 Christine Rousset-Jablonski1,2,3*
Christine Rousset-Jablonski1,2,3* Faustine Dalon4
Faustine Dalon4 Quitterie Reynaud1,2
Quitterie Reynaud1,2 Lydie Lemonnier5Clémence Dehillotte5Flore Jacoud4Marjorie Berard4
Lydie Lemonnier5Clémence Dehillotte5Flore Jacoud4Marjorie Berard4 Marie Viprey1,6
Marie Viprey1,6 Eric Van Ganse1,4,7
Eric Van Ganse1,4,7 Isabelle Durieu1,2Manon Belhassen4
Isabelle Durieu1,2Manon Belhassen4- 1Université Claude Bernard Lyon 1, Research on Healthcare Performance (RESHAPE), INSERM U1290, Lyon, France
- 2Department of Internal Medicine, Cystic Fibrosis Center, Hospices Civils de Lyon, Groupe Hospitalier Sud, Lyon, France
- 3Département de chirurgie, Centre Léon Bérard, Lyon, France
- 4PELyon, PharmacoEpidemiologie Lyon, Lyon, France
- 5Vaincre la Mucoviscidose Association, Paris, France
- 6Health Data Department, Hospices Civils de Lyon, Lyon, France
- 7Respiratory Medicine, Croix-Rousse University Hospital, Lyon, France
Background: Cystic fibrosis (CF) care and the life expectancy of affected patients have substantially improved in recent decades, leading to an increased number of patients being diagnosed with comorbidities, including cancers. Our objective was to characterize the epidemiology of cancers between 2006 and 2017 in CF patients with and without a lung transplant.
Methods: Medical records of CF patients from 2006 to 2016 in the French CF Registry were linked to their corresponding claims data (SNDS). The annual prevalence and incidence rates of cancers were estimated from 2006 to 2017 in CF patients without lung transplant and in those with lung transplant after transplantation.
Results: Of the 7,671 patients included in the French CF Registry, 6,187 patients (80.7%) were linked to the SNDS; among them, 1,006 (16.3%) received a lung transplant. The prevalence of any cancer increased between 2006 and 2017, from 0.3 to 1.0% and from 1.3 to 6.3% in non-transplanted and transplanted patients, respectively. When compared to the general population, the incidence of cancer was significantly higher in both non-transplanted [Standardized Incidence Ratio (SIR) = 2.57, 95%CI 2.05 to 3.17] and transplanted (SIR = 19.76, 95%CI 16.45 to 23.55) patients. The median time between transplant and the first cancer was 3.9 years. Among the 211 incident cancer cases, the most frequent malignant neoplasms were skin neoplasm (48 cases), lung cancers (31 cases), gastro-intestinal (24 cases), and hematologic cancers (17 cases).
Conclusion: The overall burden of cancer in CF patients is high, particularly following lung transplantation. Therefore, specific follow-up, screening and cancer prevention for CF patients with transplants are necessary.
Introduction
During recent decades, the life expectancy of people with cystic fibrosis (pwCF) has increased dramatically, and treatment with cystic fibrosis transmembrane regulator (CFTR) modulators will likely contribute to further improvements. In countries with well-developed cystic fibrosis (CF) care, more than half of pwCF followed in CF centers are adults (1, 2). However, along with this increased life expectancy, new complications have emerged, such as extra-respiratory comorbidities and cancer. Indeed, several studies have reported a greater than expected number of digestive tract cancers, particularly in the small intestine, colon, and biliary tract (3, 4). The pathogenesis of cancer in CF remains unclear, but inflammation and the role of CFTR have been discussed (5, 6). Specifically, regarding the risk of cancer for pwCF, two different situations have to be identified: pwCF who have undergone lung transplantation (LT) and those who have not.
Despite such major improvements in CF care, LT remains necessary for patients with severe CF as the ultimate option. In Italy, Spain, France, the UK and the US, between 3 and 11% of CF patients receive a LT (2, 7, 8). Despite better survival for pwCF than for patients receiving LT for other indications (due to their young age at transplantation), several US epidemiological studies have shown an increased risk of cancer for pwCF with transplants (3, 4, 9, 10), but European data are lacking.
In the literature, a particular risk of digestive tract cancers is described for non-transplanted pwCF (11). In 2013, in the US, non-transplanted pwCF were also found to be at higher risk of testicular cancer and chronic lymphocytic leukemia than the general US population (3). To the best of our knowledge, one observational study has been published in Europe, showing an increased risk for kidney, thyroid, endocrine cancers, lymphoma and non-melanoma skin cancers in Swedish patients, and another recent study described a higher risk of cancer, mainly gastrointestinal (GI), skin, breast and hematological cancers in the UK CF population (12, 13).
With recent epidemiological changes in pwCF, data need to be actualized to further discuss the necessity of specific follow-up and screening and even more for lung-transplanted pwCF. This paper characterizes the epidemiology of cancer in pwCF and incidence trends from 2006 to 2017 in France according to patient status with respect to LT.
Materials and methods
Data sources
The French CF Registry collects clinical data for all pwCF followed at CF care centers, including transplanted patients (2).
In the SNDS, the following anonymized data are prospectively recorded for all French patients covered by national health insurance: sociodemographic characteristics, date of death, out-of-hospital reimbursed healthcare expenditures (from both public and private healthcare), and hospital discharge summaries with International Classification of Diseases (ICD-10) codes, and direct information on medical diagnoses for patients who have full coverage by the NHS for all medical expenses [Chronic Disease status], including patients diagnosed with CF in France (14).
In this study, data for each patient of the CF registry were individually linked to the French administrative health care database (SNDS), using a probabilistic method (15).
Study population and study design
This study involved patients recorded in the French CF Registry between 2006 and 2016 and for whom linkage with the SNDS could be achieved. Patients were followed until December 31, 2017.
Two subgroups were defined: (1) Patients with a PLT were considered those with a medical procedure or hospital diagnosis for LT between 2006 and 2017 in the SNDS and those with a LT recorded in the CF registry before 2006. (2) Patients without any medical procedure or hospital diagnosis related to LT, either in the SNDS or in the CF registry, even before 2006. Patients with any history of other transplantation (mainly kidney, liver) were excluded from both groups.
Patients with a first diagnosis of invasive cancer (identified with ICD-10 codes from hospital admissions, Supplementary Table 1) were identified in the two groups of pwCF according to their LT status. Their incidence status was defined by the absence of chronic disease status for cancer in the SNDS before 2006 or by the absence of cancer recorded in the CF registry before 2006.
The index date was the 01/01/2006 for patients born prior to 2006, and the birth date recorded in the registry for patients born after 2006.
For non-transplanted patients, follow-up started at the index date and finished at the end of follow-up, as defined by the following events, whichever occurred first: death, loss to follow-up (date of last information recorded in the SNDS prior to a 24-month period without any reimbursement), or end of the study period in the SNDS (31/12/2017). For PLT patients, follow-up started at the PLT date, or from the index date if PLT occurred before 2006, to the end of follow-up, as defined for the other group.
Data analysis
Socio-demographic characteristics and clinical data are presented using descriptive statistics, as follows: for quantitative variables, the sample size (N), mean, standard deviation (std), median, and first and third quartiles (Q1–Q3) are reported; for qualitative and ordinal variables, the sample size (N) and frequency are reported.
Comorbidities were identified using chronic disease status, hospital diagnosis, or specific therapies.
Cases of cancer were classified as prevalent or incident. Prevalent cancer cases were defined by at least one hospitalization and/or a chronic disease status for cancer for a given cancer in a given year. Incident cancer cases were defined by a first hospitalization and/or a first chronic disease status for cancer for a given cancer in a given year. The incidence rate (per 1,000 person-years) was defined as the total number of new cancer cases (the numerator) divided by the sum of the person-time of the at-risk population (the denominator). It was estimated for each studied year, and only patients included in the studied year were counted in the denominator, that is, patients with at least 1 day of follow-up in that year. So long as a patient did not have any cancer yet, he was still considered as at risk of developing it and therefore contributed to the denominator.
We used the standardized incidence ratio (SIR), defined as the ratio of the number of cancers observed to the number of cancers expected, and we calculated 95% confidence intervals (CIs) for the SIR while assuming that the observed cases of cancer followed a Poisson distribution. The number of cancers expected during the at-risk period was determined by applying age- (within 5-year groups), sex-, and calendar year-specific incidence rates obtained from the data published by the French National Cancer Registry in 2019 (based on data from 2018) to the total person-years accumulated in the corresponding categories [16].
The time to onset of the first cancer was plotted using a cumulative incidence curve, allowing mortality to be taken into account as a competitive risk when the mortality rate was >10%.
The statistical analysis was performed with SAS Enterprise Guide® (SAS Institute, North Carolina), version 7.13.
Ethics
This observational study was conducted using anonymized data after approval by the French Institute for Health Data (approval n° 217, on December 1, 2016) and the National Informatics and Liberty Committee (approval n° DE-2018-001, on March 12, 2018).
Results
This study considered 7,671 patients included in the French CF Registry between 2006 and 2016. Probabilistic linkage with the claims database could be performed for 6,187 (80.7%) patients. Among them, 1,006 (16.3%) patients had a PLT, and 5,074 were non-transplanted patients (107 remaining patients have been transplanted from other organs, mainly kidney, liver). Table 1 presents the sociodemographic and clinical characteristics of PLT and non-transplanted pwCF.
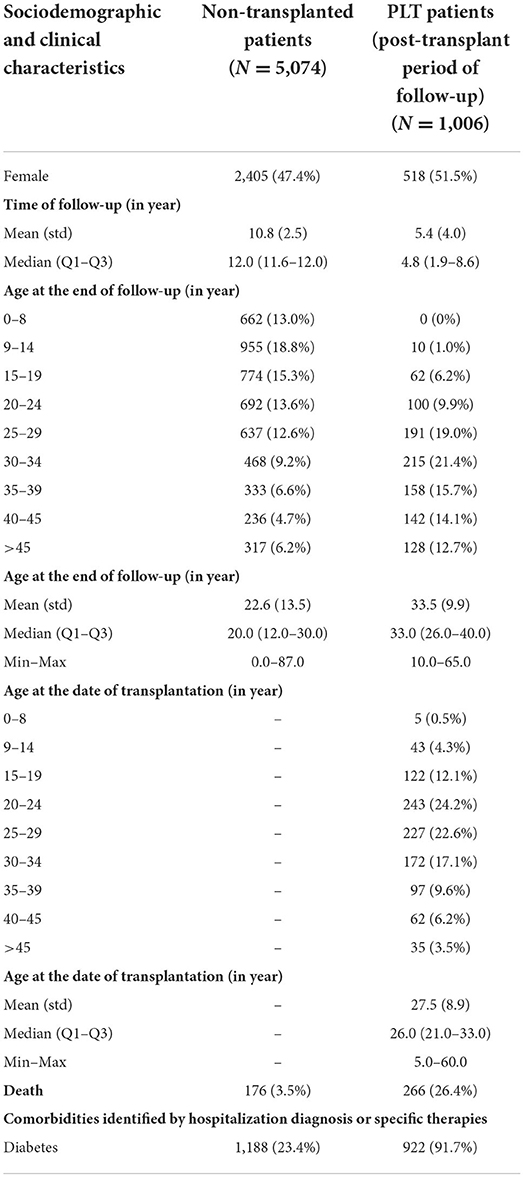
Table 1. Sociodemographic and clinical characteristics of non-transplanted and PLT pwCF.
Cancers in non-transplanted pwCF
During follow-up, 1.8% of non-transplanted pwCF had 1 to 3 cancers, with a mean age at first cancer of 35.2 (±19.5). However, the annual prevalence of cancers in this population increased with time, from 0.3% in 2006 to 1.0% in 2017 (Table 2).
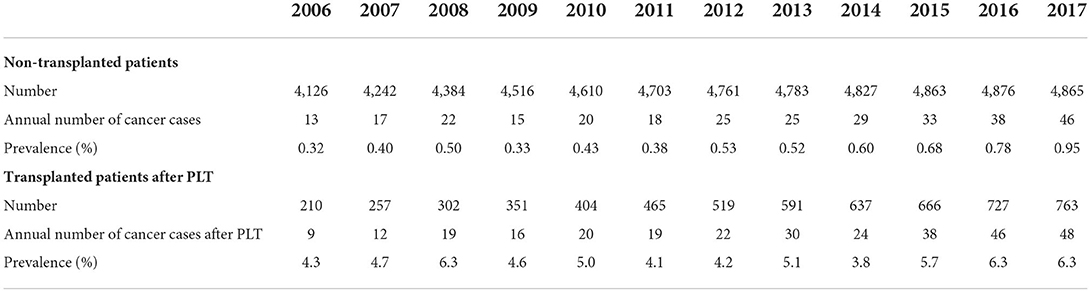
Table 2. Annual prevalence of cancer in non-transplanted and PLT patients.
Among non-transplanted patients, 86 had a first cancer during their follow-up. Figure 1 depicts the annual incidence rates of cancer between 2006 and 2017 in non-transplanted patients. Incidence rates were stable over time, from 0.5 to 2.3 per 1,000 patient-years. Table 3 presents the number of observed and expected cancers with corresponding SIR and 95%CI values among non-transplanted patients for the period from 2006 to 2017. For the 54,425 person-years of observation during the period from 2006 to 2017, 86 invasive cancers were reported in non-transplanted CF patients compared to 33.5 expected cancers in the general population (SIR = 2.57, 95%CI 2.05 to 3.17) (Table 3). There was a significantly higher number of colorectal cancer (SIR = 4.41, 95%CI 1.62 to 9.59) and of lung cancer (SIR = 4.96, 95%CI 2.57 to 8.67) in non-transplanted CF patients than in the general population.
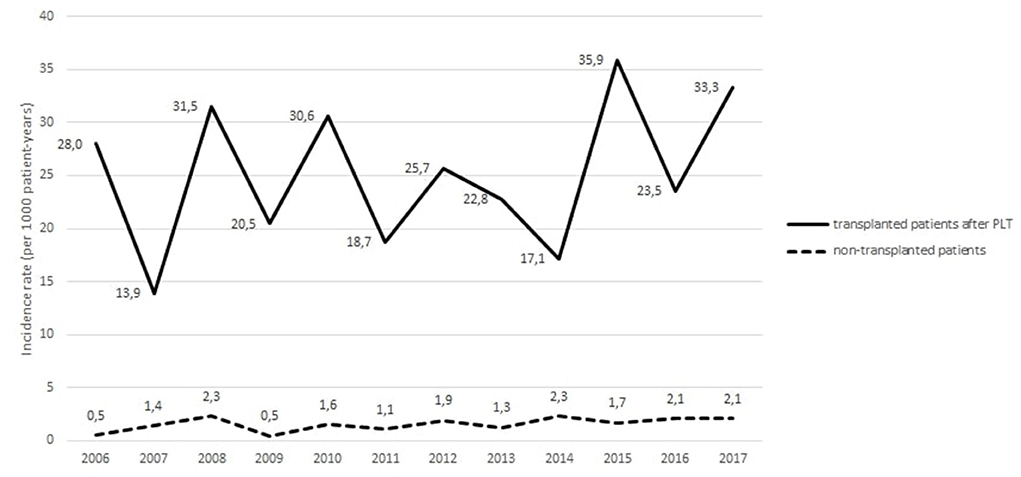
Figure 1. Temporal trends in the annual incidence rates of cancers (all sites included) occurring in non-transplanted patients and in transplanted patients after lung transplantation.
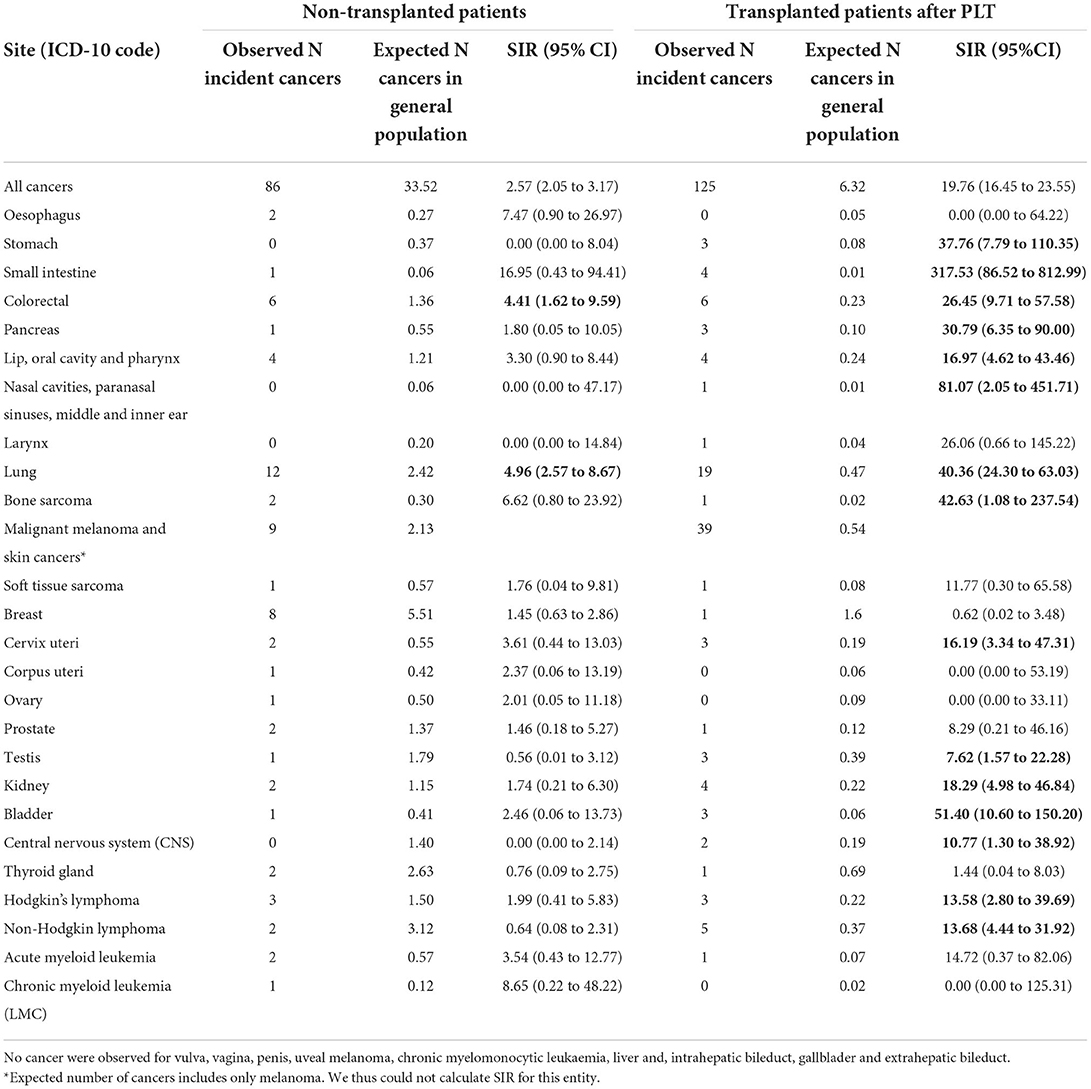
Table 3. Observed and expected numbers of cancers and SIRs among non-transplanted and PLT patients with CF in France from 2006 to 2017.
Cancers occurring after LT
Among PLT patients, 14.8% developed at least one cancer during the follow-up period (either before or after the transplantation). After transplantation, 13.7% had a diagnosis of one to five cancers, with a mean age at first cancer of 33.8 (±10.5). The annual prevalence of CF patients with any cancer occurring after PLT increased from 4.3% in 2006 to 6.3% in 2017 (Table 2).
Among PLT patients, 18 had cancer before PLT; 982 had no cancer before PLT. Among these 982 patients, 125 had a first cancer occurring after PLT. The incidence trends of cancer after PLT among transplanted patients are illustrated in Figure 1. No clear trend emerged over time, as incidence range were 28.0 per 1,000 patient-years in 2006, 18.7 per 1,000 patient-years in 2011, and 33.3 per 1,000 patient-years in 2017.
During 4,861 person-years of observation during the period from 2006 to 2017, 125 invasive cancers were reported in PLT patients after transplantation compared with 6.32 expected cancers (SIR = 19.76, 95%CI 16.45 to 23.55) (Table 3). There was a statistically higher number of stomach (SIR = 37.76, 95%CI 7.79 to 110.35), small intestine (SIR = 317.53, 95%CI 86.52 to 812.99) colorectal (SIR = 26.45, 95%CI 9.71 to 57.58) and pancreas cancers (SIR = 30.79, 95%CI 6.35 to 90.00), cancers of the lip, oral cavity and pharynx (SIR = 16.97, 95%CI 4.62 to 43.46), cervical (SIR = 16.19, 95%CI 3.34 to 47.31), testicular (SIR = 7.62, 95%CI 1.57 to 22.28), kidney (SIR = 18.29, 95%CI 4.98 to 46.84) and bladder cancers (SIR = 51.40, 95% CI 10.60 to 150.20), lung cancers (SIR = 40.36, 95%CI 24.30 to 63.03), cancers of the CNS (SIR = 40.36, 95%CI 24.30 to 63.03), Hodgkin (SIR = 13.58, 95%CI 2.80 to 39.69), and non-Hodgkin lymphomas (SIR = 13.68, 95%CI 4.44 to 31.92) after transplantation for PLT patients than in the general population.
The median time from transplantation to the first cancer was 3.9 years. The probability of having any cancer at 10 years after transplantation was estimated to be 13.7% (Figure 2).
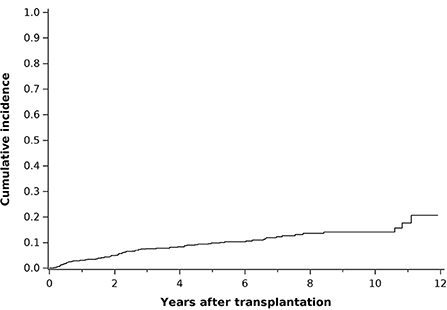
Figure 2. Cumulative incidence curve of cancers (all sites included) occurring after transplantation in PLT patients.
Discussion
The linkage between French CF Registry data and the SNDS claims data confirmed that the overall burden of cancer in CF patients is high, particularly following LT. Comparison of SIR in French pwCF with those in the general population (16) confirmed higher incidence rates in French CF patients, as previously described both in the US and the UK CF population (3, 4, 9, 10, 12).
In our study, gastro-intestinal (GI) tract cancer was one of the most documented among CF patients, as previously shown in non-transplanted and in transplanted patients (3, 4, 9, 12, 17). We were not able to calculate separately SIR for colon or rectal cancers as both are counted as colorectal cancer in the French National Cancer Registry. This observation has led to specific GI cancer screening guidelines for CF patients: systematic colonoscopy with CF-specific intensive bowel preparation should be initiated at age 40 years (18), and CRC screening for organ transplant recipients with CF should be initiated earlier, at the age of 30 years, within 2 years of transplantation (18).
Cancer risk in transplanted patients
Our study showed higher incidence rates of cancer in LT pwCF than in non-transplanted CF patients, thus confirming previous data (3, 4, 9, 10, 12, 17). Our study investigated a larger spectrum of cancer that previous studies. Indeed, in other studies, mainly GI tract cancer risk and lymphoma risk have been described among transplanted CF patients (9). In addition to the higher incidence of GI cancers in transplanted patients, we found a statistically significant higher incidence of cancers of lip, oral cavity and pharynx, cervical cancer, testicular, kidney and bladder cancers, lung cancer, CNS cancers, and Hodgkin and non-Hodgkin lymphoma.
There are several explanations for the higher incidence of cancer among transplanted patients. Transplantation itself may be responsible for this difference, being associated with an increased risk for cancers (18). Other factors, such as older age and the more severe clinical status of the transplanted group (high number of comorbidities), might play a role (19). Immunosuppression may also increase the risk of developing cancer in transplant patients through multiple mechanisms: the risk of oncoviral-driven malignancy due to long-term immunodeficiency, impaired immunosurveillance of neoplastic cells due to the non-specific mode of action of the majority of immunosuppressive drugs, and the pro-oncogenic properties of some immunosuppressive treatments (20, 21). The higher incidence of some cancers in PLT patients may also be due to reinforced cancer screening after PLT, such as cervical cancer screening, which is recommended annually for PLT patients and only every 3 to 5 years for non-transplanted patients (22, 23). Screening for skin cancer and for GI cancer is also recommended (18, 24).
Delay after transplantation should also be highlighted. The median time from transplantation to the first cancer was 3.9 years, a shorter delay than that described recently in the UK CF population. Archangelidi et al. (12) described an average time to first report of cancer of 7.1 years after transplantation. The risk of developing cancer has been shown to increase with the number of post-transplant years due to different factors: age at transplantation and aging during follow-up and the duration of exposure to immunosuppressive therapy. A comparison of our population with other transplanted populations to identify specific cancer risk related to CF might have been interesting but would have been difficult to achieve, as lung transplantation occurs in young patients in CF compared to other transplanted populations.
Cancer risk in non-transplanted patients
We found an overall higher cancer incidence among non-transplanted pwCF compared to the non-transplanted general population, as described in the literature (3, 4, 9). Previous studies have also suggested a higher incidence of specific cancers among non-transplanted patients compared to the general population, such as lymphoma and thyroid cancers, testicular cancer and lymphoid leukemia (4). Our findings did not confirm these data, and we only found a higher incidence of GI tract cancers, and of lung cancers.
This last finding is contradictory to previous studies reporting a low incidence of cancer of the respiratory tract in CF patients (25), possibly attributable to the low prevalence of smoking reported in this population (12).
We observed a high frequency of melanoma and skin cancers among non-transplanted patients, whereas studies published in the 1990s have suggested a possible protective role for CFTR in CF patients without transplant on melanoma (26, 27). Different findings have been discussed to explain this protection regarding melanoma: a possible genetic protection of the F508 del mutation during melanoma genesis and a reduced time to risk exposure for melanoma in children with CF due to the reduced time spent outdoors (3). However, our data could not be compared to the general population as non-melanoma skin cancers are excluded from cancer registries, and number of expected cancers calculated concerns only melanoma.
Pathogenesis of cancer in patients with CF
The pathogenesis of cancer in pwCF remains unclear, but multiple hypotheses have been proposed, especially for GI cancers. The specific role of CFTR in the physiopathology of GI tract cancer for pwCF has been evoked. The mechanisms underlying the actions of CFTR as a tumor suppressor are not clearly understood. Dysregulation of Wnt/β-catenin signaling and disruption of intestinal stem cell homeostasis and intestinal barrier integrity, as well as intestinal dysbiosis, immune cell infiltration, stress responses, and intestinal inflammation, have all been reported in human CF patients and in animal models (11). Lowered expression of CFTR is reported in sporadic CRC, and downregulation of CFTR is associated with poor survival (11). Furthermore, the enhanced risk for CRC extends to millions of people (more than 10 million in the US) who are heterozygous carriers of CFTR gene mutations (11). Chronic local inflammation and chronic increased GI epithelial cell turnover beginning in infancy and early childhood in CF, may also play a role (28, 29). Additionally, an inadequate immune response and intestinal stem cell regulation have been described in CFTR-knockout mice, which may offer some explanation (30).
Not specific to gastrointestinal cancers, hypotheses are proposed to explain the risk of cancer in general. Frequent exposure to radiation (i.e., X-rays and CT scans) might contribute to the increased risk of cancer in pwCF (31). The association between radiation exposure during childhood and cancer has been described for childhood acute lymphoblastic leukemia and solid tumors (32).
CF patients face some comorbidities that can influence cancer risk. CF-related diabetes was recently identified as an additional cancer risk factor, and a specific GI cancer screening among patients with CF-related diabetes has even been suggested (12). Unfortunately we were not able to make a specific analysis of the risk of cancer in the presence or absence of comorbidities. A link between diabetes or some other comorbidity and cancer risk could indeed explain some of our results as the over-representation of some cancers.
Strenghts and limitations
Among the strengths of our study, the population-based study design, and the linkage with the national CF registry should be highlighted. This design allowed us to have an exhaustive collection of cancer cases in this context of rare disease. Some limitations of our study must be acknowledged, the most important of which is the underrepresentation of children younger than 7 years. Indeed, as the linkage used the dates of spirometry and as spirometry is seldom performed before the age of 6, many younger patients could not be linked (15). For similar reasons, the linkage led to an underrepresentation of deceased patients, as it was based on the death status, which is adequately identified only for patients affiliated with general health insurance (15). Underrepresentation of children might lead to overestimation of the cancer incidence and prevalence. However, very few cases of cancer are expected among children. Underrepresentation of deceased patients may have led to an underestimation of the number of cancer cases; it may also have been offset by overestimation of lung transplanted patients, as date of transplant was used for the linkage. Cancer cases were those declared in the SNDS, but we did not have histological confirmation. This could have led to a non-differential classification bias. The number of cancers expected was calculated using calendar year-specific incidence rates obtained from the data published by the French National Cancer Registry in 2019 (based on data from 2018) (16). This may have underestimated the difference from the general population as incidence of cancers has mainly increased over time. However, for some types of cancer (larynx and stomach in particular), this could have increased the difference observed in relation to the general population, as their incidence has decreased over time in the general population. Cases of melanoma and of skin cancers could not be differentiated in CF patients, as the identification code in SNDS is common. It prevented us from comparison with the general population for all skin cancers, as non-melanoma skin cancers are excluded from cancer registries. The absence of comparison of our population with other transplanted populations without CF to identify specific cancer risk related to CF can also be cited as a limitation.
In the future, the use of CFTR modulators may influence cancer risk among CF patients.
Conclusion
This study highlights the high prevalence and incidence of cancer in CF patients. It also shows the necessity of specific follow-up and prevention for CF patients who have undergone transplantation and the need for resource allocation and training in future multidisciplinary adult CF teams with a comprehensive understanding of oncology.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This observational study was conducted using anonymized data after approval by the French Institute for Health Data (approval n° 217, on December 1, 2016) and the National Informatics and Liberty Committee (approval n° DE-2018-001, on March 12, 2018). Written informed consent from the participants legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
CR-J, ID, QR, MBel, and FD contributed substantially to the study design and interpretation of the results, and were responsible for producing the initial draft of the paper. MBer and FJ carried out the statistical analysis and including figures and tables. EV, MV, LL, and CD contributed to the data interpretation and provided written comments, and feedback during manuscript development. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the Vaincre La Mucoviscidose association that participated in providing data from their registry in the interpretation of data and in the writing of the report, and by the Comité de la Loire de la Ligue Contre le Cancer (Appel d'offres régional Auvergne-Rhône-Alpes et Saône-et-Loire de la Ligue Contre le Cancer 2018).
Acknowledgments
We thank the French NHS (Caisse Nationale de l'Assurance Maladie) for providing access to their claims data, as well as Vaincre La Mucoviscidose for providing data from their Registry. Results related to this study have been presented at the 44th European Cystic Fibrosis Conference 2021 online in June 2021.
Conflict of interest
Authors FJ, FD, MBer, and MBel are full-time employees of PELyon. EV is the scientific advisor and shareholder of PELyon.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1043691/full#supplementary-material
Abbreviations
CF, cystic fibrosis; CFTR, cystic fibrosis transmembrane regulator; CI, confidence interval; CRC, colorectal cancer; ICD, international classification of diseases; LT, lung transplant; PLT, primary lung transplant; pwCF, people with cystic fibrosis; SIR, standardized incidence ratio; SNDS, système national des données de santé; (French national health data system).,
References
1. Elborn JS, Bell SC, Madge SL, Burgel P-R, Castellani C, Conway S, et al. Report of the European Respiratory Society/European Cystic Fibrosis Society task force on the care of adults with cystic fibrosis. Eur Respir J. (2016) 47:420–8. doi: 10.1183/13993003.00592-2015
2. Vaincre la Mucoviscidose. French Cystic Fibrosis Registry - Annual Data Report 2020. Registre Français de la Mucoviscidose – Bilan des Données 2020. (2022). Available online at: www.registredelamuco.org
3. Maisonneuve P, Marshall BC, Knapp EA, Lowenfels AB. Cancer risk in cystic fibrosis: a 20-year nationwide study from the United States. J Natl Cancer Inst. (2013) 105:122–9. doi: 10.1093/jnci/djs481
4. Neglia JP, FitzSimmons SC, Maisonneuve P, Schöni MH, Schöni-Affolter F, Corey M, et al. The risk of cancer among patients with cystic fibrosis. N Engl J Med. (1995) 332:494–9. doi: 10.1056/NEJM199502233320803
5. Garg M, Ooi CY. The enigmatic gut in cystic fibrosis: linking inflammation, dysbiosis, and the increased risk of malignancy. Curr Gastroenterol Rep. (2017) 19:6. doi: 10.1007/s11894-017-0546-0
6. Assis DN, Freedman SD. Gastrointestinal disorders in cystic fibrosis. Clin Chest Med. (2016) 37:109–18. doi: 10.1016/j.ccm.2015.11.004
7. European Cystic Fibrosis Society Patient Registry. 2018 Annual Report From the European Cystic Fibrosis Society Patient Registry (2020).
8. Cystic Fibrosis Foundation. Cystic Fibrosis Foundation Patient Registry: 2019 Annual Data Report. Bethesda, MD (2020).
9. Maisonneuve P, FitzSimmons SC, Neglia JP, Campbell PW, Lowenfels AB. Cancer risk in nontransplanted and transplanted cystic fibrosis patients: a 10-year study. J Natl Cancer Inst. (2003) 95:381–7. doi: 10.1093/jnci/95.5.381
10. Fink AK, Yanik EL, Marshall BC, Wilschanski M, Lynch CF, Austin AA, et al. Cancer risk among lung transplant recipients with cystic fibrosis. J Cystic Fibrosis. (2017) 16:91–7. doi: 10.1016/j.jcf.2016.07.011
11. Scott P, Anderson K, Singhania M, Cormier R. Cystic fibrosis, CFTR, and colorectal cancer. IJMS. (2020) 21:2891. doi: 10.3390/ijms21082891
12. Archangelidi O, Cullinan P, Simmonds NJ, Mentzakis E, Peckham D, Bilton D, et al. Incidence and risk factors of cancer in individuals with cystic fibrosis in the UK; a case-control study. J Cystic Fibrosis. (2021) 21:302–8. doi: 10.1016/j.jcf.2021.07.004
13. Johannesson M, Askling J, Montgomery SM, Ekbom A, Bahmanyar S. Cancer risk among patients with cystic fibrosis and their first-degree relatives. Int J Cancer. (2009) 125:2953–6. doi: 10.1002/ijc.24679
14. Tuppin P, Rudant J, Constantinou P, Gastaldi-Ménager C, Rachas A, de Roquefeuil L, et al. Value of a national administrative database to guide public decisions: From the système national d'information interrégimes de l'Assurance Maladie (SNIIRAM) to the système national des données de santé (SNDS) in France. Rev Epidemiol Sante Publique. (2017) 65(Suppl. 4):S149–67. doi: 10.1016/j.respe.2017.05.004
15. Durieu I, Dalon F, Reynaud Q, Lemonnier L, Dehillotte C, Bérard M, et al. Temporal trends in healthcare resource use and associated costs of patients with cystic fibrosis. J Cyst Fibros. (2022) 21:88–95. doi: 10.1016/j.jcf.2021.03.025
16. Defossez G, Le Guyader-Peyrou S, Uhry Z, Grosclaude P, Colonna M, Dantony E, et al. Estimations Nationales de l'incidence et de la Mortalité par Cancer en France Métropolitaine Entre 1990 et 2018. Saint-Maurice : Santé Publique France (2019). p. 372. Available online at: http://www.santepubliquefrance.fr/; https://www.e-cancer.fr/
17. Yamada A, Komaki Y, Komaki F, Micic D, Zullow S, Sakuraba A. Risk of gastrointestinal cancers in patients with cystic fibrosis: a systematic review and meta-analysis. Lancet Oncol. (2018) 19:758–67. doi: 10.1016/S1470-2045(18)30188-8
18. Hadjiliadis D, Khoruts A, Zauber AG, Hempstead SE, Maisonneuve P, Lowenfels AB, et al. Cystic fibrosis colorectal cancer screening consensus recommendations. Gastroenterology. (2018) 154:736–45.e14. doi: 10.1053/j.gastro.2017.12.012
19. Jardel S, Reynaud Q, Durieu I. Long-term extrapulmonary comorbidities after lung transplantation in cystic fibrosis: update of specificities. Clin Transplant. (2018) 32:e13269. doi: 10.1111/ctr.13269
20. Sherston SN, Carroll RP, Harden PN, Wood KJ. Predictors of cancer risk in the long-term solid-organ transplant recipient. Transplantation. (2014) 97:605–11. doi: 10.1097/01.TP.0000436907.56425.5c
21. Mainbourg S, Durieu I, Dehillotte C, Reynaud Q. Extra-respiratory comorbidities and transplantation in the French cystic fibrosis registry. Expert Rev Respir Med. (2019) 13:799–802. doi: 10.1080/17476348.2019.1638768
22. Haute Autorité de Santé (HAS). Référentiel de Pratiques Pour la Prévention et le Dépistage du Cancer du col de L'utérus (2013).
23. Haute Autorité de Santé (HAS). Evaluation de la Recherche des Papillomavirus Humains (HPV) en Dépistage Primaire des Lésions Précancéreuses et Cancéreuses du col de L'utérus et de la Place du Double Immuno-Marquage p16/Ki67 (2019).
24. Acuna SA, Huang JW, Scott AL, Micic S, Daly C, Brezden-Masley C, et al. Cancer screening recommendations for solid organ transplant recipients: a systematic review of clinical practice guidelines. Am J Transplant. (2017) 17:103–14. doi: 10.1111/ajt.13978
25. Patel V, Majumdar T, Samreen I, Grewal H, Kaleekal T. Primary lung carcinoma in cystic fibrosis: a case report and literature review. Respir Med Case Rep. (2020) 31:101242. doi: 10.1016/j.rmcr.2020.101242
26. Warren N, Holmes JA, al-Jader L, West RR, Lewis DC, Padua RA. Frequency of carriers of cystic fibrosis gene among patients with myeloid malignancy and melanoma. BMJ. (1991) 302:760–61. doi: 10.1136/bmj.302.6779.760
27. Padua RA, Warren N, Grimshaw D, Smith M, Lewis C, Whittaker J, et al. The cystic fibrosis delta F508 gene mutation and cancer. Hum Mutat. (1997) 10:45–8.
28. Pang T, Leach ST, Katz T, Jaffe A, Day AS, Ooi CY. Elevated fecal M2-pyruvate kinase in children with cystic fibrosis: a clue to the increased risk of intestinal malignancy in adulthood? J Gastroenterol Hepatol. (2015) 30:866–71. doi: 10.1111/jgh.12842
29. Arthur JC, Perez-Chanona E, Mühlbauer M, Tomkovich S, Uronis JM, Fan T-J, et al. Intestinal inflammation targets cancer-inducing activity of the microbiota. Science. (2012) 338:120–3. doi: 10.1126/science.1224820
30. Than BLN, Linnekamp JF, Starr TK, Largaespada DA, Rod A, Zhang Y, et al. CFTR is a tumor suppressor gene in murine and human intestinal cancer. Oncogene. (2017) 36:3504. doi: 10.1038/onc.2017.3
31. O'Reilly R, Ryan S, Donoghue V, Saidlear C, Twomey E, Slattery DM. Cumulative radiation exposure in children with cystic fibrosis. Ir Med J. (2010) 103:43–6.
Keywords: cystic fibrosis, transplantation, cancer incidence, claims data, national registry
Citation: Rousset-Jablonski C, Dalon F, Reynaud Q, Lemonnier L, Dehillotte C, Jacoud F, Berard M, Viprey M, Van Ganse E, Durieu I and Belhassen M (2022) Cancer incidence and prevalence in cystic fibrosis patients with and without a lung transplant in France. Front. Public Health 10:1043691. doi: 10.3389/fpubh.2022.1043691
Received: 13 September 2022; Accepted: 28 October 2022;
Published: 22 November 2022.
Edited by:
Mohamed Farouk Allam, Ain Shams University, EgyptReviewed by:
Yuan Feng Zhang, China Traditional Chinese Medicine Science and Technology Development Center, ChinaLeonor Varela Lema, University of Santiago de Compostela, Spain
Copyright © 2022 Rousset-Jablonski, Dalon, Reynaud, Lemonnier, Dehillotte, Jacoud, Berard, Viprey, Van Ganse, Durieu and Belhassen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Rousset-Jablonski, Y2hyaXN0aW5lLnJvdXNzZXQtamFibG9uc2tpQGNodS1seW9uLmZy