 Jani P. Vaara
Jani P. Vaara Tommi Vasankari
Tommi Vasankari Harri J. Koski
Harri J. Koski Heikki Kyröläinen
Heikki Kyröläinen- 1Department of Leadership and Military Pedagogy, National Defense University, Helsinki, Finland
- 2UKK Institute of Health Promotion Research, Tampere, Finland
- 3Finnish Defence Forces, Helsinki, Finland
- 4Faculty of Sport and Health Sciences, University of Jyvaskyla, Jyväskylä, Finland
Background: There are only a few studies that have assessed awareness and knowledge regarding aerobic type of physical activity (PA) guidelines recommendations, while no previous studies have examined muscular type of activity recommendation guidelines. The aim was to assess knowledge and awareness and study the associations with demographic variables and physical activity and fitness.
Methods: Participants were 776 young (age 26 ± 7 years) men. Awareness and knowledge of PA recommendation guidelines were assessed by prompted questionnaires together with demographic variables and physical activity. In addition, physical fitness was measured.
Results: Forty percent of the participants reported being aware of the physical activity recommendation. Moreover, 7% correctly identified the recommendations for moderate aerobic physical activity and 25% for muscular type of activity. In addition, 4% correctly identified both aerobic and muscular activity recommendations. Being aware of the PA recommendations was associated with being married or partnered, having higher education level and being more physically active during leisure-time (p < 0.05). Individuals with no awareness of the recommendations had lower results in cardiorespiratory and muscular fitness compared to those being aware (p < 0.05). Being married or partnered was positively associated with the knowledge of the muscular activity recommendations (p < 0.05). Moreover, the individuals with correct knowledge of the PA recommendations had higher levels of muscular fitness (p < 0.05).
Conclusion: A low number of individuals are aware or know the physical activity recommendations among young adult men. Therefore, more vigorous attempts to promote physical activity recommendations are needed.
Introduction
Physical activity (PA) is an important factor in health promotion and disease prevention, and physical inactivity is linked with many chronic diseases and their risk factors (1). Therefore, PA recommendations have been established in order to give information to people of what is, in general, a minimum amount of PA to improve health. The aim is to increase knowledge, which would optimally to be reflected in PA behavior. The first PA recommendations were established in the publication of “Guidelines for Graded Exercise Testing and Exercise Prescription” in 1975 (2) and the recommendations were mostly aim to develop cardiorespiratory fitness. In 1990's the PA recommendations also included health-related aspects emphasizing also moderate intensity physical activity with the mention of accumulating physical activity from shorter bouts (≥10 min). These recommendations concluded that adults should accumulate 30 min or more on most days of the week (3). In addition, muscular strength was mentioned for the first time in the recommendations although no specific recommendations were then stated.
Since the early years of the first recommendations, accumulating study results had modified the content and emphasis of the recommendations. The recommendations: “Physical Activity Guidelines for Americans” introduced in 2008 (4) and “Global recommendations on Physical Activity and Health” from WHO introduced in 2010 (5) stated that the minimum recommended amount of PA for adults is aerobic activity either 2 h 30 min per week at moderate-intensity or 1 h and 15 min at vigorous-intensity, which could be accumulated from 10 min activity bouts. In addition, muscular strength and muscular endurance should be performed twice a week. The Finnish physical activity recommendation is based on the “Physical Activity Guidelines for Americans” and was introduced in 2009. In 2018, the “Physical Activity Guidelines for Americans” were revisited. The basic recommendations, mentioned above, stayed the same, however, the borderline of accumulating 10 min activity was excluded and the recommendations states that any activity counts (6).
Considering the accumulating research evidence of beneficial effects of PA from numerous studies during the recent decades, it is surprising how few studies have assessed awareness and knowledge of the recommendations. One of the first studies to assess knowledge of the recommendations was reported by Bennett et al. (7). They reported that 33% of the US adult study sample correctly identified the recommendations for moderate-intensity PA based on recommendations from 1995. Moreover, Moore et al. (8) observed that among 10,000 US adults 26% correctly identified the recommendations from 1995 considering moderate-intensity PA. Moreover, further studies have observed that the knowledge of the recommendations can vary from as less as 1% in a US study population (9) to 8–18% in UK study samples (10–12). In addition to knowledge of PA recommendations, previous studies have found that the proportions of those being aware of the recommendations, varies between 4 and 43% (9, 13–17).
The earlier studies have solely concentrated on studying the knowledge and awareness of the aerobic PA recommendations, whereas the knowledge of muscular type of activity, which is recommended by the present recommendations, have not yet been studied. Therefore, the aim of the present study was to assess awareness and knowledge of the PA recommendations both for aerobic and muscular type of activities. Moreover, the premise for the awareness and knowledge of the physical activity recommendations is that they would optimally be reflected in physical activity behavior. As physical activity is related to improved physical fitness and body composition it is of interest whether these variables are also associated with the awareness and knowledge of the recommendations. The secondary purpose was therefore to study the associations of demographic variables, body mass index (BMI), PA, and physical fitness with awareness, and knowledge of the recommendations. From a national perspective, this is a novel study assessing awareness and knowledge of PA recommendations in a Finnish study sample consisting of young adult men.
Methods
Participants
Participants were 776 young (age 26 ± 7 years) adult Finnish men, who were invited in the military refresher training organized by the Finnish Defense Forces. The call up to military refresher training and information about the study plan for participants were sent to participants 5 months before the study conduction, which were carried out in 7 different sessions during 2015. The study protocol was explained in detail to the participants before they gave their written consent. The study was approved by the ethical committees of the University of Jyväskylä and the Central Finland Health Care District, as well as the Headquarters of the Finnish Defense Forces (AM5527). Altogether, 1,106 men were called up and 823 could participate in the military refresher training (response rate 74%). The most typical reasons for non-participation to the military refresher training were related to personal reasons in life, such as work-, study-, or health-related issues. Among those men who participated in the military refresher training 32 refused to take part in the study (response rate 96%). The study sample was compared with corresponding cohorts of 20–30 years old Finnish men in the national register data (Statistics Finland) from the year 2014 for education and place of residence. Based on these analyses, the current study sample can be considered to represent a young adult Finnish man with the following limitations: Northern and Southern Finland were slightly over-represented and the proportion of those participants who had studied 13 years or more was slightly over-represented.
Assessment of Knowledge and Awareness of Physical Activity Recommendations
Knowledge and awareness of physical activity recommendations were assessed by a questionnaire similar to previous studies (7, 10, 11, 14). To assess awareness of the recommendations participants were asked whether they have seen, heard or read about physical activity recommendations? The answer options were: (1) yes, (2) no, and (3) I don't know. For knowledge of the recommendations participants were asked: “What is the recommended minimum amount of moderate-intensity aerobic physical activity per week based on the present physical activity recommendations.” The answer options were as follows: (1) 1 h 30 min, (2) 2 h 30 min, (3) 3 h, (4) 20 min per day 3 days per week, (5) 30 min per day 5 days per week, (6) 30 min per day 7 days per week, (7) 60 min per day 7 days per week, (8) none of the previous options, (9) I don't know. Furthermore, Participants were asked: “What is the recommended minimum amount of muscular strength and endurance type of activity per week based on the present physical activity recommendations.” The answer options were: (1) once per week, (2) 2 times per week, (3) 3 times per week, (4) 4 times per week, (5) 5 times per week, (6) none of the previous options, (7) I don't know. Moreover, based on the answers given, further classifications were modulated as correct knowledge (answer 2, 5), under estimation (answers 1, 4), overestimation (answers 3, 6, 7) for moderate-intensity aerobic activity knowledge and for muscular type of activity knowledge: correct knowledge (answer 2), under estimation (answers 1), over estimation (answers 3–5). Regarding moderate-intensity aerobic PA, answer option 5 (30 min per day 5 days per week) was classified as correct answer, although it is correct only based on the amount and not by the frequency of the present physical activity recommendations.
Demographic and Background Variables
Demographic variables were assessed by a questionnaire: age, marital status (married/partnered, divorced/widowed, never married), education (≤9, 10–12, 13–15, ≥16 years), employment status (employed, student, unemployed, or other), and smoking (smoker, quit smoking, non-smoker).
Assessment of Self-Reported Physical Activity
Leisure-time physical activity (LTPA) was assessed with the following question: “Which of the following definitions best describe your leisure time physical activity habits?”—(“Think of the last 3 months and consider all LTPA that lasted at least 20 min per session”). Response categories were (1) less than once a week; (2) no vigorous activities, but light or moderate physical activity at least once a week (if more often than once please define the numbers per week in an open space); (3), vigorous activity once a week; (4) vigorous activity twice a week; (5) vigorous activity 3 times a week; (6) vigorous activity at least 4 times a week. LTPA was classified as low (responses 1 or 2), moderate (responses 3 or 4), and high (responses 5 or 6) activity (18). The LTPA question used in the present study has been validated against fitness, observing that vigorous physical activity showed a consistent dose-response relationship with cardiorespiratory and muscular fitness (19). In general, acceptable to good reliability but poor to moderate validity has been reported for physical activity questionnaires (20).
Physical Fitness
The participants performed the physical fitness tests in the following order: standing long jump, isometric maximal force, cardiorespiratory fitness, and muscular endurance tests. All of the participants were familiar with the standing long jump test and muscular endurance tests because those tests have been conducted during their military service.
Standing Long Jump Test
Standing long jump test was used to test explosive force production of lower extremities (21). The participants were instructed of the correct technique prior the testing, and each of them performed several jumps after a warm-up and prior the testing, which was performed in the specifically designed gym mat. The warm-up lasted 10 min and consisted of calisthenics exercises, such as x-jumps, push-ups, sit-ups, squats, planks, and countermovement jumps. The participants were instructed to jump (horizontally) forward as far as possible from a standing position, using a prior countermovement and hands freely swinging by their sides without falling backward upon bilateral landing. The participants completed 3 trials each interspersed by a 1-min rest period. The performance was measured with 1 cm precision.
Maximal Isometric Force
Maximal isometric force was measured with horizontal bench press (both regarded as tests for maximal strength) using a dynamometer. Knee angle was set to 107° with a goniometer, and hands were placed on a handle grip in a leg extension test (22). During the maximal bench press test, the participants were in supine position with their backs flat on a bench and feet flat on the floor with elbow and shoulder positioned at 90°. A warm-up series of at least 2 submaximal sets were done prior to maximal sets. Three trials were performed using a 30-s recovery period. The best performance was included in the analysis. Each participant was advised to produce maximal force as fast as possible and to maintain it for 3 s. The participants were verbally encouraged during the maximal efforts by the test personnel. The repeatability has been reported to be high in maximal isometric strength tests (r = 0.98, C.V = 4.1%) (23).
Cardiorespiratory Fitness
Cardiorespiratory fitness (VO2 max) was determined using an indirect graded cycle ergometer test (Ergoline 800S, Ergoselect 100K, Ergoselect 200K, Bitz, Germany) until exhaustion. A progressive protocol was used, which initially started at a power output of 50 W and was increased 25 W every 2 min until exhaustion. Heart rate (HR) was continuously recorded during the test (Polar Vantage NV or S610, S710, or S810, Kempele, Finland). Predicted VO2 max was estimated from HR and maximal power (W) (Fitware, Mikkeli, Finland) with the following equation: VO2 max (ml·kg−1·min−1) = 12.35 × Pmax/kg + 3.5, where Pmax is maximal power and kg is body mass in kg. The intra class correlation has been reported to be high with this method (24).
Muscular Endurance Tests
Muscular endurance tests consisted of push-ups and sit-ups (repetitions/minute). The push-up test measured the performance of arm and shoulder extensor muscles. Before taking a starting position, the participants laid face down on the floor, feet parallel at pelvis to shoulder width and hands positioned so that thumbs could reach the shoulders while other fingers were pointing forward. Before the beginning of the test, the participants were instructed to extend their arms to the starting position and keep the feet, trunk, and the shoulders in the same line throughout the test. One successful repetition was counted when the participant lowered his torso by flexing arms to an elbow angle of 90° and returned to the starting position by extending his arms. Sit-up test was used to measure performance of abdominal and hip flexor muscles. In the starting position, the participants laid on his back while legs were supported from the ankles by an assistant. The knees were flexed at the angle of 90°, elbows pointing upward and fingers crossed behind the back of the head. One successful repetition was determined when the participant lifted his upper body from the starting position and brought elbows to the knee-level. The result of the test was expressed as a number of consecutive successful repetitions during 60 s. There was a recovery period of 5-min between the tests. Correct technique was demonstrated to participants before each test and only the trials with adequate technique were accepted. The test-retest reliability of push-up, sit-up, and repeated squat tests has been reported to be high among young adults and middle-aged adults (ICC = 0.93–0.95, ICC = 0.83–0.93, r = 0.95, respectively) (25, 26).
Body Composition
Body weight was measured to the nearest 0.1 kg and body height by a commercial scale to the nearest 0.1 cm, and further BMI was calculated.
Statistical Analysis
Data was analyzed with IBM SPSS Statistics 22.0.0.0. Descriptive statistics as frequencies, means, standard deviations and 95% confidence intervals were calculated and are presented in the tables. χ2 -tests were used to explore the associations of marital status, employment status, smoking, and PA with the awareness and knowledge of the recommendations. For continuous variables age, BMI, and physical fitness tests, the difference of means in awareness and knowledge of recommendations were assessed with analysis of variance using Bonferroni post hoc tests. Moreover, those parameters that were not normally distributed were log-transformed (maximal isometric force of upper and lower extremities).
Results
The background characteristics of the study participants is presented in the Table 1. Forty percent of the participants reported being aware and 27% not being aware of the PA recommendations. Table 2 reveals that 7% correctly identified the recommendation for moderate aerobic PA and 25% for muscular type of activity. The proportion of those who correctly identified both aerobic and muscular activity recommendations was 4% (n = 31). In addition, 16% overestimated and 25% underestimated the recommended aerobic PA and 3% underestimated and 37% overestimated the recommended muscular type of activity.
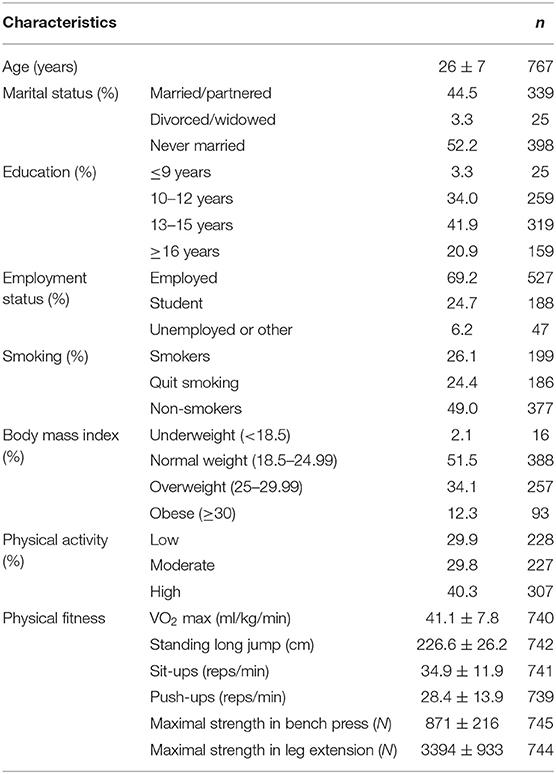
Table 1. Demographic characteristics (%), physical activity (%), and fitness (mean ± SD) of the study participants.
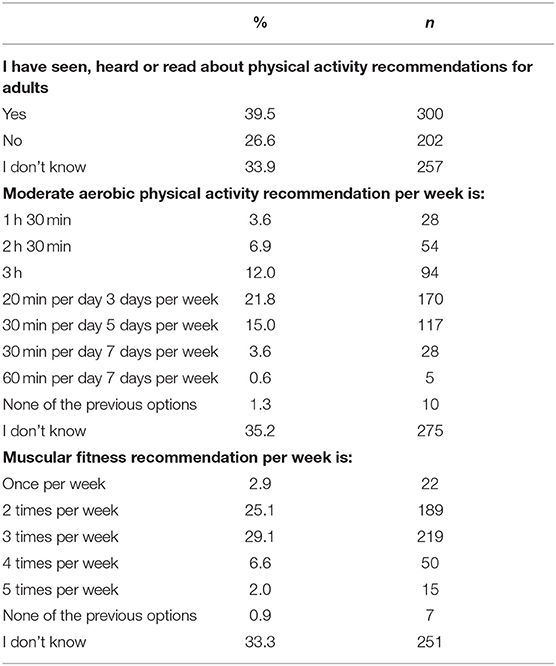
Table 2. Distributions of answers regarding awareness and knowledge of the physical activity recommendations.
Marital status (married/partnered), education level and leisure-time PA were positively associated with awareness of the recommendations (Table 3). Table 3 further demonstrates that those individuals with no awareness of the PA recommendations had lower results in cardiorespiratory fitness and sit-ups compared to those individuals being aware (p < 0.05) or those who answered don't know (p < 0.05). Furthermore, individuals with no awareness of the PA recommendations had lower results in push-ups and maximal strength of upper extremities compared to those individuals being aware (p < 0.05).
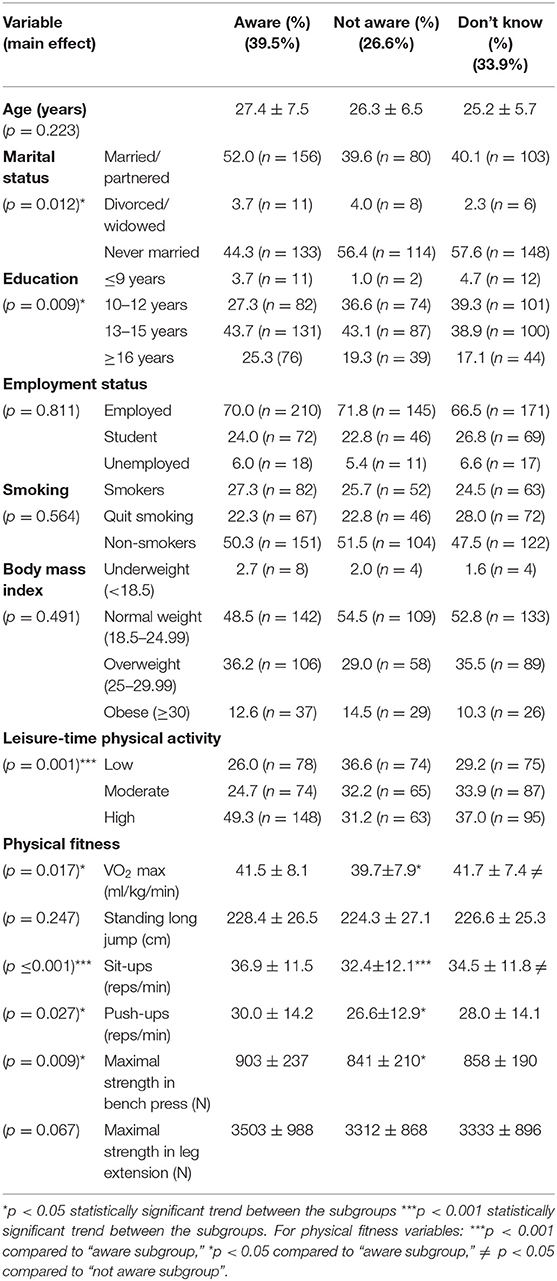
Table 3. The distributions and mean ± sd of those of being aware, not aware and those who don't know of the physical activity recommendations according to demographic variables, body composition, and physical activity and fitness.
Marital status (married/partnered) was positively associated with the knowledge of muscular type of activity recommendations (Table 5) but not with moderate aerobic PA recommendations (Table 4). Regarding knowledge of moderate aerobic PA recommendations, those who responded “don‘t know” had lower results in standing long jump compared to those individuals with correct knowledge (p < 0.05) and lower results in sit-ups compared to those individuals with correct knowledge (p < 0.05) and those who overestimated the PA recommendations (p < 0.05) (Table 4).
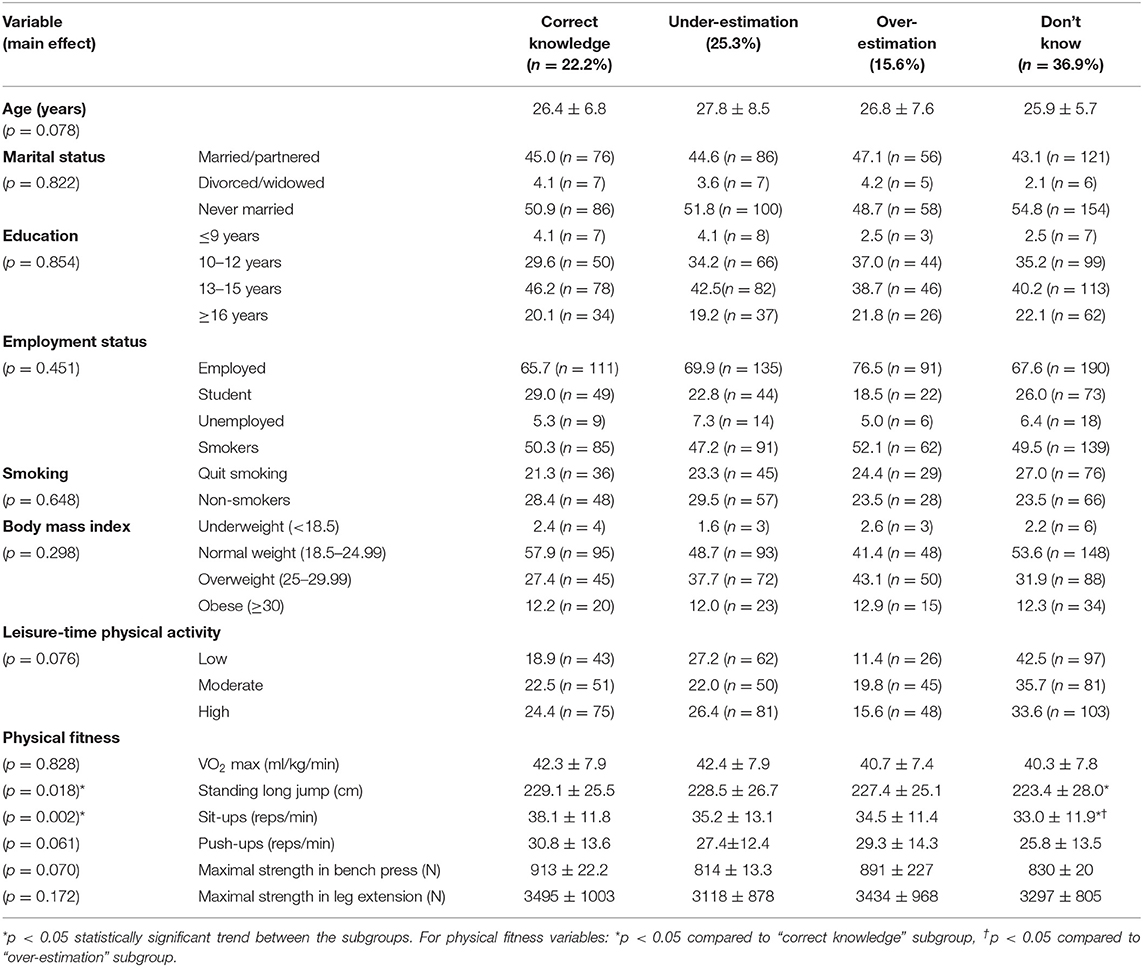
Table 4. The distributions and mean ± sd of correct, unsure, and over- and under-estimation of the moderate aerobic physical activity recommendations according to demographic variables, body composition, and physical activity and fitness.
Regarding knowledge of muscular type of PA recommendations, those who responded “don't know” had lower results in push-ups and maximal strength of upper extremities compared to those individuals with correct knowledge (p < 0.05) and those who overestimated the PA recommendations (p < 0.05) (Table 5). Moreover, those individuals who responded “don't know” and those who overestimated the muscular type of PA recommendations had lower results in sit-ups compared to individuals with correct knowledge (p < 0.05) (Table 5).
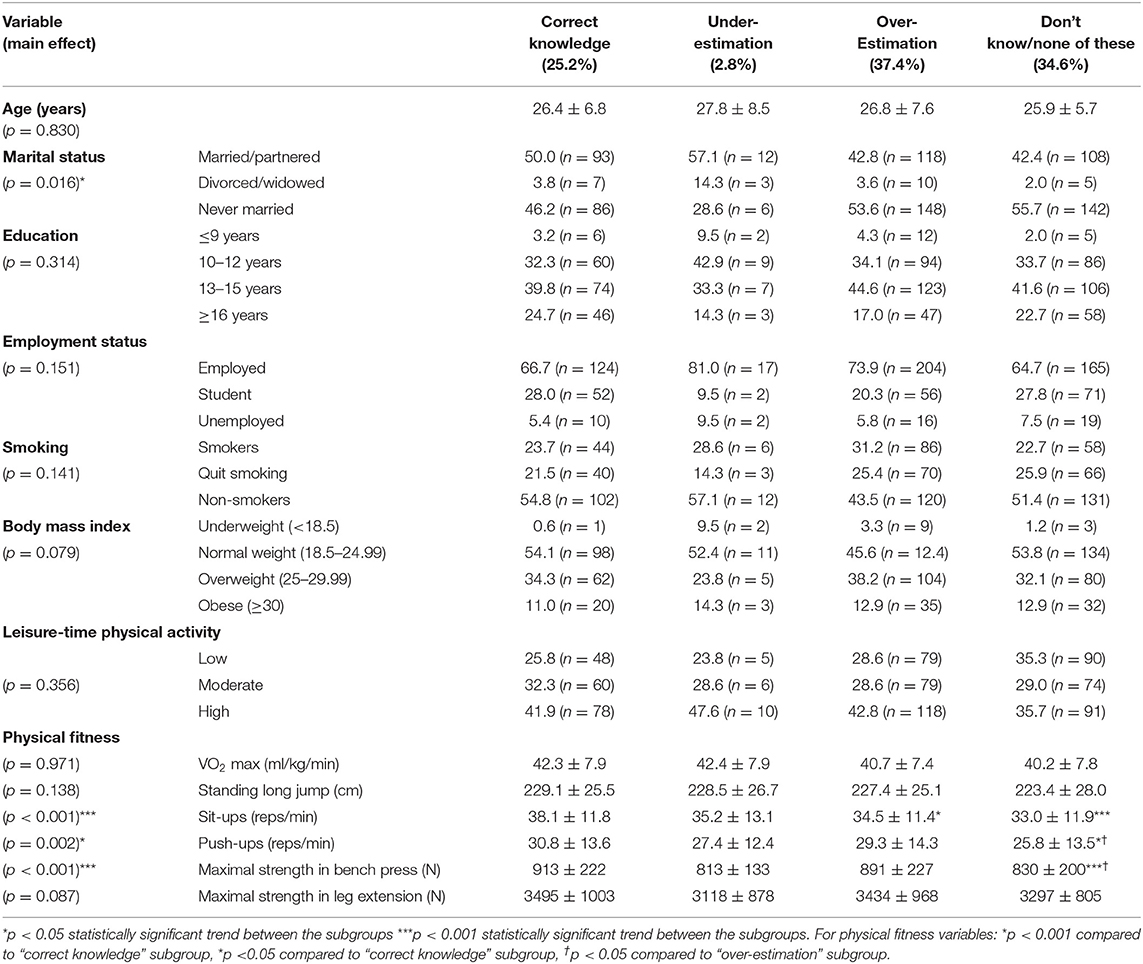
Table 5. The distributions and mean ± sd of correct, unsure, and over- and under-estimation of the muscular strength and muscular endurance recommendations according to demographic variables, body composition, and physical activity and fitness.
Discussion
Although 40% of the young adult Finnish men reported being aware of the present PA recommendations only 7% correctly identified the recommendation for moderate aerobic PA and 25% for muscular type of activity recommendation. Moreover, 4% correctly identified both moderate intensity aerobic and muscular type of activity recommendations. Marital status, education, leisure-time PA, and selected fitness variables were positively associated with awareness, whereas selected fitness variables were positively associated with correct knowledge of both aerobic and muscular PA recommendations.
The present study results showed higher awareness of the recommendations compared to most of the previous studies, where the prevalence rates have ranged from 4 to 37% (9, 13, 15). In addition, the previous studies have observed associations of age (9, 13, 16), education (9, 13, 15), gender (9, 13, 15), PA level (13), and ethnicity (9) with awareness. These previous studies do, therefore, suggest that when planning to develop awareness of PA recommendations a specific effort may be needed to target individuals in different subgroups. The present study suggests that inactive or unfit individuals, those with low education level and those not being married or partnered could be specific target groups for PA promotion compared to their counterparts among young adult men. However, it should be noted that on average, considering the present and earlier studies, there are far more individuals that are not aware of the recommendations compared to those who are aware and therefore, promotion of awareness should be vigorously attempted to whole population within its subgroups. Although professionals working with PA promotion generally have higher awareness of the recommendations than rest of the population one previous study (17) has revealed rather disappointing awareness among professionals (34%). Therefore, one of the priorities in raising awareness should also be to educate professionals as well.
Interestingly, despite the awareness of 40% of the present study sample, only 7% correctly identified moderate aerobic recommendations and 25% muscular type of activity recommendations. Nevertheless, if previous activity recommendations from 1995 (3) regarding aerobic PA was to be approved as a correct identification (30 min, 5 times per week) this proportion would have increased to 22%. Previous studies have shown highly varied prevalence of correct knowledge of the moderate aerobic PA recommendations ranging from <1 to 36% (7–12). In the present study, significant associations were observed between selected fitness variables and knowledge for both aerobic and muscular type of physical activity recommendations. In addition, marital status was related to knowledge of muscular type of activity recommendations. These results suggest that married individuals and individuals with higher fitness tend to know recommendations better than non-married individuals and individuals with lower fitness. Nevertheless, no causal relationships can be interpreted because of the cross-sectional study design. Therefore, it remains unknown whether the aware individuals have higher fitness because of the awareness or are they aware because of their higher fitness (a proxy for possibly higher interest in physical activity and fitness). Earlier studies have shown that age (11, 12, 14), education (9, 11, 12, 14), gender (7, 8, 13, 14), physical activity level (7, 8, 12, 13), ethnicity (8), income (8, 9, 12, 14), employment status (7, 11), and self-rated health (12) are associated with knowledge of the recommendations.
A higher number of individuals correctly identified muscular type of activity (25%) compared to moderate intensity aerobic activity (7%). This may be due to different answer options given or a speculatively a tendency of young adult men to be more interested in resistance training and its recommendations than aerobic exercise and recommendations. Nevertheless, if previous moderate aerobic PA recommendations would have been accepted as a correct alternative, based on its equal amount of activity (30 min, 5 times per week) altogether 22% of the participants would have been reported correct amount of moderate aerobic PA. Using this compound as a correct knowledge of aerobic activity recommendations we found that 22% of the study sample had correct knowledge, 25% underestimated, and 27% overestimated the moderate aerobic activity recommendations. The respective proportions for muscular type of activity recommendations were 22, 25, and 27%. Again, differences in given answer options in aerobic and muscular fitness questions may have affected the results because in the muscular type of activity question only exercise frequency was assessed, whereas aerobic activity question included different frequencies and volumes. The different assessment methods previous studies makes it hard to draw definite collective conclusions about the knowledge of the recommendations. However, of importance, some of the previous studies (8, 9, 12, 14) including the present study, have used prompted questionnaire, which may overestimate the prevalence of correct knowledge, whereas some other studies have used unprompted questionnaires (7, 10, 11, 14). The overestimation has been observed in a study by Cameron et al. (14), where they reported a significant difference between prompted and unprompted questions showing that the correct knowledge decreased from 37 to 4% when prompted and unprompted question format was compared. Therefore, the prevalence of knowledge of the earlier and the present study may actually be even less than reported given that prompted format was used.
A few practical conclusions regarding awareness and knowledge of the PA recommendations can be made based on the present and previous study findings. Firstly, based on low awareness and, especially, poor knowledge of the recommendations all attempts to raise awareness and knowledge should be made. Previous studies show that different methods to deliver health messages and health behavior change may work (27). The fact that the effect size of e.g., mass media campaigns on health behavior has turn out to be rather low emphasizes the need for multiple methods to raise awareness and knowledge. Besides community-wide campaigns, tools for dissemination could include e.g., social marketing through social media, online advertising and delivery of print products (28–30).
The strengths of the present study are a nationally representative study population targeted to young adult men. In addition, to the best of our knowledge, this is the first study that has investigated the knowledge of muscular type of activity recommendations. There are, however, some limitations in the current study. As noted earlier, prompted questionnaires were used in the present study, which may overestimate the proportions of knowledge and awareness individuals. Secondly, the present study did only assess knowledge of moderate-intensity aerobic physical activity recommendations and not vigorous aerobic physical activity. Therefore, future studies are warranted to assess all components of the present recommendations.
Conclusions
In conclusion, the present study revealed that 40% of the young adult Finnish men reported being aware of the present PA recommendations, however, only 7% correctly identified the recommendation for moderate aerobic activity and 25% for muscular fitness type of activity. Altogether, 4% correctly identified both moderate intensity aerobic and muscular type of activity recommendations. Marital status, education, LTPA, and selected fitness variables were positively associated with awareness, while selected fitness variables were positively associated with correct knowledge of both aerobic and muscular strength recommendations. These results underline a need to use multiple methods to raise awareness and knowledge of the physical activity recommendations among young adults.
Data Availability Statement
All datasets generated for this study are included in the article/supplementary material.
Ethics Statement
The studies involving human participants were reviewed and approved by the study was approved by the ethical committees of the University of Jyväskylä and the Central Finland Health Care District, as well as the Headquarters of the Finnish Defense Forces. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
JV performed experiments and analyzed data. JV, TV, HKo, and HKy conceived and designed the experiments, interpreted results of research, drafted, edited, critically revised paper, and approved final version of manuscript.
Funding
This work was supported by a grant from the Scientific Advisory Board for Defense.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank all the test personnel for their work in data collection and M.Sc. Elina Vaara for statistical guidance and analyses.
References
1. Booth FW, Roberts CK, Laye MJ. Lack of exercise is a major cause of chronic diseases. Compr Physiol. (2012) 2:1143–211. doi: 10.1002/cphy.c110025
2. American College of Sports Medicine. Guidelines for Graded Exercise Testing and Exercise Prescription. Philadelphia: Lea and Febiger (1975).
3. Pate RR, Pratt M, Blair SN, Haskell WL, Macera CA, Bouchard C, et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. (1995) 273:402–7. doi: 10.1001/jama.1995.03520290054029
4. Physical Activity Guidelines for Americans. (2008). Available online at: http://www.health.gov/PAGuidelines/ (accession December 21, 2018).
5. Global Recommendations on Physical Activity for Health. WHO (2010). Available online at: https://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (accession August 12, 2018).
6. Physical Activity Guidelines for Americans. 2nd ed. (2018). Available online at: https://health.gov/paguidelines/second-edition/pdf/Physical_Activity_Guidelines_2nd_edition.pdf (accession August 8, 2018).
7. Bennett GG, Wolin KY, Puleo EM, Mâsse LC, Atienza AA. Awareness of national physical activity recommendations for health promotion among US adults. Med Sci Sports Exerc. (2009) 41:1849–55. doi: 10.1249/MSS.0b013e3181a52100
8. Moore LV, Fulton J, Kruger J, McDivitt J. Knowledge of physical activity guidelines among adults in the United States, Health Styles 2003-2005. J Phys Act Health. (2010) 7:141–9. doi: 10.1123/jpah.7.2.141
9. Kay MC, Carroll DD, Carlson SA, Fulton JE. Awareness and knowledge of the 2008 physical activity guidelines for Americans. J Phys Act Health. (2014) 11:693–8. doi: 10.1123/jpah.2012-0171
10. Knox EC, Musson H, Adams EJ. Knowledge of physical activity recommendations in adults employed in England: associations with individual and workplace-related predictors. Int J Behav Nutr Phys Act. (2015) 23:69. doi: 10.1186/s12966-015-0231-3
11. Knox EC, Taylor IM, Biddle SJ, Sherar LB. Awareness of moderate-to-vigorous physical activity: can information on guidelines prevent overestimation? BMC Public Health. (2015) 17:392. doi: 10.1186/s12889-015-1705-6
12. Hunter RF, Tully MA, Donnelly P, Stevenson M, Kee F. Knowledge of UK physical activity guidelines: implications for better targeted health promotion. Prev Med. (2014) 65:33–9. doi: 10.1016/j.ypmed.2014.04.016
13. Plotnikoff RC, Lippke S, Johnson ST, Hugo K, Rodgers W, Spence JC. Awareness of Canada's physical activity guide to healthy active living in a large community sample. Am J Health Promot. (2011) 25:294–7. doi: 10.4278/ajhp.090211-ARB-60
14. Cameron C, Craig CL, Bull FC, Bauman A. Canada's physical activity guides: has their release had an impact? Can J Public Health. (2007) 98:161–9. doi: 10.1139/H07-106
15. Spence JC, Plotnikoff RC, Mummery WK. The awareness and use of Canada's physical activity guide to healthy active living. Can J Public Health. (2002) 93:394–6. doi: 10.1007/BF03404576
16. LeBlanc AG, Berry T, Deshpande S, Duggan M, Faulkner G, Latimer-Cheung AE, et al. Knowledge and awareness of Canadian physical activity and sedentary behaviour guidelines: a synthesis of existing evidence. Appl Physiol Nutr Metab. (2015) 40:716–24. doi: 10.1139/apnm-2014-0464
17. Bauman A, Finch C. Awareness and attitudes to the new physical activity recommendations – Perceptions of attenders of the 5th IOC World Congress on Sport Science. J Sci Med Sport. (2000) 3:493–501. doi: 10.1016/S1440-2440(00)80013-4
18. Vaara JP, Kyröläinen H, Fogelholm M, Santtila M, Häkkinen A, Häkkinen K, et al. Associations of leisure time, commuting, and occupational physical activity with physical fitness and cardiovascular risk factors in young men. J Phys Act Health. (2014) 11:1482–91. doi: 10.1123/jpah.2012-0504
19. Fogelholm M, Malmberg J, Suni J, Santtila M, Kyröläinen H, Mäntysaari M, et al. International physical activity questionnaire: validity against fitness. Med Sci Sports Exer. (2006) 38:753–60. doi: 10.1249/01.mss.0000194075.16960.20
20. Helmerhorst HJ, Brage S, Warren J, Besson H, Ekelund U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int J Behav Nutr Phys Act. (2012) 9:103. doi: 10.1186/1479-5868-9-103
21. Bosco C, Luhtanen P, Komi P. A simple method for measurement of mechanical power in jumping. Eur J Appl Physiol Occup Physiol. (1983) 50:273–82. doi: 10.1007/BF00422166
22. Häkkinen K, Häkkinen A. Neuromuscular adaptations during intensive strength training in middle aged and elderly males and females. Electromyogr Clin Neurophysiol. (1995) 35:137–47.
23. Viitasalo JT, Saukkonen S, Komi PV. Reproducibility of measurements of select-ed neuromuscular performance variables in man. Electromyogr Clin Neurophysiol. (1980) 20:487–501
24. Santtila MA, Häkkinen K, Pihlainen K, Kyröläinen H. Comparison between direct and predicted maximal oxygen uptake measurement during cycling. Mil Med. (2012) 178:234–8. doi: 10.7205/MILMED-D-12-00276
25. Augustsson SR, Bersås E, Thomas EM, Sahlberg M, Augustsson J, Svantesson U. Gender differences and reliability of selected physical performance tests in young women and men. Adv Physiother. (2009) 11:64–70. doi: 10.1080/14038190801999679
26. Alaranta H, Hurri H, Heliövaara M, Soukka A, Harju R. Non-dynamometric trunk performance tests: reliability and normative data. Scand J Rehabil Med. (1994) 26:211–5.
27. Anker AE, Feeley TH, McCracken B, Lagoe CA. Measuring the effectiveness of mass-mediated health campaigns through meta-analysis. J Health Commun. (2016) 21:439–56. doi: 10.1080/10810730.2015.1095820
28. Evans DW. How social marketing works in health care. BMJ. (2006) 332:1207–10. doi: 10.1136/bmj.332.7551.1207-a
29. Graham AL, Milner P, Saul JE, Pfaff L. Online Advertising as a public health and recruitment tool: comparison of different media campaigns to increase demand for smoking cessation interventions. J Med Internet Res. (2008) 10:e50. doi: 10.2196/jmir.1001
Keywords: knowledge, awareness, aerobic physical activity, muscular type of physical activity, physical activity guidelines
Citation: Vaara JP, Vasankari T, Koski HJ and Kyröläinen H (2019) Awareness and Knowledge of Physical Activity Recommendations in Young Adult Men. Front. Public Health 7:310. doi: 10.3389/fpubh.2019.00310
Received: 08 June 2019; Accepted: 11 October 2019;
Published: 30 October 2019.
Edited by:
Shane Andrew Thomas, Shenzhen International Primary Healthcare Research Institute, ChinaReviewed by:
Katie M. Heinrich, Kansas State University, United StatesBirute Strukcinskiene, Klaipeda University, Lithuania
Copyright © 2019 Vaara, Vasankari, Koski and Kyröläinen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jani P. Vaara, amFuaS52YWFyYUBtaWwuZmk=