 Camila Cardoso Rauen1*
Camila Cardoso Rauen1* Maria de Fátima Minneto2Letícia Pascelli Santos3Karime Haviaras Nogara4Elyse Bacila Matos5Ana Paula Wasilewski da Silva6Eduardo Cassanho de Oliveira2Ana Paula Viezzer Salvador7Gustavo Manoel Schier Dória8
Maria de Fátima Minneto2Letícia Pascelli Santos3Karime Haviaras Nogara4Elyse Bacila Matos5Ana Paula Wasilewski da Silva6Eduardo Cassanho de Oliveira2Ana Paula Viezzer Salvador7Gustavo Manoel Schier Dória8- 1Hospital de Clínicas, Universidade Federal do Paraná, Curitiba, Brazil
- 2Department of Education, Universidade Federal do Paraná, Curitiba, Brazil
- 3Postgraduate Program in Internal Medicine and Health Sciences, Universidade Federal do Paraná, Curitiba, Brazil
- 4Postgraduate Program in Child and Adolescent Health, Universidade Federal do Paraná, Curitiba, Brazil
- 5Postgraduate Program in Education, Universidade Federal do Paraná, Curitiba, Brazil
- 6Universidade Federal do Paraná, Curitiba, Brazil
- 7Department of Psychology, Universidade Federal do Paraná, Curitiba, Brazil
- 8Department of Psychiatry and Forensic Medicine, Universidade Federal do Paraná, Curitiba, Brazil
Introduction: Caregiver Skills Training (CST) is an evidence-based program developed by the World Health Organization (WHO) which aims to equip caregivers with skills to support children with neurodevelopmental disorders and enhance their wellbeing, particularly in low-resource settings. The COVID-19 pandemic affected CST implementation in Brazil, necessitating adaptations for remote delivery.
Methods: This qualitative study evaluated the acceptability, feasibility, and perceived effectiveness of a remote CST pilot implementation in Brazil. Focus groups were conducted with four master trainers (MTs), 11 facilitators, and 26 caregivers. The data were analyzed using Content Analysis and Descending Hierarchical Classification (IraMuTeQ®).
Results: Six thematic categories emerged from MTs, five from facilitators, and six from caregivers. Remote CST was well-received, enhancing caregiver learning, improving perceptions of children’s challenges, and facilitating modifications in family routines.
Discussion: Challenges identified included technological barriers, caregiver overload, lack of bonds between caregivers, and the need for practical training for facilitators. Engagement varied according to profile, affected by psychosocial and economic vulnerabilities. Participants valued the content and resources of the training, suggesting few adjustments. The importance of exchanges between families and the support of professionals was highlighted. A change in understanding the child’s difficulties, learning strategies and empowerment of caregivers was observed.
Conclusion: CST implementation in Brazil highlights the crucial role of caregiver training and the importance of cultural adaptation, demonstrating the program’s potential to expand access to structured interventions for families of children with neurodevelopmental disorders.
1 Introduction
Neurodevelopmental disorders are health conditions which significantly affect the personal, social, and academic functioning of individuals from childhood (American Psychiatric Association, 2014). Among them, Autism Spectrum Disorder (ASD) stands out for its implications on communication and social interaction, in addition to repetitive behavior patterns (Zeidan et al., 2022). The increasing prevalence of these disorders requires effective and accessible interventions, especially in countries with limited resources, since their public health systems have greater difficulty responding to the purpose of diagnosis and intervention (Zeidan et al., 2022; World Health Organization, 2022c). Thus, a need for structured and widely disseminated programs to meet this growing demand is evident, enabling children and their families to have access to the necessary support for more adequate and inclusive development (Salomone et al., 2019).
The World Health Organization (WHO), in partnership with Autism Speaks, developed the Caregiver Skills Training (CST) program to train family members and caregivers of children with neurodevelopmental disorders, especially ASD (Salomone et al., 2019). CST is an evidence-based program designed to be implemented by non-specialists, enabling caregivers to promote child development in everyday activities (World Health Organization, 2022b). Its methodology includes nine group sessions and three home visits focused on communication strategies and adaptive behavior (World Health Organization, 2022b). This model allows knowledge to be disseminated sustainably, reaching a greater number of families, regardless of the availability of specialized professionals. In addition, the CST approach aims to strengthen the role of caregivers as active agents in child development, reducing exclusive dependence on formal clinical services and promoting greater autonomy for families.
Nevertheless, structured and accessible support is essential since an ASD diagnosis can pose emotional and financial challenges for families (Franco, 2016). In this sense, the parental training offered by the CST program not only helps in child development, but also reduces caregivers’ stress and improves their quality of life (Postorino et al., 2017). Furthermore, projects such as CST can reduce the stigma associated with ASD, encouraging greater acceptance and social inclusion (Salomone et al., 2019). Parental training contributes to a more harmonious family environment and the wellbeing of everyone involved by strengthening caregivers’ skills in mediating daily interactions.
The WHO provides guidelines for data collection and analysis through specific guides, such as: “WHO Parent Skills Training Programme for Caregivers of Children with Developmental Disorders - Monitoring and Evaluation Framework”; “CST Draft Adaptation and Implementation Guide”; and “WHO CST Measures for Monitoring and Evaluation.” The process of adapting and validating the program in each country takes place in three stages. The first involves cultural and linguistic adaptation, including translating materials and consultation with local experts and potential target audiences. The second stage, called pre-pilot, consists of the first program test, in which its acceptability and feasibility are assessed. The third stage, the pilot, analyzes the acceptability, feasibility, relevance, and effectiveness of the CST program adapted to the local context and delivered by facilitators.
The CST has been implemented in more than 40 countries, including several low- and middle-income nations, with growing evidence of its acceptability, feasibility, and impact (Dababnah et al., 2025; Montiel-Nava et al., 2022). The program has proven flexible and adaptable to diverse sociocultural contexts and delivery modalities, while maintaining its core principles. In Italy, for instance, Ferrante et al. (2024) compared in-person and virtual versions of CST, showing that both were well-received, although the online format required adjustments related to technological access. Similarly, Wong and Chow (2022) highlighted the need to adapt components such as privacy, home visits, and family engagement pace when pre-testing the program in Hong Kong.
Another relevant aspect concerns delivery by non-specialist facilitators. Zerihun et al. (2024) demonstrated that, in rural Ethiopia, CST was perceived as acceptable and relevant, though continuous supervision was considered essential to maintain quality. Likewise, Salomone et al. (2021) found that CST implementation within the Italian National Health System was feasible and acceptable to families. Together, these findings underscore CST’s potential as a scalable intervention that promotes positive outcomes across contexts and contributes to inclusive public health policies.
The need for accessible and scalable interventions is even more evident in developing countries, where access to specialized diagnostics and treatments is limited (Zeidan et al., 2022). In this context, implementing CST reinforces its potential for replicability and adaptation to different cultural and socioeconomic realities. This global dissemination demonstrates the importance of programs which empower caregivers and promote continuous support for children with neurodevelopmental disorders (Cartwright and Mount, 2022).
Integration of the CST program into the Unified Health System (Sistema Único de Saúde - SUS) in Brazil can expand the reach of interventions for children with neurodevelopmental disorders, promoting a sustainable support network for families (World Health Organization, 2022a). To this end, validating the CST contributes to creating evidence-based intervention guidelines, enabling dissemination of effective practices throughout the country (Ingersoll and Berger, 2015).
The Capacitar Project implemented the CST in Curitiba, Brazil, through a partnership between the City Hall, the Federal University of Paraná (UFPR) and the Ico Project Institute (Rauen, 2020). UFPR conducted research to scientifically validate the acceptability, feasibility and effectiveness of the program. The pre-pilot phase took place on a small scale, in an in-person format, before the pandemic (Rauen, 2020). However, the context of the COVID-19 pandemic required adaptations in the CST delivery to make it accessible in a virtual format. Thus, the remote model was tested in several countries, including Brazil, and proved to be viable, despite limitations imposed by the lack of face-to-face interactions (Salomone et al., 2022). In this context, studies indicate that remote delivery can be an effective solution to ensure that more families have access to essential information, overcoming barriers such as transportation costs and logistical difficulties in participating in in-person sessions (Ferrante et al., 2024).
The impact of the program on autism symptoms in children with ASD (Santos, 2021) was quantitatively assessed in the pilot phase conducted in the pandemic context, as well as on the quality of life, skills, and stigma of participating caregivers (Nogara, 2024). This study deals with the final stage of CST validation research in Brazil, analyzing the participants’ perception of the feasibility, acceptability, and effectiveness of the CST pilot implementation delivered remotely in Brazil. To this end, we seek to describe the perception of facilitators and MTs on the program’s acceptability for the target population, as well as its application feasibility in the local context. In addition, we intend to identify the perception of MTs and facilitators on the quality of CST delivery when taught online, as well as their opinions on virtual supervision and training. Another essential aspect is to understand caregivers’ perceptions of its effectiveness, assessing the program’s impact on the quality of life of caregivers and on child development. Finally, we intend to explore the challenges and benefits reported by caregivers when participating in the program.
2 Materials and methods
This study is part of the final validation stage of the WHO CST Program in Brazil, and consists of a descriptive study with a qualitative approach on the acceptability, feasibility and effectiveness of the program.
2.1 Participants
The study sample consisted of four MTs, 11 facilitators and 26 caregivers of children with neurodevelopmental delays or disorders who participated in the program.
MTs are professionals specialized in neurodevelopmental disorders, certified by the WHO, with training in areas of child development, such as psychology, occupational therapy and speech therapy, and responsible for transferring technical knowledge to the facilitators. The average age of these participants was 40.5 years, three of whom were female and one was male, while the average time of experience in health or education services with interventions aimed at children with developmental delays or disorders was 15 years.
In turn, the facilitators are generalist health and education professionals linked to public services who deliver the training to the caregivers. In this study, 81.8% of the facilitators were female, with an average age of 43.9 years. Most participants had never been trained for a parent training program, while half of those who had been trained had attended courses lasting up to 5 days. The characteristics of the facilitators are described in Table 1.
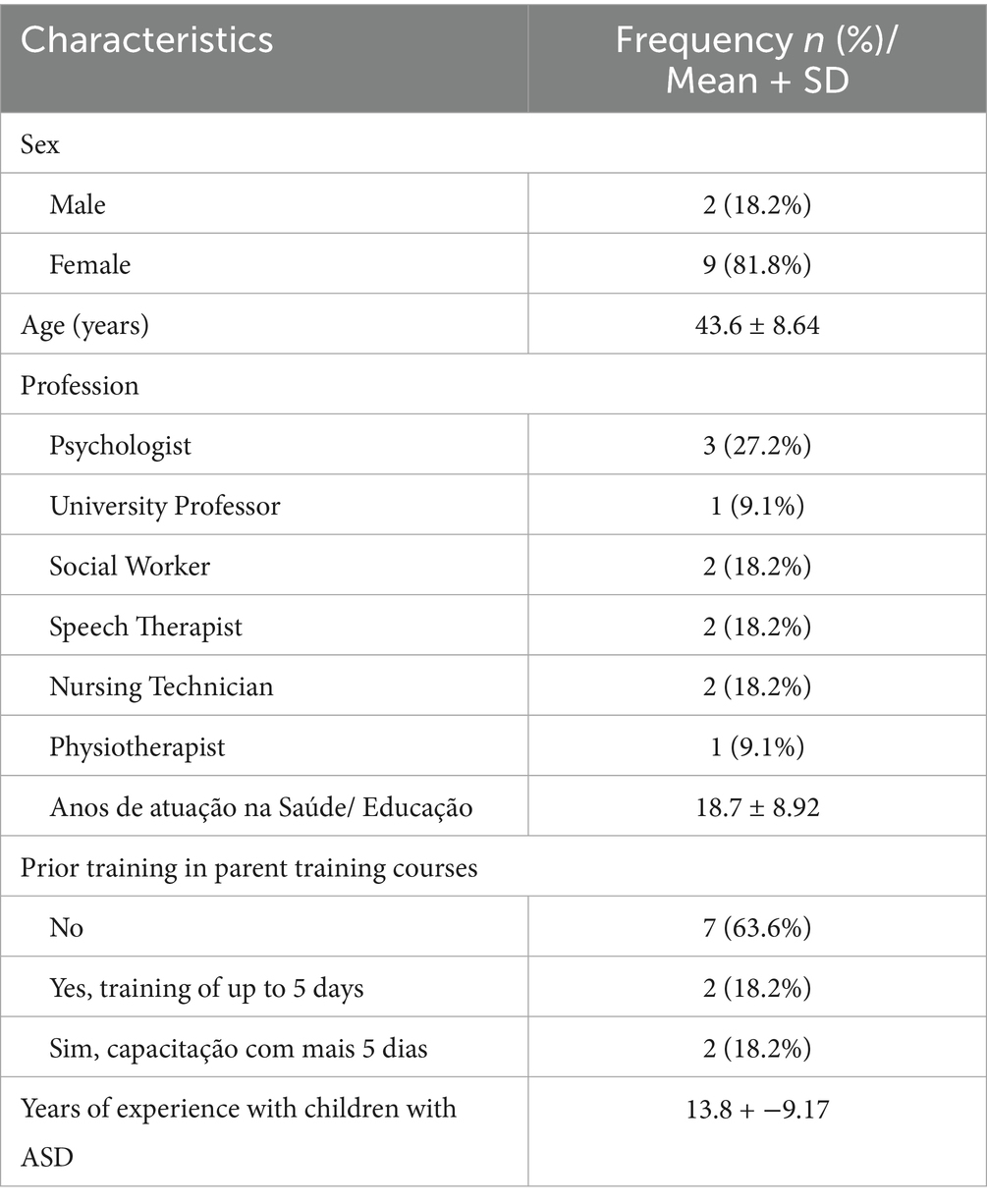
Table 1. Characteristics of the facilitators.
Caregivers are directly responsible for children referred to the Encantar outpatient clinic in Curitiba. The majority of caregivers in this study were female (92.3%), with an average age of 36.2 years, 81% of whom are the child’s mother, and 70% were married or in a stable relationship. Regarding occupation, 81% of caregivers were housewives, self-employed or unemployed, and 19% worked outside the home. The majority of caregivers (54%) had completed high school, and all were urban residents and Brazilians. Regarding ethnicity, 77% considered themselves white, 11.5% mixed race, 7.5% black and 4% Asian. Among the children whose caregivers participated in this study, 81% were male, with an average age of 62 months + −23. All children in the study had an ASD diagnosis by a health professional after applying the Modified Questionnaire for Screening Autism in Children (M-CHAT) and one of them had comorbidity with ADHD. Data on caregivers and children are described in Table 2.
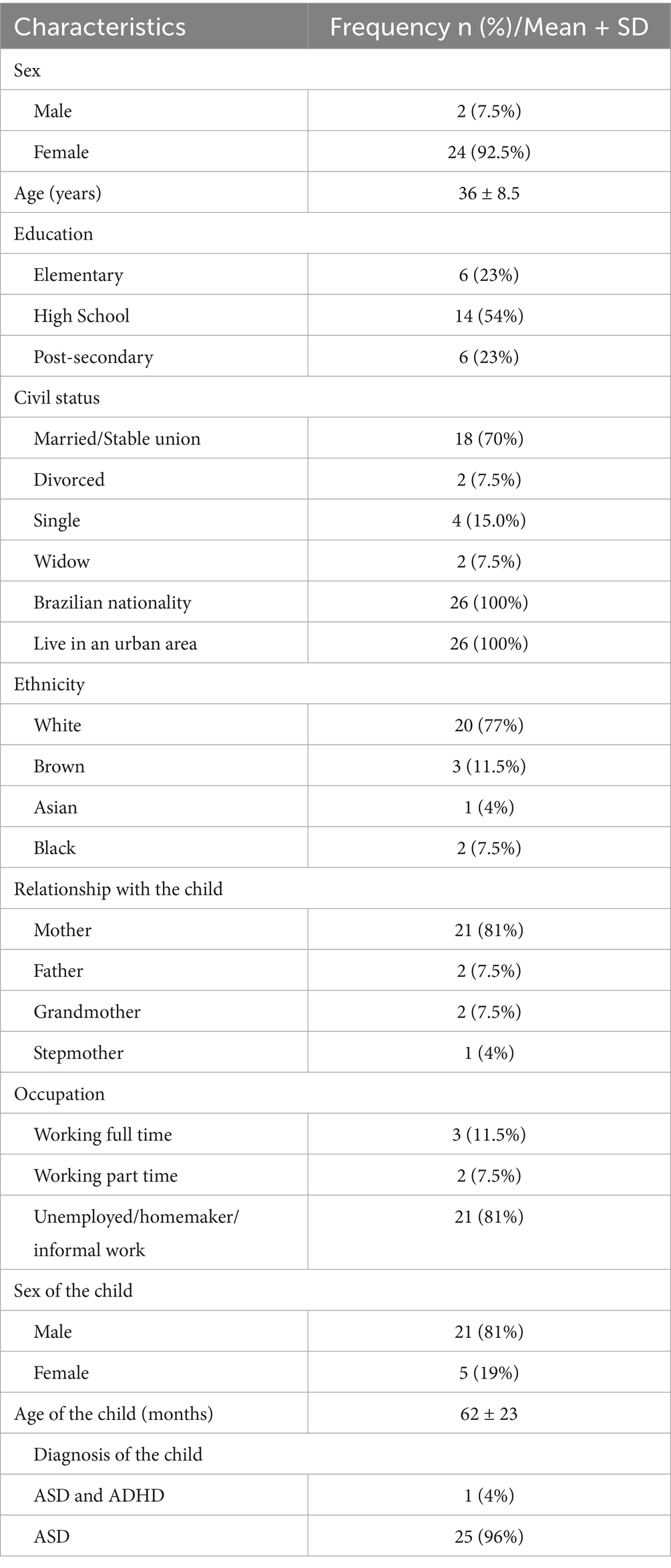
Table 2. Characteristics of caregivers and children.
2.2 Instruments
Sociodemographic forms were used to characterize the participants. The Focus Group (FG) technique was used to collect qualitative data, being considered one of the most efficient instruments for identifying and translating participants’ perceptions on a topic (Nóbrega et al., 2016). The FGs, or conversation circles, were conducted by the researchers, following a structured script based on WHO guidelines, with recording and transcription for later analysis.
The CST materials used in this study were based on the Field Trial Version 2.06-EV (© WHO, 2017, all rights reserved), Caregiver Skills Training for Families of Children with Developmental Delays or Disabilities: Introduction, translated into Portuguese and adapted for use in Brazil.
2.3 Procedures
The CST validation research was conducted in the second half of 2020, with application of five simultaneous groups delivering the CST program remotely via Zoom. Each group was composed of caregivers, a pair or trio of facilitators who delivered the program, and supervised by a MT.
The facilitators initially underwent an intensive five-day training (approximately 40 h) led by the MTs, combining synchronous morning sessions and asynchronous afternoon activities. Training materials, including manuals and instructional videos, were provided through an online learning platform. The curriculum addressed fundamentals of group session delivery, caregiver-mediated intervention strategies, facilitation techniques, and adaptations to the virtual context. Practical components included role-play simulations and a final supervised session in which facilitators rehearsed CST delivery. This preparatory phase was complemented by continuous supervision from MTs throughout the pilot.
Following this preparatory stage, the caregiver training was implemented. It consisted of nine weekly group meetings, in addition to three virtual home visits, to monitor each of the families and define individualized therapeutic objectives. Post-intervention FGs were carried out for the qualitative evaluation, mediated by the researchers with each of the participant groups.
2.4 Data collection
Data were collected through focus groups held at the end of the CST implementation with each type of participant (MTs, facilitators and caregivers), and lasted an average of 90 min. A total of seven FGs were held, one with a group of four MTs, another with a group of 11 facilitators, and the others with caregivers groups. The caregivers were divided according to the training class they were in, with five participants in group A, four in group B, five in group C, four in group D and eight in group E. Aspects related to perceptions about the acceptance, applicability and impact of the program were discussed in each of the meetings. The sessions were recorded, transcribed and qualitatively analyzed.
2.5 Data analysis
Data analysis was conducted by processing the data using the IraMuTeQ® software (Interface for R for Multidimensional Text Analysis and Questionnaires), in which the transcripts of the speeches of each of the FGs were inserted. To do so, three files were organized which originated three analysis corpuses, one for each type of participant (MTs, facilitators and caregivers).
The use of Descending Hierarchical Classification (DHC) enabled identifying semantic patterns in the texts. Based on the identification, Bardin’s Categorical Analysis method (2011) was used to interpret the qualitative data, organizing them into thematic categories to understand the perceptions about the CST program.
The choice of IRaMuTeQ® and DHC was motivated by their ability to combine lexical statistics with qualitative interpretation, thus overcoming the traditional divide between quantitative and qualitative approaches (Kami et al., 2016). DHC segments the corpus into Elementary Context Units (ECUs), which are grouped into classes according to the similarity of their vocabulary and their distinction from other classes (Reinert, 1990). This process enhances analytical transparency and reproducibility, providing a structured basis for subsequent interpretation. It is important to note, however, that IRaMuTeQ® is a tool for processing textual data and does not replace the researcher’s role in interpretation (Kami et al., 2016).
2.6 Ethical considerations
The study was approved by the Human Research Ethics Committee of CHC/UFPR (CAAE: 02994018.7.3001.0101) and by the Health Department of Curitiba (opinion number 3,158,989), in accordance with Resolution No. 466 of December 12, 2012, of the National Health Council. All participants signed the Informed Consent Form (ICF), ensuring data confidentiality and compliance with the ethical guidelines for research with human beings.
3 Results
The results were obtained from analyzing the textual corpus produced by the Focus Groups conducted with the different participant groups. The qualitative data were analyzed through Descending Hierarchical Classification (DHC), resulting in different thematic categories. The analysis of the MTs’ FG resulted in six main categories, while analysis of the facilitators’ FG resulted in five categories and that of the caregivers in six. The thematic categories are organized in Table 3 below, with the respective percentage indicating the proportion of the text corresponding to each category.
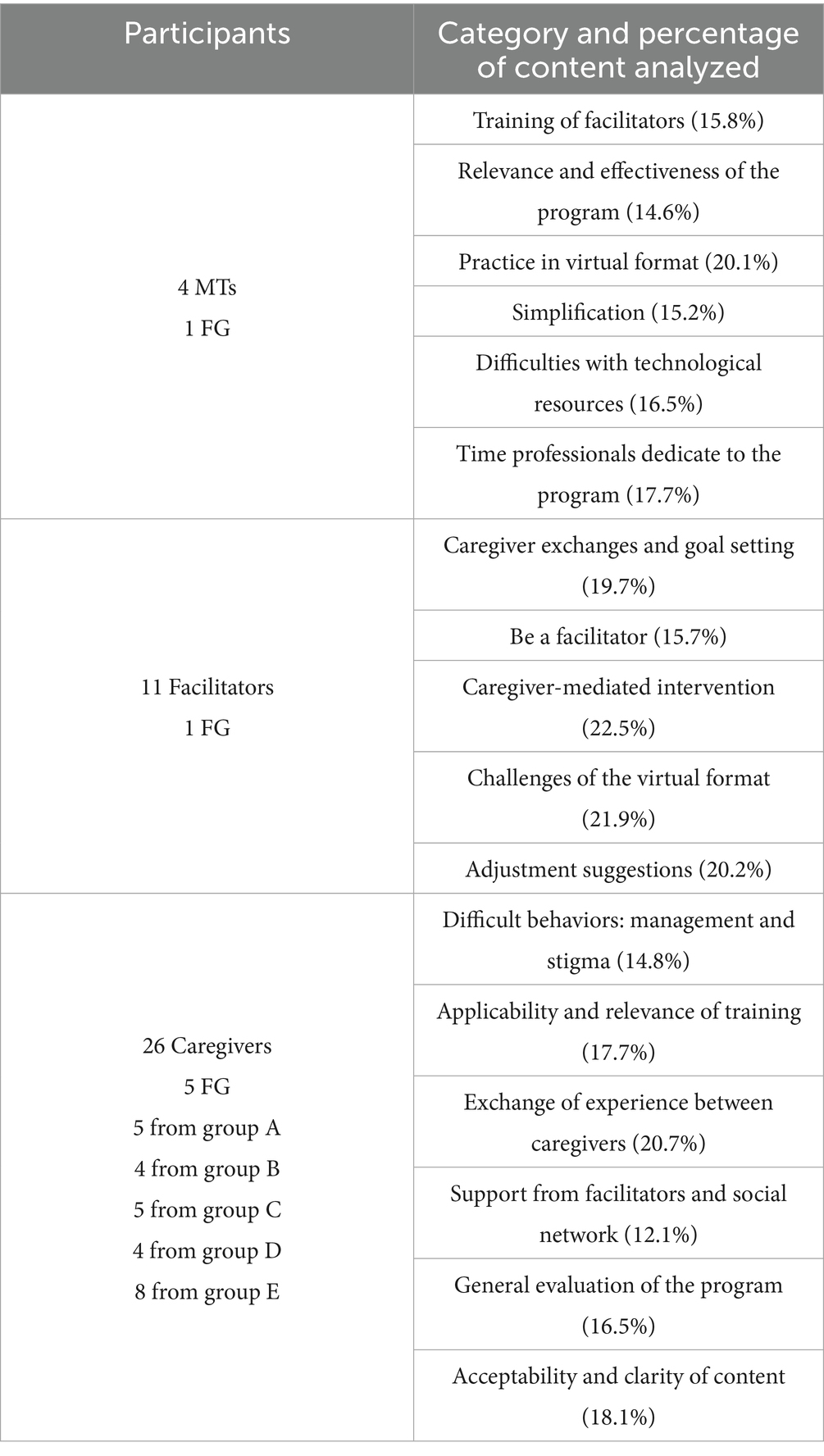
Table 3. Category themes of the focus groups.
3.1 Perception of the master trainers
Analysis of the FGs of the four MTs revealed six main categories: (1) training facilitators (15.8%); (2) relevance and effectiveness of the program (14.6%); (3) practice in the virtual format (20.1%); (4) simplification (15.2%); (5) difficulties with technological resources (16.5%); and (6) time dedicated by professionals to the program (17.7%). Table 4 presents examples of statements attributed to each category.
1. Training facilitators. Participants emphasized the facilitators’ commitment, demonstrating dedication throughout the training. However, they also identified a need to include practice with neurodivergent children in the facilitators’ training.
2. Relevance and effectiveness of the program. It was also mentioned that the graphic materials used, such as slide presentations and handouts used by professionals and caregivers, should undergo review and adjustments to improve clarity and facilitate learning.
3. Practice in the virtual format. Another relevant point raised by the participants dealt with adapting the training to the virtual format. The MTs reported that home visits are essential to model the program’s strategies in a personalized manner, but this dynamic was compromised by the online format. The visits were initially replaced by caregivers sending videos, which was considered a less effective method. There was a transition to synchronous virtual visits via video calls as the sessions progressed, which allowed professionals to have a more accurate perception of the families’ reality, but was still perceived as an inferior substitute for the in-person model.
4. Simplification. Suggestions were also made about the need to simplify some of the program’s materials and procedures to make learning and application easier.
5. Difficulties with technological resources. Other technological challenges were also widely discussed. Among them, it was listed that some families had difficulties in accessing and using the platforms, which impacted adherence to the program. In this sense, it was suggested that prior training be implemented so that caregivers could familiarize themselves with the digital tools before starting the group sessions.
6. Time dedicated by professionals to the program. Finally, participants mentioned the significant time dedicated by professionals to the program.
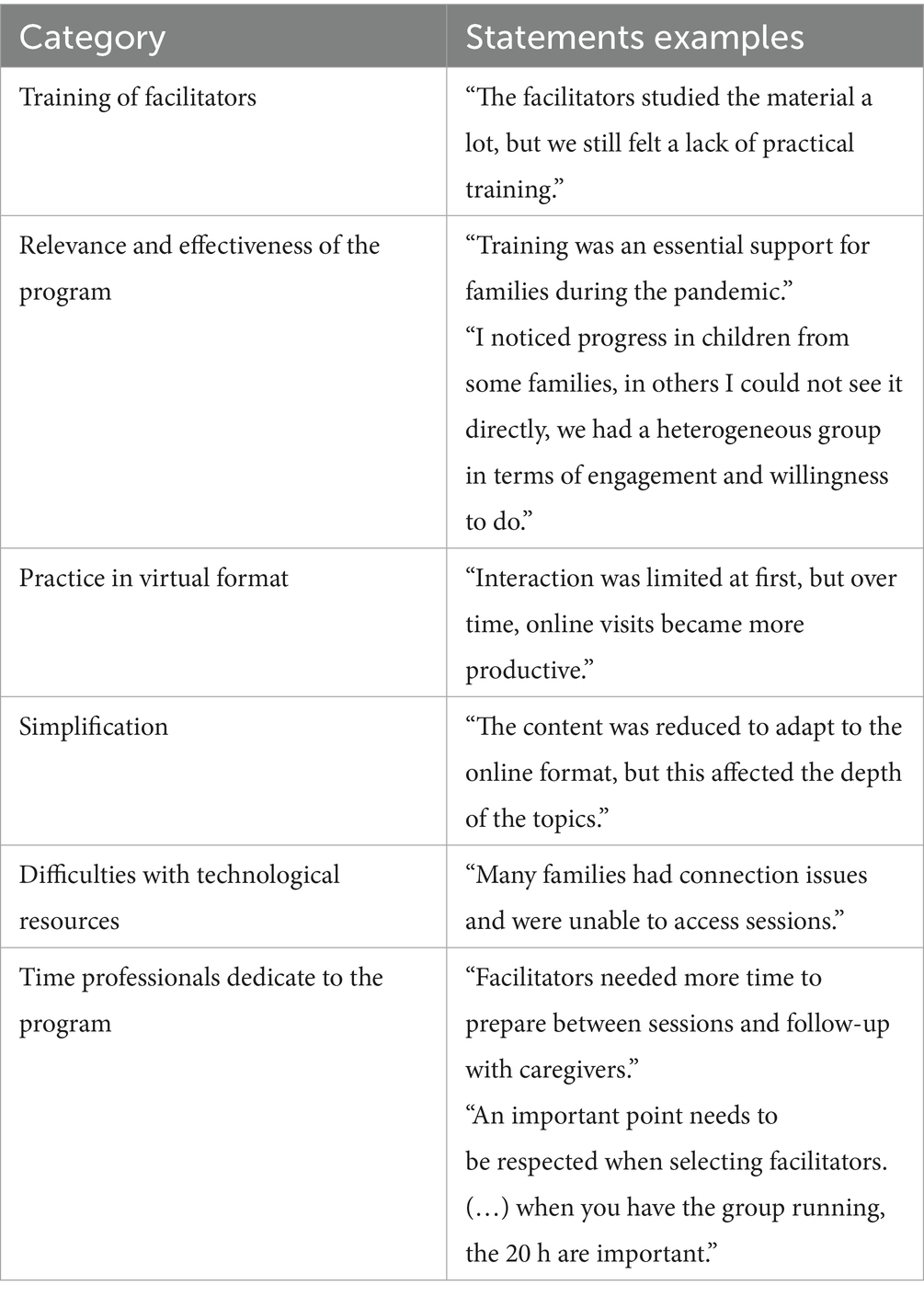
Table 4. Examples of master trainer statements for the categories.
3.2 Perception of the facilitators
The FG with the 11 facilitators resulted in five categories: (1) exchanges between caregivers and goal setting (19.7%); (2) experience of being a facilitator (15.7%); (3) intervention mediated by the caregiver (22.5%); (4) challenges of the virtual format (21.9%); and (5) suggestions for adjustments (20.2%). Table 5 shows examples of statements attributed to each of the categories.
1. Exchanges between caregivers and goal setting. The group sessions were valued in the facilitator statements, as they considered that they enabled promoting experience exchanges among caregivers, making learning more dynamic and shared.
2. Experience of being a facilitator. The facilitators reported initial insecurity about conducting the sessions, especially due to the training compactness and the lack of previous face-to-face practices. In this sense, the ongoing support offered by the MTs who accompanied the professionals was highlighted as an essential element for them to be able to implement the interventions.
3. Intervention mediated by the caregiver. The importance of ensuring that caregivers clearly understood the CST proposal as a caregiver-mediated intervention was emphasized. They noted that prior psychoeducation about the program methodology and objectives would help align expectations, promote engagement, and prevent dropouts during training.
4. Challenges of the virtual format. It was observed that the online format impacted the bond developed between the participants, so that additional effort was required on the part of the facilitators to maintain group engagement.
5. Suggestions for adjustments. The facilitators suggested improvements in the teaching material, indicating that it would be beneficial to review the slide presentation and the content structure of the graphic materials. They also highlighted the need for a more careful screening process to select families prior to participation. This measure ensures that participants’ expectations are more aligned with the CST proposal (a type of intervention mediated by the caregiver), promotes engagement and prevents dropouts during the training.
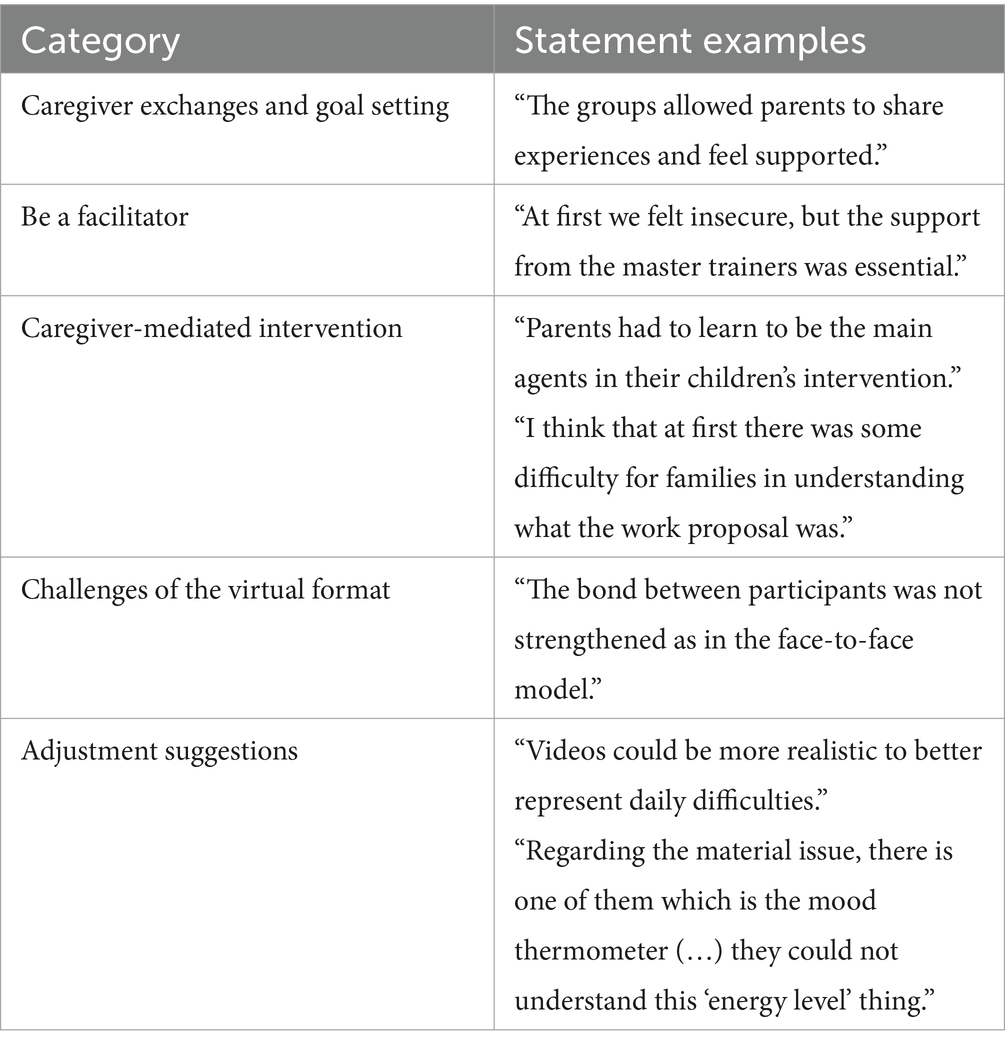
Table 5. Examples of facilitator statements for the categories.
3.3 Perception of the caregivers
The five FGs conducted with caregivers revealed six main categories: (1) difficult behaviors: management and stigma (14.8%); (2) applicability and relevance of training (17.7%); (3) exchange of experiences among caregivers (20.7%); (4) support from facilitators and social network (12.1%); (5) overall evaluation of the program (16.5%); and (6) acceptability and clarity of content (18.1%). Table 6 shows examples of statements attributed to each of the categories.
1. Difficult behaviors: management and stigma. Caregivers reported significant challenges in managing children’s difficult behavior throughout training, especially in times of crisis.
2. Applicability and relevance of training. The training was considered relevant, as it presented concrete changes in the family’s routine organization and in the caregivers’ view of child development.
3. Exchange of experiences among caregivers. Exchanging experiences with other participants was essential for them to feel more prepared and confident in applying the strategies learned during the CST sessions.
4. Support from facilitators and social network. Home visits were pointed out as one of the most important moments of the program, as they enabled closer and more individualized monitoring of the families’ reality. However, caregivers also considered that the online format represented a challenge, especially due to the difficulty in setting aside exclusive time for training amidst other daily responsibilities.
5. Overall evaluation of the program. Caregivers highlighted the value of the training for their personal and family life, recognizing its contribution to greater security in managing daily challenges and strengthening family dynamics.
6. Acceptability and clarity of content. The content was well received, with positive reports about the information clarity and usefulness of the videos and examples presented throughout the training. However, as in the other FGs, some participants in this group suggested adjustments to the audiovisual materials to make them more realistic and representative of the daily difficulties caregivers face with their children.
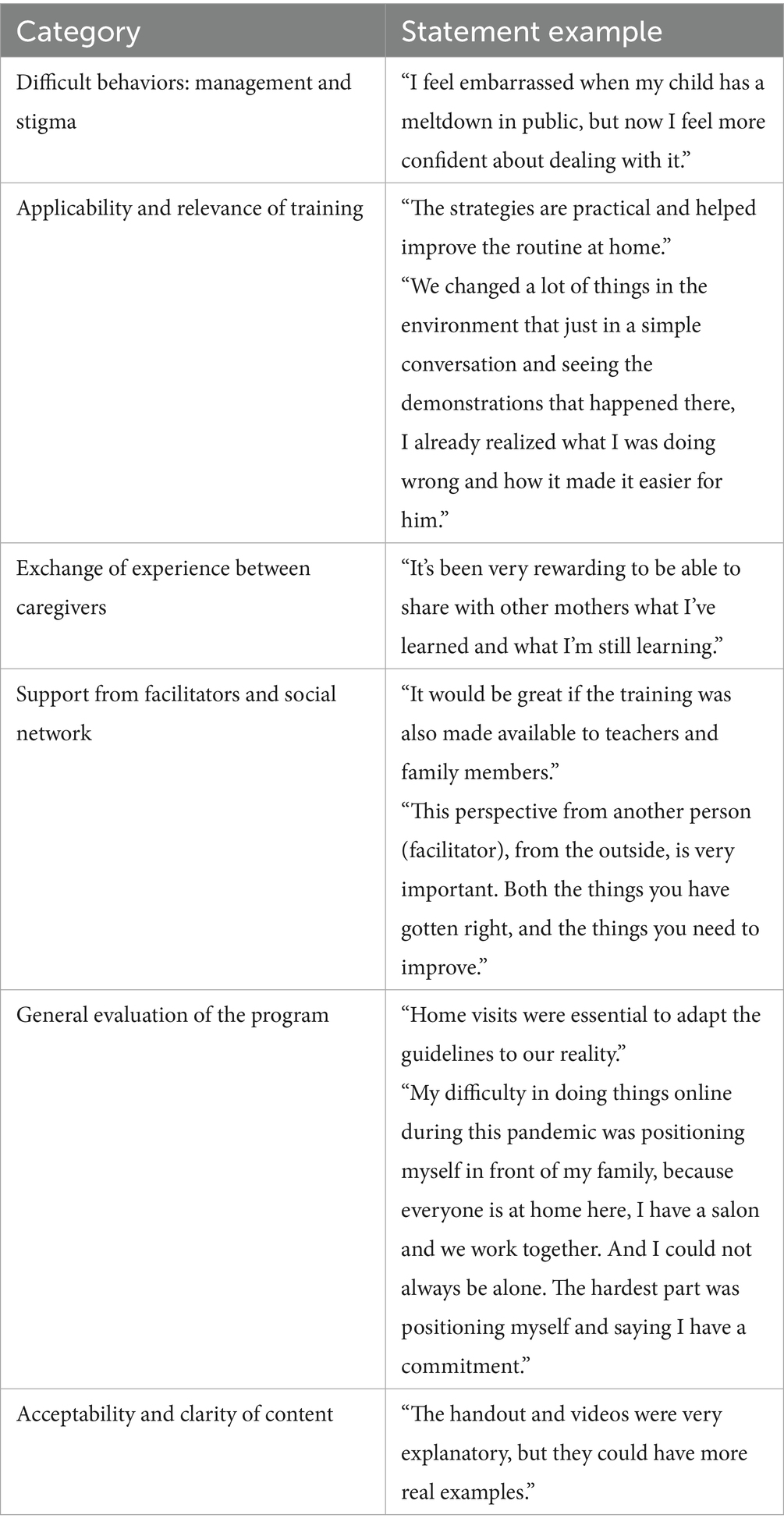
Table 6. Examples of caregiver statements for the categories.
4 Discussion
The analysis of data collected from caregivers and professionals on implementing the virtual pilot CST in Brazil allowed us to assess its acceptability, feasibility and effectiveness, in addition to identifying suggestions for future adaptations. The Brazilian experience was compared with international studies, highlighting challenges and opportunities for improvements in the intervention.
Acceptance of CST depends on cultural aspects, social values, and psychological factors (Ahern et al., 2022). Thus, adherence to the program in Brazil (75.7%) was similar to that of the pre-pilot (70%) (Santos, 2021; Rauen, 2020), but lower than in other countries (Seng et al., 2022; Ferrante et al., 2024; Tekola et al., 2020). Participants in this study considered the content acceptable and understandable, despite some difficulties with modeling through videos. In this sense, studies indicate that more realistic videos can facilitate learning (Salomone et al., 2022).
The therapeutic relationship between facilitators and caregivers was a crucial factor in promoting engagement for adherence. Facilitators with less experience demonstrated insecurity, which affected caregivers’ perception of the program. The initial training was considered insufficient, which corroborates experiences from other countries, such as Taiwan, which sought to expand the facilitators’ training, including more supervised practices (Seng et al., 2022). Furthermore, replacing home visits with sending videos made interaction difficult, and greater proximity through synchronous meetings and in-person visits was recommended (Pearson and Thurston, 2006). In addition, it is considered that a lack of home visits may reduce personalization of interventions and continuous monitoring of families.
Parental expectations also influenced program adherence. Facilitators noted that some caregivers had goals which were not aligned with the CST proposal, highlighting the need for greater prior clarification about the program’s benefits and limitations (Arnkoff et al., 2002). Caregivers’ initial resistance to the parental training model was observed, suggesting that acceptance may be influenced by cultural factors and beliefs about child development.
The program also shows encouraging acceptability and perceived impact: Choinski and Minetto (2024) reported that caregivers recognized improvements across multiple domains following CST participation, including enhanced child skill development, caregiver empowerment, better behavior management, more organized routines, improved family relationships, and the creation of support networks.
Implementing remote CST presented challenges, such as difficulties in using technology and unstable internet. In this context, it is productive to conduct specific training for caregivers and facilitators before the intervention, aiming to reduce technological barriers. On the other hand, it was highlighted that the online modality presented the benefit of saving time for facilitators and allowing greater flexibility in the schedule for conducting the sessions (Salomone et al., 2022).
When discussing program adherence, it is important to note differences between formats: earlier Brazilian pilots in person showed higher engagement, supported by direct contact and home visits (Santos, 2021; Nogara, 2024), while the virtual format in this study faced challenges with domestic overload and unstable internet. These contrasts align with international evidence indicating stronger adherence in face-to-face delivery (Salomone et al., 2021; Ferrante et al., 2024).
The duration of the sessions was considered adequate, but greater emphasis was suggested on discussions between caregivers to facilitate sharing experiences. Furthermore, caregivers reported difficulties in reconciling the program with their routines at home, which was a factor also observed in Ethiopia (Zerihun et al., 2024). In this sense, the overload of families, combined with a high level of demand of the program, can affect adherence over time.
Constant supervision of facilitators by MTs was highlighted as essential (Zerihun et al., 2024) to ensure standardization of the intervention and continuous technical support. The need for ongoing support for caregivers was also identified as a relevant aspect. Thus, hybrid models, which combine initial face-to-face meetings with ongoing virtual support, can improve viability of the program and increase its effectiveness.
Quantitative assessments of CST implementation in Brazil have shown improvements in parental learning and the management of child behavior, with caregivers reporting increased self-efficacy and confidence (Santos, 2021; Nogara, 2024). However, previous findings also indicated limited effects on caregiver wellbeing, suggesting that positive impacts on parenting skills may not directly translate into improvements in family quality of life.
Focus group data from the present study provide complementary insights. Caregivers recognized gains in their knowledge, skills, and family routines, as well as the creation of support networks and empowerment to manage child behavior. Yet, they also reported persistent emotional stress and only modest improvements in overall wellbeing. These qualitative reports are consistent with earlier quantitative results from the Brazilian CST pilot, which showed no significant improvements in quality-of-life measures (WHOQOL-Bref® and PedsQL™) for the overall sample, although caregivers without psychiatric diagnoses presented significant gains (Nogara, 2024). Together, these findings underscore that caregiver vulnerabilities—such as mental health challenges and socioeconomic precarity—substantially limited perceived benefits. In particular, 44% of caregivers reported mental health diagnoses and 64% were out of the formal labor market during the study period, factors that likely magnified stress and reduced the program’s impact on quality of life (Benevides et al., 2019; Cidav et al., 2012). Therefore, inclusion of complementary psychological support services for caregivers could increase the positive effects of the program and improve the impact on family wellbeing.
International studies reinforce this interpretation. Evidence from Italy and Hong Kong highlighted that CST promotes caregiver empowerment and child skill development, but sustaining improvements in wellbeing requires contextual adaptations and additional family support (Salomone et al., 2021; Wong and Chow, 2022). In Ethiopia, ongoing supervision was critical to maintaining intervention quality when delivered by non-specialists (Zerihun et al., 2024). These converging results suggest that CST is effective in enhancing parenting practices across diverse settings, yet broader systemic and psychosocial supports remain essential to strengthen its impact on caregiver wellbeing.
The results of the study, together with the analysis of research conducted globally on CST, enabled formulating suggestions for improvements aimed at both in-person and remote work. The proposals, which can contribute to increasing efficiency, viability and acceptance by the target audience, are presented in Table 7.
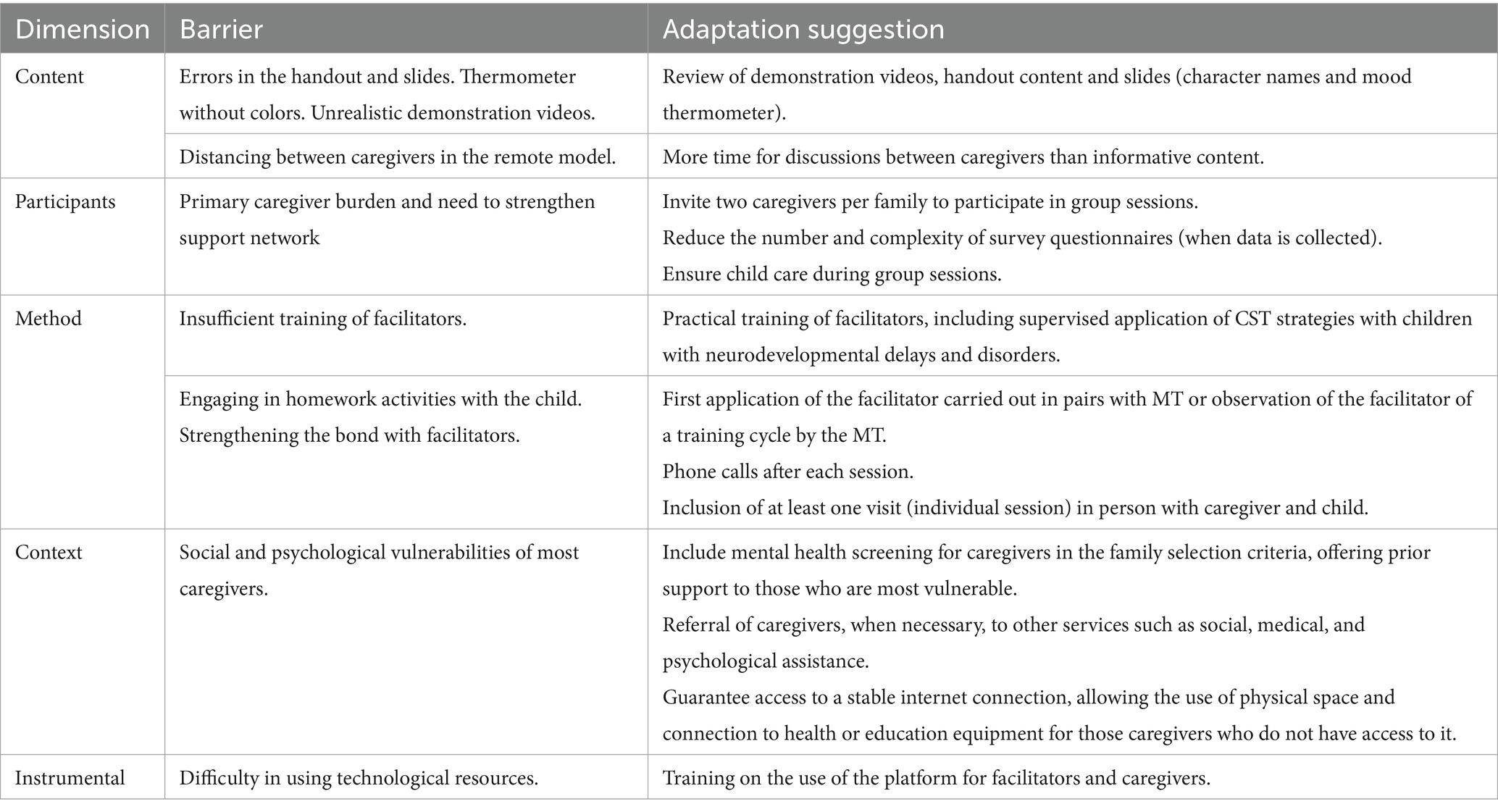
Table 7. Summary of barriers and adaptation suggestions for the Brazilian CST.
These results highlight CST’s feasibility, acceptability, and efficacy within Brazil’s public health infrastructure and underscore its promise as a scalable, culturally adapted intervention. Initiatives like the Capacitar Project could further facilitate CST’s integration into the Unified Health System (SUS), expanding access and reinforcing policies that sustain long-term caregiver training and inclusive community support.
The Brazilian CST pilot highlighted several strengths and challenges that resonate with international findings. Caregivers valued the program’s learning content and teaching strategies, which contributed to clarifying their children’s difficulties and to changes in family routines. Similar to Brookman-Frazee et al. (2018), who reported significant reductions in child problem behaviors following parental training, our results suggest that CST has the potential to positively impact both caregiver competence and child development. However, participants also recommended improvements in teaching materials, echoing observations from Postorino et al. (2017), who emphasized the importance of well-structured resources to optimize parental engagement.
Engagement varied according to caregiver profiles, with socio-emotional vulnerabilities, particularly those exacerbated by the pandemic, influencing participation. This aligns with findings from Salomone et al. (2021) and Zerihun et al. (2024), who also noted that contextual and psychosocial factors affect feasibility and adherence across different settings. Regarding delivery format, the Brazilian experience showed that while virtual implementation increased accessibility and reduced costs, it limited opportunities for role-play, modeling, and peer networking. Ferrante et al. (2024) similarly reported trade-offs between virtual and in-person delivery in Italy, and Wong and Chow (2022) stressed the importance of adapting components such as privacy, home visits, and family engagement pace to ensure effectiveness.
Another key finding concerns facilitator preparation. In Brazil, training was perceived as insufficient, while continuous supervision was viewed as essential to program quality. This is consistent with international literature underscoring the need for strong institutional support and monitoring to maintain fidelity and effectiveness (Salomone et al., 2021; Choinski and Minetto, 2024).
To optimize future CST implementations, actionable recommendations can be organized in five dimensions.
Content. Participants emphasized the need to revise and adapt CST materials, including videos, slides, and handouts, to improve clarity and cultural relevance.
Participants. Suggestions included extending time for discussions among caregivers, inviting two caregivers per family when possible, and simplifying questionnaires to reduce burden and increase engagement.
Method. Recommendations stressed extending facilitator training with more opportunities for supervised practice, ensuring ongoing support, offering childcare during sessions, and incorporating in-person visits when feasible.
Context. Caregivers highlighted the need for stable internet access, prior training for families on digital tools, and adjustments to accommodate challenges of the virtual delivery format.
Instrumental. Finally, participants recommended implementing mental health screening of caregivers to identify risks and provide appropriate referrals to psychological support when necessary.
Taken together, these suggestions illustrate that program fidelity must be balanced with contextual adaptations to strengthen feasibility, inclusiveness, and sustainability in low-resource settings.
4.1 Limitations
This study had some limitations. The main interfering factor was the context of the pandemic, which impacted both the mental health and the economic situation of the participants. This unique context may limit the generalization of the findings to typical circumstances. In addition, the study was only conducted in Curitiba, which restricted the possibility of generalizing the findings to other regions of Brazil. Furthermore, data collection occurred immediately after the intervention, not allowing the long-term effects of CST to be assessed. Therefore, it is recommended that future research analyze the impact of the program in different locations and with longitudinal monitoring.
Although the present study reflects the specific experience of implementing CST in Curitiba, its findings may generate insights applicable to other Brazilian and Latin American cities that share similar socio-economic conditions and systemic barriers in access to specialized care. Regional studies have documented recurring challenges such as stigma, scarcity of services, and structural inequities affecting families of children with neurodevelopmental disorders (Paula et al., 2020). Thus, while the results are contextually anchored in Curitiba, they hold relevance for guiding CST scale-up and adaptation in comparable urban settings across Brazil and Latin America.
Another limitation is that the study employed the Field Trial Version 2.06-EV (©WHO, 2017) of the CST materials. Although this was the most recent version available at the time of implementation (2020), WHO has since released updated materials (2022), and some of the adjustments and feedback reported by participants may partly reflect the use of the earlier package.
5 Conclusion
In summary, the Brazilian pilot demonstrates that CST is not only feasible and acceptable within the public health system but also shows encouraging signs of efficacy in supporting caregivers and children with neurodevelopmental disorders. At the same time, the findings underscore the importance of targeted adaptations—particularly in training materials, facilitator preparation, and delivery formats—to optimize outcomes. Ensuring scalability and sustainability will require continued investment in robust training and ongoing supervision for non-specialist facilitators, alongside integration into intersectoral policies spanning health, education, and social assistance. Furthermore, longitudinal studies and direct comparisons of in-person versus remote delivery will be critical to refining the program’s effectiveness and consolidating CST as a scalable, evidence-based strategy to promote inclusion and family wellbeing in Brazil.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
CR: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. MF: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. LS: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. KN: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. EM: Funding acquisition, Resources, Writing – original draft, Writing – review & editing. ASi: Conceptualization, Formal analysis, Investigation, Writing – review & editing. EO: Conceptualization, Investigation, Writing – review & editing. ASa: Conceptualization, Supervision, Writing – review & editing. GD: Conceptualization, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to express their gratitude to CHC/UFPR and the research group for their valuable contributions to this study. Special thanks to ICO Projeto for coordinating the program nationally in Brazil and to Ambulatório Encantar of the City Hall of Curitiba for the partnership and support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/feduc.2025.1651973/full#supplementary-material
References
Ahern, A. L., Richards, R., Jones, R. A., Whittle, F., Mueller, J., Woolston, J., et al. (2022). Acceptability and feasibility of an acceptance and commitment therapy-based guided self-help intervention for weight loss maintenance in adults who have previously completed a behavioural weight loss programme: the SWiM feasibility study protocol. BMJ Open 12:e058103. doi: 10.1136/bmjopen-2021-058103
American Psychiatric Association (2014). Manual diagnóstico e estatístico de transtornos mentais: DSM-5. 5th Edn. Porto Alegre: Artmed.
Arnkoff, D. B., Glass, C. R., Shapiro, S. J., and Norcross, J. C. (2002). “Expectations and preferences” in Psychotherapy relationships that work: therapist contributions and responsiveness to patients. ed. J. C. Norcross (New York: Oxford University Press), 335–356.
Benevides, T. W., Lee, J., Nwosu, N. A. O., and Franks, J. (2019). Understanding the family impact of autism spectrum disorder in a racially and ethnically diverse sample: findings from the national survey of children with special health care needs. Matern. Child Health J. 23, 951–960. doi: 10.1007/s10995-018-02724-x
Brookman-Frazee, L., Stadnick, N., Chlebowski, C., Baker-Ericzén, M., and Ganger, W. (2018). Characterizing psychiatric comorbidity in children with autism spectrum disorder receiving publicly funded mental health services. Autism. 22:938–952. doi: 10.1177/1362361317712650
Cartwright, J. E., and Mount, K. B. (2022). Adjunctive parental support within manualized parent training for children with autism spectrum disorder. Child Psychiatry Hum. Dev. 53, 1293–1308. doi: 10.1007/s10578-021-01210-w
Choinski, A. M., and Minetto, M. F. (2024). Follow-up of the World Health Organization’s caregivers skills training in Brazil. Int. J. Dev. Educ. Psychol. (Revista INFAD de Psicología) 2, 19–29. doi: 10.17060/ijodaep.2024.n1.v2.2695
Cidav, Z., Marcus, S. C., and Mandell, D. S. (2012). Implications of childhood autism for parental employment and earnings. Pediatrics 129, 617–623. doi: 10.1542/peds.2011-2700
Dababnah, S., Montiel-Nava, C., Rahman, A., Wallander, J., Yao, S., Reichow, B., et al. (2025). The World Health Organization’s Caregiver Skills Training: Advancing global implementation through research. J. Autism Dev. Disord. doi: 10.1007/s10803-025-06516-2
Ferrante, C., Sorgato, P., Fioravanti, M., Pacione, L., Arduino, G. M., Ghersi, S., et al. (2024). Supporting caregivers remotely during a pandemic: comparison of WHO caregiver skills training delivered online versus in person in public health settings in Italy. J. Autism Dev. Disord. 54, 765–784. doi: 10.1007/s10803-022-05800-y
Franco, V. (2016). Tornar-se pai/mãe de uma criança com transtornos graves do desenvolvimento. Educar em Revista 59, 35–48. doi: 10.1590/0104-4060.44689
Ingersoll, B., and Berger, N. (2015). Parent-mediated communication-focused treatment in children with autism (PACT): a randomised controlled trial. J. Child Psychol. Psychiatry 56, 158–166. doi: 10.1111/jcpp.12302
Kami, M. T. M., Larocca, L. M., Chaves, M. M. N., Lowen, I. M. V., Souza, V. M. P., and Goto, D. Y. N. (2016). Working in the street clinic: use of IRAMUTEQ software on the support of qualitative research [Trabalho no consultório na rua: uso do software IRaMuTeQ no apoio à pesquisa qualitativa]. Escola Anna Nery – Revista de Enfermagem 20:e20160069. doi: 10.5935/1414-8145.20160069
Montiel-Nava, C., Tregnago, M., Marshall, J., Sohl, K., Curran, A. B., Mahurin, M., et al. (2022). Implementing the WHO caregivers skills training program with caregivers of autistic children via telehealth in rural communities. Front. Psych. 13:909947. doi: 10.3389/fpsyt.2022.909947
Nóbrega, D. O., Andrade, E. R. G., and Melo, E. S. N. (2016). Pesquisa com grupo focal: Contribuições ao estudo das representações sociais. Psicologia & Sociedade 28, 433–441. doi: 10.1590/1807-03102016v28n3p433
Nogara, K. H. (2024). Impacto do Caregivers Skills Training, em treinamento remoto, na qualidade de vida, nas habilidades e estigma dos cuidadores de crianças com Transtorno do Espectro Autista durante a pandemia Covid-19 (Master’s dissertation). Curitiba: Universidade Federal do Paraná.
Paula, C. S., Cukier, S., Cunha, G. R., Irarrázaval, M., Montiel-Nava, C., Garcia, R., et al. (2020). Challenges, priorities, barriers to care, and stigma in families of people with autism: Similarities and differences among six Latin American countries. Autism, 24, 2228–2242. doi: 10.1177/1362361320940073
Pearson, C., and Thurston, M. (2006). Understanding mothers’ engagement with antenatal parent education services: A critical analysis of a local Sure Start service. Children & Society. 20, 348–359. doi: 10.1111/j.1099-0860.2006.00010.x
Postorino, V., Sharp, W. G., McCracken, C. E., Bearss, K., Burrell, T. L., Evans, A. N., et al. (2017). A systematic review and meta-analysis of parent training for disruptive behavior in children with autism spectrum disorder. Clin. Child Fam. Psychol. Rev. 20, 391–402. doi: 10.1007/s10567-017-0237-2
Rauen, C. C. (2020). Implementação do programa da OMS de treinamento de habilidades para pais e cuidadores de crianças com Transtorno do Espectro Autista ou outros transtornos e atraso do neurodesenvolvimento, no Brasil (Master’s dissertation). Curitiba: Universidade Federal do Paraná.
Reinert, M. (1990). Alceste: Une méthodologie d'analyse des données textuelles et une application: Aurélia de G. de Nerval. Bulletin de Méthodologie Sociologique 28, 24–54. doi: 10.1177/075910639002800103
Salomone, E., Ferrante, C., and McConachie, H. (2021). Acceptability and feasibility of the World Health Organization’s caregiver skills training implemented in the Italian National Health System. Autism 25, 1743–1755. doi: 10.1177/1362361321998892
Salomone, E., Ferrante, C., Salandin, A., Ferrara, F., Torchio, E., Foletti, G., et al. (2022). Acceptability and feasibility of the World Health Organization's caregiver skills training implemented in the Italian National Health System. Autism Int. J. Res. Pract. 26, 859–874. doi: 10.1177/13623613211035228
Salomone, E., Pacione, L., Shire, S., Brown, F. L., Reichow, B., and Servili, C. (2019). Development of the WHO caregiver skills training program for developmental disorders or delays. Front. Psych. 10:769. doi: 10.3389/fpsyt.2019.00769
Santos, L. P. S. (2021). Avaliação de crianças com Transtorno do Espectro Autista após o treinamento de habilidades dos cuidadores (Master’s dissertation). Curitiba: Universidade Federal do Paraná.
Seng, G. J., Chiu, Y. N., Tsai, W. C., Lin, H. Y., Li, S. C., Hsiao, M. N., et al. (2022). Promotion and implementation effectiveness of World Health Organization's caregiver skills training program in Taiwan. Front. Psych. 13:904380. doi: 10.3389/fpsyt.2022.904380
Tekola, B., Girma, F., Kinfe, M., Abdurahman, R., Tesfaye, M., Yenus, Z., et al. (2020). Adapting and pre-testing the World Health Organization’s caregiver skills training programme for autism and other developmental disorders in a very low-resource setting: findings from Ethiopia. Autism 24, 51–63. doi: 10.1177/1362361319848532
Wong, W. P., and Chow, S. L. (2022). Evaluation on the effectiveness of the implementation of WHO caregiver skills training (CST) programme in Hong Kong: a randomised controlled trial protocol. BMJ Open 12:e054099. doi: 10.1136/bmjopen-2021-054099
World Health Organization (2022a). Caregiver skills training for families of children with developmental delays or disabilities: adaptation and implementation guide. Geneva: World Health Organization [License: CC BY-NC-SA 3.0 IGO].
World Health Organization (2022b). Caregiver skills training for families of children with developmental delays or disabilities: introduction. Geneva: World Health Organization [License: CC BY-NC-SA 3.0 IGO].
World Health Organization (2022c). World mental health report: transforming mental health for all. Geneva: World Health Organization.
Zeidan, J., Fombonne, E., Scorah, J., Ibrahim, A., Durkin, M. S., Saxena, S., et al. (2022). Global prevalence of autism: a systematic review update. Autism 15, 778–790. doi: 10.1002/aur.2696
Zerihun, T., Kinfe, M., Koly, K. N., Abdurahman, R., and Girma, F.WHO Team, et al. (2024). Non-specialist delivery of the WHO caregiver skills training programme for children with developmental disabilities: stakeholder perspectives about acceptability and feasibility in rural Ethiopia. Autism 28, 95–106. doi: 10.1177/13623613231162155
Keywords: autism, autistic children, pervasive developmental disorders, caregivers, parent training
Citation: Rauen CC, de Fátima Minneto M, Santos LP, Nogara KH, Matos EB, da Silva APW, de Oliveira EC, Salvador APV and Dória GMS (2025) A qualitative pilot study of the virtual implementation of the WHO caregiver skills training program in Brazil. Front. Educ. 10:1651973. doi: 10.3389/feduc.2025.1651973
Edited by:
Dolores María Peñalver García, University of Murcia, SpainReviewed by:
Guan-Jye Seng, National Taiwan University Hospital, TaiwanCláudia Chambel, University of Évora, Portugal
Copyright © 2025 Rauen, de Fátima Minneto, Santos, Nogara, Matos, da Silva, de Oliveira, Salvador and Dória. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camila Cardoso Rauen, Y2FtaWxhLnJhdWVuQGhjLnVmcHIuYnI=; Y2FtaWxhLmNhcmRvc29yYXVlbkBnbWFpbC5jb20=