 Zhihui Huang
Zhihui Huang Zhaohong Li1
Zhaohong Li1 Jianyun Lu
Jianyun Lu- 1Guangzhou Baiyun District Center for Disease Control and Prevention, Guangzhou, China
- 2Guangzhou Huadu District Huadong Town Health Center, Guangzhou, China
Objective: This study aims to analyze the factors influencing dengue fever prevention knowledge, attitude, and practice (KAP) among urban residents in Guangzhou and to evaluate the effectiveness of an mHealth intervention based on the KAP model.
Methods: A cross-sectional study was conducted with 3,571 participants from an online survey. A quasi-experimental study (84 in the intervention group and 83 in the control group) was carried out over 2 months. Electronic questionnaires assessed baseline KAP levels, and the groups’ differences were compared post-intervention.
Results: The baseline survey revealed a knowledge awareness rate of 80.29%, with the lowest levels found in males aged 55 and above, low-education groups, and temporary housing residents. Significant demographic differences were observed in prevention motivation and behavior (p < 0.05). Post-intervention, the experimental group showed significant improvements in knowledge scores (p < 0.05), but no significant differences were found in prevention motivation (13.26 ± 1.92 vs. 13.32 ± 2.02) and behavior (4.08 ± 1.00 vs. 4.34 ± 0.91) (p > 0.05).
Conclusion: The mHealth intervention effectively improved knowledge, but had limited impact on belief formation and behavior change. Future interventions should integrate community-specific strategies to enhance behavioral change mechanisms.
1 Introduction
Dengue fever, a mosquito-borne viral illness, is increasingly recognized as a significant global health issue (1). It is estimated by the World Health Organization (WHO) that 390 million infections of dengue are experienced annually, and many of these infections progress to clinical manifestations (2). Dengue exists in over 100 countries, predominantly in the tropical and subtropical regions of the globe (3), where the Aedes aegypti mosquito serves as the vector (4). The rapid growth in the incidence of dengue fever is attributable to a synergy of various factors spanning urbanization, climate change, and increased mobility of populations (5). Urban areas characterized by inadequate solid waste management (particularly water-holding containers), suboptimal water storage practices, and elevated human population density demonstrate significantly higher risks of dengue virus transmission (6). This has fueled the increasing frequency of outbreaks, which in turn heightens the public health burden. In cities such as Guangzhou, the frequency of dengue outbreaks has increased, making it essential to develop effective prevention strategies (7).
While dengue vaccines have been available since 2015, vector control remains the principal intervention against dengue fever (8). One of the primary ways of promoting public health and managing dengue dissemination involves ascertaining how the knowledge, attitudes, and practices (KAP) of the inhabitants influence their preventive behavior (9). The most prevalent approach for assessing health behavior is the KAP model, which is founded on the principle that knowledge directly influences attitudes, which in turn influence behavior (10). While the majority of the KAP studies have been applied in chronic illnesses such as diabetes, HIV and coronary heart disease (11–13), fewer studies have applied the KAP model to infectious diseases such as dengue fever. Lifestyle modification represents a pivotal component in the management of cardiovascular disease. The adoption of healthy behaviors is influenced by multiple factors, including knowledge, attitudes, and practices (KAP), social support, and individual patient characteristics. The KAP model provides a valuable framework for conceptualizing and implementing behavioral change. By addressing the underlying psychological determinants of behavior, healthcare providers can more effectively facilitate the adoption of healthy lifestyles in patients (14). Similarly, by evaluating the knowledge of residents about dengue, attitudes toward prevention, and practice, public health campaigns can be more effectively tailored to the population’s needs. Furthermore, the model may be utilized to identify knowledge gaps and misconceptions that may hinder the adoption of preventive behaviors, a necessary step in the creation of effective health interventions.
In recent years, mobile health (mHealth) has emerged as a powerful mechanism for disseminating health information and promoting behavior change (15). mHealth involves the use of mobile technologies such as smartphones and tablets to deliver health-related services, including educational content, reminders, and behavioral interventions (16). The pervasiveness of mobile devices presents a unique opportunity to reach large populations at minimal cost. Research indicates that web-based health interventions demonstrate cost-effectiveness, offering novel perspectives for optimizing public health resource allocation (17). In dengue prevention, mHealth interventions have the potential to spread timely, correct information about the disease, its transmission, and prevention while promoting positive behavior change in the use of insect repellents, elimination of mosquito breeding sites, and avoidance of periods of peak mosquito activity. These interventions can also provide personalized recommendations, making them more effective through customization to individual tastes and needs (18). Previous studies have established that mHealth interventions can successfully impact health knowledge and behaviors in a variety of topics in public health, such as smoking, chronic disease management, and infectious disease prevention (19–22). However, if mHealth is to be effective in dengue prevention, it must not only bridge the knowledge gap but also influence the attitudes and behaviors of the residents in order to prompt them into action.
The aim of this study is to assess the baseline knowledge, attitude, and practice (KAP) levels of dengue fever prevention among the urban residents of Guangzhou. It also seeks to establish the impact of an mHealth intervention, based on the KAP model, in improving the KAP levels, particularly in improving the knowledge and preventive practices of the residents. By targeting specific factors that influence dengue prevention, this study aims to guide the development of more targeted and efficacious health education interventions that can be implemented in Guangzhou, and in other comparable cities with the same public health concerns.
2 Methods
2.1 Study design and participants
This study employed a two-phase, sequential design, comprising an initial cross-sectional survey followed by a quasi-experimental intervention.
2.1.1 Phase 1: cross-sectional survey
A cross-sectional survey was conducted to assess the baseline levels of knowledge, attitudes, and practices (KAP) regarding dengue prevention. Participants were recruited using a convenience sampling method. Specifically, the study distributed an online questionnaire through WeChat communities (e.g., resident groups, workplace groups) targeting permanent residents of Guangzhou. The survey was administered between September 20, 2024, and October 20, 2024, and the final cross-sectional sample consisted of 3,571 permanent residents of Guangzhou aged 18 to 70 years.
2.1.2 Phase 2: quasi-experimental study
Following the survey, a subset of participants was invited to join an mHealth intervention study. The eligibility criteria for this phase included: (1) being a permanent resident of Guangzhou; (2) aged 18–70 years; (3) ability to use WeChat; (4) having completed the baseline survey; (5) agreed to join the WeChat group and be assigned to a group. A total of 167 individuals voluntarily agreed to participate and were allocated into groups based on self-selection. Participants self-selected into either the intervention group or the control group.
2.2 Questionnaire development
The data collection instrument was a self-administered questionnaire based on the knowledge, attitude, and practices (KAP) model. Initial items were generated from a comprehensive review of relevant literature on dengue prevention. Content validity was established through consultations with a panel of five experts in public health and infectious diseases. The final questionnaire comprised 29 items across three core domains: knowledge (e.g., transmission routes, symptoms), attitudes (e.g., perceived severity, susceptibility), and practices (e.g., mosquito breeding site elimination, personal protective behaviors). Demographic information was also collected.
2.3 Questionnaire testing and reliability
Prior to the formal survey, the questionnaire was distributed to 90 residents through WeChat communities in a pilot test to assess clarity, comprehensibility, and feasibility. All questionnaires were returned (100% response rate). The internal consistency reliability of the questionnaire was evaluated using Cronbach’s alpha coefficient based on the pilot data. The overall Cronbach’s α for the questionnaire was 0.806, indicating good reliability.
2.4 Intervention details
The intervention group received a comprehensive mHealth intervention over 2 months. This included:
2.4.1 Personalized knowledge delivery
Students were given dengue-specific learning content, including symptoms, transmission modes, and prevention methods, according to their starting knowledge level.
2.4.2 Interactive engagement
The intervention comprised quizzes, polls, and WeChat discussions in order to enhance learning and provide continuous feedback.
2.4.3 Behavioral guidance
The participants were encouraged to adopt some preventive practices such as draining stagnant water, sleeping in insect-repellent coated mosquito nets, and using insect repellent.
2.4.4 Community support
Intervention enabled peer education and community engagement through the creation of a WeChat group where members educated each other and shared mutual support to take dengue prevention measures.
The control group received basic health education, including information on dengue symptoms and treatment options, but did not participate in the interactive and behavioral components of the intervention.
2.5 Data collection
Data were collected by electronic questionnaires at two time points: baseline (before intervention) and after the two-month intervention. The questionnaires assessed knowledge, attitudes, and practices for prevention of dengue. Multiple-choice questions were used to assess knowledge, a Likert scale to assess attitudes, and self-reported preventive acts to assess practices.
2.6 Statistical analysis
Data were analyzed using SPSS 24.0 software. Descriptive statistics were used to report demographic variables and KAP scores. Baseline characteristics across different groups in the cross-sectional survey were compared using t-tests, ANOVA, Chi-square, or Fisher’s exact tests as appropriate. The effect of the intervention was assessed by comparing pre- and post-intervention scores within and between the two groups with paired t-tests for continuous variables and chi-square tests for categorical variables. p < 0.05 was used as the level of statistical significance.
2.7 Ethics approval
This study was approved by the Ethics Committee of the Guangzhou Baiyun District Center for Disease Control and Prevention. All collected data were anonymized, and no personally identifiable information was obtained.
2.7.1 Baseline survey
Before accessing the online survey, all potential participants were presented with an electronic informed consent form. This form outlined the study’s objectives, procedures, voluntary participation and the confidentiality measures. Participants under 18 years of age were required to obtain parental or guardian approval before agreeing.
2.7.2 mHealth intervention trial
Eligible adults were recruited exclusively from the baseline cohort. Participation in the mHealth intervention phase commenced upon voluntary enrollment into designated WeChat groups. Participants retained the right to withdraw from the intervention at any time by exiting the WeChat group.
3 Results
3.1 Baseline survey
3.1.1 Among the knowledge awareness
The overall dengue knowledge awareness rate was 80.29%. Significant differences were found across age, gender, residential area, housing type, education level, and occupation (p < 0.05). For instance, residents aged 35–54 showed the highest awareness (82.49%), while those aged 55 and above had the lowest (64.44%). The results as shown in Table 1.
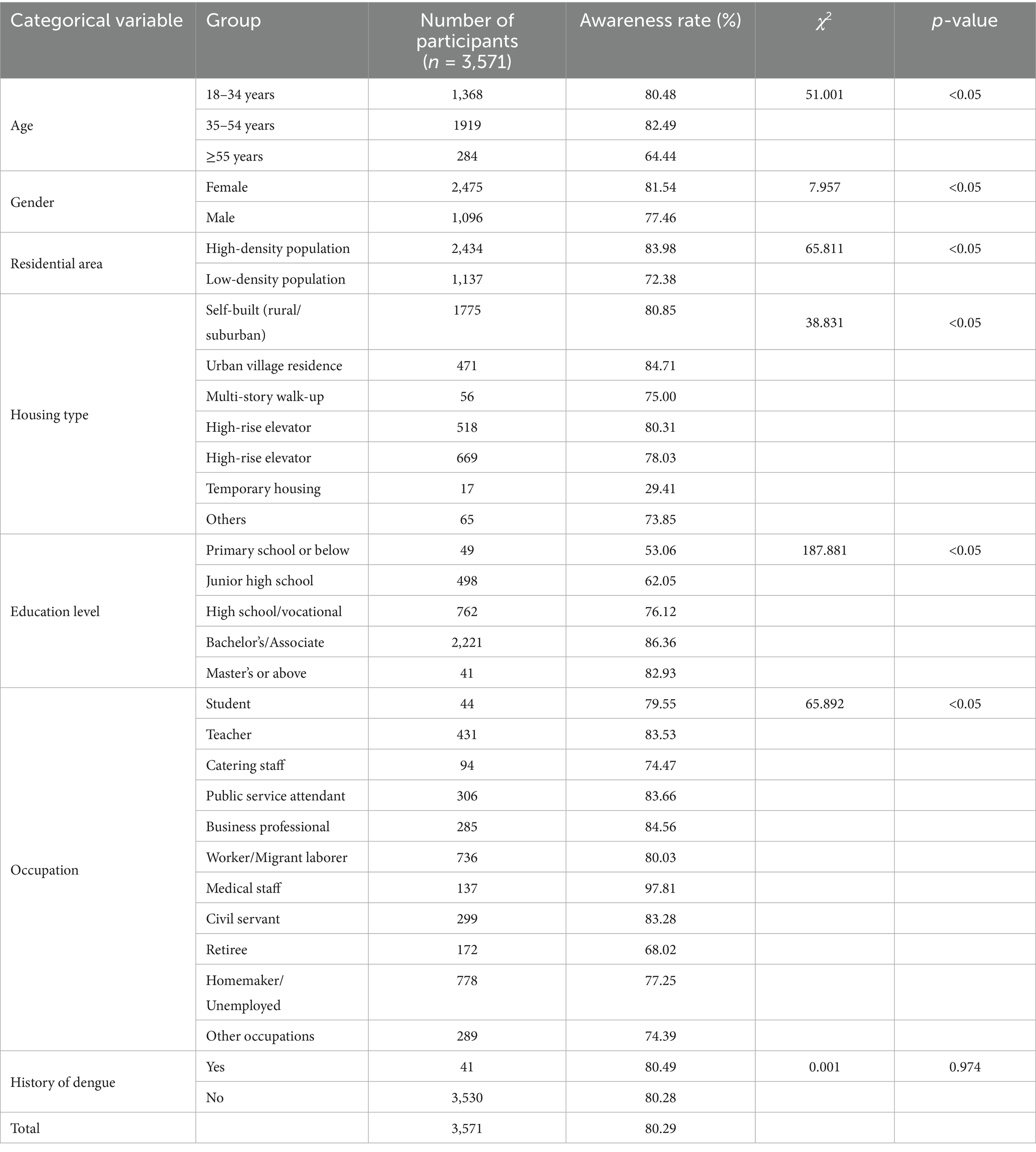
Table 1. Comparison of dengue knowledge awareness rate among different demographic groups.
3.1.2 Among the prevention motivation
Most residents held positive attitudes toward dengue severity, susceptibility, and prevention. However, significant differences were observed across education levels and occupations (p < 0.05). The results as shown in Table 2.
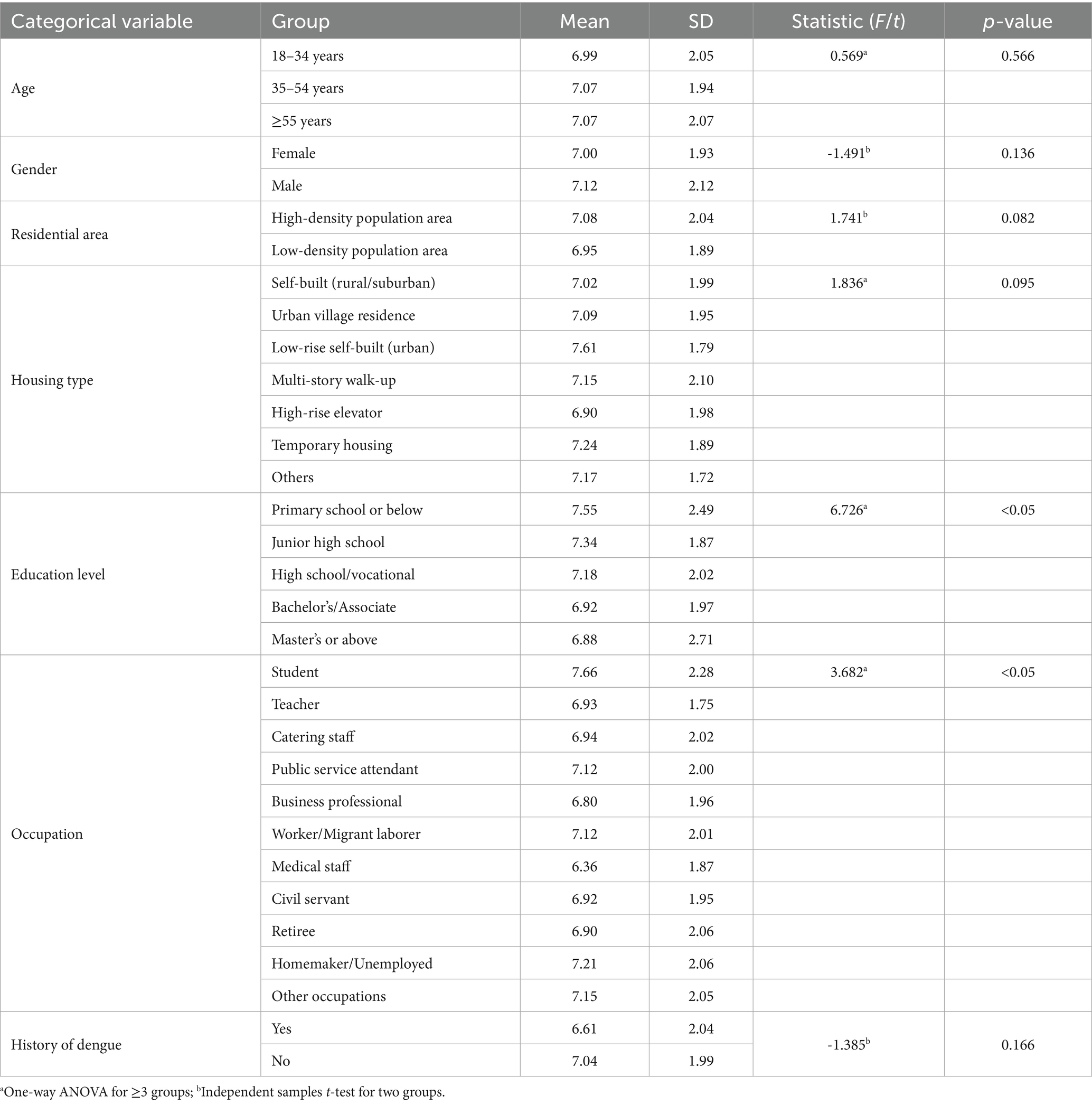
Table 2. Comparison of dengue prevention motivation among different population groups.
3.1.3 Among the prevention behavior
The average prevention behavior score was 15.05 ± 3.38. Significant differences were found across various demographic groups (p < 0.05). The results as shown in Table 3.
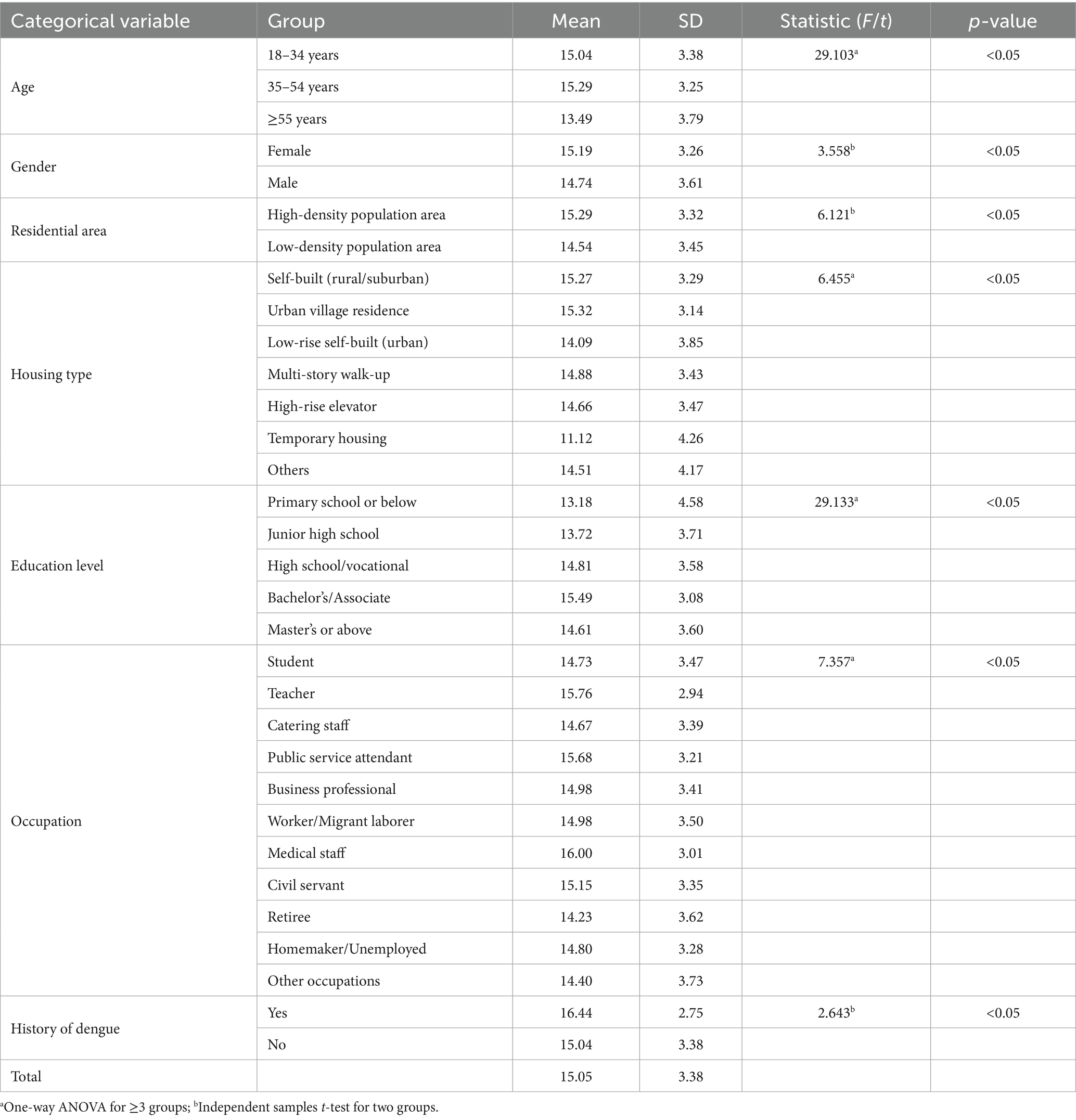
Table 3. Comparison of dengue prevention behavior scores among different population groups.
3.2 Intervention effectiveness
A total of 167 questionnaires were distributed online for the quasi-experimental phase. After excluding invalid responses, we obtained 150 valid questionnaires, achieving a response rate of 89.82%. The intervention group comprised 74 participants, while the control group included 76 participants. The two groups were largely comparable at baseline, with no statistically significant differences were observed in most demographic characteristics. The results as shown in Table 4.
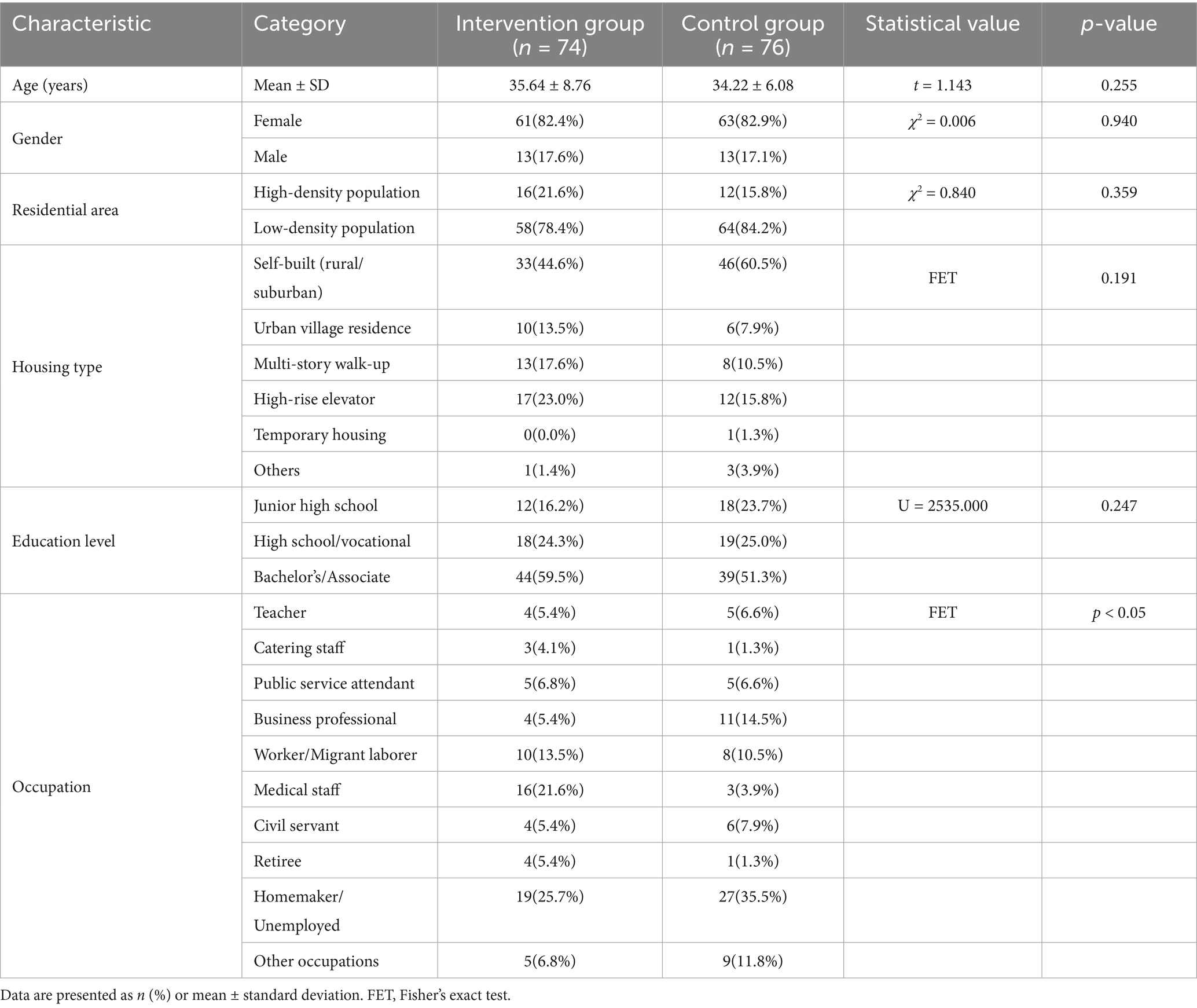
Table 4. Comparison of baseline characteristics between the intervention and control groups.
The intervention group showed a significant increase in knowledge scores post-intervention (p < 0.05), with scores rising from 5.84 ± 1.21 to 6.46 ± 0.95. The results as shown in Table 5.

Table 5. Comparison of knowledge dimension scores before and after intervention.
No significant differences were observed in prevention motivation scores between the two groups post-intervention (p > 0.05). No significant differences were observed in prevention behavior scores between the two groups post-intervention (p > 0.05). The results as shown in Tables 6, 7.

Table 6. Comparison of belief dimension scores before and after intervention.

Table 7. Comparison of behavior dimension scores before and after intervention.
4 Discussion
4.1 The factors influencing dengue fever prevention KAP
4.1.1 Knowledge levels and demographic variations
The baseline survey discovered that the overall knowledge level of dengue prevention among Guangzhou residents was relatively high (80.29%). Substantial variations exist in the awareness and knowledge of dengue fever among diverse geographical regions, with Europe exhibiting the highest levels of knowledge and Africa exhibiting the lowest (9). This suggests that the awareness level of dengue fever prevention and control knowledge among Guangzhou residents is relatively high, possibly because dengue outbreaks occur frequently in Guangdong Province, prompting the local government to place a greater emphasis on health education. This survey was conducted during a dengue outbreak in this area. In response to such outbreaks, local entities initiated emergency health education programs, thereby increasing the frequency of household health education for individuals residing in impacted regions. As a result, the respondents were able to acquire relevant knowledge relatively well within a certain period. There were, however, significant demographic disparities. Older residents (aged 55 and above), males, low-density population areas, retirees and less educated individuals had lower knowledge scores.
Similarly, the age group of 35–54 years exhibited the highest levels of awareness. This observation aligns with the findings of Kumari (23), who reported consistent age-related patterns in the Indian population. In contrast, adults aged 18–34 years demonstrated lower awareness of dengue, likely due to their familial and occupational responsibilities (24). Furthermore, their knowledge appears to be constrained by their level of educational attainment (25). Notably, individuals aged ≥55 years exhibited the lowest awareness rates, primarily due to barriers in accessing health information, including gaps in digital literacy.
Women exhibited higher levels of awareness than men. This observation is consistent with the conclusion that women generally possess superior knowledge and practices regarding mosquito control. Some studies have proposed that social roles, such as women’s increased responsibility for household sanitation, may contribute to this disparity in knowledge (26). Moreover, women represent a significant demographic on social media platforms such as WeChat, and their heightened interest in accessing health information relative to men may lead to increased engagement rates (27).
Epidemiological information, health literacy, and policy interventions are more easily disseminated in high-density areas, as dense surveillance systems and public facilities accelerate the diffusion of information (28). Television, radio, and social media were the main sources of information in the dengue study; media coverage was more concentrated in high-density areas (29, 30). In addition, high-density zones have better healthcare systems and community services, which allows for more efficient implementation of health promotion and social interventions, indirectly contributing to the reach of information (31). Urban villages in China represent high-risk zones for dengue transmission owing to inadequate governance and high population mobility. This highlights the critical need for targeted public health interventions in densely populated areas. Dengue fever disease in the main urban area of Guangzhou mainly manifests itself in the gradual spread of dengue fever disease from urban villages and old urban areas with poorer sanitary environment to the surrounding new urban areas (32). Due to government attention, residents in these high-risk areas are more likely to receive pertinent health information and preventive measures during periods of heightened dengue risk, thereby increasing awareness.
Higher education levels are associated with higher levels of dengue awareness, and literacy may be a key determinant of dengue awareness. This study shows that the level of health awareness is related to literacy; the higher the literacy level of the residents, the more attention they pay to health-related information, the more initiative they take in searching for health information, and the more diverse their sources of information. The lower the literacy level of residents, the more restricted the cognitive pathways of health education, resulting in a lower level of health awareness. Educational level independently influences health cognitive abilities, with highly literate residents being better at understanding and utilizing health information (33). The knowledge level of dengue fever also varied among occupational groups. The knowledge rate of medical personnel was significantly higher than that of other occupational groups (34), which is in line with the Ethiopian study and suggests that the resources of medical personnel should be fully utilized to disseminate dengue-related knowledge. In this study, we found that retired people had the lowest awareness of dengue fever, which may be related to their reliance on traditional media (TV/newspapers) but with low frequency of exposure and inadequate use of digital tools (35). To increase awareness and reduce the risk of infection, a combination of measures, such as strengthening health education campaigns, broadening access to information, and increasing social participation, are needed.
The demographic determinants of knowledge indicate the necessity for particularly targeting subgroups in health education campaigns. For example, older individuals may require special assistance and information to increase their knowledge and openness to prevention initiatives. Similarly, those with lower education levels may enjoy simpler messages emphasizing the short-term benefits of prevention efforts against dengue. Recognizing women’s high engagement in social media health dissemination presents significant public health opportunities. Leverage this to enhance health literacy and outcomes for women and families, maximizing social media’s public health value.
4.1.2 Motivation for dengue fever prevention
In this study, there were differences in the motivation to prevent dengue fever between people with different literacy levels and occupations, mainly in the form of higher scores of motivation to prevent in elementary school and below, and in occupations as students. Lower educated people pay more attention to prevention due to intuition, while higher educated people may underestimate the risk due to cognitive bias (36). Therefore, more in-depth and professional health education campaigns should be carried out for the more educated population, emphasizing the dangers of dengue fever and the importance of preventive measures, and improving their knowledge of dengue fever and their practical ability through scientific data and cases.
Motivation for dengue prevention also varied among different occupational groups. The motivation for prevention was significantly higher among students than among other occupational groups, which may be due to the fact that schools, as an important place for knowledge dissemination, develop students’ health awareness through classroom teaching and practical activities, leading to enhanced dengue prevention consciousness.
4.1.3 Dengue fever prevention behaviors
In this study, variations in dengue prevention behavior scores were observed among individuals of different ages, genders, residential areas, housing types, literacy levels, occupational categories, and prior experiences with dengue fever. Notably, lower levels of preventive behaviors were identified among residents aged 55 years and older, males, those residing in low-density populated areas, individuals living in temporary housing facilities, those with an education level of elementary school or below, retirees, and those who had not previously contracted dengue fever (37, 38). Compared to other age groups, individuals aged 55 years and above exhibited lower levels of dengue prevention behaviors, potentially attributable to factors such as historical environmental influences, a relative lack of health awareness within this demographic, and inadequate hygiene practices in their daily lives, which collectively contributed to their reduced mosquito prevention behaviors. Furthermore, the preventive behavior scores of females were higher than those of males, aligning with the findings of Ahmed (39).
4.2 Impact of mHealth intervention
Mobile text messaging is an effective, acceptable, and appropriate health intervention that can improve community dengue prevention practices (40). Although the SMS function is similar to WeChat’s information push, our research emphasizes community interaction, which is also a key mechanism for knowledge improvement. This study explored the impact of information, education, and communication interventions on dengue knowledge, supporting the effectiveness of mobile health interventions, with community interaction being central to knowledge improvement (41).
This study, based on the KAP model, demonstrated that WeChat mobile health interventions, through 2 months of targeted information delivery and community interaction, significantly improved community residents’ knowledge of dengue fever (p < 0.05). The mHealth intervention significantly improved knowledge in the intervention group, being evidence of effectiveness of mobile platforms in health information. The findings validate previous research that has proven mHealth interventions to successfully improve knowledge among different populations (42). This result is consistent with the effectiveness of mobile health education in the management of chronic diseases (15, 43). This study further confirms that combining multiple formats, such as popular science articles and graphics, video explanations, and expert consultations, can effectively overcome the communication bottlenecks of traditional health education (44, 45).
Behavior change theories suggest that interventions addressing both knowledge and motivational factors are needed to produce lasting behavior change. The KAP model operates on the assumption that increased knowledge directly leads to changes in attitudes and subsequent behavior (46, 47). In reality, behavioral change may be significantly moderated by external factors such as the social environment, cultural context, and economic conditions. Furthermore, the KAP model primarily focuses on individual-level determinants while overlooking the influence of macro-level factors, including policy, institutional frameworks, and the broader environment.
A study conducted in Cambodia revealed that despite participants demonstrating relatively high knowledge levels regarding dengue fever, their actual preventive behaviors did not show significant improvement (48). However, in this study, the effects of the intervention on belief restructuring and behavioral transformation were limited, which may have been influenced by factors such as the intervention strategies, characteristics of the target population, and the social environment. In a study conducted in Indonesia, although knowledge about the dengue vaccine among community members and healthcare providers improved, changes in beliefs and behaviors remained limited (49). Similarly, research in Malaysia indicates that despite a high level of knowledge, residents’ preventive behaviors have not significantly improved, suggesting that increased awareness does not directly translate into changes in behavior (50). This outcome highlights the complexity involved in effectively translating knowledge into practical application.
Further analysis shows that the interaction between sociocultural contexts and individual psychological mechanisms increases the difficulty of transforming knowledge into action. Traditional cognitive frameworks significantly influence the processing of new information at the level of beliefs. For instance, although some residents recognize that eliminating stagnant water can disrupt mosquito breeding, they are swayed by the stereotype that “dengue fever is a disease of tropical slums,” leading them to believe that their own living environment does not necessitate preventive measures. This cognitive bias closely resembles the phenomenon observed in Cambodia, where there is a misalignment between residents’ knowledge levels and their prevention practices (48).
In summary, although mobile health interventions based on the KAP model are effective in increasing knowledge levels, additional strategies are still needed to achieve comprehensive behavior change in terms of beliefs and actions.
4.3 Limitations and future directions
There are some limitations of this research. First, the non-randomized, self-selection group allocation may introduce selection bias. Second, the sample of internet and mobile phone users may limit generalizability to populations with lower digital literacy (51). Third, the two-month follow-up period prevents assessment of long-term behavior change. Finally, the use of basic statistical tests without controlling for potential confounding factors may affect the precision of the effect estimates.
Subsequent research should employ randomized controlled designs to mitigate selection bias, broaden sampling to include underrepresented groups, utilize advanced statistical models(e.g., ANCOVA) to control for confounders, and incorporate long-term follow-up to evaluate the sustainability of behavior changes. Additionally, collaboration with community-based organizations and local health authorities can enhance the effectiveness of mHealth interventions in real-world settings.
5 Conclusion
This study showed that an mHealth intervention grounded in the KAP model was successful in improving dengue prevention knowledge among Guangzhou’s urban dwellers. The intervention, though, failed to make a significant change in attitudes and behaviors, illustrating the intricacies of behavior change in public health.
To realize maximum impact of mHealth interventions, future strategies must address not just knowledge gaps but also emotional and behavioral determinants of health behavior. With personalized content, interactive learning, and community engagement, mHealth interventions can play a major role in reducing the burden of dengue and other vector-borne diseases in urban settings.
Continued study is needed to create these interventions and identify ways to facilitate long-term behavior changes, with research translating into ongoing preventive actions.
5.1 Innovation
This study provides baseline data for dengue prevention and control by identifying knowledge gaps and low-compliance populations. It also explores the integration of mHealth intervention with KAP theory, offering new insights for infectious disease prevention.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by the Ethics Committee of the Guangzhou Baiyun District Center for Disease Control and Prevention. Baseline survey: Before accessing the online survey, all potential participants were presented with an electronic informed consent form. Participants under 18 years of age were required to obtain parental or guardian approval before agreeing. mHealth Intervention Trial: Eligible adults were recruited exclusively from the baseline cohort.
Author contributions
ZH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. ZL: Data curation, Formal analysis, Investigation, Validation, Writing – original draft, Writing – review & editing. LL: Data curation, Formal analysis, Investigation, Writing – review & editing. SW: Formal analysis, Investigation, Writing – original draft. CC: Data curation, Formal analysis, Investigation, Writing – review & editing. NL: Data curation, Formal analysis, Investigation, Writing – review & editing. JL: Conceptualization, Funding acquisition, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Science and Technology Program of Guangzhou, China (Grant No. 2025A03J3687).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Bhatt, S, Gething, PW, Brady, OJ, Messina, JP, Farlow, AW, Moyes, CL, et al. The global distribution and burden of dengue. Nature. (2013) 496:504–7. doi: 10.1038/nature12060
3. World Health Organization (2025). Dengue and Severe Dengue. Available online at: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (Accessed September 15, 2024]
4. Powell, JR. Mosquito-borne human viral diseases: why Aedes aegypti? Am J Trop Med Hyg. (2018) 98:1563–5. doi: 10.4269/ajtmh.17-0866
5. Yang, X, Quam, MBM, Zhang, T, and Sang, S. Global burden for dengue and the evolving pattern in the past 30 years. J Travel Med. (2021) 28:taab146. doi: 10.1093/jtm/taab146
6. Gubler, DJ. Dengue, urbanization and globalization: the unholy trinity of the 21(st) century. Trop Med Health. (2011) 39:3–11. doi: 10.2149/tmh.2011-S05
7. Chen, LH, Marti, C, Diaz Perez, C, Jackson, BM, Simon, AM, and Lu, M. Epidemiology and burden of dengue fever in the United States: a systematic review. J Travel Med. (2023) 30:taad127. doi: 10.1093/jtm/taad127
8. Lr, B, S, D, and Pj, M. Is dengue vector control deficient in effectiveness or evidence? Systematic review and meta-analysis. PLoS Negl Trop Dis. (2016) 10:4551. doi: 10.1371/journal.pntd.0004551
9. Jahromi, AS, Jokar, M, Abdous, A, Sharifi, N, Abbasi, T, and Rahmanian, V. Global systematic review and meta-analysis of knowledge, attitudes, and practices towards dengue fever among the general population. Asian Pac J Trop Med. (2024) 17:191–207. doi: 10.4103/apjtm.apjtm_925_23
10. Chen, Z, Zhou, X, Jiang, L, Song, C, Wang, S, Zhao, H, et al. Knowledge, attitudes, and practices of family caregivers for patients with cerebral infarction toward home-based care. Front Public Health. (2024) 12:6423. doi: 10.3389/fpubh.2024.1436423
11. Reddy, PA, Saravanan, K, and Madhukar, A. To assess and compare the knowledge, attitude and practice of patients with diabetes in control and intervention groups. Biol Pharm Bull. (2023) 46:586–91. doi: 10.1248/bpb.b22-00699
12. Kalula, SZ, Blouws, T, Ramathebane, M, and Sayed, A-R. HIV and AIDS prevention: knowledge, attitudes, practices and health literacy of older persons in the Western cape and KwaZulu-Natal provinces, South Africa and in Lesotho. BMC Geriatr. (2023) 23:279. doi: 10.1186/s12877-023-04009-7
13. Zhou, Q, Qian, Y, Zhang, D, Xu, H, Yuan, B, Tian, W, et al. The effect of knowledge, attitude, and practice model-based health education on psychological well-being and self-efficacy of patients with concurrent cerebrovascular stenosis and coronary heart disease: a quasi-experimental study. Front Public Health. (2025) 12:4210. doi: 10.3389/fpubh.2024.1484210
14. Xiong, S, Ding, M, Li, P, Pan, S, Li, G, and He, W. A health education model based on knowledge, attitude, and practice used as adjunct therapy for metabolic syndrome complicated with acute pancreatitis: a case report. J Int Med Res. (2020) 48:4272. doi: 10.1177/0300060520924272
15. Marcolino, MS, Oliveira, JAQ, D’Agostino, M, Ribeiro, AL, Alkmim, MBM, and Novillo-Ortiz, D. The impact of mHealth interventions: systematic review of systematic reviews. JMIR Mhealth Uhealth. (2018) 6:e23. doi: 10.2196/mhealth.8873
16. Wood, CS, Thomas, MR, Budd, J, Mashamba-Thompson, TP, Herbst, K, Pillay, D, et al. Taking connected mobile-health diagnostics of infectious diseases to the field. Nature. (2019) 566:467–74. doi: 10.1038/s41586-019-0956-2
17. Nobis, S, Ebert, DD, Lehr, D, Smit, F, Buntrock, C, Berking, M, et al. Web-based intervention for depressive symptoms in adults with types 1 and 2 diabetes mellitus: a health economic evaluation. Br J Psychiatry. (2018) 212:199–206. doi: 10.1192/bjp.2018.10
18. Kang, M, Park, E, Cho, BH, and Lee, K-S. Recent patient health monitoring platforms incorporating internet of things-enabled smart devices. Int Neurourol J. (2018) 22:S76–82. doi: 10.5213/inj.1836144.072
19. Dugas, M, Gao, GG, and Agarwal, R. Unpacking mHealth interventions: a systematic review of behavior change techniques used in randomized controlled trials assessing mHealth effectiveness. Digit Health. (2020) 6:2055207620905411. doi: 10.1177/2055207620905411
20. Kanai, M, Miki, T, Sakoda, T, and Hagiwara, Y. The effect of combining mHealth and health professional-led intervention for improving health-related outcomes in chronic diseases: systematic review and Meta-analysis. Interact J Med Res. (2025) 14:e55835. doi: 10.2196/55835
21. Calabro, KS, Marani, SK, Le, TA, Khalil, GE, Tami-Maury, IM, and Prokhorov, AV. A pilot study for linking adolescent patients to an interactive tobacco prevention program. Health Serv Res Manag Epidemiol. (2017) 4:2333392817703208. doi: 10.1177/2333392817703208
22. Müssener, U, Thomas, K, Linderoth, C, Löf, M, Åsberg, K, Henriksson, P, et al. Development of an intervention targeting multiple health behaviors among high school students: participatory design study using heuristic evaluation and usability testing. JMIR Mhealth Uhealth. (2020) 8:e17999. doi: 10.2196/17999
23. Rathna, KG, Sri, GK, and Narendra, JB. A Compartive Study of Dengue Verses Malaria in Tertiary Care Hospital versus Government Hospital. World Journal of Current Medical and Pharmaceutical Research (2020) 2:21–29. doi: 10.37022/wjcmpr.2020.02012
24. Lu, P-J, Srivastav, A, Santibanez, TA, Christopher Stringer, M, Bostwick, M, Dever, JA, et al. Knowledge of influenza vaccination recommendation and early vaccination uptake during the 2015−16 season among adults aged ≥18years - United States. Vaccine. (2017) 35:4346–54. doi: 10.1016/j.vaccine.2017.06.074
25. Rahman, MS, Overgaard, HJ, Pientong, C, Mayxay, M, Ekalaksananan, T, Aromseree, S, et al. Knowledge, attitudes, and practices on climate change and dengue in Lao people’s Democratic Republic and Thailand. Environ Res. (2021) 193:110509. doi: 10.1016/j.envres.2020.110509
26. Duval, P, Aschan-Leygonie, C, and Valiente Moro, C. A review of knowledge, attitudes and practices regarding mosquitoes and mosquito-borne infectious diseases in nonendemic regions. Front Public Health. (2023) 11:1239874. doi: 10.3389/fpubh.2023.1239874
27. Ma, X, Lu, J, and Liu, W. Influencing factors on health information to improve public health literacy in the official WeChat account of Guangzhou CDC. Front Public Health. (2021) 9:657082. doi: 10.3389/fpubh.2021.657082
28. Chen, J, Guo, X, Pan, H, and Zhong, S. What determines city’s resilience against epidemic outbreak: evidence from China’s COVID−19 experience. Sustain Cities Soc. (2021) 70:102892. doi: 10.1016/j.scs.2021.102892
29. Basole, NT, Baliga, SS, and Mubashir, A. Knowledge regarding dengue disease among people in an urban area: a cross sectional study. Int J Community Med Public Health. (2018) 5:4498. doi: 10.18203/2394-6040.ijcmph20183999
30. Varma, P, Mohandas, A, Pattnaik, S, Balakrishna, N, and Kumar, KG. A community based study on dengue awareness and preventive practices among urban slum population in Hyderabad, South India. Int J Res Med Sci. (2021) 9:479. doi: 10.18203/2320-6012.ijrms20210427
31. Khavarian-Garmsir, AR, Sharifi, A, and Moradpour, N. Are high-density districts more vulnerable to the COVID-19 pandemic? Sustain Cities Soc. (2021) 70:102911. doi: 10.1016/j.scs.2021.102911
32. Qu, Y, Shi, X, Wang, Y, Li, R, Lu, L, and Liu, Q. Effects of socio-economic and environmental factors on the spatial heterogeneity of dengue fever investigated at a fine scale. Geospat Health. (2018) 13:13. doi: 10.4081/gh.2018.682
33. Long, Y, Jia, C, Luo, X, Sun, Y, Zuo, W, Wu, Y, et al. The impact of higher education on health literacy: a comparative study between urban and rural China. Sustainability. (2022) 14:12142. doi: 10.3390/su141912142
34. Mohammed Yusuf, A, and Abdurashid Ibrahim, N. Knowledge, attitude and practice towards dengue fever prevention and associated factors among public health sector health-care professionals: in Dire Dawa, eastern Ethiopia. Risk Manag Healthc Policy. (2019) 12:91–104. doi: 10.2147/RMHP.S195214
35. Siddiqui, TR, Ghazal, S, Bibi, S, Ahmed, W, and Sajjad, SF. Use of the health belief model for the assessment of public knowledge and household preventive practices in Karachi, Pakistan, a dengue-Endemic City. PLoS Negl Trop Dis. (2016) 10:e0005129. doi: 10.1371/journal.pntd.0005129
36. Siddique, AB, Omi, NT, Rasel, SM, Hoque, SSB, Rahman, N, Sarker, S, et al. Assessment of perceived dengue risk and prevention practices among youth in Bangladesh. Sci Rep. (2024) 14:3940. doi: 10.1038/s41598-024-54238-y
37. Elson, WH, Ortega, E, Kreutzberg-Martinez, M, Jacquerioz, F, Cabrera, LN, Oberhelman, RA, et al. Cross-sectional study of dengue-related knowledge, attitudes and practices in Villa El Salvador, Lima, Peru. BMJ Open. (2020) 10:e037408. doi: 10.1136/bmjopen-2020-037408
38. Rajapaksha, RMNU, Abeysena, C, and Balasuriya, A. Health seeking behaviours, dengue prevention behaviours and community capacity for sustainable dengue prevention in a highly dengue endemic area, Sri Lanka. BMC Public Health. (2023) 23:507. doi: 10.1186/s12889-023-15404-5
39. Ahmed, AE, Almarhabi, MA, Shami, MO, Alhazemi, AA, Alsharif, HM, Abu Hayyah, AE, et al. Knowledge, attitudes, and practices of the population in Jazan region, Saudi Arabia regarding dengue fever and its prevention measures: a community-based cross-sectional study. Int J Environ Res Public Health. (2022) 19:16812. doi: 10.3390/ijerph192416812
40. Bhattarai, AH, Sanjaya, GY, Khadka, A, Kumar, R, and Ahmad, RA. The addition of mobile SMS effectively improves dengue prevention practices in community: an implementation study in Nepal. BMC Health Serv Res. (2019) 19:699. doi: 10.1186/s12913-019-4541-z
41. Nivedita. Knowledge, attitude, behaviour and practices (KABP) of the community and resultant IEC leading to behaviour change about dengue in Jodhpur City, Rajasthan. J Vector Borne Dis. (2016) 53:279–82.
42. Lachyan, A, Zaki, RA, Banerjee, B, and Aghamohammadi, N. The effect of community-based intervention on dengue awareness and prevention among poor urban communities in Delhi, India. J Res Health Sci. (2023) 23:e00596. doi: 10.34172/jrhs.2023.131
43. Jiang, Q, Qin, G, and Zhang, L. Application effect of WeChat platform continuity of care model based on KAP theory on self-management of stroke patients with hypertension. J Clin Nurs Res. (2024) 8:303–10. doi: 10.26689/jcnr.v8i4.6841
44. Gupta, S, Goswami, B, and Madhu, SV. Effectiveness of video-based educational intervention on knowledge, attitude, and practice (KAP) of COVID-19 health care workers: lesson for future pandemic preparedness. ANAMS. (2023) 59:233–6. doi: 10.1055/s-0043-1772218
45. Ernawati, K, Azahra, H, Namira, A, Yuhen, L, Karuniawan, AG, Mecca, AA, et al. The utilization of mobile-based information technology in the management of dengue fever in the community year 2019-2020: systematic review. Int J Curr Res Rev. (2021) 13:94–105. doi: 10.31782/IJCRR.2021.131806
46. Manika, D, Papagiannidis, S, Bourlakis, M, and Clarke, RM. Drawing on subjective knowledge and information receptivity to examine an environmental sustainability policy: insights from the UK’S bag charge policy. Eur Manage Rev. (2021) 18:249–62. doi: 10.1111/emre.12453
47. Namdar Areshtanab, H, Vahidi, M, Hosseinzadeh, M, and Khani, Z. Developing the questionnaire of general population knowledge, attitudes and practices towards the COVID-19 outbreak. Nurs Open. (2024) 11:e2143. doi: 10.1002/nop2.2143
48. Kumaran, E, Doum, D, Keo, V, Sokha, L, Sam, B, Chan, V, et al. Dengue knowledge, attitudes and practices and their impact on community-based vector control in rural Cambodia. PLoS Negl Trop Dis. (2018) 12:e0006268. doi: 10.1371/journal.pntd.0006268
49. Wahab, A, Laksanawati, IS, Padmawati, RS, Mulyadi, AWE, Triadmajani, W, and Thobari, JA. Knowledge, attitude, and practice regarding dengue vaccine: a baseline study of community members and health providers in Indonesia. Clin Exp Pediatr. (2025) 68:228–37. doi: 10.3345/cep.2024.00962
50. Selvarajoo, S, Liew, JWK, Tan, W, Lim, XY, Refai, WF, Zaki, RA, et al. Knowledge, attitude and practice on dengue prevention and dengue seroprevalence in a dengue hotspot in Malaysia: a cross-sectional study. Sci Rep. (2020) 10:9534. doi: 10.1038/s41598-020-66212-5
Keywords: dengue, mobile health education, intervention, knowledge, attitude, practice (KAP)
Citation: Huang Z, Li Z, Li L, Wu S, Chen C, Li N and Lu J (2025) Analysis of factors influencing dengue prevention KAP among urban residents in Guangzhou and evaluation of mHealth intervention effects. Front. Public Health. 13:1686267. doi: 10.3389/fpubh.2025.1686267
Edited by:
Gary Low, NSW Health, AustraliaReviewed by:
Osamudiamen Omosumwen, Australian Catholic University, AustraliaMohammed Jabbar, Gulf Medical University, United Arab Emirates
Copyright © 2025 Huang, Li, Li, Wu, Chen, Li and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhihui Huang, YnJvc2V3b25nQDE2My5jb20=; Jianyun Lu, MjU4NTA2MjczQHFxLmNvbQ==