 N. Vivanco Karlsson1,2*R. Sigall-Boneh3,4K. Mårild5E. M. Hård Af Segerstad6,7
N. Vivanco Karlsson1,2*R. Sigall-Boneh3,4K. Mårild5E. M. Hård Af Segerstad6,7- 1Department of Pediatrics, Skaraborg Hospital, Skövde, Sweden
- 2Department of Pediatrics, Institute of Clinical Sciences, Sahlgrenska Academy, Gothenburg, Sweden
- 3Pediatric Gastroenterology and Nutrition Unit, The E. Wolfson Medical Center, Holon, Israel
- 4Tytgat Institute for Liver and Intestinal Research, Amsterdam Gastroenterology Endocrinology and Metabolism, University of Amsterdam, Amsterdam, Netherlands
- 5Department of Pediatrics, Institute of Clinical Sciences, Sahlgrenska Academy, Gothenburg, Sweden
- 6Pediatric Research Institute, Oslo University Hospital, Oslo, Norway
- 7Clinical Sciences, Lund University, Malmoe, Sweden
Emerging evidence from diverse populations highlights the therapeutic benefits of the Crohn’s Disease Exclusion Diet (CDED) in managing Crohn’s Disease. To improve the efficacy of the CDED, there is a need to focus on cultural adaptation and individualization to support dietary adherence to this advanced nutritional therapy. This paper provides a theoretical framework for modifying the CDED to align with a Nordic diet (Nordic-CDED), while retaining the core principles and nutritional characteristics of the original protocol. Through a comprehensive literature review and expert consensus, we propose a Nordic-CDED that incorporates European regulations on food additives, the 2023 Nordic Nutritional Recommendations, and Nordic food culture. We present a theoretical foundation for an inclusion of whole foods and discuss the selection of enteral formulas. The adaptation also emphasizes the importance of dietitian-led guidance to tailor the Nordic-CDED to the patient’s age, lifestyle, and personal preferences. Further research is required to assess the clinical effectiveness and adherence to the Nordic-CDED.
Introduction
The role of diet in the onset and progression of Crohn’s disease
The global incidence of Crohn’s disease (CD) has risen significantly in recent decades, with the most marked increase in the pediatric population from 20,897.42 cases per 100,000 persons/year reported in year 1990 to 25,658.55 cases per 100,000 persons/year reported in year 2019 (1–3). Northern Europe has one of the highest prevalence rates of inflammatory bowel diseases (IBD) in the world, with CD affecting 0.13% and ulcerative colitis affecting 0.19% of the population (3, 4). IBD is associated with high morbidity, reduced quality of life, and increased healthcare costs, which can also have a significant impact on a patient’s diet and sense of identity (5–8). While the exact mechanisms underlying CD pathogenesis remain unclear, it is believed to involve complex interactions between genetic, immune, microbial, and environmental factors (9, 10).
Recent advancements in both basic and clinical science have significantly broadened our understanding of the role dietary factors play in the development and progression of CD. Emerging evidence suggests that certain dietary components, particularly ultra-processed foods, may trigger and sustain inflammation in CD (11–14). In the 1990s, exclusive enteral nutrition (EEN) was shown to induce remission in mild to moderate active CD. In the Nordic countries, the induction therapy for pediatric patients with active luminal CD, is EEN because of its proven efficacy and feasibility (15). While the underlying mechanisms of EEN remains unknown (15–17), it has been proposed to favorably modulate the gut microbiome (18), the intestinal barrier function and immunity (19). It has also been hypothesized that part of the mechanism by which EEN works may be related to the exclusion of dietary components that are potentially pro-inflammatory (19). However, EEN is challenging to complete due to taste fatigue, poor palatability, nausea and bloating, and the social and psychological impact on the patient (20, 21). Given the onerous nature of EEN, application beyond remission is unfeasible for long-term or maintenance therapy (22). Parents of children with CD previously treated with EEN have expressed a need for a solid food-based alternative (5, 18). However, several studies have shown that partial enteral nutrition (PEN) paired with an unrestricted diet does not yield similar clinical remission rates as EEN (19, 23, 24).
In line with the emerging evidence of CD pathogenesis, a range of effective nutritional therapies for CD has evolved to include whole foods, with the goal of improving dietary adherence and quality of life (11, 16, 18, 25, 26). While most of these dietary therapies have focused on reducing inflammation during active disease (18, 22, 27), they are used for a limited period because of the extensive food restrictions that increases the risk of nutritional deficiency and reduction in quality of life. Unfortunately, within a few weeks of completing these diet therapies, there is a fast regression to the original inflammation status in the bowel (11, 16, 18, 28–30). The Crohn’s Disease Exclusion Diet (CDED), a nutritionally complete diet that combines PEN with whole foods, has emerged as an alternative therapy to EEN with a potential for long-term use. Since 2014 a growing body of evidence has continued to support its use in inducing and potentially maintaining remission in both children and adults with CD (31–38).
This paper aims to develop a theoretical framework for adapting the CDED to a Nordic context. The framework was designed with consideration of European food additives regulations, local food production, and nutritional adequacy, all in an effort to support individualization and promote long-term adherence to the dietary therapy.
Methods
Literature review on the core principles of the diet CDED
We conducted a literature review where source selection criteria were applied: studies related to the use of EEN or CDED in patients with CD, children, and adults, encompassing randomized clinical trials, observational studies, meta-analyses, systematic reviews, as well as documents containing recommendations and guidelines. Case studies, articles not published in the English language, and studies involving pregnant and breastfeeding women and athletes were excluded from the review.
The following databases were utilized: PubMed and Google Scholar. The search process employed the following search strings: “IBD and diet therapy,” “Crohn’s Disease Exclusion Diet,” “Food additives and IBD,” “Total Enteral Nutrition,” “Diet adaptation,” “Nordic Diet.” In total, 91 literature papers were collected.
Expert consensus to develop a theoretical model for adaptation of the CDED to the Nordic setting
We developed this adaptation through a group consensus in collaboration with one of the developers of the original CDED. The fundamental principles of CDED were carefully considered, leading to the development of a Nordic modification. This modified version considered regulations on food additive use in the Nordic food industry, the Nordic Dietary Guidelines, as well as Nordic dietary habits and local foods.
The design of the Nordic-CDED underwent a comprehensive review by the group of authors and was systematically compared with the original CDED. Additionally, a thorough evaluation of other published modifications was conducted, identifying elements that deviated from the original CDED but still resulted in similar clinical effects. These elements were carefully assessed and integrated into the Nordic-CDED where appropriate.
Core principles of the Crohn’s Disease Exclusion Diet
The CDED aims to exclude dietary components hypothesized to be detrimental to the gut microbiome and intestinal barrier function (13, 14, 19, 36, 39–43). The diet restricts the intake of foods rich in animal fat, red and processed meat, protein sources rich in taurine, gluten and wheat protein, as well as food additives including maltodextrin, emulsifiers, artificial sweeteners, carrageenan, and sulfites (44). The exclusion of ultra processed food is one of the most important elements of CDED and exclusion of additives based on the Israeli Food Control Services regulations (44). Moreover, the CDED includes specific fruits and vegetables that provide various dietary fibers and resistant starch, which serves as substrates for short-chain fatty acid (SCFA) producing bacteria (45, 46).
The CDED is a standardized diet consisting of 3 phases (Table 1) (36). The first phase (weeks 0–6) is highly restrictive, excluding all potential triggering ingredients, while emphasizing consumption of high-quality protein sources and microbiome-enhancing ingredients. In this phase, 50% of the energy requirements is provided by PEN, and the remaining 50% from whole foods. The diet is liberalized for weeks 6–12 (phase 2), enabling a gradual introduction of previously restricted foods and a reduction of PEN (25%). Phase 3 (weeks 13–18) permits up to twice a week, the inclusion of most unprocessed foods, along with the consumption of products containing food additives (38). Since there is limited evidence of excluding foods or additives beyond phase 3, it is advised that the patient adopts an overall healthy diet in line with general dietary guidelines after completion of Phase 3 (38).
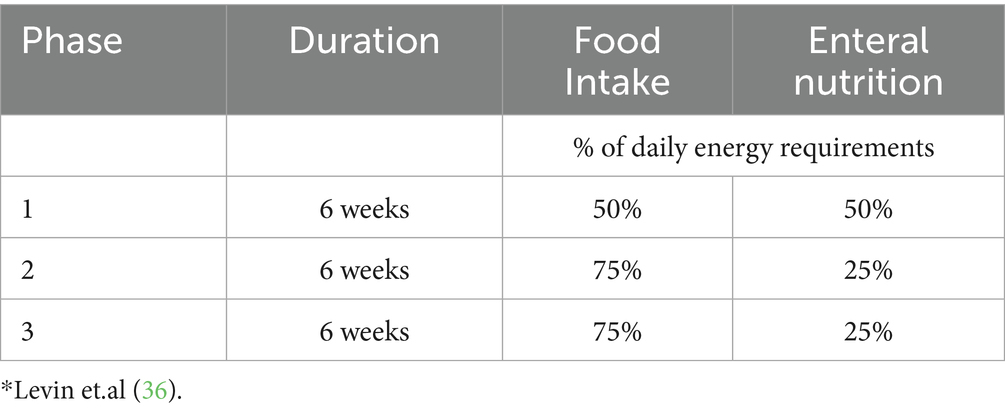
Table 1. Description of the three phases of Crohn’s disease exclusion diet*.
The CDED was designed to be adaptable across various countries and cultures, incorporating simple and internationally accessible foods, but was mostly focused on “Western” populations (26, 47, 48). It recommends chicken and egg as the main sources of protein, potatoes as the main starch source, and apples and bananas to provide soluble fiber and pectin. Additionally, it includes a list of allowed whole foods to ensure nutritional adequacy. Table 2 outlines the recommended and excluded foods, along with the rationale for their inclusion or exclusion in the various phases of the CDED.
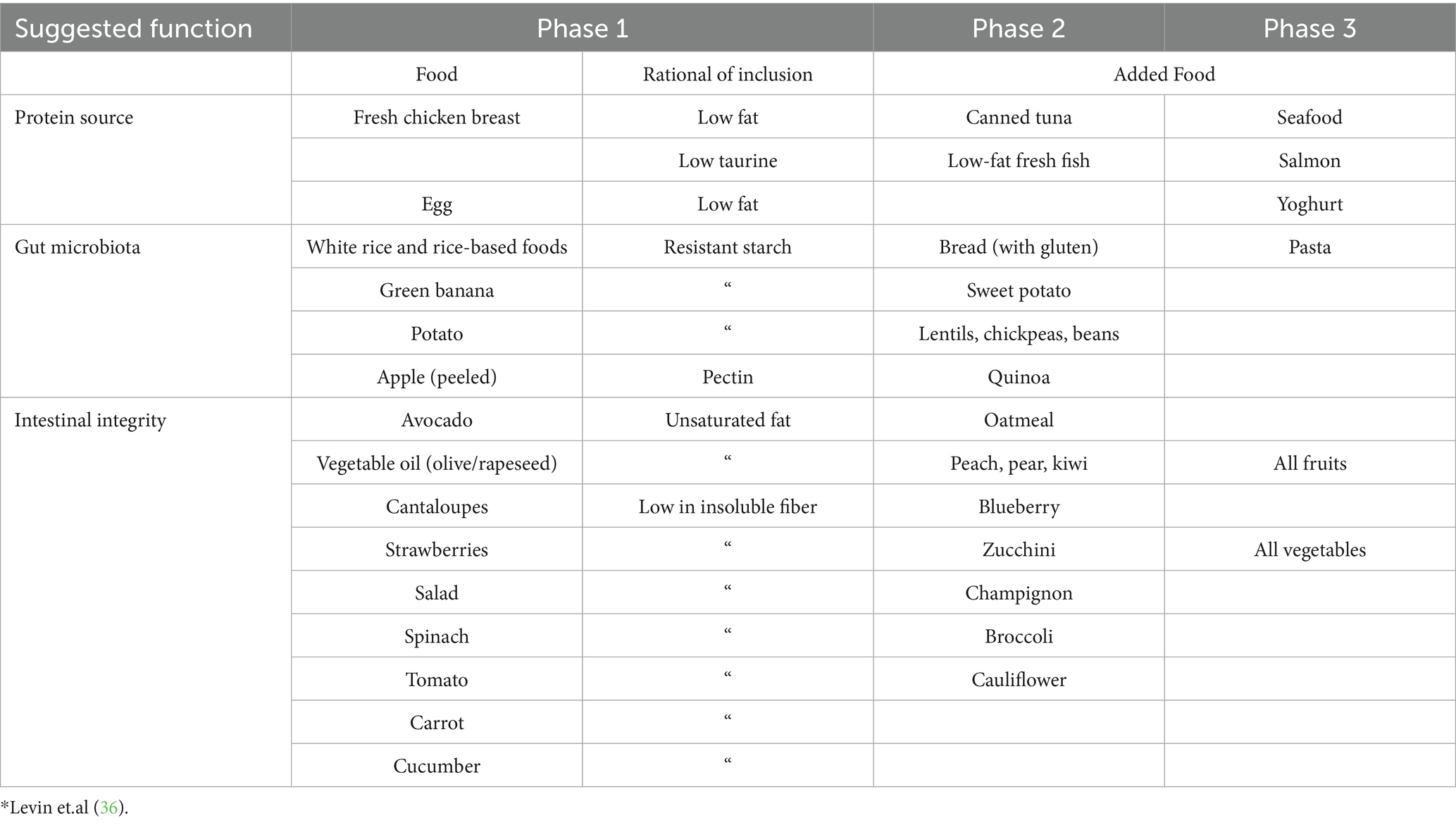
Table 2. Recommended and excluded foods in Crohn’s disease exclusion diet (CDED): rationale for selection*.
The enteral formula used in CDED’s first trials was Modulen IBD, specifically developed for patients with IBD (31, 36). This polymeric formula is rich in Transforming Growth Factor Beta (TGFβ), a potent anti-inflammatory cytokine. In murine models, TGFβ has demonstrated a positive effect on lesions associated with chronic inflammation (49, 50).
Rationale for a modified CDED: enhancing adherence and individualization
Restricted eating because of gastrointestinal symptoms is common in IBD patients and increases the risk of nutritional deficiencies and malnutrition (6, 7, 51). In various reports, nearly half of pediatric and adult IBD patients indicate that they avoid or limit their intake of fruits and vegetables because of symptom flare-ups (7). Patients with IBD use different food-related strategies to control symptoms, such as identifying and avoiding triggering foods, following restrictive diets, controlling portion size, and eating more or less frequently, which may potentially have consequences on their nutrient intake and status. Such maladaptive behaviors, combined with limited knowledge about diet in IBD, may adversely affect patients food-related quality of life and result in social isolation (52). In addition, suboptimal nutrient intake can in turn negatively impact their clinical prognosis (7, 53, 54). Furthermore, as seen in other chronic conditions such as celiac disease and food allergies, extensive exclusion diets are associated with an increased risk of maladaptive eating behaviors (55). One such condition is Avoidant/Restrictive Food Intake Disorder (ARFID), where dietary intake is significantly limited for reasons unrelated to body image, including fear of adverse physical reactions, perception of pain, or a general lack of interest in eating (38). The development of ARFID can also contribute to social anxiety and withdrawal, further impacting quality of life (56, 57).
The primary goal of any nutritional therapy is to optimize the patient’s nutritional and clinical status while supporting growth and development (26). This can be achieved by tailoring the therapy to the individual patient’s needs, while simultaneously improving dietary adherence. Since diet is a central aspect of daily life and modifying eating habits can be challenging (58–60), it is crucial to guide patients in adopting not only a clinically effective diet, but it should also be manageable, socially acceptable, and sustainable (6, 56, 61). It is essential to develop evidence-based nutritional therapies that consider adaptation and individualization, with the goal of supporting long-term healthy dietary habits (58).
Recent clinical studies on the implementation of a modified CDED in various populations exemplifies how this nutritional therapy has been adapted to diverse food cultures, religious practices, and individual nutritional needs, while maintaining alignment with national dietary guidelines and achieving improved adherence (33–35, 37, 61, 62). These adaptations have showed improved individualization, acceptability, and adherence to the diet (33, 34, 63). To date, data on adaptations of the CDED within the Scandinavian settings are limited, and its clinical application remains scarce. In our clinical practice, 10 pediatric patients have undergone CDED, with generally good adherence. However, in most cases, modifications were necessary, including an expanded list of permitted foods and enteral products to improve feasibility and patient acceptance.
Adapting the CDED to a Nordic context
The Nordic diet is characterized by native berries, legumes, apples, pears, root vegetables, cabbage, cauliflower, curly kale, and mushrooms, as well as whole grains such as barley, wheat, oats, buckwheat, and rye. It also includes regular fish consumption, seaweed, and free-range animal products (64, 65). Given these core foods in the Nordic diet, it is theoretically possible to incorporate a wider variety of foods across the different phases of the CDED, while still maintaining its presumed anti-inflammatory benefits and ensuring adequate nutritional intake. Table 3 outlines core foods in the Nordic diet. In the Nordic countries, aligned with the fundamental principles of the CDED, additional gluten-free carbohydrate sources, such as buckwheat and arrowroot, are included.
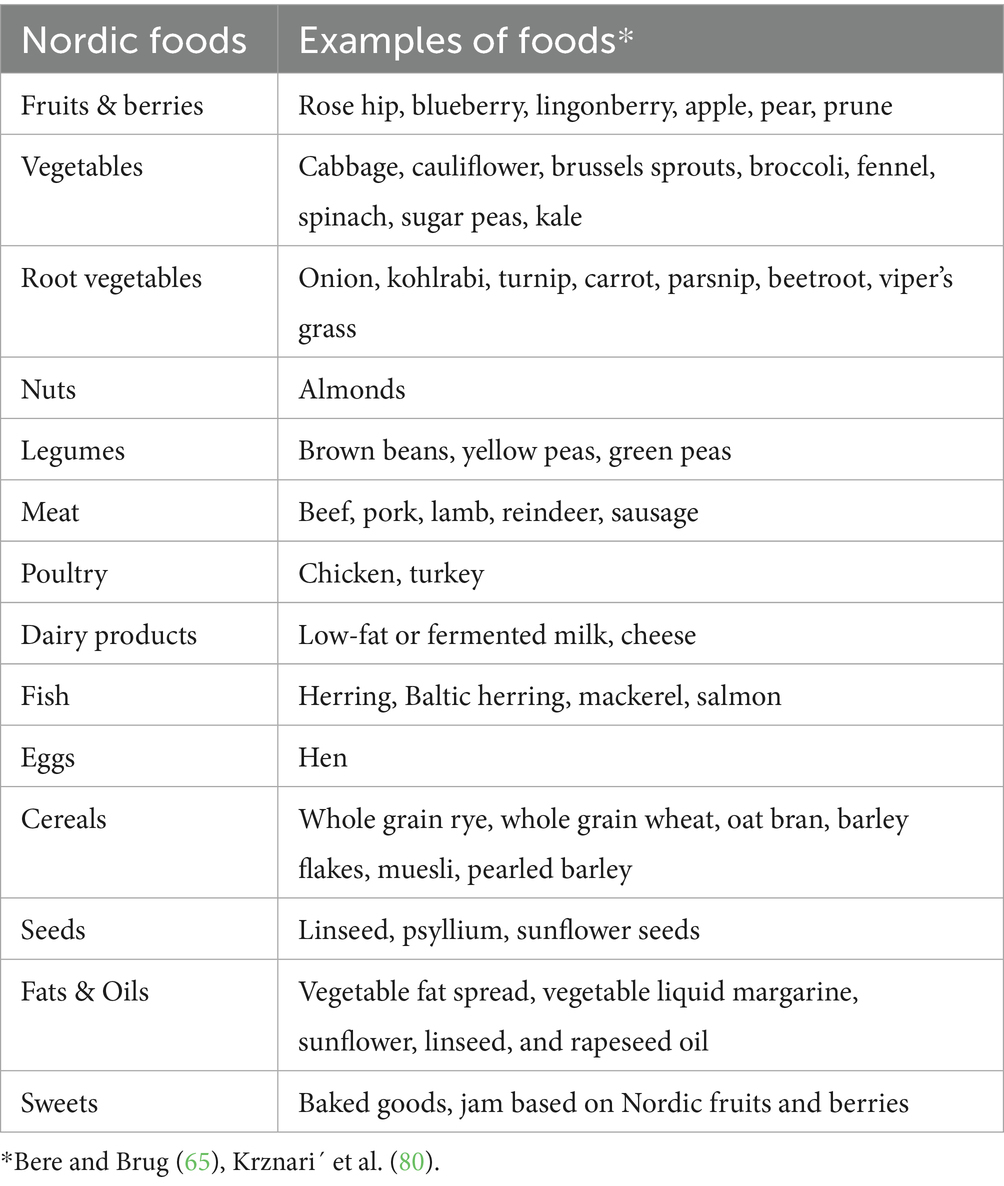
Table 3. Key foods in the Nordic diet.
The Nordic diet further includes a variety of fruits and vegetables rich in fiber and starch, such as plums and carrots, as well as fresh fish, seafood, and sources of unsaturated oils, such as almonds. Table 4 presents the whole foods recommended in the original CDED, along with suggested additions for a Nordic adaptation.
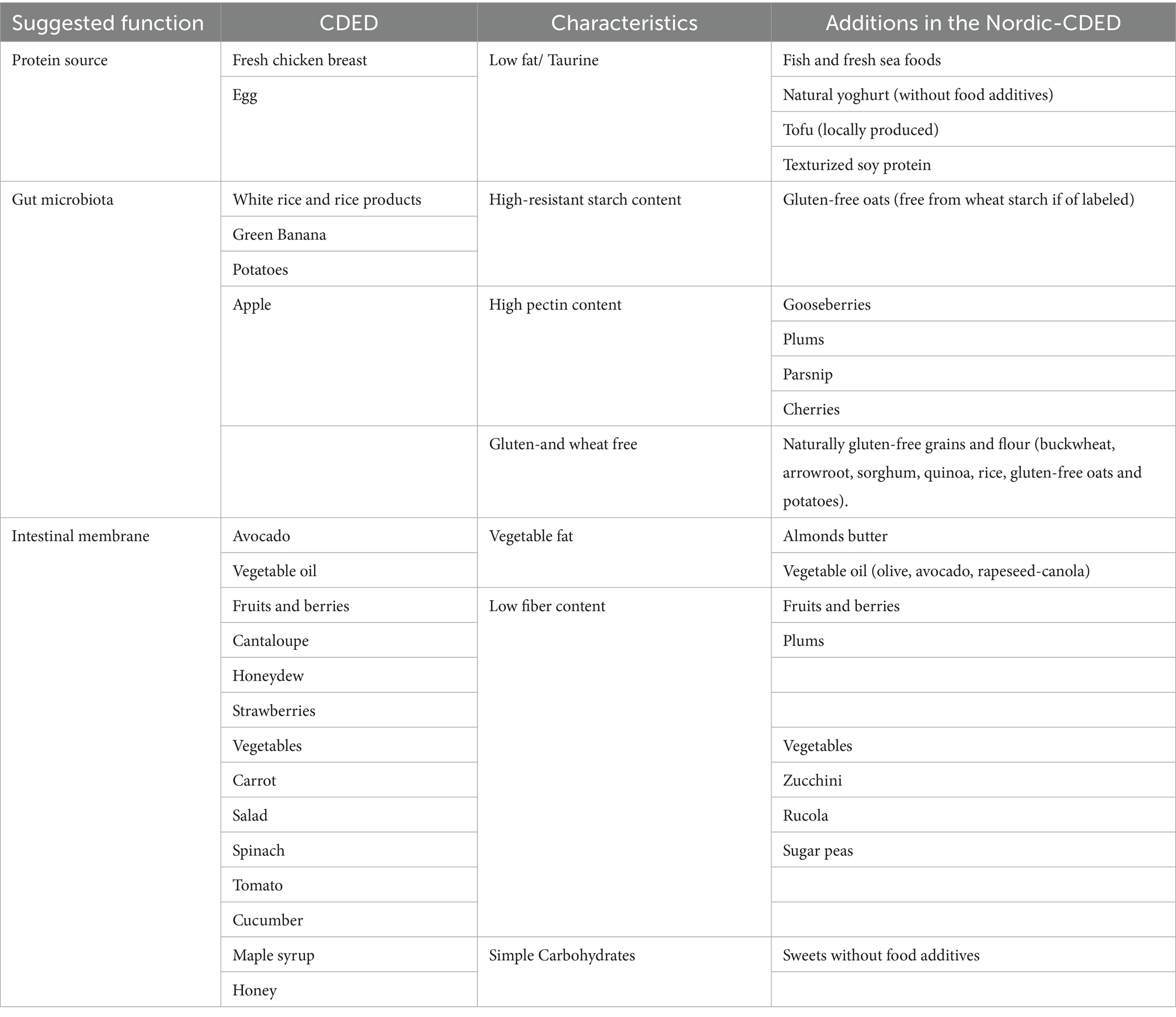
Table 4. Crohn’s disease exclusion diet (CDED) recommended whole food and suggested additions in a Nordic adaptation.
Food additives in the Nordic CDED
The European Food Safety Authority (EFSA) sets regulations for food additives permitted in the food industry in the European Union (66). These regulations are enforced across all Nordic countries and are stricter compared to those in Israel (44). For example, additives such as sulfites, carrageenan, and carboxymethylcellulose are allowed in fewer products under EFSA regulations compared to in Israel. Furthermore, while Israeli regulations permit additives like titanium dioxide, EFSA banned its use in 2022 (44). These regulatory differences present an opportunity to potentially expand the range of whole foods allowed the Nordic CDED. Table 5 lists the excluded elements of the CDED including several food additives, along with examples of foods that may contain them according to EFSA regulations (44, 66).
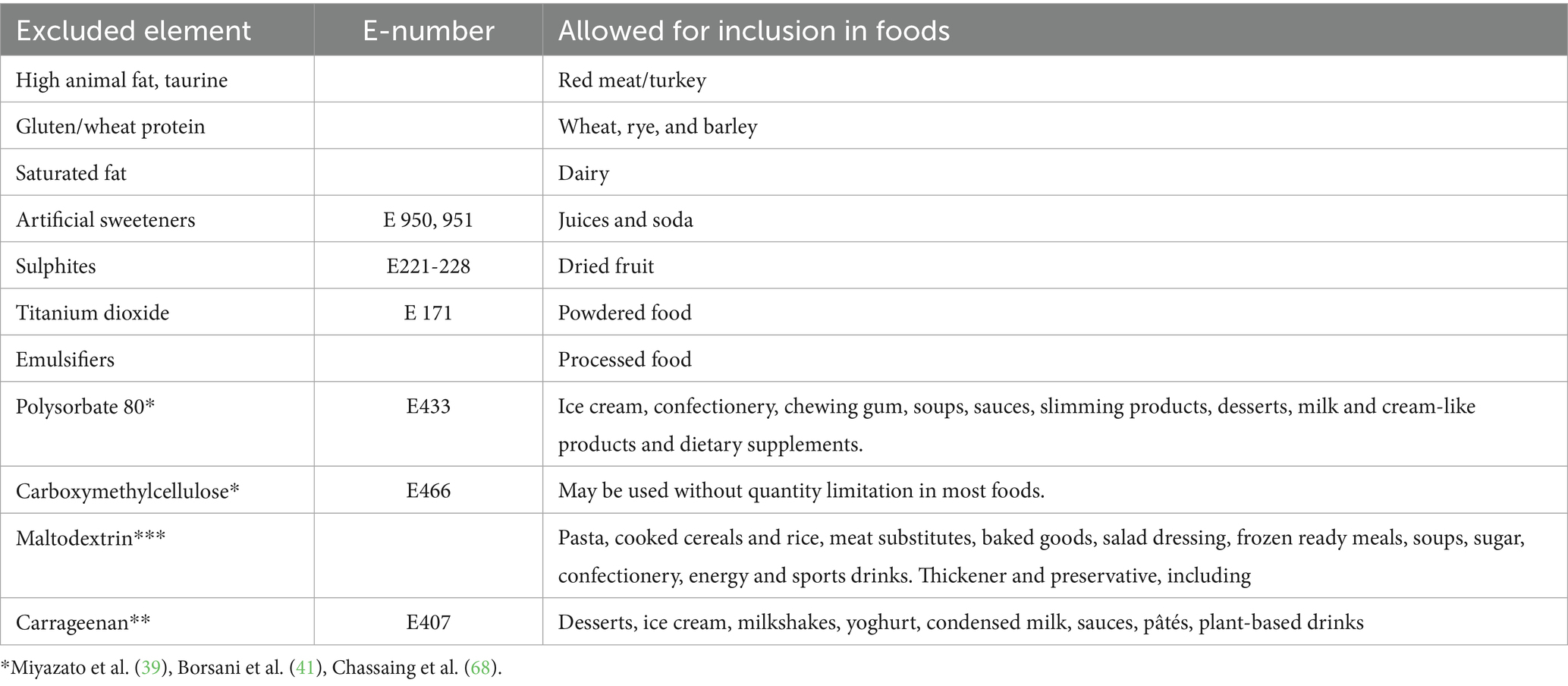
Table 5. Excluded elements of the Crohn’s disease exclusion diet (CDED) and examples of containing foods according to the European food safety authority (EFSA).
A key limitation in current research on food additives is that much of the supporting evidence comes from animal models and human cell lines (19). It is still unclear if studies translate to human physiology and the specific quantities that may induce harm (33). Additionally, as there is yet no conclusive evidence regarding the mechanisms, amounts, and types of certain food additives, much remains to be defined in the CDED (19, 32, 33, 67, 68).
Nutritional recommendations
The original CDED (36) was initially developed with mandatory whole food in suggested quantities, alongside PEN. To be nutritionally balanced, specifically for young children, the amounts of included whole foods should be adjusted, as pre-determined quantities may exceed recommended daily intakes of protein, vitamin A, and Iron (69). In further developments and modifications to the CDED, the individualization of specific amounts of whole foods has been emphasized in this regard (38, 61). According to the European Society of Parenteral and Enteral Nutrition (ESPEN), the energy and nutrient requirements for children with IBD are generally consistent with those of the general population, although specific complications may necessitate adjustments to certain nutrients (70). In the Nordic-CDED, we suggest to use age-and sex-specific recommendations when determining the appropriate amounts of the recommended whole foods, particularly for protein intake (69). Table 6 outlines the phases of the Nordic-CDED and suggested recommended daily intake of energy and macronutrients.
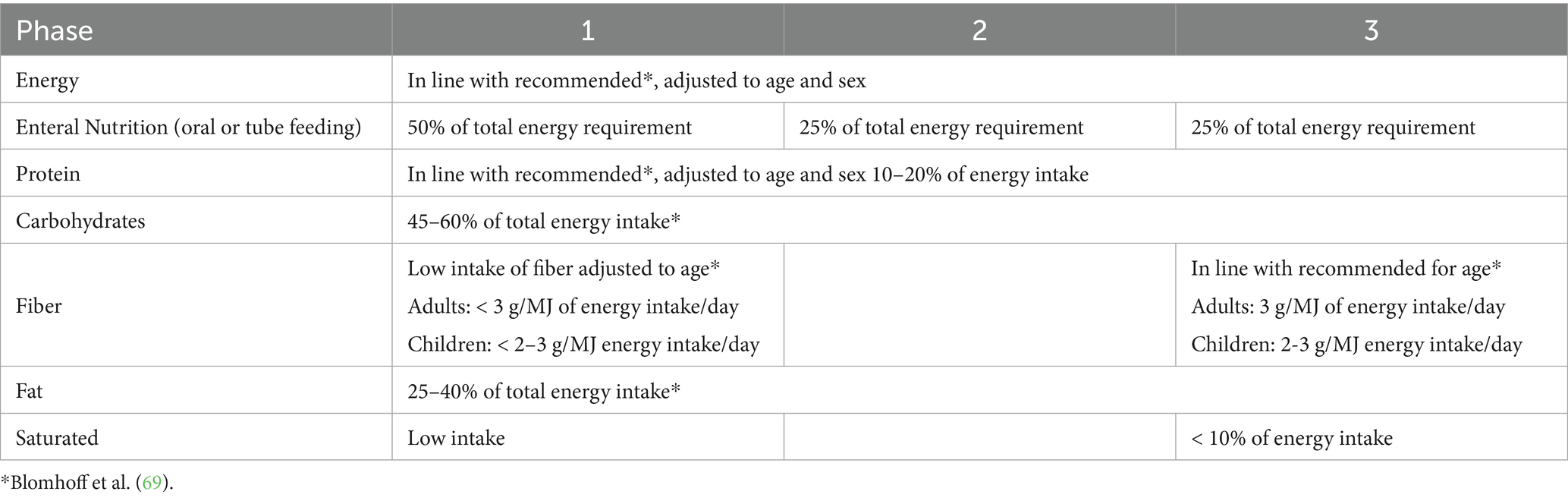
Table 6. Energy and nutrient recommendations for the three phases of the Nordic Crohn’s disease exclusion diet.
Choice of enteral nutrition or oral nutritional supplementation
A deteriorated nutritional status is common in Crohn’s disease. Children are a specifically vulnerable group as poor nutritional status affects growth and delays overall development (71). While EEN is often used as induction therapy in CD, a key secondary clinical goal is to support nutritional rehabilitation, and growth in children. This aligns with the rationale for using PEN as a maintenance therapy to ensure long-term nutritional sufficiency (35, 70). In clinical practice, there is considerable variation in the types of formulas used for EEN. Several publications, including one that examined 61 commercial enteral formulas and oral nutritional supplements used in EEN for CD (72), have demonstrated similar clinical efficacy across different formulas, regardless of the level of protein hydrolysis (polymeric, semi-elemental, or elemental), the range of food additives included, or nutrient concentration (15, 62, 70, 71).
Modulen IBD, a polymeric formula based on milk (protein and fat), that contains added soy lecithin, has been the formula of choice in most CDED trials (31, 36, 73–75). However, several studies have reported similar clinical outcomes of the CDED using other enteral formulas (31, 34, 35, 62). Most of the commonly used nutritional supplements contain food additives such as maltodextrin and emulsifiers. When adapting the Nordic-CDED, we suggest selecting an enteral formula or oral nutritional supplement that has shown a clinical effect in previous trials. Furthermore, factors such as availability, cost, and palatability should be carefully considered, as they play a crucial role in individualizing the diet and ensuring long-term adherence (5, 71, 76).
Discussion
This article presents the theoretical rational for an adaptation of the CDED to a Nordic modification. A key aspect of this adaptation involves a comprehensive review of the core principles and rationale of the original CDED. The Nordic-CDED presented is based on these core principles and proposes additional allowed whole foods, typical for the region. Furthermore, the modified Nordic-CDED incorporates current EFSA regulations on food additives and aligns with the Nordic Nutrition Recommendations to tailor nutritional requirements to individual needs. The primary goal of this adaptation is to support the individualization of the CDED. However, this theoretical framework must be validated in clinical trials to assess its clinical efficacy and impact on patient experience compared to previous findings (74). Such trials should evaluate remission rates, using objective measurements of inflammation and endoscopic outcomes, nutritional adequacy, dietary adherence, and patient-reported outcomes on quality of life and diet satisfaction.
For several decades, EEN was the sole nutritional treatment option for CD. Its efficacy has been well-documented across numerous populations and clinical settings (21, 28, 77). However, significant barriers to its use remain, primarily related to the monotonous and unpalatable taste of enteral formulas, the strict dietary restrictions required, and associated adverse effects such as nausea, vomiting, constipation, and a typically short-lived therapeutic effect (34). To address these limitations, the CDED was developed as an alternative nutritional strategy. By incorporating selected whole foods, many of the challenges associated with EEN can be considerably reduced. CDED has since been implemented in a variety of countries and cultural contexts, highlighting the importance of adapting the diet to local eating habits and food availability (59). Such adaptations aim to mitigate risks commonly associated with restrictive dietary therapies, including disordered eating behaviors, incomplete or unbalanced diets, social isolation, diminished quality of life, and reduced enjoyment of food. Furthermore, overly restrictive diets may heighten anxiety related to eating, fear of adverse events, or concerns about disease relapse factors that CDED seeks to address through a more flexible and sustainable approach (59).
Previous publications have reported on regional modifications to the CDED (33, 34). The Dietitians Crohn’s and Colitis Australian Network (DECCAN) modified the CDED for adults with CD, aligning it with Australian food groups and micronutrient recommendations. They also developed an optimal care pathway for clinical use of the CDED, which included consensus statements, a clinician toolkit, and a patient education material (33). Additionally, in Slovenia researchers compared the effects of a modified CDED versus EEN. In this modification, 75% of the energy requirement was provided by PEN using an alternative enteral formula, with the remaining 25% sourced from food (one meal per day). The Slovenian CDED included regional and locally produced fruits and vegetables, white meat, fish, and added buckwheat and millet as carbohydrate sources. After 6 weeks on the diet, both groups demonstrated similar clinical remission rates, but the CDED group showed a higher endoscopic response compared to the EEN group (34). These studies propose that the original CDED’s clinical efficacy can be maintained with modifications, such as an expanded selection of foods and the use of other enteral products beside Modulen.
As the underlying mechanisms of CDED are not yet fully understood, it is essential that any adaptations remain aligned with its core principles. There is a risk that modifications deviating too far from the original protocol may compromise its clinical efficacy. Therefore, it is crucial to systematically evaluate the impact of each adaptation to ensure that the therapeutic benefits are maintained. Any adaptation of the CDED should offer evidence-based clinical guidance on the exclusion and selection of foods, while considering the various challenges patients may face. It may be beneficial to screen patients starting nutritional therapy to identify those at risk of developing an unhealthy relationship with food. A food-based dietary therapy that provides adequate energy and nutrients could help prevent nutritional deficiencies while promoting growth and development. A clinically effective diet that reduces the risk of inflammatory flare-ups and is also accepted by patients to use long-term would support overall clinical care of patients with CD.
However, every nutritional therapy comes with potential side-effects, including clinical, nutritional, and psychological complexities that must be carefully managed to promote adherence and minimize nutrition-related complications and disordered eating (33). For many patients and their families, diet profoundly affects daily life, including school or work and social interactions (52). Therefore, it is crucial to consider the patient’s psychological state, as well as their religious, cultural, and personal practices, as these factors can influence their relationship with food and, ultimately, their overall quality of life (5, 38, 52). In this, the dietitian plays a crucial role in the success of nutritional therapy (78, 79). In pediatric patients with CD, it is essential to assess the suitability of the specific therapy, tailoring the diet to the patient’s clinical and nutritional status while also considering their preferences and quality of life (61). Effectively communicating dietary advice and adapting the therapy based on current evidence is essential. If successful, the dietitian can help the patient adopt a diet that not only addresses the disease during a flare but also has the potential to become part of a long-term lifestyle that supports gut health and reduces the risk of future flare-ups (52).
Establishing evidence-based long-term dietary therapy for IBD not only offers a potential to reduce the need for immunosuppression and lower the risk of associated side effects, but it may also serve as a bridge between medications and provide a widely accessible and cost-effective treatment option. It is important to continue developing CDED as a nutritional therapy, as a modern CDED diet could serve as a valuable long-term complement to medical treatment for Crohn’s disease.
Conclusion
We present an adaptation of the original CDED to a Nordic setting, with a theoretical framework and practical guidance aligned with updated nutritional guidelines. The adaptation incorporates a wider variety of recommended foods and guidance on individualizing the diet for CD patients. Moreover, the adaptation includes recommendations to choose enteral formulas to be used. Future research should focus on clinical studies to assess the efficacy of the Nordic-CDED, in comparison with the CDED.
Author contributions
NV: Writing – original draft, Conceptualization, Formal analysis, Investigation, Methodology. RS: Conceptualization, Methodology, Writing – review & editing, Supervision. KM: Supervision, Writing – review & editing, Conceptualization, Project administration. EH: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing, Project administration.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fiorino, GE, Lopes, DJM, Chersi, F, Allocca, M, Souto, MT, Danese, S, et al. Inflammatory bowel disease in migrant populations: should we look even further back? Curr Drug Targets. (2021) 22:1706–15. doi: 10.2174/1389450122666210203193817
2. Park, J, and Cheon, JH. Incidence and prevalence of inflammatory bowel disease across Asia. Yonsei Med J. (2021) 62:99–108. doi: 10.3349/ymj.2021.62.2.99
3. Dan Long, CW, Huang, Y, Mao, C, Yin, X, and Zhu, Y. Changing epidemiology of inflammatory bowel disease in children and adolescents. Int J Color Dis. (2024) 39:1–11. doi: 10.1007/s00384-024-04640-9
4. Johan Burisch, TJ, Martinato, M, and Lakatos, PL. The burden of inflammatory bowel disease in Europe. J Crohn's Colitis. (2013) 7:322–37. doi: 10.1016/j.crohns.2013.01.010
5. Svolos KG, V, Buchanan, E, Curtis, L, Garrick, V, Hay, J, Laird, S, et al. Dietary treatment of Crohn’s disease: perceptions of families with children treated by exclusive enteral nutrition, a questionnaire survey. BMC Gastroenterol. (2017) 17:1–6. doi: 10.1186/s12876-016-0564-7
6. Xiong, H, Zeng, H, and Xie, S. Experience of diet in patients with inflammatory bowel disease: A thematic synthesis of qualitative studies. J Clin Nurs. (2024) 1:1–11. doi: 10.1111/jocn.17186
7. Simona Gatti, MV, Quattrini, S, Aloi, M, Bramuzzo, M, Felici, E, Zuin, G, et al. Dietary habits in Italian children with inflammatory bowel disease: a case-control multicenter study. J Pediatr Gastroenterol Nutr. (2024) 79:602–609. doi: 10.1002/jpn3.12344
8. Siew, C, Ng, HYS, Hamidi, N, Underwood, FE, Tang, W, Benchimol, EI, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. (2017) 390:2769–78. doi: 10.1016/S0140-6736(17)32448-0
9. Cohen, LJ, Cho, JH, Gevers, D, and Chu, H. Genetic factors and the intestinal microbiome guide development of microbe-based therapies for inflammatory bowel diseases. Gastroenterology. (2019) 156:2174–89. doi: 10.1053/j.gastro.2019.03.017
10. Graham, DB, and Xavier, RJ. Pathway paradigms revealed from the genetics of inflammatory bowel disease. Nature. (2020) 578:527–39. doi: 10.1038/s41586-020-2025-2
11. Barros, VJS, Severo, JS, Mendes, PHM, da Silva, ACA, de Oliveira, KBV, Parente, JML, et al. Effect of dietary interventions on inflammatory biomarkers of inflammatory bowel diseases: A systematic review of clinical trials. Nutrition. (2021) 91-92:111457. doi: 10.1016/j.nut.2021.111457
12. Tracy, MK. You are what you eat? Growing evidence that diet influences the risk of inflammatory bowel. J Crohns Colitis. (2022) 16:1185–6. doi: 10.1093/ecco-jcc/jjac025
13. Lo, C-H, Khandpur, N, Rossato, SL, Lochhead, P, Lopes, EW, Burke, KE, et al. Ultra-processed foods and risk of Crohn’s disease and ulcerative colitis: a prospective cohort study. Clin Gastroenterol Hepatol. (2022) 20:e1323:–e37. doi: 10.1016/j.cgh.2021.08.031
14. Narula, N, Wong, ECL, Dehghan, M, Mente, A, Rangarajan, S, Lanas, F, et al. Association of ultra-processed food intake with risk of inflammatory bowel disease: prospective cohort study. BMJ. (2021) 374:n1554. doi: 10.1136/bmj.n1554
15. van Rheenen, PF, and Assa, A. The medical management of paediatric Crohn’s disease: an ECCO-ESPGHAN guideline update. J Crohns Colitis. (2021) 15:171–94. doi: 10.1093/ecco-jcc/jjaa161
16. Cucinotta, U, Romano, C, and Dipasquale, V. Diet and nutrition in pediatric inflammatory bowel diseases. Nutrients. (2021) 13:1–14. doi: 10.3390/nu13020655
17. Swaminath, A, Feathers, A, Ananthakrishnan, AN, Falzon, L, and Li Ferry, S. Systematic review with meta-analysis: enteral nutrition therapy for the induction of remission in paediatric Crohn's disease. Aliment Pharmacol Ther. (2017) 46:645–56. doi: 10.1111/apt.14253
18. Vaios Svolos, RH, Nichols, B, Quince, C, Ijaz, UZ, Papadopoulou, RT, Edwards, CA, et al. Treatment of active Crohn’s disease with an ordinary food-based diet that replicates exclusive enteral nutrition. Gastroenterology. (2019) 156:1354–67. doi: 10.1053/j.gastro.2018.12.002
19. Levine, A, Sigall-Boneh, R, and Wine, E. Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseases. Gut (2018) 67:1726–38. doi: 10.1136/gutjnl-2017-315866
20. Gkikas, K, Nichols, B, Ijaz, UZ, Clark, CM, Svolos, V, Gervais, L, et al. Dietary triggers of gut inflammation following exclusive enteral nutrition in children with Crohn’s disease: a pilot study. BMC Gastroenterol. (2021) 21:1–11. doi: 10.1186/s12876-021-02029-4
21. de Bie Charlotte, AK, and Escher, J. Use of exclusive enteral nutrition in paediatric Crohn's disease in the Netherlands. J Crohns Colitis. (2013) 7:263–70. doi: 10.1016/j.crohns.2012.07.001
22. Sarah, L, Melton, ASD, and Bryant, RV. Revolution in diet therapy for inflammatory bowel disease. J Gastroenterol Hepatol. (2024) 8:1–10. doi: 10.1002/jgh3.13097
23. Dale Lee, M, Baldassano, RN, and Otley, AR. Comparative effectiveness of nutritional and biological therapy in north American children with active Crohn’s disease. Inflamm Bowel Dis. (2015) 21:1786–93. doi: 10.1097/MIB.0000000000000426
24. Johnson, T, Hill, SM, and Thomas, A. Treatment of active Crohn’s disease in children using partial enteral nutrition with liquid formula: a randomised controlled trial. Gut. (2006) 55:356–61. doi: 10.1136/gut.2004.062554
25. Zhang, JL. The effect of solid food diet therapies on the induction and maintenance of remission in Crohn’s disease: a systematic review. BMC Gastroenterol. (2024) 24:1–22. doi: 10.1186/s12876-024-03315-7
26. Hart, L, Wine, E, Zachos, M, Poppen, A, Chavannes, M, Van Limbergen, J, et al. Nutritional therapies and their influence on the intestinal microbiome in pediatric inflammatory bowel disease. Nutrients. (2022) 14:1–22. doi: 10.3390/nu14010004
27. Lewis RS, JD, Brotherton, C, Brensinger, C, and Kappelman, HLMD. A randomized trial comparing the specific carbohydrate diet to a Mediterranean diet in adults with Crohn’s disease. Gastroenterology. (2021) 161:837–852.e9. doi: 10.1053/j.gastro.2021.05.047
28. Gatti, S, Galeazzi, T, Franceschini, E, Annibali, R, Albano, V, Verma, AK, et al. Effects of the exclusive enteral nutrition on the microbiota profile of patients with Crohn's disease: A systematic review. Nutrients. (2017) 9:832. doi: 10.3390/nu9080832
29. Verburgt, CM, Ghiboub, M, Benninga, MA, de Jonge, WJ, and Van Limbergen, JE. Nutritional therapy strategies in pediatric Crohn's disease. Nutrients. (2021) 13:1–20. doi: 10.3390/nu13010212
30. Christensen, CAK, Arnesen, EK, Hatlebakk, JG, Sletten, IS, and Fadnes, LT. Diet, food, and nutritional exposures and inflammatory bowel disease or progression of disease: an umbrella review. Adv Nutr. (2024) 15:1–10. doi: 10.1016/j.advnut.2024.100219
31. Sigall-Boneh, R, Segal, I, Zangen, T, Boaz, M, and Levine, A. Partial enteral nutrition with a Crohn’s disease exclusion diet is effective for induction of remission in children and young adults with Crohn’s disease. Inflamm Bowel Dis. (2014) 20:1353–60. doi: 10.1097/MIB.0000000000000110
32. Naomi Fliss-Isakov, NAC, Bromberg, A, Elbert, G, and Anbar, R. Crohn’s Disease Exclusion Diet for the Treatment of Crohn’s Disease: Real-World Experience from a Tertiary Center. J Clin Med. (2023) 12:5428.
33. Russell, EE, Day, AS, Dimitroff, C, Trakman, GL, Silva, H, Bryant, RV, et al. Practical application of the Crohn's disease exclusion diet as therapy in an adult Australian population. J Gastroenterol Hepatol. (2023) 39:446–456. doi: 10.1111/jgh.16414
34. Urlep, D, Orel, R, Kunstek, P, and Benedik, E. Treatment of active Crohn's disease in children using partial enteral nutrition combined with a modified Crohn's disease exclusion diet: a pilot prospective cohort trial on clinical and endoscopic outcomes. Nutrients. (2023) 15:4676. doi: 10.3390/nu15214676
35. Niseteo, T, Sila, S, Trivic, I, Misak, Z, Kolacek, S, and Hojsak, I. Modified Crohn's disease exclusion diet is equally effective as exclusive enteral nutrition: real-world data. Nutr Clin Pract. (2022) 37:435–41. doi: 10.1002/ncp.10752
36. Levine, A, Wine, E, Assa, A, Sigall Boneh, R, Shaoul, R, Kori, M, et al. Crohn's disease exclusion diet plus partial enteral nutrition induces sustained remission in a randomized controlled trial. Gastroenterology. (2019) 157:440–450.e8. doi: 10.1053/j.gastro.2019.04.021
37. Luca Scarallo, EB, De Blasi, A, Paci, M, Renzo, S, Naldini, S, Barp, J, et al. A real-life pediatric experience of Crohn's disease exclusion diet at disease onset and in refractory patients. J Pediatr Gastroenterol Nutr. (2024) 79:592–601. doi: 10.1002/jpn3.12283
38. Sigall Boneh CS-S, R, Albenberg, LG, Westoby, C, Oseran, I, Lionetti, P, Navas-López, VM, et al. The Crohn’s disease exclusion diet: a comprehensive review of evidence, implementation strategies, practical guidance, and future directions. Inflamm Bowel Dis. (2024) 30:1888–902. doi: 10.1093/ibd/izad255
39. Miyazato, S, YK,, Takahashi, K, Kaminogawa, S, and Hosono, A. Continuous intake of resistant maltodextrin enhanced intestinal immune response through changes in the intestinal environment in mice. Biosci Microbiota Food Health. (2016) 35:1–7. doi: 10.12938/bmfh.2015-009
40. Hye Jin Choi, JK, Park, S-H, Do, KH, Yang, H, and Moon, Y. Pro-inflammatory NF-κB and early growth response gene 1 regulate epithelial barrier disruption by food additive carrageenan in human intestinal epithelial cells. Toxicol Lett. (2011) 3:289–95. doi: 10.1016/j.toxlet.2012.04.012
41. Borsani RDS, B, Perico, V, Penagini, F, Pendezza, E, Dilillo, D, Bosetti, A, et al. The role of carrageenan in inflammatory bowel diseases and allergic reactions: where do we stand? Nutrients. (2021) 13:1–13. doi: 10.3390/nu13103402
42. Ejsing-Duun, M, Aasted, B, Buschard, K, and Hansen, AK. Dietary gluten reduces the number of intestinal regulatory T cells in mice. Scand J Immunol. (2008) 67:553–9. doi: 10.1111/j.1365-3083.2008.02104.x
43. Zevallos VR, VF, Tenzer, S, Jimenez-Calvente, C, Ashfaq-Khan, M, Rüssel, N, Pickert, G, et al. Nutritional wheat amylase-trypsin inhibitors promote intestinal inflammation via activation of myeloid cells. Gastroenterology. (2017) 152:1100–13. doi: 10.1053/j.gastro.2016.12.006
44. Service TNF In: MH Public, editor. Food control services: list of food additives according to public health regulations. Tel Aviv Israel: Health services Israel (2022). 1–117.
45. Yusuf, K, Saha, S, and Umar, S. Health benefits of dietary fiber for the management of inflammatory bowel disease. Biomedicine. (2022) 10:1242. doi: 10.3390/biomedicines10061242
46. Antoniussen, CS, Rasmussen, HH, Holst, M, and Lauridsen, C. Reducing disease activity of inflammatory bowel disease by consumption of plant-based foods and nutrients. Front Nutr. (2021) 8:733433. doi: 10.3389/fnut.2021.733433
48. Nations FAAOotU Food-based dietary guidelines - Israel. Food and Agriculture Organization of the United Nations (FAO) (2024)
49. Hartman, C, Weiss, B, and Shaoul, R. Nutritional supplementation with polymeric diet enriched with transforming growth factor-beta 2 for children with Crohn's disease. IMAJ. (2008) 10:503–7.
50. Pigneur PL, B, Mondot, S, Schmitz, J, Goulet, O, Doré, J, and Ruemmelea, FM. Mucosal healing and bacterial composition in response to enteral nutrition vs steroid-based induction therapy—a randomised prospective clinical trial in children with Crohn’s disease. J Crohns Colitis. (2019) 13:846–55. doi: 10.1093/ecco-jcc/jjy207
51. Diederen, KHK, Koole, JCD, Benninga, MA, and Kindermann, A. Diet and anthropometrics of children with inflammatory bowel disease: a comparison with the general population. Inflamm Bowel Dis. (2018) 24:1632–40. doi: 10.1093/ibd/izy027
52. Kevin Whelan, TM, Morgan, M, Cummings, F, Stansfield, C, Todd, A, Sebastian, S, et al. Food-related quality of life is impaired in inflammatory bowel disease and associated with reduced intake of key nutrients. Am J Clin Nutr. (2021) 113:832–44. doi: 10.1093/ajcn/nqaa395
53. Corina Hartman, LM, Davidson, K, Mozer-Glassberg, Y, Poraz, I, Silbermintz, A, Zevit, N, et al. Food intake adequacy in children and adolescents with inflammatory bowel disease. J Paediatric Gastroenterol Nutrit. (2016) 63:437–44. doi: 10.1097/MPG.0000000000001170
54. Rempel, J. Micronutrient deficiencies and Anemia in children with inflammatory bowel disease. Nutrients. (2021) 13:1–14. doi: 10.3390/nu13010236
55. Murray, HB, Harer, KN, and Keefer, L. Psychological considerations in the dietary management of patients with DGBI. Am J Gastroenterol. (2022) 117:985–94. doi: 10.14309/ajg.0000000000001766
56. Anne, R, Lee, BL, and Lebovits, J. Factors associated with maladaptive eating behaviors, social anxiety, and quality of life in adults with celiac disease. Nutrients. (2021) 13:1–10. doi: 10.3390/nu13124494
57. Haas, AM. Feeding disorders in food allergic children. Curr Allergy Asthma Rep. (2010) 10:258–64. doi: 10.1007/s11882-010-0111-5
58. Jaana, NA-JM. Facilitators and barriers to adherence to gluten-free diet among adults with celiac disease: a systematic review. Hum Nutr Diet. (2020) 33:786–810. doi: 10.1111/jhn.12754
59. Woodside, J. Culturally adapting the Mediterranean diet pattern – a way of promoting more ‘sustainable’ dietary change? Br J Nutr. (2022) 128:693–703. doi: 10.1017/S0007114522001945
60. Baker, EA, Schootman, M, Sawicki, M, and Motton-Kershaw, FL. Adaptation of a modified DASH diet to a rural African American community setting. Am J Prev Med. (2016) 51:967–74. doi: 10.1016/j.amepre.2016.07.014
61. Rotem Sigall Boneh, SP, Arcucci, MS, Herrador-López, M, Sarbagili-Shabat, C, Kolonimos, N, Wierdsma, N, et al. Cultural perspectives on the efficacy and adoption of the Crohn’s disease exclusion diet across diverse ethnicities: a case-based overview. Nutrients. (2024) 16:3184. doi: 10.3390/nu16183184
62. Emma Landorf, PH, Abu-Assi, R, Ellison, S, Boyle, T, Comerford, A, and Couper, R. Formula modifications to the Crohn's disease exclusion diet do not impact therapy success in paediatric Crohn's disease. J Pediatr Gastroenterol Nutr. (2024) 80:252–3. doi: 10.1002/jpn3.12413
63. EFSA Panel on Contaminants in the Food Chain (CONTAM). Scientific opinion on arsenic in food. EFSA J. (2009) 7:1351. doi: 10.2903/j.efsa.2009.1351
64. De Cosmi, V, Milani, GP, and Agostoni, C. Dietary patterns vs. dietary recommendations. Front Nutr. (2022) 8:806. doi: 10.3389/fnut.2022.883806
65. Bere, E, and Brug, J. Towards health-promoting and environmentally friendly regional diets - a Nordic example. Public Health Nutr. (2009) 12:91–6. doi: 10.1017/S1368980008001985
66. Organization EFS. Food Additives: European Food Safety Organization; (2024). Available online at: https://www.efsa.europa.eu/en/topics/topic/food-additives (Accessed February 15, 2024).
67. Fitzpatrick, JA, Smith, RL, Taylor, KM, and Halmos, EP. Clinical trial: the effects of emulsifiers in the food supply on disease activity in Crohn's disease: an exploratory double-blinded randomised feeding trial. Aliment Pharmacol Ther. (2025) 61:1276–89. doi: 10.1111/apt.70041
68. Benoit Chassaing, OK, Goodrich, J, Poole, A, and Srinivasan, S. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature. (2015) 519:92–6. doi: 10.1038/nature14232
69. Blomhoff, R, Andersen, R, Arnesen, EK, Christensen, JJ, Eneroth, H, Erkkola, M, et al. Nordic Nutrition Recommendations 2023. Copenhagen: Council of Ministers (2023).
70. Bischoff, SC, Bager, P, Escher, J, Forbes, A, Hebuterne, X, Hvas, CL, et al. ESPEN guideline on clinical nutrition in inflammatory bowel disease. Clin Nutr. (2023) 42:352–79. doi: 10.1016/j.clnu.2022.12.004
71. Dawson, R, Wands, DIF, and Bremner, G. Comparing effectiveness of a generic Oral nutritional supplement with specialized formula in the treatment of active pediatric Crohn’s disease. Inflamm Bowel Dis. (2022) 28:1859–64. doi: 10.1093/ibd/izac039
72. Michael Logan, KG, Svolos, V, Nichols, B, Milling, S, Seenan, JP, Macdonald, J, et al. Analysis of 61 exclusive enteral nutrition formulas used in the management of active Crohn’s disease—new insights into dietary disease triggers. Aliment Pharmacol Ther. (2020) 51:935–47. doi: 10.1111/apt.15695
73. Rotem Sigall Boneh, CSS, Yanai, H, Chermesh, I, Avraham, SB, Boaz, M, and Levine, A. Dietary therapy with the Crohn’s disease exclusion diet is a successful strategy for induction of remission in children and adults failing biological therapy. J Crohn's Colitis. (2017) 11:1205–12. doi: 10.1093/ecco-jcc/jjx071
74. Sigall Boneh VMN-L, R, Hussey, S, Pujol-Muncunill, G, Lawrence, S, Rolandsdotter, H, Otley, A, et al. Modified Crohn’s disease exclusion diet maintains remission in pediatric Crohn’s disease: randomized controlled trial. Clin Gastroenterol Hepatol. (2024). 26:S1542–3565. doi: 10.1016/j.cgh.2024.12.006
75. Henit Yanai, AL, Hirsch, A, Boneh, RS, Kopylov, U, Eran, HB, Cohen, NA, et al. The Crohn’s disease exclusion diet for induction and maintenance of remission in adults with mild-to-moderate Crohn’s disease (CDED-AD): an open-label, pilot, randomised trial. Lancet. Gastroenterol Hepatol. (2022) 7:49–59. doi: 10.1016/S2468-1253(21)00299-5
76. Van Limbergen, J, Griffiths, AM, and Critch, J. Toward enteral nutrition in the treatment of pediatric Crohn disease in Canada: a workshop to identify barriers and enablers. Can J Gastroenterol Hepatol. (2015) 29:351–6. doi: 10.1155/2015/509497
77. Marialaura Cuomo, M, Carobbio, A, and Aloi, M. Induction of remission with exclusive enteral nutrition in children with Crohn’s disease: determinants of higher adherence and response. Inflamm Bowel Dis. (2023) 29:1380–9. doi: 10.1093/ibd/izac215
78. Bednarczuk, B, and AC-K,. Role of nutritional support provided by qualified dietitians in the prevention and treatment of non-communicable disease. Rocz Panstw Zakl Hig. (2019) 70:235–41. doi: 10.32394/rpzh.2019.0080
79. Position of the Academy of Nutrition and Dietetics. The role of medical nutrition therapy and registered dietitian nutritionists in the prevention and treatment of prediabetes and type 2 diabetes. J Acad Nutr Diet. (2018) 118:343–53. doi: 10.1016/j.jand.2017.11.021
Keywords: pediatric Crohn’s disease, nutritional treatment, Crohn’s disease exclusion diet, enteral nutrition, Nordic diet
Citation: Vivanco Karlsson N, Sigall-Boneh R, Mårild K and Hård Af Segerstad EM (2025) Adapting the Crohn’s disease exclusion diet to a Nordic framework: a theoretical approach to cultural and nutritional customization. Front. Nutr. 12:1590847. doi: 10.3389/fnut.2025.1590847
Edited by:
Arianna Dal Buono, Humanitas Research Hospital, ItalyReviewed by:
Salvatore Vaccaro, IRCCS Local Health Authority of Reggio Emilia, ItalyArtur Delgado, São Paulo University, Brazil
Copyright © 2025 Vivanco Karlsson, Sigall-Boneh, Mårild and Hård Af Segerstad. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: N. Vivanco Karlsson, bmFsbGVsaS52aXZhbmNvLmthcmxzc29uQGd1LnNl