 Onur Mutlu Yaşar1
Onur Mutlu Yaşar1 Veli Volkan Gürses2
Veli Volkan Gürses2 Ali Erdem Ciğerci3
Ali Erdem Ciğerci3 Erdal Bal4
Erdal Bal4 Yeliz Pehlivan4
Yeliz Pehlivan4 Mustafa Baş4
Mustafa Baş4 Nedim Malkoç4
Nedim Malkoç4 Merve Bektaş4
Merve Bektaş4 Gizem Başkaya2
Gizem Başkaya2 Sare Dündar2
Sare Dündar2 Ömür Fatih Karakullukçu5
Ömür Fatih Karakullukçu5 Hamza Küçük6*
Hamza Küçük6*- 1Faculty of Health Sciences, Izmir Demokrasi University, Izmir, Türkiye
- 2Faculty of Sport Sciences, Bandırma University, Balıkesir, Türkiye
- 3Faculty of Sports Sciences, Kastamonu University, Kastamonu, Türkiye
- 4Faculty of Life Sciences, University of Health Sciences, Istanbul, Türkiye
- 5Ministry of National Education, Ankara, Türkiye
- 6Yasar Dogu Faculty of Sport Sciences, Ondokuz Mayis University, Samsun, Türkiye
Background: Traditional reliance on body mass index (BMI) to assess adiposity may misclassify physically active individuals with high lean mass. The triponderal mass index (TMI) has emerged as a potentially more accurate alternative, but evidence in physically active populations is limited.
Purpose: To examine the associations of TMI and BMI with bioimpedance-derived adiposity and selected hematological markers in physically active young adults.
Methods: In this cross-sectional study, (n = 59) participants (male = 37, female = 22; age 22.63 ± 2.29 years) underwent anthropometry, whole-body bioimpedance and venous blood sampling. TMI and BMI were calculated, and associations with body fat percentage, hemoglobin, hematocrit, neutrophil-to-lymphocyte ratio (NLR), and platelet-to-lymphocyte ratio (PLR) were examined. Normality assumptions were checked; correlations and multiple linear regressions were computed (α = 0.05). Physical activity status followed WHO/ACSM guidelines (≥150 min·week−1 of moderate-to-vigorous activity).
Results: TMI showed a stronger positive correlation with body fat percentage than BMI (r = 0.50, p < 0.001 vs. r = 0.38, p = 0.003). BMI was positively correlated with HGB (r = 0.32, p = 0.013) and HCT (r = 0.26, p = 0.046) and negatively correlated with NLR (ρ = −0.27, p = 0.041) and PLR (r = −0.30, p = 0.022). TMI was negatively correlated with NLR (p = −0.27, p = 0.039). In the multivariable model (predictors: BMI, TMI, HGB, HCT, NLR, PLR), HCT was a significant negative predictor of adiposity (β = −0.34, p = 0.021), whereas TMI showed a positive but marginally non-significant association (β = 0.25, p = 0.073). Assumptions and multicollinearity were acceptable.
Conclusion: In physically active young adults, TMI relates more strongly than BMI to bioimpedance-derived adiposity and may aid field-based screening. However, athlete-level decisions should await confirmation in sport-specific, longitudinal studies using criterion methods.
1 Introduction
Accurate assessment of body composition is critical in sports science, as it influences athletic performance, training adaptation, and long-term health outcomes (1–11). Body mass index (BMI), calculated as body mass in kilograms divided by height in meters squared (kg/m2), is one of the most widely used indices for estimating adiposity in both clinical and young active adults settings (12–16). However, BMI does not distinguish between fat mass and lean body mass, which can lead to misclassification, particularly in physically active populations with higher muscle mass (17, 18). This limitation has prompted the exploration of alternative anthropometric measures that can more accurately reflect body fatness and metabolic risk in active people.
The triponderal mass index (TMI), calculated as body mass in kilograms divided by height cubed (kg/m3), has recently emerged as a potentially superior measure for estimating body fatness, especially in adolescents and young adults (19–23). Unlike BMI, TMI appears less influenced by variations in height and pubertal maturation, offering greater stability across growth stages (24–26). Studies have reported that TMI demonstrates stronger correlations with direct measures of body fat, such as dual-energy X-ray absorptiometry (DXA), compared to BMI in youth populations (27–29). BMI is widely used for population-level screening but may insufficiently capture adiposity at the individual level. TMI has shown superior validity in pediatric and adolescent cohorts and is theoretically less sensitive to height-related allometry. However, evidence in physically active young adults is limited. TMI may demonstrates stronger relationships than BMI with bioimpedance-derived adiposity and hematological markers in active university students.
In addition to anthropometric indices, hematological parameters—such as hemoglobin (HGB), hematocrit (HCT), leukocyte differentials, and platelet indices—are important indicators of oxygen transport, inflammation, immune status, and overall physiological readiness (30–35). These markers can provide valuable insight into the metabolic and performance-related status of physically active individuals (36–38). Despite their relevance, few studies have simultaneously examined TMI, BMI, and a comprehensive hematological profile in active populations, limiting our understanding of how these indices relate to systemic health markers beyond body fat estimation alone (39–41).
Recent evidence suggests that TMI may provide equal or greater sensitivity than BMI in detecting adverse health markers, yet the majority of studies have been conducted in sedentary or clinical populations (27, 42–44). The lack of research in young, physically active individuals represents a significant gap, especially considering that accurate non-invasive screening tools are crucial for physical monitoring, training optimization, and injury prevention (45, 46). Therefore, aiming to investigate the relationships between TMI, BMI, body fat percentage, and hematological parameters among physically active young adults, to determine which index more accurately reflects systemic risk factors and adiposity could be valuable. By directly comparing these two indices alongside a detailed blood profile, this research seeks to refine anthropometric screening methods for application in sports science and exercise medicine. BMI is widely applied for population-level screening but may insufficiently capture adiposity at the individual level. TMI (mass/height3) has shown superior validity in pediatric and adolescent cohorts and is theoretically less sensitive to height-related allometry. Yet, evidence in physically active young adults remains limited. Addressing this gap, we examined whether TMI demonstrates stronger associations than BMI with bioimpedance-derived adiposity and hematological markers in active university students, while avoiding direct generalization to competitive athletes. We aimed to (i) compare the magnitude of associations between TMI/BMI and body fat percentage, and (ii) explore relationships with HGB, HCT, NLR, PLR. We hypothesized that TMI would correlate more strongly with adiposity than BMI in physically active young adults.
2 Materials and methods
2.1 Study design and setting
This cross-sectional, observational study was conducted at the Department of Exercise and Sport Sciences, Faculty of Life Sciences, Health Sciences University, Turkey. A stratified, multi-stage probability sampling method was utilized to ensure a representative distribution of participants based on sex and age among physically active individuals. The study protocol was approved by the Non-Interventional Clinical Research Ethics Committee of Health Sciences University (Approval No: 2025–2/2–27). All participants were informed about the aims and procedures of the study and provided written informed consent prior to participation. The study adhered to the ethical principles outlined in the Declaration of Helsinki.
2.2 Participants
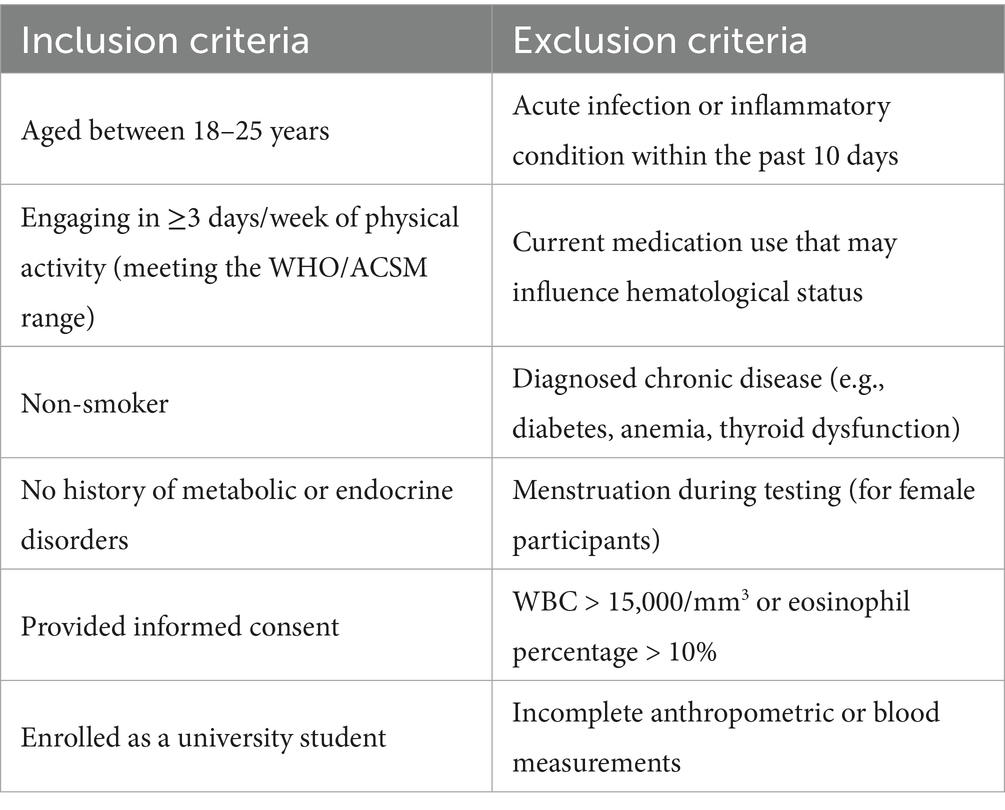
We analyzed 59 physically active students (37 men, 22 women; age 22.63 ± 2.29 years). Mean height was 171.78 ± 8.16 cm, BMI 22.78 ± 2.91 kg·m−2, and TMI 13.28 ± 1.76 kg·m−3. Mean body fat percentage was 18.45 ± 3.81%. Hemoglobin (HGB) and hematocrit (HCT) were 14.95 ± 2.03 g·dL−1 and 44.85 ± 5.04%, respectively. Inclusion criteria included engaging in physical activity on ≥3 days/week, meeting WHO/ACSM guidelines (150–300 min/week of moderate-intensity, or 75–150 min/week of vigorous-intensity aerobic activity, or an equivalent combination), non-smoking status, no chronic diseases or regular medication use, and absence of endocrine or metabolic disorders. Physical activity status was self-reported and verified by a brief activity checklist. Exclusion criteria involved menstruation, acute infection, or inflammatory disease within 10 days prior to testing; leukocyte count >15,000/mm3; or eosinophil percentage >10% following blood analysis. Participants were instructed to abstain from food and caffeine for 10 h prior to measurements.
2.3 Anthropometric assessments
Body height was measured to the nearest 0.1 cm using a stadiometer (Seca 213, Seca GmbH & Co. KG, Hamburg, Germany), with participants standing barefoot in anatomical position. Body mass and body fat percentage were assessed using a validated bioelectrical impedance analyzer (Tanita BC-545, Tanita Corp., Tokyo, Japan), with participants wearing light clothing and having emptied their bladder. Body Mass Index (BMI) was calculated using the standard formula (kg/m2), while Triponderal Mass Index (TMI) was derived as body mass (kg) divided by height cubed (m3). Waist circumference was measured at the midpoint between the lower costal margin and iliac crest using a non-elastic tape measure (Seca 203, Seca GmbH & Co. KG, Hamburg, Germany). Thigh circumference was measured at the mid-point between the trochanterion and tibiale laterale on the dominant leg.
2.4 Hematological assessments
Fasting venous blood samples were collected by a certified nurse from the antecubital vein using standard sterile techniques into EDTA-coated (purple-top) and serum-separation (yellow-top) vacutainer tubes (BD Vacutainer). Tourniquet application was limited to <60 s to avoid hemoconcentration artifacts. Each tube was gently inverted 6–8 times post-collection to ensure homogenous mixing with anticoagulants or clot activators. Samples were transported to the laboratory within 1 h and processed the same day. Hematological parameters, including red blood cell count (RBC), white blood cell count (WBC), hemoglobin (HGB), hematocrit (HCT), and platelet count (PLT), were analyzed using an automated hematology analyzer (Sysmex XN-Series, Sysmex Corp., Kobe, Japan). All procedures and analyses were supervised by a certified clinical biochemist.
2.5 Dependent and independent variables
The independent variables included BMI and TMI. The dependent variables consisted of hematological markers (RBC, WBC, HGB, HCT, PLT) and body fat percentage as assessed via bioelectrical impedance analysis. Demographic information age, lifestyle characteristics (exercise frequency, dietary habits), and anthropometric data were collected through structured questionnaires and direct measurements.
2.6 Standardization and quality control
All anthropometric and blood sampling procedures were conducted in the morning (between 08:00–10:00) to minimize diurnal variation. Instruments were calibrated before each testing session, and all measurements were performed by experienced personnel to ensure inter-rater reliability. A subset of measurements was repeated to assess test–retest consistency, with intra-class correlation coefficients (ICC) calculated to confirm reliability (ICC > 0.85 for all measures).
2.7 Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were reported as mean ± standard deviation (SD) for continuous variables and frequencies (n, %) for categorical data. Normality of distribution was assessed using the Kolmogorov–Smirnov test. Between-group comparisons were conducted using independent t-tests for normally distributed variables and Mann–Whitney U tests for non-normal data. Bivariate correlations between BMI, TMI, body fat percentage, and hematological markers were analyzed using Pearson’s or Spearman’s correlation coefficients, depending on distributional assumptions. Multiple linear regression models were built to predict body fat percentage from BMI, TMI, and hematological markers (HGB, HCT, NLR, PLR). Sex was not included as a covariate to preserve model parsimony and because preliminary checks indicated no material improvement in model fit (ΔR2 < 0.01) and potential collinearity concerns. Multicollinearity was assessed via variance inflation factor (VIF) (threshold < 10); residual diagnostics confirmed linearity, homoscedasticity, and normality. The coefficient of determination (R2), standardized beta coefficients, p-values, and 95% confidence intervals were reported for each predictor. Significance was set at p < 0.05 for all analyses. A priori power analysis using G*Power 3.1 determined a minimum sample size of 59 participants to detect a moderate correlation (r = 0.35) with 80% power at α = 0.05. Effect sizes were interpreted as small (d = 0.2), medium (d = 0.5), or large (d = 0.8), and statistical significance was set at p < 0.05. All tests were two-tailed.
3 Results
3.1 Participant characteristics
Descriptive characteristics of the study sample are presented in Table 1. We analyzed 59 physically active students (34 men, 25 women; age 22.63 ± 2.29 years). Mean height was 171.78 ± 8.16 cm, BMI 22.78 ± 2.91 kg·m−2, and TMI 13.28 ± 1.76 kg·m−3. Mean body fat percentage was 18.45 ± 3.81%. WBC averaged 7.49 ± 1.87 × 103·μL−1, PLT averaged 269.22 ± 52.88 × 103·μL−1, and NEUT averaged 4.39 ± 1.42 × 103·μL−1. The mean neutrophil-to-lymphocyte ratio (NLR) was 2.10 ± 1.05, and the mean platelet-to-lymphocyte ratio (PLR) was 127.33 ± 41.38. The distributions of WBC, PLT, and NEUT did not deviate from normality, whereas NLR deviated; accordingly, Spearman’s ρ was used for NLR in correlation analyses. BMI, TMI, body fat percentage, HGB, and HCT did not deviate significantly from normality (p > 0.05).
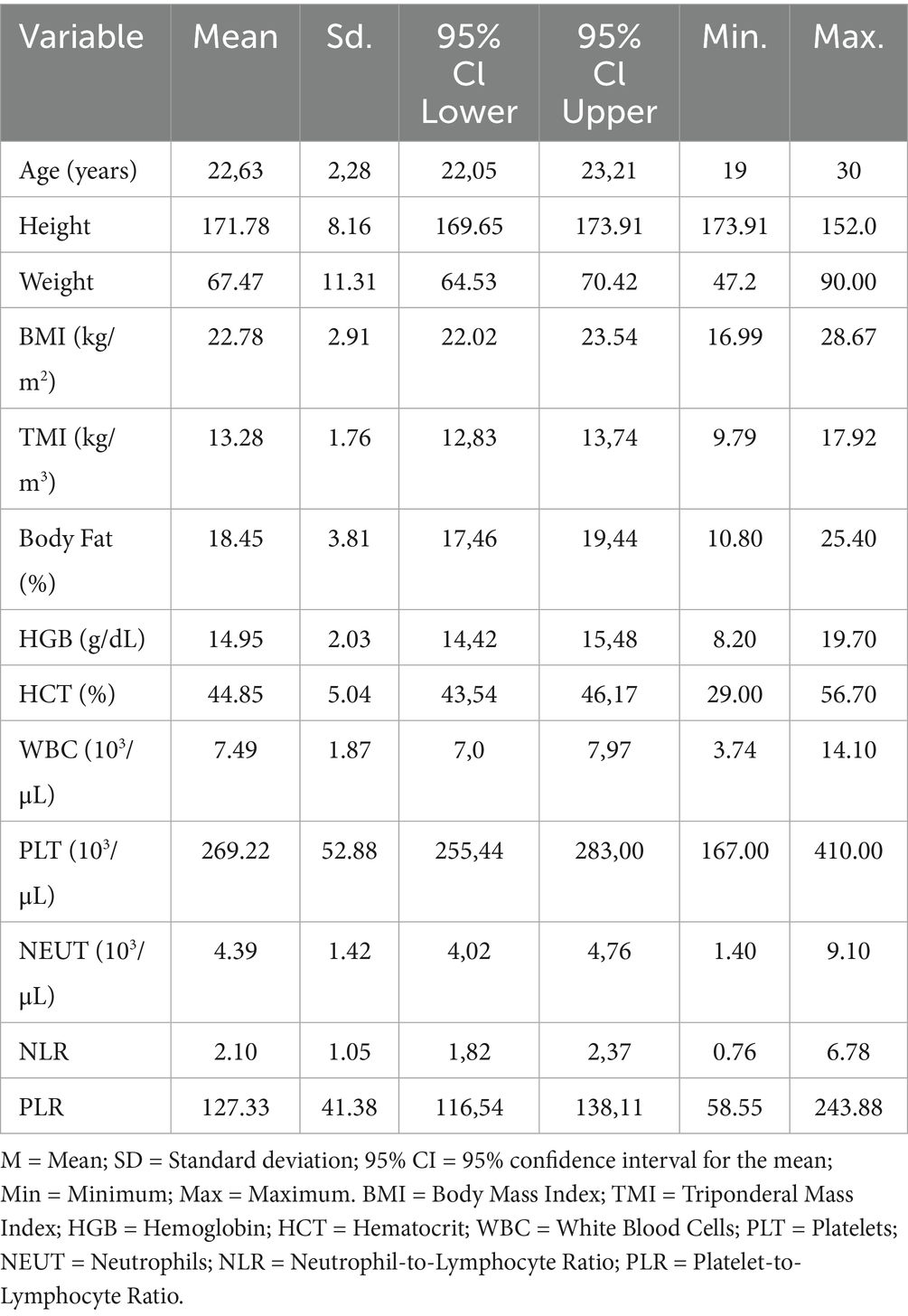
Table 1. Descriptive statistics of study variables (n = 59).
3.2 Sex-based comparisons
As expected, males exhibited higher oxygen-carrying indices, whereas females demonstrated greater adiposity. Hemoglobin (HGB) was significantly higher in males compared with females (16.09 vs. 14.49 g·dL−1; p = 0.001), as was hematocrit (HCT) (47.35 vs. 43.58%; p = 0.004). Percent body fat was markedly higher in females (19.85 vs. 13.56%; p = 0.001). Body mass index (BMI) was modestly higher in males (23.41 vs. 21.94 kg·m−2), showing a trend toward significance (p = 0.057). Platelet-to-lymphocyte ratio (PLR) tended to be higher in females (134.7 vs. 120.2; p = 0.062), whereas neutrophil-to-lymphocyte ratio (NLR) did not differ significantly between sexes (p = 0.570).
3.3 Correlation analysis
Bivariate correlation analyses (Table 2) revealed that BMI was positively correlated with body fat percentage (r = 0.38, p = 0.003), HGB (r = 0.32, p = 0.013), and HCT (r = 0.26, p = 0.046). Conversely, BMI showed significant negative correlations with NLR (rₛ = −0.27, p = 0.041) and PLR (r = −0.30, p = 0.022). TMI demonstrated a stronger positive correlation with body fat percentage (r = 0.50, p < 0.001) compared to BMI, while also exhibiting a negative correlation with NLR (rₛ = −0.27, p = 0.039). No significant associations were observed between either BMI or TMI and WBC, PLT, or NEUT counts (Figure 1).
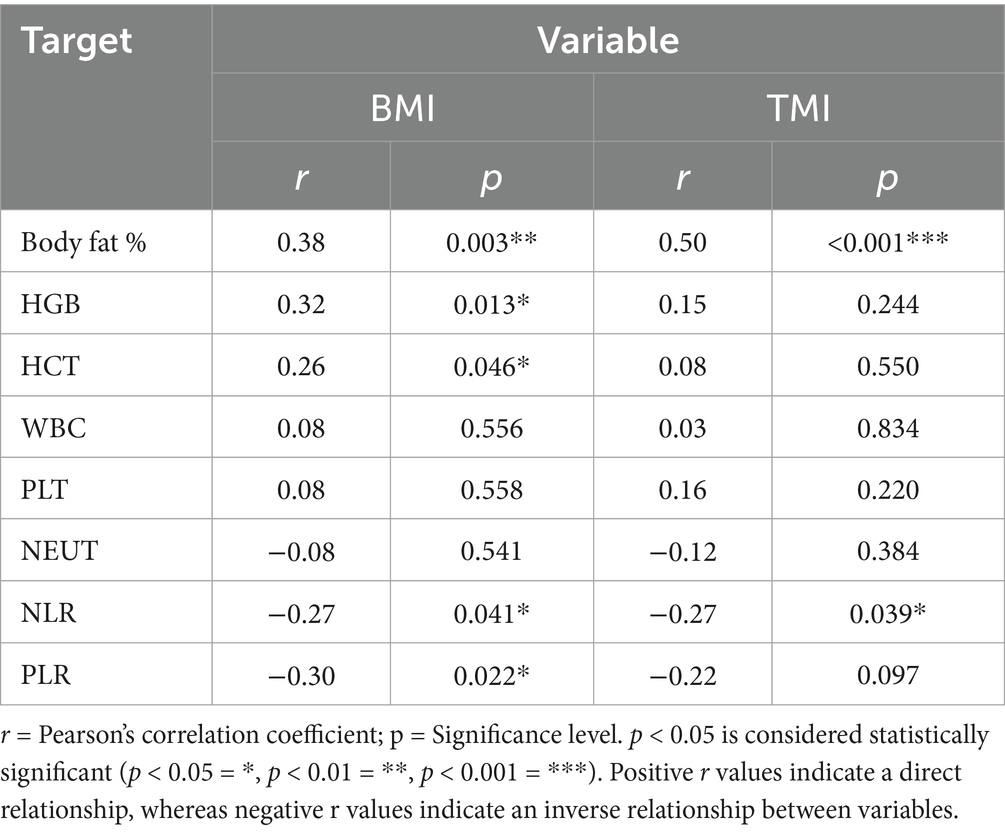
Table 2. Bivariate correlations between BMI, TMI, and hematological variables.
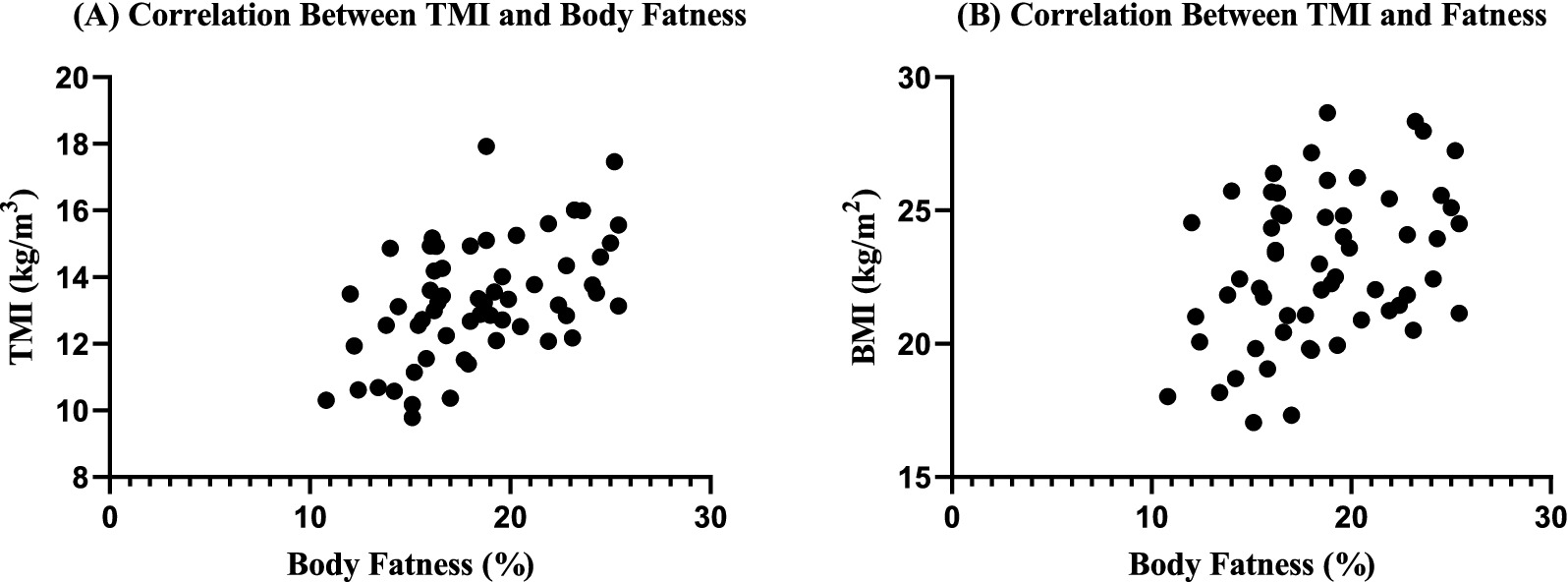
Figure 1. Bivariate correlation analysis of body fatness with BMI and TMI. Scatterplot matrix showing pairwise relationships between variables. Pearson’s correlation coefficients (r) with 95% confidence intervals. Scatterplots illustrating the correlations between body fat percentage and anthropometric indices. (A) Triponderal Mass Index (TMI, kg/m3) demonstrated a moderate positive association with body fat percentage, indicating higher TMI values correspond to greater adiposity. (B) Body Mass Index (BMI, kg/m2) also showed a positive relationship with body fat percentage, though the association appeared weaker compared to TMI. These findings support the potential utility of TMI as a more sensitive indicator of adiposity in physically active individuals.
3.4 Multiple regression analysis
A multiple linear regression model was conducted to examine the predictive capacity of BMI, TMI, HGB, HCT, NLR, and PLR for body fat percentage (Table 3). The overall model was statistically significant, F(6, 52) = 6.85, p < 0.001, explaining 44.1% of the variance in body fat percentage (Adj. R2 = 0.377). Among the predictors, HCT emerged as a significant negative predictor (β = −0.34, p = 0.021), indicating that lower hematocrit values were associated with higher body fat percentages. TMI showed a positive but marginally non-significant association (β = 0.25, p = 0.073). BMI, HGB, NLR, and PLR were not significant predictors when controlling for other variables. Multicollinearity diagnostics indicated acceptable variance inflation factor (VIF) values for all predictors, and residual plots confirmed that the assumptions of linearity, homoscedasticity, and normality were met.
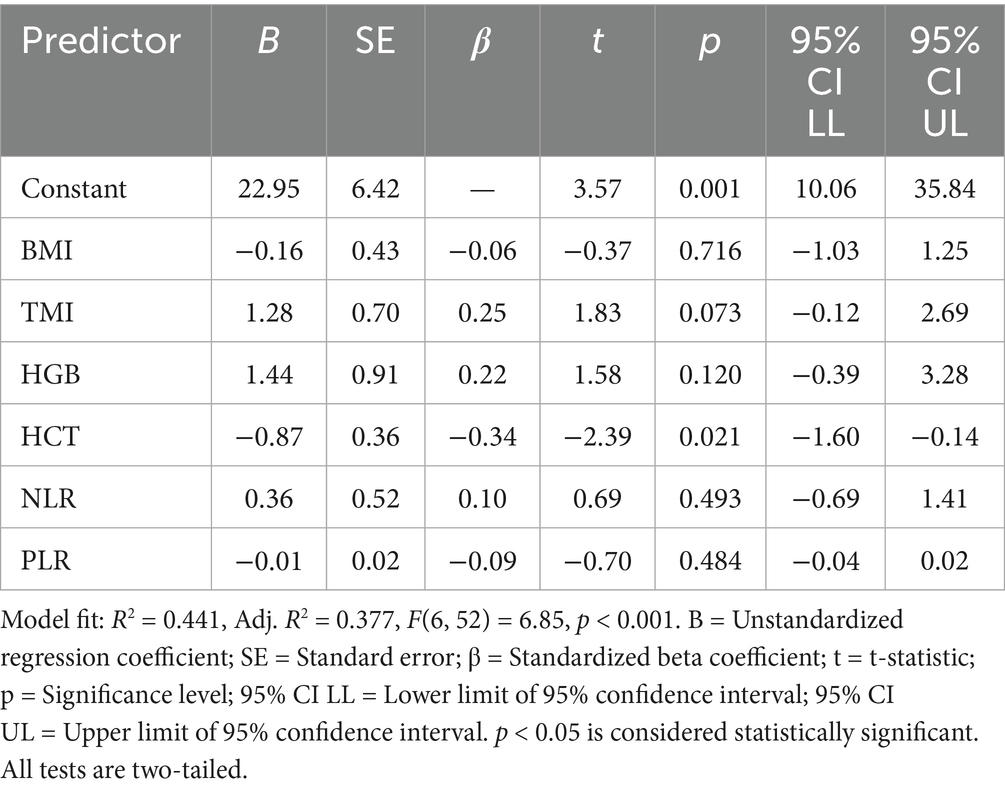
Table 3. Multiple linear regression predicting body fat percentage.
4 Discussion
This study examined how two low-cost anthropometric indices BMI and TMI relate to hematological markers of oxygen-carrying capacity and low-grade inflammation in physically active young adults. The findings suggest that TMI is a more precise anthropometric measure than BMI for estimating adiposity in active young populations and that integrating simple hematological markers particularly hematocrit (HCT) can provide additional physiological context in this group. Three findings stand out: (i) TMI correlated more strongly than BMI with bioimpedance-derived body fat percentage; (ii) BMI related positively to HGB/HCT, whereas both BMI and TMI related inversely, albeit modestly, to leukocyte-derived inflammatory ratios (NLR, PLR); and (iii) in multivariable modeling, lower HCT independently predicted higher adiposity after adjustment for anthropometry and inflammatory ratios. The HCT–adiposity association should be interpreted cautiously because it may partly reflect plasma-volume/hydration effects; mechanistic inference is further limited by the absence of ferritin and CRP. These results extend prior pediatric/adolescent evidence for TMI to an active young-adult cohort assessed under standardized conditions, but they should not be generalized to competitive athletes without sport-specific, longitudinal confirmation using criterion methods like DXA (47). In line with previous work showing that TMI can outperform BMI for estimating adiposity in youth and young adults, our data support its field-based screening utility while highlighting the need for sport-specific validation (3, 8, 31). These observations accord with recent reports that TMI better aligns with DXA-derived adiposity than BMI in non-clinical cohorts (28, 28, 48).
Below, we briefly position these findings within current evidence and outline practical implications for field based screening in physically active young adults. A central limitation of BMI in sports science is its inability to distinguish between lean and fat mass, often misclassifying muscular young active adults as overweight or obese despite low body fat levels (20). This misclassification risk is especially pronounced in adolescents and young adults engaged in resistance or mixed training, where increases in lean mass can inflate BMI without changes in fatness. By scaling mass to height cubed rather than squared, TMI more closely approximates body volume, thereby aligning more strongly with actual adiposity (22, 23). The closer coupling of TMI with adiposity aligns with a growing body of work reporting that height-cubed scaling better captures volumetric body size and fatness in populations where lean mass varies substantially (e.g., adolescents, young active adults, and active adults). In pediatric and youth cohorts, TMI has consistently outperformed BMI for classifying excess adiposity and tracking fat mass against criterion methods (22, 23). More recently, studies in sport and exercise settings have shown that TMI is less biased by muscularity and shows stronger correlations with DXA- or BIA-derived fat percentage than BMI, particularly when BMI lies in the “normal–overweight” band where misclassification risk is highest (20, 28, 47). The present results replicate earlier findings from youth and adolescent samples (27, 47) in an active young adult population, confirming that TMI correlates more robustly with bioimpedance-derived body fat percentage than BMI. For sports practitioners, this means that TMI can detect subtle changes in fatness even during periods of lean mass gain such as pre-season hypertrophy phases thereby improving the accuracy of nutritional and training adjustments. Our findings replicate this pattern in a physically active sample, supporting the practical recommendation to compute TMI alongside BMI during field screenings when DXA is unavailable.
Second, the hematology profile we observed differs from the adiposity-inflammation coupling often reported in sedentary or clinical cohorts. In those populations, higher adiposity is typically associated with elevated WBC counts and higher NLR/PLR, reflecting chronic low-grade inflammation (49, 50). In contrast, neither BMI nor TMI related to crude leukocyte or platelet counts here, and both indices showed small inverse relations with NLR/PLR. Two explanations are plausible. One is selection: these participants were physically active, a phenotype commonly characterized by lower basal inflammatory tone and favorable leukocyte trafficking at rest (51, 52). The second is range restriction: our cohort exhibited a relatively narrow, “healthy” BMI/TMI spectrum, which can attenuate or even invert associations that are monotonic in more heterogeneous samples. Together, these observations suggest that NLR/PLR may be less discriminative as risk markers in healthy active adults than in clinical screening, and that training load, fitness, and recovery status should be considered when interpreting immune-hematological ratios in fitness settings. In performance settings, precise body composition monitoring informs training load management. TMI is cost-effective and reduce the number of false positives for overweight classification in sports focused on strength and power. Furthermore, it has the capacity to discern bona fide alterations in adiposity that may not be fully apparent when using BMI, particularly with reference to seasonal fluctuations in muscle mass.
Third, the independent, negative association between HCT and adiposity in the multivariable model is physiologically coherent and has been reported in exercise studies when plasma volume status is considered. Greater adiposity especially in aerobically trained or habitually active individuals can co-occur with expanded plasma volume, producing lower HCT at a given red-cell mass (53, 54). Menstrual status and iron availability may also contribute to lower HCT among women with higher fat percentage, though we did not measure ferritin or hepcidin to test this pathway. Notably, HGB did not remain significant after adjustment, consistent with the notion that volume expansion (affecting HCT more directly) rather than reduced red-cell mass explains the signal. Practically, this underscores the value of pairing simple anthropometry with basic hematology (and, where feasible, ferritin/CRP) to contextualize field estimates of fatness in active populations.
Sex differences followed expected biological patterns higher HGB/HCT in men, higher fat percentage in women echoing recent sport-science reports and reinforcing the need for sex-aware reference frames when profiling young active adults and active adults (27, 28). Importantly, we did not find sex differences in NLR, again congruent with data suggesting training status narrows baseline inflammatory disparities (52).
BMI has long been criticized for its inability to differentiate between lean mass and fat mass, particularly in athletic populations where muscle mass is high. In such cases, young active adults with optimal or low body fat levels may still fall into the “overweight” BMI category [(20); Ode et al., 2007]. TMI, by scaling body mass to height cubed rather than squared, appears to reduce this bias and may provide a more volumetrically accurate estimate of body size (22, 23).
Our findings align with studies in adolescent and young active adults where TMI demonstrated stronger correlations with DXA-measured body fat percentage than BMI, particularly in sports emphasizing lean mass (e.g., sprinting, rowing, gymnastics) (27, 47). The advantage is especially relevant in youth sports development programs, where early detection of unhealthy fat gain or loss can inform training and nutrition adjustments without the misclassification risks inherent in BMI.
In high performance environments, anthropometric screening needs to be both accurate and feasible. While gold standard methods like DXA or hydrostatic weighing are ideal, they are not always accessible due to cost, portability, or scheduling constraints. TMI requires only body mass and height, making it: Field friendly: Easily measured on site at training facilities or competitions. Cost effective: No expensive devices are required, which is important for grassroots and youth programs. Sensitive in lean populations: More robust against the muscularity related inflation seen with BMI. Applicable in longitudinal tracking; Suitable for monitoring changes over a season or training cycle without specialized equipment.
For young active adults, TMI can help coaches and sports scientists: Differentiate training effects: Detect body composition changes that BMI might obscure, particularly when increases in lean mass are expected. Flag risk profiles: Identify early signs of excessive fat accumulation that could affect power-to-weight ratio, agility, or endurance. Support return to play protocols: Track body composition recovery after injury or illness, where muscle loss and fat gain may occur.
The inverse or null associations observed between adiposity indices and inflammatory markers (NLR, PLR) suggest that regular physical activity modulates baseline immune function. Active young adults generally exhibit lower resting inflammatory status and more favorable leukocyte distribution patterns than sedentary peers (51, 52). From a sports performance perspective, low systemic inflammation supports recovery, reduces injury risk, and may positively influence aerobic capacity. Interestingly, HCT emerged as an independent negative predictor of body fat percentage in our regression models. This may reflect plasma volume expansion, a common adaptation to endurance training rather than reduced red-cell mass (54). For coaches, monitoring HCT alongside anthropometric measures could provide additional context for athlete readiness and hydration status.
4.1 Practical applications in fitness monitoring
For field based screening in active student settings, TMI may provide a more informative anthropometric proxy of adiposity than BMI. In routine wellness checks, preseason evaluations, or campus health programs, incorporating TMI alongside BMI can help (i) flag individuals with potentially higher adiposity despite “normal” BMI, and (ii) monitor changes during lifestyle or training interventions. Until validated against criterion methods in sport-specific cohorts, athlete-level prescription or selection decisions should not rely on TMI alone; decisions should integrate performance tests, body composition by reference methods (e.g., DXA when feasible), and clinical judgment. This study adds to the growing evidence that TMI is not just a pediatric or epidemiological tool but also relevant in contexts particularly for young and active adults. While BMI remains widely used for its simplicity and historical inertia, integrating TMI into athlete health monitoring could enhance accuracy and prevent misinterpretation of muscular young active adults as “overweight.”
4.2 Limitations and future directions
This single-center study included a modest, homogeneous sample (n = 59) of physically active university students and employed a cross-sectional design. Adiposity was estimated via bioimpedance rather than a criterion method (e.g., DXA). Iron-status and inflammatory markers (e.g., ferritin, CRP) were not collected, which limits mechanistic interpretation of the observed HCT–adiposity association. Although physical activity status followed WHO/ACSM guidelines, self-report may introduce misclassification.
Validation of TMI against criterion methods is warranted in sport-specific cohorts, alongside longitudinal designs to test responsiveness to training-induced changes. Incorporating broader biochemical profiling (iron status, inflammation) and comparing sedentary, older, and youth groups would refine external validity and clarify physiological mechanisms.
5 Conclusion
In physically active young adults TMI shows stronger associations with bioimpedance-derived body fat than BMI and may aid field-based screening. Given the modest, homogeneous sample and the use of bioimpedance rather than a criterion method, confirmation in larger, sport-specific, and longitudinal studies—ideally including reference techniques (e.g., DXA) and broader hematological profiling—is recommended before informing athlete-level practice. Coupling TMI with simple hematological markers like HCT can enrich physical activity monitoring, inform individualized training, and reduce the risk of misclassification inherent in BMI. For health-related sport and exercise practitioners, this represents a low-cost, high-value upgrade to existing screening tools.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Non-Interventional Clinical Research Ethics Committee of Health Sciences University (Approval No: 2025-2/2-27). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
OY: Conceptualization, Data curation, Formal analysis, Investigation, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. VG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AC: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. EB: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. YP: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. MBa: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. NM: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. MBe: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. GB: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. SD: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. OK: Data curation, Investigation, Writing – original draft, Writing – review & editing. HK: Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ackland, TR, Lohman, TG, Sundgot-Borgen, J, Maughan, RJ, Meyer, NL, Stewart, AD, et al. Current status of body composition assessment in sport: review and position statement on behalf of the ad hoc research working group on body composition health and performance, under the auspices of the IOC medical commission. Sports Med. (2012) 42:227–49. doi: 10.2165/11597140-000000000-00000
2. Ben Mansour, G, Kacem, A, Ishak, M, Grélot, L, and Ftaiti, F. The effect of body composition on strength and power in male and female students. BMC Sports Sci Med Rehabil. (2021) 13:150. doi: 10.1186/s13102-021-00376-z
3. Castillo, M, Martínez-Sanz, JM, Penichet-Tomás, A, Sellés, S, González-Rodriguez, E, Hurtado-Sánchez, JA, et al. Relationship between body composition and performance profile characteristics in female futsal players. Appl Sci. (2022) 12:11492. doi: 10.3390/app122211492
4. Güney, Ş, Şahin, FN, Arslanoğlu, C, Güler, Ö, Aydoğmuş, M, Doğan, A, et al. Investigation of the playing digital games on shoulder flexibility, muscle strength and reaction speed in volleyball players. Front Public Health. (2024) 12:1493900. doi: 10.3389/fpubh.2024.1493900
5. Sutton, L, and Stewart, A. Body composition in sport, exercise and health. Abingdon: Routledge (2012).
6. Toselli, S. Body composition and physical health in sports practice: an editorial. Int J Environ Res Public Health. (2021) 18:4534. doi: 10.3390/ijerph18094534
7. Das, S, Barman, S, and Barman, S. Identification of body composition among sports persons In: Examining physiology, nutrition, and body composition in sports science (2024). 67–110. doi: 10.4018/979-8-3693-6317-1.ch003
8. Martín-Rodríguez, A, Belinchón-deMiguel, P, Rubio-Zarapuz, A, Tornero-Aguilera, JF, Martínez-Guardado, I, Villanueva-Tobaldo, CV, et al. Advances in understanding the interplay between dietary practices, body composition, and sports performance in young active adults. Nutrients. (2024) 16:571. doi: 10.3390/nu16040571
9. Pancar, Z, Akay, MK, İlhan, MT, Karaday, E, Karaca, B, Ulema, MS, et al. Effects of intermittent versus continuous small-sided games on athletic performance in male youth soccer players: a pilot study. Life. (2025) 15:364. doi: 10.3390/life15030364
10. Sansone, P, Makivic, B, Csapo, R, Hume, P, Martínez-Rodríguez, A, and Bauer, P. Body fat of basketball players: a systematic review and meta-analysis. Sports Medicine-Open. (2022) 8:26. doi: 10.1186/s40798-022-00418-x
11. Gürkan, AC, Eraslan, M, Aydın, S, Altuğ, T, Türkmen, M, Söyler, M, et al. Muscular strength and endurance adaptations to functional resistance training in young elite field hockey players. Front Physiol. (2025) 16:1536885. doi: 10.3389/fphys.2025.1536885
12. Jeejeebhoy, KN. Nutritional assessment. Gastroenterol Clin N Am. (1998) 27:347–69. doi: 10.1016/S0889-8553(05)70007-8
13. Muscogiuri, G, Verde, L, and Colao, A. Body mass index (BMI): still be used? Eur J Intern Med. (2023) 117:50–1. doi: 10.1016/j.ejim.2023.09.002
14. Nuttall, FQ. Body mass index: obesity, BMI, and health: a critical review. Nutr Today. (2015) 50:117–28. doi: 10.1097/NT.0000000000000092
15. Pray, R, and Riskin, S. The history and faults of the body mass index and where to look next: a literature review. Cureus. (2023) 15:e48230. doi: 10.7759/cureus.48230
16. Wu, Y, Li, D, and Vermund, SH. Advantages and limitations of the body mass index (BMI) to assess adult obesity. Int J Environ Res Public Health. (2024) 21:757. doi: 10.3390/ijerph21060757
17. Callahan, EANational Academies of Sciences, Engineering, and Medicine. The science, strengths, and limitations of body mass index In: Translating knowledge of foundational drivers of obesity into practice: Proceedings of a workshop series. Washington, DC: National Academies Press (US) (2023)
18. Riewald, S. Does the body mass index accurately reflect percent body fat in young active adults? Strength Cond J. (2008) 30:80–1. doi: 10.1519/SSC.0b013e318163bc23
19. Bharti, A, Kushwaha, A, and Yadav, SS. Tri-ponderal mass index—a reliable anthropometric index for early screening of adolescent obesity in a school-based setting: a cross-sectional study. Nutrition. (2025) 131:112639. doi: 10.1016/j.nut.2024.112639
20. De Lorenzo, A, Romano, L, Di Renzo, L, Gualtieri, P, Salimei, C, Carrano, E, et al. Triponderal mass index rather than body mass index: An indicator of high adiposity in Italian children and adolescents. Nutrition. (2019) 60:41–7. doi: 10.1016/j.nut.2018.09.007
21. Kuciene, R, and Dulskiene, V. Associations between tri-ponderal mass index, body mass index, and high blood pressure among children and adolescents: a cross-sectional study. Sci Rep. (2023) 13:18148. doi: 10.1038/s41598-023-45432-5
22. Malavazos, AE, Capitanio, G, Milani, V, Ambrogi, F, Matelloni, IA, Basilico, S, et al. Tri-ponderal mass index vs body mass index in discriminating central obesity and hypertension in adolescents with overweight. Nutr Metab Cardiovasc Dis. (2021) 31:1613–21. doi: 10.1016/j.numecd.2021.02.013
23. Peterson, CM, Su, H, Thomas, DM, Heo, M, Golnabi, AH, Pietrobelli, A, et al. Tri-ponderal mass index vs body mass index in estimating body fat during adolescence. JAMA Pediatr. (2017) 171:629–36. doi: 10.1001/jamapediatrics.2017.0460
24. Holmgren, A, Niklasson, A, Nierop, AF, Gelander, L, Aronson, AS, Sjöberg, A, et al. Pubertal height gain is inversely related to peak BMI in childhood. Pediatr Res. (2017) 81:448–54. doi: 10.1038/pr.2016.253
25. Johnson, W, Norris, T, Bann, D, Cameron, N, Wells, JK, Cole, TJ, et al. Differences in the relationship of weight to height, and thus the meaning of BMI, according to age, sex, and birth year cohort. Ann Hum Biol. (2020) 47:199–207. doi: 10.1080/03014460.2020.1737731
26. Wang, X, Ma, J, Huang, S, Dong, B, Dong, Y, Yang, Z, et al. Use of tri-Ponderal mass index in predicting late adolescent overweight and obesity in children aged 7–18. Front Nutr. (2022) 9:785863. doi: 10.3389/fnut.2022.785863
27. Bonilla, DA, Duque-Zuluaga, LT, Muñoz-Urrego, LP, Franco-Hoyos, K, Agudelo-Martínez, A, Kammerer-López, M, et al. Development and validation of a novel waist-girth-based equation to estimate fat mass in young young active adults. Nutrients. (2022) 14:4059. doi: 10.3390/nu14194059
28. Ripka, WL, Orsso, CE, Haqq, AM, Ulbrichtz, CM, Ulbricht, L, Leite, N, et al. Validity and accuracy of body fat prediction equations using anthropometrics measurements in adolescents. Eat Weight Disord. (2021) 26:879–886. doi: 10.1007/s40519-020-00918-3
29. Ramírez-Vélez, R, Correa-Bautista, JE, Carrillo, HA, González-Jiménez, E, Schmidt-RioValle, J, Correa-Rodríguez, M, et al. Tri-ponderal mass index vs. fat mass/height3 as a screening tool for metabolic syndrome prediction in Colombian children and young people. Nutrients. (2018) 10:412. doi: 10.3390/nu10040412
30. Anđelković, M, Baralić, I, Đorđević, B, Stevuljević, JK, Radivojević, N, Dikić, N, et al. Hematological and biochemical parameters in elite soccer players during a competitive half season. J Med Biochem. (2015) 34:460–6. doi: 10.2478/jomb-2014-0057
31. Clemente, FM, González-Fernández, FT, Ceylan, HI, Silva, R, Younesi, S, Chen, Y-S, et al. Blood biomarkers variations across the pre-season and interactions with training load: a study in professional soccer players. J Clin Med. (2021) 10:5576. doi: 10.3390/jcm10235576
32. Grzebisz-Zatońska, N. The relationship between inflammatory factors, hemoglobin, and VO2 max in male amateur long-distance cross-country skiers in the preparation period. J Clin Med. (2024) 13:6122. doi: 10.3390/jcm13206122
33. Haller, N, Reichel, T, Zimmer, P, Behringer, M, Wahl, P, Stöggl, T, et al. Blood-based biomarkers for managing workload in young active adults: perspectives for research on emerging biomarkers. Sports Med. (2023) 53:2039–53. doi: 10.1007/s40279-023-01866-5
34. Meurrens, J, Steiner, T, Ponette, J, Janssen, HA, Ramaekers, M, Wehrlin, JP, et al. Effect of repeated whole blood donations on aerobic capacity and hemoglobin mass in moderately trained male subjects: a randomized controlled trial. Sports Med. (2016) 2:43. doi: 10.1186/s40798-016-0067-7
35. Schuler, B, Arras, M, Keller, S, Rettich, A, Lundby, C, Vogel, J, et al. Optimal hematocrit for maximal exercise performance in acute and chronic erythropoietin-treated mice. Proc Natl Acad Sci. (2010) 107:419–23. doi: 10.1073/pnas.0912924107
36. Díaz Martínez, AE, Alcaide Martín, MJ, and González-Gross, M. Basal values of biochemical and hematological parameters in elite young active adults. Int J Environ Res Public Health. (2022) 19:3059. doi: 10.3390/ijerph19053059
37. Kelly, RS, Kelly, MP, and Kelly, P. Metabolomics, physical activity, exercise and health: a review of the current evidence. Biochim Biophysica Acta. (2020) 1866:165936. doi: 10.1016/j.bbadis.2020.165936
38. Palacios Le Blé, G, Pedrero Chamizo, R, Palacios Gil Antuñano, N, Maroto Sánchez, B, Aznar, S, and González Gross, MM. Biomarkers of physical activity and exercise. Nutr Hosp. (2015) 31:237–44. doi: 10.3305/nh.2015.31.sup3.8771
39. Cui, Y, Zhang, F, Wang, H, Zhao, L, Song, R, Han, M, et al. Temporal associations between tri-ponderal mass index and blood pressure in Chinese children: a cross-lag analysis. Nutrients. (2022) 14:1783. doi: 10.3390/nu14091783
40. Jeong, HR, Lee, HS, Shim, YS, and Hwang, JS. Positive associations between body mass index and hematological parameters, including RBCs, WBCs, and platelet counts, in korean children and adolescents. Children. (2022) 9:109. doi: 10.3390/children9010109
41. Özyildirim, C, Unsal, EN, and Ayhan, NY. Performance of triponderal mass index, body mass index z scores, and body mass index performance in the diagnosis of obesity in children and adolescents. Nutrition. (2023) 114:112116. doi: 10.1016/j.nut.2023.112116
42. Chen, R, Ji, L, Ma, L, Chen, Y, Duan, J, Ma, M, et al. Accuracy and capability of tri-ponderal mass index in assessing cardio-metabolic risk factors in Chinese children and adolescents aged 3 to 17 years, compared with body mass index. Chin Med J. (2023) 136:1339–48. doi: 10.1097/CM9.0000000000002349
43. Niu, Y, Zhang, Y, Sheng, J, Lu, W, Li, J, Mao, X, et al. Tri-ponderal mass index as a screening tool for obesity prediction in children aged 6–9 years.. Front. Endocrinol.. (2023) 14:1277125. doi: 10.3389/fendo.2023.1277125
44. Sun, J, Yang, R, Zhao, M, Bovet, P, and Xi, B. Tri-Ponderal mass index as a screening tool for identifying body fat and cardiovascular risk factors in children and adolescents: a systematic review. Front Endocrinol. (2021) 12:694681. doi: 10.3389/fendo.2021.694681
45. Alfonso, C, Haydt, V, Allen, MS, Capdevila, L, and Laborde, S. Monitoring training adaptation: a scoping review of the relationship between self-reported subjective variables and resting vagally-mediated heart rate variability (vmHRV) in adult young active adults. Int Rev Sport Exerc Psychol. (2025):1–38. doi: 10.1080/1750984X.2025.2541350
46. Saw, AE, Kellmann, M, Main, LC, and Gastin, PB. Athlete self-report measures in research and practice: considerations for the discerning reader and fastidious practitioner. Int J Sports Physiol Perform. (2017) 12:S2-127–35. doi: 10.1123/ijspp.2016-0395
47. Park, HK, and Shim, YS. Distribution of Tri-Ponderal Mass Index and its Relation to Body Mass Index in Children and Adolescents Aged 10 to 20 Years. J Clin Endocrinol Metab. (2020) 105:e826–e834. doi: 10.1210/clinem/dgaa030
48. Javed, A, Jumean, M, Murad, MH, Okorodudu, D, Kumar, S, Somers, VK, et al. Diagnostic performance of body mass index to identify obesity as defined by body adiposity in children and adolescents: a systematic review and meta-analysis. Pediatr Obes. (2015) 10:234–44. doi: 10.1111/ijpo.242
49. Grams, AC, Acevedo, AM, Price, P, Alvarez, K, Nowlen, M, Morton, R, et al. Body Mass Index Superior to Body Adiposity Index in Predicting Adiposity in Female Collegiate Athletes. Int J Exerc Sci. (2024) 16:1487–1489. doi: 10.70252/CJWQ8241
50. Kawai, T, Autieri, MV, and Scalia, R. Body fat estimation and systemic inflammation. Clin Physiol Funct Imaging. (2021) 320:C375–C391. doi: 10.1152/ajpcell.00379.2020
51. Scheffer, DDL, and Latini, A. Exercise-induced immune system response: Anti-inflammatory status on peripheral and central organs. Biochim Biophys Acta Mol Basis Dis. (2020) 1866:165823. doi: 10.1016/j.bbadis.2020.165823
52. Shao, T, Verma, HK, Pande, B, Costanzo, V, Ye, W, Cai, Y, et al. Physical Activity and Nutritional Influence on Immune Function: An Important Strategy to Improve Immunity and Health Status.. Front. Physiol. (2021) 12:751374. doi: 10.3389/fphys.2021.751374
53. Mahjoub, H. Red blood cells in sports: effects of exercise and training on oxygen supply by red blood cells. Front. Physiol. (2013) 4:332. doi: 10.3389/fphys.2013.00332
Keywords: physically active young adults, body fat, body mass index, hematology, triponderal mass index
Citation: Yaşar OM, Gürses VV, Ciğerci AE, Bal E, Pehlivan Y, Baş M, Malkoç N, Bektaş M, Başkaya G, Dündar S, Karakullukçu ÖF and Küçük H (2025) From BMI to TMI: revisiting adiposity and fitness assessment in young active adults through a historical and contemporary lens. Front. Public Health. 13:1700684. doi: 10.3389/fpubh.2025.1700684
Edited by:
Juel Jarani, Sports University of Tirana, AlbaniaReviewed by:
Robert Stanislaw Podstawski, University of Warmia and Mazury in Olsztyn, PolandBojan Masanovic, University of Montenegro, Montenegro
Copyright © 2025 Yaşar, Gürses, Ciğerci, Bal, Pehlivan, Baş, Malkoç, Bektaş, Başkaya, Dündar, Karakullukçu and Küçük. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hamza Küçük, aGFtemEua3VjdWtAb211LmVkdS50cg==