 Chendi Wang
Chendi Wang Yujian Pan
Yujian Pan Xingjian Li
Xingjian Li- Department of Construction Management and Real Estate, School of Economics and Management, Nanjing Tech University, Nanjing, China
This study examines relationships between the built environment (BE) and social interaction (SI) among older adults in care homes. A mixed-methods design combined questionnaires (n = 119), environmental measurements, and behavioral observations across three care homes. An integrated BE-SI model, developed using multivariate statistical analyses, identified key environmental determinants of SI. Results indicate that recreational spaces, lighting, functional facilities, and accessibility significantly influenced interpersonal interactions, activity engagement, resident-caregiver relations, and conflict. Objective environmental measures corroborated survey and observational findings: care homes with larger recreational areas and improved functional accessibility showed higher frequencies of resident social engagement. These findings highlight the critical role of environmental design in promoting social participation among older residents. The study offers evidence-based recommendations for designers, facility managers, and policymakers to create age-friendly care-home environments that foster social interaction and enhance residents’ wellbeing. The BE-SI model provides a practical framework for future research, facility evaluation, and policy implementation.
1 Introduction
The global aging population demands urgent enhancement of institutional care environments. By 2050, one in six people worldwide will be over 65 (1), with China projected to have 400 million older adults by 2040 (2). Care homes, serving older adults with physical or cognitive impairments (3), face critical challenges. Despite ensuring safety and professional care, they often disrupt residents’ social networks. Residents experience a 40–60% reduction in meaningful social interactions (SI) compared to peers aging in place (4), leading to “relocation shock” marked by broken community ties and limited mobility (5, 6). Unlike community settings where SI arise naturally, care homes impose constraints through physical limitations and institutional routines, resulting in interactions dominated by structured activities and caregiver mediation (7, 8). These occur within built environments (BE) prioritizing operational efficiency over social facilitation (9). This study explores residents’ subjective experiences of environmental factors affecting SI. By emphasizing lived perceptions over architectural metrics (10–12), it offers design recommendations to balance functional and social needs, guiding care homes toward social sustainability.
2 Literature review
The relationship between older adults’ social lives and their physical surroundings is powerfully explained by the Person-Environment (P-E) fit theory. This foundational theory posits that wellbeing and adaptive behavior depend on the congruence between an individual’s personal characteristics (P)—such as their needs, abilities, and preferences—and their external environment (E), which includes its demands and resources (13–15). A strong P-E fit in care homes is thus essential for fostering positive social outcomes and mitigating the challenges of aging.
2.1 Social interaction of older people
As people age, their social interaction abilities diminish due to cognitive decline, physical limitations, and sensory impairments (16, 17). This decline is more pronounced in care homes, leading to increased social isolation (5, 18). Interpersonal interactions, including group conversations, casual dialogues, and resident visits, are vital for maintaining social bonds (19–21), enhancing emotional wellbeing, and reducing loneliness (11, 12, 22). However, the frequency and quality of these interactions may be significantly influenced by the environment (23). Activity engagement in care homes presents unique characteristics shaped by aging-related limitations, institutional environments, and social dynamics. Most residents require mobility aids for participation and demonstrate higher dependence on structured group activities compared to community-dwelling peers (24). Centralized activity hubs and circular seating arrangements increase spontaneous communication (25).
Caregiver relationships are crucial for social interactions and wellbeing in care facilities (26, 27). These relationships provide social support and reduce loneliness (28, 29). Well-designed layouts that minimize physical barriers improve caregiver-resident interactions (30). Positive relationships provide emotional support, enhancing self-confidence and encouraging interaction initiation (31). Conflict in care homes is intertwined with built environment design. Environmental conditions shape conflict frequency, intensity, and resolution (32). Poorly designed recreational areas may heighten interpersonal friction by limiting residents’ autonomy (33). Conversely, intentional design with well-zoned spaces for quiet relaxation versus group activities reduces sensory overload (34), while functional layouts separating high-traffic zones from private retreats help manage group dynamics (35).
2.2 Built environment in care homes
In care homes, the built environment (BE), encompassing distinct spaces, buildings, and surroundings, serves as the primary living area for older adults (36, 37). Space design fundamentally influences residents’ mobility and social interaction (SI) (26, 38). While narrow spaces may restrict movement and heighten territorial disputes (34). Recreational areas designed with accessibility act as hubs for physical and social participation (39, 78). Spacious entrances and wide passageways encourage involvement in cultural activities (40), while well-planned zones mitigate overcrowding. Furniture and equipment arrangement directly impacts SI. Circular seating layouts foster face-to-face interactions and group cohesion (41), whereas haphazard placements fragment social groups or hinder supervision (42). Daylight-filled areas enhance visual clarity and uplift moods, while poorly lit environments may induce anxiety, particularly for those with cognitive impairments (43, 44). Distance between residential units and recreational zones shapes participation willingness, with shorter pathways encouraging frequent use of communal spaces (45).
Diverse facilities support varied activity engagements, with well-equipped rooms enabling group exercises and fostering collaboration. Inadequate facilities may limit options, leading to boredom (46). This is a classic example of poor P-E fit, where the environment fails to provide the resources needed to meet residents’ social and recreational needs. Barrier-free design principles ensure equitable access to SI, empowering residents’ autonomy and reducing dependency-related tensions (32). Private spaces enable confidential conversations, reducing conflict in shared environments (14, 15). Indoor environmental factors critically shape residents’ social behaviors (26). Stable temperatures reduce irritability during communal activities, while excessive noise disrupts dialogue. Natural daylight enhances mood and engagement, whereas poor ventilation may fragment social cohesion. Sensory-friendly designs create spaces where trust and conversation thrive (47). Collectively, these elements of the built environment constitute the “environmental press” which, according to the ecological theory of aging, interacts with residents’ personal “competence” to shape their daily social outcomes.
2.3 Research gap
Prior work linking the BE to SI typically examines single environmental attributes (e.g., walkability, greenness, or lighting) in community settings and often among mixed-age adults rather than older adults living in care homes (see Supplementary Table 1). Evidence from care homes is comparatively sparse and, where available, tends to address overall quality of life or loneliness rather than the everyday social interactions that sustain wellbeing in congregate living. Moreover, institutional studies frequently rely on self-reports and proxy indicators, provide limited within-facility comparisons, and rarely consider how multiple BE dimensions operate together (e.g., accessibility, functional facilities, and privacy) to shape different forms of SI. As a result, we still lack systematic, setting-specific evidence on how care home environmental configurations influence residents’ SI. This study addresses this gap by focusing on older adults living in care homes, examining multi-dimensional BE features and their associations with observed interpersonal, small-group, and caregiver-related interactions across facilities.
3 Conceptual model
Based on a comprehensive review of existing literature, it is clear that the built environment plays a pivotal role in influencing SI among older adults. The importance of the BE in shaping social interactions aligns with the ecological theory of aging (48, 49). This study proposes a conceptual model. Nine care-home built-environment (BE) factors are hypothesized to influence social interaction among residents, covering interpersonal interaction, activity engagement, caregiver relationship, and conflict (see Figure 1). This model extends the scope of P–E theory by applying it to care home settings and using it to explain how specific environmental features shape SI among residents. This study underscores the social needs of care home residents and the environment’s potential to support or hinder those needs. By identifying specific environmental features linked to residents’ SI, these findings provide actionable guidance for improving care home environments and, in turn, promoting residents’ mental and physical wellbeing.
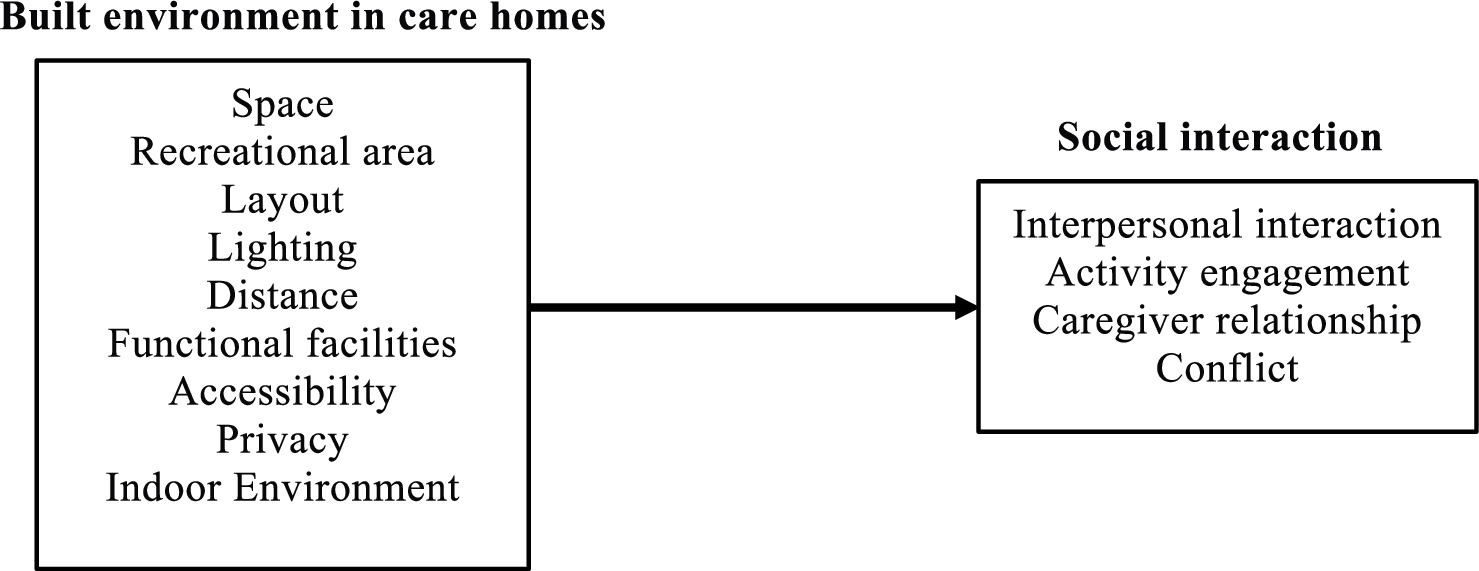
Figure 1. A conceptual BE–SI model for the older adults in care homes.
4 Research methods
4.1 Research design
This study employed a mixed-methods research design to systematically investigate the relationships between the built environment (BE) and social interaction (SI) among older adults in care homes. The overall procedural framework of the research is illustrated in Figure 2. The process began with a comprehensive literature review and the establishment of a theoretical foundation based on the ecological theory of aging and p-e fit theory, leading to the development of a conceptual BE-SI model. Subsequently, an empirical investigation was conducted in three care homes, utilizing a concurrent data collection strategy that integrated objective environmental measurements, direct behavioral observations, and a subjective questionnaire survey. Finally, the collected data were subjected to a series of statistical analyses, including factor analysis, multiple regression, and structural equation modeling (SEM), to test the conceptual model and develop a final, integrated BE-SI model.
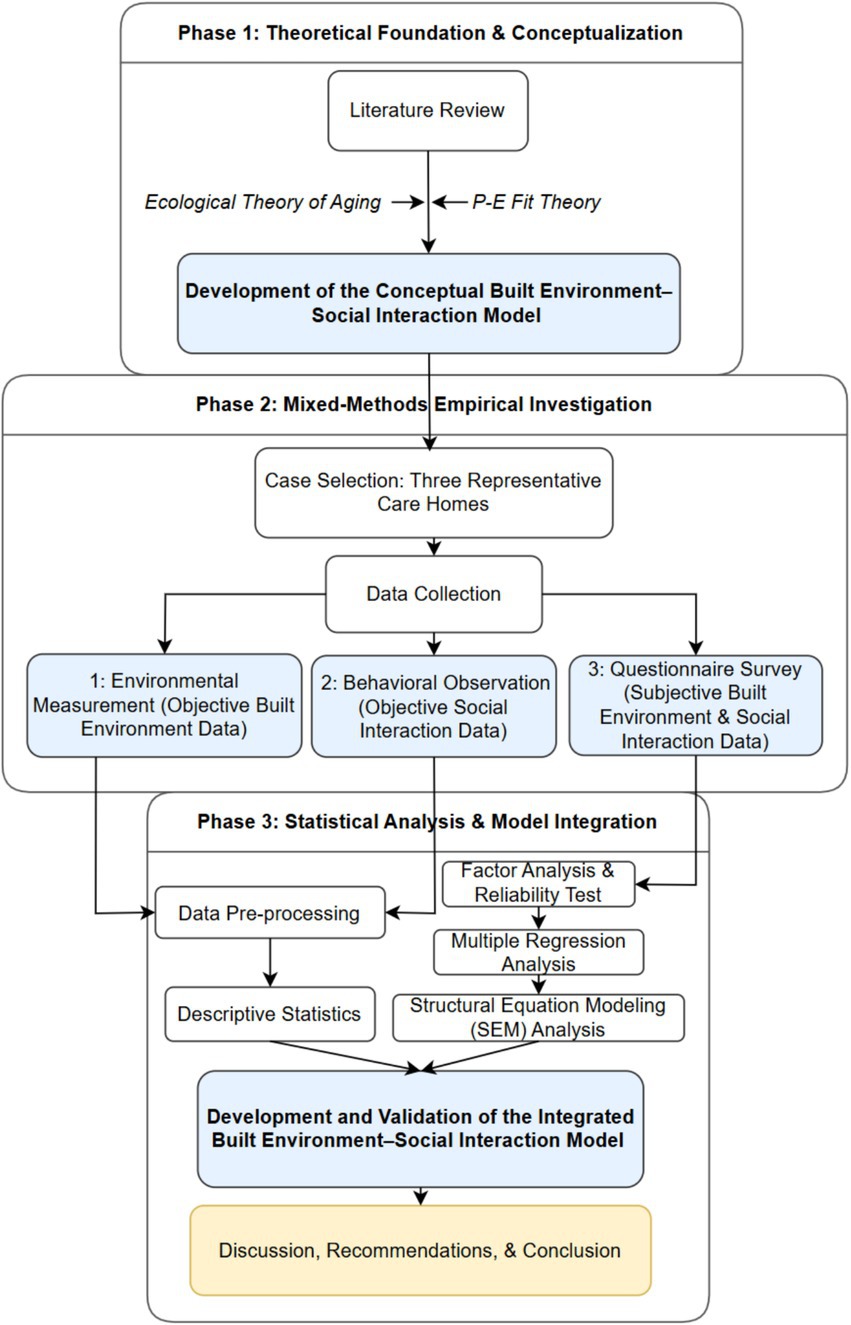
Figure 2. Research framework.
Three representative care homes were deliberately selected: The first, a large-scale public facility established in 2023, has 12 floors, spans 260,000 square meters, employs 500 staff members, and accommodates 1,000 residents. The two smaller private facilities are Home 2 and Home 3. Home 2, built in 2014, is a four-story building with 2,000 m2 of floor area, 20 staff members, and capacity for 60 residents. Home 3, completed in 2020, is a three-story facility with 3,080 m2 of floor area, 30 staff members, and capacity for 80 residents. The research procedures were reviewed and approved by the university’s research ethics committee to ensure compliance with ethical guidelines (Ethical Review Number: NJTECH-18; Date: 2024.07.03), and written consent was obtained from all participants through signed consent forms.
4.2 Environmental measurement and behavior observation
Indoor environmental measurements were conducted in each care home at approximately 10:00 a.m. on Saturdays using calibrated, high-precision instruments, following international standards. Illuminance was measured with a digital lux meter (TA636A, CEM Instruments, China) per ISO 8995-1:2002, using five points (center and four corners, ≥0.5 m from walls) at 850 mm height to represent seated eye level. The mean of these readings indicated overall lighting conditions. Air temperature and relative humidity were measured at the same five points using a digital thermohygrometer (TA620, CEM Instruments, China), following ISO 7726:1998. Measurements were taken at 1.1 m height, avoiding direct sunlight and ventilation sources. The average values reflected thermal and humidity conditions. Ambient noise was assessed using a Class 1 sound level meter (AR844, SMART SENSOR, China) in line with IEC 61672–1:2013. A-weighted equivalent continuous sound levels (LAeq) were recorded over 2-min intervals at each point, and the mean value was used to characterize the acoustic environment. Between 2:00 p.m. and 4:00 p.m. on the same day, three independent observers conducted structured behavioral observations using a standardized coding form. The final social interaction score was the average of their recorded counts.
4.3 Questionnaire survey
Based on the literature review and conceptual model (Figure 1), a questionnaire survey was designed to collect quantitative data from older adults in care homes. The questions were simple and easily understandable, focusing on participants’ subjective perceptions of the BE and their real experiences of social interactions. Given the lack of a single scale that fully integrates both environmental factors and social interactions, items of BE and SI were selected from separate scales that address each dimension independently, while ensuring their relevance to the research objectives. A five-point Likert scale (1 = strongly/extremely disagree, 5 = strongly/extremely agree) was applied to assess participants’ views on SI and BE. The scale had three sections: (1) background information; (2) SI experiences (50, 51); and (3) agreement with the description of BE (26, 39, 52). The survey was administered face-to-face in the activity room. A total of 119 residents took part in the study. These participants met the following inclusion criteria: they were aged 60 years or above, had resided in the care homes for a period exceeding 1 month, and possessed the cognitive and physical ability to understand and respond to the questionnaire items.
4.4 Statistical methods
To ensure the reliability and validity of the findings, a range of analytical methods were employed. The quantitative data collected from the questionnaire survey were analyzed using several techniques, including factor analysis, reliability testing, multiple regression analysis, and structural equation modeling (SEM). First, factor analysis was conducted to explore the dimensional structure of the SI items and to group them into distinct factors. Second, reliability tests, specifically using Cronbach’s alpha, were performed to assess the internal consistency of the BE and SI factors. Third, multiple regression analysis was utilized to develop regression models, aiming to identify the relationships between the BE in care homes and the SI of older adults. Lastly, structural equation modeling (SEM) was applied to establish structural models that reveal the relationships between latent and observed variables (53). These comprehensive analyses provided a robust framework for understanding the complex interactions between the BE and SI among older adults in care homes.
5 Results
5.1 Demographics
This study included 119 participants, with 74% aged 70 years or older (22.7% aged 70–74 years, 24.4% aged 75–79 years, and 26.9% aged 80 years or older). Females comprised 54.6% of the sample, slightly exceeding males (45.4%). Most participants (84.0%) had resided in care homes for at least 3 months, with 37.8% living there for 3 months to 1 year, 31.1% for 1–3 years, and 15.1% for over 3 years. Regarding marital status, 63.0% were widowed, while 37.0% lived with spouses. Educational attainment varied: 55.5% held college degrees or higher, 19.3% completed secondary education, 10.9% had primary education, and 14.3% received no formal education. All participants demonstrated unimpaired verbal communication abilities.
5.2 Environment measurement and behavioral observation in care homes
Table 1 compares environmental aspects across three care homes. Homes 1 and 3 have larger residential areas than Home 2. Home 3 features wall holes instead of traditional windows in the dining area. Home 1 has the most extensive recreational area. Regarding equipment, Home 1 contains fitness equipment, Home 3 has cultural items (calligraphy desks, pianos), while Home 2 lacks these amenities. Homes 1 and 3 are better equipped with elevators and call bells than Home 2. Comparative analysis of indoor environments and social interaction (SI) frequency within recreational areas, activity rooms, and dining areas revealed that Home 1 demonstrated higher Total Frequency of SI compared to Homes 2 and 3 (Table 2). The floor plans of the three care homes were briefly mapped out in this study to provide a clearer overview of the spatial structure (see Supplementary Figure 1).
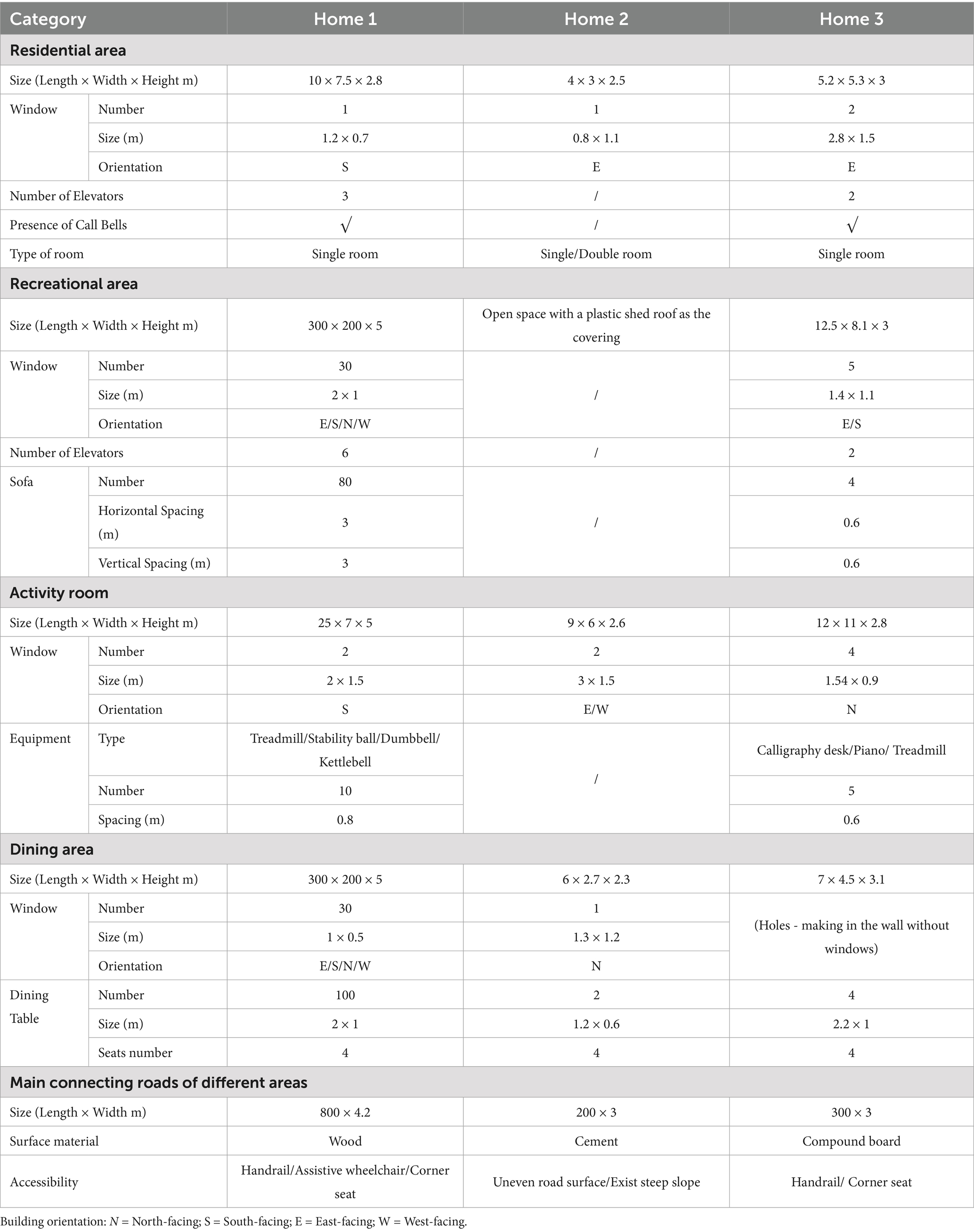
Table 1. Detailed information of selected care homes.
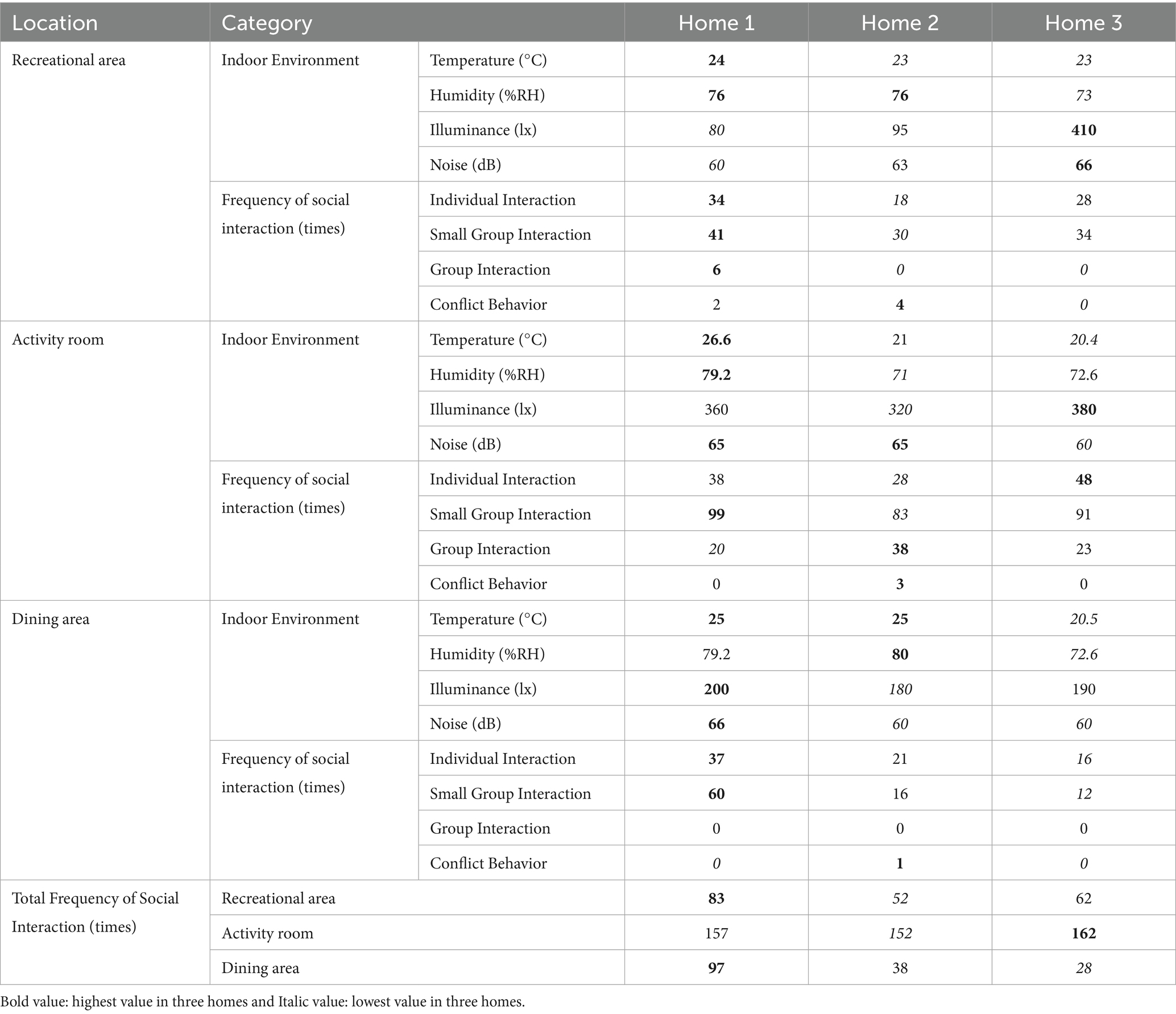
Table 2. Indoor environment and social interactions of old adults in care homes.
5.3 Factor analysis and reliability test
Social interaction (SI) factors were identified through factor analysis (Table 3). The sample-to-item ratio was 7:1, exceeding the recommended 5:1 minimum and ensuring robust statistical power (54). The descriptive results (i.e., mean, median, minimum, and maximum scores) for the independent and dependent variables were presented in Supplementary Table 2. All factor loadings were above 0.5, indicating significant item contributions (55). The Kaiser-Meyer-Olkin measure was 0.813, well above the 0.60 threshold, confirming data suitability for factor extraction (56). Internal consistency of both built environment (BE) and SI factors was evaluated using reliability tests (Tables 3, 4). Cronbach’s alpha values exceeded 0.6, considered acceptable (57), indicating agreeable internal consistency. The measures were reliable without requiring further modification, supporting construct validity.
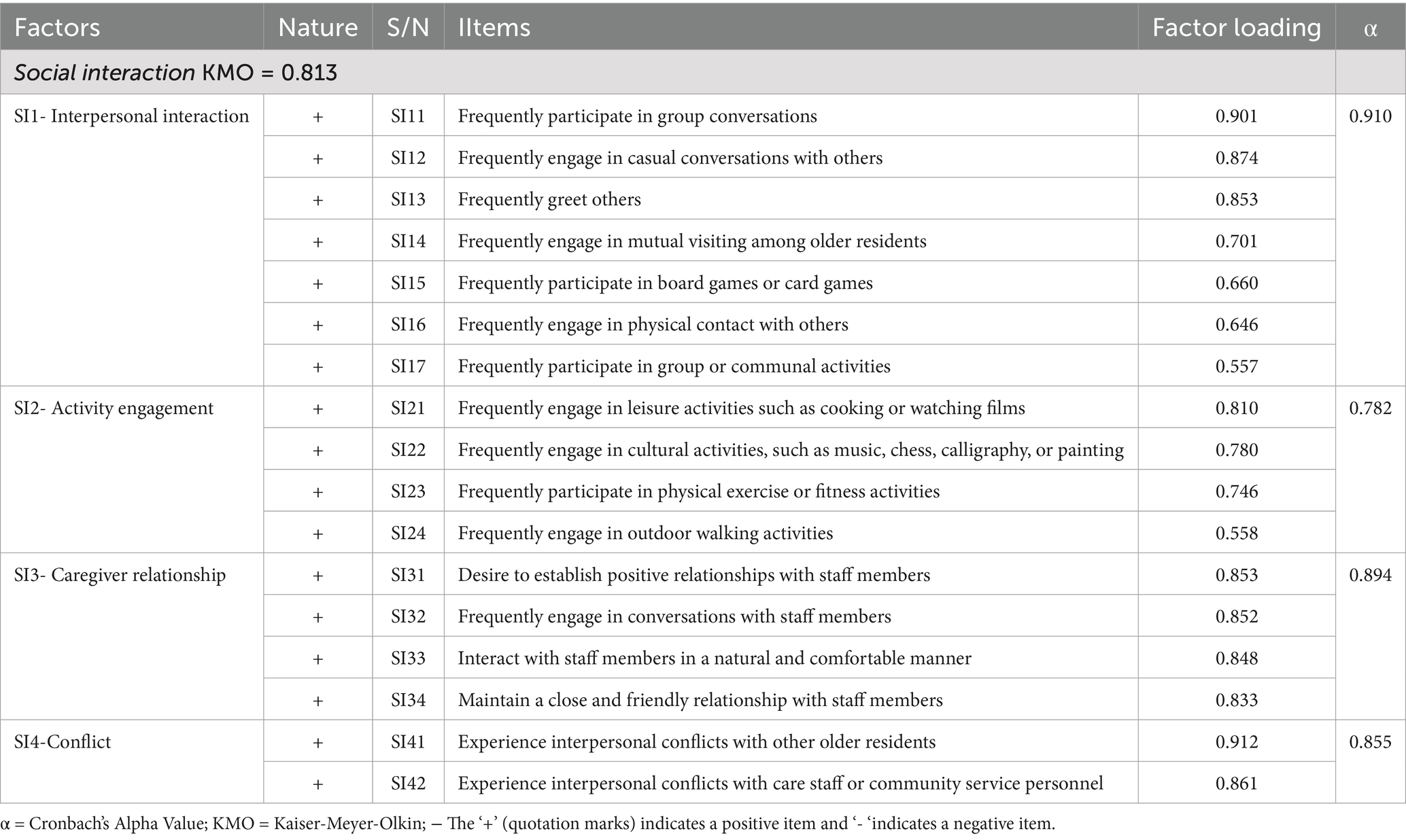
Table 3. Factor analysis and reliability of social interaction factors of older people.
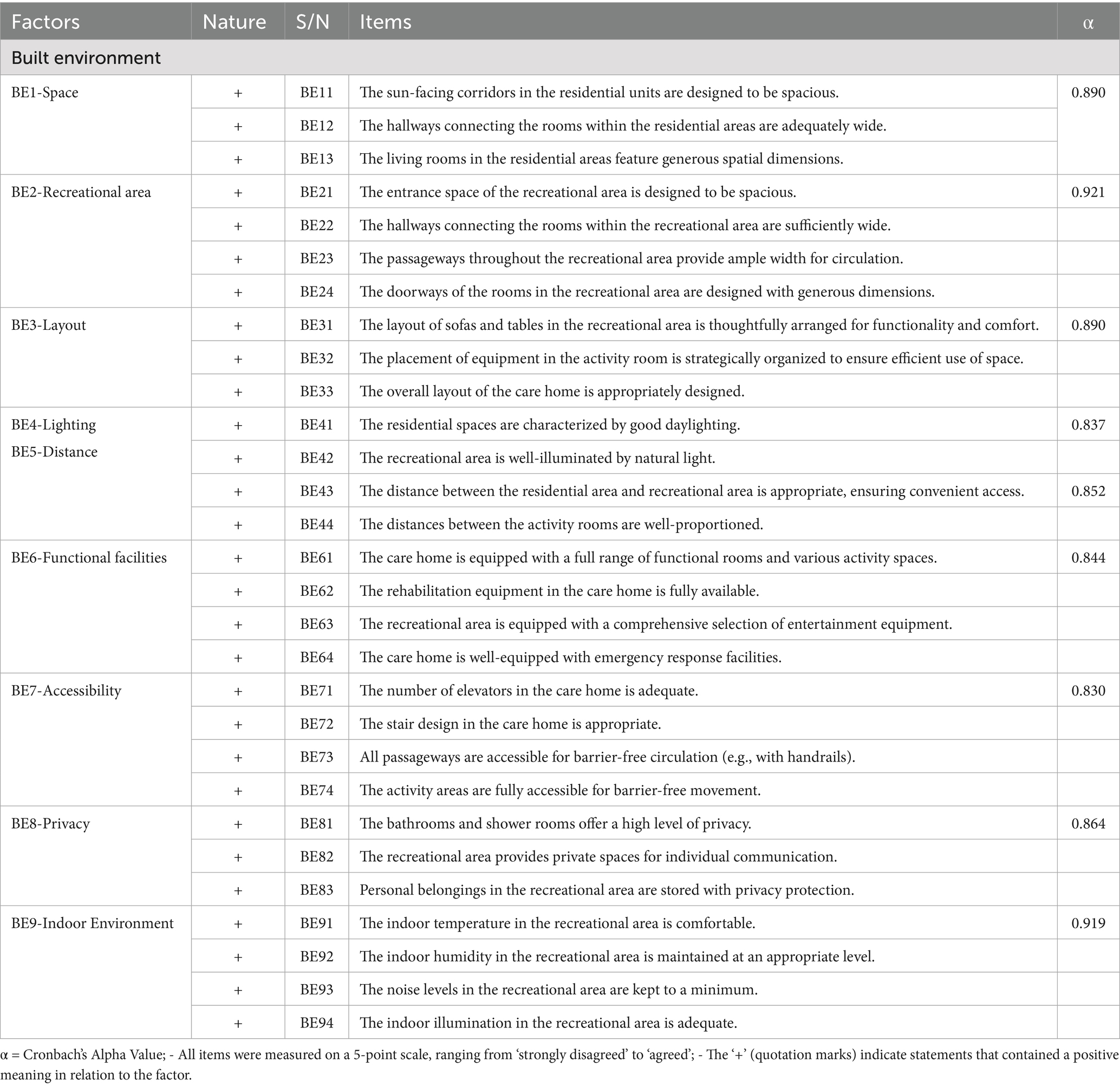
Table 4. Reliability analysis for built environment factors in care homes.
5.4 Multiple regression analysis
The multiple regression analysis was used to develop four models to examine the relationships between BE factors and SI among older adults (see Table 5). Model 1 indicated that functional facilities (BE6) positively influenced interpersonal interaction (SI1), while privacy (BE8) had a negative effect. This model explained 7.9% of the variance in SI. Model 2 demonstrated that accessibility (BE7) was a significant positive predictor of activity engagement (SI2), accounting for 16.0% of the variance. Model 3 showed that accessibility (BE7) also positively affected caregiver relationships (SI3), explaining 8.3% of the variance. Finally, Model 4 found that recreational areas (BE2) and lighting (BE4) negatively impacted conflict (SI4), with the model accounting for 21.1% of the variance. These models collectively highlighted the critical role of built environment factors in shaping SI, explaining between 7.9 and 21.1% of the variance in SI outcomes.
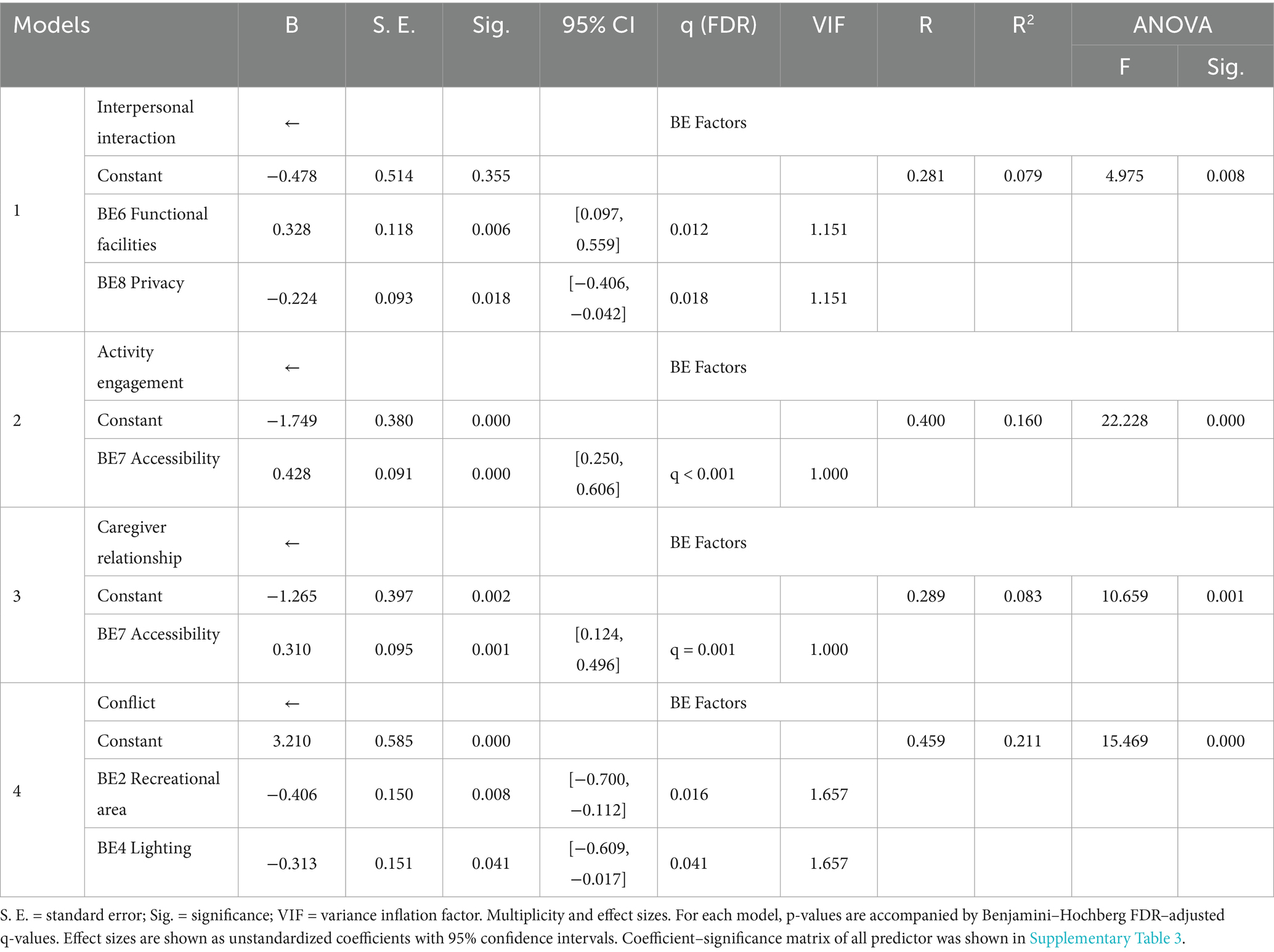
Table 5. Multiple regression model for built environment factors and social interaction of older people.
Regression assumptions were checked in SPSS (see Supplementary Figures 2a–2d). Linearity was assessed by inspecting standardized-residuals versus predicted values; plots showed approximately random scatter with no systematic curvature across models. The histogram and Normal P–P plots indicated acceptable normality for Model 3 (Shapiro–Wilk p = 0.192), with departures for Models 1, 2, and 4 (Shapiro–Wilk p = 0.005, 0.045, and < 0.001, respectively). Homoscedasticity was examined via residual plots and a Glejser test; Models 1–3 showed no evidence of heteroskedasticity (p = 0.206, 0.323, 0.133), whereas Model 4 indicated heteroskedasticity (p < 0.001). All variance inflation factors were below 2 (Max VIFs = 1.151, 1.000, 1.000, 1.657), indicating no multicollinearity. These diagnostics suggest that the multiple linear regression assumptions were adequately met for Models 1–3 and partially met for Model 4; deviations are noted and results are interpreted with appropriate caution (see Supplementary Table 5).
5.5 Structural equation model
Structural equation models (SEMs) were developed based on the multiple regression models presented in Figures 3–6. The model fit was considered acceptable when the following criteria were met: x2/df < 3, RMSEA < 0.08, GFI > 0.90, CFI > 0.90, IFI > 0.90, and TLI > 0.90 (58, 59). The values of sample-to-parameter ratio were ranged from 7:1 to 12:1, satisfying the lowest requirement of 5:1 (60). In this study, the SEMs were deemed satisfactory as at least four fit indices met recommended thresholds (61, 62). Hence, although some of the indices was not met the acceptable value (e.g., RMSEA), the model is acceptable because at least four other fit indices met recommended thresholds (79, 80). The model labeled BE-Interpersonal Interaction I was constructed based on the relationships between built environment factors and interpersonal interaction (SI1), as identified in the regression analysis (see Figure 3). To enhance model fit, an additional path was incorporated between “Frequently engage in mutual visiting among older residents” (SI14) and “Frequently engage in physical contact with others” (SI16), resulting in the revised BE-Interpersonal Interaction II model (x2/df = 2.532, RMSEA = 0.114, CFI = 0.903, IFI = 0.905, TLI = 0.901).
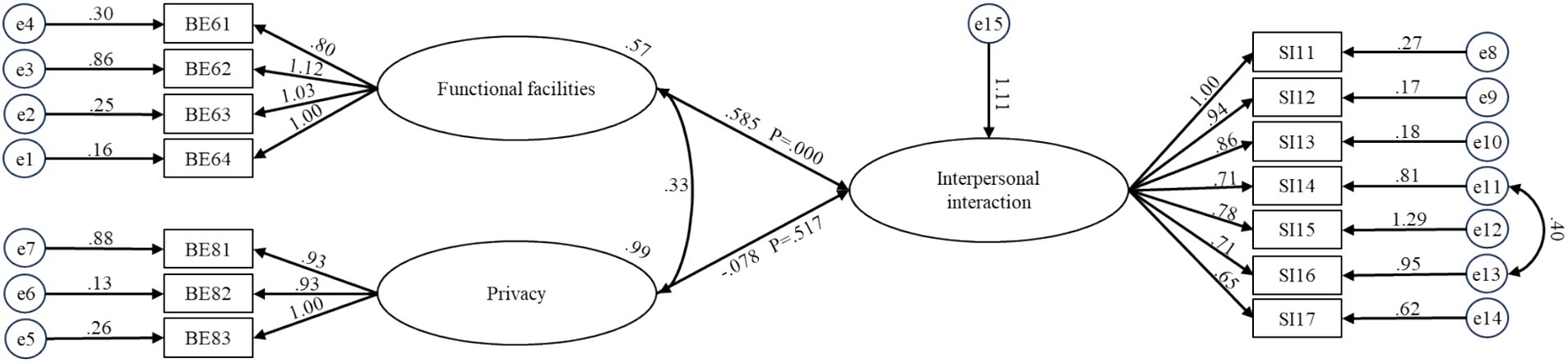
Figure 3. Structural equation model for BE-interpersonal interaction for older people in care homes.

Figure 4. Structural equation model for BE-activity engagement for older people in care homes.

Figure 5. Structural equation model for BE-caregiver relationship for older people in care homes.
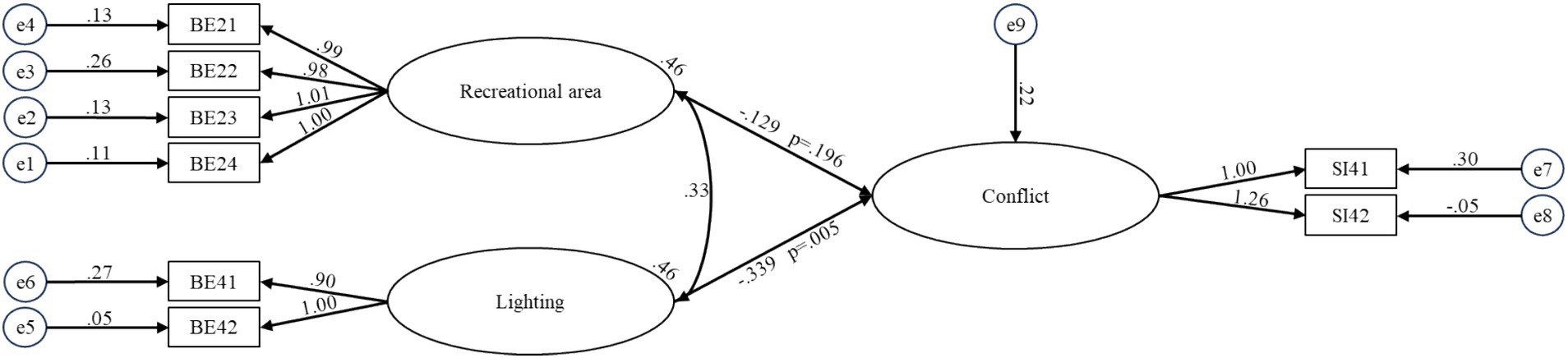
Figure 6. Structural equation model for BE-conflict for older people in care homes.
The BE-Activity Engagement model was developed to illustrate the influence of the BE on activity engagement (SI2) among older residents in care homes (see Figure 4). The model demonstrated an adequate fit with the following indices: x2/df = 2.533, RMSEA = 0.114, GFI = 0.906, CFI = 0.932, and IFI = 0.933. To assess the relationship between the BE and caregiver relationships (SI3) of older adults, the BE-Caregiver Relationship model was formulated, which also exhibited an acceptable fit (x2/df = 2.054, RMSEA = 0.095, GFI = 0.928, CFI = 0.965, IFI = 0.965) (see Figure 5). Finally, the BE-Conflict model was constructed to capture the interactions between the BE and conflict (SI4) among older residents (see Figure 6). This model exhibited excellent fit, with indices of x2/df = 1.212, RMSEA = 0.042, GFI = 0.959, CFI = 0.994, and IFI = 0.995.
The maximum likelihood estimates for the four optimal structural equation models are presented in Figures 3-6. The results reveal the following findings: older residents’ agreement with functional facilities was found to have a positive effect on interpersonal interaction, with a standardized path coefficient of 0.585, and this relationship was statistically significant (p < 0.001) (BE6-SI1). In contrast, privacy showed a negative path coefficient of −0.078, but this relationship was not statistically significant (p = 0.517), indicating no meaningful impact on interpersonal interaction (BE8-SI1). Accessibility was positively associated with both activity engagement and caregiver relationships, with standardized path coefficients of 0.541 (p < 0.001) for activity engagement (BE7-SI2) and 0.459 (p < 0.001) for caregiver relationships (BE7-SI3). The availability of recreational areas showed an inverse relationship with conflict, with a path coefficient of −0.129, but this effect was not statistically significant (p = 0.196) (BE2-SI4). Lastly, lighting had a negative path coefficient of −0.339, which was statistically significant (p = 0.005), indicating a substantial effect on conflict (BE4-SI4). SEM structural paths with effect sizes (95% CIs) and FDR-adjusted q-values were presented in Supplementary Table 4.
5.6 Model establishment
Through the construction of regression models and structural equation models (SEM), an integrated BE–SI model was developed (see Figure 7). This BE–SI model illustrates the relationships between the BE in care homes and SI among older adults. The final model demonstrates that the richness of functional facilities has a facilitating effect on interpersonal interaction, a relationship supported by both the regression model and SEM. On the other hand, an excessive emphasis on privacy appears to hinder interpersonal interaction, suggesting that an overemphasis on private space can limit opportunities for SI. Furthermore, the regression equation and SEM both indicate that good accessibility significantly enhances activity engagement and caregiver relationship. Additionally, the insufficient configuration of recreational areas and inadequate lighting can exacerbate conflicts.
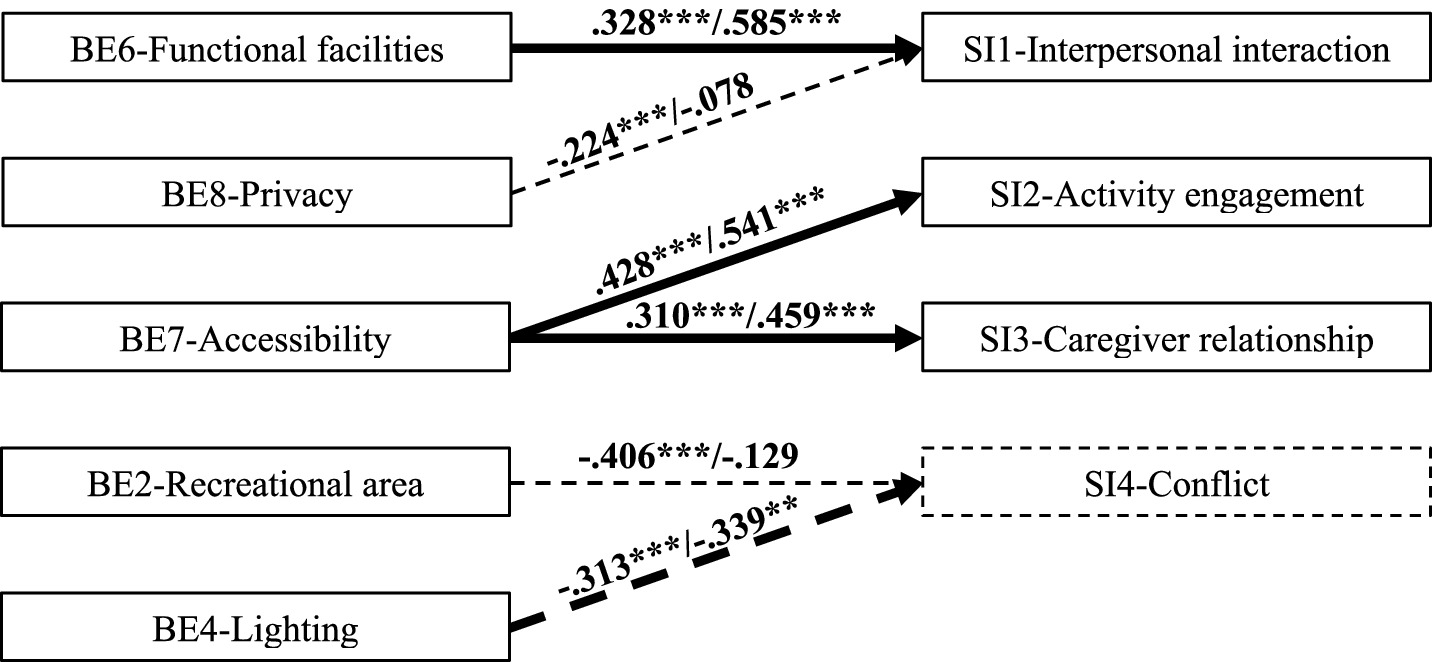
Figure 7. An integrated BE–SI model for older people in care homes.  a positive relationship confirmed by regression and SEM;
a positive relationship confirmed by regression and SEM;  a negative relationship confirmed by regression;
a negative relationship confirmed by regression;  a negative relationship confirmed by regression and SEM.
a negative relationship confirmed by regression and SEM.  positive factors;
positive factors;  negative factors.
negative factors.
6 Discussion
The study’s findings can be effectively interpreted through the lens of the ecological theory of aging, which posits that social outcomes are a function of the fit between residents’ competence and their environmental press (13). Specifically, functional facilities and privacy were found to significantly influence interpersonal interactions. Homes 1 and 3, equipped with diverse facilities such as treadmills, dumbbells, calligraphy tables, and open communal areas, recorded 38 and 48 instances of individual interactions, respectively, during a two-hour observation in activity rooms. In contrast, Home 2, lacking similar facilities, recorded only 28 instances (Table 2). Functional facilities not only promote group participation but also facilitate spontaneous exchanges during unstructured moments, such as waiting or resting in shared spaces. This pattern confirms prior evidence that amenity-rich environments are associated with greater informal contact and participation among older adults, whereas amenity-poor settings dampen spontaneous exchanges during unstructured time (63, 64). Privacy presents a more nuanced effect. While essential for residents’ sense of security and respect, excessive privacy can restrict social opportunities (14, 15). Home 2 is unique in offering double rooms, which provide lower privacy than the single rooms in Homes 1 and 3. Shared bathrooms in Home 2 may lead to privacy concerns; however, residents there engage more frequently in casual interactions and room visits. Conversely, the higher privacy of single rooms in Homes 1 and 3 limits social interactions within personal spaces, which aligns with evidence that privacy gains may trade off with fewer incidental contacts in residential care settings (63), highlighting a trade-off between privacy and social engagement in care home design.
Activity engagement depends heavily on accessibility. Observational data indicates that Home 1, with its six elevators and wide corridors (4.2 meters), recorded 41 instances of small group interaction during the observation period, compared to only 30 in Home 2, which lacks elevators and has narrower corridors (Table 2). When the environmental press in the form of physical barriers exceeds residents’ physical competence, participation is suppressed. Conversely, proper accessibility ensures a better person-environment fit, enabling residents to independently navigate between spaces and participate in activities without relying on assistance (65). This interpretation is consistent with studies showing that corridor width, circulation, and overall spatial configuration influence encounter rates and engagement in long-term care environments (63, 66). Wide corridors and barrier-free pathways, as seen in Home 1 and Home 3, allow seamless movement between different areas, fostering greater participation in both structured activities, such as group exercises, and unstructured activities, such as walking or painting. As shown in Table 1, the accessible pathway in Home 2 has an inappropriate slope and insufficient reserved space, significantly reducing the accessibility of Home 2. This increases the difficulty for older residents to reach social areas, which is reflected in the observed lower frequency of social interactions in these areas compared to the other two care homes.
The caregiver relationship dimension reflects the frequency and quality of interactions between residents and care staff. Accessibility emerged as a significant factor influencing these interactions. Observational data suggests that the accessible design of Home 1 and Home 3 reduces the environmental press on both residents and staff, providing ample and suitable space for interactions. This improved person-environment fit fosters a sense of trust and comfort, encouraging residents to engage with caregivers more frequently. For example, caregivers in Home 3 were observed moving easily between activity rooms, recreational areas, and dining spaces, increasing their visibility and availability to residents. This design fosters a sense of trust and comfort, encouraging residents to engage with caregivers more frequently. Additionally, the design of communal spaces plays an indirect but important role in caregiver relationships (65). This is consistent with studies showing that improved circulation and proximity—key aspects of accessibility—are associated with more frequent, low-effort staff communication and contact (66). Recreational areas in Home 1 are equipped with comfortable seating, large windows providing natural light, and open layouts, creating inviting environments where residents and caregivers can interact. These spaces enable staff to observe and support residents during activities, providing assistance when needed and engaging in casual conversations. In contrast, Home 2’s limited recreational area and restricted accessibility reduced opportunities for such interactions, likely contributing to weaker caregiver-resident bonds.
Conflict behavior is significantly negatively influenced by the recreational area and lighting. The size and layout of the recreational area directly influence the potential for conflicts. In Home 1, the ample space lowers the negative environmental press associated with crowding, allowing residents to participate in activities without encroaching on others’ personal space and thus reducing friction (see Table 1). By comparison, the constrained layout in Home 2 likely exacerbates tensions during group activities, as residents may feel overcrowded or frustrated by limited resources. With increasing light levels in care homes, conflicts in indoor spaces tend to decrease (see Table 2). This effect can be attributed to brighter lighting in recreational areas, activity rooms, and dining spaces, which creates a brighter and more visually comfortable environment. Such conditions contribute to the cultivation of positive emotions and the reduction of stress, ultimately leading to a decrease in conflict occurrences (67). Conversely, the dim lighting and narrow space in Home 2 create an excessive environmental press that can overwhelm residents’ coping competence, contributing to feelings of confinement or irritability and increasing the likelihood of interpersonal conflict.
7 Practical recommendations
Recreational areas are the social heart of a care home, and their design should go beyond simply providing space; it must actively cultivate a harmonious social ecosystem. As this study found that inadequate recreational areas can exacerbate conflict, the design should offer a spectrum of social opportunities. This means creating not just large, open zones for group activities, but also semi-enclosed nooks for quiet one-on-one conversations and designated areas for small group pastimes like card games. This design implication is contextually original yet consistent with prior work: studies recommend small, semi-enclosed alcoves linked to public spaces to vitalise everyday encounters in care homes (63), and research on small-scale/household settings reports benefits of dispersed, small social areas over a single large common room (68, 69). By providing this variety, residents can choose their desired level of engagement, reducing the friction that arises from competing social needs in a single, monolithic space. Furniture should then be arranged to support these diverse “social niches,” facilitating everything from intimate chats to lively group discussions.
This study’s finding that poor lighting correlates with increased conflict suggests that lighting design is not merely a technical issue of visibility, but a critical tool for regulating the emotional atmosphere of a space. The primary goal should be to create a bright, open, and non-threatening environment that promotes positive emotions and psychological security. Maximizing natural light is paramount, as it connects residents to the outdoors and daily rhythms. For artificial lighting, beyond meeting illuminance standards (300–500 lx), the focus should be on creating a gentle, warm ambiance that is psychologically calming (70). By treating light as a key factor in emotional wellbeing, we can design spaces that proactively de-escalate tension and foster more positive social interactions.
As this research demonstrates a direct link between functional facilities and increased interpersonal interaction, their provision should be viewed as an investment in the community’s social capital. Beyond simply offering a diverse range of equipment, the strategic placement of these facilities is key to transforming them into social hubs. For instance, placing comfortable seating near rehabilitation equipment or a tea station next to a calligraphy table encourages the “spontaneous exchanges during unstructured moments” observed in this study. The goal is to design for the social life that happens around the activity, not just the activity itself. This turns functional spaces into vibrant points of connection, sparking conversations and shared experiences.
Accessibility is arguably the most critical foundation for a thriving social environment, as our findings link it strongly to both activity engagement and positive caregiver relationships. The design philosophy should extend beyond mere compliance with codes; it should aim to maximize resident autonomy and dignity (71). When a resident can independently and safely navigate from their room to a recreational area, they are empowered to choose to be social. This sense of independence reduces reliance on staff for basic mobility, transforming caregiver interactions from logistical tasks into more meaningful social exchanges. Therefore, wide corridors, intuitive layouts, and ample elevators are not just conveniences; they are instruments of empowerment that grant residents control over their own social lives.
The finding that excessive privacy can negatively correlate with interpersonal interaction calls for a nuanced design approach that balances personal sanctuary with social invitation (26). Instead of “reducing privacy,” the goal should be to create a gradient of spaces. This includes the fully private resident’s room, but critically, also involves designing inviting semi-private or semi-public transitional zones—such as a small seating area outside a cluster of rooms, or a bay window with a bench in a wide corridor. These spaces act as a low-pressure “front porch,” allowing residents to observe the daily flow of life and engage in casual interactions without committing to the full social demands of a large common area. They gently lure residents out of isolation and into the life of the community.
8 Limitations and future study
This study intentionally focused on BE determinants of SI among residents rather than including demographic or personality variables. Under the Person–Environment (P–E) fit framework, previous research has emphasized that the individual (P) and environmental (E) components can be examined independently to clarify their respective mechanisms (13, 72). This study aimed to identify the environmental effects, how nine BE factors of care homes influence older residents’ SI, rather than to construct a full predictive model of social behavior. Moreover, prior evidence suggests that accessibility, facilities and layout are key drivers of social interaction in care environments (34, 35). Therefore, focusing solely on BE variables is theoretically justified and consistent with the study’s exploratory objective of isolating environmental contributions within the P–E theoretical framework. Future studies could incorporate key demographic and person-related variables to more rigorously elucidate the underlying mechanisms.
Although the R2 values of the regression models (7.9 and 8.3%) appear modest, such levels are common and theoretically acceptable in social and environmental psychology research (73), where human behavior is influenced by multiple interacting factors. Small-to-medium effect sizes can still carry substantive meaning in behavioral research, especially when the goal is to illuminate underlying mechanisms rather than to maximize predictive accuracy (74, 75). In the context of residential care settings, even a small proportion of explained variance suggests that environmental attributes make a measurable and practically relevant contribution to residents’ SI, which are otherwise shaped by diverse personal and contextual variables. Moreover, the relatively homogeneous demographic characteristics of institutional residents may further constrain the variance of SI, making modest R2 values theoretically reasonable. Future work should incorporate key demographic and person-related variables (e.g., age, sex, cognitive/functional status, length of stay) to account for residual variance in social interactions and thereby enhance model precision and inferential accuracy.
In the study, lighting, thermal, and acoustic conditions were recorded once at 10:00 on a Saturday using standard instruments, yielding a snapshot rather than a diurnal or weekly average. Because illumination (daylight), temperature/humidity (HVAC cycles and outdoor weather), and sound levels (activity schedules) fluctuate across times of day and days of the week, the estimates reflect associations at that measurement time rather than conditions throughout the facilities. To address this limitation, future studies should use repeated measurements across morning/midday/evening and weekday/weekend periods—or continuous data logging—and align time-stamped environmental data with behavioral observations to better capture temporal variability and reduce measurement error.
9 Conclusion
To promote SI among older adults in care homes, the BE must be designed carefully. All of these aspects play a critical role in supporting their SI needs. These needs encompass interpersonal interaction, activity engagement, caregiver relationships, and conflict resolution. It is essential to explore the interactions between the built environment and interpersonal interactions among older adults. This study investigates the effects of older individuals’ subjective perceptions of the BE on their social interactions. Besides questionnaire surveys among 119 older residents in three care homes, environmental measurement and behavioral observation were also conducted. An integrated BE-SI model was developed, utilizing a combination of multiple statistical methods. The final model reveals that: (1) Functional facilities positively influence interpersonal interaction, highlighting the importance of diverse and well-equipped spaces to foster engagement; (2) privacy shows a slight negative correlation with interpersonal interaction, suggesting that while privacy is essential, excessive isolation may hinder social connections; (3) Accessibility has a strong positive impact on both activity engagement and caregiver relationships, emphasizing the need for barrier-free designs; and (4) recreational areas and lighting conditions reduce the conflicts in care homes.
To foster an age-friendly environment for older adults in care homes, several key design elements are essential. Optimizing accessibility in care home design should be a primary consideration for promoting SI among older adults. The proposed measures, such as including 3-meter-wide corridors to ensure unobstructed mobility between key functional zones, strategically positioned elevators to reduce spatial exclusion, and cognitively accessible signage to empower navigation independence, collectively address both physical and perceptual barriers. This study provides valuable insights for designers, facility managers, and staff members in care homes. Furthermore, it contributes to the ecological theory of aging by empirically identifying specific built environment factors—such as functional facilities, accessibility, and lighting—that constitute critical forms of “environmental press” in modern care settings. The developed BE-SI model serves as a practical application of the P-E fit concept, offering a more nuanced framework for creating supportive environments. This enables a better understanding of the critical needs of older adults. This study offers practical guidance on how to effectively design and manage the built environment in these settings to better support the wellbeing and interpersonal interactions of older residents. This study offers insights into BE impact on SI in care homes, but despite incorporating environmental data and behavioral observations, it remains limited by self-report bias (76). Future research should adopt longitudinal designs and integrate electroencephalogram (EEG), virtual reality (VR), and machine learning for more precise analysis (77).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethical Review of Science and Technology at Nanjing Tech University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
CW: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. YP: Conceptualization, Formal analysis, Investigation, Writing – original draft. XL: Data curation, Writing – review & editing. SQ: Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The work described in this paper was fully supported by National Natural Science Foundation of China (Grant No. 72401129); Social Science Foundation of Jiangsu Province (Grant No. 24EYC008); Social Science Foundation in Jiangsu Higher Education Institutions, China (Grant No. 2023SJYB0208); Jiangsu Province Social Science Applied Research Excellent Project (Grant No. 24SYB-061).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1693935/full#supplementary-material
References
1. United Nations (2019) World population ageing. Available online at: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2020/Jan/un_2019_worldpopulationageing_re port.pdf (accessed May 6, 2019).
2. National Bureau of Statistics. (2022). Seventh national population census. Available online at: http://www.stats.gov.cn/ztjc/zdtjgz/zgrkpc/dqcrkpc/ggl/202105/t 20210519_1817693.html (accessed June 20, 2022).
3. Yue, Y, Yang, D, Owen, N, and Van Dyck, D. The built environment and mental health among older adults in Dalian: the mediating role of perceived environmental attributes. Soc Sci Med. (2022) 311:115333. doi: 10.1016/j.socscimed.2022.115333
4. Liougas, MP, Sommerlad, A, O’Rourke, HM, McGilton, KS, and Bethell, J. Social connection measures for older adults living in long-term care homes: a systematic review protocol. Syst Rev. (2024) 13:67. doi: 10.1186/s13643-024-02468-6
5. Cacioppo, JT, and Cacioppo, S. Social relationships and health: the toxic effects of perceived social isolation. Soc Personal Psychol Compass. (2014) 8:58–72. doi: 10.1111/spc3.12087
6. Perissinotto, CM, Cenzer, IS, and Covinsky, KE. Loneliness in older persons: a predictor of functional decline and death. Arch Intern Med. (2012) 172:1078–83. doi: 10.1001/archinternmed.2012.1993
7. Chapman, H, Bethell, J, Dewan, N, Liougas, MP, Livingston, G, McGilton, KS, et al. Social connection in long-term care homes: a qualitative study of barriers and facilitators. BMC Geriatr. (2024) 24:857. doi: 10.1186/s12877-024-05454-8
8. Harnett, T. Seeking exemptions from nursing home routines: residents’ everyday influence attempts in relation to institutional order. J Aging Stud. (2010) 24:292–301. doi: 10.1016/j.jaging.2010.08.001
9. Carnemolla, P, Debono, D, Hourihan, F, Hor, S, Robertson, H, and Travaglia, J. The influence of the built environment in enacting a household model of residential aged care for people living with a mental health condition: a qualitative post-occupancy evaluation. Health Place. (2021) 71:102624. doi: 10.1016/j.healthplace.2021.102624
10. Dam-Krogh, EP, Clausen, G, and Toftum, J. Indoor environment and user perceptions in offices in Greenland compared to Denmark. J Build Eng. (2024) 97:110875. doi: 10.1016/j.jobe.2024.110875
11. Li, H, Lyu, R, Wang, M, Moorhead, M, and Skitmore, M. Built environment–the secret recipe for mental health healing and recovery: a literature review. Engineering, construction and architectural management. London: Springer (2025).
12. Li, Z, Lee, JH, Yao, L, and Ostwald, MJ. Impact of built environments on human perception: a systematic review of physiological measures and machine learning. J. Building Eng. (2025) 22:112319. doi: 10.1016/j.jobe.2025.112319
14. Li, C, Li, X, Zhang, Y, and Lao, W. Interpersonal interactions, sense of loneliness and perceived depressive emotions among older adults: a cultural-psychological perspective from heterogeneous roles of different relationships. SSM-Population Health. (2024a) 27:101703. doi: 10.1016/j.ssmph.2024.101703
15. Li, W, Meng, M, Llewellyn, CE, and Sun, T. Developing an indicator framework for sustainability assessment in urban community regeneration: a case of Shanghai. Dev Built Environ. (2024b) 18:100476. doi: 10.1016/j.dibe.2024.100476
16. Kumar, M, Srivastava, S, and Muhammad, TJSR. Relationship between physical activity and cognitive functioning among older Indian adults. Sci Rep. (2022) 12:2725. doi: 10.1038/s41598-022-06725-3
17. Möller, S, Lykkegaard, J, Hansen, RS, Stokholm, L, Kjær, NK, and Ahrenfeldt, LJ. Sensory impairments and the risk of cognitive decline and dementia across sex, age, and regions: longitudinal insights from Europe. Arch Gerontol Geriatr. (2024) 127:105584. doi: 10.1016/j.archger.2024.105584
18. Roy, K, Smilowitz, S, Bhatt, S, and Conroy, ML. Impact of social isolation and loneliness in older adults: current understanding and future directions. Curr Geriatr Rep. (2023) 12:138–48. doi: 10.1007/s13670-023-00393-5
19. Fiske, AP. The four elementary forms of sociality: framework for a unified theory of social relations. Psychol Rev. (1992) 99:689–723. doi: 10.1037/0033-295X.99.4.689
20. Lopes, PN. Emotional abilities and the quality of interpersonal interaction. New Haven, CT: Yale University (2004).
21. White, C. H. (2016). Interpersonal interaction. The international encyclopedia of communication theory and philosophy, Cham Springer 1–11.
22. Autschbach, D, Hagedorn, A, and Halek, M. Addressing loneliness and social isolation through the involvement of primary and secondary informal caregivers in nursing homes: a scoping review. BMC Geriatr. (2024) 24:552. doi: 10.1186/s12877-024-05156-1
23. Yu, J, Ma, G, Ding, W, Mao, J, and Wang, J. Structural model for the relationships between age-friendly communities and quality of life of older adults in Hefei, China. Eng Constr Archit Manag. (2022) 29:1376–95.
24. Zhao, X, Yu, J, and Liu, N. Relationship between specific leisure activities and successful aging among older adults. J. Exercise Sci. Fitness. (2023) 21:111–8. doi: 10.1016/j.jesf.2022.11.006
25. Shen, X, Wang, J, Chen, J, Zhang, H, Shen, S, and Zhao, X. Relationship between participation in leisure activities and the maintenance of successful aging in older Chinese adults: a 4-year longitudinal study. BMC Geriatr. (2024) 24:1–11. doi: 10.1186/s12877-024-05574-1
26. Parker, C, Barnes, S, McKee, K, Morgan, K, Torrington, J, and Tregenza, P. Quality of life and building design in residential and nursing homes for older people. Ageing Soc. (2004) 24:941–62. doi: 10.1017/S0144686X04002387
27. Zhou, X, and Wong, H. Caregiver interactions, perceived control, and meaning in life of elderly: the moderating effect of the elderly-to-social worker ratio. BMC Geriatr. (2024) 24:431. doi: 10.1186/s12877-024-05029-7
28. Hajek, A, Kretzler, B, and König, HH. Informal caregiving, loneliness and social isolation: a systematic review. Int J Environ Res Public Health. (2021) 18:12101. doi: 10.3390/ijerph182212101
29. Song, Y, Wang, Y, Zhou, M, Suo, Z, Wang, X, Li, C, et al. Association between the perceived built environment and health behaviors in older adults: a cross-sectional study from Beijing, China. BMC Geriatr. (2024) 24:692. doi: 10.1186/s12877-024-05285-7
30. Gripko, M, and Joseph, A. The role of the built environment in supporting older adults’ engagement: a narrative literature review. HERD. (2024) 17:329–53. doi: 10.1177/19375867241250320
31. Mehrabi, F, and Béland, F. Effects of social isolation, loneliness and frailty on health outcomes and their possible mediators and moderators in community-dwelling older adults: a scoping review. Arch Gerontol Geriatr. (2020) 90:104119. doi: 10.1016/j.archger.2020.104119
32. Kuzuoglu, S, Glover, TD, Moyer, L, and Todd, J. How built environment characteristics influence social interactions during neighbourhood walks among urban inhabitants. Int J Environ Res Public Health. (2024) 21:1519. doi: 10.3390/ijerph21111519
33. Ji, Y, Feng, X, Zhao, H, and Xu, X. Study on the elderly's perception of microclimate and activity time in residential communities. Build Environ. (2024) 266:112125. doi: 10.1016/j.buildenv.2024.112125
34. Bower, M, Kent, J, Patulny, R, Green, O, McGrath, L, Teesson, L, et al. The impact of the built environment on loneliness: a systematic review and narrative synthesis. Health Place. (2023) 79:102962. doi: 10.1016/j.healthplace.2022.102962
35. Sailer, K., and Koutsolampros, P. (2021). Space syntax theory: understanding human movement, co-presence and encounters in relation to the spatial structure of workplaces. A handbook of theories on designing alignment between people and the office environment. 248–260. London Routledge.
36. Christoforou, R, Lange, S, and Schweiker, M. Individual differences in the definitions of health and wellbeing and the underlying promotional effect of the built environment. J. Building Eng. (2024) 84:108560. doi: 10.1016/j.jobe.2024.108560
37. Wu, HW, Kumar, P, and Cao, SJ. Implementation of green infrastructure for improving the building environment of elderly care centres. J Build Eng. (2022) 54:104682. doi: 10.1016/j.jobe.2022.104682
38. Rafiei, S, and Gifford, R. The meaning of the built environment: a comprehensive model based on users traversing their university campus. J Environ Psychol. (2023) 87:101975. doi: 10.1016/j.jenvp.2023.101975
39. Nordin, S, Elf, M, McKee, K, and Wijk, H. Assessing the physical environment of older people’s residential care facilities: development of the Swedish version of the Sheffield care environment assessment matrix (S-SCEAM). BMC Geriatr. (2015) 15:1–11. doi: 10.1186/1471-2318-15-3
40. Wang, D, and Lin, T. Built environments, social environments, and activity-travel behavior: a case study of Hong Kong. J Transp Geogr. (2013) 31:286–95. doi: 10.1016/j.jtrangeo.2013.04.012
41. Gao, Z, Chee, CS, Dev, RDO, Li, F, Li, R, Gao, J, et al. Exploring the role of social capital in enhancing physical activity among college and university students: a systematic review. PLoS One. (2024) 19:e0314610. doi: 10.1371/journal.pone.0314610
42. Huang, W, and Lin, G. The relationship between urban green space and social health of individuals: a scoping review. Urban For Urban Green. (2023) 85:127969. doi: 10.1016/j.ufug.2023.127969
43. Lin, Q, Zhang, C, Cai, H, Li, X, and Xiao, H. Urban night lighting evaluation system and case study: blending popular contemporary elements, cultural traditions and advanced lighting technologies. Eng Constr Archit Manag. (2024) 31:2916–31. doi: 10.1108/ECAM-11-2021-1056
44. Wong, JKW, Skitmore, M, Buys, L, and Wang, K. The effects of the indoor environment of residential care homes on dementia suffers in Hong Kong: a critical incident technique approach. Build Environ. (2014) 73:32–9. doi: 10.1016/j.buildenv.2013.12.001
45. Leung, MY, Sieh, L, and Yin, R. An integrated model for luminous environment and quality of life of older people in care and attention homes. Build Environ. (2023) 244:110821. doi: 10.1016/j.buildenv.2023.110821
46. Santos, L, do Rosário Pinheiro, M, and Rijo, D. Fostering an affiliative environment in residential youth care: a cluster randomized trial of a compassionate mind training program for caregivers enrolling youth and their caregivers. Child Abuse Negl. (2023) 139:106122. doi: 10.1016/j.chiabu.2023.106122
47. Meredith, SJ, Cox, NJ, Ibrahim, K, Higson, J, McNiff, J, Mitchell, S, et al. Factors that influence older adults’ participation in physical activity: a systematic review of qualitative studies. Age Ageing. (2023) 52:afad145. doi: 10.1093/ageing/afad145
48. Lawton, MP. An ecological theory of aging applied to elderly housing. J Archit Educ. (1977) 31:8–10. doi: 10.1080/10464883.1977.11102585
49. Satariano, W. Epidemiology of aging: An ecological approach. New York, NY: Jones & Bartlett Learning (2006).
50. Mangione, CM, Lee, PP, Pitts, J, Gutierrez, P, Berry, S, Hays, RD, et al. Psychometric properties of the National eye Institute visual function questionnaire (NEI-VFQ). Arch Ophthalmol. (1998) 116:1496–504. doi: 10.1001/archopht.116.11.1496
51. Wolffsohn, JS, and Cochrane, AL. Design of the low vision quality-of-life questionnaire (LVQOL) and measuring the outcome of low-vision rehabilitation. Am J Ophthalmol. (2000) 130:793–802. doi: 10.1016/s0002-9394(00)00610-3
52. National Institute of Building Sciences. (2022). Design guidelines for the visual environment. Available online at: https://www.nibs.org/files/pdfs/NIBS_LVDP_Guidelines_2015.pdf (accessed July 10, 2022).
53. Ullman, JB, and Bentler, PM. Handbook of psychology: Structural equation Modeling. New York, NY: Academic Press (2003).
54. O'Rourke, N, Psych, R, and Hatcher, L. A step-by-step approach to using SAS for factor analysis and structural equation modeling. New Carolina, NC: SAS Institute (2013).
56. Kaiser, HF. The varimax criterion for analytic rotation in factor analysis. Psychometrika. (1958) 23:187–200. doi: 10.1007/BF02289233
57. Hair, JF Jnr, Black, WC, Babin, BJ, and Anderson, RE. Multivariate data analysis. Cham: Springer Science & Business Media (2010).
58. Kaartina, S, Chin, YS, Fara Wahida, R, Woon, FC, Hiew, CC, Zalilah, MS, et al. Adolescent self-report and parent proxy-report of health-related quality of life: an analysis of validity and reliability of PedsQL™ 4.0 among a sample of Malaysian adolescents and their parents. Health Qual Life Outcomes. (2015) 13:1–9. doi: 10.1186/s12955-015-0234-4
59. Oriol, X, Torres, J, Miranda, R, Bilbao, M, and Ortúzar, H. Comparing family, friends and satisfaction with school experience as predictors of SWB in children who have and have not made the transition to middle school in different countries. Child Youth Serv Rev. (2017) 80:149–56. doi: 10.1016/j.childyouth.2017.06.053
60. Bentler, PM, and Chou, C-P. Practical issues in structural modeling. Sociol Methods Res. (1987) 16:78–117. doi: 10.1177/0049124187016001004
61. Gates, KM, Molenaar, PC, Hillary, FG, and Slobounov, S. Extended unified SEM approach for modeling event-related fMRI data. NeuroImage. (2011) 54:1151–8. doi: 10.1016/j.neuroimage.2010.08.051
62. Kline, RB. Principles and practice of structural equation modeling. London: Guilford publications (2023).
63. Jang, M. The relationship between spatial characteristics and social interaction of older adults with dementia in nursing homes. J Asian Archit Build Eng. (2023) 22:175–87. doi: 10.1080/13467581.2022.2043874
64. Rivera, E, Smith, C, and Hesketh, KD. Priority populations’ experiences of the accessibility and inclusion of recreation centres: a qualitative study. BMC Public Health. (2024) 24:205. doi: 10.1186/s12889-023-17595-3
65. Meyer, KN, Glassner, A, Lee, K, Pickering, CE, and White, CL. Conceptualizing how caregiving relationships connect to quality of family caregiving within the stress process model. J Gerontol Soc Work. (2022) 65:635–48. doi: 10.1080/01634372.2021.2010855
66. Xuan, X, Chen, X, and Li, Z. Impacts of nursing unit design on visibility and proximity and its influences on communication, privacy, and efficiency. HERD. (2020) 13:200–17. doi: 10.1177/1937586719881443
67. Wang, C, and Leung, MY. Effects of subjective perceptions of indoor visual environment on visual-related physical health of older people in residential care homes. Build Environ. (2023) 237:110301. doi: 10.1016/j.buildenv.2023.110301
68. Kuske, B, Hanns, S, Luck, T, Angermeyer, M, Behrens, J, and Riedel-Heller, S. Nursing home staff training in dementia care. A systematic review of evaluated programs. Das Gesundheitswesen. (2009) 71:A231. doi: 10.1017/S1041610206004352
69. Nelson, GG. Household models for nursing home environments: Symposium paper. London: Pioneer Network (2024).
70. Che, L, Zhang, J, Liu, J, Ma, M, Si, X, An, J, et al. Interior luminous environment for the elderly: recommended values of lighting parameters and comfort discriminant model. Build Environ. (2025) 274:112787. doi: 10.1016/j.buildenv.2025.112787
71. Rivera, E, Veitch, J, Loh, VH, Salmon, J, Cerin, E, Mavoa, S, et al. Outdoor public recreation spaces and social connectedness among adolescents. BMC Public Health. (2022) 22:165. doi: 10.1186/s12889-022-12558-6
72. Wahl, HW, Iwarsson, S, and Oswald, F. Aging well and the environment: toward an integrative model and research agenda for the future. The Gerontologist. (2012) 52:306–16. doi: 10.1093/geront/gnr154
73. Richard, FD, Bond, CF Jr, and Stokes-Zoota, JJ. One hundred years of social psychology quantitatively described. Rev Gen Psychol. (2003) 7:331–63. doi: 10.1037/1089-2680.7.4.331
74. Falk, RF, and Miller, NB. A primer for soft modeling. Akron, OH: University of Akron Press (1992).
75. Cohen, J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates (1988).
77. Jin, S. Interdisciplinary perspective on architectural programming: current status and future directions. Engineering, construction and architectural management. Cham: Springer (2024).
78. Lee, HS, Shepley, M, and Huang, CS. Evaluation of off-leash dog parks in Texas and Florida: A study of use patterns, user satisfaction, and perception. Land urban plan. (2009) 92:314–324.
79. Hu, LT, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal. (1999) 6:1–55.
Keywords: built environment, older people, social interaction, care homes, mixed-methods investigation
Citation: Wang C, Pan Y, Li X and Qiang S (2025) A mixed-methods investigation for effects of built environments on older people’s social interaction in care homes. Front. Public Health. 13:1693935. doi: 10.3389/fpubh.2025.1693935
Edited by:
Lambert Zixin Li, National University of Singapore, SingaporeReviewed by:
Peilin Yang, Barcelona Graduate School of Economics, SpainYanghe Liu, University of Calgary, Canada
Copyright © 2025 Wang, Pan, Li and Qiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yujian Pan, MjAyNDYxMjEzMjQ3QG5qdGVjaC5lZHUuY24=