 Carmen Corral-Partearroyo1,2,3
Carmen Corral-Partearroyo1,2,3 Alba Sánchez-Viñas1,3,4
Alba Sánchez-Viñas1,3,4 Montserrat Gil-Girbau1,5,6
Montserrat Gil-Girbau1,5,6 María Teresa Peñarrubia-María1,3,7,8
María Teresa Peñarrubia-María1,3,7,8 Ignacio Aznar-Lou1,3
Ignacio Aznar-Lou1,3 Antoni Serrano-Blanco1,3,4,5
Antoni Serrano-Blanco1,3,4,5 Cristina Carbonell-Duacastella1,3,9
Cristina Carbonell-Duacastella1,3,9 Carmen Gallardo-González1,6,7,8
Carmen Gallardo-González1,6,7,8 Maria del Carmen Olmos-Palenzuela6,7
Maria del Carmen Olmos-Palenzuela6,7 Maria Rubio-Valera1,3,5*
Maria Rubio-Valera1,3,5*- 1Health Technology Assessment in Primary Care and Mental Health (PRISMA) Research Group, Institut de Recerca Sant Joan de Déu, Esplugues de Llobregat, Spain
- 2Department of Paediatrics, Obstetrics, Gynaecology and Preventive Medicine, Univ Autonoma de Barcelona, Bellaterra, Spain
- 3Consortium for Biomedical Research in Epidemiology and Public Health (CIBER en Epidemiología y Salud Pública), Madrid, Spain
- 4Facultat de Medicina i Ciències de la Salut, Universitat de Barcelona, Barcelona, Spain
- 5Parc Sanitari Sant Joan de Déu, Sant Boi de Llobregat, Spain
- 6Research Network on Chronicity, Primary Care and Health Promotion (RICAPPS), Barcelona, Spain
- 7Primary Care Centre Bartomeu Fabrés Anglada, Direcció D'Atenció Primària Regió Metropolitana Sud, Institut Català de la Salut, Barcelona, Spain
- 8Unitat de Suport a la Recerca Regió Metropolitana Sud, Fundació Institut Universitari per a la Recerca a l'Atenció Primària de Salut Jordi Gol i Gurina (IDIAPJGol), Barcelona, Spain
- 9Facultat de Farmàcia, Universitat de Barcelona, Barcelona, Spain
Introduction: The Initial Medication Adherence (IMA) intervention is a multidisciplinary and shared decision-making intervention to improve initial medication adherence addressed to patients in need of new treatments for cardiovascular diseases and diabetes in primary care (PC). This pilot study aims to evaluate the feasibility and acceptability of the IMA intervention and the feasibility of a cluster-RCT to assess the effectiveness and cost-effectiveness of the intervention.
Methods: A 3-month pilot trial with an embedded process evaluation was conducted in five PC centers in Catalonia (Spain). Electronic health data were descriptively analyzed to test the availability and quality of records of the trial outcomes (initiation, implementation, clinical parameters and use of services). Recruitment and retention rates of professionals were analyzed. Twenty-nine semi-structured interviews with professionals (general practitioners, nurses, and community pharmacists) and patients were conducted to assess the feasibility and acceptability of the intervention. Three discussion groups with a total of fifteen patients were performed to review and redesign the intervention decision aids. Qualitative data were thematically analyzed.
Results: A total of 901 new treatments were prescribed to 604 patients. The proportion of missing data in the electronic health records was up to 30% for use of services and around 70% for clinical parameters 5 months before and after a new prescription. Primary and secondary outcomes were within plausible ranges and outliers were barely detected. The IMA intervention and its implementation strategy were considered feasible and acceptable by pilot-study participants. Low recruitment and retention rates, understanding of shared decision-making by professionals, and format and content of decision aids were the main barriers to the feasibility of the IMA intervention.
Discussion: Involving patients in the decision-making process is crucial to achieving better clinical outcomes. The IMA intervention is feasible and showed good acceptability among professionals and patients. However, we identified barriers and facilitators to implementing the intervention and adapting it to a context affected by the COVID-19 pandemic that should be considered before launching a cluster-RCT. This pilot study identified opportunities for refining the intervention and improving the design of the definitive cluster-RCT to evaluate its effectiveness and cost-effectiveness.
Clinical trial registration: ClinicalTrials.gov, identifier NCT05094986.
Introduction
The prevalence of non-initiated pharmacological treatments ranges from 2 to 40%, varying between medications and contexts and depending on patient characteristics and motivations (1–3). Non-initiation of chronic treatments, such as those for cardiovascular disease (CVD) and diabetes, generates a high burden on the healthcare system, which is aggravated by poor adherence (2, 4–8). Reducing non-initiation and improving long-term adherence is, therefore, a priority (9). Previous studies have evaluated interventions to reduce non-initiation but none of these interventions were theory-based and most of the studies showed a high risk of bias (10–15). To date, few interventions have focused on shared decision-making (SDM) strategies to improve adherence, which present promising results regarding improved health outcomes (16–19).
Carefully designing and piloting an intervention improves the likelihood of its effectiveness, transferability and sustainability (20, 21), especially in the case of complex interventions such as those aiming to change patients' and healthcare professionals' behavior. The Non-Initiation project followed the Medical Research Council (MRC) framework for complex interventions to gain an in-depth understanding of this behavior and contribute to the appropriate use of medications in primary care (PC) (20). Between 2014 and 2019, phase I, or the development phase, was carried out and epidemiological studies and qualitative research with patients and healthcare professionals were conducted to understand initiation behavior and design the Initial Medication Adherence (IMA) intervention (22–27). It is a complex, multidisciplinary, SDM intervention to improve initiation, secondary adherence, and clinical parameters in patients who receive a new prescription for CVDs or diabetes in PC. As per the non-initiation model (25, 26), the intervention works on two levels: the patient's intrapersonal level, based on the empowerment of the patient by increasing health literacy and SDM (28–30); and the patient's interpersonal level, based on the interaction between the patient and healthcare professionals, and their support (31–33). The intervention includes decision aids that target patients >18 years old with a risk of CVD and diabetes and were designed in collaboration with healthcare professionals.
This paper describes the results of phase II, or feasibility phase, which aimed to evaluate the feasibility and acceptability of the IMA intervention, the feasibility of the evaluation study, a pragmatic cluster-Randomized Controlled Trial (34, 35), and to ultimately optimize the IMA intervention and its evaluation design. The specific aims were to (1) test the availability and quality of data used to assess the effectiveness and cost-effectiveness of the IMA intervention, (2) evaluate the feasibility and acceptability of the IMA intervention in PC, and (3) revise and redesign the intervention decision aids.
Materials and methods
Study design
This pilot study was a cluster non-randomized controlled trial with an embedded process evaluation. The availability and quality (completion rate and reliability) of Real-World Data (RWD) records of the pilot trial were explored (aim 1), recruitment and retention rates were estimated and intervention group participants were interviewed (aim 2) and discussion groups with PC patients were conducted to review and redesign the decision aids (aim 3).
The results of this study are reported according to the Consolidated Standards of Reporting Trials (CONSORT) extension to pilot and feasibility trials (36).
Figure 1 shows the timeline of the pilot study, which was affected by the Coronavirus Disease (COVID-19) pandemic and the need to adapt it to this context. The intention was to carry out the intervention from March 2020 to May 2020, but adaptations were applied and it was finally launched in November 2020 and continued until January 2021.
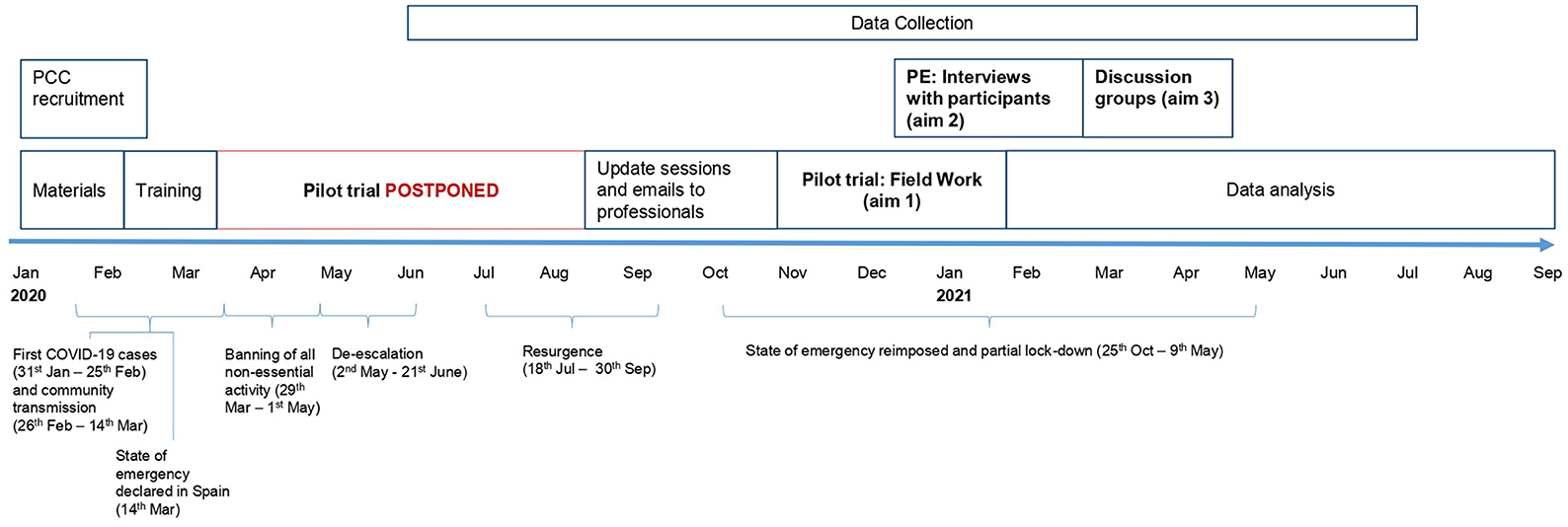
Figure 1. Timeline of the pilot study and COVID-19 periods in Spain. PCC, primary care center; PE, process evaluation. Aim 1: To test the availability and quality of data used to assess the effectiveness and cost-effectiveness of the IMA intervention. Aim 2: To evaluate the feasibility and acceptability of the IMA intervention in PC. Aim 3: To review the intervention decision aids to ultimately redesign them.
Setting
Healthcare in Spain is based on universal coverage for all citizens with free access at the point of use (with some exceptions) and is mostly funded by taxes (37). PC is the gatekeeper of the healthcare system, providing healthcare, health education, prevention activities, and community services. It consists essentially of a team of general practitioners (GP), nurses, and social workers, who are based in PC centers. Patients have an assigned GP and nurse. Prescription medicines are dispensed in community pharmacies by pharmacists who have access to the electronic prescription system (37). Patients can fill a prescription at any community pharmacy. The e-prescription system includes a warning that alerts the pharmacist to first prescriptions of inhalers, platelet aggregation inhibitors, anticoagulation, and insulin treatments.
Pilot study
Participants and group assignment
A convenience sample of five PC centers in Catalonia (Spain) participated in the study. GPs and nurses at the selected PC centers, together with pharmacists from community pharmacies in the reference area of the PC centers, were invited to participate. Professionals that agreed to participate provided signed informed consent. No other inclusion criteria were applied.
The study targeted patients (>18 years old) who received a new prescription of antihypertensive, lipid-lowering, antiplatelet, and/or antidiabetic (oral and/or insulin) medications. A prescription was considered new in the absence of prescriptions for medications of the same pharmacotherapeutic group during the previous 6 months. Patients' informed consent was obtained by simplified means (see “Ethics statement”) (38). No other inclusion criteria were applied.
Using convenience criteria, two PC centers were assigned to the control group and three to the intervention group. Healthcare professionals and patients were classified into intervention and control groups according to the reference PC centers and due to the nature of the intervention; professionals and patients were not blind to it.
Sample size calculation was not estimated prior to the pilot trial, although the sample was designed to be representative of the target cRCT population and was based on the same inclusion/exclusion criteria (39).
Description of intervention
The IMA intervention standardizes care and provides knowledge, skills, and tools to GPs to promote SDM when prescribing a new treatment for CVDs or diabetes, and to nurses and pharmacists to explore patients' doubts and offer supplementary information, promoting consistency and coordination of care. By applying the principles of SDM the patient is encouraged to express their concerns and preferences and actively participate in the decision process at their preferred level (29, 30). The implementation strategy has two main inputs: training for professionals on the motives underlying non-initiation, communication skills, health literacy, SDM, and the use of the decision aids; and decision aids (leaflets and a website) with information on the disease and treatment options to increase patients' health literacy and support SDM. The GP delivers the intervention at least once during the prescription process. Nurses and pharmacists deliver intervention on patients' demand during follow-up consultations and medication dispensing.
No training or decision aids were provided to professionals in the control group, who were asked to provide care as usual.
The IMA intervention was designed to be applied during face-to-face consultations, yet it was adapted to the COVID-19 context during the pilot study. When the new treatment was prescribed by phone, the GP emailed the leaflet contents to patients, and/or they were invited to collect it at the pharmacy. Additionally, the GP or nurse phoned the patient a week after the prescription to check whether questions had arisen.
Availability and quality of RWD for the trial (aim 1)
Trial outcomes and data collection
The primary trial outcome was initiation, defined as having a dispensing record following a new prescription (the index prescription) (40). A single prescription filled was considered an alternative outcome for initiation in sensitivity analysis. Secondary outcomes included implementation, clinical parameters [systolic and diastolic blood pressure, total cholesterol, low-density lipoprotein, high-density lipoprotein, blood glucose, glycated hemoglobin, estimated glomerular filtration rate, and cardiovascular risk (41)] and costs (use of healthcare services and days of sick leave).
Other variables included patient characteristics (sex, age, and diagnosis) and PC center characteristics according to non-initiation predictors (22): reference population, type of center (resident-training center or not), and socioeconomic status of the area divided into four urban categories based on quartiles, from low (urban 4) to high (urban 1), and a rural category.
All data were obtained from electronic health records registered at the public primary healthcare system database in Catalonia (Institut Català de Salut; ICS): System for the development of Research in Primary Care (SIDIAP) (42). Data were extracted for the follow-up period from June 2020 to June 2021.
Analysis
Descriptive analysis (counts, proportions, and means) was conducted using Stata 17 to explore all available variables and identify missing data and outliers.
First, the sociodemographic profile of the PC centers and participants at a prescription level (a patient can have more than one new prescription) was described.
Secondly, initiation was assessed by considering the time of prescription at the PC center and the dispensing month at the community pharmacy. Non-initiation was defined as not having collected the treatment prescribed (i.e., absence of dispensing records) within 3 months after the index prescription. A single prescription filled was defined as one dispensation only during the follow-up period. Costs were measured by taking into account the use of healthcare services, which included visits to PC professionals (GP or nurse), secondary care referrals, diagnostic tests, and days of sick leave. We assessed the reliability of recorded visits to PC professionals by calculating the proportion of new prescriptions and clinical parameters with a visit record on the same day.
Thirdly, the quality of clinical parameter records in the electronic health records was assessed. We calculated clinical parameter values and the proportion of prescribed treatments that had a clinical parameter registered during the follow-up period following care quality standards based on clinical practice guidelines (43–46).
Feasibility and acceptability of the IMA intervention (aim 2)
A process evaluation was integrated into the pilot study, collecting quantitative and qualitative data to measure professional recruitment and retention rates, assess the context and implementation of the IMA intervention in terms of fidelity to study protocol and the COVID-19 pandemic, and describe professionals' and patients' experiences and perceptions of the intervention in terms of feasibility and acceptability.
Quantitative data collection and analysis
Professional recruitment rates were registered in study forms before the pilot trial (March 2020) and after the trial was stopped and restarted (November 2020). Those professionals recruited in November were interviewed to estimate retention rates.
We used descriptive statistics (frequency and proportion) to estimate professionals' recruitment and retention rates.
Qualitative data collection and analysis
Following purposive sampling criteria, all the professionals and a selection of patients from the intervention group were invited to participate in the process evaluation. The research team contacted nineteen GPs, three nurses, and sixteen pharmacists by phone and email. GPs from the intervention group contacted five patients and invited them to participate in the study and to be interviewed by a researcher. All the participants signed informed consent prior to the interview.
Semi-structured telephone interviews with professionals were performed during and after the study was completed using a topic guide based on the intervention and the health theories and models it is based on (range 15–25 min). Field notes were made during and after the call. To increase the validity of the results, answers were summarized at the end of the interview and participants were asked to validate them.
Semi-structured face-to-face and telephone interviews with patients followed a topic guide based on the intervention and their intention to initiate the new medication after the intervention (range 20–40 min). These were recorded, anonymized, and transcribed by the research team.
Field notes and transcripts from semi-structured interviews were included as narrative data and analyzed following the principles of thematic content analysis (47) by two qualitative researchers. Data were organized and grouped by professionals and patients. Firstly, the researchers familiarized themselves with the data by re-reading notes and listening to recordings. Each researcher created a coding framework following a deductive and inductive approach. Open coding was applied to the data and codes were then organized into themes as per the research questions, based on pre-existing categories of the intervention, and new categories extracted about the mechanisms of action and context of the intervention and the attitude of patients regarding their pathology and treatment. Coding frameworks were triangulated, and themes were reviewed and refined by the two researchers before applying them to all the data.
Redesign of the IMA intervention tools (aim 3)
Patients from the PC system in Catalonia were recruited following a maximum variation sampling strategy based on some of the predictors of non-initiation: nationality, age, educational level, and presence of CVD and diabetes risk (22). Twenty-four patients were contacted. Patients that agreed to participate provided signed informed consent.
Data collection and analysis
Three discussion groups (duration 90–120 min) were conducted with four to six participants using a topic guide based on the protocol and IMA intervention decision aids, focusing particularly on health literacy and SDM. Discussion groups were recorded, anonymized, and transcribed by the research team.
Discussion groups were analyzed following a thematic analysis approach (47) by four researchers. Firstly, the researchers familiarized themselves with the data by listening to the recordings. Comments of the discussion groups were transcribed and rearranged to follow the intervention protocol, pre-existing categories of the decision aids, and new categories involving these tools that arose in the discussion groups. For each category, the main ideas were coded and reviewed to determine themes and identify patterns and, finally, the findings were triangulated between the researchers. No new themes emerged after coding the second discussion group.
Results
Participants
During the pilot trial, 901 new treatments of antihypertensive, lipid-lowering, antiplatelet, and/or antidiabetic (oral and/or insulin) medications were prescribed to 604 patients, 314 in the intervention group (see Figure 2 for details on recruitment and follow-up).
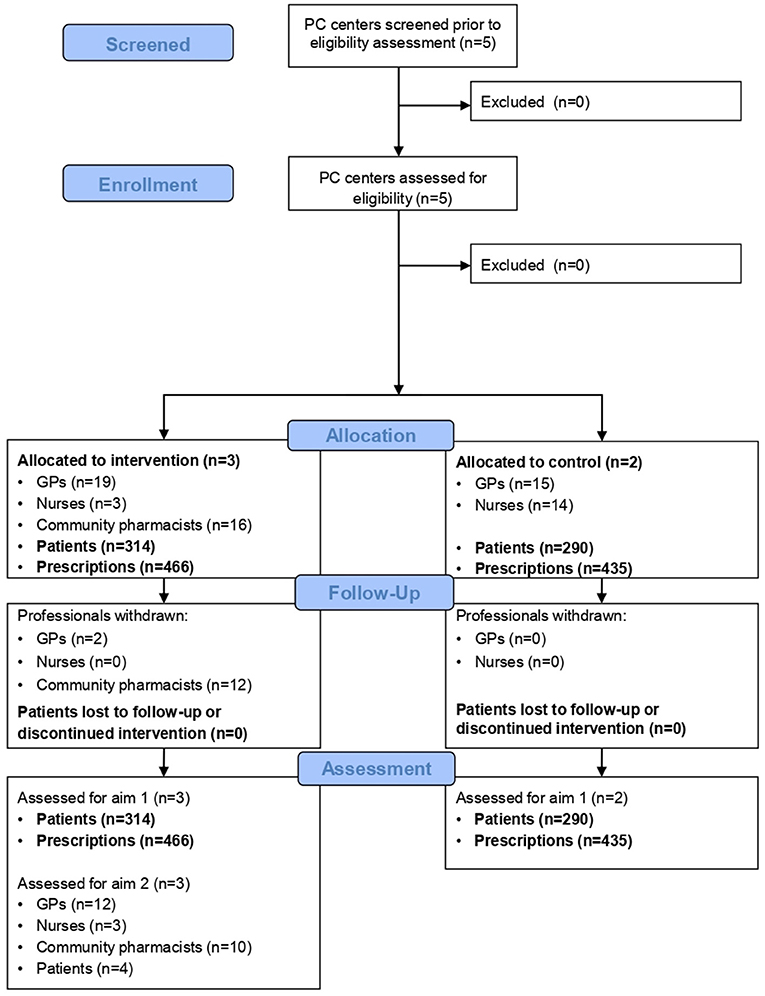
Figure 2. CONSORT Flow diagram (36). GP, general practitioner; PC, primary care. Aim 1: To test the availability and quality of data used to assess the effectiveness and cost-effectiveness of the IMA intervention. Aim 2: To evaluate the feasibility and acceptability of the IMA intervention in PC.
Tables 1, 2 show the characteristics of the participant PC centers and patients. PC centers were located in urban areas with different socioeconomic status, size and proportion of immigrant population and most were training centers (Table 1). Half of the medications were prescribed to women (50.83%), with the mean age of patients being 62.6 years old. Most of the prescriptions had a diagnosis record (89.7%); with the highest frequency being hypertensive disease (59.6%). There were almost no differences between women and men in terms of age and diagnoses, except for diabetes (Table 2).
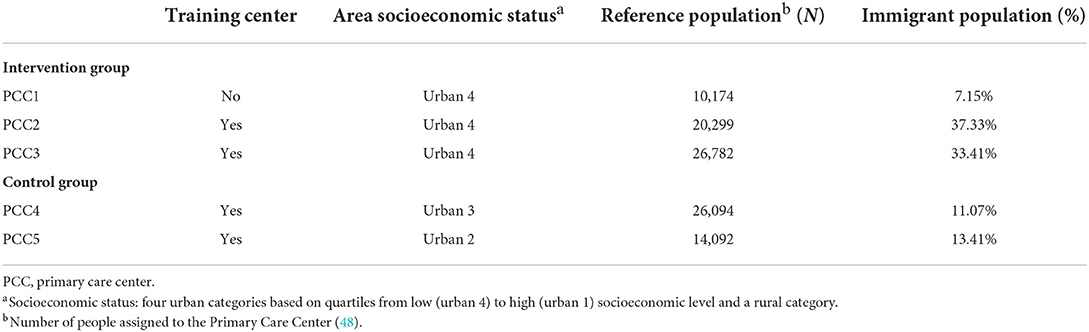
Table 1. Characteristics of the PC centers.
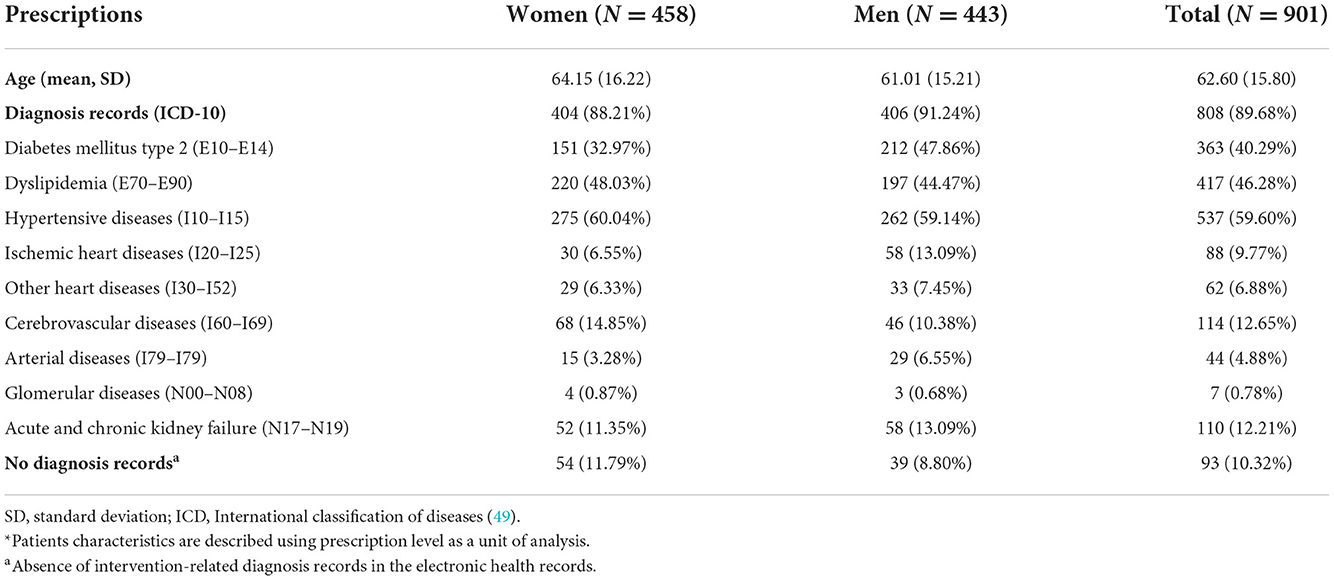
Table 2. Characteristics of the patients*.
The process evaluation involved 12 GPs, three nurses, 10 pharmacists, and four patients. Two GPs declined the invitation to participate due to time restrictions, and the rest failed to reply. One patient declined to participate in the study. Over half of the professionals were women, ranging between 41 and 52 years old and with more than 10 years of experience in PC. Half of the patients were women, ranging between 50 and 68 years old, and they were prescribed different medications and had different work and educational levels. Finally, 15 patients from the PC system in Catalonia agreed to participate in the discussion groups, varying by sex, age, cardiovascular risk, and educational level. Characteristics of the participants are shown in Supplementary Tables 1–3.
Availability and quality of RWD for the trial (aim 1)
Initiation and implementation
These variables have no missing data. In total, 10.7% of prescriptions were not initiated 3 months after the index prescription, and 18.4% were single prescriptions filled.
Table 3 summarizes indicators of data availability and quality for clinical parameters. Missing records in patient electronic health records were >50% in all cases before the index prescription, and between 39.7% (systolic and diastolic blood pressure) and 85.2% (cardiovascular risk) after the index prescription, with the lowest being cardiovascular risk in both cases. All parameter values were within plausible ranges except one estimated glomerular filtration rate CKD-EPI value which was recorded manually.
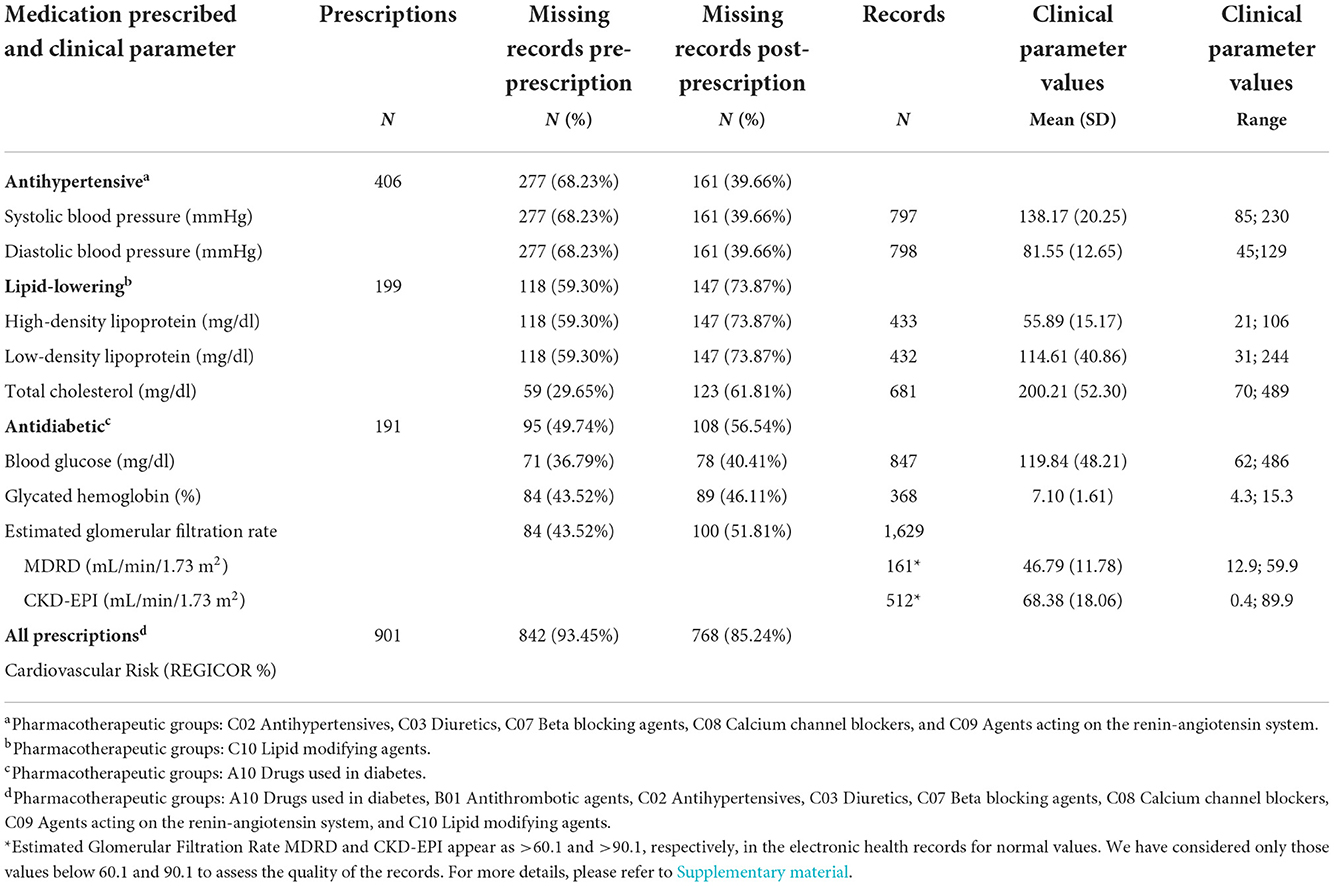
Table 3. Data availability and quality for clinical parameters for baseline (pre-prescription) and follow-up (post-prescription) assessment.
Tables 4, 5 summarize indicators of data availability and quality for use of services and productivity losses. A 33.3% of prescriptions didn't have a visit registered on the day of a new prescription, while there were 13.8–27% of clinical parameter measures without any visit records on the same day (Table 4). After the index prescription all values for healthcare services and productivity losses were within plausible ranges, and no outliers were detected (Table 5).
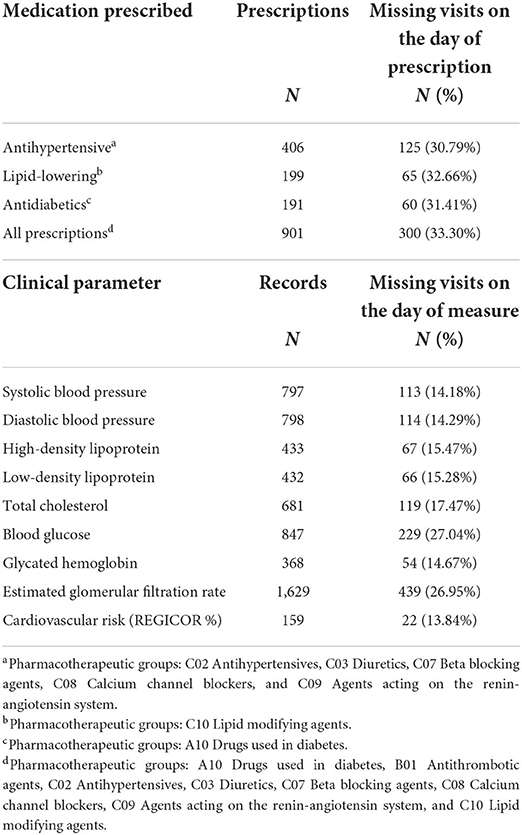
Table 4. Data availability of visits the day prescriptions were issued and clinical parameters were measured.

Table 5. Data quality for use of services (number of services used) and productivity losses (number of days of sick leave) (N prescriptions = 901).
Feasibility and acceptability of the IMA intervention (aim 2)
Professional recruitment and retention rates
Table 6 shows the professional recruitment and retention rates. Overall, recruitment was lower for nurses than for GPs and pharmacists. Retention was the highest for GPs and nurses. Only two GPs were lost due to sick leave. Low retention rates of pharmacists were attributed to the study being postponed and the COVID-19 distance measures in place.
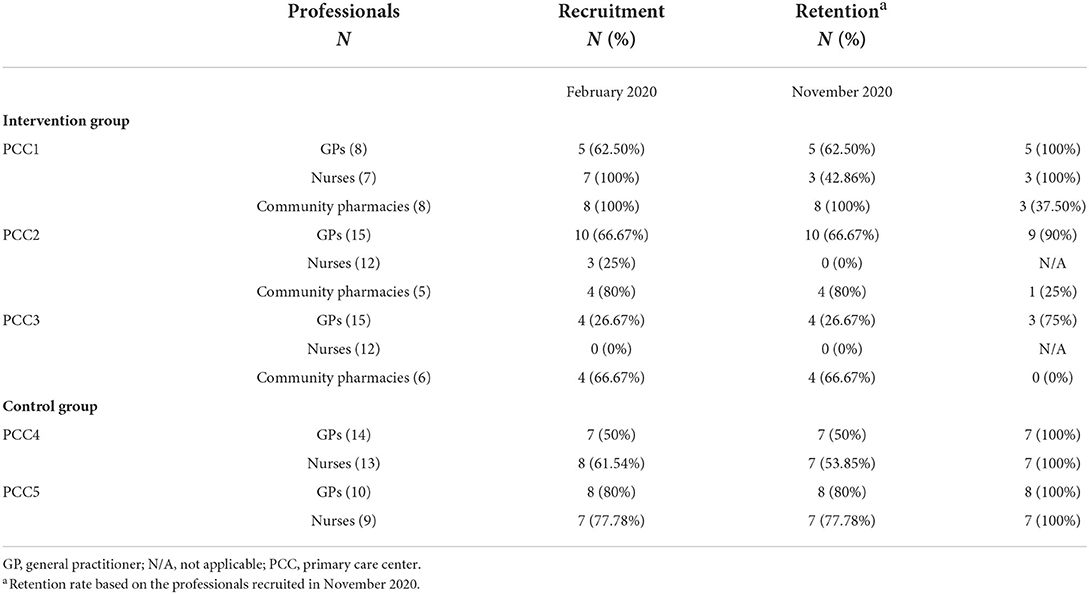
Table 6. Professional recruitment and retention rates.
Context and implementation of the IMA intervention
The COVID-19 pandemic influenced the implementation of the IMA intervention and fidelity to the study protocol. Training was completed long before the pilot was finally carried out, and professionals described more consultations for acute health problems, fewer follow-up and preventive consultations and therefore fewer chronic medication prescriptions. All along with an increased workload at both PC centers and pharmacies. All professionals described an increase in telephone consultations and, as a result, an increase in the duration of face-to-face consultations (reporting ~15 min per patient). Nevertheless, different practices within different organizations were reported. One of the PC centers in the intervention group had returned to face-to-face consultations by November 2020, whereas the other two were doing mainly telephone consultations. In the case of community pharmacies, most had increased the physical distance from patients due to the pandemic.
The implementation strategy and processes of the IMA intervention, contextual factors, and the grade of fidelity to the study protocol and grade of adaptability to the intervention are described below and summarized in Figure 3.
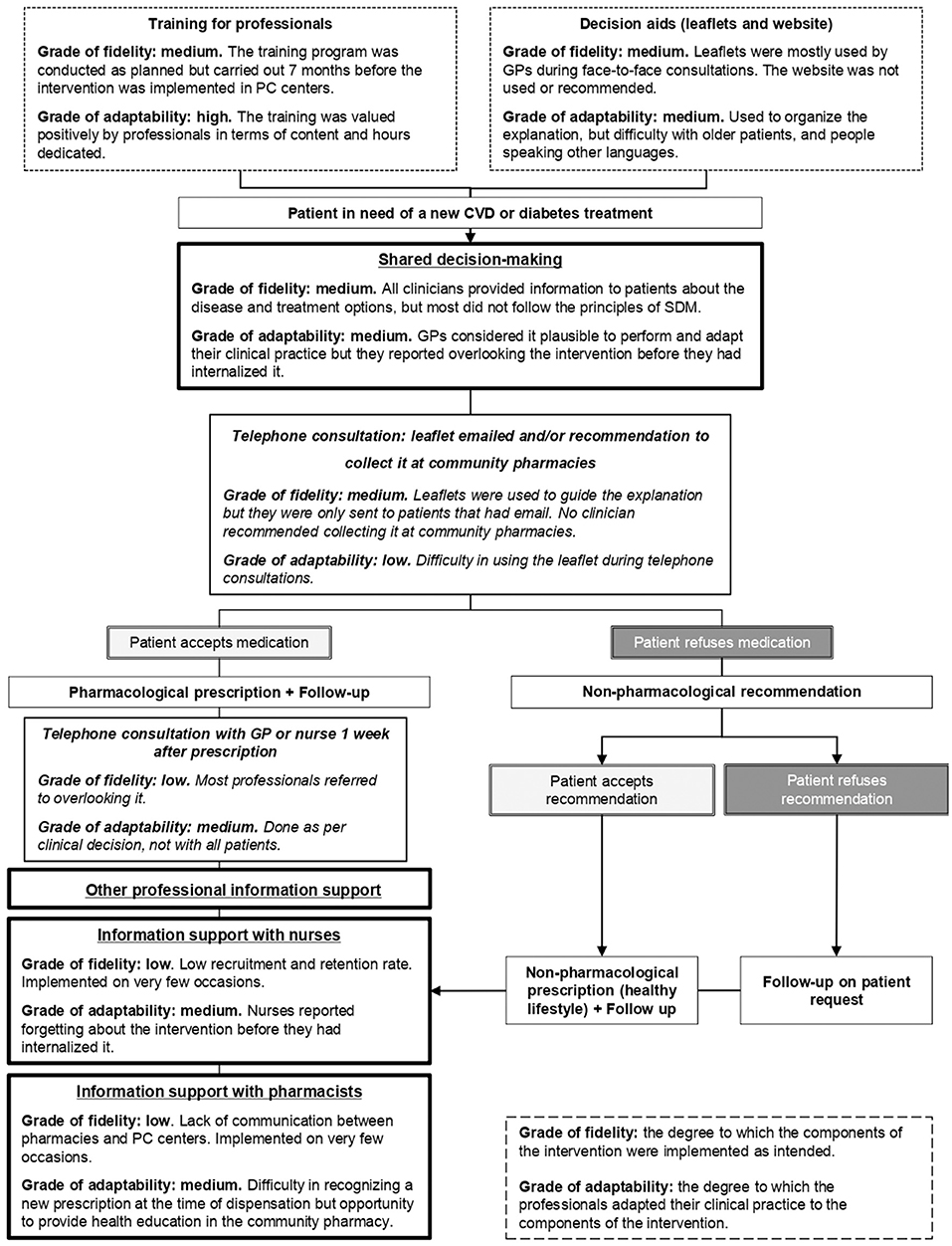
Figure 3. Grade of fidelity and adaptability to the implementation strategy and processes of the IMA intervention. CVD, cardiovascular disease; GP, general practitioner; PC, primary care. Text in italics describes the intervention adaptations made due to the COVID-19 pandemic.
Training for professionals
The training was generally valued positively in terms of content and hours dedicated. Professionals understood non-initiation as a public health problem, GPs recognized situations in which the patient accepted a new prescription during a consultation but never initiated it, and appreciated the tools provided during training to approach new prescriptions. Nevertheless, due to the delay of the pilot study, some GPs and nurses and most pharmacists, mentioned that they had forgotten about it.
Decision aids
PC professionals agreed that the leaflet was helpful in organizing the information given to patients. However, some found it challenging and questioned its utility when used with older patients and people who did not speak Spanish or Catalan. Most of the pharmacists reported not using the leaflets, and none of the professionals reported using the website or recommending it to patients.
GPs considered it was easier to implement the intervention face-to-face using the leaflets than by telephone consultations. Those that implemented it by telephone used the leaflet to guide themselves through the explanation and sent it online only to those patients that had email. Three out of four patients stated that GPs used a leaflet during the explanation of the new prescription, one of them through telephone consultation. In the last case, the leaflet was sent by email and the GP phoned the patient some days later to ensure the information was understood.
Shared decision-making
At the time of a new prescription, GPs considered that the intervention was easy to apply and adapted their clinical practice accordingly. They mainly reported applying the intervention during face-to-face consultations and having enough time to do so. Providing information to the patient about the disease and treatment options was considered part of the standard practice of the GP, and all of them reported doing so. Nonetheless, only two GPs reported following the principles of SDM when recommending a new medication. The majority stated that the patient agreed with the prescription, and only two mentioned that the patient decided with them to issue the prescription.
Of the patients that stated that the GP provided information using the leaflet, only one reported SDM during the prescribing process. In the other cases, the GP did not ask their opinion or preferences and prescribed the medication only after they explained the disease and the treatment. When patients were asked about participating in the decision process, some of them considered it was not a decision for them to make. Some considered they need not be involved because of a lack of knowledge in the field but also because they trusted the GP's decision.
Other professional information support
Both GPs and nurses considered the fact that few nurses participated in the study to be a barrier to the intervention. Nurses were believed to have an important role in the follow-up and identification of patients with CVDs or diabetes. Additionally, professionals at the PC centers and pharmacists cited a lack of communication between one another. Pharmacists were often not considered as part of the multidisciplinary PC team, which was seen as a barrier to implementing the intervention at all levels; GPs as prescribers, and nurses and pharmacists as central supporters.
Most nurses and pharmacists participating reported implementing the intervention on very few occasions, and none of the patients interviewed confirmed that the nurse or the pharmacist implemented the intervention with them. Some visited the nurse after the prescription for a follow-up on the chronic disease and all mentioned that the pharmacist dispensed the medication without any explanation.
Broadly, the main barrier to implementing the intervention was forgetfulness. Professionals tended to overlook it before they had internalized it as their standard practice. In addition, pharmacists found it difficult to recognize a new prescription at the time of dispensation, especially if the alert on the e-prescription system was not available.
Professionals' and patients' experiences and perceptions in terms of feasibility and acceptability: Key themes
Summarized below are the key themes regarding feasibility and acceptability, such as the experiences and perceptions of the GPs as prescribers, nurses, and pharmacists as key supporters, and patients as recipients of the IMA intervention.
Perceived effect of the IMA intervention by professionals
Professionals believed that, even though the information was very similar to that of usual care, patients understood it better when the leaflet was used to structure the information and considered this could have a direct impact on adherence. A negative effect in terms of initiation was related to giving more information about medication adverse effects to patients with chronic conditions with no symptoms. Some professionals believed patients may be more afraid of adverse effects than future complications associated with the disease.
Relationship and trust between the professional and patient
Trust in professional recommendations was perceived to be affected by the relationship between the professional and the patient, which was considered to be mainly influenced by the length of time the patient had visited the same professional. Trust was described as the main facilitator. From the professional's point of view, it makes it easier to maintain a conversation with the patient and explore their perceptions, while from the patient's perspective, it makes it easier to ask questions and express their opinion.
Motivation for professionals to adapt their clinical practice
Even though most professionals described the COVID-19 pandemic as a difficult situation, some GPs emphasized they were more willing to make changes as they considered the IMA intervention as reinforcement of the importance of SDM in their routine practice. Similarly, pharmacists saw it as an opportunity to provide health education in the community pharmacy, especially to those patients that were not able to visit the PC center during the pandemic.
Redesign of the IMA intervention tools (aim 3)
PC patients highlighted the advantages and disadvantages of the pilot leaflets according to their needs. As for disadvantages, they emphasized a lack of topic titles to introduce the content, the medical jargon, and the large amount of information provided. As advantages, they highlighted the structure of the leaflet and specific contents such as the epidemiological data on the disease, data on the consequences of the decision not to treat, and the encouragement to express their doubts and opinions and participate in the decision process.
Moreover, patients recommended that the new leaflets should clarify whether the non-pharmacological measures are an alternative to the medication or an addition to it, so the patient is encouraged to adopt non-pharmacological measures in the case of a pharmacological prescription. Additionally, patients suggested that only the most common adverse effects of the medication should be mentioned so that the risk-benefit assessment of the medication is balanced.
Patients acknowledged they looked on the internet when they had questions about their disease or treatment after consultation with clinicians. However, they found it very difficult to find a website that was reliable and supported by official organizations, and with easy-to-understand content. With respect to the website that was being designed for the definitive trial, they considered it should have links to other patients' associations, as well as to the Catalan Electronic Health System, so they had the option to contact a PC professional directly if they had any queries.
Discussion
The results of this pilot study suggest that implementing an intervention based on SDM to improve adherence to medications for CVDs and diabetes in PC is feasible and that the intervention is well-accepted. Carrying out a pragmatic cRCT to evaluate the effectiveness and cost-effectiveness of such an intervention is also feasible but weaknesses in the study design and the implementation of the intervention were identified and the knowledge gained should be used to refine the intervention and the study (50).
A non-initiation rate of 11% is in line with previous studies that were used to calculate the sample size of the cRCT (22, 27). The study identified weaknesses in the electronic health records by recognizing a high prevalence of missing registered visits. This could be explained, in the context of the COVID-19 pandemic, and by an increased number of telephone and emergency consultations (51). At the time of the pilot study the workload in PC centers was high, which could partly explain flaws in data records. This is not expected to happen during the cRCT, but if missing visit records are identified, and taking into account that all prescriptions would be issued in PC centers in the public health system, every prescription would be imputed as one visit to the GP so costs are not underestimated. Additionally, there was a high proportion of missing clinical parameter records that could be explained by the COVID-19 situation, when face-to-face visits were kept to the minimum, and by the short follow-up period (5 months). Care quality standards based on clinical practice guidelines from the Catalan Health System recommend taking measurements at least every 12 months for all parameters except cholesterol, which is recommended every 18 months (43–46). During the training stage for professionals, the importance of registering clinical parameters according to clinical practice guidelines will be reinforced to reduce the percentage of missing data obtained through RWD during the trial. However, values of the parameters were mainly within the expected range. Special attention will be paid to records entered manually that are expected to increase during the cRCT. The sample size of the trial exceeded the estimates determined in previous feasibility study research (39, 52, 53).
The COVID-19 pandemic impacted the recruitment of nurses and the retention of pharmacists, as professionals reported, although recruitment rates of PC professionals were already low in some centers in February 2020, especially in the case of nurses. Other studies have also identified difficulties in recruitment and retention rates of healthcare professionals in PC, particularly due to lack of time, high workload, and low engagement with the research topic (54, 55). To improve professional recruitment rates and promote participation, before contacting PC professionals, we will inform stakeholders of PC and pharmacy organizations in Catalonia, as well as managers and directors of PC centers. Furthermore, the IMA-cRCT will be presented in a short session to professionals at each selected PC center and pharmacy, and they will be given time to ask the research team questions and deliberate participation in the study. Additionally, the research team will contact professionals participating in the trial regularly to troubleshoot, provide support, and therefore improve retention.
In general, professionals failed to apply the principles of SDM and both professionals and patients perceived some of the barriers and facilitators that have previously been cited in the literature (56, 57). For instance, professionals reported overlooking the intervention and both professionals and patients questioned patients' willingness to get involved in the decision process. However, patient preferences for SDM are influenced by the perception of professionals regarding SDM and its approach when inviting the patient to take part in the process (29, 56). Professionals recognized that SDM could increase patients' knowledge and improve adherence to medications, and even though time has been reported as a barrier before (56), none considered time to be a restriction to applying the intervention in this study. SDM is the foundation of the IMA intervention, involving patients in the decision process empowers them and increases self-efficacy by increasing health literacy and awareness of their pathologies and treatment options, and therefore the potential to increase adherence to treatment plans (17, 30). Patients are invited to express their opinions and if they decide not to start the medication the prescription is not issued. Likewise, they are actively involved in the treatment follow-up, information on medication effects and adverse events is given so patients can take them into account in the decision-making process as well as identify them and act accordingly if the treatment is initiated. To increase professionals' understanding and engagement with SDM, the training will be extended to 6 h, with 3 h dedicated to SDM. To balance professionals' schedules, it will be divided into two sessions. Session one would cover non-initiation as a public health problem and the development of the IMA intervention, as well as its practical aspects, such as records and ethical requirements. Session two will focus on communication skills and SDM and this preparation has been designed by an expert in the field. All professionals will be trained together to increase cohesion between GPs, nurses, and pharmacists, and reinforce the role of the latter two in providing information and supporting the patient in the decision process when a new chronic pharmacological treatment is prescribed.
The main advantages and disadvantages of the decision aids were identified and will be used to redesign and respect the preferred information format for patients as recommended by SDM models (29). The leaflets will contain essential information written in plain language, with a clear distinction between non-pharmacological measures and pharmacological treatments, and a section encouraging patients to express their opinion and professionals to write recommendations to patients. Additionally, they will be translated into the most widely-spoken languages in Catalonia. The content of the website will be appraised by healthcare organizations in Catalonia and the layout will be designed to make it more user-friendly. It will be divided into pathologies and pharmacological treatments and the leaflets will be easier to acquire as patients and professionals will be able to download them from the website.
The COVID-19 pandemic has inevitably impacted the implementation of the intervention during the pilot study. However, not all the consequences were negative. As described by professionals, the pandemic encouraged them to adapt their clinical practice to new situations and reinforced the role of pharmacists in providing health education. Additionally, the duration of face-to-face consultations was increased, which might have favored the implementation of the IMA intervention. Organizational changes during the COVID-19 pandemic and the reintroduction of usual practices in PC centers and pharmacies would need to be considered carefully during the implementation of the IMA intervention in a pragmatic PC setting during the upcoming cRCT.
Some limitations need to be acknowledged. First, the duration proposed for this pilot study was 3 months of fieldwork and 6 months of follow-up before and after the index prescription. However, due to the COVID-19 pandemic, the duration of the follow-up period dropped to 5 months, which might have impacted the access to parameter data in the electronic health records. Second, the study was only carried out in one region of Catalonia in the context of a pilot study, and even though PC centers had dissimilar socioeconomic characteristics, the results obtained might have been different if various regions of Catalonia had been included. Third, the low recruitment rate of nurses, especially after the COVID-19 pandemic, might have limited the assessment of the role of nurses in the IMA intervention. Lastly, not all the professionals who participated in the trial were interviewed and we might have missed some important insights. Nevertheless, the percentage of participation among professionals was high, all were invited to participate and had the opportunity to be interviewed at their preferred date and time.
Involving patients in the decision-making process is fundamental in achieving better clinical outcomes, although patient-centered care requires modifications to clinical practice in PC. We identified barriers and facilitators to implementing the intervention as well as adapting it to a context affected by the COVID-19 pandemic. This pilot study contributes information regarding the feasibility and acceptability of the IMA intervention and its evaluation design in a pragmatic setting. It has helped to identify strengths and weaknesses and refine the IMA intervention and its evaluation design accordingly before the definitive cRCT to evaluate the effectiveness and cost-effectiveness of the IMA intervention.
Data availability statement
The datasets presented in this article are not readily available because the research team is not the quantitative data owner as it only analyzes information that is property of public health institutions. The data that support the findings of this study are available from SIDIAP but restrictions apply to the availability of these data, which were used under license for the current study, and thus are not publicly available. However, data are available from the authors upon reasonable request and with the permission of SIDIAP. Qualitative data and the study protocol are available from the authors upon reasonable request. Requests to access the datasets should be directed to bWFyaWEucnViaW9Ac2pkLmVz.
Ethics statement
This study was reviewed and approved by the Drug Research Committee (CEIm) at the IDIAP Jordi Gol, codeCEIm 19/198-P. The pilot study is a low-intensity intervention clinical trial where groups of subjects are allocated to the control and the intervention group. Informed consent was obtained by simplified means which requires that the same information stated under Article 30 of Regulation (EU) No 536/2014 is provided before anyone is enrolled in the trial, and after being informed, the patient does not object to participating (38). All conditions described in Regulation (EU) No 536/2014 and the Real Decreto 1090/2015 were fulfilled (38, 58). Informed consent in the present study was obtained by displaying posters in prominent locations of the participating PC centers notifying people that a clinical trial was being conducted in the center and that patients could be part of this comparative study. Posters contained information on how and why the trial was being conducted and what the implications of participating in the study were. Furthermore, professionals in the intervention and control groups were trained to deal with patients' queries regarding the study. If patients declined to participate in the study, this information was documented by clinicians in the electronic health records and data from those patients was not used for the study. Finally, patients could withdraw at any time from the study without any detriment.
Participation in this study was entirely voluntary. Professionals that agreed to participate signed informed consent at the training session and agreed to be interviewed as part of the process evaluation. Patients who participated in the process evaluation and discussion groups signed informed consent after recruitment and prior to the beginning of data collection. All participants had the right to refuse to participate and to withdraw from the study at any time.
Author contributions
MR-V led the design of the study and obtained funding for the study. IA-L, MG-G, and MP-M advised and contributed to the study design. MR-V, IA-L, MG-G, MP-M, and CC-D designed the decision aids. MR-V, IA-L, MG-G, and MP-M recruited and trained professionals. CC-P, AS-V, IA-L, and MR-V developed the statistical analysis plan and analyzed quantitative data. CC-P, MG-G, MP-M, and AS-V collected and analyzed qualitative data. CC-P wrote the first draft of the manuscript. All authors added to and approved the final manuscript.
Funding
The project IMA-cRCT has received funding from the European Research Council (ERC) under the European Union's Horizon 2020 research and innovation programme (GA No. 948973) from January 1st 2021. Thanks to this grant we can apply the results to adapt the final intervention and its assessment and disseminate the results of the study that was funded by a research grant from the College of Pharmacists of Barcelona (Col·legi de Farmacèutics de Barcelona) in 2019 in order to develop the intervention, the fieldwork and the analysis. IA-L had a CIBERESP contract (CIBER in Epidemiology and Public Health, CB16/02/00322) during the development of this study. MP-M has the 14th ICS support for the promotion of group research strategies through the intensification of researchers (7Z22/009) and 16th ICS support for the promotion of group research strategies through the intensification of researchers (7Z20/028), from the IDIAP Jordi Gol. CG-G has the 17th ICS support for the promotion of group research strategies through the intensification of researchers (7Z21/019), from the IDIAP Jordi Gol. CC-D had a PFIS research contract both from the Institute of Health Carlos III (ISCIII), Ministry of Economy and Competitiveness (Spain) (FI20/00007) when the study was developed.
Acknowledgments
We thank those that contributed to the development of the IMA intervention: Guillermo Bagaría de Casanova, Maria Giner Soriano, Rosa Morros Pedrós, Montserrat Iracheta Todó, and Daniel Planchuelo Calatayud. We thank Alexandra L. Dima for her inputs and revising the final manuscript. Finally, we thank Stephen Kelly for his help with language editing. This work has been carried out within the framework of the Ph.D. program in Methodology of Biomedical Research and Public Health at the Universitat Autònoma de Barcelona.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a shared research network (Research Network in Chronicity, Primary Care and Health Promotion RICAPPS) with the authors MG-G, MO-P, and CG-G at the time of the review.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1038138/full#supplementary-material
Abbreviations
CONSORT, Consolidated Standards of Reporting Trials; COVID-19, Coronavirus Disease; cRCT, cluster-Randomized Controlled Trial; CVD, Cardiovascular Disease; GP, General Practitioner; MRC, Medical Research Council; IMA, Initial Medication Adherence; PC, Primary Care; RWD, Real-World Data; SDM, Shared Decision Making; SIDIAP, System for the development of Research in Primary Care.
References
1. Menckeberg TT, Bouvy ML, Bracke M, Hugtenburg JG, Lammers JW, Raaijmakers JAM. Patients' understanding of the reasons for starting and discontinuing inhaled corticosteroids. Br J Clin Pharmacol. (2008) 66:255–60. doi: 10.1111/j.1365-2125.2008.03168.x
2. Lemstra M, Nwankwo C, Bird Y, Moraros J. Primary nonadherence to chronic disease medications: a meta-analysis. Patient Prefer Adherence. (2018) 12:721–31. doi: 10.2147/PPA.S161151
3. Zeber JE, Manias E, Williams AF, Hutchins D, Udezi WA, Roberts CS, et al. A systematic literature review of psychosocial and behavioral factors associated with initial medication adherence: a report of the ISPOR medication adherence & persistence special interest group. Value Heal. (2013) 16:891–900. doi: 10.1016/j.jval.2013.04.014
4. Bitton A, Choudhry NK, Matlin OS, Swanton K, Shrank WH. The impact of medication adherence on coronary artery disease costs and outcomes: a systematic review. Am J Med. (2013) 126:357.e7–e27. doi: 10.1016/j.amjmed.2012.09.004
5. Xu T, Yu X, Ou S, Liu X, Yuan J, Tan X, et al. Adherence to antihypertensive medications and stroke risk: a dose-response meta-analysis. J Am Heart Assoc. (2017) 6:e006371. doi: 10.1161/JAHA.117.006371
6. Bouchard MH, Dragomir A, Blais L, Bérard A, Pilon D, Perreault S. Impact of adherence to statins on coronary artery disease in primary prevention. Br J Clin Pharmacol. (2007) 63:698–708. doi: 10.1111/j.1365-2125.2006.02828.x
7. Kim Y-Y, Lee J-S, Kang H-J, Park SM. Effect of medication adherence on long-term all-cause-mortality and hospitalization for cardiovascular disease in 65,067 newly diagnosed type 2 diabetes patients. Sci Rep. (2018) 8:12190. doi: 10.1038/s41598-018-30740-y
8. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ Open. (2018) 8:e016982. doi: 10.1136/bmjopen-2017-016982
9. World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization (2003). Available from: https://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf?sequence=1&isAllowed=y (accessed September 05, 2022).
10. Derose SF, Green K, Marrett E, Tunceli K, Cheetham TC, Chiu VY, et al. Automated outreach to increase primary adherence to cholesterol-lowering medications. JAMA Intern Med. (2013) 173:38–43. doi: 10.1001/2013.jamainternmed.717
11. Fischer MA, Choudhry NK, Bykov K, Brill G, Bopp G, Wurst AM, et al. Pharmacy-based interventions to reduce primary medication nonadherence to cardiovascular medications. Med Care. (2014) 52:1050–4. doi: 10.1097/MLR.0000000000000247
12. Fischer MA, Jones JB, Wright E, Van Loan RP, Xie J, Gallagher L, et al. A randomized telephone intervention trial to reduce primary medication nonadherence. J Manag care Spec Pharm. (2015) 21:124–31. doi: 10.18553/jmcp.2015.21.2.124
13. O'Connor PJ, Schmittdiel JA, Pathak RD, Harris RI, Newton KM, Ohnsorg KA, et al. Randomized trial of telephone outreach to improve medication adherence and metabolic control in adults with diabetes. Diabetes Care. (2014) 37:3317–24. doi: 10.2337/dc14-0596
14. Kerner DE, Knezevich EL. Use of communication tool within electronic medical record to improve primary nonadherence. J Am Pharm Assoc. (2017) 57:S270–3.e2. doi: 10.1016/j.japh.2017.03.009
15. McCarthy ML, Ding R, Roderer NK, Steinwachs DM, Ortmann MJ, Pham JC, et al. Does providing prescription information or services improve medication adherence among patients discharged from the emergency department? A randomized controlled trial. Ann Emerg Med. (2013) 62:212–23.e1. doi: 10.1016/j.annemergmed.2013.02.002
16. Saheb Kashaf M, McGill ET, Berger ZD. Shared decision-making and outcomes in type 2 diabetes: a systematic review and meta-analysis. Patient Educ Couns. (2017) 100:2159–71. doi: 10.1016/j.pec.2017.06.030
17. Mathijssen EGE, van den Bemt BJF, van den Hoogen FHJ, Popa CD, Vriezekolk JE. Interventions to support shared decision making for medication therapy in long term conditions: a systematic review. Patient Educ Couns. (2019) 103:254–65. doi: 10.1016/j.pec.2019.08.034
18. Coronado-Vázquez V, Canet-Fajas C, Delgado-Marroquín MT, Magallón-Botaya R, Romero-Martín M, Gómez-Salgado J. Interventions to facilitate shared decision-making using decision aids with patients in Primary Health Care: a systematic review. Medicine. (2020) 99:e21389. doi: 10.1097/MD.0000000000021389
19. Milky G, Thomas J. Shared decision making, satisfaction with care and medication adherence among patients with diabetes. Patient Educ Couns. (2020) 103:661–9. doi: 10.1016/j.pec.2019.10.008
20. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:a1655. doi: 10.1136/bmj.a1655
21. Eldridge SM, Lancaster GA, Campbell MJ, Thabane L, Hopewell S, Coleman CL, et al. Defining feasibility and pilot studies in preparation for randomised controlled trials: development of a conceptual framework. PLoS ONE. (2016) 11:e0150205. doi: 10.1371/journal.pone.0150205
22. Aznar-Lou I, Fernández A, Gil-Girbau M, Fajó-Pascual M, Moreno-Peral P, Peñarrubia-María MT, et al. Initial medication non-adherence: prevalence and predictive factors in a cohort of 16 million primary care patients. Br J Clin Pharmacol. (2017) 83:1328–40. doi: 10.1111/bcp.13215
23. Aznar-Lou I, Iglesias-González M, Gil-Girbau M, Serrano-Blanco A, Fernández A, Peñarrubia-María MT, et al. Impact of initial medication non-adherence to SSRIs on medical visits and sick leaves. J Affect Disord. (2018) 226:282–6. doi: 10.1016/j.jad.2017.09.057
24. Aznar-Lou I, Pottegård A, Fernández A, Peñarrubia-María MT, Serrano-Blanco A, Sabés-Figuera R, et al. Effect of copayment policies on initial medication non-adherence according to income: a population-based study. BMJ Qual Saf. (2018) 27:878–91. doi: 10.1136/bmjqs-2017-007416
25. Gil-Girbau M, Aznar-Lou I, Peñarrubia-María MT, Moreno-Peral P, Fernández A, Bellón J, et al. Reasons for medication non-initiation: a qualitative exploration of the patients' perspective. Res Soc Adm Pharm. (2020) 16:663–72. doi: 10.1016/j.sapharm.2019.08.002
26. Peñarrubia-María MT, Gil-Girbau M, Gallardo-González MC, Aznar-Lou I, Serrano-Blanco A, Mendive Arbeloa JM, et al. Non-initiation of prescribed medication from a Spanish health professionals' perspective: a qualitative exploration based on Grounded Theory. Health Soc Care Community. (2022) 30:e213–21. doi: 10.1111/hsc.13431
27. Vilaplana-Carnerero C, Aznar-Lou I, Peñarrubia-María MT, Serrano-Blanco A, Fernández-Vergel R, Petitbò-Antúnez D, et al. Initiation and single dispensing in cardiovascular and insulin medications: Prevalence and explanatory factors. Int J Environ Res Public Health. (2020) 17:3358. doi: 10.3390/ijerph17103358
28. Edwards M, Wood F, Davies M, Edwards A. The development of health literacy in patients with a long-term health condition: the health literacy pathway model. BMC Public Health. (2012) 12:130. doi: 10.1186/1471-2458-12-130
29. Elwyn GJ, Edwards A, Kinnersley P, Grol R. Shared decision making and the concept of equipoise: the competences of involving patients in healthcare choices. Br J Gen Pract. (2000) 50:892–9. Available online at: https://bjgp.org/content/bjgp/50/460/892.full.pdf
30. Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. (2012) 27:1361–7. doi: 10.1007/s11606-012-2077-6
31. Rimer B, Glanz K. Theory at a Glance: A guide For Health Promotion Practice. 2nd ed. Bethesda, MD: National Cancer Institute (2005).
32. Cragg L, Davies M, McDowall W. Using theory to guide change at the individual level. In: McGraw-Hill, editor. Health Promotion Theory. 2nd ed. London: Open University Press (2013).
33. Gil-Girbau M, Pons-Vigués M, Rubio-Valera M, Murrugarra G, Masluk B, Rodríguez-Martín B, et al. Theoretical models of health promotion in primary healthcare everyday practice. Gac Sanit. (2021) 35:48–59. doi: 10.1016/j.gaceta.2019.06.011
34. Sánchez-Viñas A, Corral-Partearroyo C, Gil-Girbau M, Peñarrubia-María MT, Gallardo-González C, Olmos-Palenzuela MC, et al. Effectiveness and cost-effectiveness of an intervention to improve initial medication adherence to treatments for cardiovascular diseases and diabetes in primary care: study protocol for a pragmatic cluster randomised controlled trial and economic model (the IMA-cRCT study). BMC Prim Care. (2022) 23:170. doi: 10.1186/s12875-022-01727-6
35. Corral-Partearroyo C, Sánchez-Viñas A, Gil-Girbau M, Peñarrubia-María M, Aznar-Lou I, Gallardo-González C, et al. Complex multidisciplinary intervention to improve Initial Medication Adherence to cardiovascular disease and diabetes treatments in primary care (the IMA-cRCT study): Mixed methods process evaluation protocol. BMJ Open. (2022) 12:e067468. doi: 10.1136/bmjopen-2022-067468
36. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Br Med J. (2016) 355:i5239. doi: 10.1136/bmj.i5239
37. Bernal E, Sandra D, Juan G-A, Fernando O, Sánchez Martínez I, Ramón J, et al. Spain: health system review. Health Syst Transit. (2018) 20:1–179. Available online at: https://www.euro.who.int/__data/assets/pdf_file/0008/378620/hit-spain-eng.pdf
38. European Union. Regulation (EU) No 536/2014 of the European Parliament and of the Council of 16 April 2014 on Clinical Trials on Medicinal Products for Human Use, and Repealing Directive 2001/20/EC Text With EEA Relevance. Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A32014R0536 (accessed September 05, 2022).
39. Thabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. (2010) 10:1. doi: 10.1186/1471-2288-10-1
40. Vrijens B, De Geest S, Hughes DA, Przemyslaw K, Demonceau J, Ruppar T, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. (2012) 73:691–705. doi: 10.1111/j.1365-2125.2012.04167.x
41. Marrugat J, Solanas P, D'Agostino R, Sullivan L, Ordovas J, Cordón F, et al. Estimación del riesgo coronario en España mediante la ecuación de Framingham calibrada. Rev Esp Cardiol. (2003) 56:253–61. doi: 10.1016/S0300-8932(03)76861-4
42. SIDIAP. Sistema d'Informació per al desenvolupament de la Investigació en Atenció Primària. Available from: https://www.sidiap.org/ (accessed September 05, 2022).
43. Coll de Tuero G, Dalfó i Baqué A, de la Figuera Von Wichmann M, Gibert i Llorach E, Isnard Blanchar M, Martínez Alonso V, et al. Guies de pràctica clínica. Barcelona: Hipertensió Arterial Institut Català de la Salut (2012).
44. Baena Díez J, Barcelo Colomer E, Ciurana Misol R, Franzi Sisó A, García Cerdán M, Ríos Rodríguez M, et al. Guies de pràctica clínica. Colesterol i risc coronari. Vol 1. Barcelona: Institut Català de Salut (2009).
45. Mata M, Cos FX, Morros R, Diego L, Barrot J, Berengué M, et al. Guies de pràctica clínica. Abordatge de la diabetes mellitus tipus 2. Barcelona: Institut Català de la Salut (2013).
46. Verdú Rotellar J, Pacheco Huergo V, Amado Guirado E, Esgueva de Haro N, López Pareja N, Alemany Vilches L, et al. Guies de pràctica clínica. Insuficiència cardíaca. Barcelona: Institut Català de la Salut (2008). Available online at: https://scientiasalut.gencat.cat/bitstream/handle/11351/4516/insuficiencia_cardiaca_guies_practica_clinica_2007_versio_extensa.pdf?sequence$=$1&isAllowed$=$y (accessed September 05, 2022).
47. Green J, Thorogood N. Qualitative Methods for Health Research. 4th ed. London: SAGE (2018). 440 p.
48. Servei Català de la Salut. Població de referència del Servei Català de la Salut per a l'any 2020 - Dades per ABS i UP assignada. (2020). Available from: https://catsalut.gencat.cat/web/.content/minisite/catsalut/proveidors_professionals/registres_catalegs/documents/poblacio-referencia.pdf (accessed September 05, 2022).
49. World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. Available from: https://icd.who.int/browse10/2019/en (accessed September 05, 2022).
50. Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, et al. Framework for the development and evaluation of complex interventions: gap analysis, workshop and consultation-informed update. Health Technol Assess. (2021) 25:1–132. doi: 10.3310/hta25570
51. Feldman J, Szerencsy A, Mann D, Austrian J, Kothari U, Heo H, et al. Giving your electronic health record a checkup after COVID-19: a practical framework for reviewing clinical decision support in light of the telemedicine expansion. JMIR Med Informat. (2021) 9:e21712. doi: 10.2196/21712
52. Teare D, Dimairo M, Hayman A, Shephard N, Whitehead A, Walters S. Sample size requirements for pilot randomised controlled trials with binary outcomes: a simulation study aims. Trials. (2013) 14:O21. doi: 10.1186/1745-6215-14-S1-O21
53. Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. (2016) 25:1057–73. doi: 10.1177/0962280215588241
54. Johnston S, Liddy C, Hogg W, Donskov M, Russell G, Gyorfi-Dyke E. Barriers and facilitators to recruitment of physicians and practices for primary care health services research at one centre. BMC Med Res Methodol. (2010) 10:109. doi: 10.1186/1471-2288-10-109
55. Krebs F, Lorenz L, Nawabi F, Lück I, Bau AM, Alayli A, et al. Recruitment in health services research-A study on facilitators and barriers for the recruitment of community-based healthcare providers. Int J Environ Res Public Health. (2021) 18:10521. doi: 10.3390/ijerph181910521
56. Gravel K, Légaré F, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: a systematic review of health professionals' perceptions. Implement Sci. (2006) 1:16. doi: 10.1186/1748-5908-1-16
57. Légaré F, Ratté S, Gravel K, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: update of a systematic review of health professionals' perceptions. Patient Educ Couns. (2008) 73:526–35. doi: 10.1016/j.pec.2008.07.018
Keywords: primary care, complex intervention, shared decision-making (SDM), medication adherence, pilot, feasibility study
Citation: Corral-Partearroyo C, Sánchez-Viñas A, Gil-Girbau M, Peñarrubia-María MT, Aznar-Lou I, Serrano-Blanco A, Carbonell-Duacastella C, Gallardo-González C, Olmos-Palenzuela MdC and Rubio-Valera M (2022) Improving Initial Medication Adherence to cardiovascular disease and diabetes treatments in primary care: Pilot trial of a complex intervention. Front. Public Health 10:1038138. doi: 10.3389/fpubh.2022.1038138
Received: 06 September 2022; Accepted: 10 November 2022;
Published: 06 December 2022.
Edited by:
Ana Clavería, Instituto de Investigación Sanitaria Galicia Sur (IISGS), SpainReviewed by:
Patrick Okwen, Effective Basic Services (eBASE) Africa, CameroonMartin Schulz, Freie Universität Berlin, Germany
Copyright © 2022 Corral-Partearroyo, Sánchez-Viñas, Gil-Girbau, Peñarrubia-María, Aznar-Lou, Serrano-Blanco, Carbonell-Duacastella, Gallardo-González, Olmos-Palenzuela and Rubio-Valera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Rubio-Valera, bWFyaWEucnViaW9Ac2pkLmVz