 Cláudia Ferreira1*†
Cláudia Ferreira1*† Joana Pereira1†
Joana Pereira1† David Skvarc2
David Skvarc2 Sara Oliveira1Ana Galhardo1,3
Sara Oliveira1Ana Galhardo1,3 Nuno B. Ferreira4Paola Lucena-Santos1
Nuno B. Ferreira4Paola Lucena-Santos1 Sérgio A. Carvalho1,5Inês Matos-Pina1
Sérgio A. Carvalho1,5Inês Matos-Pina1 Bárbara S. Rocha6Francisco Portela7
Bárbara S. Rocha6Francisco Portela7 Inês A. Trindade1,8*
Inês A. Trindade1,8*- 1CINEICC, Faculty of Psychology and Education Sciences, University of Coimbra, Coimbra, Portugal
- 2EMBRACE Lab, School of Behavioural, Social and Legal Sciences, University of Örebro, Örebro, Sweden
- 3Instituto Superior Miguel Torga, Coimbra, Portugal
- 4School of Social Sciences, University of Nicosia, Nicosia, Cyprus
- 5HEI-Lab: Digital Human-Environment Interaction Lab, School of Psychology and Life Sciences, Lusófona University, Lisbon, Portugal
- 6Center for Neuroscience and Cell Biology, Faculty of Pharmacy, University of Coimbra, Coimbra, Portugal
- 7Coimbra University Hospital [CHUC], Gastroenterology Service, Coimbra, Portugal
- 8School of Behavioural, Social and Legal Sciences, University of Örebro, Örebro, Sweden
Objectives: This study tested the acceptability and efficacy of an Acceptance and Commitment Therapy and compassion-based intervention (LIFEwithIBD) in people with IBD through a two-arm RCT.
Methods: Participants were recruited at the Gastroenterology Department of the Coimbra University Hospital between June and September 2019. Of the 355 patients screened, those who accepted to participate were randomly assigned to one of two conditions: experimental group (LIFEwithIBD; n = 25) or control group (waitlist; n = 29). Participants completed self-report measures at baseline (T0), post-intervention (T1), and 3-month (T2) and 12-month (T3) follow-ups. Intervention acceptability was assessed. Efficacy was examined using intent-to-treat ANCOVA at post-intervention after adjusting for baseline values of depressive, anxiety, and stress symptoms (primary outcomes). Linear mixed models for all longitudinal outcomes were also analysed. Inflammatory and disease biomarkers were determined at T0 and T3.
Results: Acceptability results revealed a high level of satisfaction and perceived usefulness regarding the intervention. Both groups experienced a significant decrease in stress symptoms and IBD symptom perception at T1. No significant differences were observed at follow-up for the primary outcomes. The experimental group reported significantly lower Crohn’s disease Symptom severity at T2 than the control group. Post-hoc analyses designed to mitigate floor effects revealed substantial treatment effects for the experimental group regarding anxiety symptoms. No significant differences were observed in clinical biomarkers from T0 to T3.
Conclusion: The LIFEwithIBD intervention shows promising, although preliminary, benefits for managing disease activity and reducing anxiety symptoms in IBD patients with high severity of psychological distress.
Clinical trial registration: https://www.clinicaltrials.gov/ct2/show/NCT03840707, identifier NCT03840707.
1 Introduction
Inflammatory bowel disease (IBD) considerably impacts the quality of life and raises the risk of developing mental health problems (Knowles et al., 2018). People with IBD have a higher prevalence of anxiety and depression than the general population (Barberio et al., 2021). Depression can increase IBD symptoms through the production of proinflammatory (Taché and Bernstein, 2009), which may itself increase levels of depressive symptoms (Keefer and Kane, 2017). In conjunction with medical care, psychological therapies might have beneficial effects on disease activity, mental health, and quality of life in people with IBD (Paulides et al., 2021).
Third-wave cognitive and behavioural therapies (CBT) (e.g., Mindfulness-Based Interventions, Acceptance and Commitment Therapy [ACT], and Compassion Focused Therapy [CFT]). have been suggested as particularly pertinent in populations with illness (Graham et al., 2016; Ferreira et al., 2018; Trindade et al., 2018). ACT intends to increase psychological flexibility through acceptance- and mindfulness-promoting techniques that increase willingness to go through adverse internal experiences (e.g., thoughts, feelings, sensations) while engaging with commitment in actions that promote a valued and meaningful life (Hayes et al., 2011).
Recent findings have highlighted that ACT-based interventions seem to be efficacious in reducing symptoms of stress (Lavelle et al., 2022), depression and anxiety (Romano et al., 2023) as well as feasible and well-accepted by adults living with IBD (Dober et al., 2021; Lavelle et al., 2022; Romano et al., 2023). Although these studies present limitations that limit the generalizability of results (e.g., small sample sizes) (Lavelle et al., 2022), they highlight the need for further research and replication (for example, through a full-scale randomized controlled trial) to further assess the efficacy of ACT-based interventions within the scope of IBD (Romano et al., 2023). To our knowledge, only two Randomized Controlled Trials (RCT) on ACT interventions have been performed in this population. These trials showed improvements in stress (Rowan et al., 2017; Wynne et al., 2019), depression, and general well-being (Wynne et al., 2019) compared to a control group.
Mindfulness-based interventions that aim to promote present-moment awareness and a non-judgmental attitude towards internal experiences have been tested in the context of IBD (Ewais et al., 2019). Mindfulness-Based Stress Reduction (MBSR) interventions have been shown to increase the quality of life (Jedel et al., 2014; Goren et al., 2022) and reduce psychological symptoms (Drent et al., 2016; Goren et al., 2022), fatigue (Goren et al., 2022), and the concentration of C-reactive Protein (CRP) and faecal calprotectin in IBD (Berrill et al., 2014; Gonzalez-Moret et al., 2020).
Compassion-focused therapy addresses aspects such as shame, stigma and self-criticism, which are often reported by people with IBD and influence their psychosocial functioning (Taft et al., 2017; Trindade et al., 2020a). Self-compassion, defined as the sensitivity and the desire to alleviate one’s suffering and the ability to extend kindness and understanding towards the self when facing personal setbacks or inadequacies, has been shown to have a protective effect against psychological distress in IBD (Trindade and Sirois, 2021). The integration of compassion-based components in psychological interventions in this population may thus be beneficial and has been proven effective in other chronic conditions (Brown et al., 2019; Gooding et al., 2020).
Previous studies that tested the efficacy of integrative programs based on self-compassion components, ACT and mindfulness-based in chronic health conditions appear to be feasible and efficacious in improving quality of life, mental health, psychological flexibility, or shame (Skinta et al., 2015; Trindade et al., 2020b). Nonetheless, this kind of integrative interventions have yet to be tested in IBD.
The present RCT tests the acceptability and preliminary efficacy of a face-to-face intervention tailored for IBD patients, the “Living with Intention, Fullness, and Engagement with Inflammatory Bowel Disease” intervention (Trindade et al., 2021), in comparison with a waitlist control condition (“psychological treatment as usual” in Portugal). This study’s main research questions relate to whether the LIFEwithIBD intervention presents acceptability among participants and efficacy in improving psychological distress when compared to the control condition. It is expected that the LIFEwithIBD intervention will be well-accepted by participants and will lead to decreases in anxiety and depression, over the ones that might be reported by the control group.
2 Methods and materials
2.1 Study design
A detailed study protocol with a session-by-session description of the LIFEwithIBD intervention, its implementation, and methodology for the current RCT is available in open access elsewhere (Trindade et al., 2020b). The planning and implementation of this study respected the ethical recommendations by the American Psychological Association and the World Medical Association’s Declaration of Helsinki. Ethical approval was obtained from the Portuguese Data Protection Authority and the Research Ethics Committee of the Coimbra Hospital and University Center (CHUC).
2.2 Participants
2.2.1 Participants’ recruitment and selection
Participants were recruited from June to September 2019 at the Gastroenterology Department of the Centro Hospitalar e Universitário de Coimbra (Coimbra University Hospital). A total of 355 patients were screened by psychologists from the research team through an in-person eligibility interview (Figure 1). Inclusion criteria were: (a) 18 to 65 years old, (b) being able to read and write Portuguese, (c) having an IBD diagnosis for at least 6 months, and (d) being able to give informed consent. Exclusion criteria were: (a) having started a new treatment for IBD in the previous 6 months (in the case of anti-TNF and immunosuppressive therapy) or 2 months (in the case of steroid or aminosalicylate therapy), (b) presenting a diagnosed psychiatric disorder (major depressive disorder, psychotic disorder, bipolar disorder, substance abuse), severe depression, or suicidal ideation (assessed by the Patient Health Questionnaire-9)1, (c) undergoing any other form of psychological intervention, and (d) current pregnancy. Patients who were non-eligible due to exclusion criteria (b) were referred to national mental healthcare services. Please see the RCT’s study protocol for a more detailed presentation of the study’s recruitment and allocation (Trindade et al., 2021).
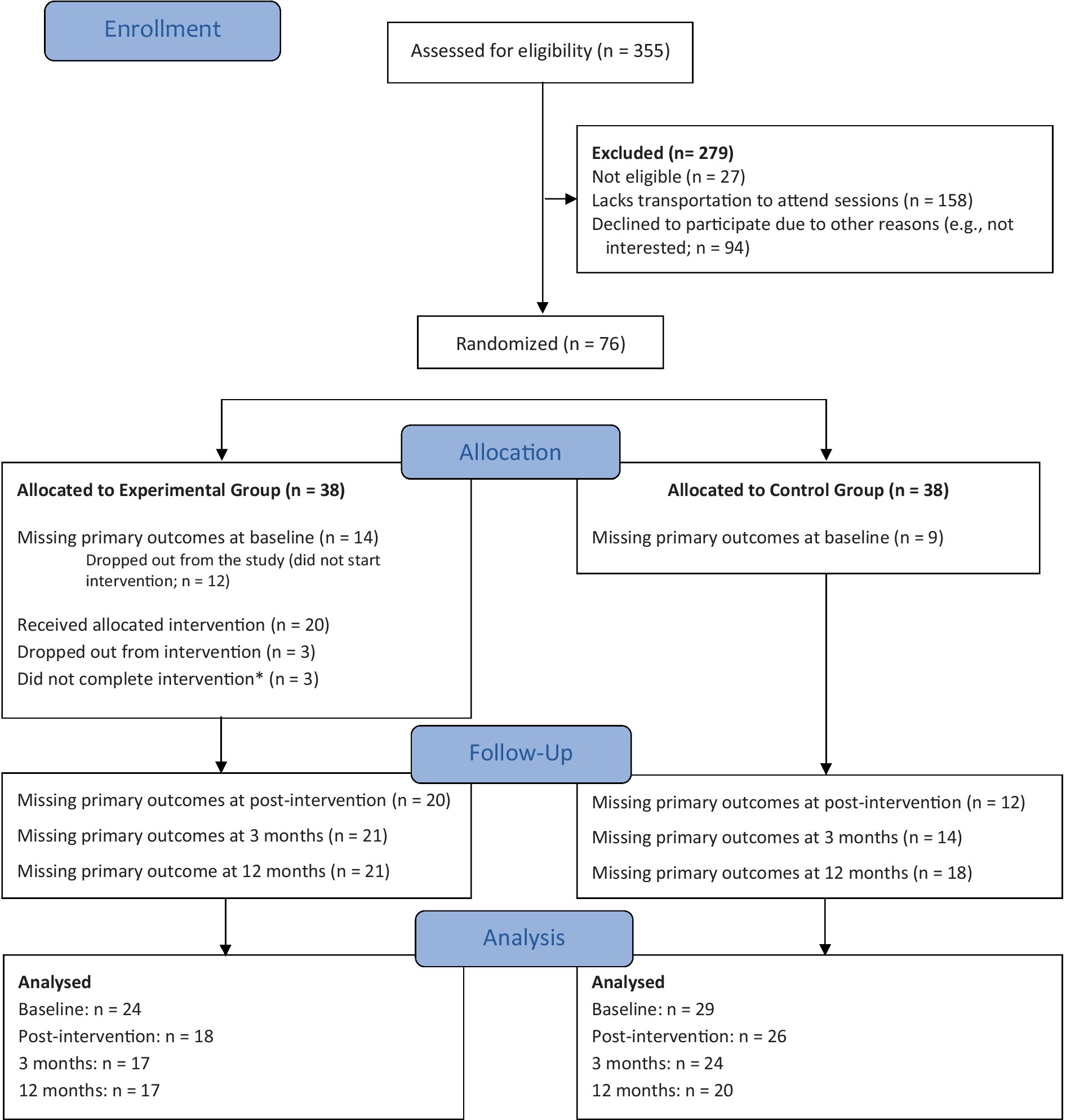
Figure 1. CONSORT flow diagram. *Participants with three consecutive absences or who attended less than two-thirds of the intervention were considered intervention non-completers.
2.2.2 Participants’ description
A total of 76 participants were selected and randomly assigned to one of two conditions: the experimental group (EG; LIFEwithIBD + TAU: n = 38) or the control group (CG; TAU: n = 38) (Figure 1). Before the intervention began for the EG, all participants were contacted by phone. In this process, 23 participants (14 for the EG and 9 for the CG) self-excluded themselves from the study due to a lack of resources to attend the sessions (e.g., lack of time or transportation) or loss of contact.
The sociodemographic and clinical characteristics of the sample are presented in Table 1.
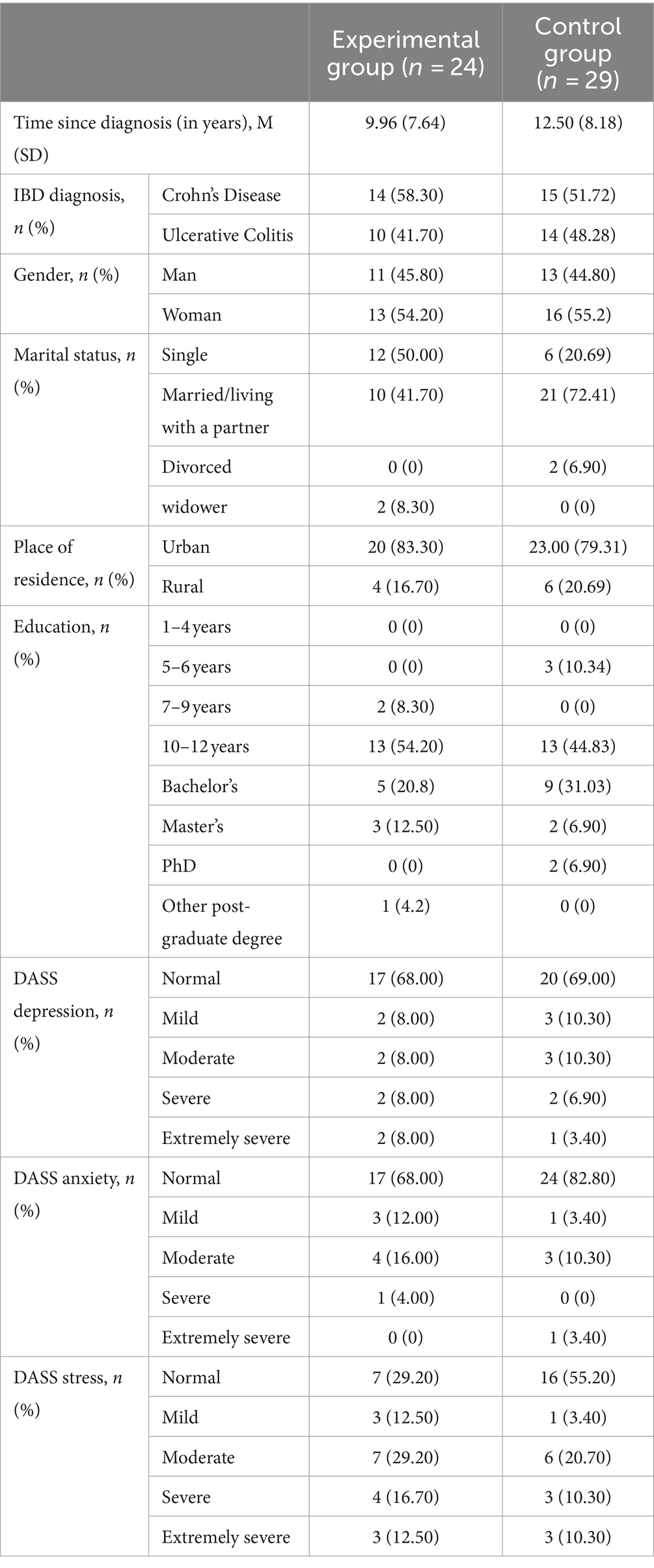
Table 1. Demographic and clinical characteristics of the study groups at baseline.
2.2.3 Measures
Participants completed the following self-reported measures at T0 (baseline), T1 (post-treatment), T2 (3 months follow-up), and T3 (1-year follow-up):
• Primary outcome:
• Psychological distress (DASS-21)
• Secondary outcomes:
- Functional impairment (WSAS).
- General quality of life (EUROHIS-QOL 8-item index).
- Health-related quality of life (IBDQ-UK).
- Chronic illness-related shame (CISS).
- IBD symptom perception (IBD symptoms scale).
- Disease activity: Mayo Score, Harvey-Bradshaw Score.
- Self-Compassion (SCS).
- Psychological flexibility (CompACT).
- Biomarkers complete blood count with erythrocytic indexes, serum albumin, C Reactive Protein (CRP) and faecal calprotectin. Differences of each biomarker were analysed at T0 and T3.
• To assess the intervention’s acceptability, participants in the EG answered a questionnaire post-intervention regarding the following topics:
• Quality of intervention (1 = poor to 10 = excellent);
• Usefulness of intervention (1 = nothing useful to 10 = extremely useful);
• Individual perception of change during and after the intervention - physical symptoms related to IBD, emotion regulation skills, and quality of life (1 = no difference to 10 = much better);
• How do significant others (e.g., family, friends) perceive changes in terms of calmness, kindness, happiness, and emotional stability (1 = much less to 10 = much more);
• Recommendation of the intervention to other people with IBD (yes/no);
• Personal comment or experience about intervention (open response).
Each instrument is described in detail in this RCT’s study protocol (Trindade et al., 2021), which also presents the study’s Recommendations for Interventional Trials (CONSORT) figure.
2.2.4 Data analysis
Descriptive statistics (means, standard deviations, and frequencies) were computed for characterisation purposes and to assess the acceptability of the intervention. The primary outcome was psychological distress (DASS-21 - depression, anxiety, and stress) measured at 9 weeks (immediately after intervention) between the two intervention groups and adjusting for baseline scores using ANCOVA. We examined the ANCOVA’s assumptions through standard tests and residual plots, and no transformations or corrections were required. We then calculated the magnitude of the differences between treatment groups as the standardised mean difference. Between-groups’ differences at post-treatment were examined for the following continuous outcomes: IBD symptom perception (IBDSS); psychological processes (SCS, CompACT); chronic illness-related shame (CISS); work and social adjustment (WSAS); quality of life (EUROHIS-QOL-8, IBDQ-UK), and disease activity (Mayo Score for ulcerative colitis participants; and Harvey-Bradshaw Score for Crohn’s Disease participants). All analyses were conducted using ANCOVA with baseline values as a covariate, and all analyses were intent-to-treat. All analyses were performed using the car packages (Fox et al., 2012) and emmeans (Lenth et al., 2018) in R and GAMLj in Jamovi.
2.2.4.1 Longitudinal outcomes
We used Mixed Models of Repeated Measures (MMRM) to examine for Condition*Time interaction effects on each of the continuous outcomes from baseline, 9 weeks, 3 and 12 months. The Satterthwaite method for degrees of freedom was used for all linear models. We attempted to fit polynomial contrast estimates for the repeated linear, quadratic, and cubic measurements.
2.2.4.2 Exploratory post-hoc analyses
Given the exploratory nature of the pilot study, we persisted with our interrogation of the data even in the absence of statistically significant omnibus main effects or interactions. No correction was made for post-hoc multiple comparisons. To account for the possibility of floor effects due to generally low levels of psychological distress symptoms, we performed additional exploratory analyses of the primary outcomes, excluding participants who did not at least report mild symptoms at T0.
The clinical significance of changes of each participant was analysed by computing the reliable change index (RCI) and considering mixed models of repeated measures.
2.2.4.3 Biomarkers
The results are expressed as the mean ± SEM of the values in each group. Two-way ANOVA followed by Sidak’s multiple comparison test was used to compare faecal calprotectin, CRP, albumin and haematological parameters between T0 and T3. A probability value (p) of less than 0.05 was considered significant. Statistical analysis was performed using GraphPad prism software version 9.0.
2.2.4.4 Data integrity
Please see Supplementary material.
3 Results
3.1 Acceptability assessment
An overview of the acceptability of the LIFEwithIBD intervention is presented in Table 2. In general, most participants from the EG considered the intervention to be of high quality and useful. Participants reported perceived changes in IBD-related physical symptoms, psychological well-being outcomes, and quality of life after the intervention. Also, participants indicated that significant others (e.g., spouse, family, friends) identified positive changes regarding calmness, kindness, and happiness. All participants stated that the LIFEwithIBD intervention had been worthwhile and that they would recommend it to another person with IBD. Some participants left statements about the intervention (Table 3).
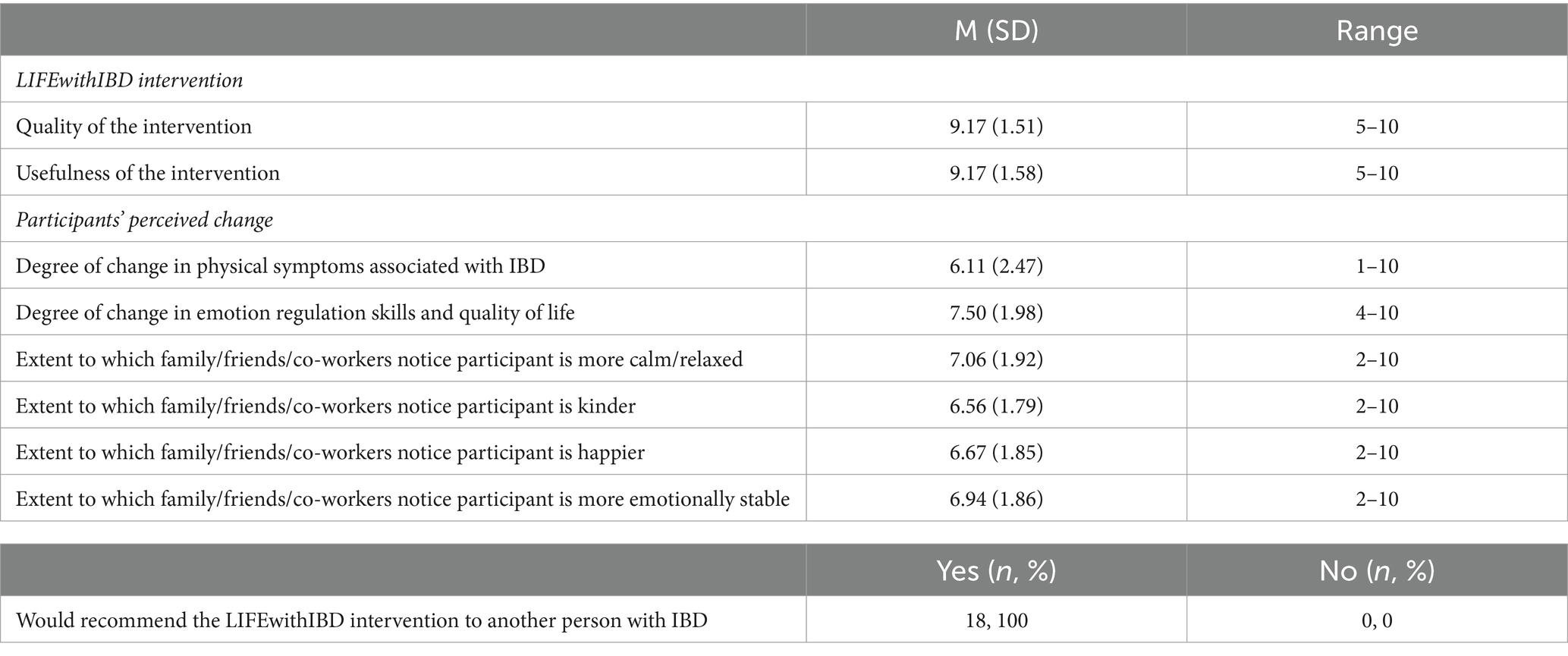
Table 2. Acceptability evaluation of the LIFEwithIBD intervention (experimental group; n = 18).
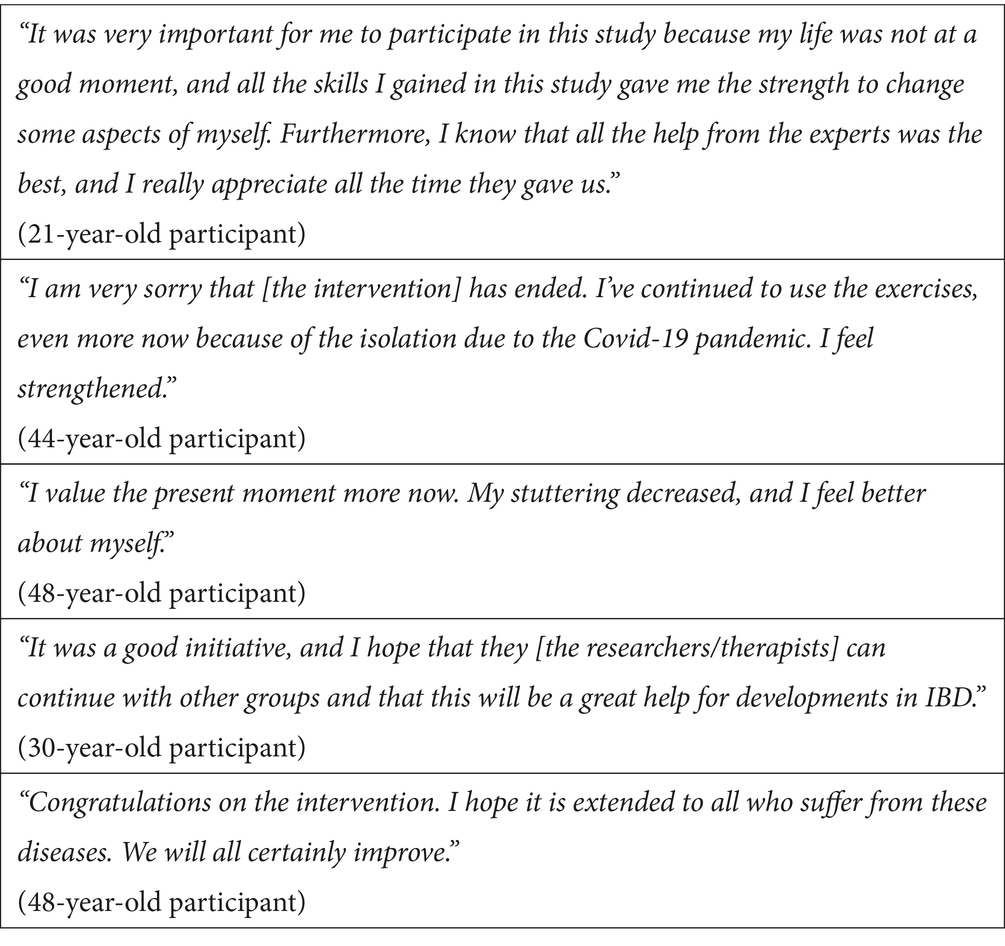
Table 3. Patient statements about the LIFEwithIBD intervention.
3.2 Efficacy assessment
No substantial differences at T0 for any demographic variable were observed, but significant differences between groups for anxiety, self-critical attitude, and psychological flexibility were found (Table 4).
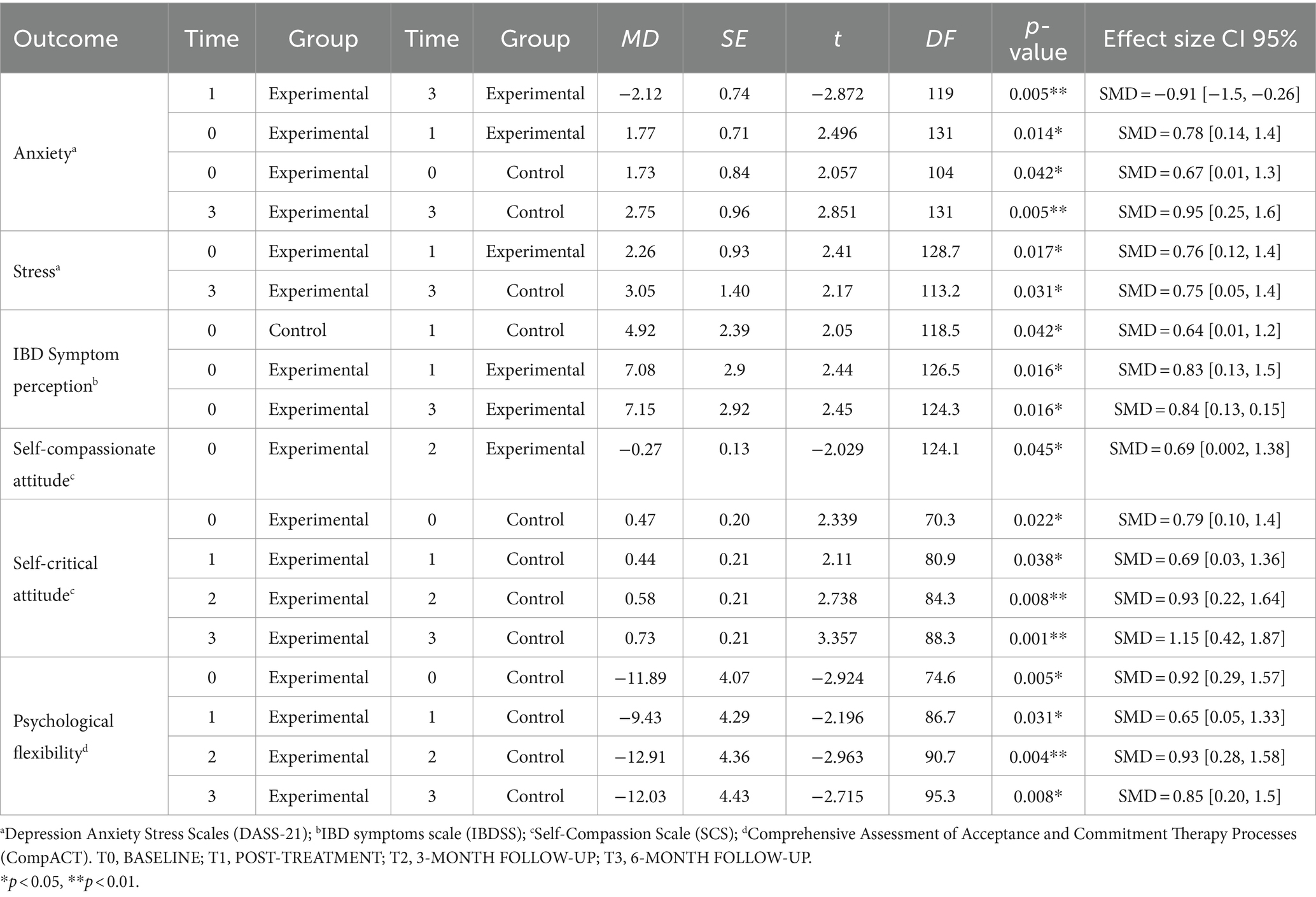
Table 4. Analysis of simple effects.
3.2.1 Primary outcome analyses
We observed no significant differences between groups at T1 on any of the DASS sub-scales after adjusting for T0 symptom scores.
3.2.2 Secondary outcome analyses
In every outcome examined, T0 symptom scores significantly predicted symptom scores at T1 (or T2 for the Harvey-Bradshaw or Mayo score). In contrast, group membership in either experimental or control conditions was almost entirely unrelated to follow-up scores, with the sole exception of the Harvey-Bradshaw score. Once the T2 Harvey-Bradshaw severity was adjusted for baseline values, the EG reported significantly fewer symptoms than the CG (ηp2 = 0.155, p = 0.042; Table 5).
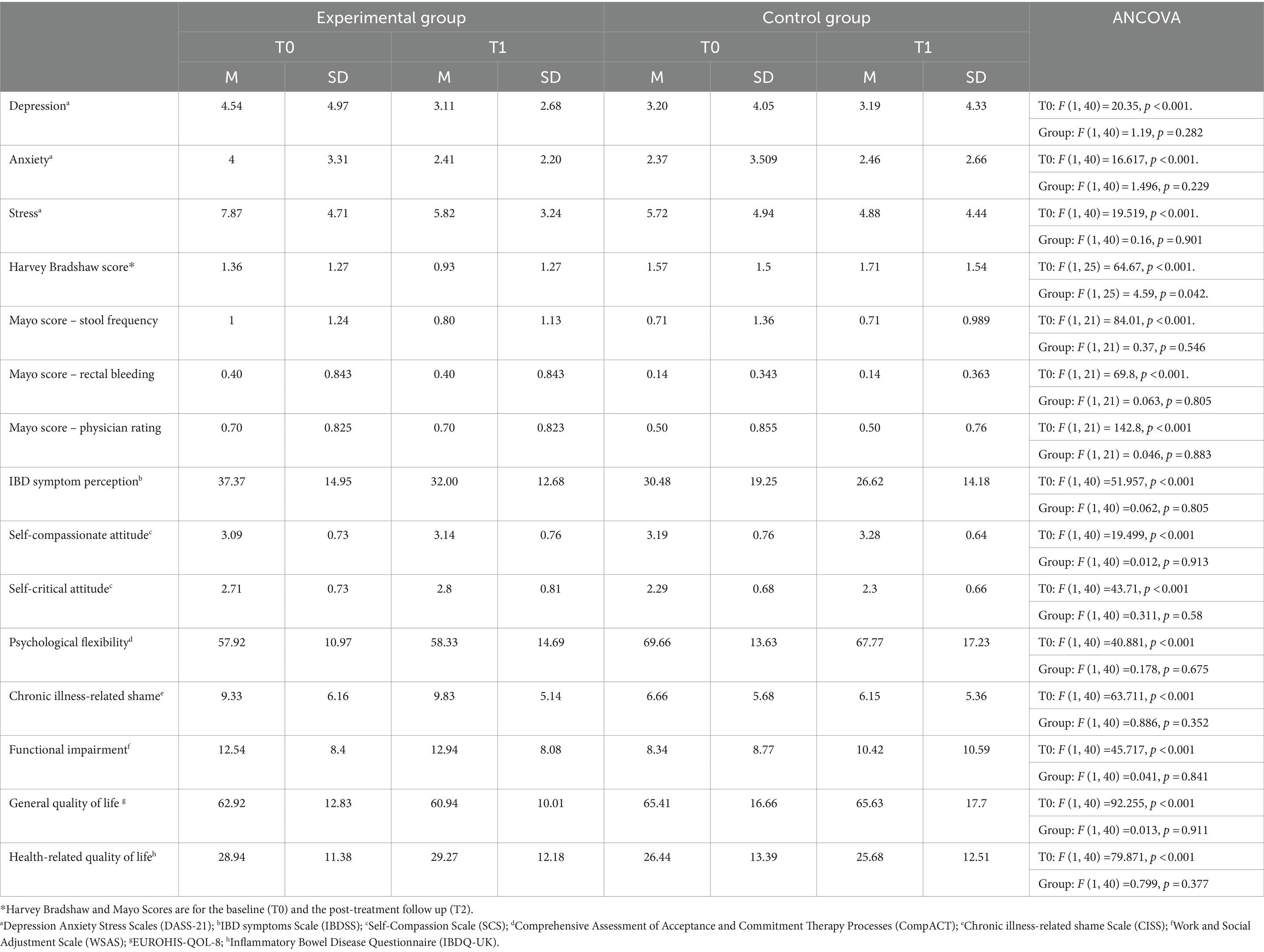
Table 5. Primary and secondary outcome analysis.
We observed negative linear effects of time for stress symptoms and IBD symptom perception that did not differ between the groups and a weak positive quadratic effect of time for self-compassionate attitude. We observed between groups effects for self-critical attitude and psychological flexibility, with the EG reporting a poorer function in both (Table 6).
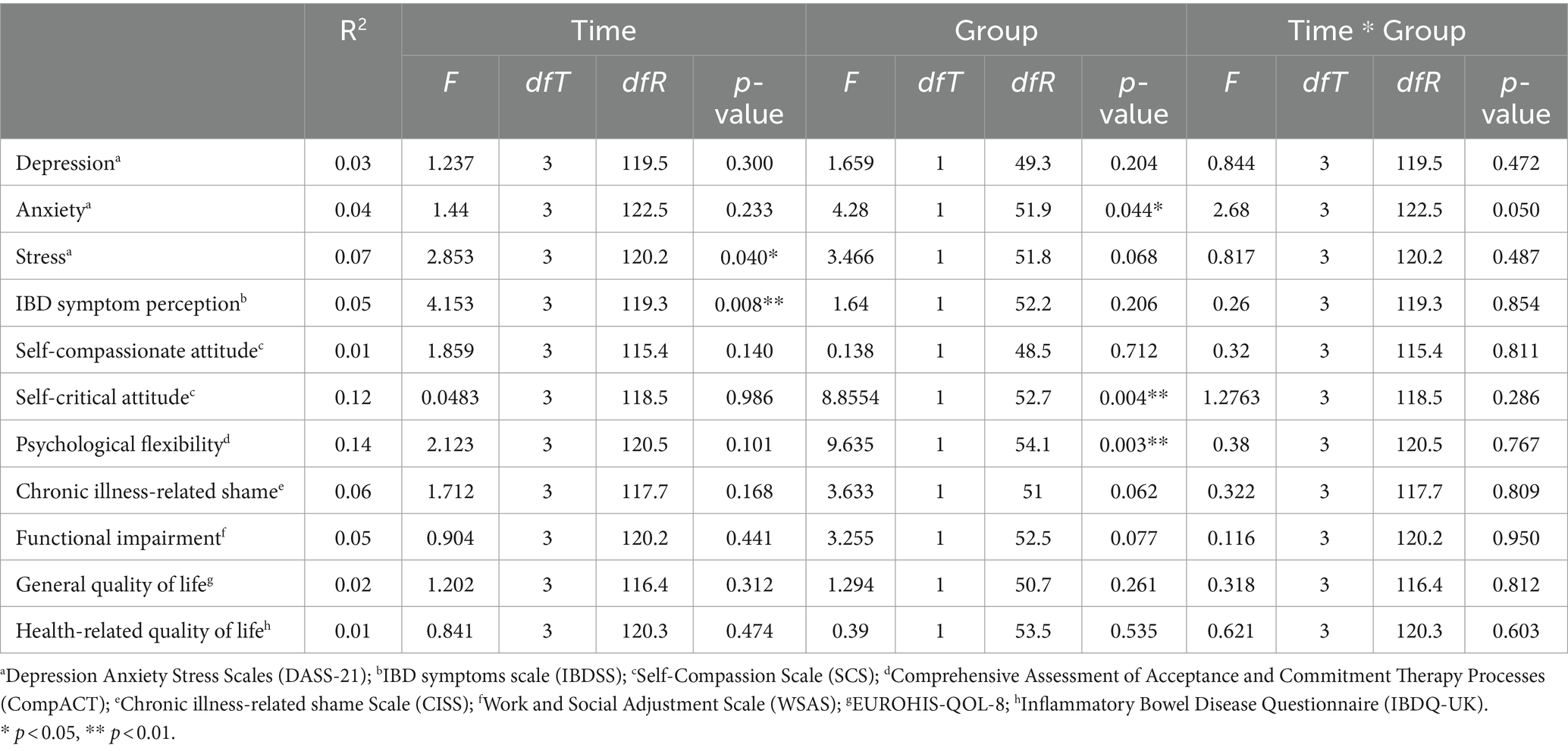
Table 6. Longitudinal analyses—omnibus effects for all outcomes.
Finally, we observed a single time by group quadratic interaction for anxiety symptoms, where the EG demonstrated an improvement from T0 to T1 but then stabilised at baseline levels (Table 7).
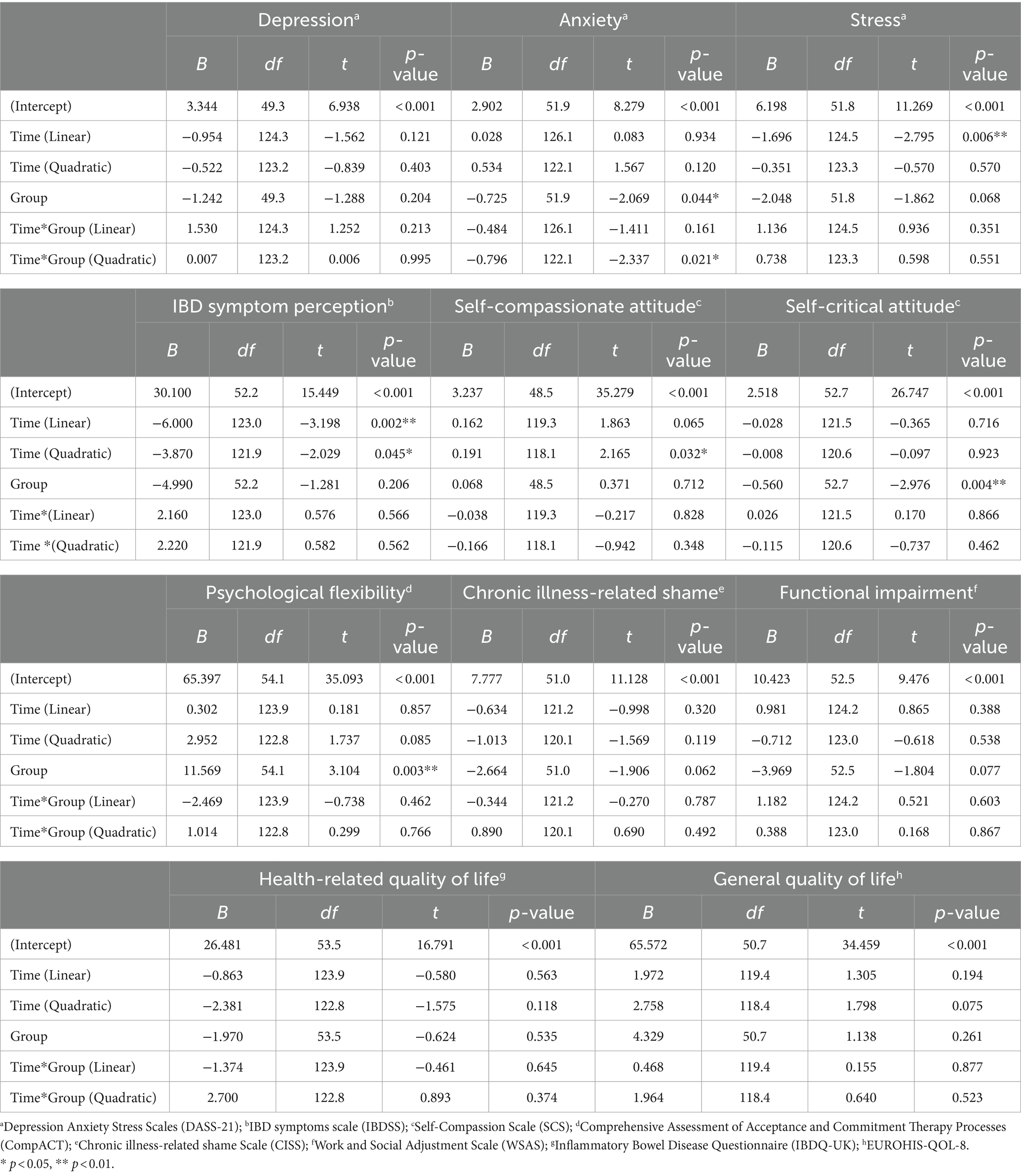
Table 7. Longitudinal outcomes—fixed effects parameters.
3.2.3 Simple effects analyses
From T0 to T1, the EG experienced a reduction in symptoms of anxiety and stress, but this effect did not persist beyond this period (Table 4).
3.2.4 Exploratory factorial ANOVA – DASS-21 severity classification
We observed no between-groups differences in symptoms at T1 after adjusting for T0 symptom scores for depression [F(1,13) = 3.613, p = 0.08, ηp2 = 0.217] or for stress [F(1,4) = 1.65, p = 0.268, ηp2 = 0.292]. However, a significant difference in T1 between-groups anxiety symptoms [F(1,13) = 7.56, p = 0.017, ηp2 = 0.368] was found.
3.2.5 Biomarkers
Regarding the complete blood count, including the erythrogram, leukogram and platelets, no significant alterations were observed between T0 and T3 in both CG and EG. Minor deviations from the reference range, without clinical relevance, were observed for a few patients and are described in detail in the Supplementary Figure S2. Also, no significant differences were observed between T0 and T3 for gender-matched groups from both groups. In the CG, the mean value of albumin significantly increased between T0 and T3 (p = 0.004), whereas in the EG, there was a trend suggesting an increase of serum albumin 1 year after the intervention (T3) but without statistical significance (p = 0.066) (Supplementary Figure S3). No significant differences were observed in serum CRP nor faecal calprotectin between T0 and T3 in either CG or EG (Supplementary Figures S4, S5).
Results from reliable change indices (RCIs) analyses, did not provide evidence of any particular subgroup of participants who managed to obtain clinically significant improvements over time.
4 Discussion
The present study aimed to investigate the acceptability and preliminary efficacy of a face-to-face, group ACT and compassion-based intervention for people with IBD (LIFEwithIBD) through a two-arm RCT. The results for the intervention acceptability were encouraging, as most participants reported a high level of satisfaction with the intervention and considered it useful. Specifically, all participants stated that participating in the intervention was worthwhile and would recommend it to other people with IBD. These results align with the high acceptability presented by previous studies on ACT and compassion-based interventions in chronic illness populations (Trindade et al., 2020b; Dober et al., 2021; Romano et al., 2023). Patients may particularly well accept these third-wave CBT approaches due to their focus on universal psychological processes rather than on symptoms, which may help decrease stigma around the disease and participation in psychotherapy.
No significant differences in depression, anxiety, and stress were found between the EG and the CG. A possible floor effect due to generally low levels of psychological distress at baseline may explain these results [most participants scored below the DASS-21 cut-offs for moderate depression or anxiety (Lovibond, 1995)]. There may not have been enough room for significant improvement, as would have been the case if participants had started at higher levels of psychological distress. From baseline to post-treatment, the EG experienced a significant reduction in symptoms of anxiety and stress, but this effect did not persist during the follow-up periods. This suggests that including booster sessions following the LIFEwithIBD intervention could potentially help maintain the benefits of the intervention. There is evidence that interventions with booster sessions provide better results at follow-up than those without sessions following the main interventional period (Gearing et al., 2013; Wesner et al., 2015). Alternatively, there might also be room for other types of follow-up material like bibliotherapy or online support. In IBS, for example, Ferreira et al. (2018) used an ACT-based self-help manual to support practice in the long-term with positive gains in outcomes obtained from the intervention being sustained at 6 months follow-up.
Moreover, there were no significant differences between groups concerning secondary outcomes (functional impairment, general and health-related quality of life, chronic illness-related shame, IBD symptoms, self-compassion, and psychological flexibility). These unexpected results suggest that the LIFEwithIBD intervention did not influence these outcomes. This, again, may be linked to the low levels of psychological distress at baseline. A significant decrease in stress symptoms and IBD symptom perception was found over time, but there were no differences between groups in this outcome.
The intervention presented effects on disease activity in participants with Crohn’s Disease but not for participants with ulcerative colitis. Participants with Crohn’s Disease from the EG reported significantly lower Harvey-Bradshaw scores at the first follow-up compared to the CG. Only one study using the Harvey-Bradshaw score as an outcome in a psychological intervention trial has found a similar pattern of reduction in symptoms after a CBT and mindfulness-based intervention (Goren et al., 2022).
To determine if the subset of our participants with higher psychological distress particularly benefited from the LIFEwithIBD intervention, we performed a post hoc analysis considering mild to severe DASS-21 scores as contributing factors to the response to the intervention. No between-group differences were observed in depression or stress symptoms at post-treatment after adjusting for baseline symptom scores. A significant difference between groups in anxiety symptoms was observed at post-treatment, with the EG reporting a larger reduction in symptoms than the CG. This result should be interpreted considering two points. First, the LIFEwithIBD intervention does seem effective for reducing psychological distress, but since most participants presented lower levels of distress at baseline, the results did not reach statistical significance. Second, in a post hoc analysis, limiting the sample size reduces the statistical power, and only the largest effect sizes are detected. Regarding primary outcomes, depression is near to reaching statistical significance (p = 0.08). Further investigation is needed regarding the use of this intervention, particularly in patients who are likely to experience comorbid psychological distress.
In addition to the psychological self-reported evaluation, inflammatory biomarkers were assessed. The serum albumin results were unsurprising since this plasma protein tends to decrease quickly in severely ill patients. All participants in this study were under clinical remission, and, as expected, serum albumin remained within the reference interval in all participants from CG and EG, both at baseline and T3. The same rationale holds true for CRP and faecal calprotectin. Our results showed no significant differences regarding both biomarkers between the CG and EG at T3. Similarly, no differences were observed in the total blood count of participants. These results suggest that, from a bioanalytical point of view, disease activity in our sample remained under control throughout the study. The question remains as to whether the LIFEwithIBD intervention could have an impact on gut microbiota phenotype. Indeed, it would be interesting to characterize the gut microbiota of these patients before and after the intervention to ascertain if the modulation of the microbiota-gut-brain axis could be the mechanism underlying the impact of the treatment on psychological (dis)tress herein observed since similar reports have been made regarding IBS (Halkjær et al., 2018).
Overall, these findings need to be interpreted considering several limitations. Due to this study’s relatively small sample size, further studies are required to test the efficacy of the LIFEwithIBD intervention in larger samples. Similarly to previous RCTs testing group interventions in the IBD context (Mikocka-Walus et al., 2017; Wynne et al., 2019), the study showed a considerable attrition rate. This may be due to the time commitment needed to participate in the intervention, combined with the simultaneous management of different life contexts, the lack of monetary compensation for participating in the study, and the lack of transportation to attend the intervention (most screened patients lived outside Coimbra, in the suburbs or in other cities in Portugal). Furthermore, the stigma associated with mental health still present in Portuguese society, which is regarded as one of the main barriers to access to psychological treatment in Portugal (Palha and Palha, 2016), may have also contributed to the study’s limited enrolment rate. Participants from both groups did not indeed present levels of psychological distress, which might have reduced the sensitivity to changes in the outcome measures. This is suggestive that including patients with higher psychological distress (rather than this being an exclusion criterion, such as in the present study) could be of interest in future studies testing the LIFEwithIBD intervention. Another limitation of this study was the use of self-report questionnaires. Although the efficacy of psychological interventions is often assessed through self-assessment, critics believe that the evaluation and interpretation of treatment efficacy can be impaired by the occurrence of a “response shift,” which could contaminate (reduce or amplify) treatment effects. Also, our findings revealed minor changes in anxiety and stress symptoms that may be interpreted as collateral, since the purpose of ACT, mindfulness and self-compassion-based therapies is to improve quality of life, which in our study was considered a secondary outcome which did not show any change. Furthermore, self-report measures that are not very close to each person’s reality may compromise the results, as these measures may not be sensitive to change. For example, in a study conducted in a sample of patients with fibromyalgia, it was found that the most sensitive instrument to the effects of the intervention was the self-report of longitudinal experiences based on questions about the participants’ daily lives in several weeks before and after of the intervention (de la Coba et al., 2022). Further studies should integrate qualitative methods to complement the assessment of intervention efficacy. Finally, although the EG and CG presented similar demographic characteristics, they presented differences in important outcomes at baseline (EG presented a higher level of self-critical attitude and lower levels of psychological flexibility, which may have influenced results). Furthermore, it is important to consider the circumstances under which the study’s assessments occurred. The post-treatment assessment and the second follow-up coincided with two periods of lockdown in Portugal due to the COVID-19 pandemic. It is difficult to hypothesize their possible effects on this study, as studies show that the effects of lockdown periods on mental health are not the same for each individual (Prati and Mancini, 2021).
Despite these limitations, this is the first study to investigate the preliminary efficacy of psychological and disease outcomes and biomarkers of an integrative face-to-face ACT and compassion-based intervention in the context of IBD. Preliminary findings suggest that the LIFEwithIBD intervention may be better suited for IBD patients presenting with high levels of psychological distress. Given that these patients are more likely to self-exclude from these interventions, future studies should address ways of engaging these patients. One possibility would be the use of non-face-to-face approaches such as online interventions. Further research is needed to reach more comprehensive conclusions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by Ethics Committee of the Coimbra University Hospital (CHUC). It was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CF: Conceptualization, Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft. JP: Data curation, Investigation, Methodology, Resources, Writing – original draft. DS: Conceptualization, Formal analysis, Writing – original draft. SO: Data curation, Investigation, Methodology, Resources, Writing – review & editing. AG: Investigation, Writing – review & editing. NF: Conceptualization, Validation, Writing – review & editing. PL-S: Writing – review & editing. SC: Validation, Writing – review & editing. IM-P: Data curation, Investigation, Writing – review & editing. BR: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. FP: Conceptualization, Investigation, Methodology, Resources, Validation, Writing – review & editing. IT: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This project was peer-reviewed in the context of the 2017 R&D projects grant call of the Portuguese Foundation for Science and Technology (Fundação para a Ciência e Tecnologia), having successfully been granted funding (Grant no. PTDC/PSI-ESP/28602/2017).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2024.1367913/full#supplementary-material
References
Barberio, B., Zamani, M., Black, C. J., Savarino, E. V., and Ford, A. C. (2021). Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 6, 359–370. doi: 10.1016/s2468-1253(21)00014-5
Berrill, J. W., Sadlier, M., Hood, K., and Green, J. T. (2014). Mindfulness-based therapy for inflammatory bowel disease patients with functional abdominal symptoms or high perceived stress levels. J. Crohn's Colitis 8, 945–955. doi: 10.1016/j.crohns.2014.01.018
Brown, L., Karmakar, C., Flynn, M., Motin, M. A., Palaniswami, M., Celano, C. M., et al. (2019). A self-compassion group intervention for patients living with chronic medical illness: treatment development and feasibility study. The primary care companion for CNS disorders. 21:23193. doi: 10.4088/pcc.19m02470
de la Coba, P., Rodríguez-Valverde, M., and Hernández-López, M. (2022). Online act intervention for fibromyalgia: an exploratory study of feasibility and preliminary effectiveness with smartphone-delivered experiential sampling assessment. Internet Interv. 29:100561. doi: 10.1016/j.invent.2022.100561
Dober, M., Mikocka-Walus, A., Evans, S., Beswick, L., Emerson, C., and Olive, L. (2021). Perspectives on an acceptance and commitment therapy (ACT) based program for patients with inflammatory bowel disease and comorbid anxiety and/or depressive symptoms. Psychother. Res. 31, 668–681. doi: 10.1080/10503307.2020.1813915
Drent, G., Kuiken, M., Mooibroek, J., Dijkstra, G., and Schroevers, M. (2016). The beneficial effects of mindfulness training on fatigue and psychosocial functioning in patients with inflammatory bowel disease and irritable bowel syndrome: a pilot study. J. Crohn's Colitis 10, S493.1–S4S493. doi: 10.1093/ecco-jcc/jjw019.875
Ewais, T., Begun, J., Kenny, M., Rickett, K., Hay, K., Ajilchi, B., et al. (2019). A systematic review and meta-analysis of mindfulness based interventions and yoga in inflammatory bowel disease. J. Psychosom. Res. 116, 44–53. doi: 10.1016/j.jpsychores.2018.11.010
Ferreira, N. B., Gillanders, D., Morris, P. G., and Eugenicos, M. (2018). Pilot study of acceptance and commitment therapy for irritable bowel syndrome: a preliminary analysis of treatment outcomes and processes of change. Clin. Psychol. 22, 241–250. doi: 10.1111/cp.12123
Fox, J., Weisberg, S., Adler, D., Bates, D., Baud-Bovy, G., Ellison, S., et al. (2012). Package ‘car’. Vienna: R Foundation for Statistical Computing.
Gearing, R. E., Schwalbe, C. S., Lee, R., and Hoagwood, K. E. (2013). The effectiveness of booster sessions in CBT treatment for child and adolescent mood and anxiety disorders. Depress. Anxiety 30, 800–808. doi: 10.1002/da.22118
Gonzalez-Moret, R., Cebolla, A., Cortes, X., Banos, R. M., Navarrete, J., de la Rubia, J. E., et al. (2020). The effect of a mindfulness-based therapy on different biomarkers among patients with inflammatory bowel disease: a randomised controlled trial. Sci. Rep. 10:6071. doi: 10.1038/s41598-020-63168-4
Gooding, H., Stedmon, J., and Crix, D. (2020). ‘All these things don’t take the pain away but they do help you to accept it’: making the case for compassion-focused therapy in the management of persistent pain. Br. J. Pain 14, 31–41. doi: 10.1177/2049463719857099
Goren, G., Schwartz, D., Friger, M., Banai, H., Sergienko, R., Regev, S., et al. (2022). Randomized controlled trial of cognitive-behavioral and mindfulness-based stress reduction on the quality of life of patients with Crohn disease. Inflamm. Bowel Dis. 28, 393–408. doi: 10.1093/ibd/izab083
Graham, C. D., Gouick, J., Krahé, C., and Gillanders, D. (2016). A systematic review of the use of acceptance and commitment therapy (ACT) in chronic disease and long-term conditions. Clin. Psychol. Rev. 46, 46–58. doi: 10.1016/j.cpr.2016.04.009
Halkjær, S. I., Christensen, A. H., Lo, B. Z. S., Browne, P. D., Günther, S., Hansen, L. H., et al. (2018). Faecal microbiota transplantation alters gut microbiota in patients with irritable bowel syndrome: results from a randomised, double-blind placebo-controlled study. Gut 67, 2107–2115. doi: 10.1136/gutjnl-2018-316434
Hayes, S. C., Strosahl, K. D., and Wilson, K. G. (2011). Acceptance and commitment therapy: The process and practice of mindful change. New York: Guilford press.
Jedel, S., Hoffman, A., Merriman, P., Swanson, B., Voigt, R., Rajan, K., et al. (2014). A randomized controlled trial of mindfulness-based stress reduction to prevent flare-up in patients with inactive ulcerative colitis. Digestion 89, 142–155. doi: 10.1159/000356316
Keefer, L., and Kane, S. V. (2017). Considering the bidirectional pathways between depression and IBD: recommendations for comprehensive IBD care. Gastroenterol Hepatol (N Y) 13, 164–169
Knowles, S. R., Keefer, L., Wilding, H., Hewitt, C., Graff, L. A., and Mikocka-Walus, A. (2018). Quality of life in inflammatory bowel disease: a systematic review and meta-analyses—part II. Inflamm. Bowel Dis. 24, 966–976. doi: 10.1093/ibd/izy015
Lavelle, J., Storan, D., Eswara Murthy, V., De Dominicis, N., Mulcahy, H. E., and McHugh, L. (2022). Brief and telehealth acceptance and commitment therapy (ACT) interventions for stress in inflammatory bowel disease (IBD): a series of single case experimental design (SCED) studies. J. Clin. Med. 11:2757. doi: 10.3390/jcm11102757
Lenth, R., Singmann, H., Love, J., Buerkner, P., and Herve, M. (2018). Emmeans: estimated marginal means, aka least-squares means. R package version 1.1.3.
Lovibond, S. H. (1995). Manual for the depression anxiety stress scales. Sydney: Sydney Psychology Foundation.
Mikocka-Walus, A., Bampton, P., Hetzel, D., Hughes, P., Esterman, A., and Andrews, J. M. (2017). Cognitive-behavioural therapy for inflammatory bowel disease: 24-month data from a randomised controlled trial. Int. J. Behav. Med. 24, 127–135. doi: 10.1007/s12529-016-9580-9
Palha, J., and Palha, F. (2016). Perspetiva sobre a Saúde mental em Portugal: perspective on mental health in Portugal. Gazeta Médica,
Paulides, E., Boukema, I., Van Der Woude, C. J., and De Boer, N. K. (2021). The effect of psychotherapy on quality of life in IBD patients: a systematic review. Inflamm. Bowel Dis. 27, 711–724. doi: 10.1093/ibd/izaa144
Prati, G., and Mancini, A. D. (2021). The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 51, 201–211. doi: 10.1017/s0033291721000015
Romano, D., Chesterman, S., Fuller-Tyszkiewicz, M., Evans, S., Dober, M., Gearry, R., et al. (2023). Feasibility, acceptability, and preliminary efficacy of acceptance commitment therapy for adults living with inflammatory bowel disease and distress. Inflamm. Bowel Dis. doi: 10.1093/ibd/izad122
Rowan, C. R., Wynne, B., McHugh, L., Keegan, D., Byrne, K., Hartery, K., et al. (2017). A randomised controlled trial of acceptance and commitment therapy (ACT) for the treatment of stress in inflammatory bowel disease. Gastroenterology 152:S138. doi: 10.1016/S0016-5085(17)30793-X
Skinta, M. D., Lezama, M., Wells, G., and Dilley, J. W. (2015). Acceptance and compassion-based group therapy to reduce HIV stigma. Cogn. Behav. Pract. 22, 481–490. doi: 10.1016/j.cbpra.2014.05.006
Taché, Y., and Bernstein, C. N. (2009). Evidence for the role of the brain–gut axis in inflammatory bowel disease: depression as cause and effect? Gastroenterology 136, 2058–2061. doi: 10.1053/j.gastro.2009.04.032
Taft, T., Bedell, A., Naftaly, J., and Keefer, L. (2017). Stigmatization toward irritable bowel syndrome and inflammatory bowel disease in an online cohort. Neurogastroenterol Motil 29:e12921. doi: 10.1111/nmo.12921
Trindade, I. A., Ferreira, C., and Pinto-Gouveia, J. (2018). The longitudinal effects of emotion regulation on physical and psychological health: a latent growth analysis exploring the role of cognitive fusion in inflammatory bowel disease. Br. J. Health Psychol. 23, 171–185. doi: 10.1111/bjhp.12280
Trindade, I. A., Ferreira, C., and Pinto-Gouveia, J. (2020a). Shame and emotion regulation in inflammatory bowel disease: effects on psychosocial functioning. J. Health Psychol. 25, 511–521. doi: 10.1177/1359105317718925
Trindade, I. A., Ferreira, C., and Pinto-Gouveia, J. (2020b). Acceptability and preliminary test of efficacy of the mind programme in women with breast cancer: an acceptance, mindfulness, and compassion-based intervention. J. Contextual Behav. Sci. 15, 162–171. doi: 10.1016/j.jcbs.2019.12.005
Trindade, I. A., Pereira, J., Galhardo, A., Ferreira, N. B., Lucena-Santos, P., Carvalho, S. A., et al. (2021). The LIFEwithIBD intervention: study protocol for a randomized controlled trial of a face-to-face acceptance and commitment therapy and compassion-based intervention tailored to people with inflammatory bowel disease. Front Psychiatry 12:699367. doi: 10.3389/fpsyt.2021.699367
Trindade, I. A., and Sirois, F. M. (2021). The prospective effects of self-compassion on depressive symptoms, anxiety, and stress: a study in inflammatory bowel disease. J. Psychosom. Res. 146:110429. doi: 10.1016/j.jpsychores.2021.110429
Wesner, A. C., Gomes, J. B., Detzel, T., Guimarães, L. S., and Heldt, E. (2015). Booster sessions after cognitive-behavioural group therapy for panic disorder: impact on resilience, coping, and quality of life. Behav. Cogn. Psychother. 43, 513–525. doi: 10.1017/s1352465814000289
Keywords: Acceptance and Commitment Therapy, compassion, inflammatory bowel disease, mindfulness, randomized controlled trial
Citation: Ferreira C, Pereira J, Skvarc D, Oliveira S, Galhardo A, Ferreira NB, Lucena-Santos P, Carvalho SA, Matos-Pina I, Rocha BS, Portela F and Trindade IA (2024) Randomized controlled trial of an Acceptance and Commitment Therapy and compassion-based group intervention for persons with inflammatory bowel disease: the LIFEwithIBD intervention. Front. Psychol. 15:1367913. doi: 10.3389/fpsyg.2024.1367913
Edited by:
Carmen María Galvez-Sánchez, University of Jaén, SpainReviewed by:
De-La-Coba Pablo, University of Extremadura, SpainFátima Franco Servián, Valencian International University, Spain
Copyright © 2024 Ferreira, Pereira, Skvarc, Oliveira, Galhardo, Ferreira, Lucena-Santos, Carvalho, Matos-Pina, Rocha, Portela and Trindade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cláudia Ferreira, claudiaferreira@fpce.uc.pt; Inês A. Trindade, ines.trindade@oru.se
†These authors share first authorship