 Pedro E. Rodríguez
Pedro E. Rodríguez Ayda Pantoja-Santander
Ayda Pantoja-Santander Alejandra Sapene
Alejandra Sapene Cástulo Cisneros3†
Cástulo Cisneros3†- 1Department of Psychosocial Studies, Faculty of Psychology, University of the Valley, Cali, Colombia
- 2Asociación Civil Trazando Espacios, Caracas, Venezuela
- 3Fundación Universitaria San Martín, Bogotá, Colombia
Ethnic minorities are exposed to greater risks of mental health problems than other groups, intensified during specific developmental periods by gender, psychosocial factors, racism, stigmatization, and social exclusion. In Colombia’s Pacific region, the Emberá Indigenous population has experienced a significant number of youth suicides in recent years, described as a “suicide epidemic.” This study aimed to deepen the understanding of suicide among Emberá youth by analyzing its characteristics, the institutional and professional strategies addressing it, and the processes of institutional racism and social exclusion at play. A collective case study approach was applied, drawing on primary and secondary sources, including interviews and a documentary review of 76 materials, to provide a contextualized understanding of suicide incidence in the Chocó region and to inform future educational, community, and activist actions. Findings indicate that suicidal behavior in this group has distinctive characteristics requiring approaches that go beyond nominal cultural sensitivity, engaging directly with lived realities and structural conditions. Current strategies reveal significant weaknesses, particularly in coordination and in adopting intersectional perspectives to address multi-problematic contexts. Results also highlight the impact of racism and exclusion on the emotional experiences of Emberá youth, expressed through both institutional discrimination and internalized racism. The study concludes by proposing the strengthening of institutional racism and psychosocial exclusion as analytical tools for addressing violence and invisibility in suicide cases, while emphasizing future pathways for action, particularly the active participation of young people in the design, implementation, and monitoring of protective strategies against suicide risk.
1 Introduction
Subjected to historical conditions of vulnerability and precariousness, as well as significant processes of defenselessness due to limited state protection, indigenous communities in Colombia face high rates of poverty, victimization from armed conflict, displacement, barriers to services, and elevated physical and mental health risks, including suicidal behavior (Ministerio de Salud y Protección Social, 2016; Departamento Administrativo Nacional de Estadística – DANE, 2021; Estévez-Paz et al., 2024; Centro Nacional de Memoria Histórica Ministerio de Cultura—Museo Nacional de Colombia, 2017). Constitutional Court Ruling 004 of 2009 recognized several Indigenous groups as at risk of extinction. Precautionary measures by the Inter-American Commission on Human Rights (2015) and the Constitutional Court’s Judgment T-302 of 2017 regarding the Wayuu (Corte Constitucional, 2017) also acknowledged violations of fundamental rights to different indigenous communities.
Indigenous peoples have endured violence and dehumanization from colonial times to the present. Episodes such as the 1967 murder of 16 Cuiba in the Colombian plains, where the defense argued that hunting Indigenous people was a common practice and that the accused were therefore unaware they were committing a crime (Castro, 1976; García, 2013, 2022), as well as massacres such as the 1971 Planas massacre, carried out by military forces, and the 2002 Bojayá massacre in Chocó, in which at least 79 people were killed during combat between FARC and paramilitary groups (National Center for Historical Memory, 2012), which together illustrate a persistent dehumanization dating back to the Conquest (Gómez-López et al., 2012; Martínez Silva et al., 2020; Urrego-Mendoza et al., 2017; Urrego-Mendoza et al., 2017), repeatedly denying Indigenous peoples full recognition of their personhood.
In addition to these historical inequalities, Indigenous and Afro-descendant groups are also central to studies of racialization, psychosocial exclusion, and political change due to their demographic importance. According to DANE, 14.4% of Colombia’s population self-identifies as Indigenous or Afro-descendant. In the 2018 Census, 1,905,617 people identified as Indigenous, belonging to 115 communities and 65 languages, placing Colombia among the countries with the greatest Indigenous diversity.
Constitutionally, Colombia has shifted from a mestizo ideal of “national homogeneity” to a multicultural vision that embraces “difference,” however, such discursive transformations have not ended practices of racial and ethnic invisibility, exclusion, and discrimination (Viveros-Vigoya, 2015; Wade, 2021).
Among the various forms of vulnerability and psychosocial suffering experienced by Indigenous peoples, the so-called “suicide epidemic” among Emberá youth, reported since at least 2003, stands out as both a pressing research problem and an urgent challenge for policy and intervention.
The Emberá live in Colombia, Panama, and Ecuador. In Colombia, they inhabit the Pacific region (Chocó, Cauca, Nariño, Antioquia, Córdoba, Risaralda, and Quindío). The 2018 census reported 77,714 Emberá, predominantly in Chocó. Family lines include Chamí, Katío, Dóbida, and Eperara Siapidaara. They share a common language with internal variations between families and a worldview of “three worlds,” a strong territorial bond, and traditional medicine to sustain balance and harmony. Subsistence relies on hunting, fishing, gathering, and shifting agriculture; however, following colonization and, more recently, as a result of mobility restrictions and climate change, communities have experienced territorial dispersion and increasing sedentarization. Social organization centers on the extended family with gender- and age-based divisions of labor. The economy is largely endogenous, with minimal participation in external markets. Traditional authorities include the family head (often the eldest) and the jaibaná, ancestral doctor and key figure in their religious practices. Legal reforms introduced the Indigenous Council, and younger members have emerged as leaders (Romero-López et al., 2019).
The Emberá have historically suffered multiple violations of living conditions. According to a report by the Association of Indigenous Councils and Authorities of the Chocó Department [OREWA], between 1985 and 2012, more than 30,000 Emberá were displaced from their territories by the armed conflict, representing 30% of their population (Romero-López et al., 2019; Orewa, 2013). They have also faced extractivism (Urrego-Mendoza et al., 2017; Bello and Rangel, 2002), acculturation and complex intergroup relations (de Sepúlveda López Mesa, 2008; UNICEF, 2012; Ministerio de Salud y Protección Social and Organización Panamericana de la Salud, 2016; Martínez Silva et al., 2020), and diverse forms of vulnerability and discrimination (UNICEF, 2012, 2017; Dolezal et al., 2021; National Alliance of Mental Illness, 2021; World Health Organization, 2014, 2021).
Among the highest-risk groups, the literature presents a historical record of elevated rates of suicidal behavior among indigenous peoples (UNICEF, 2012; Vargas et al., 2017; Dolezal et al., 2021; National Alliance of Mental Illness, 2021; World Health Organization, 2021; Estévez-Paz et al., 2024; Pollock et al., 2018). In Colombia, among cases where group identity was identified, 87% involved Indigenous, Afro-descendant, palenqueros and gypsies (Instituto Nacional de Medicina Legal y Ciencias Forenses, 2023). Other reports indicate suicide risk was 2.7 times higher among Indigenous people than non-Indigenous in Amazonas between 2008 and 2016 (Estévez-Paz et al., 2024), and higher than the national rate in Vaupés (Martínez Silva et al., 2020). Thus, evidence suggests that the suicide rates in Indigenous communities substantially exceed general and national prevalence (Departamento Administrativo Nacional de Estadística – DANE, 2021; Ministerio de Salud y Protección Social, 2018; World Health Organization, 2014).
In the case of the Emberá, despite significant underreporting, the prevalence is higher than among other Indigenous groups in Colombia, with patterns that diverge from national and global trends in terms of gender, causes, and symptoms (MINSALUD/PAHO, 2016). Humanitarian organizations estimate that in parts of Chocó the rate may be eight times the national rate (Romero-Peñuela, 2024). In September 2024, Asociación Orewa (2024) stated: “We receive daily reports from the territories about suicides in our communities, especially among young people and adolescents, which concerns us even more”.
Research on Indigenous mental health, and on the Emberá in particular, remains limited, producing contradictions and gaps. Most records come from state institutions and show recurrent underreporting, partial data, and, at times, non-comparable or biased information (Tuesca-Molina et al., 2019). Regarding racism and psychosocial exclusion, documentation is limited to mere acknowledgements of their presence, without the support of systematic or rigorous empirical investigations.
Across the social and health sciences, models of suicidal behavior include sociological (Durkheim, 2008), psychodynamic (Freud, 1996), cognitive (Beck, 1976), interpersonal (Van Orden et al., 2010), contextual–existential (González González et al., 2021), and, more recently, the neurobiological stress–diathesis model (Ganança et al., 2015). Approaches to Emberá youth suicide can be grouped into clinical, cultural, and psychosocial perspectives. These perspectives have coexisted without major contradictions due to the different emphases of their approaches.
Despite the value of these approaches and the efforts to avoid psychologizing suicide, the Emberá case exposes challenges in accounting for situated social and cultural factors. For example, Vásquez (2023) found that prior psychiatric diagnoses did not sufficiently predict suicidal behavior in the Colombian population; socioeconomic and spatial indicators did. From the earliest theories, suicide behavior has a strong social content (Durkheim, 2008). Likewise, psychological models have shifted from individual explanations to empirical, contextual recognition of inequality and exclusion (Rodríguez, 2021). Yet the effects of racialization and psychosocial exclusion on the Emberá remain scarcely documented.
We argue that understanding the “suicide epidemic” among Emberá youth benefits from the lenses of psychosocial exclusion and institutional racism. Psychosocial exclusion highlights intersectional factors often neglected by psychological approaches and is defined as the systematic denial of opportunities to participate in the material, political, ideological, technical, and symbolic benefits of culture for a given group, either by denial or by the absence of a psychosocial niche to desire them (Rodríguez, 2021). These processes constitute major mental health risks by integrating multiple sources of vulnerability (Andersen, 2006).
Racism is understood as a set of discursive, practical, and representational operations (Hall, 2017; Wallerstein and Balibar, 1988) that manifest as violence, discrimination, humiliation, intolerance, segregation, and dispossession, articulated through prejudice, inferiorization, invisibility, stigmatization, stereotyping, and physical and social exclusion (Buraschi and Aguilar-Idañez, 2019; Wallerstein and Balibar, 1988). It produces both racist communities and racialized communities that, “as in a mirror, are forced to perceive themselves as a community” (Wallerstein and Balibar, 1988, p. 32), introducing the contradiction of attributing identities to communities that, as Fanon (2009) pointed out, are at the same time denied the right to define themselves; thus, racism involves different social and institutional actors with different interests and positions of power, expressed in historical, political and economic frameworks which, despite their variations, share processes and mechanisms that produce suffering and social harm.
This study proposes focusing on the notion of institutional racism as a way to explore the dimension of racialization. The notion was originally formulated by Carmichael and Hamilton (1967), referring to the legal framework and behavioral patterns of oppression towards Black people. Following Buraschi and Aguilar-Idañez (2019), we understand institutional racism as a system of policies, discourses, practices, and procedures implemented by institutional entities, their agents, and professionals within care systems. These actions undermine the rights of individuals and groups on racial and ethnic grounds, manifesting in prejudiced processes, ignorance, stereotypes, and disregard, among other forms of discrimination.
Institutional racism in Indigenous contexts has been only partially addressed on the continent. Existing approaches have primarily examined the criminal justice system (Rotta-Almeida et al., 2021) and barriers to healthcare access (Thomazinho, 2024) in Brazil, as well as enforced disappearance (Mora, 2017) and governmental discourse (Orozco-López, 2018) in Mexico, thereby reflecting diverse perspectives with different points of emphasis. In the case of Colombia, the scarce references available tend to focus predominantly on Afro-Colombian communities (Restrepo, 2009; Mosquera Rosero-Labbé and León Díaz, 2015; Martelo Ortiz, 2021).
The notions of institutional racism and psychosocial exclusion constitute valuable analytical tools for examining the problem of suicide among Indigenous youth, insofar as they make it possible to discern multiple dimensions related to health, living conditions, and the interactions between Indigenous social actors and those from other contexts. Authors such as Cortez-Gómez et al. (2020), for example, in their analysis of health-related dimensions, have identified as manifestations of racism towards Indigenous communities the absence of programs or resources, geographical barriers to care, as well as discriminatory practices by health personnel. Institutions as Ministerio de Salud y Protección Social (2016) and Ministerio de Salud y Protección Social and Organización Panamericana de la Salud (2016), have documented the weight of prejudice and racialization affecting Indigenous communities in Colombia. An approach that more broadly explores the intersectionalities associated with the phenomenon of suicide among Emberá youth could provide an opportunity not only to deepen understanding of the phenomenon, but also to inform public policy debates and diversify potential avenues for intervention.
This study has the general objective to provide a deeper understanding of suicide among Emberá Indigenous youth in the Colombian Pacific through the analysis of racialization and psychosocial exclusion. Specifically, it aims to describe the characteristics of suicide among Emberá youth as reported by Indigenous, institutional, and professional actors. Secondly, it is proposed to examine institutional and professional mechanisms and strategies addressing suicide among Emberá youth. Finally, it aims to analyze the mechanisms of institutional racism and psychosocial exclusion involved in the suicide phenomenon among Emberá youth.
To fulfill its research objective, this study employs a collective case study design, which enables the incorporation of the widest possible range of voices and social actors involved in the issue of suicide among Emberá youth. To this end, a multi-source approach will be employed. The findings are expected to foster dialogue with public and private institutions, as well as with the communities involved, with the aim of contributing to decision-making processes and analytical inputs for public policy, the design of contextualized interventions, and greater awareness of the needs and perspectives of Indigenous communities facing these living-condition challenges.
2 Materials and methods
2.1 Design
This research is a collective case study (Stake, 1995), understood as a design in which multiple cases or units of analysis are examined to provide a detailed and comprehensive understanding of a phenomenon. In this study, the general objective was to deepen the understanding of suicide among Emberá Indigenous youth in the Colombian Pacific by analyzing processes of racialization and psychosocial exclusion. To this end, the study incorporated various primary and secondary data sources related to cases of suicide among young people in the Emberá community.
2.2 Study population
The unit of analysis comprised verbal data concerning suicide among Emberá Indigenous youth, originating from a total of six sources, as presented in Table 1.
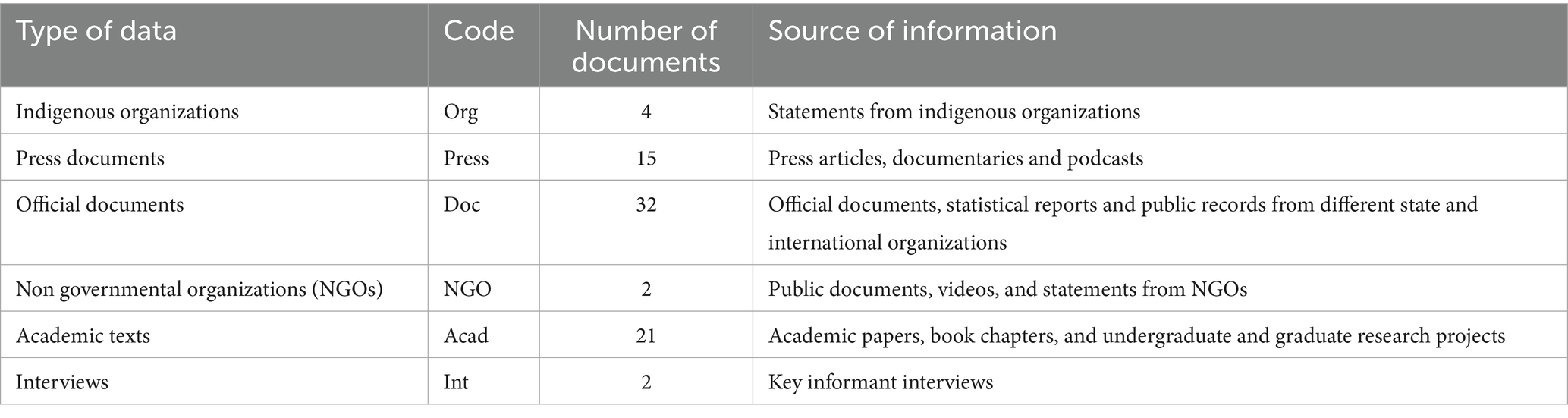
Table 1. Type of data and source of information.
The selected data came from two major analytical sets: interviews and documents.
Interviews: Two in-depth semi-structured interviews were conducted with two key informants, selected according to a criterion of convenience. The first interview involved an Indigenous woman who had lived in the territory under study. This interview, conducted prior to the present research, explored participant’s subjective experiences concerning mental health in relation to her ethnic identity. The second interview involved the local coordinator of an NGO with extensive experience in interventions in the context of interest for this research. This semi-structured interview addressed the phenomenon of suicide among Emberá youth, intervention practices, case characterizations, and the participant’s observations on racism and exclusion.
Documents: In the case of the documents used for this study, materials were selected if they:
1. Addressed suicide or mental health among Emberá youth in the Colombian Pacific.
2. Related to suicide or mental health in other Colombian Indigenous populations; or.
3. Consisted of official or institutional Colombian reports on Indigenous suicide or mental health.
Two main strategies were used to collect the documents:
1. Review of materials collected by the authors in intervention and advisory activities prior to the research; and
2. Conducting search of materials from Indigenous organizations, public institutions, and NGOs, as well as academic materials available digitally.
The search criteria corresponded to the terms: “suicide,” “Indigenous Emberá People,” “Colombia,” “suicide epidemic.” Academic materials were identified using the following search engines: Scopus, Google Scholar, Redalyc, Scielo, and Dialnet. Both peer-reviewed publications and gray literature were included.
2.3 Sample size
As this was a collective case study, the design did not aim for generalization but rather the deepest possible exploration of the materials related to the case. Once the data for the study were collected and selected, a total of 76 data were included. The complete list of materials is presented in the Supplementary material.
2.4 Analysis strategy
The methods followed the four steps for case study research described by Yin (2009):
1. Defining and selecting the cases: the case study was defined by relevant data on suicide among Emberá youth. For this purpose, all available data were initially considered, and classified into six large sets of data producers according to the reported selection criteria.
2. Using multiple cases: data were obtained from Indigenous Organizations, Press Documents, Official Documents, NGOs, Academic Publications, and Interviews, consolidating a total of six large sets of information that provided diverse perspectives and interests.
3. Strengthening the evidence using different data sources and techniques: the documents were treated as “standardized artifacts” and grouped based on their specific production formats (Wolff, 2004). Each type of data was given an abbreviated code, later used to categorize each piece of data based on a number and the year of production.
4. Analyzing the evidence: once the materials were collected, an initial relevance filter was performed. Two categories were consolidated: (a) data related to the Emberá people, particularly youth; and (b) data related to other Colombian indigenous communities.
Following an initial review, a categorical aggregation (Stake, 1995) was performed using an analytic induction process (Mitchell, 2000), seeking patterns of correspondence between data and their possible associations with other relevant themes. This process was conducted through thematic content analysis (Bardin, 1986), in three general phases: pre-analysis; exploitation of the material, and treatment and interpretation of the results. The aim was to identify “nuclei of meaning” that make up the communication and whose presence, or frequency of appearance, could mean something for the chosen analytical objective” (p. 80). The three stages involved the realization of processes of coding, categorization and inference, resulting in the themes presented in the results.
In line with the research objectives, metacategories were initially organized as a theoretical reference using the three criteria proposed by Devereux (1961) concerning ethnographic aspects of suicidal behavior in the Mohave Indian Tribe. These were: (a) Self-image; (b) Lay characterizations; (c) Professional characterizations. Once the categorization process was completed, the researchers established three broad metacategories.
1. Characterization of Suicide: findings on the characteristics of suicide in the Emberá group.
2. Intervention devices and strategies: findings related to professional and institutional intervention processes.
3. Suicide, racism, and exclusion: themes related to racism and psychosocial exclusion.
These three metacategories correspond to the specific objectives of the research.
Although the process allowed for the consolidation of a relevant dataset reflecting diverse voices and interests, some limitations and biases must be acknowledged. First, due to the difficulty of accessing informants, the findings depended heavily on the quality of the available materials, which may not fully capture the complexity of the phenomenon. Furthermore, the sources are not free from potential contradictions as well as professional and academic biases.
2.5 Ethics statement
Giving the highly vulnerable conditions of the studied group, this research adopted a minimally invasive design, excluding direct contact with members of the Emberá population, including survivors or family members. To this end, the data used in this research relied on both primary and secondary sources.
Primary data involving human subjects, collected prior to the start of the study, were approved by the Ethics Committee of the Faculty of Psychology at Universidad del Valle, Cali, Colombia (no. CEIFP-47-24) in response to a formal request for approval made by APS. Primary data collected during the study included signed informed consent. Secondary data were obtained from publicly available documentary sources and did not require the request for informed consent. All procedures were conducted in accordance with local legislation and institutional requirements.
3 Results
3.1 Metacategory 1: characterization of suicide
3.1.1 Characteristics of suicide
Assuming the limitations of underreporting, the occurrence of suicidal acts in remote locations, as well as possible cultural biases, it is possible to present the following characterization of suicides among the Emberá people in the Chocó region.
3.1.1.1 Young people as the predominant age group
Sources indicate that the age group most at risk is children and adolescents (Acad.3.2023; Acad.3.2017; Doc.5.2016; Acad.2.2021; Press.2.2024; Press.3.2024; Doc.4.2024). Between 2003 and 2006, at least 20 suicides were reported, mostly among adolescents and young adults (Press.1.2003; Acad.1.2008). Another report cites 30 cases between 2009 and 2015 (Acad.1.2017). Indigenous organizations documented at least 200 youth suicides from 2000 to 2016 (Org.1.2016), and in 2020 more than 10 cases were reported in the municipality of Bojayá (Org.2.2020). Of the 22 suicides recorded in 2021, 20 involved individuals under 18 years of age (Press.2.2021). Similar proportions are reported among the Dobidá, where adolescents and youth account for the majority compared to adults (Acad.1.2017). In 2023, an Indigenous leader reported 343 cases recorded by his organization since the beginning of the so-called “epidemic” (Doc.1.2023).
3.1.1.2 Gender variations
Official and unofficial sources show changing gender patterns. Current reports indicate that suicide rates among young Emberá women are equal to or higher than those among men (Acad.1.2017; Acad.1.2020; Acad.2.2021; Press.1.2024). This contrasts with other Colombian Indigenous groups and global epidemiological trends, where male suicides typically predominate at ratios of up to 7:3 (Acad.1.2020; Doc.6.2023).
Regarding the gender issue, the data show some differential patterns, such as physical aggression prior to suicide in women (Acad.1.2017), greater cultural shocks in women due to the impossibility of accessing Western products, as well as exposure to different lifestyles by non-indigenous professional women (Acad.1.2017), greater willingness to replicate the suicidal act (Acad.1.2017).
3.1.1.3 Location
Although there are references to suicides from the 1990s (Doc.5.2016), documented cases begin in 2003 on the Salaquí River (Press.1.2003; Acad.1.2008). Reports from Indigenous organizations describe a dispersed pattern across Chocó, including Quibdó, Juradó, Istmina, Litoral del San Juan, Bojayá, Medio San Juan, Riosucio, and Bahía Solano (Doc.1.2023). Official registries also indicate differential victimization patterns linked to armed conflict affecting the Emberá (Alto and Bajo Baudó, Bojayá, Carmen del Darién), Emberá Katío (Bagadó), Emberá Chamí (Quibdó, San José del Palmar), Emberá Dobidá (Bojayá, Medio Baudó), and Wounaan (Litoral del San Juan, Bajo Baudó) (Doc.2.2021). These dynamics are crucial for detection and intervention, given the relationship between violence and suicidal behavior.
3.1.1.4 Suicide techniques
Methods vary over time. In the first decade, poisoning predominated, consistent with national trends; more recently, hanging has become the most frequent method (Doc.5.2016; Acad.3.2017). It typically involves the paruma (traditional Emberá skirt) and may occur either at home (tambo) or in remote areas (Acad.1.2008). No data specify gender or motive differences. This contrasts with findings from the National Institute of Forensic Medicine, which documented predominance of male suicides and poisoning between 2010 and 2014 in the general population (Doc.1.2014).
3.1.1.5 Symptoms and manifestations
Distinctive patterns are observed among young Emberá, some of which are not documented either in the general Colombian population or in other Indigenous groups (Acad.1.2008; Acad.1.2012; Acad.2.2014; Acad.1.2017; Acad.1.2020; Acad.3.2023). Table 2 shows these symptoms and manifestations as reported by both native professional and institutional characterization.
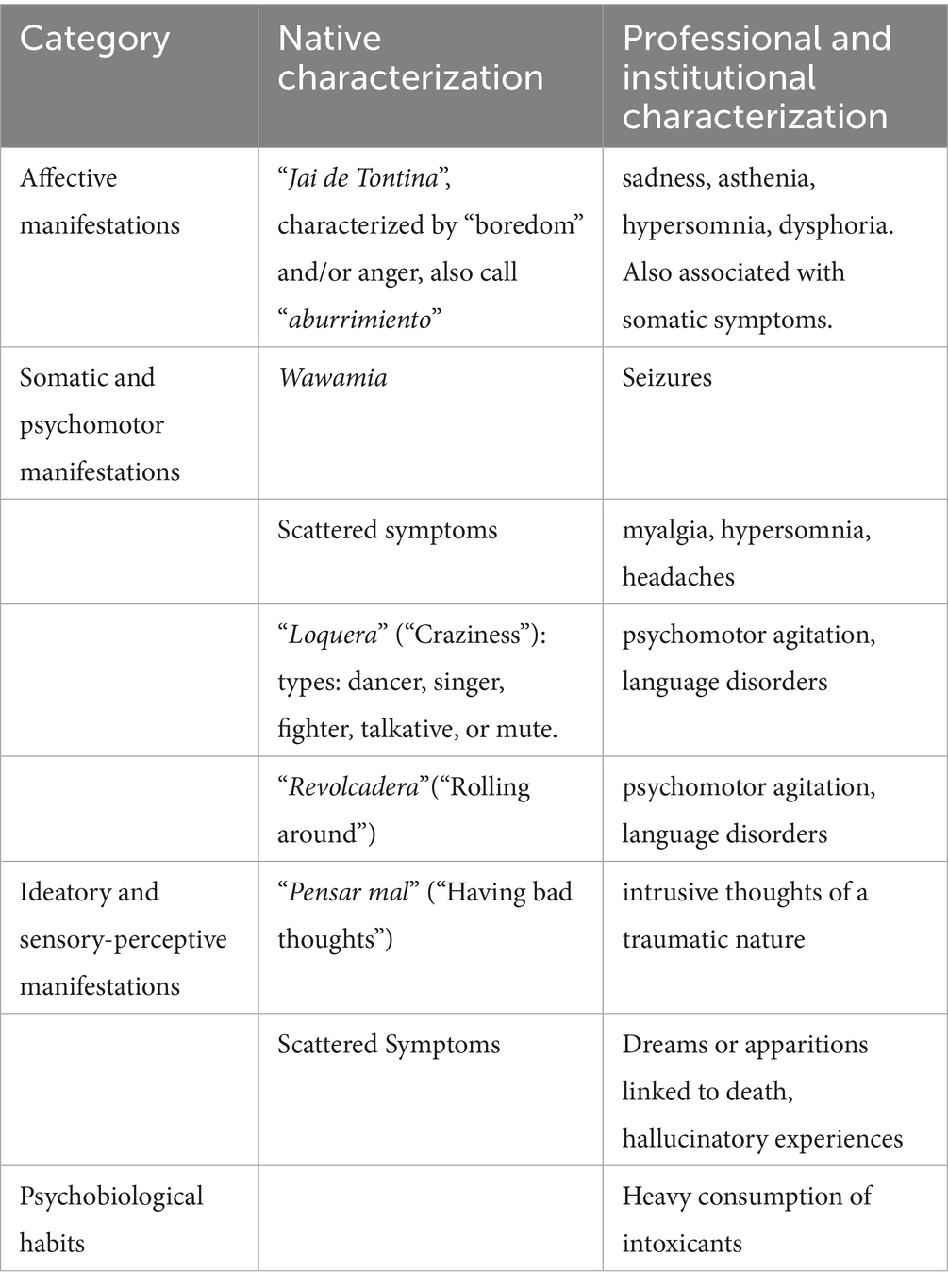
Table 2. Symptoms and manifestations.
The classification presented omits dynamic elements and possible variations between groups. Nor does it correspond to a clinical pattern. For example, while almost all suicide cases have manifested Wawamia, not all Wawamia cases lead to suicide attempts (Acad.1.2012).
Some illustrations: “Before killing herself, after tontina and revolcadera, she dreamed a lot” (Acad.1.2008). Another illustration of aburrimiento: “One gets aburrido (bored), maybe they do not like you and all that, then one gets bored like that. That’s why one thinks a lot of things… one stays bored, ehh… like sick, loses one’s mind. Well, they do a lot of things. On that side, many people have also been killed like that.” (Acad.1.2022). Other: “She started with that tontina, that jai that would not leave her alone. Headache, her bones feeling like they were being squeezed… well, like she was sick with malaria, that’s all. But then she started with that thought. She pensaba mal (thought badly) and pensaba mal (thought badly). She told me she missed her children a lot (…) that there was nothing to eat, what were we going to do (…) that life wasn’t worth living like this…” (Acad.1.2008).
3.1.1.6 Types and causes of suicidal behavior
Considering the native and historical categories of Indigenous peoples, the material allows us to identify three types of suicide, each associated with different causes. There are potential overlaps between types and causes, particularly regarding the effects of violence from armed conflict and illegal groups. The classification presented here seeks to aid understanding; in practice, motives and causes are dynamic, cumulative, and interdependent, as reported by multiple sources (Acad.1.2008, Acad.1.2022).
3.1.1.7 Suicide as a native category
Interview reports and bibliographical material allow suicide to be characterized as the result of the action of evil spirits, “curses,” and disharmonies marked by spiritual components and the relationship with the territory. At the same time, both official and investigative literature report this type of suicide as a culturally situated modality.
To facilitate the presentation of the material, the results are shown in Table 3.
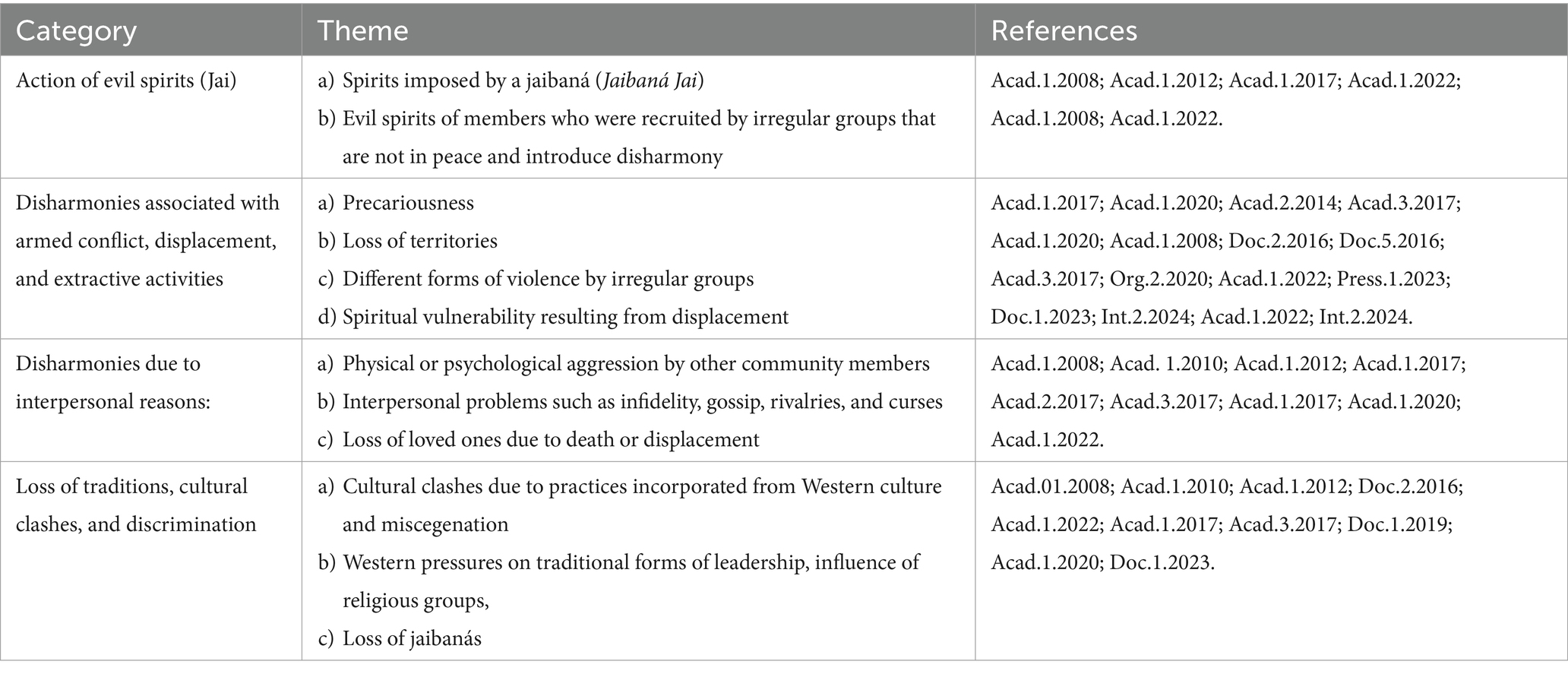
Table 3. Types and causes of suicide in native category.
It is necessary to emphasize that in this case, there is significant cultural contextualization in the group. While disharmony may encompass different elements that could be interpreted by external groups as a unity, the available material allows specificities that are not always captured.
Perhaps the best example is the category of displacement and armed conflict. In this context, indigenous informants’ reports provide insight into the weight of the armed conflict, incorporating nuances specific to their worldview. Disharmony is not only caused by the violent actions of armed groups, but is also perceived through the harm and blame assigned to young people who are recruited or choose to join these groups in pursuit of better livelihoods. In such cases, the responsibility of young people is seen as a factor that predisposes them to the actions of evil jais.
Another important illustration can be found in the complex handling of the figure of jaibanás. It is documented that, at the beginning of the wave of suicides, some groups interpreted the responsibility as the manipulation of evil jai for selfish purposes, such as controlling certain young women for sexual purposes. This entailed various reprisals, including the murder of jaibanás or the banishment of others (Acad.1.2008). However, just as some spiritual figures were assumed to be responsible, there is a coexisting belief that the possibility of recovery and cure in some cases could only occur through the action of “good” jaibanás who could perform the corresponding ceremonial actions while also assuming responsibility for cases that, from their perspective, would require Western therapeutic strategies.
3.1.1.8 Suicide as a professional and institutional category
The professional and institutional category allows us to differentiate three broad sets of causes or motives. To facilitate the presentation of the material, the results are shown in Table 4.
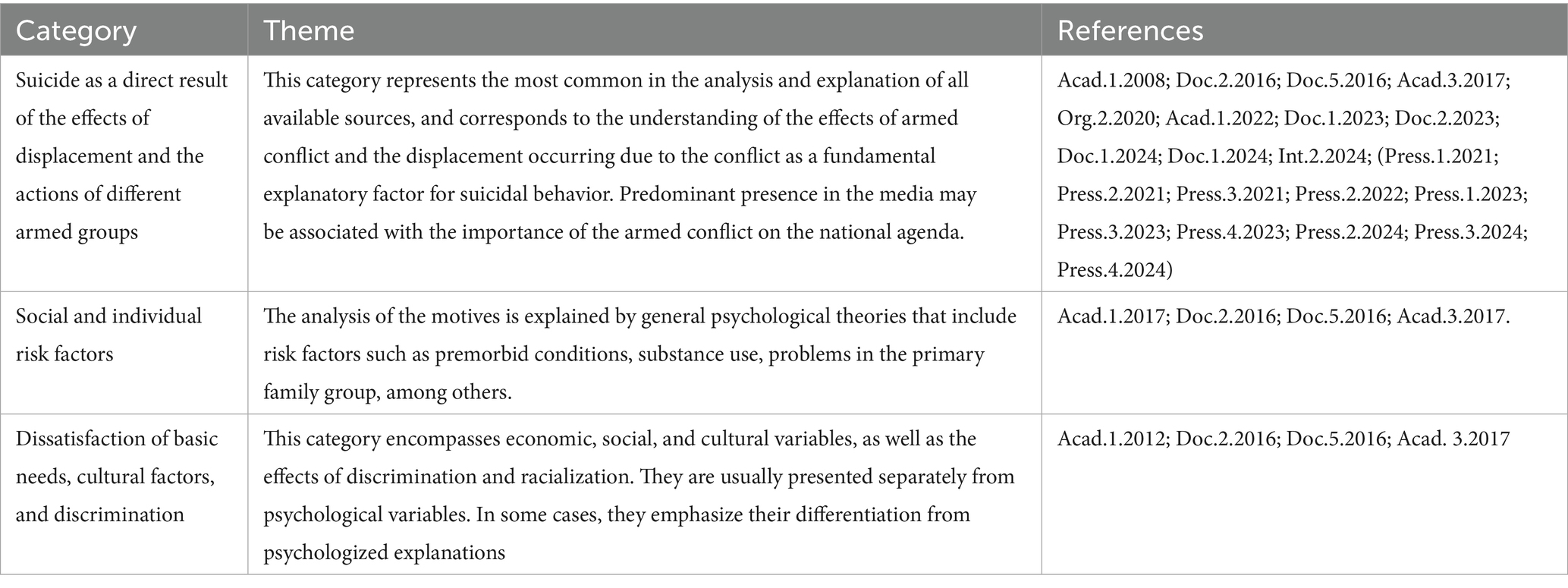
Table 4. Types and Causes as a professional and institutional category.
3.1.1.9 Collective suicide
In addition to the native and professional categories, it is possible to include a final category that could be called collective suicide, and in which native and professional records are found. Both Emberá informants, official and academic literature offer characterizations that could be attributed to contagion, as well as to individual reactions of protest or resistance. Although there are no direct reports of collective suicides among the Emberá people, others have been reported in the history of Colombian indigenous peoples, as well as in other geographical contexts. What is possible to affirm is that, in the Emberá case, the category exists as a possibility for collective suicidal action (Press.1.2007; Acad.2.2014).
Table 5 shows the different forms of collective suicide found in the analysis of the material.
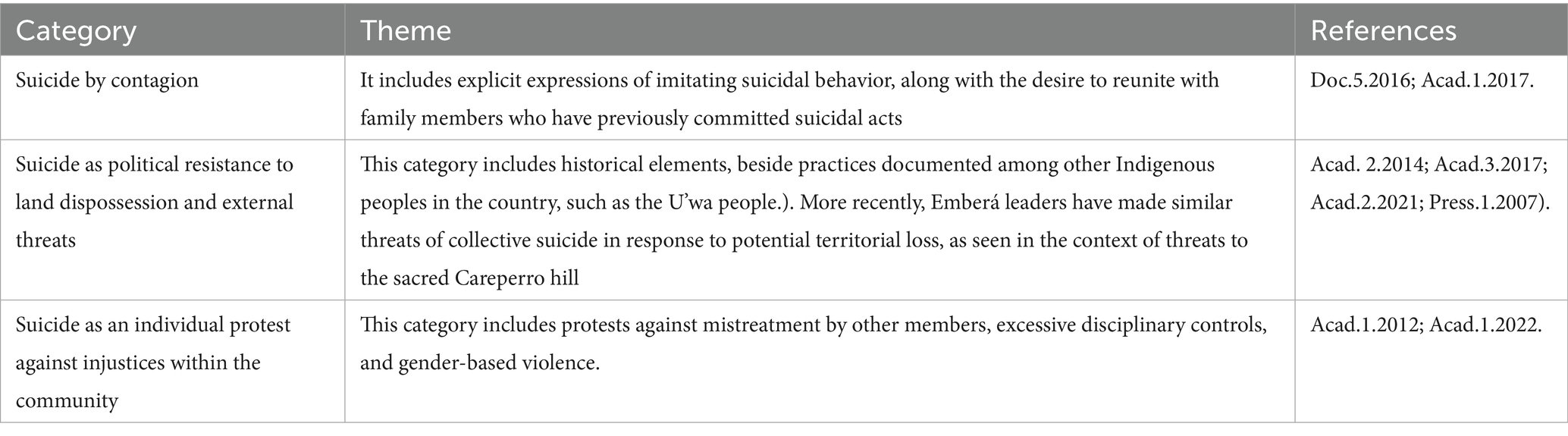
Table 5. Types of collective suicide.
Two illustrations are offered regarding this category. In relation to the issue of contagion, an informant reported: “And then this is going to happen here and it’s going to spread to another region, to another municipality, and that’s what’s happening. Look what happened… it started in Riosucio, from Riosucio it spread to the municipality of Quibdó, from Quibdó it spread to the municipality of Juradó, and from Juradó it spread to the municipality of Alto Baudó. And it’s spreading…” (Acad.1.2017).
In cases of suicide as an individual protest, suicide has an agentic interest in expressing discontent to the rest of the community. It is significant that reports in this category are associated with the suicide of women and that protests are often accompanied by elements of gender-based violence perpetrated by parents, authorities, and husbands. Reports of anger and aburrimiento (“boredom”) in response to these events are common (Acad.1.2012; Acad.1.2022). An illustration from a young Emberá girl: “If someone does not let you get married, you kill yourself. With that, you scare them, but it’s also because a voice tells you to kill, because you get bored. Then, you start thinking a lot, you get that thinking in the night and then you say that you want to kill and say that you want to kill, when you get angry…” (Acad.1.2022).
3.2 Metacategory 2: intervention devices and strategies
This section presents findings related to intervention strategies and devices for suicidal behavior. While there are elements related to the case of Emberá youth, the literature reviewed focuses on the broader set of interventions for the indigenous group across the country, which implies a more general vision than one focused on developmental periods.
3.2.1 Structural, operational, and administrative difficulties
Reports indicate that Chocó, with more than half a million inhabitants, had only one psychiatrist for the entire department in 2023 (Int.2.2024). Institutional reports indicate 314 health service providers: 2% public and 98% private, with just one secondary-level hospital in Quibdó leaving most indigenous communities without access to specialized care (Doc.3.2023; Doc.5.2024; Int.2.2024). As a result, indigenous mental health needs are frequently ignored, unreported or insufficiently addressed (Org.2.2020; Acad.1.2021).
A professional describes the gap: “There is a fundamental problem, what they do in Bogotá are evidence-based routes, so they have the best existing knowledge and that is valid, but when you arrive, leave Bogotá and take this route to any other department in Colombia, you already have a problem because of the professionals’ actions, there is no one to do it. Vaupés has 3 psychologists and there are 46,000 people, Amazonas has 6 and the problem is that those 3 psychologists are in urban areas and 80% of the population locates in rural areas, then what route works there?” (Acad.2.2020).
Institutional documents also report this situation. With insufficient staff to monitor suicidal behavior, patients must be referred outside the department. Delays often prevent access, compromising follow-up and recovery. An agent from an educational institution states: “At the school, there is only one psychologist as a school counselor. Their role is to receive and refer. Whether they provide interventions is their own matter, not their responsibility. I believe there should be another psychologist. There are 1,300 students at the school, 200 at the boarding school, 200-something at the “Nicolasito” school, and 100-something at the other campus. Only one professional for 2,000 students or so” (Doc.2.2022).
Various administrative barriers that hinder their implementation’s effectiveness are also identified (Doc.4.2016; Doc.1.2020; Doc.2.2022; Acad.1.2023). These include restricted budgets, evaluation processes, and insufficient staff for projects that must be completed within 12 months (Doc.1.2020). Professionals are sometimes required to use their financial resources to cover certain elements necessary for the intervention (Doc.1.2020; Doc.2.2022). There are also extensive administrative procedures that reduce the time and quality of interventions, and poor inter-institutional coordination delays suicide care pathways (Doc.2.2022). Access barriers for indigenous peoples also arise from language, as institutions lack translators or interpreters (Int.2.2024).
International Cooperation Organizations (ICOs) contribute to the humanitarian response in the territory. They provide general and mental health services, usually limited to emergencies: initial assessments, suicide risk identification, safety plans, and temporary support. Yet the professionals note that, despite interdisciplinary teams, institutional services remain limited by connectivity, language, and geographic barriers (Int.2.2024). Their actions, however, cannot overcome the structural difficulties. Thus, in meetings and committees, some international organizations state: “No care is provided for children and adolescents” (Doc.1.2023).
3.2.2 Monitoring limitations
Official documents monitoring suicide-related care policies are scarce. Only ICBF reports provide follow-up, specifically on suicide among indigenous youth in Vaupés (Doc.1.2020) and among the Guainía ethnic group (Doc.2.2022). This limited evidence makes it difficult to assess the efficiency and implementation of proposed models. Although all documents present explicit proposals regarding the need for community outreach, there is not enough evidence of its implementation (Doc.1.2020). One example is the technical guidelines for the prevention of suicidal behavior in the indigenous population, which advocate an intercultural approach, community participation and traditional practices (Doc.2.2016). While these guidelines emphasize strengthening families, communities, and individuals, it is not clear whether this strategy is being applied on a sustained basis, or even whether these guidelines have been implemented.
These limitations may contribute to indigenous groups’ criticism and rejection of health institutions due to deficiencies in service (Acad.3.2023), as well as to the limited impact of information and support campaigns run by both Health Secretariats and indigenous authorities (Acad.3.2017).
3.2.3 Challenges of interculturality
Since 1991, Colombia has been constitutionally recognized as a multiethnic and multicultural country, mandating the inclusion of interculturality in intervention proposals. This framework incorporates healthcare, ethno-education, prior consultation, safeguard plans, and differentiated protection mechanisms. Interculturality also values traditional therapeutic practices and requires participatory approaches involving indigenous communities in the design, implementation, and evaluation of services, with the aim of overcoming historical barriers of exclusion and discrimination (Doc.5.2016).
In 2010, indigenous leaders proposed creating the Indigenous Health System (Doc.1.2016), approved in 2014 by National Goverment. It is articulated with the general social security system in health and grounded on the strategic axes of indigenous peoples: (1) comprehensive laws of life, (2) autonomy, self-determination, and self-government, (3) territory and territoriality, and (4) complementarity for health care and “Buen Vivir” (Good Living) (Doc. 1.2016). However, professionals note that its development remains a debt of the national government (Doc.1.2016; Doc.1.2023).
Since 2016, several intervention designs have adopted a “cultural sensitivity” perspective with clear and structured strategies and interventions (Doc.1.2015; Doc.5.2016; Doc.2.2017; Doc.1.2020). The document “Guidelines for the implementation of community health devices” (Doc.2.2020) highlights differential care devices as an opportunity for promoting mental health and preventing psychoactive substance consumption. Yet, implementation faces obstacles in communities affected by armed conflict (Doc.1.2015; Doc.5.2016; Doc.2.2017; Doc.2.2020).
Thus, despite the recommendations established in Colombia’s health and interculturality regulations, there are situations in which care systems do not accommodate interculturality. This can be illustrated by the suicide registration and alert service official reporting system. While the system exists and represents a potentially useful strategy, it is inadequate for the early reporting and follow-up of cases in indigenous communities, either due to geographically dispersed locations, connectivity, language, or the lack of intercultural dialogue on risk and protective factors in mental health (Doc.5.2016; Doc.1.2020).
Despite regulatory advances, health systems often fail to accommodate interculturality. For example, the suicide registration and alert system provided by the Ministry of Healths. While potentially useful, it is inadequate for indigenous contexts due to geographic dispersion, connectivity, language barriers, and lack of intercultural dialogue (Doc.5.2016; Doc.1.2020). Although there has been a desire and interest in generating this dialogue, in practice, it has not been easy to achieve this objective. As an ICBF report observes: “The design of protocols, routes, plans, and programs are conceived with compliance in mind with institutional requirements. This means that, upon reaching the communities, they must respond to the operational and political needs that dictate institutional work” (Doc.1.2020; Acad.2.2020).
This is reflected in subtle elements, such as scheduling community meetings during office hours, ignoring the fact that these times correspond precisely to the communities’ daily activities. These difficulties are exacerbated by language differences. In the case of the Emberá Chamí ethnic group, they retain their native language, which is a blend of dialects from other indigenous ethnic groups, making it very distinctive. Although it gives it an important intangible value compared to other communities, it makes communication even more complex (Acad.2.2023). Related to this issue, it is striking that the clinical practice guide provided by the Ministry of Health to address the issue of suicide in Colombia states the need for an interpreter only in cases of language difficulties, without considering the cultural subtleties that the native language entails in the socio-emotional management of suicide (Doc. 2.2017).
Nevertheless, some interculturally grounded initiatives exist. One example is a support program with indigenous women, combining cultural practices such as weaving with the co-creation of radio messages in native languages to promote harmony, life, and well-being in the context of displacement (NGO.2.2023).
3.2.4 Contradictions between professional and native perspectives
Significant tensions exist between professional views of suicide and indigenous interpretations. It occurs even with interventions carried out from culturally focused perspectives. This is evidenced in the following comment: “It was found that the families of some Tikuna indigenous people who have committed suicide view this event as an evil or a curse (…); while the participant from [An Organization with an Intercultural Approach] believes that suicide should not be viewed as a negative aspect; it is owing to their worldview, for death is viewed as something positive.” A contrast is also observed between opinions related to the influence of education on potential suicide prevention. While community interviewees interpret it as having a positive influence, the interveners view it as negative because it violates their community’s traditions and customs (Acad.2.2020). This can also be seen in the evaluation of care routes: community members reported serious limitations in an intervention, while organizations claim 85–95% effectiveness (Acad.2.2020).
All of these elements foreground the difficulties institutional practices face in integrating indigenous elements into their interventions. Despite the evident positive intentions and clarity of the programs, there are various obstacles that institutional mechanisms generate in producing culturally sensitive interventions. In this regard, one government institution explains: “The institutional rejection of traditional indigenous child rearing and care practices hinders open dialogue between institutions and communities about these practices and other sensitive issues such as abandonment, violence, suicide, and community conflicts” (Doc.1.2020). Another report indicated: “The professionals forge they are working with the Emberá population and do not use appropiate language to be understood or to achieve the objective of the activity” (Doc.1.2023).
The journey has involved the critique and the transformation of interventions and models based on “imposed needs” in processes such as schooling and professionalization outside the framework of the groups’ worldview, clashes in the understandings of suicide, as well as psychological emphases reported in previous years (Acad.3.2017).
3.2.5 Intervention focal points focused on conflict and displacement
The initial presence of humanitarian response organizations in the Chocó department was due to the continued forced displacement scenarios caused by the violence of the armed conflict and the presence of illegal armed groups (Acad.1.2008); thus far, “there are armed confrontations in the territory, which has resulted in displacement and confinement of communities, and restrictions on daily activities” (Doc.6.2024). Many territories continue to be affected by the armed groups’ actions, causing internal displacement of communities. Most of these displacements reach the urban center of Quibdó, capital of the department of Chocó. This local context is also affected by the presence of armed and criminal groups and a weak institutional response structure in health, education, and protection for the affected population. Therefore, basic humanitarian response actions are continuously activated (Int.2.2024).
For this reason, a significant proportion of institutional literature rightly focuses its intervention on elements inherent to the dynamics of conflict and displacement. While this focus is justified, it can overshadow other factors also relevant to the problem of suicide in communities. This is the case with internal conflicts within social groups, where different forms of tension can be seen between traditional authorities, new leaders, and youth groups (Acad.1.2017), also in the manifestations of gender-based violence and disciplinary strategies (Acad.1.2008; Doc.1.2022; Press.2.2023), as well as different forms of rationalized suffering associated with discrimination and the narrowing of realistic opportunities for improvement and well-being for younger groups (Acad.2.2014; Acad.1.2014; Acad.1.2012).
Sometimes, it is also possible to observe that some indigenous organizations and informants also emphasize armed conflict and displacement as the cause of suicides, omitting elements of their worldview (Org.1.2016). The importance of armed conflict and displacement is even more evident in press articles, which frequently report them as the root cause of the suicide epidemic (Press.1.2021; Press.2.2021; Press.3.2021; Press.2.2022; Press.1.2023; Press.3.2023; Press.4.2023; Press.2.2024; Press.3.2024; Press.4.2024).
3.2.6 Multilevel intervention needs
Documents highlight different strategies for planning interventions. These include the existence of a national mental health observatory, regulatory advances in interculturality, guidelines for incorporating an intercultural approach into human talent training processes for the health care of indigenous peoples, ethnoeducation, regulatory guidelines for the protection of indigenous peoples exposed to manifestations of violence due to armed conflict, recognition of autonomy in their governments, and protection of territories (Doc.1.2020; Doc.2.2022; Acad.2.2020; Doc.1.2021; Doc.3.2024). Models focused on psychosocial intervention, productive projects, and strengthening of Indigenous organizations also have been documented (Acad. 1.2008); nevertheless, a major challenge is the coordination of multilevel interventions that allow the development of actions on the material, social, and psychological levels with optimal utilization of the communities and institutional resources. An Indigenous organization expressed this in the following terms: “The attention we demand must be comprehensive and coordinated among institutions, Indigenous organizations, and their Councils. Health care must be supported by the Ministry of Agriculture, the ICBF, and the DPS; with productive projects that allow for the achievement and guarantee of food sovereignty, the Ministry of Transportation must guarantee the opening of rural roads in some areas” (Org.1.2016).
The importance of coordination was also raised by an Indigenous leader from the Departmental Indigenous Women’s Program, who emphasized the importance of cooperation between organizations coordinating projects and programs with Indigenous organizations. In some cases, they arrive unannounced in the territories and without adequate professionals (Doc.1.2023).
Some institutional documents reveal different efforts in this direction. A report of experiences with the Guainía ethnic group reveals a real interest in integrating traditional and Western medicine. It states: “The departmental hospital has expressed interest in including Indigenous authorities and traditional doctors in the planning of health interventions. Indeed, it has created spaces for intercultural encounters where the needs of traditional doctors and midwives have been heard, and joint planning for the coordination of health actions has begun.” However, despite efforts to coordinate health interventions, the same document states that “the recognition of traditional medicine and its coordination with Western medicine has not been achieved” (Doc.2.2022).
A proposal in this direction can be seen in some attempts to understand suicidal behavior in the Vapués communities, which integrate structural elements (such as racism, colonialism, and modernization) with processes of breaking cultural norms and dialogue between otherness, in-group elements, and elements of one’s worldview (Acad.1.2020).
Regarding youth groups, it is documented the importance of interventions that address their lack of life prospects and future interests and opportunities for dialogue with elders and family figures (Acad.1.2012), along with the development of activities that strengthen community participation and belonging have been documented. As one Emberá youth leader commented: “Young people feel alone” (Doc.1.2023).
3.3 Metacategory 3: suicide, racism, and exclusion
3.3.1 Victimization
By 2015, 94.0% of victimizing incidents were forced displacement, with a higher incidence than the general population (Doc.3.2016). Chocó ranked fifth nationwide in victim percentage in 2015 and rose second in 2023 (Doc.5.2023).
In health, although the Emberá are not the municipality with the highest maternal and prenatal mortality, they ranked first in Mandatory Notifiable Events (19.95% between 2009–2014) (Doc.3.2016). The department also showed the country’s highest risk indicators—low birth care, limited prenatal care, few licensed health centers, and fewer beds—meeting 70% of significantly high-risk indicators, likely linked to isolation (Doc.1.2018).
In education, 40% of Emberá people are illiterate; 51.2% completed only primary school; and 3.2% of those over 25 report no educational attainment (Doc.2.2021). Socioeconomic reports place Indigenous peoples—along with Afro-Colombians—at the bottom of wealth distribution: 57.8% are in the lowest quintile (Doc.2.2015; Doc.1.2018). No other group reports worse conditions. These data reveal sustained inequities that heighten psychosocial risk for youth.
3.3.2 Barriers to registration and visibility
Chocó region is one of the Indigenous regions with the highest pattern of non-random census omissions in 2005 and 2018 (Doc.3.2022). It is likewise one of the regions with major coordination difficulties in health, education, and security assistance (Org.2.2020; Acad. 1.2021), which is frequently interpreted as omissions by the State. As noted: “The State shows no interest and fails to comply with the obligations of victims of displacement due to violence. There are delays in restoring rights and guaranteeing well-being or priority protection, causing difficult situations for Indigenous people” (Acad.3.2017).
These factors are compounded by limited access to isolated or unwilling communities (Doc.2.2015); possible record-keeping failure, as reported by indigenous Tikuna people, who point out that the police do not record reported suicides (Acad.2.2020), and culturally based information omissions, as occur among the Wiwa people, who believe that the disease should not be discussed (Org.1.2020). Diverse locations and contexts also shape understanding. Thus, it can be seen how the Emberá Katío place particular importance on armed conflict as a trigger for the suicide epidemic, while the Emberá Chamí emphasize disharmony (Acad.1.2022).
These barriers hinder reporting and, thus, intervention design. An example can be seen in the Forensic Epidemiological Alert System for 2023 (Doc.1.2025). When examining the available tool and comparing it with the report from Indigenous organizations for the first months of 2023, the following significant differences are found (see Table 6).

Table 6. Comparison of suicides January – April 2023.
Even if all the reports from the Epidemiological Alert System for 2023 are added, the total number of reports would be only 13 cases, which corresponds to only 59% of the total number of cases reported by Indigenous organizations in the first four months of the year (Doc.4.2023 and Doc.1.2023). This pattern was repeated from 2010 to 2014, when Forensic Medicine reported only one suicide in a Dobidá reservation, where 14 suicides and more than 150 attempts occurred until 2015 (Acad.1.2017).
Underreporting is widely documented (Doc.2.2018; Acad.1.2022; Press.1.2024; Acad.1.2024). The Constitutional Court’s T-302/2017 ruling included registration limits in the “Unconstitutional State of Affairs” (Doc1.2017). In Amazonas, only one in three Indigenous suicides was reported between 2008–2016 (Acad.1.2024). This element constitutes a primary and determining factor in invisibility.
3.3.3 Tensions, interactions, and acculturation
The history of Indigenous peoples and Western culture is marked by different forms of material and symbolic violence. This relationship has developed a dynamic process of confrontation between worldviews, as well as different forms of legitimate appropriation by Indigenous groups. In the matter of suicidal behavior, this element can be seen in the Emberá case from different angles. On one hand, in the penetration of the Judeo-Christian religious imaginary regarding dimensions of good and evil (Acad.1.2008), modifying the understanding of spiritual elements with diabolical ones, along with changes in the understanding of free unions between young people (Acad.1.2008; Acad.1.2017; Acad.3.2017).
It is also possible to document the impact of Western discourse on the part of the State and the different organizations with whom there have been interactions and different forms of dialogue, as corresponds to the incorporation of the notion of a “suicide epidemic,” as well as categories of insanity and mental illness (Acad.1.2008).
Another notable element of these complex interactions with foreign agents and groups is the manifestation of fears of miscegenation, perceived by the elders as a form of contamination of their own group in the face of new demographic patterns (Acad.1.2017; Acad.1.2022; Acad.1.2008). This makes it possible to document different tensions, sometimes associated with anxieties about racial contamination or changes in cultural patterns, among members of the Emberá community that directly affect the younger groups. This is manifested in the negative perception of miscegenation among Emberá youth with whites and Afro-descendants (Acad.1.2008), changes in the roles of power and success, shifting from the elders to teachers, professionals, and politicians (Acad.1.2017), the new organizations of the cabildos and their tensions with traditional authorities or “heads of families” (Acad.1.2012). It is significant that some myths, as well as the reports of some affected by Jai Tontina, report that the jai has an Afro-descendant’s physiognomy (Acad.1.2017; Acad.1.2022), besides, it is documented as sinful to have sexual relations with Afro-Colombians and chilapos (mestizos) (Acad.1.2008).
Thus, it is possible to affirm that it is a community in which there are different patterns of assimilation and tensions towards other ethnic groups, as well as greater or lesser interaction with urban spaces and institutions, which affects subjective processes, influences, and expectations of well-being. At times, Emberá organizations explicitly demand State intervention and accountability for unmet constitutional duties (Org.1.2016; Org.2.2020; Org.1.2024; Doc.1.2023).
3.3.4 Subtle prejudice and other forms of racialization
Prejudice and discrimination against indigenous groups in general, particularly the Emberá group, appear to be marked by dynamics of subtle prejudice and forms of symbolic, institutional, and structural rationalization.
Research on prejudice towards Indigenous groups in Colombia is scarce, and none specifically targets the Emberá. Searches on suicide among Emberá youth show low frequencies (Acad.1.2025), suggesting limited interest. General studies report fewer negative stereotypes towards Indigenous peoples than Afro-descendants; some positive traits appear (cultural richness, introversion) (Acad.2.2012). When prejudice surfaces, it is often subtle (Acad.1.2019). As an Indigenous artist states: “So many cases of racial discrimination, invisible or reported privately or publicly, for more than five centuries, and still today we experience subtle signs of racism” (Acad.1.2014).
All of these elements seem to correspond more to an action of disinterest and invisibility. As the aforementioned visual and Indigenous artist states: “In a country that ignores the geography, history, and past of the Indigenous people, it is an easy way out to associate a single feathered Indigenous person with all the Indigenous people in the country and to confuse the specificities and individualities of each population lightly, without respect, without appreciation, and in a biased and irresponsible manner: it does not matter in a country that wants nothing to do with Indigenous peoples” (Acad.1.2014).
However, this profile of invisibility and disinterest seems to change dramatically in contexts where social groups are directly exposed to protests and displacement of Indigenous groups to population centers, situations in which significant elements of racialization, dehumanization, and stigmatization of Indigenous groups emerge, as documented in public and social media reports regarding protests by the Emberá group in urban centers (Press.1.2022). Young groups are aware of this dynamic, experiencing significant tensions between the appropriation of Western culture’s positive objects, such as money, clothing, and the privileges of city life but fear ridicule over Spanish and discrimination (Acad.1.2012).
Regarding the dynamics of structural and institutional racialization, the Colombian Constitutional Court has determined the “widespread, unreasonable, and disproportionate violation of the children’s fundamental rights of an indigenous ethnic group, caused by the structural failures of national and territorial entities” (Doc.1.2017). In one of the documents analyzed, an informant expressed it in this phrase: “It is better to die quickly and not to feel so much misery and loneliness and suffer so many blows and insults” (Acad.1.2012).
3.3.5 Internalized racism, self-deprecating mythical narratives and victim blaming
Exploring self-perceptions, it is possible to find various pieces of evidence of internalized racism. While it can not be claimed that they explain suicidal behavior, they can certainly be considered an important risk factor.
In an interview conducted by one of this text’s authors with an Indigenous woman settled in a town in the Colombian Pacific, she reported: “I say that there are people who think we are cool as Indigenous people, they think our culture is cool, but when I was little I did not know my origins, I felt like I wasn’t part of it (…) I thought of myself more as Black than Indigenous. As I grew up, I saw how beautiful women wore the paruma and the necklaces, but I said: I’m not going to dress like that, I’m not going to let them look at my chest, until one day I realized that I was from the people (…) I started liking all of that, the way of living, the food, the paintings, the clothing, everything until I became part of all this” (Int.1.2024).
An example of self-deprecating elements can be found in the myth reported by some Emberá peoples about the difference in poverty between white men and the Emberá. This myth, reed in the Emberá group’s Jaikerazabi community but also present with variations in the Dobidá group, describes the origin of the Emberá’s poverty as the result of their laziness in performing the tasks assigned by the god Karagabí (Acad.2.2024).
When an informant was asked if the indigenous people had been punished for the actions of some of its members, he replied: “Yes. And so, in terms of the Emberá, in terms of the elders, it’s nature itself that’s taking its toll. It’s an element of restoring order. It’s necessary to return to harmony. So the elders, the elders, are saying: There’s a whole lesson here: either we return to the path our Ancoré showed us, or this is the end of the Indigenous people, of all Indigenous people. Physically and culturally” (Acad.1.2017).
Another element that could include victim-blaming processes is references to divine abandonment for the actions of the people themselves. An example is an Emberá teacher’s statement that “For failure to obey divine norms, God has abandoned us, and that is why humanity is allowing evil to rule” (Acad.2.2017). A jaibaná reported in his view that the suicides occurred “because of a punishment from God. In that community, many people were killed, and it was said that some members of that family belonged to the guerrillas or the paramilitaries; that is why God punished them and sent jai to take their lives” (Acad.1.2008). For his part, an Emberá Chamí teacher stated in an interview that, for disobeying divine norms, “God has abandoned us, and that is why humanity is allowing evil to rule” (Acad.2.2017).
4 Discussion
This collective case study examined suicidal behavior among Emberá youth using primary and secondary sources, with contributions from different social actors. The data analyzed indicate that suicide patterns among the Emberá differ significantly from other Indigenous groups in Colombia and from the general population. These patterns do not suggest a uniform process but rather a distinctive trend of theoretical and practical relevance. Notably, suicide is concentrated among youth, with the number of women equaling or surpassing that of men, and it presents identifiable physical, somatic, and psychological manifestations such as Jai de Tontina, Wawamia, and Pensar mal, which the group organizes according to its worldview. Variations in motives and precipitating elements exist even among families located in different territories. Together, these elements highlight a specificity that requires a situated understanding. One possible explanatory route lies in Devereux’s (1973) notion of “ethnic disorder,” in which a cultural group interprets symptoms, causes, and evolution according to its own frame of reference, rendering behavior “not only predictable, but especially predictable in terms of the cultural frame of reference” (p. 71). Although such disorders can be classified within modern nosological strategies, their structure and function remain cultural. This is crucial given the professional tendency to interpret suicidal behavior within Western frameworks, thereby overlooking the cultural functions it represents for the Emberá.
A second area of discussion concerns the causes and types of suicide found in the data. Comparing native accounts with those of professionals and institutions reveals important similarities, especially regarding victimization. Alongside historical inequalities, the Emberá face armed violence, displacement, and the loss of ancestral territories (de Sepúlveda López Mesa, 2008; Comisión de la Verdad, 2020), as well as extractive economies linked to mining (Urrego-Mendoza et al., 2017; Bello and Rangel, 2002). These factors expose them to precarious health, food security, and safety conditions (Ministerio de Salud y Protección Social, 2016; Ministerio de Salud y Protección Social and Organización Panamericana de la Salud, 2016). Both native and professional perspectives also point to disrupted traditions, compromised subsistence, and emerging threats such as acculturation, miscegenation, internal conflicts, harsh disciplinary practices, gender violence, and the burden of internalized racism, self-blame, and hopelessness, all of which heighten the risk of suicidal behavior (Cisneros Rivera, 2024).
Where the perspectives diverge is in the interpretation of disharmony as a native category. For the Emberá, suicidal behavior is explained through interconnected spiritual, social, economic, and environmental variables that challenge Western categories. From this perspective, disharmony encompasses causes ranging from armed conflict, displacement, and extractive activities (associated with precariousness, loss of territory, violence by irregular groups, and spiritual vulnerability) to interpersonal tensions (such as physical or psychological aggression, infidelity, gossip, rivalries, and curses), as well as losses related to tradition, cultural clashes, and discrimination (pressures from Western leadership models, the influence of religious groups, and the decline of jaibanás). The potential triggers identified operate at different levels of impact and through distinct pathways of action, yet these nuances risk being obscured when subsumed under overly broad categorizations of disharmony by professionals and institutions. An indigenous informant provides an insight into the variety of elements that can coexist in the decision to commit a suicidal act within the community. In her words: “She started with that tontina, that jai that would not leave her alone. Headache, her bones feeling like they were being squeezed… well, like she was sick with malaria, that’s all. But then she started with that thought. She pensaba mal (thought badly) and pensaba mal (thought badly). She told me she missed her children a lot (…) that there was nothing to eat, what were we going to do (…) that life wasn’t worth living like this…”.
By professionals and institutions, analysis of interventions revealed two main sets of results. The first concerns structural and design-related difficulties, including operational, administrative, and monitoring limitations. These issues undermine the effectiveness of actions, even when interventions display theoretical and methodological rigor. While institutional discourses often acknowledge inequity, responses remain largely symbolic, reproducing vulnerability.
The second set relates to intercultural challenges: contradictions between professional and native perspectives, tensions in contextualization, and differences in priorities, particularly in addressing armed and historical violence. It is important to note that these tensions arise even when professionals and institutions demonstrate a genuine interest in cultural sensitivity. This underscores the need to review analytical categories, with particular emphasis on exploring the group’s perspectives, sensibilities, and needs.
A key theme is the fragility of multilevel interventions. As Thomazinho (2024) has also noted, these difficulties appear to be linked to limited coordination among different actors, a situation that ultimately reinforces institutional racism. Another factor shaping this dynamic is the challenge of addressing intersectional issues; challenges that, nonetheless, represent unavoidable commitments in the development of interventions in these contexts.
A good example of the challenges of multi-level intervention can be seen in this comment from an indigenous informant: “The attention we demand must be comprehensive and coordinated among institutions, Indigenous organizations, and their Councils. Health care must be supported by the Ministry of Agriculture, the ICBF [Colombian Institute of Family Welfare], and the DPS [Administrative Department for Social Prosperity]; with productive projects that allow for the achievement and guarantee of food sovereignty”. Although the link between agriculture and mental health may not be obvious to a Western audience, it is coherent within the Indigenous interpretation.
Another notable element that emerges from the analysis of the interventions is the limited presence of young people’s voices in the interventions. A professional from an international institution expressed himself harshly when pointed out: “No care is provided for children and adolescents.” Although this statement may require qualification, evidence of interventions effectively addressing young people’s needs and expectations remains limited.
Emerging categories associated with racism and exclusion can also be grouped into two sets. The first involves mechanisms of institutional racism, including victimization, barriers to registration and visibility, and processes of acculturation. The second reflects the direct psychosocial effects of racialization, such as subtle prejudice, internalized racism, self-deprecating mythical narratives, and victim-blaming. Although further empirical evidence is needed, the findings reveal consistent reports of self-denigration and internalized racism, along with heightened suffering linked to vulnerable conditions. One informant’s account illustrates this point: “It is better to die quickly and not feel so much misery and loneliness and suffer so many blows and insults”.
There are not any major references to contrast these findings and analyses with respect to Institucional Racism and Psychosocial Exclusion in the study population. However, the existence of elements regarding vulnerability and the long history of effects is consistent. Our proposal here is to view violence in its different forms and invisibility as key elements of analysis that can be integrated into different models of suicidal behavior. We share the proposal of Restrepo (2009), for whom the different forms of violence (and, in this case, also invisibility), far from representing “simple anomalies,” correspond to constitutive elements of relations of inequality. In this case, this inequality is the result of a long historical process regarding the Emberá people as a marginalized group.
An analysis based on institutional racism, framed through the metaphor of “the rules of the game” (Romero, 1998), helps to understand how institutions reproduce racialization while appearing to recognize inequity. As North (1990) suggests, institutions establish the rules and obligations of human interaction. Thus, although official discourse specifies routes, recommendations, and mechanisms within legality, actions often fail to mitigate inequities. Racism and exclusion are therefore expressed not in explicit discrimination, but in diffuse and fragmented interventions, precarious implementation, and limited integration of Indigenous voices.
These difficulties interact with other factors such as the presence of illegal armed groups, geographic isolation, and limited human and material resources, which restrict effective responses and reinforce social distance. As Aguilar-Idañez and Buraschi (2016) argue, “physical distance is inversely proportional to social distance” (p. 30), and humanitarian approaches often extend compassion without assuming moral responsibility (Buraschi and Aguilar-Idañez, 2019). This generates a paradox: while Indigenous peoples are sometimes recognized with compassion and symbolic worth (Ojeda and González, 2012), closer interaction often triggers racialization and fear, as they occur in interactions with these groups in large cities where they sometimes go to protest (Cuitiva, 2022). The Emberá thus embody a paradoxical position, simultaneously rendered invisible through isolation and subjected to discrimination through proximity. Despite frequent references to racism and exclusion, these categories are rarely translated into concrete strategies, which limits opportunities for transformation. As Tuesca-Molina et al. (2019) note, biases in Indigenous health research can also perpetuate harm.
These findings highlight the need for interventions that move beyond recognition of intercultural realities to achieve substantive impact. Multidimensional interventions are essential, given the complex conditions of psychosocial exclusion (Rodríguez, 2021). However, multidimensionality itself presents theoretical and technical challenges that cannot be solved merely by involving multiple actors. True multidimensionality requires grounding in justice and must begin with ensuring minimum conditions of security and sustainable livelihoods, balancing macrosocial determinants of vulnerability with microsocial ones. A useful parallel is the Latin American tradition of community psychology, where participation is understood as the construction of shared knowledge with epistemological, political, theoretical, and methodological foundations (Montero, 2006; Montero, 2011a, 2011b).
For Emberá youth, one particularly promising path lies in the development of stronger community education alternatives. By granting youth a central role in their design and implementation, such initiatives could both problematize the structural and racialized violence they face and generate realistic alternatives for self-realization in accordance with their values, while also facilitating access to the material and symbolic benefits of society.
One practical implication of this study is the need to critically examine the use of general social and psychological concepts. Armed conflict illustrates this point: whereas a Western perspective might assume a direct causal link between stressors, Emberá interpretations connect it not only to violence and confinement but also to the symbolic loss of territory, rituals, and subsistence, as well as to forced recruitment, gender-based violence, and heightened generational tensions. For professionals, the challenge is to engage with these diverse meanings of disharmony rather than reduce them to a single explanatory category. This is especially relevant for understanding displacement as a key determinant of suicidal behavior. While its central role should not be overlooked, analyzing displacement in relation to the multiple disharmonies it produces at social, community, and individual levels may foster broader possibilities for intercultural dialogue.
A second implication concerns the incorporation of the identified indicators into the design of multidimensional interventions capable of addressing the intersectional and multi-problem challenges faced by the population.
Regarding public policies, it is essential to strengthen internal auditing and monitoring strategies that support the development of interventions which are not only culturally sensitive but also responsive to the population’s real needs and sustainable over time.
This study has several limitations. The main limitation is the predominance of secondary sources and the inability to recruit informants from the communities who had directly experienced personal or family exposure to suicidal behavior. This limitation also involves the difficulty of achieving a dynamic understanding of the data, a goal constrained by the characteristics of the study design. A second limitation concerns data quality, as some sources were vague and difficult to compare. Another limitation is the lack of data and analysis of suicide attempts, which had to be discarded due to quality issues.
Beyond these limitations, there are also several potential risks of bias. The first relates to the limited availability of previous empirical research on the population, which hinders the establishment of reliable comparison patterns. A second source of bias stems from the impossibility of subjecting the collected material to processes of analysis, validation, and discussion with members of the Emberá community. Finally, studies of this kind inevitably carry risks of overgeneralization and ethnocentric bias on the part of the authors”.
Taken together, these limitations and risks highlight the need for more robust and participatory approaches in future research. First, it is necessary to deepen understanding of the cultural frameworks through which Emberá youth interpret suicidal behavior, in order to strengthen prevention, support, and intervention strategies. Second, studies and interventions must be designed to address the lack of coordination and the shortcomings in responding to intersectional challenges.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
Ethical approval was not required for the studies involving humans because the data used in this research include both primary and secondary sources. Primary data involving human subjects, collected prior to the start of the study, were approved by the Ethics Committee of the Faculty of Psychology at Universidad del Valle, Cali, Colombia (no. CEIFP-47-24) in response to a formal request for approval made by APS. Primary data collected during the course of the study included signed informed consent. Secondary data were obtained from publicly available documentary sources. All procedures were conducted in accordance with local legislation and institutional requirements. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because the human data pre-existed the research, resulting from intervention activities. The remaining data are documentary.
Author contributions
PER: Writing – original draft, Writing – review & editing. APS: Writing – original draft, Writing – review & editing. AS: Conceptualization, Data curation, Investigation, Writing – review & editing. CC: Conceptualization, Data curation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We acknowledge Mery Lemos, from Heartland Alliance international Office in Quibdó (2023–2024), and to all the people, communities, organizations and institutions that have been working for decades for the rights, justice and opportunities of the Emberá community, some of whose voices have been collected in this study. The authors also acknowledge Emiliana Rodríguez Sapene for her text review.
Conflict of interest
APS works for Heartland Alliance International Colombia as senior specialist in Mental Health and Psychosocial Support. The organization did not provide funding for this study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2025.1603754/full#supplementary-material
References
Andersen, M. (2006). Race, gender, and class stereotypes: new perspectives on ideology and inequality. Norteamérica, 1, pp. 69–91. Available online at: https://www.redalyc.org/pdf/1937/193715171005.pdf (Accessed 01/23/2025).
Asociación Orewa . (2024). Asorewa se une al día mundial del suicidio. Comunicado de Prensa No. 14, 10 September. Asorewa. Available online at: https://asorewa.org/asorewa-se-une-al-dia-mundial-de-la-prevencion-del-suicidio/ (Accessed 01/14/2025).
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York: International University Press.
Bello, A. , and Rangel, M. (2002). La equidad y la exclusión de los pueblos indígenas y afrodescendientes en América Latina y el Caribe. Rev. CEPAL, 76, pp. 39–54. Available online at: https://www.cepal.org/es/publicaciones/10800-la-equidad-la-exclusion-pueblos-indigenas-afrodescendientes-america-latina (Accessed 02/05/2025).
Buraschi, D. , and Aguilar-Idañez, M. J. (2019). Racismo y antirracismo: comprender para transformar. Cuenca: Ediciones de la Universidad de Castilla-La Mancha.
Carmichael, S. , and Hamilton, C. V. (1967). Black power: The politics of liberation in America. New York: Random House.
Centro Nacional de Memoria Histórica Ministerio de Cultura—Museo Nacional de Colombia . (2017). Endulzar la palabra, memorias indígenas para pervivir. Bogotá: Centro Nacional de Memoria Histórica Ministerio de Cultura—Museo Nacional de Colombia. Available online at: https://www.museonacional.gov.co/Publicaciones/Expo_en_casa/Documents/ENDULZAR.WEB.pdf (Accessed: 09 January 2025).
Cisneros Rivera, C. (2024). Ageísmo, discriminación y suicidio, Medicina (Bogotá). 46, 754–763. Available at: https://doi.org/10.56050/01205498.2405 (Accessed 09 January 2025).
Comisión de la Verdad (2020). El aporte de los pueblos indígenas en la construcción de país. Available online at: https://web.comisiondelaverdad.co/actualidad/noticias/aporte-pueblos-indigenas-en-la-construccion-de-pais. (Accessed 02/09/2025).
Corte Constitucional (2017). Sentencia T-302-17 sobre el Estado de Cosas Inconstitucionales frente a la protección especial de los derechos al agua, salud y alimentación para las comunidades indígenas Wayuu de la Guajira. Available online at: https://www.corteconstitucional.gov.co/relatoria/2017/t-302-17.htm (Accessed 02/11/2025).
Cortez-Gómez, R. , Muñoz-Martínez, R. , and Ponce-Jiménez, P. (2020). Structural vulnerability of indigenous peoples in the face of COVID-19. Boletín Sobre COVID-19, 1(7–8), 7–10. Available online at: https://www.researchgate.net/publication/343403302_Vulnerabilidad_estructural_de_los_pueblos_indigenas_ante_el_COVID-19 (Accessed 09/08/2025).
Cuitiva, L. M. Las violencias invisibles que sufren los indígenas embera en Bogotá. Rev. Camb., (2022), 22 October. Available online at: https://cambiocolombia.com/articulo/pais/las-violencias-invisibles-que-sufren-los-indigenas-embera-en-bogota (Accessed 02/05/2025).
de Sepúlveda López Mesa, R. I. (2008). “Vivir las ideas, idear la vida”: adversidad, suicidio y flexibilidad en el ethos de los emberá y wounaan de Riosucio, Chocó. Antípoda Rev. Antropol. Arqueol. 1, 245–270. doi: 10.7440/antipoda6.2008.12
Departamento Administrativo Nacional de Estadística – DANE . (2021). Censo Nacional de Población y Vivienda – CNPV – 2018. Dirección de Censos y Demografía (DCD). Available online at: https://www.dane.gov.co/index.php/estadisticas-por-tema/demografia-y-poblacion/censo-nacional-de-poblacion-y-vivenda-2018 (Accessed 02/09/2025).
Devereux, G. (1961). Mohave Ethnopsychiatry and suicide. The psychiatric knowledge and the psychic disturbances of an Indian tribe. Washington: United States Government Printing Office.
Dolezal, S. , Winterowd, C. , and Farra, A. (2021). The relationship of self-compassion and suicide risk factors in American Indian/Alaska native people. Am. Indian Alsk. Native Ment. Health Res. 28, 103–124. doi: 10.5820/aian.2801.2021.103
Estévez-Paz, M. A. , Moreno-Martín, F. , Ayllón Alonso, E. , and Díaz-Guerra Romero, A. (2024). Estudio etnográfico del suicidio indígena en la Amazonía colombiana: riesgo suicida comparado con la población no indígena y análisis del subregistro de los datos oficiales. Rev. Colomb. Psiquiatr. doi: 10.1016/j.rcp.2023.12.005
Fanon, F. (2009). “Piel negra, máscaras blancas” in Akal. Peau noire, masques blancs (Paris: Éditions du Seuil).
Ganança, L. , Oquendo, M. A. , Tyrka, A. R. , Cisneros-Trujillo, S. , Mann, J. J. , and Sublette, M. E. (2015). The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology 63, 296–310. doi: 10.1016/j.psyneuen.2015.10.008
García, L. F. (2013). La reconstrucción del espejo: 1969. ¿El indígena como persona?Revista Prolegómenos. Derechos y Valores 16, 87–97. doi: 10.18359/dere.721
García, M. (2022). “Masacre de La Rubiera: les dieron sancocho a 16 indígenas y los mataron”, El Tiempo 16 de febrero. Available online at: https://www.eltiempo.com/colombia/otras-ciudades/matanza-de-la-rubirea-asi-fue-el-asesinato-de-16-indigenas-en-los-llanos-678380 (Accessed 01/15/2025).
Gómez-López, A. J. , Molina-Gómez, N. , and Suárez-Pérez, C. (2012). Vichada: éxodo y etnocidio indígena: el avance de la ganadería extensiva y de la colonización. Rev. Maguaré, 26, pp. 75–121. Available online at: https://revistas.unal.edu.co/index.php/maguare/article/view/35263/35569
González González, M. , García-Haro, J. M. , García-Pascual, H. , Sánchez Pérez, M. T. , Barrio-Martínez, S. , and Voces Oviedo, J. (2021). Hacia un enfoque contextual-existencial del suicidio: recomendaciones para la prevención. Clín. Contemp. 12, 1–10. doi: 10.5093/cc2021a3
Hall, S. (2017). The fateful triangle. Race, Ethnicity, Nation. Cambridge: Harvard University Press.
Instituto Nacional de Medicina Legal y Ciencias Forenses (2023) Forensis: datos para la vida. Available online at: https://www.medicinalegal.gov.co/cifras-estadisticas/forensis
Inter-American Commission on Human Rights (2015) Medida cautelar No. 51–15. Available at: https://www.oas.org/es/cidh/decisiones/pdf/2015/MC51-15-Es.pdf (Accessed 02/03/2025).
Martelo Ortiz, L. O. (2021). La cátedra de estudios Afrocolombianos, una política educativa racializada, que refleja el racismo institucional por parte del Estado Colombiano. Rev. inter. edu. 1, 161–195. doi: 10.32735/S2735-65232021000492
Martínez Silva, P. A. , Dallos Arenales, M. I. , Prada, A. M. , Rodríguez Van der Hammen, M. C. , and Mendoza Galvis, N. (2020). Un modelo explicativo de la conducta suicida de los pueblos indígenas del departamento del Vaupés, Colombia. Revista Colombiana de Psiquiatría 49, 170–177. doi: 10.1016/j.rcp.2018.07.005
Ministerio de Salud y Protección Social . (2016). Perfil de salud de la población indígena y medición de desigualdades en salud. Colombia 2016 (E-book). Ministerio de Salud y Protección Social. Available online at: https://www.minsalud.gov.co/sites/rid/lists/bibliotecadigital/ride/vs/ed/psp/perfil-salud-pueblos-indigenas-colombia-2016.pdf (Accessed 01/16/2025).
Ministerio de Salud y Protección Social and Organización Panamericana de la Salud . (2016). Revisión bibliográfica sobre prevención y atención integral a la conducta suicida en población indígena colombiana. Available online at: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/ENT/Revision-bibliografica-suicidos-indigenas.pdf (Accessed 02/01/2025).
Ministerio de Salud y Protección Social . (2018). Boletín de salud mental: conducta suicida. Subdirección de Enfermedades No Transmisibles. Available online at: https://www.minsalud.gov.co/sites/rid/lists/bibliotecadigital/ride/vs/pp/ent/boletin-conducta-suicida.pdf (Accessed 01/16/2025).
Mitchell, J. C. (2000). “Case and situation analysis” in Case study method: Key issues, key texts. eds. R. Gomm , M. Hammersley , and P. Foster (London: Sage), 165–186.
Montero, M. (2011a). Hacer para transformar: el método en la psicología comunitaria. Buenos Aires: Paidós.
Montero, M. (2011b). A critical look at critical community psychology. Soc. Personal. Psychol. Compass 5, 950–959. doi: 10.1111/j.1751-9004.2011.00403.x
Mora, M. Desaparición forzada, racismo institucional y pueblos indígenas en el caso Ayotzinapa, México. LASA Forum, (2017), 48, pp. 29–30. Available online at: http://lasa.international.pitt.edu/forum/files/vol48-issue2/Debates-AntiRacistStruggles-3.pdf (Accessed 08/08/2025).
Mosquera Rosero-Labbé, C. , and León Díaz, R. E. (2015). Entre la negación del racismo institucional y la etnización de la diversidad étnico-racial negra en programas de combate a la pobreza. Trab. Soc. 17, 47–59.
National Alliance of Mental Illness (2021). Suicide prevention in indigenous communities. Arlington, VA: NAMI.
National Center for Historical Memory (2012). Bojayá: la guerra sin límites. Bogotá: CNMH. Available at: https://centrodememoriahistorica.gov.co/bojaya-la-guerra-sin-limites/ (Accessed 02/03/2025).
North, D. (1990). Institutions, institutional change and economic performance. Cambridge: Cambridge University Press.
Ojeda, D. E. R. , and González, M. P. G. (2012). Estereotipos de estudiantes universitarios hacia compañeros afrocolombianos e indígenas. Rev. CES Psicol. 5, 101–118.
Orewa, A . (2013). Plan de salvaguarda pueblo embera. Documento unificado planes regionales. Bogotá: Ministerio del Interior. Available online at: https://www.mininterior.gov.co/direccion-de-asuntos-indigenas-rom-y-minorias/planes-de-salvaguarda/ (Accessed May 1, 2025).
Orozco-López, E. (2018). “El Estado tiene memoria”: racismo desde las instituciones de gobierno y exclusión de los pueblos originarios en el contexto del discurso intercultural y de los derechos humanos. Ra Ximhai 14, 33–48. doi: 10.35197/rx.14.02.2018.02.eo
Pollock, N. J. , Naicker, K. , Loro, A. , Mulay, S. , and Colman, I. (2018). Global incidence of suicide among indigenous peoples: a systematic review. BMC Med. 16:145. doi: 10.1186/s12916-018-1115-6
Restrepo, M. L. A. Racismo institucional, violencia y políticas culturales: legados coloniales y políticas de la diferencia en Colombia. Hist. Crit., (2009), pp. 218–245. Available online at: http://www.redalyc.org/articulo.oa?id=81112369012 (Accessed 01/24/2025).
Rodríguez, P. E. (2021). Dimensiones de la exclusión psicosocial. Elementos para la teoría, la investigación y la intervención. Cali: Programa Editorial Universidad del Valle.
Romero, J. J. (1998). La democracia y sus instituciones. Ciudad de México: Instituto Federal Electoral, Capacitación Electoral y Educación Cívica. Available online at: https://portalanterior.ine.mx/documentos/DECEYEC/vgn_ivestigacion/democracia_y_sus_instituciones.htm (Accessed 01/17/2025).
Romero-López, A. , Muñoz, A. , and Burbano, L. (2019). Caracterización del pueblo Emberá Chamí. Bogotá: Procuraduría General de la Nación & Red Colombiana de Organizaciones Comunitarias y Ambientalmente Amigables. Available online at: https://www.procuraduria.gov.co/portal/media/docs/CaracterizacionCHAMI.pdf (Accessed 02/13/2025).
Romero-Peñuela, N. . (2024). Día Mundial para prevenir la tragedia en Chocó. La Silla Vacía. 10 septembre. Available online at: https://www.lasillavacia.com/red-de-expertos/red-etnica/dia-mundial-para-prevenir-el-suicidio-y-la-tragedia-silenciosa-en-choco/ (Accessed 02/05/2025).
Rotta-Almeida, B. , Bonato-Gomes, T. , and Hoilsar-Sallet, B. (2021). Racismo institucional e povos indígenas: das práticas assimiladas às estratégias de enfrentamento. Rev. Direito.UnB 5, 153–182.
Thomazinho, G. (2024). Descoordenação a serviço do racismo institucional: considerações sobre o acesso de indígenas à política de saúde. Saúde Soc. 33:e230408pt. doi: 10.1590/S0104-12902024230408pt (Accessed August 16, 2025).
Tuesca-Molina, R. , Idrovo, Á. J. , Martínez-Silva, P. A. , and Fernández-Niño, J. A. (2019). Health conditions among Wayuu people: medical care data are insufficient and biased. Mil. Med. 184, 171–172. doi: 10.1093/milmed/usz089
UNICEF . (2012). Suicidio adolescente en pueblos indígenas: tres estudios de caso. Available online at: https://iwgia.org/images/publications/0575_suicidios-unicef.pdf (Accessed 04/02/2025).
UNICEF (2017). Comunicación, infancia y adolescencia: guía para periodistas. Buenos Aires: UNICEF Argentina. ISBN 978-92-806-4892-8. Available at: https://www.unicef.org/argentina/media/1536/file/suicidio.pdf (Accessed 02/03/2025).
Urrego-Mendoza, Z. C. , Bastidas-Jacanamijoy, M. A. , Coral-Palchucán, G. A. , and Bastidas-Jacanamijoy, L. O. (2017). Narrativas sobre la conducta suicida en pueblos indígenas colombianos, 1993–2013. Rev. Fac. Nac. Salud Publica 35, 400–409. doi: 10.17533/udea.rfnsp.v35n3a10
Van Orden, K. A. , Witte, T. K. , Cukrowicz, K. C. , Braithwaite, S. R. , Selby, E. A. , and Joiner, T. E.Jr. (2010). The interpersonal theory of suicide. Psychol. Rev. 117, 575–600. doi: 10.1037/a0018697
Vargas, A. E. , Villamizar, J. G. , Puerto, J. L. , Rojas, M. V. , Ramírez, O. M. , and Urrego, Z. M. (2017). Conducta suicida en pueblos indígenas: una revisión del estado del arte. Rev. Fac. Med. 65, 129–135. doi: 10.15446/revfacmed.v65n1.54928
Vásquez, D. (2023). Geospatial analysis of suicide rates in Colombia, and its association with sociodemographic and socioeconomic indexes : Research Square.
Viveros-Vigoya, M. (2015). Social mobility, whiteness, and whitening in Colombia. J. Lat. Am. Caribb. Anthropol. 20, 496–511. doi: 10.1111/jlca.12176
Wade, P. (2021). Racismos latinoamericanos desde una perspectiva global. Nueva Soc., 292:25–44. Available online at: https://library.fes.de/pdf-files/nuso/nuso-292.pdf (Accessed 01/28/2025).
Wolff, S. (2004). “Analysis of documents and records” in A companion to qualitative research. eds. U. Flick , E. von Kardorff , and I. Steinke (London: Sage), 284–289.
World Health Organization . (2014). Preventing suicide: a global imperative. Geneva: WHO. ISBN 978-92-4-156477-9. Available at: https://iris.paho.org/handle/10665.2/54141 (Accessed 02/03/2025).
World Health Organization . (2021). LIVE LIFE: An implementation guide for suicide prevention in countries. Washington, D.C.: World Health Organization. Available online at: https://www.who.int/publications/i/item/9789240026629 (Accessed 01/12/2025).
Yin, R. K. (2009). “How to do better case studies” in The sage handbook of applied social research methods. eds. L. Bickman and D. Rog (London: Sage), 254–282.
Glossary
Aburrimiento (also aburrido or burrido) - Characterized by isolation from the community, loss of interest, and hypersomnia.
Jai - Refers to spirits or supernatural forces that can influence people’s lives in a positive or negative way.
Jaibaná - Tribal doctor. He embodies a figure of spiritual, wise, and moral nature. His power can be used for good or evil.
Jaibaná Jai - Spirits imposed by a jaibaná.
Jai de Tontina - Possession of a male spirit in the body and spirit of a woman. It is usually attributed to spells cast by jaibanás. Characterized by “boredom” and/or anger.
Loquera - Informal expression in Spanish for “madness.” It can present different types: dancer, singer, fighter, talkative, or mute.
Pensar mal - Informal expression in Spanish for “To think badly.” An ideational state of fixed ideas, often associated with painful or traumatic experiences.
Revolcadera - Informal expression in Spanish, characterized by a state of psychomotor agitation.
Wawamia - It can be understood as a spirit that induces suicide. It also corresponds to manifestations similar to seizures.
Keywords: suicide, Emberá youth, institutional racism, psychosocial exclusion, community mental health
Citation: Rodríguez PE, Pantoja-Santander A, Sapene A and Cisneros C (2025) Violence and invisibility: a collective case study on suicide among Emberá Indigenous youth in the Colombian Pacific. Front. Educ. 10:1603754. doi: 10.3389/feduc.2025.1603754
Edited by:
Sipho Dlamini, University of Johannesburg, South AfricaReviewed by:
Najuwa Arendse, University of South Africa, South AfricaHuberta Jackson-Lowman, Florida Agricultural and Mechanical University, United States
Copyright © 2025 Rodríguez, Pantoja-Santander, Sapene and Cisneros. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro E. Rodríguez, cGVkcm8uZS5yb2RyaWd1ZXpAY29ycmVvdW5pdmFsbGUuZWR1LmNv; Ayda Pantoja-Santander, YXlkYS5wYW50b2phQGNvcnJlb3VuaXZhbGxlLmVkdS5jbw==
†ORCID: Pedro E. Rodríguez, https://orcid.org/0000-0001-6862-7326
Ayda Pantoja Santander, https://orcid.org/0009-0001-4882-0329
Alejandra Sapene, https://orcid.org/0000-0001-7843-2987
Cástulo Cisneros, https://orcid.org/0009-0009-6767-6535