 Susana Orrego Villegas1,2,3*
Susana Orrego Villegas1,2,3* Eric Adjei Boakye4
Eric Adjei Boakye4 Jafet Arrieta1,5,6
Jafet Arrieta1,5,6 Karine Posada España2,3
Karine Posada España2,3 Melisa Naranjo Vanegas7Gloria Prado Pino1,8,9
Melisa Naranjo Vanegas7Gloria Prado Pino1,8,9- 1Harvard Medical School, Boston, MA, United States
- 2Universidad CES, Medellín, Colombia
- 3Seguros SURA, Medellín, Colombia
- 4Department of Public Health Sciences, Henry Ford Health, Detroit, MI, United States
- 5Institute for Healthcare Improvement, Boston, MA, United States
- 6Harvard TH Chan School of Public Health, Boston, MA, United States
- 7Bioscience Center – Ayudas Diagnósticas Sura, Medellín, Colombia
- 8Universidad Tecnológica del Chocó Diego Luis Córdoba UTCH, Quibdó, Colombia
- 9Organización Panamericana de la Salud (PAHO), Washington, DC, United States
Background: With the onset of the COVID-19 pandemic in Colombia, telemedicine (TM) became a key strategy to sustain healthcare delivery for both acute and chronic conditions. This study aimed to describe the utilization and characteristics of TM during the pandemic in Colombia.
Methods: We conducted a retrospective, descriptive study using administrative and clinical records from a major Colombian health insurance provider covering approximately 15% of the national population. We analyzed all TM consultations between March 2020 and June 2021, assessing sociodemographic, geographic, and clinical characteristics. TM users and the overall insured population were described, and primary care unit (PCU) locations were georeferenced.
Results: A total of 10,016,931 individuals were enrolled in the health insurance plan, of whom 2,633,564 used TM services during the study period. TM users were predominantly female (62.8%) and aged 19–45 years (55.3%). Most belonged to low-income groups (64.9%) and were affiliated with the subsidized income level group. The most frequent diagnosis was COVID-19 (28.3%), followed by general symptoms and unspecified conditions (19.4%). Telemedicine was used nationwide, with higher concentrations in central and northern departments such as Antioquia and Bogotá.
Conclusion: During the pandemic, telemedicine was widely adopted across Colombia and reached large segments of low-income populations, suggesting its potential to support healthcare access in diverse settings. While our descriptive design does not allow for causal claims about effectiveness or equity, these findings highlight the value of TM as a complementary healthcare delivery model. Continued investment in digital infrastructure, workforce training, and primary care networks will be essential for its long-term integration into Colombia’s health system.
1 Introduction
Before the COVID-19 pandemic, telemedicine (TM) in Colombia was underutilized and not fully integrated into the healthcare system. Although the Ministry of Health and Social Protection (MHSP) enacted regulations between 2007 and 2019 to promote and standardize TM (1, 2), its implementation remained limited to a few public and private health insurances providers (3, 4). The onset of the pandemic and the nationwide mandatory quarantine from March 24 to July 15, 2020, radically altered healthcare delivery. Routine outpatient visits and elective procedures were suspended, and the healthcare system faced the urgent need to offer medical services virtually (5–7). In response, the Colombian government encouraged both public and private insurers to rapidly expand telemedicine services. As a result, over 3 million TM consultations were conducted in the first 2 months of the pandemic alone (7), and more than 42 million by January 2021 (8–10).
SURA, one of the largest insurers in the country, provided 2.6 million telemedicine consultations between March 2020 and June 2021. SURA covers approximately 30% of the insured population in Colombia, reaching around 13 million individuals across urban and rural regions, with benefit package and copayment structure comparable to those of other major insurers. The broad and diverse coverage reduces the risk of strong selection bias and allows findings from SURA to be more generalizable both within Colombia and to other middle-income countries with similar mixed health systems (11). Despite this massive expansion, there is limited evidence on the profile and distribution of TM users during this period. This knowledge gap has important implications: without a clear understanding of who accessed telemedicine services, policies and programs risk reinforcing inequities in access to healthcare. Evidence from other Latin American countries illustrates these consequences. In Brazil, targeted investments in digital health infrastructure during the pandemic improvement continuity of care in underserved areas, reducing disparities in service use (12, 13). By contrast, in Peru, limited adoption and lack of equitable access to TM left vulnerable populations further marginalized during the health emergency.
This study aims to describe the sociodemographic characteristics of TM within a major Colombian insurance provider. The findings may inform future healthcare policies, training and digital health interventions. Moreover, they can provide insights for other health systems in low-and middle-income countries seeking to sustain and scale telemedicine services beyond the pandemic.
2 Methods
2.1 Study design and population
We conducted a retrospective cohort study of individuals enrolled in the Colombian healthcare insurance provider SURA, which offers coverage under public insurance (EPS SURA), workers´ insurance (ARL SURA), and private insurance plans (Polizas SURA). The study population included all patients who accessed telemedicine (TM) services between March 1, 2020, and June 30, 2021. To contextualized characteristics, we include all individuals enrolled in SURA health plans in 2020 and 2022, regardless of telemedicine use.
2.2 Setting
Colombia is a middle-income country with Universal Health Coverage (UHC) since 1993. Individuals are required to enroll in an Entidad Promotora de Salud (EPS), and if employed, they are also covered by an occupational risk insurer (ARL). Additionally, individuals may purchase private insurance plans (Polizas) for extended benefits. Each patient is assigned to a Primary Care Unit (PCU), referred to as IPS (Institución Prestadora de Salud). SURA is one of the main insurers in Colombia, offering all three types of coverage.
2.3 Telemedicine access channels
During the study period, SURA offered telemedicine services through four distinct access channels designed to accommodate varying levels of digital literacy and connectivity. These included a mobile application, a toll-free telephone line, a dedicated website, and WhatsApp messaging. This multichannel strategy was implemented to enhance accessibility and ensure broad coverage among diverse population groups.
2.4 Data sources and georeferencing
Sociodemographic and clinical data were obtained from SURA electronic health records (EHRs), which encompass all patient interactions across insurance types (EPS, ARL and Polizas). For geospatial analysis, we georeferenced each patient’s assigned Primary Care Unit (PCU) rather than relying on self-reported locations and the time of telemedicine use. The geographic coordinates (latitude and longitude) of each PCU were extracted from the administrative registry and used to generate geographic information system (GIS) heat maps that visualized the spatial distribution and intensity of telemedicine utilization across the country.
2.5 Variables and measures
We analyzed several sociodemographic and clinical variables. Age was categorized into five groups: children (0–10 years), adolescents (11–18 years), young adults (19–45 years), middle-aged adults (46–60 years), older adults (61–70 years), and older adults (>70 years). Educational attainment was classified into five categories: primary education, secondary/high school, occupational/technical degree (e.g., electrician, culinary training), graduated education (specialization, master’s, PhD, postdoctoral), and unknown or not reported. Income level was determined based on the 2023 Colombian Minimum Monthly Wage (MMW), defined as 1,160,000 Colombian pesos (approximately 240.5 USD at an exchange rate of 1 USD = 4,824.25 COP on March 21, 2023). Income categories included: subsidized (unemployed), low income (1–2 × MMW), middle income (3–5 × MMW), and high income (>5 × MMW). Geographically, patients were grouped into five microregions based on administrative divisions and patterns of healthcare organization: Antioquia, Center-East-South, Eje Cafetero, North, and West. Ethnicity was recorded using standard Latin American classifications, including Black, White, Indigenous, Mestizo (Indigenous and European ancestry), Mulato (African and European ancestry), and Zambo (African and Indigenous ancestry). Additionally, diagnoses made during telemedicine encounters were extracted from EHRs using ICD-10 codes to assess the distribution of health conditions addressed through TM.
2.6 Statistical analysis
Descriptive statistics (frequencies and proportions) were computed for all variables of interest. For spatial analysis, we used ArcGIS Pro software to generate density-based heat maps of telemedicine utilization. Locations with the highest concentration of TM users—defined as clusters with over 100,000 consultations—were highlighted using red markers. All statistical analyses were conducted using StataBE 17 and Microsoft Excel.
3 Results
3.1 Telemedicine use and population characteristics
Between March 2020 and June 2021, a total of 10,016,931 individuals were enrolled in a Colombian health insurance plan; of whom 2,633,564 accessed at least one TM consultation. Among TM users, 94.0% had one appointment, 4.5% had two, and 1.4% had three or more consultations during the study period. Table 1 presents the sociodemographic characteristics of TM users and the overall insured population enrolled between 2020 and 2022. Approximately 63% of the TM users were female, 55.3% were aged 19 to 45 years, 53.1% were assigned to primary care units (PCUs) located in the department of Antioquia, 16.3% reported being mestizo as their ethnicity, 28.6% indicated that their highest educational attainment was a technical or occupational degree, and 64.9% were classified as belonging to a low-income category, defined as earning between one and two Colombian Minimum Monthly Wages (MMW) in 2023. In the entire insured population, 48.4% were female, 51.3% were aged 19 to 45 years, 41.8% were located in the department of Antioquia, 28.9% reported being mestizo as their ethnicity, 20.1% indicated that their highest educational attainment as technical or occupational degree, and 65.5% were classified as being in a low-income category.

Table 1. Characteristics of the telemedicine users vs. entire population in health plan.
3.2 Diagnoses and disease burden among telemedicine users
Table 2 details the top ICD-10 diagnoses made during TM consultations. The most frequent clinical diagnosis among TM users was COVID-19 (28.3%). Chronic non-communicable diseases were also common, with hypertension diagnosed in 10.0% and type 2 diabetes mellitus in 3.2% of cases. Acute respiratory infections, mental health disorders, and musculoskeletal complaints were also among the top 10 diagnoses, reflecting a diverse range of clinical needs addressed through TM.
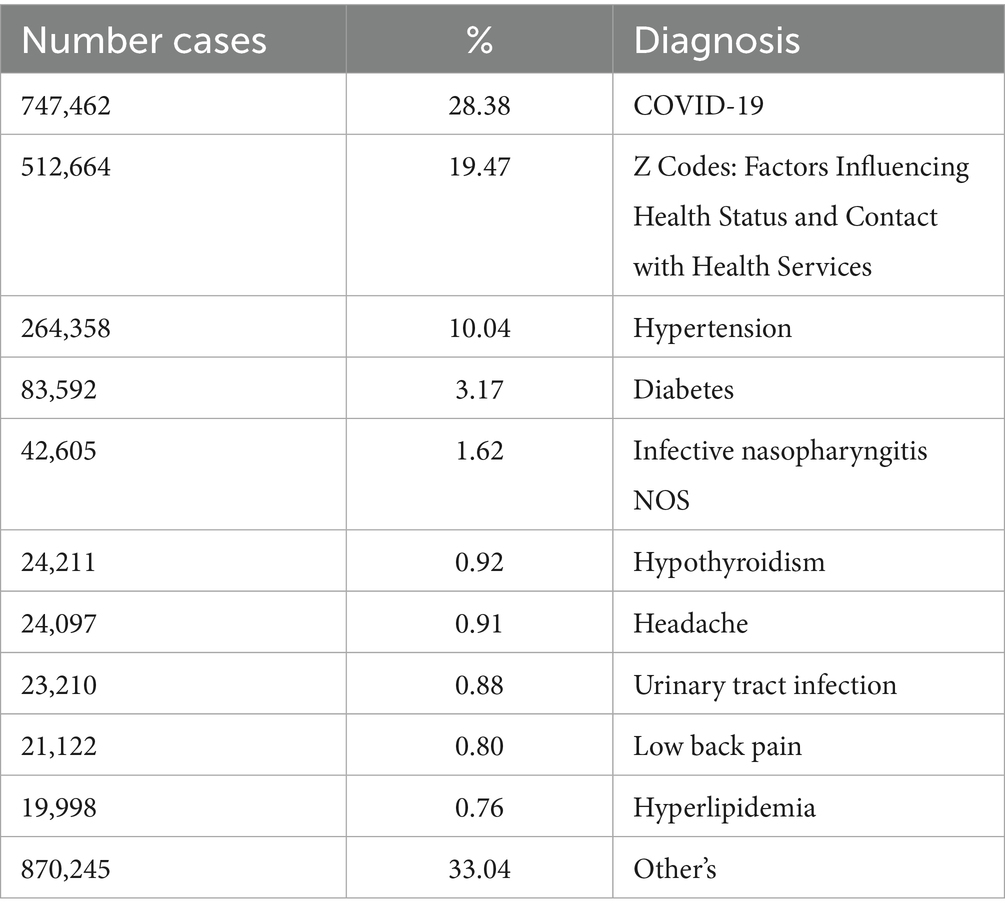
Table 2. Principal ICD-10 diagnoses among the telemedicine users.
To further characterize the health status of TM users, we analyzed the presence of chronic conditions registered prior to their first TM contact. Table 3 summarizes the top 10 Chronic comorbidities in the TM users and the overall insured population. Among TM users, hypertension was the most prevalent pre-existing condition (15.0%), followed by asthma (3.9%), hyperlipidemia (3.3%), and type 2 diabetes (3.1%). Among the general insured population, the most prevalent pre-existing condition was hypertension (11.9%), hyperlipidemia (9.0%), asthma (4.2%), and type 2 diabetes (3.8%).

Table 3. Chronic conditions among telemedicine users vs. health plan population as a whole.
TM users stratified by income level. In the subsidized group (predominantly unemployed), 70.0% of users were female whereas 56.1% were in the high-income group (Table 4). Approximately 52% of TM users aged 19–45 years were in the subsidized group whereas 55.3% were in the high-income group. Most TM users were mestizo ethnicity in both the subsidized (74.2%) and high-income groups. Finally, 86.8% of TM users who were in the subsidized group had occupational degree and 80.0% who had occupational degree were in the higher-income group. In terms of number of preexisting conditions, a higher proportion of TM users had zero followed by 1 and 2 across all income level groups (Table 5).
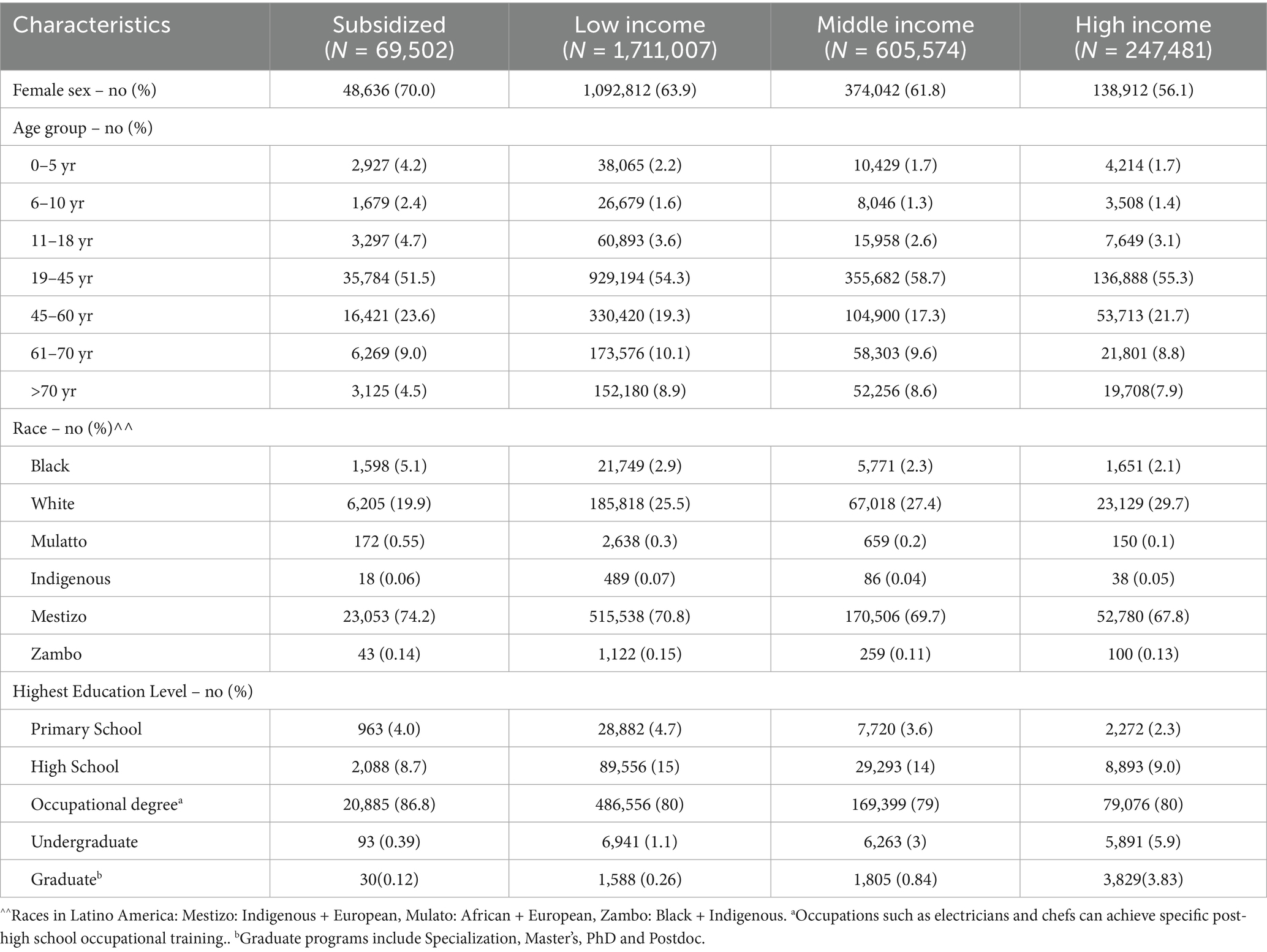
Table 4. Sociodemographic characteristics by income level among the TM population.
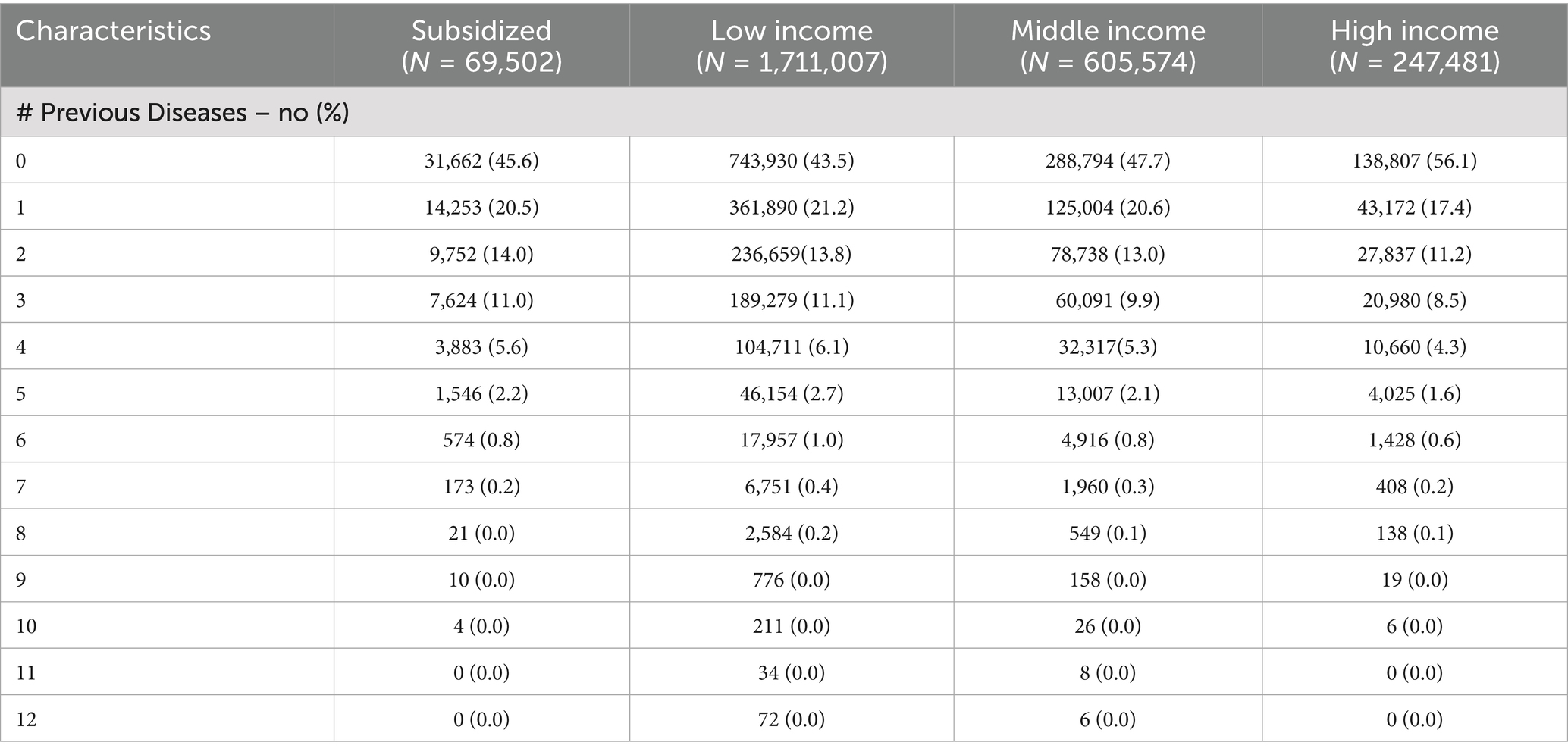
Table 5. Number of preexisting conditions of telemedicine users by income level.
3.3 Geographical distribution of telemedicine use
For the graphical analysis, we used ArcGIS Pro as the GIS mapping software to plot the latitude and longitude coordinates. A heat map was generated according to the distribution of users. Red dots represent concentrations of more than 100,000 patients, yellow dots represent 50,000–100,000 patients, and green dots represent fewer than 50,000 users.
In addition, we created a 3D map of Primary Care Units (PCUs) across Colombia, reflecting the places affiliated with users at the time of their telemedicine consultation. To protect confidentiality, we did not use the exact addresses provided during medical consultations. A total of 108 PCUs across the country were mapped using a geographic information system (GIS). The greatest density of TM use was concentrated in urban areas, particularly in the departments of Antioquia, Bogotá D. C., Valle del Cauca (Cali), and Atlántico (Barranquilla).
Figure 1 presents a national heat map illustrating the distribution of TM consultations across Colombia. Figure 2 illustrates the four main cities of Colombia—Medellín, Cali, Bogotá, and Barranquilla—and specifically highlights the areas of concentration of the patients’ Primary Care Units (PCUs), allowing the reader to visualize their geographic distribution in the urban, semiurban and rural areas.

Figure 1. A GIS map displaying the geographical location of primary care units for the telemedicine users between March 2020 and June 2021. A total of 108 primary care units distributed between the center and north of Colombia. >100.000 High concentration of TM users.
100.000–50.000 Middle concentration of TM users.
< 50.000 Less concentration of TM users.
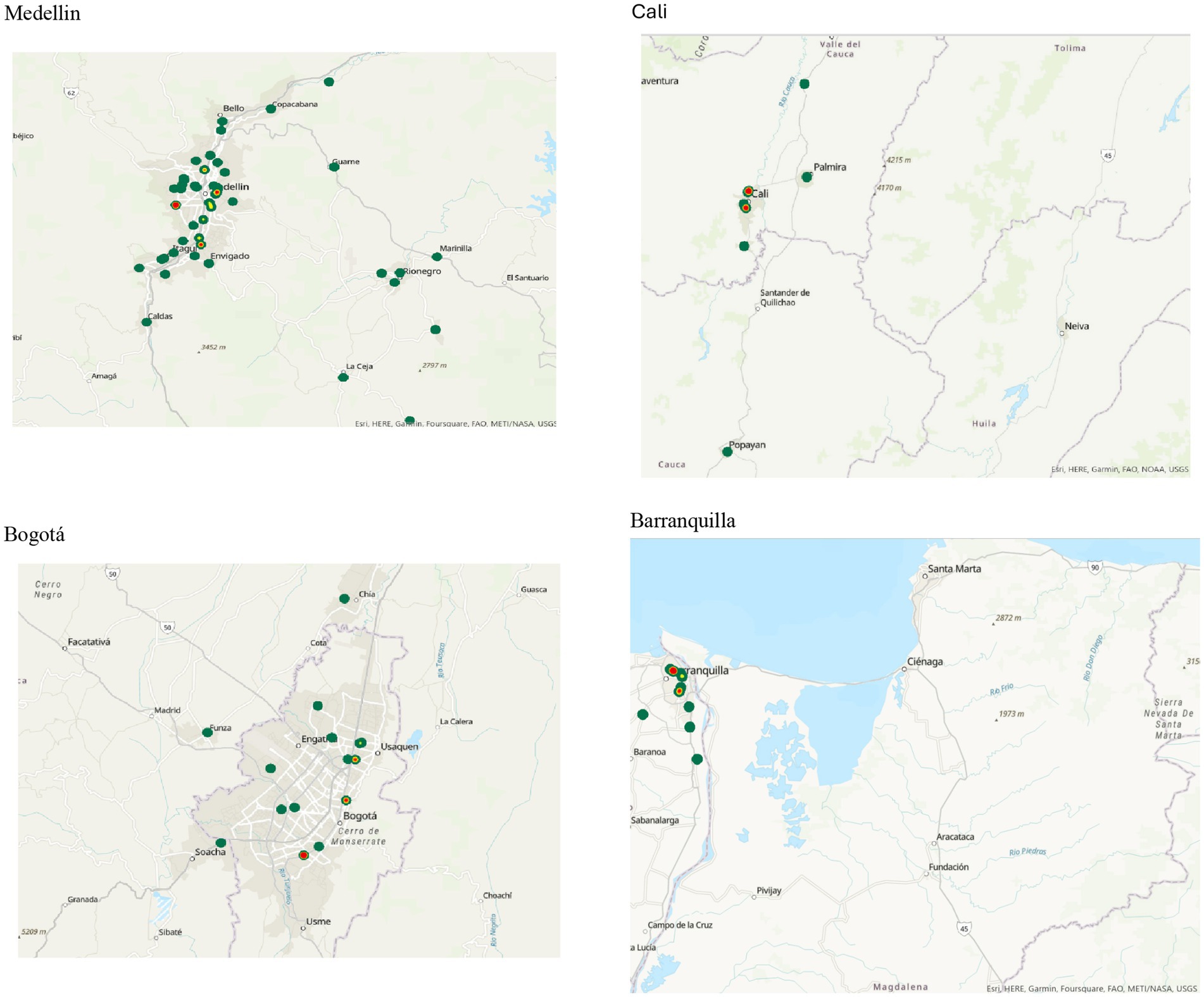
Figure 2. A GIS map showing the location of primary care units in the main cities of Colombia, including Medellin, Bogotá, Cali, and Barranquilla. (A) Medellin. (B) Bogotá. (C) Cali. (D) Barranquilla.
4 Discussion
The aim of this study was to describe the sociodemographic characteristics and health conditions of telemedicine (TM) users within a large Colombian insurance provider during the COVID-19 pandemic. Our principal findings show that over 2.6 million insured individuals used telemedicine services, spanning diverse demographic groups and health conditions (8–10). The adoption of telemedicine occurred not only among individuals with chronic conditions, such as hypertension and diabetes, but also in a wide range of non-chronic conditions. Usage extended to both pediatric and older adult populations, indicating a systematic shift in the delivery of care that transcended age, gender and socioeconomic status.
One of the most significant findings is that a higher proportion of individuals from low-income and subsidized groups were primary users of telemedicine. This challenges the pervasive notion that digital health may inherently widen inequalities due to disparities in internet access or digital literacy (14, 15). In our context, telemedicine appeared to function as a mechanism of health equity, allowing vulnerable populations to access timely care without the barriers of transportation costs, time off work, or exposure to infections (14). This is consistent with findings in other settings, such as in the United States, where Cantor et al. (2021) showed that telehealth expansion during the pandemic helped maintain access across sociodemographic groups (16). However, it contrasts with findings in low-resource settings like Ghana and Nigeria, where Dodoo et al. (17) described persistent inequalities in telemedicine access, emphasizing that context-specific infrastructure and governance play a decisive role in shaping digital health equity.
Women accounted for nearly two-thirds of all TM users. This may reflect increased healthcare-seeking behavior among women but could also point to their central role in family health management, particularly during public health emergencies (18, 19). These findings mirror regional and global patterns, where women are more likely to access primary care and chronic disease services, and may be disproportionately responsible for coordinating care for children and older relatives. From a geographical standpoint, telemedicine services were delivered across nearly all departments of Colombia, even though the insurer does not operate in every region. The strategic deployment of primary care units (PCUs) as nodes for virtual care made it possible to overcome some of the limitations imposed by the country’s persistent digital divide (20). The Economic Commission for Latin America and the Caribbean (CEPAL, 2020) has emphasized that such digital gaps remain one of the most pressing structural challenges to inclusive telehealth in the region (20). Nevertheless, the present study shows that even in a middle-income country with unequal connectivity, a rapid and massive adoption of telemedicine was possible, highlighting the latent capacity for digital transformation within health systems when aligned with urgent public health needs (21, 22).
Importantly, the structure and timing of this study offer unique insights. Unlike most reports from Colombia during the pandemic, which focused on specific hospitals, cities, or disease categories, our analysis captures the full spectrum of patients utilizing telemedicine in a large insurance network. It reveals not only who used telemedicine, but also how usage patterns varied by sociodemographic and clinical factors—critical information for scaling digital health solutions in a post-pandemic landscape. The inclusion of diagnostic categories further enriches our understanding of the types of conditions managed virtually, ranging from respiratory symptoms and acute infections to endocrine and mental health conditions. These results also provide empirical support for the conceptualization of telemedicine not as a temporary substitute during crisis, but as a viable and scalable modality for sustained healthcare delivery (23, 24). The rapid uptake of virtual consultations by both providers and patients underscores a level of digital readiness in the Colombian health system that had not previously been quantified. Moreover, the shift was accomplished without significant exclusions along income or age lines, suggesting a window of opportunity for institutionalizing telemedicine as part of the routine healthcare model.
For health professionals, these findings highlight the need for strengthened training in telemedicine competencies to ensure high-quality virtual care. For policymakers, they emphasize the importance of sustained investments in digital infrastructure, equitable findings models, and comprehensive regulatory frameworks to guarantee continuity, quality, and data protection. For researchers, future work should assess patient outcomes, satisfaction, and long-term health impacts; explore provider perspectives and barriers to adoption; and conduct longitudinal and comparative analyses to evaluate the sustainability and equity of telemedicine services (20). Taken together, the Colombian experience demonstrates that, beyond its role in public health emergencies, telemedicine has the potential to address persistent challenges in healthcare delivery – such as geographic inequities, provider shortages, continuity of care for chronic conditions, and access for marginalized populations. It should no longer be viewed merely as an emergency response, but as a strategic component of resilient, patient-centered health systems capable of adapting to the evolving needs of diverse populations.
5 Limitations
This study offers valuable insights into telemedicine use in Colombia; however, some limitations should be acknowledged. While the dataset encompasses a large and diverse sample of over 2.6 million individuals, it represents enrollees from a single health insurance provider, which may not fully capture the heterogeneity of the national population. Nonetheless, this insurer covers a broad geographic and demographic spectrum, offering a meaningful lens into real-world implementation. Additionally, to protect patient confidentiality, geographic information was limited to primary care unit assignments, restricting detailed analysis of urban–rural disparities. Although we did not include measures of digital literacy, internet access, or user experience—key aspects of digital equity—our findings still provide a foundational understanding of sociodemographic access patterns. Finally, while disaggregation of some variables was limited due to privacy considerations, the overall trends observed offer a robust starting point for future research and policy development in digital health.
5.1 Implications for policy and practice
The findings have clear implications for public health strategy and health system planning in Colombia and similar LMICs. First, they confirm that telemedicine can be an equity-promoting intervention when deployed at scale and integrated into existing care networks, especially primary care. To maintain and expand this success, investments must be made in broadband connectivity, especially in underserved regions, and in the digital capacity of primary care units and health professionals. Policies that ensure telemedicine reimbursement parity, promote interoperability between platforms, and establish quality-of-care benchmarks will be critical for long-term sustainability. Furthermore, national telehealth strategies must prioritize digital inclusion by addressing structural barriers such as internet affordability and technological accessibility. Digital health literacy campaigns and community-based education efforts can help close usage gaps and empower patients to take an active role in their healthcare. Lessons from this study can guide both the refinement of telemedicine infrastructure and the design of hybrid care models that combine virtual and in-person services according to clinical appropriateness and patient preference.
6 Conclusion
This study provides population-level evidence that telemedicine was central to preserving healthcare access in Colombia during the COVID-19 pandemic. Its widespread adoption across age, gender, and socioeconomic groups underscores its role as a mechanism for advancing health equity rather than serving solely as a temporary substitute. The Colombian experience demonstrates the country’s capacity for digital health innovation and offers a scalable reference for other LMICs seeking to integrate telemedicine into routine care. To secure lasting transformation, sustained political commitment, strategic infrastructure investment, and equity-oriented policies will be essential.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité de Etica de Sura (CEI-SURA), Harvard Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SV: Funding acquisition, Software, Formal analysis, Writing – review & editing, Project administration, Data curation, Validation, Conceptualization, Writing – original draft, Methodology, Resources, Supervision, Investigation, Visualization. EB: Validation, Writing – review & editing, Project administration, Writing – original draft, Supervision, Investigation. JA: Investigation, Writing – original draft, Formal analysis, Conceptualization, Project administration, Writing – review & editing, Methodology. KE: Conceptualization, Writing – review & editing, Validation, Project administration, Writing – original draft, Methodology. MV: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. GP: Investigation, Writing – review & editing, Methodology, Writing – original draft, Resources.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We thank the teaching team at Harvard Medical School’s Master of Global Health Delivery program for their invaluable guidance throughout the research process. We also wish to acknowledge the dedication and efforts of the hundreds of healthcare professionals who served tirelessly during the COVID-19 pandemic. Our gratitude extends to SURA, Colombia, for generously providing the raw data that made this study possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Ministerio de Salud y protección social Análisis de situación de salud (ASIS) Colombia, 2021 (2021). Bogotá, Colombia.
3. Karine Posada SOAMOMMY. E-health: the way to improve coordinated care in a private insurance company in COLOMBIA, 2019. In: International conference on e-health (2019). Lisbon, Portugal.
4. Orrego, Susana KPAMO and MMY. Wellness in Your Pocket: Update Your Health. (2019). Medellín, Colombia.
5. Ministerio de Salud y Protección Social Colombia (2019). Telesalud, mayor acceso y equidad para todos los colombianos. Bogotá, Colombia.
6. Ministerio de Salud y Protección Social Colombia (2021). 101 millones de atenciones en telemedicina en Colombia durante el último año (Boletín de Prensa No 321 de 2021). Bogotá, Colombia.
7. Ministerio de Salud y Protección Social Colombia (2020). Durante la pandemia se consolidó la telemedicina en el país (Boletín de Prensa No 875 de 2020) Bogotá, Colombia.
8. Hernández Rincón, EH, Pimentel González, JP, Aramendiz Narváez, MF, Araujo Tabares, RA, and Roa González, JM. Description and analysis of primary care-based COVID-19 interventions in Colombia. Medwave. (2021) 21:8147. doi: 10.5867/medwave.2021.03.8147
9. Hincapié, MA, Gallego, JC, Gempeler, A, Piñeros, JA, Nasner, D, and Escobar, MF. Implementation and usefulness of telemedicine during the COVID-19 pandemic: a scoping review. J Prim Care Community Health. (2020) 11:612. doi: 10.1177/2150132720980612
10. Bezerra, GMF, De Lucena Feitosa, ES, Vale Catunda, JG, Nogueira Sales Graça, C, Lucena De Aquino, P, Bezerra Neto, AG, et al. Telemedicine application and assessment during the COVID-19 pandemic In: J Ye, editor. Studies in health technology and informatics. London: IOS Press BV (2022). 854–7.
12. Opinión y análisis / opinion and analysis Serie Sobre Equidad En Salud Y Desarrollo Sostenible / Series On Equity In Health And Sustainable Development. (2025). Bogotá, Colombai.
13. Patalay, P, and Gage, SH. Changes in millennial adolescent mental health and health-related behaviours over 10 years: a population cohort comparison study. Int J Epidemiol. (2019) 48:1650–64. doi: 10.1093/ije/dyz006
14. Beheshti, L, Kalankesh, LR, Doshmangir, L, and Farahbakhsh, M. Telehealth in primary health care: a scoping review of the literature. (2019)
15. Khairat, S, Haithcoat, T, Liu, S, Zaman, T, Edson, B, Gianforcaro, R, et al. Advancing health equity and access using telemedicine: a geospatial assessment. J Am Med Inform Assoc. (2019) 26:796–805. doi: 10.1093/jamia/ocz108
16. Cantor, JH, McBain, RK, Pera, MF, Bravata, DM, and Whaley, CM. Who is (and is not) receiving telemedicine care during the COVID-19 pandemic. Am J Prev Med. (2021) 61:434–8. doi: 10.1016/j.amepre.2021.01.030
17. Dodoo, JE, Al-Samarraie, H, and Alzahrani, AI. Telemedicine use in sub-Saharan Africa: barriers and policy recommendations for Covid-19 and beyond. Int J Med Inform. (2021) 151:104467. doi: 10.1016/j.ijmedinf.2021.104467
18. van Olmen, J. The promise of digital self-management: a reflection about the effects of patient-targeted e-health tools on self-management and wellbeing. Int J Environ Res Public Health. (2022) 19:1360. doi: 10.3390/ijerph19031360
19. Mahdavi, S, Fekri, M, Mohammadi-Sarab, S, Mehmandoost, M, and Zarei, E. The use of telemedicine in family medicine: a scoping review. BMC Health Serv Res. (2025) 25:376. doi: 10.1186/s12913-025-12449-7
20. Economic Commission for Latin America and the Caribbean (CEPAL) (2020). Universalizar el acceso a las tecnologías digitales para enfrentar los efectos del COVID-19.
21. da Silva, JB, Lima, NT, Garcia-Saisó, S, Fitzgerald, J, Bascolo, E, Galiano, SG, et al. Towards 2030: ministerial agreements on information systems and digital transformation for resilient health systems. Pan Am J Pub Health. (2024) 48:1–12. doi: 10.26633/RPSP.2024.137
22. Eccher, C, Babitsch, B, Saleem, MS, and Werner, L. How digital transformation can accelerate data use in health systems. (2025)
23. Myers, CR. Using telehealth to remediate rural mental health and healthcare disparities. Issues Ment Health Nurs. (2019) 40:233–9. doi: 10.1080/01612840.2018.1499157
Keywords: telemedicine, COVID-19 pandemic, healthcare access, Colombia, digital health equity
Citation: Villegas SO, Boakye EA, Arrieta J, España KP, Vanegas MN and Pino GP (2025) The role of telemedicine in the context of the COVID-19 pandemic in Colombia. Front. Public Health. 13:1667349. doi: 10.3389/fpubh.2025.1667349
Edited by:
Zisis Kozlakidis, International Agency for Research on Cancer (IARC), FranceReviewed by:
Luigi Di Biasi, University of Salerno, ItalyBiplav Tiwari, University of Georgia, United States
Copyright © 2025 Villegas, Boakye, Arrieta, España, Vanegas and Pino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susana Orrego Villegas, c3VzYW5hb3JyZWdvdmlsbGVnYXNAYWx1bW5pLmhhcnZhcmQuZWR1