 Åsa Svensson
Åsa Svensson Maria Warne1
Maria Warne1- 1Department of Health Sciences, Mid Sweden University, Östersund, Sweden
- 2Department of Health Sciences, Mid Sweden University, Sundsvall, Sweden
Objectives: To describe the intake of energy drinks (EDs) among a sample of Swedish adolescents while considering health-related variables, and to investigate the longitudinal associations between ED consumption, health, and norm-breaking behavior. Longitudinal studies on this topic are scarce.
Methods: Questionnaire data were collected in the northern part of Sweden in 2010–2011 from 1,622 adolescents in grades 6–9. Analyses were performed using a chi-squared test and logistic regression.
Results: Seventy-four percent of the boys and 54% of the girls had consumed EDs (P < 0.001). ED consumption was associated with variables related to low health, low support levels, and norm-breaking behavior. The associations were generally stronger among the girls and the boys who consumed EDs at least once a week. ED consumption was a predictor of worse health and norm-breaking behavior 1 year later. Adjusted odds ratios ranged from 1.53 (95% CI: 1.07, 2.20; school-related stress) to 4.88 (95% CI: 2.28, 10.43; gaming-related truancy).
Conclusions: Health promotion activities benefit from a broad approach but could focus on girls who consume EDs and those boys with the highest consumption levels.
Introduction
There is no evidence that limited consumption of energy drinks (EDs) is harmful, and the associated health risks are mostly related to the caffeine content (1). However, there have been reports of intoxication from excessive ED consumption (2, 3). It has been found that EDs put stress on the cardiovascular and neurological systems, which can cause arrhythmias and seizures (2, 4). In several cases, cardiovascular events have occurred as a result of ED intake in combination with alcohol or illicit drugs (3). Adolescents have reported adverse events after ED consumption, such as headache and sleeping problems (5, 6).
EDs can be described as soft drinks that contain sweeteners (whether they be sugar or artificial), caffeine, taurine, d-glucuronolactone, and B-vitamins (7, 8). Examples of other ingredients include guarana, ginseng, carnitine, creatine, gingko biloba, and different vitamins (8). The caffeine content varies, but it can be up to 400 mg/L (8). In Sweden, a can of ED usually contains 250 ml of liquid and 320 mg caffeine per liter, that is, the same amount of caffeine as a cup of coffee (7). Caffeine is a stimulant that acts on the central nervous system. Caffeine intake >400 mg could cause caffeine intoxication with serious negative health effects, especially among subgroups with cardiac or psychiatric conditions (9). However, limited amounts of caffeine are generally considered harmless, even for children and adolescents who have lower body mass and less tolerance (9).
Nevertheless, consumers of EDs have reported more adverse events compared to consumers of coffee (5). The pharmacological properties of the various herbal supplements in EDs and the possible interactions between the different agents are not fully known, and there could also be harmful effects of EDs that are not related to the caffeine content (2, 4, 9). Dietary habits in childhood and adolescence often carry forward into adulthood (10). Fortunately, health inequalities later in life can be counteracted by working to ensure that children eat healthy diets.
Adolescents' consumption of EDs is of concern not only because of the potential negative health effects of the ingredients, but also because of the associations with health risk behaviors and worse health. Associations have been found between the consumption of EDs and substance use (e.g., alcohol, cigarettes, or marijuana) (11), the use of illicit drugs (12), the consumption of other high-sugar beverages (13), and less hours of sleep (14) or late bedtime (6). One review in particular found that ED consumption was associated with mental health problems such as stress, anxiety, and depression among a majority of those included in the relevant studies (15). However, it should be noted that most of the included studies in this work used cross-sectional data, and the review itself considered null findings as well (15). Nevertheless, ED consumption among teens has also been associated with a higher body mass index (BMI) (13).
Adolescence is a time during which young individuals experience both physical and mental changes. Ultimately, during adolescence, they test the limits of what behavior is accepted in the context in which they live. This explains why breaking societal norms is most common among adolescents, and why it can be seen as a natural part of maturity (16). On the other hand, breaking societal norms has been associated with certain health problems (17) along with lower school achievement (18). Norm-breaking behavior has been described as behavior related to the use of alcohol and/or illicit drugs (19), issues with school adjustment (18), or the committing of crimes (17). In their study on students between the years of 7–9 in compulsory school, Nygren et al. (17) included questions about patterns of behavior involving breakfast, tobacco, alcohol, drugs, crime (e.g., carrying a knife as weapon), bullying, and truancy. In line with this approach, our study defined norm-breaking behavior as the transgression of laws (specifically those pertaining to tobacco, alcohol, and drug use as well as truancy) or health risk behaviors (not eating breakfast or lunch every school day).
There is a need for more studies examining the associations between ED consumption and other health and behavioral outcomes; it is also critical that the directions of the associations be considered as well. Previous studies on adolescents' ED consumption and the association with health and health-related behaviors have mainly used cross-sectional data, and thus there is a lack of longitudinal studies that have been conducted in a Scandinavian setting.
The objectives of this study were to describe the intake of EDs among a sample of Swedish adolescents in relation to their social backgrounds, levels of support, health and norm-breaking behaviors, and to investigate the longitudinal associations of ED consumption with respect to health and norm-breaking behavior.
Methods
Setting and Participants
The study was based on data collected between 2010 and 2011 for the project on “Youth Health Development.” This particular project was conducted in a medium-sized municipality with ~59,000 inhabitants in the northern part of Sweden. The overall aim of the project was to explore factors relevant to mental health among the youth, and to develop methods for school health promotion. The data in the present study comes from a questionnaire distributed in January of 2010 and 2011. All public and independent schools in the municipality with junior high school students (aged 12–16 years through grades 6–9) were invited to participate. One of the four independent schools and all nine of the public schools accepted the invitation. Parents and students received an informational letter articulating the voluntary nature of the study. Parents could actively decline the participation of their children. The study was reviewed and approved by Regional Ethical Review Board in Umeå, Sweden (Dnr: 09-179M).
The electronic questionnaire was built with Easy Research software and distributed to the students via their school e-mail accounts; each student received their own unique identification information. The students completed the questionnaire during school hours in a computer room. They were informed that they could decline participation at any time. The targeted resources were administered such that at least one member of the school staff could be present to make sure that all students were able to complete the questionnaire without being disturbed by others. A total of 1,622 adolescents participated in 2010, including 828 (51%) girls and 794 (49%) boys. The response rate was 77.3%. In 2011, 982 of these adolescents participated, including 530 (54%) girls and 452 (46%) boys. Grades 6–9 were evenly represented in the data.
Measurements
Consumption frequencies of EDs was the dependent variable. The central question was as follows:
“How often do you drink EDs (e.g., Red Bull, Monster, Burn, Power King, and other similar beverages)?” The six response alternatives were: (1) “I don't drink EDs”; (2) “every day”; (3) “several times per week”; (4) “at least once a week, but not every day”; (5) “less than once a week”; and (6) “seldom.”
The independent variables included in the present study were chosen based on previous research on the associations between ED consumption and health-related behavior. We grouped the variables into the categories of social background, levels of support, health conditions, and participation in norm-breaking behavior. The included variables are described in Table 1.
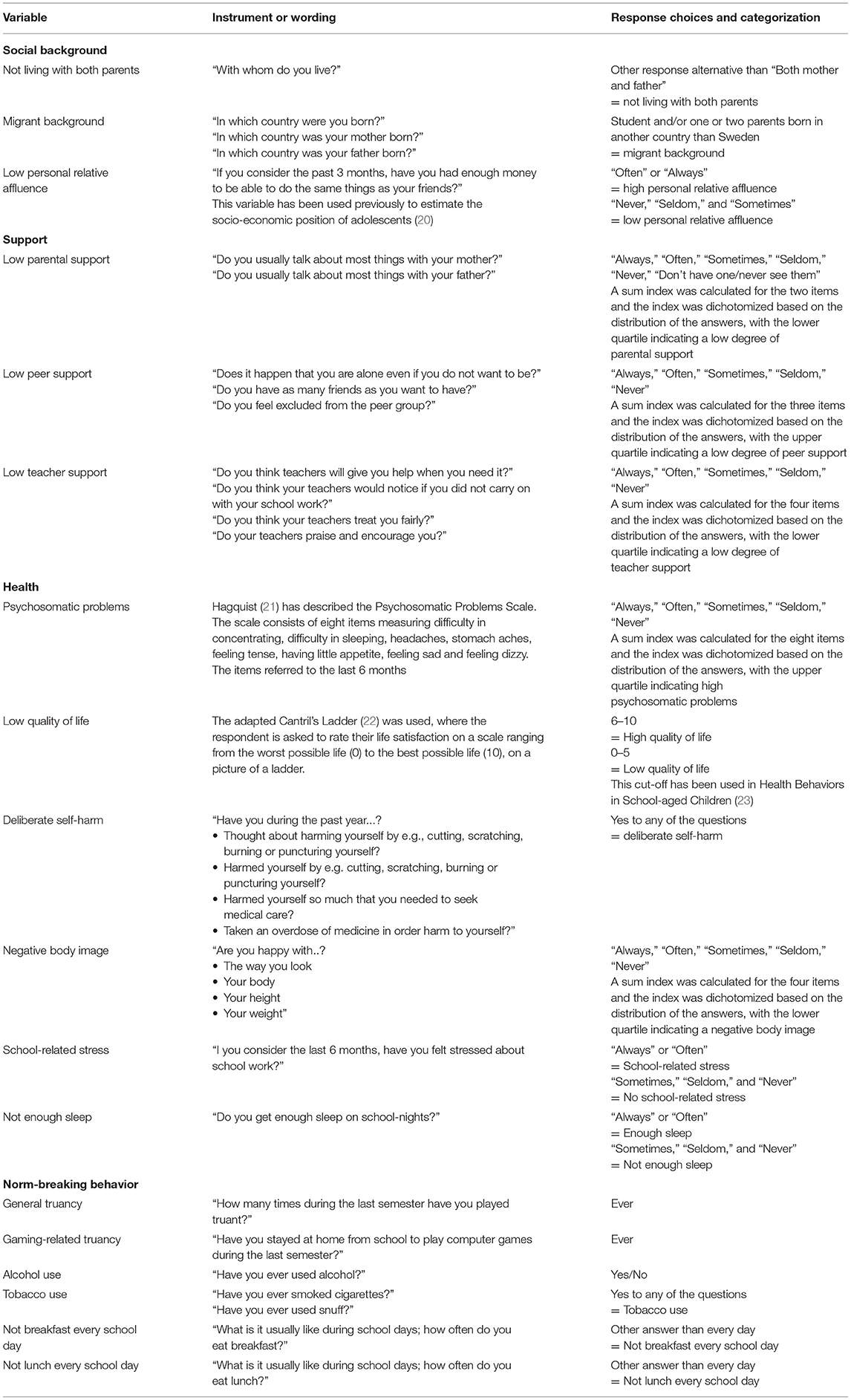
Table 1. Overview of the included variables.
Statistical Analysis
Statistical analysis was performed with IBM SPSS Statistics version 22, and p ≤ 0.05 were considered significant. For the cross-sectional analyses, data from 2010 was used. Descriptive data was presented as frequencies and percentage proportions. In order to investigate the cross-sectional associations between consumption of EDs (“never” vs. “ever,” and, in an additional analysis for boys, “never” vs. “once a week or more”) and social background, levels of support, health conditions, and participation in norm-breaking behavior, Pearson's chi-squared test was used. Longitudinal analyses were conducted for data collected in 2010 and 2011 using logistic regression models for both the entire sample and separately for boys and girls. The following example explains the procedure of the longitudinal analysis: We investigated alcohol consumption (“never” vs. “ever”) in 2011 as a function of ED consumption (“never” vs. “ever”) at the baseline in 2010 for the sub-sample who had not consumed alcohol. Additionally, models were performed following the same rationale but with the variables reversed, i.e., ED consumption in 2011 was investigated as a function of alcohol consumed at the baseline for the sub-sample that had not consumed EDs. This method has been used previously (24). Logistic regression models were similarly conducted to investigate the longitudinal associations between ED consumption and the presence of: (1) significant psychosomatic problems, low quality of life, deliberate self-harm, negative body image, school-related stress, insufficient sleep, general truancy, gaming-related truancy, tobacco use, not eating breakfast every school day, and not eating lunch every school day. The categorization of response alternatives are described in more detail in Table 1. Grade (6, 7, 8, or 9) and personal relative affluence (low vs. other) were included as covariates. For boys, additional analyses were conducted in a similar way albeit with a variable ED consumption of once a week or more since we wanted to investigate the boys with the highest levels of consumption. Few girls consumed EDs, and therefore “ever” represented the girls with the highest levels of consumption. Logistic regression models with variable categories and n < 10 are not presented.
Results
Descriptive Statistics
Self-reported consumption of EDs in 2010 and 2011 is presented in Table 2. Frequent consumption of EDs was more common among boys than girls (p < 0.001 in 2010 and 2011), and the majority of both boys and girls either never or seldom consumed EDs (Table 2).
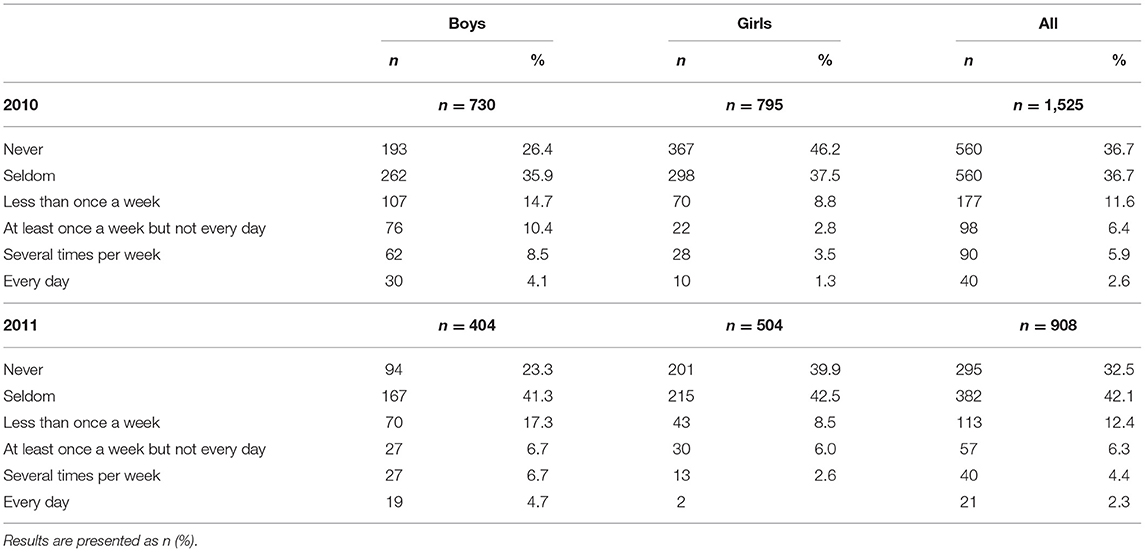
Table 2. Consumption of energy drinks among Swedish boys and girls in grades 6–9 in 2010 and 2011 (only those participating in 2010).
Descriptive statistics of the variables representing social background, levels of support, health conditions, and participation in norm-breaking behavior in 2010 are presented in Table 3.
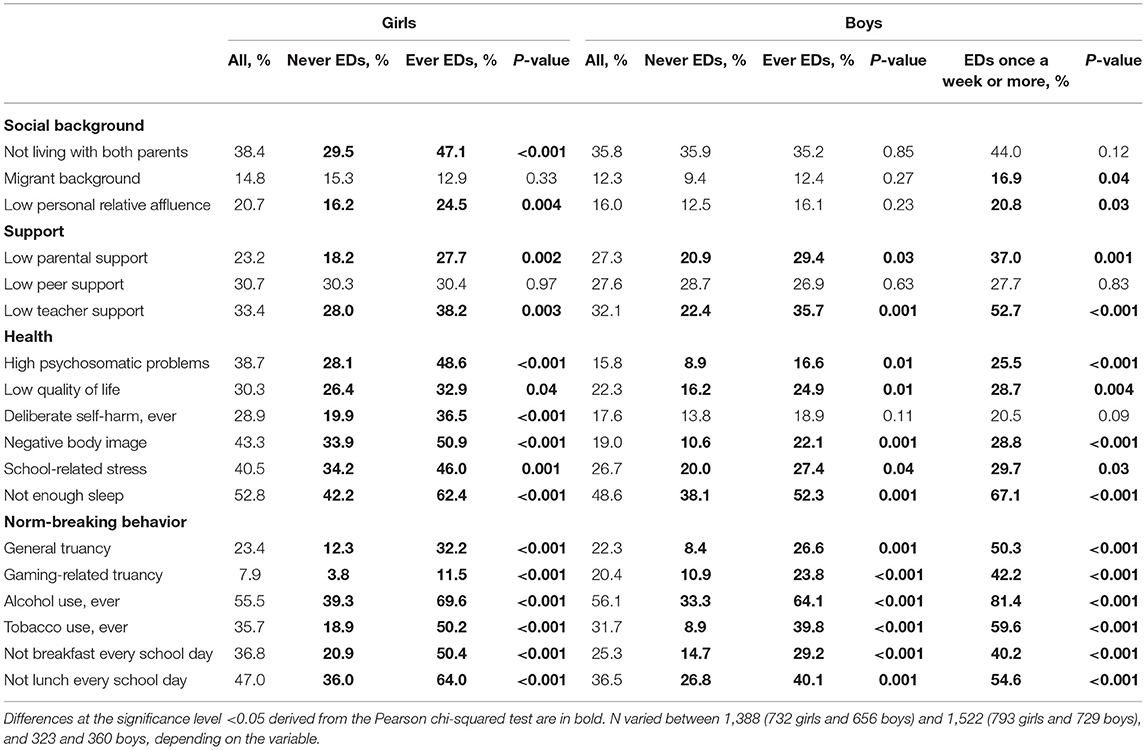
Table 3. Characteristics (percentages) of girls and boys who reported to never or ever consume energy drinks (EDs), and boys who reported to consume EDs once a week or more, in 2010.
Cross-Sectional Associations
Several variables were associated with ED consumption (Table 3). Among the girls, consumption of EDs was more common among those (1) not living with both parents, and (2) reporting low personal relative affluence. Furthermore, the girls who reported low levels of parental and teacher support were more likely to consume EDs. All investigated health-related and norm-breaking behavior variables were associated with ED consumption among the girls. For the boys, low levels of parental and teacher support were associated with ED consumption, as was the case with all of the norm-breaking behavior variables and health-related variables except for deliberate self-harm. Additional analyses were performed for the boys by comparing characteristics of those who reported to never consume EDs and those who reported to consume EDs once a week or more. This analysis showed stronger associations between ED consumption and low levels of support, worse health, and increased rates of norm-breaking behavior (Table 3). Furthermore, ED consumption was associated with a migrant background and low personal relative affluence in this analysis (Table 3).
Longitudinal Associations
We tested for longitudinal associations between ED consumption and health-related and norm-breaking behaviors. Controlling the analyses for grade and personal relative affluence did not substantially alter the results, and the adjusted odds ratio (OR) values are presented in Table 4. The analyses showed positive associations between ED consumption in 2010 and school-related stress, general truancy, gaming-related truancy, tobacco use, and not eating breakfast every school day in 2011 among the subsamples that did not report such issues in 2010 (Table 4). The OR values were higher when analyzing the sample of boys who reported consuming EDs at least once per week in comparison to the larger sample of boys who reported to have ever consumed EDs (Table 4). For both the subset of girls and the total sample, associations were also observed among ED consumption in 2010 and deliberate self-harm, not getting enough sleep, and alcohol consumption in 2011 (Table 4). For boys, an association was observed between ED consumption in 2010 and significant psychosomatic problems in 2011 among the sample of those who consumed EDs at least once per week (Table 4).

Table 4. Results of logistic regression models adjusted for grade (6–9) and personal relative affluence in 2010.
Among those who did not consume EDs in 2010, the variables that predicted ED consumption in 2011 were school-related stress, not getting enough sleep, and not eating breakfast every school day in 2010 (Table 4). Except for school-related stress, which was seen only among girls, these results were observed among those in the total sample.
Discussion
In the present study, boys consumed EDs more frequently than girls, although it is important to note that most of the participants either seldom or never consumed EDs. Consumption of EDs was positively associated with a majority of the analyzed variables of low levels of support, worse health, and more frequent participation in norm-breaking behaviors. The longitudinal analyses showed that, above all, ED consumption preceded both norm-breaking behavior and worse health 1 year later. The associations were generally stronger for the girls than the boys, and especially the boys with the highest levels of ED consumption.
The consumption of EDs in the present study is not comparable with the levels reported by a recent Swedish national dietary survey (25) since the latter investigated amounts whereas the present study relied on frequencies of consumption. In the national survey, administered to students in grades 5, 8, and year 2 of upper secondary school, 5% of both boys and girls consumed EDs during the 2-day data collection period (25). However, a higher intake among boys as compared to girls was seen with respect to the larger amounts of ED that were consumed (12 and 9 g per day, respectively) (25). The same national survey also collected data from youth not attending school, and in this smaller sample, 22% of boys and 9% of girls consumed EDs. A larger intake among boys has also been shown in other studies (14, 26, 27). A report from the European Food Safety Authority showed that among adolescents between 10 and 18 years of age in the European Union, ~68% were consumers of EDs (at least once during the last year) on average in the 16 surveyed countries (8).
This study used a variable for personal relative affluence to categorize adolescents' socio-economic status. This variable was associated with ED consumption among girls and the boys that consumed EDs once a week or more. This is in line with reports on differences in diet quality that result from health inequalities (28). Furthermore, previous studies on differences in ED consumption based on socio-economic have revealed both associations (26) as well as no associations (14).
In the present study, ED consumption was associated with worse health (e.g., worse mental health, less sleep, and more stress). Concerns about this type of associations, as well as concerns about ED consumption and health risk behaviors (such as smoking and drinking alcohol) among adolescents have been raised previously (4, 11, 15, 29). Thus, the results of the present study strengthen the evidence for these associations.
Implications for Policy and Practice
ED consumption has been shown to have longitudinal associations with worse health and increased participation in norm-breaking behavior in the present study among both girls and boys. One year later, the consumption of EDs was found to be a predictor of deliberate self-harm, school-related stress, not getting enough sleep, general and gaming-related truancy, having used alcohol and tobacco, and not eating breakfast every day, but for most variables, there was no such relationship the other way round. In other words, ED consumption seems to occur before other health risk behaviors, and thus it can be construed as an indicator of worse health and increased participation in norm-breaking behavior later on. Based on the results of this study sample, ED consumption can be interpreted as a red flag that predicts other health risk behaviors such as alcohol consumption and the use of tobacco. The reason why ED consumption is prior to other behaviors could be due to the fact that such drinks are simply easier to get a hold of. In Sweden, there is an age limit to buy alcohol and tobacco, but not EDs. There have been initiatives to make retailers restrict the sale of EDs to children and adolescents by encouraging an age limit. However, several major supermarkets still do not have an age limit for EDs. Furthermore, the consumption of EDs among the young is generally more socially acceptable than the consumption of alcohol and tobacco. Nevertheless, such differences could also be a function of levels of discouragement by parents and other adults, and therefore consuming such substances is simply exciting. Peer support was not associated with ED consumption in the present study, although low levels of parental and teacher support was. It is possible, therefore, that ED is used as a “pause drink” when it is accepted by those in the peer group and other options such as alcohol are unavailable. Costa et al. (30) found that EDs were consumed by adolescents as an alternative to other drinks to provide energy and foster interaction in social contexts. Sensation-seeking has also been associated with ED consumption (11). Since ED consumption can be the first step toward further norm-breaking behaviors, an age limit is recommended to prevent further negative behaviors. In fact, students have suggested this approach themselves in a study from the United Kingdom (31). Ultimately, an age limit would send the message that EDs are not intended for children and young people (31).
It is widely known that health risk behaviors among adolescents cluster (32). Distal determinants are probably responsible for the negative patterns of behavior, including the consumption of EDs among the adolescents surveyed for the present study. Since adolescence is formative, when it comes to lifestyle, it is important to promote healthy behaviors during this critical period. An environment that supports healthy behaviors irrespective of socio-economic status is especially important for adolescents. If attention is given to the differences in health behaviors among this group, socio-economic differences in adulthood can potentially be counteracted. With this objective in mind, the “whole school” approach is a means by which adults can work broadly to ensure the health of all students (33). For example, schools could aim to promote health literacy among the students, thereby building competencies that aid healthy dietary choices (34). Schools could also work to ensure that healthy alternatives to EDs are available in school cafeterias. Furthermore, supportive relations with parents and teachers are associated with students' improved health (35). Among the girls and boys surveyed in the present study, 23–33% reported low levels of support from parents and teachers, which shows that there is certainly some room for improvement. In general, adolescents consuming EDs should be observed when it comes to the issue of monitoring health risk behaviors, and in this respect, exchanges with school nurses could be used as an opportunity to discuss this issue (36). However, it has been shown that students who engage in health risk behaviors such as smoking and drinking are less likely to reflect on the content of the dialogue and follow the nurse's advice than students who do not participate in such activities (37).
Although the consumption of EDs was found to be more common among boys than girls, the stronger association for girls with most of the investigated variables indicates that girls who consume EDs are a more specific risk group. For boys, the associations were stronger when analyzing those who consumed EDs more frequently than once a week. Therefore, to identify boys most at risk for worse health and increased rates of norm-breaking behavior, one might need to use a higher limit of consumption for screening.
Methodological Considerations
The strengths of the present study include the longitudinal school-based design, the relatively large sample size, and the low drop-out rate. However, some limitations should be kept in mind when interpreting the results. First, the questionnaire was not designed to study ED consumption specifically. Therefore, only one question about this core variable was included, and the time-period that the question referred to was not specified. Accordingly, many of the participants replied “seldom” to the question of ED consumption. However, the analysis used broad categories of ED consumption (“never” vs. “ever” and “never” vs. “once a week or more”), and these alternatives probably attenuated the effects of any recall bias. Even these broad categories of consumption showed strong associations with many of the investigated variables. Furthermore, even though the sample was large to begin with, there were fewer responses to some of the variables and some response categories. Because of this, the sample size for some of the longitudinal analyses might have been too small to detect statistically significant associations. Moreover, the high number of hypothesis tests in this study increased the risk of false positives. The questionnaire contained questions about issues that could be perceived as sensitive (such as alcohol consumption). Previous research have found that asking adolescents about risky behavior does not increase the behavior (38). At the end of the questionnaire, the student were asked to indicate if they had been affected by the questions and wished to be contacted by the school nurse or counselor.
Conclusions
To summarize, the results showed that adolescents' consumption of EDs was associated with worse health and increased participation in norm-breaking behaviors both concurrently as well as 1 year later. The associations were generally stronger for girls than boys, suggesting that the relatively smaller group of girls who consume EDs is more at risk. More specifically, stronger associations were observed for boys when including those who consumed EDs once a week or more often. Ultimately, it is apparent that young consumers of EDs are important to target with health promotion activities. Health promotion activities should have a broad approach, but there is also reason to focus especially on girls who consume EDs and the boys with the highest the ED consumption rates. The underlying risk factors of ED consumption and its health effects need to be studied further. Future research should focus on disentangling the relationships between ED consumption, the participation in health-related behaviors, and health conditions, as well as investigating any common determinants. Therefore, study designs should be longitudinal and include enough participants to be able to control for several confounders to ensure that there is enough power to detect the relevant associations.
Data Availability Statement
The datasets presented in this article are not readily available because of ethical reasons. Requests to access the datasets should be directed to Katja Gillander Gådin, a2F0amEuZ2lsbGFuZGVyZ2FkaW5AbWl1bi5zZQ==.
Ethics Statement
The studies involving human participants were reviewed and approved by Regional Ethical Review Board in Umeå, Sweden (Dnr: 09-179M). Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author Contributions
ÅS analyzed the data and drafted the manuscript. MW and KG acquired the data and critically revised the manuscript for important intellectual content. All authors contributed to the design of the study and approved the final version and take responsibility for the content.
Funding
This work was supported by The Public Health Agency of Sweden [Grant number HFÅ2008/212].
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the students who participated in the study, and the school staff for valuable help with data collection.
References
1. Breda JJ, Whiting SH, Encarnação R, Norberg S, Jones R, Reinap M, et al. Energy drink consumption in Europe: a review of the risks, adverse health effects, and policy options to respond. Front Public Health. (2014) 2:134. doi: 10.3389/fpubh.2014.00134
2. Ali F, Rehman H, Babayan Z, Stapleton D, Joshi DD. Energy drinks and their adverse health effects: a systematic review of the current evidence. Postgrad Med. (2015) 127:308–22. doi: 10.1080/00325481.2015.1001712
3. Wassef B, Kohansieh M, Makaryus AN. Effects of energy drinks on the cardiovascular system. World J Cardiol. (2017) 9:796–806. doi: 10.4330/wjc.v9.i11.796
4. Seifert SM, Schaechter JL, Hershorin ER, Lipshultz SE. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics. (2011) 127:511–28. doi: 10.1542/peds.2009-3592
5. Hammond D, Reid JL, Zukowski S. Adverse effects of caffeinated energy drinks among youth and young adults in Canada: a Web-based survey. CMAJ Open. (2018) 6:E19–25. doi: 10.9778/cmajo.20160154
6. Koivusilta L, Kuoppamäki H, Rimpelä A. Energy drink consumption, health complaints and late bedtime among young adolescents. Int J Publ Health. (2016) 61:299–306. doi: 10.1007/s00038-016-0797-9
7. National Food Agency in Sweden. Riksmaten Ungdom 2016-17. Såäter Ungdomar i Sverige. [In Swedish]. National Food Agency in Sweden (2018). Available online at: https://www.livsmedelsverket.se/bestall-ladda-ner-material/sok-publikationer/artiklar/2018/2018-nr-14 (accessed August 20, 2020).
8. Zucconi S, Volpato C, Adinolfi F, Gandini E, Gentile E, Loi A, et al. Gathering Consumption Data on Specific Consumer Groups of Energy Drinks. European Food Safety Authority (2013). Available online at: http://www.efsa.europa.eu/en/supporting/pub/en-394 (accessed August 20, 2020).
9. Temple JL. Review: trends, safety, and recommendations for caffeinne use in children and adolescents. J Am Acad Child Adolesc Psychiatry. (2019) 58:36–45. doi: 10.1016/j.jaac.2018.06.030
10. Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC. Tracking of obesity-related behaviours from childhood to adulthood: a systematic review. Maturitas. (2011) 70:266–84. doi: 10.1016/j.maturitas.2011.08.005
11. Azagba S, Langille D, Asbridge M. An emerging adolescent health risk: Caffeinated energy drink consumption patterns among high school students. Prevent Med. (2014) 62:54–9. doi: 10.1016/j.ypmed.2014.01.019
12. Arria AM, Caldeira KM, Bugbee BA, Vincent KB, O'Grady KE. Trajectories of energy drink consumption and subsequent drug use during young adulthood. Drug Alcoh Depend. (2017) 179:424–32. doi: 10.1016/j.drugalcdep.2017.06.008
13. Williams RD, Housman JM, Odum M, Rivera AE. Energy drink use linked to high-sugar beverage intake and BMI among teens. Am J Health Behav. (2017) 41:259–65. doi: 10.5993/AJHB.41.3.5
14. Christensen LM, Iversen JD, Biltoft-Jensen A, Petersen MA, Søndergaard AB, Matthiessen J. Consumption of Energy Drinks Among 10-35-y-Old Danes (in Danish With an English Summary). National Food Institute; Technical University of Denmark (2014).
15. Richards G, Smith AP. A review of energy drinks and mental health, with focus on stress, anxiety and depression. J Caff Res. (2016) 6:49–63. doi: 10.1089/jcr.2015.0033
16. Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. In: Beaver KM, Walsh A, editors. Biosocial Theories of Crime. London: Routledge (2017). p. 69–96.
17. Nygren K, Janlert U, Nygren L. Norm compliance and self-reported health among Swedish adolescents. Scand J Publ Health. (2011) 39:44–50. doi: 10.1177/1403494810389846
18. Määttä S, Stattin H, Nurmi JE. Achievement strategies in peer groups and adolescents' school adjustment and norm-breaking behavior. Scand J Psychol. (2006) 47:273–80. doi: 10.1111/j.1467-9450.2006.00517.x
19. Dijkstra JK, Lindenberg S, Verhulst FC, Ormel J, Veenstra R. The relation between popularity and aggressive, destructive, and norm-breaking behaviors: moderating effects of athletic abilities, physical attractiveness, and prosociality. J Res Adolesc. (2009) 19:401–13. doi: 10.1111/j.1532-7795.2009.00594.x
20. Zetterström Dahlqvist H, Landstedt E, Gillander Gådin K. What students do schools allocate to a cognitive-behavioural intervention? Characteristics of adolescent participants in Northern Sweden. Int J Circumpolar Health. (2015) 74:29805. doi: 10.3402/ijch.v74.29805
21. Hagquist C. Psychosomatic health problems among adolescents in Sweden - are the time trends gender related? Eur J Publ Health. (2009) 19:331–6. doi: 10.1093/eurpub/ckp031
23. Levin KA, Currie C. Reliability and validity of an adapted version of the cantril ladder for use with adolescent samples. Soc Indic Res. (2014) 119:1047–63. doi: 10.1007/s11205-013-0507-4
24. Hunsberger M, Lehtinen-Jacks S, Mehlig K, Gwozdz W, Russo P, Michels N, et al. Bidirectional associations between psychosocial well-being and body mass index in European children: longitudinal findings from the IDEFICS study. BMC Publ Health. (2016) 16:949. doi: 10.1186/s12889-016-3626-4
25. National Food Agency in Sweden Energidrycker [In Swedish]. (2019). Available online at: https://www.livsmedelsverket.se/livsmedel-och-innehall/mat-och-dryck/drycker-och-alkohol/energidrycker (retrieved January 6, 2019).
26. Degirmenci N, Fossum IN, Strand TA, Vaktskjold A, Holten-Andersen MN. Consumption of energy drinks among adolescents in norway: a cross-sectional study. BMC Publ Health. (2018) 18:1391. doi: 10.1186/s12889-018-6236-5
27. Reid JL, McRory C, White CM, Martineau C, Vanderkooy P, Fenton N, et al. Consumption of caffeinated energy drinks among youth and young adults in Canada. Prevent Med Rep. (2017) 5:65–70. doi: 10.1016/j.pmedr.2016.11.012
28. Faught EL, McLaren L, Kirkpatrick SI, Hammond D, Minaker LM, Olstad D. Socioeconomic disadvantage across the life course is associated with diet quality in young adulthood. Nutrients. (2019) 11:242. doi: 10.3390/nu11020242
29. Harris JL, Munsell CR. Energy drinks and adolescents: whats the harm? Nutr Rev. (2015) 73:247–57. doi: 10.1093/nutrit/nuu061
30. Costa BM, Hayley A, Miller P. Young adolescents' perceptions, patterns, and contexts of energy drink use. A focus group study. Appetite. (2014) 8:183–9. doi: 10.1016/j.appet.2014.05.013
31. Visram S, Crossley SJ, Cheetham M, Lake A. Children and young people's perceptions of energy drinks: a qualitative study. PLoS ONE. (2017) 12:e0188668. doi: 10.1371/journal.pone.0188668
32. Carlerby H, Erling E, Viitasara E, Knutsson A, Gillander Gådin K. Risk behaviour, parental background, and wealth: a cluster analysis among Swedish boys and girls in the HBSC study. Scand J Publ Health. (2012) 40:368–76. doi: 10.1177/1403494812449926
33. Hunt P, Barrios L, Telljohann SK, Mazyck D. A whole school approach: collaborative development of school health policies, processes, and practices. J School Health. (2015) 85:802–9. doi: 10.1111/josh.12305
34. St Leger L. Schools, health literacy and public health: possibilities and challenges. Health Promot Int. (2001) 16:197–205. doi: 10.1093/heapro/16.2.197
35. Warne M, Snyder K, Gillander Gådin K. Participation and support – associations with Swedish pupils' positive health. Int J Circump Health. (2017) 76:1373579. doi: 10.1080/22423982.2017.1373579
36. Rising Holmström M, Asplund K, Kristiansen L. Promoting a relationship-based health practice: a challenge for school nurses. Br J School Nurs. (2013) 8:30–8. doi: 10.12968/bjsn.2013.8.1.30
37. Borup IK, Holstein BE. How do students who smoke and drink respond to the school nurse? Br J School Nurs. (2010) 5:128–33. doi: 10.12968/bjsn.2010.5.3.47458
Keywords: health behavior, risk groups, school health, support, truancy
Citation: Svensson Å, Warne M and Gillander Gådin K (2021) Longitudinal Associations Between Energy Drink Consumption, Health, and Norm-Breaking Behavior Among Swedish Adolescents. Front. Public Health 9:597613. doi: 10.3389/fpubh.2021.597613
Received: 25 August 2020; Accepted: 13 May 2021;
Published: 11 June 2021.
Edited by:
Saidur Mashreky, Centre for Injury Prevention and Research (CIPRB), BangladeshReviewed by:
Louis Kobina Dadzie, University of Cape Coast, GhanaM. Atiqul Haque, Bangabandhu Sheikh Mujib Medical University (BSMMU), Bangladesh
Copyright © 2021 Svensson, Warne and Gillander Gådin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Åsa Svensson, YXNhLm0uc3ZlbnNzb25AbWl1bi5zZQ==