 Yuanji Zhong
Yuanji Zhong Wenhao Guo
Wenhao Guo Pengwei Chen
Pengwei Chen Yongshun Wang
Yongshun Wang- 1School of Physical Education and Arts, Jiangxi University of Science and Technology, Ganzhou, Jiangxi, China
- 2School of Recreational Sports and Tourism, Beijing Sport University, Beijing, China
- 3College of Physical Education, Huaqiao University, Quanzhou, China
Background: Core training (CT) has been increasingly recognized as a promising intervention for improving balance in older adults, a demographic particularly susceptible to falls and fall-related injuries. This systematic review and meta-analysis sought to evaluate the efficacy of CT on balance in older adults, providing substantial evidence to establish its role in fall prevention strategies.
Methods: A comprehensive and systematic search of multiple databases, including PubMed, Cochrane Library, Web of Science, EBSCOhost, Embase and Google Scholar, was conducted to identify relevant studies. Eligible studies included single-group trials or randomized controlled trials that assessed the impact of CT on balance outcomes in healthy older adults (aged ≥60 years). It utilized the Cochrane Risk of Bias 2 (RoB 2) tool to assess the risk of bias across all included studies. Data were extracted from eleven studies and analyzed using Review Manager software version 5.4 and Stata 17.0, evaluating both dynamic and static balance parameters.
Results: The findings revealed statistically significant improvements in both dynamic and static balance metrics, including Gait Test (GT) (SMD = 0.32; 95% CI = 0.02, 0.63; p < 0.05), Functional Reach Test (FRT) (SMD = 0.82; 95% CI = 0.50, 1.24; p < 0.00001), Timed Up and Go (TUG) test (SMD = −0.81; 95% CI = −1.62, 0.00; p = 0.05), and One-Leg Stance Test (OLST) (MD = 3.19; 95% CI = 1.74, 4.64; p < 0.001). Subgroup analyses further indicated that CT had the most significant effect on dynamic balance, particularly in FRT. Additionally, longer intervention durations (≥45 min) resulted in more pronounced benefits for dynamic balance compared to shorter sessions. CT demonstrated superior effects on GT compared to Pilates Training (PT).
Conclusion: CT is a highly effective intervention for enhancing balance in older adults, supporting its integration into fall prevention programs. However, given the heterogeneity across studies, further rigorously designed trials with standardized intervention protocols and outcome measures are necessary to confirm the long-term benefits and optimal parameters for balance enhancement.
Systematic review registration: Inplasy.com, INPLASY202412006.
1 Introduction
Population aging has emerged as an unprecedented global challenge, with profound implications for health systems and societal structures. Projections from the World Health Organization (WHO) indicate that by 2030, individuals aged 60 years and older will constitute one-sixth of the global population (1). This dramatic demographic shift has brought “healthy aging” to the forefront of global policy agendas, emphasizing the need to promote well-being and functional independence among older adults. As individuals age, physiological changes, such as reductions in muscle strength and bone density, undermine the integrity of the musculoskeletal system and compromise joint stability. These alterations significantly elevate the risk of falls, which are not only a leading cause of injury but also the second most common cause of unintentional injury-related mortality worldwide (2, 3). Among older adults, falls pose an especially serious threat, accounting for a substantial proportion of injuries and fatalities. Epidemiological data reveal that the incidence of falls ranges from 28 to 35% among those aged 60 and older, with the prevalence increasing to 42% in individuals over 70 years of age (4). Given the considerable health and economic burdens associated with falls in the aging population, the urgency of developing effective fall prevention strategies cannot be overstated. Identifying and implementing interventions that address fall risk factors is paramount to safeguarding the health, autonomy, and quality of life of older adults while alleviating the strain on healthcare systems.
Balance is a critical factor in fall prevention, playing a fundamental role in maintaining stability and mobility. It is defined as the ability to maintain the body’s center of mass within its base of support, achieved through the seamless integration of the visual, vestibular, and proprioceptive systems (5). This coordination ensures stability under both static and dynamic conditions, making balance a critical determinant of physical functionality in older adults. Among the myriad factors influencing falls in the older population, the enhancement of balance is widely regarded as a cornerstone strategy for improving postural stability and mitigating fall risks (6). Declines in balance, often associated with aging, have prompted an increasing volume of research dedicated to identifying effective interventions aimed at bolstering balance performance in older adults (7). Among these approaches, CT has emerged as a highly targeted and efficacious solution, garnering significant attention for its role in enhancing postural control and reducing fall susceptibility (8, 9).
CT primarily focuses on enhancing the stability, coordination, and functional capacity of the trunk muscles, including the abdominal muscles, erector spinae, and iliopsoas (10). For instance, Swiss ball core strengthening exercises have been demonstrated to yield significant improvements in spinal stability and overall muscular strength (11). Evidence suggests that, compared to younger populations, older adults experience more pronounced improvements in balance and gait performance following CT, a phenomenon likely attributable to the decline in balance associated with aging (2). Despite a growing body of literature demonstrating that CT can effectively enhance balance, reduce fall risk, and decrease fall incidence in older adults (8, 9, 12, 13), several studies are hindered by limitations such as small sample sizes, inconsistent intervention protocols, and variability in outcome measures, which undermine the generalizability of their findings. Systematic review and meta-analysis, an advanced methodological approach for systematically synthesizing and quantifying the results of multiple studies, offers a robust solution to these limitations (14). Specifically, systematic review and meta-analysis facilitates the aggregation of data across studies, calculation of effect sizes, and generation of robust evidence for clinical practice and policy development (15). Therefore, conducting a meta-analysis to evaluate the effects of CT on balance in older adults is essential to provide comprehensive and actionable insights for clinical and public health applications.
In recent years, numerous systematic reviews and meta-analyses have explored the effects of CT and related physical activities on balance outcomes in older adults. These studies have investigated the effects of interventions such as PT (16–20), Tai Chi (21, 22), balance training (23), and resistance training (24), which share certain similarities with CT in targeting balance enhancement. However, unlike these interventions, CT is unique in its training modalities and objectives, potentially leading to different effects on balance in older adults. More importantly, CT often serves as the foundational component of these exercise regimes (25), yet research specifically examining its impact on balance in older adults is limited. Although a systematic review and meta-analysis examining the effects of CT on balance in older adults has been conducted (26), the findings were limited to samples from Chinese populations. These results, which emphasize the effectiveness of CT in improving dynamic balance and reducing fall risk, may not be generalizable to other populations. Cultural, lifestyle, and physiological differences between regions may significantly influence exercise outcomes, highlighting the need for studies incorporating diverse populations. Consequently, while existing research highlights the benefits of CT in improving balance among older adults, further studies are required to assess its applicability across diverse demographic and cultural settings. This would provide more comprehensive insights into its global relevance and clinical utility.
This meta-analysis evaluates the impact of CT on balance performance in older adults and examines factors contributing to heterogeneity across studies. Additionally, it reviews the existing literature, highlights methodological and contextual limitations, and provides actionable recommendations for future studies. The findings provide critical insights for older adult health management, the design of exercise interventions, and the development of evidence-based public health policies. These findings will inform clinical practices and assist policymakers in formulating targeted strategies to prevent falls and enhance the quality of life among older adults.
2 Methods
There was adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines throughout the entire process of conducting this systematic review (27), and the review protocol has been registered on Inplasy.com (INPLASY202412006).
2.1 Search strategy
Prominent academic databases were considered to search the related literature, including PubMed, EBSCOhost, Embase, Cochrane Library, Web of Science, as well as supplementary searches through the Google Scholar search engine, until 30th Nov 2024. For each independent database, a strategic search query was conducted by the title and abstract (Supplementary Table S1). The primary keywords considered for gathering related studies were: (“core strength training” OR “core-muscle training” OR “core training” OR “core-stability exercise” OR “core exercise”) AND (“balance” OR “static balance” OR “dynamic balance” OR “functional balance” OR “postural balance”) AND (“old” OR “aged” OR “senior” OR “elder”).
2.2 Eligibility criteria
The literature search was conducted using the PICOS framework. To be deemed eligible, studies were required to satisfy all the inclusion criteria specified (Table 1). The inclusion criteria were: (a) participants were healthy older adults with a mean age ≥ 60 years; (b) CT should be specifically isolated and explicitly discussed, with a minimum intervention duration of 4 weeks; (c) the comparison in studies should be either single-group or multiple-group trials; (d) The study outcomes must include the assessment of at least one behavioral balance outcome; (e) articles must be written in English and adhere to an experimental design, including single-group trials or randomized controlled trials.
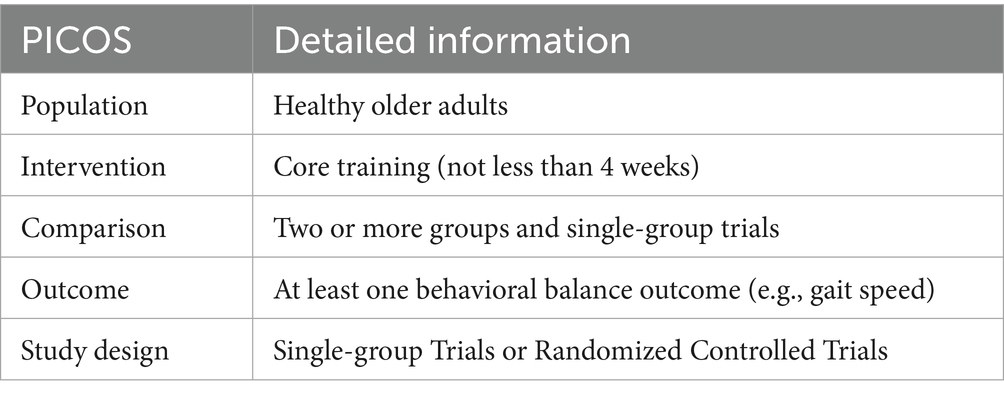
Table 1. PICOS eligibility criteria.
Studies were excluded if they met any of the following conditions: (a) non-original or grey literature, including reviews, dissertations, conference abstracts, or technical reports, as these sources generally lack peer review and standardized reporting, which may increase the risk of bias; (b) absence of outcome indicators directly related to balance performance; (c) duplicate publications or repeated analyses, in which case the most recent or methodologically rigorous version was retained; (d) unavailability of the full text, which prevented quality assessment and data extraction; (e) articles not published in English, excluded to maintain methodological consistency and avoid misinterpretation due to language barriers; (f) insufficient data reporting, specifically studies that did not provide both mean and standard deviation for balance outcomes and where such information could not be extracted or obtained from the authors; (g) study populations involving older adults with conditions such as significant cognitive impairments (e.g., Alzheimer’s disease, dementia), major orthopedic disorders (e.g., lower limb fractures), neurological diseases (e.g., stroke, Parkinson’s disease), or other comorbidities that substantially restricted mobility; and (h) unpublished studies, which often lack methodological transparency and accessible data, making them unsuitable for reliable meta-analytic synthesis.
2.3 Selection process
All records retrieved from the databases were imported into reference management software (EndNote X9). An independent researcher (YZ) identified and removed duplicate entries. The remaining records were subsequently screened according to predefined inclusion and exclusion criteria. A two-step screening process was conducted by the primary researchers (WG and YZ). The first step involved an initial assessment based on titles and abstracts, followed by a second phase of full-text screening. Study eligibility was evaluated using the PICOS framework. Figure 1 illustrates the details of the selection procedure.
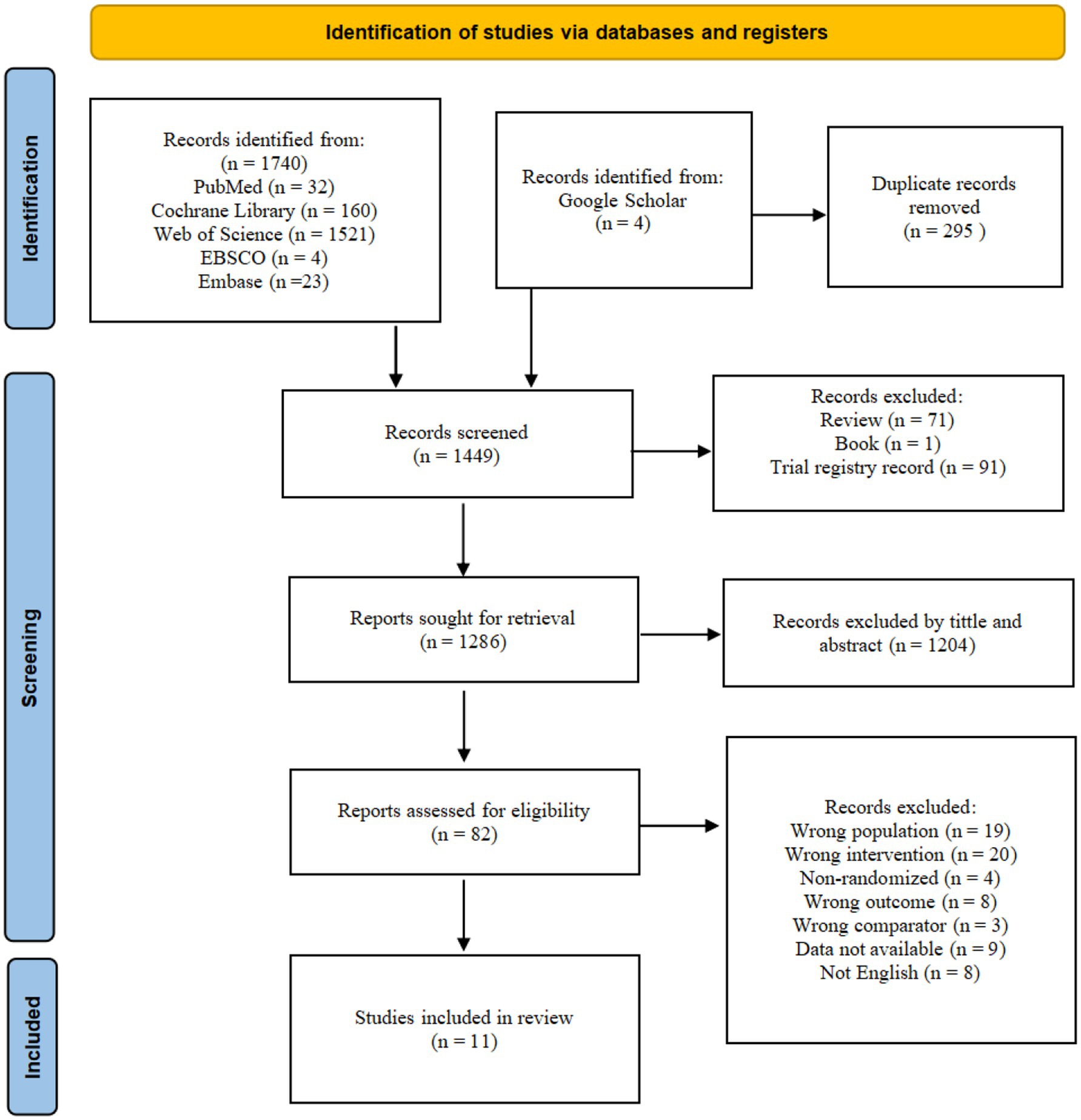
Figure 1. Summary Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart identifying the study selection process.
2.4 Data extraction
Data extraction was conducted independently by two authors (WG and PC) using a standardized data extraction form. The extracted information included the general characteristics of the studies (authors, publication year, and country where the study was conducted), participant characteristics (age, gender, and the number of participants in each group), detailed information about the intervention group (CT type, frequency, intensity, and duration), detailed information about the control group (type, frequency, intensity, and duration of training), outcome measures, and primary results. Any discrepancies during the extraction process were resolved through discussion between the authors.
2.5 Risk of bias
Two reviewers (YZ and WG) independently appraised the risk of bias for each included study using the Cochrane Risk of Bias 2 (RoB 2) tool (28). The assessment covered five domains: the randomization process, deviations from intended interventions, missing outcome data, measurement of outcomes, and selection of the reported result. Prior to the formal assessment, the reviewers completed a calibration exercise on a subset of studies to harmonize interpretations of RoB 2 signaling questions and to agree on explicit decision rules for domain-level judgments. Discrepancies at the item or domain level were reconciled through structured discussion with reference to the RoB 2 guidance. If consensus could not be reached, a third author (PC) was consulted to conduct further evaluation and provide the final judgment. All decisions were documented with concise rationales, and overall risk-of-bias ratings were derived from domain-level judgments according to the RoB 2 algorithm.
2.6 Data analysis
Balance outcomes were categorized into static balance, dynamic balance, or a combination of both. Dynamic balance test (DBT) was defined as the ability to maintain stability while moving through space, regardless of whether foot movement was involved (e.g., GT, FRT, TUG Test). Static balance test (SBT) referred to the ability to maintain an upright posture with both feet in full contact with the ground (e.g., OLST, Balance Board Test). Studies included in the meta-analysis were required to report outcome measures that effectively reflected changes in balance.
The mean (M), standard deviation (SD), and sample size (N) of the outcome measures from the included studies were recorded. These data, based on either post-intervention values for the experimental and control groups or pre- and post-intervention differences, were recorded in Microsoft Excel (Microsoft 2016, Santa Rosa, California) for meta-analysis. Statistical analyses of the outcome measures were conducted using Review Manager software version 5.4.
Initially, a heterogeneity test was performed using the I2 statistic to evaluate the degree of heterogeneity across studies. According to the Cochrane Handbook, no heterogeneity is indicated when I2 = 0, and a fixed-effects model is employed for I2 < 50%. Conversely, a random-effects model is used if I2 > 50%. For studies with consistent outcome measurement units, mean difference (MD) was used as the effect size; otherwise, standardized mean difference (SMD) was applied. Both were calculated with 95% confidence intervals, and results were considered statistically significant at p < 0.05. Subgroup analyses were conducted to explore the sources of heterogeneity in the effects of CT on balance outcomes. Finally, the present study employed Begg’s rank correlation method and Egger’s linear regression method within Stata 17.0 to assess publication bias, with trim and fill methods applied to address any significant publication bias detected (29, 30).
3 Results
3.1 Study selection
Figure 1 presents the PRISMA flow diagram, illustrating the detailed screening process. An initial database search identified a total of 1,740 articles, with 4 additional articles retrieved from Google Scholar. After removing duplicates, reviews, books, and trial records, 1,286 articles remained for screening based on titles and abstracts. Subsequently, 82 full-text articles were reviewed for eligibility, resulting in the inclusion of 11 studies (12, 31–40).
3.2 Study characteristics
The studies reviewed, published between 2005 and 2024, span a period of 20 years, with their characteristics summarized in Table 2. These studies were conducted in various geographical regions, including Italy, Germany, South Korea, the United States, Spain, France, and Iran, collectively involving 442 older adults. The key characteristics of the studies are as follows: (1) Gender: Four studies specifically focused on female participants (32, 34, 37, 38), while the remaining studies included mixed-gender samples. (2) Age: All studies reported the age of participants, with an age range of 60 to 85 years identified across the eight studies. (3) Interventions: In terms of interventions, eight studies employed CT methods, such as core muscle training, core instability strength training, core resistance training, or core stability training (12, 31–35, 39, 40). The remaining three studies incorporated Pilates-based CT approaches (36–38). (4) Training frequency: All studies reported the frequency of training sessions, which ranged from 1 to 3 sessions per week. (5) Duration per Session: The duration of each training session varied between 20 and 60 min across all studies. (6) Intervention duration: All included studies reported the total intervention duration, ranging from 6 to 18 weeks. (7) Outcome measures: The studies predominantly employed well-established balance assessment methods, such as GT (32, 33, 36, 37), the TUG test (33, 35, 38), FRT (12, 31, 33, 36), and OLST (32, 35, 38).
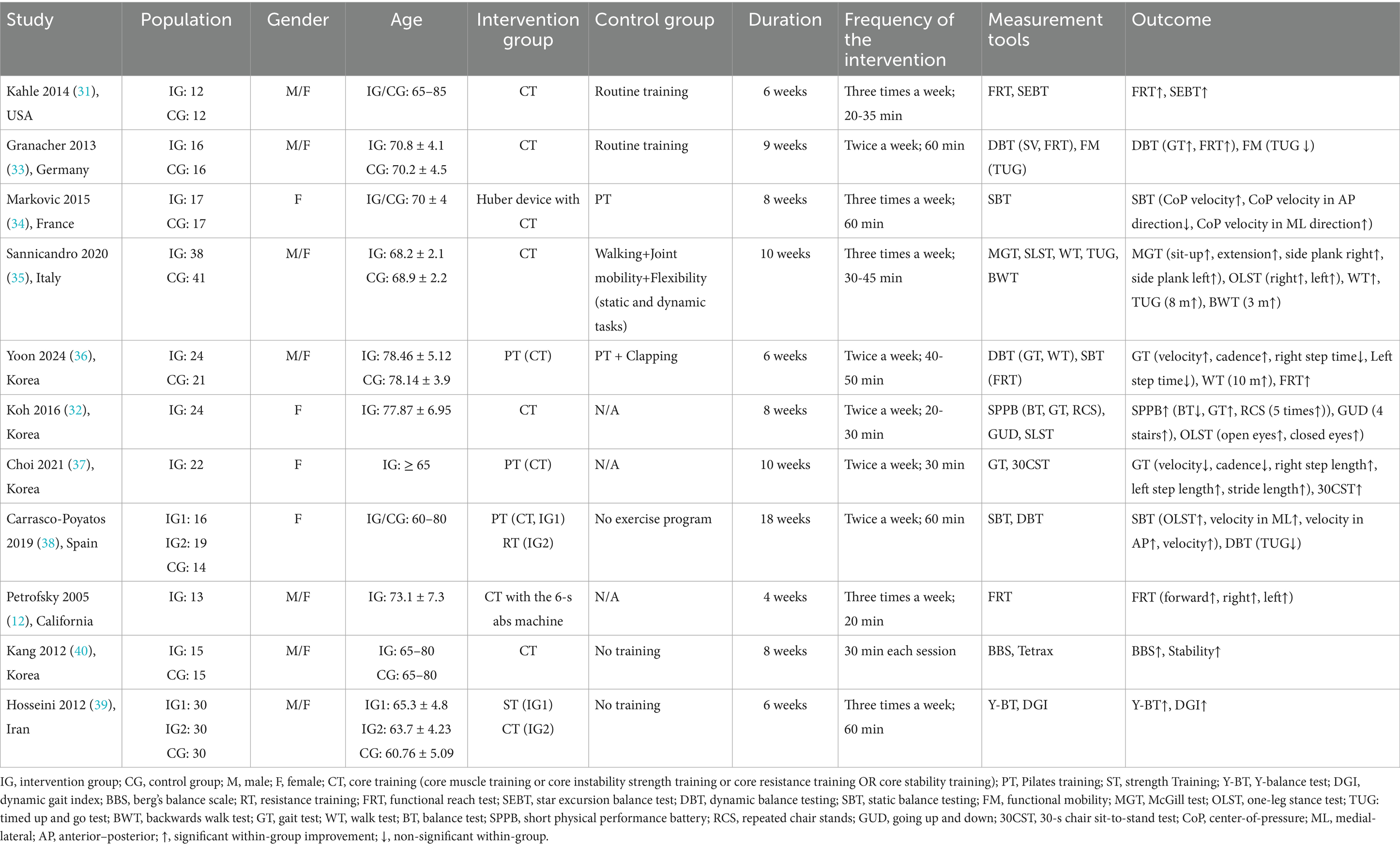
Table 2. Study characteristics.
In addition to these primary assessment tools, several studies employed alternative tests to evaluate various dimensions of balance and physical performance. These included the Star Excursion Balance Test (SEBT), Center-of-Pressure (CoP) test, Backward Walk Test (BWT), Short Physical Performance Battery (SPPB), Repeated Chair Stands (RCS), Going Up and Down (GUD), Strength Training (ST); Y-Balance Test (Y-BT); Dynamic gait index (DGI); Berg’s balance scale (BBS) and the Chair Sit-to-Stand Test (CST).
3.3 Risk of bias
The risk of bias assessment for individual studies, conducted using the RoB 2 tool, is depicted in Figure 2, while Figure 3 provides an aggregate overview of the overall risk of bias across all included studies. In these visualizations, green indicates low risk, yellow denotes some concerns, and red signifies high risk of bias. Regarding biases in the randomization process, seven studies explicitly reported their randomization methods, ensuring transparency and reliability. In contrast, four studies lacked sufficient details (12, 32, 35, 37), with three of them (12, 32, 37) employing single-group designs, leading to a high-risk rating. Deviations from intended interventions posed unique challenges in exercise training research due to the direct involvement of participants in interventions and the frequent dual role of researchers as outcome assessors. While only three studies (34, 37, 38) explicitly implemented blinding procedures, the lack of such measures in the remaining studies did not appear to influence outcomes. For missing outcome data, all studies were rated as low risk, indicating that the absence of data did not substantially impact the results. However, in the domain of bias related to outcome measurement, four studies (32, 35, 36, 40) did not clearly address whether outcome measurement differed between groups. In terms of selective reporting bias, all studies were assessed as low risk, reflecting adequate reporting practices. Regarding overall bias, five studies (31, 33, 34, 38, 39) demonstrated a low risk of bias. Meanwhile, three studies (35, 36, 40) raised some concerns, and three study (12, 32, 37) was identified as having a high risk of bias.
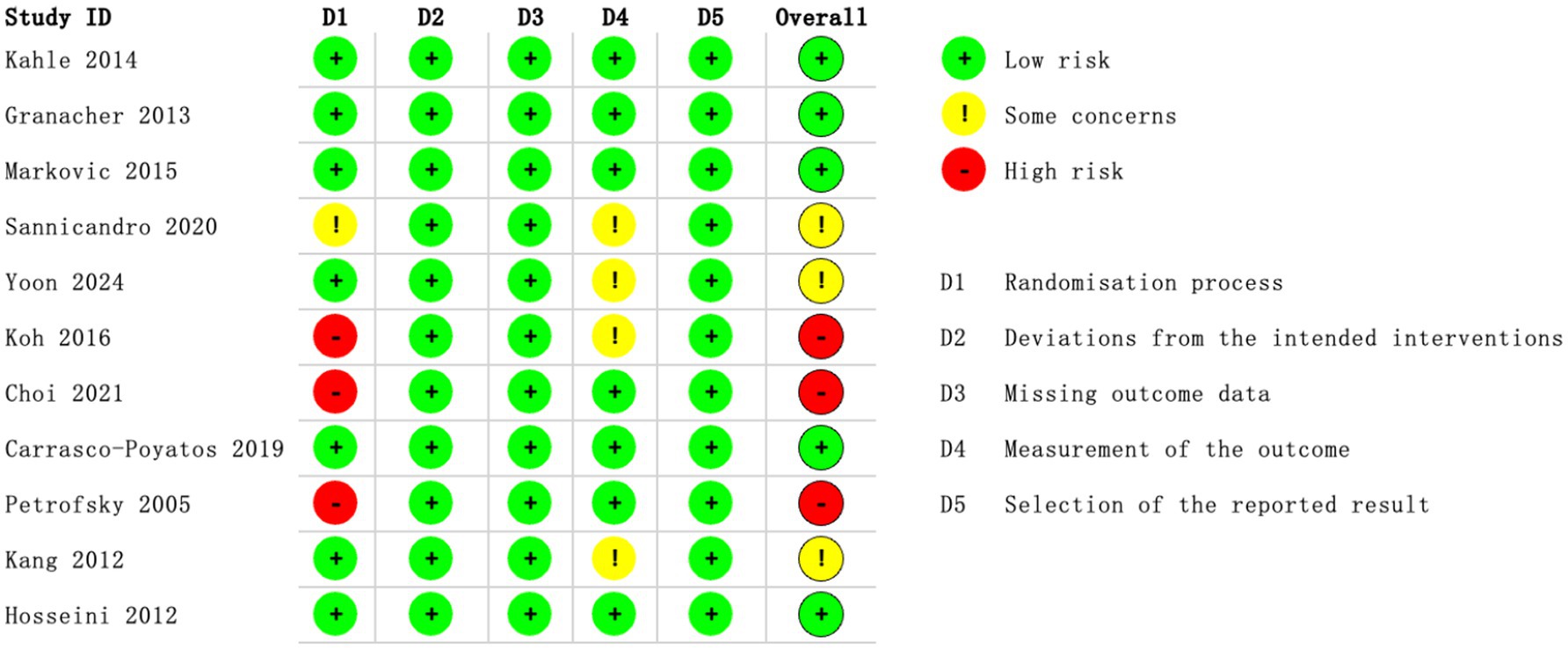
Figure 2. Risk of bias summary: methodological quality of each item for the each included study.
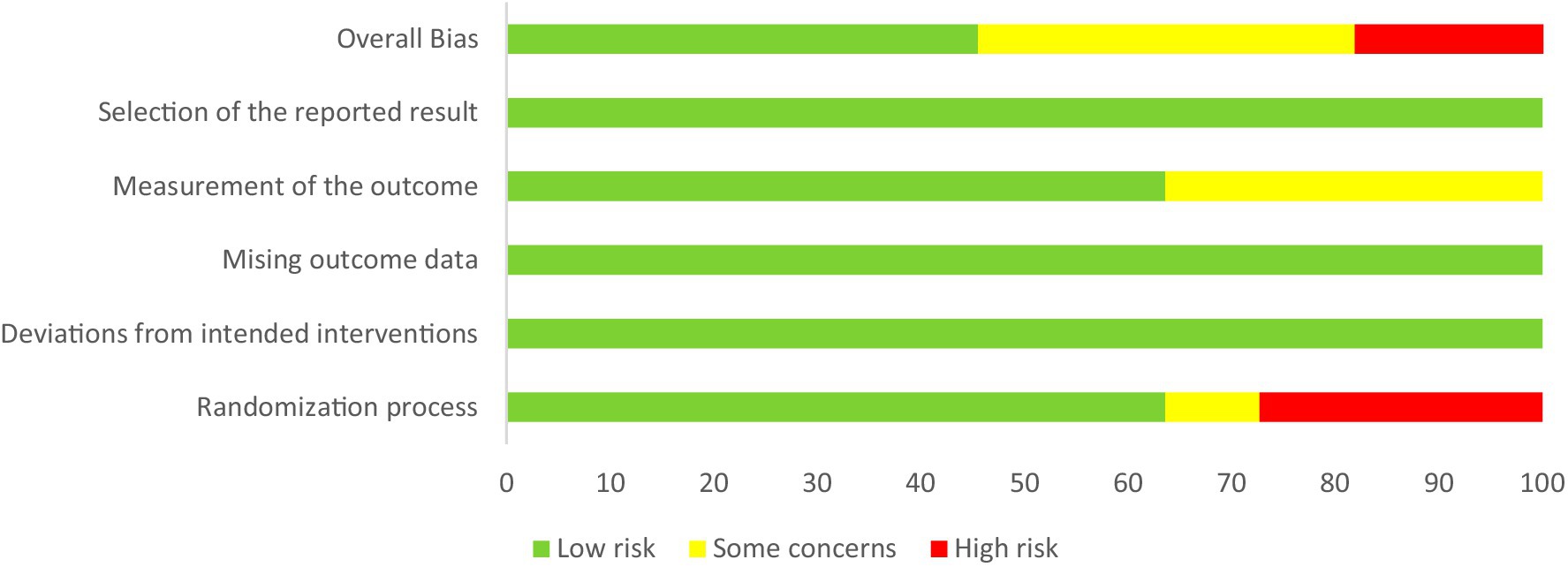
Figure 3. Risk of overall bias.
3.4 Meta-analysis results
A total of eleven studies were included in the meta-analysis, focusing on outcome measures related to both dynamic and static balance. For DBT, three specific assessments were examined: the GT, reported in four studies (32, 33, 36, 37); the FRT, included in Four studies (12, 31, 33, 36); and the TUG Test, also evaluated in three studies (33, 35, 38). For SBT, the OLST was analyzed across three studies (32, 35, 38). These outcome measures collectively provide a robust framework for evaluating the effects of CT interventions on balance, encompassing both dynamic and static dimensions, and offering a comprehensive synthesis of evidence across the included studies.
3.4.1 Effect of CT on DBT (GT velocity, FRT distance, and TUG time)
Four studies (n = 169) (32, 33, 36, 37) examined the effect of CT on GT velocity in older adults. As illustrated in the Figure 4, I2 = 28%, indicating moderate heterogeneity, and a fixed-effects model was applied. The meta-analysis demonstrated an (SMD = 0.32; 95%CI = 0.02, 0.63; p < 0.05). These findings suggest that CT significantly improves GT velocity in older adults, with the experimental group outperforming the control group.

Figure 4. Forest plot of CT on GT.
Four studies (n = 127) (12, 31, 33, 36) investigated the effect of CT on FRT distance in older adults. As shown in the Figure 5, I2 = 0%, indicating low heterogeneity, and a fixed-effects model was applied. The meta-analysis yielded an (SMD = 0.82; 95%CI = 0.50, 1.24; p < 0.00001). These results indicate that CT significantly improves FRT distance in older adults, with the experimental group demonstrating superior performance compared to the control group.

Figure 5. Forest plot of CT on FRT.
Three studies (n = 141) (33, 35, 38) explored the effect of CT on TUG time in older adults. As illustrated in the Figure 6, I2 = 78%, indicating substantial heterogeneity, and a random-effects model was employed. The meta-analysis revealed an (SMD = −0.81; 95% CI = −1.62, 0.00; p = 0.05). These findings suggest that CT significantly improves TUG time in older adults, with the experimental group showing superior performance compared to the control group.

Figure 6. Forest plot of CT on TUG.
3.4.2 Effect of CT on SBT (OLST time)
Three studies (n = 157) (32, 35, 38) evaluated the effect of CT on OLST time in older adults. As depicted in the Figure 7, I2 = 0%, indicating no heterogeneity, and a fixed-effects model was applied. The meta-analysis showed an (MD = 3.19; 95% CI = 1.74, 4.64; p < 0.001). These results demonstrate that CT significantly enhances OLST time in older adults, with the experimental group performing better than the control group.
![Forest plot comparing experimental and control groups from three studies: Carrasco-Poyatos 2019, Koh 2016, and Sannicandro 2020. The mean differences with 95% confidence intervals are shown, with overall mean difference being 3.19 [1.74, 4.64]. The heterogeneity is low with Chi-squared = 1.65, df = 2 (P = 0.44); I-squared = 0%. The overall effect test shows Z = 4.32 (P < 0.0001), indicating a favor towards the experimental group.](https://www.frontiersin.org/files/Articles/1661460/fpubh-13-1661460-HTML-r1/image_m/fpubh-13-1661460-g007.jpg)
Figure 7. Forest plot of CT on OLST(s).
3.5 Subgroup analysis
In this study, subgroup analyses were performed for DBT, the TUG test, and GT to explore the sources of heterogeneity in the outcome measures.
The results suggest that the type of DBT assessment method significantly contributes to the observed heterogeneity in DBT outcomes (Figure 8). Specifically, the subgroup using the FRT exhibited a statistically significant effect (SMD = 0.82; 95%CI = 0.50, 1.24; p < 0.00001; I2 = 0%), as did the TUG subgroup (SMD = −0.81; 95% CI: −1.62, 0.00; p = 0.05; I2 = 78%). In contrast, the GT subgroup did not demonstrate a statistically significant result (SMD = 0.33; 95% CI: −0.03, 0.69; p = 0.07; I2 = 28%). These findings indicate that the variability in DBT outcomes is likely due to the differences in the assessment methods used. Notably, CT had the most pronounced effect on FRT performance in older adults, while its impact on TUG and GT was less significant.
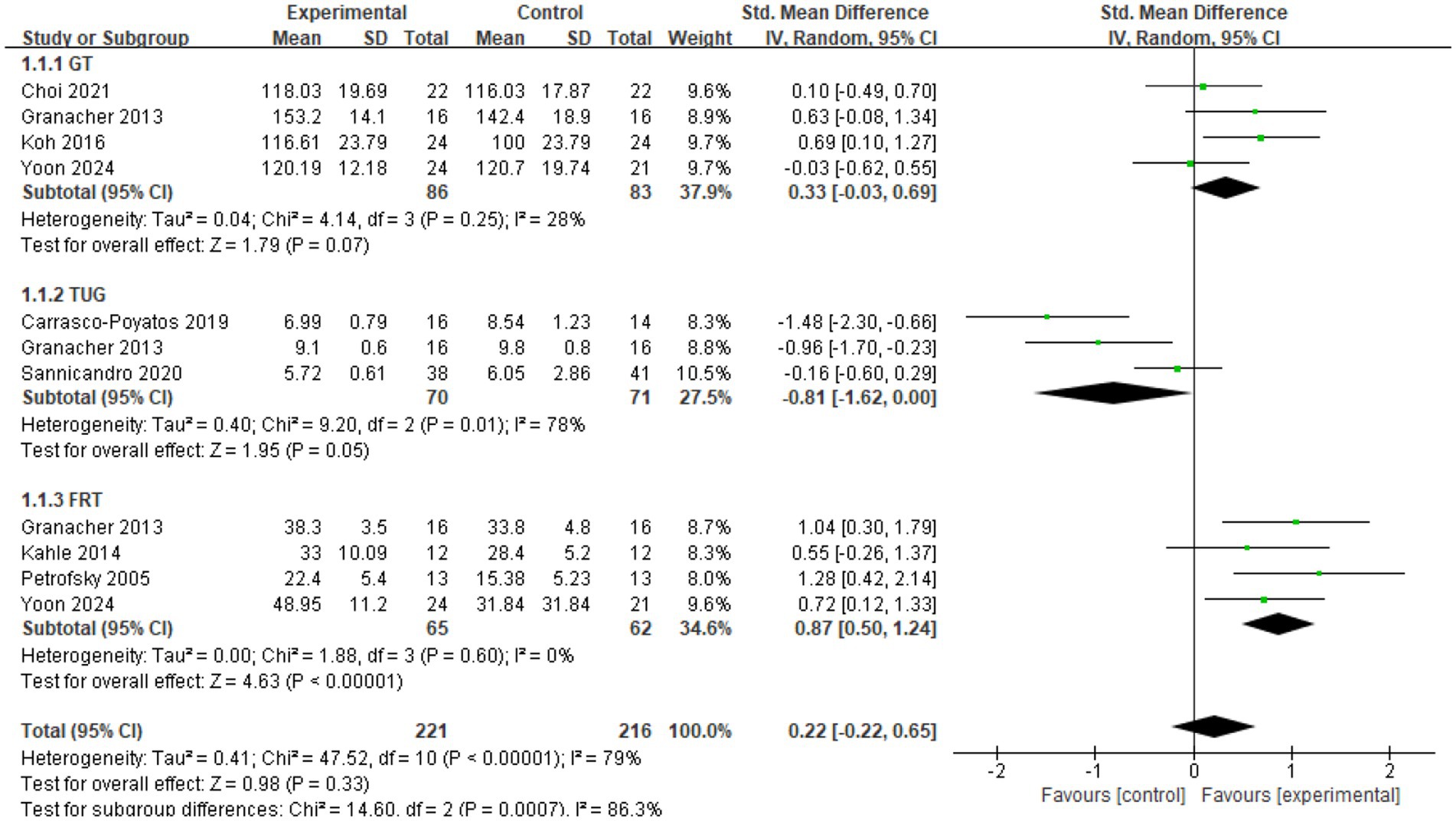
Figure 8. Subgroup analysis of DBT.
The analysis also revealed that intervention duration plays a key role in the heterogeneity observed in the TUG outcome measure (Figure 9). When participation duration was considered, the subgroup with an intervention time of ≥45 min demonstrated a significant effect (SMD = −1.20; 95% CI: −1.74, −0.65; p < 0.0001; I2 = 0%). This choice of 45 min was not arbitrary; earlier meta-analyses on balance training, as well as reviews of Tai Chi and Pilates, have repeatedly demonstrated that programs with sessions of at least this length are more likely to produce meaningful improvements in postural stability among older adults (19, 23, 41). Drawing on this body of evidence, we applied 45 min as a practical and evidence-based threshold for subgrouping in the present study. However, the subgroup with an intervention time of <45 min did not show statistically significant results (SMD = −0.16; 95% CI: −0.60, 0.29; p = 0.49). The overall effect size was calculated as (SMD = −0.81; 95% CI: −1.62, 0.00; p = 0.05). These findings underscore the importance of intervention duration in the variability of TUG outcomes. The subgroup with a longer intervention duration (≥45 min) exhibited a significantly higher effect size, suggesting that extended training periods have a more substantial impact on TUG performance. This highlights the advantages of longer training sessions over shorter ones in improving balance through CT, particularly for older adults.
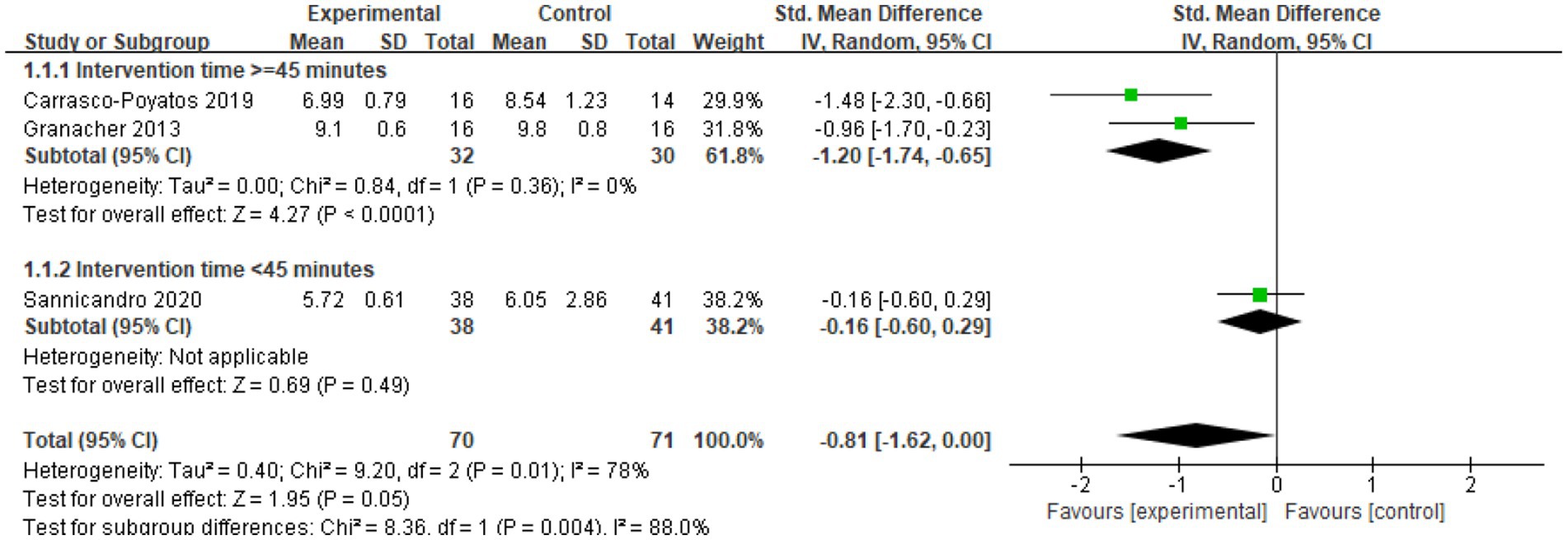
Figure 9. Subgroup analysis of TUG.
Finally, the analysis of intervention types revealed that different approaches to intervention contribute significantly to the heterogeneity observed in GT outcomes (Figure 10). The CT subgroup demonstrated a statistically significant effect (SMD = 0.66; 95% CI: 0.21, 1.12; p < 0.005; I2 = 0%), whereas the PT subgroup did not show statistically significant results (SMD = 0.04; 95% CI: −0.38, 0.45; p > 0.05; I2 = 0%). The overall effect size was calculated as (SMD = 0.32; 95% CI: 0.02, 0.63; p < 0.05). These findings suggest that the variation in GT outcomes is attributable to the type of intervention used. Importantly, the effectiveness of CT was substantially greater than that of PT, highlighting the stronger impact of CT interventions on GT performance in older adults.
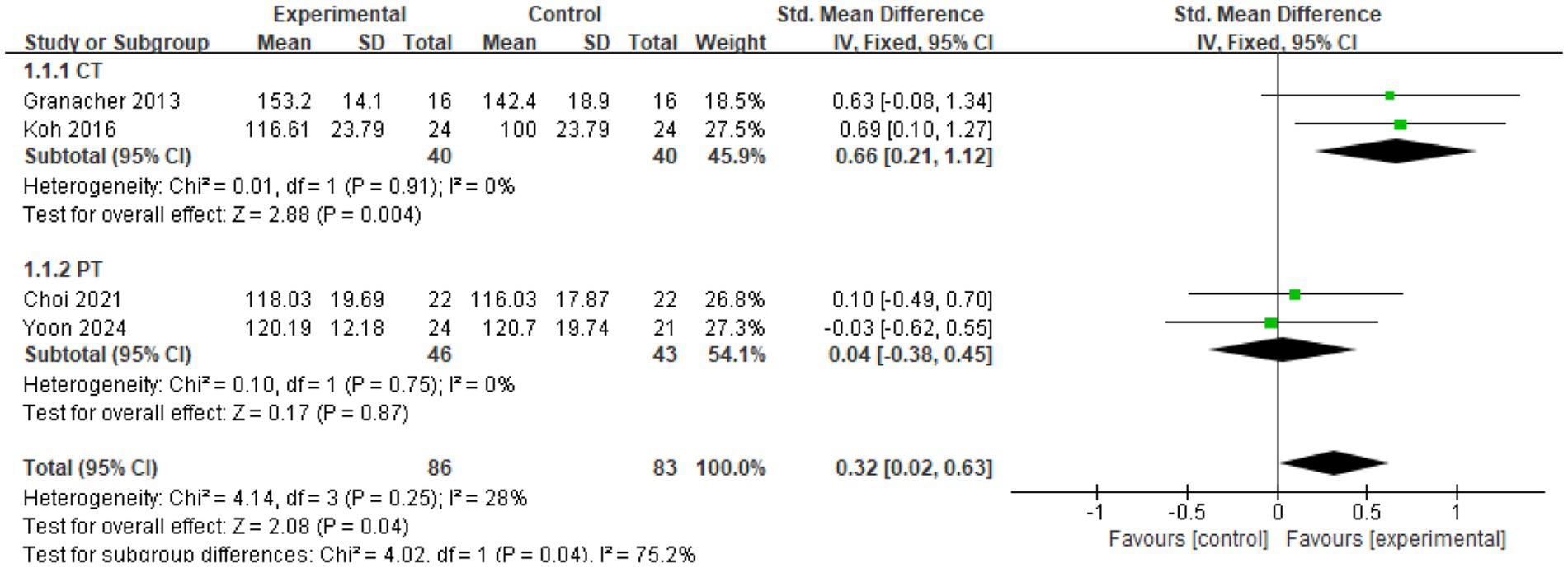
Figure 10. Subgroup analysis of GT.
3.6 Publication bias test
In this study, given the limited number of articles, publication bias was assessed using Begg’s rank correlation method and Egger’s linear regression method. A p-value exceeding 0.05 suggests minimal publication bias, whereas values below this threshold indicate substantial bias. The trim and fill method, which assesses and corrects for publication bias based on asymmetry in funnel plots, was employed to mitigate the impact of bias on the meta-analysis results. This method involves adding “missing” studies to the funnel plot to balance the graphic representation, thereby reducing the influence of publication bias.
Table 3 presents the publication bias assessment for this research. For GT, FRT, OLST, and DBT, both Begg’s and Egger’s test values were above 0.05, suggesting little evidence of publication bias. However, for the TUG outcome, Egger’s test was significant (p = 0.01), while Begg’s test remained non-significant (p = 0.30), indicating a potential risk of bias. Subsequent application of the trim-and-fill method revealed that Hedges’s g shifted from −0.81 (95% CI: −1.59, −0.03) to −0.16 (95% CI, −1.10, 0.79) after imputing missing studies (Table 4). This adjustment substantially attenuates the effect size, suggesting that the observed benefit on TUG performance may have been overestimated and should therefore be interpreted with caution.
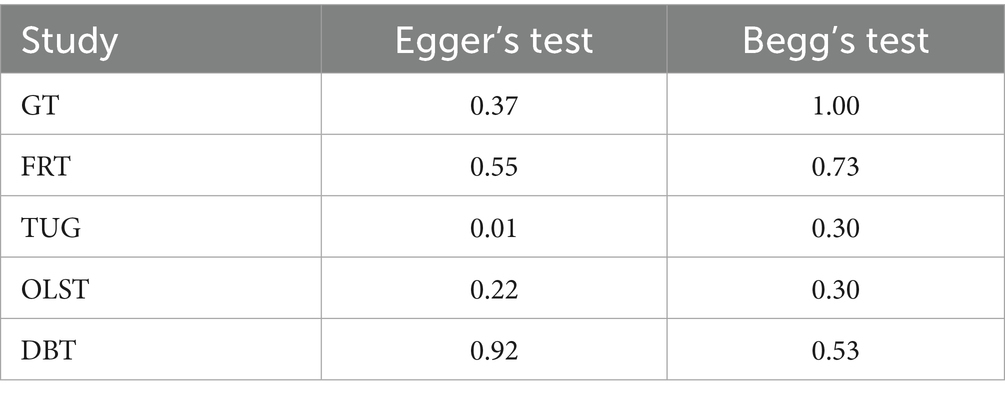
Table 3. Publication Bias Test.
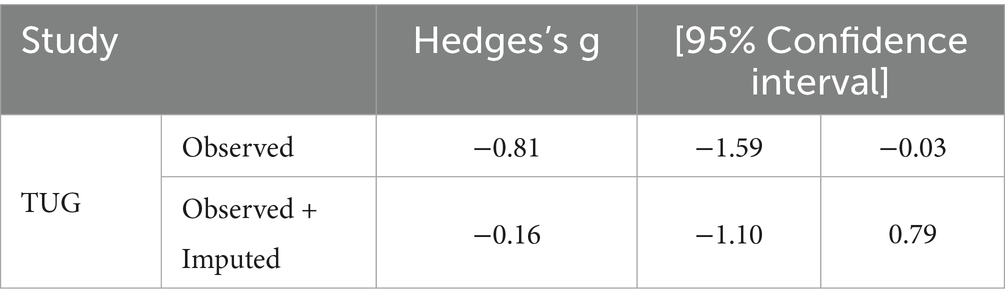
Table 4. Trim and fill method.
4 Discussion
4.1 Study findings
This study conducted a systematic review and meta-analysis to evaluate the effects of CT on balance performance in older adults. The findings demonstrate a significant positive impact of CT on balance, particularly in both dynamic and static balance assessments. Specifically, CT not only yielded beneficial effects in the short term, but these improvements were consistently observed across multiple balance measures. The results indicate that CT significantly enhanced balance in older adults, particularly in dynamic balance assessments such as the FRT, the TUG test, and GT, as well as in static balance assessments like the OLST. These findings highlight the crucial role of CT in enhancing multidimensional balance abilities.
4.2 The impact of CT on balance performance in older adults
Subgroup analyses revealed that CT had the most pronounced effect on dynamic balance in the FRT. This outcome is likely attributable to the critical role of core muscles in controlling the center of mass and maintaining trunk stability. The FRT requires older adults to manage their center of mass while leaning forward, and CT enhances the strength and stability of the core muscles, thereby significantly improving performance in this dynamic balance task. In contrast, the effects of CT were less pronounced in the GT and the TUG test. For the TUG outcome, the results warrant cautious interpretation. Egger’s test indicated significant funnel asymmetry (p = 0.01), and when the trim-and-fill method was applied, the pooled effect declined from −0.81 to −0.16, with the confidence interval spanning zero (Tables 3, 4). These findings suggest that, once potential missing studies are considered, the benefit of CT for TUG is less certain. It is also worth noting that gait control depends not only on core stability but also on lower-limb strength and motor coordination, which may help explain the comparatively modest effects of CT on GT and TUG.
Further analysis showed that training sessions lasting more than 45 min yielded better results in dynamic balance. This finding may be linked to the relationship between training duration and neuromuscular adaptation. Longer sessions provide participants with more opportunities for repeated practice, which not only strengthens the core muscles but also enhances the nervous system’s ability to coordinate and remember movement patterns (42). For older adults, extended training times contribute to improved neuromuscular coordination, enabling more precise control over body movements, thereby enhancing overall balance. Conversely, shorter training sessions may not allow for sufficient neuromuscular adaptation. CT requires prolonged stimulation to activate muscle groups and induce adaptive changes and short sessions may only lead to basic strength gains without improving complex dynamic balance capabilities (10). Extending the training duration enhances not only core muscle strength but also the body’s ability to adapt to a variety of movement challenges, which is especially critical for dynamic balance. Dynamic balance requires maintaining stability in an ever-changing environment, and this ability is often best achieved through sustained, long hours of training.
In terms of different intervention types, CT showed superior effects on GT compared to PT. This result is theoretically supported, as gait performance is closely related to dynamic body control, particularly in terms of step coordination, stride length, and gait symmetry. CT enhances the stability of the trunk, hips, abdomen, and back muscles, which in turn improves the stability of these regions during gait. A stable core effectively regulates lower limb movement, preventing unnecessary energy expenditure and unbalanced movement patterns, thus enhancing gait efficiency and stability. While Pilates also emphasizes core strength, its focus on flexibility, breath control, and body awareness may be less effective than CT in improving core strength and stability.
In comparison to the existing literature, the results of this study corroborate several previous findings. Previous research (43) similarly reported significant improvements in balance following CT, particularly in dynamic balance tasks. Strengthening the core musculature enables older adults to markedly enhance their balance control, a conclusion that closely aligns with our findings. Moreover, this study is the first to perform a systematic review across diverse cultural contexts, thus broadening the scope of the existing literature. While similar results were reported in Wang Hangping’s study (262,019), which primarily focused on a specific regional and age group, our research, by synthesizing data from various geographical and demographic groups, offers more generalized conclusions, further substantiating the positive effects of CT on balance in older adults.
4.3 The potential physiological mechanisms of CT on balance performance in the older adult
From a mechanistic perspective, CT effectively strengthens the core musculature, particularly the abdominal and lumbar muscles, which are essential for overall body stability and postural control (44). By enhancing core strength, older adults become better equipped to maintain stable postures, especially during standing or walking, thereby reducing the risk of falls. The beneficial effects on balance may be attributed to improvements in self-support capacity, postural adjustments, and coordination across various body segments. From a neurological standpoint, long-term engagement in such training not only increases muscle strength but also optimizes the adaptive capacity of the nervous system, thereby enhancing control over movement tasks in older adults (42). Studies in older adults have provided direct evidence that CT induces measurable physiological changes, such as hypertrophy of trunk muscles, improvements in isometric trunk strength, and enhanced neuromuscular control, thereby lending empirical support to these proposed mechanisms (33). Strengthened core musculature improves the feedback mechanisms within the nervous system that regulate postural adjustments, enabling older individuals to stabilize their balance rapidly in unstable conditions, contributing to enhanced dynamic balance performance. Furthermore, core-focused exercises may enhance proprioception, enabling quicker responses to instability (45). This mechanism is critical for both static and dynamic balance assessments and is particularly valuable in daily activities, where this type of training significantly enhances stability and independence.
This study not only provides empirical evidence for the effects of CT on balance in older adults but also contributes to the advancement of exercise physiology and training theory. Much of the existing literature has predominantly focused on the effects of CT in younger athletes (46, 47), whereas this study expands the scope by examining its unique benefits for the older population. Furthermore, this research provides new evidence supporting the “functional training theory,” which posits that exercise interventions should emphasize enhancing functional abilities relevant to daily life, such as balance, stability, and coordination (48). Our findings demonstrate that CT significantly improves balance in older adults, particularly dynamic balance, thereby validating the functional training theory and bolstering its practical application in promoting older adult health.
4.4 The potential of CT for practical enhancement in older adult care
From a practical perspective, CT has been shown to significantly improve balance, particularly dynamic balance. As such, it should be adopted as a standard intervention to enhance stability and prevent falls among older adults. Policymakers can utilize the findings of this study to integrate CT into health promotion initiatives targeting older populations, thereby facilitating improvements in their overall quality of life. Beyond its role in improving balance, this intervention also enhances independence in daily activities. Given the mobility challenges and heightened fall risk faced by this demographic, CT empowers older adults to perform routine tasks with greater confidence. Consequently, educators and community service organizations should actively advocate for its implementation as a critical component of programs designed to promote health and quality of life in the older adult.
4.5 Limitation and future research
While this study contributes to the understanding of CT and balance in older adults, several limitations should be considered when interpreting the findings. A small number of the included trials adopted single-group designs, which may reduce the strength of causal inferences. Although strict data extraction procedures were applied, the possibility of publication bias cannot be excluded. Results from the trim-and-fill analysis suggested that this bias may have influenced the pooled estimates to some extent, though the overall conclusions appear relatively stable.
Although heterogeneity was systematically examined and prespecified subgroup analyses were conducted, the limited number of included studies precluded meta-regression, which restricts the ability to quantify moderator effects more precisely. Moreover, the relatively small number of available trials means that some results should be interpreted with caution, as the restricted evidence base may reduce the stability and generalizability of the findings.
The methodological quality of the included studies also reflects the typical challenges of exercise intervention research. Blinding procedures were often difficult to implement, and sample sizes tended to be modest, which may limit statistical precision and increase the likelihood of small-study effects. Furthermore, the evidence base is weighted toward short-term interventions, offering limited information on whether the benefits of CT can be maintained over longer periods or translated into meaningful reductions in fall risk.
Variation in intervention protocols represents another limitation. Differences in training intensity, session length, adherence monitoring, and reporting practices complicate direct comparisons across studies and make it difficult to determine optimal training parameters. Regarding subgroup analyses, the 45-min threshold had already been justified earlier on the basis of prior research, and in this context was applied pragmatically to distinguish between shorter and longer training sessions. Nonetheless, residual heterogeneity is likely shaped by factors beyond duration and intervention type, including participants’ baseline balance capacity, intervention settings, adherence levels, and even differences in outcome measurement procedures, such as walkway length in the TUG or arm positioning in the OLST. In addition, some subgroup comparisons were based on relatively few studies, which restricts the precision of estimates and raises the possibility of small-study effects.
Finally, cultural and geographical concentration of the included studies may limit the broader applicability of the findings, as exercise behaviors and responses are often shaped by social norms, healthcare systems, and lifestyle contexts.
Taken together, these limitations highlight the need for future trials to recruit larger and more diverse samples, implement standardized intervention protocols, and extend follow-up durations to evaluate the long-term sustainability of training effects. Expanding research across varied cultural contexts would further enhance the generalizability of findings and provide a more comprehensive picture of how CT contributes to balance and fall prevention in older adults.
5 Conclusion
This systematic review and meta-analysis provides an in-depth examination of the effects of CT on balance performance in older adults. The findings demonstrate significant improvements across dynamic and static balance measures, including GT, FRT, TUG and OLST. Nevertheless, the TUG results should be interpreted with caution. These results highlight the efficacy of CT as a targeted intervention for enhancing balance and reducing fall risk in this vulnerable population. This study contributes to the growing body of literature advocating CT as a crucial component in improving health outcomes for older adults. The findings hold particular relevance for clinicians and practitioners designing rehabilitation programs, especially those focused on promoting balance and fall prevention.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Author contributions
YZ: Investigation, Conceptualization, Writing – original draft, Writing – review & editing, Methodology, Validation. WG: Software, Investigation, Data curation, Project administration, Validation, Methodology, Writing – original draft, Formal analysis, Writing – review & editing. PC: Writing – review & editing, Investigation, Validation, Methodology. YW: Supervision, Writing – review & editing, Conceptualization, Writing – original draft, Methodology.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We are especially grateful to all the participants who actively participated in this study and to the School of Physical Education and Arts of Jiangxi University of Science and Technology for their strong support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1661460/full#supplementary-material
References
1. World Health Organization. Ageing and health. (2021). Available online at: https://www.who.int/zh/news-room/fact-sheets/detail/ageing-and-health (Accessed March 15, 2025).
2. Wang, J, Li, Y, Yang, GY, and Jin, K. Age-related dysfunction in balance: a comprehensive review of causes, consequences, and interventions. Aging Dis. (2025) 16:714–37. doi: 10.14336/AD.2024.0124-1
3. World Health Organization. Falls. (2021). Available online at: https://www.who.int/zh/news-room/fact-sheets/detail/falls (Accessed March 15, 2025).
4. Wu, Y, Wang, GL, Nie, ZT, Liang, W, Du, Y, Li, Q, et al. Interpretation of the 2022 edition of the “world guidelines: prevention and management of falls in older adults”. Chin Gen Pract. (2023) 26:1171:1159–63. doi: 10.12114/j.issn.1007-9572.2022.0842
5. Pollock, AS, Durward, BR, Rowe, PJ, and Paul, JP. What is balance? Clin Rehabil. (2000) 14:402–6. doi: 10.1191/0269215500cr342oa
6. Sturnieks, DL, St George, R, and Lord, SR. Balance disorders in the elderly. Neurophysiol Clin. (2008) 38:467–78. doi: 10.1016/j.neucli.2008.09.001
7. Zhong, YJ, Meng, Q, and Su, CH. Mechanism-driven strategies for reducing fall risk in the elderly: a multidisciplinary review of exercise interventions. Healthcare (Basel). (2024) 12:2394. doi: 10.3390/healthcare12232394
8. Xu, Y. Impact of core fitness on balance performance in the elderly. Rev Bras Med Esporte. (2022) 28:713–5. doi: 10.1590/1517-8692202228062022_0096
9. Ponde, K, Agrawal, R, and Chikte, NK. Effect of core stabilization exercises on balance performance in older adults. Int J Contemp Med. (2021) 9:12–7. doi: 10.37506/ijocm.v9i1.2926
10. McGill, S. Core training: evidence translating to better performance and injury prevention. Strength Cond J. (2010) 32:33–46. doi: 10.1519/SSC.0b013e3181df4521
11. Corbett, B. The effectiveness of Swiss ball training on balance in older adults [master’s thesis]. Melbourne (Australia): Victoria University (2005).
12. Petrofsky, JS, Cuneo, M, Dial, R, Pawley, AK, and Hill, J. Core strengthening and balance in the geriatric population. J Appl Res Clin Exp Ther. (2005) 5:423–33.
13. Arnold, C, Lanovaz, J, Oates, A, Craven, B, and Butcher, S. The effect of adding core stability training to a standard balance exercise program on sit to stand performance in older adults: a pilot study. J Aging Phys Act. (2015) 23:95–102. doi: 10.1123/japa.2013-0115
14. Borenstein, M, Hedges, LV, Higgins, JPT, and Rothstein, HR. Introduction to meta-analysis. Chichester (UK): Wiley (2021).
15. Murad, MH, Asi, N, Alsawas, M, and Alahdab, F. New evidence pyramid. Evid Based Med. (2016) 21:125–7. doi: 10.1136/ebmed-2016-110401
16. Barker, AL, Bird, ML, and Talevski, J. Effect of Pilates exercise for improving balance in older adults: a systematic review with meta-analysis. Arch Phys Med Rehabil. (2015) 96:715–23. doi: 10.1016/j.apmr.2014.11.021
17. Moreno-Segura, N, Igual-Camacho, C, Ballester-Gil, Y, Blasco-Igual, MC, and Blasco, JM. The effects of the Pilates training method on balance and falls of older adults: a systematic review and meta-analysis of randomized controlled trials. J Aging Phys Act. (2018) 26:327–44. doi: 10.1123/japa.2017-0078
18. Casonatto, J, and Yamacita, CM. Pilates exercise and postural balance in older adults: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Med. (2020) 48:102232. doi: 10.1016/j.ctim.2019.102232
19. Sampaio, T, Encarnação, S, Santos, O, Narciso, D, Oliveira, JP, Teixeira, JE, et al. The effectiveness of Pilates training interventions on older adults’ balance: a systematic review and meta-analysis of randomized controlled trials. Healthcare (Basel). (2023) 11:3083. doi: 10.3390/healthcare11233083
20. De Campos Júnior, JF, De Oliveira, LC, Dos Reis, AL, De Almeida, LIM, Branco, LV, and De Oliveira, RG. Effects of Pilates exercises on postural balance and reduced risk of falls in older adults: a systematic review and meta-analysis. Complement Ther Clin Pract. (2024) 57:101888. doi: 10.1016/j.ctcp.2024.101888
21. Li, L, Guo, S, Ding, B, and Zhang, J. Effectiveness of tai chi exercise on balance, falls, and motor function in older adults: a meta-analysis. Front Med. (2024) 11:1486746. doi: 10.3389/fmed.2024.1486746
22. Li, Y, Liu, M, Zhou, K, Dong, G, Manor, B, Bao, D, et al. The comparison between effects of Taichi and conventional exercise on functional mobility and balance in healthy older adults: a systematic literature review and meta-analysis. Front Public Health. (2023) 11:1281144. doi: 10.3389/fpubh.2023.1281144
23. Lesinski, M, Hortobágyi, T, Muehlbauer, T, Gollhofer, A, and Granacher, U. Effects of balance training on balance performance in healthy older adults: a systematic review and meta-analysis. Sports Med. (2015) 45:1721–38. doi: 10.1007/s40279-015-0375-y
24. Šarabon, N, and Kozinc, Ž. Effects of resistance exercise on balance ability: systematic review and meta-analysis of randomized controlled trials. Life (Basel). (2020) 10:284. doi: 10.3390/life10110284
26. Wang, HP, Nie, ZX, Sun, ZW, and Yuan, FM. Meta-analysis of core strength training on balance ability and fall risk prevention in middle-aged and older adults. Chin Geriatr. (2019) 20:5009–15.
27. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
28. Higgins, JPT, Thomas, J, Chandler, J, Cumpston, M, Li, T, Page, MJ, et al. Cochrane handbook for systematic reviews of interventions. 2nd ed. Chichester (UK): Wiley-Blackwell (2019).
29. Song, F, and Gilbody, S. Bias in meta-analysis detected by a simple, graphical test: increase in studies of publication bias coincided with increasing use of meta-analysis. BMJ. (1998) 316:471. doi: 10.1136/bmj.316.7129.471
30. Rothstein, HR, Sutton, AJ, and Borenstein, M. Publication bias in meta-analysis In: HR Rothstein, AJ Sutton, and M Borenstein, editors. Publication bias in meta-analysis. 1st ed. Chichester (UK): Wiley (2005). 1–7.
31. Kahle, N, and Tevald, MA. Core muscle strengthening’s improvement of balance performance in community-dwelling older adults: a pilot study. J Aging Phys Act. (2014) 22:65–73. doi: 10.1123/japa.2012-0132
32. Koh, K, Park, YS, Park, DW, Hong, CK, and Shim, JK. Development of core strength training equipment and its effect on the performance and stability of the elderly in activities of daily living. Korean J Sport Biomech. (2016) 26:229–36. doi: 10.5103/KJSB.2016.26.2.229
33. Granacher, U, Lacroix, A, Muehlbauer, T, Roettger, K, and Gollhofer, A. Effects of core instability strength training on trunk muscle strength, spinal mobility, dynamic balance and functional mobility in older adults. Gerontology. (2013) 59:105–13. doi: 10.1159/000343152
34. Markovic, G, Sarabon, N, Greblo, Z, and Krizanic, V. Effects of feedback-based balance and core resistance training vs. Pilates training on balance and muscle function in older women: a randomized controlled trial. Arch Gerontol Geriatr. (2015) 61:117–23. doi: 10.1016/j.archger.2015.05.009
35. Sannicandro, I. Effects of integrative core stability training on balance and walking speed in healthy elderly people. Adv Phys Educ. (2020) 10:421–35. doi: 10.4236/ape.2020.104034
36. Yoon, D, and Yim, J. Enhancing balance and strength in older adults: the impact of Pilates and vibro-swing exercises. Med Sci Monit. (2024) 30:e945212. doi: 10.12659/MSM.945212
37. Choi, W, Joo, Y, and Lee, S. Pilates exercise focused on ankle movements for improving gait ability in older women. J Women Aging. (2021) 33:30–40. doi: 10.1080/08952841.2019.1618129
38. Carrasco-Poyatos, M, Ramos-Campo, DJ, and Rubio-Arias, JA. Pilates versus resistance training on trunk strength and balance adaptations in older women: a randomized controlled trial. PeerJ. (2019) 7:e7948. doi: 10.7717/peerj.7948
39. Hosseini, SS, Asl, AK, and Rostamkhany, H. The effect of strength and core stabilization training on physical fitness factors among elderly people. World Appl Sci J. (2012) 16:479–84.
40. Kang, KY, Choi, JH, and Lee, SB. Effect of core strengthening exercise programs on symmetric double limb support and balance ability for the elderly. J Int Acad Phys Ther Res. (2012) 3:378–82. doi: 10.5854/JIAPTR.2012.3.1.378
41. Cui, Z, Xiong, J, Li, Z, and Yang, C. Tai chi improves balance performance in healthy older adults: a systematic review and meta-analysis. Front Public Health. (2024) 12:1443168. doi: 10.3389/fpubh.2024.1443168
42. Hibbs, AE, Thompson, KG, French, D, Wrigley, A, and Spears, I. Optimizing performance by improving core stability and core strength. Sports Med. (2008) 38:995–1008. doi: 10.2165/00007256-200838120-00004
43. Barrio, ED, Ramirez-Campillo, R, Garcia De Alcaraz Serrano, A, and Hernandez-García, RR. Effects of core training on dynamic balance stability: a systematic review and meta-analysis. J Sports Sci. (2022) 40:1815–23. doi: 10.1080/02640414.2022.2110203
44. Faries, MD, and Greenwood, M. Core training: stabilizing the confusion. Strength Cond J. (2007) 29:10–25. doi: 10.1519/00126548-200704000-00001
45. Tarrant, ML. How to improve proprioception: focus on the lower body to train balance. IDEA Health Fit Source. (2003) 21:31–8.
46. Dong, K, Yu, T, and Chun, B. Effects of core training on sport-specific performance of athletes: a meta-analysis of randomized controlled trials. Behav Sci (Basel). (2023) 13:148. doi: 10.3390/bs13020148
47. Rodríguez-Perea, Á, Reyes-Ferrada, W, Jerez-Mayorga, D, Chirosa Ríos, L, Van Den Tillar, R, Chirosa Ríos, I, et al. Core training and performance: a systematic review with meta-analysis. Biol Sport. (2023) 40:975–92. doi: 10.5114/biolsport.2023.123319
Keywords: core training, balance, older adults, fall prevention, meta-analysis
Citation: Zhong Y, Guo W, Chen P and Wang Y (2025) Effects of core training on balance performance in older adults: a systematic review and meta-analysis. Front. Public Health. 13:1661460. doi: 10.3389/fpubh.2025.1661460
Edited by:
Bojan Masanovic, University of Montenegro, MontenegroReviewed by:
Yi Jia, North University of China, ChinaSeda Ercan Yildiz, Eskisehir Osmangazi Universitesi, Türkiye
Copyright © 2025 Zhong, Guo, Chen and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yongshun Wang, d3lzQGhxdS5lZHUuY24=