 Lan Shi
Lan Shi Min Liu4†
Min Liu4†- 1Shengli Clinical Medical College of Fujian Medical University, Fuzhou, Fujian, China
- 2Department of Intensive Care Medicine, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, Fujian, China
- 3Department of Nursing, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, Fujian, China
- 4School of Nursing, Fujian Medical University, Fuzhou, Fujian, China
- 5Department of Emergency, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, Fujian, China
- 6Department of Emergency Intensive Care Medicine, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, Fujian, China
- 7State University of New York at Buffalo, Buffalo, NY, United States
Objective: To develop a structured “Disaster Nursing Practice Week” training program for undergraduate nursing interns, tailored to the context of mobile cabin hospitals, with the aim of enhancing disaster nursing competencies and providing a theoretical foundation for practical training.
Methods: The program was designed using the disaster management continuum theory in conjunction with the 2019 International Council of Nurses (ICN) updated Disaster Nursing Core Competencies framework. The Delphi method was employed to conduct two rounds of expert consultation, involving 15 professionals with expertise in nursing education, nursing management, disaster nursing, and emergency medicine.
Results: The response rate for both Delphi rounds was 100%. The expert authority coefficient was calculated at 0.93. The coefficient of variation ranged from 0.000 to 0.205 in the first round and from 0.000 to 0.125 in the second round. Kendall’s coefficient of concordance (W) was 0.252 and 0.300, respectively (p < 0.001). The finalized training program comprised 8 primary indicators, 14 secondary indicators, and 47 tertiary indicators.
Conclusion: The training program demonstrated a high degree of relevance and alignment with the practical needs of undergraduate nursing interns. It provides a systematic framework designed to enhance clinical competencies and strengthen disaster nursing preparedness within mobile cabin hospital environments.
1 Introduction
Globally, numerous unpredictable natural disasters, human-made accidents, and public health emergencies occur annually, posing complex challenges to society. These events not only threaten public health but also compromise the stability of economic and social systems and the sustainability of ecological environments (1–4). As a country with frequent disaster occurrences, China faces unique and urgent challenges in the domain of disaster management (1, 5, 6). Healthcare professionals serve as indispensable components of disaster response teams (7). Among them, nurses represent the largest group and play critical, non-substitutable roles across the full spectrum of disaster management, including mitigation, preparedness, emergency response, and post-disaster recovery phases (1, 2, 7–10). The level of disaster nursing competency directly affects the effectiveness and efficiency of relief efforts undertaken by the broader disaster response teams (11). In addition to qualified nursing professionals, undergraduate nursing students constitute an essential part of the nursing workforce and serve as important human resources for health service delivery in disaster settings. In the event of a disaster, nursing students may be mobilized to support licensed nurses in relief efforts, thereby reinforcing the overall capacity of the healthcare system (12–14). Evidence indicates that nursing students, though not yet licensed, have acquired fundamental clinical skills through formal education and are therefore capable of contributing positively to disaster response efforts (7). During the Coronavirus Disease 2019 (COVID-19) pandemic, numerous nursing graduates entered clinical settings, where they provided critical assistance to patients and helped alleviate workforce shortages (12, 15). These findings highlight the importance of fostering disaster response competencies among undergraduate nursing students.
Currently, in the field of disaster medicine/nursing education, several countries have established influential educational models. For example, the National Disaster Life Support (NDLS) curriculum in the United States focuses on standardized response protocols, while the Emergency Preparedness and Response (EPR) framework in the UK emphasizes command systems and multi-agency collaboration. These models provide important theoretical foundations and a global perspective for this study. Globally, disaster nursing education and training programs for nursing students have demonstrated gradual growth, although significant regional disparities remain (16). Most existing programs prioritize disaster preparedness and emergency response, often emphasizing specific operational skills such as triage and psychological first aid, while underrepresenting comprehensive training in all phases of disaster management—namely, mitigation, preparedness, response, and recovery (4, 10). As a result, current educational interventions often fall short of meeting international standards for disaster preparedness (17). In China, disaster nursing education was initiated relatively late, and traditional training models also face numerous challenges. Including inconsistent curricula and variability in syllabi across academic institutions (18, 19). Furthermore, most programs remain confined to classroom-based learning, with limited integration of disaster nursing practice during clinical internships. The suddenness and irreproducibility of disasters result in the current disaster care training courses having low scene authenticity. There is a critical need to provide structured educational programs that equip nursing students and professionals with both theoretical knowledge and practical competencies in disaster nursing. The most recent edition of the International Council of Nurses (ICN) Disaster Nursing Core Competencies V2.0 underscores the necessity of delivering multilevel training across all phases of disaster management (9).
Mobile cabin hospitals are composed of interconnected modular units, such as vehicles, tents, and cabin units, equipped to deliver a range of medical services including emergency treatment, surgery, radiologic imaging, laboratory diagnostics, and life support. These modular units can be assembled into enclosed, self-contained zones that can function independently of external environmental conditions, enabling medical teams to provide a full range of clinical services (20). The modular configuration allows for flexible assembly into field hospitals of various sizes, depending on the demands of specific disaster scenarios.
Owing to their high mobility, rapid deployment capabilities, and adaptability to diverse environments, mobile cabin hospitals have become essential in emergency medical response and have played a significant role in China’s earthquake relief efforts and responses to public health emergencies (21). The current study aimed to construct a week-long clinical training program in disaster nursing, termed the “Disaster Nursing Practice Week,” specifically designed for undergraduate nursing interns. This program was developed within the context of mobile cabin hospital deployment and was guided by the ICN Disaster Nursing Core Competencies framework (1, 9). The objective of the program is to enhance nursing interns’ disaster nursing competencies, increase their ability to assess and respond effectively in disaster contexts, promote willingness to participate in disaster relief efforts, and contribute to the development of a resilient and skilled disaster nursing workforce.
2 Participants and methods
2.1 Participants
2.1.1 Research team establishment
The research team comprised seven members, including three associate chief nurses, two charge nurses, and two staff nurses. Their responsibilities included designing the expert consultation questionnaires, selecting appropriate consultation experts, and conducting statistical analyses of the consultation results.
2.1.2 Selection of consultation experts
The selection of experts is a critical component of the rigor and credibility of the Delphi consultation process, as the representativeness and authority of the panel directly affect the scientific validity and reliability of the findings. It is generally recommended that 10 to 50 experts be selected to ensure representativeness with practical feasibility (11). Panels with fewer participants may lack diversity and diminish the authority of the results, while larger panels may increase logistical complexity and data processing demands. Based on the specific needs of this study, the following inclusion criteria were applied for the selection of expert participants: (1) Voluntary participation, with a high degree of motivation and ability to engage in both rounds of consultation; (2) Possession of a bachelor’s degree or higher and a professional title at the intermediate level or above; (3) A minimum of 10 years of relevant work experience; (4) Previous experience in disaster relief or recognized expertise in the field of disaster nursing; and (5) Experience in disaster nursing education or research, familiarity with disaster nursing training program development, or service on disaster relief teams, professional disaster nursing committees, or as nursing managers in critical care, rehabilitation, or related specialties.
2.2 Methods
2.2.1 Preliminary construction of the mobile cabin hospital “disaster nursing practice week” training program
The initial development of the training program—hereinafter referred to as the “training program”—was guided by the disaster management continuum theory and the 2019 ICN Disaster Nursing Core Competencies, which outline eight core dimensions relevant to nursing practice in disaster contexts. Through systematic literature review, practical experience of disaster relief in cabin hospitals, and preliminary research, the relevant components of nursing intern training plan in mobile makeshift hospital environment were preliminarily determined. Following iterative internal discussions among research team members, a preliminary version of the training program was constructed, which included eight primary indicators, 13 secondary indicators, and 42 tertiary indicators.
2.2.2 Expert consultation process for training program development
The draft training program was incorporated into the first-round expert consultation questionnaire. The questionnaire comprised four sections: (1) An introductory section outlining the research background, objectives, and methodology; (2) A Delphi survey section, wherein experts were asked to assess the importance of each indicator using a 5-point Likert scale: “very important,” “important,” “moderately important,” “not very important,” and “not important,” corresponding to scores from 5 to 1. Experts were also invited to indicate additions, deletions, or revisions to the listed indicators; (3) A section assessing the authority of participating experts, which included a self-assessment of familiarity with the subject matter and the criteria used evaluating the indicators; and (4) A demographic and professional profile section, collecting information such as education, disaster relief and training experience, and other relevant professional qualifications.
2.2.3 Distribution of Delphi questionnaires
Two rounds of expert consultation were conducted between October 2023 and March 2024. Prior to distributing the questionnaires, brief telephone communications were initiated with selected experts to introduce the study background, objectives, and methodology. Upon obtaining informed consent, the Delphi questionnaires were distributed via email with instructions for return within 2 weeks. A one-month interval was maintained between the two rounds of consultation.
The framework underwent validation through two rounds of Delphi expert consultations, during which items were scored for their importance while incorporating expert revisions and new suggestions. Its reliability and validity were quantitatively assessed using statistical indicators including expert authority coefficients, coefficient of variation, and Kendall’s W-coefficient of concordance. Finally, a standardized process was implemented with multiple rounds of revisions until all domain items met the consistency threshold, after which the final indicator system was aligned with the ICN competency framework. This process ensured the reproducibility of training program design and demonstrated broader potential for promotion and application.
2.2.4 Statistical analysis
All completed questionnaires were coded and subjected to data verification. Double data entry was performed using Excel 2020, and statistical analysis was conducted using SPSS version 26.0. The statistical indicators included: (1) Descriptive statistics for expert demographic characteristics (frequency, composition ratio, mean ± standard deviation); (2) Response rate, calculated as the proportion of valid questionnaires returned; (3) Indicators of opinion concentration, including mean, standard deviation, full score ratio, and selection rate; (4) Measures of agreement among expert responses, assessed using the coefficient of variation and Kendall’s W coefficient; and (5) Assessment of expert authority, reported through the authority coefficient. A significance threshold of p < 0.05 was applied.
2.2.5 Quality control
To ensure the scientific validity, reliability, and feasibility of the consultation process, quality control measures were implemented at each stage. These included: (1) Applying strict inclusion and exclusion criteria and inviting a multidisciplinary panel to ensure broad representation; (2) Obtaining informed consent through direct communication following expert selection; (3) Designing Delphi questionnaires using concise and precise language; (4) Sending timely reminders to experts after distribution to maximize the questionnaire return rate; and (5) Including revised results from the first consultation round into the second-round questionnaire, allowing experts to review changes and provide updated evaluations.
3 Results
3.1 General characteristics of experts
A total of 15 experts participated in and completed both rounds of the Delphi consultation. The panel comprised professionals from four regions in China, Beijing, Fujian, Sichuan, and Yunnan, and included representation from the fields of nursing education, nursing management, disaster nursing, and emergency medicine. Among them, 3 were male and 12 were female. Their ages ranged from 35 to 56 years (mean = 44.07, SD = 6.58), and their work experience ranged from 10 to 38 years (mean = 23.00, SD = 8.50). Regarding educational background, 3 held doctoral degrees, 11 held master’s degrees, and 1 held a bachelor’s degree. In terms of professional titles, 5 were at the intermediate level, 7 at the associate senior level, and 3 at the senior level. A total of 11 experts had prior experience in disaster relief. The general characteristics of the consultation experts are presented in Table 1.
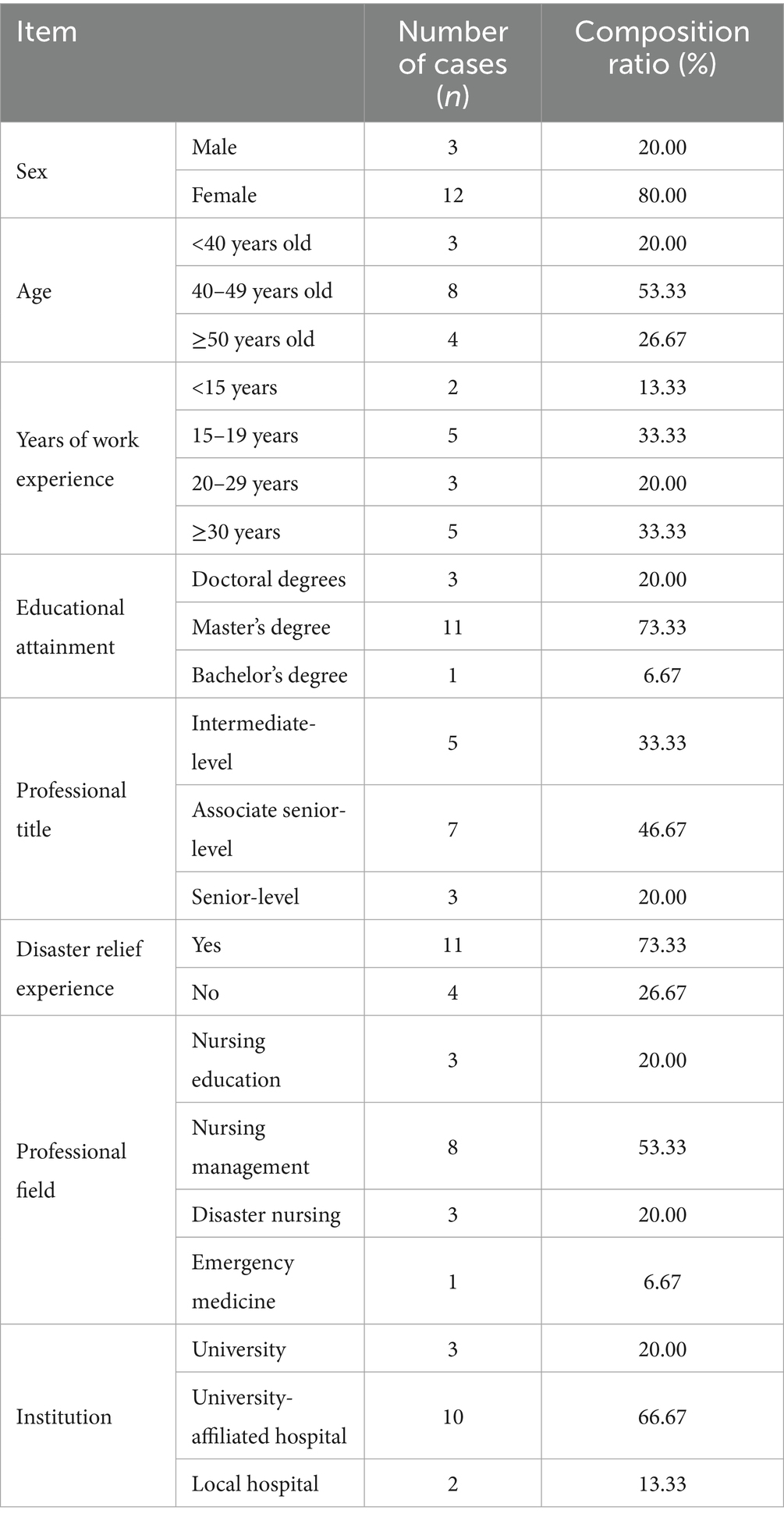
Table 1. Demographic and professional characteristics of consultation experts.
3.2 Expert response rate
The response rate for both rounds of expert consultation was 100%. In the first round, 9 experts (60%) provided a total of 37 comments. In the second round, 5 experts (33%) submitted 8 comments. These response patterns reflect strong engagement and enthusiasm among the experts for participation in the study.
3.3 Expert authority level
The authority of the expert panel was evaluated using two components: the judgment basis coefficient and the familiarity coefficient. The judgment basis coefficient was 0.930, and the familiarity coefficient was 0.880. The overall authority coefficient was 0.905. These values indicate a high level of expertise among the participants, supporting the reliability of the consultation outcomes.
3.4 Expert opinion coordination level
The coefficient of variation for expert opinions ranged from 0.000 to 0.205 in the first round and from 0.000 to 0.125 in the second round. The decrease in the coefficient of variation during the second round indicates improved convergence of expert opinions. Kendall’s coefficient of concordance (W) was 0.252 in the first round and 0.300 in the second round. Both coefficients were statistically significant (p < 0.001). These findings demonstrate meaningful level of agreement among the experts. Detailed results for coordination levels are presented in Table 2.

Table 2. Coordination of expert opinions: coefficient of variation and Kendall’s W.
3.5 Expert opinion concentration level
Following two rounds of Delphi consultation, the finalized training program included 8 primary indicators, 14 secondary indicators, and 47 tertiary indicators. The mean importance score for all indicators ranged from 4.80 to 5.00. The standard deviation ranged from 0 to 0.52. The full score rate varied between 73.33 and 100%, while the selection rate ranged from 93.33 to 100%. The coefficient of variation for all indicators was between 0 and 0.125. These metrics reflect a high level of consensus among the experts. The results of the second-round expert consultation on the training program are presented in Table 3.
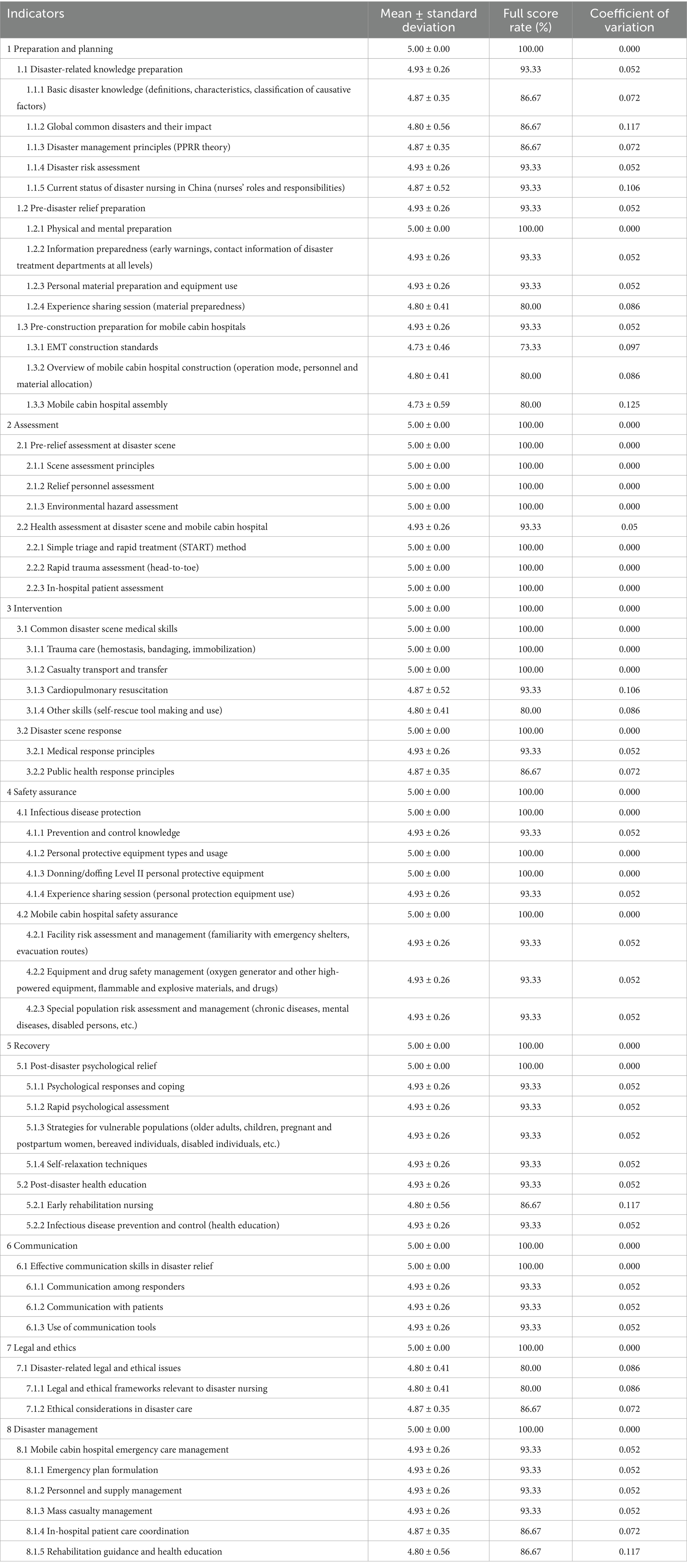
Table 3. Summary of second-round expert consultation results for training program indicators.
3.6 Consultation results for training hours and teaching methods
Experts proposed revisions to the allocation of instructional time, particularly within the modules addressing preparation and planning, assessment, and disaster management. Following comprehensive discussion, the majority of expert recommendations were incorporated into the final training plan. The finalized training schedule included a total of 35 class hours, with 7 class hours allocated per day. While the instructional duration of each module remained unchanged, additional time for reflection and discussion was included in the implementation plan. We mapped the training items to the ICN Framework of Disaster Nursing Competencies (2019). Among these, Level I competencies such as “fundamental disaster knowledge,” “basic triage skills,” and “personal protection” were all encompassed in this program. Certain Level II competencies, including “interdisciplinary team coordination” and “overall operation management of mobile cabin hospitals,” were also addressed through secondary indicators within Module 8 (Disaster Management). In terms of instructional methods, a multi-modal approach was adopted, incorporating several complementary teaching strategies tailored to the structure of the training program. Details regarding the allocation of training hours and teaching methods are presented in Table 4. In addition, regarding the teaching methods, a multimodal teaching approach combining several optimal instructional methods is adopted in accordance with the training program. As for the selection of teaching faculty, all teaching Homo sapiens possess extensive rescue experience, clinical and academic teaching experience, and are members of the National Emergency Rescue Team (Fujian Province).
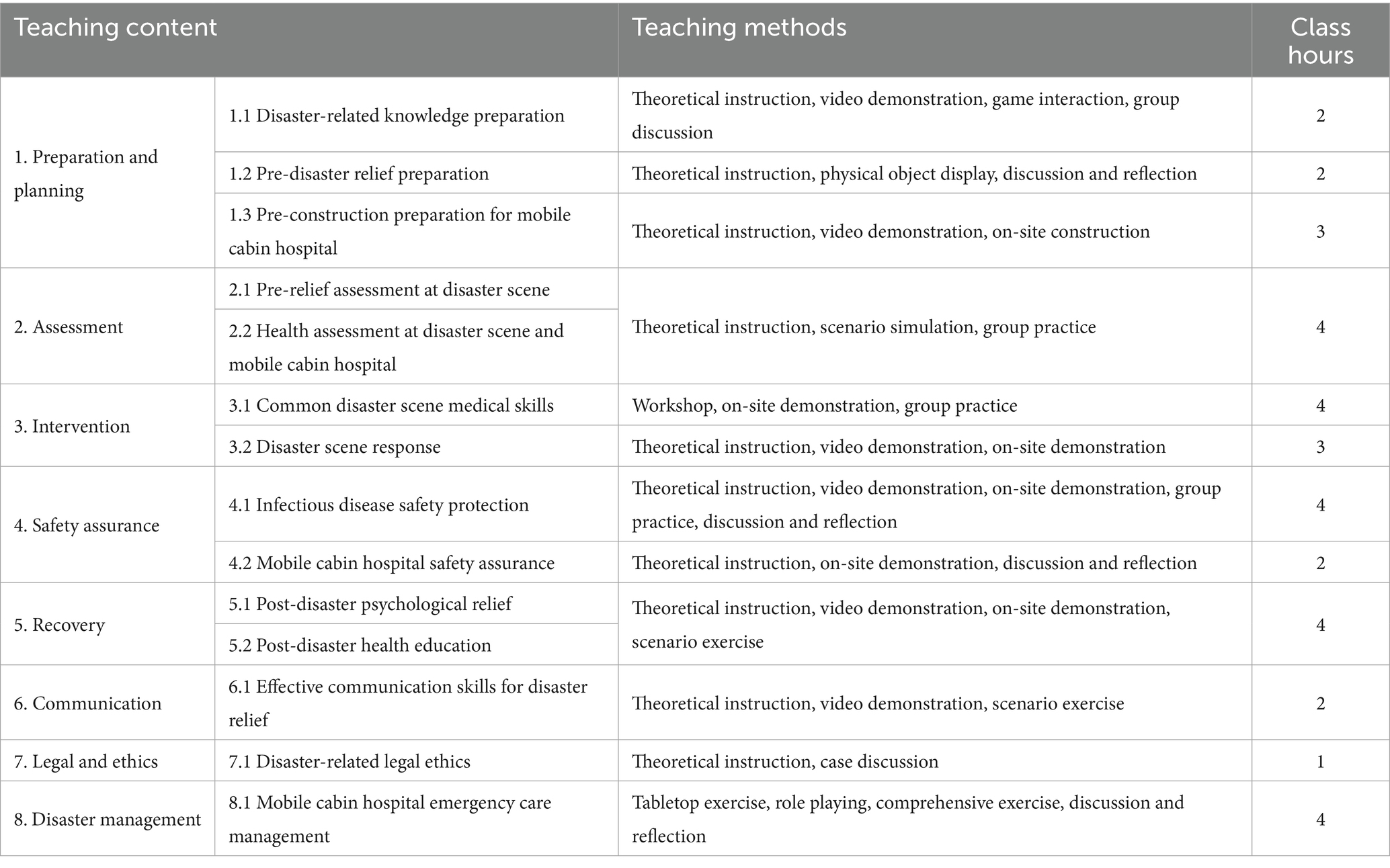
Table 4. Finalized training hours and instructional methods based on expert consultation.
4 Discussion
4.1 Importance of training program construction
Previous research has consistently demonstrated that newly graduated nurses often exhibit inadequate preparedness for disaster response, whereas nurses who have received disaster-specific training report significantly higher levels of readiness (7, 22–27). As a result, the development of disaster nursing competency is recognized as a critical factor in improving overall disaster response capability among nurses (28). Undergraduate nursing students are at a formative stage of professional development, during which their attitudes and conceptual understanding are particularly receptive to targeted educational interventions. This stage is considered the optimal period for integrating disaster nursing education into the curriculum (16, 27, 28).
The training program developed in the present study differs from conventional disaster training models that primarily emphasize preparedness and emergency response. Instead, this program adopts a structured, week-long format aligned with the complete disaster management cycle, including mitigation, preparedness, response, and recovery phases. Unlike the NDLS curriculum, this program not only emphasizes disaster triage and treatment protocols but also uniquely incorporates a “cabin hospital construction and operation” module—a feature rarely seen in existing international training systems. While the EPR framework focuses on cross-institutional collaboration, this program highlights efficient operations and team coordination within single-institutional settings with limited resources. As a result, it offers distinctive advantages in global disaster care education. Moreover, it incorporates practical clinical training in real-world mobile cabin hospital environments. Engaging nursing students early in such experiential learning is expected to enhance their awareness, improve disaster-related competencies, and increase their willingness to participate in future relief efforts. This approach may contribute to the development of a more resilient clinical reserve workforce capable of responding effectively in a variety of disaster contexts.
4.2 Scientific validity and reliability analysis of training program setup
At present, disaster nursing practical training programs tailored to undergraduate nursing interns in China remain in the exploratory phase, lacking a unified or standardized structure (4). In response to this gap, the present study utilized the ICN disaster competency framework and relevant literature as foundational references. Through the application of the Delphi, comprehensive expert feedback was gathered to guide the design and validation of the proposed Disaster Nursing Practice Week program. The training model was constructed through a rigorous and systematic process, ensuring both scientific validity and structural feasibility. The credibility of this methodological approach is supported by high expert response rates, elevated levels of expert authority, and a strong degree of consensus achieved across consultation rounds.
4.2.1 Representativeness of consultation experts
The expert panel included 15 experts from Beijing, Fujian, Sichuan, and Yunnan. Participants ranged in age from 35 to 56 years, with 20% under the age of 40, ensuring a reasonable age stratification. This allowed for the integration of senior experts’ in-depth professional experience and the innovative perspectives of younger professionals. Educational qualifications were generally high, with 93.3% of experts holding a master’s degree or above, indicating reliable academic and clinical backgrounds. The panel comprised experts from tertiary hospitals and academic institutions, representing diverse fields such as nursing education, nursing management, clinical nursing, emergency medicine, and disaster medical rescue. Furthermore, 11 experts had disaster relief experience (73.33%), 10 held associate senior-level or higher titles (66.67%), and 13 had over 15 years of professional experience (86.66%). This combination of geographic diversity, academic and clinical expertise, and appropriate stratification enhanced the representativeness and comprehensiveness of the expert panel.
4.2.2 Enthusiasm and authority of consultation experts
High response rates in Delphi consultations are indicative of strong engagement and alignment between the study topic and participants’ expertise (29). In the present study, both rounds of consultation achieved a 100% response rate, with 14 experts submitting detailed opinions across the two rounds. These results reflect a high degree of participation and interest. Expert authority was further assessed through self-reported familiarity and the rational basis for indicator evaluation. The calculated authority coefficient was 0.93, exceeding the accepted threshold of 0.80, thereby indicating that the experts possessed high levels of expertise and familiarity with disaster nursing, contributing to the credibility and reliability of the consultation findings.
4.2.3 High degree of consensus among consultation experts
Across the two rounds of expert consultation, the indicators in the training program consistently met established thresholds: mean importance scores ≥ 4.0, full score rate ≥ 20%, selection rate ≥ 80%, and coefficient of variation ≤ 0.20 (29). Based on expert feedback and internal discussions, the training modules, instructional content, duration, and teaching methods were finalized. The Kendall’s W coefficient reached 0.300 following the second round, aligning with the recommended coordination coefficient range of 0.3 to 0.5, with a p value <0.001 indicating statistical significance (30). These results indicate a high degree of consensus and coordination among expert opinions, supporting the reliability and validity of the finalized training program.
4.3 Rationality analysis of training program setup
4.3.1 Alignment with the eight core competencies of disaster nursing
The ICN and the World Health Organization (WHO) have jointly emphasized that nurses must be equipped with foundational knowledge and skills in disaster management in order to fulfill their roles effectively across all phases of disaster response (1). In 2009, the ICN and WHO released the disaster nursing competency framework, which was updated in 2019 to define core disaster nursing competencies tailored to nurses at varying levels of responsibility (9). These competencies encompass eight key domains: preparation and planning, communication, disaster management, safety assurance, assessment, intervention, recovery, and legal and ethical responsibilities. The development of these capabilities establishes the foundation for nursing personnel to assume effective roles during disasters. Level I competencies, applicable to registered nurses, include the ability to utilize basic first aid and professional nursing skills in disaster response scenarios (9, 11). As undergraduate nursing students represent a key reserve resource for disaster relief, the training program in this study was designed in accordance with the competencies outlined for registered nurses in the ICN framework. The primary indicators directly apply the eight core competencies of disaster nursing, closely adjusting the eight indicators according to the entire disaster management process, ultimately resulting in 47 secondary indicators. The program integrates competencies spanning pre-disaster preparation and planning, intervention during disasters, and post-disaster recovery, thereby facilitating comprehensive enhancement of disaster nursing competency among nursing interns. Compared to classic international models such as the National Disaster Life Support (NDLS) curriculum from the United States, the training program designed in this study also emphasizes core competencies such as ‘triage and on-site rescue,’ reflecting global consensus. However, the uniqueness of this training program lies in using mobile cabin hospitals as the core teaching scenario, designing a complete and immersive training process, providing a more aligned with real combat and systematic operational experience.
4.3.2 Integration with mobile cabin hospital training contexts
Disaster events are inherently unpredictable and are characterized by abrupt onset, high risk, and operational complexity, making real-world disaster scenario training impractical. As a result, simulation-based training has emerged as a highly effective educational strategy (22, 31–34). Simulation enables learners to develop skills and practice response techniques in controlled environments without endangering actual patients, while also improving assessment proficiency (22). Evidence from multiple studies indicates that simulated disaster environments enhance understanding of nursing roles, promote interdisciplinary collaboration, and strengthen team-based disaster mitigation and response efforts (22, 31–35). In the present training program, mobile cabin hospitals are used as the central context for simulation-based instruction. The curriculum includes pre-deployment preparation, facility setup, patient assessment, safety protocols, and management of the disaster response continuum. Compared to previous training, the training based on mobile cabin hospital mainly includes the following new aspects: First, it covers the preparation before the construction of a mobile cabin hospital and the setup process, which was not included in previous courses. This primarily trains medical staff’s organizational and planning abilities, as well as the process of building a hospital upon arriving at a disaster site, to familiarize them with the various functional units of the mobile hospital. Second, it focuses on the safety assurance of mobile field hospitals, which differs from routine safety assessments at disaster sites by adding management of the hospital environment, electricity, oxygen usage, etc. Third, it involves conducting various treatment techniques within mobile cabin hospitals, as well as psychological care. Third, it includes various treatment techniques conducted within mobile cabin hospitals, as well as psychological care and early rehabilitation care for patients after treatment. These components create immersive large-scale scenarios that allow students to experience and participate in each phase of disaster relief, thereby improving their perception and operational capabilities in disaster contexts.
4.3.3 Consideration of the specific demands of disaster relief
The training program was designed with explicit attention to the unique challenges of disaster relief. Given the urgent, unpredictable nature of disaster events, the curriculum includes modules on disaster knowledge, preparation of personal emergency equipment, and mobile cabin hospital readiness. To address the clinical challenges associated with mass casualty events and the need to care for vulnerable populations—including older adults, children, pregnant and postpartum women, bereaved individuals, and persons with disabilities—the program incorporates targeted modules on injury assessment, medical interventions, and population-specific nursing care. The program also incorporates components that address infectious disease containment, psychological support for both responders and victims, post-disaster health education, and ethical and legal challenges encountered in disaster scenarios. Additionally, recognizing the importance of interprofessional coordination during disaster response, the training also includes dedicated content on communication skills to enhance collaborative response effectiveness.
4.3.4 Alignment with the practical focus of clinical training
Currently, disaster nursing training in our country mainly targets in-school students, with relevant chapters added only to critical care nursing courses, or conducted sporadically as elective courses, without any clinical practice courses. A well-documented limitation in disaster nursing education is the gap between theoretical instruction and practical application in clinical settings (28). To address this gap, the current program focuses on the practical training needs of undergraduate nursing interns. The curriculum emphasizes hands-on participation in mobile cabin hospital deployment, triage procedures, trauma assessment, and essential clinical interventions such as hemostasis, bandaging, immobilization, transport, transfer, and cardiopulmonary resuscitation. Technical instruction includes the use of Level II personal protective equipment, rapid psychological assessment techniques, self-regulation strategies, and communication techniques. Through direct engagement with these practical tasks, nursing interns are better equipped to translate theoretical knowledge into practical competencies applicable in real-world disaster contexts.
4.4 Multi-modal training methods enhance instructional effectiveness
The number of disaster nursing training programs has steadily increased in recent years. While traditional training methods have relied heavily on didactic instruction, recent approaches have incorporated group discussion, action learning, problem-based learning, virtual platforms, disaster scenario simulations, tabletop exercises, and flipped classroom formats (22, 31–40). Although individual instructional methods can yield positive outcomes, the multifaceted nature of disaster nursing and the diverse learning preferences among students limit the effectiveness of single-mode approaches (23). Ngo et al. advocated for multi-modal, integrated training strategies as an effective approach to disaster education (41). Moreover, research indicates that no single instructional format has demonstrated superiority across all competency domains (22). Consequently, multi-modal teaching methods are recommended to optimize student engagement and competency acquisition. These methods have been shown to enhance performance in critical areas such as disaster perception, triage, clinical skills, crisis management, and problem-solving. For example, training conducted in mobile cabin hospital contexts has been demonstrated to improve situational awareness, while virtual reality and tabletop simulations have demonstrated effectiveness in improving disaster-related skills and perceptions (25, 42–45). Additional studies have reported that the use of disaster scene imagery, video demonstrations, case analyses, and personal narratives can increase nurses’ awareness of the need for continuous professional development, and enhance their confidence and motivation for participating in relief efforts (44). Therefore, the present training program incorporates a variety of instructional methods tailored to specific content domains, aiming to improve learning outcomes, increase student interest, and strengthen the acquisition of core disaster nursing competencies.
4.5 Research limitations
This study also has certain limitations. Firstly, the scheme established by this study heavily relies on the opinions of the expert panel. Although we invited experienced experts in the field, the majority of the panel members come from the same domestic healthcare system, which has geographical and institutional limitations. This may result in the scheme being more tailored to the specific operational model and cultural background of our country’s makeshift hospitals, and its general applicability, especially in different countries or healthcare systems, still needs further evaluation. Secondly, the current study has only completed the theoretical construction and preliminary validation of the scheme, without large-scale empirical application and effectiveness verification in real mobile makeshift hospitals. Therefore, the actual effectiveness of the scheme in improving team collaboration and patient outcomes still needs to be confirmed by subsequent empirical research. Finally, when constructing the scheme, this study mainly considered the typical static workflow of makeshift hospitals and did not fully incorporate their highly dynamic operational characteristics, such as sudden fluctuations in the number of patients, temporary supplementation of medical resources, dynamic expansion or reduction of cabin space, etc. These dynamic factors impose requirements for the flexibility and adaptability of the training scheme, which need to be key considerations in future research and updates to the scheme.
5 Conclusion
The present study adopted the revised Disaster Nursing Core Competencies released by the ICN in 2019 as the guiding theoretical framework and integrated these competencies with the operational context of mobile cabin hospitals. Through a comprehensive literature review and expert consultation process, a structured “disaster practice week” training program was developed for undergraduate nursing interns. The finalized program comprises 8 primary indicators, 14 secondary indicators, and 47 tertiary indicators. It incorporates clearly defined training content, instructional methods, and a designated schedule of training hours. The result is a comprehensive, practical, and adaptable model tailored to the specific demands of disaster nursing education. This program offers a standardized framework for the future implementation of disaster nursing training among nursing interns and holds significant potential for strengthening the preparedness and professional development of future disaster nursing personnel. In the future, we will conduct small-scale pilot studies through simulation exercises, using a pre-and-post comparison design, to preliminarily test the effectiveness and feasibility of the training program.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Fujian Provincial Hospital (Approval number: K2023-01-023). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LS: Data curation, Funding acquisition, Investigation, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. ML: Methodology, Project administration, Software, Validation, Visualization, Writing – review & editing. G-RJ: Data curation, Investigation, Project administration, Validation, Visualization, Writing – review & editing. J-MC: Conceptualization, Formal analysis, Methodology, Resources, Visualization, Writing – review & editing. Y-RL: Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft. SJ: Formal analysis, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Fujian Medical University Education and Teaching Research Project (J22019); Fujian Province Natural Science Foundation Youth Project (2024J08259).
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
ICN, International Council of Nurses; COVID-19, Coronavirus Disease 2019.
References
1. World Health Organization. International Council of Nurses ICN Framework of Disaster Nursing Competencies. Geneva Switzerland: WHO (2009).
2. Hung, MSY, Lam, SKK, Chow, MCM, Ng, WWM, and Pau, OK. The effectiveness of disaster education for undergraduate nursing students' knowledge, willingness, and perceived ability: an evaluation study. Int J Environ Res Public Health. (2021) 18:10545. doi: 10.3390/ijerph181910545
3. Motsepe, TL, and Schmollgruber, S. Emergency nurses' disaster preparedness competencies: a focused mapping review and synthesis. Health SA. (2025) 30:2770. doi: 10.4102/hsag.v30i0.2770
4. Kalanlar, B, and Akkaya, G. Nursing student's experiences of role-play scenario-based disaster triage (START) training: a qualitative research. Nurse Educ Today. (2024) 141:106307. doi: 10.1016/j.nedt.2024.106307
5. Zhang, YY, Zhu, LL, Sheng, Y, Li, XH, Xu, XH, and Wang, QY. Disaster nursing development in China and other countries: a bibliometric study. J Nurs Scholarsh. (2018) 50:567–76. doi: 10.1111/jnu.12401
6. Zheng, D, Zhang, H, Yuan, Y, Deng, Z, Wang, K, Lin, G, et al. Natural disasters and their impacts on the silica losses from agriculture in China from 1988 to 2016. Phys Chem Earth (Pt A/B/C). (2020) 115:102840. doi: 10.1016/j.pce.2020.102840
7. Yildirim, M, Bozdağ, F, and Başdaş, Ö. Experiences of nursing students providing support in disaster areas: a qualitative study. Public Health Nurs. (2024) 41:1622–32. doi: 10.1111/phn.13412
8. Firouzkouhi, M, Kako, M, Abdollahimohammad, A, Balouchi, A, and Farzi, J. Nurses' roles in nursing disaster model: a systematic scoping review. Iran J Public Health. (2021) 50:879–87. doi: 10.18502/ijph.v50i5.6105
9. International Council of Nurses. Core competencies in disaster nursing. (2019). (2019-11-05) [2024-02-10]. Available online at: https://www.icn.ch/sites/default/files/2023-04/ICN_Disaster-Comp-Report_WEB.pdf.
10. Bayageldi, NK, and Kaloğlu Binici, D. Are nursing students ready to respond to disasters? A study on self-efficacy of nursing students to apply psychological first aid. Nurse Educ Today. (2024) 143:106367. doi: 10.1016/j.nedt.2024.106367
11. Huang, XY, Mao, XR, Ma, QH, and Yang, WL. Interpretation of the 2019 edition of "Core competencies for disaster nursing" and its enlightenment to the development of disaster nursing in China. Chin Nurs Res. (2021) 35:2821–4. doi: 10.12102/j.issn.1009-6493.2021.16.001
12. Iserson, KV. Augmenting the disaster healthcare workforce. West J Emerg Med. (2020) 21:490–6. doi: 10.5811/westjem.2020.4.47553
13. Ranse, J, Ituma, OWN, Bail, K, and Hutton, A. Disaster education in undergraduate nursing curriculum: a Delphi study to prioritise content for nursing students. Collegian. (2022) 29:8. doi: 10.1016/j.colegn.2022.02.001
14. Shujuan, L, Mawpin, T, Meichan, C, Weijun, X, Jing, W, and Biru, L. The use of virtual reality to improve disaster preparedness among nursing students: a randomized study. J Nurs Educ. (2022) 61:93–6. doi: 10.3928/01484834-20211213-05
15. Gómez-Ibáñez, R, Watson, C, Leyva-Moral, JM, Aguayo-González, M, and Granel, N. Final-year nursing students called to work: experiences of a rushed labour insertion during the COVID-19 pandemic. Nurse Educ Pract. (2020) 49:102920. doi: 10.1016/j.nepr.2020.102920
16. Hardiyati, H, Iskandar, S, and Hernawaty, T. Nursing students' roles and experiences of disasters in a nursing school. Jurnal Keperawatan Padjadjaran. (2019) 7:1–19. doi: 10.24198/jkp.v7i1.410
17. Loke, AY, Guo, C, and Molassiotis, A. Development of disaster nursing education and training programs in the past 20 years (2000-2019): a systematic review. Nurse Educ Today. (2021) 99:104809. doi: 10.1016/j.nedt.2021.104809
18. Zhang, LY, Lang, HJ, Hu, SB, Xu, L, and Liu, XW. Teaching design of the course "field and disaster nursing". China J Emerg Resusc Disaster Med. (2020) 15, 1114–7. doi: 10.3969/j.issn.1673-6966.2020.09.029
19. Li, N, Zhong, ZY, Cheng, LN, and Tian, ZX. Bibliometric study on disaster nursing curriculum. Chin Evid Based Nurs. (2018) 4:4.
20. Han, JS, Wu, QJ, Wang, LZ, and Tan, SL. Design of the cabin-tent passage for mobile hospital. Chin J Med Instrum. (2017) 38:5. doi: 10.7687/j.issn1003-8868.2017.08.021
21. Wang, HJ, Yu, X, Wang, ZY, Tian, JJ, and Jiang, XQ. Design of a new intelligent expandable mobile cabin hospital. Chin Med Equip. (2020) 17:197–200. doi: 10.3969/J.ISSN.1672-8270.2020.05.043
22. Noh, J, Oh, EG, Kim, SS, Jang, YS, Chung, HS, and Lee, O. Development and evaluation of a multimodality simulation disaster education and training program for hospital nurses. Int J Nurs Pract. (2020) 26:e12810. doi: 10.1111/ijn.12810
23. Jose, MM, and Dufrene, C. Educational competencies and technologies for disaster preparedness in undergraduate nursing education: an integrative review. Nurse Educ Today. (2014) 34:543–51. doi: 10.1016/j.nedt.2013.07.021
24. Austin, EN, Hannafin, NM, and Nelson, HW. Pediatric disaster simulation in graduate and undergraduate nursing education. J Pediatr Nurs. (2013) 28:393–9. doi: 10.1016/j.pedn.2012.12.004
25. Currie, J, Kourouche, S, Gordon, C, Jorm, C, and West, S. Mass casualty education for undergraduate nursing students in Australia. Nurse Educ Pract. (2018) 28:156–62. doi: 10.1016/j.nepr.2017.10.006
26. Alexander, AJ, Bandiera, GW, and Mazurik, L. A multiphase disaster training exercise for emergency medicine residents: opportunity knocks. Acad Emerg Med. (2005) 12:404–9. doi: 10.1197/j.aem.2004.11.025
27. Huh, SS, and Kang, HY. Effects of an educational program on disaster nursing competency. Public Health Nurs. (2019) 36:28–35. doi: 10.1111/phn.12557
28. Kula, Y, Cohen, O, Clempert, N, Grinstein-Cohen, O, and Slobodin, O. Educating nursing students for cultural competence in emergencies: a randomized controlled trial. BMC Nurs. (2021) 20:184. doi: 10.1186/s12912-021-00704-1
29. Hu, X. Research on competency-based disaster nursing training curriculum [dissertation]. Hubei: Huazhong University of Science and Technology (2019).
30. Zeng, G. Modern epidemiology: methods and applications. Beijing: Peking Union Medical College Press. (1994).
31. Heyn, LG, Brembo, EA, Byermoen, KR, Cruaud, C, Eide, H, Flo, J, et al. (2023). Exploring facilitation in virtual simulation in nursing education: A scoping review. PEC innovation, 3:100233. doi: 10.1016/j.pecinn.2023.100233
32. Kaplan, BG, Connor, A, Ferranti, EP, Holmes, L, and Spencer, L. Use of an emergency preparedness disaster simulation with undergraduate nursing students. Public Health Nurs. (2012) 29:44–51. doi: 10.1111/j.1525-1446.2011.00960.x
33. Park, YM, and Hwang, WJ. Development and effect of a simulation-based disaster nursing education program for nursing students using standardized patients. J Nurs Res. (2024) 32:e314. doi: 10.1097/jnr.0000000000000596
34. Emaliyawati, E, Ibrahim, K, Trisyani, Y, and Songwathana, P. The effect of integrated simulation experiential learning disaster nursing for enhancing learning outcomes among undergraduate nursing students: a quasi-experimental study. Adv Med Educ Pract. (2025) 16:311–21. doi: 10.2147/AMEP.S489163
35. Chan, SS, Chan, WS, Cheng, Y, Chan, SSS, Chan, W‐s, Fung, OWM, et al. Development and evaluation of an undergraduate training course for developing International Council of Nurses disaster nursing competencies in China. J Nurs Scholarsh. (2010) 42:405–13. doi: 10.1111/j.1547-5069.2010.01363.x
36. Sun, J. Construction of core knowledge system for disaster nursing specialist nurse training course [dissertation]. Shandong: Shandong University (2014). Available at: https://kns.cnki.net/kcms2/article/abstract?v=w3MPIJRjtYHNVmiC61vT1tu_PlHg8oRQ8lBcUsBgUreAae0k2sFsLrrRWJ-b9WfxEY2rmfeK1BmSUm9q8J4BgTARQsh7ttgsbgwOaoIPia0xniQvZVt8JmHqw9qAuuu0By0lbufb552tKkuEERn0SWuACHrVCCRS8xV6WEECh49L7dykScY4dQ==&uniplatform=NZKPT&language=CHS
37. Hung, MSY, Lam, SKK, and Chow, MCM. Nursing students' experiences and perceptions of learner-centred education in a disaster nursing course: a qualitative study. Nurse Educ Pract. (2020) 47:102829. doi: 10.1016/j.nepr.2020.102829
38. Evans, CA, and Baumberger-Henry, M. The tabletop matrix: determining reliability for a criterion-referenced performance measure. J Nurs Educ. (2017) 56:509–13. doi: 10.3928/01484834-20170712-12
39. Kim, SK, Lee, Y, Yoon, H, and Choi, J. Adaptation of extended reality smart glasses for Core nursing skill training among undergraduate nursing students: usability and feasibility study. J Med Internet Res. (2021) 23:e24313. doi: 10.2196/24313
40. Gandhi, S, Glaman, R, Yeager, J, and Smith, M. Evaluation of anxiety and self-confidence among baccalaureate nursing students post pandemic simulation exercise. Clin Simul Nurs. (2021) 56:91–8. doi: 10.1016/j.ecns.2021.04.007
41. Ngo, J, Schertzer, K, Harter, P, and Smith-Coggins, R. Disaster medicine: a multi-modality curriculum designed and implemented for emergency medicine residents. Disaster Med Public Health Prep. (2016) 10:611–4. doi: 10.1017/dmp.2016.8
42. Jian, GR, Shi, L, Ye, CD, Chen, Y, and Jin, S. Application effect and influencing factors of scenario-based teaching method based on mobile cabin hospital in the training of nurses' disaster nursing ability. Chin J Disaster Med. (2018) 6:11–4. doi: 10.13919/j.issn.2095-6274.2018.01.003
43. Collander, B, Green, B, Millo, Y, Shamloo, C, Donnellan, J, and DeAtley, C. Development of an "all-hazards" hospital disaster preparedness training course utilizing multi-modality teaching. Prehosp Disaster Med. (2008) 23:63–7. doi: 10.1017/s1049023x00005598
44. Guan, XP. Two suggestions for disaster rescue nursing training. Chin J Nurs. (2009) 44:638. doi: 10.3761/j.issn.0254-1769.2009.07.024
Keywords: Delphi method, disaster nursing, mobile cabin hospital, practical training program, undergraduate nursing interns
Citation: Shi L, Liu M, Jian G-R, Chen J-M, Li Y-R and Jin S (2025) Development of a disaster nursing training program for undergraduate interns in mobile cabin hospital settings. Front. Public Health. 13:1672455. doi: 10.3389/fpubh.2025.1672455
Edited by:
Ebtsam Aly Abou Hashish, Alexandria University, EgyptReviewed by:
Rajamohanan Pillai, Kerala University of Health Sciences, IndiaAyşe Yildiz Keskin, Mersin University, Türkiye
Katherine Holbrook, University of California, San Francisco, United States
Copyright © 2025 Shi, Liu, Jian, Chen, Li and Jin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lan Shi, c2hpbGFuQGZqbXUuZWR1LmNu; Shuang Jin, amluczAzMDVAMTYzLmNvbQ==
‡ORCID: Lan Shi, orcid.org/0000-0002-6018-6869
†These authors have contributed equally to this work