged from 0.27 to 7.5, see Table 4.
According to the authors’ assessment using the CASP checklist (43), all selected publications demonstrated appropriate methodological rigour (Table 3). Overall, CASP scores ranged between 8/10 and 10/10, and the majority of included studies had scores of 9 or higher (56 studies out of 65), suggesting excellent quality. One common area of limitation was the relationship between researchers and participants (Criterion 6), either unclear or unreported in 28 out of 65 studies, followed by the recruitment strategy (Criterion 4), insufficiently described in six studies (Table 3).
The cohabitation committed—caregivers’ strategies towards the other
Declaration of intent—adapting roles and responsibilities in caregiving for better or worse
Several caregivers described a commitment to fulfil the moral obligation of the partnership whilst adopting a strategy to manage their emotions and feelings, and work on them and change them in alignment with certain ideals and perceived marital expectations (46–55, 127). They revealed shifts in household and care responsibilities following illness or disability, with many cohabiting caregivers commonly experiencing the need to adapt to new roles and expanded duties (46–51, 53, 55–72, 127).
Several cohabiting caregivers found evident shifts in domestic tasks, with caregivers taking over tasks previously managed by their partners, including cooking, grocery shopping, home maintenance, and financial responsibilities (46–51, 53, 55–70, 72, 127). For many male cohabiting caregivers, the traditional gendered divisions of household was altered and they had to learn and perform activities traditionally associated with female roles, however their strategies drew upon using skills as leadership and problem-solving, gained through prior life challenges and work experiences (46, 49–51, 56, 58, 61, 62, 73). In addition to household tasks, many caregivers transitioned into more professional roles, including medication management, monitoring health conditions, assistance with mobility and hygiene, and interactions with health and social care systems (46–51, 53, 55–72, 74–77, 127).
Some caregivers used Information and Communication Technology (ICT) for medical documentation, health tracking apps to help train the memory, and care coordination, acting as experts without necessary support from the health care system (127). Other caregivers described the need for close follow-up to remind their partners to use their assistive technologies such as portable alarms, GPS-tracking, phones and other safety measures (59). Some cohabiting caregivers developed strategies of being present and able to adapt to shifting needs and tailor their support, finding assistive technologies helpful, as they promoted independence (59, 78, 79). However, some caregivers reported that these roles were often accompanied by a lack of familiarity and formal guidance and thus led to uncertainty and confusion (56, 59, 62, 64, 76, 80).
Many caregivers experienced emotional and identity challenges as they adjusted to expanded responsibilities (46–51, 53, 55–65, 67–72, 127). With the progression of illness, caregivers’ responsibilities grew while their personal freedom diminished. Some caregivers linked their current situation to serving a prison sentence (65, 81), or a loss of freedom (60). Cohabiting caregivers and care receivers emphasised the need for constant presence and supervision as key strategies to prevent harm, such as falls or accidents (54, 59, 60, 70, 82–87). However, such responsibility with ongoing presence and supervision often led to emotional exhaustion and a sense of being overburdened among caregivers, especially when care receivers resisted help in an effort to preserve independence (59, 60, 82, 84, 85, 88).
Balancing couplehood while negotiating support and care
Many cohabiting caregivers expressed that caregiving shifted the dynamics of couplehood, which led to their relationships characterised by mutual vulnerability, where both partners beared physical and emotional burdens and uncertainty in face of illness and caregiving (46, 48, 50, 55, 59, 60, 62, 64, 70, 73, 81, 82, 89, 90, 127). They experienced tensions between their roles as being a partner and a caregiver, describing a strategy of taking a more pragmatic and task-oriented approach to the situation and the practicalities that needed to be done (47, 56, 58, 60, 74, 127). Many highlighted the tension between respecting their partner’s independence and the increasing need to intervene for safety and well-being (55, 59, 70, 82, 127).
Caregivers often engaged in emotional work to preserve their partners’ dignity and identity, actively striving to maintain the marital relationship instead of letting illness and dependency completely redefine it (46–48, 50, 53, 55, 57–59, 64, 69, 70, 127). There were examples of caregivers that might balance the act of being a lover and being a caregiver, reminiscing the important and good times, and receiving small verbal and non-verbal gestures seemed to be a coping strategy for the change in the attentiveness of their partner (47, 49, 53, 64, 80, 89). A common strategy mentioned was keeping a positive climate between the partners, avoiding triggering anger or hostility, often by putting their own needs second (48, 57, 59, 91). Doing so seemed to get easier when understanding the disease and its different symptoms and how it affected the person they cared for (59, 70, 86). However, the overwhelming responsibilities sometimes caused caregivers to put their lives on hold to focus on caring for the other, at the expense of their own social and emotional needs (49, 66, 89).
A strategy used by some cohabiting caregivers was to redefine responsibility, viewing their new roles and tasks as a privilege that brought purpose to their changed circumstances and to life more broadly (54, 56, 87, 90). Despite noticeable changes in reciprocity between partners, some caregivers adopted the strategy of focusing on the positive aspects of the relationship during caregiving as a way to cope and support their own well-being (50, 71). However, there seemed to be a diversity in the need for maintaining an active life outside of caregiving, providing pleasure, productivity and restoration while others chose to use their time with the care receiver (69, 82).
Creating space for ‘me’ in ‘us’—caregivers’ strategies towards themselves
Navigating caregiving and coping with emotional and social isolation
Caregivers often paused their own lives to dedicate themselves to caring for the other, at the expense of taking care of their own illnesses and physical ailments (52, 54, 65, 66, 79, 83–86, 90, 92–95) and their own social and emotional needs (49, 66, 89). Loneliness was closely tied to caregivers’ internalised sense of responsibility, often leading to extended isolation and hopelessness, as well as feelings of frustration, resentment, and guilt directed at the care receiving partner (64, 65, 82, 87, 89).
Caregivers employed myriad strategies to reduce loneliness and preserve normalcy, emphasising self-care, meaningful activities, and relationships beyond their caregiving role to support their wellbeing (48, 49, 73, 84, 87, 89, 91, 95). Often this included socialising, engaging in hobbies and activities, and using technology to stay connected. In some cases, pets offered relief from loneliness (89). Many caregivers sought social contact outside of their relationship with friends and family (55, 57, 61, 84, 87, 90, 91, 127), such as caregiver support groups to bond over shared experiences (48, 79, 82). Others carved out time for skill-based classes, outdoor physical activities or leisure/hobbies, or to read or watch television programs on their own (49, 55, 64, 77, 82, 84, 87, 89). Some caregivers found relief in their faith and spirituality (55, 77). Some caregivers even opted to include their partner during activities rather than miss out on the opportunity to participate (73, 78) or found time for themselves by maintaining activities in their partners’ lives by keeping them engaged in enjoyable pastimes despite their declining condition (81).
Use of social technology was also a strategy utilised by caregivers to both get a break from caregiving activities and to socially and emotionally connect with others. It was a way to find new online friendships (127). In some cases, when care recipients spent time on the computer, caregivers could also take a break from caregiving and run errands (127). Social media sites and apps (e.g., Facebook, Instagram) provide opportunities to connect with people in similar caregiving situations (48) and stay in touch with friends and family (93, 127). Some caregivers noted that video calling apps (i.e., Zoom) seemed too impersonal of a platform for sharing their situation (55). Technology such as smartphones and tablets offered a variety of distracting app-based games, some of which had an embedded social element played virtually with others. A shared interest of, e.g., watching boats and the use of a boat information app provided entertainment and connection to beloved pastimes aided by technology during in-person interactions (127).
However, some caregivers adopted emotional distancing or passive endurance as a strategy, or because of a result of a lack of external support (48, 58, 88, 89, 96). In some cases, caregivers became apathetic, stating there was ‘nothing they could do’ or they were ‘fed up’ (88). Loneliness even manifested as a physical pain for some caregivers (89). The overwhelming responsibilities associated with caregiving had some partners wishing for death on themselves (48) or their partners to relieve the suffering of both partners (48, 96). Yet at the same time, caregivers also expressed fear of the loneliness they will feel when their partner dies, which was deemed worse than the burden of caregiving itself (96). Few caregivers opted for divorce (58, 96).
Shared responsibility and the role of informal support networks
Many caregivers adopted a strategy of actively seeking support from family, friends and neighbours to manage their daily lives as caregivers (49, 54, 55, 60, 62, 68, 83, 84, 87, 90, 93, 97, 98). Such support consisted of assisting with household maintenance (98), preparing of food (97), helping with the physical and emotional care of the ill partner (55, 85), emotional support of the cohabiting caregiver (7, 49, 97), and enabling outdoor activities for the cohabiting caregiver (84). The support also consisted of advice and information provision (65, 83, 98). Some caregivers benefitted from having a close family member being a health professional (57), or a retired health worker as neighbours who could address medical complications (97). Others were struggling to find the right information and support (65). The amount of support received from family and friends differed greatly. Cohabiting caregivers recognised factors such as travel distance (84), family obligations, and health issues limited the support they received from family and friends (54). Support from others could ease the cohabiting caregiver’s burden by creating a sense of shared responsibility (60). However, some received little support and had to beg for help (67), while others feared becoming a burden (84). Other cohabiting caregivers first assessed a person’s ability and willingness to provide effective support before asking for help (68). Some caregivers also viewed faith communities as part of their informal support network (98).
Connecting with caregiver support groups was another strategy to manage daily life (48, 55, 59, 68, 70, 79, 81, 82, 87, 97). Caregiver support groups offered help through the sharing of experiences (55, 68, 70, 79, 81, 97), benefitting from knowing other people who were experiencing similar situations (55), easing feelings of guilt and helping to normalise their feelings (48, 59), sharing information (68, 70, 79, 81, 97). Several caregivers were happy to be able to share the information they had compiled (55, 68), giving them a feeling of becoming experts (81). They were more likely to use informal support networks if they could offer social support to others in the same situation encouraging independence and “giving back” rather than dependence (81). However, support groups did not necessarily suit everybody and were described as helpful to a certain point (48). Some cohabiting caregivers got anxious when the amount of information was impossible to digest (87). Other caregivers received support from other people in similar circumstances on the internet if they were not able to leave the house (48). Others again did not have experiences with caregiver support groups but asked for the opportunity to join one (85).
Negotiating Independence and decisions about the future
The utilization of respite care constituted a deliberate strategy by caregivers to manage their caregiving responsibilities, safeguard their own well-being, and facilitate the continued residence of the care recipient in the home environment for as long as feasible (48, 58, 63, 67, 84, 87, 93). Respite care enabled caregivers to complete tasks such as grocery shopping (48) and gardening (58), regaining their energy (93), emotional and physical recovery, engaging in meaningful activities, and maintaining essential social relationships (67). It also offered time to grieve, reflect on life’s changes, and consider future living arrangements (84). Others hesitated to use respite care because they were reluctant to send their partner away from home (87), or feared the emotional consequences of doing so (84, 93).
While the use of respite care represented one aspect of the caregiving strategy, the decision to transition the care recipient to a nursing home was a considerably more consequential and emotionally fraught choice (56, 63, 68, 85, 89, 90, 99), especially when the care recipient refused (85, 89, 99), or when cohabiting caregivers believed that care homes offered inferior care or could even pose a fatal risk to their relative (56). Cohabiting caregivers frequently encountered significant uncertainty regarding the trajectory of the care recipient’s condition and the implications for their own caregiving role (47, 55, 62, 63, 65, 78, 91). This uncertainty often centered on concerns about disease progression (65, 78), the caregiver’s capacity to maintain their responsibilities over time (62, 65, 94), and the anticipated disruption of shared daily life with their partner (47, 63). In response, caregivers employed various strategies to manage the psychological and practical demands of their role. Some engaged in proactive planning, while others adopted a present-focused approach, deliberately avoiding long-term considerations as a means of emotional self-regulation (91). For certain individuals, the recognition of inevitable decline led to a strategic emphasis on the present moment, reflecting a perceived lack of control over future outcomes (80).
Balancing professional involvement—caregivers’ strategies towards formal care
Seeking support and navigating services
Seeking and navigating care services were central and often challenging aspects of life for caregivers in a cohabiting couple. As a result of shifting responsibilities, many caregivers had to be more proactive in identifying and accessing formal support, with home care services playing a key role in sustaining ageing at home (46, 47, 54, 56, 58, 59, 62, 67, 70, 74, 79, 84, 90, 92, 99–102). Other caregivers demonstrated a reluctance to accept public services, reflecting personal preferences and societal expectations of independence (46, 73, 74). Some caregivers found formal care easily accessible (46, 99, 101), but this was not a straightforward process. Some caregivers had to fight for services, switch to new, lower-quality products (e.g., incontinence aids), navigate opaque bureaucratic systems, manage financial matters like reimbursements, and deal with shifting regulations (56, 62, 67, 74, 79, 99–101). Access to formal care was not taken for granted by caregivers, knowing that overuse could affect others’ access or reflect negatively on their caregiving abilities (99). Cultural and linguistic accessibility was also viewed by some caregivers as key to comfort and communication through care navigation (90). In some cases, caregivers described using social leverage, through other family members or appealing to higher authorities, to obtain needed care (101).
While caregivers frequently performed many tasks themselves, formal services like home care support helped with essential activities of daily living, such as dressing, medication adherence or practical challenges, like incontinence (e.g., (49, 54, 69, 79)), which enabled them to attend to their other needs or responsibilities (79, 99). Beyond home care support, caregivers collaborated with other health professionals, including physical and occupational therapists, district nurses, general practitioners, and palliative care nurses (54, 92, 99). Some caregivers also recognised the importance of professional input for their own well-being, expressing a desire for greater involvement of doctors or social workers in addressing issues like loneliness and fatigue (92) and rationalising their life situation (47, 62). In other cases, caregivers were left entirely unsupported, having to beg for help or deal with inexplicable service withdrawals (67). Other caregivers sought alternative treatments through personal research and online purchases when conventional support felt limited (70). While some caregivers found creative ways to engage with services, others struggled with barriers that left them feeling isolated and overwhelmed.
Collaboration and power in care decisions
When balancing their responsibilities, several caregivers asserted their desire to be involved in decision-making (103) and to maintain control over the delivery of care and the cohabiting couples’ daily living (56) while avoiding intrusion in their intimacy and routines (84). However, they often faced challenges in establishing trustful relationships and collaboration with formal care providers (49, 56, 62, 66, 74, 84, 85, 99, 103). Some caregivers described feeling disempowered when formal caregivers dismissed their input and observations (49, 55, 69, 74, 87, 100, 103). Uncertainty about receiving support at a specific time disrupted some caregivers’ daily routines, often leaving those caregivers to resort to carrying out the tasks themselves (84) or to conclude that it would have been simpler without (74). Often, caregivers recognised that most attention by formal care was around the older care recipients, where the needs and responsibilities of caregivers themselves were not recognised or considered; for example, the need for their own daily schedule to be synchronised with the delivery of home care services and caregivers’ well-being (48, 49, 55, 66, 69, 87, 103). When responsibilities became overwhelming (49) or when disease-related complications occurred (85, 103), caregivers recognised the value of formal care (49, 62, 74, 89, 99, 100, 103), especially when the scope of tasks was overwhelming (49) or when they lacked knowledge about disease-related complications (85, 103).
To avoid repeating past suboptimal care experiences (59), some caregivers strove for more control over the care provision as a result of mistrust (59, 61, 74). The presence of formal caregivers might also be experienced as an intrusion in the home, which became a contested space, both physically (e.g., bedrooms) and relationally (56) and re-allocating of rooms (e.g., bedrooms) (86). Some caregivers found this intrusion difficult, to the point of limiting or rejecting formal support, even when needs were extensive (84). In some cases, involvement of formal carers was perceived as a threat to their caregiving role (90), leading to feelings of judgment or exclusion or ‘not fitting in’ (48, 56). In other cases, caregivers viewed the company of the health professionals as a way to reduce their potential loneliness (89, 90). The continuous dialogue with health professionals was essential to adapt strategies when previous ones failed (59, 84). Other caregivers feared being displaced by professionals or other family members, signalling an assertion of their authority within the dyad (74, 104). Struggling between being decision-makers and the ones left behind, caregivers often faced morally conflicting decisions (74), where revealing symptoms, such as aggressive behaviours (48), could unintentionally mean exposing their partner to harm or institutionalisation (104).
From the perspective of some caregivers, building trust with ‘allied’ staff members became a vital strategy for gaining influence, others also relied on private communications with professionals to convince them of their views on the care situation (74). This happened when professionals included family carers as part of the team (99, 105). Many caregivers found that a strong relationship with formal care professionals, marked by mutual recognition of roles, compassionate communication, and information sharing, could improve service responsiveness (62, 103), particularly in urgent situations (99). Such relationships were seen as key to the success of own caregiving strategies (57, 62, 63, 75, 98, 100, 103, 105).
Managing the quality of care—or the lack thereof
Successful collaboration with formal care providers was associated with quality of care when professionals demonstrated competence, continuity and accommodation to the reality of caregivers, offering problem-solving support and social interaction (48, 49, 57, 62, 63, 67, 75, 82, 98, 99). Such collaboration was highly dependent on the invisible labour of informal caregivers, involving advocacy efforts, coordination, and monitoring (49, 55, 74, 86, 101, 105). Some caregivers preferred not to make all decisions (104) and took a more hands-off role (81), mainly monitoring daily care (59).
This invisible labour was applied specifically to fill systemic gaps and failures resulting from under-resourcing and fragmented services (68, 86, 99, 101). Caregivers often described needing to advocate persistently or persuade professionals to adapt care to their lived reality (74). Some caregivers filled in where formal services failed, for example, by providing hands-on care in hospitals (66), preparing for emergencies (105), and coaching professionals (105). In some cases, the trust in professionals was so low that caregivers preemptively trained staff to ensure safe care delivery (105) or preferred doing the care themselves (48, 66). Frequent changes in staff (86) and limited number of home visits (67) as well as inadequate transfer of information (e.g., discharge notes) created burdens for some caregivers who had to ensure care continuity (48, 101). Other resources like respite care were perceived as inconsistent with caregivers’ desire to maintain normalcy and avoid stigmatisation, e.g., being labelled as part of another generational group (57). The act of ‘surrendering’ a partner to others’ care was experienced as both necessary and devastating, fraught with doubt, grief, and the fear of abandonment (104).
Sometimes, caregivers strategically withheld information to steer decisions (74), revealing underlying tensions between the perceived expertise of professionals and caregivers’ intimate knowledge (106). Some caregivers weighed the risk of deteriorating relationships with service providers against the potential benefits of advocating for better care (101). Strategic efforts were deployed to maintain person-centredness in a context of heavy care standardisation (71, 106) and professionalisation (56), which often was translated into levelling down care quality by ignoring individual needs and emotional aspects (48, 71, 85, 101). As such, managing care quality was not just about ensuring appropriate medical treatment; it was an active and often moral engagement with a system that frequently fell short.
Discussion
The discussion focuses on two main findings, namely a role transition from being a partner to being a caregiver and the new responsibilities and strategies associated with it, and how the strategy of involving formal care at home combined practical, moral, and emotional labour of the older cohabiting caregivers to ensure good care for their partner. Furthermore, the method’s strengths and limitations are discussed.
The findings revealed a role transition from being a cohabiting partner to becoming both a partner and a primary caregiver that brought new responsibilities and strategies with it. According to van Gennep (107), a transition process often begins with a phase of separation. This involves a gradual detachment from the familiar, shared identity as equal partners. Typically triggered by the onset of illness, frailty, or disability, the caregiving partner becomes increasingly aware that their relationship is no longer defined solely by mutuality but is now shaped by new roles, responsibilities and dependencies. This stage may be marked by emotional turmoil, including a sense of loss and anticipatory grief, as the couple’s previous balance begins to dissolve and the structures that supported their shared life begin to shift (108, 109). Following separation, van Gennep (107) describes a liminal phase in the transition, which is defined as an ambiguous space characterised by uncertainty and ambivalence. In this state, the individual is no longer simply a partner, but not yet fully identified with the caregiving role, capturing the in-betweenness of this experience. The findings showed how the caregiving partner inhabits a dual role, navigating the emotional demands of intimacy and companionship alongside the practical and moral demands and responsibilities of care. This role is often unstable and fraught with internal tensions. At the same time, they are engaged in an ongoing moral negotiation about what they owe their partner, how much they can realistically give, and how their own needs and well-being fit into the equation. Liminality is not only experienced individually, but can also affect the couple’s shared identity, as they renegotiate what it means to be together in a context of increasing asymmetry (110). Over time, the caregiving partner may reach a stage of incorporation (107), wherein they re-enter the social world with a newly stabilised identity with the development of strategies that work as well as possible for the balance of the partnership and for the individual caregiver partner. At this point, they may begin to self-identify as a caregiver and receive external recognition in that role. This incorporation was, as shown in the findings, reinforced through strategies of social activities, participation in support groups, engagement with health and social services, or adjustments in daily life and routines. However, incorporation is not always a neat or complete process. The nature of long-term caregiving means that roles continue to evolve, and the balance between care and companionship often remains in flux. Even so, as the findings revealed, many caregivers found strategies to integrate elements of their former partnership, such as shared rituals, emotional closeness, or mutual recognition, into this new phase of life, resulting in a layered and complex sense of identity. The shift from partner to caregiver is not merely practical but is a significant social and moral transformation (111). It involves crossing multiple thresholds in terms of identity, relationship, and social status, including changed responsibilities within partnership and the development of new everyday strategies. As the findings pointed out, the transition towards being a caregiver was also a question about the health conditions of the cohabiting caregiver. In many older cohabiting couples, both partners are ill or frail (112, 113). However, the neoliberal governance of care support at home often assumes that the less ill partner can take responsibility and act on behalf of the couple (114). Yet unlike traditional rites of passage, this transition is often unmarked by formal rituals or societal recognition, making it an invisible yet deeply consequential process in the lives of ageing couples, including responsibility and role distribution. Traditional gendered roles typically push women to take on caregiving roles more often than men, and those caring for older adults are less likely to be paid for their labour, which paradoxically restricts their availability for paid work (115). The overlapping roles of caregiving and couplehood leaves little room for self-care, leisure, and even paid work, thereby reinforcing social isolation, marginalisation and undermining health and economic security (116). As it often occurs in private households, informal caregiving remains hidden from policy frameworks or formal systems of support, uncaptured through conventional institutional measurements (117). To better support caregivers in these transitions to older couplehood and ageing-in-place, future studies should explore the rites of passage in older cohabiting couples when life conditions change and new roles and responsibilities emerge.
Furthermore, the findings showed different strategies in which informal caregivers actively engaged with formal care systems to maintain their life at home. Caregivers often walk a thin line between self-reliance and institutional dependency, continually reassessing what is ‘enough,’ ‘acceptable,’ and ‘possible’ in the shifting landscapes of care. As shown in the findings, caregivers frequently described navigating services as a continuous and often burdensome responsibility and strategy. Funk (118) shows that navigation supports remain fragmented and condition-specific, leaving many older adults and caregivers struggling to access care. At political and provider levels, this calls for patient-centred strategies, including improving information, expanding public support, and integrating services (118). The support of home care services, particularly for tasks such as personal hygiene, mobility, and medication management, was acknowledged as essential to sustaining ageing-in-place. However, access to these services was rarely straightforward or reliable. Instead, caregivers were required to become strategic agents, continuously evaluating, combining, and supplementing formal resources to meet complex and evolving care needs. This suggests a form of practical-moral reasoning, wherein carers make judgments not only about what is possible, but about what is right and necessary in their particular circumstances (119). Seeking support is not merely a logistical task; it is an ongoing moral practice shaped by care ethics, social inequalities, emotional strain, and systemic (dis)function, as also shown by Lilleheie et al. (120). For some, accepting help from outside the family represents a failure of moral responsibility or a breach of relational commitment. For others, particularly those navigating progressive care needs, it is a necessary, even urgent, adaptation to protect both themselves and their partners. Care systems require caregivers to become ‘moral entrepreneurs’ (121), who must advocate, argue, and even battle for access to support (122). The findings highlighted that cohabiting caregivers expressed frustration with inconsistent or absent follow-up from services, necessitating a proactive stance just to obtain basic help. This reveals a troubling dynamic. Even when caregivers formally ‘belong’ to the care system, they are expected to demonstrate their worthiness or urgency through persistence, suggesting a system that implicitly delegates responsibility onto the very people it is meant to support (123, 124). At the same time, caregivers’ efforts to navigate and coordinate services also reveal forms of agency, creativity, and resilience. The results suggested that some found ways to integrate different supports, combining formal rehabilitation with respite care or learning techniques from professionals to better manage behavioural symptoms. These practices can be understood as situated acts of moral repair (119) in which caregivers attempt to restore a sense of order and coherence amid fragmented care environments. However, the emotional toll of this work is significant. The burden of constant form-filling, follow-up calls, and struggles for consistency was not only exhausting but demoralising, as shown in the findings. Caregivers sometimes felt ignored or unheard, and when services were subpar, it was experienced not just as a failure of quality, but as a violation of the personhood and dignity of the person cared for. Such failures represent a breach in the moral fabric of care, undermining the trust and mutuality that caregivers strive to uphold. Older cohabiting caregivers operate within care systems that are at once enabling and limiting, requiring them to negotiate ethical tensions between duty, exhaustion, and systemic inadequacy (119). The unevenness of support thus reflects not only structural fragmentation but also a failure to recognise the moral significance of caregivers’ knowledge, efforts, and experiences. This pointed to the need for more responsive, relationally attuned services that do not just provide care, but actively support the moral labour of caregiving itself. These findings call for Ageing-in-place policies that explicitly recognise the invisible, morally-driven labour undertaken by cohabiting caregivers. To ensure the relevance and responsiveness of national and local eldercare strategies, caregivers’ perspectives must be considered in the design and evaluation of care programmes. In addition, it is important that policymakers address issues such as broken agreements and inadequate support by implementing stronger quality assurance mechanisms and accessible complaint procedures, also bridging formal and informal care systems. Future studies about the moral labour of caregiving are needed to understand the contextual and relational complexities in the encounters between informal and formal caregiving when ageing-in-place.
The study’s strengths and limitations
The study has several strengths and limitations. For pragmatic reasons, the results were based on articles that included cohabiting partners aged 60 and above. However, the notion that age can be reduced to a mere number oversimplifies the complexity of human experience, biological diversity, and the social influences that shape the ageing process. Firstly, biological ageing is not uniform. Individuals of the same chronological age can differ significantly in physical health, cognitive function, and overall vitality. Secondly, the social construction of age imposes rigid expectations. Society assigns roles, privileges, and limitations based on chronological age, from birth to death. Yet, these categories are often arbitrary and fail to reflect individual capabilities. Moreover, emotional and psychological ageing do not always align with numerical age depending on the lived lives. Defining a person’s stage of life solely by the number of years lived disregards these nuances. While using age as a numerical measure may be convenient, it is an inadequate and overly simplistic representation of the ageing process (30). As with most literature reviews, it was not possible to cover the full range of conditions experienced in relation to caregiving, with nearly half of our studies focusing on dementia (31 out of 65 studies). Whereas dementia brings complex relational challenges greatly affecting the caregiving experience, this overrepresentation might also be the result of a sampling limitation, where more demanding conditions are more frequently reported than other, less demanding ones. Our qualitative interpretation, combined with the detailed context of each study, supports the transferability of our findings, thus addressing this limitation, and future studies focusing on a broader range of experiences are encouraged.
While our results touched upon the gendered aspects of caregiving, a more explicit focus could have illuminated critical nuances in this review and enriched our interpretations, and these should be addressed in future studies. The review covers studies published between 2015 and 2024, spanning pre- and post-COVID-19 contexts. Although the pandemic likely intensified challenges such as isolation, reduced service access, and increased moral labour, these dynamics were unevenly addressed across studies. Future research could more directly examine how caregiving roles shifted during and after the pandemic. The included studies also span 20 countries with diverse healthcare systems, welfare models, and cultural understandings of family care. Such heterogeneity shapes how caregiving is supported and experienced, for instance, strong formal care infrastructures may ease family responsibilities, whereas family-based systems place greater demands on relatives (125). Cultural norms around gender, ageing, and obligation further influence how moral labour is perceived and enacted. While this diversity enriches the current review, it limits direct transferability of findings. Future research should investigate how systemic and cultural factors mediate caregiving experiences to inform context-sensitive policy and practice. Furthermore, only relevant articles in English were found. It appears that the formal search did not lead to articles in French or Scandinavian languages; even the Pearl Search did not locate such articles. Yet, articles do exist; for example, Vedsegaard and Wind (112). However, many lower-ranked journals are not indexed in the major scholarly databases. In addition, English has become the leading language in academia, the lingua franca (126), which is why most research is published in English-language journals. We used the Web of Science database to ensure the inclusion of newer publications that cited these articles, assessing their relevance for the current literature review. It seems that the initial search was not precise enough, as about a third of the included articles were found through pearl search. One explanation is that articles that did not use the term ‘older adults’ to describe this group of people have been difficult to capture in the search. For example, Aaltonen et al. (74) did not use the term ‘old*’ or ‘older adults’ but used the term ‘people with memory disorders.’ A subsequent review of the articles found through pearl search also reveals that other articles could have been found by adding keywords such as ‘family living’ and/or ‘couplehood’ to the primary searches, e.g., Andréasson et al. (127). However, the first author subsequently discussed the uncaptured articles with the expert university librarian involved, concluding that the extensive pearl search had successfully identified the articles missed in the initial search. Furthermore, the search found a lot of articles related to the aim, but many of the articles did not separate older adults from other caregivers in the results. All articles where it was not possible to distinguish cohabiting older adults (caregivers) from other caregivers were excluded. This means that the results clearly represent this group, but at the same time, additional knowledge about this group may be present in the excluded studies, which could not be differentiated in this literature review.
Conclusion
Focusing on the perspectives of cohabiting older caregivers, the results showed that when transitioning from their roles as partners to that of caregivers, cohabiting older adults transformed the couple’s relationship to enact new responsibilities. Caregivers took responsibility for both their partner and for holding together fragile systems of care. Their work was driven not just by necessity, but by a commitment to sustaining relationships, honouring personhood, and doing what they understood to be ‘the right thing,’ even when systems failed to adequately support them. This pointed to the need for more responsive, relationally attuned services that do not just provide care, but actively support the moral labour of caregiving itself. This also calls for user-involving research and participatory designs within home care, with the aim of supporting the needs of older adult cohabiting couples in a time when political trends advocate for ageing-in-place.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
SG: Supervision, Methodology, Writing – review & editing, Conceptualization, Formal analysis, Writing – original draft, Project administration. HX: Writing – review & editing, Methodology, Writing – original draft, Formal analysis. R-ES: Writing – review & editing, Writing – original draft, Formal analysis. CS: Writing – original draft, Writing – review & editing, Formal analysis. GW: Writing – original draft, Formal analysis, Writing – review & editing. RG: Writing – review & editing, Writing – original draft, Methodology. P-LT: Writing – review & editing, Formal analysis, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors thank Krister Aronsson (Librarian at support for research and learning, Library & ICT, Faculty of Medicine, Lund University) for his dedicated assistance and work in designing and performing the literature searches.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Correction note
A correction has been made to this article. Details can be found at: 10.3389/fpubh.2025.1734743.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. AI was used as a support tool for language translations.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. (2024). Ageing and health. Available online at: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (Accessed September 2, 2025)
2. World Health Organization. (2015). World report on ageing and health. Available online at: https://www.who.int/publications/i/item/9789241565042 (Accessed September 2, 2025)
3. World Health Organization. (2017). Integrated care for older people: guidelines on community-level interventions to manage declines in intrinsic capacity. Available online at: https://www.who.int/publications/i/item/9789241550109 (Accessed September 2, 2025)
4. Gulestø, R, Ågotnes, G, and Glasdam, S. ‘Ageing in place’ in Norway – a Fairclough-inspired discourse analysis of political documents. Health & Place, (2025) 94, 103497 doi: 10.1016/j.healthplace.2025.103497
5. Geerts, J, and Van den Bosch, K. Transitions in formal and informal care utilisation amongst older Europeans: the impact of national contexts. Eur J Ageing. (2011) 9:27–37. doi: 10.1007/s10433-011-0199-z
6. Pavolini, E, and Ranci, C. Restructuring the welfare state: reforms in long-term care in Western European countries. J Eur Soc Policy. (2008) 18:246–59. doi: 10.1177/0958928708091058
7. Pani-Harreman, KE, Bours, GJJW, Zander, I, Kempen, GIJM, and van Duren, JMA. Definitions, key themes and aspects of ‘ageing in place’: a scoping review. Ageing Soc. (2021) 41:2026–59. doi: 10.1017/S0144686X20000094
8. Stones, D, and Gullifer, J. ‘At home it's just so much easier to be yourself’: older adults' perceptions of ageing in place. Ageing Soc. (2016) 36:449–81. doi: 10.1017/S0144686X14001214
9. Tsertsidis, A, Kolkowska, E, and Hedström, K. Factors influencing seniors’ acceptance of technology for ageing in place in the post-implementation stage: a literature review. Int J Med Inform. (2019) 129:324–33. doi: 10.1016/j.ijmedinf.2019.06.027
10. Jacobsen, FF. Understanding public elderly care policy in Norway: a narrative analysis of governmental white papers. J Aging Stud. (2015) 34:199–205. doi: 10.1016/j.jaging.2015.04.006
11. Jacobsen, FF. The imaginaries of home making and home care in public policies In: B Pasveer, O Synnes, and I Moser, editors. Ways of home making in care for later life. Singapore: Springer Nature Singapore Pte Ltd (2020) 85–108. doi: 10.1007/978-981-15-0406-8
12. Glasdam, S, and Jacobsen, FF. Indledning: Livet som ældre i en skandinavisk kontekst [Introduction: Life as an elderly person in a Scandinavian context]. In Glasdam S, Jacobsen FF (Eds.), Gerontologi - Perspektiver på ældre mennesker [Gerontology - Perspectives on older people] Gads Forlag (2018), 9–17.
13. Gibson, K, Kingston, A, McLellan, E, Robinson, L, and Brittain, K. “Successful” ageing in later older age: a sociology of class and ageing in place. Soc Sci Med. (2024) 358:117258. doi: 10.1016/j.socscimed.2024.117258
14. Blix, BH, and Ågotnes, G. Aging successfully in the changing Norwegian welfare state: a policy analysis framed by critical gerontology. Gerontologist. (2023) 63:1228–37. doi: 10.1093/geront/gnac177
15. Pasveer, B, Synnes, O, and Moser, I. Doing home with care in ageing societies In: B Pasveer, O Synnes, and I Moser, editors. Ways of home making in care for later life. London: Palgrave (2020). 1–18.
16. Synnes, O, and Frank, AW. Home as cultural imaginary at the end of life In: B Pasveer, O Synnes, and I Moser, editors. Ways of home making in care for later life. London: Palgrave (2020). 19–40.
17. Gulestø, R, Lillekroken, D, Bjørge, H, and Halvorsrud, L. Interactions between healthcare personnel and family caregivers of people with dementia from minority ethnic backgrounds in home-based care—An explorative qualitative study. Journal of Advanced Nursing, (2022) 78, 1389–1401. doi: 10.1111/jan.15101
18. Plöthner, M, Schmidt, K, de Jong, L, Zeidler, J, and Damm, K. Needs and preferences of informal caregivers regarding outpatient care for the elderly: a systematic literature review. BMC Geriatr. (2019) 19:82. doi: 10.1186/s12877-019-1068-4
19. Bertogg, A, and Strauss, S. Spousal care-giving arrangements in Europe. The role of gender, socio-economic status and the welfare state. Ageing Soc. (2020) 40:735–58. doi: 10.1017/S0144686X18001320
20. Calvó-Perxas, L, Vilalta-Franch, J, Litwin, H, Turró-Garriga, O, Mira, P, and Garre-Olmo, J. What seems to matter in public policy and the health of informal caregivers? A cross-sectional study in 12 European countries. PLoS One. (2018) 13:e0194232–12. doi: 10.1371/journal.pone.0194232
21. Greenwood, N, and Smith, R. The oldest carers: a narrative review and synthesis of the experiences of carers aged over 75 years. Maturitas. (2016) 94:161–72. doi: 10.1016/j.maturitas.2016.10.001
22. Potier, F, Degryse, J-M, Bihin, B, Debacq-Chainiaux, F, Charlet-Renard, C, Martens, H, et al. Health and frailty among older spousal caregivers: an observational cohort study in Belgium. BMC Geriatr. (2018) 18:291. doi: 10.1186/s12877-018-0980-3
23. Bergland, A, and Slettebø, Å. Older women's experience of everyday life in old age: past, present and future. Phys Occup Ther Geriatr. (2018) 36:279–96. doi: 10.1080/02703181.2018.1508169
24. Escourrou, E, Laurent, S, Leroux, J, Oustric, S, and Gardette, V. The shift from old age to very old age: an analysis of the perception of aging among older people. BMC Prim Care. (2022) 23:3. doi: 10.1186/s12875-021-01616-4
25. Cash, B, Hodgkin, S, and Warburton, J. Till death us do part? A critical analysis of obligation and choice for spousal caregivers. J Gerontol Soc Work. (2013) 56:657–74. doi: 10.1080/01634372.2013.823472
26. Lawler, EJ, Thye, SR, and Yoon, J. Social exchange and micro social order. Am Sociol Rev. (2008) 73:519–42. doi: 10.1177/000312240807300401
27. Morgan, T, Bharmal, A, Duschinsky, R, and Barclay, S. Experiences of oldest-old caregivers whose partner is approaching end-of-life: a mixed-method systematic review and narrative synthesis. PLoS One. (2020) 15:e0232401. doi: 10.1371/journal.pone.0232401
28. Wranker, LS, Elmståhl, S, and Cecilia, F. The health of older family caregivers - a 6-year follow-up. J Gerontol Soc Work. (2021) 64:190–207. doi: 10.1080/01634372.2020.1843098
29. Swinkels, JC, Tilburg, TG, and van Groenou, MB. Why do spouses provide personal care? A study among care-receiving Dutch community-dwelling older adults. Health Soc Care Community. (2022) 30:953–61. doi: 10.1111/hsc.13497
30. Bjerkmo, L, Helgesen, AK, Larsen, TA, and Blix, BH. "falling off the wagon": older adults' experiences of living with frailty in rural arctic communities. Int J Circumpolar Health. (2021) 80:1957569–9. doi: 10.1080/22423982.2021.1957569
31. Nicholson, C, Meyer, J, Flatley, M, Holman, C, and Lowton, K. Living on the margin: understanding the experience of living and dying with frailty in old age. Soc Sci Med. (2012) 75:1426–32. doi: 10.1016/j.socscimed.2012.06.011
32. Voie, KS, Blix, BH, Helgesen, AK, Larsen, TA, and Mæhre, KS. Professional home care providers' conceptualisations of frailty in the context of home care: a focus group study. Int J Older People Nursing. (2023) 18:e12511-n/a. doi: 10.1111/opn.12511
33. Smith-Carrier, T, Pham, T-N, Akhtar, S, Seddon, G, Nowaczynski, M, and Sinha, SK. ‘It’s not just the word care, it’s the meaning of the word…(they) actually care': caregivers’ perceptions of home-based primary care in Toronto, Ontario. Ageing Soc. (2018) 38:2019–40. doi: 10.1017/S0144686X1700040X
34. Bjerkmo, L, Helgesen, AK, and Blix, BH. Being and becoming ‘a frail older adult’: meaning-making and resistance through storytelling. J Aging Stud. (2023) 65:101128–8. doi: 10.1016/j.jaging.2023.101128
35. Biran, RMPY, Setyawati, MB, and Siwi, AS. Family caregiver burden of elderly with dementia: a literature review. J Berita Ilm Keperawatan. (2022) 15:93–103. doi: 10.23917/bik.v15i1.17043
36. Donison, V, Toledano, N, Sigal, A, McGilton, KS, Alibhai, SMH, and Puts, M. Care provided by older adult caregivers to a spouse in active cancer treatment: a scoping review. Support Care Cancer. (2022) 30:8679–88. doi: 10.1007/s00520-022-07176-2
37. Egilstrod, B, Ravn, MB, and Petersen, KS. Living with a partner with dementia: a systematic review and thematic synthesis of spouses’ lived experiences of changes in their everyday lives. Aging Ment Health. (2019) 23:541–50. doi: 10.1080/13607863.2018.1433634
38. Steenfeldt, VØ, Aagerup, LC, Jacobsen, AH, and Skjødt, U. Becoming a family caregiver to a person with dementia: a literature review on the needs of family caregivers. SAGE Open Nurs. (2021) 7:23779608211029073. doi: 10.1177/23779608211029073
39. Yu, DSF, Cheng, S-T, and Wang, J. Unravelling positive aspects of caregiving in dementia: an integrative review of research literature. Int J Nurs Stud. (2018) 79:1–26. doi: 10.1016/j.ijnurstu.2017.10.008
40. Bettany-Saltikov, J, and McSherry, R. How to do a systematic literature review in nursing: A step-by-step guide. 2nd ed. Maidenhead: McGraw-Hill Education/Open University Press (2016).
41. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
42. Khan, KS, Kunz, R, Kleijnen, J, and Antes, G. Systematic reviews to support evidence-based medicine: How to review and apply findings of healthcare research. 2nd ed. London: The Royal Society of Medicine Press Limited (2004).
43. Critical Appraisal Skills Program (2018). CASP qualitative checklist. Oxford. Available online at: https://caspuk.net/casp-tools-checklists/ (Accessed September 2, 2025).
44. Long, HA, French, DP, and Brooks, JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. (2020) 1:31–42. doi: 10.1177/2632084320947559
46. Cash, B, Warburton, J, and Hodgkin, S. Expectations of care within marriage for older couples. Australas J Ageing. (2019) 38:E19–24. doi: 10.1111/ajag.12590
47. Clark, S, Prescott, T, and Murphy, G. The lived experiences of dementia in married couple relationships. Dementia. (2019) 18:1727–39. doi: 10.1177/1471301217722034
48. Hammar, LM, Williams, CL, Meranius, MS, and McKee, K. Being “alone” striving for belonging and adaption in a new reality: the experiences of spouse carers of persons with dementia. Dementia. (2021) 20:273–90. doi: 10.1177/1471301219879343
49. Melilla, HS, Sverre, BL, Eilertsen, G, and Tønnessen, S. Narratives of health-promoting experiences by older husbands and wives providing care to their home-dwelling spouses receiving home-care services in Norway. BMC Health Serv Res. (2024) 24:1600. doi: 10.1186/s12913-024-12097-3
50. Merrick, K, Camic, PM, and O’Shaughnessy, M. Couples constructing their experiences of dementia: a relational perspective. Dementia. (2016) 15:34–50. doi: 10.1177/1471301213513029
51. Miller, M, Neiterman, E, Keller, H, and McAiney, C. Being a husband and caregiver: the adjustment of roles when caring for a wife who has dementia. Can J Aging. (2024) 44:68–77. doi: 10.1017/S0714980824000291
52. Olivier, CL, Phillips, J, and Toy, DE. To be or not to be? A caregiver’s question: the lived experience of a stroke family during the first 18 months. Scand J Caring Sci. (2018) 32:270. doi: 10.1111/scs.12458
53. Shiff, HM, Allison, TA, Halim, M, Covinsky, KE, Smith, AK, Barnes, DE, et al. “I aim to fulfill my promise”: dementia caregiving from the perspective of spouses and partners. J Appl Gerontol. (2025) 44:1414–23. doi: 10.1177/07334648241310707
54. Turner, M, Milligan, C, Thomas, C, Brearley, SG, Payne, S, King, C, et al. Caring for a dying spouse at the end of life: “it’s one of the things you volunteer for when you get married”: a qualitative study of the oldest carers’ experiences. Age Ageing. (2016) 45:421–6. doi: 10.1093/ageing/afw047
55. White, DR, and Palmieri, PA. There is ‘no cure for caregiving’: the experience of women caring for husbands living with Parkinson’s disease. Int J Qual Stud Health Well-being. (2024) 19:1989. doi: 10.1080/17482631.2024.2341989
56. Cole, L, Drennan, VM, Manthorpe, J, Hatzidimitriadou, E, and Iliffe, S. Experiences of intimate continence care and the impact on the family dyad relationship for people living at home with dementia and their co-resident family members. Dementia. (2022) 21:1556–73. doi: 10.1177/14713012221076667
57. Hale, L, Mayland, E, Jenkins, M, Buttery, Y, Norris, P, Butler, M, et al. Constructing normalcy in dementia care: Carers’ perceptions of their roles and the supports they need. Gerontologist. (2020) 60:905–15. doi: 10.1093/geront/gnz151
58. Hellström, I, Hakanson, C, Eriksson, H, and Sandberg, J. Development of older men’s caregiving roles for wives with dementia. Scand J Caring Sci. (2017) 31:957–64. doi: 10.1111/scs.12419
59. Häikiö, K, Sagbakken, M, and Rugkåsa, J. Dementia and patient safety in the community: a qualitative study of family carers’ protective practices and implications for services. BMC Health Serv Res. (2019) 19:635. doi: 10.1186/s12913-019-4478-2
60. Jarling, A, Rydström, I, Ernsth-Bravell, M, Nyström, M, and Dalheim-Englund, A-C. A responsibility that never rests – the life situation of a family caregiver to an older person. Scand J Caring Sci. (2020) 34:44–51. doi: 10.1111/scs.12703
61. LaManna, JB, Loerzel, V, and Conner, NE. Lived experiences of older male caregivers: “that was the worst!”. Geriatr Nurs. (2024) 55:277–85. doi: 10.1016/j.gerinurse.2023.12.006
62. Lethin, C, Hallberg, IR, Karlsson, S, and Janlöv, A. Family caregivers’ experiences of formal care when caring for persons with dementia through the process of the disease. Scand J Caring Sci. (2016) 30:526–34. doi: 10.1111/scs.12275
63. Meyer, J, Cullough, JM, and Berggren, I. A phenomenological study of living with a partner affected with dementia. Br J Community Nurs. (2016) 21:24–30. doi: 10.12968/bjcn.2016.21.1.24
64. Musgrave-Takeda, M, Ishibashi, M, and Masaki, H. The experience of being a spouse of a person with dementia in respect to their marital relationship in Japan. Dementia. (2022) 21:2020–34. doi: 10.1177/14713012221107529
65. Papa, R, and Lamura, G. The caregivers’ iceberg: qualitative narratives of Italian caregivers’ roles and challenges. J Gerontol Geriatr. (2019) 67:56–67.
66. Pedreira, LC, Ferreira, AMC, Silva, GTR, Silva, RO d O, and Freitas, CM. Older brazilian caregivers and their lived experiences of caring—a hermeneutic phenomenological study. J Clin Nurs. (2018) 27:3314–23. doi: 10.1111/jocn.14207
67. Riekkola, J, Isaksson, G, Lilja, M, and Rutberg, S. Possibilities and challenges for older couples to continue ageing in place. J Aging Stud. (2024) 69:101229. doi: 10.1016/j.jaging.2024.101229
68. Sadeghi-Mahalli, N, Mohammadi-shahboulaghi, F, Arsalani, N, Fallahi-Khoshknab, M, Foroughan, M, and Atazadeh, M. Getting sincere and efficient support: a grounded theory study of older spousal caregivers of people with Alzheimer's disease. Geriatr Nurs. (2024) 60:511–20. doi: 10.1016/j.gerinurse.2024.10.011
69. Stefánsdóttir, OÁ, Munkejord, MC, and Sveinbjarnardóttir, EK. Maintaining or letting go of couplehood: perspectives of older male spousal dementia caregivers. Scand J Caring Sci. (2022) 36:742–51. doi: 10.1111/scs.13035
70. Tolhurst, E, and Weicht, B. Navigating the impacts of dementia: the experience of male spousal Carers. Healthcare. (2023) 11:2492. doi: 10.3390/healthcare11182492
71. Tyrrell, M, Hillerås, P, Skovdahl, K, Fossum, B, and Religa, D. Voices of spouses living with partners with neuropsychiatric symptoms related to dementia. Dementia. (2019) 18:903–19. doi: 10.1177/1471301217693867
72. Zhang, X, Clarke, CL, and Rhynas, SJ. A thematic analysis of Chinese people with dementia and family caregivers’ experiences of home care in China. Dementia. (2020) 19:2821–35. doi: 10.1177/1471301219861466
73. Rykkje, L, and Tranvåg, O. Caring for one’s wife with dementia—at home: older husbands’ experiences with managing challenges of everyday life. SAGE Open. (2019) 9:4453. doi: 10.1177/2158244019834453
74. Aaltonen, MS, Martin-Matthews, A, Pulkki, JM, Eskola, P, and Jolanki, OH. Experiences of people with memory disorders and their spouse carers on influencing formal care: “they ask my wife questions that they should ask me.”. Dementia. (2021) 20:2307–22. doi: 10.1177/1471301221994300
75. Bendixen, BE, Kirkevold, M, Graue, M, and Haltbakk, J. Experiences of being a family member to an older person with diabetes receiving home care services. Scand J Caring Sci. (2018) 32:805–14. doi: 10.1111/scs.12511
76. Sun, W, Ashtarieh, B, and Zou, P. The safety challenges of therapeutic self-care and informal caregiving in home care: a qualitative descriptive study. Geriatr Nurs. (2021) 42:491–501. doi: 10.1016/j.gerinurse.2020.07.013
77. Yang, C-F, Tseng, C-N, Liao, Y-L, Gao, Z-X, Chen, H-P, Chang, P-C, et al. Experiences of family caregivers providing home care to older patients with cancer: a qualitative study. J Nurs Res. (2023) 31:1–11. doi: 10.1097/jnr.0000000000000579
78. Smith, LJ, and Shaw, RL. Learning to live with Parkinson's disease in the family unit: an interpretative phenomenological analysis of well-being. Med Health Care Philos. (2017) 20:13–21. doi: 10.1007/s11019-016-9716-3
79. Wammes, JD, Labrie, NHM, Agogo, GO, Monin, JK, de Bekker-Grob, EW, and Vroomen, JLM. Persons with dementia and informal caregivers prioritizing care: a mixed-methods study. Alzheimers Dement. (2021) 7:12193. doi: 10.1002/trc2.12193
80. Cooper, RA, and Pitts, MJ. Caregiving spouses’ experiences of relational uncertainty and partner influence in the prolonged relational transition of Alzheimer’s disease and related dementias. J Soc Pers Relat. (2022) 39:1434–59. doi: 10.1177/02654075211058084
81. Donnellan, WJ, Bennett, KM, and Soulsby, LK. What are the factors that facilitate or hinder resilience in older spousal dementia carers? A qualitative study. Aging Ment Health. (2015) 19:932–9. doi: 10.1080/13607863.2014.977771
82. Atler, K, Moravec, A, Seidle, JS, Manns, A, and Stephans, L. Caregivers’ experiences derived from everyday occupations. Phys Occup Ther Geriatr. (2016) 34:71–87. doi: 10.3109/02703181.2015.1120843
83. Cao, S, Huang, H, Zhao, Q, Bo, S, Feng, M, Liang, Y, et al. What influences informal caregivers’ risk perceptions and responses to home care safety of older adults with disabilities: a qualitative study. Front Public Health. (2022) 10:901457. doi: 10.3389/fpubh.2022.901457
84. Carabante, JR, Rutberg, S, Lilja, M, and Isaksson, G. Spousal caregivers’ experiences of participation in everyday life when living in shifting contexts. Scand J Occup Ther. (2019) 25:457–65. doi: 10.1080/11038128.2017.1337810
85. Munkejord, MC, Stefansdottir, OA, and Sveinbjarnardottir, EK. Who cares for the carer? The suffering, struggles and unmet needs of older women caring for husbands living with cognitive decline. Int Pract Dev J. (2020) 10:1–11. doi: 10.19043/ipdj.10Suppl.005
86. Thomas, C, Turner, M, Payne, S, Milligan, C, Brearley, S, Seamark, D, et al. Family carers’ experiences of coping with the deaths of adults in home settings: a narrative analysis of carers’ relevant background worries. Palliat Med. (2018) 32:950–9. doi: 10.1177/0269216318757134
87. Turjamaa, R, Salpakari, J, and Koskinen, L. Experiences of older spousal caregivers for caring a person with a memory disorder. Healthcare. (2020) 8:95. doi: 10.3390/healthcare8020095
88. Abulaiti, B, Zhang, X, Guan, T, Wang, M, Jia, S, and Wang, A. The dyadic care experiences of elderly individuals with disabilities and caregivers in the home setting from the perspective of family resilience: a qualitative study. Front Psychol. (2022) 13:963101. doi: 10.3389/fpsyt.2022.963101
89. Chistell, F, Stängle, S, and Fringer, A. “Loneliness is a monotonous thing”: descriptive qualitative research on the loneliness of caring relatives. BMC Nurs. (2023) 22:1–12. doi: 10.1186/s12912-023-01327-4
90. Horsfall, D, Blignault, I, Perry, A, and Antonopoulos, P. Love stories: understanding the caring journeys of aged Greek-Australian carers. Health Soc Care Community. (2016) 24:194–202. doi: 10.1111/hsc.12206
91. Yang, L, Ye, H, and Sun, Q. Family caregivers’ experiences of interaction with people with mild-to-moderate dementia in China: a qualitative study. Int J Nurs Pract. (2021) 27:e12892–8. doi: 10.1111/ijn.12892
92. Cheng, KM, Zhao, IY, Leung, AYM, Maneze, D, and Holroyd, E. Family caregivers’ perceptions and experiences of supporting older people to cope with loneliness: a qualitative interview study. Int J Ment Health Nurs. (2024) 33:2284–92. doi: 10.1111/inm.13398
93. Riekkola, J, Rutberg, S, Lilja, M, and Isaksson, G. Strategies of older couples to sustain togetherness. J Aging Stud. (2019) 48:60–6. doi: 10.1016/j.jaging.2019.01.005
94. Tatangelo, G, McCabe, M, Macleod, A, and You, E. I just don't focus on my needs. The unmet health needs of partner and offspring caregivers of people with dementia: a qualitative study. Int J Nurs Stud. (2018) 77:8–14. doi: 10.1016/j.ijnurstu.2017.09.011
95. Vos, WH, Boekel, LC, Janssen, MM, Leenders, RTAJ, and Luijkx, KG. Exploring the impact of social network change: experiences of older adults ageing in place. Health Soc Care Community. (2020) 28:116–26. doi: 10.1111/hsc.12846
96. Hochwald, IH, Arieli, D, Radomyslsky, Z, Danon, Y, and Nissanholtz-Gannot, R. Emotion work and feeling rules: coping strategies of family caregivers of people with end stage dementia in Israel—a qualitative study. Dementia. (2022) 21:1154–72. doi: 10.1177/14713012211069732
97. Pickering, J, Crooks, VA, Snyder, J, and Milner, T. Relational, community-based and practical: support systems used by Canadian spousal caregivers living seasonally in the United States. Health Soc Care Community. (2022) 30:2311–9. doi: 10.1111/hsc.13781
98. Read, J, Cable, S, Bartl, G, Löfqvist, C, Iwarsson, S, and Schrag, A. The lived experience of caregiving and perception of service provision among family-caregivers of people with late-stage Parkinson’s: a qualitative study. Parkinsons Dis. (2023) 2023:3517. doi: 10.1155/2023/4483517
99. Compton, RM, Olirus Owilli, A, Caine, V, Berendonk, C, Jouan-Tapp, D, Sommerfeldt, S, et al. Home first: exploring the impact of community-based home care for older adults and their family caregivers. Can J Aging. (2020) 39:432–42. doi: 10.1017/S0714980819000461
100. Greenwood, N, Brearley, S, Smith, R, and Pound, C. A qualitative study of older informal carers’ experiences and perceptions of their caring role. Maturitas. (2019) 124:1–7. doi: 10.1016/j.maturitas.2019.03.006
101. Häikiö, K, Sagbakken, M, and Rugkåsa, J. Family carers’ involvement strategies in response to sub-optimal health services to older adults living with dementia – a qualitative study. BMC Geriatr. (2020) 20:290. doi: 10.1186/s12877-020-01663-z
102. Redley, M, Poland, F, O, RL, and Orrell, M. Supporting a family member with dementia to live at home: the experiences of caregivers. Healthcare. (2025) 13:171. doi: 10.3390/healthcare13020171
103. Guo, P, Zhang, S, Niu, M, Wang, P, Li, L, Wu, C, et al. A qualitative study of the interaction experiences between family caregivers and community nurses for disabled elderly people at home. BMC Geriatr. (2023) 23:243. doi: 10.1186/s12877-023-03917-y
104. Larsson, H, Rämgård, M, Kumlien, C, and Blomqvist, K. Spouses’ existential loneliness when caring for a frail partner late in life - a hermeneutical approach. Int J Qual Stud Health Well-being. (2020) 15:4166. doi: 10.1080/17482631.2020.1734166
105. Schaepe, C, and Ewers, M. “I see myself as part of the team” – family caregivers’ contribution to safety in advanced home care. BMC Nurs. (2018) 17:40–10. doi: 10.1186/s12912-018-0308-9
106. Pejner, MN, and Brobeck, E. Couples in need of home care services: experiences with support from care professionals. Home Health Care Manag Pract. (2018) 30:116–21. doi: 10.1177/1084822318755379
108. Arruda, EH, and Paun, O. Dementia caregiver grief and bereavement: an integrative review. West J Nurs Res. (2017) 39:825–51. doi: 10.1177/0193945916658881
109. Crawley, S, Sampson, EL, Moore, KJ, Kupeli, N, and West, E. Grief in family carers of people living with dementia: a systematic review. Int Psychogeriatr. (2023) 35:477–508. doi: 10.1017/S1041610221002787
110. Hernandez, E, Spencer, B, Ingersoll-Dayton, B, Faber, A, and Ewert, A. “We are a team”: couple identity and memory loss. Dementia. (2019) 18:1166–80. doi: 10.1177/1471301217709604
111. Velasco, HJL, Sanches, RN d C, Radovanovic, CAT, Carreira, L, and Salci, MA. Influences of overload in the spouse of the caregiver of the frail elderly. J Nurs UFPE. (2018) 12:658–64. doi: 10.5205/1981-8963-v12i3a25349p658-664-2018
112. Vedsegaard, H, and Wind, G. Sammen om omsorg og sygdom. Ældre ægtepars hverdagsliv hvor begge er syge [Together in care and illness: The everyday lives of elderly couples where both are ill]. Tidsskrift for Forskning I Sygdom Og Samfund, (2024) 23. doi: 10.7146/tfss.v23i41.141378
113. Korporaal, M, van Groenou, MIB, and van Tilburg, TG. Health problems and marital satisfaction among older couples. J Aging Health. (2013) 25:1279–98. doi: 10.1177/0898264313501387
114. Schwiter, K, Berndt, C, and Truong, J. Neoliberal austerity and the marketisation of elderly care. Soc Cult Geogr. (2015) 19:379–99. doi: 10.1080/14649365.2015.1059473
115. Patterson, SE, Agree, EM, Birditt, K, Truskinovsky, Y, and Freedman, VA. A perspective on making "invisible" care visible through time use data. J Aging Soc Policy. (2025) 1–16:1–16. doi: 10.1080/08959420.2025.2528587
116. Lerner, D. (2022). Invisible overtime: What employers need to know about caregivers. Americus, Georgia (GA): Rosalynn Carter Institute for Caregivers. Available online at: https://rosalynncarter.org/wp-content/uploads/2022/03/Invisible-Overtime-White-Paper.pdf (Accessed September 2, 2025)
117. Okamura, T, Ura, C, Kugimiya, Y, Okamura, M, Yamamura, M, Okado, H, et al. Inaccessibility, unresponsiveness, inconsistency, and invisibility of informal caregivers of older persons with cognitive impairment: community-based participatory research. BMC Geriatr. (2023) 23:812. doi: 10.1186/s12877-023-04542-5
118. Funk, LM. Relieving the burden of navigating health and social Services for Older Adults and Caregivers. IRPP study 73. Montreal: Institute for Research on Public Policy (2019).
120. Lilleheie, I, Debesay, J, Bye, A, and Bergland, A. Informal caregivers' views on the quality of healthcare services provided to older patients aged 80 or more in the hospital and 30 days after discharge. BMC Geriatr. (2020) 20:97. doi: 10.1186/s12877-020-1488-1
121. Freidson, E. Profession of medicine: A study of the sociology of applied knowledge. Chicago: University of Chicago Press (1988).
122. Kleinman, A. Caregiving as moral experience. Lancet. (2012) 380:1550–1. doi: 10.1016/S0140-6736(12)61870-4
123. Baines, D, Cunningham, I, and Fraser, H. Constrained by managerialism: caring as participation in the voluntary social services. Econ Ind Democr. (2010) 32:329–52. doi: 10.1177/0143831X10377808
124. Katzman, ER, and Kinsella, EA. ‘It’s like having another job’: the invisible work of self-managing attendant services. Disabil Soc. (2018) 33:1436–59. doi: 10.1080/09687599.2018.1497949
125. Abellan, A, Perez, J, Pujol, R, Sundström, G, Jegermalm, M, and Malmberg, B. Partner care, gender equality, and ageing in Spain and Sweden. Int J Ageing Later Life. (2017) 11:69–89. doi: 10.3384/ijal.1652-8670.16-305
126. Horner, B, and Boldy, DP. The benefit and burden of “ageing-in-place” in an aged care community. Australian health review: a publication of the Australian Hospital Association, (2008). 32, 356–365. doi: 10.1071/ah080356
127. Andréasson, F, Mattsson, T, and Hanson, E. ‘The balance in our relationship has changed’: everyday family living, couplehood and digital spaces in informal spousal care. J Fam Stud. (2023) 29:719–37. doi: 10.1080/13229400.2021.1980421
128. Backhouse, T, Jeon, YH, Killett, A, Green, J, Khondoker, M, and Mioshi, E. Nurturing attentiveness: a naturalistic observation study of personal care interactions between people with advanced dementia and their caregivers. Gerontologist. (2024) 64:gnae004. doi: 10.1093/geront/gnae004
129. Hemberg, J, Nyqvist, F, and Näsman, M. “Homeless in life” – loneliness experienced as existential suffering by older adults living at home: a caring science perspective. Scand J Caring Sci. (2019) 33:446–56. doi: 10.1111/scs.12642
Keywords: ageing-in-place, caregiver burden, cohabiting partners, older adults, qualitative systematic literature review, responsibilities, roles
Citation: Glasdam S, Xu H, Slåtsveen R-E, Stilwell C, Wind G, Gulestø RJA and Turcotte P-L (2025) Older caregivers’ responsibilities and strategies for their cohabiting partners living at home—a qualitative systematic literature review. Front. Public Health. 13:1658095. doi: 10.3389/fpubh.2025.1658095
Edited by:
Roger O'sullivan, Institute of Public Health, IrelandReviewed by:
Donna de Levante Raphael, Alzheimer’s Foundation of America, United StatesXueting Ding, University of California, Irvine, United States
Imke Heuer, University Medical Center Hamburg-Eppendorf, Germany
Copyright © 2025 Glasdam, Xu, Slåtsveen, Stilwell, Wind, Gulestø and Turcotte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stinne Glasdam, c3Rpbm5lLmdsYXNkYW1AbWVkLmx1LnNl
†ORCID: Stinne Glasdam, orcid.org/0000-0002-0893-3054
Hongxuan XU, orcid.org/0000-0002-0750-2279
Ruth-Ellen Slåtsveen, orcid.org/0000-0003-1924-6409
Christie Stilwell, orcid.org/0000-0001-8234-3522
Gitte WInd, orcid.org/0000-0002-4907-4225
Ragnhild JA Gulestø, orcid.org/0000-0001-6238-3770
Pier-Luc Turcotte, orcid.org/0000-0002-2343-8836