 Marcos Puebla
Marcos Puebla Luis Korrodi-Gregório
Luis Korrodi-Gregório Luca Trentin2
Luca Trentin2- 1Alira Health SLU, Barcelona, Spain
- 2Alira Health Srl, Milan, Italy
Introduction: Over the last decades, Health Technology Assessment (HTA) has become pivotal in guiding decision-making concerning the inclusion of new health technologies in health systems worldwide. As HTA continues to evolve, the importance of patient participation to achieve a more informed, transparent, and legitimate decision-making process has gained increased recognition. Yet practices vary widely and are often modest in scope.
Methods: We conducted a comparison and ranking of 56 HTA systems across five regions based on levels of patient participation throughout the HTA process. Participation was measured by applying a scoring framework we developed to publicly available information for each system.
Results: Many HTA systems include patient participation, but the level of involvement shows substantial variation across systems and tends to be comparatively modest. Some systems demonstrate active engagement throughout the process, while others show limited participation.
Discussion: To our knowledge, this is the first attempt to quantify patient participation on a wider scale to enable comparisons across a large sample of HTA systems. The findings offer policymakers, healthcare professionals, patients, and researchers a comprehensive view of current approaches and highlight opportunities to enhance patient involvement in HTA.
1 Introduction
Healthcare systems have limited resources and often have to make difficult decisions regarding the allocation of these resources in the service of providing effective, valuable, and timely care in an equitable manner (1). These decisions are complex and require a clear, comprehensive, and transparent process to ensure that they are fair and are acceptable to the population served. Health technology assessment (HTA), a multidisciplinary process that systematically summarizes and evaluates the medical, economic, social, and ethical issues related to the use of a health technology, is one of the most widely used methods for informing the decision-making process (2, 3).
As the role and methods of HTA continue to evolve, patient participation in HTA has emerged as imperative (4). In this article, “patients” is used as an umbrella term to encompass various roles representing patients, such as individual patients, caregivers, patient organization representatives, patient advocates, or patient experts. These roles are integral for making more informed, transparent, accountable, and legitimate decisions regarding health technologies. Despite several worldwide initiatives aimed at involving patients in HTA, practices for patient participation remain limited in many regions across the world (5–8). Such limitations often stem from barriers including limited resources, insufficient familiarity of patients with technical processes, lack of standardized methodologies, and uncertainty about how to meaningfully integrate patient input. In many systems, participation remains sporadic or tokenistic rather than institutionalized (4, 9, 10).
One of the main arguments for involving patients in HTA is based on the rights of patients to participate in the planning and delivery of their healthcare. Since the HTA process typically determines the health services and procedures available to patients, it follows that patients have a right to be heard as part of the HTA process (11). Beyond respecting patients' rights, such engagement has the added value of building public trust in the health system processes and in increasing transparency (8). Patients can also provide valuable perspectives on their experiences, attitudes, beliefs, values, and expectations regarding health, illness, the impact of health technologies, and their utilization–information that is not obtainable from clinical trials or medical practitioners (12). Consequently, integrating patients into HTA processes is expected to result in the delivery of care that is responsive to their unique needs and values (13). Beyond sharing their experiential knowledge, it is believed that involving patients in health decision-making can foster a sense of empowerment and contribute to more effective solutions when it comes to allocating limited healthcare resources (4). While evidence of the impact of patient participation on market access, whether in terms of accelerating availability or broadening access, remains limited and more time and systematic evaluation will be needed to fully understand its overall effects, there are documented cases where it has influenced HTA recommendations, such as the Patient and Clinician Engagement (PACE) process in Scotland (14), patient evidence shaping appraisal outcomes at NICE in the United Kingdom (15), and patient submissions and consultations contributing to reimbursement decisions at CONITEC in Brazil (16). Ultimately, incorporating patient perspectives ensures that the specific requirements and values of patients are considered, enhancing both the legitimacy and the relevance of HTA decisions (9).
As outlined by Facey (17), patient involvement in HTA can be understood through two distinct but complementary approaches: patient-based evidence and patient participation. Patient-based evidence refers to data systematically generated through research, such as studies on experiences from patients, preferences, and outcomes, usually published in peer-reviewed literature. By contrast, patient participation draws directly on the perspectives and lived experiences of individual patients, caregivers, or patient groups, without necessarily following formal research methods. While both approaches enrich the HTA process, this article focuses specifically on patient participation mechanisms. As described in Figure 1, patient participation can occur at every step of the HTA process, from topic selection and scoping to assessment, appraisal, and implementation and reporting. Within these phases, participation can take different forms depending on the purpose and context, such as identifying and prioritizing health technologies, submitting input about a disease or health technology individually or through patient groups, reviewing HTA documentation, or serving as patient representatives on HTA committees (8, 17).

Figure 1. Description of HTA phases.
While there is already a notable acknowledgement of the relevance of patient participation in the HTA process, the breadth and depth of that participation can vary significantly from one country to another, or even across HTA systems in the same country. It can still be perceived as an add-on rather than an indispensable component; hence, its absence is not necessarily viewed as a critical deficiency in an HTA, and there is still room for improvement (5–8).
Given the degree of heterogeneity present in both HTA systems themselves and the amount and type of patient participation observed in their processes, it can be difficult to make comparisons across systems (17). Attempts have been made to o classify patient participation in HTA (18), as well as to describe and catalogue the role of patients in HTA in individual countries and there are various published studies comparing a particular activity or set of practices between countries or across groups of countries (19–26).
However, to the best of our knowledge, the present study is the first attempt to systematize and, in particular, quantify, the level of participation on a wider scale to enable comparisons across countries and geographies and recognize leaders and areas for improvement. Previous studies have been primarily descriptive, while this study, in developing a weighted index, aims to quantify participation to allow for a more robust comparison across HTA systems and capture a snapshot of the current state of affairs, that can be used as a baseline against which future developments can be measured.
2 Materials and methods
2.1 Scope and variables definition
Prior to identifying or evaluating any HTA systems, the scope of HTA and the set of activities in which patient participation was deemed to be important were established. The list was based on published literature (4, 10, 17–19, 21, 27–30) and was designed to capture a comprehensive yet manageable set of recognized practices, spanning all HTA phases and balancing structural mechanisms (e.g., voting rights, committee membership), procedural practices (e.g., consultations, submissions, report reviews), and transparency measures (e.g., lay summaries, feedback on input use). The phases of HTA that were considered in scope for the purposes of this study were identification and prioritization of health technologies, scoping of evaluation, assessment, appraisal, and implementation and reporting, which parallel those defined by Goodman (31). Within each HTA phase, relevant activities were defined as variables, and a set of categories were developed for each variable to measure the level of patient participation. Additionally, a few variables were independent of these phases and applied to the overall HTA process. Table 1 presents the 17 variables and their main categories used to assess patient participation in the study. Three of the 17 variables were not classified within the phases due to their application to the general HTA process. A more detailed breakdown of the categories and variables can be found in Supplementary Table 1.
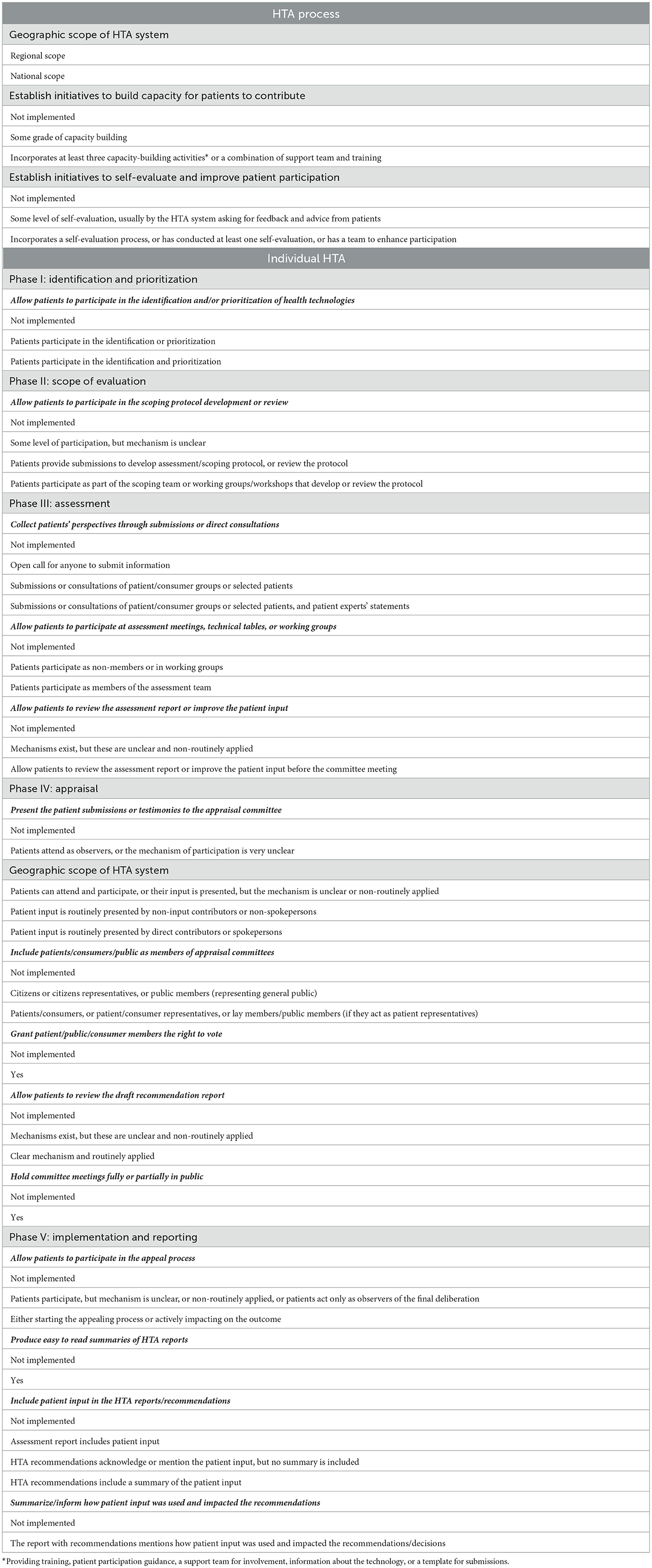
Table 1. Patient participation variables and categories.
These formed the components of a scoring system (range 0–10), in which activities were weighted based on their significance to the HTA process and outcome and labelled as Low, Medium, High, or Very High relevance. Weights were determined using a simplified three-factor framework that considered: (i) the depth and role of engagement (symbolic, consultative, or empowered), (ii) the influence the activity can exert on HTA outputs, and (iii) its contribution to transparency or the institutionalization of patient participation. Activities that embedded patients structurally or granted decision-making power (e.g., voting rights, committee membership) were assigned Very High weights, whereas activities offering active but non-structural participation (e.g., assessment meetings, scoping, patient testimonies) were assigned High weights. Medium weights were applied to activities that support participation or enhance transparency without strong influence (e.g., self-evaluation, draft review, public meetings), while Low weights reflected activities that were largely symbolic or informative (e.g., lay summaries, report mentions). The full table detailing weight assignments and corresponding rationales is provided in Supplementary Table 2.
Each activity was assessed using a 0–1 scoring system to capture the level of implementation across HTA agencies. For every activity, predefined categories described graduated levels of patient participation, ranging from 0 (not implemented) to 1 (highest level of participation), with partial scores (e.g., 0.2, 0.4, 0.5, 0.6, 0.8) reflecting intermediate levels. Partial points were determined by activity-specific criteria, including the clarity and formalization of the participation mechanism, frequency of its application (routine vs. non-routine), and type of participants involved (with higher scores for direct patient or patient-organization involvement compared to general public representation). This approach aligns with the paper's primary focus on patient participation, although public participation was also considered, recognizing its potential to convey the patient perspective in certain contexts. The term “patient participation” is used throughout the text to refer to both patient and public participation, unless otherwise specified. By combining flexibility with comparability, this scoring system captures the nuanced variability of implementation within and across HTA systems while maintaining comparability. The complete list of activity-specific categories and their corresponding scores is provided in Supplementary Table 3. Total HTA system scores were calculated by summing the weighted activity scores, yielding a final score between 0 and 10.
2.2 Country selection
In the first phase of the process of identifying and evaluating HTA systems, countries for inclusion in the analysis were selected. Firstly, through a scouting exercise, countries with formal HTA systems were identified and evaluated for inclusion in the analysis. Starting from the list of United Nations member states (plus Taiwan), each country was cross-referenced with various publicly available lists of HTA systems (INAHTA, EUnetHTA, WHO, publications, reports, etc.) to see if there were any formal HTA body present in the country. In addition, for each country, the Human Development Index (HDI) category and gross domestic product (GDP) were recorded.
Once the check for HTA systems was complete and the HDI and GDP information had been collected, the country selection process began. Countries were selected for inclusion based on the presence of HTA systems, as well as their HDI category and GDP. Countries without at least one formal HTA body were excluded from the study. Next, a filter for HDI category was applied, in which those countries with a very high HDI (all countries meeting this criterion) or high/medium HDI (and with a GDP above 250 million to ensure representativeness of countries) were included. Then a GDP cut-off was applied to the remaining countries, with only those countries whose GDP was above 200 million USD advancing to the next stage. In the final stage of the selection process, the type of the HTA body was evaluated. Countries with at least one entity that was an agency, committee, or similar, and that had a web presence were included, while those whose HTA systems were units, directorates, or technical groups within the country's Ministry of Health, social security organization, national commission, or medicines agency, or who lacked a web presence, were excluded. The rationale for this selection phase was to be judicious and follow a process that could be replicated in the future and at the same time ensure that there would be sufficient information available on each country for the evaluation phase.
2.3 HTA system selection
In the second phase, following the conclusion of the country selection process, further information was collected about the HTA systems in the remaining countries to determine which HTA systems from these countries would be analyzed in the study. The HTA systems in each country were identified and basic information (name, geographic scope, remit, website, etc.) was compiled about each of the systems.
HTA systems with a national scope were preferentially identified. However, in certain cases, such as when HTA was also taking place at a sub-national level, a few regional systems were also included. If a particular nation had more than one HTA body with a national scope, with one for pharmaceuticals and another for medical devices, for example, or one for inpatient and another for outpatient drugs, then multiple systems were included. Systems responsible for HTA of pharmaceuticals, medical devices, or both were included, while systems that exclusively focused on medical procedures or diagnostics were excluded. In addition, when more than one national HTA body evaluated pharmaceuticals and/or medical devices, only the body whose assessments inform decision-making regarding the inclusion and coverage was included. Within the HTA systems that inform decision-making, processes or programs not related to coverage, such as multiple technology assessment (MTA) in France or the development of clinical guidelines in Colombia, were not included. There was an emphasis on public systems performing HTA activities related to public healthcare systems, with the exception of the United States and Brazil, where private activity was also considered. This exception was made because, unlike in most countries, the United States and Brazil do not rely on a single national public HTA system. In the US, where coverage decisions are decentralized across public and private payers, influential private HTA bodies such as ICER complement the work of public agencies like AHRQ and directly shape reimbursement practices. Similarly, in Brazil, the health ecosystem includes both the public SUS (CONITEC) and a large regulated private sector where COSAUDE conducts HTA.
2.4 Data collection and analysis
The third phase was data identification and extraction. For each HTA agency selected in phase two searches were performed to identify additional sources of relevant information, after which data on the various facets of patient participation in the HTA process were extracted from the publicly available information into a spreadsheet. Triangulation of three data sources was undertaken to support data verification: sources of information primarily included: official HTA organization websites (identified during the scouting phase), published research papers, and grey literature (e.g., government or international organization reports). In all cases, the HTA body's own website as well as other official national or regional websites with information about the workings of that particular entity and its processes were reviewed in detail. Relevant published papers were identified via PubMed and manual searching of the references in already identified publications or reports. Translation tools were used as needed. Only secondary/desk research was conducted—the HTA systems were not contacted.
Data extraction for each agency was performed by a single reviewer, who filled in the spreadsheet with the available information, as well as the source or sources for each data point. Using this information, the reviewer then followed a rubric to assign a number for each data point that represented the degree to which each of the pre-identified criteria were fulfilled. A second reader then reviewed both the information collected for each HTA body and the degree of fulfillment assigned by the first reviewer in order to ensure accuracy and consistency in the application of the rubric across all systems evaluated. Discrepancies were resolved by consensus, with a third reviewer acting as referee if necessary.
After completing data extraction and application of the rubric, the sub-section (variable level), section (HTA phase level), and overall scores (0–10) were calculated for each HTA body, which can be found in Supplementary Table 4. The three variables that were not assigned to one of the four HTA phases only counted individually and for the overall score. These scores were then compared to each other and the HTA systems ranked accordingly. A qualitative analysis was also performed to explore trends, describe best practices, and identify the areas where patient participation was most lacking.
3 Results
In the first phase of country selection, out of the 194 countries considered for inclusion in the universe of the study, one or more formal HTA systems were detected during the scouting phase in 88 countries, with the remaining 106 excluded at this stage. In the second phase, a further 27 and 19 were excluded based on HDI and GDP, respectively, leaving 42 countries. Finally, an additional five countries were excluded based on the type of HTA organization or because the identified HTA systems lacked websites, with the result that a total of 37 countries were included in the analysis.
In the third phase, from the 37 countries selected, a total of 56 HTA systems were included in the analysis. Out of the 56, 29 HTA systems were in Europe, 12 in Asia, seven in North America, five in Latin America, and three in Oceania. No HTA systems from the region of Africa met the filtering criteria for inclusion in the analysis. Only a single HTA body was evaluated in 25 countries, two systems were evaluated in seven countries, three systems in three countries, and four systems in two countries. Twelve HTA systems were exclusively dedicated to the HTA of pharmaceuticals, 12 exclusively to medical devices, and 32 covered both. Eight countries had separate systems for drugs vs. medical devices. Forty-nine HTA systems were national in their geographic scope, while seven systems were regional. The full list of HTA systems and further details can be found in Table 2.
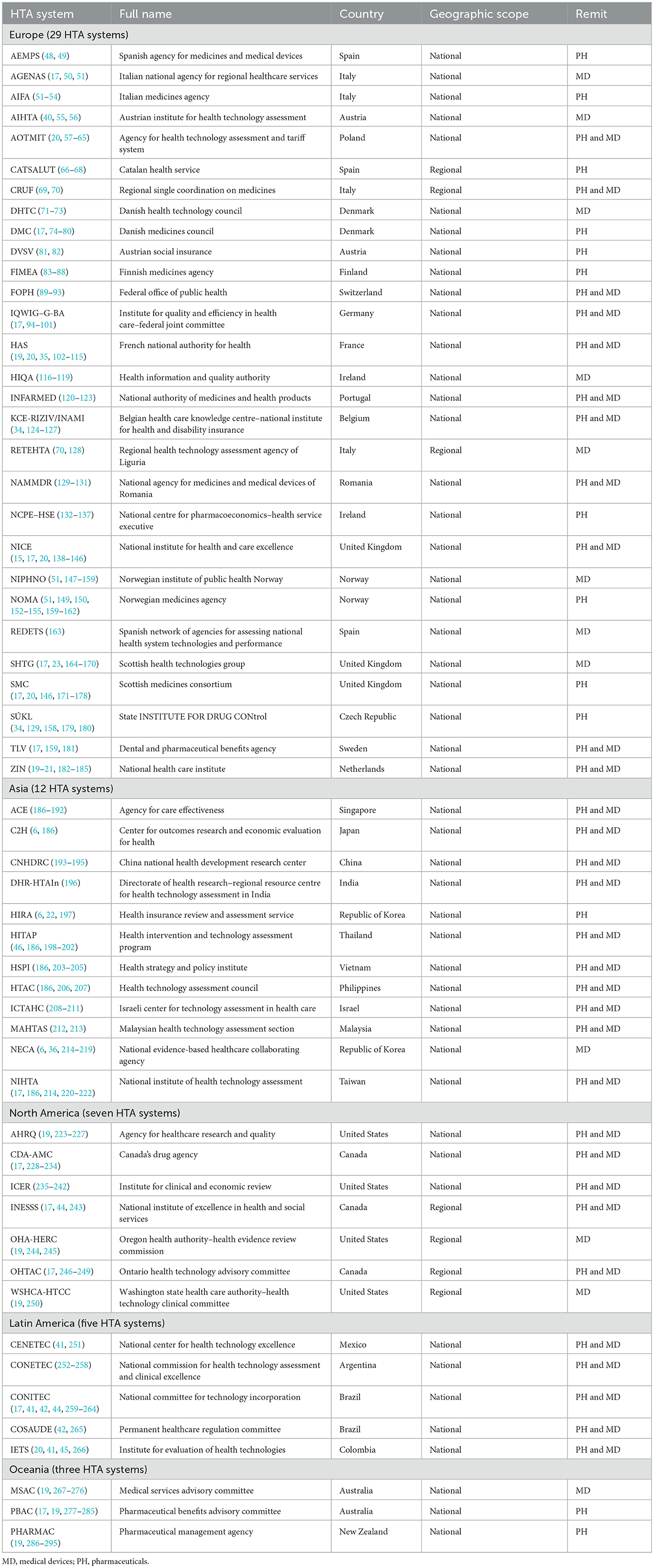
Table 2. Distribution per region, geographic scope and remit of the final list of analyzed HTA systems.
3.1 Phases and variables results: occurrence of patient participation by phase and variable across all HTA systems
Figure 2 displays the occurrence of patient participation per phase across all HTA systems, without delving into the degree of participation. Notably, patient participation was most frequent in the assessment and appraisal phases, with the scoping phase exhibiting the least.
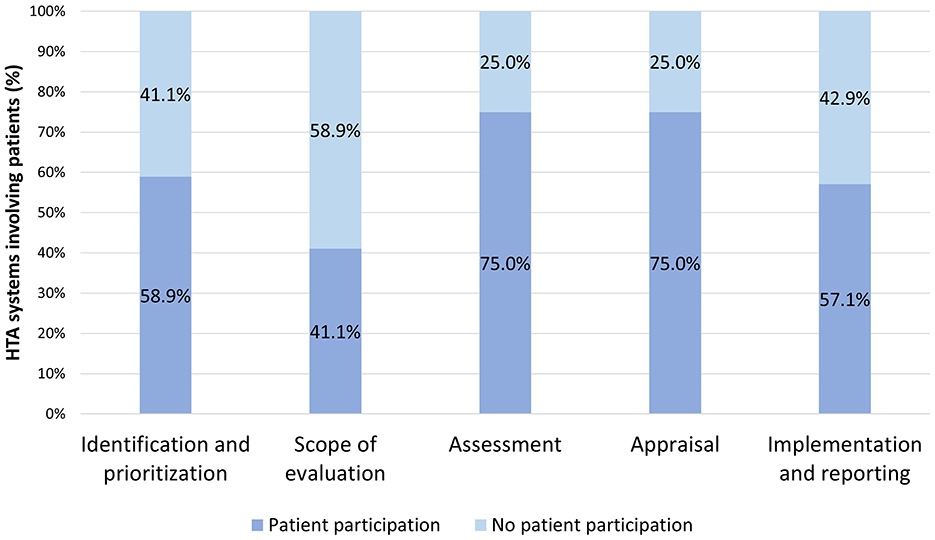
Figure 2. Occurrence of patient participation per phase across all HTA systems.
Figure 3 outlines the occurrence of patient participation per variable across all HTA systems, without considering the depth of participation per variable. Of the 16 variables used to evaluate patient participation -excluding the variable of “geographic scope of the HTA system” as greater emphasis was placed on those directly related to patient participation-, the three with the highest occurrence were, in descending order: allowing patients to identify and/or prioritize health technologies for evaluation (58.9% of HTA systems), building capacity for patients to contribute (57.1%), collecting patients' perspectives through patient submissions or direct consultation, and including patients/consumers/public as members of appraisal committees (55.4% for both). The three variables that least commonly included patient participation were, in ascending order: summarizing/informing how patient input was used and impacted the recommendations (7.1%), holding committee meetings in public (16.1%), and allowing patients to participate in the appeal process (21.4%).
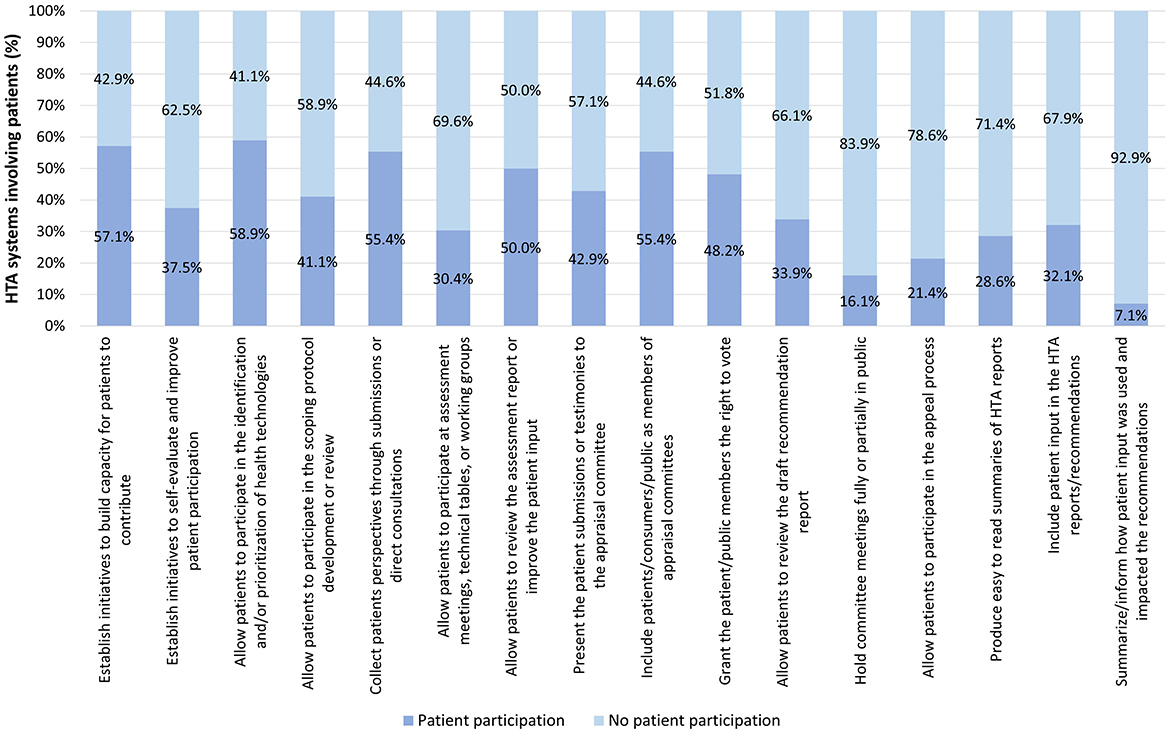
Figure 3. Occurrence of patient participation per variable across all HTA systems.
3.2 Phases and variables results: deep dive into the comprehensiveness of patient participation across phases and their respective variables and categories in all HTA systems
Table 3 displays the distribution of patient participation by variable and category across all HTA systems, offering insight into the depth of the patient participation per variable, Additionally, it provides examples within each category to further illustrate the findings. The categories within the variables in this table have been simplified for clarity. The full, detailed table can be found in Supplementary Table 5.
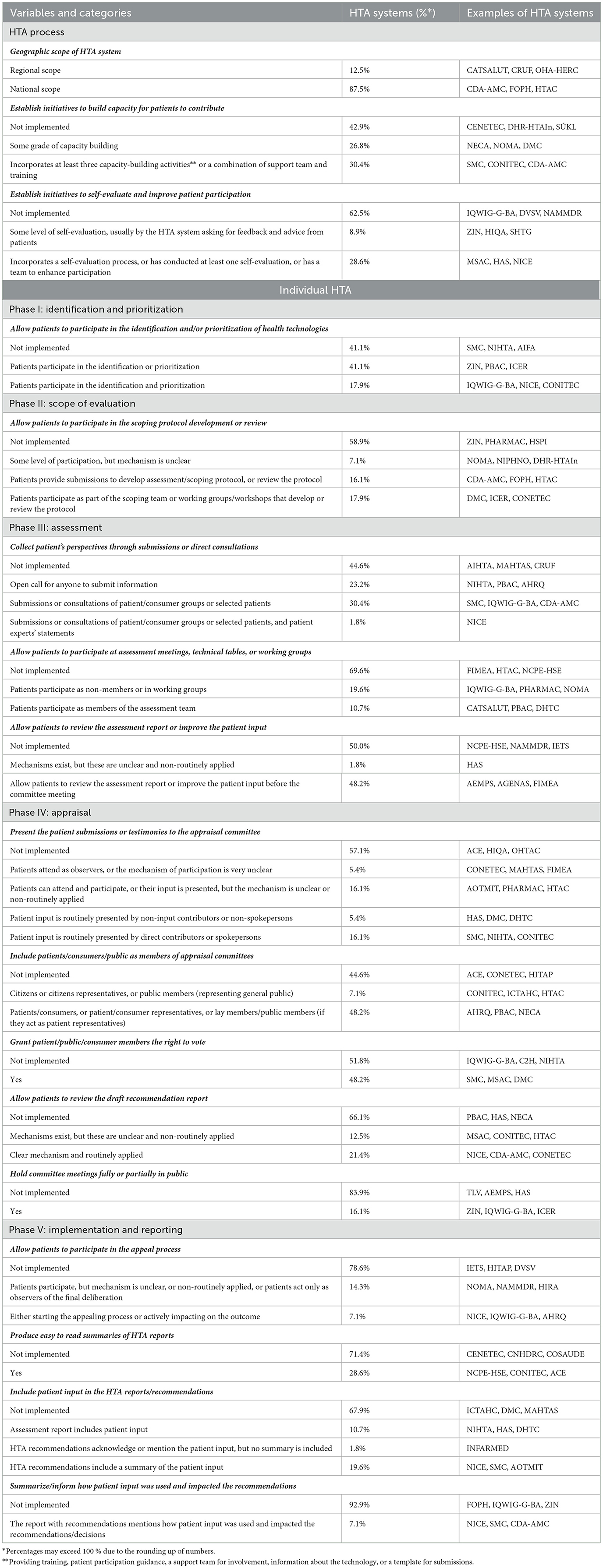
Table 3. Distribution of patient participation by variable and category across all HTA systems.
3.3 Ranking of HTA systems and classification into tiers
In addition to establishing a ranking of HTA systems based on their overall score from 0 to 10, four tiers were established to represent the performance of HTA systems worldwide in terms of patient participation. Each HTA body was assigned to a tier based on its overall score, and the tiers are the following: tier 4 (score from 0 to 2.5), Tier 3 (score from 2.5 to 5), Tier 2 (score from 5 to 7.5), and Tier 1 (score from 7.5 to 10). In general, Tier 1 systems have a fully comprehensive patient participation program, Tier 2 systems have strong patient participation programs, Tier 3 systems include patient participation to a certain extent, but have notable room for improvement, and Tier 4 systems have very limited patient participation.
Out of the 56 HTA systems analyzed, two (3.57%) HTA systems were included in Tier 1 with scores of 9.20 and 8.08, respectively, and an average score of 8.64. In Tier 2, the 14 (25%) HTA systems included had an average score of 6.22, and the scores ranged from 5.04 to 7.44. Tier 3 included 22 (39.29%) HTA systems, with scores between 2.56 and 4.94, and an average score of 3.58. Tier 4 comprised 19 (34.5%) HTA systems, with scores ranging from 0.00 to 2.44 and an average score of 1.05. The results and the breakdown by tiers can be found in Table 4. The total set of 56 HTA systems had an average score of 3.61, and 92.86% of all HTA systems analyzed incorporate some sort of patient participation.
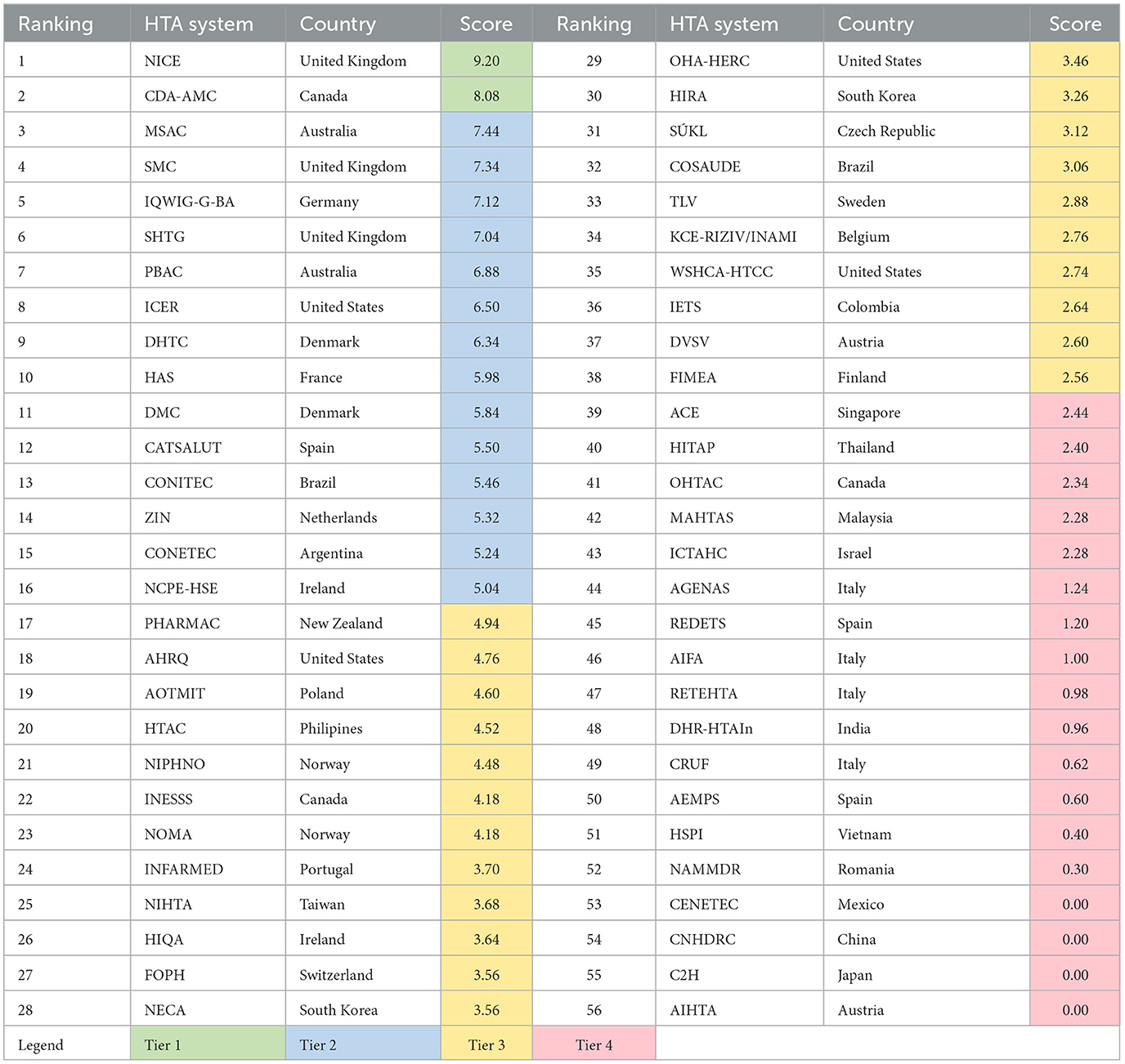
Table 4. HTA systems ranking and overall score.
3.4 HTA tier spread across geographies
The performance of the regions regarding the average score of their HTA systems, and its distribution across the four tiers, as well as showing the top two HTA systems per region in terms of average score can be found in Table 5.
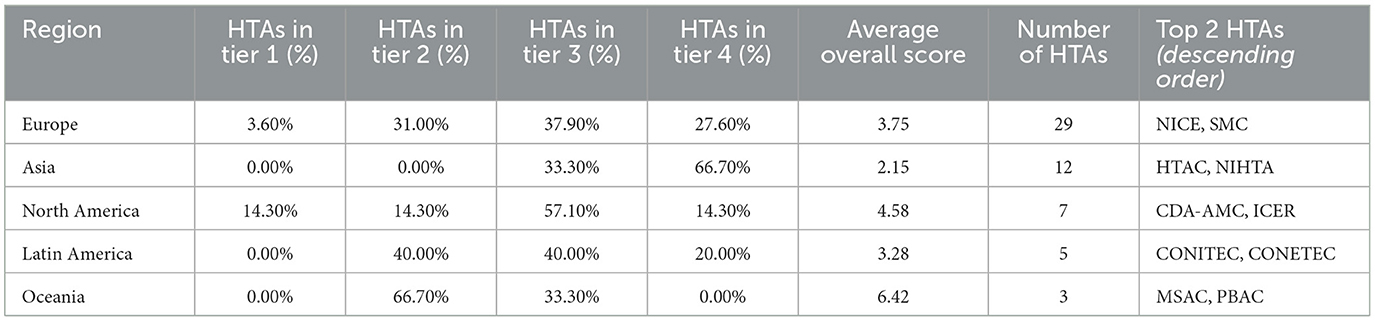
Table 5. Distribution of HTA systems across tiers per region, average score per region and top 2 HTA systems.
In terms of the distribution of HTA systems per tier across regions, Europe hosted one Tier 1 HTA system, with the majority distributed relatively evenly across Tiers 2, 3, and 4. Asia had some HTA systems in Tier 3, and most were ranked Tier 4. North America housed one Tier 1 HTA system, with the majority falling into Tier 3. In Latin America, most HTA systems were in Tiers 2 and 3. Oceania, boasting the highest average score, had most systems in Tier 2.
3.5 Top five HTA systems by phase
The top five HTA systems by phase based on their score per phase can be found in Table 6. In the case that more than one HTA achieved the same score for a certain phase, all those with the qualifying score were included in the same ranking group.
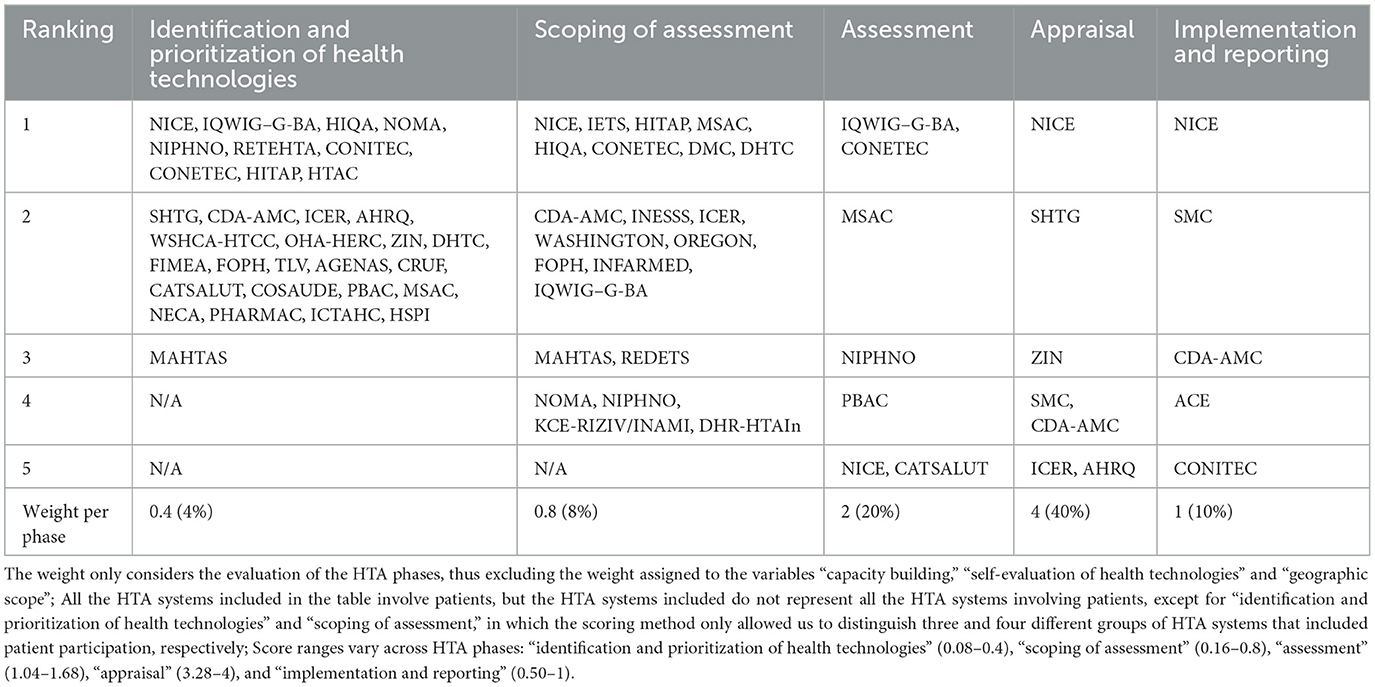
Table 6. Top five HTA systems by phase based on their score per phase.
Regarding the phase of identification and prioritization of health technologies, 10 HTA systems shared the highest ranking. For the scoping of assessment phase, eight HTA systems ranked the highest. The assessment phase was led by IQWIG–G-BA and CONETEC. Both the appraisal and implementation and reporting phases were led by NICE.
3.6 Occurrence of patient participation by tier and phase
The occurrence of patient participation (without considering the depth of participation per variable) by tier and phase can be found in Figure 4. All HTA systems in Tier 1 involve patients across the five HTA phases. In Tier 2 and 3 HTA systems, the occurrence of patient participation is similar in different phases, and is most common during assessment and appraisal, while it is least common in the scope of evaluation phase. Regarding Tier 4 HTA systems, the occurrence of patient participation is below 50% for all phases, and the scope of evaluation phase hosts the least occurrence.
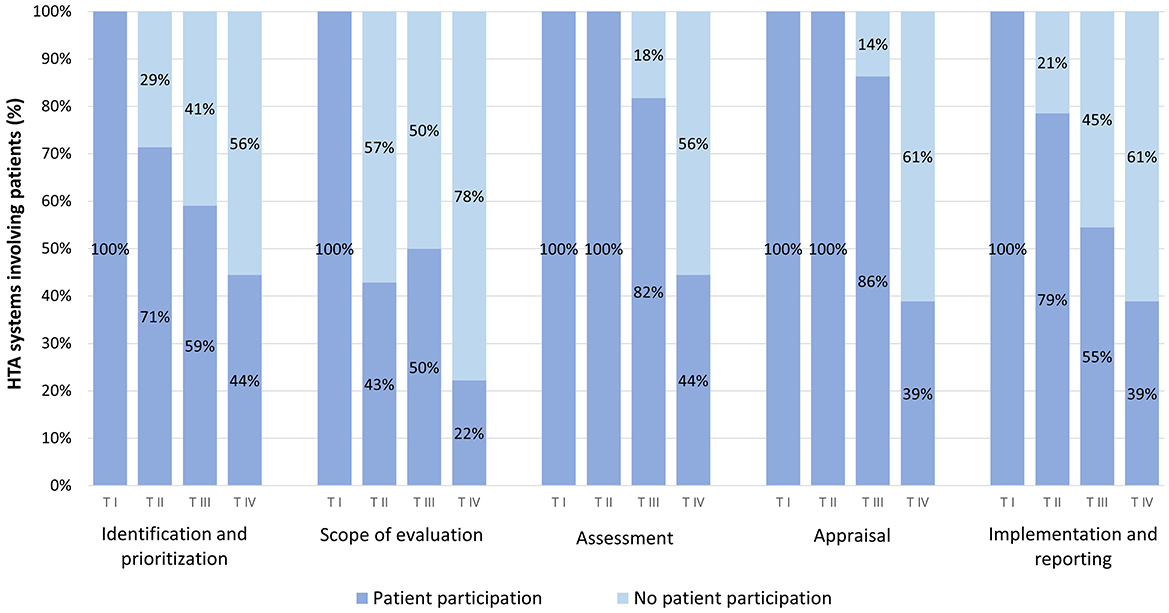
Figure 4. Occurrence of patient participation by phase and tier.
3.7 Occurrence of patient participation by tier and variable
Regarding the occurrence of patient participation by tier and variable, Tier 1 HTA systems involved patients in all but three variables (excluding the variable “geographic scope of the HTA system”), without considering the depth of participation per variable. Neither of the Tier 1 HTA systems allowed patients to participate at assessment meetings, technical tables, or working groups during assessment. Additionally, CDA-AMC did not hold committee meetings in public, nor did it allow patients to participate in the appeal process. Further details can be found in Figure 5.
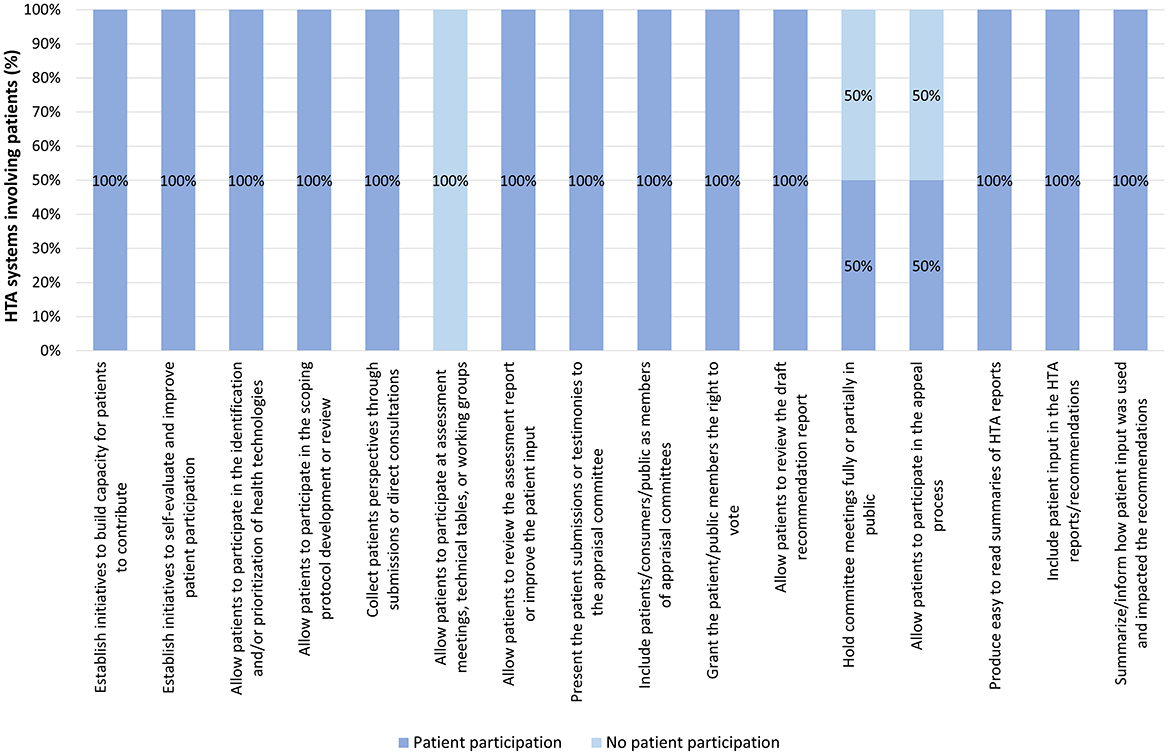
Figure 5. Occurrence of patient participation per variable across Tier 1 HTA systems.
In Tier 2 systems, the three variables with the highest occurrence were, in descending order: building capacity for patients to contribute and including patients/consumers/public as members of appraisal committees (93% for both), and granting them the right to vote (86%). Further details can be found in Figure 6.
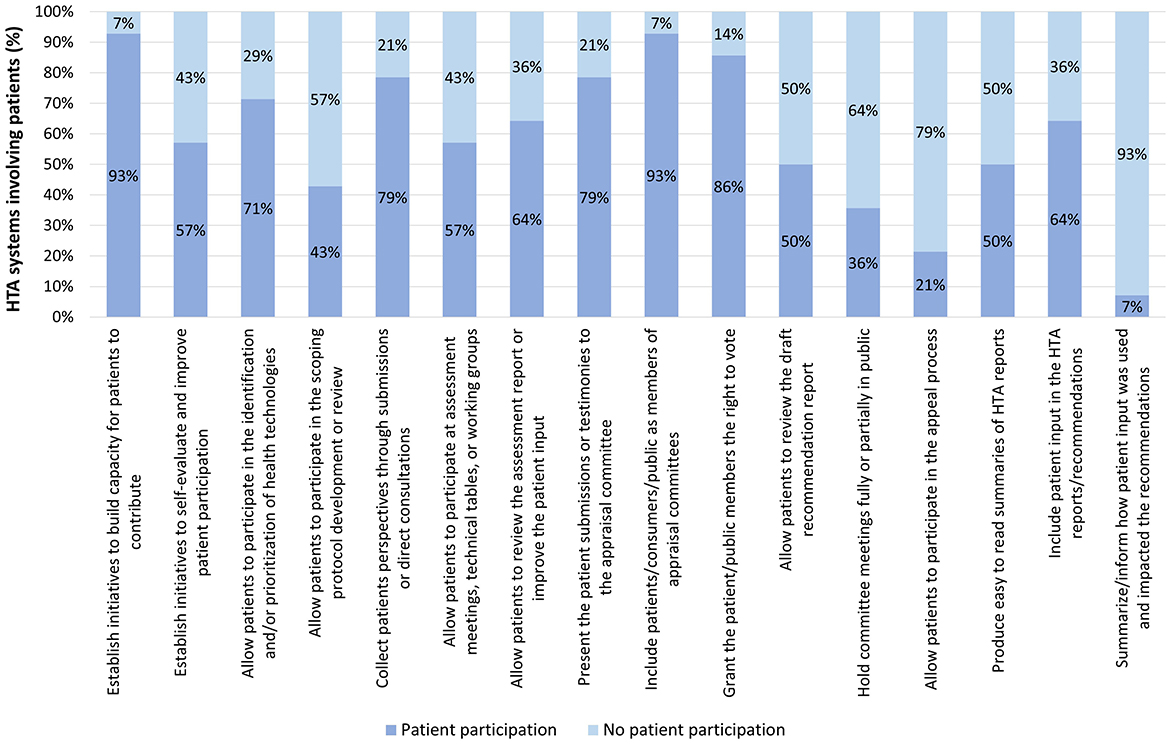
Figure 6. Occurrence of patient participation per variable across Tier 2 HTA systems.
For those systems in Tier 3, the three variables with the highest occurrence were, in descending order: collecting patients' perspectives through patient submissions or direct consultation and including patients/consumers/public as members of appraisal committees (68% for both), building capacity for patients to contribute, and allowing patients to participate in the identification and/or prioritization of health technologies for evaluation (59% for both). Further details can be found in Figure 7.
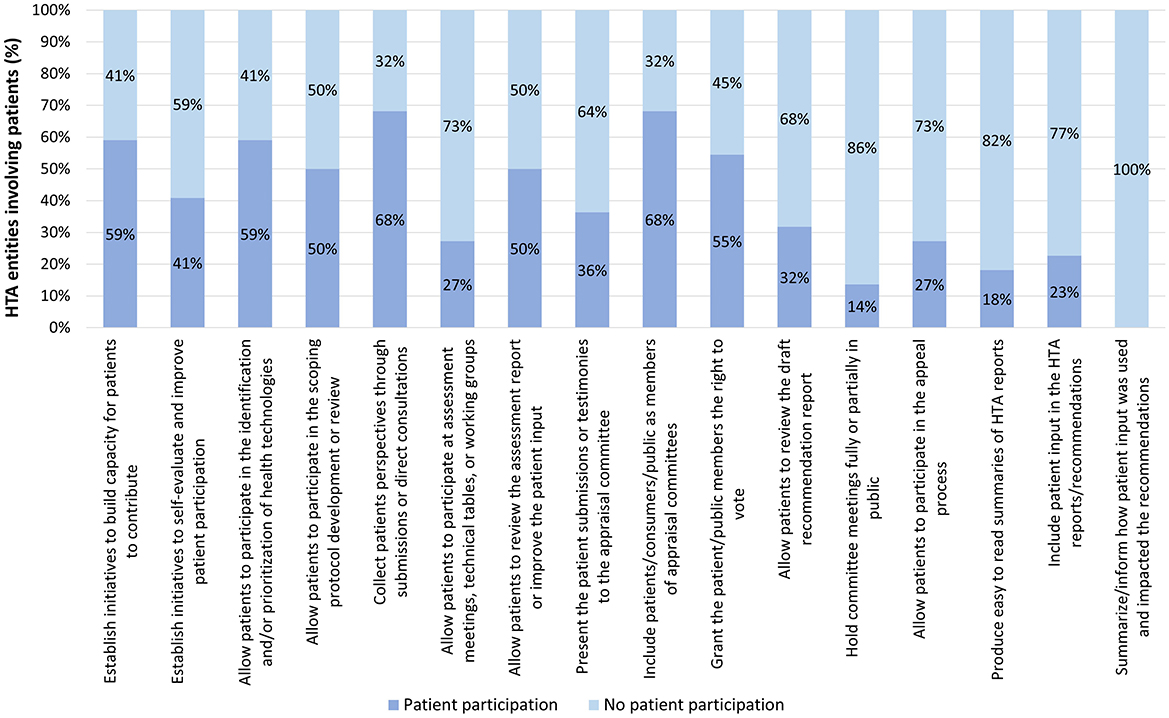
Figure 7. Occurrence of patient participation per variable across Tier 3 HTA systems.
Finally, in Tier 4 systems, the three variables with the highest occurrence were, in descending order: allowing patients to participate in the identification and/or prioritization of health technologies (44%), allowing patients to review the assessment report or improve the patient input (33%), building capacity for patients to contribute and allowing patients to participate in the scoping protocol development or review (22% for both), and collecting patients' perspectives through patient submissions or direct consultation, allowing patients to participate at assessment meeting, technical tables or working groups, presenting the patient submissions or testimonies to the appraisal committee, allowing patients to review the draft recommendations report, and producing easy to read summaries of HTA reports (17% for all of them). Further details can be found in Figure 8.
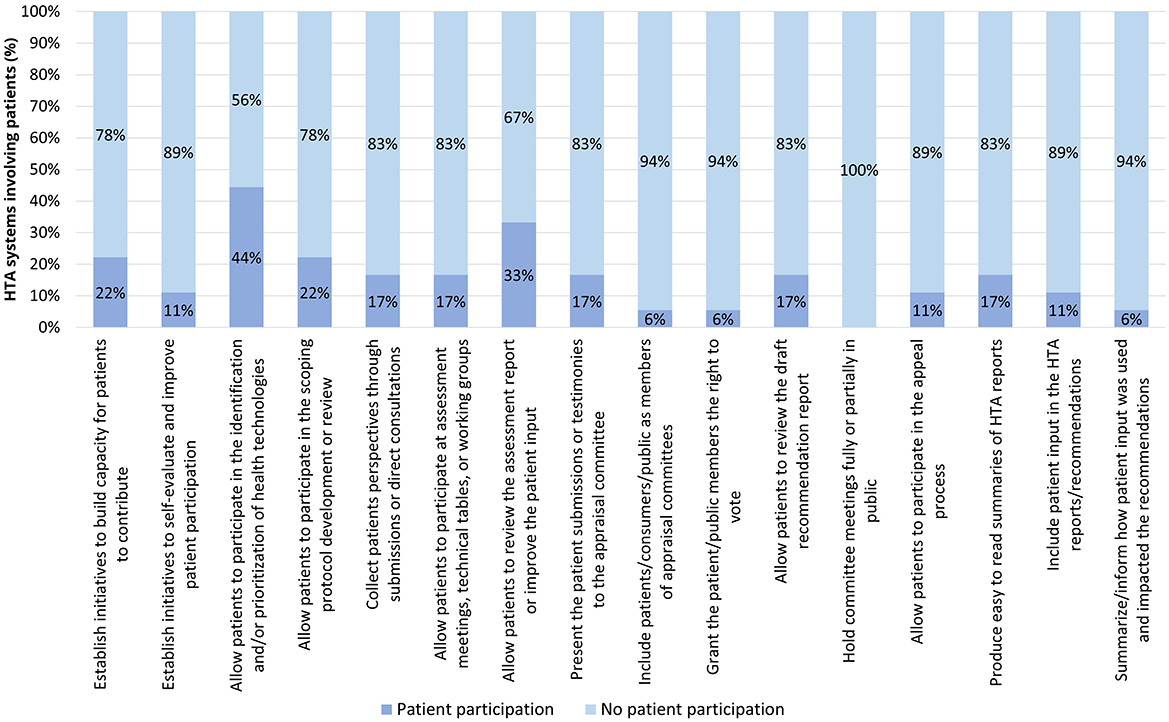
Figure 8. Occurrence of patient participation per variable across Tier 4 HTA systems.
4 Discussion
While previous articles have described and compared patient participation within HTA systems (6, 17, 19–26), to our knowledge, this publication, though limited to publicly available information, represents the first comprehensive, structured, comparative review and ranking of HTA systems worldwide focusing on the breadth and depth of patient participation in their HTA processes.
There are prior attempts to classify patient participation in HTA (18). The framework developed by Gauvin, for example, emphasized the type of participant, the stage of the HTA process, and the levels of involvement, while the range of specific participation mechanisms received less attention. In contrast, our framework placed priority on these mechanisms (e.g., submission of input, patient membership, voting rights), as we considered them central to understanding how participation is operationalized. While inspired by existing models and comparisons, we therefore developed a new framework tailored to this objective. In addition, our evaluation incorporated a quantitative scoring approach. Such measures can facilitate standardized cross-country comparisons, enhance HTA processes, promote accountability and transparency, empower patient advocacy groups to argue for stronger involvement, and support evidence- based policymaking.
In the context of our ranking of the HTA systems, the two systems in Tier 1 (NICE in England and Wales and CDA-AMC in Canada) and some Tier 2 HTA systems (e.g., MSAC and PBAC in Australia, SMC in Scotland, IQWIG and G-BA in Germany) have previously garnered recognition for their substantial efforts in integrating patient participation throughout their HTA processes (6, 11, 15, 17, 25). This reaffirms their status as exemplary cases of patient participation within HTA systems. In contrast, other Tier 2 ranked systems, such as HAS in France, DMC and DHTC in Denmark, or ICER in the United States, represent more recent developments in terms of patient participation. In general, best practice examples are characterized by a substantial breadth and depth of patient participation throughout the HTA process, utilizing a variety of participation mechanisms and leveraging them meaningfully. These HTA systems notably engage the patient community, either in conjunction with or distinct from the broader public or citizenry.
It is worth noting that the top performing HTA systems overall may not excel in all phases. For example, NICE, while ranked 1st overall, falls to the 5th group in the assessment phase–a category led by G-BA (ranked 5th overall) and CONETEC (ranked 16th overall) in Argentina. This could be attributed to various factors, such as the diversity of HTA processes and the resulting opportunities for participation in each phase.
Our results show that 92.86% of all HTA systems analyzed incorporate some sort of patient and/or public participation, a higher figure than previously reported studies, which range from 50 to 81% (32–34). This discrepancy may be due to our inclusion of both patient and public participation, as well as participation in HTAs for both pharmaceuticals and medical devices, whereas previous studies often separated these categories, possibly resulting in lower figures. Other factors such as the increasing trend of patient participation in HTA (4, 7), differences in the sample of HTA systems analyzed, or the variables used to assess participation, may also explain this difference. However, despite this high participation rate, when considering that only 28.57% fall into Tier 1 or Tier 2, and that the average score for the entire set of HTA systems is 3.61, there appears to be substantial room for global improvement in the depth of patient participation, as highlighted in the literature (4, 7, 8). This gap between the breadth and depth of patient participation might be explained by several reasons, such as HTA systems still considering patient participation as an optional extra rather than a vital component and considering patient participation as a “token” activity (7). The variability in patient participation among HTA systems can be attributed to multiple causes. For instance, some articles have underscored barriers to patient participation in HTA, such as the need for resources, limited patient understanding of the HTA process, administrative burdens and delays, and a lack of knowledge on how to effectively utilize patient input (6, 17). Additionally, the specific context of individual countries, including national administrative traditions and the characteristics of healthcare and HTA systems, has been identified as a challenge to the transferability of patient participation practices and guidelines from one country to another (5, 35). Finally, given that HTA is relatively recent in certain regions such as in Asia or Africa (36, 37), the time between the establishment of the HTA system and the initiation of patient involvement may also impact the degree of patient participation, necessitating further investigation.
In terms of patient participation across the phases of the HTA process, our results, indicating that 19.6% of HTAs involve the patient community in all phases, regardless of the level of participation, align to some extent with international comparisons (34). That study also underscores patient participation at every phase of HTA, but discrepancies in methodologies used by this and other articles hinder a direct comparison of the results with our research. The elevated occurrence of participation during the assessment and appraisal phases, as identified in our research, may be attributed to factors such as the perceived significance of these phases in the overall HTA process, a tendency to involve patients later in the evaluation process, increased opportunities for participation, or a tendency to engage patients when recommendations are made. Nonetheless, further exploration and standardization of methodologies in future studies could contribute to a more comprehensive understanding of patient participation across phases.
According to our findings and supported by previous studies (17, 19–21), patient participation is incorporated through a variety of mechanisms during the HTA process, one of the most common being the participation of the public or patients as members of appraisal committees. This might be indicative of the increasing level of patient participation, given the recognized relevance of this mode of participation (17). In contrast, the least common mechanism of participation is reporting how patient input was used and impacted HTA recommendations. This finding aligns with previous studies (4, 6, 22, 38), suggesting that, despite the evident trend toward involving the patient community, the actual influence of patients on decision-making remains unclear.
When analyzing HTA systems by region and their distribution in tiers and average scores, it should be noted that the varying number of systems assessed per region can make it challenging to draw broad conclusions.
Although Oceania had the highest average score, only three systems were analyzed. The MSAC and PBAC in Australia are noteworthy examples of effective patient and public involvement in HTA. Ranked 3rd and 7th, respectively, these systems actively engage the consumer community throughout the HTA process. They allow consumer nominations for technology evaluation, invite input through open calls, include consumers as members in assessment teams and appraisal committees, and consumer input is summarized in public documents, demonstrating a commitment to transparency and inclusivity. In the scoping phase, MSAC takes an additional step by including a consumer member in the scoping team.
In North America, which had the second highest average, a few national systems stand out, while the regional systems analyzed involve the patient community to a lesser but growing degree. CDA-AMC, ranked 2nd, showcases a comprehensive commitment to engaging the public and, notably, the patient community throughout the entire HTA process (6). Patient groups are encouraged to contribute information to submissions early in the HTA process, and patient representatives serve as members on appraisal committees. CDA-AMC extends support through guidance, training, travel awards, and access to a specialized team, and regularly evaluates and refines its processes, placing significant value on the feedback provided by stakeholders. An example of an emerging case is ICER in the US, ranked 8th. In 2020, ICER initiated a Patient Engagement Program, and although it is of recent creation, it already reflects a strong commitment to patient participation within its framework (39).
In Europe, the larger number of systems assessed might explain the even distribution across tiers, coming in 3rd place in terms of average score. Notably, NICE and SMC, secured the 1st and 4th rankings, respectively, showcasing exemplary systems. NICE is globally recognized for the comprehensive involvement of the public and patient community throughout the entire HTA process. It incorporates diverse perspectives, offers extensive support through its Patient Participation Program, and actively seeks feedback and implements self-evaluation strategies to continuously improve patient participation. Similarly, SMC actively encourages patient contribution, facilitating participation through a dedicated Public Participation Team, submission templates, and a user-friendly website. Improvements have been seen in certain HTA systems, such as HAS (ranked 10th), DHTC and DMC (ranked 9th and 11th), or KCE-INAMI/RIZIV in Belgium (ranked 33rd). HAS, for example, began involving the patient community in 2016, developing an online contribution process, including patient representatives as voting members in appraisal committees, and publicly disclosing a comprehensive self-evaluation of their user/citizen participation methods. In contrast, AIHTA in Austria, despite having expressed intentions to involve patients, it showed limited evidence of patient participation (40). Importantly, HTA in Europe is undergoing significant changes toward more unified market access, particularly through the introduction of the Joint Clinical Assessment (JCA). JCA will centralize the clinical evidence assessment phase at the European level, and consequently, patient involvement in this phase will be coordinated at the European level. However, since the appraisal phase will remain the responsibility of individual countries, patient involvement in this phase will vary depending on national policies. This evolving framework highlights the importance of updating our study to align with these changes.
Latin America, where only a few HTA systems were analyzed, placed fourth in terms of average score. As reflected in both our study results and previous literature (41), although patient and public participation is generally lacking, notable examples exist, including CONITEC (ranked 13th) in Brazil and CONETEC (ranked 15th) in Argentina. CONITEC, recognized in the literature (41–43), allows technology nominations, patient submissions, and participation during appraisal committee meetings. However, testimonials suggest that patient participation may be insufficient (44). CONETEC also firmly incorporates patient participation, especially in the assessment phase, including an open call for disease experience submissions, a patient panel guiding technical teams, or appointing patient representatives in technical teams. In Colombia, while patients play a significant role in the development of clinical guidelines by the IETS, patient participation in HTA is less prominent (41, 45).
In Asia, HTA adoption has been historically low, and has grown considerably over the last two decades, which may contribute to the current scarcity of patient participation, as indicated by both average scores and the HTA systems distribution across tiers (36). Two cases that incorporate patient participation are the HSPI in the Philippines and NIHTA in Taiwan, ranked 20th and 25th, respectively. HSPI includes patient and public participation primarily through consultations conducted throughout the HTA process. Moreover, a citizen's representative holds a voting position in the appraisal committee. NIHTA conducts an open call for information submissions by patients and patient groups, and patient representatives can participate in committee meetings (6). In Thailand (ranked 40th), while HITAP initiated patient participation as early as 2009 and introduced patient participation guidance in 2012 (6, 46), its ranking reflects our understanding that implementation is limited. Currently, patients participate in the identification and prioritization phase and provide input during the scoping and assessment phases. Although HTA agencies in Asia are relatively new, HTA is gaining recognition. Moreover, valuable initiatives have emerged, notably HTAsiaLink, a network established in 2011 to strengthen HTA capacity in Asia, with patient involvement being one of their topics of discussion. Consequently, we anticipate a growth in patient participation (47).
A key lesson from higher-ranked HTA systems is that strong patient participation requires both breadth and depth: mechanisms must be available across all phases of the HTA process, and they must go beyond symbolic consultation to provide patients with structured, influential roles. Exemplary systems, such as NICE in the United Kingdom, or CDA-AMC in Canada, combine multiple layers of engagement, from early identification of topics to voting rights on appraisal committees, supported by dedicated resources such as patient engagement teams, training programs, and feedback mechanisms that show how patient input was used. By contrast, lower-ranked systems often limit participation to later phases or to isolated mechanisms (e.g., open consultations without follow-up), which risks tokenism and undermines trust. For policymakers, the implication is clear: institutionalizing patient participation effectively requires embedding participation structurally (e.g., committee membership, voting rights), procedurally (e.g., systematic calls for input, dedicated capacity-building for patient groups), and in terms of transparency (e.g., public reporting on how input influenced recommendations).
In this study, the term “patient participation” was used broadly to include both patients and the general public. While public involvement can sometimes capture elements of the patient voice, it is not equivalent to direct patient input, and this approach may overestimate the true extent of patient participation. For example, the inclusion of citizen representatives on committees or open public consultations does not necessarily ensure that the lived experiences and specific needs of patients with the condition under evaluation are represented. We adopted this inclusive definition to avoid overlooking mechanisms that contribute to legitimacy and transparency, but acknowledge that future research should distinguish more clearly between patient and public involvement.
Future research should incorporate structured validation with local experts and stakeholders, and explore consensus methods such as Delphi panels to refine weighting schemes. This would increase reproducibility and alignment with international initiatives on patient involvement in HTA.
5 Conclusion
In conclusion, this paper represents a significant effort in the field of international HTA by offering a structured and comparative review of HTA systems worldwide, focusing on patient participation. Patient participation in HTA is crucial, as it brings valuable perspectives to the forefront, making healthcare coverage decisions more patient-centered and equitable.
Our findings reveal variety in practices across regions and tiers, with some systems setting examples in patient participation, while others are on a journey of development, highlighting room for improvement globally.
While our study found that most HTA systems include some level of patient or public participation, the average scores across countries and their distribution in ranking tiers suggest a generally low depth of patient involvement in these programs worldwide. As HTA evolves, we anticipate greater patient impact and a more even distribution of systems across ranking tiers.
This study serves as a foundation for further research and as a point of reference for HTA systems looking to strengthen their patient engagement initiatives. Continuous improvement is key to ensuring that HTA processes worldwide are not only rigorous but also patient-centered, ultimately contributing to more informed, fair, and patient-focused healthcare decisions.
Considering that both HTA and patient participation in it are gaining recognition worldwide, updating our study accordingly would be beneficial.
6 Limitations
This research has certain limitations that could influence the comprehensiveness of the data and scoring for HTA systems. Chief among these was that data collection relied exclusively on secondary research, with no primary research or systematic surveys conducted. The availability and detail of information vary across systems, potentially leading to over- or under-representation due to publication bias. This raises concerns about accessibility, as experts might struggle to find data, indicating potential challenges for the general public and patients. Moreover, because the study relied exclusively on desk research, the findings have not been verified with HTA bodies or local experts. Such validation would be important in future work to reduce the risk of omissions or misclassifications and to strengthen the robustness of comparisons across systems.
Language barriers also posed a limitation, with non-English literature likely under-represented in databases like PubMed. The ability of the study team to conduct searches in local languages or access grey literature was limited.
There is also a significant degree of heterogeneity in the structure and processes of the HTA systems analyzed in this study. In particular, it was sometimes difficult to partition the HTA process into distinct phases, mapping the procedures of specific bodies to these phases, and identifying the various bodies comprising an HTA system, particularly in cases where more than one body is involved.
In addition, the scoring system did not distinguish between a lack of patient participation and a lack of information on patient participation. Additionally, the scoring system considered the frequency of patient participation, but inconsistencies in reporting could have influenced scores. It was sometimes unclear whether patient participation was representative of typical practice or limited to specific assessments.
Distinguishing between implemented and planned patient participation was another challenge, potentially affecting the accuracy of our assessment. Finally, there is no consensus on measuring patient participation in HTA, and our methodology represents just one perspective, with the variables used not encompassing all possible forms of involvement.
An additional limitation lies in the subjectivity of the weighting system applied to participation activities. While conceptually grounded in the depth, influence, and transparency of each activity, the assignment of Low, Medium, High, or Very High weights was not externally validated (for instance through a Delphi panel or stakeholder consultation). This introduces an element of judgement that could affect reproducibility if applied by other reviewers.
Finally, our inclusive definition of patient participation, which also encompassed broader public involvement, may have inflated estimates of actual patient input.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
MP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. LK-G: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing. LT: Conceptualization, Project administration, Supervision, Validation, Writing – review & editing, Methodology, Visualization. AD: Conceptualization, Project administration, Supervision, Validation, Writing – review & editing. NB: Conceptualization, Project administration, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
LT was employed by Alira Health Srl.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1693886/full#supplementary-material
References
1. Ramponi F, Twea P, Chilima B, Nkhoma D, Kazanga Chiumia I, Manthalu G, et al. Assessing the potential of HTA to inform resource allocation decisions in low-income settings: the case of Malawi. Front Public Health. (2022) 10:1010702. doi: 10.3389/fpubh.2022.1010702
2. Overview - European Commission. (n.d.). Available online at: https://health.ec.europa.eu/health-technology-assessment/overview_en#documents (Accessed April 19, 2024).
3. Wang Y, Rattanavipapong W, Teerawattananon Y. Using health technology assessment to set priority, inform target product profiles, and design clinical study for health innovation. Technol Forecast Soc Change. (2021) 172:121000. doi: 10.1016/j.techfore.2021.121000
4. Gagnon MP, Tantchou Dipankui M, Poder TG, Payne-Gagnon J, Mbemba G, Beretta V. Patient and public involvement in health technology assessment: update of a systematic review of international experiences. Int J Technol Assess Health Care. (2021) 37:e38. doi: 10.1017/S0266462321000064
5. Dimitrova M, Jakab I, Mitkova Z, Kamusheva M, Tachkov K, Nemeth B, et al. Potential barriers of patient involvement in health technology assessment in central and eastern European countries. Front Public Health. (2022) 10:922708. doi: 10.3389/fpubh.2022.922708
6. Mesana L, Syed I, Constantin J, Tardivel C, Wang X, Pruce D, et al. Patient involvement in health technology assessments: an international comparison. Value Health. (2018) 21:S54. doi: 10.1016/j.jval.2018.07.407
7. Werkö SS, Staniszewska S. Patient and public involvement in health technology assessment: a new dawn? Int J Technol Assess Health Care. (2021) 37:e38. doi: 10.1017/S0266462321000234
8. Wale JL, Thomas S, Hamerlijnck D, Hollander R. Patients and public are important stakeholders in health technology assessment but the level of involvement is low – a call to action. Res Involv Engagem. (2021) 7:52. doi: 10.1186/s40900-020-00248-9
9. Facey K, Boivin A, Gracia J, Hansen HP, Lo Scalzo A, Mossman J, et al. Patients' perspectives in health technology assessment: a route to robust evidence and fair deliberation. Int J Technol Assess Health Care. (2010) 26:334–40. doi: 10.1017/S0266462310000395
10. Abelson J, Wagner F, DeJean D, Boesveld S, Gauvin FP, Bean S, et al. Public and patient involvement in health technology assessment: a framework for action. Int J Technol Assess Health Care. (2016) 32:256–64. doi: 10.1017/S0266462316000362
11. Wale J, Scott AM, Hofmann B, Garner S, Low E, Sansom L. Why patients should be involved in health technology assessment. Int J Technol Assess Health Care. (2017) 33:467–73. doi: 10.1017/S0266462317000241
12. Hailey D. Involvement of patients in health technology assessment: further perspectives for informing decision-makers HPR hospital practices and research. Hosp Pract Res. (2017) 2:58–62. doi: 10.15171/hpr.2017.16
13. Bertelsen N, Oehrlein E, Lewis B, Westrich-Robertson T, Elliott J, Willgoss T, et al. Patient engagement and patient experience data in regulatory review and health technology assessment: where are we today? Ther Innov Regul Sci. (2025) 59:737–52. doi: 10.1007/s43441-025-00770-6
14. Belgaied W, Fourati W, Caban A. HTA247 impact of patient and clinician engagement (PACE) meetings on Scottish medicines consortium recommendations. Value Health. (2024) 27:S403. doi: 10.1016/j.jval.2024.10.2072
15. Norburn L, Thomas L. Expertise, experience, and excellence. Twenty years of patient involvement in health technology assessment at NICE: an evolving story. Int J Technol Assess Health Care. (2020) 36:432–38. doi: 10.1017/S0266462320000860
16. Lopes SGP, Luiza VL, da Silva RM. Reversal of the recommendations issued by the National Commission for the Incorporation of Technologies in SUS after Public Consultations. Cien Saude Colet. (2023) 28:561–73.
17. Facey K, Single ANV, Hansen HP. Patient Involvement in Health Technology Assessment. Singapore: Springer (2017). Available online at: https://www.research.ed.ac.uk/en/publications/patient-involvement-in-hta (Accessed April 19, 2024).
18. Gauvin FP, Abelson J, Giacomini M, Eyles J, Lavis JN. “It all depends”: conceptualizing public involvement in the context of health technology assessment agencies. Soc Sci Med. (2010) 70:1518–26. doi: 10.1016/j.socscimed.2010.01.036
19. Menon D, Stafinski T. Role of patient and public participation in health technology assessment and coverage decisions. Expert Rev Pharmacoecon Outcomes Res. (2011) 11:75–8. doi: 10.1586/erp.10.82
20. Weeks L, Polisena J, Scott AM, Holtorf AP, Staniszewska S, Facey K. Evaluation of patient and public involvement initiatives in health technology assessment: a survey of international agencies. Int J Technol Assess Health Care. (2017) 33:715–23. doi: 10.1017/S0266462317000976
21. Scott AM, Wale JL. Patient advocate perspectives on involvement in HTA: an international snapshot. Res Involv Engagem. (2017) 3:2. doi: 10.1186/s40900-016-0052-9
22. Single A, Cabrera A, Fifer S, Tsai J, Paik JY, Hope P. Patient advocacy group involvement in health technology assessments: an observational study. Res Involv Engagem. (2021) 7:79. doi: 10.1186/s40900-021-00327-5
23. Single ANV, Facey KM, Livingstone H, Silva AS. Stories of patient involvement impact in health technology assessments: a discussion paper. Int J Technol Assess Health Care. (2019) 35:266–72. doi: 10.1017/S0266462319000552
24. Kreis J, Schmidt H. Public engagement in health technology assessment and coverage decisions: a study of experiences in France, Germany, and the United Kingdom. J Health Polit Policy Law. (2013) 38:89–122. doi: 10.1215/03616878-1898812
25. Dinboeck M, Noopur N, Kumari C. Patient involvement in regulatory and HTA processes: a call for enhanced alignment patient involvement with regulators in decision making. Value Health. (2022) 25:S423. doi: 10.1016/j.jval.2022.09.2104
26. Nabarette H, Chastenay MH, Dupont JCK, Ganache I, Single ANV. Patient and citizen participation at the organizational level in health technology assessment: an exploratory study in five jurisdictions. Int J Technol Assess Health Care. (2023) 39:e41. doi: 10.1017/S0266462323000417
27. Gagnon MP, Candas B, Desmartis M, Gagnon J, Roche D, La Rhainds M, et al. Involving patient in the early stages of health technology assessment (HTA): a study protocol. BMC Health Serv Res. (2014) 14:273. doi: 10.1186/1472-6963-14-273
28. Hunter A, Facey K, Thomas V, Haerry D, Warner K, Klingmann I, et al. EUPATI guidance for patient involvement in medicines research and development: health technology assessment. Front Med. (2018) 5:231. doi: 10.3389/fmed.2018.00231
29. Anke Peggy Holtorf NB. Patient Involvement in HTA in Europe: Recommendations From a 360o Perspective View of Current Patient Involvement Practices. (2023) Available online at: https://healthtai.sharepoint.com/sites/IGWebsiteContent/Shared%20Documents/Forms/AllItems.aspx?id=%2Fsites%2FIGWebsiteContent%2FShared%20Documents%2FPatient%20and%20Citizen%20Involvement%2FResources%20%26%20Materials%2F9%5FOTHER%20USEFUL%20RESOURCES%2F360%2DHTAi%2DPCIG%2DResearch%2Din%2DPatient%2DInvolvement%2DPractices%2Din%2DHTA%2Din%2DEurope%2DOct%2D2%2Epdf&parent=%2Fsites%2FIGWebsiteContent%2FShared%20Documents%2FPatient%20and%20Citizen%20Involvement%2FResources%20%26%20Materials%2F9%5FOTHER%20USEFUL%20RESOURCES&p=true&ga=1 (Accessed September 24, 2025).
30. HTAi. Introduction to Health Technology Assessment (HTA). (2013). Available online at: https://healthtai.sharepoint.com/sites/IGWebsiteContent/Shared%20Documents/Forms/AllItems.aspx?id=%2Fsites%2FIGWebsiteContent%2FShared%20Documents%2FPatient%20and%20Citizen%20Involvement%2FResources%20%26%20Materials%2F1%5FGetting%20Started%2FPCISG%2DResource%2DIntro%5Fto%5FHTA%5F%5FKFacey%5F%5FJun13%2Epdf&parent=%2Fsites%2FIGWebsiteContent%2FShared%20Documents%2FPatient%20and%20Citizen%20Involvement%2FResources%20%26%20Materials%2F1%5FGetting%20Started&p=true&ga=1 (Accessed September 24, 2025).
31. Goodman CS. HTA 101 Introduction to Health Technology Assessment. (2004). p. 33–4. Available online at: https://www.inahta.org/wp-content/uploads/2014/09/HTA-101_Goodman_2004.pdf (Accessed August 5, 2025).
32. Whitty JA. An international survey of the public engagement practices of health technology assessment organizations. Value Health. (2013) 16. doi: 10.1016/j.jval.2012.09.011
33. European Patients' Forum (EPF). Patient Involvement in Health Technology Assessment in Europe: Results of the EPF Survey. (2013) Available online at: https://www.eu-patient.eu/globalassets/projects/hta/hta-epf-final-report2013.pdf (Accessed May 8, 2024).
34. EUnetHTA. An Analysis of HTA and Reimbursement Procedures in EUnetHTA Partner Countries. (2018). Available online at: https://web.archive.org/web/20241025184141/https://www.msac.gov.au/internet/msac/publishing.nsf/ (Accessed May 5, 2024).
35. Cavazza M, Jommi C. Stakeholders involvement by HTA organisations: why is so different? Health Policy. (2012) 105:236–45. doi: 10.1016/j.healthpol.2012.01.012
36. Liu G, Wu EQ, Ahn J, Kamae I, Xie J, Yang H. The development of health technology assessment in Asia: current status and future trends. Value Health Reg Issues. (2020) 21:39–44. doi: 10.1016/j.vhri.2019.08.472
37. Hollingworth S, Fenny AP, Yu SY, Ruiz F, Chalkidou K. Health technology assessment in sub-Saharan Africa: a descriptive analysis and narrative synthesis. Cost Eff Resour Alloc. (2021) 19:1–13. doi: 10.1186/s12962-021-00293-5
38. Mason RJ, Searle KM, Bombard Y, Rahmadian A, Chambers A, Mai H, et al. Evaluation of the impact of patient involvement in health technology assessments: a scoping review. Int J Technol Assess Health Care. (2020) 36:217–23. doi: 10.1017/S0266462320000239
39. Institute for Clinical and Economic Review. Our History & Impact. (2023). Available online at: https://icer.org/who-we-are/history-impact/ (Accessed May 8, 2024).
40. Fried A, Wild C. Involvement of Citizens and Patients in HTA Processes. International Experiences and Good Practice Examples. LBI-HTA Project Report No.: 86; 2016. Vienna: Ludwig Boltzmann Institute for Health Technology Assessment [in German] (2016). Available online at: https://eprints.aihta.at/1088/1/HTA-Projektbericht_Nr.86.pdf (Accessed May 6, 2024).
41. Pichon-Riviere A, Soto N, Augustovski F, Sampietro-Colom L. Stakeholder involvement in the health technology assessment process in Latin America. Int J Technol Assess Health Care. (2018) 34:248–53. doi: 10.1017/S0266462318000302
42. de Freitas Lopes AC, Novaes HMD, de Soárez PC. Patient and public involvement in health technology decision-making processes in Brazil. Rev Saude Publica. (2020) 54:1–10. doi: 10.11606/s1518-8787.2020054002453
43. Carvalho VKDS, De Sousa MSA, Barreto JOM, Da Silva EN. Public engagement in health technology assessment in Brazil: the case of the Trastuzumab public consultation. BMC Health Serv Res. (2019) 19:1–11. doi: 10.1186/s12913-019-4555-6
44. Health Technology Assessment International - HTAi. How Patient Involvement is Making a Difference in HTA Perspectives of Impact. (2022). Available online at: https://www.youtube.com/watch?v=eEA-RaN3StY&list=LL&index=499&t=2490s (Accessed May 3, 2024).
45. Rivera DE, Fernández EC, Rengifo AM, Instituto de Evaluación Tecnológica en Salud. Manual de Participación y Deliberación. Bogotá D.C.: IETS (2014). Available online at: https://www.iets.org.co/Archivos/65/Manual%20Participacion.pdf (Accessed May 4, 2024). Spanish.
46. Velasco RP, Chaikledkaew U, Youngkong S, Tantivess S, Teerawattananon Y. Health Technology Assessment Process Guidelines for Use at the Health Intervention and Technology Assessment Program. (2012). Available online at: https://www.hitap.net/wp-content/uploads/2014/09/health_technology_assessment_process_guidelines_english_finalversion_01march2012.pdf (Accessed May 5, 2024).
47. HTAsiaLink. (2017). Available online at: https://htasialink.org/ (Accessed May 9, 2024).
48. Spanish Agency for Medicines and Medical Devices [in Spanish]. (n.d.). Available online at: https://www.aemps.gob.es/?lang=en (Accessed April 26, 2024).
49. Badia X, Vico T, Shepherd J, Gil A, Poveda-Andrés JL, Hernández C. Impact of the therapeutic positioning report in the P&R process in Spain: analysis of orphan drugs approved by the European Commission and reimbursed in Spain from 2003 to 2019. Orphanet J Rare Dis. (2020) 15:1–13. doi: 10.1186/s13023-020-01507-4
50. Marina C, Annamaria A, Cavallo V, Chiarolla A, Corio E, Gillespie M, et al. HTA Procedures Manual [in Italian]. (2018). Available online at: https://www.agenas.gov.it/images/agenas/hta/Manuale_delle_procedure_HTA_def_20.9.2018_full.pdf (Accessed May 7, 2024).
51. European Network for Health Technology Assessment (EUnetHTA). An Analysis of HTA and Reimbursement Procedures in EUnetHTA Partner Countries: Final Report. (2017) Available online at: https://www.eunethta.eu/wp-content/uploads/2018/02/WP7-Activity-1-Report.pdf (Accessed May 8, 2024).
52. Italian Medicines Agency. Regulation on the Organization and Functioning of the Technical and Scientific Advisory Committee and the Pricing and Reimbursement Committee [in Italian]. (2024). Available online at: https://www.aifa.gov.it/documents/20142/2323301/Regolamento_CSE_17.04.2024.pdf (Accessed May 7, 2024).
53. Italian Medicines Agency. Guidelines for Compiling the Dossier in Support of the Application for Reimbursement and Pricing of a Medicinal Product [in Italian]. (2020). Available online at: https://www.aifa.gov.it/documents/20142/1283800/Linee_guida_dossier_domanda_rimborsabilita.pdf (Accessed May 7, 2024).
54. Zozaya N, Villaseca J, Abdalla F, Fernández I, Hidalgo-Vega Á. The Evaluation and Financing Process of Medications in Spain: Where are We and Where are We Going? [in Spanish]. Weber (2022). Available online at: https://weber.org.es/wp-content/uploads/2022/07/Informe-Proceso-Evaluacion-y-Financiacion-Medicamentos-Weber.-Julio-2022.pdf (Accessed May 7, 2024).
55. Austrian Institute for Health Technology Assessment. Patient Involvement in HTA Processes [in German]. (2016). Available online at: https://aihta.at/page/patientenbeteiligung/de (Accessed May 6, 2024).
56. Austrian Institute for Health Technology Assessment. Manual of Methods for Health Technology Assessment [in German]. (2012). Available online at: https://aihta.at/uploads/tableTool/UllCmsPage/gallery/methodenhandbuch-aihta1.pdf (Accessed May 6, 2024).
57. Agency for Health Technology Assessment and Tariff System. Detailed Training Curriculum for Training Offered as Part of the Project “Rational Decisions in the Healthcare System, with Particular Reference to the Regional Health Policy” [in Polish]. (2018). Available online at: https://www.aotm.gov.pl/wp-content/uploads/2020/07/Program_szkolenia_POWER.pdf (Accessed April 26, 2024).
58. Agency for Health Technology Assessment and Tariff System. Training/Materials [in Polish]. (n.d.). Available online at: https://www.aotm.gov.pl/en/for-patients/training-materials/ (Accessed April 26, 2024).
59. Agency for Health Technology Assessment and Tariff System. Transparency Council [in Polish]. (2024). Available online at: https://bipold.aotm.gov.pl/index.php/rada-przejrzystosci/5619-rada-p (Accessed May 3, 2024).
60. Agency for Health Technology Assessment and Tariff System. Participation in Transparency Council Meetings [in Polish]. (n.d.). Available online at: https://www.aotm.gov.pl/en/for-patients/participation-in-transparency-council-meetings/ (Accessed May 3, 2024).
61. Agency for Health Technology Assessment and Tariff System. Transparency Council [in Polish]. (n.d.). Available online at: https://www.aotm.gov.pl/en/about-us/transparency-council/ (Accessed May 3, 2024).
62. Lach K, Dziwisz M, Rémuzat C, Toumi M. Towards a more transparent HTA process in Poland: new Polish HTA methodological guidelines. J Mark Access Health Policy. (2017) 5:1355202. doi: 10.1080/20016689.2017.1355202
63. Wranik WD, Zielińska DA, Gambold L, Sevgur S. Threats to the value of Health Technology Assessment: qualitative evidence from Canada and Poland. Health Policy. (2019) 123:191–202. doi: 10.1016/j.healthpol.2018.12.001
64. Agency for Health Technology Assessment and Tariff System. Health Technology Assessment Guidelines [in Polish]. (2016). Available online at: https://www.aotm.gov.pl/wp-content/uploads/2020/07/20160913_Wytyczne_AOTMiT.pdf (Accessed May 3, 2024).
65. Agency for Health Technology Assessment and Tariff System. Regulations of the Work of the Tariff Council Operating Under the President of the Agency for Health Technology Assessment and Tarification of September 30, 2020 [in Polish]. (2020). Available online at: https://bipold.aotm.gov.pl/assets/files/taryfikacja/Regulaminy/regulamin_pracy_rdst_projekt_pos_zdalne_20201002.pdf (Accessed May 3, 2024).
66. Catalan Health Service. Evaluation Procedure for Part of the Pharmacotherapeutic Harmonization Program [in Spanish]. (2024). Available online at: https://catsalut.gencat.cat/web/.content/minisite/catsalut/proveidors_professionals/medicaments_farmacia/harmonitzacio/normativa/procedimiento-programa-armonizacion-2024.pdf (Accessed May 3, 2024).
67. Catalan Health Service. Pharmacotherapeutic Harmonization Program [in Catalan]. (2017). Available online at: https://scientiasalut.gencat.cat/bitstream/handle/11351/2965/catsalut_instruccio_05_2017.pdf?sequence=1&isAllowed=y (Accessed May 3, 2024).
68. Diariofarma. Evaluation Procedure Part of the Pharmacotherapeutic Harmonization Program (PAF) of CatSalut [In Spanish]. (2018). Available online at: https://diariofarma.com/2018/06/17/procedimiento-de-evaluacion-por-parte-del-programa-de-armonizacion-farmacoterapeutica-paf-del-catsalut (Accessed May 3, 2024).
69. Unified Regional Coordination on Pharmaceuticals - Veneto Region [in Italian]. (n.d.). Available online at: https://web.archive.org/web/20170619085208/https://www.regione.veneto.it/web/sanita/coordinamento-regionale-sul-farmaco (Accessed May 6, 2024).
70. Cerbo M CAAALSACMPMCA, FAFC. Investigation on Health Technology Assessment Activities in Italy - National Agency for Regional Health Services and Italian Society by HTA Rome [in Italian]. (2016). Available online at: https://www.quotidianosanita.it/allegati/allegato909462.pdf (Accessed May 6, 2024).
71. Danish Health Technology Council. Procedural Framework for the Danish Health Technology Council. (2021). Available online at: https://behandlingsraadet.dk/media/en5nsj02/procedural-framework-for-the-danish-health-technology-council.pdf (Accessed May 3, 2024).
72. Danish Health Technology Council. The Specialist Committees [in Danish]. (n.d.). Available online at: https://behandlingsraadet.dk/om-behandlingsradet/fagudvalgene (Accessed May 3, 2024).
73. Danish Health Technology Council. The Danish Health Technology Council's Process Guide. (2021). Available online at: https://behandlingsraadet.dk/media/2tubtbn2/the-danish-health-technology-council-s-process-guide.pdf (Accessed May 3, 2024).
74. Danish Medicines Council. Involvement of Patients in Specialist Committees [in Danish]. (n.d.). Available online at: https://medicinraadet.dk/om-os/fagudvalg/inddragelse-af-patienter-i-fagudvalg (Accessed May 3, 2024).
75. Danish Medicines Council. Information for Patients/Patient Representatives About the Medical Council's Specialist Committee [in Danish]. (n.d.). Available online at: https://medicinraadet.dk/om-os/fagudvalg/patientrepraesentant-i-fagudvalg (Accessed May 3, 2024).
76. Danish Medicines Council. The Advice [in Danish]. (n.d.). Available online at: https://medicinraadet.dk/om-os/radet (Accessed May 3, 2024).
77. Danish Medicines Council. Process and Methods Guide – How the Danish Medicines Council Develops Joint Regional Assessments of the Added Clinical Value of New Medicines and New Indications Version 1.1. (2017). Available online at: https://medicinraadet.dk/media/re5gfbp5/process-and-methods-guide-join-regional-assessment-of-the-clinical-added-value-of-new-medicines-and-indications-002_adlegacy.pdf (Accessed May 3, 2024).
78. Danish Medicines Council. The Danish Medicines Council's Process Guide for Assessing New Pharmaceuticals. (2022). Available online at: https://medicinraadet.dk/media/ckyg1cde/the-danish-medicines-councils-process-guide-for-assessing-new-pharmaceuticals-version-1-2.pdf (Accessed May 3, 2024).
79. Hansen HP, Lee A, Van Randwijk CB. Patient aspects: a review of fifty-eight Danish HTA reports. Int J Technol Assess Health Care. (2011) 27:330–6. doi: 10.1017/S0266462311000535
80. Sigmund H, Kristensen FB. Health technology assessment in Denmark: strategy, implementation, and developments. Int J Technol Assess Health Care. (2009) 25 Suppl 1(SUPPL.S1):94–101. doi: 10.1017/S0266462309090485
81. Ingrid Wilbacher M. Umbrella Association of Austrian Social Insurance Institutions [in German]. (2021). Available online at: https://www.lisavienna.at/fileadmin/user_upload/LISAvienna/Files_News/BT_Medtech_Regulatory_2021/B1_HTA_und_Innovationen_in_der_Sozialversicherung_Dachverband_Ingrid_Wilbacher.pdf (Accessed May 6, 2024).
82. Umbrella Association of Social Insurance Institutions. Welcome to the Austrian social Insurance Portal [in German]. (2024). Available online at: https://www.sozialversicherung.at/cdscontent/?contentid=10007.821628&portal=svportal (Accessed May 6, 2024).
83. Choices in Health Care. Recommendations, Criteria and Statements - Choices in Health Care. (n.d.). Available online at: https://palveluvalikoima.fi/en/recommendations-and-statements (Accessed May 7, 2024).
84. Council for Choices in Health Care in Finland. Recommendation of the Council for Choices in Health Care in Finland (PALKO/COHERE Finland). (2020). Available online at: https://segm.org/sites/default/files/Finnish_Guidelines_2020_Minors_Unofficial%20Translation.pdf (Accessed May 7, 2024).
85. Finnish Medicines Agency. Topic Selection [in Finnish]. (2022). Available online at: https://fimea.fi/en/development/therapeutic_and_economic_value_of_medicines/topic-selection (Accessed May 7, 2024).
86. Finnish Coordinating Center for Health Technology Assessment. Suggest a Topic Service [in Finnish]. (2023). Available online at: https://web.archive.org/web/20250804094936/https://oys.fi/fincchta/ehdota-aihetta/ (Accessed May 7, 2024).
87. Finnish Medicines Agency. Development and HTA: Patient Advisory Board [in Finnish]. (2020). Available online at: https://fimea.fi/kehittaminen_ja_hta/potilasneuvottelukunta (Accessed May 7, 2024).
88. Kleme J, Pohjanoksa-Mäntylä M, Airaksinen M, Enlund H, Kastarinen H, Peura P, et al. Patient perspective in health technology assessment of pharmaceuticals in Finland. Int J Technol Assess Health Care. (2014) 30:306–11. doi: 10.1017/S0266462314000282
89. Federal Office of Public Health. HTA Programme. (2023). Available online at: https://www.bag.admin.ch/bag/en/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/hta/hta-programm.html (Accessed April 27, 2024).
90. Federal Office of Public Health. HTA Topic Submission. (2022). Available online at: https://www.bag.admin.ch/bag/en/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/hta/hta-themeneingabe.html (Accessed April 27, 2024).
91. Federal Office of Public Health. HTA Projects. (2022). Available online at: https://www.bag.admin.ch/bag/en/home/versicherungen/krankenversicherung/krankenversicherung-leistungen-tarife/hta/hta-projekte.html (Accessed April 27, 2024).
92. Federal Office of Public Health. Extra-Parliamentary Committees. (2017). Available online at: https://www.bag.admin.ch/bag/en/home/das-bag/organisation/ausserparlamentarische-kommissionen.html (Accessed April 27, 2024).
93. Federal Office of Public Health. Interest Ties. (2024). Available online at: https://www.admin.ch/ch/d/cf/ko/interessenbindung_7731.html (Accessed April 27, 2024).
94. Federal Joint Committee. Patient Participation in the Federal Joint Committee [in German]. (2023). Available online at: https://patientenvertretung.g-ba.de/ (Accessed May 4, 2024).
95. Federal Joint Committee. Patient Involvement Department of the G-BA [in German]. (2022). Available online at: https://patientenvertretung.g-ba.de/wer-wir-sind/stabsstelle-patientenbeteiligung/ (Accessed May 4, 2024).
96. Federal Joint Committee. Concerns to the Patient Representatives [in German]. (2022). Available online at: https://patientenvertretung.g-ba.de/was-wir-tun/anliegen-an-die-patientenvertretung-zur-antragstellung-beim-g-ba/ (Accessed May 4, 2024).
97. Institute for Quality and Efficiency in Health Care. ThemenCheck Reports [in German]. (2023). Available online at: https://www.iqwig.de/en/about-us/methods/results/themencheck-reports/ (Accessed May 4, 2024).
98. Institute for Quality and Efficiency in Health Care. Involvement of People Affected in the Dossier Assessment. (2017). Available online at: https://www.iqwig.de/printprodukte/involvement-of-people-affected_dossier-assessment.pdf (Accessed May 4, 2024).
99. Institute for Quality and Efficiency in Health Care. Contributing the Perspective of Patients [in German]. (2023). Available online at: https://www.iqwig.de/en/participation/contributing-the-patients-perspective/ (Accessed May 4, 2024).
100. Jommi C, Bertolani A. Patients' associations and HTA for medicines: actual and future role in Italy [in Italian]. Glob Reg Health Technol Assess. (2018) 5:77–82. doi: 10.1177/2284240318770966
101. Institute for Quality and Efficiency in Health Care. Who We Are: Patient Participation in the Federal Joint Committee [in German]. (2022). Available online at: https://patientenvertretung.g-ba.de/wer-wir-sind/ (Accessed May 4, 2024).
102. French National Authority for Health. Framework for Cooperation With Users and Their Associations [in French]. (2020). Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2021-10/has_50_cadrage_cadre_cooperation_usagers_coi_2021_09_vmel.pdf (Accessed May 4, 2024).
103. French National Authority for Health. Contributions of Patient and User Associations to Health Product Evaluations - Descriptive Analysis [in French]. (2020) Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2020-04/analyse_descriptive_contributions.pdf (Accessed May 4, 2024).
104. French National Authority for Health. Participate in the Work of the HAS [in French]. (2015). Available online at: https://www.has-sante.fr/jcms/r_1498361/en/participer-aux-travaux-de-la-has (Accessed May 4, 2024).
105. French National Authority for Health. Contribute to the Evaluation of Medicines and Devices [in French]. (2017). Available online at: https://www.has-sante.fr/jcms/c_2666630/fr/contribuer-a-l-evaluation-des-medicaments-et-des-dispositifs (Accessed May 4, 2024).
106. French National Authority for Health. Contribution of Patient and User Associations to Evaluations of Medicines and Medical Devices: Guide for Patient and User Associations [in French]. (2019). Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2016-11/contribution_asso_patients_guide_v3.pdf (Accessed May 4, 2024).
107. French National Authority for Health. Contribute to the Evaluation of Medicines With a View to Their Reimbursement or Early Access Authorization [in French]. (2024). Available online at: https://www.has-sante.fr/jcms/p_3114053/fr/contribution-des-associations-de-patients-et-d-usagers-aux-evaluations-de-medicaments (Accessed May 4, 2024).
108. French National Authority for Health. Transparency Commission [in French]. (2023). Available online at: https://www.has-sante.fr/jcms/c_412210/fr/commission-de-la-transparence#toc_1_2 (Accessed May 4, 2024).
109. French National Authority for Health. Internal Regulations of the Transparency Commission [in French]. (2022). Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2020-11/reglement_interieur_commission__de_la_transparence__19112020.pdf (Accessed May 4, 2024).
110. French National Authority for Health. National Commission for the Evaluation of Medical Devices and Health Technologies [in French]. (2023). Available online at: https://www.has-sante.fr/jcms/c_419486/fr/commission-nationale-d-evaluation-des-dispositifs-medicaux-et-des-technologies-de-sante (Accessed May 4, 2024).
111. French National Authority for Health. Understanding the Evaluation of Medicines [in French]. (2021). Available online at: https://www.has-sante.fr/jcms/c_412115/ (Accessed May 4, 2024).
112. French National Authority for Health. Early Access to Medicines Guide for Patient and User Associations and Groups for Their Contribution to Evaluations [in French]. (2022). Available online at: https://www.has-sante.fr/upload/docs/application/pdf/2022-04/guide_associations_aap_vf_mel_20220413.pdf (Accessed May 4, 2024).
113. Fried A, Wild C. Involvement of Citizens and Patients in HTA Processes. International Experiences and Good Practice Examples [in German]. (2016). Available online at: https://eprints.aihta.at/1088/1/HTA-Projektbericht_Nr.86.pdf (Accessed May 4, 2024).
114. Rochaix L, Xerri B. National Authority for Health: France. Issue brief. New York, NY: The Commonwealth Fund (2009).
115. Gesbert C, André-Vert J, Guerrier M, Galbraith M, Devaud C, Dupont JCK, et al. The contribution of French patient and consumer groups to health technology assessments over a 2-year period: an observational retrospective study. Int J Technol Assess Health Care. (2021) 37:e22. doi: 10.1017/S0266462321000180
116. Health Information and Quality Authority. A Guide to Health Technology Assessment at HIQA. (2016). Available online at: https://www.hiqa.ie/sites/default/files/2017-01/A-Guide-to-Health-Technology-Assessment.pdf (Accessed May 3, 2024).
117. Health Information and Quality Authority. Health Technology Assessments. (n.d.). Available online at: https://www.hiqa.ie/reports-and-publications/health-technology-assessments?field_hta_topics_target_id=All&field_covid_19_topics_target_id=All&tid_1=All&keys=&page=0 (Accessed May 3, 2024).
118. PPI Hub. HTA Prioritisation Advisory Group. (n.d.). Available online at: https://ppihub.ipposi.ie/item/hta-prioritisation-advisory-group-2/ (Accessed May 3, 2024).
119. Health Information and Quality Authority. Guidelines for Stakeholder Engagement in Health Technology Assessment in Ireland. (2014). Available online at: https://www.hiqa.ie/sites/default/files/2017-01/HTA-Guidelines-Stakeholder-Engagement.pdf (Accessed May 3, 2024).
120. National Authority of Medicines and Health Products. Project INCLUIR [in Portuguese]. (2015). Available online at: https://www.infarmed.pt/documents/15786/2304493/Projeto+INCLUIR/14ee5af7-743a-4f99-b463-ee78efd0a775 (Accessed May 6, 2024).
121. Oliveira M. Inclusion Project: Patient Involvement in Health Technology Assessment in Portugal. (2019). Available online at: https://cddf.org/wp-content/uploads/2019/07/Day1_1630_Margarida-Oliveira.pdf (Accessed May 6, 2024).
122. Vinhas J, Dias S, Gouveia AM, Correia A, Dias CV, Sousa D, et al. Pharmacotherapeutic Assessment Methodology, Version 3.0. Lisbon: Committee for Health Technology Assessment, INFARMED - Autoridade Nacional do Medicamento e Produtos de Saúde, I.P (2022). Available online at: https://www.infarmed.pt/documents/15786/1963929/METOD_AFT_v3.0_ENvf_fev2023/b0cb1c54-adca-721a-6466-75ba04cdd542 (Accessed May 6, 2024).
123. Perelman J SMMCDAFRFLSPVPFCCSTMSM. Methodological Guidelines for Economic Evaluation Studies. Lisbon: INFARMED - National Authority of Medicines and Health Products, I.P (2019). Available online at: https://www.infarmed.pt/documents/15786/4001413/Orienta%C3%A7%C3%B5es+metodol%C3%B3gicas+para+estudos+de+avalia%C3%A7%C3%A3o+econ%C3%B3mica+de+tecnologias+de+sa%C3%BAde+%28EN%29/ebcfd930-94e2-c7e1-100a-ee1df3d76882 (Accessed May 6, 2024).
124. National Institute of Sickness and Disability Insurance. The Bodies of the Medical Evaluation and Control Service [in French]. (n.d.). Available online at: https://www.inami.fgov.be/fr/l-inami/nos-organes/les-organes-du-service-d-evaluation-et-de-controle-medicaux- (Accessed May 5, 2024).
125. Cleemput I, Dauvrin M, Kohn L, Christiaens W, Léonard C. Position of KCE on Patient Involvement in Health Care Policy Research. (2019). Available online at: https://kce.fgov.be/sites/default/files/2021-12/KCE_320C_Patient_involvement_health_care_policy_research_Synthesis_0.pdf (Accessed May 5, 2024).
126. Leopold C, Lu CY, Wagner AK. Integrating public preferences into national reimbursement decisions: a descriptive comparison of approaches in Belgium and New Zealand. BMC Health Serv Res. (2020) 20:1–10. doi: 10.1186/s12913-020-05152-2
127. E&A Consultants. It's Official: The Reimbursement Procedure for Medicine Will be Reformed!. (2024). Available online at: https://www.eaconsultants.be/news/its-official-the-reimbursement-procedure-for-medicine-will-be-reformed (Accessed May 13, 2024).
128. Alisa - Healthcare System of Liguria Region. Health Technology Assessment [in Italian]. (2021). Available online at: https://www.alisa.liguria.it/organizzazione/ https://www.alisa.liguria.it/organizzazione/direzione-generale/ricerca-innovazione-hta-gestione-processi-ospedalieri-assistenza-specialistica/assistenza-ospedaliera-hta-e-sistemi-dell-emergenza/health-technology-assessment.html (Accessed May 6, 2024).
129. World Health Organization. HTA Country Profiles. (2021). Available online at: https://cdn.who.int/media/docs/default-source/health-economics/hta-country-profiles-2020-21/hta_updated_merged_final.pdf?sfvrsn=75ac91f6_5 (Accessed May 6, 2024).
130. Rais C, Kaló Z, Csanádi M, Negulescu V. Current and future perspectives for the implementation of health technology assessment in Romania. Health Policy Technol. (2020) 9:45–52. doi: 10.1016/j.hlpt.2019.11.007
131. Lopert R, Ruiz F, Gheorghe A, Chanturidze T. Technical Assistance for Institution Building of Health Technology Assessment Structure, Including Training for the National Agency for Medicines & Medical Devices Deliverable 1: Situational Analysis of Romanian HTA. (2017). Available online at: https://ms.ro/media/documents/Inception-Report-en.pdf (Accessed May 6, 2024).
132. National Centre for Pharmacoeconomics. For Patients. (n.d.). Available online at: https://www.ncpe.ie/for-patients/ (Accessed April 28, 2024).
133. PPI Hub. Patient Organisation Submission Process. (n.d.). Available online at: https://ppihub.ipposi.ie/item/patient-organisation-submission-process-2/ (Accessed April 28, 2024).
134. PPI Hub. HSE Drugs Group. (n.d.). Available online at: https://ppihub.ipposi.ie/item/hse-drugs-group-2/ (Accessed April 28, 2024).
135. National Centre for Pharmacoeconomics. Patient Submission Process Overview. (n.d.). Available online at: https://www.ncpe.ie/for-patients/patient-submission-process-overview/ (Accessed April 28, 2024).
136. Health Service Executive. Drugs Group Minutes. (2024). Available online at: https://www.hse.ie/eng/about/who/cpu/drugs-group-minutes/ (Accessed April 28, 2024).
137. National Centre for Pharmacoeconomics. Completing a Patient Organisation Submission of Evidence Template: Guidelines for Patient Organisations for Health Technology Assessment and Appraisal of Medicines. (2022). Available online at: https://www.ncpe.ie/wp-content/uploads/2022/05/Guidelines-for-Patient-Organisations-v-1.3.pdf (Accessed May 3, 2024).
138. Hashem F, Calnan MW, Brown PR. Decision making in NICE single technological appraisals: how does NICE incorporate patient perspectives? Health Expect. (2018) 21:128. doi: 10.1111/hex.12594
139. National Institute for Health and Care Excellence. NICE's Approach to Public Involvement in Guidance and Standards: A Practical Guide. (2015). Available online at: https://www.nice.org.uk/media/default/About/NICE-Communities/Public-involvement/Public-involvement-programme/PIP-process-guide-apr-2015.pdf (Accessed April 27, 2024).
140. National Institute for Health and Care Excellence. Public Involvement Programme. NICE. (n.d.). Available online at: https://www.nice.org.uk/about/nice-communities/nice-and-the-public/public-involvement/public-involvement-programme (Accessed April 27, 2024).
141. National Institute for Health and Care Excellence. Guides to Developing Our Guidance. NICE. (n.d.). Available online at: https://www.nice.org.uk/about/nice-communities/nice-and-the-public/public-involvement/support-for-vcs-organisations/help-us-develop-guidance/guides-to-developing-our-guidance (Accessed April 27, 2024).
142. National Institute for Health and Care Excellence. NICE Health Technology Evaluations: The Manual. (2023). Available online at: https://www.nice.org.uk/process/pmg36/resources/nice-health-technology-evaluations-the-manual-pdf-72286779244741 (Accessed April 27, 2024).
143. National Institute for Health and Care Excellence. NICE Health Technology Evaluation Topic Selection: The Manual. (2022). Available online at: https://www.nice.org.uk/process/pmg37/resources/nice-health-technology-evaluation-topic-selection-the-manual-pdf-72286780924357 (Accessed April 27, 2024).
144. National Institute for Health and Care Excellence. Patient and Public Involvement Policy. NICE. (n.d.). Available online at: https://www.nice.org.uk/about/nice-communities/nice-and-the-public/public-involvement/public-involvement-programme/patient-public-involvement-policy (Accessed April 27, 2024).
145. National Institute for Health and Care Excellence. Guide to the Processes of Technology Appraisal. (2018). Available online at: https://www.nice.org.uk/process/pmg19/resources/guide-to-the-processes-of-technology-appraisal-pdf-72286663351237 (Accessed April 27, 2024).
146. Wale JL, Sullivan M. Exploration of the visibility of patient input in final recommendation documentation for three health technology assessment bodies. Int J Technol Assess Health Care. (2020) 36:197–203. doi: 10.1017/S0266462320000240
147. Norwegian Institute of Public Health. Development Plan in the Health Services Area [in Norwegian]. (2017). Available online at: https://www.fhi.no/globalassets/dokumenterfiler/omrade-for-helsetjenester-utviklingsplan.pdf (Accessed May 6, 2024).
148. EUnetHTA. Report on Yearly Training Courses for EUnetHTA Partners and Associates, and Stakeholders. (2015). Available online at: https://web.archive.org/web/20201229203744/https://eunethta.eu/wp-content/uploads/2018/01/Report-on-yearly-training-courses-on-EUnetHTA-tools-and-methodology.pdf (Accessed May 6, 2024).
149. Mwaura D, Solli O, Hjelvin E. Introduction of new health technologies – is the patient being heard? Tidsskrift for Den norske legeforening. (2022) 142:2022–0504. doi: 10.4045/tidsskr.22.0068
150. New Methods. Who Does What in New Methods [in Norwegian]. (2024). Available online at: https://www.nyemetoder.no/om-systemet/hvem-gjor-hva (Accessed May 6, 2024).
151. New Methods. Ordering Forum for New Methods [in Norwegian]. (2024). Available online at: https://www.nyemetoder.no/om-systemet/bestillerforum-for-nye-metoder (Accessed May 6, 2024).
152. New Methods. Input to Methods [in Norwegian]. (2023). Available online at: https://www.nyemetoder.no/om-systemet/innspill-til-metoder (Accessed May 6, 2024).
153. New Methods. (2024). Available online at: https://www.nyemetoder.no/english (Accessed May 6, 2024).
154. New Methods. Background: Why Do We Have New Methods? [in Norwegian]. (2024). Available online at: https://www.nyemetoder.no/om-systemet/bakgrunn-hvorfor-har-vi-nye-metoder (Accessed May 6, 2024).
155. Proba. Evaluation of the System for New Methods in the Specialist Health Service [in Norwegian]. (2021). Available online at: https://www.regjeringen.no/contentassets/09874a0573eb480384061da473458ed1/rapport-evaluering-nye-metoder-2021115-ferdig.pdf (Accessed May 6, 2024).
156. Norwegian Institute of Public Health. Reviews and Health Technology Assessments - NIPH [in Norwegian]. (2018). Available online at: https://www.fhi.no/en/ab/departments-and-centres/reviews-and-health-technology-assessments/ (Accessed May 6, 2024).
157. Nye Metoder to Increase Patient Involvement in Decision-Making Process. (2023). Available online at: https://www.navlindaily.com/article/17604/nye-metoder-to-increase-patient-involvement-in-decision-making-process (Accessed May 6, 2024).
158. Chamova J. Mapping of HTA National Organisations, Programmes and Processes in EU and Norway. (2017). Available online at: https://health.ec.europa.eu/system/files/2018-02/2018_mapping_npc_en_0.pdf (Accessed May 5, 2024).
159. Chamova J. Mapping of HTA National Organisations, Programmes and Processes in EU and Norway: Anexes. (2017). Available online at: https://health.ec.europa.eu/document/download/4a2df425-2347-404d-bb06-a7959cc95c38_en (Accessed May 6, 2024).
160. Norwegian Medical Products Agency. Method Assessment of Medical Products - The Directorate for Medical Products. (2024). Available online at: https://web.archive.org/web/20240812143520/https://www.dmp.no/offentlig-finansiering/metodevurdering-av-legemidler (Accessed May 6, 2024).
161. Norwegian Medical Products Agency. Appeal Against an Administrative Decision [In Norwegian]. (2024). Available online at: https://www.dmp.no/en/about-us/organisation-and-tasks/appeal-against-an-administrative-decision (Accessed May 6, 2024).
162. Norwegian Medical Products Agency. Method Notice or Request [In Norwegian]. (2023). Available online at: https://www.dmp.no/offentlig-finansiering/metodevarsling (Accessed May 6, 2024).
163. Toledo-Chávarri A, Triñanes Pego Y, Rodrigo ER, Roteta NI, Novella-Arribas B, Vicente Edo MJ, et al. Evaluation of patient involvement strategies in health technology assessment in Spain: the viewpoint of HTA researchers. Int J Technol Assess Health Care. (2021) 37:e25. doi: 10.1017/S0266462320000586
164. Scottish Health Technologies Group. Patient and Public Involvement. (n.d.). Available online at: https://shtg.scot/get-involved/patient-and-public-involvement/ (Accessed April 28, 2024).
165. Scottish Health Technologies Group. What We Do. (n.d.). Available online at: https://shtg.scot/what-we-do/ (Accessed April 28, 2024).
166. Scottish Health Technologies Group. Range of Advice Products. (n.d.). Available online at: https://shtg.scot/what-we-do/range-of-advice-products/ (Accessed April 28, 2024).
167. Scottish Health Technologies Group. Contribute to Advice. (n.d.). Available online at: https://shtg.scot/get-involved/contribute-to-advice/ (Accessed April 28, 2024).
168. Scottish Health Technologies Group. Guide to Support Patient Organisation Submissions. (2021). Available online at: https://shtg.scot/media/1802/guide-to-support-patient-organisation-submissions.pdf (Accessed April 28, 2024).
169. Scottish Health Technologies Group. Attending a SHTG Council Meeting. (n.d.). Available online at: https://shtg.scot/media/2128/patient-organisation-guide-for-shtg-council-meetings-v10.pdf (Accessed April 28, 2024).
170. Stewart JA, Clifton E, Macpherson K, Angelova N, Morrison G. Scottish health technologies group: enhancing patient engagement. Int J Technol Assess Health Care. (2021) 37:e21. doi: 10.1017/S026646232000224X
171. Scottish Medicines Consortium. A Guide for Patient Group Partners Advising on New Medicines for Scotland Scottish Medicines Consortium A Guide for Patient Group Partners. (2022). Available online at: https://www.scottishmedicines.org.uk/media/6784/smc-guide-revised-march-2022-0-4.pdf (Accessed April 27, 2024).
172. Scottish Medicines Consortium. Public Involvement Network Advisory Group. (n.d.). Available online at: https://www.scottishmedicines.org.uk/about-us/public-involvement/public-involvement-network-advisory-group/ (Accessed April 27, 2024).
173. Scottish Medicines Consortium. Public Involvement. (n.d.). Available online at: https://www.scottishmedicines.org.uk/about-us/public-involvement/ (Accessed April 27, 2024).
174. Scottish Medicines Consortium. Patient Group Partners. (n.d.). Available online at: https://www.scottishmedicines.org.uk/about-us/public-involvement/patient-group-partners/ (Accessed April 27, 2024).
175. Scottish Medicines Consortium. Public Partners. (n.d.). Available online at: https://www.scottishmedicines.org.uk/about-us/public-involvement/public-partners/ (Accessed April 27, 2024).
176. Scottish Medicines Consortium. Making a Submission. (n.d.). Available online at: https://www.scottishmedicines.org.uk/making-a-submission/ (Accessed April 27, 2024).
177. Scottish Medicines Consortium. Attending a Virtual SMC Committee Meeting Information for Participating Patient Group Partners SMC Committee Meetings. (n.d.). Available online at: https://www.scottishmedicines.org.uk/media/5519/information-for-participating-patient-group-partners-v41_final.pdf (Accessed April 27, 2024).
178. Scottish Medicines Consortium. Public Involvement Network (PIN) Advisory Group Terms of Reference. (n.d.). Available online at: https://www.scottishmedicines.org.uk/media/3067/pin-advisory-group-terms-of-reference.pdf (Accessed April 27, 2024).
179. Vostalová L, Mazelová J, Samek J, Vocelka M. Health technology assessment in evaluation of pharmaceuticals in the Czech Republic healthcare system and its financing in brief. Int J Technol Assess Health Care. (2017) 33:339–44. doi: 10.1017/S0266462317000204
180. Kluszczynski T, Nemeth B, Władysiuk M, Czech M, Kamusheva M, Fotin N, et al. Optimizing patient access to orphan medicinal products: lessons from central and eastern Europe. J Mark Access Health Policy. (2025) 13:24. doi: 10.3390/jmahp13020024
181. Wilsdon T, Fiz E, Haderi A. A Comparative Analysis of the Role and Impact of Health Technology Assessment. (2013). Available online at: https://www.efpia.eu/media/25706/a-comparative-analysis-of-the-role-and-impact-of-health-technology-assessment-2013.pdf (Accessed May 7, 2024).
182. Enzing JJ, Knies S, Boer B, Brouwer WBF. Broadening the application of health technology assessment in the Netherlands: a worthwhile destination but not an easy ride? Health Econ Policy Law. (2021) 16:440–56. doi: 10.1017/S1744133120000237
183. Smit C. Personal reflections of a patient representative in an appraisal committee. Patient. (2015) 8:5–10. doi: 10.1007/s40271-014-0086-8
184. Stolk EA, de Bont A, van Halteren AR, Bijlmer RJ, Poley MJ. Role of health technology assessment in shaping the benefits package in the Netherlands. Expert Rev Pharmacoecon Outcomes Res. (2009) 9:85–94. doi: 10.1586/14737167.9.1.85
185. Jönsson B, Oortwijn W, Rutten F, Wailoo A. Health Technology Assessment Methodology Programme: Review of External Evaluation Committee. (2015). Available online at: https://www.eerstekamer.nl/overig/20180124/evaluation_health_technology/document (Accessed May 3, 2024).
186. Teerawattananon Y, Rattanavipapong W, Lin LW, Dabak SV, Gibbons B, Isaranuwatchai W, et al. Landscape analysis of health technology assessment (HTA): systems and practices in Asia. Int J Sci Res. (2019) 35:416. doi: 10.1017/S0266462319000667
187. Tan P-T. The Future of Patient and Public Involvement in Health Technology Assessment in Singapore. (2021). Available online at: https://www.duke-nus.edu.sg/docs/librariesprovider5/slides/slides-ace-cee-the-future-of-patient-and-public-involvement-in-hta-in-singapore-181121.pdf?sfvrsn=17d96d5b_0 (Accessed May 5, 2024).
188. Agency for Care Effectiveness. Drug and Vaccine Evaluation Methods and Process Guide. (2021). Available online at: https://isomer-user-content.by.gov.sg/68/f000a2dd-628b-42b1-8be3-0b512584155d/drug-and-vaccine-evaluation-methods-and-process-guide-version-3-1-(september-2023).pdf (Accessed May 5, 2024).
189. Agency for Care Effectiveness. Medical Technologies Evaluation Methods and Process Guide. (2022). Available online at: https://www.ace-hta.gov.sg/docs/default-source/process-methods/ace-med-tech-evaluation-methods-and-process-guide-(mar-2022).pdf (Accessed May 5, 2024).
190. Agency for Care Effectiveness. ACE Technology Guidances. (2022). Available online at: https://www.ace-hta.gov.sg/healthcare-professionals/ace-technology-guidances#cat~Drug%20Guidances,Medical%20Technology%20Guidances&type~Published&page~1 (Accessed May 5, 2024).
191. Agency for Care Effectiveness. Patients & Community. (2022). Available online at: https://www.ace-hta.gov.sg/Patients-And-Community (Accessed May 5, 2024).
192. Duke-NUS Medical School. CAPE Regional Multi-Stakeholder Roundtable Report: Embedding Patient Engagement for Sustainable Health Systems. (2021). Available online at: https://www.duke-nus.edu.sg/docs/librariesprovider5/publications/2021_r001_core_cape-regional-multi-stakeholder-roundtable-report-embedding-patient-engagement-for-sustainable-health-systems.pdf?sfvrsn=53e81827_0 (Accessed May 5, 2024).
193. Hu S. Patient Involvement in HTA in China. (2017). Available online at: https://www.ispor.org/docs/default-source/presentations/1070.pdf?sfvrsn=3401bdf2_1 (Accessed May 5, 2024).
194. Bailey C, Cox I. ISPOR - Health Technology Assessment: Challenges and Lessons Learned in Asia. (2020). Available online at: https://www.ispor.org/publications/journals/value-outcomes-spotlight/vos-archives/issue/view/september-2020-supplement-spotlight-on-asia-pacific/health-technology-assessment-challenges-and-lessons-learned-in-asia (Accessed May 5, 2024).
195. China National Health Development Research Center. (2024). Available online at: http://www.cnhdrc.cn/ (Accessed May 5, 2024).
196. Rajsekar K. Health Technology Assessment in India: A Manual. (2018). Available online at: https://www.researchgate.net/publication/366066447_Health_Technology_Assessment_in_India_A_Manual (Accessed May 5, 2024).
197. Health Insurance Review and Assessment Service. List of Members by Committee. (2022). Available online at: https://www.hira.or.kr/dummy.do?pgmid=HIRAA030051000006 (Accessed May 5, 2024).
198. Leelahavarong P, Doungthipsirikul S, Kumluang S, Poonchai A, Kittiratchakool N, Chinnacom D, et al. Health technology assessment in Thailand: institutionalization and contribution to healthcare decision making: review of literature. Int J Technol Assess Health Care. (2019) 35:467–73. doi: 10.1017/S0266462319000321
199. Mohara A, Youngkong S, Velasco RP, Werayingyong P, Pachanee K, Prakongsai P, et al. Using health technology assessment for informing coverage decisions in Thailand. J Comp Eff Res. (2012) 1:137–46. doi: 10.2217/cer.12.10
200. IAPOvoice. Parallel Session 4 Health Technology Assessment and Value Based Healthcare in Asia Pacific - YouTube. (2023). Available online at: https://www.youtube.com/watch?v=OAZHdT3q374 (Accessed May 5, 2024).
201. Tantivess S, Chalkidou K, Tritasavit N, Teerawattananon Y. Health technology assessment capacity development in low- and middle-income countries: experiences from the international units of HITAP and NICE. F1000Res. (2017) 6. doi: 10.12688/f1000research.13180.1
202. Doungthipsirikul S, Kittiratchakool N, Chinnacom D. HTAsiaLink. Patient Involvement on HTA. (2017). Available online at: https://www.hitap.net/wp-content/uploads/2017/05/HTAsialink-10-for-web-26_4_2017.pdf (Accessed May 5, 2024).
203. Lee HY, Nguyen TTT, Park S, Hoang VM, Kim WH. Health technology assessment development in Vietnam: a qualitative study of current progress, barriers, facilitators, and future strategies. Int J Environ Res Public Health. (2021) 18:8846. doi: 10.3390/ijerph18168846
204. Vo TQ. Health technology assessment in developing countries: a brief introduction for Vietnamese health-care policymakers. Asian J Pharm. (2018). doi: 10.22377/ajp.v12i01.2340
205. Van Minh H, Thi Phung T, Thuy Duyen N, Quynh Mai V. Technical Assistance Consultant's Report: Socialist Republic of Viet Nam: Strengthening the Policy and Institutional Framework of Social Health Insurance. (2021). Available online at: https://www.adb.org/sites/default/files/project-documents/50139/50139-002-tacr-en_2.pdf (Accessed May 5, 2024).
206. Health Technology Assessment Unit Department of Health - Philippines. Philippine HTA Methods Guide. (2020). Available online at: https://hta.dost.gov.ph/philippine-hta-methods-guide/ (Accessed May 5, 2024).
207. Health Technology Assessment Unit Department of Health - Philippines. Philippine HTA Process Guide. (2020). Available online at: https://hta.dost.gov.ph/philippine-hta-process-guide/ (Accessed May 5, 2024).
208. Health Technology Assessment International (HTAi). Good Practice Examples of Patient and Public Involvement in Health Technology Assessment. (2014). Available online at: https://healthtai.sharepoint.com/sites/IGWebsiteContent/Shared%20Documents/Forms/AllItems.aspx?id=%2Fsites%2FIGWebsiteContent%2FShared%20Documents%2FPatient%20and%20Citizen%20Involvement%2FGood%5FPractice%5FExamples%5FFeb%5F2015%2Epdf&parent=%2Fsites%2FIGWebsiteContent%2FShared%20Documents%2FPatient%20and%20Citizen%20Involvement&p=true&ga=1 (Accessed May 5, 2024).
209. Shemer J, Shani M, Tamir O, Siebzehner MI. Health technology management in Israel: HTA in action. Int J Technol Assess Health Care. (2019) 25:134–9. doi: 10.1017/S0266462309090540
210. Shani S, Siebzehner MI, Luxenburg O, Shemer J. Setting priorities for the adoption of health technologies on a national level - the Israeli experience. Health Policy. (2000) 54:169–85. doi: 10.1016/S0168-8510(00)00109-3
211. Greenberg D, Siebzehner MI, Pliskin JS. The process of updating the national list of health services in Israel: is it legitimate? Is it fair? Int J Technol Assess Health Care. (2009) 25:255–61. doi: 10.1017/S026646230999016X
212. Ghazali I, Sabirin J. Patient Involvement on HTA. (2017). Available online at: https://www.hitap.net/wp-content/uploads/2017/05/HTAsialink-10-for-web-26_4_2017.pdf (Accessed May 5, 2024).
213. Malaysian Health Technology Assessment Section. Ministry of Health. Health Technology Assessment Manual. (n.d.). Available online at: https://www.moh.gov.my/moh/resources/HTA_MANUAL_MAHTAS.pdf (Accessed May 5, 2024).
214. HITAP Thailand. HTAsiaLink 2022: Plenary 1 - Reimagining the Post-COVID Health System & Health Technology Assessment. (2023). Available online at: https://www.youtube.com/watch?v=5fElJn9vsmc (Accessed May 5, 2024).
215. MDWorks Korea. New Health Technology Assessment (nHTA). (n.d.). Available online at: http://www.mdworkskorea.com/eng/sub/sub04_01.php (Accessed May 5, 2024).
216. National Evidence-Based Healthcare Collaborating Agency. Center for New Health Technology Assessment. Committee of nHTA. (n.d.). Available online at: https://nhta.neca.re.kr/nhta/eng/nhtaENG0201V.ecg (Accessed May 5, 2024).
217. Potter B. Patient Involvement in Health Technology Assessment. (2018). Available online at: https://slideplayer.com/slide/12841321/ (Accessed May 5, 2024).
218. Bae EY, Hong JM, Kwon HY, Jang S, Lee HJ, Bae SJ, et al. Eight-year experience of using HTA in drug reimbursement: South Korea. Health Policy. (2016) 120:612–20. doi: 10.1016/j.healthpol.2016.03.013
219. Bae EY. Role of health technology assessment in drug policies: Korea. Value Health Reg Issues. (2019) 18:24–9. doi: 10.1016/j.vhri.2018.03.009
220. Shih YR, Liao KH, Chen YH, Lin FJ, Hsiao FY. Reimbursement lag of new drugs under Taiwan's national health insurance system compared with United Kingdom, Canada, Australia, Japan, and South Korea. Clin Transl Sci. (2020) 13:916–22. doi: 10.1111/cts.12778
221. Chen KA, Huang LY, Gau CS. Patient involvement in the health technology assessment process in Taiwan. Front Med Technol. (2021) 3:732160. doi: 10.3389/fmedt.2021.732160
222. Center for Drug Evaluation. Health Technology Assessment [in Taiwanese]. (n.d.). Available online at: https://www.cde.org.tw/eng/HTA/ (Accessed May 4, 2024).
223. Centers for Medicare & Medicaid Services. Medicare Evidence Development & Coverage Advisory Committee. (2024). Available online at: https://www.cms.gov/medicare/regulations-guidance/advisory-committees/evidence-development-coverage (Accessed May 2, 2024).
224. Centers for Medicare & Medicaid Services. Factors CMS Considers in Referring Topics to the Medicare Evidence Development & Coverage Advisory Committee. (2006). Available online at: https://www.cms.gov/medicare-coverage-database/view/medicare-coverage-document.aspx?MCDId=10 (Accessed May 2, 2024).
225. Centers for Medicare & Medicaid Services. National Coverage Determination Process & Timeline. (2023). Available online at: https://www.cms.gov/cms-guide-medical-technology-companies-and-other-interested-parties/coverage/national-coverage-determination-process-timeline (Accessed May 2, 2024).
226. Centers for Medicare & Medicaid Services. Factors CMS Considers in Commissioning External Technology Assessments. (2006). Available online at: https://www.cms.gov/medicare-coverage-database/view/medicare-coverage-document.aspx?MCDId=7 (Accessed May 2, 2024).
227. Agency for Healthcare Research and Quality. Technology Assessment Program. (2024). Available online at: https://www.ahrq.gov/research/findings/ta/index.html#tapubrev (Accessed May 2, 2024).
228. Canadian Agency for Drugs and Technologies in Health. Guidance for Providing Patient Input. (2024). Available online at: https://www.cadth.ca/sites/default/files/Drug_Review_Process/Guidance%20for%20Providing%20Patient%20Input.pdf (Accessed April 28, 2024).
229. Canadian Agency for Drugs and Technologies in Health. Topic Identification and Prioritization Process. (2015). Available online at: https://www.cadth.ca/sites/default/files/pdf/HTA_OU_Topic_ID_and_Prioritization_Process.pdf (Accessed April 28, 2024).
230. Canadian Agency for Drugs and Technologies in Health. Procedures for the CADTH Common Drug Review and Interim Plasma Protein Product Review. (2020). Available online at: https://www.cadth.ca/sites/default/files/cdr/process/Procedure_and_Guidelines_for_CADTH_CDR.pdf (Accessed April 28, 2024).
231. Canadian Agency for Drugs and Technologies in Health. Procedures for CADTH Reimbursement Reviews. (2024). Available online at: https://www.cadth.ca/sites/default/files/Drug_Review_Process/CADTH%20Drug%20Reimbursement%20Review%20Procedures.pdf (Accessed April 28, 2024).
232. Canadian Agency for Drugs and Technologies in Health. Patient Input and Feedback. (2021). Available online at: https://www.cadth.ca/patient-input-and-feedback (Accessed April 28, 2024).
233. Canadian Agency for Drugs and Technologies in Health. The pCODR Expert Review Committee (pERC). (2024). Available online at: https://www.cadth.ca/pcodr-expert-review-committee-perc-0 (Accessed April 28, 2024).
234. Canadian Agency for Drugs and Technologies in Health. CADTH Framework for Patient Engagement in Health Technology Assessment. (2019). Available online at: https://www.cadth.ca/cadth-framework-patient-engagement-health-technology-assessment-0 (Accessed April 28, 2024).
235. Institute for Clinical and Economic Review. Patients. (n.d.). Available online at: https://icer.org/patients/ (Accessed May 2, 2024).
236. Institute for Clinical and Economic Review. Leadership Staff . (n.d.). Available online at: https://icer.org/who-we-are/people/leadership-staff/ (Accessed May 2, 2024).
237. Institute for Clinical and Economic Review. Opportunities for Input. (n.d.). Available online at: https://icer.org/respond-to-our-work/ (Accessed May 2, 2024).
238. Institute for Clinical and Economic Review. Share Your Patient Experience. (n.d.). Available online at: https://icer.org/share-your-patient-experience/ (Accessed May 2, 2024).
239. Institute for Clinical and Economic Review. Participate In ICER's Public Meeting. (n.d.). Available online at: https://icer.org/participate-in-icers-public-meeting (Accessed May 2, 2024).
240. Institute for Clinical and Economic Review. New England Comparative Effectiveness Public Advisory Council (NE-CEPAC). (2024). Available online at: https://icer.org/who-we-are/people/independent-appraisal-committees/new-england-cepac/ (Accessed May 2, 2024).
241. Institute for Clinical and Economic Review. California Technology Assessment Forum (CTAF). (2024). Available online at: https://icer.org/who-we-are/people/independent-appraisal-committees/ctaf/ (Accessed May 2, 2024).
242. Institute for Clinical and Economic Review. Topic Selection. (n.d.). Available online at: https://icer.org/our-approach/methods-process/value-assessment-framework/topic-selection/ (Accessed May 2, 2024).
243. The National Institute of Excellence in Health and Social Services. Patients, Caregivers and Citizens. (n.d.). Available online at: https://www.inesss.qc.ca/naviguer-selon-le-profil/patients.html (Accessed May 3, 2024).
244. Oregon Health Authority - Health Evidence Review Commission. Health Evidence Review Commission. (n.d.). Available online at: https://www.oregon.gov/oha/HPA/DSI-HERC/Pages/index.aspx (Accessed May 2, 2024).
245. Oregon Health Authority - Health Evidence Review Commission. How to Participate. (n.d.). Available online at: https://www.oregon.gov/oha/HPA/DSI-HERC/Pages/public-input-opportunities.aspx (Accessed May 2, 2024).
246. Gauvin F-P, Abelson J, Lavis JN. Strengthening Public and Patient Engagement in Health Technology Assessment in Ontario. (2014). Available online at: https://www.mcmasterforum.org/docs/default-source/product-documents/evidence-briefs/public-engagement-in-health-technology-assessement-in-ontario-eb.pdf?sfvrsn=2 (Accessed May 2, 2024).
247. Health Quality Ontario. Health Technology Assessment. (n.d.). Available online at: https://web.archive.org/web/20250731142131/ (Accessed May 2, 2024).
248. Health Quality Ontario. Ontario Health Technology Advisory Committee. (n.d.). Available online at: https://web.archive.org/web/20250926191958/ (Accessed May 2, 2024).
249. Ontario Health Technology Advisory Committee. Public Engagement in Health Technology Assessment in Ontario. (n.d.). Available online at: https://www.mcmasterforum.org/docs/default-source/product-documents/evidence-briefs/public-engagement-in-health-technology-assessement-in-ontario-eb.pdf?sfvrsn=2 (Accessed May 2, 2024).
250. Washington State Health Care Authority. How to Participate. (n.d.). Available online at: https://www.hca.wa.gov/about-hca/programs-and-initiatives/health-technology-assessment/how-participate# (Accessed May 2, 2024).
251. Blanco RMC, de la Rosa AP, Calvo Bretón LP, San Román EH, Centro Nacional de Excelencia Tecnológica en Salud. Health Technology Assessment: Methodological Document [in Spanish]. (2010). Available online at: https://www.gob.mx/cms/uploads/attachment/file/272272/Documento_metodologico_ETES.pdf (Accessed May 4, 2024).
252. National Commission for the Evaluation of Health Technologies and Clinical Excellence. Argentinian Government. Citizen Participation [in Spanish]. (2023). Available online at: https://www.argentina.gob.ar/salud/conetec/convocatorias (Accessed May 4, 2024).
253. Merck Sharp and Dohme. Protagonist Patients [in Spanish]. (2021). Available online at: https://web.archive.org/web/20230922204508/ (Accessed May 4, 2024).
254. National Commission for the Evaluation of Health Technologies and Clinical Excellence. Government of Argentina. Functioning. (2023). Available online at: https://www.argentina.gob.ar/salud/conetec/funcionamiento (Accessed May 4, 2024).
255. Institute of Clinical and Health Effectiveness. Consultation Form for Patients and The General Public of a Health Technology Evaluation Document [in Spanish]. (2024). Available online at: https://ets.iecs.org.ar/formulario-consulta-publica/pacientes/2177 (Accessed May 4, 2024).
256. Institute of Clinical and Health Effectiveness. Methodology for Preparation of Health Technology Assessment Reports [in Spanish]. (2023). Available online at: https://iecs.org.ar/metodosets2/#tab-1-5 (Accessed May 4, 2024).
257. National Commission for the Evaluation of Health Technologies and Clinical Excellence. Ministry of Health of Argentina. Structure and Operation Operational Manual [in Spanish]. (2020). Available online at: https://www.argentina.gob.ar/sites/default/files/conetec_-_anexo_i._manual_operativo_2020.pdf (Accessed May 4, 2024).
258. National Commission for the Evaluation of Health Technologies and Clinical Excellence. Ministry of Health of Argentina. Prioritization Process for Evaluation of Health Technologies [in Spanish]. (2023). Available online at: https://web.archive.org/web/20231206081550/ (Accessed May 4, 2024).
259. Silva AS, de Sousa MSA, da Silva EV, Galato D. Social participation in the health technology incorporation process into Unified Health System. Rev Saude Publica. (2019) 53:109. doi: 10.11606/S1518-8787.2019053001420
260. Pereira VC, Barreto JOM, Da Rocha Neves FA. Health technology reassessment in the Brazilian public health system: analysis of the current status. PLoS ONE. (2019) 14:e0220131. doi: 10.1371/journal.pone.0220131
261. EuroScan International Network. A Toolkit for the Identification and Assessment of New and Emerging Health Technologies [in Portuguese]. (2014). Available online at: https://www.gov.br/conitec/pt-br/midias/radar/2014/manual_metodologico_mht.pdf (Accessed May 5, 2024).
262. National Commission for the Incorporation of Technologies into the Unified Health System. Ministry of Health of Brazil. Submission of Proposals [in Portuguese]. (2024). Available online at: https://www.gov.br/conitec/pt-br/assuntos/avaliacao-de-tecnologias-em-saude/submissao-de-propostas#form_submissao (Accessed May 5, 2024).
263. National Commission for the Incorporation of Technologies into the Unified Health System. Ministry of Health of Brazil. Get to Know CONITEC [in Portuguese]. (2024). Available online at: https://www.gov.br/conitec/pt-br/assuntos/a-comissao/conheca-a-conitec (Accessed May 5, 2024).
264. National Commission for the Incorporation of Technologies into the Unified Health System. Ministry of Health of Brazil. Patient Perspective [in Portuguese]. (2024). Available online at: https://www.gov.br/conitec/pt-br/assuntos/participacao-social/perspectiva-do-paciente-1 (Accessed May 5, 2024).
265. Permanent Committee for the Regulation of Health Care. Ministry of Health of Brazil. COSAÚDE - Permanent Committee for the Regulation of Health Care [in Portuguese]. (2021). Available online at: https://www.gov.br/ans/pt-br/acesso-a-informacao/participacao-da-sociedade/comites-e-comissoes-1/cosaude-comite-permanente-de-regulacao-da-atencao-a-saude (Accessed May 5, 2024).
266. Instituto de Evaluación Tecnológica en Salud. Virtual Courses [in Spanish]. (2024). Available online at: https://www.iets.org.co/cursos/ (Accessed May 4, 2024).
267. Australian Government. Department of Health and Aged Care. Welcome to the Office of Health Technology Assessment (OHTA) Consultation Hub. (n.d.). Available online at: https://ohta-consultations.health.gov.au/ (Accessed May 3, 2024).
268. Australian Government. Department of Health and Aged Care. Health Technology Assessment Consumer Consultative Committee. (2023). Available online at: https://www.health.gov.au/committees-and-groups/health-technology-assessment-consumer-consultative-committee#related-committees-or-groups (Accessed May 3, 2024).
269. Australian Government. Department of Health and Aged Care. MSAC Membership. Canberra: Australian Government Department of Health (2024).
270. Australian Government. Department of Health and Aged Care. Frequently Asked Questions. (2023). Available online at: https://web.archive.org/web/20241014184811 (Accessed May 3, 2024).
271. Australian Government. Department of Health and Aged Care. MSAC and its Sub-Committees. (2017). Available online at: https://web.archive.org/web/20241014184149 (Accessed May 3, 2024).
272. Australian Government. Department of Health and Aged Care. Public Consultation. (2016). Available online at: https://web.archive.org/web/20230123162100 (Accessed May 3, 2024).
273. Australian Government. Department of Health and Aged Care. Engaging With MSAC: Information for Applicants. (2021). Available online at: https://web.archive.org/web/20241112191805 (Accessed May 3, 2024).
274. Australian Government. Department of Health and Aged Care. MSAC Terms of Reference. (2020). Available online at: http://www.msac.gov.au/internet/msac/publishing.nsf/Content/msac-terms-of-reference (Accessed May 3, 2024).
275. Australian Government. Department of Health and Aged Care. ESC Membership. (2024). Available online at: http://www.msac.gov.au/internet/msac/publishing.nsf/Content/esc-membership (Accessed May 3, 2024).
276. Australian Government. Department of Health and Aged Care. MSAC Consultation Process. (2021). Available online at: http://www.msac.gov.au/internet/msac/publishing.nsf/Content/MSAC-Consultation-Process (Accessed May 3, 2024).
277. Australian Government. Department of Health and Aged Care. Medicine Status Website. (n.d.). Available online at: https://www.pbs.gov.au/medicinestatus/home.html (Accessed May 2, 2024).
278. Australian Government. Department of Health and Aged Care. Health Technology Assessment Consumer Consultative Committee. (2023). Available online at: https://www.health.gov.au/committees-and-groups/health-technology-assessment-consumer-consultative-committee (Accessed May 2, 2024).
279. Australian Government. Department of Health and Aged Care. Pharmaceutical Benefits Advisory Committee (PBAC) Membership. (2024). Available online at: https://www.pbs.gov.au/pbs/industry/listing/participants/pbac (Accessed May 2, 2024).
280. Australian Government. Department of Health and Aged Care. Public Summary Documents Explained. (n.d.). Available online at: https://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/psd/pbac-psd-psd-explained (Accessed May 2, 2024).
281. Australian Government. Department of Health and Aged Care. Consumer Input. (n.d.). Available online at: https://www.pbs.gov.au/info/industry/listing/procedure-guidance/6-consideration-submissions/6-7-consumer-input (Accessed May 2, 2024).
282. Australian Government. Department of Health and Aged Care. PBAC Meeting Agenda and Consumer Comments. (2023). Available online at: https://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/pbac-consumer-comments (Accessed May 2, 2024).
283. Australian Government. Department of Health and Aged Care. Economics Sub Committee (ESC). (2024). Available online at: https://www.pbs.gov.au/info/industry/listing/participants/economics-subcommittee-esc (Accessed May 2, 2024).
284. Guidelines International Network. Participation Throughout the HTA Process. (n.d.). Available online at: https://g-i-n.net/toolkit/participation-throughout-the-hta-process (Accessed May 2, 2024).
285. Single A, Bean J. Recommendations to Improve the Patient Voice in Health Technology Assessment in Australia. (2018). Available online at: https://www.patientvoiceinitiative.org/wp-content/uploads/2019/09/Patient-Voice-Initiative-Recommendations-to-Improve-Patient-Voice-in-Health-Technology-Assessment-in-Australia.pdf (Accessed May 3, 2024).
286. PHARMAC. Pharmacology and Therapeutics Advisory Committee (PTAC). (2024). Available online at: https://pharmac.govt.nz/about/expert-advice/pharmacology-and-therapeutics-advisory-committee-ptac (Accessed May 3, 2024).
287. PHARMAC. Consumer Advisory Committee (CAC). (2024). Available online at: https://pharmac.govt.nz/about/expert-advice/consumer-advisory-committee-cac (Accessed May 3, 2024).
288. PHARMAC. Consumer Advisory Committee (CAC) Terms of Reference. (2021). Available online at: https://pharmac.govt.nz/about/expert-advice/consumer-advisory-committee-cac/cac-tor (Accessed May 3, 2024).
289. PHARMAC. Priority Lists for Funding Applications. (2024). Available online at: https://pharmac.govt.nz/medicine-funding-and-supply/the-funding-process/priority-lists (Accessed May 3, 2024).
290. PHARMAC. Operating Policies and Procedures of PHARMAC. (2017). Available online at: https://pharmac.govt.nz/assets/operating-policies-and-procedures-4th-ed.pdf (Accessed May 3, 2024).
291. PHARMAC. Guidelines for Funding Applications to Pharmac. (2023). Available online at: https://pharmac.govt.nz/assets/supplier-guidelines.pdf (Accessed May 3, 2024).
292. PHARMAC. From Application to Funded Medicine: Pharmac's Process. (2024). Available online at: https://pharmac.govt.nz/medicine-funding-and-supply/the-funding-process/from-application-to-funded-medicine-how-we-fund-a-medicine (Accessed May 3, 2024).
293. PHARMAC. How Pharmac Works. (2023). Available online at: https://pharmac.govt.nz/about/what-we-do/how-pharmac-works (Accessed May 3, 2024).
294. PHARMAC. Pharmacology and Therapeutics Advisory Committee (PTAC) Terms of Reference July 2021. (2021). Available online at: https://pharmac.govt.nz/about/expert-advice/pharmacology-and-therapeutics-advisory-committee-ptac/ptac-terms-of-reference-july-2021 (Accessed May 3, 2024).
Keywords: health technology, health technology assessment (HTA), patient engagement (PE), patient involvement, public involvement, patient participation
Citation: Puebla M, Korrodi-Gregório L, Trentin L, De Maria A and Blanqué N (2025) A comparative analysis of patient participation in health technology assessment systems worldwide: trends and practices. Front. Public Health 13:1693886. doi: 10.3389/fpubh.2025.1693886
Received: 27 August 2025; Accepted: 13 October 2025;
Published: 31 October 2025.
Edited by:
Gabriel Gomes De Oliveira, State University of Campinas, BrazilReviewed by:
Rok Hren, Syreon Research Institute, HungaryEva Reviriego Rodrigo, Basque Foundation for Health Innovation and Research, Spain
Copyright © 2025 Puebla, Korrodi-Gregório, Trentin, De Maria and Blanqué. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcos Puebla, bWFyY29zLnB1ZWJsYUBhbGlyYWhlYWx0aC5jb20=; Annabel De Maria, YW5uYWJlbC5kZW1hcmlhQGFsaXJhaGVhbHRoLmNvbQ==; Nerea Blanqué, bmVyZWEuYmxhbnF1ZUBhbGlyYWhlYWx0aC5jb20=