 Yaqin Li1,2†
Yaqin Li1,2† Chengyang Xie1†
Chengyang Xie1† Yan Yue1
Yan Yue1 Weihao Kong1
Weihao Kong1 Yuexuan Ma1
Yuexuan Ma1 Kefan Chen1
Kefan Chen1 Biyao Liu1
Biyao Liu1 Xiaoli Liao3
Xiaoli Liao3 Lingli Li1,4*
Lingli Li1,4*- 1West China Hospital, Sichuan University/West China School of Nursing, Sichuan University, Chengdu, China
- 2School of Nursing, The Hong Kong Polytechnic University, Hong Kong, Hong Kong SAR, China
- 3School of Nursing, The Sun Yat-sen University, Guangzhou, China
- 4Nursing Key Laboratory of Sichuan Province, Chengdu, China
Objective: Positive attitudes and strong confidence toward oral healthcare among nursing students are essential prerequisites for providing quality oral healthcare, which directly impacts the likelihood and effectiveness of their post-training care practices. However, no validated scale is currently available in China to measure nursing students’ attitudes toward oral healthcare and confidence. This study aims to adapt the original English version of the attitude and confidence with oral healthcare among nursing students (ACORN) scale into Chinese culture and assess its psychometric properties.
Methods: This study followed the Brislin Translation Model, including forward translation, back translation, and expert consultation (consultation of the differences between the original English version and the synthesized back-translated version of the ACORN scale with the original author, pilot testing, expert consultation, and bilingual testing). The formal experiment was conducted across eight universities offering bachelor’s nursing programs in China (Chengdu and Shenyang City), involving 536 nursing students who had completed oral healthcare courses. Item analysis, exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and reliability testing (internal consistency and test–retest reliability) were conducted. The data were divided into two equal sets using the random number table function in SPSS, one for EFA and the other for CFA.
Results: The EFA extracted three dimensions: attitudes toward oral care (8 items), confidence in oral care practices (4 items), and confidence in diagnosing oral diseases (10 items), with a cumulative variance contribution rate of 66.33%. The CFA confirmed the three-factor structure with excellent model fit indicators. The overall Cronbach’s alpha for the Chinese version of the ACORN scale was 0.95, with the three dimensions having values of Cronbach’s alphas of 0.92, 0.85, and 0.94, respectively. Twenty nursing students participated in a test–retest survey after a two-week interval, resulting in a test–retest value of 0.76.
Conclusion: The Chinese version of the ACORN scale exhibits strong reliability and validity performances and can be used to assess the oral care-related attitudes and confidence of nursing students in China.
1 Introduction
Oral health refers to the integrity and well-being status of the mouth, teeth, and orofacial structures that enable individuals to perform essential physiological functions (e.g., eating, breathing, and speaking) (1), as well as prompting psychosocial functions (e.g., decreasing discomfort/embarrassment in daily life and enhancing confidence in socialization) (1). To be specific, the oral cavity is a prominent facial feature that significantly shapes an individual’s self-image and self-perception through both its appearance and function (2). Oral diseases frequently impair dental aesthetics or cause bad breath (3, 4), which can lead to people’s dissatisfaction with their appearance and, consequently, diminish their self-esteem and social confidence (5–9). Moreover, many oral conditions involve functional limitations and chronic pain, substantially reducing patients’ quality of life by interfering with essential activities such as eating, long-term nutrition, and sleep (10–12). Periodontal disease and dental caries pose the most significant oral disease burden globally (13). Research indicates that periodontal disease affects over half of the world’s population, with severe cases accounting for 10.5 to 12.0% of this group (14). Similarly, dental caries in permanent teeth remains highly prevalent, affecting approximately 33.7 to 37.3% of people globally (15). Research consistently shows that poor oral hygiene is a primary cause of oral diseases (e.g., dental caries and periodontal disease). A systematic review and meta-analysis of 56 studies established that inadequate oral hygiene and plaque accumulation are significant drivers of periodontitis. The analysis found that the risk of developing periodontitis is two to five times higher in individuals with moderate-to-poor oral hygiene than in those with better hygiene (16). A survey of 250 preschool and primary school children linked irregular brushing, the practice of finger brushing, and a lack of parental supervision to a higher incidence of untreated cavities and their subsequent complications (17). The implications of these oral conditions extend beyond the mouth, as they were recognized as risk factors for serious systemic diseases. A joint symposium by the European Federation of Periodontology and the World Organization of Family Doctors (Europe) has established consensus: periodontitis is an independent risk factor for several systemic conditions, including cardiovascular disease, diabetes, chronic obstructive pulmonary disease, obstructive sleep apnea, and COVID-19 complications (18). Furthermore, one systematic review of studies in patients aged 65 and older found a link between periodontal disease and Alzheimer’s disease, suggesting that treating periodontal disease could be a potential strategy for Alzheimer’s prevention (19). Similarly, another systematic review of 50 studies indicated a positive correlation between periodontal disease and an increased risk of several cancers, including oral, lung, and pancreatic cancer (20).
Regular high-quality oral healthcare can not only prevent/decrease the prevalence of oral diseases, relieve patient suffering (21), improve their quality of life (22), and enhance their holistic well-being (23). Nurses/future nurses are the first-line oral health defenders of the whole society, including assessing oral status, providing regular oral health education, and delivering high-quality oral healthcare (24–26), as vital components included in their daily work routines in various clinical settings, including clinical wards (24, 25), communities (26), and long-term facilities (27). According to the Knowledge, Attitude/Belief, Practice (KAP) theory, human behavior change involves three consecutive processes: acquiring knowledge, forming beliefs/attitudes, and shaping behavior (28). Besides obtaining knowledge/skills, according to the Social Cognitive Theory (SCT) (29, 30), the quality of future nursing practice mostly results from the interplay among nursing students’ personal factors, including physiological aspects (e.g., race, gender, body height), psychological attributes (e.g., cognition, attitude, confidence), environmental factors (e.g., social supports/barriers, cultural background), and behavioral aspects (e.g., health behaviors, learning behaviors, and related outcome expectations). Under these two frameworks, it is not hard to see that among the above factors that can affect oral healthcare practices, psychological attributes (e.g., attitude, confidence) are one of the most modifiable factors at the individual level. Attitude refers to a psychological tendency that is expressed by evaluating a particular entity with some degree of favor or disfavor (31), influenced by individuals’ affection, behavioral tendency, and cognition level (e.g., knowledge/direct experience) (32). While confidence refers to the level of one’s belief in themselves, based on previous experience/evidence, that certain future events will occur as expected (33), influenced by personal expertise, authority, past experience/record, evidence/precedent, identity, belief, and shared group reinforcement (34). Studies (29, 30) indicate that confidence is more likely to be influenced by past success and accomplishments compared to attitude. In summary, attitude and confidence can shape nursing practitioners’/future nursing practitioners’ oral healthcare practices.
Nurses are frontline professionals who play a critical role in managing oral health in clinical, long-term care, and community settings. Their responsibilities include conducting routine oral assessments, providing specialized care for at-risk patients, and delivering essential oral health education (24, 27). Nursing students, who will be future oral care practitioners, are in their vital period of cultivating their attitudes and confidence towards oral healthcare, which may have a substantial impact on their future oral healthcare practices. Additionally, lack of positive attitude and confidence can lead to increased occurrences of missed oral healthcare in practice (35, 36), which may subsequently result in the development of oral diseases (37), social and psychological issues (38), and even severe diseases like cardiovascular disease, diabetes, chronic obstructive pulmonary disease, obstructive sleep apnea (18), Alzheimer’s disease (19) and cancers (20). Multiple studies (39–42) investigated oral healthcare-related attitudes among nursing students, and the levels of these attitudes are generally acceptable globally. For instance, a study (43) from Japan found that nursing students (N = 101) showed a medium level of attitudes towards assessing patients’ oral health, scoring 32.50 out of 40, in 2020. Three studies (44–46) conducted in 2012, 2018, and 2020 (N = 723/426/1672) in China showed that 53.8% of nursing students expressed interest in oral healthcare, and 65.3 and 79.7% of medical students held positive attitudes towards oral healthcare. Since all the above participants were students during their medical education period, and attitudes stem from knowledge and direct experience, regardless of the quality and quantity of oral healthcare education they received (47, 48), students’ attitudes towards oral healthcare are generally acceptable. However, a review of the literature reveals that the status of confidence in oral healthcare among nursing students is concerning (39–42). For instance, a study (49) conducted in 2016 (N = 31) in the United States found that nursing students had a low confidence level, with an average score of 13.13 out of 30 in providing pediatric oral healthcare, and 34% lacked confidence in oral diagnosis of dental caries. Another study (43) from Japan showed that nursing students (N = 101) had a confidence score of only 22.09 out of 45 in identifying the categories of oral diseases. Confidence is influenced by previous success and accomplishments (29, 30); therefore, it can be inferred that, with insufficient successful direct experience, as a result of most nursing students having limited opportunity (e.g., limited chance to do clinical practice) to gain substantial successful experiences, this affected their confidence substantially. Lastly, although there are some studies on nursing students’ attitudes and confidence in oral healthcare worldwide, a literature review conducted by the authors of this study found a great paucity of research in this field in China.
Regular measurement of nursing students’ status and associated factors in oral healthcare-related attitudes and confidence can not only prompt a comprehensive understanding of the current status but also provide clues for deploying specific interventions (50). Through a review of the literature, we found that most existing scales are not suitable for measuring nursing students’ attitudes and confidence towards oral healthcare (43, 51, 52) and have the following characteristics: (a) Attitudes and confidence are only sub-dimensions but not the primary focus of measurement. For instance, the Chinese version of the Short Form of Health Literacy Dental scale (51) was introduced into China in 2020 by Yan Wen, which primarily aims to assess oral health literacy among Chinese healthcare professionals. The Oral Health Examination Competency Questionnaire (43), developed by Haresaku in 2019, paid more attention to the oral measurement ability of nursing students, including the ability to read the oral check pictures(e.g., X-ray) and whether an oral referral will be needed; (b) however, it did not possess the necessary validity and reliability outcome indicators. For example, the scale (52) was optimized from the original Prenatal Oral Health Program (53) by Dsouza in 2017 to evaluate nursing students’ knowledge, attitudes, and behaviors regarding oral health services; however, it lacks a comprehensive validation process and validity/reliability outcome indicators. Furthermore, the Dental Coping Beliefs Scale, developed by Wardh in 2005 to evaluate nursing students’ oral health care priorities, also lacks a comprehensive validation process (54). To address these gaps, we found that a scale called the Attitudes and Confidence in Oral Healthcare for Nursing students (ACORN), developed by Jacqueline Rojo (50) among 244 nursing undergraduates in Australia in 2023, specifically designed to measure nursing students’ attitudes and confidence towards oral healthcare. This scale includes two dimensions (attitudes and confidence) and 24 items, with an Item-Level Content Validity Index (I-CVI) of 0.80, a Scale-Level Content Validity Index (S-CVI) of 0.80, an overall Cronbach’s alpha of 0.94, Cronbach’s alpha of the attitude sub-scale of 0.92, and Cronbach’s alpha of the confidence sub-scale of 0.96. All indicators suggest that the ACORN has excellent reliability. It also has strong validity, as indicated by confirmatory factor analysis (CFA), χ2 = 327.28, df = 215, p < 0.01, GFI = 0.83, TLI = 0.95, CFI = 0.96, RMSEA = 0.06, which fully supports the two-dimensional theoretical model.
Therefore, this study aims to adapt the original ACORN scale to Chinese culture to provide a validated measurement tool for evaluating the attitudes and confidence toward oral healthcare among Chinese nursing students, thereby promoting the provision of high-quality oral healthcare in future clinical practice.
2 Materials and methods
2.1 Study design
A cross-sectional survey was conducted in this study.
2.2 Settings
Convenience sampling was used to recruit universities that offer nursing programs for bachelor’s degrees, while cluster and convenience sampling were used to recruit nursing students in these universities. In this study, Chengdu city (Southwest China) and Shenyang city (Northeast China) were chosen based on the geographic locations of the research team members. The data collection was conducted from March 2023 to April 2023. A total of 14 universities offering bachelor’s degree programs in nursing (9 in Chengdu and 5 in Shenyang) were identified through the China Higher Education Student Information Network (CHSI). The research team contacted representatives from 8 of these schools (5 in Chengdu and 3 in Shenyang; more details are in Supplementary Table S1) using a convenience sampling method to explain the study’s purpose, methodology, and contents and to seek their participation and informed consent.
Currently, China’s oral health education system for nurses remains underdeveloped. It is characterized by a lack of standardized curricula, significant regional disparities in teaching materials, and an absence of assessments (55–58). This is compounded by the fact that only 14 institutions nationwide offer specialized oral healthcare programs, with enrollment numbers failing to meet clinical demand (57). Consequently, most dental nurses come from general nursing backgrounds and often exhibit deficits in specialized knowledge and practical skills (55–58). Given the context above and based on a preliminary survey by researchers in this study of the participating universities’ oral health education curricula, this study operationally defines “oral health education” as follows: students must have begun systematic study in both Basic Nursing and Adult Nursing courses, be in their sophomore year or above, and have started oral clinical practicums.
2.3 Sample size estimation
The sample size requirement for a cross-sectional survey of the scale is 5–10 times the total number of scale entries (59). In this study, we calculated the sample size by multiplying the number of entries by 10 to 20 times due to both the Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) (60), each of which requires 5 to 10 times the number of total entries, and the total is 10 to 20 times. Additionally, accounting for a 20% attrition rate, the estimated sample size ranged from 288 to 576 participants.
2.4 Data collection procedures
Upon receiving approval and informed consent from the representatives of the universities, the researchers tailored data collection plans based on the unique circumstances of each region. In Chengdu, five schools opted for on-site data collection using electronic questionnaires. The research team explained the study’s details to potential participants in classrooms and invited them to scan a QR code to access the e-questionnaire. However, in Shenyang, three to four questionnaire distributors were assigned to each university to handle the one-on-one distribution of the electronic questionnaires to nursing students; data collection in all three Shenyang schools was conducted online. The procedure is as follows: the distributors added potential participants on WeChat/QICQ apps, explained the study’s details, and shared the QR code with eligible students to complete the questionnaire. Students were required to scan the QR code to access the e-questionnaire, which also included an informed consent form. The distributors regularly updated the research team via WeChat to ensure data authenticity.
The questionnaires were hosted on WenJuan Xing,1 a widely used online survey platform in China. The platform automatically recorded and stored the data. Each e-questionnaire includes an informed consent form, a separate guidance page explaining the study’s purpose, completion instructions, and estimated time required. The survey officially began only after participants indicated their informed consent. To ensure data integrity, the electronic survey was designed to be submitted only after 100% completion, and each device can submit only once. Only questionnaires completed within a reasonable time frame (at least 120 s) were considered valid. Invalid responses, such as those completed too quickly, those that selected the same option throughout, or those that followed a predictable pattern (e.g., “11111” or “12345”), were excluded from the final dataset.
2.5 Inclusion and exclusion criteria for the participants and their questionnaires
Inclusion criteria: (a) full-time nursing students (studying their bachelor’s degree in these universities) who have received oral healthcare education before; (b) ability to read and complete the questionnaire; (c) informed consent provided for voluntary participation.
Exclusion criteria: (a) questionnaires completed in less than 120 s; (b) responses that show a consistent pattern (e.g., selecting the same option repeatedly or following a predictable sequence like 11111 or 12345).
2.6 Instruments
2.6.1 Social demographic information
This questionnaire enquires participants’ social demographic information, including participants’ gender, age, school, and grade, and was designed by the research team after a review of the literature (43, 50, 52, 61–67).
2.6.2 The Attitudes and Confidence in Oral Healthcare for Nursing students (ACORN) scale
The ACORN scale, developed by Jacqueline Rojo in 2023 (50) consists of two dimensions, attitude and confidence, covering a total of 24 items. Each item was rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). The scale demonstrated favorable validity and reliability with an Item-Level Content Validity Index (I-CVI) > 0.78, a Scale-Level Content Validity Index (S-CVI) = 0.8, an overall Cronbach’s alpha of 0.94, the attitude subscale’s Cronbach’s alpha of 0.92, and the confidence subscale’s Cronbach’s alpha of 0.96. EFA extracted two factors (attitude and confidence), and CFA yielded χ2 of 327.28, df of 215, p < 0.01, GFI of 0.83, TLI of 0.95, CFI of 0.96, and RMSEA of 0.06 (68).
2.7 Translation and cultural adaptation procedures
After contacting the original scale author via email, the researchers obtained authorization to translate/introduce the original English version of the ACORN scale into Chinese culture on October 3, 2023, as illustrated in Supplementary Figure S1. The translation and cultural adaptation procedure in this study totally followed the translation, adaptation, and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline, including forward translation, back translation, and expert consultation (consultation of the differences between the original English version and the synthesized back-translated version of the ACORN scale with the original author, pilot testing, expert consultation, and bilingual testing) (69).
2.7.1 Forward translation
Two master’s subjects in nursing (LZ) and Chinese language and literature (QG) independently; both were proficient in English and translated the ACORN scale from English to Chinese independently. A third nursing master (XXX), who is also proficient in English, along with the researcher (CX), compared the two translated drafts with the original version. After discussion among the researchers (CX, YL, LL) and three translators, a consensus was reached, and a synthesized Chinese version of ACORN was formed (XXX, CX); more details are in Table S2.
2.7.2 Back translation
Two master’s subjects in nursing (XLF) and Chinese language and literature (YLY) separately, both were proficient in English but had no prior knowledge of the original scale. They independently translated the synthesized Chinese version of ACORN into English. An expert committee composed of the researcher (CX), scale construction expert (YL, LL), and all translators (QG, LZ, XXX, YLY, and XLF) compared the two back-translated drafts. They discussed differences between the back-translated version and the original scale. After a consensus was reached, the synthesized back-translated version of the ACORN (CX) scale was finalized. More details are listed in Table S3.
2.7.3 Expert consultation (cultural adaptation)
2.7.3.1 Consultation of the differences between the original English version and the synthesized back-translated version of the ACORN scale with the original author
The synthesized back-translated ACORN (CX) scale was sent to the original English version author (Jacqueline Rojo) via email to clarify ambiguities discussed by the expert committee and differences between the original English version and the synthesized back-translated version of the ACORN scale. After adjustments, the Chinese version of the ACORN (CX) scale was developed, with additional details shown in Supplementary Figure S2 and Supplementary Table S4.
2.7.3.2 Pilot testing
Methodological literature outlines a standard procedure for scale translation and cross-cultural adaptation, which includes forward translation, synthesis of the forward translations, back translation, synthesis of the back translations, pilot testing, bilingual testing, and formal research (69). Pilot testing involves a preliminary study with 10–40 participants from the target population to assess the clarity and comprehensibility of the scale’s instructions, items, and response format (69). Additionally, the engagement of an expert consultation throughout this process is highly recommended to evaluate and ensure the conceptual and content equivalence of all items (69). Twenty nursing students who met the inclusion/exclusion criteria of the formal survey and provided informed consent were invited through convenience sampling to participate in pilot testing. We assessed whether each item in the scale was clear and easy to understand by using the adjusted Chinese version of ACORN, along with two options, “YES” or “NO” for response selection, and an extra blank line for feedback on whether there will be any other suggestions, at the end of each item. Items would be revised unless 100% of respondents selected “Yes”. Based on this criterion, the results indicated that students understood most items well. While five items fell below the 100% threshold and were revised, the remaining 19 out of 24 items achieved a perfect understanding rate. Additionally, based on their suggestions, we added explanations for certain terminologies to the ACORN (CX) scale to improve readability, including dental referrals, plaque, tartar, receding gums, and worn-down teeth. Demographic information for the pilot testing participants is available in Supplementary Table S5. The items of the adjusted Chinese version ACORN, along with participants’ corresponding ‘Yes’ response rates, participants’ feedback, and our subsequent revisions, are provided in Supplementary Table S6.
All 20 participants, who were from the eight universities included in this study and who met the identical inclusion and exclusion criteria used in both the pilot and formal studies, voluntarily continued the formal survey.
2.7.3.3 Expert consultation
Ten experts were invited for the Delphi method (70) (including six experts from clinical nursing, three from nursing education, and one from nursing research). They were invited to assess the importance of items, the relevance of content, and the clarity of language expression. The Chinese version of the ACORN scale was further revised based on all this feedback. Some explanations for certain terminologies were added to the ACORN (CX) scale-pressure area care, healthy teeth, and oral pain, as well as some other revisions were made, including added word “recommend” before “dental referrals” and changed “lip ulcers” to “oral ulcer.” More details, including experts’ demographic information and the revised scale, are presented in Supplementary Tables S7, S8.
2.7.3.4 Bilingual testing
To establish standard equivalence and further validate the conceptual, semantic, content, and structural equivalence of a scale, a bilingual test was conducted (69). This involves a pilot study with a minimum of five bilingual participants (69). Bilingual testing derives its value from the unique bicultural perspective of bilingual individuals, who act as “conceptual proofreaders” and “cultural detectors” (69). Their direct comparison of language versions reveals deep-seated issues-such as conceptual nuances, cultural misalignments, and awkward idioms-that professional translation and monolingual testing typically miss. This is critical for establishing true conceptual and cultural equivalence, thus ensuring the validity and comparability of cross-cultural research. Ten nursing students who met the inclusion criteria of this study and were proficient in English (there was no overlap between participants in the pilot testing and the bilingual testing) were invited to complete a questionnaire comprising both the original English ACORN scale and a randomly shuffled Chinese version of the ACORN scale to measure the equivalence between the two scales. Participants in the bilingual testing voluntarily participated in the subsequent formal survey because they met the inclusion and exclusion criteria of this study and were also from the eight universities included in this study. Demographic information of participants, the questionnaire applied, and statistical results from the bilingual assessment are shown in Supplementary Tables S9–S11, respectively.
2.8 Ethical consideration
This study was approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University (Reference Number: 2024–279). This study received data collection permissions from all included universities. Informed consent was obtained from all participants in this study. All procedures conducted in this study were in accordance with the Declaration of Helsinki (71).
2.9 Data analysis methods
2.9.1 Item analysis
This study employs both the critical ratio (CR) method and the coefficient correlation method to assess the suitability and reliability of scale items. In the CR method, the total scale scores are ordered from lowest to highest, with the lowest 27% forming the low-score group and the highest 27% forming the high-score group. A t-test was performed on the same item for the high- and low-score groups. If the difference is not statistically significant (p > 0.05, the tests involving p-values throughout this study were all two-tailed) or the CR is less than 3.00, the item was removed. In the correlation coefficient method, which examines the correlation between each item’s score and the overall scale score. Items with a correlation coefficient of r ≥ 0.40 (p < 0.05) were retained.
2.9.2 Content validity
In this study, ten experts were involved in the cultural adaptation process, assessing the content validity of the scale. Experts were requested to rate each item’s relevance to oral healthcare attitudes and confidence by using a Likert scale ranging from “not important” to “very important” (score from 1 to 4). The I-CVI and the S-CVI were calculated. Both of the I-CVI and S-CVI ≥ 0.80 will be taken as good content validity of the scale (72).
2.9.3 Structural validity—EFA
This study employed both EFA and CFA to assess the structural validity of the scale. Employing the random number table method in SPSS 26.0, we split the data into two independent, equal-sized subsamples (EFA: N = 268; CFA: N = 268). This rigorous partitioning ensures that the cases in each set are mutually exclusive, thereby eliminating information leakage and upholding the validity of the statistical tests derived from the CFA.
Before conducting the EFA, the suitability of the data for analysis was evaluated using the Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity. EFA was deemed appropriate if the KMO value exceeded 0.50 and Bartlett’s test produced a p-value less than 0.05 (73). The EFA was conducted using principal component analysis and varimax orthogonal rotation, extracting common factors with eigenvalues of at least 1.000. Structural validity was considered strong if item factor loadings on their respective factors exceeded 0.50, no items showed multiple loadings, and the cumulative variance contribution of the scale was above 50% (74).
2.9.4 Reliability check
Internal consistency reliability was used to assess the internal consistency of each domain and the whole scale. The test–retest reliability coefficient was used to examine the stability of the scale.
2.9.4.1 Cronbach’s alpha coefficient
Internal consistency refers to the correlation between items, and a high correlation among items in the same dimension indicates high internal consistency (75). It is evaluated by calculating Cronbach’s alpha coefficient of the dimension/whole scale. If Cronbach’s alpha coefficient is >0.70, it means good internal consistency reliability of the scale (76).
2.9.4.2 Test–retest reliability
Test–retest reliability refers to administering the same measurement tool to the same group at different time points to evaluate the consistency and stability of the results/scale (77). In this study, we tested test–retest reliability using the same scale within the same subjects after a 2-week interval. A random sampling of 20 nursing students in one of the universities in Chengdu was re-surveyed to assess the scale’s test–retest reliability. The correlation coefficient of the scores obtained from these two surveys was calculated by the Pearson product–moment correlation coefficient which ranges from 0 to 1, and the higher of the results indicates the better consistency between two tests, as well as good stability of the scale. The test–retest reliability coefficient value greater than 0.70 will be considered satisfactory and excellent (78).
2.9.5 Structural validity—CFA
Following EFA, CFA was performed to validate the scale’s structure. A good model fit was indicated if the chi-square/degree of freedom ratio (χ2/df) was less than 5, the CFI and IFI were 0.90 or higher (79), and the RMSEA was below 0.08 (80).
2.10 Statistical analysis
In this study, SPSS 26.0 and AMOS 26.0 were applied for statistical analysis. Descriptive statistical analysis was applied by using mean ± standard deviation (x̄ ± s), frequency, and percentages (%) to present the results. In item analysis, we employed the CR method and the correlation coefficient method, and content validity and structural validity were assessed. The reliability test involved internal consistency and the test–retest reliability coefficient method. Differences were considered statistically significant if p < 0.05.
3 Results
This study included eight universities: five from Chengdu and three from Shenyang. A total of 550 questionnaires were distributed, except 14 questionnaires were excluded as their completion was within 120 s. Five hundred thirty-six questionnaires were included with a retrieval rate of 97.45%, of which 298 participants (55.60%) were from Chengdu, and 238 (44.40%) were from Shenyang. Participants’ age ranged from 19 to 24 years, with a mean age of (21.17 ± 1.16) years. Most participants were female (N = 389, 72.57%), comprising sophomores (25.00%), juniors (34.51%), and seniors (40.49%). More details are presented in Supplementary Table S12.
3.1 Item analysis
Item analysis was conducted to screen for potentially irrelevant items. Using the CR method, a significant difference was found between the top 27% of scorers (156.80 ± 5.81; min total score = 149, max total score = 168) and the bottom 27% (105.88 ± 15.37; min = 24, max = 123). All items demonstrated high discriminant validity, with CR values ranging from 13.12 to 23.14. An independent-samples t-test confirmed that the score differences between these groups were statistically significant (p < 0.05). Furthermore, all items showed strong positive correlations with the total scale score (r = 0.56 to 0.78, p < 0.05), indicating excellent homogeneity for both the entire scale and each item. Based on these robust results, all items were retained. Detailed results are presented in Supplementary Table S13.
3.2 Content validity-expert evaluation
The Item-Level Content Validity Index of 24 items ranges from 0.80 to 1.00, and the Scale-Level Content Validity Index was 0.94, indicating a favorable content validity of the Chinese version (72, 81). More details, including the demographics of the expert involved, are in Supplementary Tables S7,S8.
3.3 Exploratory factor analysis (EFA)
The results indicate that the Kaiser–Meyer–Olkin (KMO) index was 0.954, and Bartlett’s test of sphericity showed statistical significance (p < 0.001), confirming the applicability of factor analysis (74). The results of EFA demonstrated that the optimal factor structure comprises three factors with a total of 22 items and a cumulative variance contribution rate of 66.33%. The first factor, consisting of 8 items (Q1-Q8), explains 25.10% of the variance; the second factor, with four items (Q9-Q12), explains 12.62% of the variance; and the third factor, including 10 items (Q13-Q22), explains 28.61% of the variance. The items in each dimension are shown in Table 1.
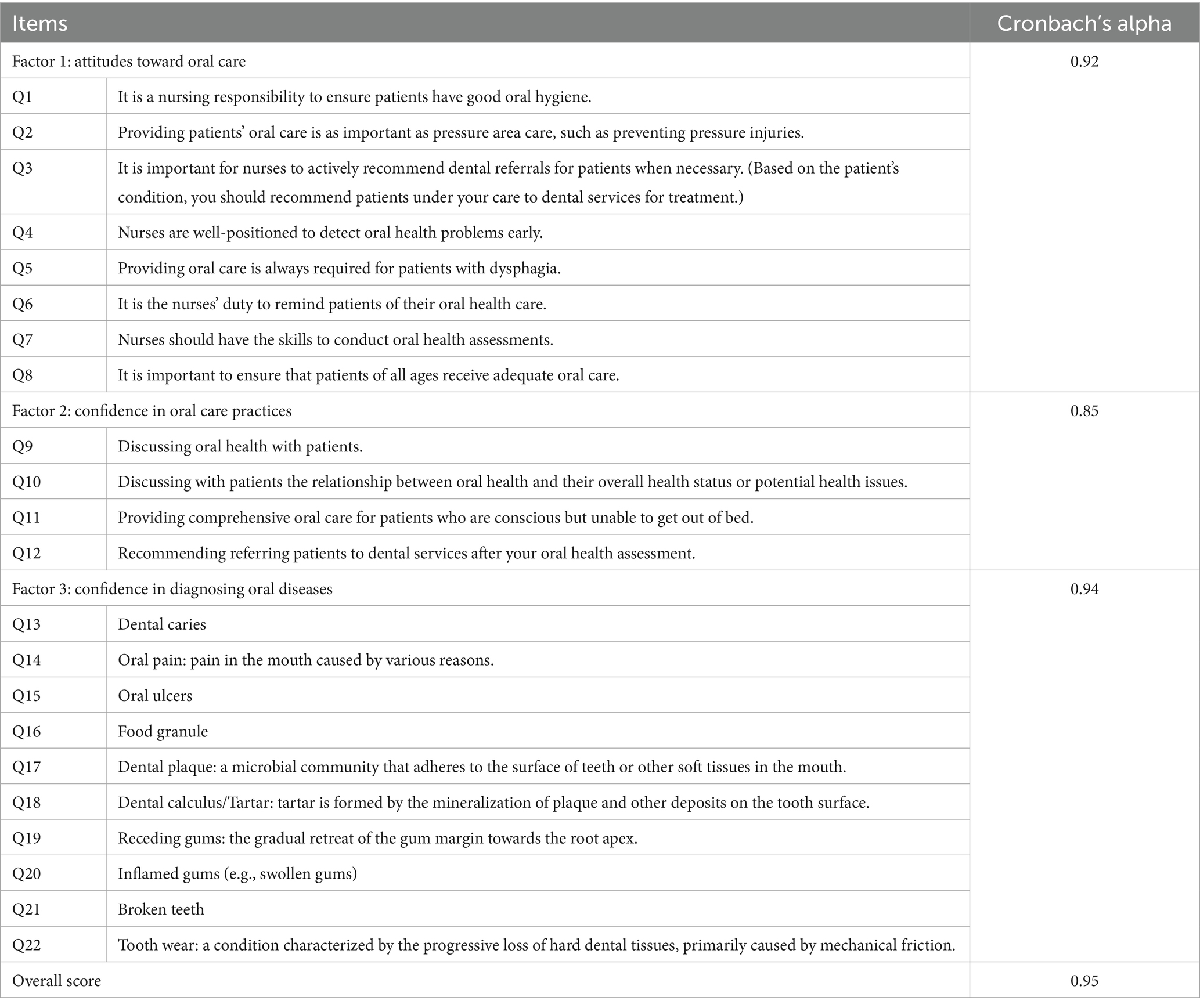
Table 1. Cronbach’s alpha coefficients for the Chinese version of the ACORN scale.
3.4 Confirmatory factor analysis (CFA)
The CFA results demonstrated a satisfactory model fit (82), with χ2/df = 1.97, GFI = 0.88, CFI = 0.95, NFI = 0.90, TLI = 0.94, and RMSEA = 0.06. Additionally, the model structure has standardized regression weights ranging from 0.67 to 0.82, as depicted in Figure 1.
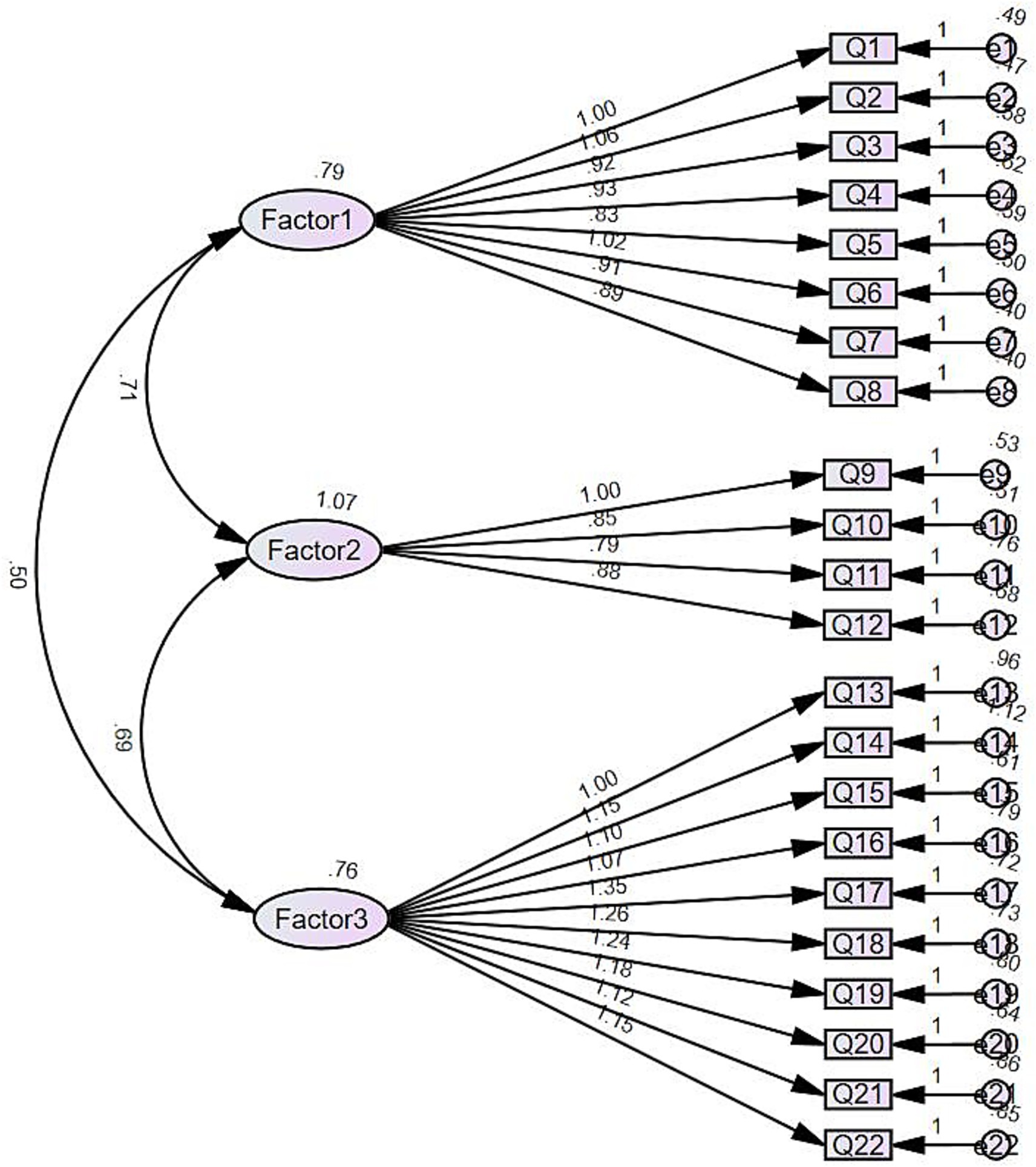
Figure 1. Path diagram from CFA.
3.5 Reliability
The Cronbach’s alpha coefficient of the whole Chinese version scale was 0.95, with 0.92 for the attitude subscale, 0.85 for confidence in performing, and 0.94 for confidence in identifying, which were all excellent (83), as presented in Table 1. Additionally, the test–retest reliability of the Chinese version scale was satisfactory and excellent (78), as indicated by an intraclass correlation coefficient value of 0.76.
4 Discussion
Driven by international advocacy, recently, many countries, including the United States, Turkey, and China, are progressively integrating oral health education into undergraduate nursing curricula (41, 42, 84–86). However, due to the delayed recognition of the importance of oral healthcare, there is a substantial lack of awareness among nursing students, affecting their attitudes and confidence in oral healthcare. Additionally, upon a review of the literature (43, 51, 52), we found that, currently, there is no available, not even to say validated scale, to help in measurement of Chinese nursing students’ attitude and confidence related to oral healthcare. The Attitude and Confidence with Oral Healthcare among Nursing Students (ACORN) scale, with moderate item quantity and operational feasibility, enables dynamic and real-time measurements of Chinese nursing students’ attitude and confidence related to oral healthcare, which can provide related stakeholders with insights into students’ status of their attitude/confidence related to oral healthcare, and also empower nursing students themselves to shape their future practices in oral healthcare. Thus, in this study, we introduced and tested the psychometric properties of this novel and practical attitude and confidence measurement scale for nursing students in Chinese culture.
In this study, a total of 8 universities in Chengdu city and Shenyang city were surveyed separately, with 536 effective questionnaires (97.5%) retrieved. The sample size in this study was not only sufficient for structural validity checking, for both the Exploratory factor analysis (EFA) and Confirmatory Factor Analysis (CFA), comparatively speaking, it had twice sampled as much as in the original English version (N = 244) and a higher retrieval rate than the original English version study (94.20%) (50), which makes the results from this study more robust and trustful. Similarly with the original English version study, most nursing students in this study were also female (85.30%, in this study, the proportion was 72.57%), and young students (mean age was 27.83 and 28.67 in group 1 and group 2, separately, in the original English version, while 21.17 ± 1.16 years in this study).
According to the Knowledge, Attitude/Belief, Practice (KAP) theory, human behavior change encompasses three sequential processes: acquiring knowledge, forming beliefs and attitudes, and shaping behavior (28). While the Social Cognitive Theory (SCT) emphasizes that an individual’s actions are the result of multiple interacting factors, including personal, environmental, and behavioral factors (29, 30). It is evident that personal factors, particularly psychological attributes, play a critical role in the formation and modification of behavior and are the easiest to change. Among these personal factors, attitudes and confidence are especially important, as they directly influence nursing students’ behavior and actions according to the theories mentioned above, and even their future oral healthcare practices. This study suggests that there may be a substantial link between a person’s attitude, self-confidence, and their resulting behavior and actions. However, a literature review conducted by the authors of this study indicates a lack of a theoretical framework explaining how an individual’s attitude and self-confidence contribute to their behavior and ultimately lead to action. We can make a bold assumption that attitude and self-confidence may directly influence behavior, which in turn leads to specific actions.
In this study, 536 questionnaires were randomly divided into two equal groups using SPSS’s random number table function. On the one hand, one group underwent an EFA to investigate the structure of the 22 items across the three dimensions of the Chinese version of ACORN (attitudes toward oral care, confidence in oral care practices, and confidence in diagnosing oral diseases). The EFA revealed that the three factors of the ACORN scale accounted for a cumulative variance contribution rate of 66.33%, indicating a strong contribution. There is a substantial distinction between the original English version scale with the Chinese version scale is, the split of the previously “confidence” dimension in the original English version, into “confidence in oral care practices,” and “confidence in diagnosing oral diseases” dimensions in the Chinese version ACORN. In the original scale, there are only two dimensions, attitude and confidence, with the confidence dimension treated as a single overarching category. However, the scale’s format separates the confidence dimension into two modules, “confidence in oral care practices” and “confidence in diagnosing oral diseases.” After cultural adaptation into China, this division into modules” confidence in oral care practices” and “confidence in diagnosing oral diseases,” was maintained in the Chinese context, which substantially enhances the understanding of confidence and its practical categorization and application, emphasizing the distinct aspects of confidence demonstrated by nursing students in oral healthcare practice. A more detailed classification helps enriching the details of the Chinese version ACORN scale, and authors believe that this classification can help clarify the sources of nursing students’ confidence when facing clinical tasks. Additionally, it may also be related to the fact that nursing students have less knowledge/practice/experience about the diagnosis of oral diseases (87), leading to the large difference between these two dimensions. On the other hand, the second group was used for CFA, which demonstrated a good model fit. In summary, the Chinese version of ACORN demonstrated excellent structural validity.
Also, the reliability performance of the Chinese version of ACORN is excellent. In this study, the Item-Level Content Validity Index ranges from 0.80 ~ 1.00 and the value of Scale-Level Content Validity Index was 0.94, both were greater than 0.80 (72), indicating the authenticity and accuracy of the content expressed in the Chinese version of the ACORN scale. Additionally, this study utilized Cronbach’s alpha coefficient to evaluate the internal consistency reliability of the Chinese version of the ACORN scale (75). The Cronbach’s alpha coefficients for the overall scale was 0.95, and for each dimension were 0.92, 0.85, and 0.94separately, which all greater than 0.70 (76), demonstrating a good internal consistency of the Chinese ACORN scale. Furthermore, the test–retest reliability coefficient was 0.76, which is greater than 0.70 (78) and reflects the scale’s good stability.
Convenience sampling was used in this study to include nursing universities that offer a bachelor’s degree in nursing; however, these universities were located only in the northeast (Shenyang city) and southwest (Chengdu city) regions of China, which may have led to an inadequate representation of the sample. Future research will be needed to validate and assess the psychological properties of the Chinese version of the ACORN scale in other regions of China before its widespread use in this country.
5 Conclusion
The Chinese version of the ACORN scale was translated, back-translated, and culturally adapted in strict accordance with Brislin’s translation process. The Chinese version scale has demonstrated excellent reliability and validity, serving as a specific and reliable tool for measuring nursing students’ attitudes and confidence in oral healthcare. However, it is important to acknowledge that this study’s reliance on convenience and cluster sampling may have introduced selection bias, reduced the statistical independence of responses within clusters, and limited the generalizability of the findings. Future measurements among Chinese nursing students can guide the development of interventions to improve nursing students’ attitudes and confidence in oral healthcare, ultimately contributing to the provision of high-quality oral healthcare services by future nurses.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving humans were approved by the Biomedical Ethics Committee of West China Hospital, Sichuan University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YL: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. CX: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. YY: Data curation, Investigation, Writing – review & editing. WK: Data curation, Investigation, Writing – review & editing. YM: Investigation, Writing – review & editing. KC: Investigation, Writing – review & editing. BL: Investigation, Writing – review & editing. XL: Writing – review & editing. LL: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the National Natural Science Foundation of China (grant number: 52373237).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1689136/full#supplementary-material
Footnotes
References
1. health, Oral: World Health Organization (2020). Available online at: https://www.who.int/health-topics/oral-health/#tab=tab_1.
2. Stanford, ND, Ip, TB, and Durham, J. Adult orthodontic patients' views regarding dentofacial normality: a qualitative study. Am J Orthod Dentofacial Orthop. (2014) 145:287–95. doi: 10.1016/j.ajodo.2013.11.016
3. Silva, CR, Silva, CC, and Rodrigues, R. Etiology of halitosis in pediatric dentistry. Arch Pediatr. (2022) 29:467–74. doi: 10.1016/j.arcped.2022.05.009
4. Delanghe, G, Ghyselen, J, van Steenberghe, D, and Feenstra, L. Multidisciplinary breath-odour clinic. Lancet. (1997) 350:187. doi: 10.1016/S0140-6736(05)62354-9
5. Briceag, R, Caraiane, A, Raftu, G, Horhat, RM, Bogdan, I, Fericean, RM, et al. Emotional and social impact of halitosis on adolescents and young adults: a systematic review. Medicina. (2023) 59:564. doi: 10.3390/medicina59030564
6. Theodoridou, MZ, Heraclides, A, and Lamnisos, D. Need for orthodontic treatment and oral health-related quality of life in children and adolescents - a systematic review. Community Dent Health. (2024) 41:5–13. doi: 10.1922/CDH_00125Theodoridou09
7. Bahar, AD, Sagi, MS, Mohd Zuhairi, FA, and Wan Hassan, WN. Dental aesthetics and self-esteem of patients seeking orthodontic treatment. Healthcare. (2024) 12:1576. doi: 10.3390/healthcare12161576
8. Schertel Cassiano, L, Abdullahi, F, Leite, FRM, López, R, Peres, MA, and Nascimento, GG. The association between halitosis and oral-health-related quality of life: a systematic review and meta-analysis. J Clin Periodontol. (2021) 48:1458–69. doi: 10.1111/jcpe.13530
9. Al-Sahan, MM, MacEntee, MI, and Bryant, SR. A metatheory explaining how patients manage tooth loss. Gerodontology. (2020) 37:258–70. doi: 10.1111/ger.12457
10. Haag, DG, Peres, KG, Balasubramanian, M, and Brennan, DS. Oral conditions and health-related quality of life: a systematic review. J Dent Res. (2017) 96:864–74. doi: 10.1177/0022034517709737
11. Schierz, O, Baba, K, and Fueki, K. Functional oral health-related quality of life impact: a systematic review in populations with tooth loss. J Oral Rehabil. (2021) 48:256–70. doi: 10.1111/joor.12984
12. Wong, LB, Yap, AU, and Allen, PF. Periodontal disease and quality of life: umbrella review of systematic reviews. J Periodontal Res. (2021) 56:1–17. doi: 10.1111/jre.12805
13. Duangthip, D, and Chu, CH. Challenges in Oral hygiene and Oral health policy. Front Oral Health 2020;1:575428, doi: 10.3389/froh.2020.575428
14. Kassebaum, NJ, Bernabé, E, Dahiya, M, Bhandari, B, Murray, CJ, and Marcenes, W. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J Dent Res. (2014) 93:1045–53. doi: 10.1177/0022034514552491
15. Kassebaum, NJ, Bernabé, E, Dahiya, M, Bhandari, B, Murray, CJ, and Marcenes, W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. (2015) 94:650–8. doi: 10.1177/0022034515573272
16. Lertpimonchai, A, Rattanasiri, S, Arj-Ong Vallibhakara, S, Attia, J, and Thakkinstian, A. The association between oral hygiene and periodontitis: a systematic review and meta-analysis. Int Dent J. (2017) 67:332–43. doi: 10.1111/idj.12317
17. Gudipaneni, RK, Patil, SR, Assiry, AA, Karobari, MI, Bandela, V, Metta, KK, et al. Association of oral hygiene practices with the outcome of untreated dental caries and its clinical consequences in pre- and primary school children: a cross-sectional study in a northern province of Saudi Arabia. Clin Exp Dent Res. (2021) 7:968–77. doi: 10.1002/cre2.438
18. Herrera, D, Sanz, M, Shapira, L, Brotons, C, Chapple, I, Frese, T, et al. Association between periodontal diseases and cardiovascular diseases, diabetes and respiratory diseases: consensus report of the joint workshop by the European Federation of Periodontology (EFP) and the European arm of the world Organization of Family Doctors (WONCA Europe). J Clin Periodontol. (2023) 50:819–41. doi: 10.1111/jcpe.13807
19. Borsa, L, Dubois, M, Sacco, G, and Lupi, L. Analysis the link between periodontal diseases and Alzheimer's disease: a systematic review. Int J Environ Res Public Health. (2021) 18:9312. doi: 10.3390/ijerph18179312
20. Michaud, DS, Fu, Z, Shi, J, and Chung, M. Periodontal disease, tooth loss, and Cancer risk. Epidemiol Rev. (2017) 39:49–58. doi: 10.1093/epirev/mxx0006
21. Griffin, SO, Jones, JA, Brunson, D, Griffin, PM, and Bailey, WD. Burden of Oral disease among older adults and implications for public health priorities. Am J Public Health. (2012) 102:411–8. doi: 10.2105/AJPH.2011.300362
22. Spanemberg, JC, Cardoso, JA, Slob, E, and López-López, J. Quality of life related to oral health and its impact in adults. J Stomatol Oral Maxillofac Surg. (2019) 120:234–9. doi: 10.1016/j.jormas.2019.02.004
23. Peres, MA, Daly, B, Guarnizo-Herreño, CC, Benzian, H, and Watt, RG. Oral diseases: a global public health challenge reply. Lancet. (2020) 395:186–7. doi: 10.1016/S0140-6736(19)32997-6
24. Shibayama, T, Kudoh, R, and Hidaka, K. Factors associated with the practice of periodontal management by diabetes educator nurses for outpatients with diabetes: a nationwide survey in Japan. Prim Care Diabetes. (2021) 15:819–24. doi: 10.1016/j.pcd.2021.05.004
25. Dolce, MC, Haber, J, and Shelley, D. Oral health nursing education and practice program. Nurs Res Pract. (2012) 2012:149673. doi: 10.1155/2012/149673
26. Daly, B, and Smith, K. Promoting good dental health in older people: role of the community nurse. Br J Community Nurs. (2015) 20:431–6. doi: 10.12968/bjcn.2015.20.9.431
27. Ahmad, MS, Abuzar, MA, Razak, IA, Rahman, SA, and Borromeo, GL. Educating medical students in oral health care: current curriculum and future needs of institutions in Malaysia and Australia. Eur J Dent Educ. (2017) 21:E29–38. doi: 10.1111/eje.12211
28. Han, P, Xu, S, Dong, B, and Li, X. Effect of grasping force circle training based on knowledge, attitude and practice theory in lung cancer patients with peripherally inserted central catheter. Chin J Mod Nurs. (2023) 29:2592–7. doi: 10.3760/cma.j.cn115682-20220810-03893
29. Bandura, A. Social cognitive theory: an agentic perspective. Annu Rev Psychol. (2001) 52:1–26. doi: 10.1146/annurev.psych.52.1.1
31. Verplanken, B, and Orbell, S. Attitudes, habits, and behavior change. Annu Rev Psychol. (2022) 73:327–52. doi: 10.1146/annurev-psych-020821-011744
32. Hsu, CL, and Lin, JCC. Effect of perceived value and social influences on mobile app stickiness and in-app purchase intention. Technol Forecast Soc Change. (2016) 108:42–53. doi: 10.1016/j.techfore.2016.04.012
33. Earle, TC, and Siegrist, M. Morality information, performance information, and the distinction between trust and confidence. J Appl Soc Psychol. (2006) 36:383–416. doi: 10.1111/risa.14015
34. Gottlieb, M, Chan, TM, Zaver, F, and Ellaway, R. Confidence-competence alignment and the role of self-confidence in medical education: a conceptual review. Med Educ. (2022) 56:37–47. doi: 10.1111/medu.14592
35. Coker, E, Ploeg, J, Kaasalainen, S, and Carter, N. Nurses’ oral hygiene care practices with hospitalised older adults in postacute settings. Int J Older People Nursing. (2017) 12:1–12. doi: 10.1111/opn.12124
36. Kalisch, BJ, McLaughlin, M, and Dabney, BW. Patient perceptions of missed nursing care. Jt Comm J Qual Patient Saf. (2012) 38:161–7. doi: 10.1016/S1553-7250(12)38021-5
37. Si, Y, Guo, Y, Yuan, C, Xu, T, and Zheng, SG. Comprehensive oral health care to reduce the incidence of severe early childhood caries (s-ECC) in urban China. Chin J Dent Res. (2016) 19:55–63. doi: 10.3290/j.cjdr.a35698
38. Kisely, S. No mental health without Oral health. Can J Psychiatry-Revue Canadienne De Psychiatrie. (2016) 61:277–82. doi: 10.1177/0706743716632523
39. Eskici, GT, and Baykal, U. Frequency, reasons, correlates and predictors of missed nursing care in Turkey: a multi-hospital cross-sectional study. Int J Nurs Pract. (2022) 28:1–17. doi: 10.1111/ijn.13050
40. Kalisch, BJ, Xie, BQ, and Dabney, BW. Patient-reported missed nursing care correlated with adverse events. Am J Med Qual. (2014) 29:415–22. doi: 10.1177/1062860613501715
41. Bhagat, V, Hoang, H, Crocombe, LA, and Goldberg, LR. Incorporating oral health care education in undergraduate nursing curricula-a systematic review. BMC Nurs. (2020) 19. doi: 10.1186/s12912-020-00454-6
42. Garrocho-Rangel, A, López-Torre, ME, Santos-Díaz, MA, Torre-Delgadillo, G, Flores-Arriaga, JC, Saadia, M, et al. Assessment of pediatricians' knowledge, practices, and attitudes on oral health/care in children in the last decade: a systematic scoping review and critical reflection. J Clin Pediatr Dent. (2022) 46:262–72. doi: 10.22514/1053-4625-46.4.2
43. Haresaku, S, Miyoshi, M, Kubota, K, Aoki, H, Kajiwara, E, Monji, M, et al. Effect of interprofessional education on oral assessment performance of nursing students. Clin Exp Dent Res. (2020) 6:51–8. doi: 10.1002/cre2.248
44. Shuang, F. Impact of team-based collaborative learning teaching method on nasogastric indwelling catheter success probability and learning interest in nursing students. Chin Med Her. (2019) 16:77–80. Available online at: https://med.wanfangdata.com.cn/Paper/Detail/PeriodicalPaper_yycyzx201919020
45. Xin, L, Sheng-kai, L, Jun-jie, W, Qian-qian, H, Sheng, J, Zhi-jia, X, et al. Investigation on the knowledge, attitude and practice of oral health and the influencing factors among medical college and university undergraduate in Anhui Province. Chin J Gen Pract. (2020) 18:984–8. doi: 10.16766/j.cnki.issn.1674-4152.001409
46. Li, LZ, Zhang, HY, Guan, XL, and Hao, N. Investigation of oral health status among freshmen in a medical university. Chin J Pract Stomatol. (2012) 5:358–60. doi: 10.3969/j.issn.1674-1595.2012.06.009
47. Veerasamy, A, Lyons, K, Crabtree, I, and Brunton, P. Geriatric oral health care content and barriers to its incorporation in undergraduate nursing curricula: New Zealand survey. J Dent Educ. (2023) 87:70–7. doi: 10.1002/jdd.13088
48. Azodo, CC, Ezeja, EB, Ehizele, AO, and Ehigiator, O. Oral assessment and nursing interventions among Nigerian nurses-knowledge, practices and educational needs. Ethiop J Health Sci. (2013) 23:265–70. doi: 10.4314/ejhs.v23i3.9
49. Pai, M, Ribot, B, Tane, H, and Murray, J. A study of periodontal disease awareness amongst third-year nursing students. Contemp Nurse. (2016) 52:686–95. doi: 10.1080/10376178.2016.1222241
50. Rojo, J, George, A, Ramjan, L, Hunt, L, and Salamonson, Y. Development and psychometric testing of the attitude and confidence with oral healthcare among nursing students (ACORN) scale. Nurse Educ Pract. (2023) 71:103736. doi: 10.1016/j.nepr.2023.103736
51. Yan, W, Xiangqun, J, Lisa, J, and Liu, F. Sinicization and reliability and validity test of the short-form of health literacy in dentistry (HeLD-14). Chin Nurs Res. (2021) 35:3612–6. doi: 10.12102/j.issn.1009-6493.2021.20.007
52. Dsouza, R, Quinonez, R, Hubbell, S, and Brame, J. Promoting oral health in nursing education through interprofessional collaborative practice: a quasi-experimental survey study design. Nurse Educ Today. (2019) 82:93–8. doi: 10.1016/j.nedt.2019.07.010
53. Leone, SM, Quinonez, RB, Chuang, A, Begue, A, Kerns, A, Jackson, J, et al. Introduction of prenatal Oral health into medical students' obstetrics training. J Dent Educ. (2017) 81:1405–12. doi: 10.21815/JDE.017.100
54. Wardh, I, and Sorensen, S. Development of an index to measure oral health care priority among nursing staff. Gerodontology. (2005) 22:84–90. doi: 10.1111/j.1741-2358.2005.00063.x
55. Liu, J, Lu, TT, Li, Y, Dai, HY, and Li, L. Exploring the psychological experience of novice nurses in stomatological hospitals in China: a phenomenological study. BMC Nurs. (2024) 23:223. doi: 10.1186/s12912-024-01879-z
56. Feng, XW, Xiao, W, Shen, F, Ye, ZW, Su, WY, Cai, AQ, et al. Development and validation of an evaluation index system of health education competence for dental nurses in China: a mixed methods study. BMC Nurs. (2025) 24:480. doi: 10.1186/s12912-025-03107-8
57. Yin, Y, Han, J, Fu, L, and Zhang, H. The status of cultivation of nurses specialized in stomatology. Chin J Nurs Educ. (2022) 19:182–7. doi: 10.3761/j.issn.1672-9234.2022.02.016
58. Jiang, XC, Lian, J, Ding, ZG, Wang, WF, Cao, WJ, Qiu, XL, et al. Developing the core knowledge system of dental hygienists training in China: a modified Delphi study. BMC Med Educ. (2025) 25:819. doi: 10.1186/s12909-025-07310-8
60. Sakaluk, JK, and Short, SD. A methodological review of exploratory factor analysis in sexuality research: used practices, best practices, and data analysis resources. J Sex Res. (2017) 54:1–9. doi: 10.1080/00224499.2015.1137538
61. Smith, CM, Horne, CE, and Wei, H. Nursing practice in modern healthcare environments: a systematic review of attributes, characteristics, and demonstrations. J Adv Nurs. (2024) 80:3481–98. doi: 10.1111/jan.16088
62. Gohri, J, Kalra, S, and Hegde, S. Factors influencing empathy level among healthcare professionals: a systematic review and meta-analysis. J Educ Health Promot. (2025) 14:389. doi: 10.4103/jehp.jehp_1647_24
63. Kwon, CS, Jacoby, A, Ali, A, Austin, J, Birbeck, GL, Braga, P, et al. Systematic review of frequency of felt and enacted stigma in epilepsy and determining factors and attitudes toward persons living with epilepsy-report from the international league against epilepsy task force on stigma in epilepsy. Epilepsia. (2022) 63:573–97. doi: 10.1111/epi.17135
64. Venables, H, Wells, Y, Fetherstonhaugh, D, and Wallace, H. Factors associated with nursing students' attitudes toward older people: a scoping review. Gerontol Geriatr Educ. (2023) 44:131–50. doi: 10.1080/02701960.2021.2012466
65. Jiang, QJ, Lu, YH, Ying, YP, and Zhao, HH. Attitudes and knowledge of undergraduate nursing students about palliative care: an analysis of influencing factors. Nurse Educ Today. (2019) 80:15–21. doi: 10.1016/j.nedt.2019.05.040
66. Zhang, JH, Pang, SQ, Ge, L, Wang, GM, Luo, ZT, Hong, XP, et al. Research ability and research motivation of postgraduate nursing students in traditional Chinese medicine colleges. Nurs Open. (2022) 9:408–17. doi: 10.1002/nop2.1079
67. Sibandze, BT, and Scafide, KN. Among nurses, how does education level impact professional values? A systematic review. Int Nurs Rev. (2018) 65:65–77. doi: 10.1111/inr.12390
68. Brown, TA, and Moore, MT. Confirmatory factor analysis In: Handbook of structural equation modeling, vol. 361 (2012). 379. New York, NY: Guilford Publications.
69. Sousa, VD, and Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. J Eval Clin Pract. (2011) 17:268–74. doi: 10.1111/j.1365-2753.2010.01434.x
70. Jorm, AF. Using the Delphi expert consensus method in mental health research. Aust N Z J Psychiatry. (2015) 49:887–97. doi: 10.1177/0004867415600891
71. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
72. Almanasreh, E, Moles, R, and Chen, TF. Evaluation of methods used for estimating content validity. Res Social Adm Pharm. (2019) 15:214–21. doi: 10.1016/j.sapharm.2018.03.066
73. Melkamu Asaye, M, Gelaye, KA, Matebe, YH, Lindgren, H, and Erlandsson, K. Valid and reliable neonatal near-miss assessment scale in Ethiopia: a psychometric validation. Glob Health Action. (2022) 15:2029334. doi: 10.1080/16549716.2022.2029334
74. Floyd, FJ, and Widaman, KF. Factor analysis in the development and refinement of clinical assessment instruments. Psychol Assess. (1995) 7:286–99. doi: 10.1037/1040-3590.7.3.286
75. Revelle, W, and Zinbarg, RE. Coefficients alpha, beta, omega, and the glb: comments on Sijtsma. Psychometrika. (2009) 74:145–54. doi: 10.1007/s11336-008-9102-z
76. Shilbayeh, SAR, and Ibrahim, AA. The anti-clot treatment scale (ACTS): validation of the translated Arabic version among patients undergoing warfarin therapy in Saudi Arabia. Health Qual Life Outcomes. (2020) 18:215. doi: 10.1186/s12955-020-01471-4
77. Park, MS, Kang, KJ, Jang, SJ, Lee, JY, and Chang, SJ. Evaluating test-retest reliability in patient-reported outcome measures for older people: a systematic review. Int J Nurs Stud. (2018) 79:58–69. doi: 10.1016/j.ijnurstu.2017.11.003
78. Shiner, B, Ronconi, JM, McKnight, S, Young-Xu, Y, Mills, PD, and Watts, BV. Test-retest reliability of the VA National Center for patient safety culture questionnaire. J Eval Clin Pract. (2016) 22:985–9. doi: 10.1111/jep.12589
79. Cai, F, Xue, S, Zhang, M, Chen, X, Zhang, J, Bao, Y, et al. Assessing reliability and validity of the Chinese version of the crown-crisp experience index and its application in pneumoconiosis patients. BMC Psychiatry. (2023) 23:263. doi: 10.1186/s12888-023-04731-x
80. Liu, Z, Tian, L, Chang, Q, Sun, B, and Zhao, Y. A competency model for clinical physicians in China: a Cross-sectional survey. PLoS One. (2016) 11:e0166252. doi: 10.1371/journal.pone.0166252
81. Orts-Cortés, MI, Moreno-Casbas, T, Squires, A, Fuentelsaz-Gallego, C, Maciá-Soler, L, and González-María, E. Content validity of the Spanish version of the practice environment scale of the nursing work index. Appl Nurs Res. (2013) 26:e5–9. doi: 10.1016/j.apnr.2013.08.006
82. Bentler, PM. Comparative fit indexes in structural models. Psychol Bull. (1990) 107:238–46. doi: 10.1037/0033-2909.107.2.238
83. Jung, M, Kang, U, Kim, S, Yoo, HW, Kim, HY, Kim, M, et al. Psychological distress and perceived burden in parents of Korean children with IgE-mediated food allergy. J Korean Med Sci. (2023) 38:e208. doi: 10.3346/jkms.2023.38.e208
84. Albougami, A. Oral health literacy levels of nursing professionals and effectiveness of integrating oral health training into nursing curricula: a systematic review. Appl Sci. (2023) 13:10403. doi: 10.3390/app131810403
85. Rojo, J, George, A, Smith, BW, Ramjan, LM, Hunt, L, Hartnett, E, et al. Integration of oral healthcare into undergraduate health professional educational programs: a scoping review. Collegian. (2022) 29:755–66. doi: 10.1016/j.colegn.2022.01.002
86. Chu-jin, Q, Feng-ying, Z, and Xian-qiong, F. Application of multi-view recording and broadcasting system in oral care operation teaching for undergraduate nursing students. J Nurs. (2020) 27:15–9. doi: 10.16460/j.issn1008-9969.2020.07.015
Keywords: transcultural adaptation, psychometric evaluation, attitude, confidence, oral healthcare, nursing students
Citation: Li Y, Xie C, Yue Y, Kong W, Ma Y, Chen K, Liu B, Liao X and Li L (2025) Transcultural adaptation and psychometric evaluation of the Chinese version of attitude and confidence with oral healthcare among nursing students scale: a cross-sectional survey in China. Front. Public Health. 13:1689136. doi: 10.3389/fpubh.2025.1689136
Edited by:
Filiz Hisar, Necmettin Erbakan University, TürkiyeReviewed by:
Kubra Sultan Dengiz, Necmettin Erbakan Üniversitesi, TürkiyePui Ki Tsui, Vocational Training Council (VTC), China
Copyright © 2025 Li, Xie, Yue, Kong, Ma, Chen, Liu, Liao and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lingli Li, bGlsaW5nbGkyMDAwQDEyNi5jb20=
†These authors have contributed equally to this work and share first authorship