 Francisco Javier Bedoya-Rodríguez
Francisco Javier Bedoya-Rodríguez Carlos Eduardo Guevara-Fletcher1,3
Carlos Eduardo Guevara-Fletcher1,3 Jonathan S. Pelegrin
Jonathan S. Pelegrin- 1Grupo de Investigación en Ecología y Conservación de la Biodiversidad (EcoBio), Equipo de Paleobiología, Ecología y Evolución (PaleoEco), Facultades de Ciencias Básicas y Educación, Universidad Santiago de Cali, Campus Pampalinda, Cali, Colombia
- 2Escuela de Ingeniería de Sistemas y Computación, Facultad de Ingeniería, Universidad del Valle, Sede Norte, Santander de Quilichao, Colombia
- 3Escuela de Ciencias Agrícola Pecuarias y del Medio Ambiente, Universidad Nacional Abierta y a Distancia, Cali, Colombia
Background: Mosquito-borne diseases (MBD) continue to represent a critical public health challenge, particularly in tropical regions where environmental and socioeconomic factors facilitate transmission.
Methods and materials: This study assessed the knowledge, attitudes, and practices (KAP) related to MBD among 172 residents of an urban area in Santander de Quilichao, Colombia. A structured survey, validated and adapted from the Pan American Health Organization, was performed for data collection.
Results: The mean knowledge score was 57%, indicating moderate awareness of MBD. While 63.4% of participants reported adequate preventive practices, the majority (94.8%) demonstrated indifferent attitudes toward MBD prevention. Multinomial logistic regression analysis revealed a statistically significant association between marital status and knowledge levels (p < 0.05), with married participants exhibiting higher knowledge. Socioeconomic analysis showed that 41.3% of participants earned the legal minimum wage, and 68.6% of households included at least one woman of childbearing age. Despite moderate knowledge and preventive practices, the prevalence of indifferent attitudes may hinder effective MBD prevention.
Conclusion: These findings emphasize the need for targeted community engagement and educational interventions. Incorporating KAP assessments into public health strategies can enhance the design and implementation of effective educational and vector control programs in urban areas of tropical countries.
1 Introduction
Globally, arthropod-borne vector-borne diseases (VBD) represent a public health challenge, with an estimated 700,000 deaths per year. Approximately 17% of the world’s infectious diseases are attributable to VBD (1). Approximately 80% of the global population resides in areas with a high risk of VBD transmission, particularly in tropical and subtropical regions (1, 2). The persistent threat of these diseases, particularly mosquito-borne diseases (MBD), is exacerbated by factors such as inadequate public awareness and the spread of misinformation, which hinder effective prevention and control efforts (1). Mosquitoes (Diptera, Culicidae) are the primary vectors for numerous MBD, including dengue, Zika, chikungunya, and yellow fever (transmitted by Aedes spp.), as well as malaria (Anopheles spp.), Japanese encephalitis, and West Nile virus (both mainly transmitted by Culex spp.) (1, 3–5). These arboviruses, a diverse group encompassing the Peribunyaviridae, Flaviviridae, Togaviridae, Reoviridae, and Orthomyxoviridae families (6), represent a significant challenge to healthcare systems worldwide. The increasing overlap in the geographical distribution of these diseases creates diagnostic challenges and can complicate clinical management (7).
In Americas, the most prevalent arboviruses are the dengue, Zika, and chikungunya viruses (8). These viruses are primarily transmitted by Aedes mosquitoes, especially Aedes aegypti (Linnaeus, 1762) and Aedes albopictus (Skuse, 1894), and have spread extensively throughout the region (9). While dengue virus is the most widespread, with an estimated 96 million cases annually, chikungunya and Zika also contribute significantly to the disease burden (10). The Americas and Caribbean reported in 2024, 13,027,747 cases, approximately three times higher than the previous year (11). Also, 16,239 cases of Oropouche (102) and 186,274 cases of chikungunya were reported at the same year (12). The rapid increase in the cases, with the presence of other arboviruses, such as yellow fever virus, West Nile virus, and those causing equine encephalitis (8), showing the urgent need for improved surveillance and control strategies. The rapid distribution of Ae. aegypti and Ae. albopictus has amplified the arboviral diseases (9). Other aspects, such as climate change, and urbanization increase in natural areas present a challenge to disease control and prevention (13). Notwithstanding the implementation of environmental controls and educational strategies (14), community participation in activities of adoption of preventive practices are imperative (15, 16).
Studies on knowledge, attitudes, and practices (KAP) related to MBD have been important tools for developing public health interventions both urban and rural areas (17). Various studies have shown the important of the educational process in preventing and mitigating of MBD across diverse socio-environmental and cultural contexts (18–22). KAP studies are frequently used to assess community knowledge, behaviors, and responses to MBD (23). Van den Berg et al. (24) carried out studies on insecticide management practices to control mosquito. They founded poor knowledge about its use demonstrating the necessity to involve the community in good management to eradicate mosquito.
The significance of KAP studies is widely acknowledged due to their relationship with social and cultural factors that influence the understanding of environmental challenges (25). In Asia, KAP studies realized in Bangladesh have evaluated public perspectives on dengue dynamics across different educational and industrial sectors (26). These studies have demonstrated that KAP can significantly enhance knowledge, promote preventive actions, and refine public health strategies (27–29). Furthermore, KAP studies have been related with socioeconomic factors and climate change impacts both urban and rural areas (30–35). A comparative study involving non-endemic (Turkey) and dengue-endemic countries (Bangladesh, India, and Malaysia) demonstrated the value of KAP in improving dengue diagnosis and treatment within healthcare systems (36). Analogous KAP analyses on dengue have been conducted in other endemic regions, including Yemen and Malaysia, as well as non-endemic regions, such as Hong Kong (37–39). Other studies carried out in China, Vietnam, India, and Singapore have investigated beliefs, behaviors, perceptions, willingness, and awareness related to MBD prevention and control (40–44). The collection of KAP data demonstrated that the development of educative strategies enhancing knowledge and promoting behavioral change between human and mosquitoes (45). This assertion is confirmed by studies conducted in diverse settings, including patient populations, healthcare facilities, and educational institutions (46–48).
In Africa, some studies affirmed that scarce ecological knowledge regarding MBD carry to use pesticide and not to implement educational strategies (28). In Tanzania, studies were focus on KAP with the purpose of prevent dengue and to understand mosquito ecology (49). In Kenya, the studies have linked knowledge, beliefs and management of MBD to socioeconomic factors within the livestock sector (50). In the Americas, KAP studies carried out in countries such as United States, Mexico, Brazil, and Peru have examined preventive behaviors in relation to beliefs, personality traits, social responsibility, and sociodemographic factors across urban, rural, and marginalized contexts (51–55). In Colombian where MBD are endemic, KAP studies have related knowledge with sociodemographic characteristics, risk perception, and population experiences (56–60).
In order to better understand and address the impact of mosquitoes on human health, it is essential to analyze MBD using the KAP framework. Assessing KAP can inform strategies aimed at preventing and controlling mosquito populations by promoting positive changes in human behavior (61). This research purpose to analyze the role of neighborhood and individual factors in the KAP related to MDB in the municipality of Santander de Quilichao, Cauca, southwest Colombia, using community surveys. The climate in this area is favorable for the presence of MBD, particularly dengue and malaria (62, 63).
2 Materials and methods
2.1 Study area and participants
The KAP community survey was conducted in two neighborhoods in the urban area of Santander de Quilichao, located in the Cauca department, in southwestern Colombia (3°00′32.0”N 76°28′39.4”W) (Figure 1). The neighborhoods were selected due to its socioeconomic status (low middle income), which represents a significant segment of the city’s population (62). The study area is situated in tropical deciduous woodland bio-climatic zone. The survey was conducted from October 2022 to February 2023. This municipality has a total population of 53,856 inhabitants in the urban area (63).
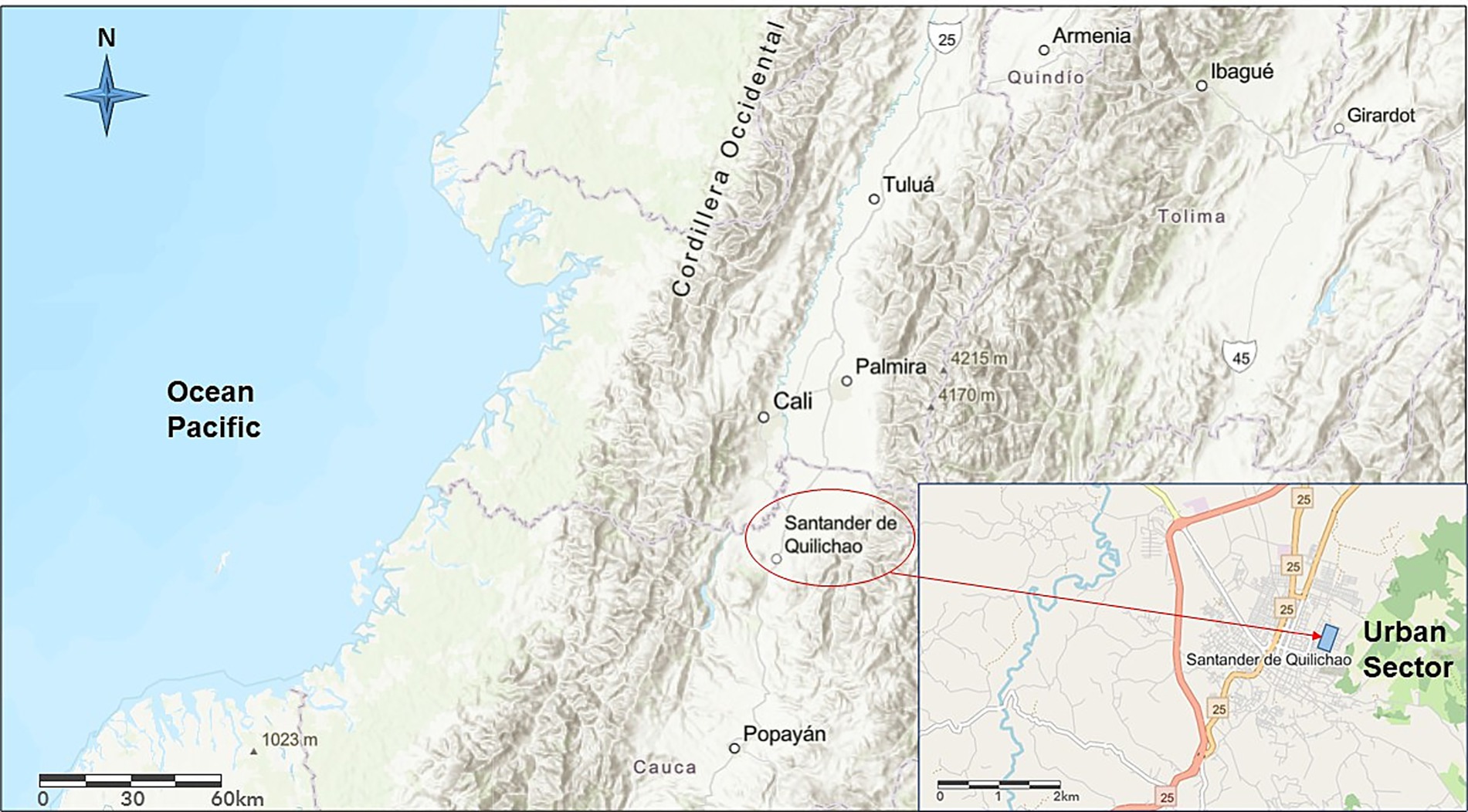
Figure 1. Location of the study area in Santander de Quilichao, Department of Cauca, southwestern Colombia. The study area is identified (blue rectangle).
The sample size was calculated using the formula for estimating a proportion in a finite population, with a 95% confidence level (Z = 1.96), and a margin of error of 5%. For the 310 households in the study area, this yielded a required sample size of 172. The sample size was verified using the online SurveyMonkey application.1 Households were selected by simple random sampling from the municipal census list. Each household was contacted by telephone or visited directly if no phone number was available. Eligible participants were adults (≥18 years), responsible for the household, and residents of the community with access to a mobile phone and internet. If a household declined or could not be reached, another was randomly selected to ensure the sample size was achieved. The main hypothesis was that sociodemographic factors influence KAP regarding MBD.
2.2 Questionnaire design
The survey used in this study was designed using Google Forms.2 The design process included elements such as informed consent, socio-demographic data and a series of questions on KAP related to MBD and mosquito control (Supplementary Table 1). The survey instrument used in this study was adapted from the KAP questionnaire developed by the Pan American Health Organization (64). This instrument has been previously validated and widely employed in mosquito-borne disease research, providing a robust framework for assessing community knowledge and behaviors related to vector control. The survey provided a foundation upon which the questionnaire was adapted through a series of expert consultations with local entomologists, public health officials, and community leaders. The objective of these survey was to show the relevance of the questionnaire at the local context and the specific MBD prevalent in the region (64). A pilot study was conducted with 30 households according to Bujang et al. (65), in order to know the reliability, clarity, and cultural appropriateness of the questionnaire. The feedback from the pilot study was used to refine the questionnaire before the main data survey. Specifically, we modified items related to disease symptomatology to better reflect locally prevalent illnesses, simplified wording in attitude-related questions to enhance comprehension, and added culturally relevant examples within practice items. These adjustments aimed to optimize the instrument’s clarity, relevance, and respondent engagement. Cronbach’s alpha was calculated to analyze the internal consistency of knowledge, attitude, and practice scales (acceptable at 70.2%). Exploratory factor analysis (EFA) was performed with Varimax rotation to determine construct validity (23). These analyses will provide evidence of the questionnaire’s reliability and validity.
The research met ethical standards with approval from the Ethics Committee of the Faculty of Education at the University of Santiago de Cali and the local Community Action Committee. Informed consent was obtained via Google Forms, and an unbiased sample was maintained by randomly replacing non-participating households.
The questionnaire included both general items on mosquito-borne diseases and disease-specific items, particularly related to dengue. This approach was chosen due to the high prevalence of dengue in the study area at the time of data collection. The questionnaire was divided in four sections: sociodemographic characteristics (nine questions), knowledge (12 questions), attitudes (11 questions), and practices (eight questions) respect to MBD and mosquito control. The sociodemographic section included variables such as gender, age, marital status, education level, occupation, number of dependents, monthly income, and the number of reproductive women, and pregnant women. These data allow understand how these factors may influence KAP regarding MBD. A knowledge index was developed based on 10 most relevant questions, with ranging between 0 and 10 (44). Each correct or positive answer received a score of 1, while incorrect or negative answer received a score of 0. This scoring system facilitated the categorization of knowledge into six sub-categories as follows: 0 (without knowledge), 1–2 (very low knowledge), 3–4 (low knowledge), 5 (medium knowledge), 6–8 (high knowledge), and 9–10 (very high knowledge). Questions 11 and 18 were designed to assess participants’ comprehension of mosquito biology and their disease transmission. Questions 17 and 19 analyzed the dengue and its prevalence in the study area. In this context, responses were organized such as ‘correct and indifferent’ (1) or ‘incorrect’ (0), thereby contributing to the calculation of the overall knowledge score. In this case, ‘indifferent’ responses indicate partial knowledge without misinformation, and were rated as correct (1) in the knowledge index to distinguish uncertainty from incorrect knowledge. Question 10 asked participants if they were familiar with the term mosquito-borne disease (MBD). Those who responded negatively were excluded from the knowledge score analysis, as their lack of basic awareness rendered subsequent knowledge items inapplicable, ensuring the accuracy and validity of the knowledge assessment. This methodological approach was taken to ensure an accurate assessment of knowledge levels and to maintain the integrity of the study.
The classification of attitudes was divided into three subcategories. The scores from 0 to 14 indicated a negative attitude, scores from 15 to 34 indicated an indifferent attitude, and scores from 35 to 44 reflected a positive attitude toward MBD and mosquito control. The responses to the Practice Index questions were categorized and scored as follows: each affirmative or correct practice was assigned one point, resulting in a cumulative score ranging from 0 to 8. Scores ranging from 0 to 2 indicated inadequate practices, scores from 3 to 5 reflected moderate practices, and scores from 6 to 8 indicated adequate practices. The thresholds for attitude and practice scores were determined using a combination of adaptations from previous CAP studies (19, 30, 34, 44), ensuring their contextual relevance and replicability.
2.3 Data analysis
In order to analyze the relationship between sociodemographic variables and knowledge levels, we employed a multinomial logistic regression model. The knowledge index, categorized into five levels, served as the dependent variable, with the lowest category used as the reference. All independent variables were included simultaneously in the model, including gender, age, marital status, education, occupation, income, number of dependents, presence of reproductive women, and pregnant women in the household. This approach enables the estimation of the effect of each predictor on the odds of belonging to each knowledge category relative to the reference. The same set of variables was applied across all outcome categories, ensuring the comparability and interpretability of the associations. The regression model was built using gender, age, marital status, education and occupation as independent variables. These factors have been consistently identified in the literature as the most robust and theoretically relevant predictors of knowledge, attitudes and practices regarding MBD (c, 39, 51). Other registered variables were not included in the model because they did not demonstrate sufficient variability or statistical association in preliminary analyses.
A comprehensive statistical analysis was conducted to explore the statistical association between socio-demographic factors and KAP outcomes. Thus, descriptive statistical analyses were used to describe the relationships between different socio-demographic aspects and KAP scores. Prior to conducting the multinomial logistic regression, bivariate analyses were performed to examine the relationship between each socio-demographic variable and the levels of KAP. Chi-square tests were used to assess the association between categorical variables (marital status, gender, occupation, education level) and KAP levels. Variables with a p-value < 0.05 in the bivariate analyses were selected for inclusion in the multinomial logistic regression model. Variance inflation factors (VIF) were calculated to assess multicollinearity among the independent variables, if VIF values exceeded 5, the variable with the highest VIF was considered for removal from the model. Specifically, a multinomial logistic regression model was used, implemented through the SPSS version 25 statistical package. In this model, socio-demographic variables served as independent variables, while KAP scores served as dependent variables. This analytical approach aimed to uncover significant associations between these variables, thereby providing insights into how socio-demographic characteristics influence KAP levels within the studied population (66).
3 Results
3.1 Instrument reliability and validation on KAP dimensions
To ensure the questionnaire’s relevance and cultural appropriateness, consultations were conducted with local entomologists, public health officials, and community leaders. The consensus and agreement from these consultations were quantitatively evaluated using Cohen’s Kappa coefficient for inter-rater reliability, yielding a substantial agreement with a Kappa value of 0.78 (95% CI: 0.70–0.85), which indicated high concordance among experts. Feedback from these consultations guided the refinement of specific questionnaire items to improve clarity and local contextual relevance.
Cronbach’s alpha coefficients for the knowledge, attitude, and practice scales were 0.70, 0.75, and 0.79, respectively, indicating acceptable to good internal consistency. An exploratory factor analysis (EFA) was performed on the CAP scale items to evaluate their underlying factor structure and the construct validity of the instrument. A Varimax rotation analysis was applied in order to identify the three factor dimensions that constitute the instrument. The analysis yielded a three-factor solution that explained 86.27% of the total variance. Please refer to Table 1, which presents the factor loadings grouped according to the CAP dimensions. The knowledge dimension grouped 12 items and explained 46.55% of the variance, with average factor loadings around 0.53, indicating an adequate association between the items and that dimension. The attitude dimension, which comprises 11 items, contributed 16.51% of the variance and had an average factor loading close to 0.75, reflecting a strong relationship between the items and this factor. The practice dimension, consisting of eight items, explained 23.22% of the total variance and showed the highest average factor loadings (0.79), evidencing a strong link between preventive measures and this dimension. All items exhibited clear and interpretable factor loadings, consistent with their theoretical assignment. Following the analysis, no items were excluded or modified, indicating stable psychometric properties and robust construct validity.
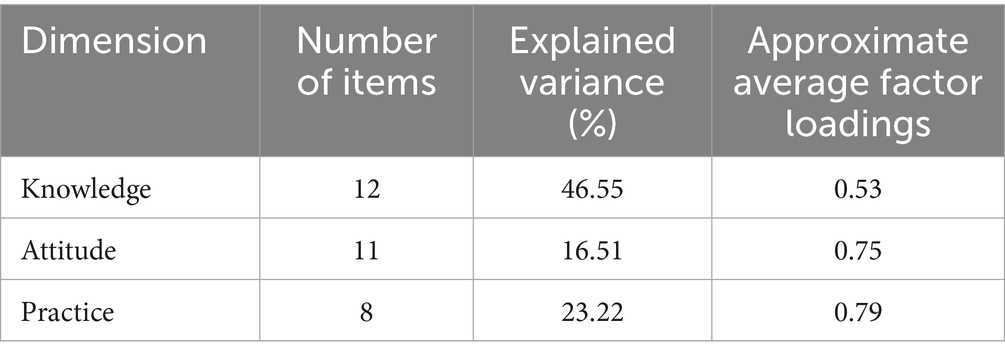
Table 1. Summary of average factor loadings and variance explained by dimension in exploratory factor analysis (Varimax rotation).
3.2 Sociodemographic characteristics and KAP
Key variables such as age, gender distribution, and educational level are summarized to provide a concise overview, providing the participants’ demographics and offering essential context for further analysis (Table 2). In Colombia, “technical” education is short-term and skills-focused, while “technological” education is more advanced and prepares students for mid-level professional roles.
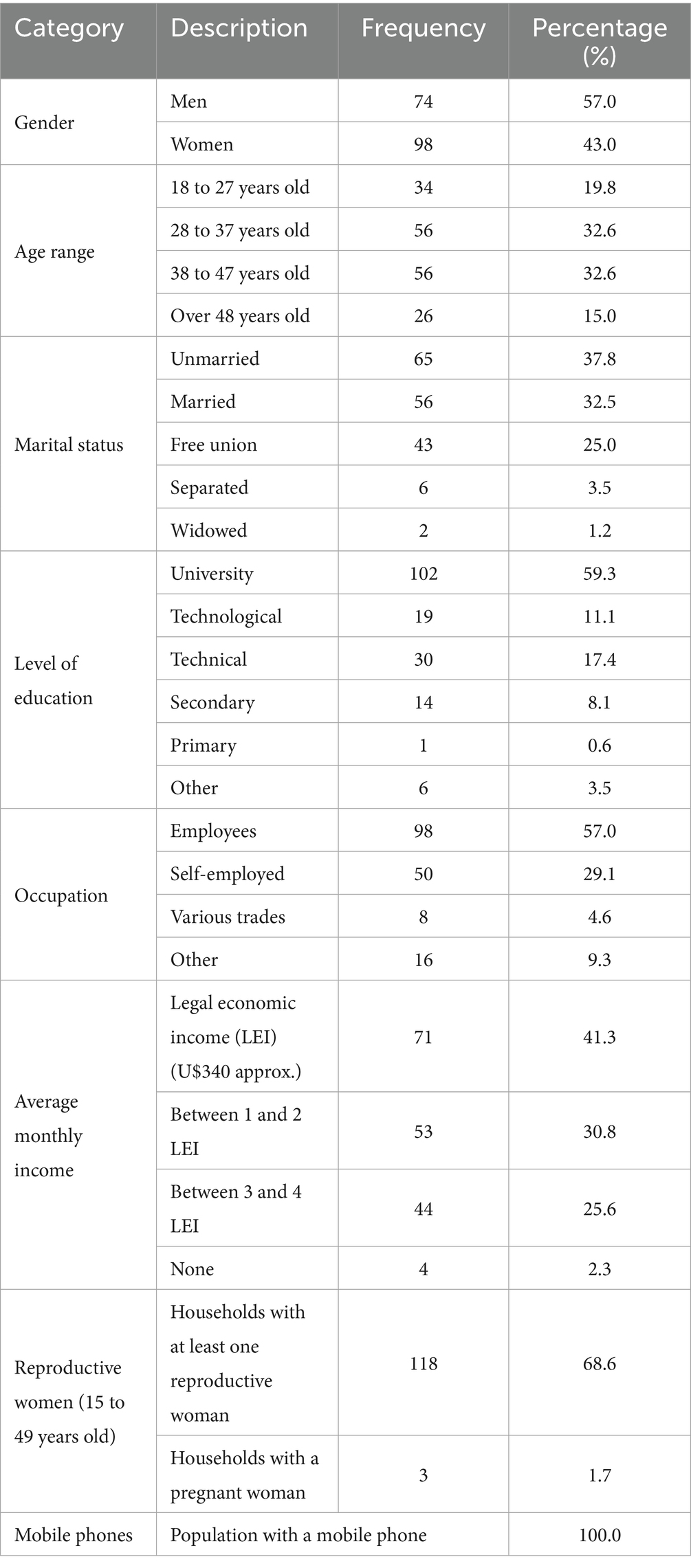
Table 2. Sociodemographic characterization of the target population in a local area from municipality of Santander de Quilichao, Colombia.
3.3 Knowledge of mosquito-borne diseases
A total of 62.8% of participants, were aware of MBD. Moreover, 91.9% are aware of the life cycle of mosquitoes, which are critical vectors in both natural and man-made environments. While 57.6% of participants acquired knowledge of those cycles many years ago, only 12.8% learned about them during the surveys. The information about MBD was obtained mainly by TV (31.4%), followed by interpersonal (24.4%) and family (19.2%) communications. Social networks and internet represented 18.6 and 5.4%, respectively. Perceived susceptibility to MBD was reported by 66.9% of participants; in contrast, 21.5% were ambivalent and 9.9% were unaware of their risk status. Furthermore, when asked about personal experience within their community, 66.9% did not know anyone who had sickness by MBD.
Interestingly, while 91.9% acknowledge that anyone can contract MBD, only 21.5% correctly identify dengue as a viral disease, despite its strong association with mosquito transmission (90.1%). Knowledge of dengue symptoms such as fever and muscle pain were recognized by the population (60%); however, the 12.2% remain uninformed about these symptoms. Preventive strategies against MBD are mainly focused on environmental management, with 84.9% supporting the elimination of stagnant water as the most important strategy, followed by cleaning water storage containers (75.6%) and fumigation efforts (71.5%). According to 58.7% of respondents, treatment for MBD is available. With respect to knowledge of MBD, the participants showed very high (9.9%), high (57%) medium (15%) and between low and very low (16.3%) levels.
3.4 Attitudes on mosquito-borne diseases
The majority of interviewees (58.5%) responded that MBD are an important problem for the community, 29.1% was agreed, 9.9% were indifferent, 1.2% disagreed and 4.1% totally disagreed. The probability of contracting a MBD in the next six-month, were as follows: 21.1% expressed a strong agreement, 23.8% indicated an agreement, 34.3% remained indifferent, 14.5% expressed disagreement, and 5.2% strongly disagreed. In the moment to contract a MBD, 13.4% were strongly agreed that the information should remain confidential, 13.4% agreed, 29.1% were indifferent, 18.6% disagreed, and 25.6% strongly disagreed. In cases of family could be discriminated for contracting MBD, they responded that 72.1% strongly disagreed, 12.2% disagreed, and 8.1% were indifferent. 90% considered that the responsibility of each individual to adopt preventive measures to avoid MBD, followed by health staff (24.4%). At home, the responsibility is personal (62.2%), or head of household (46.5%) and healthcare providers (16.3%). The responsibility in the community is to, municipal administration (43.6%), personal responsibility (41.3%), health personnel (35.5%) and community leaders (33.7%). The question about the effective treatment of individuals infected with MBD, showed that the treatment should be administered in a hospital (72.7%), by a private doctor (49.4%), in a public health center (36%), in a pharmacy (8.1%) or by an unqualified practitioner (1.7%). It was evident that 51.7% of the participants did not have enough information about MBD. The 94.8% displayed an indifferent attitude, while 5.2% showed a positive attitude (Table 3).
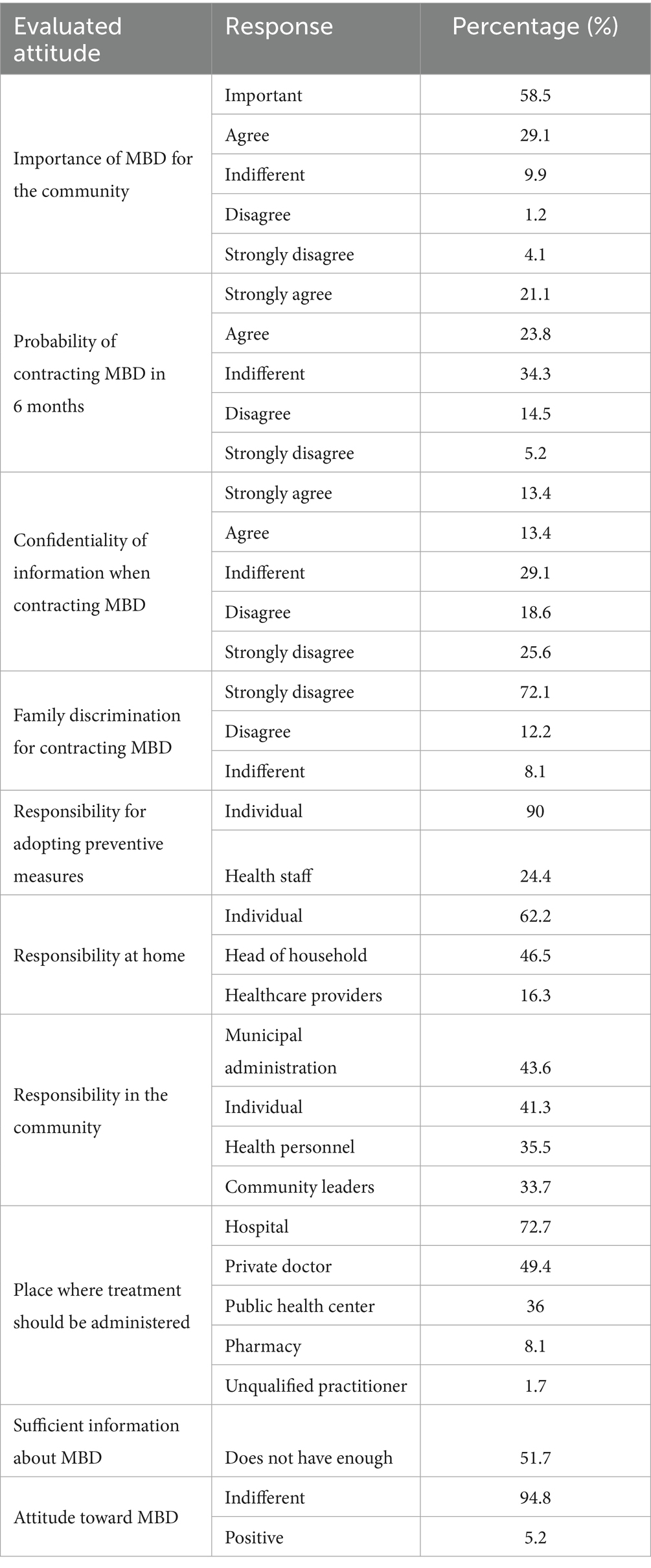
Table 3. Summary of key attitudes toward MBD.
3.5 Practices on mosquito-borne diseases
A total of 72.1% of participants carried out preventive measure to avoid contracting MBD. The main methods of protection were (a) Elimination of stagnant water: 94.2% considered that eliminating all types of stagnant water reduce the mosquito populations, (b) Personal protection: 88.4% protecting themselves from MBD. 10.5% of participants considered that local organizations were doing enough to prevent MBD, represented by local government (11.6%) and national government (13.4%). 75.6% reported cleaning tanks, storage containers or stagnant water the last week. This behavior is crucial in reducing potential breeding sites for mosquito and reflects a commitment to maintaining a healthier environment. The survey showed a strong willingness among participants to participate in vaccination campaigns against MBD, 76.7% accepting a vaccine if is available. Adequate practices for the prevention of MBD were observed in 63.4% of participants, whereas 36.6% had moderate practices (Table 4).
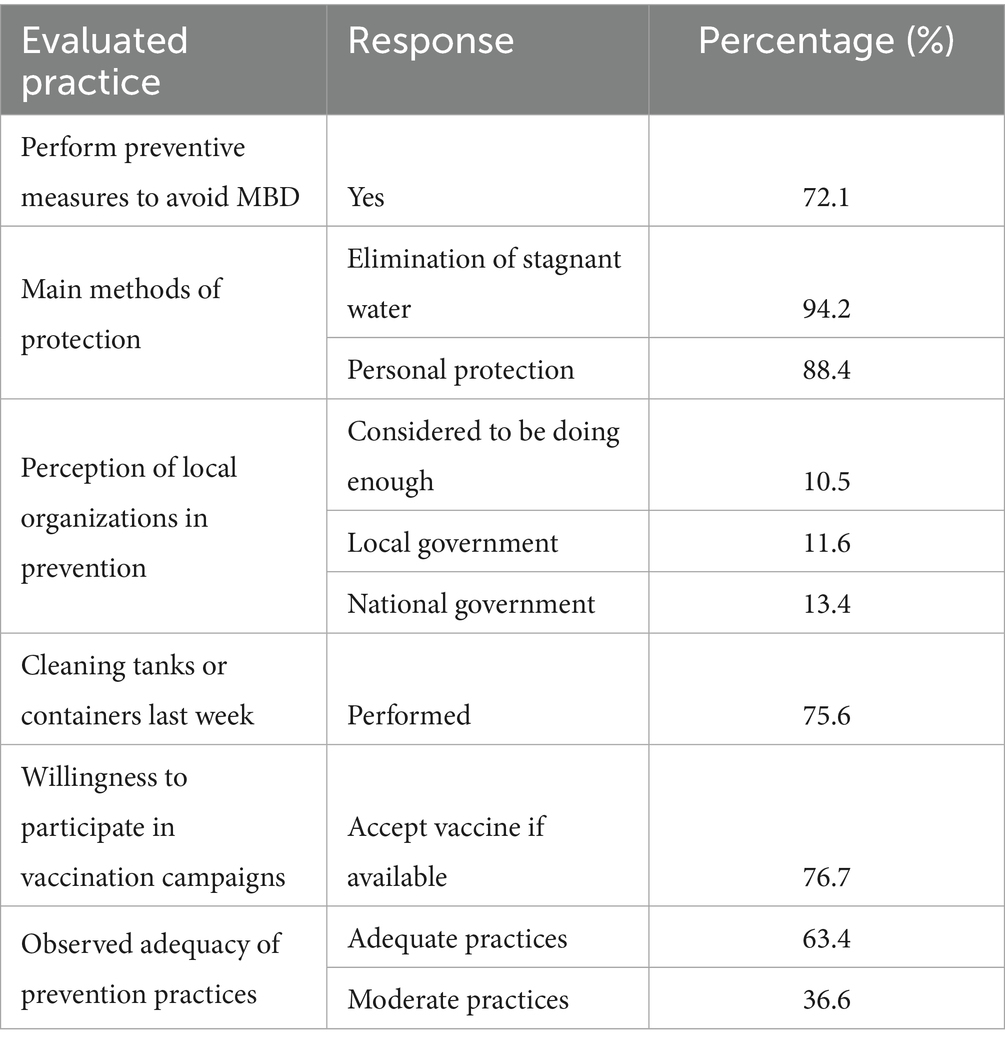
Table 4. Summary of key practices in MBD prevention.
3.6 Association between sociodemographic variables and KAP
There were differences in knowledge levels about MBD according to key sociodemographic variables, specifically age (38 to 47 years old) and marital status. The results demonstrated a highly significant relationship between higher knowledge levels and being aged between 38 and 47 years (χ2 = 446.211, p < 0.001). Similarly, marital status showed significant associations: unmarried (χ2 = 93.193, p < 0.001), married (χ2 = 100.373, p < 0.001), and living in a free union (χ2 = 96.674, p < 0.001). Additionally, no significant relationship was found between any of the sociodemographic variables and either attitude or practice toward MBD.
Bivariate analyses revealed statistically significant relationship between marital status (p < 0.001) and age (p = 0.02) with knowledge levels. Multinomial logistic regression analysis (Table 5) showed that marital status is a critical factor influencing knowledge about diseases, particularly among participants with high knowledge. For example, individuals aged 38 to 47 years had markedly higher odds of high knowledge compared to those over 48 years [Exp(B) = 6.43 × 107; 95% CI: 9.27 × 106–4.45 × 108; p < 0.001]. Conversely, being unmarried substantially decreased the odds of high knowledge [Exp(B) = 4.68 × 10−13; 95% CI: 4.48 × 10−15–4.89 × 10−11; p < 0.001]. Other factors, such as gender and occupation, were not significant predictors across all knowledge levels. Although education level showed positive trends, significance was only marginal for low and very high knowledge groups (p = 0.068 and 0.075, respectively).
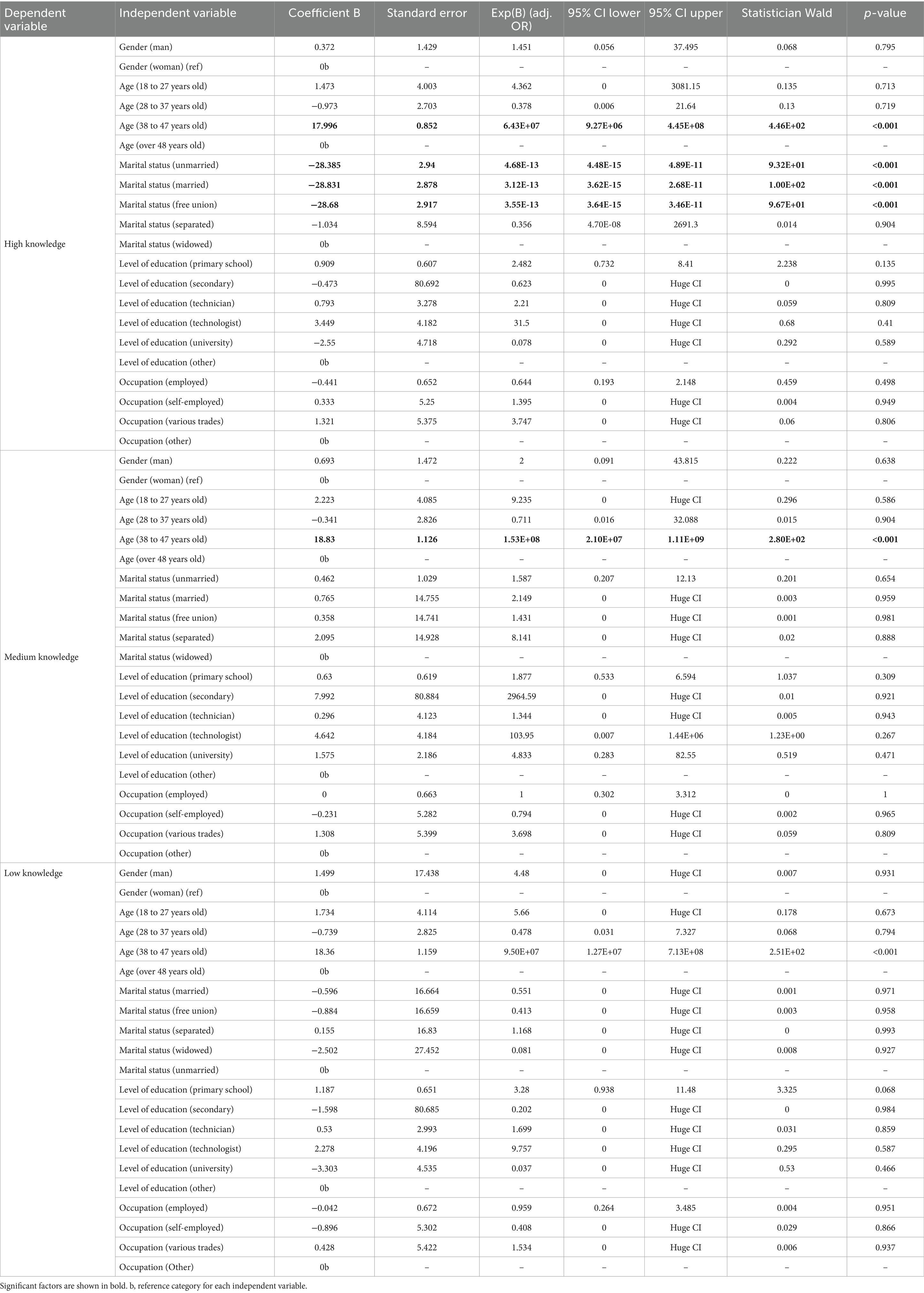
Table 5. Multinomial logical regression analysis of sociodemographic factors associated with knowledge about MBD in a local area from Santander de Quilichao, Colombia.
The results from Tables 6, 7 indicate that there were no statistically significant associations between sociodemographic variables and either attitudes or practices regarding MBD in the studied population. Specifically, none of the independent variables-including gender, age, marital status, level of education, or occupation-showed significant effects on having a positive attitude (Table 6) or adequate practice (Table 7), consistent with high p-values and Exp(B) values near unity.
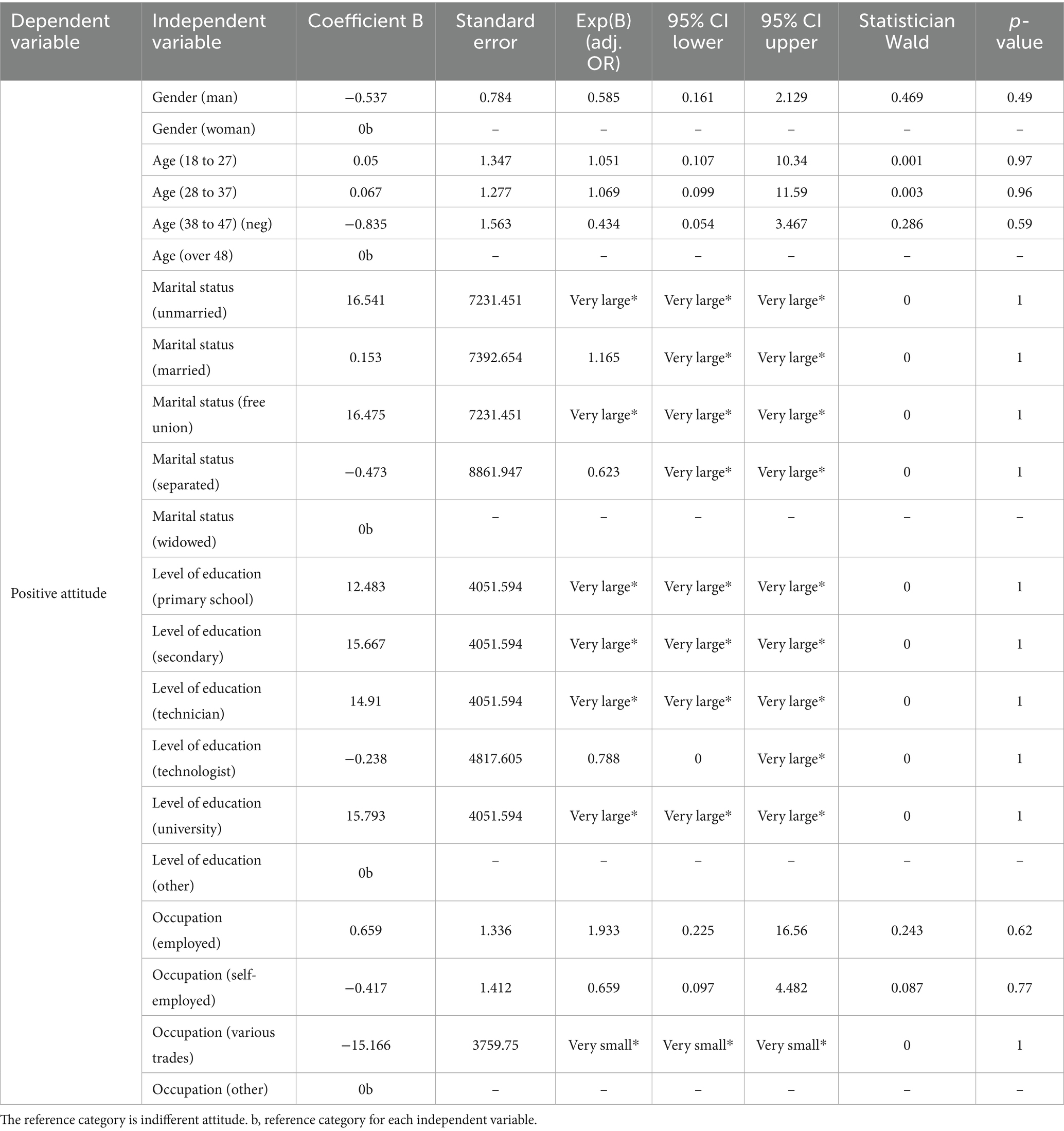
Table 6. Multinomial logical regression analysis of sociodemographic factors associated with attitude about MBD in a local area from Santander de Quilichao, Colombia.
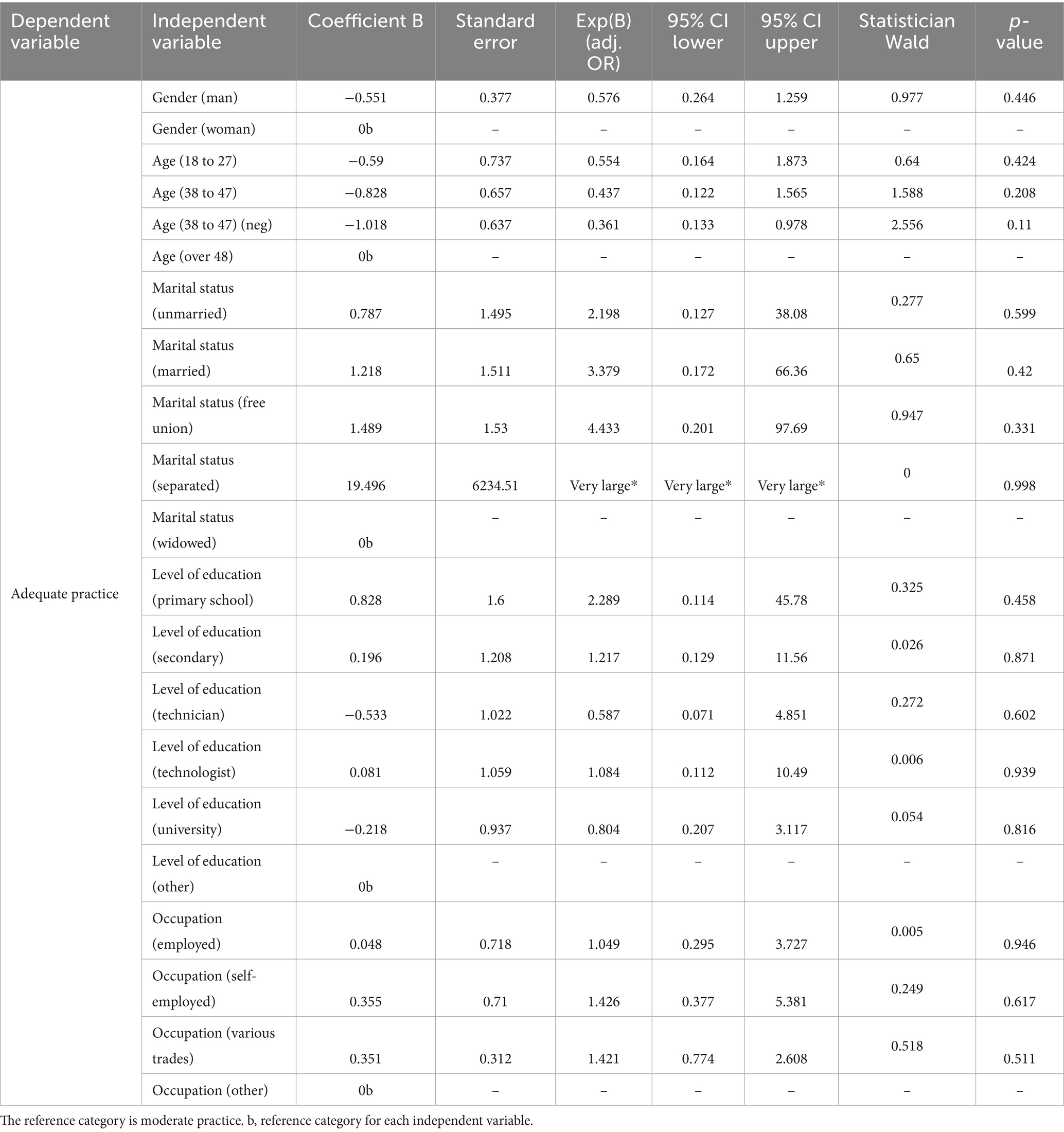
Table 7. Multinomial logical regression analysis of sociodemographic factors associated with practice about MBD in a local area from Santander de Quilichao, Colombia.
4 Discussion
Sociodemographic factors significantly influence KAP regarding MBD, informing effective interventions in tropical and subtropical regions (31). Community participation in various activities related to the prevention and mitigation of MBD is crucial for maintaining public health (77). A significant proportion of participants in this study identified mosquitoes as the primary vector of MBD (18, 31, 103, 104). In addition, knowledge of dengue symptoms was widespread, consistent with the findings of Selvarajoo et al. (38). Television, followed by social media and the Internet, were important sources of information about MBD and mosquito control. This is consistent with studies conducted in diverse countries such as Saudi Arabia (105), Bangladesh (27, 29), Colombia (58), Thailand (32, 34), and Malaysia (106). However, it contrasts with the findings of Suwanbamrung et al. (48), which showed that teachers were the main source of information on this topic. This reliance on traditional channels presents both a challenge and an opportunity: public health campaigns must leverage digital platforms to reach broader and younger audiences, thereby enhancing the effectiveness and scalability of MBD prevention efforts.
This study highlights a critical gap between general awareness of MBD and specific biomedical knowledge, with only 21.5% of participants correctly identifying dengue as a viral disease despite widespread recognition of mosquito transmission. This disconnect mirrors global trends and underscores the urgent need for targeted educational strategies that move beyond symptom recognition to foster pathogen specific understanding, which is essential for effective prevention and timely healthcare-seeking behavior (32, 58).
A majority of respondents recognized the importance of seeking medical attention for the diagnosis of MBD, whether at hospitals, private physicians’ offices, or public health centers. This finding is consistent with research conducted in Cameroon (104) and Colombia (70). In contrast, studies in Mexico have found that traditional medicine and home remedies are often preferred (103). The high level of knowledge about mosquito life cycles (91.9%) stands in stark contrast to the low recognition of clinical treatment protocols. This pattern is similar to results observed in Tanzania and Bangladesh, where ecological knowledge tends to surpass biomedical knowledge (29, 49). Notably, the reliance on television (31.4%) and interpersonal networks (a combined 43.6%) as primary sources of information highlights the continued influence of traditional communication channels, as opposed to the widespread use of digital platforms observed elsewhere (39, 44).
The most commonly reported preventive measure was the elimination of stagnant water, which is consistent with findings from other studies such as Alghazali et al. (107) and Desjardins et al. (57). However, some studies have found a preference for mosquito nets (18, 29, 50, 105) or chemical based methods like insecticides (104, 108). The strong emphasis on environmental management evidenced by 84.9% of participants prioritizing the elimination of stagnant water indicates effective public health messaging. Nevertheless, this contrasts with lower engagement in personal protection measures, a pattern also observed in urban communities in Brazil and Mexico (13, 51). Notably, only 58.7% of respondents acknowledged the existence of treatments for mosquito-borne diseases, suggesting potential gaps in healthcare access or distrust in medical systems a phenomenon previously associated with marginalized populations in Peru and Kenya (50, 56).
Regarding responsibility for MBD prevention, most participants believed it should be an individual responsibility, followed by actions carried out by the municipal administration (47). In this study, responses demonstrated high levels of knowledge and good practices in the management of MBD, similar to findings reported by Cochero et al. (59), Udayanga et al. (67), Phuyal et al. (68), and Barua et al. (69). A striking finding is the pronounced disconnect between high levels of knowledge and the prevalence of indifferent attitudes (94.8%), which fails to translate into consistent preventive practices (70). This gap signals that informational interventions alone are insufficient; psychosocial barriers, low risk perception, and limited institutional trust must be addressed through multifaceted strategies that integrate community empowerment and robust public sector engagement (66, 68).
Despite high literacy rates, the prevalence of indifferent attitudes (94.8%) challenges the assumption of a direct link between knowledge and behavior. This finding supports the hypothesis of van den Berg et al. (24) that psychosocial and infrastructural factors mediate the relationships between KAP. Indifference toward MBD and mosquitoes should be critically examined, considering possible underlying factors such as lack of knowledge, low risk perception, information fatigue, and cultural or socioeconomic barriers. Public health policy must prioritize interventions that bridge the gap between knowledge and action. This requires not only improving biomedical literacy but also fostering community engagement, building institutional trust, and deploying digital tools for health communication. Policies should be informed by local KAP profiles and designed to empower communities as active partners in disease prevention, ensuring that individual efforts are matched by effective organizational support.
This research provides evidence supporting the hypothesis that urban populations in MBD endemic regions develop selective health literacies shaped by cultural narratives and historical exposure to outbreaks. Our principal contribution is quantifying the gap between knowledge of mosquito control (91.9%) and pathogen specific understanding (21.5%), which represents a critical barrier to effective clinical prevention. The finding that 51.7% of participants desire more information about MBD offers an actionable pathway for community engaged interventions, particularly through mobile platforms that are already widely adopted.
The multinomial logistic regression model revealed a significant association between higher knowledge levels and participants’ marital status, in line with findings by Selvarajoo et al. (38) and Naing et al. (71), which demonstrated that being married is often linked to greater knowledge of mosquito-borne disease (MBD) management. In this study, both unmarried, married, and cohabiting individuals exhibited high knowledge, potentially due to differing life circumstances: unmarried individuals, typically younger, may access more recent information through academic environments, while married or cohabiting adults are more likely to participate in environmental education workshops as part of their employment (38). Furthermore, marital or partnered relationships can facilitate a positive feedback loop and mutual transfer of knowledge, especially when children are present, heightening concern for family health and well-being (72–75). However, despite these associations with knowledge, neither age nor marital status predicted attitudes or practices, underscoring that knowledge alone does not necessarily translate into behavior change. Consequently, effective interventions must go beyond demographic targeting to address broader structural and psychosocial determinants that shape health-related behaviors at the community level.
While the KAP framework has proven valuable for understanding community responses to mosquito-borne diseases, contemporary public health discourse increasingly situates such assessments within broader ecological paradigms. The concept of Nature Quotient (NQ), which emphasizes humanity’s capacity to coexist harmoniously with nature (76), offers a complementary lens through which to interpret our findings. From this perspective, cultivating public KAP regarding MBD represents a subdomain within the larger endeavor of nurturing societal ecological intelligence and fostering sustainable coexistence with natural ecosystems (61, 76). This ecological intelligence manifests not only in everyday behaviors and perceptions but also in transformative public health achievements, exemplified historically by Tu Youyou’s discovery of artemisinin from traditional herbal knowledge (76). Our findings reveal that participants possessed substantial knowledge about mosquito ecology (91.9%) yet demonstrated limited understanding of pathogen-specific mechanisms (21.5%), suggesting that ecological literacy alone is insufficient without deeper biomedical integration. To bridge this gap and enhance NQ at the community level, targeted education and communication strategies become paramount (68, 77, 78).
Evidence from systematic reviews and field interventions demonstrates that effective health education for MBD prevention requires multifaceted, culturally resonant approaches that transcend traditional information dissemination (68, 78, 79). Community-based participatory education, involving workshops, peer educators, and household visits, has consistently demonstrated efficacy in improving knowledge scores, reducing vector indices, and promoting sustained preventive behaviors across diverse settings (79–82). School-based health promotion programs utilizing interactive methodologies and audiovisual materials have proven particularly effective, as students serve as change agents who amplify health messages throughout their families and communities (14, 83–85). Innovative communication strategies, including narrative storytelling and digital health technologies, show promise for engaging underserved populations and overcoming psychosocial barriers to behavior change (68, 86–88). Storytelling approaches that incorporate culturally specific narratives, personal testimonies, and traditional communication mediums resonate more deeply with communities, fostering emotional engagement and facilitating the translation of knowledge into practice (68, 86, 89). Digital platforms, including mobile health applications, SMS-based interventions, and participatory surveillance tools, offer scalable solutions for real-time disease monitoring, rapid information dissemination, and bidirectional communication between health authorities and communities (88, 90–92).
Integrating these educational and communicative strategies within the One Health framework enhances their effectiveness by addressing the multidimensional drivers of vector-borne diseases (77, 93–96). The One Health approach recognizes that human health, animal health, and environmental health are interconnected and that collaborative, multisectoral interventions yield superior outcomes (93–98). Successful implementation requires strong governance, sustained funding, community empowerment, and the strategic use of digital technologies for integrated surveillance and response (77, 90, 95, 98, 99). In our study context, the pronounced disconnect between high knowledge levels and prevalent indifferent attitudes (94.8%) underscores the necessity of moving beyond cognitive interventions to address affective and contextual determinants of health behavior. Future interventions should prioritize participatory approaches that co-design solutions with communities, leverage culturally appropriate communication channels, integrate digital tools for sustained engagement, and embed MBD prevention within broader environmental health and sustainability education (78–80, 97, 100, 101). By reframing MBD prevention as an integral component of developing societal NQ, public health programs can foster ecological consciousness that supports not only disease control but also broader goals of environmental stewardship and One Health implementation (76, 77, 94, 96).
Finally, it is important to highlight Colombia’s commitment to addressing public health challenges through community based and empirical research. Strengths of this study include the use of information and communications technologies and the review of novel documentation on MBD as potential keys for future health management interventions. A key limitation of this study is its cross-sectional design and urban, highly educated sample, which restricts the generalizability of findings to rural or less-educated populations where the burden of MBD may be greater (11). Additionally, while the sample size was sufficient for estimating population proportions, it may have limited the statistical power and generalizability of our multinomial logistic regression analyses, particularly in subgroup comparisons. Future research should employ larger, stratified samples along with mixed methods and validated, disease-specific instruments to disentangle the drivers of attitudinal indifference and assess the long-term impact of digital and community-based interventions.
The KAP strategy has been successfully implemented in a number of tropical regions around the world. The results obtained in these regions are consistent with those from local communities in other countries, including significant studies from the Lao Democratic Republic, Thailand (34) and Hong Kong (37). In Colombia, KAP surveys have been instrumental in exploring the interaction between sociodemographic factors and community health behaviors, particularly in urban centers such as Riohacha (56) and Cali (57, 66). The data processing methods used, particularly multivariate analysis, enhance the robustness of the results and contribute to the refinement of MBD prevention strategies and mosquito management practices. This analytical approach not only facilitates a deeper understanding of community dynamics but also informs targeted interventions that are critical for effective disease control.
The existence of unanswered questions highlights the need for further research. First, how do socioeconomic gradients within urban areas influence KAP profiles? Second, it is important to determine the role of misinformation in sustaining indifferent attitudes despite high literacy rates. Third, could the strong emphasis on individual responsibility (90%) potentially hinder collective action against mosquito proliferation? Future studies should employ mixed methods to explore cultural perceptions of MBD and assess the long-term effectiveness of digital education campaigns in bridging the KAP gap.
5 Conclusion
The findings indicate that while marital status is significantly associated with knowledge levels and education shows a positive trend, no sociodemographic factors influence attitudes or the adoption of preventive practices against mosquito-borne diseases. There is a general awareness of basic control measures but limited understanding of the viral etiology and a prevailing indifference that fails to translate into personal protection. This underscores that mere information dissemination is insufficient to effect behavioral change; therefore, context-specific educational interventions are needed to foster active engagement and institutional trust, address psychosocial and risk-perception barriers, and leverage digital tools and school settings to empower communities and bridge the gap between knowledge and practice.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Faculty of Education of the University of Santiago de Cali Colombia. Junta de Acción Comunal of the urban sector of the municipality of Santander de Quilichao Colombia. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FB-R: Resources, Conceptualization, Validation, Investigation, Writing – original draft, Writing – review & editing, Formal analysis, Software, Data curation, Visualization. CG-F: Validation, Writing – review & editing, Supervision, Methodology, Visualization. JP: Visualization, Funding acquisition, Supervision, Project administration, Validation, Methodology, Resources, Writing – review & editing, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research has been funded by the Directorate General for Research of the University of Santiago de Cali under call No. DGI-01-2025.
Acknowledgments
We would like to thank the community of the municipality of Santander de Quilichao that participated in the project. Also, to Dirección General de Investigaciones of Universidad Santiago de Cali for their economical and institutional support under call No. DGI-01-2025.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1682827/full#supplementary-material
Footnotes
References
1. World Health Organization. Vector-borne diseases (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/vector-borne-diseases (Accessed 20 June, 2022)
2. Pan American Health Organization. Global vector control response 2017–2030 (2017). Available online at: https://www.paho.org/en/documents/global-vector-control-response-2017-2030-0 (Accessed 20 June, 2022)
3. Cavalcante, JM, Keppler, RLF, and Hamada, N. Family Culicidae In: N Hamada, DC Rogers, and JH Thorp, editors. Thorp and Covich's freshwater invertebrates. 4th ed. Oxford: Academic Press (2018). 723–45.
4. Foster, WA, and Walker, ED. Mosquitoes (Culicidae) In: GR Mullen and LA Durden, editors. Medical and veterinary entomology. 3rd ed. Oxford: Academic Press (2019). 261–325.
5. Pombi, M, and Montarsi, F. Mosquitoes (Culicidae) In: N Rezaei, editor. Encyclopedia of infection and immunity. Denver, USA: Elsevier. (2022). 801–18.
6. Martín-Park, A, Che-Mendoza, A, Contreras-Perera, Y, Pérez-Carrillo, S, Puerta-Guardo, H, Villegas-Chim, J, et al. Pilot trial using mass field-releases of sterile males produced with the incompatible and sterile insect techniques as part of integrated Aedes aegypti control in Mexico. PLoS Negl Trop Dis. (2022) 16:e0010324. doi: 10.1371/JOURNAL.PNTD.0010324
7. Lowe, R, and Codeço, CT. Harmonizing multisource data to inform vector-borne disease risk management strategies. Annu Rev Entomol. (2024) 70:337–58. doi: 10.1146/annurev-ento-040124-015101
8. Pan American Health Organization. Guidelines for the detection and surveillance of emerging arboviruses in the context of the circulation of other arboviruses. (2024a). Available online at: https://www.paho.org/en/documents/guidelines-detection-and-surveillance-emerging-arboviruses-context-circulation-other (Accessed 15 December, 2024)
9. Madewell, ZJ. Arboviruses and their vectors. South Med J. (2020) 113:520–3. doi: 10.14423/SMJ.0000000000001152
10. Rocha, BA, Souto, GR, Grossmann, SDMC, Souza, PEA, Soares, RV, and Horta, MCR. Oropouche fever: an emerging arbovirus disease from the Americas with possible oral manifestations. J Oral Diagn. (2024) 10:e276. doi: 10.5327/2525-5711.276
11. Pan American Health Organization. Epidemiological alert - risk of dengue outbreaks due to increased circulation of DENV-3 in the Americas region (2025a). Available online at: https://www.paho.org/sites/default/files/2025-02/2025-feb-7-phe-epi-alert-dengue-final.pdf (Accessed 17 March, 2025)
12. Pan American Health Organization. Epidemiological update - chikungunya in the region of the Americas - 22 April 2024 (2024b). Available online at: https://www.paho.org/en/documents/epidemiological-update-chikungunya-region-americas-22-april-2024 (Accessed 15 December, 2024)
13. de Souza, WM, and Weaver, SC. Effects of climate change and human activities on vector-borne diseases. Nat Rev Microbiol. (2024) 22:476–91. doi: 10.1038/S41579-024-01026-0
14. Estallo, EL, Madelon, MI, Benítez, EM, Camacho-Rodríguez, D, Martín, ME, Stewart-Ibarra, AM, et al. Empowering communities through citizen science: dengue prevention in Córdoba. Biology. (2024) 13:826. doi: 10.3390/biology13100826
15. Parker, C, Garcia, F, Menocal, O, Jeer, D, and Alto, B. A mosquito workshop and community intervention: a pilot education campaign to identify risk factors associated with container mosquitoes in San Pedro Sula, Honduras. Int J Environ Res Public Health. (2019) 16:2399. doi: 10.3390/ijerph16132399
16. Pan American Health Organization. Epidemiological Update Dengue, chikungunya and Zika. (2023). Available online at: https://www.paho.org/en/documents/epidemiological-update-dengue-chikungunya-and-zika-25-january-2023 (Accessed 5 July, 2023)
17. Alqassim, AY, Mahfouz, MS, Alharbi, AA, Muaddi, MA, Jareebi, MA, Makeen, AM, et al. Evaluating the public’s readiness to combat vector-borne disease threats in Jazan, Saudi Arabia: A cross-sectional survey. Medicine. (2024) 103:e39114. doi: 10.1097/MD.0000000000039114
18. Nieto, T, Mendez, F, and Carrasquilla, G. Knowledge, beliefs and practices relevant for malaria control in an endemic urban area of the Colombian Pacific. Soc Sci Med. (1999) 49:601–9. doi: 10.1016/S0277-9536(99)00134-3
19. Endale, A, Medhin, G, Hilo, AA, Abegaz, WE, and Legesse, M. Knowledge, attitude, and practice of Jinka University students about yellow fever, Ethiopia: a cross-sectional study. Risk Manag Healthc Policy. (2020) 13:1225–36. doi: 10.2147/RMHP.S250930
20. Buxton, M, Buxton, MP, Machekano, H, Nyamukondiwa, C, and Wasserman, RJ. A survey of potentially pathogenic-incriminated arthropod vectors of health concern in Botswana. Int J Environ Res Public Health. (2021) 18:10556. doi: 10.3390/ijerph181910556
21. Annan, E, Guo, J, Angulo-Molina, A, Yaacob, WFW, Aghamohammadi, N, Guetterman, TC, et al. Community acceptability of dengue fever surveillance using unmanned aerial vehicles: a cross-sectional study in Malaysia, Mexico, and Turkey. Travel Med Infect Dis. (2022) 49:102360. doi: 10.1016/j.tmaid.2022.102360
22. Bedoya-Rodríguez, FJ, Guevara-Fletcher, CE, and Vera-Lizcano, O. Identification, ecological indices and management of mosquitoes (Diptera: Culicidae) influencing environmental education processes in Colombian high schools. Int J Trop Insect Sci. (2022) 42:1401–20. doi: 10.1007/s42690-021-00657-7
23. Matlack, M, Covert, H, Shankar, A, Zijlmans, W, Abdoel Wahid, F, Hindori-Mohangoo, A, et al. Development of a pilot literacy scale to assess knowledge, attitudes, and behaviors towards climate change and infectious disease dynamics in Suriname. Int J Environ Res Public Health. (2023) 20:7178. doi: 10.3390/ijerph20247178
24. van den Berg, H, da Silva Bezerra, HS, Chanda, E, Al-Eryani, S, Nagpal, BN, Gasimov, E, et al. Management of insecticides for use in disease vector control: a global survey. BMC Infect Dis. (2021) 21:468. doi: 10.1186/s12879-021-06155-y
25. Kolimenakis, A, Latinopoulos, D, Bithas, K, Richardson, C, Lagouvardos, K, Stefopoulou, A, et al. Exploring public preferences, priorities, and policy perspectives for controlling invasive mosquito species in Greece. Trop Med Infect Dis. (2019) 4:83. doi: 10.3390/TROPICALMED4020083
26. Islam, S, Haque, CE, Hossain, S, and Walker, D. Association among ecological and behavioural attributes, dengue vector and disease control: a cross-sectional study of the city of Dhaka, Bangladesh. Int Health. (2020) 12:444–54. doi: 10.1093/inthealth/ihz079
27. Bashar, K, Mahmud, S, Tusty, EA, and Zaman, AB. Knowledge and beliefs of the city dwellers regarding dengue transmission and their relationship with prevention practices in Dhaka city, Bangladesh. Public Health Pract. (2020) 1:100051. doi: 10.1016/j.puhip.2020.100051
28. Abir, T, Ekwudu, OM, Kalimullah, NA, Nur-A Yazdani, DM, Al Mamun, A, Basak, P, et al. Dengue in Dhaka, Bangladesh: hospital-based cross-sectional KAP assessment at Dhaka north and Dhaka South City corporation area. PLoS One. (2021) 16:e0249135. doi: 10.1371/JOURNAL.PONE.0249135
29. Das, S, Rahman, MM, Rahaman, MM, Noor, M, Akter, M, Uddin, MJ, et al. Knowledge, attitude and prevention practices of garment factory workers regarding the largest dengue outbreak on record in Bangladesh. Transbound Emerg Dis. (2021) 69:360–8. doi: 10.1111/tbed.13987
30. Roslan, MA, Ngui, R, Vythilingam, I, Fatt, CK, Soon, OP, Keat, LC, et al. Survey of dengue knowledge and prevention practices associated with sociodemographic status: a cross-sectional study among the community living in an urban area of Selangor, Malaysia. J Am Mosq Control Assoc. (2020) 36:115–9. doi: 10.2987/19-6904.1
31. Hossain, MI, Alam, NE, Akter, S, Suriea, U, Aktar, S, Shifat, SK, et al. Knowledge, awareness and preventive practices of dengue outbreak in Bangladesh: A countrywide study. PLoS One. (2021) 16:e0252852. doi: 10.1371/journal.pone.0252852
32. Rahman, MS, Ekalaksananan, T, Zafar, S, Poolphol, P, Shipin, O, Haque, U, et al. Ecological, social, and other environmental determinants of dengue vector abundance in urban and rural areas of northeastern Thailand. Int J Environ Res Public Health. (2021a) 18:5971. doi: 10.3390/IJERPH18115971
33. Rahman, MS, Karamehic-Muratovic, A, Baghbanzadeh, M, Amrin, M, Zafar, S, Rahman, NN, et al. Climate change and dengue fever knowledge, attitudes and practices in Bangladesh: A social media–based cross-sectional survey. Trans R Soc Trop Med Hyg. (2021b) 115:85–93. doi: 10.1093/TRSTMH/TRAA093
34. Rahman, MS, Overgaard, HJ, Pientong, C, Mayxay, M, Ekalaksananan, T, Aromseree, S, et al. Knowledge, attitudes, and practices on climate change and dengue in Lao People's Democratic Republic and Thailand. Environ Res. (2021c) 193:110509. doi: 10.1016/j.envres.2020.110509
35. Rahman, MS, Pientong, C, Zafar, S, Ekalaksananan, T, Paul, RE, Haque, U, et al. Mapping the spatial distribution of the dengue vector Aedes aegypti and predicting its abundance in northeastern Thailand using machine-learning approach. One Health. (2021d) 13:100358. doi: 10.1016/j.onehlt.2021.100358
36. Koonisetty, KS, Aghamohammadi, N, Urmi, T, Yavaşoglu, Sİ, Rahman, MS, Nandy, R, et al. Assessment of knowledge, attitudes, and practices regarding dengue among physicians: a web-based cross-sectional survey. Behav Sci. (2021) 11:105. doi: 10.3390/bs11080105
37. Chan, EYY, Lo, ESK, Huang, Z, Lam, HCY, Yeung, MPS, Kwok, KO, et al. Sociodemographic predictors of knowledge, mosquito bite patterns and protective behaviors concerning vector borne disease: the case of dengue fever in Chinese subtropical city, Hong Kong. PLoS Negl Trop Dis. (2021) 15:e0008993. doi: 10.1371/journal.pntd.0008993
38. Selvarajoo, S, Liew, JWK, Tan, W, Lim, XY, Refai, WF, Zaki, RA, et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: A cross-sectional study. Sci Rep. (2020) 10:9534. doi: 10.1038/S41598-020-66212-5
39. Guad, RM, Mangantig, E, Low, WY, Taylor-Robinson, AW, Azzani, M, Sekaran, SD, et al. Development and validation of a structured survey questionnaire on knowledge, attitude, preventive practice, and treatment-seeking behaviour regarding dengue among the resident population of Sabah, Malaysia: an exploratory factor analysis. BMC Infect Dis. (2021) 21:893. doi: 10.1186/s12879-021-06606-6
40. Xu, JW, Liu, H, Yaw, B, and Nbwi, HS. The health beliefs, dengue knowledge and control behaviors among internally displaced persons versus local residents in Kachin special region II, Myanmar. PLoS Negl Trop Dis. (2020) 14:e0008321. doi: 10.1371/journal.pntd.0008321
41. Liu, H, Fang, CJ, and Xu, JW. The health perceptions, dengue knowledge and control willingness among Dai ethnic minority in Yunnan Province, China. BMC Public Health. (2021) 21:1843. doi: 10.1186/s12889-021-11864-9
42. Nguyen-Tien, T, Pham, LT, Vu, DT, Tran, SH, Vu, LT, Bui, VN, et al. Knowledge and practice on prevention of mosquito-borne diseases in livestock-keeping and non-livestock-keeping communities in Hanoi city, Vietnam: A mixed-method study. PLoS One. (2021) 16:e0246032. doi: 10.1371/journal.pone.0246032
43. Soh, LT, Ong, Z, Vasquez, K, Chen, I, Li, X, Niah, W, et al. A household-based survey to understand factors influencing awareness, attitudes and knowledge towards Wolbachia-Aedes technology. Int J Environ Res Public Health. (2021) 18:11997. doi: 10.3390/ijerph182211997
44. Akhiljith, VA, Sreerag, KR, Shalavadi, MH, Morabad, S, and Keshannavar, MG. Assessment of knowledge, attitude, practice towards vector borne diseases in urban area of Bagalkote, Karnataka, India. Int J Res Med Sci. (2024) 12:133. doi: 10.18203/2320-6012.ijrms20233988
45. Aerts, C, Revilla, M, Duval, L, Paaijmans, K, Chandrabose, J, Cox, H, et al. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vector-borne diseases in Guyana. PLoS Negl Trop Dis. (2020) 14:e0008149. doi: 10.1371/JOURNAL.PNTD.0008149
46. Giang, HTN, Sayed, AM, Dang, T, Iqtadar, S, Tuan, NM, Khiem, NT, et al. Survey of knowledge, attitude and practice of healthcare professionals on dengue transmission, diagnosis and clinical classification. BMC Infect Dis. (2021) 21:1130. doi: 10.1186/s12879-021-06816-y
47. Jayawickreme, KP, Jayaweera, DK, Weerasinghe, S, Warapitiya, D, and Subasinghe, S. A study on knowledge, attitudes and practices regarding dengue fever, its prevention and management among dengue patients presenting to a tertiary care hospital in Sri Lanka. BMC Infect Dis. (2021) 21:981. doi: 10.1186/S12879-021-06685-5
48. Suwanbamrung, C, Saengsuwan, B, Sangmanee, T, Thrikaew, N, Srimoung, P, and Maneerattanasak, S. Knowledge, attitudes, and practices towards dengue prevention among primary school children with and without experience of previous dengue infection in southern Thailand. One Health. (2021) 13:100275. doi: 10.1016/j.onehlt.2021.100275
49. Msellemu, D, Gavana, T, Ngonyani, H, Mlacha, YP, Chaki, P, and Moore, SJ. Knowledge, attitudes and bite prevention practices and estimation of productivity of vector breeding sites using a habitat suitability score (HSS) among households with confirmed dengue in the 2014 outbreak in Dar Es Salaam, Tanzania. PLoS Negl Trop Dis. (2020) 14:e0007278. doi: 10.1371/journal.pntd.0007278
50. Nyangau, PN, Nzuma, JM, Irungu, P, and Kassie, M. Evaluating livestock farmers knowledge, beliefs, and management of arboviral diseases in Kenya: A multivariate fractional probit approach. PLoS Negl Trop Dis. (2021) 15:e0009786. doi: 10.1371/journal.pntd.0009786
51. Elson, WH, Ortega, E, Kreutzberg-Martinez, M, Jacquerioz, F, Cabrera, LN, Oberhelman, RA, et al. Cross-sectional study of dengue-related knowledge, attitudes and practices in Villa El Salvador, Lima, Peru. BMJ Open. (2020) 10:e037408. doi: 10.1136/bmjopen-2020-037408
52. Manuli, ER, Pereira, GM, Bernat, MC, Novaes, CR, Sabino, EC, and Avelino-Silva, VI. Knowledge about clinical presentation, prevention strategies and sexual transmission of Zika virus infection among women of reproductive age in an endemic area. Braz J Infect Dis. (2021) 25:101629. doi: 10.1016/j.bjid.2021.101629
53. Bohmann, AK, Martinez-Berman, L, Senger, AR, and de Wise Valz, MR. Personality and city culture predict attitudes and practices toward mosquitoes and mosquito-borne diseases in South Texas. Front Public Health. (2022) 10:919780. doi: 10.3389/fpubh.2022.919780
54. Jiménez-Alejo, A, Pacheco-Soriano, AL, Liedo, P, Marina, CF, Bond, JG, Rodríguez-Ramos, JC, et al. Acceptance of a sterile male releases pilot project to reduce Aedes aegypti (Linnaeus, 1762) (Diptera: Culicidae) populations and its associated factors: a community-based cross-sectional survey in South Chiapas, Mexico. Acta Trop. (2022) 233:106573. doi: 10.1016/j.actatropica.2022.106573
55. Dowling, R, Thompson, AB, and Kolokotronis, SO. Knowledge, attitudes and practices about Zika virus infection among women of reproductive age in Central Brooklyn, New York City, USA. J Community Health. (2024) 49:78–85. doi: 10.1007/s10900-023-01258-w
56. Benítez-Díaz, L, Diaz-Quijano, FA, and Martínez-Vega, RA. Experiencia y percepción del riesgo asociados a conocimientos, actitudes y prácticas sobre dengue en Riohacha, Colombia. Ciênc Saúde Colet. (2020) 25:1137–46. doi: 10.1590/1413-81232020253.08592018
57. Desjardins, MR, Casas, I, Victoria, AM, Carbonell, D, Dávalos, DM, and Delmelle, EM. Knowledge, attitudes, and practices regarding dengue, chikungunya, and Zika in Cali, Colombia. Health Place. (2020) 63:102339. doi: 10.1016/j.healthplace.2020.102339
58. Bedoya-Rodríguez, FJ, Guevara-Fletcher, CE, and Pelegrin, JS. Citizen science and multimedia didactic resources: knowledge of mosquito-borne diseases in an urban area of southwestern Colombia. Trop Med Infect Dis. (2024) 9:256. doi: 10.3390/tropicalmed9110256
59. Cochero, BEO, Esquivel, VLP, and Jiménez, NNV. Perceptions of dengue fever from the perspective of a rural community on the Caribbean coast in Colombia. Mundo Saude. (2024) 48:e15982024. doi: 10.15343/0104-7809.202448e15982024P
60. Jaramillo-Ramirez, GI, Tacugue, MC, Power, GM, Qureshi, R, Seelig, F, Quintero, J, et al. A qualitative analysis of the perceptions of stakeholders involved in vector control and vector-borne disease research and surveillance in Orinoquia, Colombia. Trop Med Infect Dis. (2024) 9:43. doi: 10.3390/tropicalmed9020043
61. Duval, P, Aschan-Leygonie, C, and Valiente Moro, C. A review of knowledge, attitudes and practices regarding mosquitoes and mosquito-borne infectious diseases in nonendemic regions. Front Public Health. (2023) 11:1239874. doi: 10.3389/fpubh.2023.1239874
62. Gobernación del Cauca. Plan de Desarrollo Departamental Cauca 2024-2027 La Fuerza del Pueblo. (2023). Available online at: https://goo.su/r9kiTS (Accessed 17 June, 2025)
63. Alcaldía municipal de Santander de Quilichao. Plan de desarrollo municipal 2024–2027 (2024). Available online at: https://goo.su/eGt4fh (Accessed 20 September, 2024).
64. Pan American Health Organization. Knowledge, attitudes and practice surveys: Zika virus disease and potential complications: Resource pack. (2016). Available online at: https://www.paho.org/es/documentos/encuestas-conocimientos-actitudes-practicas-enfermedad-viral-zika-sus-posibles (Accessed 20 June, 2022).
65. Bujang, MA, Omar, ED, Foo, DHP, and Hon, YK. Sample size determination for conducting a pilot study to assess reliability of a questionnaire. Restor Dent Endod. (2024) 49:e3. doi: 10.5395/rde.2024.49.e3
66. Casas, I, Desjardins, M, and Delmelle, E. Knowledge, attitudes, and practices (KAP) toward dengue fever in Cali, Colombia. Geogr Rev. (2023) 114:70–98. doi: 10.1080/00167428.2023.2169882
67. Udayanga, L, Gunathilaka, N, Iqbal, MCM, Pahalagedara, K, Amarasinghe, US, and Abeyewickreme, W. Socio-economic, knowledge attitude practices (KAP), household related and demographic based appearance of non-dengue infected individuals in high dengue risk areas of Kandy District, Sri Lanka. BMC Infect Dis. (2018) 18:88. doi: 10.1186/s12879-018-2995-y
68. Phuyal, P, Kramer, IM, Kuch, U, Magdeburg, A, Groneberg, DA, Lamichhane Dhimal, M, et al. The knowledge, attitude and practice of community people on dengue fever in Central Nepal: a cross-sectional study. BMC Infect Dis. (2022) 22:454. doi: 10.1186/s12879-022-07404-4
69. Barua, P, Mahjuba, S, Biswas, MR, Alamgir Khan, A, Rahman, MK, and Musa, S. Socio-demographic factors associated with the knowledge, attitude and practice (KAP) of dengue patients of Dhaka city during 2021 dengue outbreak. Bangladesh J Zool. (2024) 52:167–84. doi: 10.3329/bjz.v52i2.77271
70. Diaz-Quijano, FA, Martínez-Vega, RA, Rodriguez-Morales, AJ, Rojas-Calero, RA, Luna-González, ML, and Díaz-Quijano, RG. Association between the level of education and knowledge, attitudes and practices regarding dengue in the Caribbean region of Colombia. BMC Public Health. (2018) 18:143. doi: 10.1186/S12889-018-5055-Z
71. Naing, C, Ren, WY, Man, CY, Fern, KP, Qiqi, C, Ning, CN, et al. Awareness of dengue and practice of dengue control among the semi-urban community: a cross sectional survey. J Community Health. (2011) 36:1044–9. doi: 10.1007/s10900-011-9407-1
72. Callejón-Chinchilla, MD, and Gila-Ordóñez, JM. Necesidad de trabajar las relaciones de pareja saludable desde contextos socio-educativos. Sophia. (2018) 14:31–8. doi: 10.18634/sophiaj.14v.1i.703
73. Doss, BD, Knopp, K, Roddy, MK, Rothman, K, Hatch, SG, and Rhoades, GK. Online programs improve relationship functioning for distressed low-income couples: results from a nationwide randomized controlled trial. J Consult Clin Psychol. (2020) 88:283–94. doi: 10.1037/ccp0000479
74. da Conceição Pacheco, A, Lino, MN, and Tilman, CB. Family characteristics, basic sanitation trought health promotion moderating in prevention dengue in Dom Alexo, Dili 2024. Asian J Healthy Sci. (2024) 3:278–89. doi: 10.58631/ajhs.v3i10.146
75. Jiménez, NNV, and Constanzo, AZ. The empowered family: new narratives to rethink dengue prevention and control in Córdoba, Colombia. Salud Colect. (2024) 20:e4800. doi: 10.18294/sc.2024.4800
76. Vuong, QH, and Nguyen, MH. On nature quotient. Pac Conserv Biol. (2025) 31:PC25028. doi: 10.1071/PC25028
77. Robbiati, C, Milano, A, Declich, S, and Dente, MG. One health prevention and preparedness to vector-borne diseases: how should we deal with a multisectoral, multilevel and multigroup governance? One Health Outlook. (2024) 6:21. doi: 10.1186/s42522-024-00114-8
78. Heyrani, A, Barzegar, G, Valizadeh, R, Fazlzadeh, M, Moradi, G, and Carson-Chahhoud, K. A comprehensive scoping review of global educational strategies and outcomes in Aedes-borne disease control. BMC Public Health. (2024) 24:2723. doi: 10.1186/s12889-024-20199-0
79. Lachyan, A, Sarfraz, M, Tariq, I, and Sarfraz, Z. The effect of community-based intervention on dengue prevention in poor urban areas: a quasi-experimental study. Int J Prev Med. (2023) 14:150. doi: 10.4103/ijpvm.ijpvm_407_21
80. Tiffin, HS, Peper, ST, Wilson, A, Jervis, S, Ezeonu, C, Meuti, M, et al. One health, many approaches: integrated vector management as a holistic approach to vector-borne disease control. Front Insect Sci. (2025) 5:1549348. doi: 10.3389/finsc.2025.1549348
81. LaBeaud, AD, Kuile, FO, Solomon, T, King, CH, Malhotra, I, Grossi-Soyster, E, et al. School-based health promotion for mosquito-borne disease prevention: a pilot study. Am J Trop Med Hyg. (2009) 80:1030–6. doi: 10.1016/j.jpeds.2009.03.009
82. Walton, C, Manrique-Saide, P, Vazquez-Prokopec, GM, Coleman, PG, Sterrett, JI, Cordon-Rosales, C, et al. Community-based biological control and larval source management for the prevention of mosquito-borne disease: a systematic review. Lancet Planet Health. (2021) 5:e788–803. doi: 10.1016/S2542-5196(21)00220-5
83. Barrera, R, Acevedo, V, Felix, GE, Hemme, RR, Vazquez, J, Munoz, JL, et al. Impact of autocidal gravid ovitraps on chikungunya virus incidence in Aedes aegypti (Diptera: Culicidae) in areas with and without traps. J Med Entomol. (2017) 54:387–95. doi: 10.1093/jme/tjw187
84. Kittayapong, P, Ninphanomchai, S, Limohpasmanee, W, Chansang, C, Chansang, U, and Mongkalangoon, P. Combined sterile insect technique and incompatible insect technique: the first proof-of-concept to suppress Aedes aegypti vector populations in semi-rural settings in Thailand. PLoS Negl Trop Dis. (2019) 13:e0007771. doi: 10.1371/journal.pntd.0007771
85. Al-Eryani, SMA, Akramah, YS, Al-Shuaibi, SA, and Al-Tahish, AH. School-based educational intervention for dengue fever prevention in Yemen. East Mediterr Health J. (2021) 27:346–54. doi: 10.26719/emhj.20.139
86. Schiavo, R. Health communication: From theory to practice. 2nd ed. San Francisco: Jossey-Bass (2014).
87. Hinyard, LJ, and Kreuter, MW. Using narrative communication as a tool for health behavior change: a conceptual, theoretical, and empirical overview. Health Educ Behav. (2007) 34:777–92. doi: 10.1177/1090198106291963
88. Carrillo, MA, Kroeger, A, Sanchez, LM, Monsalve, S, and Ranzinger, SR. The use of mobile phones for the prevention and control of arboviral diseases: a scoping review. BMC Public Health. (2021) 21:110. doi: 10.1186/s12889-020-10126-4
89. Houston, TK, Allison, JJ, Sussman, M, Horn, W, Holt, CL, Trobaugh, J, et al. Culturally appropriate storytelling to improve blood pressure: a randomized trial. Ann Intern Med. (2011) 154:77–84. doi: 10.7326/0003-4819-154-2-201101180-00004
90. Tilahun, B, Gashu, KD, Mekonnen, ZA, Endehabtu, BF, and Angaw, DA. Mapping the role of digital health technologies in the case detection, management, and treatment outcomes of neglected tropical diseases: a scoping review. Trop Med Health. (2021) 49:17. doi: 10.1186/s41182-021-00307-1
91. Majumder, MS, Santillana, M, Mekaru, SR, McGinnis, DP, Khan, K, and Brownstein, JS. Utilizing nontraditional data sources for near real-time estimation of transmission dynamics during the 2015-2016 Colombian Zika virus disease outbreak. JMIR Public Health Surveill. (2016) 2:e30. doi: 10.2196/publichealth.5814
92. Marques-Toledo, CA, Degener, CM, Vinhal, L, Coelho, G, Meira, W, Codeço, CT, et al. Dengue prediction by the web: tweets are a useful tool for estimating and forecasting dengue at country and city level. PLoS Negl Trop Dis. (2017) 11:e0005729. doi: 10.1371/journal.pntd.0005729
93. Mackenzie, JS, and Jeggo, M. The one health approach—why is it so important? Trop Med Infect Dis. (2019) 4:88. doi: 10.3390/tropicalmed4020088
94. Zinsstag, J, Schelling, E, Waltner-Toews, D, and Tanner, M. From "one medicine" to "one health" and systemic approaches to health and well-being. Prev Vet Med. (2011) 101:148–56. doi: 10.1016/j.prevetmed.2010.07.003
95. World Health Organization. One Health. (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/one-health (Accessed December 15, 2024)
96. Aenishaenslin, C, Brunet, P, Lévesque, F, Gouin, GG, Simon, A, Saint-Charles, J, et al. Understanding the connections between dogs, health and Inuit through a mixed-methods study. EcoHealth. (2019) 16:151–60. doi: 10.1007/s10393-018-1386-6
97. Conrad, PA, Meek, LA, and Dumit, J. Operationalizing a one health approach to global health challenges. Comp Immunol Microbiol Infect Dis. (2013) 36:211–6. doi: 10.1016/j.cimid.2013.03.006
98. Yopa, DS, Panda, M, Kouaméhoué, E, Diop, B, Diallo, AH, Bakou, SN, et al. Barriers and enablers to the implementation of one health: a scoping review. PLoS Negl Trop Dis. (2023) 17:e0011693. doi: 10.1371/journal.pntd.0011693
99. Lee, K, and Brumme, ZL. Operationalizing the one health approach: the global governance challenges. Health Policy Plan. (2013) 28:778–85. doi: 10.1093/heapol/czs127
100. Destoumieux-Garzón, D, Mavingui, P, Boetsch, G, Boissier, J, Darriet, F, Duboz, P, et al. The one health concept: 10 years old and a long road ahead. Front Vet Sci. (2018) 5:14. doi: 10.3389/fvets.2018.00014
101. Monroe, MC, Plate, RR, Oxarart, A, Bowers, A, and Chaves, WA. Identifying effective climate change education strategies: a systematic review of the research. Environ Educ Res. (2019) 25:791–812. doi: 10.1080/13504622.2017.1360842
102. Pan American Health Organization. Epidemiological update Oropouche in the Americas region (2025b). Available online at: https://www.paho.org/sites/default/files/2025-02/2025-feb-10-epi-update-oropoucheeng-final_0.pdf (Accessed 17 March, 2025)
103. Nava-Doctor, JE, Sandoval-Ruiz, CA, and Fernández-Crispín, A. Knowledge, attitudes, and practices regarding vector-borne diseases in Central Mexico. J Ethnobiol Ethnomed. (2021) 17:45. doi: 10.1186/s13002-021-00471-y
104. Bamou, R, Tchuinkam, T, Kopya, E, Awono-Ambene, P, Njiokou, F, Mwangangi, J, et al. Knowledge, attitudes, and practices regarding malaria control among communities living in the South Cameroon forest region. IJID Reg. (2022) 5:169–76. doi: 10.1016/j.ijregi.2022.11.003
105. Khairy, S, Al-Surimi, K, Ali, A, Shubily, HM, Al Walaan, N, Househ, M, et al. Knowledge, attitude and practice about malaria in South-Western Saudi Arabia: A household-based cross-sectional survey. J Infect Public Health. (2017) 10:499–506. doi: 10.1016/j.jiph.2016.09.021
106. Aslam, F, Bibi, R, Lal Din, I, Anwar, S, Mehboob, DY, Habib, U, et al. Effect of educational interventions on awareness of dengue fever and its preventive measures among high school students: educational interventions on awareness of dengue fever. NURSEARCHER (J Nurs Midwifery Sci). (2024) 4:24–9. doi: 10.54393/nrs.v4i03.114
107. Alghazali, KA, Teoh, BT, Sam, SS, Abd-Jamil, J, Johari, J, Atroosh, WM, et al. Dengue fever among febrile patients in Taiz City, Yemen during the 2016 war: clinical manifestations, risk factors, and patients knowledge, attitudes, and practices toward the disease. One Health. (2020) 9:100119. doi: 10.1016/j.onehlt.2019.100119
Keywords: arboviruses, health and biological education, mosquito control, knowledge, attitudes and practices, mosquito-borne diseases
Citation: Bedoya-Rodríguez FJ, Guevara-Fletcher CE and Pelegrin JS (2025) Knowledge, attitudes, and practices regarding mosquito-borne diseases in an urban sector of southwestern Colombia. Front. Public Health. 13:1682827. doi: 10.3389/fpubh.2025.1682827
Edited by:
Minh-Hoang Nguyen, Phenikaa University, VietnamReviewed by:
Sandra Helena Suescún Carrero, University of Boyaca, ColombiaHemma Yulfi, Universitas Sumatera Utara Departemen Parasitologi, Indonesia
Copyright © 2025 Bedoya-Rodríguez, Guevara-Fletcher and Pelegrin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco Javier Bedoya-Rodríguez, ZnJhbmNpc2NvLmJlZG95YTAwQHVzYy5lZHUuY28=; Jonathan S. Pelegrin, am9uYXRoYW4ucGVsZWdyaW4wMEB1c2MuZWR1LmNv