 Morin Lang
Morin Lang Chiara Cazzuffi
Chiara Cazzuffi Ginés Viscor
Ginés Viscor Johana Soto-Sánchez
Johana Soto-Sánchez- 1Department of Physical Therapy, Faculty of Medicine, University of Chile, Santiago, Chile
- 2Faculty of Medicine, School of Kinesiology, Universidad Finis Terrae, Santiago, Chile
- 3Centro de Economía y Políticas Sociales (CEAS), Facultad de Ciencias Sociales y Artes, Universidad Mayor, Santiago, Chile
- 4Centro de Biomedicina, Laboratorio de Actividad Física, Ejercicio y Salud, Santiago, Chile
- 5Department of Cell Biology, Physiology and Immunology, Faculty of Biology, Universitat de Barcelona, Barcelona, Spain
- 6Centro de Biomedicina, Laboratorio de Actividad Física, Ejercicio y Salud, Universidad Mayor, Huechuraba, Chile
Women working in high-altitude (HA) mining environments are exposed to chronic intermittent hypoxia (CIH), a physiological stressor resulting from rotating work shifts between sea level and elevations typically above 3,000 meters above sea level (m.a.s.l). CIH involves repeated exposure to hypobaric hypoxia, imposing significant biological, psychological, and social demands. Despite increasing female participation in the mining sector, the long-term cardiovascular risks specific to women in these conditions remain poorly characterized. This mini-review introduces the Gender-Integrated Biopsychosocial Model (GBM). This conceptual framework integrates biological, psychological, and social dimensions to examine how sex hormones, emotional burden, and gendered occupational exposures shape cardiovascular and autonomic responses to CIH. Unlike existing models that primarily reflect male physiology, the GBM emphasizes the role of natural cycling hormonal fluctuations, contraceptive use, menopause, and structural inequities in modulating cardiovascular adaptation. By advancing a multidimensional, sex and gender informed perspective, the GBM offers a novel approach to understanding women's health in extreme environments and highlights the need for occupational and environmental physiology research to recognize gender not merely as a biological variable, but as a determinant of cardiovascular risk. This article contributes to the understanding of environmental and occupational hazards in extreme workplaces by introducing an integrative model that addresses gendered exposures and physiological responses under chronic intermittent hypoxia.
Introduction
Women working in high-altitude (HA) mining operations in Chile are exposed to intricate physiological, psychological, and social stressors, attributable to the 7 × 7-day rotating shift schedule. This schedule alternates between work at elevations exceeding 3,000 m.a.s.l. and rest at sea level. Such a pattern serves as an empirical model of chronic intermittent hypobaric hypoxia (CIH), a condition acknowledged in Decree No. 28 (1). Regarding its hazards to the cardiopulmonary and neurological systems, research involving male miners has demonstrated immediate elevations in blood pressure (BP) and heart rate (HR), along with a reduction in oxygen saturation during initial exposure at high altitude (HA) (2), with numerous cases surpassing diagnostic hypertension thresholds under 24-h ambulatory monitoring (3). However, these findings have seldom been generalized to women, as they may exhibit different cardiovascular responses owing to hormonal, emotional, and social factors.
Although traditional cardiovascular risk factors (e.g., hypertension, obesity, smoking, physical inactivity) are prevalent among miners (4). Research has not sufficiently addressed how these risks manifest in women under sex-specific exposures. Factors such as menstrual cycle, contraceptive use, work-family conflict, perceived discrimination, and symbolic violence in male-dominated settings may exacerbate cardiovascular strain. Despite increased female participation in mining (15% as of 2022), equity gaps persist, especially in access to data on workload, work shift patterns, and job roles (5, 6).
To address these intersecting challenges, we introduce a Gender-Integrated Biopsychosocial Model (GBM), grounded in George L. Engel's original framework (7), and adapted to the environmental and gendered context of high-altitude mining. This model conceptualizes cardiovascular risk as a dynamic product of: (a) biological factors: hormonal regulation and reproductive history, cardiovascular and cardiac autonomic responses, and physical workload and nutritional status under hypoxia; (b) psychological factors: mental workload, emotional strain and coping perception, and circadian and neuroendocrine stress; and (c) social factors: work-family balance, workplace dynamics, and structural barriers to women's health.
The GBM provides a novel interdisciplinary framework for evaluating how these dimensions interact under conditions of CIH. It also establishes a foundation for developing interventions aimed at improving cardiovascular health from a gender-equitable and context-sensitive perspective. The GBM synthesizes biological, psychological, and social determinants to explain cardiovascular risk in women exposed to CIH, providing a structured framework for the review, as illustrated in Figure 1.
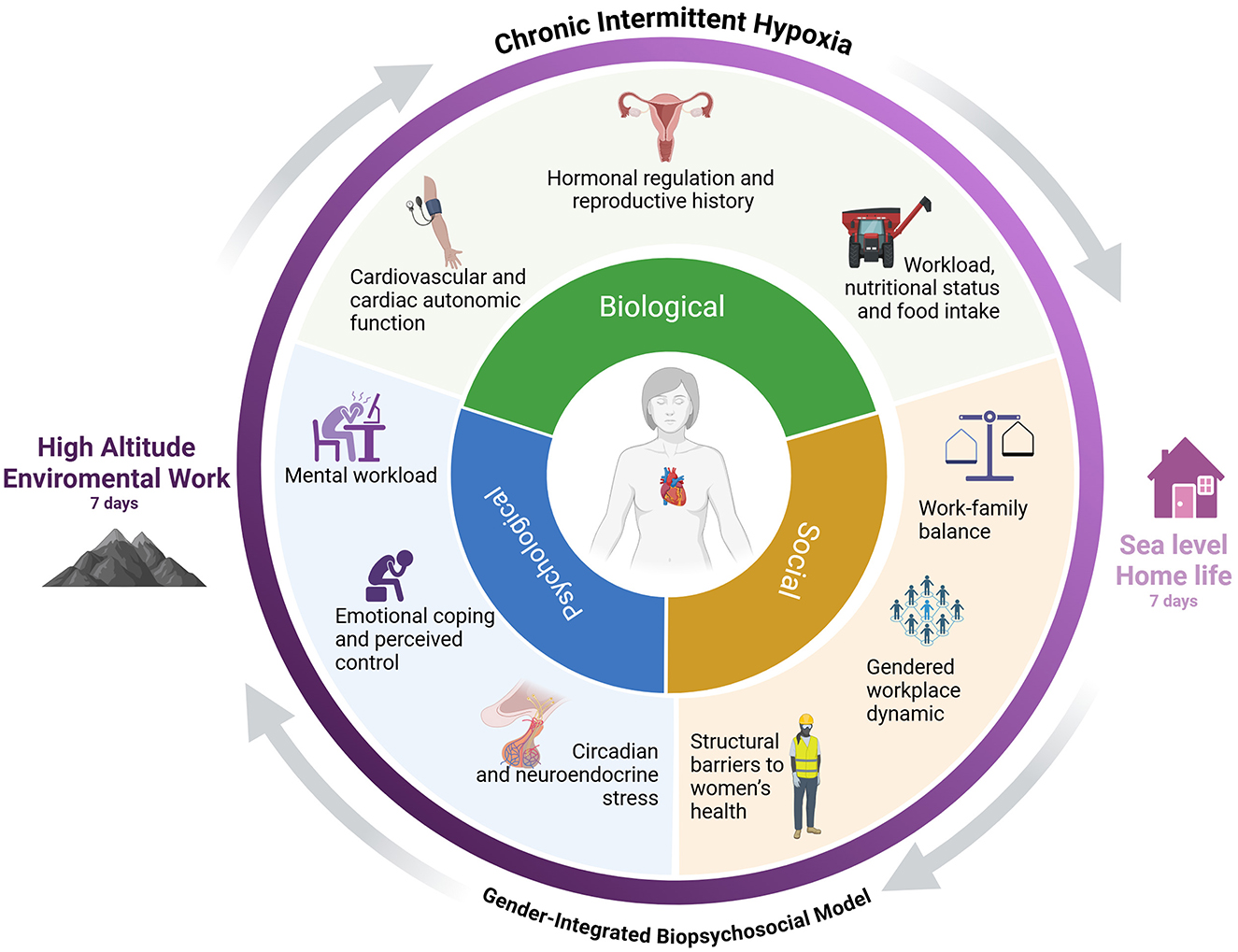
Figure 1. Gender-Integrated Biopsychosocial Model (GBM) of cardiovascular risk in women exposed to chronic intermittent hypoxia. This conceptual model illustrates three interrelated dimensions: Biological, Psychological, and Social, each comprising key subcomponents that contribute to cardiovascular risk in women working under conditions of chronic intermittent hypoxia (CIH), such as high-altitude mining. Biological factors include hormonal regulation and reproductive history, cardiovascular and autonomic responses, workload, nutritional status, and food intake. Psychological factors involve mental workload, emotional strain, and circadian or neuroendocrine stress. Social factors encompass work–family balance, gendered workplace dynamics, and structural barriers to women's health. Created in https://BioRender.com.
The aim of this mini-review is to introduce and contextualize the GBM as a guiding framework for future research design, facilitating a deeper understanding of cardiovascular risk in women exposed to CIH, with a particular focus on sex- and gender-specific mechanisms that are still critically understudied within environmental and occupational physiology. Table 1 consolidates the main sex-based (biological) and gender-based (sociocultural) determinants of cardiovascular risk encompassed within the GBM framework.
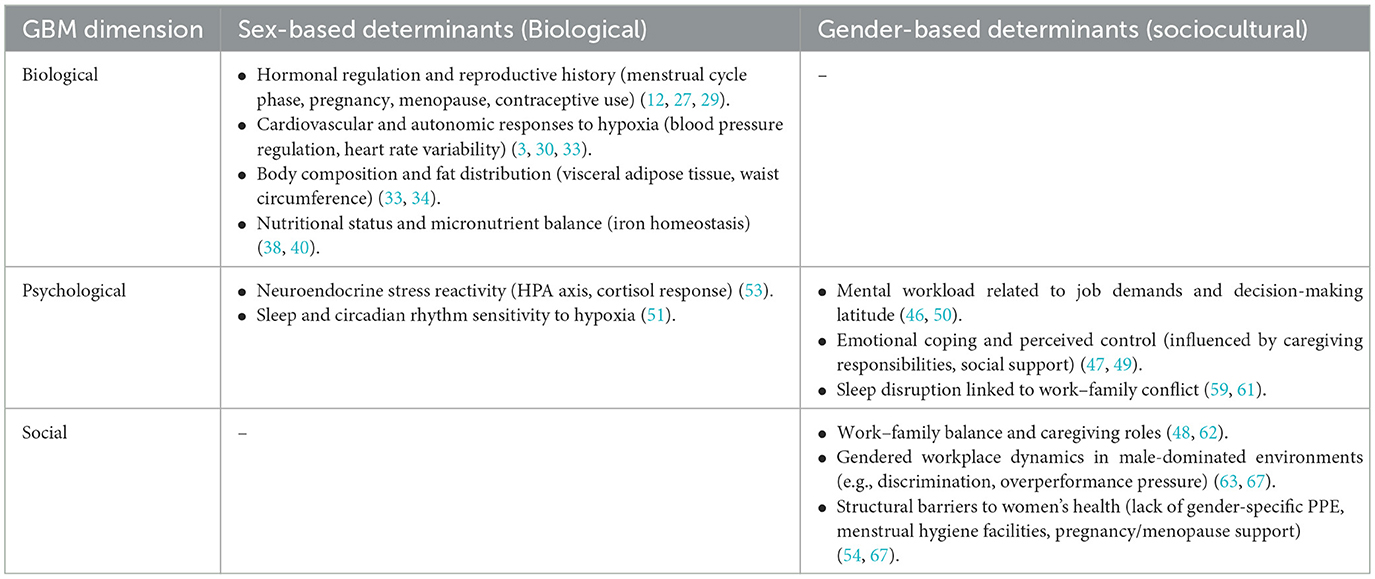
Table 1. Sex-based (biological) and gender-based (sociocultural) determinants of cardiovascular risk in women exposed to chronic intermittent hypoxia according to the Gender-Integrated Biopsychosocial Model (GBM).
Biological dimension
Working at high altitudes encompasses a broad spectrum of risks, both climatic, ranging from frostbite to heat stroke, and occupational, including fatigue and circadian rhythm disturbances, which can affect individuals irrespective of gender or age. The focus will be on how sex and gender differences markedly influence cardiovascular biology and disease progression. In specific underlying conditions such as hypertension, obesity, and diabetes, women frequently display unique epidemiological profiles; however, clinical guidelines continue to underrepresent sex-specific considerations in diagnosis and treatment (8–10). In HA mining environments, women continue to be underrepresented in physiological research, thereby constraining our comprehension of their adaptations to CIH (11). In the GBM model (Figure 1), the biological dimension is organized into three primary subcomponents: hormonal status and reproductive history, cardiovascular and autonomic function, as well as physical workload, nutritional status, and food intake. These elements are further elaborated upon in this section under more specific thematic subtitles.
Women's cardiovascular risk profile
Cardiovascular (CV) risk profiles differ between women and men due to sex-specific factors. Women face additional risks related to their reproductive history, such as adverse pregnancy outcomes, including preeclampsia and gestational diabetes (12, 13). Conditions such as polycystic ovary syndrome, early menopause, and autoimmune diseases further increase the risk (14, 15). Traditional risk factors such as diabetes and smoking confer greater relative risks in women (16, 17), and the menopause transition accelerates vascular and metabolic changes (18). Recognizing these factors facilitates the early identification of women at high risk and enables the implementation of targeted prevention strategies (19). Their presence may exacerbate cardiovascular strain in combination with environmental stressors such as CIH.
Hormonal regulation and cardiovascular response
Hormonal regulation plays a crucial role in cardiovascular physiology, autonomic function, and body composition, directly impacting cardiovascular risk. Estradiol (E2) facilitates vasodilation via nitric oxide (NO) synthesis, thereby enhancing endothelial function and reducing blood pressure (20–22). Conversely, progesterone (P4) and androgens promote sodium retention, sympathetic nervous system activity, autonomic imbalance, and an increase in visceral adiposity and waist circumference, thereby collectively elevating cardiovascular risk (23–26). E2 has demonstrated vasoprotective and hypotensive effects across multiple vascular beds (22, 27, 28). In eumenorrheic women, hormonal fluctuations throughout the menstrual cycle substantially influence cardiovascular autonomic regulation. The follicular phase, characterized by elevated (E2), favors parasympathetic dominance, resulting in relative bradycardia and hypotension. Conversely, the luteal phase, marked by increased (P4), encourages sympathetic activation, leading to higher blood pressure (BP), increased HR, reduced heart rate variability (HRV), and heightened cardiovascular strain (27, 29–31). Furthermore, androgen-dominant conditions, such as the use of oral contraceptives (OCs) exhibiting high androgenic activity or menopause without the administration of hormone replacement therapy (HRT), are correlated with estrogen deprivation, persistent sympathetic activation, reduced vasodilation, and increased autonomic imbalance (32).
Conversely, women generally demonstrate a higher total fat mass at a specific body mass index (BMI), primarily characterized by gluteofemoral adipose tissue accumulation. In comparison, men exhibit greater fat-free mass (FFM) but possess a higher amount of visceral adipose tissue (VAT), which is a significant risk factor for CVD (33). Nonetheless, increased androgen levels in females (such as obesity, PCOS, and post-menopause) may modify their typical fat deposition patterns, increasing VAT and waist circumference (WC), thereby increasing cardiovascular risk (26, 34–36).
Therefore, it is essential to comprehensively consider hormonal profiles, contraceptive use, and menopausal status when evaluating cardiovascular risk, particularly in women exposed to CIH at HA. We hypothesize that variations in hormonal status substantially influence cardiovascular and autonomic responses in women subjected to CIH. States characterized by estrogen dominance are presumed to promote cardiovascular adaptation, whereas states dominated by progesterone and androgens may elevate cardiovascular strain during exposure to hypobaric hypoxia. Figure 2 summarizes the hypothetical responses corresponding to hormonal status relevant to high-altitude occupational exposure in women.
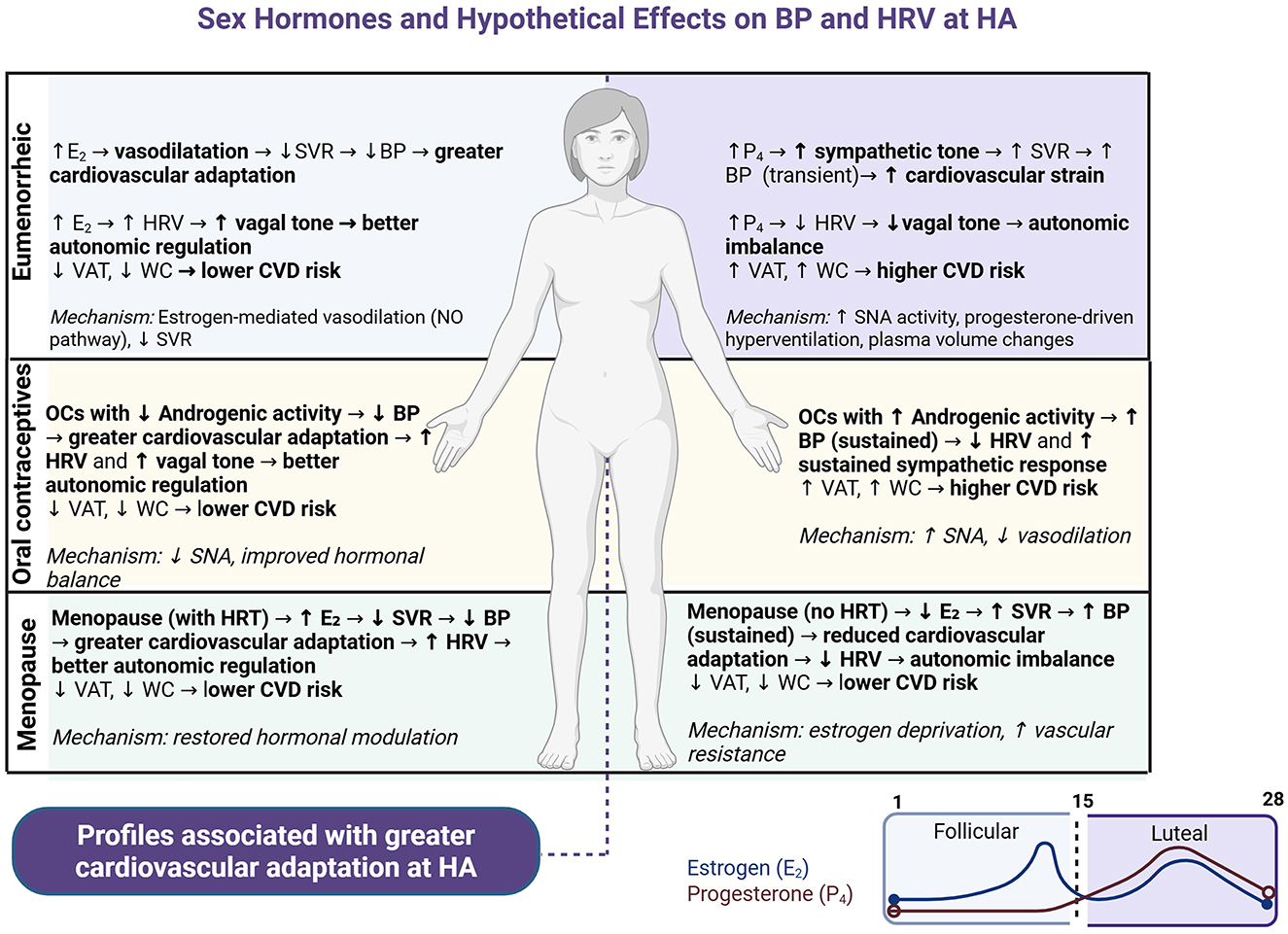
Figure 2. Hypothetical effects of sex hormones on Blood Pressure (BP), Heart Rate Variability (HRV), and body composition in women exposed to Chronic Intermittent Hypoxia (CIH). This diagram illustrates proposed cardiovascular, autonomic, and body composition responses across different hormonal profiles in women. Estrogen-dominant states [e.g., follicular phase, low-androgenic oral contraceptives (OCs), menopause with hormone replacement therapy (HRT)] promote vasodilation, enhanced HRV, decreased visceral adipose tissue (VAT), and waist circumference (WC), collectively contributing to improved cardiovascular adaptation. Conversely, progesterone-dominant or androgenic conditions (e.g., luteal phase, androgenic OCs, menopause without HRT) increase sympathetic nervous activity, reduce HRV, and elevate VAT and WC, thereby increasing cardiovascular strain. “Transient” BP changes refer to short-term elevations typically observed during luteal-phase hormonal shifts. “Sustained” BP indicates chronic or long-lasting elevations associated with persistent hormonal environments in women residing at high altitude.
Workload, nutrition, and food intake sex-based responses to hypoxia
Workload and nutritional status critically interact with hormonal and reproductive factors to modulate cardiovascular and reproductive strain in women working at HA. Mining activities generally entail extended periods of standing, manual exertion, and continuous physical effort in cold, dry, and hypoxic environments. These operations impose considerable physiological stress owing to decreased oxygen availability resulting from a hypobaric setting. In comparison to men, women consistently demonstrate higher HR, increased ventilatory responses, and greater perceived exertion at comparable levels of workload (30, 37). These characteristics are further influenced by the menstrual cycle, wherein increased P4 levels during the luteal phase enhance sympathetic activity and ventilatory drive, thereby intensifying cardiovascular burden (27).
Nutritional status considerably impacts physiological adaptation to HA. Inadequate energy intake and deficiencies in micronutrients, especially iron, can compromise vascular function, intensify oxidative stress, and disturb hormonal equilibrium. Women residing at altitude are susceptible to iron depletion, which adversely affects both cardiovascular performance and reproductive health (38, 39). Furthermore, the menstrual cycle influences iron homeostasis by connecting hormonal fluctuations to nutrient metabolism (38, 40). Both iron deficiency and overload are associated with adverse reproductive outcomes, underscoring the sensitivity of female fertility to nutritional balance (41, 42). Importantly, these nutritional factors align with hormonal influences on body composition, particularly leading to increased VAT and WC in androgenic profiles (obesity, PCOS, post-menopause). This central fat redistribution directly contributes to heightened cardiovascular risk, as previously described (26, 34).
Despite these well-established links, current occupational health frameworks seldom account for sex-specific nutritional, cardiovascular, and hormonal interactions. An integrated approach is necessary to safeguard the wellbeing and optimize the performance of women operating in extreme environments, such as high-altitude mining.
Hypertension, a prominent cardiovascular risk factor among the Chilean population, has been extensively documented in male miners exposed to CIH (3, 43). Nevertheless, limited research has assessed the interaction between workload intensity and nutritional status with sex-specific mechanisms in influencing blood pressure regulation among women engaged in employment HA.
Pregnancy and CIH exposure
Although Chilean occupational health regulations explicitly prohibit pregnant women from working at altitudes exceeding 3,000 meters above sea level (1). There is no unified international legal framework governing pregnancy and occupational exposure to high altitudes. Nonetheless, international clinical and mountaineering guidelines generally advise against prolonged work or physical exertion at elevations exceeding 2,500–3,000 meters, particularly beyond 20 weeks of pregnancy and in the presence of risk factors such as anemia, hypertension, or a history of pregnancy complications (70, 71, 74). These recommendations are grounded in evidence indicating that hypobaric hypoxia has the potential to impair maternal–fetal oxygen exchange, elevate the risk of pre-eclampsia, and contribute to fetal growth restriction, especially in women who are not chronically acclimated to high altitude.
In the rare event that a pregnant worker is unintentionally exposed to CIH such as during unrecognized pregnancy or in countries without occupational restrictions, the combined hemodynamic load of pregnancy and the hypoxic stress of high-altitude work could exacerbate oxygen supply demand mismatches in the maternal circulation (44), a non-atherothrombotic ischemic event associated with increased morbidity and mortality. This pathophysiological mechanism is recognized in humans as a precipitant of Type 2 myocardial infarction. Clinical studies have shown that hypoxemia and anemia, both relevant to CIH, are independent predictors of worse outcomes in Type 2 MI. While no direct data exist for pregnant women under CIH, the overlap of these risk factors underscores the importance of early pregnancy detection, careful cardiovascular risk assessment, and adherence to preventive measures even in settings without legal prohibitions.
Psychological dimension
Despite operating within a secure environment concerning gender equality and mutual sexual respect, women employed in the HA mining sector encounter a multifaceted set of psychological stressors that may augment cardiovascular risk. These encompass elevated cognitive demands, emotional stress associated with work–family conflicts, social isolation, and disturbances in sleep patterns. Such factors interact with neuroendocrine and autonomic systems, resulting in increased sympathetic activity and impaired BP regulation, which are indicative of cardiovascular dysregulation.
Mental workload
A notable construct is mental workload, which pertains to the cognitive and emotional demands imposed by the work environment. Extended 12-h shifts, night work, and critical decision-making under pressure, particularly in hypoxic conditions, may lead to cognitive fatigue and impair executive functioning (45). According to the Demand-Control-Support model (46), Psychological strain intensifies when employees encounter high demands, limited autonomy, and minimal social support. These factors interact with neuroendocrine and autonomic systems, resulting in increased sympathetic activity and impaired BP regulation, which are characteristic of cardiovascular issues dysregulation.
Emotional coping and perceived control
Women engaged in HA mining frequently encounter a conflict between their professional roles and caregiving responsibilities. Although this conflict is mediated by social factors, its psychological impacts are significant. Emotional tension, feelings of guilt, and diminished perceived control, especially among single mothers or individuals with limited familial support, can accumulate and manifest as chronic stress responses (47, 48). From a psychological standpoint, Bandura's theory of self-efficacy (49) highlights the protective role of perceived control in buffering these effects. Nevertheless, within male-dominated hierarchical settings, women frequently report diminished self-efficacy and limited decision-making autonomy (50).
These emotional stressors activate the hypothalamic-pituitary-adrenal (HPA) axis, thereby initiating the general stress response, or general adaptation syndrome (GAS). This leads to elevated cortisol levels, sympathetic overactivation, and vagal withdrawal. Such neuroendocrine imbalance disrupts cardiovascular homeostasis, fostering vascular inflammation, endothelial dysfunction, and heightened blood pressure variability, particularly during sleep and early morning hours.
Circadian and neuroendocrine stress
Sleep disturbances represent among the most widespread psychological and physiological stressors encountered in high-altitude environments. High-altitude exposure adversely affects REM sleep and overall sleep efficiency, with a notably greater impact observed in women, who demonstrate increased susceptibility to these effects (51). Poor sleep quality is correlated with diminished parasympathetic activity and heightened cardiovascular stress (52). Recent evidence indicates that psychological stress at HA may also influence neuroendocrine pathways implicated in mood regulation and circadian physiology, notably the tryptophan–serotonin–melatonin axis, which is affected by hypoxic exposure. In women, sex-specific differences in serotonin synthesis and the modulatory role of estrogen amplify these modifications (51). Hypoxia-induced insomnia, coupled with diminished levels of serotonin and melatonin, may result in compromised thermoregulation and synaptic plasticity, thereby disrupting memory consolidation and emotional regulation. This sequence creates a neurobehavioral feedback loop in which stress, insomnia, and mood instability reinforce each other, exacerbating autonomic dysregulation and elevating cardiovascular workload over time.
Together, these psychological stressors facilitate cardiovascular dysregulation via persistent activation of the HPA axis, autonomic imbalance, and disruption of circadian rhythms. This neuroendocrine imbalance promotes vascular inflammation, endothelial dysfunction, and blood pressure dysregulation, which are fundamental mechanisms in the pathogenesis of cardiovascular disease (53). Within the GBM framework, these mechanisms emphasize the importance of assessing mental workload, coping capacity, and sleep quality as pivotal determinants of cardiovascular risk in women subjected to CIH.
Social dimension
Psychosocial wellbeing, defined as the interaction among emotional, cognitive, and social functions, is integral to both mental and physical health. In high-altitude mining, social determinants of health include hierarchical workplace relationships, gendered role expectations, and the organization and social interpretation of work (54, 55). These environments are characterized by chronic intermittent hypoxia (CIH), extreme isolation, and rotational or fly-in, fly-out (FIFO) work schedules (4, 56). For women, these structural and cultural conditions may amplify the psychological stressors described above, particularly work–family conflict, limited decision-making autonomy, and reduced social support. While the physiological mechanisms, such as autonomic imbalance, vascular inflammation, and blood pressure dysregulation, are discussed in the psychological dimension, here we emphasize that the origin and persistence of these responses are strongly shaped by social context. Moreover, prolonged exposure to gendered workplace dynamics and inadequate health infrastructure may also impact reproductive health through hormonal disruptions and fertility-related issues (57, 58).
Work-family balance
Women in mining work report higher levels of work-family conflict compared to men (59, 60). Extended work shifts, camp-based rotations, and FIFO arrangements may lead to extended periods of separation from children and family members. The logistical challenges of caregiving, whether involving bringing children into camp settings lacking childcare services or leaving them behind, can induce ongoing stress characterized by persistent feelings of guilt, anxiety, and emotional strain, particularly among single mothers who lack reliable caregiving support (47, 48, 61, 62). These stressors are not solely psychological; they trigger neuroendocrine responses derived from the general stress response, which elevate allostatic load and potentially increase cardiovascular strain over time.
Gendered workplace dynamics
A secondary approach concerns the challenges related to workplace dynamics in predominantly male mining environments, which are generally characterized by isolated settings (63–66). Women frequently observe the necessity to exert exceptional effort to establish credibility, encounter limited access to decision-making roles, and endure scrutiny concerning their reproductive or maternal status (48, 50, 67). These conditions promote persistent hypervigilance, emotional suppression, and even burnout—factors directly correlated with elevated sympathetic tone, reduced HRV, and an increased risk of hypertension (55).
Structural barriers to women's health
Certain infrastructural deficiencies and policy shortcomings may further exacerbate women's vulnerability to stress. Numerous mining sites are inadequately equipped with gender-specific protective equipment, menstrual hygiene amenities, and comprehensive healthcare support, particularly during pregnancy or menopause (54, 67). Even when women develop coping strategies, they often do so independently, in isolation, and without specialized institutional support. Such circumstances exert pressure to internalize and somatize systemic stressors as individual burdens, thereby increasing perceived helplessness and diminishing psychosocial resilience. Consequently, this may elevate cardiovascular risk (54, 67). Together, these social stressors do not operate independently; they interact dynamically with biological (e.g., hormonal) and psychological (e.g., sleep, mood) factors, collectively contributing to an elevated risk of persistent hypertension and cardiovascular dysregulation in women subjected to CIH.
Prognostic implications of CIH in women
Prolonged exposure to chronic intermittent hypobaric hypoxia (CIH) may predispose women to cardiovascular changes that extend beyond immediate adaptation. Evidence from human studies involving rotating-shift workers subjected to high-altitude CIH indicates elevations in asymmetric dimethylarginine (ADMA), a biomarker of endothelial dysfunction and a predictor of hypoxia-induced pulmonary hypertension (72). These alterations, together with persistent hypoxaemia, surges in hypertension, and elevated sympathetic activity, facilitate a mismatch between oxygen supply and demand (68), a key pathophysiological mechanism in Type 2 myocardial infarction (44, 73).
Type 2 myocardial infarction, a non-atherothrombotic ischemic event, generally exhibits a poorer prognosis in women, particularly when hypoxaemia and anemia are present, conditions commonly observed in workers exposed to CIH. Furthermore, sex-specific factors such as iron deficiency, autoimmune disorders, hormonal fluctuations, and microvascular dysfunction may augment cardiovascular risk in this population women (69). Despite the absence of epidemiological data directly linking CIH to Type 2 myocardial infarction in women underscores the necessity for sex-specific preventive strategies, occupational monitoring, and longitudinal surveillance to facilitate early detection of cardiovascular deterioration among female workers at high altitudes.
Integrative perspective
The interaction between hormonal, psychological, and social determinants under chronic intermittent hypoxia (CIH) reveals a complex, mutually reinforcing pathway to cardiovascular dysregulation in women. Hormonal status, whether marked by estrogen dominance, progesterone predominance, or androgenic profiles, modulates vascular tone, autonomic balance, and metabolic efficiency (27, 29). These biological responses are not isolated; they are amplified or attenuated by psychological stressors such as mental workload, circadian disruption, and emotional coping demands, which in turn activate neuroendocrine pathways (e.g., HPA axis) that further influence blood pressure regulation and vascular function (51, 53). Social stressors, including work–family conflict, gendered workplace dynamics, and structural barriers to health, provide the environmental context in which these physiological and psychological responses occur (61, 67). Within the GBM framework, these domains converge to shape cardiovascular adaptation or maladaptation, underscoring the necessity for integrated, context-specific preventive strategies in high-altitude occupational settings.
Illustrative case scenario
Consider the case of a 38-year-old female mining operator working on a 7 × 7 shift rotation between sea level and 3,500 m.a.s.l., currently in the luteal phase of her menstrual cycle and using a combined oral contraceptive with moderate androgenic activity. During her high-altitude shift, elevated progesterone levels promote sympathetic activation, increasing heart rate and blood pressure, while hypobaric hypoxia imposes additional ventilatory and cardiovascular load (3, 27). Concurrently, she faces extended 12-h night shifts, high cognitive demands, and fragmented sleep due to circadian misalignment, compounding autonomic imbalance (51). Socially, she experiences persistent work–family conflict, being separated from her young children during rotation, and perceives subtle gender bias in task assignments (48, 67). In combination, these factors create a scenario of elevated allostatic load, reduced heart rate variability, and transient nocturnal hypertension, conditions that, if sustained over years, may increase her risk for endothelial dysfunction and Type 2 myocardial infarction (44, 69). This example illustrates how the GBM framework can be operationalized to identify risk profiles and guide targeted interventions in women exposed to CIH.
Conclusion
Despite increasing interest in the health implications of CIH, most studies in the high-altitude mining populations have predominantly employed cross-sectional comparisons between individuals working at varying elevations. These research designs have seldom incorporated female participants and frequently neglect factors such as hormonal status, psychosocial burden, and occupational heterogeneity. Consequently, the fundamental mechanisms underlying cardiovascular risk in female workers subjected to real-world CIH exposure remain inadequately understood.
This mini-review presents the GBM as a conceptual framework for comprehending cardiovascular risk among women working at high altitudes. By integrating biological aspects (such as hormonal fluctuations and reproductive health), psychological factors (including emotional burden and sleep disturbances), and social dimensions (notably gendered workplace dynamics and caregiving roles), the GBM offers a contextually sensitive and equity-informed perspective for assessing cardiovascular adaptation under environmental stress.
Future research must progress beyond mere cross-sectional snapshots. There is an urgent need for longitudinal cohort studies to investigate how sex hormones, autonomic function, emotional stress, and structural inequities interact over time to influence the development of cardiovascular risks in women throughout their working lives. This is especially imperative given that female participation in high-altitude mining tasks is recent but rapidly increasing, while the long-term health implications remain largely unknown. The generation of sex- and gender-stratified physiological data, employing within-subject designs, and including targeted assessments of hormonal and psychosocial variables will be essential for advancing precision health methodologies and establishing equitable occupational health guidelines. Additionally, this model may inform occupational health policies and tailored surveillance strategies for women working in other high-altitude sectors such as astronomical observatories, military deployment, and border control.
Author contributions
ML: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CC: Investigation, Software, Validation, Visualization, Writing – review & editing. GV: Software, Validation, Visualization, Writing – review & editing. JS-S: Funding acquisition, Investigation, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors thank the Superintendencia de Seguridad Social (SUSESO) for prioritizing and supporting this research line through the project Desafiando la Altura: Mujeres Chilenas y la Hipoxia Intermitente Crónica (ACHS 321-2024), which is currently in its implementation phase.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. Generative AI was used to assist with general language editing, rephrasing, and structural improvements of the manuscript. All scientific content, interpretations, and conclusions were developed by the author(s), who take full responsibility for the final version.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ministry of Health of Chile. Guía Tecnica sobre Exposicion Ocupacional a Hipobaria Intermitente Cronica por Gran Altitud. Ocupacional DDS, editor. Chile: División de Políticas Públicas Saludables y Promoción (2013).
2. Farias JG, Jimenez D, Osorio J, Zepeda AB, Figueroa CA, Pulgar VM. Acclimatization to chronic intermittent hypoxia in mine workers: a challenge to mountain medicine in Chile. Biol Res. (2013) 46:59–67. doi: 10.4067/S0716-97602013000100009
3. Lang M, Paéz V, Maj G, Silva-Urra J, Labarca-Valenzuela C, Caravita S, et al. Blood pressure response in miners exposed to chronic intermittent hypoxia in Chile. Front Cardiovasc Med. (2021) 8:701961. doi: 10.3389/fcvm.2021.701961
4. Muñoz S, Nazzal C, Jimenez D, Frenz P, Flores P, Alcantara-Zapata D, et al. Health effects of chronic intermittent hypoxia at a high altitude among chilean miners: rationale, design, and baseline results of a longitudinal study. Ann Work Expo Health. (2021) 65:908–18. doi: 10.1093/annweh/wxab029
5. Msc-Eleva Alliance. Workforce Study in the Chilean Large-Scale Mining Industry. 9th ed. Chile: Msc-Eleva Alliance (2023).
6. Lahiri-Dutt K. New directions in research on women and gender in extractive industries. Extract Indus Soc. (2022) 9:101048. doi: 10.1016/j.exis.2022.101048
7. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. (1977) 196:129–36. doi: 10.1126/science.847460
8. Barnes JN, Charkoudian N. Integrative cardiovascular control in women: regulation of blood pressure, body temperature, and cerebrovascular responsiveness. FASEB J. (2021) 35:e21143. doi: 10.1096/fj.202001387R
9. Regensteiner JG, Reusch JEB. Sex differences in cardiovascular consequences of hypertension, obesity, and diabetes: JACC focus seminar 4/7. J Am Coll Cardiol. (2022) 79:1492–505. doi: 10.1016/j.jacc.2022.02.010
10. Burnier M, Brguljan J, Algharably EAE, Kjeldsen SE, Narkiewicz K, Egan B, et al. Women's health, cardiovascular risk and hypertension: the perspective still needs to improve. Blood Press. (2023) 32:2193648. doi: 10.1080/08037051.2023.2193648
11. Eftedal I, Mrakic-Sapost S, LANG M. Editorial: women in environmental physiology 2022. Front Physiol. (2023) 14:1175366. doi: 10.3389/fphys.2023.1175366
12. O'kelly AC, Michos ED, Shufelt CL, Vermunt JV, Minissian MB, Quesada O, et al. Pregnancy and reproductive risk factors for cardiovascular disease in women. Circ Res. (2022) 130:652–72. doi: 10.1161/CIRCRESAHA.121.319895
13. Nguyen AH, Hurwitz M, Sullivan SA, Saad A, Kennedy JLW, Sharma G. Update on sex specific risk factors in cardiovascular disease. Front Cardiovasc Med. (2024) 11:1352675. doi: 10.3389/fcvm.2024.1352675
14. Young A, Rogers W. A review of digital transformation in mining. Min Metall Explor. (2019) 36:683–99. doi: 10.1007/s42461-019-00103-w
15. Appelman Y, Van Rijn BB, Ten Haaf ME, Boersma E, Peters SA. Sex differences in cardiovascular risk factors and disease prevention. Atherosclerosis. (2015) 241:211–8. doi: 10.1016/j.atherosclerosis.2015.01.027
16. Rajendran A, Minhas AS, Kazzi B, Varma B, Choi E, Thakkar A, et al. Sex-specific differences in cardiovascular risk factors and implications for cardiovascular disease prevention in women. Atherosclerosis. (2023) 384:117269. doi: 10.1016/j.atherosclerosis.2023.117269
17. Bairey Merz CN, Ramineni T, leong D. Sex-specific risk factors for cardiovascular disease in women-making cardiovascular disease real. Curr Opin Cardiol. (2018) 33:500–5. doi: 10.1097/HCO.0000000000000543
18. Maffei S, Guiducci L, Cugusi L, Cadeddu C, Deidda M, Gallina S, et al. Women-specific predictors of cardiovascular disease risk - new paradigms. Int J Cardiol. (2019) 286:190–7. doi: 10.1016/j.ijcard.2019.02.005
19. Harvey RE, Coffman KE, Miller VM. Women-specific factors to consider in risk, diagnosis and treatment of cardiovascular disease. Womens Health. (2015) 11:239–57. doi: 10.2217/WHE.14.64
20. Gerdts E, Sudano I, Brouwers S, Borghi C, Bruno RM, Ceconi C, et al. Sex differences in arterial hypertension. Eur Heart J. (2022) 43:4777–88. doi: 10.1093/eurheartj/ehac470
21. Dubey RK, Oparil S, Imthurn B, Jackson EK. Sex hormones and hypertension. Cardiovasc Res. (2002) 53:688–708. doi: 10.1016/S0008-6363(01)00527-2
22. White RE. Estrogen and vascular function. Vascul Pharmacol. (2002) 38:73–80. doi: 10.1016/S0306-3623(02)00129-5
23. Cicinelli E, Ignarro LJ, Matteo MG, Galantino P, Schonauer LM, Falco N. Effects of estrogen replacement therapy on plasma levels of nitric oxide in postmenopausal women. Am J Obstet Gynecol. (1999) 180:334–9. doi: 10.1016/S0002-9378(99)70209-7
24. Jordan J, Tank J, Stoffels M, Franke G, Christensen NJ, Luft FC, et al. Interaction between beta-adrenergic receptor stimulation and nitric oxide release on tissue perfusion and metabolism. J Clin Endocrinol Metab. (2001) 86:2803–10. doi: 10.1210/jcem.86.6.7567
25. Maranon R, Reckelhoff JF. Sex and gender differences in control of blood pressure. Clin Sci. (2013) 125:311–8. doi: 10.1042/CS20130140
26. Lovejoy JC, Bray GA, Bourgeois MO, Macchiavelli R, Rood JC, Greeson C, et al. Exogenous androgens influence body composition and regional body fat distribution in obese postmenopausal women–a clinical research center study. J Clin Endocrinol Metab. (1996) 81:2198–203. doi: 10.1210/jcem.81.6.8964851
27. Tagliapietra G, Citherlet T, Raberin A, Bourdillon N, Krumm B, Narang BJ, et al. Effect of menstrual cycle phase on physiological responses in healthy women at rest and during submaximal exercise at high altitude. Sci Rep. (2024) 14:27793. doi: 10.1038/s41598-024-79702-7
28. Brunt VE, Miner JA, Kaplan PF, Halliwill JR, Strycker LA, Minson CT. Short-term administration of progesterone and estradiol independently alter carotid-vasomotor, but not carotid-cardiac, baroreflex function in young women. Am J Physiol Heart Circ Physiol. (2013) 305:H1041–9. doi: 10.1152/ajpheart.00194.2013
29. Pechère-Bertschi A, Burnier M. Female sex hormones, salt, and blood pressure regulation. Am J Hypertens. (2004) 17:994–1001. doi: 10.1016/j.amjhyper.2004.08.009
30. Citherlet T, Raberin A, Manferdelli G, Bourdillon N, Millet GP. Impact of the menstrual cycle on the cardiovascular and ventilatory responses during exercise in normoxia and hypoxia. High Alt Med Biol. (2025) 26:55–62. doi: 10.1089/ham.2024.0048
31. De Zambotti M, Nicholas CL, Colrain IM, Trinder JA, Baker FC. Autonomic regulation across phases of the menstrual cycle and sleep stages in women with premenstrual syndrome and healthy controls. Psychoneuroendocrinology. (2013) 38:2618–27. doi: 10.1016/j.psyneuen.2013.06.005
32. Brahmbhatt Y, Gupta M, Hamrahian S. Hypertension in premenopausal and postmenopausal women. Curr Hypertens Rep. (2019) 21:74. doi: 10.1007/s11906-019-0979-y
33. Bredella MA. Sex differences in body composition. Adv Exp Med Biol. (2017) 1043:9–27. doi: 10.1007/978-3-319-70178-3_2
34. Srikanthan P Horwich TB Calfon Press M Gornbein J Watson KE. Sex differences in the association of body composition and cardiovascular mortality. J Am Heart Assoc. (2021) 10:e017511. doi: 10.1161/JAHA.120.017511
35. Kautzky-Willer A, Harreiter J, Pacini G. Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocr Rev. (2016) 37:278–316. doi: 10.1210/er.2015-1137
36. Pasquali R, Gambineri A. A comprehensive approach in diagnosing the polycystic ovary syndrome. Womens Health. (2015) 11:501–12. doi: 10.2217/WHE.15.13
37. Páez V, Rodriguez-Fernandez M, Silva-Urra J, Núñez-Espinosa C, Lang M. Maximal pulmonary ventilation and lactate affect the anaerobic performance in young women exposed to hypobaric hypoxia. Front Physiol. (2023) 14:1110477. doi: 10.3389/fphys.2023.1110477
38. Badenhorst CE, Goto K, O'brien WJ, Sims S. Iron status in athletic females, a shift in perspective on an old paradigm. J Sports Sci. (2021) 39:1565–75. doi: 10.1080/02640414.2021.1885782
39. Pasricha SR. Anemia: a comprehensive global estimate. Blood. (2014) 123:611–2. doi: 10.1182/blood-2013-12-543405
40. Miller EM. The reproductive ecology of iron in women. Am J Phys Anthropol. (2016) 159:S172–95. doi: 10.1002/ajpa.22907
41. Li X, Duan X, Tan D, Zhang B, Xu A, Qiu N, et al. Iron deficiency and overload in men and woman of reproductive age, and pregnant women. Reprod Toxicol. (2023) 118:108381. doi: 10.1016/j.reprotox.2023.108381
42. Fontana R, Della Torre S. The deep correlation between energy metabolism and reproduction: a view on the effects of nutrition for women fertility. Nutrients. (2016) 8:87. doi: 10.3390/nu8020087
43. Barake F, Paccot M, Rivera M, Neira C, Reyes V, Escobar MC. Chile's public healthcare sector hypertension control rates before and during the pandemic and HEARTS implementation. Rev Panam Salud Publica. (2022) 46:e126. doi: 10.26633/RPSP.2022.126
44. Bularga A, Taggart C, Mendusic F, Kimenai DM, Wereski R, Lowry MTH, et al. Assessment of oxygen supply-demand imbalance and outcomes among patients with type 2 myocardial infarction: a secondary analysis of the high-STEACS cluster randomized clinical trial. JAMA Netw Open. (2022) 5:e2220162. doi: 10.1001/jamanetworkopen.2022.20162
45. Bloch KE, Buenzli JC, Latshang TD, Ulrich S. Sleep at high altitude: guesses and facts. J Appl Physiol (1985) 119. (2015) 1466–80. doi: 10.1152/japplphysiol.00448.2015
46. Karasek RA Jr. Job demands, job decision latitude, and mental strain: implications for job redesign. Administr Sci Quart. (1979) 24:285–308. doi: 10.2307/2392498
47. Caro P, Madrid D, Cardenas M. Work-parenthood conflicts at the operator and professional levels in Chile's mining industry: a gender analysis. J Fam Stud. (2022) 29:1–30. doi: 10.1080/13229400.2022.2053336
48. Caro P, Roman Alonso H. Mujeres en altos cargos en minería en Chile. Agencia y tensiones de género Convergencia. Rev Ciencias Soc. (2021) 28:1. doi: 10.29101/crcs.v28i0.14438
49. Bandura A. Self-Efficacy: The Exercise of Control. New York, NY: W H Freeman; Times Books/Henry Holt and Co. (1997).
50. Rubin M, Subasic E, Giacomini A, Paolini S. An exploratory study of the relations between women miners' gender-based workplace issues and their mental health and job satisfaction: RUBIN et al. J Appl Soc Psychol. (2017) 47:400–11. doi: 10.1111/jasp.12448
51. Alcantara-Zapata DE, Lucero N, De Gregorio N, Astudillo Cornejo P, Ibarra Villanueva C, Baltodano-Calle MJ, et al. Women's mood at high altitude sexual dimorphism in hypoxic stress modulation by the tryptophan-melatonin axis. Front Physiol. (2022) 13:1099276. doi: 10.3389/fphys.2022.1099276
52. Oliveira-Silva L, Peçanha T, Fecchio RY, Rezende RA, Abreu A, Silva G, et al. Poor sleep quality is associated with cardiac autonomic dysfunction in treated hypertensive men. J Clin Hypertens. (2020) 22:1484–90. doi: 10.1111/jch.13949
53. Steptoe A, Kivimäki M. Stress and cardiovascular disease: an update on current knowledge. Annu Rev Public Health. (2013) 34:337–54. doi: 10.1146/annurev-publhealth-031912-114452
54. Eiter BM, Dugdale ZJ, Robinson T, Nixon CT, Lawson H, Halldin CN, et al. Occupational safety and health of women in mining. J Womens Health. (2023) 32:388–95. doi: 10.1089/jwh.2023.0034
55. Bridges D, Wulff E, Bamberry L. Resilience for gender inclusion: developing a model for women in male-dominated occupations. Gend Work Organiz. (2023) 30:263–79. doi: 10.1111/gwao.12672
56. Vearrier D, Greenberg MI. Occupational health of miners at altitude: adverse health effects, toxic exposures, pre-placement screening, acclimatization, and worker surveillance. Clin Toxicol. (2011) 49:629–40. doi: 10.3109/15563650.2011.607169
57. Esenamanova MK, Kochkorova FA, Tsivinskaya TA, Vinnikov D, Aikimbaev K. Chronic intermittent high altitude exposure, occupation, and body mass index in workers of mining industry. High Alt Med Biol. (2014) 15:412–7. doi: 10.1089/ham.2013.1150
58. Mccarthy A, damiran N. Non-Communicable disease risk factors among a cohort of mine workers in Mongolia. J Occup Environ Med. (2019) 61:1072–7. doi: 10.1097/JOM.0000000000001755
59. Mcdonnell D, Mcallister B. Psychosocial risks in the Canadian construction and extractive industries. Extract Indus Soc. (2024) 19:101515. doi: 10.1016/j.exis.2024.101515
60. Castañeda-Burciaga S, Guirette-Barbosa OA, Ramírez-Salazar MA, Celaya-Padilla JM, García-Estrada LI. Inclusion of women in the mining sector: challenges and opportunities through education. Educ Sci. (2025) 15:69. doi: 10.3390/educsci15010069
61. Caro Molina P, Román Alonso H, Armijo Garrido L. Cuerpos de mujeres, significados de género y límites simbólicos en la gran minería en Chile. Polis. (2020) 19:186–211. doi: 10.32735/S0718-6568/2020-N55-1448
62. Sharma S, Rees S. Consideration of the determinants of women's mental health in remote Australian mining towns. Aust J Rural Health. (2007) 15:1–7. doi: 10.1111/j.1440-1584.2007.00842.x
63. Lahiri-Dutt K. Digging women: towards a new agenda for feminist critiques of mining. Gender Place Cult. (2012) 19:193–212. doi: 10.1080/0966369X.2011.572433
64. Jenkins K. Women, mining and development: an emerging research agenda. Extract Indus Soc. (2014) 1:329–9. doi: 10.1016/j.exis.2014.08.004
65. Lutz-Ley AN, Buechler SJ. Mining and women in northwest Mexico: a feminist political ecology approach to impacts on rural livelihoods. Hum Geogr. (2020) 13:74–84. doi: 10.1177/1942778620910901
66. Musonda J. Undermining gender: women mineworkers at the rock face in a Zambian underground mine. Anthropol S Afr. (2020) 43:32–42. doi: 10.1080/23323256.2020.1736945
67. Botha D, Cronjé F. Occupational health and safety considerations for women employed in core mining positions. SA J Hum Resour Manag. (2015) 13:652. doi: 10.4102/sajhrm.v13i1.652
68. Anand A, Lee KK, Chapman AR, Ferry AV, Adamson PD, Strachan FE, et al. High-sensitivity cardiac troponin on presentation to rule out myocardial infarction: a stepped-wedge cluster randomized controlled trial. Circulation. (2021) 143:2214–24. doi: 10.1161/CIRCULATIONAHA.120.052380
69. Sciomer S, Moscucci F, Maffei S, Gallina S, Mattioli AV. Prevention of cardiovascular risk factors in women: the lifestyle paradox and stereotypes we need to defeat. Eur J Prev Cardiol. (2019) 26:609–10. doi: 10.1177/2047487318810560
70. Keyes LE, Hackett PH, Luks AM. Outdoor activity and high altitude exposure during pregnancy: a survey of 459 pregnancies. Wilderness Environ Med. (2016) 27:227–35. doi: 10.1016/j.wem.2016.02.010
71. Luks AM, Beidleman BA, Freer L, Grissom CK, Keyes LE, McIntosh SE, et al. Wilderness medical society clinical practice guidelines for the prevention, diagnosis, and treatment of acute altitude illness: 2024 update. Wilderness Environ Med. (2024) 35(1_suppl):2S–19S. doi: 10.1016/j.wem.2023.05.013
72. Lüneburg N, Siques P, Brito J, De La Cruz JJ, León-Velarde F, Hannemann J, et al. Long-term intermittent exposure to high altitude elevates asymmetric dimethylarginine in first exposed young adults. High Altitude Med Biol. (2017) 18:226–33. doi: 10.1089/ham.2016.0123
73. Parati G, Agostoni P, Basnyat B, Bilo G, Brugger H, Coca A, et al. Clinical recommendations for high altitude exposure of individuals with pre-existing cardiovascular conditions: a joint statement by the European Society of Cardiology, the Council on Hypertension of the European Society of Cardiology, the European Society of Hypertension, the International Society of Mountain Medicine, the Italian Society of Hypertension and the Italian Society of Mountain Medicine. Eur Heart J. (2018) 39:1546–54. doi: 10.1093/eurheartj/ehx720
74. UIAA Medical Commission. Advice for Women Going to Altitude (2018). Available online at: https://www.theuiaa.org/advice-for-women-going-to-altitude/
Keywords: high-altitude physiology, risk factors, chronic intermittent hypoxia, women's health, occupational health
Citation: Lang M, Cazzuffi C, Viscor G and Soto-Sánchez J (2025) A gender-integrated biopsychosocial model to understand cardiovascular risk in women working under environmental hazards: the case of chronic intermittent hypoxia. Front. Public Health 13:1672503. doi: 10.3389/fpubh.2025.1672503
Received: 24 July 2025; Accepted: 29 August 2025;
Published: 22 September 2025.
Edited by:
Sasho Stoleski, Saints Cyril and Methodius University of Skopje, North MacedoniaReviewed by:
Ermanno Vitale, Kore University of Enna, ItalyFrancesco Angeli, University of Bologna, Italy
Copyright © 2025 Lang, Cazzuffi, Viscor and Soto-Sánchez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johana Soto-Sánchez, am9oYW5hLnNvdG9AdW1heW9yLmNs