 Marie Jönsson
Marie Jönsson Cecilia Pettersson
Cecilia Pettersson Mialinn Arvidsson Lindvall
Mialinn Arvidsson Lindvall- 1Department of Health Sciences, Örebro University, Örebro, Sweden
- 2Department of Health Sciences, Hogskolan Kristianstad, Kristianstad, Sweden
- 3Department of Health Sciences, Malardalens Universitet, Västerås, Sweden
Background: There is ample evidence that senior day centres can provide rehabilitation, increase activity and support social participation for older adults.
Aim: The aim of this scoping review is to provide an overview of the scientific literature in this field and investigate whether there is scientific evidence for the efficacy of rehabilitation interventions at senior day centres for older adults.
Methods: The scoping review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). Data were collected from databases between January 2010 and December 2020 and updated December 2023. The scoping review was conducted in the databases CINAHL, Cochrane Library and PubMed and 29 articles were identified for inclusion.
Results: Rehabilitation interventions at the senior day centres varied considerably. The main findings concern interventions of a physical, cognitive and/or social character. The most common dimensions of outcome were improvements in physical and cognitive ability and quality of life. There was also considerable variation in the professionals involved. Other important factors to observe when participating in interventions at senior day centres could be loneliness and risk of falls.
Conclusion: While rehabilitation interventions at senior day centres are striving towards person-centred care, there is room for improvement to meet older adults’ individual needs. In conclusion, this scoping review shows that greater focus is needed to strengthen the evidence base for examine interventions that are most effective in these settings.
Introduction
Senior day centres provide rehabilitation in community-based services that provide support and create opportunities for older adults to engage in various activities and interact with their peers (1). Senior day centres are characterised as facilitators of activity, companionship and social interaction (2–4), fostering independence and enabling older adults to age in place while minimising avoidable hospitalisations (5). These centres also offer services intended to promote active and healthy ageing (2), although it is notable that they are described in terms of various interventions.
In healthcare and social care for older adults, senior day centres are described as preventing ill health and loneliness (1, 2, 6). For example, these centres act as a point of delivery of services for an estimated 46 million older adults in the United States (7) and can provide activities that promote social interactions and healthy ageing (2, 6). In this study, the term health outcomes refer broadly to physical, cognitive, and social dimensions of health among older adults, which is in line with the World Health Organisation’s holistic definition of health (8, 9). These outcomes may include improvements in mobility, cognitive functioning, emotional well-being, social participation, and perceived quality of life (8, 9). Senior day centres are described as community-based services including rehabilitation interventions designed to support older adults living at home by providing structured daytime programmes that combine social, and physical activities. These daytime programmes include opportunities for social interaction and engagement in meaningful activities, access to rehabilitation and preventive care provided by various professions and may also give respite support for informal caregivers (10, 11). In order to support healthy ageing, the World Health Organisation (WHO) has developed a policy framework that defines healthy ageing as “the process of developing and maintaining the functional ability that enables wellbeing in older age” (9). Functional ability is also dependent on interactions with relevant environmental characteristics. These environmental characteristics include factors such as policies, the built environment, relationships, values and attitudes (9). Interaction with other people is valuable; loneliness is a major risk factor for physical and mental illness, as well as frailty (12). As a confounding effect for physical and mental health in later life, loneliness and social isolation among older adults have therefore garnered significant attention in recent decades (13, 14). Maintaining social contact with other people facilitates healthier ageing (13). To this end, well-functioning municipal senior day centres are described as important for relieving the burden on assisted-living services, home-care services and primary healthcare (1, 6), where staff are often stretched to the limit. Previous research on senior day centres in general has shown that rehabilitation interventions are diverse in order to attract a wide range of clients (2), create opportunities to maintain meaningful activities, encourage social interactions (2) and reduce feelings of loneliness (2, 6, 15). It is unclear whether the rehabilitation interventions offered at senior day centres meet the direct needs of the older adults. For example, whether the types of physical and social activities offered are person-centred and address older adults’ interests and individual needs. To enable person-centred care at senior day centres, it is important to investigate whether these interventions are individualised and needs-based. According to a person-centred approach, both clients and staff must be involved in planning interventions (16).
With regard to existing research into senior day centres for older adults, we conclude that the empirical evidence is limited. In a broader healthcare context, senior day care is a service with the potential to help older adults remain healthier and support them to age in place. Furthermore, attending a senior care centre can help to maintain abilities that can potentially prevent unnecessary hospitalisation or institutional care (5, 17). An understanding of interventions, outcomes, tools and the involved professional practitioners is vital to developing future complex, multicomponent interventions (18). In order to broaden knowledge concerning the subject, a scoping review was conducted (19). The aim of this scoping review was to summarise the range of rehabilitation interventions implemented in senior day centres for older adults in terms of outcomes, tools and professional involvement.
Method
A scoping review approach was chosen to gather and summarise literature and identify knowledge gaps (20). To address the limited research available, this scoping review provides an overview of existing studies and highlights emerging evidence on the topic (20). Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (21), we undertook a systematic literature search of articles published in international journals. The following stages were implemented: (1) identifying the research question; (2) identifying relevant articles; (3) selecting articles; (4) charting the data; (5) collating, summarising and reporting the results; and (6) consulting. In reporting, we adhere to the PRISMA guidelines for scoping reviews (21). The literature search was conducted in spring 2020 by an academic librarian together with the last author and was subsequently updated by the first and last author in December 2023. All authors have substantial experience in rehabilitation of older adults and rehabilitation interventions. The first and second authors are occupational therapists (OTs), and the last author is a physiotherapist (PT).
1. Identifying the research question. Based on the aim of the scoping review, the following research questions were formulated:
• What interventions were implemented?
• Which outcome dimensions were used to capture the effects of those interventions?
• What tools and assessment methods were used?
• What effects of the interventions have been demonstrated?
• Which professions have been involved in the interventions?
2. Identifying relevant articles. A systematic literature search was conducted in the databases CINAHL and PubMed, using the following keywords in various combinations: Senior Centres, Adult Day Care Centres, Day Care, Medical, Day care program, physical and creative. The selection criterion was studies published in international peer-reviewed scientific journals between January 2010 and December 2020 (later updated in January 2021 and December 2023) involving subjects 65 years of age or over who attend senior day centres. An additional search was conducted in Cochrane Library for the same search period. Studies published in a language other than English were not considered. Since different databases use different concepts for the same phenomenon, each specific keyword was modified for each database and the search was adapted for the different databases. The limit “aged 65 + years” was applied to the literature search. All types of studies were considered. No grey literature was considered for inclusion in this scoping review. Grey literature was excluded because it was deemed unlikely to provide evidence relevant to the research questions concerning senior day centres (22).
3. Selecting the articles. As recommended by Tricco et al. (21), the selection process is presented as a flow diagram (Figure 1). The first and last authors reviewed the articles independently and examined the titles and abstracts of the articles identified. The Rayyan systematic review programme was used by the authors when performing their independently systematic work (23). The first step was to assess whether the abstracts were potentially relevant for inclusion. In the second step, the first and the last author independently screened the records, resulted in 29 full-text studies. Thereafter, all three authors independently read these studies abstracts and then discussed the studies in relation to inclusion and exclusion criteria. The same three authors subsequently read the remaining full-text studies in full text to reach a consensus on which original publications met the selection criterion. All publications included in this review are presented in Table 1.
4. Charting the data. According to the research questions formulated for this study, data were synthesised systematically following the reporting guidelines provided by PRISMA-ScR (21) and Arksey and O’Malley’s methodological framework (20). After initially conducting independent screenings in the Rayyan systematic review software, the first and last authors discussed any conflicting inclusion decisions until consensus was reached. Following this, data extraction was carried out using a structured data charting process, designed to present the information in a clear and logical manner for the reader (24). The extracted data included, for example, author(s), year of publication, country of origin, study aim, population, methodology, and findings relevant to the research questions. Results from the selected studies (n = 27) were then systematically extracted and transcribed in relation to the predefined research questions. This process was applied consistently across all included studies (Table 1). Several joint discussions took place between all authors in the research team regarding the relevance of articles in relation to the inclusion criterion.
5. Collating, summarising and reporting, is described in the Result section.
6. Consulting, optional and was not included in this scoping review.
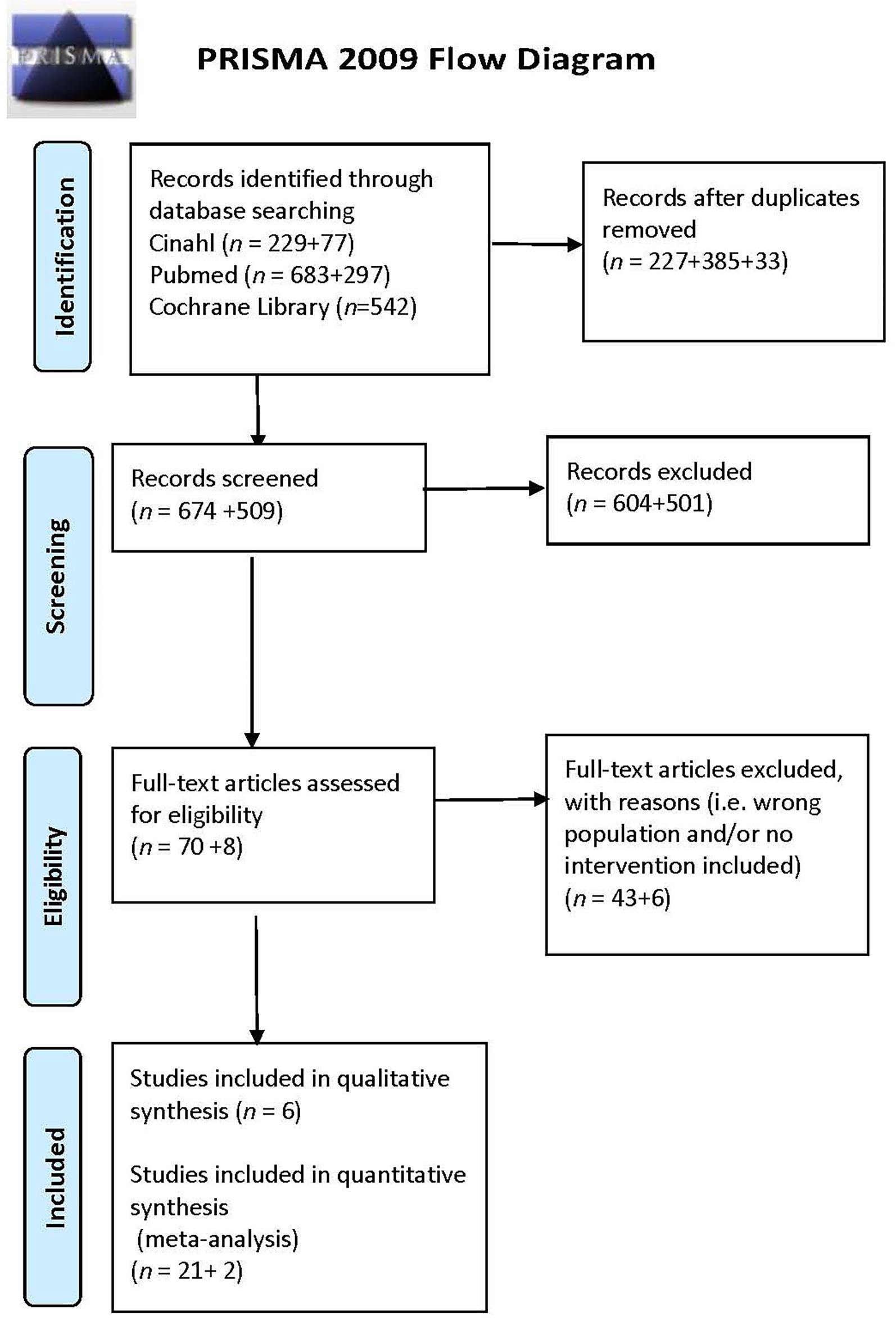
Figure 1. PRISMA flow diagram from Moher et al., 2009.

Table 1. Characteristics of the included articles.
Results
The result are presented in text and in greater detail in Table 1, which is structured based on the five research questions. A total of 29 articles (quantitative n = 23, qualitative n = 6) were included (Table 1). The studies were conducted in countries and region: Canada (n = 1), Finland (n = 1), Germany (n = 1), India (n = 1), Iran (n = 1), Israel (n = 5), Italy (n = 1), Japan (n = 1), Netherlands (n = 1), Norway (n = 5), Spain (n = 2), Taiwan (n = 2), United Kingdom (n = 2) and United States (n = 4; Table 1).
Interventions at senior day centres
The most common interventions at senior day centres were various types of group activities with a social focus, such as music, choirs and bands, art and crafts, cooking, playing board games and gardening (15, 25–37). Some interventions involved interactions with the older adults, such as reading newspapers, conversation in groups, playing theatre, and language and computer classes (15, 25, 31, 34, 35, 37–42). There were also interventions based on specific dates in the calendar such as Easter and Valentine’s Day, as well and activities related to local history and culture, including tours to local sites of historical interest (32, 43). The interventions included activities targeting physical, cognitive and social functioning (26, 28, 34, 35, 37, 40, 43–48). For example, interventions focused on social functioning might involve health education, medical check-ups or nursing services (42, 46), but also social activities such as taking coffee breaks and meals together during the day (35, 42, 49). There were some interventions involving problem-solving therapy (intended to improve communication skills) (38, 41), humour therapy (50), activities designed specifically for people with dementia (25, 34–36, 45, 48, 51, 52) and for socially isolated older adults (40, 44, 53). Physical interventions included physiotherapy sessions such as mobility games focusing on strength and balance training (29, 32, 35, 37, 44, 47–49), dance, exercise, tai chi, table tennis, yoga, aerobics, gateball, and general mobility exercises to improve gross and fine motor skills. Interventions related to cognitive function were performed by occupational therapists and could include cognitive activation, memorising, recognition, forming associations, special cognitive abilities such as language comprehension, and logic exercises using pen-and-paper (35, 41), sometimes combined with training in the activities of daily living (ADL) (41). Activities such as beauty treatments and bathing and services such as laundry and transportation were also offered, usually characterised as welfare-related (49).
The outcome dimensions used to capture the effects of the intervention
The outcomes following the intervention at senior day centres were categorised in domains and elaborated upon in the text and partially described in Table 2. The results from the interventions demonstrated improvements for example in domains as physical ability, cognitive ability, social relationships and ADL. The positive outcome dimensions were mainly improved physical ability (26, 29, 32, 42–44, 46–49), followed by improved cognitive ability (26, 29, 35, 37, 41–43, 47), health-related quality of life (28–30, 32, 41–43, 49), general wellbeing (25, 30, 32, 44, 46, 50, 53) and social relationships (28, 30, 38, 39, 51). User satisfaction (33, 36, 38, 52), ADL (26, 30, 32, 35, 42, 47), depression (41, 42, 46), comorbidity (42), loneliness (28, 39, 40, 44) and self-esteem (28) were other outcome dimensions described in the studies. The outcome dimensions for user satisfaction had increased and included the participants’ communication and interactions with staff (33, 38, 52).
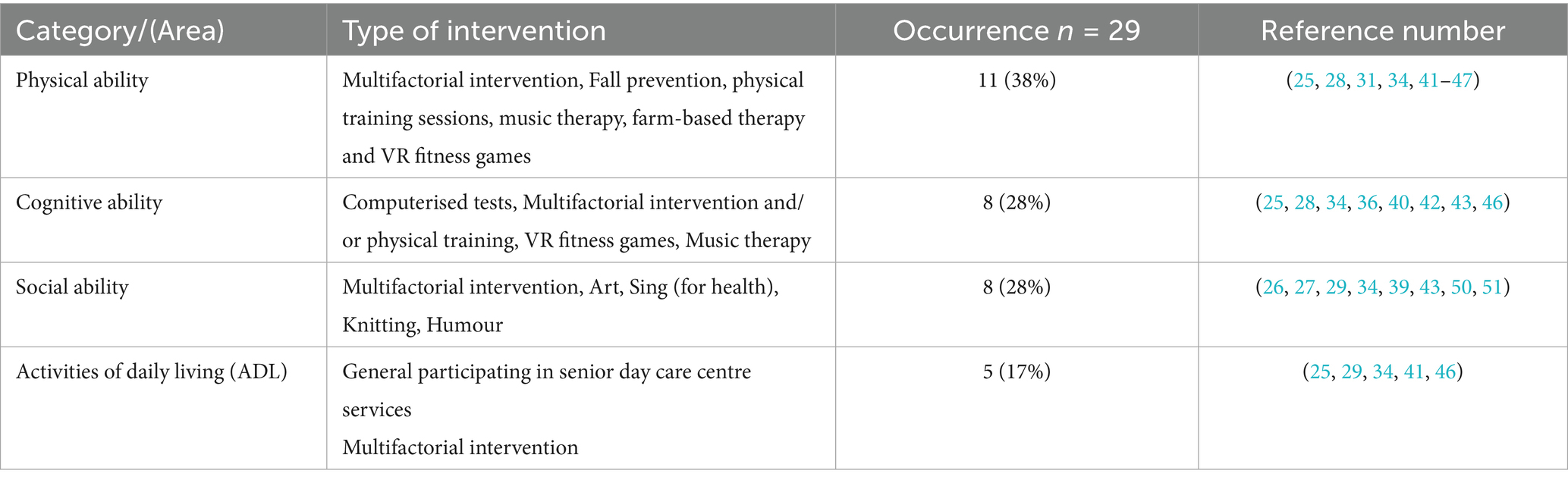
Table 2. Overview of main findings of the interventions at senior day centres for older adults (category/area, type of intervention occurrence and reference number).
Tools/metrics used in interventions at senior day centres
Various tools and metrics were used in the studies. These can be divided into four different areas: health-related quality of life, user satisfaction, cognitive ability and ability to perform activities of daily life (ADLs), and health conditions. Data from three of the qualitive studies (25, 34, 36) describe the participants’ perceptions of the interventions and were related to general wellbeing in the area of user satisfaction.
Health-related quality of life
Seven studies (29, 30, 32, 41–43, 49) used various outcome measures to describe quality of life and six studies used assessments of general wellbeing (27, 28, 32, 46, 50, 53). The measurements used in these studies were: the Short Form Health Survey 36 (SF 36) (54), Self-Rated Health, Korean version of Short-form 36 (55), the Short Form Health Survey 12 (56), the World Health Organisation Quality of Life (WHO QOL) (57) and The World Health Organisation Quality of Life-OLD (58). To describe general wellbeing measurements, tools such as the RAND Health Status Questionnaire shortened version (59), Satisfaction with Life Scale (60), Scale of Social Well-Being (61), MacArthur Scale of Subjective Social Status (62), Rosenberg Self-Esteem Scale (63), General Well-Being Schedule (GWB) (64), The Oslo Social support Scale (OSS-3) (65) and Brief Symptom Inventory (BSI) (66) were used.
User satisfaction
User satisfaction was observed, measured and evaluated in five studies (27, 33, 36, 38, 52). Two studies used a self-assessment questionnaire (38, 52) and one in-depth interviews (36). In the study by Rowe et al. (33) and Eaton (27), the interactions between staff and older adults were observed and measured when performing various group activities. User satisfaction was also assessed on the Philadelphia Geriatric Centre Affect Rating Scale (ARS) (67).
Cognitive ability and ability to perform ADLs
Ten studies (26, 29, 35, 37, 40–43, 45, 47) measured changes in cognitive ability related to an intervention. Four studies (35, 37, 41, 42) used the Mini Mental Status Examination (MMSE) (68) to assess cognitive function. The Abbreviated Mental Test Score (69), Mental Component Summary Score in SF-36 (54), Montreal Cognitive Assessment (MoCA) (70), Short Portable Mental Status Questionnaire (SPMSQ) (71), The Alzheimer’s Disease Assessment Scale (ADAS-Cog) (72), Clinical Dementia Rating (CDR) Scale (73), Executive Interview (EXIT-25) (74), Chinese Version of the Verbal Learning Test (CVVLT) (75) and near-infra red spectroscopy (NIRS) were also used.
ADLs were described and measured in six of the included studies (26, 30, 32, 35, 42, 47). Tools used in these studies included the Katz Index of Independence in Activities of Daily Living (76), the Erlangen Test of Activities of Daily Living (ETAM) (77) and the modified Barthel Index (78). Fillenbaum’s (78) and Lawton’s (79) instruments were also used to examine the ability to perform instrumental activities of daily living (IADLs).
Health conditions
All of the studies described various health factors such as body weight, height, socioeconomic status, blood pressure and chronic conditions without any specific measurements. Some specific metrics of physical aspects such as walking (80), balance (81), muscle power (82), handgrip strength (83), curvature of the spine (using Spinal Mouse®) (84), and sleep (using ActiSleep) (85) were assessed in the studies (26, 42, 43, 45). The Physical Self-Maintenance Scale (PSMS) (79) was also used. Sarkar et al. (41) and Schmitt et al. (42) used the Geriatric Depression Scale (GDS) (86) to measure depression. Loneliness was measured on the UCLA Loneliness Scale (87) in the studies by Ayalon et al. (39) and Galinha et al. (28) respectively with Beck Depression Inventory (BDI) (88) in the study by Böen et al. (44). Risk of falls was measured using the Tinetti test (89) and the Short Physical Performance Battery (SPPB) (90). One study (42) presented comorbidity among the older adults using the Charlson Comorbidity Index (CCI) (91).
The effects of interventions or programmes
Participating and having multifactorial interventions (26, 29, 30, 32, 35, 41–43, 45–47, 49) at senior day care centres including physical, cognitive and psychosocial aspects seemed to be of importance in order to increase or maintain abilities in older adults. Overall, the most common effect of interventions was on quality of life (28–30, 32, 41–43, 49) and wellbeing (32, 40, 46, 50, 53). Physical improvements in older adults were for example found in interventions involving fall prevention, physical training sessions, music therapy, farm-based therapy and VR fitness games (26, 43, 45–49). Improvements in cognitive ability and the ability to perform activities of daily living between groups were also seen in some studies (35, 47) as well as gradual improvements in global cognitive function and memory function when using computerised neurocognitive tests (37). Another positive effect observed was that attending senior day centres could reduce the probability of depression by about 51%, There were also improvements in the WHO QOL scores in the social domain among those attending centres more than once a month (41). Other benefits of attending senior day centres included reduced loneliness and improved sociability (28–31, 39, 40, 44, 51). Participating in creative group interventions had a positive impact on social interactions and relationships in older adults with or without dementia (26, 28–31, 33, 51). The use of humour- (50), art- (27), respectively singing- (28) therapy was associated with positive effects on mental health, including lower levels of anxiety and depression, as well as improved general wellbeing but should be examined in further studies (50) (Table 2).
Professions involved in the interventions
The interventions included a broad range of professionals and contributors with varying roles and qualifications. Professions involved in interventions included healthcare professionals such as nurses, assistant nurses, occupational therapists and physiotherapists, as well as social workers and activity staff (25, 26, 31–33, 35, 36, 38, 41, 42, 45–53). OTs or PTs often led tailored group activity sessions, and physical sessions. Others involved were exercise specialists, healthy volunteers, a humourist, art and music teachers, visual art facilitators, family caregivers and other relatives (26, 27, 29, 34, 37, 43, 50, 53). These were often responsible for promoting general well-being, psychosocial support, and fostering social interaction.
Discussion
The findings of this scoping review indicate substantial variation in the types of interventions, outcome measures, reported effects, and professional involvement, reflecting the complexity of the field. The studies we have examined also represent a range of settings in which senior day centres deliver a variety of programmes. Attending a senior day centre can be valuable for older adults, helping them to maintain or improve their physical, cognitive and social functioning. However, this scoping review reveals the difficulty in describing the most effective, evidence-based rehabilitation interventions for older adults attending senior day centres. This highlights the need for rigorous research to identify the most effective intervention components and their impact on key outcomes among older adults attending senior day centres.
Older adults participating in activities at senior day centres can be supported and engaged in various interventions, including social interactions or activities that can improve or maintain their ability to age in place (2, 4, 92). Our results are in line with previous research in as much as the interventions implemented at the senior day centres often involved group activities with a social focus, such as music, crafts and board games (26–28, 31, 33, 34, 50), and therapeutic activities intended to improve social, physical, and/or cognitive functioning (25, 29, 30, 35, 37, 38, 43, 45–48, 51) and illustrated in Tables 1, 2. These various activities are of importance to supply with regular physical activity and these activities may also be person-centred, meaning they can be tailored to what is meaningful and important in the older adult’s daily life, supporting for example maintain abilities to age in place and quality of life (11, 43, 92).
One question that does arise is whether and if so to what extent older adults have the opportunity to choose an activity when attending a senior day centre. Studies have shown that meaningful participation is often dependent on identifying individual wishes and needs, thus facilitating person-centred interventions (16, 92). In their study, Brataas et al. (25) touch on this, noting that the occupational therapist organising the programme at one senior day centre did so together with the participants. However, it is unclear how the participants’ individual wishes and needs were assessed. If individual needs are not met, this may mean that older adults participating in activities at social day centres are less motivated, despite the fact that they would probably ‘benefit from it’. Moreover, the group of older adults can hardly be viewed as homogeneous, meaning that rehabilitation interventions at senior day centres should be based on person-centred plans and activities. Senior day centres also appear to have weaknesses when it comes to implementing preventive interventions to promote healthy ageing; developing health-promotion strategies to support functional ability should be of importance and may promote healthier ageing among the older adults who attend senior day centres (93). To ensure evidence-based practice at senior day centres, findings from related settings, such as long-term care facilities and nursing homes could be tested and integrated to a higher degree. As these studies have shown, i.e., multicomponent exercise programme improved general functionality as strength, balance, blood pressure and fall risk in older adults (43, 94, 95). This approach can help validate interventions and support adaptation in the senior day centre context, ultimately leading to more effective and sustainable health-promotion strategies.
The outcome dimensions use in the studies covered in this scoping review were mainly focused on physical and cognitive ability (26, 29, 30, 35, 37, 41–43, 45, 47), health-related quality of life (28, 30, 42, 49, 50) and/or social relationships (28, 39, 51). This is hardly surprising, as experienced health problems, support needs and cognitive ability change with age (96). Measuring cognitive ability is also important given that maintaining cognitive ability is one of the main determinants of whether an individual can continue to live independently. However, it was surprising that structured fall risk assessments are not conducted more extensively. Falls are a leading cause of injury, hospitalisation, and loss of independence among older adults (97). Therefore, implementing systematic fall risk assessments should be considered as a component of preventive care at senior day centres, helping to identify at-risk individuals and guide interventions to maintain safety and functional ability (95, 97). It would therefore be extremely valuable to examine these aspects in a structured manner at senior day centres. Regarding the activities of daily living, this was often measured on the Barthel Index (26, 32, 48) or some other measure of IADL (30, 35, 47). So, to a large extent the effects of interventions in senior day centres focus on ability to perform ADLs. This is an important reflection, since rehabilitative interventions at senior day centres not only strive to maintain independence and quality of life, but also to promote general ability and social engagement with other people. It is therefore crucial to take activities other than ADL into account as outcome dimensions, such as social and leisure activities. Previous research has found that the ability to maintain social relationships or social activities is important to maintaining everyday activities at home (5, 98). This aspect has been described by Lees (99), who questions how various professionals were able to identify older adults with a fragile social support network living in involuntary loneliness at home. On the other hand, there might be cultural differences between the countries represented in the studies included in this scoping review. Previous research (100, 101), has indicated that senior day centres can function as arenas for interpretation and translation, thereby fostering enhanced wellbeing among older adults. Furthermore, staff members were found to play a crucial role in facilitating connections between older adults and other key stakeholders within the care system, such as the municipalities and additional service providers. These findings are consistent with and further supported by the results of the present scoping review. Greater attention must therefore be paid to outcome dimensions that measure social support or social network along with functional needs at senior day centres.
Overall, interventions at senior day centres had a greater impact on quality of life and wellbeing than on loneliness and social status. One important effect of participating in interventions at senior day centres was that older adults showed higher levels of subjective social status and lower levels of loneliness (39). Since many older adults experience loneliness and desire social inclusion (13), it is important to reach those in this group of older adults and offer individualised interventions at senior day centres. A key solution for participating in interventions at senior day centres may be to participate for only part of the day or having regular telephone contacts as described in the study by Newall et al. (53).
A variety of professional disciplines were represented across the studies, highlighting the diverse expertise engaged in delivering the interventions. The professions involved in the studies were often nurses, assistant nurses, OTs, and PTs, who provided rehabilitation including for example assessments and various group activities. Furthermore, there are some unclear designations of staff working at the senior day centres, such as medical professionals and humourist. “Healthy volunteers” were involved in the study by Battaglia (43), but it is not clear what this means. This leads to a lack of clarity regarding the profession’s role and responsibility in performing the interventions at the senior day centres. Moreover, it is unclear which professions are most suited to the role. This diversity reflects the interdisciplinary nature of the interventions and the multifaceted approach to promoting health and well-being in senior day centres. There are some important questions to be answered about staffing at senior day centres, including whether licensed healthcare professionals are required and who has the requisite knowledge or is best suited to assessing individual needs, offering meaningful activities and facilitating participation. Multidisciplinary teams are essential in geriatric rehabilitation. Effective collaboration among professionals can lead to better care coordination and supports healthy ageing (102, 103) where professionals as assistant nurses (for engagement and participation in meaningful activities), OTs (for cognitive and ADL ability), PTs (for physical ability) and social workers (for emotional and service support) should be the minimum requirements for core competencies at senior day centres. In addition, the reviews by Fields et al. (104) and Lunt et al. (92) describe a lack of standardised definitions of services and content at senior day centres, something that makes any assessment and evaluation of efficacy difficult. In conclusion, to strengthen the evidence base and inform clinical practice, future research should include large-scale, methodologically robust randomised controlled trials incorporating results from related contexts as long-term care facilities and nursing homes (43, 94, 95). Such studies would also benefit from incorporating structured multidisciplinary person-centred rehabilitation interventions. The interventions should be guided by the principles of person-centred care, meaning that the individual’s goals, preferences, values, and lived experiences are central to the planning and delivery of care (105, 106). In addition, the interventions should be supported by MRC Guidance (107) to leverage technological solutions, ensuring active stakeholder involvement, and combining quantitative and qualitative methodologies to capture both outcomes and contextual factors.
Strength and limitations
Using the two databases CINAHL and PubMed might be a limitation and searching other databases such as the Cochrane Library, and PsycInfo may have yielded other published papers relevant to the aims of this scoping review. The authors involved in this study have prior experience of working with older adults and various rehabilitative interventions. Previous experience can both support and limit the research in terms of formulating research questions and data analysis. To enhance the credibility in this study, continuous engagement with data were performed by first and last author and continuously discussed by all authors. This process is a form of triangulation, which is considered to strengthen trustworthiness of the findings (108). A key strength of this scoping review lies in its comprehensive overview of interventions in senior day centres for older adults, including how these have been reported and categorised. Even if the interventions and outcome dimensions varied, the findings are an important first step towards developing complex interventions for older adults attending senior day centres (109). This scoping review has also highlighted the need for an appropriate framework to specify and describe the interventions at senior day centres for older adults. On the other hand, factors such as culture, relative income, and subjective well-being may vary among individuals in different countries or regions. Nevertheless, individuals with higher relative income, as well as those who, for instance, accept income inequality, have been found to report higher levels of subjective well-being (110) which is in line with the results in this study. A framework defining the concept of senior day centres may help those involved to tailor or choose interventions that promote a social and active life for older adults.
Conclusion
This scoping review revealed that, despite diverse interventions delivered in senior day centres, evidence remains insufficient to determine which interventions are the most effective. Greater focus on person-centred approaches and rigorous evaluation of intervention components, outcomes, and professional roles is needed to strengthen the evidence base for rehabilitation in this setting.
Implications for rehabilitation
• Senior day centres for older adults are poorly organised and described to address person-centred needs in older adults.
• Future initiatives should prioritise the development of structured assessment procedures and targeted interventions at senior day centres to enhance their role in supporting ageing in place.
• Clear handovers and documentation of rehabilitation outcomes interventions from senior day centres for older adults to outpatient healthcare are essential.
• Adequate levels of rehabilitation competence must be ensured among staff at senior day centres.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
MJ: Conceptualization, Funding acquisition, Methodology, Software, Writing – original draft, Writing – review & editing. CP: Conceptualization, Formal analysis, Methodology, Writing – review & editing. ML: Conceptualization, Formal analysis, Methodology, Software, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Region of Orebro County, Sweden.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Samuelsson, L, Malmberg, B, and Hansson, JH. Daycare for elderly people in Sweden: a national survey. Scand J Soc Welf. (1998) 7:310–9.
2. Aday, RH, Wallace, B, and Krabill, JJ. Linkages Between the Senior Center as a Public Place and Successful Aging. Act Adapt Aging. (2018) 43:211–31. doi: 10.1080/01924788.2018.1507584
3. Anetzberger, GJ. Community resources to promote successful aging. Clin Geriatr Med. (2002) 18:611–25. doi: 10.1016/S0749-0690(02)00018-6
4. Gomes da Silva, M, and Gameiro, M. Patterns of Sedentary Behavior of People Older than 75 Attending Day Care: Association with Quality of Life. Act Adapt Aging. (2021) 45:27–38. doi: 10.1080/01924788.2020.1719583
5. Jonsson, M, Fredriksson, C, and Holmefur, M. Everyday activities at home - Experiences of older repeatedly readmitted people. Scand J Occup Ther. (2020) 29:555–62. doi: 10.1080/11038128.2020.1849393
6. Orellana, K, Manthorpe, J, and Tinker, A. Day centres for older people - attender characteristics, access routes and outcomes of regular attendance: findings of exploratory mixed methods case study research. BMC Geriatr. (2020) 20:158. doi: 10.1186/s12877-020-01529-4
7. Bobitt, J, and Schwingel, A. Evidence-Based Programs for Older Adults: A Disconnect Between U.S. National Strategy and Local Senior Center Implementation. J Aging Soc Policy. (2017) 29:3–19. doi: 10.1080/08959420.2016.1186465
8. Organization(WHO) WH. Disability and health. (2015). Available online at: http://www.who.int/mediacentre/factsheets/fs352/en/2018 (Accessed October 3, 2018).
9. World Health Organization. World report on ageing and health (2015). Available online at: http://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_eng.pdf?sequence=1 (Accessed on 2018 October 3)
10. Larsson Ranada, Å, and Österholm, J. Promoting Active and Healthy Ageing at Day Centers for Older People. Act Adapt Aging. (2022) 46:236–50. doi: 10.1080/01924788.2022.2028050
11. Lunt, C, Dowrick, C, and Lloyd-Williams, M. What is the impact of day care on older people with long-term conditions: A systematic review. Health Soc Care Community. (2021) 29:1201–21. doi: 10.1111/hsc.13245
12. Sha, S, Xu, Y, and Chen, L. Loneliness as a risk factor for frailty transition among older Chinese people. BMC Geriatr. (2020) 20:300. doi: 10.1186/s12877-020-01714-5
13. Dahlberg, L, Agahi, N, and Lennartsson, C. Lonelier than ever? Loneliness of older people over two decades. Arch Gerontol Geriatr. (2018) 75:96–103. doi: 10.1016/j.archger.2017.11.004
14. Dahlberg, L, Andersson, L, and Lennartsson, C. Long-term predictors of loneliness in old age: results of a 20-year national study. Aging Ment Health. (2018) 22:190–6. doi: 10.1080/13607863.2016.12474210
15. Kim, J, and Kim, J. Exploring Health Benefits through Senior Center Engagement: A Qualitative Investigation of Older Korean Immigrants. Act Adapt Aging. (2021) 45:1–13. doi: 10.1080/01924788.2019.1698121
16. Slater, P, McCance, T, and McCormack, B. The development and testing of the Person-centred Practice Inventory - Staff (PCPI-S). Int J Qual Health Care. (2017) 29:541–7. doi: 10.1093/intqhc/mzx066
17. Gitlin, LN, Hauck, WW, Dennis, MP, Winter, L, Hodgson, N, and Schinfeld, S. Long-term effect on mortality of a home intervention that reduces functional difficulties in older adults: results from a randomized trial. J Am Geriatr Soc. (2009) 57:476–81. doi: 10.1111/j.1532-5415.2008.02147.x
18. Craig, P, Dieppe, P, Macintyre, S, Michie, S, Nazareth, I, and Petticrew, M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:a1655. doi: 10.1136/bmj.a1655
19. Peters, MDJ, Marnie, C, Tricco, AC, Pollock, D, Munn, Z, Alexander, L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. (2020) 18:2119–26. doi: 10.11124/JBIES-20-00167
20. Arksey, H, and O'malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8:19–32. doi: 10.1080/1364557032000119616
21. Tricco, AC, Lillie, E, Zarin, W, O'Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
22. Davies, H, Watkins, PM, Freeman-Sanderson, A, Nickels, MR, Ankravs, M, Ridley, EJ, et al. Scoping review of review methodologies used for guiding evidence-based practice in critical care: a protocol. BMJ Open. (2024) 14:e082661. doi: 10.1136/bmjopen-2023-082661
23. Harrison, H, Griffin, SJ, Kuhn, I, and Usher-Smith, JA. Software tools to support title and abstract screening for systematic reviews in healthcare: an evaluation. BMC Med Res Methodol. (2020) 20:7. doi: 10.1186/s12874-020-0897-3
24. Boland, A, Gemma Cherry, M, and Dickson, R. Doing a systematic review - A student's guide. 2nd ed. Thousand Oaks, California: Sage (2017).
25. Brataas, HV, Bjugan, H, Wille, T, and Hellzen, O. Experiences of day care and collaboration among people with mild dementia. J Clin Nurs. (2010) 19:2839–48. doi: 10.1111/j.1365-2702.2010.03270.x
26. Chan, SY, and Chen, CF. Effects of an Active Music Therapy Program on Functional Fitness in Community Older Adults. J Nurs Res. (2020) 28:e111. doi: 10.1097/JNR.0000000000000391
27. Eaton, J. Let us progress! Implementing professionally led arts-based programming in senior centers. Educ Gerontol. (2022) 48:415–28. doi: 10.1080/03601277.2022.2045536
28. Galinha, IC, Garcia-Martin, MA, and Lima, ML. Sing4Health: Randomised controlled trial of the effects of a singing group program on the subjective and social well-being of older adults. Appl Psychol Health Well Being. (2022) 14:176–95. doi: 10.1111/aphw.12297
29. Hedayati, M, Sum, S, Pourhadi, S, Hosseini, SR, and Faramarzi, M. Effect of Group Physical Games on Life Quality of Older Adults at Adult Daycare Centers. Elderly Health J. (2022) 8:6–13. doi: 10.18502/ehj.v8i1.9949
30. Iecovich, E, and Biderman, A. Attendance in adult day care centers of cognitively intact older persons: reasons for use and nonuse. J Appl Gerontol. (2013) 32:561–81. doi: 10.1177/0733464811432141
31. Keisari, S, Gesser-Edelsburg, A, Yaniv, D, and Palgi, Y. Playback theatre in adult day centers: A creative group intervention for community-dwelling older adults. PLoS One. (2020) 15:e0239812. doi: 10.1371/journal.pone.0239812
32. Murphy, F, Hugman, L, Bowen, J, Parsell, F, Gabe-Walters, M, Newson, L, et al. Health benefits for health and social care clients attending an Integrated Health and Social Care day unit (IHSCDU): a before-and-after pilot study with a comparator group. Health Soc Care Community. (2017) 25:492–504. doi: 10.1111/hsc.12329
33. Rowe, JM, Savundranayagam, MY, Lang, J, and Montgomery, RJV. Characteristics of Creative Expression Activities: The Links Between Creativity, Failure-Free, and Group Process With Levels of Staff-Participant Engagement and Participant Affect in an Adult Day Center. Act Adapt Aging. (2011) 35:315–30. doi: 10.1080/01924788.2011.625216
34. Shoesmith, E, Charura, D, and Surr, C. Acceptability and feasibility study of a six-week person-centred, therapeutic visual art intervention for people with dementia. Arts Health. (2021) 13:296–314. doi: 10.1080/17533015.2020.1802607
35. Straubmeier, M, Behrndt, EM, Seidl, H, Ozbe, D, Luttenberger, K, and Graessel, E. Non-Pharmacological Treatment in People With Cognitive Impairment. Dtsch Arztebl Int. (2017) 114:815–21. doi: 10.3238/arztebl.2017.0815
36. Tretteteig, S, Vatne, S, and Rokstad, AM. The influence of day care centres designed for people with dementia on family caregivers - a qualitative study. BMC Geriatr. (2017) 17:5. doi: 10.1186/s12877-016-0403-2
37. Weintruab-Youdkes, A, Prisant, B, Ben-Israel, J, and Merims, D. A Novel Modification of the “Method of Loci” to Improve Memory in Older Adults. Act Adapt Aging. (2015) 39:307–17. doi: 10.1080/01924788.2015.1090281
38. Armadans, I, Codina, N, and Pestana, JV. Empowering Senior Citizens in Leisure Settings Through Mediation: Becoming a Mediator. Educ Gerontol. (2014) 41:282–91. doi: 10.1080/03601277.2014.958019
39. Ayalon, L. Subjective Social Status as a Predictor of Loneliness: The Moderating Effect of the Type of Long-Term Care Setting. Res Aging. (2019) 41:915–35. doi: 10.1177/0164027519871674
40. Pitkala, KH, Routasalo, P, Kautiainen, H, Sintonen, H, and Tilvis, RS. Effects of socially stimulating group intervention on lonely, older people's cognition: a randomized, controlled trial. Am J Geriatr Psychiatry. (2011) 19:654–63. doi: 10.1097/JGP.0b013e3181f7d8b0
41. Sarkar, S, Kattimani, S, Premarajan, KC, and Roy, G. Impact of attendance in a daycare centre on depression among elderly in rural Puducherry: A pre- & post-intervention study. Indian J Med Res. (2017) 146:S68–76. doi: 10.4103/ijmr.IJMR_857_15
42. Schmitt, EM, Sands, LP, Weiss, S, Dowling, G, and Covinsky, K. Adult day health center participation and health-related quality of life. Gerontologist. (2010) 50:531–40. doi: 10.1093/geront/gnp172
43. Battaglia, G, Bellafiore, M, Alesi, M, Paoli, A, Bianco, A, and Palma, A. Effects of an adapted physical activity program on psychophysical health in elderly women. Clin Interv Aging. (2016) 11:1009–15. doi: 10.2147/CIA.S109591
44. Bøen, H, Dalgard, OS, Johansen, R, and Nord, E. A randomized controlled trial of a senior centre group programme for increasing social support and preventing depression in elderly people living at home in Norway. BMC Geriatr. (2012) 12:20. doi: 10.1186/1471-2318-12-20
45. Finnanger Garshol, B, Ellingsen-Dalskau, LH, and Pedersen, I. Physical activity in people with dementia attending farm-based dementia day care - a comparative actigraphy study. BMC Geriatr. (2020) 20:219. doi: 10.1186/s12877-020-01618-4
46. Kogan, AC, Gonzalez, J, Hart, B, Halloran, S, Thomason, B, Levine, M, et al. Be Well: results of a nutrition, exercise, and weight management intervention among at-risk older adults. J Appl Gerontol. (2013) 32:889–901. doi: 10.1177/0733464812440043
47. Liao, YY, Tseng, HY, Lin, YJ, Wang, CJ, and Hsu, WC. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur J Phys Rehabil Med. (2020) 56:47–57. doi: 10.23736/S1973-9087.19.05899-4
48. Lopez-Garcia, A, and Sanchez-Ruiz, ME. Feasible Intervention through Simple Exercise for Risk of Falls in Dementia Patients: A Pilot Study. Int J Environ Res Public Health. (2022) 19:1–8. doi: 10.3390/ijerph191911854
49. Kim, HS, Harada, K, Miyashita, M, Lee, EA, Park, JK, and Nakamura, Y. Use of senior center and the health-related quality of life in Korean older adults. J Prev Med Public Health. (2011) 44:149–56. doi: 10.3961/jpmph.2011.44.4.149
50. Ganz, FD, and Jacobs, JM. The effect of humor on elder mental and physical health. Geriatr Nurs. (2014) 35:205–11. doi: 10.1016/j.gerinurse.2014.01.005
51. Gjernes, T. Knitters in a Day Center: The Significance of Social Participation for People With Mild to Moderate Dementia. Qual Health Res. (2017) 27:2233–43. doi: 10.1177/1049732317723890
52. Haeften-van, M, Dijk, A, Hattink, BJJ, Meiland, FJM, Bakker, T, and Droes, RM. Is socially integrated community day care for people with dementia associated with higher user satisfaction and a higher job satisfaction of staff compared to nursing home-based day care? Aging Ment Health. (2017) 21:624–33. doi: 10.1080/13607863.2016.1144710
53. Newall, NE, and Menec, VH. Targeting Socially Isolated Older Adults: A Process Evaluation of the Senior Centre Without Walls Social and Educational Program. J Appl Gerontol. (2015) 34:958–76. doi: 10.1177/0733464813510063
54. Ware, JE, Kosinski, M, Bayliss, MS, and Raczek, A. SF 36 Health Sivey Manual and Interpretation Guide. Boston, MA: New England Medical Center, The Health Institute (1993).
55. Ware, JE, Kosinski, M, Bayliss, MS, McHorney, CA, Rogers, WH, and Raczek, A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. Med Care (1995);33:As264–79.
56. Singh, A, Gnanalingham, K, Casey, A, and Crockard, A. Quality of life assessment using the Short Form-12 (SF-12) questionnaire in patients with cervical spondylotic myelopathy: comparison with SF-36. Spine. (2006) 31:639–43. doi: 10.1097/01.brs.0000202744.48633.44
57. Skevington, SM, Lotfy, M, and O'Connell, KA. The World Health Organization's WHOQOL-BREF quality of life assessment: psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. (2004) 13:299–310. doi: 10.1023/B:QURE.0000018486.91360.00
58. Power, M, Quinn, K, and Schmidt, S. Development of the WHOQOL-old module. Qual Life Res. (2005) 14:2197–214. doi: 10.1007/s11136-005-7380-9
59. REE, Young.. National Evaluation of the Department of Health’s Integrated Care Pilots. Final Report: Summary Version. Santa Monica (2012). Available online at: https://www.rand.org/pubs/technical_reports/TR1164z1.html (Accessed on 2023 September 29)
60. Diener, E, Emmons, RA, Larsen, RJ, and Griffin, S. The Satisfaction With Life Scale. J Pers Assess. (1985) 49:71–5.
61. Keyes, CLM. Atlanta: Brief description of the mental health continuum short form (MHC-SF) (2009). Available online at: https://www.google.com/search?q=keyes+brief+description+of+the+mental+health&oq=keyes+brief+description+of+the+mental+health&aqs=edge.69i57j0i546l2j0i546i649j69i60.2168j0j1&sourceid=chrome&ie=UTF-8 (Accessed October 4, 2022).
62. Adler, NE, Epel, ES, Castellazzo, G, and Ickovics, JR. Relationship of subjective and objective social status with psychological and physiological functioning: preliminary data in healthy white women. Health Psychol. (2000) 19:586–92. doi: 10.1037/0278-6133.19.6.586
64. Dupuy, HJ. Measuring Health: A Guide to Rating Scales and Questionnaires. New York: Oxford University Press (1987).
65. Kocalevent, RD, Berg, L, Beutel, ME, Hinz, A, Zenger, M, Harter, M, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. (2018) 6:31. doi: 10.1186/s40359-018-0249-9
66. Derogatis, LR, and Melisaratos, N. The Brief Symptom Inventory: an introductory report. Psychol Med. (1983) 13:595–605.
67. Lawton, MP, Van Haitsma, K, and Klapper, J. Observed affect in nursing home residents with Alzheimer's disease. J Gerontol B Psychol Sci Soc Sci. (1996) 51:P3–P14.
68. Folstein, MF, Folstein, SE, and McHugh, PR. "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98.
69. Foroughan, M, Wahlund, LO, Jafari, Z, Rahgozar, M, Farahani, IG, and Rashedi, V. Validity and reliability of Abbreviated Mental Test Score (AMTS) among older Iranian. Psychogeriatrics: Official J Japanese Psychogeriatric Society. (2017) 17:460–5. doi: 10.1111/psyg.12276
70. Nasreddine, ZS, Phillips, NA, Bédirian, V, Charbonneau, S, Whitehead, V, Collin, I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
71. Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc. (1975) 23:433–41.
72. Kueper, JK, Speechley, M, and Montero-Odasso, M. The Alzheimer's Disease Assessment Scale-Cognitive Subscale (ADAS-Cog): Modifications and Responsiveness in Pre-Dementia Populations. A Narrative Review J Alzheimers Dis. (2018) 63:423–44. doi: 10.3233/JAD-170991
73. Hughes, CP, Berg, L, Danziger, WL, Coben, LA, and Martin, RL. A new clinical scale for the staging of dementia. Br J Psychiatry. (1982) 140:566–72.
74. Royall, DR, Mahurin, RK, and Gray, KF. Bedside assessment of executive cognitive impairment: the executive interview. J Am Geriatr Soc. (1992) 40:1221–6.
75. Chang, CC, Kramer, JH, Lin, KN, Chang, WN, Wang, YL, Huang, CW, et al. Validating the Chinese version of the Verbal Learning Test for screening Alzheimer's disease. J Int Neuropsychol Soc. (2010) 16:244–51. doi: 10.1017/S1355617709991184
76. Katz, S, Downs, TD, Cash, HR, and Grotz, RC. Progress in development of the index of ADL. Gerontologist. (1970) 10:20–30.
77. Luttenberger, K, Reppermund, S, Schmiedeberg-Sohn, A, Book, S, and Graessel, E. Validation of the Erlangen Test of Activities of Daily Living in Persons with Mild Dementia or Mild Cognitive Impairment (ETAM). BMC Geriatr. (2016) 16:111. doi: 10.1186/s12877-016-0271-9
78. Fillenbaum, GG. Screening the elderly. A brief instrumental activities of daily living measure. J Am Geriatr Soc. (1985) 33:698–706.
79. Lawton, MP, and Brody, EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86.
80. Podsiadlo, D, and Richardson, S. The timed "Up & Go": a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. (1991) 39:142–8.
81. Sung, KW. The effect of a health maintenance program on physical function and mental health of the elderly in nursing homes. Taehan Kanho Hakhoe Chi. (2007) 37:478–89. doi: 10.4040/jkan.2007.37.4.478
82. Rikli, RE, and Jones, CJ. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist. (2013) 53:255–67. doi: 10.1093/geront/gns071
83. Jeon, EY, Kim, SY, and Yoo, HS. Effects of music therapy and rhythmic exercise on quality of life, blood pressure and upper extremity muscle strength in institution-dwelling elderly women. J Korean Acad Nurs. (2009) 39:829–39. doi: 10.4040/jkan.2009.39.6.829
84. Csuhai, EA, Nagy, AC, Varadi, Z, and Veres-Balajti, I. Functional Analysis of the Spine with the Idiag SpinalMouse System among Sedentary Workers Affected by Non-Specific Low Back Pain. Int J Environ Res Public Health. (2020) 17:1–14. doi: 10.3390/ijerph17249259
85. Erickson, KI, Barr, LL, Weinstein, AM, Banducci, SE, Akl, SL, Santo, NM, et al. Measuring physical activity using accelerometry in a community sample with dementia. J Am Geriatr Soc. (2013) 61:158–9. doi: 10.1111/jgs.12050
86. Friedman, B, Heisel, MJ, and Delavan, RL. Psychometric properties of the 15-item geriatric depression scale in functionally impaired, cognitively intact, community-dwelling elderly primary care patients. J Am Geriatr Soc. (2005) 53:1570–6. doi: 10.1111/j.1532-5415.2005.53461.x
87. Hughes, ME, Waite, LJ, Hawkley, LC, and Cacioppo, JT. A Short Scale for Measuring Loneliness in Large Surveys: Results From Two Population-Based Studies. Res Aging. (2004) 26:655–72. doi: 10.1177/0164027504268574
88. Wang, YP, and Gorenstein, C. Psychometric properties of the Beck Depression Inventory-II: a comprehensive review. Braz J Psychiatry. (2013) 35:416–31. doi: 10.1590/1516-4446-2012-1048
89. Kegelmeyer, DA, Kloos, AD, Thomas, KM, and Kostyk, SK. Reliability and validity of the Tinetti Mobility Test for individuals with Parkinson disease. Phys Ther. (2007) 87:1369–78. doi: 10.2522/ptj.20070007
90. Gómes-Montes, JF. Validity and reliability of the Short Physical Performance Battery (SPPB):A pilot study on mobility in the Colombian Andes. Colomb Med. (2013) 44:165–71. doi: 10.25100/cm.v44i3.1181
91. Charlson, ME, Pompei, P, Ales, KL, and MacKenzie, CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. (1987) 40:373–83.
92. Lunt, C, Dowrick, C, and Lloyd-Williams, M. The role of day care in supporting older people living with long-term conditions. Curr Opin Support Palliat Care. (2018) 12:510–5. doi: 10.1097/SPC.0000000000000391
93. Nuwere, E, Barone Gibbs, B, Toto, PE, and Taverno Ross, SE. Planning for a Healthy Aging Program to Reduce Sedentary Behavior: Perceptions among Diverse Older Adults. Int J Environ Res Public Health. (2022) 19:1–14. doi: 10.3390/ijerph19106068
94. Pepera, G, Christina, M, Katerina, K, Argirios, P, and Varsamo, A. Effects of multicomponent exercise training intervention on hemodynamic and physical function in older residents of long-term care facilities: A multicenter randomized clinical controlled trial. J Bodyw Mov Ther. (2021) 28:231–7. doi: 10.1016/j.jbmt.2021.07.009
95. Pepera, G, Krinta, K, Mpea, C, Antoniou, V, Peristeropoulos, A, and Dimitriadis, Z. Randomized Controlled Trial of Group Exercise Intervention for Fall Risk Factors Reduction in Nursing Home Residents. Can J Aging. (2023) 42:328–36. doi: 10.1017/S0714980822000265
96. Santoni, G, Angleman, S, Welmer, AK, Mangialasche, F, Marengoni, A, and Fratiglioni, L. Correction: age-related variation in health status after age 60. PLoS One. (2015) 10:e0130024. doi: 10.1371/journal.pone.0130024
97. Phelan, EA, and Ritchey, K. Fall Prevention in Community-Dwelling Older Adults. Ann Intern Med. (2018) 169:ITC81–96. doi: 10.7326/AITC201812040
98. Pettersson, C, Zingmark, M, and Haak, M. Enabling social participation for older people: The content of reablement by age, gender, and level of functioning in occupational therapists' interventions. Scand J Occup of Ther. (2022) 29:522–9. doi: 10.1080/11038128.2021.1967442
100. Carlsson, H, Pijpers, R, and Van Melik, R. Day-care centres for older migrants: spaces to translate practices in the care landscape. Soc Cult Geogr. (2020) 23:250–69. doi: 10.1080/14649365.2020.1723135
101. Vitman-Schorr, A, and Khalaila, R. Utilization of ADCCs and quality of life among older adults: ethno-regional disparities in Israel. BMC Geriatr. (2022) 22:18. doi: 10.1186/s12877-021-02674-0
102. Jönsson, M, Appelros, P, Holmefur, M, and Fredriksson, C. The broken care chain—report from a country with a low number of hospital beds. Front Health Services. (2025) 5:5. doi: 10.3389/frhs.2025.1632220
103. Westgard, T, Andersson Hammar, I, Dahlin-Ivanoff, S, and Wilhelmson, K. Can Comprehensive Geriatric Assessment Meet Frail Older People's Needs? Results from the Randomized Controlled Study CGA-Swed. Geriatrics (Basel). (2020) 5:1–17. doi: 10.3390/geriatrics5040101
104. Fields, NL, Anderson, KA, and Dabelko-Schoeny, H. The effectiveness of adult day services for older adults: A review of the literature from 2000–2011. J Appl Gerontol. (2014) 33:130–63. doi: 10.1177/0733464812443308
105. De Coninck, L, Declercq, A, Bouckaert, L, Dopp, C, Graff, MJL, and Aertgeerts, B. Promoting meaningful activities by occupational therapy in elderly care in Belgium: the ProMOTE intervention. BMC Geriatr. (2024) 24:275. doi: 10.1186/s12877-024-04797-6
106. Richards, K, Mills, N, and Hitch, D. Role of occupational therapy in person-centred dementia care: Exploring family member and clinician perceptions. Australas J Ageing. (2024) 43:140–7. doi: 10.1111/ajag.13269
107. Skivington, K, Matthews, L, Simpson, SA, Craig, P, Baird, J, Blazeby, JM, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. (2021) 374:n2061. doi: 10.1136/bmj.n2061
108. Hadi, MA, and Jose, CS. Ensuring rigour and trustworthiness of qualitative research in clinical pharmacy. Int J Clin Pharm. (2016) 38:641–6. doi: 10.1007/s11096-015-0237-6
109. Craig, P, and Petticrew, M. Developing and evaluating complex interventions: Reflections on the 2008 MRC guidance. Int J Nurs. (2013) 50:585–7. doi: 10.1016/j.ijnurstu.2012.09.009
Keywords: day care, interventions, elderly, professions, tools
Citation: Jönsson M, Pettersson C and Lindvall MA (2025) Rehabilitation interventions at senior day centres for older adults: a scoping review. Front. Public Health. 13:1659493. doi: 10.3389/fpubh.2025.1659493
Edited by:
Madia Lozupone, University of Bari Aldo Moro, ItalyReviewed by:
Garyfallia Pepera, University of Thessaly, GreeceFilipe Lopes, Federal University of Minas Gerais, Brazil
Copyright © 2025 Jönsson, Pettersson and Lindvall. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie Jönsson, bWFyaWUuam9uc3NvbkBvcnUuc2U=