 Jordi Pich
Jordi Pich Maria del Mar Bibiloni
Maria del Mar Bibiloni Antoni Pons
Antoni Pons Josep A. Tur
Josep A. Tur- Research Group on Community Nutrition and Oxidative Stress, CIBEROBN (Physiopathology of Obesity and Nutrition CB12/03/30038), University of the Balearic Islands, Palma de Mallorca, Spain
Adolescents’ self-control weight behaviors were assessed (N = 1961; 12–17 years old; 2007–2008) in the Balearic Islands, Spain. The study analyzed the relationships between body weight status, body image, and self-weight concern, and actual attempts to lose weight by restrained eating and/or increased exercising. In terms of regulatory focus theory (RFT), we considered that efforts to lose or to maintain weight (successful or failed) would be motivated either by a “promotion focus” (to show an attractive body), or a “prevention focus” (to avoid social rejection of fatness), or both. Results showed that 41% of overweight boys and 25% of obese boys stated that they had never made any attempt to lose weight, and 13 and 4% in females. Around half of overweight boys and around a quarter of obese boys stated that they were “Not at all” concerned about weight gain, and girls’ percentages decreased to 13 and 11%, respectively. By contrast, 57% of normal weight girls monitored their weight and stated that they had tried to become slim at least once. Weight self-regulation in females attempted to combine diet and exercise, while boys relied almost exclusively on exercise. Apparent lack of consciousness of body weight status among overweight boys, and more important, subsequent absence of behaviors to reduce their weight clearly challenges efforts to prevent obesity. We argue that several causes may be involved in this outcome, including unconscious, emotional (self-defense), and cognitive (dissonance) mechanisms driven by perceived social stigmatization of obesity. The active participation of social values of male and female body image (strong vs. pretty), and the existence of social habituation to overweight are suggested. A better knowledge of psychosocial mechanisms underlying adolescent weight self-control may improve obesity epidemics.
Introduction
Results from US National Health and Nutrition Examination Surveys (NHANES) pointed out that the obesity prevalence remained stable over past 10 years (1). However, several cross-surveys in Western countries showed that around 30% of adolescents boys and 25% of girls are still overweighed (2, 3), mainly due to high-calorie food intake and sedentary lifestyle.
The increased prevalence in adolescent overweight contrasts paradoxically with the prevailing social appreciation of thinness (4–6), which is more pronounced among females (7, 8). The flip side of that appreciation is society’s rejection of obesity, whether expressed openly or through implicit attitudes (9).
Longitudinal surveys and psychiatric studies have long warned that adolescents’ weight self-regulation practices promoted by thinness goals sometimes fuel unhealthy habits such as smoking, alcohol and drug use, purges, or vomits, or even result in anorexia and bulimia disorders (10).
Comprehensible alarm resulting from these potential hazards has tended to obscure the positive role that body weight self-regulation processes, motivated by concern with body image, may represent by promoting a more balanced food intake and regular physical activity during adolescence. In our view, the relationship between ideal body image and weight self-regulation process can be connected through Higgins’ (11, 12) regulatory focus theory (RFT). Essentially, RFT describes the processes by which individuals try to self-regulate or adjust their attitudes and behaviors to achieve a positive goal by means of two differentiated strategies: promotion focus goals (“making good things happen”) or prevention focus goals (“avoiding bad things happen”). Some studies on adults have explored the relationship between individuals’ dominant focus and several dimensions of eating behavior, such as fruit consumption (13), restrained eating (14), emotional, external and restrained eating (15), or food choice motives (16).
In this theoretical framework, we consider that adolescents’ weight self-regulation efforts either by losing excessive weight, or by maintaining it in reasonable magnitudes, would involve a motivational “promotion focus” (i.e., the desire to show an attractive personal body image in alignment with present beauty standards) as well as a “prevention focus” (i.e., to avoid social rejection linked to deviance of body standards).
However, as any human motivated behavior, weight-control may turn into a serious mental illness (17). Anorexia would represent the most dramatic case of healthy weight self-regulation failure. On the other side, adolescents’ hypothetical involvement in a promotion focus, a prevention one, or both can contribute to initiating positive attempts to eat a more balanced diet and/or practice regular physical activity. In this direction, after remarking that during adolescence, body attractiveness tends to be a stronger motive than health when adopting healthy habits; Nowak (18) observed that boys and girls who attempted weight loss reduced consumption of sweet foods and snacks, while concurrently increasing consumption of healthy foods, such as fruit and yogurt. More recently, another study has also recorded that most obese and overweight boys and girls who manifested their desire to slim reported a congruently healthy lower consumption of several high-calorie food groups (19).
Until now, many cross-sectional surveys have assessed the relationship between losing weight behaviors and body image attitudes. These studies have pointed out the common inclination of the obese and overweight population to underestimate their weight (20–23). On the same lines, some longitudinal studies also have pointed out a propensity to judge their body image as not being excessively overweight, which seems to be consistent with a general decline in students’ dissatisfaction with their body-image (24). In particular, Anglo-American countries have registered a significant increase in the percentage of overweight subjects, in both adults (25, 26) and adolescents (27, 28), who defined their weight as “normal.” In previous studies, roughly half of the overweight boys and a quarter of obese ones also claimed to be normal weight, a belief that was not shared and dropped sharply among girls (20, 21).
With reference to measured body fat, half of the girls with above-average values also considered themselves to be normal weight (29), and 4% even defined themselves as underweight. Contrarily, 33% of normal-weight girls overestimated their weight (30).
In agreement with these unexpected findings within a context of obesity rejection, one longitudinal study found a dip in interest among teenagers in controlling their weight (31). Moreover, in a multi-ethnic sample of British adolescents, 65% of overweight boys and 36% of obese boys stated that they have never tried to lose weight, and these proportions fell to 41 and 23%, respectively, among girls (21). By contrast, the ideal of being slim has been shown to spur girls with normal weight to perceive themselves as “fat” (20, 23), and most of them admit to have dieted on some occasions (21).
Incongruences between self-regulatory theoretical predictions and empirical findings demand a better understanding of self-weight goals among adolescents. The aim of this study was to assess the relationship between body mass status, body image perception, self-weight concern, and the personal motivation to actually engage in healthy weight control behaviors through cutting down food intake and/or regular exercise in a representative sample of adolescents living in a Mediterranean area. Body image satisfaction according to weight status, age, and gender was also assessed.
Materials and Methods
Study Design and Population
The study is part of a broader population-based cross-sectional survey carried out on Balearic Islands’ 12- to 17-year-old adolescents between 2007 and 2008. The sample was selected by means of a multiple-step, simple random sampling, taking into account, first, the location, with towns from all over the Balearic Islands being represented (Palma de Mallorca, Calvià, Inca, Manacor, Maó, Eivissa, Llucmajor, Santa Margalida, S’Arenal, Sant Jordi de Ses Salines), and then by random selection of schools within each town. Sample size was stratified by age and gender.
To calculate a representative number of adolescents, a variable BMI was selected with the greatest variance for this age group, based on data from the literature at the time of the study (32). Sampling was determined for the distribution of this variable, with a confidence interval (CI) established at 95% with a ±0.25 error. The total number of subjects (2400) were uniformly distributed within the towns and proportionally distributed by gender and age. Exclusion criteria were: type 2 diabetes, pregnancy, alcohol or drug abuse, and non-directly related nutritional medical conditions.
The sample was oversized to prevent loss of information and was needed to do the fieldwork in complete classrooms. In each school, classrooms were randomly selected from among those of the same grade, or level, and all the adolescents in one classroom were asked to participate in the survey. A letter informing the nature and purpose of the study was sent to parents or legal guardians. After receiving their written consent, the adolescents were then considered for inclusion in the study. All responses to questionnaires were filled in by the adolescents. Once the field study had been completed, the adolescents who did not fulfill the inclusion criteria were excluded. Finally, the sample was adjusted by a weighting factor in order to balance the sample according to the distribution of the Balearic Islands’ population and to guarantee that each of the groups, already defined by the previously mentioned factors (age and gender), were representative. The final number of subjects included in the study, 1961 adolescents (82% participation; 47.9% male), were a representative sample of the Balearic Islands’ adolescent population. Reasons for not taking part were: (a) the subject declined to be interviewed, and (b) the parents did not authorize the interview.
The study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the Balearic Islands’ Ethics Committee (Palma de Mallorca, Spain) under number IB-530/05-PI. Written informed consent was obtained from all subjects and also from the next of kin, careers, or guardians on the behalf of the minors involved in the study.
Body Composition
Height was calculated to the nearest millimeter using a mobile anthropometer (Kawe 44444, Kirchner & Wilhelm GmBH Co., KG, Asperg, Germany), with the subject’s head placed in the Frankfurt plane. Body weight was determined to the nearest 100 g using a digital scale (Tefal, sc9210, Groupe SEB, Rumilly, France). The subjects were weighed barefoot, wearing light underwear, as previously described (33). BMI was computed as weight (kg) divided by height (m2), and study participants were specifically categorized by age and gender using the BMI cut-offs developed and proposed by the International Obesity Task Force (IOTF) (34) and Cole et al. (35, 36): normal weight: 18.5 ≥ BMI < 24.9; overweight: 25.0 ≥ BMI < 29.9; obesity: BMI ≥ 30.
Self-Reported Body Weight
The subjects were asked to estimate their current height and weight prior to measurement. Estimates within ±2 kg of real weight were classified as correct, <2 kg under real weight were considered as an underestimate, and >2 kg than real weight were considered as an overestimate.
Body Image Perception
Subjects had to choose the most similar silhouette to their image (“real silhouette”), and the silhouette they would like to have from other similar series (“ideal silhouette”) using Stunkard’s Figure Rating Scale (Figure 1), which includes nine different body silhouettes (37). The difference between the two values was classified as acceptance of body image (ideal = real), dissatisfaction with being overweight (ideal thinner than real), and dissatisfaction with being underweight (ideal weightier than real).
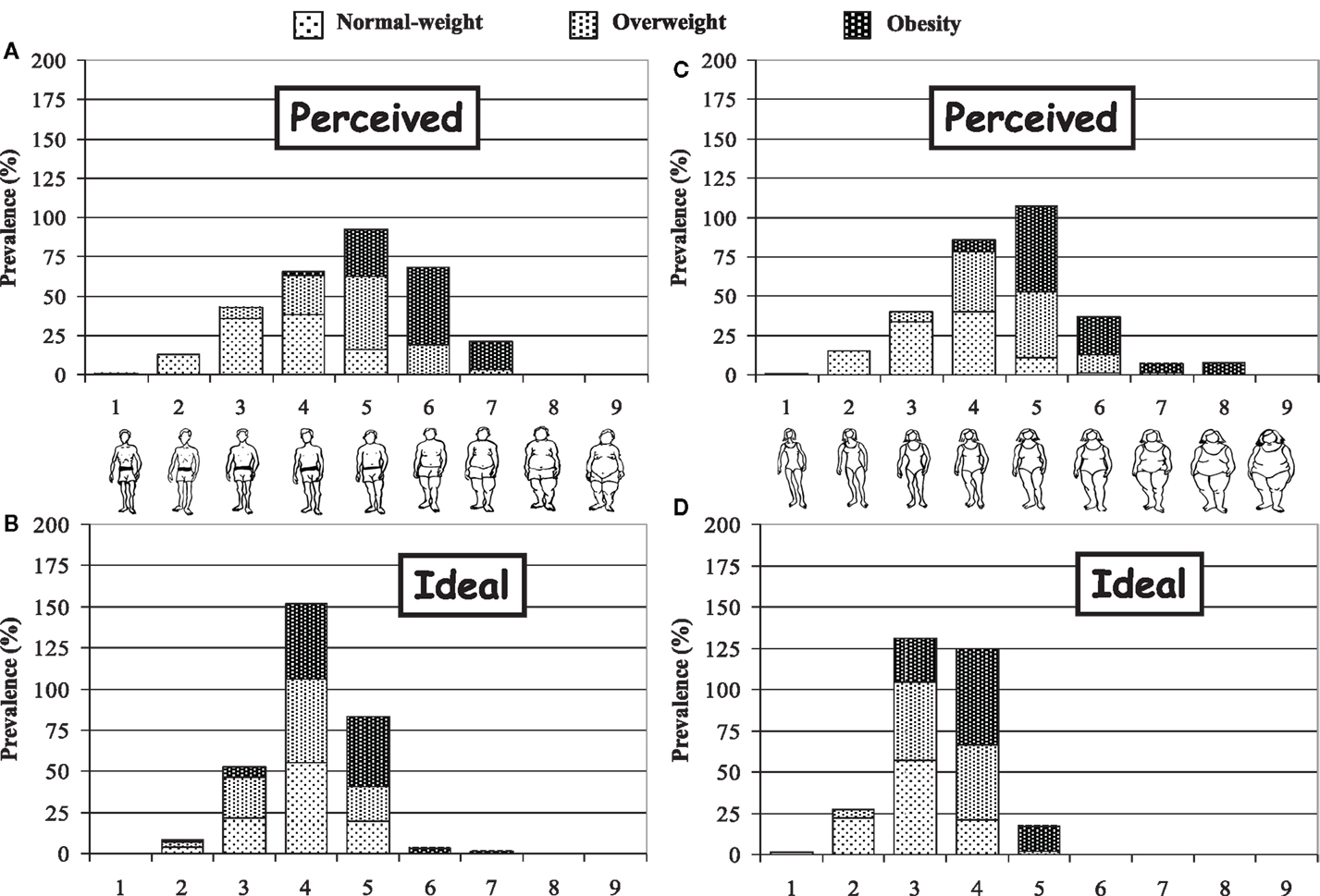
Figure 1. Perceived and ideal silhouettes chosen by boys (A,B) and girls (C,D).
Attitudes toward Self-Body Weight
The subjects were given multiple choice answers to the question, “Would you say that to gain weight is something that worries you? Not at all – Somewhat – A lot,” followed by the question and multiple choice answers, “I consider myself obese: Yes – No.”
Behaviors toward Body Weight Self-Control
The subjects responded to the question, “Have you ever tried to control your weight? (Yes – Never)” followed by the question, “If you answered yes, have you done so by: dieting (Yes – No); regular sport practice (Yes – No).”
Statistics
Analyses were performed with the Statistical Package for the Social Sciences, version 21.0 (SPSS, Inc., Chicago, IL, USA). Significant differences in prevalence were calculated by means of χ2. The level of significance for acceptance was P < 0.05.
Results
As shown in Table 1, a quarter of the sample showed higher weight than recommended. Around 20% of adolescents were overweight and around 6% were obese, and the incidence in both categories did not differ between genders and ages. Underweight adolescents just represented 0.8% of total sample. Therefore, they were analyzed together with normal weight adolescents.
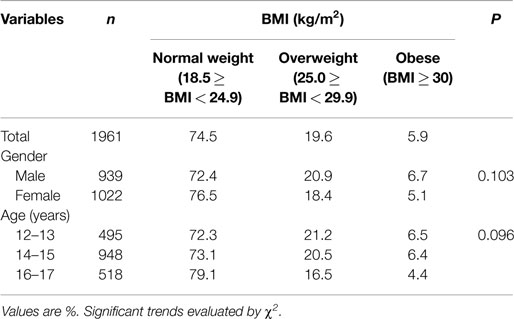
Table 1. BMI distribution in the sample of adolescents according to the different variables in the study.
Figure 1 shows body image self-perceptions. Adolescents tended to attribute silhouettes to themselves with lower signs of body fat than was inferred from the BMI measured. Around 35% of overweight girls ranked themselves as a 4 – normal weight appearance – while almost half of the boys ranked themselves as a 5, a more robust size, but still with no clear signs of being overweight. The same parameters increased by one size among obese adolescents. Moreover, the choice of ideal silhouettes tended to be a larger size in boys, and rose consistently in line with BMI.
Table 2 shows that one-tenth of the subjects did not specify their weight. “Don’t know” answers increased with age and BMI, reaching the 27.8% in the obese group. Weight underestimations increased as BMI increased but decreased with age, and the opposite occurred with overestimation. Girls estimated their weight better than boys, a knowledge that increased with age.
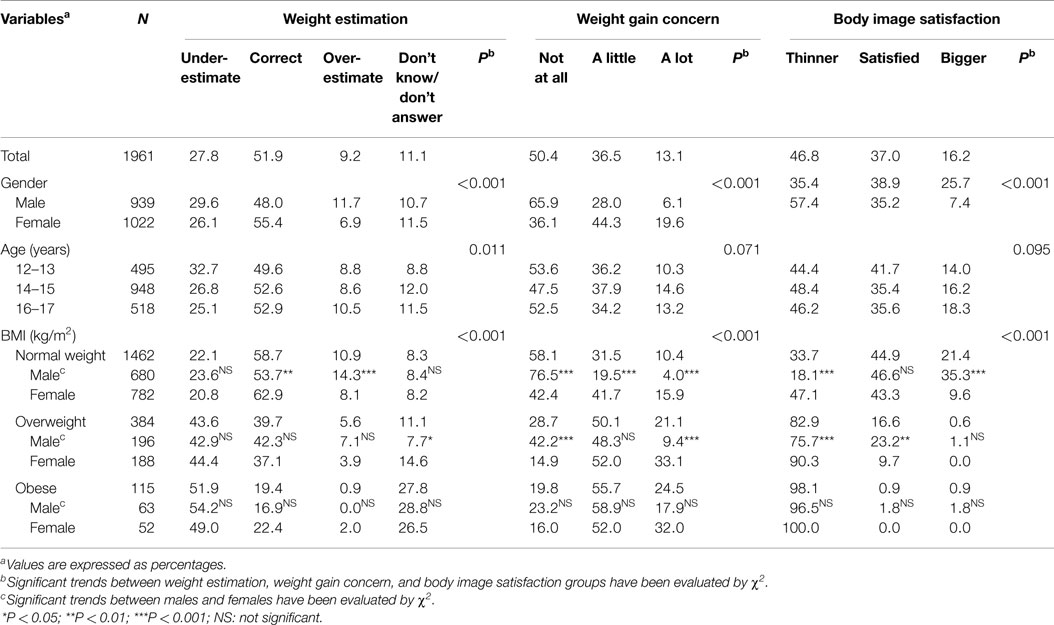
Table 2. Weight estimation, weight gain concern, and body image satisfaction by gender, age, and BMI group.
The difference between the real and ideal silhouette selected by each subject is shown in the body image satisfaction columns, which reveal that nearly half of the teenagers would like to be thinner. However, 25.7% of boys would like to have a larger silhouette.
The percentages of satisfied boys and girls were similar among subjects of normal weight, but girls still wished to be thinner and boys to be larger. Acceptance of being overweight was significantly higher amongst boys.
The Weight gain concern columns in Table 2 clearly reflect girls’ greater concern about gaining weight, which was not affected by age but increased with BMI. Specifically, 47 and 21% of overweight and obese boys, respectively, stated that they were “Not at all” worried about weight concern. These percentages were significantly lower in girls. This unexpected lack of concern about their weight helps to explain the matching lack of any behavior attempt to lose weight in the corresponding column. In effect, 41% of overweight boys and 25% of obese boys stated that they had “Never” attempted to lose weight, and these percentages decreased significantly among females.
Table 3 shows that half of adolescents declared that they had tried to lose weight at least once. This general pattern to lose weight fits for the combination of diet and exercise, but the evolution is quite different when focus is just addressed to exercise, them most of the youngest age group (12-13), and normal weight boys tried more to lose weight with physical activity only.
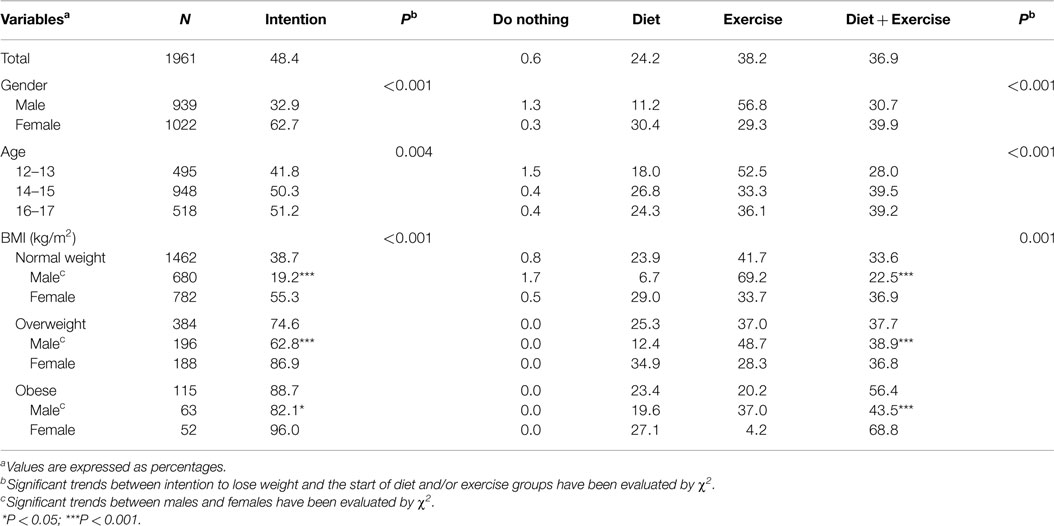
Table 3. Influence of gender, age, and gender within each BMI group on the intention to lose weight and the start of diet and/or exercise.
Discussion
Among the Balearic Islands’ adolescents, the prevalence of overweight is higher and the prevalence of obesity is lower than in the Spanish adolescent population (38). Our study points to important gender differences in weight self-regulation attitudes and behaviors arose in the adolescent period. These findings agree with previous research (39, 40), and are in line with the superior worth given to thinness among girls, a phenomenon usually attributed to different beauty standards in boys and girls (8).
Our data confirm that girls have a more accurate knowledge of their weight than boys (probably by checking it frequently at home); they desire a thinner ideal body image; are much more concerned about weight gain and; as in adults (41), they make more efforts to keep their weight under control. At the studied ages, it was more likely to underestimate than overestimate, similarly to previous findings (42). The obtained results showed that underestimation decreased and overestimation increased with adolescent age. It could be inferred that as much older the adolescent is, as much worried on body weight may be. However, obtained answers on weight gain concern and body image satisfaction did not show it.
According to RFT, the personal motivation to weight self-control may be triggered by the wish to be attractive and/or to avoid to be rejected, being last case more influential, as an individual perceives himself/herself more deviant from social body standard.
However, it is a well-known psychological principle that losing weight is an objective hard to attain, as our adolescents’ figures actually reveal. Clearly, changing comforting habits requires difficult psychological skills, which include an ability to tolerate uncomfortable internal reactions due to hunger or fatigue and a reduction of pleasure, as well as and a behavioral commitment to clearly defined values (43). Therefore, cognitive and emotional expectations about the sacrifices demanded by weight self-regulatory behaviors may dissuade many male and female candidates, while unpleasant experiences from diet and exercise probably lead others to surrender in their first attempts.
This failure may result in frustration and anger (44), a decrease in self-efficacy (45), or even to eat more (46, 47). These psychological outcomes usually arise when people feel unable to control themselves as they wish, or as societal rules dictated (17). In fact, changes in self-regulatory cognitive processes have been demonstrated in the context of adult overeating problems (48, 49).
However, in a social context where the stigma of obesity is a long way of being relaxed (50), the high percentages particularly of overweight males seemingly unconscious of their weight status, unconcerned about weight gain, and consequently unwilling to lose weight, were not. Accordingly, in agreement with similar studies, it can be concluded that most overweight and many obese boys seem to be satisfied with their physical appearance. Therefore, according to the Transtheorical Model (TTM) stages of change (51, 52), this adolescent population should be located in the “pre-contemplation step,” i. e., healthy weight loss practices are not to be expected if subjects do not recognize excess weight, do not consider overweight to be a problem, or that is not a problem serious enough to engage in demanding weight self-regulatory behaviors.
Looking for alternative explanations, one may conjecture that the obese stigmatization actually threatens the self-esteem, particularly of the most weighted individuals, thus setting up subconscious ego self-defense denial mechanisms to protect self-esteem (53–55). High percentage of obese who declared that they did not know their weight would fit this interpretation.
Moreover, social stigma may also pose a cognitive dissonance conflict to overweighed population. Thus, biased body image perception and weight underestimations might be a reflection of a compromise between the social “ought” to body self-image and the perceived body self-image. In other words, self-indulgent weight judgments would be attempts to restore cognitive consonance by claiming “I’m not so fat!” This would explain why half of overweight and obese boys underestimated their weight.
However, our data reveal that most overweight and obese girls do not seem to be affected by the same emotional and cognitive processes. Therefore, beyond the superior worth given to thinness among girls, other psychological parameters are needed to explain the high percentage of boys not concerned about weight gain, or even willing to gain it (65.9 and 25% respectively). Because in male population, masculinity is frequently correlated with a big body, many boys may have considered that to look “manly,” one should better be “well built” than “slim.” This aim at looking “strong” parallels the girls’ concern at looking “pretty.” Thus, in the case of males, being overweight is not always associated to a negative social value, but rather to a positive one if associated to strength. Accordingly, to be a very thin boy may trigger more negative social consequences that to be moderately overweight (luckily, the percentage of underweight boys in our sample was irrelevant). Indeed, a silhouette that represents a slightly overweight boy could be interpreted as a silhouette representing a muscular boy (i.e., a “well-built” boy). This could also explain the discrepancy between the ideal silhouettes chosen by boys and girls.
In conclusion, “the lesser of two evils principle” is somewhat pertinent in this context: when confronted to the choice “being a bit overweight” vs. being a “bit too thin,” perhaps, most boys would choose the first option.
Complementarily, our results could indicate the emergence of a process of social habituation to people exhibiting signs of overweight, a phenomenon comparable to the familiarity with shaved heads, which made it acceptable to be bald. In this direction, Rand and Resnick (56) not only asked teenagers to choose a real and ideal silhouette from a series, but also to check those that were socially acceptable. This study reported that 85% of overweight teenagers and 54% of obese ones considered that their current shape was within the socially acceptable margins of body size, regardless of whether or not they would like to have a slimmer figure. These results are compatible with the social habituation process hypothesis, which deserves further research including estimations of the “regular” or “average” silhouette. Moreover, new researches on body image attitudes demand a better methodology, thus substituting the classical but rather imprecise drawings we employed (e.g., silhouette that represents a slightly overweight boy could be interpreted as a silhouette representing a muscular boy). Instead, the employ of distorted pictures of the subjects (57) asking them to adjust on a computer screen should be encouraged.
Beyond the influence of body image attitudes on weight self-control, it has recently been suggested that personality factors, such as impulsivity and reward/punishment sensitivity, may also play a role in the observed gender motivational and behavioral differences in weight self-monitoring and control (58). The perfectionism personality trait has also previously been related to weight self-regulation, with adult women, who are highly perfectionistic, being more likely to see themselves as overweight and to be more dissatisfied with their bodies (59).
Nowadays, when public efforts to prevent overweight are multiplying (60–62), and many specific school-based interventions have been addressed to cope with the problem (63, 64), a deeper comprehension of factors involved in adolescent weight self-control may contribute to increase their efficiency. Accordingly, our results suggest that to stimulate the use of tailored messages regarding different boys and girls, body image attitudes could be beneficial to obesity epidemics.
Moreover, messages must face the fact that many overweight and obese boys do not actually feel the necessity to lose weight, rather to attribute their physical status to laziness, lack of will-power, or other common negative social stereotypes of overweight people (50).So, in the field of obesity prevention, researches should bear in mind Obelix’s [a character from a well-known French comic book, (65)] famous denial, “I’m not fat. My chest just slipped a bit!,” and adapt their messages suitably.
Another practical finding of our study is the important gender difference we observe in behaviors to achieve a healthy weight. In fact, girls typically used diet and exercise to lose weight, and boys used only exercise. The different competing body image motivations between boys and girls (e.g., to “look like strong” vs. to “look like pretty”) probably boosts the males’ link between sport and muscles and the females’ one between diet and slenderness, thus explaining the girls’ increased confidence in diet and the boys in exercise. Moreover, boys are perhaps more reluctant to go hungry, and girls have a greater fear of having their figures criticized. Therefore, interventions to prevent obesity should suitably accommodate and highlight the benefits of diet among boys, and physical activity among girls.
Afterward, interventions should focus on the advantages of maintaining a reasonable weight by healthy eating and exercise habits by means of presenting well described, attractive strategies to achieve that goal.
Author Contributions
JT, MB, AP, and JP conceived, designed, devised and supervised the study. MB, JP, and JT collected and supervised the samples. MB, AP, and JT analyzed the data and JP, MB, and JT wrote the manuscript. AP and JT obtained funding. All authors read and approved the final manuscript. The study sponsor had no role in study design.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The study was supported by the Spanish Ministry of Health and Consumption Affairs (Program of Promotion of Biomedical Research and Health Sciences, Projects 05/1276, 08/1259, 11/01791, and PI14/00636, Red Predimed-RETIC RD06/0045/1004, and CIBEROBN CB12/03/30038), Grant of support to research groups no. 35/2011 (Balearic Islands Gov. and EU FEDER funds), Spanish Ministry of Education and Science (FPU Program, Ph.D. fellowship to MB). The Research Group on Community Nutrition and Oxidative Stress, University of the Balearic Islands, belong to the Centre Català de la Nutrició (IEC) and Exernet Network.
References
1. Yanovski SZ, Yanovski JA. Obesity prevalence in the United States – up, down or sideways? N Engl J Med (2011) 11:987–91. doi: 10.1056/NEJMp1009229
2. Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999-2004. J Am Med Assoc (2006) 295:1549–55. doi:10.1001/jama.295.13.1549
3. Bibiloni MM, Martínez E, Llull R, Juárez D, Pons A, Tur JA. Prevalence and risk factors for obesity in Balearic Islands adolescents. Br J Nutr (2010) 103:99–106. doi:10.1017/S000711450999136X
4. Grogan S. Body Image: Understanding Body Dissatisfaction in Men, Women and Children. London: Routledge (1999).
5. Gómez-Peresmitre G, Acosta MV. Valoración de la delgadez. Un estudio transcultural (México/España). Psicothema (2002) 14:221–6.
6. Smolak L. Body image in children and adolescents: where do we go from here? Body Image (2004) 1:15–28. doi:10.1016/S1740-1445(03)00008-1
7. Silverstein B, Peterson B, Purdue L. Some correlates of the then standard of physical attractiveness of women. Int J Eat Disord (1986) 5:898–905. doi:10.1002/1098-108X(198607)5:5$<$895:AID-EAT2260050510$>$3.0.CO;2-W
8. Poppe HG, Olivardia R, Borowiecki JJ, Cohane GH. The growing commercial value of the male body: a longitudinal survey of advertising in women’s magazine. Psychother Psychosom (2001) 7:189–92. doi:10.1159/000056252
9. Vartanian LR, Herman CP, Polivy J. Implicit and explicit attitudes toward fatness and thinness: the role of the internalization of societal standards. Body Image (2005) 2:373–81. doi:10.1016/j.bodyim.2005.08.002
10. Neumark-Sztainer RD, Wall M, Guo J, Story M, Haines J, Eisenberg M. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: how do dieters fare 5 years later? J Am Diet Assoc (2006) 106(4):559–68. doi:10.1016/j.jada.2006.01.003
11. Higgins ET. Beyond pleasure and pain. Am Psychol (1997) 52:1280–300. doi:10.1037/0003-066X.52.12.1280
12. Higgins ET. Promotion and prevention: regulatory focus as a motivational principle. In: Zanna MP, editor. Advances in Experimental Social Psychology. San Diego, CA: Academic Press (1998). p. 1–46.
13. Spiegel S, Grant-Pillow H, Higgins ET. How regulatory fit enhances motivational strength during goal pursuit. Eur J Soc Psychol (2004) 34:39–54. doi:10.1002/ejsp.180
14. Vartanian LR, Herman CP, Polivy J. Does regulatory focus play a role in dietary restraint? Eat Behav (2006) 7:333–41. doi:10.1016/j.eatbeh.2005.11.007
15. Pfattheicher S, Sassenrath C. A regulatory focus perspective on eating behavior: how prevention and promotion focus relates to emotional, external, and restrained eating. Front Psychol (2014) 5:1314. doi:10.3389/fpsyg.2014.01314
16. Pula K, Parks CD, Ross CF. Regulatory focus and food choice motives. prevention orientation associated with mood, convenience, and familiarity. Appetite (2014) 78:15–22. doi:10.1016/j.appet.2014.02.015
17. Strauman TJ, Goetz EL. Self-regulation failure and health: pathways to mental and physical illness. In: Leary MR, Tangney JP, editors. Handbook of Self and Identity. New York, NY: The Guildford Press (2012). p. 247–67.
18. Nowak M. The weight-conscious adolescent: body image, food intake, and weight-related behavior. J Adolesc Health (1998) 23(6):389–98. doi:10.1016/S1054-139X(97)00263-2
19. Bibiloni MM, Pich J, Pons A, Tur JA. Body image and eating patterns among adolescents. BMC Public Health (2013) 13:1104. doi:10.1186/1471-2458-13-1104
20. Strauss RS. Self-reported weight status and dieting in a cross-sectional sample of young adolescents. National Health and Nutrition Examination Survey III. Arch Pediatr Adolesc Med (1999) 153:741–7. doi:10.1001/archpedi.153.7.741
21. Viner RM, Haines MM, Taylor SJC, Head J, Booy R, Stansfeld S. Body mass, weight control behaviours, weight perception and emotional well-being in a multiethnic sample of early adolescents. Int J Obes (2006) 30:1514–21. doi:10.1038/sj.ijo.0803352
22. Sherry B, Jefferds ME, Grummer-Strawn LM. Accuracy of adolescent self-report of height and weight in assessing overweight status: a literature review. Arch Pediatr Adolesc Med (2007) 161:1154–61. doi:10.1001/archpedi.161.12.1154
23. Standley R, Sullivan V, Wardle J. Self-perceived weight in adolescents: over-estimation or under-estimation? Body Image (2009) 6:56–9. doi:10.1016/j.bodyim.2008.08.004
24. Cash TF, Morrow JA, Hrabosky JI, Perry AA. How has body image changed? A cross-sectional investigation of college women and men from 1983 to 2001. J Consult Clin Psychol (2004) 72(6):1081–9. doi:10.1037/0022-006X.72.6.1081
25. Johnson-Taylor WL, Fisher RA, Hubbard VS, Staerke-Reed P, Eggers OS. The change in weight perception of weight status among the overweight: comparison of NHANES III (1988-1994) and 1999–2004 NHANES. Int J Behav Nutr Phys Act (2008) 2008(5):9. doi:10.1186/1479-5868-5-9
26. Johnson F, Cooke L, Croker H, Wardle J. Changing perceptions of weight in Great Britain: comparison of two population surveys. Br Med J (2008) 337:a494. doi:10.1136/bmj.a494
27. Brener ND, Eaton DK, Lowry R, McManus T. The association between weight perception and BMI among high school students. Obes Res (2004) 12(11):1866–74. doi:10.1038/oby.2004.232
28. Elgar FJ, Roberts C, Tudor-Smith C, Moore L. Validity of self-reported height and weight and predictors of bias in adolescents. J Adolesc Health (2005) 37(5):371–5. doi:10.1016/j.jadohealth.2004.07.014
29. Scott DJ, Duncan EK, Scholfiels G. Associations between weight perception, weight control and body fatness in a multiethnic sample of adolescents girls. Public Health Nutr (2011) 14:93–100. doi:10.1017/S1368980010000236
30. Deschamps V, Salanave B, Chan-Chee C, Vernay M, Castetbon K. Body-weight perception and related preoccupations in a large national sample of adoelscents. Pediatr Obes (2015) 10:15–22. doi:10.1111/j.2047-6310.2013.00211.x
31. Jones DC. Body image among adolescent boys and girls: a longitudinal study. Dev Psychol (2004) 40:823–35. doi:10.1037/0012-1649.40.5.823
32. Moreno LA, Fleta J, Mur L, Feja C, Sarriá A, Bueno M. Indices of body fat distribution in Spanish children aged 4.0 to 14.9 years. J Pediatr Gastroenterol Nutr (1997) 25:175–81. doi:10.1097/00005176-199708000-00008
33. WHO. Physical status: the use and interpretation of anthropometry. Technical Report Series. Geneva: World Health Organization (1995).
34. International Association for the Study of Obesity (IASO). (2013). Available from: http://www.iaso.org/resources/aboutobesity/child-obesity/newchildcutoffs/ (accessed July 15, 2013)
35. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. Br Med J (2000) 320:1240–3. doi:10.1136/bmj.320.7244.1240
36. Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut-offs to define thinness in children and adolescents: international survey. BMJ (2007) 335:194–202. doi:10.1136/bmj.39238.399444.55
37. Stunkard AJ, Sorensen T, Schulsinger F. Use of the Danish adoption register for the study of obesity and thinness. In: Kety SS, Rowland LP, Sidman RL, Matthysse SW, editors. Genetics of Neurological and Psychiatric Disorders. New York, NY: Raven Press (1983). p. 115–20.
38. Serra-Majem L, Ribas-Barba L, Aranceta-Bartrina J, Pérez-Rodrigo C, Saavedra-Santana P, Peña-Quintana L. Childhood and adolescent obesity in Spain. Results of the enKid Study (1998-2000). Med Clin (Barc) (2003) 121:725–32.
39. Boutelle K, Neumark-Sztainer D, Story M, Resnick M. Weight control behaviors among obese, overweight, and non-overweight adolescents. J Pediatr Psychol (2002) 27(6):531–40. doi:10.1093/jpepsy/27.6.531
40. Halvarsson K, Lunner K, Westerberg J, Anteson F, Sjödén P. A longitudinal study of the development of dieting among 7-17-year-old Swedish girls. Int J Eat Disord (2002) 31:32–42. doi:10.1002/eat.10004
41. Lemon SC, Rosal MC, Zapka J, Borg A, Andersen V. Contributions of weight perceptions to weight loss attempts: differences by body mass index and gender. Body Image (2009) 6:90–6. doi:10.1016/j.bodyim.2008.11.004
42. Park E. Overestimation and underestimation: adolescents’ weight perception in comparison to BMI-based weight status and how it varies across socio-demographic factors. J Sch Health (2011) 81:57–64. doi:10.1111/j.1746-1561.2010.00561.x
43. Forman EM, Butryn ML. A new look at the science of weight control: how acceptance and commitment strategies can address the challenge of self-regulation. Appetite (2015) 84:171–80. doi:10.1016/j.appet.2014.10.004
44. Hofmann W, Vohs KD, Baumeister RF. What people desire, feel conflicted about, and try to resist in everyday life. Psychol Sci (2012) 23(6):582–8. doi:10.1177/0956797612437426
46. Herman CP, Polivy J. Restrined eating. In: Stunkard A, editor. Obesity. Philadelphia, PA: Saunders (1980). p. 208–25.
47. Lowe MR, Doshi SD, Katterman SN, Feig EH. Dieting and restrained eating as prospective predictors of weight gain. Front Psychol (2013) 4:557. doi:10.3398/fpsyg.2013.00577
48. Polivy J, Herman CP, McFarlane T. Effects of anxiety on eating: does palatability moderate distress-induced overeating in dieters? J Abnorm Psychol (1994) 103:505–10. doi:10.1037/0021-843X.103.3.505
49. Scholz U, Nagy G, Gohner W, Lusczynska A, Kliegel M. Changes in self-regulatory cognitions as predictors of changes in smoking and nutrition behavior. Psychol Health (2009) 24:545–61. doi:10.1080/08870440801902519
50. Puhl RM, Heuer CA. The stigma of obesity: a review and update. Obesity (2009) 17:941–64. doi:10.1038/oby.2008.636
51. Prochaska JO, DiClemente CC. Trans-theoretical therapy – toward a more integrative model of change. Psychother Theor Res Pract (1982) 19:276–88. doi:10.1037/h0088437
52. Prochaska JO, DiClemente CC. The transtheoretical approach. 2nd ed. In: Norcross JC, Goldfried MR, editors. Handbook of Psychotherapy Integration. New York, NY: Oxford University Press (2005). p. 147–71.
53. Freud A. The Ego and the Mechanisms of Defense. London: Hogarth Press and Institute of Psycho-Analysis (1937).
54. Baumeister RF, Dale K, Sommer KL. Freudian defense mechanisms and empirical findings in modern social psychology: reaction formation, projection, displacement, undoing, isolation, sublimation, and denial. J Pers (1998) 66(6):1081–124. doi:10.1111/1467-6494.00043
55. Zoccalia R, Brunoa A, Muscatelloa MR, Micòa U, Coricab F, Meduria M. Defense mechanisms in a sample of non-psychiatric obese subjects. Eat Behav (2008) 9:120–3. doi:10.1016/j.eatbeh.2007.06.005
56. Rand CSW, Resnick JL. The “good enough” body size as judged by people varying age and weight. Obes Res (2008) 8:309–16. doi:10.1038/oby.2000.37
57. Docteur A, Urdapilleta I, Defrance C, Raison J. Body perception and satisfactions in obese, severely obese, and normal weight female patients. Obesity (2010) 18(7):1464–5. doi:10.1038/oby.2009.418
58. Dietrich A, Federbusch M, Grellmann C, Villringer A, Hortsmann A. Body weight status, eating behavior, sensitivity to reward/punishment, and gender: relationships and interdependencies. Front Psychol (2014) 5:1073. doi:10.3398/fpsyg.2014.01073
59. Vohs KD, Bardone AM, Joiner TE Jr, Abramson LY, Heatherton TF. Perfectionism, perceived weight status, and self-esteem interact to predict bulimic symptoms: a model of bulimic symptom development. J Abnorm Psychol (1999) 108:695–700. doi:10.1037/0021-843X.108.4.695
60. Brug J, Oenema A, Ferreira I. Theory, evidence and Intervention Mapping to improve behavior nutrition and physical activity interventions. Int J Behav Nutr Phys Act (2005) 2:2. doi:10.1186/1479-5868-2-2
61. US Department of Health and Human Services. The Surgeon General’s call to action to prevent and decrease overweight and obesity. Rockville, MD: US Department of Health and Human Services, Office of the Surgeon General (2001). Available from: http://www.surgeongeneral.gov/topics/obesity/
62. Sassi F. Obesity and the Economics of Prevention. Fit not Fat (2013). Available from: http://www.oecd.org/els/health-systems/obesity-and-the-economics-of-prevention-9789264084865-en.htm (accessed September 13, 2013)
63. Campbell K, Waters E, O’Meara S, Summerbell C. Interventions for preventing obesity in children. A systematic review. Obes Rev (2001) 2(3):149–57. doi:10.1046/j.1467-789x.2001.00035.x
64. Traill WB, Shankar B, Brambilla-Macias J, Bech-Larsen T, Aschemann-Witzel J, Strand M, et al. Interventions to promote healthy eating habits: evaluation and recommendations. Obes Rev (2010) 11(12):895–8. doi:10.1111/j.1467-798X.2010.0017.x
Keywords: adolescents, body image, overweight, obesity, weight self-control, dieting, exercising
Citation: Pich J, Bibiloni MM, Pons A and Tur JA (2015) Weight self-regulation process in adolescence: the relationship between control weight attitudes, behaviors, and body weight status. Front. Nutr. 2:14. doi: 10.3389/fnut.2015.00014
Received: 30 January 2015; Accepted: 21 April 2015;
Published: 08 May 2015
Edited by:
Miguel Alonso-Alonso, Harvard Medical School, USACopyright: © 2015 Pich, Bibiloni, Pons and Tur. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josep A. Tur, Research Group on Community Nutrition and Oxidative Stress, Universitat de les Illes Balears, Guillem Colom Building, Campus, Palma de Mallorca E-07122, Spain,cGVwLnR1ckB1aWIuZXM=