 Noriaki Watanabe1Masayoshi Kamijo1Kazuki Ashida2Fumihito Sasamori3Masao Okuhara4Suchinda Jarupat Maruo5Hisaaki Tabuchi6
Noriaki Watanabe1Masayoshi Kamijo1Kazuki Ashida2Fumihito Sasamori3Masao Okuhara4Suchinda Jarupat Maruo5Hisaaki Tabuchi6 Koji Terasawa7*
Koji Terasawa7*- 1Graduate School of Medicine, Science and Technology, Shinshu University, Ueda, Japan
- 2National Institute of Technology, Nagano College, Nagano, Japan
- 3Faculty of Engineering, Shinshu University, Nagano, Japan
- 4Department of Applied Information Engineering, Faculty of Engineering, Suwa University of Science, Chino, Japan
- 5Department of Occupational Health and Safety, Faculty of Public Health, Mahidol University, Bangkok, Thailand
- 6Department of Psychology, University of Innsbruck, Innsbruck, Austria
- 7Graduate School of Medicine, Shinshu University, Matsumoto, Japan
Extending healthy life expectancy requires attention not only to physical fitness but also to the development of cognitive self-regulation skills during childhood, which play a critical role in establishing lifelong health behaviors. Early health education has traditionally emphasized physical activity and lifestyle, yet cognitive aspects of self-control and inhibitory processes have received comparatively little attention. Inhibitory control is a central component of executive function, enabling children to regulate impulses, follow rules, and adapt to changing environments. Deficits in this capacity are associated with academic challenges, risk-taking behaviors, and poorer health outcomes later in life. Thus, incorporating assessments of cognitive inhibitory control into early health education may provide valuable insights for both educational and preventive health strategies. This pilot longitudinal study examined the feasibility of using the go/no-go task to assess inhibitory control in children aged 3–14 years in Nagano Prefecture, Japan. Assessments were conducted in 1998, 2008, and 2018, enabling exploration of changes over two decades. The task included three phases—formation, differentiation, and reverse differentiation—allowing for evaluation of both reaction times and error rates as indicators of speed–accuracy trade-offs in inhibitory performance. Results showed that children in 2018 exhibited significantly shorter reaction times but higher error rates compared with those assessed in 2008, suggesting a shift toward prioritizing speed over accuracy. These changes may reflect broader environmental and behavioral influences, such as increased exposure to digital devices, altered patterns of daily activity, or evolving educational contexts. Importantly, these findings indicate that inhibitory control, as captured by a simple cognitive paradigm, can reveal population-level shifts in child development over time. Incorporating cognitive tasks such as the go/no-go paradigm alongside conventional physical fitness testing in school-based health education may therefore enrich understanding of children's self-regulatory capacity. This approach has the potential to strengthen early identification of cognitive and behavioral trends, support tailored educational interventions, and inform broader community health promotion programs. By linking cognitive development with public health practice, it may contribute to strategies aimed at extending healthy life expectancy across the lifespan.
Introduction
The WHO (1) reports that regular physical activity is effective in preventing and treating non-communicable diseases (NCDs), such as heart disease, stroke, diabetes, breast cancer, and colorectal cancer; preventing hypertension, overweight, and obesity; and improving mental health, quality of life (QOL), and well-being. However, the WHO (2) also suggests that 70% of the world's population does not achieve 150 min of moderate physical activity per week. Therefore, the WHO (3, 4) set a goal to reduce this number by 15% by 2030. However, it is estimated that it is difficult for people around the world to maintain exercise habits. Since 1988, five districts in Nagano Prefecture, Japan, have implemented comprehensive social capital-oriented health education based on incorporating dementia prevention activities into systematic health education programs for older adult individuals and promoting empathy and collaboration (5–9). Therefore, to examine the implementation of health education, we utilized the PDCA (Plan, Do, Check, Action) cycle, which is an incentive requirement of the international standard ISO9001, ranging from checking on planning health education to reviewing after implementation (we obtained ISO9001 certification in 2014 and moved to self-declaration in 2021) (10–16).
In 1940, the Ministry of Education and the Ministry of Health, Labour and Welfare (17, 18) conducted physical fitness tests for 17–19-year-olds to improve physical fitness and prevent tuberculosis. Afterward, the jurisdiction of physical fitness tests was transferred from the Ministry of Education to the Sports Agency (19); since 2008, these tests have been conducted for 6–79-year-olds with the aim of maintaining and promoting lifelong health from childhood to old age. Therefore, it is necessary to consider the health of older adult individuals, occupational health, and early childhood health. Among these aspects, research has shown that participation in comprehensive early-stage health education programs reduces the likelihood of indulging in unhealthy habits and excessive alcohol, tobacco, and illegal drug use (20). Hence, the effectiveness of early health education from an early age has been examined (21, 22). However, to date, no established health education methods have been reported for early childhood, school-age, or adolescent individuals. In addition, health education for older adult individuals, along with physical fitness testing, is useful as a screening test for dementia as a form of cognitive inhibitory control. However, go/no-go tasks such as cognitive inhibitory control have not been implemented alongside physical fitness tests for early childhood, school-age, and adolescent individuals. In this study, the foundation of health promotion that has been developed through school-based physical fitness testing in Japan since 2008 was regarded as the basis of early health education. The study explored the possibility of positioning this framework as an educational approach for fostering self-regulation and inhibitory control in children. The go/no-go task was introduced as an objective tool for evaluating these cognitive abilities, and the study was conducted as a pilot investigation to examine its feasibility. Because this task has been used in health programs for older adult populations, the present study aimed to confirm its applicability to early childhood and school-age populations. The go/no-go paradigm has been widely used to evaluate age-related differences in inhibitory control and executive functioning, as performance in this task reflects developmental changes in attention, self-regulation, and response inhibition across the lifespan (5–7, 9–16). By assessing accuracy and reaction time at different ages, this task can identify specific stages of cognitive development and detect shifts in the balance between speed and accuracy. These features make it a valuable tool for examining how cognitive inhibitory control evolves from early childhood to older adulthood. This addition clarifies the relevance of the go/no-go task for identifying developmental stages of inhibitory control and aligns the present study with its broader application across the lifespan. Accordingly, the term health education was retained in the title to reflect the broader educational and public health significance of this work.
Therefore, the purpose of this study is to examine whether go/no-go tasks can be feasibly used as a health education program to measure cognitive inhibitory control in early childhood, school-age, and adolescent individuals in addition to physical fitness tests, as seen in the older adult population.
Methods
Participants
This longitudinal study was conducted three times over a 20-year period—in 1998, 2008, and 2018—targeting children in Nagano Prefecture, Japan. A go/no-go task was employed as a measure of cognitive inhibitory control in a pilot study aimed at informing future developments in early health education. The study included children attending the same affiliated preschools, elementary schools, and junior high schools in Nagano Prefecture.
In 1998, children in the first grade of elementary school were aged 6–7 years, born between April 2, 1992, and April 1, 1993; for consistency, their age was recorded as 6 years. The age for second-grade elementary school students was similarly set at 7 years.
Participation in parent meetings was voluntary, and non-participation had no negative consequences. Parents received detailed explanations about the study objectives and procedures, including potential risks, prior to participation. All methods were conducted in accordance with relevant guidelines and regulations. Written informed consent was obtained from all participants and their parents. Consent could be withdrawn at any time without penalty. Parents were assured that all data would be kept strictly confidential and handled securely.
The study protocol was approved by the Ethics Committee of Shinshu University (approval numbers: 003 and 180; approval dates: July 14, 2007, and April 14, 2012, respectively).
Brain function tests
This method was originally developed by Masaki and Moriyama in 1989 (23) and later applied by Terasawa et al. in 2014 (24), confirming its feasibility among young participants, and has since been adapted in subsequent studies (9, 24). Based on these previous studies, the present experiment followed the same basic procedure, which consisted of three components: formation, differentiation, and reverse differentiation.
In the formation experiment, participants were instructed to squeeze a rubber ball in response to randomly appearing red lights. Five trials were conducted.
In the differentiation experiment, participants squeezed the ball in response to a red light and refrained from squeezing in response to a yellow light. Twenty trials were conducted (10 per condition).
In the reverse differentiation experiment, participants were instructed to squeeze the ball in response to a yellow light and refrain from squeezing in response to a red light, with 20 trials conducted similarly. The stimulus durations ranged from 200 to 1,100 ms, and the interstimulus intervals varied randomly from 1,300 to 7,500 ms.
A miss was defined as a failure to squeeze the ball when required (go errors), and a mistake was defined as an incorrect squeeze when it was not required (no-go errors). We calculated the average reaction time for each of the three tasks, as well as the overall average reaction time. In addition, the total number of misses for the go tasks and the number of mistakes for the no-go tasks were recorded in both the differentiation and reverse differentiation conditions.
The go/no-go task was administered individually in a quiet classroom or gymnasium within each participating kindergarten or school. Participants were seated approximately 50 cm from the display monitor and instructed to press a button as quickly and accurately as possible in response to the stimuli presented on the screen. The stimuli were presented using the standardized Go/No-Go Task System Version 5.1, Faculty of Engineering, Shinshu University, Japan, which has been validated in previous studies involving both children and older adults (9–16). All sessions were conducted under standardized instructions and supervision by trained staff, following the same protocol during each measurement period 1998, 2008, and 2018.
Participants in each survey year were independently recruited, and no individuals were measured repeatedly across cohorts. Therefore, the data were treated as cross-sectional rather than longitudinal. One-way and two-way analyses of variance were used to examine differences by age group and measurement year. In future longitudinal studies, linear mixed-effects models will be considered to account for within-subject variability over time.
Statistical analysis
This study included a total of 1,164 children aged 3 to 14 years, with 443 in 1998, 391 in 2008, and 330 in 2018. Because this was an exploratory longitudinal study aiming to assess feasibility rather than to test a specific hypothesis, no a priori power calculation was conducted. However, the total sample size exceeded 1,000 participants across the three survey periods, which is sufficient to detect medium effect sizes (η2 > 0.02) in repeated-measures ANOVA. These results can therefore serve as a reference for determining sample sizes in future confirmatory studies. Reaction times and related variables from the go/no-go tasks were analyzed using two-way repeated measures ANOVA, with survey year (1998, 2008, 2018) and participant age (3–14 years) as factors. When significant interactions were observed, simple main effects were examined. The Bonferroni method was used for multiple comparisons if significant effects were found. Reaction time data for 1998 were not available at all ages; thus, they were excluded from analysis.
All statistical analyses were conducted using SPSS Statistics version 29 (IBM Corp.). Statistical significance was set at p < 0.05.
Results
The number of participants was 443 in 1998, 391 in 2008, and 330 in 2018, totaling 1,164 children aged 3 to 14 years (Table 1). Figure 1 illustrates the average reaction times for the formation, differentiation, and reverse differentiation tasks in 2008 and 2018.

Table 1. The number of participants by age in 1998, 2008 and 2018.
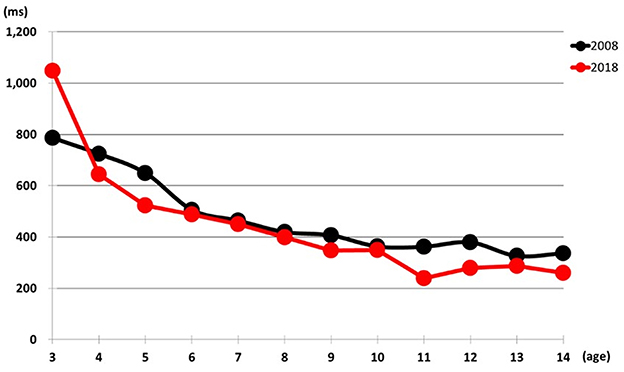
Figure 1. Comparison of average reaction times between 2008 and 2018.
A significant interaction was observed in total reaction time [F (11,697) = 8.973, p < 0.001]. Specifically, 3-year-olds showed significantly longer reaction times in 2018 than in 2008 (1,048 ms vs. 786 ms, p < 0.001). In contrast, children aged 4, 5, 11, 12, and 14 years demonstrated significantly shorter reaction times in 2018 than in 2008 (p < 0.01 to p < 0.001), indicating a trend toward faster responses among older children in more recent years (Figure 1, Table 2).

Table 2. Relationship between in 2008 and 2018.
Regarding the difference in reaction time between differentiation and formation tasks, no significant interaction was observed [F (11,697) = 0.696, p = 0.743). However, the main effects revealed that the average difference was significantly smaller in 2018 (69 ms) compared to 2008 (156 ms), suggesting improved cognitive efficiency in more recent cohorts (Figure 2, Table 3).
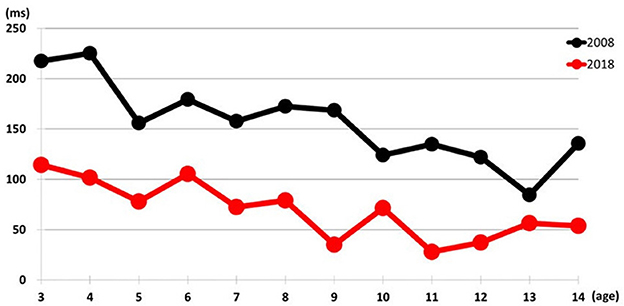
Figure 2. Comparison of differentiation minus formation reaction time in 2008 and 2018.

Table 3. Relationship between in 2008 and 2018.
As shown in Figure 3, the total number of misses in differentiation and reverse differentiation tasks decreased with age across all 3 years. No significant interaction was found (F (11,697) = 0.651, p = 0.889], and children aged four and older consistently made fewer than two misses, indicating increased attentional control with age (Table 4).
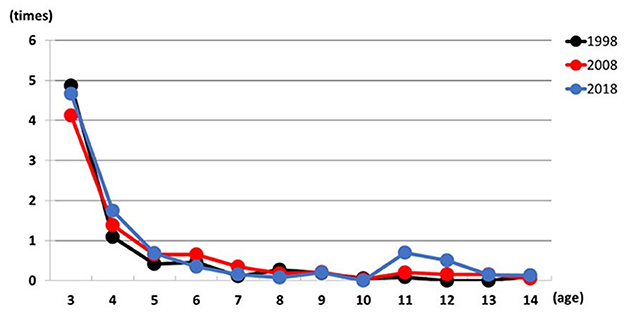
Figure 3. Relationship between total number misses and age in 1998, 2008, and 2018.

Table 4. Results of two-way ANOVA for reaction time, misses, and mistakes by survey year and age group.
Figure 4 presents the total number of mistakes in differentiation and reverse differentiation tasks. A significant interaction was found [F (22,1128) = 2.074, p < 0.01]. Children aged 6, 8, 9, and 11 years showed significantly higher mistake rates in 2018 than in previous years. For example, 6-year-olds made 8.5 mistakes in 2018, compared to 3.6 in 1998 and 3.4 in 2008 (p < 0.001). Similar trends were seen in other age groups, including notable increases among 7, 10, and 13–14-year-olds in 2018 vs. 1998, and among 12-year-olds in 2018 vs. 2008. Additionally, 3-year-olds consistently had higher mistake counts than most other age groups in both 1998 and 2008, while 6-year-olds in 2018 outperformed 5, 13, and 14-year-olds (p < 0.05). These results indicate age-specific patterns in error rates that have shifted over time (Table 5).
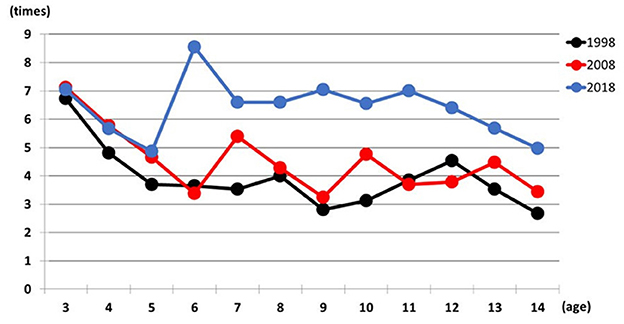
Figure 4. Relationship between total number mistakes and age in 1998, 2008, and 2018.

Table 5. Relationship between in 1998, 2008 and 2018.
Discussion
This study was a pilot investigation aimed at supporting the future development of early health education. It was conducted longitudinally over a 20-year period (1998, 2008, and 2018) and involved children in Nagano Prefecture, Japan. The purpose was to assess whether health education incorporating cognitive inhibitory control tasks—similar to those used for the older adult—could be applied to younger populations using the go/no-go paradigm.
Our findings revealed significantly shorter reaction times in the differentiation-minus-formation task and a significantly higher number of mistakes in 2018 compared to 2008. This suggests that greater emphasis may have been placed on speed, potentially at the cost of accuracy. Prior studies indicate that inhibition is more difficult at faster response speeds (25, 26). The observed reductions in both differentiation and formation task times further suggest that the time required to process and respond to stimuli was shortened in 2018. Consequently, some decisions may have been made too hastily, leading to incorrect responses.
Environmental changes in children's lifestyles may partially account for these shifts. For example, brain function differs depending on whether one solves arithmetic problems mentally or with a calculator, with significantly lower cerebral blood flow observed during calculator use (27). Increasing activities that stimulate the brain may lead to more complex neural connections and enhanced cognitive function (28, 29).
Dual-task training in older adult adults, combining physical activity with mental tasks such as arithmetic, has demonstrated positive effects on go/no-go performance. One study reported that such training increased cerebral blood flow during the go task and reduced it during the no-go task (30). Initially, older adults showed faster reaction times but made more errors. After walking approximately 7,000 steps daily for a year, their error rates decreased even as decision-making time increased. Continued training in the second year further reduced both reaction times and errors due to improved decision accuracy (7).
These findings suggest that similar dual-task interventions—combining physical exercise and cognitive tasks—might be effective for children as well. While causality remains unclear, our results support the idea that early health education incorporating both physical and cognitive elements, such as the go/no-go task, may be valuable. These tasks could serve as effective tools for promoting self-regulatory development in children, analogous to their use in older adult health programs.
This pilot study did not aim to use the go/no-go task as a direct intervention tool, but rather to examine its feasibility as a cognitive assessment component within health education. Performance on the go/no-go task generally improves with age and develops in association with the maturation of neural circuits in the prefrontal cortex responsible for executive functions. These characteristics are consistent with previous studies showing that sustained attention and response inhibition gradually improve throughout development (31–33). Accordingly, this study positioned the go/no-go task as a potential framework for evaluating and understanding children's self-regulation and attention in early health education. The go/no-go task has long been applied in health education and cognitive assessments among older adults. Extending this framework to children and adolescents, the present study explored the possibility of incorporating cognitive components into early health education. Future research should develop specific training protocols that include diverse stimuli, increased trial numbers, and multiple sessions to examine the potential of the go/no-go task as a tool for improving inhibitory control. As information on participants' educational background and physical or mental health was not collected in this study, this has been identified as a limitation. These factors will be examined in future longitudinal studies to deepen the understanding of individual differences in cognitive development.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets generated and analyzed for this study are not publicly available due to ethical and privacy restrictions. Individual-level data contain sensitive information on children and cannot be shared openly. Requests to access the datasets should be directed to the corresponding author (a3RlcmFzYUBzaGluc2h1LXUuYWMuanA=) and will be considered in accordance with institutional and ethical guidelines. Requests to access these datasets should be directed to a3RlcmFzYUBzaGluc2h1LXUuYWMuanA=.
Ethics statement
The studies involving humans were approved by Ethics approval all procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Ethics Committee of Shinshu University (control numbers: 003 and 180; receipt: 7/14/2007 and 4/14/2012). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants‘ legal guardians/next of kin. Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
NW: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. MK: Conceptualization, Project administration, Supervision, Writing – review & editing. KA: Investigation, Visualization, Writing – review & editing. FS: Investigation, Visualization, Writing – review & editing. MO: Methodology, Visualization, Writing – review & editing. SM: Investigation, Writing – original draft, Writing – review & editing. HT: Methodology, Writing – original draft, Writing – review & editing. KT: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported by the Ministry of Education, Culture, Sports, Science and Technology (MEXT) Encouraged Research-A (10780017 and 1998–2000), Grants-in-A for Scientific Research (25257101 and 2013–2015), Challenging Exploratory Research (26560380 and 2014–2016), and Grant-in-A for Scientific Research (16H02713 and 2016–2018).
Acknowledgments
The authors would like to express their gratitude to the kindergarteners, students, and all the teachers at the Shinshu University Faculty of Education Kindergarten, Shinshu University Faculty of Education Elementary School, and Shinshu University Faculty of Education Junior High School who cooperated in this research.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization Eastern Mediterranean Region. (2024). Available online at: https://www.who.int/about/accountability/results/who-results-report-2024-2025/region-EMRO/ (Accessed September 1, 2025).
2. World Health Organization Nearly 1.8 Billion Adults at Risk of Disease From not Doing enough Physical Activity. (2024). Available online at: https://www.who.int/news/item/26-06-2024-nearly-1.8-billion-adults-at-risk-of-disease-from-not-doing-enough-physical-activity/ (Accessed September 1, 2025).
3. World Health Organization Physical Activity. (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/physical-activity/ (Accessed September 1, 2025).
4. World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. (2024). Available online at: https://www.who.int/publications/i/item/9789241514187/ (Accessed September 1, 2025).
5. Nakade K, Abe K, Fujiwara T, Terasawa K, Okuhara M, Nakajima K, et al. The influence of two different health education programs on go/no-go task, physical fitness test and blood test. J Physiol Anthropol. (2009) 14:143–153 (Japanese). doi: 10.20718/jjpa.14.3_143
6. Murata Y, Watanabe T, Terasawa S, Nakajima K, Kobayashi T, Zhang Y, et al. Effect of a two-year health program on brain function, physical fitness and blood chemistry. J Community Med Health Educ. (2015) 5:1–6. doi: 10.4172/2161-0711.1000349
7. Nakade K, Fujimori S, Watanabe T, Murata Y, Terasawa S, Maruo SJ, et al. A case study of health education from Nagano prefecture in Japan: the relationship between health education and medical expenses. J Community Med Health Educ. (2017) 7:1–6. doi: 10.4172/2161-0711.1000529
8. Fujimori S, Ashida K, Watanabe N, Nishino T, Sasamori F, Okuhara M, et al. Human rights health care measures reporting physical fitness test for ages 6 to 17 with 10-year follow-up. Int J Hum Rights Healthc. (2024) 18:92–106. doi: 10.1108/IJHRH-12-2023-0092
9. Watanabe N, Kamijo M, Nishino T, Ashida K, Sasamori F, Okuhara M, et al. The feasibility of using the go/no-go task as a dementia screening test assessed with a cross-sectional design. Sci Rep. (2024) 14:29834. doi: 10.1038/s41598-024-81301-5
10. Fujimori S, Maruo JS, Piaseu N, Kalampakorn S, Sasimonthonkul S, Nakade N, et al. The effectiveness of a Japanese style health program: comparison between Minowa, Japan and Rayong, Thailand. Heliyon. (2017) 4:e.00961. doi: 10.1016/j.heliyon.2018.e00961
11. Fujimori S, Maruo JS, Watanabe T, Taki N, Sasamori F, Kobayashi K, et al. Effectiveness of a Japanese-style health program in Minowa Town, Matsumoto city and Nagano 255 city Japan. Int J Hum Rights Healthc. (2020) 13:1–17. doi: 10.1108/IJHRH-01-2020-0002
12. Maruo JS, Sanongdetch W, Choeychom S, Chansirikarn S, Thrakul S, Phuphaibul R, et al. Comparing the effectiveness of health program in Thailand and Japan. J Nurs Care. (2015) 4:1–6. doi: 10.4172/2167-1168.1000298
13. Putu GA, Terasawa K, Maruo JS, Nakade N, Watanabe T, Terasawa S, et al. The effect of health education as non-pharmacological therapy on physical fitness, blood chemistry and brain function among senior citizen in both rural and urban areas of Bali, Indonesia. Int J Pharm Pharm Sci. (2021) 13:24–8. doi: 10.22159/ijpps.2021v13i2.40151
14. Maruo JS, Piasue N, Kalampakom S, Utthiya P, Sasimonthonkul S, Tabuchi H, et al. The effectiveness of a health promotion program using the International Organization for Standardization in Klongyong and Nikhompattana, Thailand. Asian J Pharm Clin Res. (2020) 13:1–6. doi: 10.22159/ajpcr.2020.v13i3.36506
15. Terasawa K, Putu GA, Nyoman I, Maruo JS, Kalampakorn S, Watanabe T, et al. Implementation of a health education program in Asia, comparing Thailand, Indonesia, and Japan. Technol Health Care. (2022) 30:775–85. doi: 10.3233/THC-202583
16. Aznar SP, Nino ISP, Sergio JRS, Rigan PAA, Maruo JS, Sasamori F, et al. A report on attempts to acquire exercise habits through Japanese health education for adult workers from Cebu, Philippines. Health Scope. (2023) 12:e134198. doi: 10.5812/healthscope-134198
17. Ministry Ministry of Education Culture Sports Science and Technology. New Physical Fitness Test Implementation Guidelines. (2009). Available online at: https://www.mext.go.jp/a_menu/sports/stamina/03040901.htm (Accessed September 1, 2025).
18. Ministry Ministry of Health Labour and Welfare. White Paper Towards the realization of a society of healthy longevity - Year 1 of health and prevention -Chapter 1: Changes in health-related policies in Japan. (2014). p 4–42. Available online at: https://www.mhlw.go.jp/wp/hakusyo/kousei/14/dl/1-01.pdf (Accessed September 1, 2025).
19. Japan Sports Agency. Physical Fitness and Athletic Ability Survey - Summary of Results, 2003-2023. (2017). Available online at: https://www.mext.go.jp/sports/b_menu/toukei/chousa04/tairyoku/1368148.htm (Accessed September 1, 2025).
20. UNICEF. Annual Report 2022. (2022). Available online at: https://www.unicef.org (Accessed September 1, 2025).
21. Ramon I, Chattopadhyay SK, Barnett WS, Hahn RA, Community Preventive Services Task Force. Early childhood education to promote health equity: a community guide economic review. J Public Health Manag Pract. (2018) 24:8–15. doi: 10.1097/PHH.0000000000000557
22. Ekwaru PJ, Ohinmaa A, Dabravolskaj J, Maximova K, Veugelers JP. Cost-effectiveness and return on investment of school-based health promotion programmes for chronic disease prevention. Eur J Public Health. (2021) 31:345–51. doi: 10.1093/eurpub/ckab130
23. Masaki T, Moriyama G. Study on Types of Human Higher Nervous Activity. Tokyo: Tokyo University of Science Press. 4:69–81. (Japanese).
24. Terasawa K, Tabuchi H, Yanagisawa H, Yanagisawa A, Shinohara K, Terasawa S, et al. Comparative survey of go/no-go results to identify the inhibitory control ability change of Japanese children. BioPsychoSoc Med. (2014) 8:1–7. doi: 10.1186/1751-0759-8-14
25. Aron AR, Poldrack RA. Cortical and subcortical contributions to stop signal response inhibition: Role of the subthalamic nucleus. J Neurosci. (2006) 26:2424–33. doi: 10.1523/JNEUROSCI.4682-05.2006
26. Bari A, Robbins TW. Inhibition and impulsivity: behavioral and neural basis of response control. Prog Neurobiol. (2013) 108:44–79. doi: 10.1016/j.pneurobio.2013.06.005
27. Murata Y, Tabuchi H, Watanabe T, Terasawa S, Nakajima K, Kobayashi T, et al. Comparison of cortical activation during subtraction in mental calculation and with a calculator. Biochem Anal Biochem. (2015) 4:2–5. doi: 10.4172/2161-1009.1000185
28. Draganski B, Gaser C, Busch V, Schuierer G, Bogdahn U, May A. Neuroplasticity: changes in grey matter induced by training. Nature. (2004) 427:311–22. doi: 10.1038/427311a
29. Erickson KI, Colcombe JS, Wadhwa R, Bherer L, Peterson SM, Scalf EP, et al. Training-induced functional activation changes in dual-task processing: an fMRI study. Cereb Cortex. (2007) 17:192–204. doi: 10.1093/cercor/bhj137
30. Kaneko K, Sasamori F, Okuhara O, Maruo JS, Ashida K, Tabuchi H, et al. Evaluation of a dementia prevention program to improve health and social care and promote human rights among older adults. Int J Hum Rights Healthc. (2024) 17:274–85. doi: 10.1108/IJHRH-12-2021-0206
31. Casey BJ, Tottenham N, Liston C, Durston S. Imaging the developing brain: what have we learned about cognitive development? Trends Cogn Sci. (2005) 9:104–10. doi: 10.1016/j.tics.2005.01.011
32. Luna B, Garver KE, Urban TA, Lazar NA, Sweeney JA. Maturation of cognitive processes from late childhood to adulthood. Child Dev. (2004) 75:1357–72. doi: 10.1111/j.1467-8624.2004.00745.x
Keywords: early health education, cognitive inhibitory control, go/no-go task, health behavior, children
Citation: Watanabe N, Kamijo M, Ashida K, Sasamori F, Okuhara M, Maruo SJ, Tabuchi H and Terasawa K (2025) Early health education and cognitive inhibitory control in children: a 20-year pilot study using the go/no-go task in Japan. Front. Public Health 13:1703017. doi: 10.3389/fpubh.2025.1703017
Received: 10 September 2025; Accepted: 23 October 2025;
Published: 20 November 2025.
Edited by:
Carlos Alberto De Oliveira Magalhães Júnior, State University of Maringá, BrazilReviewed by:
Gabriel Barg, Catholic University of Uruguay, UruguayLei Xu, South China University of Technology, China
Copyright © 2025 Watanabe, Kamijo, Ashida, Sasamori, Okuhara, Maruo, Tabuchi and Terasawa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Koji Terasawa, a3RlcmFzYUBzaGluc2h1LXUuYWMuanA=