 Tinu Mary Samuel1†
Tinu Mary Samuel1† Qianling Zhou1†‡
Qianling Zhou1†‡ Francesca Giuffrida1
Francesca Giuffrida1 Daniel Munblit2,3
Daniel Munblit2,3 Valérie Verhasselt4
Valérie Verhasselt4 Sagar K. Thakkar5*
Sagar K. Thakkar5*- 1Nestlé Research, Lausanne, Switzerland
- 2Department of Paediatrics and Paediatric Infectious Diseases, Institute of Child's Health, Sechenov First Moscow State Medical University, Moscow, Russia
- 3Inflammation, Repair and Development Section, National Heart and Lung Institute, Faculty of Medicine, Imperial College London, London, United Kingdom
- 4University de Nice Sophia Antipolis, Nice, France
- 5Nestlé Research, Singapore, Singapore
Human milk (HM) is dynamic and shows a high inter- and intra-individual variability. To characterize HM with precision, it is necessary to understand the factors that modulate its composition. The objective of this narrative review is to summarize the maternal, infant and methodological factors that affect HM composition. We searched SCOPUS and PubMed databases for articles related to factors that are known to or could potentially influence HM composition and volume across lactation periods. Our comprehensive review encompasses various maternal-, infant-related, and methodological factors that modulate aspects of HM composition including macro- and micronutrients, vitamins and minerals, as well as volume. The most profound changes were observed in HM lipids and lipophiles. Evidence exists for many of the infant-related factors known to affect the nutritive and non-nutritive components of HM (e.g., birth weight, gestational age, infant age/stage of lactation). In contrast, less is known with respect to maternal factors; where there is either limited research or conflicting evidence (e.g., maternal lifestyle, obstetric history, medical conditions), except for the mother's diet, for which there is a relatively well-established understanding. Equally, although many of the methodological factors (e.g., HM sampling, handling and analytics) are known to impact HM composition, few studies have investigated this as a primary outcome, making it an important area of future research in HM. Here we propose a systematic capture of numerous maternal- and infant-related characteristics to facilitate associative comparisons of HM data within and across studies. Additionally, it would be prudent to standardize the methodological aspects known to affect HM composition in analytics, not only for HM lipids and lipophiles, but also for those nutrients whose variability is yet less well-understood. Defining the factors determining HM composition with accuracy will open perspectives for maternal intervention to optimize milk composition for specific needs of infants.
Introduction
Breastfeeding i.e., human milk (HM1) feeding either from the infant's own mother, or wet nurses as in the past, was and continues to remain the feeding norm for new-born infants. Benefits of breastfeeding for both infants and mothers, in short- and long-term are well-documented (1–5). A recent publication indicates a protective effect of breastfeeding against childhood infections and malocclusion, increases in intelligence, and probable reductions in overweight and diabetes later in life (6). Mothers may also benefit from breastfeeding in that risk of breast, uterine and ovarian cancer is reduced, and post-partum weight loss is promoted (6). With multiple benefits of breastfeeding, it is no surprise that characterization of HM composition is of increasing interest in order to gain insights into the underlying factors that contribute to the benefits of breastmilk.
HM is a highly complex, and dynamic biological fluid rich in nutritive (e.g., lipids, proteins, carbohydrates, fatty acids, amino acids, minerals, vitamins, trace elements, etc.) and non-nutritive bioactive components (e.g., cells, Ig, cytokines, chemokines, hormones, growth factors, glycans, mucins, etc.). It provides protection against infection and inflammation, and contributes to immune maturation, organ development, microbiota colonization and overall infant health (7–9).
It is hypothesized that HM is tailor-made by each mother to meet the nutritional needs of her growing infant; plasticity of HM composition may be key to early infant growth and programming of health in later life. Studying HM composition is essential to not only understand the nutritional needs but also to correlate with other developmental outcomes of infants (e.g., neurodevelopment, immune development, and gut maturation). Understanding the associations between HM composition and developmental outcomes can also lead to strategies for modifying maternal nutrition in cases where needed and to adapt fortification strategies for preterm infants.
While there exist published reviews in which a selection of factors that influence the composition of HM is described, to our knowledge no review considers the numerous aspects that affect the composition and volume of HM. With our narrative review we aim to collate the most relevant factors that influence nutritional and non-nutritional composition of HM, namely both maternal- and infant-related factors. In addition, we highlight methodological aspects that affect the quantification of HM components in research settings, which in turn leads to a set of scientific recommendations for HM sampling, handling, and analytical characterization when embarking on research in this field. On the one hand, we attempt to be as comprehensive as possible. On the other, it would simply be too much for one paper to provide an in-depth review of all topics that modulate HM composition and volume. Therefore, the purpose here is to identify and focus on the most important factors including maternal diet, supplementation, galactagogues, maternal anthropometry, obstetric history, socio-demographic factors, medical conditions, as well as infant-related factors such as infant birth weight and sex. Temporal changes in HM volume and composition are also included. In addition, methodological factors affecting the quantification of HM components are assessed. Other factors are deprioritized but summarized and listed as further reading.
Methodology
Literature Search
We conducted a narrative literature review and search using SCOPUS and PubMed database with predefined keywords for all scientific literature related to factors that are known to or could potentially influence HM composition and volume across lactation.
An initial search was performed limited to titles, key words, and abstracts to assess the potential yield of the search strategy. Based on the results, search terms were modified (e.g., wild characters) or additional terms were included. A subsequent search included MeSH terms. The search terms were grouped into 2 different concepts, which were combined with Boolean term “AND.” Terms within each concept were combined with the Boolean term “OR.”
Concept 1: human milk, breast milk, mothers' milk, mothers' own milk, colostrum
Concept 2: maternal/mothers' diet, supplementation, anthropometry, smoking, alcohol consumption, coffee consumption, physical activity, breastfeeding frequency, parity, mode of delivery, cesarean section, age, socioeconomic status, psychology, drugs, galactagogues, infant sex/gender, gestational age at birth, small for gestational age, low birth weight, foremilk/midmilk/hindmilk, preterm, feeding time, type of expression, storage temperature/length, milk processing/pasteurization.
The search was limited to English language abstracts and articles only.
Selection Criteria
We did not eliminate any kind of study design for initial screening as long as it met search criteria. Articles include original research, literature review and conference abstracts/papers/presentations that were published up to December 2018. After a final selection by reading the abstract of each article, 260 relevant papers were included.
Results
Factors that impact HM composition and/or volume are summarized into the following two categories:
1. Maternal and infant characteristics affecting HM components
2. Methodological parameters affecting the quantification of HM components
The resulting information leads to a set of scientific recommendations for reproducible HM analysis in interventional as well as observational studies (see Methodological factors affecting the quantification of HM components in a research setting).
Maternal Factors Affecting HM Volume and Composition
Maternal Diet
Maternal diet is an important factor that influences the volume and composition of HM. Some components have been studied extensively, while others require further research to draw strong conclusions. The results of our analysis are summarized in Table 1. Furthermore, a systematic analysis of the influence of maternal diet on HM composition, micro- and macronutrients, emphasized the relation of fatty acid intake, the intake of fat-soluble vitamins, vitamin B1, and vitamin C to their content in HM (10).
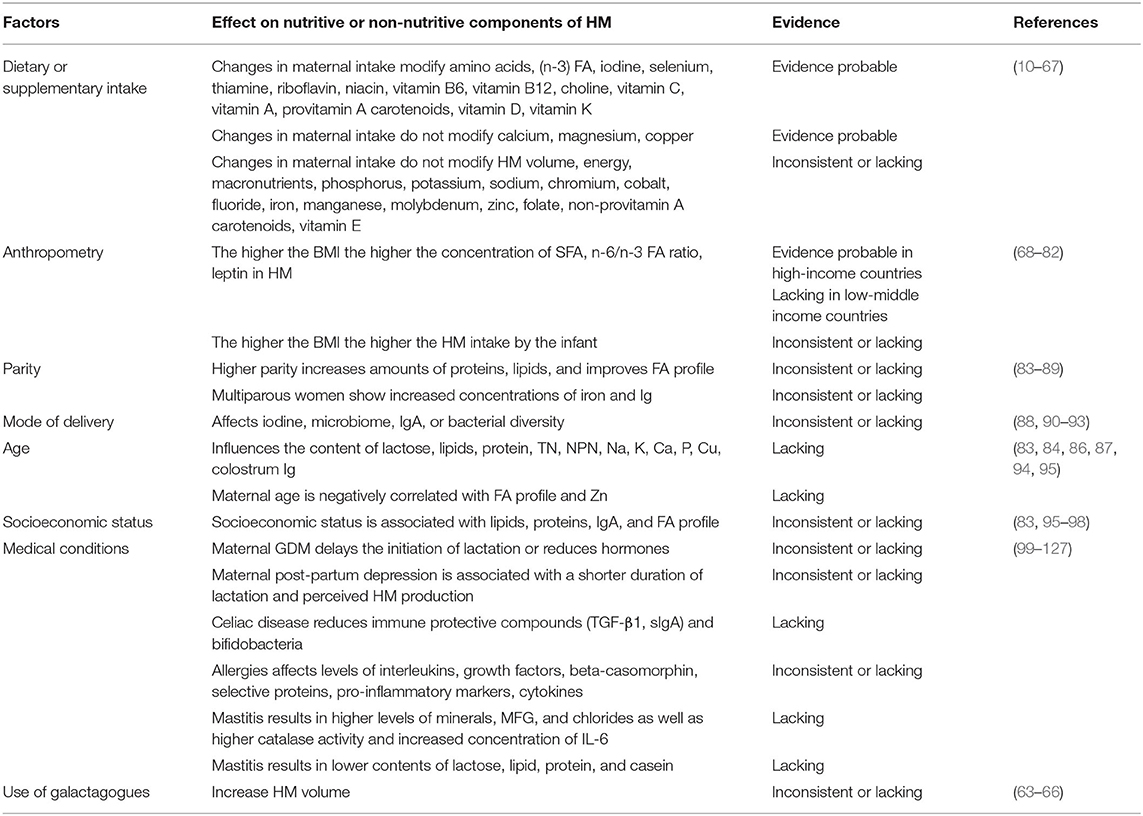
Table 1. Maternal factors affecting nutritive and non-nutritive components of human milk.
Effects of maternal diet on macronutrient content in HM
The macronutrient composition of HM is relatively constant across populations despite variations in the nutritional status of the mother (7). The effect of maternal energy intake on HM volume has shown conflicting results. Some studies showed that provision of additional calories (11, 128), energy restriction (12), or fasting (13) had no impact on HM volume, while others showed that a low calorie diet (1,200 kcal per day for 3 days) (14) or low energy intake (15) resulted in reduced HM production. In terms of macronutrient composition, an isocaloric high fat diet (16) and increased dietary consumption of proteins (17) and carbohydrates (18) demonstrated an increased HM fat concentrations at different stages. No significant differences in energy content of HM were found up to 12-weeks post-partum supplemented with a commercially available product, despite the higher energy intake (19). The same study revealed a greater volume of HM in mothers with a low mid upper arm circumference (<24.1 cm) following supplementation. Several reviews have highlighted the population differences in HM fatty acid composition and the influence of maternal diet on levels of PUFAs [including HM linoleic acid (LA), α-linolenic acid (ALA), and DHA] (20–22). A study provided supporting evidence that the quality of fatty acid intake during pregnancy and lactation is important (23). In this study the abundance of n-6 fatty acids (FA) and low n-3 FA, was reflected in the fatty acid composition of HM, in as such that DHA concentrations were significantly reduced particularly during lactation compared to pregnancy, while arachidonic acid (AA) did not follow the same development. On the contrary, women who consumed 2 portions of salmon per week from 20 week of pregnancy until delivery showed higher proportions of EPA (80%), DPA (30%), and DHA (90%) on day 5 post-partum (24). The impact of omega-3 supplementation during pregnancy and/or lactation on HM FA is well-studied: a systematic review found a positive relationship between the consumption of omega-3 sources and their concentration in HM, despite differences in the methods used, timing of supplementation, source of omega-3 source used, and the sample size (25). Supplementation with fish oil starting at 20 weeks of pregnancy until delivery not only increased the long-chain omega-3 FAs in HM during early lactation (up to 6 weeks post-partum), furthermore DHA levels at day 3, 6, weeks and 6 months were positively associated with infant DHA status at 1 year (26). Supplementing lactating women 4–6 weeks post-partum with either 200 mg or 400 mg DHA for 6 weeks with usual diets led to a 50 and 123% respective increase in HM DHA levels (27).
In terms of carbohydrate type, a randomized crossover study revealed that the consumption of a high-fructose corn syrup–sweetened beverage increased concentrations of fructose in HM, which stayed elevated for 5 h (28). No such effects were found for glucose or lactose. The consequences of habitual consumption of high-fructose sweetened beverages for early development need to be further investigated, but evidence exists that fructose in HM is positively associated with infant's body composition (29).
Effect of maternal mineral supplementation on mineral content of HM
Iodine supplementation (75–400 mg iodine/day) increased HM iodine concentrations (30–32), although a lower dose (75 or 150 μg/d) through either supplementation (31) or fortification (33) may be insufficient to ensure adequate iodine status in women or their infants. Equally, administering a single dose of 400 mg iodine as oral iodized oil to mothers may be an effective strategy to provide adequate iodine to their infants through HM for at least 6 months compared with direct supplementation to infants (30). The results of Mulrine et al. where iodine concentrations in HM were 1.3 and 1.7 times higher in women supplemented with 75 and 150 μg per day would also suggest a dose-response relationship (31). A systematic review of epidemiological and clinical data suggested that a high dose as well as daily iodine supplementation were effective in increasing iodine concentrations in HM (34). The same authors also concluded that iodine concentrations of around 150 μg/l during the first 6 months of lactation are enough to meet infants' needs. Selenium (Se) supplementation at a dose of 20 μg/day, approximating the quantity secreted into HM, (35) or 200 μg/day (36) increased HM selenium concentrations accompanied by an increase in infant Se intake. It is known that HM concentrations of minerals such as zinc and iron are not largely altered by deficiency or excesses in the maternal diet as these have well-regulated homeostatic processes (37). Zinc supplementation studies (10–50 mg/day) provided inconsistent findings, with some reporting an increase or prevention in decline in HM zinc concentration compared with placebo (38), while others did not find an effect of zinc supplementation (39, 40). Observational studies show reduced levels of iron in the HM of anemic mothers (41) and iron supplementation among women with low baseline levels of iron, was shown to increase HM iron concentrations (42). However, studies among healthy lactating women have failed to demonstrate an association between iron intake of the mother and HM iron concentrations (37, 43). There are physiological changes that happen during lactation, such as changes in calcium and bone metabolism, that provide sufficient calcium for HM production independent of maternal calcium supply in populations where calcium intakes are close to current recommendations (44). Furthermore, dietary nutrient consumption had no strong association with calcium concentrations in HM of three different ethnic groups in New Zealand (45). In this study, calcium intake of the mothers varied from 736 to 1,041 mg/day, but had no significant effect on the calcium concentration in HM.
Effect of maternal vitamin supplementation on vitamin content of HM
Maternal supplementation of B vitamins during lactation is known to rapidly increase their concentrations in HM as reviewed extensively Allen et al. (46). Evidence suggests that HM concentrations of thiamine, similar to those observed in well-nourished mothers, can be maintained by maternal thiamine intake of 2 mg/d (47). The concentrations of vitamin B6 in HM (ranging from 0.89 to 1.31 nmol/L) appear to be saturated at an intake of 2.5 mg/d of vitamin B6 (48, 49). Vitamin B12 supplementation (50 μg/d) was shown to maintain elevated concentrations of B12 in HM only during the supplementation period (6-week post-partum) (50) and the concentrations observed were much lower than those reported with a higher dose of 250 μg/d dose (97 vs. 235 pmol//L) (51). Choline supplementation of 750 mg/d increased HM concentrations of free choline, betaine, and phosphocholine (52), while a higher dose (930 mg/d) resulted in significantly higher concentrations of phosphocholine and glycerylphosphorylcholine (GPC), the main choline metabolites in HM as well as HM trimethylamine N-Oxide (TMAO), which is essential for maintaining osmotic balance and glycine concentrations (critical for production of glutathione that appear limiting in early development) (53). Similarly, higher lutein and zeaxanthin concentrations in HM have also been observed with lutein supplementation of 6 mg/d (140% higher) and 12 mg/d (250% higher) compared with the placebo (54). Further evidence comes from a study with Korean mothers, where a higher dietary intake of lutein was associated with higher lutein content in HM (55). In this study, the mean intake of lutein was 4.7 mg/day, with a range from 0.64 to 17.05 mg/day, while the mean lutein concentration in HM was 3.5 μg/dl, with a range from 0.5 to 31.3 μg/dl. Although no intervention studies have been reported so far, observational data suggest that the concentrations of biotin in the HM decreased over the course of lactation despite an intake of 57 mg biotin/d which is 63% higher than the adequate intake of 35 mg biotin/d, suggesting that a low intake of biotin may accelerate the decrease (56). There is strong evidence that retinol or beta carotenoid concentrations in colostrum (1–5 days) or mature (>14 days) HM are increased through supplementation of vitamin A during lactation either as retinyl palmitate (658–7,218 μg per day), as multivitamins containing β-carotenoids (providing 90 mg/d beta carotene) or as part of a diet enriched with vegetable oils like red palm oil (providing 90 mg/d beta carotene), soybean oil or sunflower oil (22). The same is true for a higher vitamin A consumption (range of 50–7,205 μg retinol activity equivalents), which led to higher, but non-significant, retinol concentrations (57). A strong positive association was demonstrated between maternal vitamin D intake during exclusive breastfeeding and infant serum 25-hydroxyvitamin D levels (58), although doses at the current recommended daily intake of vitamin D may not be sufficient for adequate transfer from mother to the breastfed infant (58) and supplementation during lactation with 4,000–6,400 IU/d of vitamin D may be needed to prevent vitamin D deficiency in the mother and her breastfed infant (59). The mode of supplementation needs to be taken into account, as a randomized controlled study demonstrated that a single bolus led to a higher production of vitamin D, compared with a daily dose (60), and levels remained elevated for at least 28 days. Among women with adequate folate status, HM folate secretion was shown to reach a maximum threshold and was not affected by the maternal folate status, except in clinically folate-deficient mothers (46). Maternal supplementation with alpha-tocopherol was shown to increase the vitamin E concentrations in colostrum, although the evidence is limited (61).
Galactagogues
Adequate lactation is fundamental for the (premature) infant's health, hence there is an increasing interest in galactagogues. Galactagogues are substances that have the potential to assist in various stages of milk production, such as initiation, continuation, or augmentation (62). Pharmaceutical agents, such as domperidone, or more recently herbs such as silymarin-phosphatidylserine and galega are widely used (63, 64). Many herbal concoctions have been proposed as galactagogues around the world. However, there is more anecdotal evidence rather than scientific rigor. There is a huge cultural as well as regional aspects on what is considered or promoted as a galactagogues. From many herbal galactagogues, fenugreek has most number of clinical trials reported in the literature and a recent network meta-analysis demonstrated its efficacy against placebo (65). Moreover, a study reported that a herbal tea containing stinging nettle, among other herbs, increased milk production in 36 mothers with premature infants by 80%, a significant increase when compared with the placebo and control group (66). Overall, the quality of galactagogue literature was found to be poor and the field would benefit from well-designed double blinded and randomized controlled studies.
Maternal Anthropometry
Influence of maternal weight/body composition on HM lipids and fatty acid profile
HM of overweight women is reported to contain higher amounts of SFAs, lower amounts of n-3 FAs, a lower ratio of PUFAs to SFAs and a higher ratio of n-6 to n-3 FAs, compared with normal weight women, even after adjusting for maternal diet (68). A study with 80 women reported a significant maternal age and body mass index (BMI) interaction with calorie and fat. BMI alone was significantly associated and protein content (69). Calorie and fat contents were found to be lower in overweight mothers in their 20s but higher in older, overweight mothers. The reason for this unique finding is not fully understood. The overall nutritional status of the mother and the stage of lactation may be important factors that deserve attention while studying the association between maternal BMI and HM macronutrient concentrations. To exemplify this, studies among well-nourished lactating women have failed to demonstrate any association between maternal fat stores and HM lipids (70), while those conducted among marginally nourished populations showed a positive relation both in early (<90 d) and late (≥90 d) lactation (71, 72).
Influence of maternal weight/body composition on volume of HM
Maternal body composition not only influences the composition of HM in terms of its macronutrient composition, but is also associated with the volume of HM transferred to infants when assessed using the “dose to the mother” deuterium dilution method (73). This was shown in infants from Kenya, where HM intake was positively correlated to maternal triceps and mid upper arm circumference during pregnancy (74). In contrast, among low-income Honduran women maternal anthropometric status was not found to be a significant predictor of HM volume or infant energy intake between 4 and 6 months of age after accounting for confounding factors such as birth weight and milk energy density. This highlights the ability of the infant to self-regulate intake in response to milk energy density and infant weight (75). Furthermore, studies reported positive associations between maternal BMI and HM leptin levels (76–79). One study found higher maternal %FM associated with higher leptin but not adiponectin concentrations (80). The same authors hypothesized that HM adiponectin levels are less likely to be impacted by maternal adiposity as the majority of HM adiponectin may be synthesized and controlled by the mammary gland. Others reported positive associations between HM leptin and adiponectin concentrations with infant weight gain (77, 78, 81) as well as HM adiponectin concentrations and fat mass in the infants up to 2 years (82).
Maternal Obstetric History
The influence of parity on HM composition
Parity has been found to be an independent factor influencing proteins and lipids content (83) and FA profile (84). However, findings are not consistent in the literature. Bachour et al. (83) reported an increased lipid concentration of HM associated with higher parity among Lebanese mothers. In contrast, among rural Gambian women, the amount of HM fed to the infant and the proportion of endogenous FAs in HM was markedly lower among those who had borne 10 or more children, implying an impairment of the ability to synthesize HM FAs de novo for high parity women (85). In terms of mineral content, increased amounts of iron were found in multiparous women (86). Islam et al. (87) did not find an association between parity and colostrum Ig concentration (including IgA, IgM, IgG, and peripheral immune cells) among women from Bangladesh, yet another study showed, increased IgA and IgM in colostrum of primiparous compared with multiparous Brazilian women (88). It is further hypothesized that a mother's breastfeeding of higher birth-order infants would be exposed to a wider array of organisms from their other children, and these could affect milk cytokine levels (89).
The influence of mode of delivery
Mode of delivery, including cesarean and vaginal delivery, was shown to affect protein content in colostrum (90), HM choline level (91), HM iodine concentration (92) and IgA concentration (88). Some data also suggested that vaginal delivery is associated with higher protein content in colostrum when compared with cesarean delivery (90). Ozarda et al. (91) found higher levels of choline in HM after cesarean vs. vaginal delivery. Iodine concentration in the transitional milk was found to be higher in women with cesarean section (349.9 μg/kg) in comparison with those with vaginal delivery (237.5 μg/kg, p < 0.001) (92). Higher IgA concentration was found in colostrum of women having undergone cesarean section rather than vaginal delivery, because of the occurrence of labor together with surgical stress (88). However, in a multi-center study, mode of delivery was not found to be a significant factor in IgA concentrations in HM (93). The effect of the mode of delivery on HM IgA concentration is suggested to be confirmed in larger cohorts (89). While we have started to observe the differences in HM composition between groups, further studies should focus on the implications of such differences on the health outcomes of the infants.
Maternal and Socio-Demographic Factors
Maternal age
The potential influence of maternal age on HM composition is still being debated. Early studies indicated that the lactose, fat, total nitrogen, protein nitrogen, non-protein nitrogen, sodium, potassium, calcium, and phosphorous concentrations differed little between adolescent and adult breastfeeding mothers (94). Likewise, maternal age was not related to colostrum Ig concentration (including IgA, IgM, IgG, and peripheral immune cells) (83, 87), milk lipids (83, 95), proteins (83), and copper contents (86). In contrast, Antonakou et al. reported maternal age as an independent factor, demonstrating a strong negative association between maternal age and MUFAs, including oleic acid proportions particular during the first months of lactation (84). Also, Silvestre et al. reported lower zinc contents in HM from older women when compared with HM from younger women (86).
Maternal socioeconomic status
There is no consistent evidence about the influence of maternal socioeconomic status on HM lipid contents. Rocquelin et al. did not find an association between socioeconomic status, e.g., mothers' education/occupation and HM lipid content among Congolese mothers of 5 month old infants (95). Bachour et al. found a notable but not statistically significant association between maternal residential area and milk lipids, proteins and IgA levels (83). In contrast, Al-Tamer and Mahmood demonstrated an effect of maternal socioeconomic status of lactating mothers in Iraq on HM lipid content, TG and FA composition, especially the proportions of long-chain omega-3 FAs decreased with decreasing socioeconomic status (96). Similarly, a study in low-income Indian women demonstrated an association of socioeconomic factors, particularly maternal education, with HM composition in as such that a higher education resulted in lower concentrations of SFAs and PUFAs (97). In Chinese women a higher education was positively associated with concentrations of carotenoids and tocopherol in HM (98).
Geographical location
There is consistent evidence in the literature that HM FA composition varied according to geographical location, and variation was frequently attributed to the differences in maternal diet (129–133). For example, Chulei et al. reported different concentrations of DHA and AA: DHA ratio in HM in five distinct geographical regions (pastoral, rural, urban 1, urban 2, and marine) of People's Republic of China (130). Roy et al. revealed differences in HM n-6 and n-3 PUFAs between urban and suburban mothers in Bengali, India, and contributed the rural and urban differences to the mothers' alimentary habits (134). A study comparing the levels of omega-3 and omega-6 PUFAs in HM of Swedish and Chinese women demonstrated a more favorable balance of those FAs in Swedish women (135). In addition to lipid content, mineral composition of HM, namely phosphorous was found to vary among three different regions among 444 Chinese lactating women (92). Oligosaccharide profiles in colostrum varied between Italian and Burkinabe women, in as such that in contrast to Italian women, the Burkinabe women had higher concentrations of 2 fucosyllactose and lower concentrations of lacto-N-fucopentaose in colostrum (136). The relevance of these findings is not clear. Like FAs, growth factors vary according to geographical location. For example, 228 breastfeeding mothers from 3 regions in People's Republic of China revealed significant differences in the content of epidermal growth factor (EGF) and TGF-α content in HM by region (137). Differences in diet may explain some of the findings as the concentration of EGF in HM significantly decreased with increasing intake of proteins, total energy, vegetables, fruits, soy products and dairy foods, while the TGF-α content in HM significantly increased with increasing intake of carbohydrates and dairy products and decreased with increasing intake of proteins and meat. Overall, we hypothesize that geography is a proxy factor for underlying factors that drives the differences in HM composition. The major factor that remains common to a cohort in geography such as diet or life style are usually the underlying causes of demonstrated differences in HM composition.
The influence of maternal exposure to toxins on levels of toxins in HM
Human milk of mothers with different childhood exposures differs significantly. It might be possible that exposure of the mother during her own infancy primes her intestinal immune cell development in as such that when immune cells migrate from the maternal intestine to the mammary gland, results in altered HM composition. It was reported that women who were breastfed during infancy and grew up on the Baltic coast of Sweden had high levels of polychlorinated biphenyl (PCBs) and polychlorinated dibenzo-p-dioxins (PCDDs)/polychlorinated dibenzo-furans (PCDFs) in HM. Exposure early in life to HM and consumption of contaminated fish from the Baltic sea were the reasons for high toxic level of PCBs and PCDDs in their HM (138). Also, toxic metal contamination in HM is of concern (139). The authors found, for example, arsenic in 64% of HM samples in Lebanese women and identified an association with cereal and fish intake. In general, inter-country studies reported varying levels of perfluorinated carboxylic acids in HM samples from Japanese, Chinese and Korean mothers, with the highest levels in Japanese mothers (140). More specifically, a strong positive association of perfluoroalkyl substances in HM with maternal age, BMI and parity was reported from an analysis of HM from 128 Korean mothers (141). The same authors reported the consumption of snack, milk, and eating-out frequency to be associated with increased levels of perfluoroalkyl substances.
Maternal Medical Conditions
Effects of gestational diabetes mellitus (GDM) on composition of HM
Maternal prenatal metabolic profile influences the composition of HM (99). It was shown that mothers with diabetes experienced lactogenesis II later than healthy mothers (100). A relatively small study showed that levels of ghrelin, an appetite-stimulating hormone, were lower in HM of early lactation of mothers with GDM as compared with mothers without GDM, but that ghrelin levels were restored to normal in mature HM (101). These data need to be confirmed in a larger group of women. Moreover, mothers with a higher pre-pregnancy BMI combined with GDM or lower insulin sensitivity had higher insulin concentrations in mature HM compared with normal glycaemic mothers (102). Galipeau et al. found that the presence of gestational diabetes increased the risk of an elevated HM sodium level at 48 h after delivery (127). However, Klein et al. did not find any significant differences in HM free AAs content between GDM and healthy women, regardless of it being colostrum or mature HM (103).
Influence of celiac disease on composition of HM
In comparison to healthy mothers, HM of mothers with celiac disease was found to have a reduced abundance of immune protective compounds (TGF-β1 and sIgA) and bifidobacteria (104). On the other hand, HM of 42 mothers with celiac disease who followed a gluten-free diet showed no difference in anti-gliadin antibodies compared with HM from 41 mothers with a normal, gluten-containing diet (105). This suggests that rather than diet, the immunological memory defines the presence of these antibodies in HM.
Influence of maternal atopy/allergy on composition of HM
The association between maternal atopy/allergy and HM composition is not consistent in the literature. Higher IL-4, IL-5, IL-13 (106), and beta-casomorphin-5 (107) in colostrum, and higher levels of IL-4 (108), lower levels of TGF-β1 (109, 110), TGF-β2 (111), IL-10 (108) and proteome (including protease inhibitors and apolipoproteins) (112) in HM were found in women with history of allergic disease compared with non-allergic women. Higher levels of sCD14 were found in mothers with a positive vs. negative allergic history (113). On the contrary, Marek et al. (109) did not find any difference in IL-4 and IL-10 levels in HM between allergic and non-allergic mothers. Likewise, no differences were reported in pro-inflammatory markers and cytokine concentrations (111, 114, 115) and FA composition (111) in HM between allergic and non-allergic mothers. A study among Danish mothers with atopic dermatitis, mothers with other types of atopy, and non-atopic mothers reported that the HM FA composition was not affected (116). In contrast, women with a combination of eczema and respiratory allergy had lower HM levels of several PUFAs (AA, EPA, DHA, and DPA), and had a lower ratio of long-chain n-3 PUFAs/n-6 PUFAs, even though the fish consumption was not different between groups (117). Their PUFA levels differed not only from that of healthy women, but also from that of women with only respiratory allergy, who had a FA pattern like that of healthy women.
Mastitis
Early evidence indicated that HM of mothers with mastitis showed a higher content of minerals, chlorides, and catalase activity, and lower levels of lactose, fat, total proteins, and total casein fractions, in comparison with HM from healthy women (118). This observation is likely because mastitis inflammation can produce pro-inflammatory cytokines and damage the milk fat globule (MFG). Mizuno et al. found that HM of mothers with mastitis contained larger MFG and higher IL-6 levels in the diseased breast than HM from the healthy breast (119). The same authors reported that this difference was larger if accompanied by systemic symptoms of mastitis (fever/malaise). In a separate study, Buescher and Hair reported that HM of mothers with mastitis had the same anti-inflammatory components and characteristics of HM from healthy mothers; although elevation in selected components/activities was observed (TNFα, soluble TNF receptor II, and IL-1RA and bioactivities that cause shedding of soluble TNF receptor I from human polymorphonuclear neutrophils) (120). These components may help protect the nursing infant from developing clinical illness due to intake of HM from mothers with mastitis.
Post-partum depression
About 85% of women experience a so called “post-partum blues,” which is transitional and lasts ~2–3 weeks after birth (121). The “blues” does not resolve in some women, and about 10–20% of new mothers experience post-partum depression (122). Post-partum depression is frequently found to be related with a shorter breastfeeding duration (123, 124). Currently, there are no randomized controlled trials to demonstrated causality. A population-based prospective cohort study showed that maternal depression was associated with maternal perceptions of insufficiency of HM but not actual milk quantity (125). This finding was supported in lactating mothers of preterm and term infants, where the perceived mood states had no apparent effect on HM volume (126).
Other Maternal Factors Influencing HM Composition and Volume
For the sake of greater focus on the most relevant factors influencing HM composition and volume, this chapter lists but not discuss in detail other topics that could be considered for planning and conducting research in this area but are not discussed in detail. Instead, further reading is proposed (see Table 2). Indeed, many factors have significant impact on human milk composition, however, how those differential composition impacts infant outcomes should be a topic of future studies.
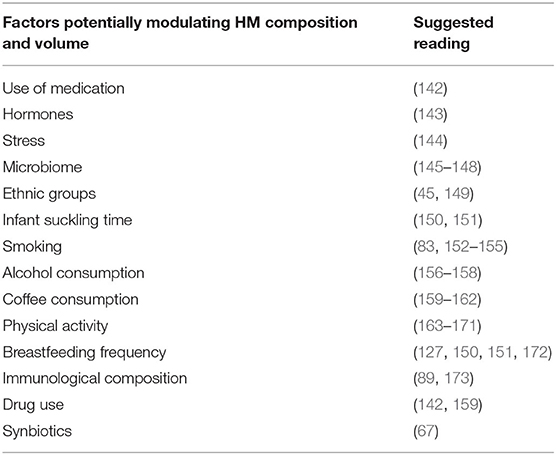
Table 2. Further reading for factors with potential impact on human milk.
Infant-Related Factors Affecting HM Volume and Composition
The main factors have been summarized in Table 3.
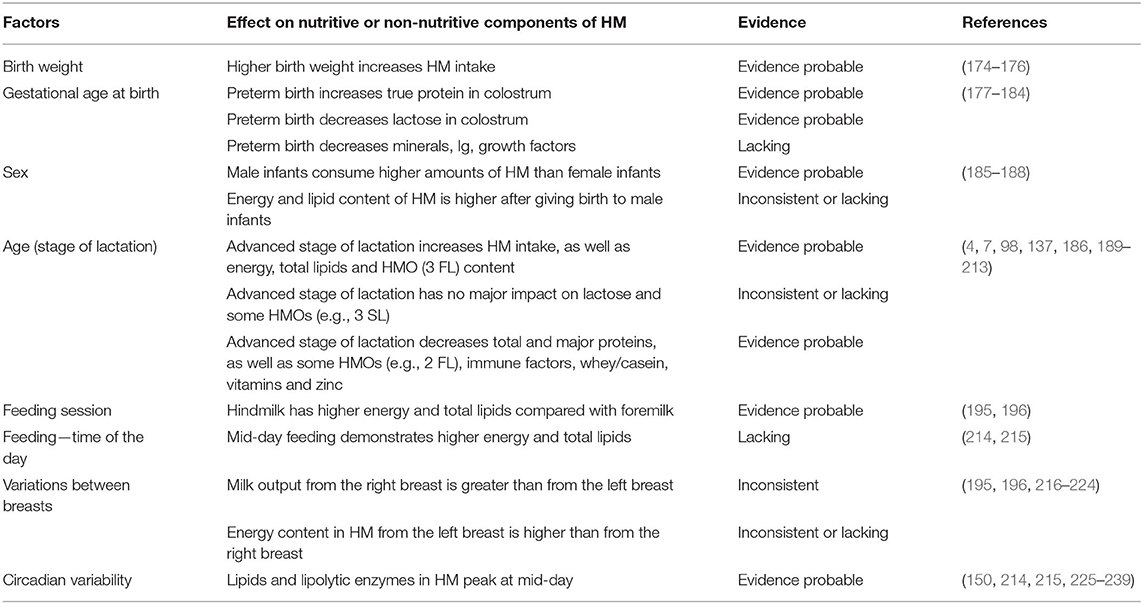
Table 3. Infant-related factors affecting nutritive and non-nutritive components of human milk.
Infant Birth Weight
A positive relationship has been suggested between birth weight and HM intake attributed mainly to increased sucking strength, frequency or feeding duration (70). In the DARLING study, weight at 3 months and total time nursing were positively associated with HM intake at 3 months, while no maternal variable (such as age, parity or anthropometric indices) was significantly correlated with intake, volume extracted, or residual milk volume, indicating that infant demand was the main determinant of lactation performance (174). In contrast, no differences were observed in absolute and relative HM transfer volumes and HM zinc concentrations of small for gestational age vs. appropriate for gestational age infants born to low-income, marginally nourished Bangladeshi mothers (175).
Infant Gestational Age at Birth and Term vs. Preterm Delivery
A meta-analysis of 41 studies indicated significantly higher concentrations of “true protein,” excluding the non-protein nitrogen, in the first few days post-partum. Lower lactose concentrations (in the first 3 days and some later time points) were found in preterm compared with term HM, although no differences were observed for fat and energy content (177). Compared with term HM, preterm HM was shown to have a highly variable human milk oligosaccharides (HMO) content and was richer in glycosaminoglycans. The latter allows HMOs to competitively bind to pathogens and prevent them from adhering to the enterocytes (178). With respect to mineral content, preterm compared with term HM is reported to have higher concentrations of copper and zinc that decline across lactation and lower concentrations of calcium that remains constant over lactation (178). HM from preterm mothers was shown to have higher levels of IgA, IL-6, EGF, TGF-β1, and TGF-β2 in colostrum compared with term HM (179). Ozgurtas et al. found higher levels of vascular endothelial growth factor, basic fibroblast growth factor (b-FGF) and insulin-like growth factor-1 (IGF-1) in HM from the mothers of preterm infants (180). Similarly, preterm delivery also affects hormone concentrations in HM. In a study with 40 lean mothers, those of the preterm infants showed higher concentrations of obestatin and higher expressions of ghrelin mRNA in mammary epithelial cells, however the latter did not result in higher ghrelin concentration in HM (181). It may be speculated that the synthesis of these peptides and their transport from maternal circulation could contribute to the finding that the transcript level of the gene does not correspond to the peptide level in HM. While the HM of mothers of preterm babies seemed to have a higher concentration of immunological markers, there is conflicting evidence on the ability of gestation age to influence HM PUFA composition. One study showed lower levels of EPA and DHA in HM from mothers of preterm infants (182), while others did not find any association (183). Limited data showed that gestation age may influence HM minerals composition. For example, Ustundag et al. reported lower zinc levels in HM from mothers of premature infants with a similar trend seen in colostrum copper levels (184).
Sex of the Infant
The sex of the infant may also be one of the determinants of HM volume and composition of HM, for example, the HM of mothers with male infants had 25% greater milk energy content than mothers delivering female infants (185). Furthermore, at 4 months of age, HM for male infants compared with females were higher in energy and lipid content by 24 and 39%, respectively (186). The same study revealed lipids such as linoleic acid, phospholipids and gangliosides were increased in HM of male infants in later lactation, potentially based on the higher energy requirement of a male infant (186). Interestingly, in resource poor setting, HM for female infants was richer in lipids, while in a resource sufficient setting, the milk for male infants was richer suggesting that infant sex and maternal socioeconomic status showed an interaction and should be studied further (187). HM intake, assessed using stable isotope methodology, was shown to be higher in males than in females over the first 12 months of lactation, likely related to the fact that males have greater lean mass than females during infancy (188).
Temporal Changes in HM Volume and Composition
Changes in HM Volume Across Lactation
HM is a dynamic fluid that changes its composition and volume depending on the stage of lactation and adapts to the evolving nutritional requirements of the infant (4, 189–192). Stable isotope studies in infants aged 0–24 months have shown that the volume of HM intake increased over the first 3–4 months and remained above 0.80 kg/d until 6–7 months in order to meet the increasing energy requirements of the infant (188).
Branched-chain FAs may reduce the incidence of necrotizing enterocolitis, but evidence is limited. One study found branched-chain FAs decreased with increased lactation (193). Most growth factors (EGF, IGF, and TGF) significantly decrease over the course of lactation from colostrum, over transitional and mature milk, while TGF-α content in HM revealed a significantly increased trend over the course of lactation (137). The time of lactation had an influence on the concentration of oligosaccharides, on 4 out of 22 oligosaccharides measured. (194). However, published data are hampered by large variation and results need to be interpreted with caution.
Changes Observed Within Feed and Between Breasts
The energy content of HM is not constant and changes within a feeding (195). Significantly higher energy content has been observed in hind milk than in foremilk since the lipid content increases markedly with emptying of the breast. The fat content of hind milk is reported to being approximately two- to three-fold that of foremilk and included 25–35 kcal/100 mL more energy on average than foremilk (195). Milk volume differences between left and right breasts have also been a topic of study. Reports indicated that milk output from the right breast was usually greater than the left breast (216–219, 240). However, the opposite has also been reported where the left breast showed a greater milk output in pump-dependent mothers of non-nursing preterm infants (220). Perhaps studying physiological implications of left cradling bias that occurs in 70–85% of the women may help shed light on the observed between breast variability (221). When milk composition from the left and right breasts was assessed over 12 months in fore and hind milk the content of fat was found to vary slightly between breasts, with a mean CV of 47.6 (SE 2.1) % (n 76) and 46.7 (SE 1.7) % (n 76) for left and right breasts (196). These variations resulted in differences in the amount of fat delivered to the infant over 24 h. This indicated that a rigorous sampling routine should take into account all levels of variation in order to accurately determine infant HM intake (196). Different levels of sodium, chloride, glucose, lipid, and zinc were reported in the HM of breasts but differences were either transient and/or random (222). In a different study the levels of sodium, the levels have shown a difference, potentially due to underlying mastitis localized to only one breast (223).
Changes Due to Circadian Variability
Diurnal variation in the lipid content of HM was first studied more than a century ago (225). Later it was shown that diurnal variations were unrelated to the degree of emptying of the breast in the previous feeding and to maternal meal times (226). Since then it has been a topic of interest for many teams of scientists in normal term (150, 227–229, 241) as well as preterm infants (230). It is noteworthy that not only lipids in HM but lipolytic enzymes of HM show a circadian rhythm and peak at mid-day, which has been shown for serum-stimulated lipase and lipoprotein lipase but not bile salt-stimulated lipase (214, 215). In a study with 6 women, HM volume, along with total lipids were found to be significantly higher between 08:00–12:00 and 16:00–20:00 (231). The same team suggested that if 24-h sampling was not possible, single samplings at 12h00, 20h00, and 24h00 may be most representative for lipid yield and may predict the value within 97–124%. Since lipids provide more than 50% of total energy in HM, it is not surprising that energy content of HM was positively related to fat content (232). Though lipids have been studied the most, milk minerals also have received some attention. However, the evidence was not very conclusive and did not demonstrate a cyclic change at a different stage of lactation (233–237). Endocrine factors and melatonin are hypothesized to improve nocturnal sleep and reduce infantile colic (238). Indeed, it has been shown that melatonin is found at significantly higher concentrations in night time HM (7.3 pg/mL) as opposed to day time HM (1.5 pg/mL) (239).
Longitudinal Changes Across Lactation
Among all the factors covered in this paper, longitudinal changes observed across progressing stages of lactation have been studied the most. Key differences include the presence of a relatively high abundance of immune related factors in early compared with later stages of lactation (7). Additionally, a higher concentration of total proteins has been observed in colostrum and transitional compared with mature milk (190). In contrast, lipids are present at higher concentration in mature milk (186, 196). In next section we review the different aspects of changes across lactation as reported in the literature.
Changes in the macronutrient composition of HM
The energy content of HM showed an initial decrease followed by an increase over the course of lactation, which was directly related to the HM lipid content (186, 196). With respect to carbohydrates, several studies showed that lactose concentrations remained constant throughout lactation (186, 195, 197), however, there is also some evidence to the contrary, indicating an increase in HM lactose from 56 to 69 g/l over the first 4 months of lactation (198). The other significant carbohydrates found in HM are oligosaccharides, the concentrations of most of which, not all, have been shown to decline during the course of lactation although HM concentrations of 3-FL either increased throughout lactation or remained at relatively constant concentrations starting at 1 month onwards (199, 200). The colostrum to milk transition was also associated with significant changes in concentrations of free sugars and polyols (increased in concentrations of lactose and glucose, decreased in concentrations of Myo-inositol and glycerol) over the first 3 days after birth and thereafter reaching a steady state (201).
Colostrum contains very high concentrations of protein (ranging from 20 to 30 g/L), which decreases significantly thereafter, and reaches 7–8 g/L after 6 months of breastfeeding (202). This observation coincides with lower protein intake and lower growth rate of breastfed infants in the latter half of the first year of lactation (203). A systematic review reported on the reduction in HM protein concentration (g/L) from about 25 in colostrum (age 1–5 days) to 17 in transitional milk (age 6–14 days) and then to 13 (8–21) in mature milk (at age of >14 days and <6 weeks) (204). The protein profile of the HM also evolves over lactation. At the beginning of lactation the whey: casein ratio was around 90:10, reduced to 70:30 in transition milk, then to 60:40 in mature milk and ultimately reached 50:50 ratio in mature milk after 6 months of lactation (205, 206). The concentration of lactoferrin in HM (second most abundant whey protein in HM known for its antimicrobial activities) was high during early lactation (<28 days lactation), decreased by almost 50% in the first 5 days of lactation, and thereafter remained relatively stable (207). The total nitrogen and total AAs in HM decreased in the first 2months of lactation and thereafter remained relatively unchanged, while the free AAs (glutamic acid and glutamine) increased over lactation, peaked around 3–6 months, and thereafter decreased (208).
The most variable macronutrient in the HM is fat, which is dependent on a number of factors and includes the fat content of colostrum; it is usually very low (1–2%) but was shown to increase rapidly during the first week of lactation (204). The mean lipid content of HM (g/L) increased from 22 in colostrum (age 1–5 days), to 30 in transitional milk (age 6–14 days), and 38 in mature milk (age >14 days and <6 weeks) (204). There were also stage-based changes reported in the ganglioside content of HM with some decreasing and others increasing over the time (209).
Changes in micronutrient composition of HM
The concentrations of antioxidant vitamins such as A and E are known to be lower in mature milk compared with colostrum and decrease over the course of lactation, while the total antioxidant status of mature milk was higher than colostrum indicating an increase in total antioxidant properties (210). Non-provitamin A carotenoids (lutein and lycopene) decreased while there was no significant change in the provitamin A carotenoids (α- and β-cryptoxanthin) with advancing lactation stage (211). Over the course of lactation (up to 240 days) significant changes of carotenoids and tocopherol were reported in a population of 540 Chinese women (98). In this population, the concentrations of lutein, zeaxanthin, and α-tocopherol were higher the first 4 days, decreased until 12 days post-partum to remain stable afterwards. Zeaxanthin and γ-tocopherol remained stable over time.
Zinc concentrations in HM decline dramatically over the first 3–5 months of lactation and even an increase in HM volume during the early weeks post-partum is not sufficient to overcome this decline (212). A marked decrease in HM cobalamin was also observed at 4 months and this has been associated with an accompanying decrease in plasma cobalamin and holotranscobalamin in infants, indicating an impaired cobalamin status (213).
Methodological Factors Affecting the Quantification of HM Components in a Research Setting
The main factors identified have been summarized in Table 4.
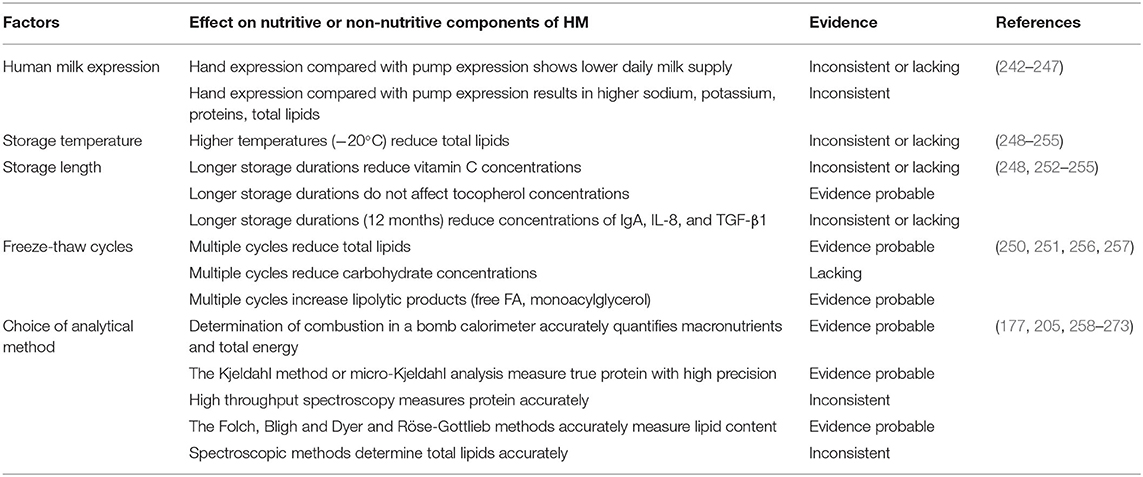
Table 4. Methodological factors affecting nutritive and non-nutritive components of human milk.
Sample Collection—Hand Expression vs. Electric Pump Expression
It is well-known that there are multiple ways of expressing milk from mothers' breasts, be it for feeding to the new-born, for donation or for research purposes. The methods may include but are not limited to, hand expression, manual pump and electric pump (242). In a randomized trial of mothers delivering very low birth weight infants, hand expression produced significantly lower cumulative daily milk volume in comparison with electric pump expression (243). Sodium concentration was shown to be significantly affected by method of pumping. Higher sodium content was found in hand expressed milk as opposed to electric pump-expressed milk (244). In a Cochrane review of methods for HM expression, sodium, potassium, protein, and fat constituents of HM were reported to differ between methods. However, no consistent effect was found related to prolactin change or effect on oxytocin release with pump type or method (242). A randomized trial indicated that HM expressed manually contained higher fat than that expressed electrically (245). Morton et al. (246) indicated that a combination of manual technique and electric pumping resulted in high levels of fat-rich, calorie-dense milk, unrelated to production differences. An experiment from 57 lactating women showed that macronutrient content (fat, carbohydrate, protein, and energy contents) of mid expression HM is unaffected by maternal handedness, breast size or breast side dominance (247, 274).
Post-collection Handling of HM Samples
Utmost care must be observed with HM samples immediately after the milk is expressed from the mothers' breast into the collection container. Collection tubes may need to be acid washed prior to collection if the intention is to measure minerals. Similarly, maintenance of a cold chain until laboratory analyses, ensuring optimal storage temperature and duration, limiting freeze-thaw cycles, amount of oxygen exposures etc. comes into the scope of post-collection handling variability. It is our general observation that not many systematic studies exist that assess and guide the future HM research scientist, but few observational as well as data supported statements are mentioned in this section.
Storage temper and duration
Lipids, more than carbohydrates or proteins in HM, are sensitive to storage over long periods. Chang and colleagues demonstrated that even storage at −20°C for 2 days leads to ~9% reduction in HM total lipid content (248). It is likely that bile salt-stimulated lipases present in HM may still maintain some activity at cooler temperatures and lead to enzymatic hydrolysis of lipids (249). Indeed this was confirmed in a separate study where storage at −20°C was also done with pre-heating milk samples at 80°C (90 sec) to destabilize the lipolytic enzyme (250). Therefore, if possible, samples should be stored at the minimum possible temperature, preferably at −80°C, from the day of collection. However, others have argued that freezing at −80°C reduced the energy content of both fat and carbohydrates and suggested HM should be stored at −20°C (251). Furthermore, even vitamin C was reduced significantly over time in cold storage but not tocopherols and total FAs (252, 253). Bacterial composition (quantitative or qualitative) of HM was stable with cold storage at −20°C for 6 weeks (254). Long-term storage of HM may affect immunological composition. According to Ramirez-Santana et al. freezing storage of colostrum at −20 and −80°C for a 12-month period produced a decrease in the concentrations of IgA, IL-8, and TGF-β1 (255).
Freeze-thaw cycles
Freeze (−20°C) and thaw (5°C) cycles have been shown to activate lipolysis and increase the presence of lipolytic product in HM, such as free FAs, monoacylglycerols and diacylglycerols (250, 256). Structural effects such as increasing size of milk fat globules due to freezing have also been observed (257). Carbohydrate content was significantly reduced in thawed HM samples when compared with fresh samples (251).
Analytical Procedures
The choice of analytical methods to measure the nutrient of interest in HM is important, especially in comparative and longitudinal studies, where differences among populations and lactation stages could be due to biological variation or may reflect methodological biases and errors. Several factors influence the analysis of HM and in the following paragraph, we will discuss the most relevant ones. This is not intended to be a review on methodologies for determination of nutrients in HM, but to demonstrate the consequence of using unsuitable methodologies.
Sample preparation
Using the correct preparation and storage of samples are important elements of maintaining the integrity of HM during storage, as previously mentioned. In our experience, maintaining sample homogeneity is an issue both when frozen samples are thawed at room temperature or in a 37°C water bath. Often, probe sonication should be used if the measure is based on optical analyses, such as the commonly used mid infrared spectroscopy. HM must be immersed in warm water (30–40°C) and gently mixed, prior to analysis, in order to rapidly thaw and minimize phase separation. Homogenization is an important step in preparing milk samples for total fat determination by infrared (IR) spectroscopy techniques, as it decreases the variability in fat globule size and the light-scattering effect of larger globules, improving the accuracy of the measurement (258).
Selectivity/Specificity and accuracy
When quantitative data are required, the analytical methods chosen must demonstrate enough selectivity and accuracy. Selectivity is the ability of the method to distinguish between the analyte and other substances present in the matrix. In absence of selectivity, accurate values cannot be obtained. The accuracy expresses the closeness of a result to an accepted reference value and it is normally studied as two components: trueness, which represents the closeness of agreement between the average value obtained from a series of results and a reference value and precision, which is the closeness of agreement between independent test results obtained under stipulated conditions (ISO 5725) (259). In the following paragraphs, several methodologies are discussed with respect to selectivity and accuracy.
Energy
Two approaches have been used to measure energy in HM: direct energy quantification by combusting in a bomb calorimeter and calculated energy using Nichols et al. (260) energy multiplication factors for protein, fat and carbohydrate. Lack of accuracy has been shown by Gidrewicz et al. (177) for the measurement of energy when calculated using values for the energy contributions from fat, protein and carbohydrate rather when measured by bomb calorimetry. Differences as high as 13%, which likely represent clinically important differences, were reported (177). Since HM contains a large amount (~12%) of non-digestible oligosaccharides, they will contribute a significant amount of energy when using bomb calorimetry for energy measurement, but since they are essentially non-digestible, they should contribute significantly less energy to the infant. Overall, the choice of analytical methods can determine outcome and interpretation of HM analyses. Therefore, adoption of standard methods when possible and/or rigorous assessment of alternative methods is needed. To assure equivalence of two analytical methods, we recommend evaluating the accuracy of the alternative method and to check the presence of systematic and/or proportional bias by performing analysis of differences and a regression analysis, respectively.
Proteins
Amino acid analysis is the most accurate method for determining true protein content (205). The Kjeldahl method, based on complete combustion of the sample, measures total nitrogen (TN) and it is the most accurate indirect determination of total protein content in HM (261). The true protein content can also be estimated by the chemical determination of non-protein nitrogen (NPN) (262), and subsequent subtraction from TN. Unfortunately, AA analysis is costly and time consuming and the Kjeldahl method requires large amounts of sample. Alternatively micro-Kjeldahl (263) analyses can be used with high precision to determine true protein because it has been shown to correlate well with AA analysis (264) if corrections are made for NPN. High throughput approaches requiring low sample amounts such as spectroscopy and colorimetric methods have been investigated (258, 262, 265–268). Absence of accuracy was shown (258, 266) when comparing near- and mid IR spectroscopy equipment for determination of total protein against chemical reference methods. Casadio et al. (265) compared Miris HMA vs. Bradford for total protein determination and reported overestimation of protein content. On the other hand, Silvestre et al. (267) reported underestimation of protein content when Miris HM analysis was compared vs. Bradford for total protein determination. This observation illustrates that spectroscopy methods can vary in accuracy depending on the calibration of the instrument and reference method; hence the appropriate methods should be selected with care. Keller and Neville (262) compared micro-Kjeldahl to different spectrophotometric methods to determine proteins in HM: Biuret assay, Lowry-Peterson assay, Bio-Rad Coomassie Blue assay and Pierce Bicinchoninic acid assay (BCA). The Pierce BCA assay demonstrated better accuracy, and was recommended for total protein analysis in HM. Lonnerdal et al. (268) showed the BCA method consistently overestimated Kjeldahl protein by 30%. However, parameters such as incubation time and temperature highly influenced the accuracy of the BCA method (269).
Lipid
In order to accurately quantify HM lipid, the first step is disruption of the biological membrane enveloping triacylglycerol core, e.g., ultrasound treatment, followed by lipid separation from milk protein by the addition of organic solvent [e.g., methanol (270, 271)] or acids or bases [NH3 (272)] which triggers protein precipitation. At this point, lipid can be extracted from the matrix by using organic solvents. Since most of the lipid in HM is represented by triacylglycerol (98%), solvents like diethyl ether and petroleum benzene (272) can be used. Lipid extraction methods are time consuming and other approaches like Gerber, creamatocrit, and spectroscopy have been applied for the quantification of lipid in HM. The Gerber method is based on protein precipitation and further separation of fat by centrifugation. A collaborative study (273) performed on crude and homogenized pasteurized cow milk showed that the Gerber method underestimated the amount of fat by 0.02–0.06% compared with the official method of Röse-Gottlieb. A critical point of the method is the accuracy of butyrometers. The supplier should calibrate the butyrometer at delivery and supply a test certificate. The internal surface of the butyrometers must be smooth and free of defects. Recently, spectroscopy techniques have been employed to measure total lipid in HM, and showed conflicting results on precision and accuracy of these techniques (258, 265, 266). The reasons were mainly due to selection of chemical reference methods for the comparison and calibration of spectroscopy instruments. Therefore, the Folch, Bligh, and Dyer and Röse-Gottlieb extraction methods are highly recommended to perform absolute quantification of lipid in human milk (261) and they have to be used for calibrating near- and mid IR spectroscopy equipment.
Lactose
Indirect methods, such as colorimetric methods can show poor selectivity. Casadio et al. (265) reported the lack of selectivity of the enzymatic essay to measure lactose in HM, due to lactose overestimation when compared with HPLC measurements. Attempts have been made to quantify lactose by near- and mid IR spectroscopy (258), however neither of the approaches were accurate or precise (261, 266).
Below the main considerations, for successful HM collections and analyses in observational as well as interventional studies, are summarized (see Table 5).
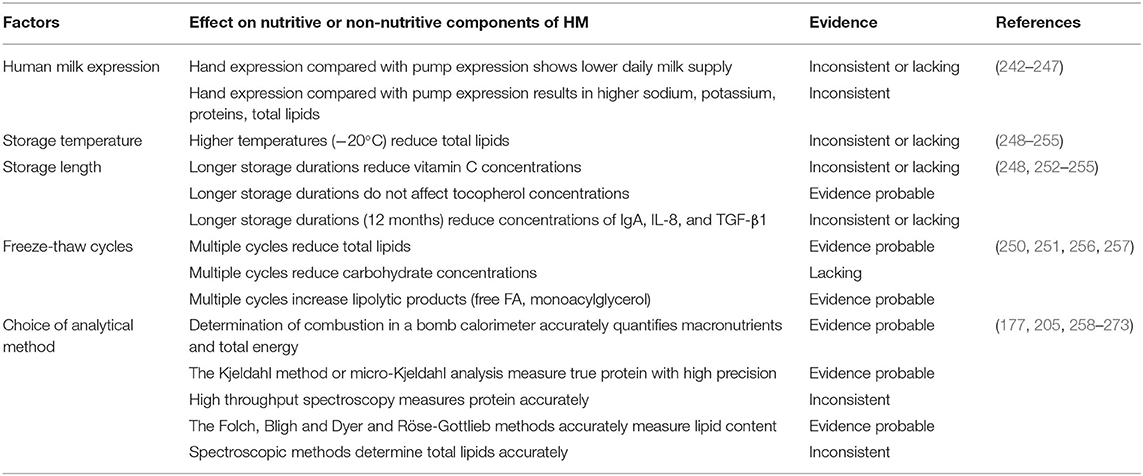
Table 5. Recommendations for collecting and handling of HM samples.
Conclusions and Further Recommendations
To our knowledge, this is the first comprehensive literature review that provides a holistic overview of a broad range of factors affecting HM composition and volume. Several maternal and infant characteristics as well as study methodological aspects were found to impact HM composition and volume. Study procedures should be systematically recorded and/or standardized in individual studies, whenever possible, to facilitate appropriate analysis, and interpretation of data and comparisons across studies. HM lipids and lipophiles were the nutrients found to be most vulnerable to maternal, infant and methodological factors. We therefore recommend standardizing the sampling of the HM, especially for characterization of lipids, lipophiles, and for those nutrients whose variability is yet unknown. Keen attention should be given to the choice of the analytical method to characterize and quantify nutrients in HM, with respect to their selectivity, accuracy and precision.
Our review not only summarizes recommendations for standardization of HM sampling and handling for future research protocols, but also sheds light on the dynamic and highly variable nature of HM. This knowledge is crucial to better understand the controversial impact HM may have on developmental outcomes of infant early life. We also illustrate the agility of HM to adapt to changes in the environment of the mother and evolving nutritional requirements of the infant. There is an apparent need of systematic reviews of existing evidence in the field. It is particularly crucial to better understand those maternal dietary, lifestyle, and environmental exposures that can be modified to significantly impact HM composition and thereby positively impact infants' developmental and health outcomes.
Author Contributions
ST conceived the idea of the review paper. TS, QZ, FG, and ST wrote sections of the manuscript with critical inputs from DM and VV. All authors read and approved the final version of the manuscript.
Funding
This work was supported by Nestlé Research, Switzerland.
Conflict of Interest
TS, FG, and ST are employed by Nestlé Research. QZ was an employee of Nestlé Research when this work was undertaken, and is currently employed by School of Public Health, Peking University, Beijing, the People's Republic of China. DM has received consultancy payment from Dairy Goat Co-operative (NZ) Ltd. and has given paid lectures for the Merck Sharp & Dohme and Bayer. VV has received funding from Nestlé Research to contribute to the writing of this review while she was employed by INSERM, France.
Acknowledgments
We are thankful to Dr. Frank Thielecke who provided scientific expertise and editing.
Abbreviations
HM, human milk; PUFA, polyunsaturated fatty acid; LA, linoleic acid; ALA, alpha-linolenic acid; DHA, docosahexaenoic acid; FA, fatty acid; AA, arachidonic acid; EPA, eicosapentaenoic acid; DPA, docosapentaenoic acid; GPC, glycerylphosphorylcholine; TMAO, trimethylamine N-Oxide; BMI, body mass index; Ig, immunoglobulin; EGF, epidermal growth factor; PCBs, polychlorinated biphenyl; PCDDs, polychlorinated dibenzo-p-dioxins; PCDFs, polychlorinated dibenzo-furans; GDM, gestational diabetes mellitus; IL, interleukin; MFG, milk fat globule; HMO, human milk oligosaccharides; b-FGF, fibroblast growth factor; IGF-1, insulin-like growth factor-1; TN, total nitrogen; NPN, non-protein nitrogen; HMA, human milk analyser.
Footnotes
1. ^2 FL, 2′-fucosyllactose; i, 3′-Fucosyllactose; 3 SL, 3′sialyllactose; AA, Amino acid; BCA, bicinchoninic acid assay; EGF, epidermal growth factor; FM, fat mass; b-FGF, fibroblast growth factor; GDM, gestational diabetes mellitus; GPC, glycerylphosphorylcholine; HM, human milk; HMO, human milk oligosaccharides; IR, infrared; IGF-1, insulin-like growth factor-1; MFG, milk fat globule; NPN, non-protein nitrogen; PCBs, polychlorinated biphenyl; PCDFs, polychlorinated dibenzo-furans; PCDDs, polychlorinated dibenzo-p-dioxins; TN, total nitrogen; TMAO, trimethylamine N-oxide.
References
1. Hellmuth C, Uhl O, Demmelmair H, Grunewald M, Auricchio R, Castillejo G, et al. The impact of human breast milk components on the infant metabolism. PLoS ONE. (2018) 13:e0197713. doi: 10.1371/journal.pone.0197713
2. Hollis BW, Wagner CL, Howard CR, Ebeling M, Shary JR, Smith PG, et al. Maternal versus infant Vitamin D supplementation during lactation: a randomized controlled trial. Pediatrics. (2015) 136:625–34. doi: 10.1542/peds.2015-1669
3. Hurley WL, Theil PK. Perspectives on immunoglobulins in colostrum and milk. Nutrients. (2011) 3:442–74. doi: 10.3390/nu3040442
4. Lind MV, Larnkjaer A, Molgaard C, Michaelsen KF. Breastfeeding, breast milk composition, and growth outcomes. Nestle Nutr Inst Workshop Ser. (2018) 89:63–77. doi: 10.1159/000486493
5. Patel N, Dalrymple KV, Briley AL, Pasupathy D, Seed PT, Flynn AC, et al. Mode of infant feeding, eating behaviour and anthropometry in infants at 6-months of age born to obese women - a secondary analysis of the UPBEAT trial. BMC Pregnancy Childbirth. (2018) 18:355. doi: 10.1186/s12884-018-1995-7
6. Victora CG, Bahl R, Barros AJD, França GVA, Horton S, Krasevec J, et al. Breastfeeding in the 21st century: epidemiology, mechanisms, lifelong effect. Lancet. (2016) 387:475–90. doi: 10.1016/S0140-6736(15)01024-7
7. Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am. (2013) 60:49–74. doi: 10.1016/j.pcl.2012.10.002
8. Turfkruyer M, Verhasselt V. Breast milk and its impact on maturation of the neonatal immune system. Curr Opin Infect Dis. (2015) 28:199–206. doi: 10.1097/QCO.0000000000000165
9. Dror DK, Allen LH. Overview of nutrients in human milk. Adv Nutr. (2018) 9:278S−94S. doi: 10.1093/advances/nmy022
10. Keikha M, Bahreynian M, Saleki M, Kelishadi R. Macro- and micronutrients of human milk composition: are they related to maternal diet? A comprehensive systematic review. Breastfeed Med. (2017) 12:517–27. doi: 10.1089/bfm.2017.0048
11. Prentice AM, Whitehead RG, Roberts SB, Paul AA, Watkinson M, Prentice A, et al. Dietary supplementation of Gambian nursing mothers and lactational performance. Lancet. (1980) 2:886–8. doi: 10.1016/S0140-6736(80)92048-6
12. McCrory MA, Nommsen-Rivers LA, Mole PA, Lonnerdal B, Dewey KG. Randomized trial of the short-term effects of dieting compared with dieting plus aerobic exercise on lactation performance. Am J Clin Nutr. (1999) 69:959–67. doi: 10.1093/ajcn/69.5.959
13. Neville MC, Sawicki VS, Hay WW Jr. Effects of fasting, elevated plasma glucose and plasma insulin concentrations on milk secretion in women. J Endocrinol. (1993) 139:165–73. doi: 10.1677/joe.0.1390165
14. Okamura T, Takeuchi T, Nishii O, Yaginuma T, Kawana T. Effects of low-caloric diet in puerperium on prolactin, TSH estradiol and milk secretion. Nihon Sanka Fujinka Gakkai Zasshi. (1987) 39:2059–65.
15. Motil KJ, Montandon CM, Hachey DL, Boutton TW, Klein PD, Garza C. Relationships among lactation performance, maternal diet, and body protein metabolism in humans. Eur J Clin Nutr. (1989) 43:681–91.
16. Mohammad MA, Sunehag AL, Haymond MW. Effect of dietary macronutrient composition under moderate hypocaloric intake on maternal adaptation during lactation. Am J Clin Nutr. (2009) 89:1821–7. doi: 10.3945/ajcn.2008.26877
17. Nommsen LA, Lovelady CA, Heinig MJ, Lonnerdal B, Dewey KG. Determinants of energy, protein, lipid, and lactose concentrations in human milk during the first 12 mo of lactation: the DARLING study. Am J Clin Nutr. (1991) 53:457–65. doi: 10.1093/ajcn/53.2.457
18. Nikniaz L Jr, Mahdavi R, Arefhoesseini SR, Sowti Khiabani M. Association between fat content of breast milk and maternal nutritional status and infants' weight in Tabriz, Iran. Malays J Nutr. (2009) 15:37–44.
19. Huynh DTT, Tran NT, Nguyen LT, Berde Y, Low YL. Impact of maternal nutritional supplementation in conjunction with a breastfeeding support program on breastfeeding performance, birth, and growth outcomes in a Vietnamese population. J Matern Fetal Neonatal Med. (2018) 31:1586–94. doi: 10.1080/14767058.2017.1320984
20. Demmelmair H, Koletzko B. Lipids in human milk. Best Pract Res Clin Endocrinol Metab. (2018) 32:57–68. doi: 10.1016/j.beem.2017.11.002
21. Innis SM. Impact of maternal diet on human milk composition and neurological development of infants. Am J Clin Nutr. (2014). 99:734–41S. doi: 10.3945/ajcn.113.072595
22. Voortman T, Garcia AH, Braun KVE, Thakkar SK, Tielemans MJ, Stroobant W, et al. Effects of Maternal Nutrition on Quantity and Nutritional Quality of Breast Milk: Systematic Review, in WCPGHAN. Montreal, QC (2016).
23. Barrera C, Valenzuela R, Chamorro R, Bascunan K, Sandoval J, Sabag N, et al. The impact of maternal diet during pregnancy and lactation on the fatty acid composition of erythrocytes and breast milk of chilean women. Nutrients. (2018) 10:839. doi: 10.3390/nu10070839
24. Urwin HJ, Miles EA, Noakes PS, Kremmyda LS, Vlachava M, Diaper ND, et al. Salmon consumption during pregnancy alters fatty acid composition and secretory IgA concentration in human breast milk. J Nutr. (2012) 142:1603–10. doi: 10.3945/jn.112.160804
25. Amaral YN, Marano D, Silva LM, Guimaraes AC, Moreira ME. Are there changes in the fatty acid profile of breast milk with supplementation of omega-3 sources? a systematic review. Rev Bras Ginecol Obstet. (2017) 39:128–141. doi: 10.1055/s-0037-1599094
26. Dunstan JA, Mitoulas LR, Dixon G, Doherty DA, Hartmann PE, Simmer K, et al. The effects of fish oil supplementation in pregnancy on breast milk fatty acid composition over the course of lactation: a randomized controlled trial. Pediatr Res. (2007) 62:689–94. doi: 10.1203/PDR.0b013e318159a93a
27. Sherry CL, Oliver JS, Marriage BJ. Docosahexaenoic acid supplementation in lactating women increases breast milk and plasma docosahexaenoic acid concentrations and alters infant omega 6:3 fatty acid ratio. Prostaglandins Leukot Essent Fatty Acids. (2015) 95:63–9. doi: 10.1016/j.plefa.2015.01.005
28. Berger PK, Fields DA, Demerath EW, Fujiwara H, Goran MI. High-fructose corn-syrup-sweetened beverage intake increases 5-hour breast milk fructose concentrations in lactating women. Nutrients. (2018) 10:669. doi: 10.3390/nu10060669
29. Goran MI, Martin AA, Alderete TL, Fujiwara H, Fields DA. Fructose in breast milk is positively associated with infant body composition at 6 months of age. Nutrients. (2017) 9:146. doi: 10.3390/nu9020146
30. Bouhouch RR, Bouhouch S, Cherkaoui M, Aboussad A, Stinca S, Haldimann M, et al. Direct iodine supplementation of infants versus supplementation of their breastfeeding mothers: a double-blind, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. (2014) 2:197–209. doi: 10.1016/S2213-8587(13)70155-4
31. Mulrine HM, Skeaff SA, Ferguson EL, Gray AR, Valeix P. Breast-milk iodine concentration declines over the first 6 mo postpartum in iodine-deficient women. Am J Clin Nutr. (2010) 92:849–56. doi: 10.3945/ajcn.2010.29630
32. Sukkhojaiwaratkul D, Mahachoklertwattana P, Poomthavorn P, Panburana P, Chailurkit LO, Khlairit P, et al. Effects of maternal iodine supplementation during pregnancy and lactation on iodine status and neonatal thyroid-stimulating hormone. J Perinatol. (2014) 34:594–8. doi: 10.1038/jp.2014.62
33. Nazeri P, Mirmiran P, Tahmasebinejad Z, Hedayati M, Delshad H, Azizi F. The effects of iodine fortified milk on the iodine status of lactating mothers and infants in an area with a successful salt iodization program: a randomized controlled trial. Nutrients. (2017) 9:180. doi: 10.3390/nu9020180
34. Dror DK, Allen LH. Iodine in human milk: a systematic review. Adv Nutr. (2018) 9:347S−57S. doi: 10.1093/advances/nmy020
35. Dylewski ML, Picciano MF. Milk selenium content is enhanced by modest selenium supplementation in extended lactation. J Trace Elem Exp Med. (2002) 15:191–199. doi: 10.1002/jtra.10016
36. Trafikowska U, Sobkowiak E, Butler JA, Whanger PD, Zachara BA. Organic and inorganic selenium supplementation to lactating mothers increase the blood and milk Se concentrations and Se intake by breast-fed infants. J Trace Elem Med Biol. (1998) 12:77–85. doi: 10.1016/S0946-672X(98)80029-1
37. Domellof M, Lonnerdal B, Dewey KG, Cohen RJ, Hernell O. Iron, zinc, and copper concentrations in breast milk are independent of maternal mineral status. Am J Clin Nutr. (2004) 79:111–5. doi: 10.1093/ajcn/79.1.111
38. Salmenpera L, Perheentupa J, Nanto V, Siimes MA. Low zinc intake during exclusive breast-feeding does not impair growth. J Pediatr Gastroenterol Nutr. (1994) 18:361–70. doi: 10.1097/00005176-199404000-00019
39. O'Brien CE, Krebs NF, Westcott JL, Dong F. Relationships among plasma zinc, plasma prolactin, milk transfer, and milk zinc in lactating women. J Hum Lact. (2007) 23:179–83. doi: 10.1177/0890334407300021
40. de Figueiredo CS, Palhares DB, Melnikov P, Moura AJ, dos Santos SC. Zinc and copper concentrations in human preterm milk. Biol Trace Elem Res. (2010) 136:1–7. doi: 10.1007/s12011-009-8515-6
41. El-Farrash RA, Ismail EA, Nada AS. Cord blood iron profile and breast milk micronutrients in maternal iron deficiency anemia. Pediatr Blood Cancer. (2012) 58:233–8. doi: 10.1002/pbc.23184
42. Marin GH, Mestorino N, Errecalde J, Huber B, Uriarte A, Orchuela J. Personalised iron supply for prophylaxis and treatment of pregnant women as a way to ensure normal iron levels in their breast milk. J Med Life. (2012) 5:29–32.
43. Cai C, Granger M, Eck P, Friel J. Effect of daily iron supplementation in healthy exclusively breastfed infants: a systematic review with meta-analysis. Breastfeed Med. (2017) 12:597–603. doi: 10.1089/bfm.2017.0003
44. Olausson H, Goldberg GR, Laskey MA, Schoenmakers I, Jarjou LM, Prentice A. Calcium economy in human pregnancy and lactation. Nutr Res Rev. (2012) 25:40–67. doi: 10.1017/S0954422411000187
45. Butts CA, Hedderley DI, Herath TD, Paturi G, Glyn-Jones S, Wiens F, et al. Human milk composition and dietary intakes of breastfeeding women of different ethnicity from the Manawatu-Wanganui region of New Zealand. Nutrients. (2018) 10:1231. doi: 10.3390/nu10091231
46. Allen LH. B Vitamins in breast milk: relative importance of maternal status and intake, and effects on infant status and function. Adv Nutr. (2012) 3:362–9. doi: 10.3945/an.111.001172
47. Prentice AM, Roberts SB, Prentice A, Paul AA, Watkinson M, Watkinson AA, et al. Dietary supplementation of lactating Gambian women. I. Effect on breast-milk volume and quality. Hum Nutr Clin Nutr. (1983) 37:53–64.
48. Chang SJ, Kirksey A. Pyridoxine supplementation of lactating mothers: relation to maternal nutrition status and vitamin B-6 concentrations in milk. Am J Clin Nutr. (1990) 51:826–31. doi: 10.1093/ajcn/51.5.826
49. Chang SJ, Kirksey A. Vitamin B6 status of breast-fed infants in relation to pyridoxine HCl supplementation of mothers. J Nutr Sci Vitaminol. (2002) 48:10–7. doi: 10.3177/jnsv.48.10
50. Duggan C, Srinivasan K, Thomas T, Samuel T, Rajendran R, Muthayya S, et al. Vitamin B-12 supplementation during pregnancy and early lactation increases maternal, breast milk, and infant measures of vitamin B-12 status. J Nutr. (2014) 144:758–64. doi: 10.3945/jn.113.187278
51. Siddiqua TJ, Ahmad SM, Ahsan KB, Rashid M, Roy A, Rahman SM, et al. Vitamin B12 supplementation during pregnancy and postpartum improves B12 status of both mothers and infants but vaccine response in mothers only: a randomized clinical trial in Bangladesh. Eur J Nutr. (2016) 55:281–93. doi: 10.1007/s00394-015-0845-x
52. Fischer LM, da Costa KA, Galanko J, Sha W, Stephenson B, Vick J, et al. Choline intake and genetic polymorphisms influence choline metabolite concentrations in human breast milk and plasma. Am J Clin Nutr. (2010) 92:336–46. doi: 10.3945/ajcn.2010.29459
53. Davenport C, Yan J, Taesuwan S, Shields K, West AA, Jiang X, et al. Choline intakes exceeding recommendations during human lactation improve breast milk choline content by increasing PEMT pathway metabolites. J Nutr Biochem. (2015) 26:903–11. doi: 10.1016/j.jnutbio.2015.03.004
54. Sherry CL, Oliver JS, Renzi LM, Marriage BJ. Lutein supplementation increases breast milk and plasma lutein concentrations in lactating women and infant plasma concentrations but does not affect other carotenoids. J Nutr. (2014) 144:1256–63. doi: 10.3945/jn.114.192914
55. Kim H, Yi H, Jung JA, Chang N. Association between lutein intake and lutein concentrations in human milk samples from lactating mothers in South Korea. Eur J Nutr. (2018) 57:417–21. doi: 10.1007/s00394-017-1414-2
56. Perry CA, West AA, Gayle A, Lucas LK, Yan J, Jiang X, et al. Pregnancy and lactation alter biomarkers of biotin metabolism in women consuming a controlled diet. J Nutr. (2014) 144:1977–84. doi: 10.3945/jn.114.194472
57. Deminice TMM, Ferraz IS, Monteiro JP, Jordao AA, Ambrosio L, Nogueira-de-Almeida CA. Vitamin A intake of Brazilian mothers and retinol concentrations in maternal blood, human milk, and the umbilical cord. J Int Med Res. (2018) 46:1555–69. doi: 10.1177/0300060518757155
58. Thiele DK, Senti JL, Anderson CM. Maternal vitamin D supplementation to meet the needs of the breastfed infant: a systematic review. J Hum Lact. (2013) 29:163–70. doi: 10.1177/0890334413477916
59. Dawodu A, Tsang RC. Maternal vitamin D status: effect on milk vitamin D content and vitamin D status of breastfeeding infants. Adv Nutr. (2012) 3:353–61. doi: 10.3945/an.111.000950
60. Ketha H, Thacher TD, Oberhelman SS, Fischer PR, Singh RJ, Kumar R. Comparison of the effect of daily versus bolus dose maternal vitamin D3 supplementation on the 24,25-dihydroxyvitamin D3 to 25-hydroxyvitamin D3 ratio. Bone. (2018) 110:321–5. doi: 10.1016/j.bone.2018.02.024
61. Clemente HA, Ramalho HM, Lima MS, Grilo EC, Dimenstein R. Maternal supplementation with natural or synthetic vitamin E and its levels in human colostrum. J Pediatr Gastroenterol Nutr. (2015) 60:533–7. doi: 10.1097/MPG.0000000000000635
62. Zuppa AA, Sindico P, Orchi C, Carducci C, Cardiello V, Romagnoli C. Safety and efficacy of galactogogues: substances that induce, maintain and increase breast milk production. J Pharm Pharm Sci. (2010) 13:162–74. doi: 10.18433/J3DS3R
63. Mortel M, Mehta SD. Systematic review of the efficacy of herbal galactogogues. J Hum Lact. (2013) 29:154–62. doi: 10.1177/0890334413477243
64. Serrao F, Corsello M, Romagnoli C, D'Andrea V, Zecca E. The long-term efficacy of a galactagogue containing sylimarin-phosphatidylserine and galega on milk production of mothers of preterm infants. Breastfeed Med. (2018) 13:67–9. doi: 10.1089/bfm.2017.0169
65. Khan TM, Wu DB, Dolzhenko AV. Effectiveness of fenugreek as a galactagogue: a network meta-analysis. Phytother Res. (2018) 32:402–12. doi: 10.1002/ptr.5972
66. Ozalkaya E, Aslandogdu Z, Ozkoral A, Topcuoglu S, Karatekin G. Effect of a galactagogue herbal tea on breast milk production and prolactin secretion by mothers of preterm babies. Niger J Clin Pract. (2018) 21:38–42. doi: 10.4103/1119-3077.224788
67. Nikniaz L, Mahdavi R, Ostadrahimi A, Nikniaz Z, Aliasgharzadeh S. Does maternal synbiotic supplementation affect conjugated linoleic acid level in breast milk? A randomized placebo-controlled clinical trial. Breastfeed Med. (2018) 13:81–4. doi: 10.1089/bfm.2017.0053
68. Makela J, Linderborg K, Niinikoski H, Yang B, Lagstrom H. Breast milk fatty acid composition differs between overweight and normal weight women: the STEPS study. Eur J Nutr. (2013) 52:727–35. doi: 10.1007/s00394-012-0378-5
69. Hahn WH, Jeong T, Park S, Song S, Kang NM. Content fat and calorie of human milk is affected by interactions between maternal age and body mass index. J Matern Fetal Neonatal Med. (2018) 31:1385–8. doi: 10.1080/14767058.2017.1315660
70. Butte NF, Garza C, Stuff JE, Smith EO, Nichols BL. Effect of maternal diet and body composition on lactational performance. Am J Clin Nutr. (1984) 39:296–306. doi: 10.1093/ajcn/39.2.296
71. Brown KH, Akhtar NA, Robertson AD, Ahmed MG. Lactational capacity of marginally nourished mothers: relationships between maternal nutritional status and quantity and proximate composition of milk. Pediatrics. (1986) 78:909–19.
72. Prentice A, Prentice AM, Whitehead RG. Breast-milk fat concentrations of rural African women. 2. Long-term variations within a community. Br J Nutr. (1981) 45:495–503. doi: 10.1079/BJN19810128
73. Infante C, Hurtado J, Salazar G, Pollastri A, Aguirre E, Vio F. The dose-to-mother method to measure milk intake in infants by deuterium dilution: a validation study. Eur J Clin Nutr. (1991) 45:121–9.
74. Ettyang GA, van Marken Lichtenbelt WD, Esamai F, Saris WH, Westerterp KR. Assessment of body composition and breast milk volume in lactating mothers in pastoral communities in Pokot, Kenya, using deuterium oxide. Ann Nutr Metab. (2005) 49:110–7. doi: 10.1159/000084744
75. Perez-Escamilla R, Cohen RJ, Brown KH, Rivera LL, Canahuati J, Dewey KG. Maternal anthropometric status and lactation performance in a low-income Honduran population: evidence for the role of infants. Am J Clin Nutr. (1995) 61:528–34. doi: 10.1093/ajcn/61.3.528
76. Fields DA, Demerath EW. Relationship of insulin, glucose, leptin, IL-6 and TNF-alpha in human breast milk with infant growth and body composition. Pediatr Obes. (2012) 7:304–12. doi: 10.1111/j.2047-6310.2012.00059.x
77. Miralles O, Sanchez J, Palou A, Pico C. A physiological role of breast milk leptin in body weight control in developing infants. Obesity. (2006) 14:1371–7. doi: 10.1038/oby.2006.155
78. Schuster S, Hechler C, Gebauer C, Kiess W, Kratzsch J. Leptin in maternal serum and breast milk: association with infants' body weight gain in a longitudinal study over 6 months of lactation. Pediatr Res. (2011) 70:633–7. doi: 10.1203/PDR.0b013e31823214ea
79. Uysal FK, Onal EE, Aral YZ, Adam B, Dilmen U, Ardicolu Y. Breast milk leptin: its relationship to maternal and infant adiposity. Clin Nutr. (2002) 21:157–60. doi: 10.1054/clnu.2001.0525
80. Kugananthan S, Gridneva Z, Lai CT, Hepworth AR, Mark PJ, Kakulas F, et al. Associations between maternal body composition and appetite hormones and macronutrients in human milk. Nutrients. (2017) 9:252. doi: 10.3390/nu9030252
81. Doneray H, Orbak Z, Yildiz L. The relationship between breast milk leptin and neonatal weight gain. Acta Paediatr. (2009) 98:643–7. doi: 10.1111/j.1651-2227.2008.01192.x
82. Brunner S, Schmid D, Zang K, Much D, Knoeferl B, Kratzsch J, et al. Breast milk leptin and adiponectin in relation to infant body composition up to 2 years. Pediatr Obes. (2015) 10:67–73. doi: 10.1111/j.2047-6310.2014.222.x
83. Bachour P, Yafawi R, Jaber F, Choueiri E, Abdel-Razzak Z. Effects of smoking, mother's age, body mass index, and parity number on lipid, protein, and secretory immunoglobulin a concentrations of human milk. Breastfeed Med. (2012) 7:179–88. doi: 10.1089/bfm.2011.0038
84. Antonakou A, Skenderi KP, Chiou A, Anastasiou CA, Bakoula C, Matalas AL. Breast milk fat concentration and fatty acid pattern during the first six months in exclusively breastfeeding Greek women. Eur J Nutr. (2013) 52:963–73. doi: 10.1007/s00394-012-0403-8
85. Prentice A, Jarjou LMA, Drury PJ, Dewit O, Crawford MA. Breast-milk fatty acids of rural Gambian mothers: effects of diet and maternal parity. J Pediatr Gastroenterol Nutr. (1989) 8:486–90. doi: 10.1097/00005176-198905000-00011
86. Silvestre MD, Lagarda MJ, Farre R, Martinez-Costa C, Brines J, Molina A, et al. A study of factors that may influence the determination of copper, iron, and zinc in human milk during sampling and in sample individuals. Biol Trace Elem Res. (2000) 76:217–27. doi: 10.1385/BTER:76:3:217
87. Islam SK, Ahmed L, Khan MN, Huque S, Begum A, Yunus AB. Immune components (IgA, IgM, IgG, immune cells) of colostrum of Bangladeshi mothers. Pediatr Int. (2006) 48:543–8. doi: 10.1111/j.1442-200X.2006.02291.x
88. Striker GA, Casanova LD, Nagao AT. [Influence of type of delivery on A, G and M immunoglobulin concentration in maternal colostrum]. J Pediatr. (2004) 80:123–8. doi: 10.2223/1151
89. Munblit D, Boyle RJ, Warner JO. Factors affecting breast milk composition and potential consequences for development of the allergic phenotype. Clin Exp Allergy. (2015) 45:583–601. doi: 10.1111/cea.12381
90. Dizdar EA, Sari FN, Degirmencioglu H, Canpolat FE, Oguz SS, Uras N, et al. Effect of mode of delivery on macronutrient content of breast milk. J Matern Fetal Neonatal Med. (2014) 27:1099–102. doi: 10.3109/14767058.2013.850486
91. Ozarda Y, Cansev M, Ulus IH. Breast milk choline contents are associated with inflammatory status of breastfeeding women. J Hum Lact. (2014) 30:161–6. doi: 10.1177/0890334413508004
92. Zhao A, Ning YB, Zhang YM, Yang XG, Wang JK, Li WJ, et al. Mineral compositions in breast milk of healthy chinese lactating women in urban areas and its associated factors. Chin Med J. (2014) 127:2643–8. doi: 10.3760/cma.j.issn.0366-6999.20133258
93. Munblit D, Sheth S, Abrol P, Treneva M, Peroni DG, Chow LY, et al. Exposures influencing total IgA level in colostrum. J Dev Orig Health Dis. (2016) 7:61–7. doi: 10.1017/S2040174415001476
94. Motil KJ, Kertz B, Thotathuchery M. Lactational performance of adolescent mothers shows preliminary differences from that of adult women. J Adolesc Health. (1997) 20:442–49. doi: 10.1016/S1054-139X(97)00036-0
95. Rocquelin G, Tapsoba S, Dop MC, Mbemba F, Traissac P, Martin-Prével Y. Lipid content and essential fatty acid (EFA) composition of mature congolese breast milk are influenced by mothers' nutritional status: impact on infants' EFA supply. Eur J Clin Nutr. (1998) 52:164–71. doi: 10.1038/sj.ejcn.1600529
96. Al-Tamer YY, Mahmood AA. The influence of Iraqi mothers' socioeconomic status on their milk-lipid content. Eur J Clin Nutr. (2006) 60:1400–5. doi: 10.1038/sj.ejcn.1602470
97. Nayak U, Kanungo S, Zhang D, Ross Colgate E, Carmolli MP, Dey A, et al. Influence of maternal and socioeconomic factors on breast milk fatty acid composition in urban, low-income families. Matern Child Nutr. (2017) 13:e12423. doi: 10.1111/mcn.12423
98. Xue Y, Campos-Gimenez E, Redeuil KM, Leveques A, Actis-Goretta L, Vinyes-Pares G, et al. Concentrations of carotenoids and tocopherols in breast milk from urban chinese mothers and their associations with maternal characteristics: a cross-sectional study. Nutrients. (2017) 9:1229. doi: 10.3390/nu9111229
99. VandenBerg P, O'Connor D, Hanley A Dr. Impact of gestational diabetes on breast milk composition and subsequent infant development. Can J Diabetes. (2012) 36:52–3. doi: 10.1016/j.jcjd.2012.04.005
100. Hartmann P, Cregan M. Lactogenesis and the effects of insulin-dependent diabetes mellitus and prematurity. J Nutr. (2001) 131:3016S−20S. doi: 10.1093/jn/131.11.3016S
101. Aydin S, Geckil H, Karatas F, Donder E, Kumru S, Kavak EC, et al. Milk and blood ghrelin level in diabetics. Nutrition. (2007) 23:807–11. doi: 10.1016/j.nut.2007.08.015
102. Ley SH, Hanley AJ, Sermer M, Zinman B, O'Connor DL. Associations of prenatal metabolic abnormalities with insulin and adiponectin concentrations in human milk. Am J Clin Nutr. (2012) 95:867–74. doi: 10.3945/ajcn.111.028431
103. Klein K, Bancher-Todesca D, Graf T, Garo F, Roth E, Kautzky-Willer A, et al. Concentration of free amino acids in human milk of women with gestational diabetes mellitus and healthy women. Breastfeed Med. (2013) 8:111–5. doi: 10.1089/bfm.2011.0155
104. Olivares M, Albrecht S, De Palma G, Ferrer MD, Castillejo G, Schols HA, et al. Human milk composition differs in healthy mothers and mothers with celiac disease. Eur J Nutr. (2015) 54:119–28. doi: 10.1007/s00394-014-0692-1
105. Roca M, Vriezinga SL, Crespo-Escobar P, Auricchio R, Hervas D, Castillejo G, et al. Anti-gliadin antibodies in breast milk from celiac mothers on a gluten-free diet. Eur J Nutr. (2018) 57:1947–55. doi: 10.1007/s00394-017-1476-1
106. Bottcher MF, Jenmalm MC, Garofalo RP, Bjorksten B. Cytokines in breast milk from allergic and nonallergic mothers. Pediatr Res. (2000) 47:157–62. doi: 10.1203/00006450-200001000-00026
107. Sidor K, Jarmolowska B, Kaczmarski M, Kostyra E, Iwan M, Kostyra H. Content of beta-casomorphins in milk of women with a history of allergy. Pediatr Allergy Immunol. (2008) 19:587–91. doi: 10.1111/j.1399-3038.2007.00711.x
108. Prokesova L, Lodinova-Zadnikova R, Zizka J, Kocourkova I, Novotna O, Petraskova P, et al. Cytokine levels in healthy and allergic mothers and their children during the first year of life. Pediatr Allergy Immunol. (2006) 17:175–83. doi: 10.1111/j.1399-3038.2006.00395.x
109. Marek A, Zagierski M, Liberek A, Aleksandrowicz E, Korzon M, Krzykowski G, et al. TGF-beta(1) A, IL-10 and IL-4 in colostrum of allergic and nonallergic mothers. Acta Biochim Pol. (2009) 56:411–4. doi: 10.18388/abp.2009_2474
110. Rigotti E, Piacentini GL, Ress M, Pigozzi R, Boner AL, Peroni DG. Transforming growth factor-beta and interleukin-10 in breast milk and development of atopic diseases in infants. Clin Exp Allergy. (2006) 36:614–8. doi: 10.1111/j.1365-2222.2006.02483.x
111. Laiho K, Lampi AM, Hamalainen M, Moilanen E, Piironen V, Arvola T, et al. Breast milk fatty acids, eicosanoids, and cytokines in mothers with and without allergic disease. Pediatr Res. (2003) 53:642–7. doi: 10.1203/01.PDR.0000055778.58807.C8
112. Hettinga KA, Reina FM, Boeren S, Zhang L, Koppelman GH, Postma DS, et al. Difference in the breast milk proteome between allergic and non-allergic mothers. PLoS ONE. (2015) 10:e0122234. doi: 10.1371/journal.pone.0122234
113. Snijders BE, Damoiseaux JG, Penders J, Kummeling I, Stelma FF, van Ree R, et al. Cytokines and soluble CD14 in breast milk in relation with atopic manifestations in mother and infant (KOALA study). Clin Exp Allergy. (2006) 36:1609–15. doi: 10.1111/j.1365-2222.2006.02613.x
114. Rudloff S, Niehues T, Rutsch M, Kunz C, Schroten H. Inflammation markers and cytokines in breast milk of atopic and nonatopic women. Allergy. (1999) 54:206–11. doi: 10.1034/j.1398-9995.1999.00765.x
115. Munblit D, Treneva M, Peroni DG, Colicino S, Chow L, Dissanayeke S, et al. Colostrum and mature human milk of women from London, Moscow, and Verona: determinants of immune composition. Nutrients. (2016) 8:695. doi: 10.3390/nu8110695
116. Lauritzen L, Halkjaer LB, Mikkelsen TB, Olsen SF, Michaelsen KF, Loland L, et al. Fatty acid composition of human milk in atopic Danish mothers. Am J Clin Nutr. (2006) 84:190–6. doi: 10.1093/ajcn/84.1.190
117. Johansson S, Wold AE, Sandberg AS. Low breast milk levels of long-chain n-3 fatty acids in allergic women, despite frequent fish intake. Clin Exp Allergy. (2011) 41:505–15. doi: 10.1111/j.1365-2222.2010.03678.x
118. Ramadan MA, Salah MM, Eid SZ. Effect of breast infection on the composition of human milk. Int J Biochem. (1972) 3:543–8. doi: 10.1016/0020-711X(72)90009-2
119. Mizuno K, Hatsuno M, Aikawa K, Takeichi H, Himi T, Kaneko A, et al. Mastitis is associated with IL-6 levels and milk fat globule size in breast milk. J Hum Lact. (2012) 28:529–34. doi: 10.1177/0890334412455946
120. Buescher ES, Hair PS. Human milk anti-inflammatory component contents during acute mastitis. Cell Immunol. (2001) 210:87–95. doi: 10.1006/cimm.2001.1813
121. Gale S, Harlow BL. Postpartum mood disorders: a review of clinical and epidemiological factors. J Psychosom Obstet Gynecol. (2003) 24:257–66. doi: 10.3109/01674820309074690
122. O'Hara MW, Neunaber DJ, Zekoski EM. Prospective study of postpartum depression: prevalence, course, predictive factors. J Abnorm Psychol. (1984) 93:158–71. doi: 10.1037/0021-843X.93.2.158
123. Dias CC, Figueiredo B. Breastfeeding and depression: a systematic review of the literature. J Affect Disord. (2015) 171:142–54. doi: 10.1016/j.jad.2014.09.022
124. Mathews ME, Leerkes EM, Lovelady CA, Labban JD. Psychosocial predictors of primiparous breastfeeding initiation and duration. J Hum Lact. (2014) 30:480–7. doi: 10.1177/0890334414537707
125. Rahman A, Hafeez A, Bilal R, Sikander S, Malik A, Minhas F, et al. The impact of perinatal depression on exclusive breastfeeding: a cohort study. Matern Child Nutr. (2015) 12:452–62. doi: 10.1111/mcn.12170
126. Hill PD, Aldag JC, Demirtas H, Zinaman M, Chatterton RT. Mood states and milk output in lactating mothers of preterm and term infants. J Hum Lact. (2006) 22:305–14. doi: 10.1177/0890334406290003
127. Galipeau R, Goulet C, Chagnon M. Infant and maternal factors influencing breastmilk sodium among primiparous mothers. Breastfeed Med. (2012) 7:290–4. doi: 10.1089/bfm.2011.0022
128. Cisse AS, Dossou N, Ndiaye M, Gueye AL, Diop el HI, Diaham B, et al. Stable isotope aided evaluation of community nutrition program: effect of food supplementation schemes on maternal and infant nutritional status. Food Nutr Bull. (2002) 23(3 Suppl):169–73. doi: 10.1177/15648265020233S133
129. Fidler N, Salobir K, Stibilj V. Fatty acid composition of human milk in different regions of Slovenia. Ann Nutr Metab. (2000) 44:187–93. doi: 10.1159/000046682
130. Chulei R, Xiaofang L, Hongsheng M, Xiulan M, Guizheng L, Gianhong D, et al. Milk composition in women from five different regions of China: the great diversity of milk fatty acids. J Nutr. (1995) 125:2993–8. doi: 10.1093/jn/125.12.2993
131. Chen ZY, Kwan KY, Tong KK, Ratnayake WMN, Li HQ, Leung SSF. Breast milk fatty acid composition: a comparative study between Hong Kong and Chongqing Chinese. Lipids. (1997) 32:1061–7. doi: 10.1007/s11745-997-0137-6
132. Nishimura RY, Castro GS, Jordao AA Jr, Sartorelli DS. Breast milk fatty acid composition of women living far from the coastal area in Brazil. J Pediatr. (2013) 89:263–8. doi: 10.1016/j.jped.2012.11.007
133. Zhang WL, Wu SM, Qian JH, Wu YL, Gao XL, Yang HW, et al. Comparison of contents of polyunsaturated fatty acids of breast milk among different regions of China and between colostrums and mature milk. Chin J Clin Rehabil. (2004) 8:2389–91.
134. Roy S, Dhar P, Ghosh S. Comparative evaluation of essential fatty acid composition of mothers' milk of some urban and suburban regions of West Bengal, India. Int J Food Sci Nutr. (2012) 63:895–901. doi: 10.3109/09637486.2012.683778
135. Xiang M, Harbige L, Zetterström R. Long-chain polyunsaturated fatty acids in Chinese and Swedish mothers: diet, breast milk and infant growth. Acta Paediatr. (2005) 94:1543–9. doi: 10.1080/08035250500251601
136. Musumeci M, Simpore J, D'Agata A, Sotgiu S, Musumeci S. Oligosaccharides in colostrum of Italian and Burkinabe women. J Pediatr Gastroenterol Nutr. (2006) 43:372–8. doi: 10.1097/01.mpg.0000228125.70971.af
137. Lu M, Jiang J, Wu K, Li D. Epidermal growth factor and transforming growth factor-alpha in human milk of different lactation stages and different regions and their relationship with maternal diet. Food Funct. (2018) 9:1199–204. doi: 10.1039/C7FO00770A
138. Lignell S, Aune M, Darnerud PO, Soeria-Atmadja D, Hanberg A, Larsson S, et al. Large variation in breast milk levels of organohalogenated compounds is dependent on mother's age, changes in body composition and exposures early in life. J Environ Monitor. (2011) 13:1607–16. doi: 10.1039/c1em10151j
139. Bassil M, Daou F, Hassan H, Yamani O, Kharma JA, Attieh Z, et al. Lead, cadmium and arsenic in human milk and their socio-demographic and lifestyle determinants in Lebanon. Chemosphere. (2018) 191:911–21. doi: 10.1016/j.chemosphere.2017.10.111
140. Fujii Y, Yan J, Harada KH, Hitomi T, Yang H, Wang P, et al. Levels and profiles of long-chain perfluorinated carboxylic acids in human breast milk and infant formulas in East Asia. Chemosphere. (2012) 86:315–21. doi: 10.1016/j.chemosphere.2011.10.035
141. Lee S, Kim S, Park J, Kim HJ, Choi G, Choi S, et al. Perfluoroalkyl substances (PFASs) in breast milk from Korea: time-course trends, influencing factors, infant exposure. Sci Total Environ. (2018) 612:286–92. doi: 10.1016/j.scitotenv.2017.08.094
142. Rowe H, Baker T, Hale TW. Maternal medication, drug use, and breastfeeding. Pediatr Clin North Am. (2013) 60:275–94. doi: 10.1016/j.pcl.2012.10.009
143. Lu M, Xiao H, Li K, Jiang J, Wu K, Li D. Concentrations of estrogen and progesterone in breast milk and their relationship with the mother's diet. Food Funct. (2017) 8:3306–10. doi: 10.1039/C7FO00324B
144. Abou-Dakn M, Schäfer-Graf U, Wöckel A. Psychological stress and breast diseases during lactation. Breastfeed Rev. (2009) 17:19–26.
145. Cabrera-Rubio R, Collado MC, Laitinen K, Salminen S, Isolauri E, Mira A. The human milk microbiome changes over lactation and is shaped by maternal weight and mode of delivery. Am J Clin Nutr. (2012) 96:544–51. doi: 10.3945/ajcn.112.037382
146. Cabrera-Rubio R, Mira-Pascual L, Mira A, Collado MC. Impact of mode of delivery on the milk microbiota composition of healthy women. J Dev Orig Health Dis. (2015) 7:54–60. doi: 10.1017/S2040174415001397
147. Fitzstevens JL, Smith KC, Hagadorn JI, Caimano MJ, Matson AP, Brownell EA. Systematic review of the human milk microbiota. Nutr Clin Pract. (2017) 32:354–64. doi: 10.1177/0884533616670150
148. Toscano M, De Grandi R, Peroni DG, Grossi E, Facchin V, Comberiati P, et al. Impact of delivery mode on the colostrum microbiota composition. BMC Microbiol. (2017) 17:205. doi: 10.1186/s12866-017-1109-0
149. Su LL, Thamarai Chelvi SK, Lim SL, Chen Y, Tan EAT, Pai NN, et al. The infl uence of maternal ethnic group and diet on breast milk fatty acid composition. Ann Acad Med Singap. (2010) 39:675–9.
150. Khan S, Hepworth AR, Prime DK, Lai CT, Trengove NJ, Hartmann PE. Variation in fat, lactose, and protein composition in breast milk over 24 hours: associations with infant feeding patterns. J Hum Lact. (2013) 29:81–9. doi: 10.1177/0890334412448841
151. Kent JC, Mitoulas LR, Cregan MD, Ramsay DT, Doherty DA, Hartmann PE. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics. (2006) 117:e387–95. doi: 10.1542/peds.2005-1417
152. Agostoni C, Marangoni F, Grandi F, Lammardo AM, Giovannini M, Riva E, et al. Earlier smoking habits are associated with higher serum lipids and lower milk fat and polyunsaturated fatty acid content in the first 6 months of lactation. Eur J Clin Nutr. (2003) 57:1466–72. doi: 10.1038/sj.ejcn.1601711
153. Baheiraei A, Shamsi A, Khaghani S, Shams S, Chamari M, Boushehri H, et al. The effects of maternal passive smoking on maternal milk lipid. Acta Medica Iranica. (2014) 52:280–5.
154. Mandour RA, Ghanem AA, El-Azab SM. Correlation between lead levels in drinking water and mothers' breast milk: Dakahlia, Egypt. Environ Geochem Health. (2013) 35:251–6. doi: 10.1007/s10653-012-9480-0
155. Szlagatys-Sidorkiewicz A, Martysiak-Zurowska D, Krzykowski G, Zagierski M, Kamińska B. Maternal smoking modulates fatty acid profile of breast milk. Acta Paediatr. (2013) 102:e353–9. doi: 10.1111/apa.12276
156. Chien YC, Huang YJ, Hsu CS, Chao JCJ, Liu JF. Maternal lactation characteristics after consumption of an alcoholic soup during the postpartum 'doing-the-month' ritual. Public Health Nutr. (2009) 12:382–8. doi: 10.1017/S1368980008002152
157. Heil SH, Subramanian MG. Alcohol and the hormonal control of lactation. Alcohol Health Res World. (1998) 22:178–84.
158. Mennella JA, Pepino MY. Breastfeeding and prolactin levels in lactating women with a family history of alcoholism. Pediatrics. (2010) 125:e1162–70. doi: 10.1542/peds.2009-3040
159. Liston J. Breastfeeding and the use of recreational drugs–alcohol, caffeine, nicotine and marijuana. Breastfeed Rev. (1998) 6:27–30.
160. Nehlig A, Debry G. Consequences on the newborn of chronic maternal consumption of coffee during gestation and lactation: a review. J Am Coll Nutr. (1994) 13:6–21. doi: 10.1080/07315724.1994.10718366
161. Oo CY, Burgio DE, Kuhn RC, Desai N, McNamara PJ. Pharmacokinetics of caffeine and its demethylated metabolites in lactation: predictions of milk to serum concentration ratios. Pharm Res. (1995) 12:313–6. doi: 10.1023/A:1016207832591
162. Stavchansky S, Combs A, Sagraves R, Delgado M, Joshi A. Pharmacokinetics of caffeine in breast milk and plasma after single oral administration of caffeine to lactating mothers. Biopharm Drug Dispos. (1988) 9:285–99. doi: 10.1002/bod.2510090307
163. Carey GB, Quinn TJ, Goodwin SE. Breast milk composition after exercise of different intensities. J Hum Lact. (1997) 13:115–20. doi: 10.1177/089033449701300211
164. Davies GA, Wolfe LA, Mottola MF, MacKinnon C, Arsenault MY, Bartellas E, et al. Exercise in pregnancy and the postpartum period. J Obstetr Gynaecol Can. (2003) 25:516–29. doi: 10.1016/j.jogc.2017.11.001
165. Dewey KG, Lovelady CA, Nommsen-Rivers LA, McCrory MA, Lönnerdal B. A randomized study of the effects of aerobic exercise by lactating women on breast-milk volume and composition. New Engl J Med. (1994) 330:449–53. doi: 10.1056/NEJM199402173300701
166. Lovelady CA, Hunter CP, Geigerman C. Effect of exercise on immunologic factors in breast milk. Pediatrics. (2003) 111:E148–52. doi: 10.1542/peds.111.2.e148
167. Lovelady CA, Lonnerdal B, Dewey KG. Lactation performance of exercising women. Am J Clin Nutr. (1990) 52:103–9. doi: 10.1093/ajcn/52.1.103
169. Quinn TJ, Carey GB. Does exercise intensity or diet influence lactic acid accumulation in breast milk? Med Sci Sports Exerc. (1999) 31:105–10. doi: 10.1097/00005768-199901000-00017
170. Wallace JP, Inbar G, Ernsthausen K. Infant acceptance of postexercise breast milk. Pediatrics. (1992) 89:1245–7.
171. Wright KS, Quinn TJ, Carey GB. Infant acceptance of breast milk after maternal exercise. Pediatrics. (2002) 109:585–9. doi: 10.1542/peds.109.4.585
172. Gridneva Z, Rea A, Hepworth AR, Ward LC, Lai CT, Hartmann PE, et al. Relationships between breastfeeding patterns and maternal and infant body composition over the first 12 months of lactation. Nutrients. (2018) 10:45. doi: 10.3390/nu10010045
173. Munblit D, Peroni DG, Boix-Amoros A, Hsu PS, Van't Land B, Gay MCL, et al. Human milk and allergic diseases: an unsolved puzzle. Nutrients. (2017) 9:894. doi: 10.3390/nu9080894
174. Dewey KG, Heinig MJ, Nommsen LA, Lonnerdal B. Maternal versus infant factors related to breast milk intake and residual milk volume: the DARLING study. Pediatrics. (1991) 87:829–37.
175. Islam MM, Brown KH. Zinc transferred through breast milk does not differ between appropriate- and small-for-gestational-age, predominantly breast-fed Bangladeshi infants. J Nutr. (2014) 144:771–6. doi: 10.3945/jn.113.189308
176. Butte NF, Garza C, Johnson CA, Smith EO, Nichols BL. Longitudinal changes in milk composition of mothers delivering preterm and term infants. Early Hum Dev. (1984) 9:153–62. doi: 10.1016/0378-3782(84)90096-3
177. Gidrewicz DA, Fenton TR. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. (2014) 14:216. doi: 10.1186/1471-2431-14-216
178. Underwood MA. Human milk for the premature infant. Pediatr Clin North Am. (2013) 60:189–207. doi: 10.1016/j.pcl.2012.09.008
179. Castellote C, Casillas R, Ramirez-Santana C, Perez-Cano FJ, Castell M, Moretones MG, et al. Premature delivery influences the immunological composition of colostrum and transitional and mature human milk. J Nutr. (2011) 141:1181–7. doi: 10.3945/jn.110.133652
180. Ozgurtas T, Aydin I, Turan O, Koc E, Hirfanoglu IM, Acikel CH, et al. Vascular endothelial growth factor, basic fibroblast growth factor, insulin-like growth factor-I and platelet-derived growth factor levels in human milk of mothers with term and preterm neonates. Cytokine. (2010) 50:192–4. doi: 10.1016/j.cyto.2010.02.008
181. Slupecka-Ziemilska M, Wolinski J, Herman AP, Romanowicz K, Dziegielewska Z, Borszewska-Kornacka MK. Influence of preterm delivery on ghrelin and obestatin concentrations in maternal plasm, milk and their expression in mammary epithelial cells. J Physiol Pharmacol. (2017) 68:693–8.
182. Berenhauser AC, Pinheiro do Prado AC, da Silva RC, Gioielli LA, Block JM. Fatty acid composition in preterm and term breast milk. Int J Food Sci Nutr. (2012) 63:318–25. doi: 10.3109/09637486.2011.627843
183. Granot E, Ishay-Gigi K, Malaach L, Flidel-Rimon O. Is there a difference in breast milk fatty acid composition of mothers of preterm and term infants? J Matern Fetal Neonatal Med. (2016) 29:832–5. doi: 10.3109/14767058.2015.1020785
184. Ustundag B, Yilmaz E, Dogan Y, Akarsu S, Canatan H, Halifeoglu I, et al. Levels of cytokines (IL-1beta, IL-2, IL-6, IL-8, TNF-alpha) and trace elements (Zn, Cu) in breast milk from mothers of preterm and term infants. Mediators Inflamm. (2005) 2005:331–6. doi: 10.1155/MI.2005.331
185. Powe CE, Knott CD, Conklin-Brittain N. Infant sex predicts breast milk energy content. Am J Hum Biol. (2010) 22:50–4. doi: 10.1002/ajhb.20941
186. Thakkar SK, Giuffrida F, Cristina CH, De Castro CA, Mukherjee R, Tran LA, et al. Dynamics of human milk nutrient composition of women from Singapore with a special focus on lipids. Am J Hum Biol. (2013) 25:770–9. doi: 10.1002/ajhb.22446
187. Fujita M, Roth E, Lo YJ, Hurst C, Vollner J, Kendell A. In poor families, mothers' milk is richer for daughters than sons: a test of trivers-Willard hypothesis in agropastoral settlements in Northern Kenya. Am J Phys Anthropol. (2012) 149:52–9. doi: 10.1002/ajpa.22092
188. da Costa TH, Haisma H, Wells JC, Mander AP, Whitehead RG, Bluck LJ. How much human milk do infants consume? Data from 12 countries using a standardized stable isotope methodology. J Nutr. (2010) 140:2227–32. doi: 10.3945/jn.110.123489
189. Czosnykowska-Lukacka M, Krolak-Olejnik B, Orczyk-Pawilowicz M. Breast milk macronutrient components in prolonged lactation. Nutrients. (2018) 10:1893. doi: 10.3390/nu10121893
190. Lonnerdal B, Erdmann P, Thakkar SK, Sauser J, Destaillats F. Longitudinal evolution of true protein, amino acids and bioactive proteins in breast milk: a developmental perspective. J Nutr Biochem. (2017) 41:1–11. doi: 10.1016/j.jnutbio.2016.06.001
191. Verd S, Ginovart G, Calvo J, Ponce-Taylor J, Gaya A. Variation in the protein composition of human milk during extended lactation: a narrative review. Nutrients. (2018) 10:1124. doi: 10.3390/nu10081124
192. Yang T, Zhang L, Bao W, Rong S. Nutritional composition of breast milk in Chinese women: a systematic review. Asia Pac J Clin Nutr. (2018) 27:491–502. doi: 10.6133/apjcn.042017.13
193. Jie L, Qi C, Sun J, Yu R, Wang X, Korma SA, et al. The impact of lactation and gestational age on the composition of branched-chain fatty acids in human breast milk. Food Funct. (2018) 9:1747–54. doi: 10.1039/C7FO01979C
194. Thurl S, Munzert M, Boehm G, Matthews C, Stahl B. Systematic review of the concentrations of oligosaccharides in human milk. Nutr Rev. (2017) 75:920–33. doi: 10.1093/nutrit/nux044
195. Saarela T, Kokkonen J, Koivisto M. Macronutrient and energy contents of human milk fractions during the first six months of lactation. Acta Paediatr. (2005) 94:1176–81. doi: 10.1111/j.1651-2227.2005.tb02070.x
196. Mitoulas LR, Kent JC, Cox DB, Owens RA, Sherriff JL, Hartmann PE. Variation in fat, lactose and protein in human milk over 24 h and throughout the first year of lactation. Br J Nutr. (2002) 88:29–37. doi: 10.1079/BJN2002579
197. Chang N, Jung JA, Kim H, Jo A, Kang S, Lee SW, et al. Macronutrient composition of human milk from Korean mothers of full term infants born at 37-42 gestational weeks. Nutr Res Pract. (2015) 9:433–8. doi: 10.4162/nrp.2015.9.4.433
198. Coppa GV, Gabrielli O, Pierani P, Catassi C, Carlucci A, Giorgi PL. Changes in carbohydrate composition in human milk over 4 months of lactation. Pediatrics. (1993) 91:637–41.
199. Austin S, De Castro CA, Benet T, Hou Y, Sun H, Thakkar SK, et al. Temporal change of the content of 10 oligosaccharides in the milk of Chinese urban mothers. Nutrients. (2016) 8:346. doi: 10.3390/nu8060346
200. Sprenger N, Lee LY, De Castro CA, Steenhout P, Thakkar SK. Longitudinal change of selected human milk oligosaccharides and association to infants' growth, an observatory, single center, longitudinal cohort study. PLoS ONE. (2017) 12:e0171814. doi: 10.1371/journal.pone.0171814
201. Jozwik M, Jozwik M, Teng C, Jozwik M, Battaglia FC. Human breast milk sugars and polyols over the first 10 puerperium days. Am J Hum Biol. (2013) 25:198–204. doi: 10.1002/ajhb.22352
202. Lonnerdal B. Human milk proteins: key components for the biological activity of human milk. Adv Exp Med Biol. (2004). 554:11–25. doi: 10.1007/978-1-4757-4242-8_4
203. van't Hof MA, Haschke F, Darvay S. Euro-Growth references on increments in length, weight, and head and arm circumferences during the first 3 years of life. Euro-Growth Study Group. J Pediatr Gastroenterol Nutr. (2000) 31(Suppl 1):S39–47. doi: 10.1097/00005176-200007001-00004
204. Hester SN, Hustead DS, Mackey AD, Singhal A, Marriage BJ. Is the macronutrient intake of formula-fed infants greater than breast-fed infants in early infancy? J Nutr Metab. (2012) 2012:891201. doi: 10.1155/2012/891201
205. Lonnerdal B. Nutritional and physiologic significance of human milk proteins. Am J Clin Nutr. (2003) 77:1537S−43S. doi: 10.1093/ajcn/77.6.1537S
206. Kunz C, Lonnerdal B. Re-evaluation of the whey protein/casein ratio of human milk. Acta Paediatr. (1992) 81:107–12. doi: 10.1111/j.1651-2227.1992.tb12184.x
207. Rai D, Adelman AS, Zhuang W, Rai GP, Boettcher J, Lonnerdal B. Longitudinal changes in lactoferrin concentrations in human milk: a global systematic review. Crit Rev Food Sci Nutr. (2014) 54:1539–47. doi: 10.1080/10408398.2011.642422
208. Zhang Z, Adelman AS, Rai D, Boettcher J, Lonnerdal B. Amino acid profiles in term and preterm human milk through lactation: a systematic review. Nutrients. (2013) 5:4800–21. doi: 10.3390/nu5124800
209. Giuffrida F, Elmelegy IM, Thakkar SK, Marmet C, Destaillats F. Longitudinal evolution of the concentration of gangliosides GM3 and GD3 in human milk. Lipids. (2014) 49:997–1004. doi: 10.1007/s11745-014-3943-2
210. Szlagatys-Sidorkiewicz A, Zagierski M, Jankowska A, Luczak G, Macur K, Baczek T, et al. Longitudinal study of vitamins A, E and lipid oxidative damage in human milk throughout lactation. Early Hum Dev. (2012) 88:421–4. doi: 10.1016/j.earlhumdev.2011.10.007
211. Lipkie TE, Morrow AL, Jouni ZE, McMahon RJ, Ferruzzi MG. Longitudinal survey of carotenoids in human milk from urban cohorts in China, Mexico, the USA. PLoS ONE. (2015) 10:e0127729. doi: 10.1371/journal.pone.0127729
212. Krebs NF, Reidinger CJ, Hartley S, Robertson AD, Hambidge KM. Zinc supplementation during lactation: effects on maternal status and milk zinc concentrations. Am J Clin Nutr. (1995) 61:1030–6. doi: 10.1093/ajcn/61.5.1030
213. Greibe E, Lildballe DL, Streym S, Vestergaard P, Rejnmark L, Mosekilde L, et al. Cobalamin and haptocorrin in human milk and cobalamin-related variables in mother and child: a 9-mo longitudinal study. Am J Clin Nutr. (2013) 98:389–95. doi: 10.3945/ajcn.113.058479
214. Lavine ME, Clark RM, Hundrieser KE, Ferris AM. Within-day variation of lipolytic activity in human milk. J Dairy Sci. (1986) 69:1784–6. doi: 10.3168/jds.S0022-0302(86)80601-4
215. Freed LM, Neville MC, Hamosh P, Hamosh M. Diurnal and within-feed variations in lipase activity and triglyceride content of human milk. J Pediatr Gastroenterol Nutr. (1986) 5:938–42. doi: 10.1097/00005176-198611000-00021
216. Cox DB, Owens RA, Hartmann PE. Blood and milk prolactin and the rate of milk synthesis in women. Exp Physiol. (1996) 81:1007–20. doi: 10.1113/expphysiol.1996.sp003985
217. Kent JC, Mitoulas L, Cox DB, Owens RA, Hartmann PE. Breast volume and milk production during extended lactation in women. Exp Physiol. (1999) 84:435–47. doi: 10.1111/j.1469-445X.1999.01808.x
219. Engstrom JL, Meier PP, Jegier B, Motykowski JE, Zuleger JL. Comparison of milk output from the right and left breasts during simultaneous pumping in mothers of very low birthweight infants. Breastfeed Med. (2007) 2:83–91. doi: 10.1089/bfm.2006.0019
220. Hill PD, Aldag JC, Zinaman M, Chatterton RT Jr. Comparison of milk output between breasts in pump-dependent mothers. J Hum Lact. (2007) 23:333–7. doi: 10.1177/0890334407307575
221. Bourne VJ, Todd BK. When left means right: an explanation of the left cradling bias in terms of right hemisphere specializations. Dev Sci. (2004) 7:19–24. doi: 10.1111/j.1467-7687.2004.00318.x
222. Neville MC, Keller R. Accuracy of single- and two-feed test weighing in assessing 24 h breast milk production. Early Hum Dev. (1984) 9:275–81. doi: 10.1016/0378-3782(84)90038-0
223. Fetherston CM, Lai CT, Hartmann PE. Relationships between symptoms and changes in breast physiology during lactation mastitis. Breastfeed Med. (2006) 1:136–45. doi: 10.1089/bfm.2006.1.136
224. Daly SE, Owens RA, Hartmann PE. The short-term synthesis and infant-regulated removal of milk in lactating women. Exp Physiol. (1993) 78:209–20. doi: 10.1113/expphysiol.1993.sp003681
226. Gunther M, Stanier JE. Diurnal variation in the fat content of breast-milk. Lancet. (1949) 2:235–7. doi: 10.1016/S0140-6736(49)91242-8
227. Jackson DA, Imong SM, Silprasert A, Ruckphaopunt S, Woolridge MW, Baum JD, et al. Circadian variation in fat concentration of breast-milk in a rural Northern Thai population. Br J Nutr. (1988) 59:349–63. doi: 10.1079/BJN19880044
228. Lammi-Keefe CJ, Ferris AM, Jensen RG. Changes in human milk at 0600, 1000, 1400, 1800, and 2200 H. J Pediatr Gastroenterol Nutr. (1990) 11:83–8. doi: 10.1097/00005176-199007000-00017
229. Lubetzky R, Littner Y, Mimouni FB, Dollberg S, Mandel D. Circadian variations in fat content of expressed breast milk from mothers of preterm infants. J Am Coll Nutr. (2006) 25:151–4. doi: 10.1080/07315724.2006.10719526
230. Moran-Lev H, Mimouni FB, Ovental A, Mangel L, Mandel D, Lubetzky R. Circadian macronutrients variations over the first 7 weeks of human milk feeding of preterm infants. Breastfeed Med. (2015) 10:366–70. doi: 10.1089/bfm.2015.0053
231. Stafford J, Villalpando S, Aguila BU. Circadian variation and changes after a meal in volume and lipid production of human milk from rural Mexican women. Ann Nutr Metab. (1994) 38:232–7. doi: 10.1159/000177816
232. Garza C, Butte NF. Energy concentration of human milk estimated from 24-h pools and various abbreviated sampling schemes. J Pediatr Gastroenterol Nutr. (1986) 5:943–8. doi: 10.1097/00005176-198611000-00022
233. Singh RK, Nakra VK, Pandey HN, Arora SR. Studies on circadian periodicity of plasma, breast milk and urinary calcium in lactating Indian women. Trop Geogr Med. (1984) 36:345–9.
234. Krebs NF, Hambidge KM, Jacobs MA, Mylet S. Zinc in human milk: diurnal and within-feed patterns. J Pediatr Gastroenterol Nutr. (1985) 4:227–9. doi: 10.1097/00005176-198504000-00012
235. Gillies ME, Neill AE. Variations in the mineral concentrations in breast milk during a single nursing, diurnally and on consecutive days. Hum Nutr Appl Nutr. (1985) 39:370–5.
236. Karra MV, Kirksey A. Variation in zinc, calcium, and magnesium concentrations of human milk within a 24-hour period from 1 to 6 months of lactation. J Pediatr Gastroenterol Nutr. (1988) 7:100–6. doi: 10.1097/00005176-198801000-00019
237. Hussain M, Sikder ZU, Wahed MA, Haque AT, Jahan F. Zinc concentration of breast milk and its diurnal variation in Bangladeshi mothers. Bangladesh Med Res Counc Bull. (1996) 22:70–3.
238. Cohen RS, McCallie KR. Feeding premature infants: why, when, and what to add to human milk. JPEN J Parenter Enteral Nutr. (2012) 36(Suppl. 1):20–4S. doi: 10.1177/0148607111421342
239. Katzer D, Pauli L, Mueller A, Reutter H, Reinsberg J, Fimmers R, et al. Melatonin concentrations and antioxidative capacity of human breast milk according to gestational age and the time of day. J Hum Lact. (2016) 32:NP105–10. doi: 10.1177/0890334415625217
240. Daly SE, Di Rosso A, Owens RA, Hartmann PE. Degree of breast emptying explains changes in the fat content, but not fatty acid composition, of human milk. Exp Physiol. (1993) 78:741–55. doi: 10.1113/expphysiol.1993.sp003722
241. Jackson DA, Imong SM, Silprasert A, Preunglumpoo S, Leelapat P, Yootabootr Y, et al. Estimation of 24 h breast-milk fat concentration and fat intake in rural Northern Thailand. Br J Nutr. (1988) 59:365–71. doi: 10.1079/BJN19880045
242. Becker GE, Smith HA, Cooney F. Methods of milk expression for lactating women. Cochrane Database Syst Rev. 2015:CD006170. doi: 10.1002/14651858.CD006170.pub4
243. Lussier MM, Brownell EA, Proulx TA, Bielecki DM, Marinelli KA, Bellini SL, et al. Daily breastmilk volume in mothers of very low birth weight neonates: a repeated-measures randomized trial of hand expression versus electric breast pump expression. Breastfeed Med. (2015) 10:312–7. doi: 10.1089/bfm.2015.0014
244. Lang S, Lawrence CJ, Orme RL. Sodium in hand and pump expressed human breast milk. Early Hum Dev. (1994) 38:131–8. doi: 10.1016/0378-3782(94)90224-0
245. Mangel L, Ovental A, Batscha N, Arnon M, Yarkoni I, Dollberg S. Higher fat content in breastmilk expressed manually: a randomized trial. Breastfeed Med. (2015) 10:352–4. doi: 10.1089/bfm.2015.0058
246. Morton J, Wong RJ, Hall JY, Pang WW, Lai CT, Lui J, et al. Combining hand techniques with electric pumping increases the caloric content of milk in mothers of preterm infants. J Perinatol. (2012) 32:791–6. doi: 10.1038/jp.2011.195
247. Pines N, Mandel D, Mimouni FB, Moran Lev H, Mangel L, Lubetzky R. The effect of between-breast differences on human milk macronutrients content. J Perinatol. (2016) 36:549–551. doi: 10.1038/jp.2016.17
248. Chang YC, Chen CH, Lin MC. The macronutrients in human milk change after storage in various containers. Pediatr Neonatol. (2012) 53:205–9. doi: 10.1016/j.pedneo.2012.04.009
249. Lindquist S, Hernell O. Lipid digestion and absorption in early life: an update. Curr Opin Clin Nutr Metab Care. (2010) 13:314–20. doi: 10.1097/MCO.0b013e328337bbf0
250. Morera Pons S, Castellote Bargallo AI, Lopez Sabater MC. Evaluation by high-performance liquid chromatography of the hydrolysis of human milk triacylglycerides during storage at low temperatures. J Chromatogr A. (1998) 823:467–74. doi: 10.1016/S0021-9673(98)00273-8
251. Lev HM, Ovental A, Mandel D, Mimouni FB, Marom R, Lubetzky R. Major losses of fat, carbohydrates and energy content of preterm human milk frozen at−80 degrees C. J Perinatol. (2014) 34:396–8. doi: 10.1038/jp.2014.8
252. Lozano B, Castellote AI, Montes R, Lopez-Sabater MC. Vitamins, fatty acids, and antioxidant capacity stability during storage of freeze-dried human milk. Int J Food Sci Nutr. (2014) 65:703–7. doi: 10.3109/09637486.2014.917154
253. Buss IH, McGill F, Darlow BA, Winterbourn CC. Vitamin C is reduced in human milk after storage. Acta Paediatr. (2001) 90:813–5. doi: 10.1080/080352501750315753
254. Marín ML, Arroyo R, Jiménez E, Gómez A, Fernández L, Rodríguez JM. Cold storage of human milk: effect on its bacterial composition. J Pediatr Gastroenterol Nutr. (2009) 49:343–8. doi: 10.1097/MPG.0b013e31818cf53d
255. Ramirez-Santana C, Perez-Cano FJ, Audi C, Castell M, Moretones MG, Lopez-Sabater MC, et al. Effects of cooling and freezing storage on the stability of bioactive factors in human colostrum. J Dairy Sci. (2012) 95:2319–25. doi: 10.3168/jds.2011-5066
256. Berkow SE, Freed LM, Hamosh M, Bitman J, Wood DL, Happ B, et al. Lipases and lipids in human milk: effect of freeze-thawing and storage. Pediatr Res. (1984) 18:1257–62. doi: 10.1203/00006450-198412000-00006
257. Takahashi K, Mizuno K, Itabashi K. The freeze-thaw process and long intervals after fortification denature human milk fat globules. Am J Perinatol. (2012) 29:283–8. doi: 10.1055/s-0031-1295659
258. Fusch G, Rochow N, Choi A, Fusch S, Poeschl S, Ubah AO, et al. Rapid measurement of macronutrients in breast milk: how reliable are infrared milk analyzers? Clin Nutr. (2015) 34:465–76. doi: 10.1016/j.clnu.2014.05.005
259. ISO 5725-1-5 Accuracy (Trueness and Precision) of Measurements Method and Results. Geneva: ISO Organization (1994).
260. Nichols BL. Atwater and USDA nutrition research and service: a prologue of the past century. J Nutr. (1994) 124(Suppl. 9):1,718–27s. doi: 10.1093/jn/124.suppl_9.1718S
261. Boyce C, Watson M, Lazidis G, Reeve S, Dods K, Simmer K, et al. Preterm human milk composition: a systematic literature review. Br J Nutr. (2016) 116:1033–45. doi: 10.1017/S0007114516003007
262. Keller RP, Neville MC. Determination of total protein in human milk: comparison of methods. Clin Chem. (1986) 32:120–3. doi: 10.1093/clinchem/32.1.120
263. Hambraeus L, Forsum E, Abrahamsson L, Lonnerdal B. Automatic total nitrogen analysis in nutritional evaluations using a block digestor. Anal Biochem. (1976) 72:78–85. doi: 10.1016/0003-2697(76)90508-X
264. Lonnerdal B, Forsum E, Hambraeus L. The protein content of human milk. I. a transversal study of Swedish normal material. Nutr Rep Int. (1976) 13:125–34.
265. Casadio YS, Williams TM, Lai CT, Olsson SE, Hepworth AR, Hartmann PE. Evaluation of a mid-infrared analyzer for the determination of the macronutrient composition of human milk. J Hum Lact. (2010) 26:376–83. doi: 10.1177/0890334410376948
266. Billard H, Simon L, Desnots E, Sochard A, Boscher C, Riaublanc A, et al. Calibration adjustment of the mid-infrared analyzer for an accurate determination of the macronutrient composition of human milk. J Hum Lact. (2016) 32:Np19–27. doi: 10.1177/0890334415588513
267. Silvestre D, Fraga M, Gormaz M, Torres E, Vento M. Comparison of mid-infrared transmission spectroscopy with biochemical methods for the determination of macronutrients in human milk. Matern Child Nutr. (2014) 10:373–82. doi: 10.1111/j.1740-8709.2012.00431.x
268. Lonnerdal B, Woodhouse LR, Glazier C. Compartmentalization and quantitation of protein in human milk. J Nutr. (1987) 117:1385–95. doi: 10.1093/jn/117.8.1385
269. Bergqvist Y, Karlsson L, Fohlin L. Total protein determined in human breast milk by use of coomassie brilliant blue and centrifugal analysis. Clin Chem. (1989) 35:2127–9. doi: 10.1093/clinchem/35.10.2127
270. Folch J, Lees M, Sloane Stanley GH. A simple method for the isolation and purification of total lipides from animal tissues. J Biol Chem. (1957) 226:497–509.
271. Bligh EG, Dyer WJ. A rapid method of total lipid extraction and purification. Can J Biochem Physiol. (1959) 37:911–7. doi: 10.1139/o59-099
272. Association of Official Analytical Chemists. Methods of Analysis of the Association of Official Analytical Chemists. 11th ed. Washington, DC (1979).
273. Kleyn DH, Lynch JM, Barbano DM, Bloom MJ, Mitchell MW. Determination of fat in raw and processed milks by the Gerber method: collaborative study. J AOAC Int. (2001) 84:1499–508. doi: 10.1093/jaoac/84.5.1499
Keywords: human milk, lactation, maternal, infant, human milk sampling, standardization, human milk composition
Citation: Samuel TM, Zhou Q, Giuffrida F, Munblit D, Verhasselt V and Thakkar SK (2020) Nutritional and Non-nutritional Composition of Human Milk Is Modulated by Maternal, Infant, and Methodological Factors. Front. Nutr. 7:576133. doi: 10.3389/fnut.2020.576133
Received: 25 June 2020; Accepted: 19 August 2020;
Published: 16 September 2020.
Edited by:
Daniel Cozzolino, University of Queensland, AustraliaReviewed by:
Giuseppe Annunziata, University of Naples Federico II, ItalyJorry Dharmawan, Singapore Institute of Technology, Singapore
Copyright © 2020 Samuel, Zhou, Giuffrida, Munblit, Verhasselt and Thakkar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sagar K. Thakkar, c2FnYXIudGhha2thckByZC5uZXN0bGUuY29t
†These authors have contributed equally to this work and share first authorship
‡Present address: Qianling Zhou, Department of Maternal and Child Health, School of Public Health, Peking University, Beijing, China