 Chiara Gandossi1*
Chiara Gandossi1* Helen Jessop2Anne Hahn3Lisa Heininger3
Helen Jessop2Anne Hahn3Lisa Heininger3 Jörg Henes3Alexia Marina Radaelli1Anna Carmagnola1
Jörg Henes3Alexia Marina Radaelli1Anna Carmagnola1 Enrico Morello4,5Chiara Renica4,5Alice Bertulli4,5
Enrico Morello4,5Chiara Renica4,5Alice Bertulli4,5 Lorenzo Lazzari1Michelle Kenyon6
Lorenzo Lazzari1Michelle Kenyon6 Tobias Alexander7Ariadna Domenech8†
Tobias Alexander7Ariadna Domenech8† Raffaella Greco1*†
Raffaella Greco1*†- 1Hematology and Bone Marrow Transplantation Unit, IRCCS San Raffaele Hospital, Vita-Salute San Raffaele University, Milan, Italy
- 2Department of Haematology, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, United Kingdom
- 3Department of Internal Medicine II (Hematology, Oncology, Clinical Immunology and Rheumatology), University Hospital Tuebingen, Tuebingen, Germany
- 4Blood Diseases and Cell Therapies Unit, Bone Marrow Transplant Unit" ASST-Spedali Civili" Hospital of Brescia, Brescia, Italy
- 5Department of Clinical and Experimental Sciences, University of Brescia, Brescia, Italy
- 6Department of Haematology, King's College Hospital, London, United Kingdom
- 7Department of Rheumatology and Clinical Immunology, Charité - Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin Institute of Health, Berlin, Germany
- 8Bone Marrow Transplant Unit, Department of Hematology, Hospital Clínic of Barcelona, Barcelona, Spain
Autoimmune diseases (ADs) represent a heterogeneous group of conditions affecting 5–10% of the global population. In recent decades, hematopoietic stem cell transplant (HSCT), mainly autologous, has been successfully adopted to treat patients affected by severe/refractory ADs. In this context malnutrition has a detrimental impact on relapse, mortality, infection rate, engraftment, long-term survival, and prolongation of hospitalization. However, in this population, the management of nutrition should be improved since nutritional assessment is partially performed in routine clinical practice. A panel of nurses and physicians from the European Society for Blood and Marrow Transplantation (EBMT) reviewed all available evidence based on current literature and expert practices from centers with extensive experience in HSCT for ADs, on the nutritional management of ADs patients during HSCT procedure. In this context, adequate nutritional status predicts a better response to treatment and improves quality of life. Herein, a systematic and comprehensive monitoring of nutritional status before, during and after HSCT, with adequate nutritional support in the case of ADs patients, in addition to assessing the dietary requirements associated with HSCT has been covered. Moreover, given the singularity of each AD, the underlying disease should be considered for an appropriate approach. The management and evaluation of nutritional status must be carried out by a multidisciplinary team to assess the needs, monitor the effectiveness of each intervention, and prevent complications, especially in complex situations as patients affected by ADs.
Introduction
Autoimmune diseases (ADs) have had an increasing incidence in recent years (1). They constitute a heavy burden for affected patients, also resulting in considerable socioeconomic costs (2).
Over the last 3 decades, hematopoietic stem cell transplantation (HSCT) has been increasingly considered as treatment option for patients affected by severe/refractory ADs, inducing a total and stable remission of the disease (3–5). The European Society for Blood and Marrow Transplantation (EBMT) Autoimmune Diseases Working Party (ADWP) has played a central role in this development, with overall 3,992 HSCT (3,831 autografts and 91 allografts) registrations for ADs in adult patients (median age 39 years, range 18–76). Recent data has improved the evidence to support HSCT in Multiple Sclerosis (MS) and Systemic Sclerosis (SS), along with a wide range of other indications (3). More than half of the HSCTs registered in the ADWP database (Figure 1) have been performed on patients diagnosed with MS, followed by SS, and in a smaller group with Crohn’s Disease (CD).
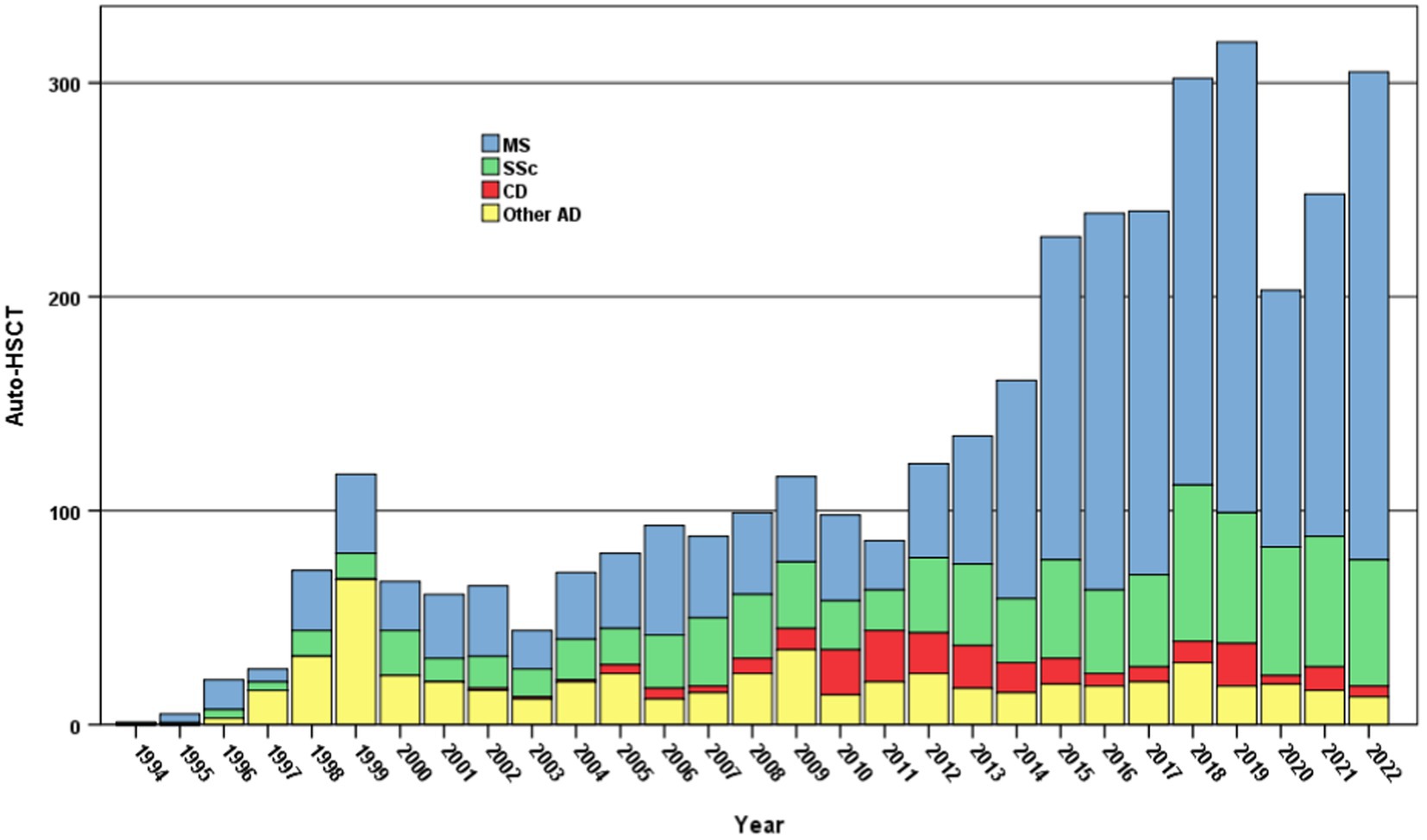
Figure 1. Autologous HSCT for ADs in adult patients - 1994-2022. Number of autologous HSCT reported to the EBMT-ADWP Registry data, per year and indication, from 1994 through 2022 (n = 3,831). AD, autoimmune disease; ADWP, Autoimmune Diseases Working Party; EBMT, European Society for Blood and Marrow Transplantation; HSCT, hematopoietic stem cell transplantation; MS, multiple sclerosis; SSc, systemic sclerosis; CD, crohn’s disease.
The continuous effort in ameliorating supportive care represents one of the cornerstones to improve the overall HSCT outcome in these patients. Nowadays, more than ever, nutritional support is considered a key feature for the success of HSCT procedure.
The conditioning regimen administered before HSCT generally causes inflammatory damage to the gastrointestinal tract, which determines the disruption of the mucosal barrier, leading to mucositis, loss of appetite, diarrhea, nausea, vomiting and dysgeusia (6). These symptoms, together with the catabolic state and infections sequelae, often result in suboptimal nutritional intake followed by loss of weight and lean body mass before and after transplant (7). These gastrointestinal complications, added to psycho-emotional factors, fatigue, decreased physical activity and prolonged hospitalization, are the main reasons for a severe and rapid nutritional decline after transplant (8, 9). The nutritional status deeply impacts on hospitalization, quality of life, infection rate and survival after HSCT (10–12). Moreover, in the allogeneic setting, nutritional impairment and gastroenteric damage may also trigger intestinal graft-versus-host disease (GvHD), which can further negatively affect food intake and gut absorption (6). It is crucial to consider that these alterations tend to persist long after transplant, having reported that 50% of the patients have not regained their weight after a year from HSCT, a fact that makes even more relevant the need to monitor the nutritional status of our patients before, during and after the procedure (13). In this context, the intestinal microbiota deeply affects the clinical outcome of HSCT patients in terms of mortality (14), infections (15, 16), and GvHD (17) including severely treatment-resistant AD patients, because of its interaction with the host’s immune system and its contribution toward immune-related complications related to the nature of the disease and its undergoing therapy (3). Moreover, the loss of fecal intestinal diversity in the peri-engraftment period after autologous HSCT is associated with decreased risk of death or progression (18).
Even if all these implications are widely studied, in real-world clinical practice, both awareness and consideration of nutritional issues remain poor and nutritional assessment is not routinely performed (6).
The aim of this review, developed on behalf of the European Society for Blood and Marrow Transplantation (EBMT) Autoimmune Diseases Working Party (ADWP) and Nurses Group, is to summarize the current literature and expert practices from experienced centers about nutritional assessment in AD patients undergoing HSCT, developing practical expert-based recommendations for the day-to-day care by healthcare professionals.
Nutritional screening and support during HSCT procedure
In all patients eligible for HSCT, the clinical guidelines of the European Society for Parenteral and Enteral Nutrition (ESPEN) recommend the systematic and comprehensive monitoring of nutritional status before, during and after transplant, together with an adequate nutritional support, when required (19, 20). Literature shows that between 10 and 15% of patients have malnutrition prior to transplant (6).
For this reason, before HSCT admission, all patients must receive a nutritional assessment and screening in order to implement corrective measures as soon as possible (6). There are different tools to assess the nutritional status of the patients and detect the risk of malnutrition, but currently one of the most used is the Malnutrition Universal Screening Tool (MUST). This tool helps in detecting not only patients with malnutrition but also those at risk and who could benefit from preventive nutritional interventions (21).
Among nutritional assessment tools, Patient-generated Subjective Global Assessment (PG-SGA) has the advantage of scoring patients’ reported outcomes regarding gastrointestinal symptoms, food intake and subjective perception. The alpha-numeric score could be useful in the assessment of malnutrition, triage and monitoring during the follow-up (22).
Patients at nutritional risk should undergo a complete evaluation to effectively diagnose malnutrition, through the assessment of phenotypic and etiologic criteria. Body composition analysis could help physicians in detecting malnourished patients who may have low muscle mass or sarcopenia, which are often hidden and overlooked, especially in patients with normal weight or excess adiposity (6). When malnutrition is diagnosed, a nutritional intervention aimed at maintaining or recovering appropriate nutritional status should be promptly initiated and tailored according to current nutritional status, clinical condition, planned treatment, and the expected outcome (6).
Where an assessment has not been carried out before, a screening for determining the risk of malnutrition should be performed using validated tools within 48 h of hospital admission, according to the Global Leadership Initiative on Malnutrition (23).
During the post-transplant period, patients may present increased nutritional requirements combined with impaired metabolism and difficulty in maintaining oral intake (19). Some suggested interventions during the procedure should involve adjusting the intake, modifying the diet and evaluating the need to administer oral nutritional supplements (ONS). In patients predicted to be unable to ingest and absorb adequate nutrients for a prolonged period, the implementation of Parenteral Nutrition (PN) or Enteral Nutrition (EN) is indicated (19). ESPEN guidelines prefer EN as first choice for nutritional support, associated with a lower incidence of infective complications, better overall survival and faster neutrophil engraftment. In the context of allogeneic HSCT, EN reduces the incidence of acute GvHD, mainly for severe and gut forms (24). In pediatric population undergoing HSCT, EN promotes a more favorable intestinal microbial network as compared to PN (25). Moreover, it is more physiological, and contributes to the preservation of gut mucosal integrity and function. On the other hand, limitations in the choice of EN, together with difficulties in positioning and tolerating the nasogastric tube or stoma, usually lead to a preferential use of PN in patients undergoing HSCT (6).
Nutrition and oropharyngeal mucositis
Oropharyngeal Mucositis (OM) refers to the inflammation of the oral and gastrointestinal mucosa. It is characterised by erythema and ulceration of the mucosal membrane which may result in pain, difficulty in swallowing, impaired taste and quality of life (QoL) for several weeks (26, 27). OM is common in patients receiving myeloablative doses of chemotherapy and can affect around 60 to 80% of HSCT recipients (28).
In this regard, a recent single centre, retrospective study demonstrated that patients receiving a myeloablative conditioning experienced grade 2–4 and grade 3–4 mucositis in 61 and 41% of cases, respectively (29). In this study, the mean duration was 4.2 days for grade 2–4 and 1.4 days for grade 3–4. In intensive regimes, based on busulfan or total body irradiation, OM may be prolonged.
OM may be prevented by cryotherapy, expecially in High Dose Melphalan conditioning (30).
OM may be reduced by good oral care, which is based on four key principles: accurate assessment, individualized care plans, initiation of timely preventative measures and correct treatment (31). Assessment should begin prior to commencing treatment and include a dental evaluation and an accurate patient history to assess risk factors for oral damage (32).
Inspection of the oral cavity should include the cheeks, lips, soft palate, floor of the mouth and tongue and should be initiated on admission, continued daily throughout treatment and at appropriate time points post discharge, until full healing has occurred. Patient education is a key aspect and patients should receive both verbal and written information about oral care to facilitate prompt reporting of problems.
As OM develops, healthcare professionals should manage pain medication and nutritional support (4). Although these measures may not reduce the severity of OM, many products can provide patient comfort and therefore help to maintain some food and fluid intake and enable rest (32). Adequate nutrition is vital to maintain mucosal integrity and reduce deterioration of existing damage enhancing repair (32).
Mucositis also affects the lower gastrointestinal tract and may lead to profuse diarrhea. Patients with CD, for example, will have a higher predisposition to this event. Other causes, such as infections, should be determined by stool cultures and appropriate treatment should be instigated. If cultures are negative, an antidiarrheal agent can be safely prescribed and close monitoring of fluids and electrolytes will be required, including liquid replacement as necessary (32).
In summary, the severity of OM in patients undergoing HSCT for ADs is very variable and centers will need to develop strategies to manage it depending on the underlying disease of the patient and the conditioning regimen used.
Nutrition and infections
Despite advances in supportive care, infections remain a significant cause of morbidity and mortality in the setting of HSCT (33, 34). The resultant injury on the gastrointestinal epithelial barrier by chemotherapy (CT) or radiotherapy (RT), and the extensive use of antibiotics during the neutropenic phase, may lead to gut microbiota dysbiosis (35). When dysbiosis occurs within the damaged gut epithelium and the equilibrium of the microbial composition becomes fluctuant, the dominant bacteria can potentially invade the bloodstream, causing bacteremia (16). These considerations make the intestinal microbiota an independent predictor of clinical outcome and mortality in patients undergoing HSCT (14, 15, 36). Diet and nutrition could positively affect microbiome diversity during HSCT procedure, as growing evidence suggests a link between them (37).
Various measures have been adopted to minimize the incidence of infections, including the use of a low-bacterial diet (LBD) that excludes raw food, fresh fruits, and vegetables (33). The rationale behind the use of LBD is to prevent the introduction of dangerous bacteria into the gastrointestinal tract, already damaged by CT or RT (33, 38). Regarding nutritional support with LBD or non-restrictive diet (NRD), the literature points out that the former has shown no benefit on infection rates or survival, in contrast with the routine use of low-microbial foods in clinical practice (39). Moreover, results from a recent randomized study by Stella et al. (33) demonstrated that the frequency of infections, deaths, nutritional outcomes, and acute GvHD was not different in patients receiving LBD versus NRD during the neutropenic phase after HSCT. These results suggest that the use of a restrictive diet is an unnecessary burden for patients’ QoL, even if, undoubtedly, data are more mature in the autologous HSCT setting in which LBD should no longer be recommended.
In the case of patients with ADs and an indication for transplant, in addition to assessing the nutritional requirements associated with the HSCT, it is essential to consider the underlying disease, since the singularity of each AD is important to carry out an adequate approach regarding nutritional indications.
Specific nutritional aspects for multiple sclerosis
Multiple sclerosis (MS) is an autoimmune-mediated neurodegenerative disease of the central nervous system characterised by inflammatory demyelination with axonal transection (40). MS typically presents in young adults and can lead to physical disability, cognitive impairment, and decreased QoL (40). A total of 2.8 million people is estimated to live with MS worldwide (35.9 per 100,000 population). The mean age of diagnosis is 32 years, with a female to male ratio of 2:1 (41).
Autologous HSCT represent a standard-of-care approach in patients with highly active relapsing remitting MS failing to respond to disease modifying therapies (DMTs) (42). This population of patients need a formal metabolic-nutritional assessment, as some of the factors affecting MS pathogenesis are genetic and/or environmental and may include obesity and malnutrition (43). MS patients may experience signs and symptoms such as loss of vision, weakness, numbness, gait difficulty and bowel and bladder disturbances (9). In particular, the sensorimotor symptoms affecting the gastroenteric trait may lead to dysphagia and gastrointestinal problems such as fecal incontinence, diarrhea and constipation that have a strong impact on nutritional status (43).
Many studies have reported a significant connection between intestinal microbiota, eating habits, and the development of chronic-degenerative diseases such as MS (44). An increasing number of studies tried to investigate the potential role of the diet in MS (45).
Even though no definitive dietary recommendations have been scientifically proven to be beneficial in changing the course of MS, literature shows that maintaining balanced, low saturated fats and high-fiber diet, which is also rich in probiotics and vitamins, is associated with a decreased risk for MS-related disability and fatigue and with higher QoL (43). In facts, a low-fats diet reduces the risk of developing cardiovascular disease and diabetes, comorbidities associated with increased disability and decreased QoL in patients with MS (46).
It is also currently unclear whether salt, gluten or dairy are specifically harmful in MS, even though diets high in salt, processed gluten-free foods, and processed dairy substitutes are often less healthy and should be limited to benefit overall health (47–49). A diet high in vitamins (A, B2, B7, D), lipoic acid, omega-3 polyunsaturated fatty acids and amino acids (L-carnitine) may also have direct effects on the immune system and the brain (43). Moreover, various studies have encouraged the use of pre and probiotics in patients with MS due to their benefits in maintaining the homeostasis of the central nervous system and regulating the composition and balance of the gut microbiota (50). In the setting of allogeneic HSCT, there are several studies whose findings suggest that synbiotic intake before and during the conditioning regimen of HSCT patients may lead to a reduction in the incidence and severity of acute GvHD and contribute to the improvement of transplant outcomes, such as infections rate (51, 52). Indeed, more studies are needed to confirm the indication in prebiotics and probiotics intake in this specific population of patients undergoing HSCT. Moreover, the general deconditioning occurring after HSCT procedure can be associated with a transient increase in functional impairment and decrease in body mass, requiring an early implementation of rehabilitation strategies in MS population (53), together with nutritional support.
Rigorous head-to-head comparisons of dietary interventions are needed to address whether a specific diet is more effective at improving fatigue and QoL, as well as traditional MS outcomes such as relapse rate, MRI disease activity and accumulated disability.
Specific nutritional aspects for systemic sclerosis
Systemic sclerosis (SSc) is a complex autoimmune connective tissue disease involving chronic and progressive tissue and organ fibrosis. Besides the skin, the gastrointestinal tract is the second most affected organ as approximately 70% of patients with SSc experience gastrointestinal symptoms within the first year (54, 55). Oropharyngeal and esophageal dysphagia, together with gastroesophageal reflux disease, malabsorption, constipation, diarrhea and fecal incontinence are the main complications (54). As the skin is the main organ involved, the lips are narrow and the forehead can no longer be moved; the opening of the mouth is restricted, the surface of the tongue becomes atrophic and its mobility restricted by the sclerotic hard lingual frenulum; moreover, the oral mucosa becomes dry (56). All the above aspects can lead to nutrient deficiencies because they affect food intake and absorption. The most frequently observed nutritional deficits in SSc are iron deficiency anemia and vitamin D deficiency (57).
Autologous HSCT is an effective therapeutic option for patients with severe SSc (58–60) as it can delay the progression of the disease and obtain improvements in organ function and skin condition (61). Autologous HSCT for early severe diffuse cutaneous SSc patients is now recommended as standard treatment (4). In this context, organ toxicity may be due to the preparative regimen and any underlying organ damage from SSc. The procedure comes with side effects affecting the gastrointestinal tract, and the prevalence of malnutrition is approximately 35% in SSc patients after HSCT (62). Gastrointestinal endoscopy has revealed gastric antral vascular ectasia (GAVE) in 22% of SSc patients screened before HSCT (63). Literature shows different ways to detect and document malnutrition as relying solely on BMI is not sufficient and the MUST tool is commonly used (64).
Nutritional therapy using enteral or parenteral support should be tailored to the clinical phenotype and severity of the disease. Parenteral nutrition is necessary when oral and/or enteral nutrition is inadequate or cannot be tolerated (65). As previously described, increased diarrhea may occur due to the SSc involvement of the gastrointestinal tract and may be related to food intolerances (particularly to gliadin, lactose and fructose) or can be the result of taking medication, particularly Nintedanib (66). Regarding the development of food intolerances, once identified through breath tests, the patient must receive nutritional advice on food modification. Anti-inflammatory diet and dietary measures aiming to promote gastric emptying, such as diets low in fats and fibers, are recommended (67). In addition, foods with a soft consistency are recommended. Eating several small portions throughout the day and drinking enough fluids is also helpful. An upright posture while eating and thorough chewing of food is recommended (54).
Specific nutritional aspects for Crohn’s disease
Crohn’s Disease (CD) is a chronic, autoimmune, inflammatory bowel disease (IBD) that causes inflammation and irritation of the gastrointestinal tract, which evolves recurrently with flare-ups. The most frequent location is the terminal ileum and colon and the main symptoms presented in patients with CD include abdominal pain, diarrhea, weight loss, fever, fatigue and rectal bleeding (68–70). The global prevalence of IBD has been increasing since 2000, due to low mortality and improved survival among these patients, affecting 1 in 200 individuals in Western Countries (71). It usually occurs in people younger than 30 and the prognosis is associated with the time of evolution of the disease from diagnosis, the extension of the disease, the severity of flares, the types of complications, and the preceding history of surgical treatment. Treatment-refractory CD is associated with adverse QoL, recurrent hospitalization and treatment-related morbidity (72). In this scenario, autologous HSCT can be considered a therapeutic option in patients with objective evidence of inflammatory activity, severe course of the disease over the years, inadequate response to different therapies, and when surgery is not a viable option or is accompanied by significant risks (73). Many groups reported a correlation between chronic intestinal inflammation in IBD and intestinal microbiota characteristics (44).
In this specific setting, the nutritional status and the impact of conditioning regimens on the gastrointestinal system must be carefully considered and patients with CD should receive nutritional counseling before the start of the transplant procedure (74).
Malnutrition affects 65–75% of patients diagnosed with IBD due to reduced intestinal absorption, changes in the intestinal microbiota and varied symptoms, such as loss of appetite, nausea and vomiting. Gastrointestinal symptoms, such as nausea, vomiting, diarrhea, and abdominal pain, have been often reported in CD patients after HSCT. In addition, a series of nutritional deficiencies characterize this group of patients, such as a lack of folate and vitamins A and D, and B12 malabsorption in the case of extensive bowel resections (74). Nutrition plays a fundamental role in reducing the symptoms associated with CD or in maintaining remission (75), and those with refractory disease present frequently with signs of malnutrition and cachexia (73). Furthermore, TGF-beta2 enriched food for special medical purposes could reduce inflammation and bowel damage in active disease (76), incidence of severe and gut acute GvHD, pneumonia and hospitalization costs (77).
Artificial nutrition which may include EN or PN, is a part of the treatment, especially in those undergoing elective surgery. In fact, in some centers, parenteral nutrition and nil-by-mouth regimens are implemented from the day of stem cell infusion until the engraftment (19, 78). Meanwhile, literature indicates that during PN intestinal digestive enzyme activity and exocrine pancreatic function decrease and, in addition, there is evidence that the ileum and jejunum show reductions in mucosal mass and function. For this reason, it is fundamental to consider using a weaning protocol during the transition from PN to oral intake. Tolerance to oral intake should be confirmed and, during the transition, it is mandatory to avoid overfeeding and consider reductions if nutrition and hydration remain stable (79). The ESPEN guidelines recommend evaluating the need for oral or intravenous fluids and electrolyte supplementation, preparing a nutritional monitoring plan after PN is stopped to ensure a safe transition to complete oral nutrition.
Finally, when talking about oral diet, literature includes the use of other diets, such as the specific carbohydrate diet, the low FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diet and the semi-vegetarian diet (74).
Recommendations for nurse management of nutritional status in ADs undergoing HSCT
Nurses play a fundamental role in the early detection of signs and symptoms of malnutrition and are pivotal in monitoring the effectiveness of supportive therapies. However, the literature lacks specific guidelines regarding nutritional support in AD patients undergoing HSCT.
Based on current literature and expert practices from centers with extensive experience in HSCT for ADs, the panel of nurses and physicians from EBMT ADWP and Nurses Group has developed expert-based recommendations on nutritional management of AD patients undergoing HSCT (Figure 2). Guidance was primarily based on literature, collection of common practice data and personal opinions of the experts involved in the current manuscript. A significant preparatory work based on a comprehensive literature review was carried out by the experts, serving as the basis for the discussions. Given the lack of high-quality evidence in the context of ADs undergoing HSCT, recommendations were not graded. They therefore represent the consensus views of all the authors.
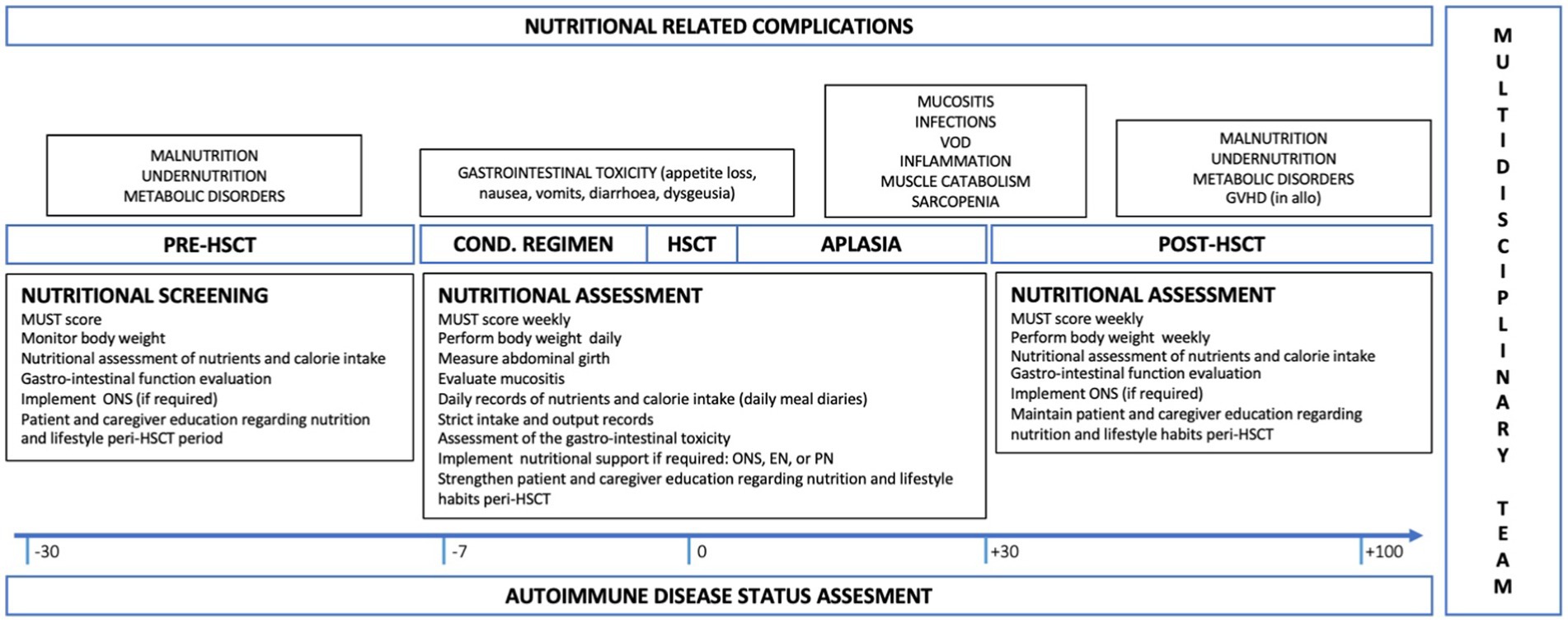
Figure 2. Flow chart of the ideal timing of assessment and interventions regarding nutritional support in AD patients undergoing HSCT. Nutritional interventions regarding each phase of the transplant procedure are here listed as regard to the literature suggestion and expert-base practices. All these interventions must be considered together with the nutritional-related complications, their severity and impact on patients’ food intake and QoL. AD, autoimmune disease; HSCT, hematopoietic stem cell transplantation; QoL, Quality of Life; MUST, Malnutrition Universal Screening Tool; ONS, Oral Nutritional Supplement; EN, Enteral Nutrition; PN, Parenteral Nutrition; VOD; Veno-Occlusive Disease; GvHD, Graft Versus Host Disease.
As nutritional support is a dynamic process across different phases, the first nutritional assessment must be performed before admission by a multidisciplinary team (8) or at least within 48 h after admission in the HSCT department (6). During the assessment, the healthcare team must evaluate the patient’s risk of developing malnutrition by obtaining and registering anthropometric parameters and baseline biochemical results together with using specific tools (i.e., MUST, NRS 2002, MNA, PG-SGA) (6). Other important information to collect is weight loss in the last 3–6 months and the patient’s inability to maintain his autonomy in daily living activities. If assessed before admission, as suggested by the centers involved, the collection of daily meal diaries helps to correct or integrate patients’ nutritional habits.
Once the assessment is done, the nursing team must carry out surveillance and control measures that facilitate the early detection of deterioration in the patient’s nutritional status since, in early stages, malnutrition can go unnoticed (6). It is mandatory to record complications associated with gastrointestinal toxicity derived from the conditioning regimen that may interfere with optimal oral intake and malabsorption. In the immediate post-HSCT, the team must consider the presence of neutropenia and the occurrence of infections that may influence patients’ nutritional status, producing weight loss and changes in body composition.
In addition, we recommend carrying out a nutritional record of daily intakes, to determine the appropriate inclusion of nutrients and calories, and the monitoring of MUST or similar tools once a week.
The nurse’s role is fundamental not only in detecting a possible deterioration in nutritional status but also in the education of patients and caregivers regarding what to eat, how to do that and when. In this regard, nurses must explain the rationale beside the nutritional support chosen and try to advocate patients’ preferences regarding nutrition when talking to the multidisciplinary team.
Importantly, nutritional support in patients undergoing autologous HSCT for ADs is a complex matter and must consider the underlying disease. Nutritional deficiencies and malabsorption must be suspected in the case of CD. Dysphagia and sensorimotor symptoms that affect the gastrointestinal tract are frequent in patients with MS, while chronic organ fibrosis that make chewing and swallowing difficult may occur in the case of SSc.
Conclusion and future perspectives
The annual number of patients treated with autologous HSCT is constantly increasing (3) and AD are among the fastest growing disease category reported to the EBMT for autologous HSCT (80). An adequate nutritional status predicts a better response to therapy and improved QoL for patients undergoing HSCT procedure (6). For this reason, management and assessment of the nutritional aspects must be performed by a multidisciplinary team before, during and after transplant, to evaluate the nutritional needs, monitor the effectiveness of each intervention, and prevent complications. Education of patients and caregivers on these aspects is essential. Moreover, therapeutic approaches targeting microbiota, such as probiotics, prebiotics and postbiotics, can manipulate and influence the microbiota–host interactions (81–83).
In ADs, it is essential to consider the underlying disease as patients may present with different organs and systems affections, making it challenging to achieve adequate nutritional intake. There is evolving rationale, experience and forward vision of clinical experience by nurses and physicians in this setting. Further studies are needed to increase knowledge in this population, starting from the comparison of expert-based approaches and practices across the transplant and disease-specific communities.
Author contributions
CG: Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing, Formal analysis, Validation. HJ: Writing – original draft, Writing – review & editing. AH: Writing – original draft, Writing – review & editing. LH: Writing – original draft, Writing – review & editing. JH: Writing – original draft, Writing – review & editing. AR: Writing – original draft, Writing – review & editing. AC: Writing – original draft, Writing – review & editing. EM: Writing – original draft, Writing – review & editing. CR: Writing – original draft, Writing – review & editing. AB: Writing – original draft, Writing – review & editing. LL: Writing – original draft, Writing – review & editing. MK: Writing – original draft, Writing – review & editing. TA: Writing – original draft, Writing – review & editing. AD: Data curation, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Acknowledgments
The authors contribute this article on behalf of ADWP and Nurses Group of the EBMT. We are grateful for the support by EBMT, ADWP, and Nurse Group without which this work would not have been possible. The authors thank Manuela Badoglio and Myriam Labopin in the EBMT Paris Office, EBMT centers for their contributions to the EBMT registry and those active in the ADWP.
Conflict of interest
RG discloses speaking honoraria from Biotest, Pfizer, Medac, Neovii and Magenta. TA received study support from Amgen, Janssen and honoraria from Neovii, GSK, Astra-Zeneca, Abbvie.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rose, NR. Prediction and prevention of autoimmune disease in the 21st century: a review and preview. Am J Epidemiol. (2016) 183:403–6. doi: 10.1093/aje/kwv292
2. Tappenden, P, Wang, Y, Sharrack, B, Burman, J, Kazmi, M, Saccardi, R, et al. Evaluating the clinical effectiveness of autologous haematopoietic stem cell transplantation versus disease-modifying therapy in multiple sclerosis using a matching-adjusted indirect comparison: an exploratory study from the Autoimmune Diseases Working Party (ADWP) of the European Society of Bone and Marrow Transplantation (EBMT). Bone Marrow Transplant. (2019) 55:1473–5. doi: 10.1038/s41409-019-0747-2
3. Alexander, T, and Greco, R. Hematopoietic stem cell transplantation and cellular therapies for autoimmune diseases: overview and future considerations from the Autoimmune Diseases Working Party (ADWP) of the European Society for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. (2022) 57:1055–62. doi: 10.1038/s41409-022-01702-w
4. Snowden, J.A., Ismail, A., Burt, R.K., and Jessop, H. Early toxicity and supportive care of HSCT for autoimmune diseases in Hematopoietic stem cell transplantation and cellular therapies for auto-immune diseases Eds. Burt, R.K., Farge, D., Ruiz, M.A., Saccardi, R., and Snowden, J. A (2022).
5. Snowden, JA, Sánchez-Ortega, I, Corbacioglu, S, Basak, GW, Chabannon, C, De la Camara, R, et al. European Society for Blood and Marrow Transplantation (EBMT). Indications for haematopoietic cell transplantation for haematological diseases, solid tumours and immune disorders: current practice in Europe. Bone Marrow Transplant. (2022) 57:1217–39. doi: 10.1038/s41409-022-01691-w
6. Casirati, A, Salcedo, I, Cereda, E, Chabannon, C, Ruggeri, A, Kuball, J, et al. The European Society for Blood and Marrow Transplantation (EBMT) roadmap and perspectives to improve nutritional care in patients undergoing hematopoietic stem cell transplantation on behalf of the Cellular Therapy and Immunobiology Working Party (CTIWP) and the Nurses Group (NG) of the EBMT. Bone Marrow Transplant. (2023) 58:965–72. doi: 10.1038/s41409-023-02018-z
7. Kiss, N, Seymour, JF, Prince, HM, and Dutu, G. Challenges and outcomes of a randomized study of early nutrition support during autologous stem-cell transplantation. Curr Oncol. (2014) 21:334–9. doi: 10.3747/co.21.1820
8. Botti, S, Liptrott, SJ, Gargiulo, G, and Orlando, L. Nutritional support in patients undergoing haematopoietic stem cell transplantation: a multicentre survey of the Gruppo Italiano Trapianto Midollo Osseo (GITMO) transplant programmes. Ecancermedicalscience. (2015) 9:545. doi: 10.3332/ecancer.2015.545
9. Katz Sand, I. The role of diet in multiple sclerosis: mechanistic connections and current evidence. Curr Nutr Rep. (2018) 7:150–60. doi: 10.1007/s13668-018-0236-z
10. Baumgartner, A, Zueger, N, Bargetzi, A, Medinger, M, Passweg, JR, Stanga, Z, et al. Association of nutritional parameters with clinical outcomes in patients with acute myeloid leukemia undergoing haematopoietic stem cell transplantation. Ann Nutr Metab. (2016) 69:89–98. doi: 10.1159/000449451
11. Rzepecki, P, Barzal, J, and Oborska, S. Blood and marrow transplantation and nutritional support. Support Care Cancer. (2010) 18:57–65. doi: 10.1007/s00520-009-0730-3
12. Szovati, S, Morrison, CF, and Couch, SC. Nutritional status of allogeneic hematopoietic stem cell transplant recipients and post-transplant outcomes. Nutr Cancer. (2023) 75:1200–10. doi: 10.1080/01635581.2023.2186261
13. Iestra, JA, Fibbe, WE, Zwinderman, AH, Van Staveren, WA, and Kromhout, D. Body weight recovery, eating difficulties and compliance with dietary advice in the first year after stem cell transplantation: a prospective study. Bone Marrow Transplant. (2002) 29:417–24. doi: 10.1038/sj.bmt.1703375
14. Peled, JU, Gomes, ALC, Devlin, SM, Littmann, ER, Taur, Y, Sung, AD, et al. Microbiota as predictor of mortality in allogeneic hematopoietic-cell transplantation. N Engl J Med. (2020) 382:822–34. doi: 10.1056/NEJMoa1900623
15. Mancini, N, Greco, R, Pasciuta, R, Barbanti, MC, Pini, G, Morrow, OB, et al. Enteric microbiome markers as early predictors of clinical outcome in allogeneic hematopoietic stem cell transplant: results of a prospective study in adult patients. Open Forum Infect Dis. (2017) 4:ofx215. doi: 10.1093/ofid/ofx215
16. Taur, Y, Xavier, JB, Lipumam, L, Ubeda, C, Goldberg, J, Gobourne, A, et al. Intestinal domination and the risk of bacteremia in patients undergoing allogeneic hematopoietic stem cell transplantation. Clin Infect Dis. (2012) 55:905–14. doi: 10.1093/cid/cis580
17. Jenq, RR, Taur, Y, Devlin, SM, Ponce, DM, Goldberg, JD, Ahr, KF, et al. Intestinal blautia is associated with reduced death from graft-versus-host disease. Biol Blood Marrow Transplant. (2015) 21:1373–83. doi: 10.1016/j.bbmt.2015.04.016
18. Khan, N, Lindner, S, Gomes, ALC, Devlin, SM, Shah, GL, Sung, AD, et al. Fecal microbiota diversity disruption and clinical outcomes after auto-HCT: a multicenter observational study. Blood. (2021) 137:1527–37. doi: 10.1182/blood.2020006923
19. August, DA, and Huhmann, MB. American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors. A.S.P.E.N. clinical guidelines: nutrition support therapy during adult anticancer treatment and in hematopoietic cell transplantation. JPEN J Parenter Enteral Nutrition. (2009) 33:472–500. doi: 10.1177/0148607109341804
20. Cederholm, T, Barazzoni, R, Austin, P, Ballmer, P, Biolo, G, Bischoff, SC, et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin Nutr. (2016) 36:49–64. doi: 10.1016/j.clnu.2016.09.004
21. Elia, M. The 'MUST' report. Nutritional screening for adults: a multidisciplinary responsibility. Development and use of the 'Malnutrition Universal Screening Tool' (MUST) for adults British Association for Parenteral and Enteral Nutrition (Redditch: BAPEN) (2003).
22. Nakyeyune, R, Ruan, X, Shen, Y, Shao, Y, Niu, C, Zang, Z, et al. Diagnostic performance of SGA, PG-SGA and MUST for malnutrition assessment in adult cancer patients: a systematic literature review and hierarchical bayesian meta-analysis. Nutr Cancer. (2022) 74:903–15. doi: 10.1080/01635581.2021.1942080
23. Cederholm, T, Jensen, GL, Correia, MITD, Gonzalez, MC, Fukushima, R, Higashiguchi, T, et al. GLIM criteria for the diagnosis of malnutrition - a consensus report from the global clinical nutrition community. Clin Nutr. (2019) 38:1–9. doi: 10.1016/j.clnu.2018.08.002
24. Zama, D, Gori, D, Muratore, E, Leardini, D, Rallo, F, Turroni, S, et al. Enteral versus parenteral nutrition as nutritional support after allogeneic hematopoietic stem cell transplantation: a systematic review and meta-analysis. Transplant Cell Ther. (2021) 27:180.e1–8. doi: 10.1016/j.jtct.2020.11.006
25. Fabbrini, M, D'Amico, F, Leardini, D, Muratore, E, Barone, M, Belotti, T, et al. Levofloxacin prophylaxis and parenteral nutrition have a detrimental effect on intestinal microbial networks in pediatric patients undergoing HSCT. Commun Biol. (2023) 6:36. doi: 10.1038/s42003-023-04436-7
26. Al-Dasoogi, N, Soni, SST, Bowen, JM, Bateman, E, Blijlevens, N, Gibson, RJ, et al. Emerging evidence of the pathology of mucositis. Support Care Cancer. (2013) 21:3233–41. doi: 10.1007/s00520-013-1900-x
27. Kashiwasaki, H, Matsushita, T, Sugita, J, Shigematsu, A, Kawashi, K, Yamazaki, Y, et al. Professional oral healthcare reduces oral mucositis and febrile neutropenia in patients treated with allogeneic bone marrow transplantation. Support Care Cancer. (2012) 20:367–73. doi: 10.1007/s00520-011-1116-x
28. Burt, RK, Farge, D, Ruiz, MA, Saccardi, R, and Snowden, JA. Hematopoietic Stem Cell Transplantation and Cellular Therapies for Autoimmune Diseases. (2021).
29. Nakagaki, M, Kennedy, GA, Gavin, NC, Clavarino, A, and Whitfield, K. The incidence of severe oral mucositis in patients undergoing different conditioning regimens in haematopoietic stem cell transplantation. Support Care Cancer. (2022) 30:9141–9. doi: 10.1007/s00520-022-07328-4
30. Riley, P, Glenny, AM, Worthington, HV, Littlewood, A, Clarkson, JE, and McCabe, MG. Interventions for preventing oral mucositis in patients with cancer receiving treatment: oral cryotherapy. Cochrane Database Syst Rev. (2015) 2015:CD011552. doi: 10.1002/14651858.CD011552.pub2
31. Quinn, B, Campbell, F, Fulmann, L, Harding, J, Dargan, S, Mathlin, J, et al. Oral care of patients in the cancer setting. Cancer Nurs Pract. (2020) 19:35–42. Available at: https://journals.rcni.com/cancer-nursing-practice/cpd/oral-care-of-patients-in-the-cancer-setting-cnp.2020.e1706/print/abs.
32. Wallhult, E, Kenyon, M, and Quinn, B. Early and acute complications and the principles of HSCT nursing care In: M Kenyon and A Babic, editors. The European blood and marrow transplantation textbook for nurses. Springer, Cham. (2023) doi: 10.1007/978-3-031-23394-4_10
33. Stella, F, Marasco, V, Levati, GV, Guidetti, A, De Filippo, A, Pennisi, M, et al. Nonrestrictive diet does not increase infections during post-HSCT neutropenia: data from a multicenter randomized trial. Blood Adv. (2023) 7:5996–6004. doi: 10.1182/bloodadvances.202301034.
34. Styczynski, J, Tridello, G, Koster, L, Knelange, N, Wendel, L, Van Biezen, A, et al. Decrease of lethal infectious complications in the context of causes of death (COD) after hematopoietic cell transplantation: COD-2 and COD-1 study of the Infectious Diseases Working Party EBMT. Bone Marrow Transplant. (2023) 58:881–92. doi: 10.1038/s41409-023-01998-2
35. Chong, PP, and Koh, AY. The gut microbiota in transplant patients. Blood Rev. (2020) 39:100614. doi: 10.1016/j.blre.2019.100614
36. Taur, Y, Jenq, RR, Perales, MA, Littmann, ER, Morjaria, S, Ling, L, et al. The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation. Blood. (2014) 124:1174–82. doi: 10.1182/blood-2014-02-554725
37. David, LA, Maurice, CF, Carmody, RN, Gootenberg, DB, Button, JE, Wolfe, BE, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. (2014) 505:559–63. doi: 10.1038/nature12820
38. Sonbol, M, Firwana, B, and Diab, M. The effect of a neutropenic diet on infection and mortality rates in cancer patients: a meta-analysis. Nutr Cancer. (2015) 67:1232–40. doi: 10.1080/01635581.2015.1082109
39. Baumgartner, A, Hoskin, K, and Schuetz, P. Optimization of nutrition during allogeneic hematologic stem cell transplantation. Curr Opin Clin Nutr Metab Care. (2018) 21:152–8. doi: 10.1097/MCO.0000000000000461
40. McGinley, MP, Goldschmidt, CH, and Rae-Grant, AD. Diagnosis and treatment of multiple sclerosis: a review. JAMA. (2021) 325:765–79. doi: 10.1001/jama.2020.26858
41. Walton, C, King, R, Rechtman, L, Kaye, W, Leray, E, Marrie, RA, et al. Rising prevalence of multiple sclerosis worldwide: insights from the Atlas of MS, third edition. Mult Scler. (2020) 26:1816–21. doi: 10.1177/1352458520970841
42. Sharrack, B, Saccardi, R, Alexander, T, Badoglio, M, Burman, J, Farge, D, et al. European Society for Blood and Marrow Transplantation (EBMT) Autoimmune Diseases Working Party (ADWP) and the Joint Accreditation Committee of the International Society for Cellular Therapy (ISCT) and EBMT (JACIE). Autologous haematopoietic stem cell transplantation and other cellular therapy in multiple sclerosis and immune-mediated neurological diseases: updated guidelines and recommendations from the EBMT Autoimmune Diseases Working Party (ADWP) and the Joint Accreditation Committee of EBMT and ISCT (JACIE). Bone Marrow Transplant. (2020) 55:283–306. doi: 10.1038/s41409-019-0684-0
43. Stoiloudis, P, Kesidou, E, Bakirtzis, C, Sintila, SA, Konstantinidou, N, Boziki, M, et al. The role of diet and interventions on multiple sclerosis: a review. Nutrients. (2022) 14:1150. doi: 10.3390/nu14061150
44. Alexander, T, Snowden, JA, Burman, J, Chang, HD, Del Papa, N, Farge, D, et al. Intestinal microbiome in hematopoietic stem cell transplantation for autoimmune diseases: considerations and perspectives on behalf of autoimmune diseases working party (ADWP) of the EBMT. Front Oncol. (2021) 22:722436. doi: 10.3389/fonc.2021.722436
45. Katz Sand, I, Benn, EKT, Fabian, M, Fitzgerald, KC, Digga, E, Deshpande, R, et al. Randomized-controlled trial of a modified Mediterranean dietary program for multiple sclerosis: a pilot study. Mult Scler Relat Disord. (2019) 36:101403. doi: 10.1016/j.msard.2019.101403
46. Marrie, RA, Horwitz, R, Cutter, G, and Tyry, T. Cumulative impact of comorbidity on quality of life in MS. Acta Neurol Scand. (2012) 125:180–6. doi: 10.1111/j.1600-0404.2011.01526.x
47. Farez, MF, Fiol, MP, Gaitán, MI, Quintana, FJ, and Correale, J. Sodium intake is associated with increased disease activity in multiple sclerosis. J Neurol Neurosurg Psychiatry. (2015) 86:26–31. doi: 10.1136/jnnp-2014-307928
48. Fitzgerald, KC, Tyry, T, Salter, A, Cofield, SS, Cutter, G, Fox, R, et al. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology. (2018) 90:e1–e11. doi: 10.1212/WNL.0000000000004768
49. Rodrigo, L, Hernandez-Lahoz, C, Fuentes, D, Mauri, G, Alvarez, N, Vega, J, et al. Randomised clinical trial comparing the efficacy of a gluten-free diet versus a regular diet in a series of relapsing-remitting multiple sclerosis patients. Int J Neurol Neurother. (2014) 1:012. doi: 10.23937/2378-3001/1/1/1012
50. Riccio, P, and Rossano, R. Nutrition facts in multiple sclerosis. ASN Neuro. (2015) 7:175909141456818. doi: 10.1177/1759091414568185
51. Andermann, TM, Rezvanim, A, and Bhatt, AS. Microbiota manipulation with prebiotics and probiotics in patients undergoing stem cell transplantation. Curr Hematol Malig Rep. (2016) 11:19–28. doi: 10.1007/s11899-016-0302-9
52. Yazdandoust, E, Hajifathali, A, Roshandel, E, Zarif, MN, Pourfathollah, AA, Parkhideh, S, et al. Gut microbiota intervention by pre and probiotics can induce regulatory T cells and reduce the risk of severe acute GVHD following allogeneic hematopoietic stem cell transplantation. Transpl Immunol. (2023) 78:101836. doi: 10.1016/j.trim.2023.101836
53. Roberts, F, Hobbs, H, Jessop, H, Bozzolini, C, Burman, J, Greco, R, et al. Rehabilitation before and after autologous haematopoietic stem cell transplantation (AHSCT) for patients with multiple sclerosis (MS): consensus guidelines and recommendations for best clinical practice on behalf of the Autoimmune Diseases Working Party, Nurses Group, and Patient Advocacy Committee of the European Society for Blood and Marrow Transplantation (EBMT). Front Neurol. (2020) 11:556141. doi: 10.3389/fneur.2020.556141
54. Asunción Recasens, M, Puig, C, and Ortiz-Santamaria, V. Nutrition in Systemic Sclerosis. Reumatol Clin. (2012) 3:135–40. doi: 10.1016/j.reumae.2011.09.003
55. Launay, D, Montani, D, Hassoun, P, Cottin, V, Le Pavec, J, and Clerson, P. Clinical phenotypes and survival of pre-capillary pulmonary hypertension in systemic sclerosis. PLoS One. (2018) 13:13(5). doi: 10.1371/journal.pone.0197112
56. Hunzelmann, N, and Krieg, T. Sklerodermie In: G Plewig, T Ruzicka, R Kaufmann, and M Hertl, editors. Braun-Falco’s Dermatologie, Venerologie und Allergologie. Heidelberg: Springe. (2018). 919–35.
57. Ortiz-Santamaria, V, Puig, C, Soldevillla, C, Barata, A, Cuquet, J, and Recasens, A. Nutritional support in patients with systemic sclerosis. Reumatol Clin. (2014) 10:283–7. doi: 10.1016/j.reuma.2013.12.011
58. Burt, RK, Shah, SJ, Dill, K, Grant, T, Gheorghiade, M, Schroeder, J, et al. Autologous non-myeloablative haemopoietic stem-cell transplantation compared with pulse cyclophosphamide once per month for systemic sclerosis (ASSIST): an open-label, randomised phase 2 trial. Lancet. (2011) 378:498–506. doi: 10.1016/S0140-6736(11)60982-3
59. Sullivan, KM, Goldmuntz, EA, Keyes-Elstein, L, McSweeney, PA, Pinckney, A, Welch, B, et al. Myeloablative autologous stem-cell transplantation for severe scleroderma. N Engl J Med. (2018) 378:35–47. doi: 10.1056/NEJMoa1703327
60. Van Laar, JM, Farge, D, Sont, JK, Naraghi, K, Marjanovic, Z, Larghero, J, et al. Autologous hematopoietic stem cell transplantation vs intravenous pulse cyclophosphamide in diffuse cutaneous systemic sclerosis a randomized clinical trial. JAMA. (2014) 311:2490–8. doi: 10.1001/jama.2014.6368
61. Henes, JC, Wirths, S, and Kötter, I. Autologous stem cell transplantation in systemic sclerosis. Z Rheumatol. (2016) 75:762–9. doi: 10.1007/s00393-016-0168-1
62. Atkins, L, Steer, B, Ray, H, and Kiss, N. Implementing and sustaining an evidence-based nutrition service in a haematology unit for autologous stem cell transplant patients. Support Care Cancer. (2019) 27:951–8. doi: 10.1007/s00520-018-4384-x
63. Hung, EW, Mayes, MD, Sharif, R, Assassi, S, Machicao, VI, Hosing, C, et al. Gastric antral vascular ectasia and its clinical correlates in patients with early diffuse systemic sclerosis in the SCOT trial. J Rheumatol. (2013) 40:455–60. doi: 10.3899/jrheum.121087
64. Wojteczek, A, Dardzinska, J, Malgorzewicz, S, Gruszecka, A, and Zbigniew, Z. Prevalence of malnutrition in systemic sclerosis patients assessed by different diagnostic tools. Clin Rheumatol. (2019) 39:227–32. doi: 10.1007/s10067-019-04810-z
65. Harrison, E, Herrick, A, McLaughlin, J, and Lal, S. Malnutrition in systemic sclerosis. Rheumatology. (2012) 51:1747–56. doi: 10.1093/rheumatology/kes160
66. Distler, O, Highland, KB, Gahlemann, M, Azuma, A, Fischer, A, Mayes, MD, et al. Nintedanib for systemic sclerosis-associated interstitial lung disease. N Engl J Med. (2019) 380:2518–28. doi: 10.1056/NEJMoa1903076
67. Furnari, M, Savarino, V, de Bortoli, N, and Savarino, E. Interstitial lung disease in systemic sclerosis patients may benefit more from anti-reflux therapies than from immunosuppressants. Autoimmun Rev. (2016) 15:1208–9. doi: 10.1016/j.autrev.2016.09.025
68. Feuerstein, JD, and Cheifetz, AS. Crohn’s disease: epidemiology, diagnosis, and management. Mayo Clin Proc. (2017) 92:1088–103. doi: 10.1016/j.mayocp.2017.04.010
69. Sands, BE. From symptom to diagnosis: clinical distinctions among various forms of intestinal inflammation. Gastroenterology. (2004) 126:1518–32. doi: 10.1053/j.gastro.2004.02.072
70. Veauthier, B, and Hornecker, JR. Crohn's disease: diagnosis and management. Am Fam Physician. (2018) 98:661–9.
71. Roda, G, Chien, NGS, Kotze, PG, Argollo, M, Panaccione, R, Spinelli, A, et al. Crohn’s disease. Nat Rev Dis Primers. (2020) 6:22. doi: 10.1038/s41572-020-0156-2
72. Van der Valk, ME, Mangen, MJ, Leenders, M, Dijkstra, G, van Bodegraven, AA, Fidder, HH, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFα therapy: results from the COIN study. Gut. (2014) 63:72–9. doi: 10.1136/gutjnl-2012-303376
73. Snowden, JA, Hawkey, C, Hind, D, Swaby, L, Mellor, K, Emsley, R, et al. Autologous stem cell transplantation in refractory Crohn's disease - low intensity therapy evaluation (ASTIClite): study protocols for a multicentre, randomised controlled trial and observational follow up study. BMC Gastroenterol. (2019) 19:82. doi: 10.1186/s12876-019-0992-2
74. Caio, G, Lungaro, L, Caputo, F, Zoli, E, Giancola, F, Chiarioni, G, et al. Nutritional treatment in Crohn's disease. Nutrients. (2021) 13:1628. doi: 10.3390/nu13051628
75. Więcek, M, Panufnik, P, Pomorska, K, Lewandowski, K, and Rydzewska, G. Diet as therapeutic intervention in Crohn's disease. Prz Gastroenterol. (2022) 17:96–102. doi: 10.5114/pg.2022.116376
76. Ferreira, TMR, Albuquerque, A, Cancela Penna, FG, Macedo Rosa, R, Correia, MITD, Barbosa, AJA, et al. Effect of oral nutrition supplements and TGF-β2 on nutrition and inflammatory patterns in patients with active Crohn's disease. Nutr Clin Pract. (2020) 35:885–93. doi: 10.1002/ncp.10448
77. Morello, E, Brambilla, G, Bernardi, S, Villanacci, V, Carlessi, M, Farina, M, et al. Nutritional intervention with TGF-beta enriched food for special medical purposes (TGF-FSMP) is associated with a reduction of malnutrition, acute GVHD, pneumonia and may improve overall survival in patients undergoing allogeneic hematopoietic stem transplantation. Transpl Immunol. (2023) 81:101954. doi: 10.1016/j.trim.2023.101954
78. Snowden, JA, Panés, J, Alexander, T, Allez, M, Ardizzone, S, Dierickx, D, et al. Autologous haematopoietic stem cell transplantation (AHSCT) in Severe Crohn's disease: a review on Behalf of ECCO and EBMT. J Crohns Colitis. (2018) 12:476–88. doi: 10.1093/ecco-jcc/jjx184
79. Worthington, P, Balint, J, Bechtold, M, Bingham, A, Chan, L-N, Durfee, S, et al. When is parenteral nutrition appropriate? J Parenter Enter Nutr. (2017) 41:324–77. doi: 10.1177/0148607117695251
80. Passweg, JR, Baldomero, H, Chabannon, C, Basak, GW, de la Camara, R, Corbacioglu, S, et al. Hematopoietic cell transplantation and cellular therapy survey of the EBMT: monitoring of activities and trends over 30 years. Bone Marrow Transplant. (2021) 56:1651–64. doi: 10.1038/s41409-021-01227-8
81. Andermann, TM, Fouladi, F, Tamburini, FB, Sahaf, B, Tkachenko, E, Greene, C, et al. A Fructo-Oligosaccharide Prebiotic Is Well Tolerated in Adults Undergoing Allogeneic Hematopoietic Stem Cell Transplantation: A Phase I Dose-Escalation Trial. Transplant Cell Ther. (2021) 27:932.e1–932.e11. doi: 10.1016/j.jtct.2021.07.009
82. D'Amico, F, Decembrino, N, Muratore, E, Turroni, S, Muggeo, P, Mura, R, et al. Oral lactoferrin supplementation during induction chemotherapy promotes gut microbiome eubiosis in pediatric patients with hematologic malignancies. Pharmaceutics. (2022) 14:1705. doi: 10.3390/pharmaceutics14081705
Keywords: nutrition, nutritional support, hematopoietic stem cell transplantation, autoimmune diseases, multiple sclerosis, systemic sclerosis, Crohn’s disease
Citation: Gandossi C, Jessop H, Hahn A, Heininger L, Henes J, Radaelli AM, Carmagnola A, Morello E, Renica C, Bertulli A, Lazzari L, Kenyon M, Alexander T, Domenech A and Greco R (2024) Nutritional aspects in autoimmune diseases undergoing hematopoietic stem cell transplantation: overview and recommendations on behalf of the EBMT ADWP and Nurses Group. Front. Nutr. 11:1394518. doi: 10.3389/fnut.2024.1394518
Edited by:
Geórgia das Graças Pena, Federal University of Uberlandia, BrazilReviewed by:
Edoardo Muratore, University of Bologna, ItalyMaria Teresa Cencioni, Imperial College London, United Kingdom
Copyright © 2024 Gandossi, Jessop, Hahn, Heininger, Henes, Radaelli, Carmagnola, Morello, Renica, Bertulli, Lazzari, Kenyon, Alexander, Domenech and Greco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chiara Gandossi, Z2FuZG9zc2kuY2hpYXJhQGhzci5pdA==; Raffaella Greco, Z3JlY28ucmFmZmFlbGxhQGhzci5pdA==
†These authors have contributed equally to this work