 José L. Martín-Conty1,2†
José L. Martín-Conty1,2† Begoña Polonio-López1,2†
Begoña Polonio-López1,2† Ancor Sanz-García1,3*
Ancor Sanz-García1,3* Carlos del Pozo Vegas3,4,5
Carlos del Pozo Vegas3,4,5 Laura Mordillo-Mateos1Juan José Bernal-Jiménez1Rosa Conty-Serrano6Miguel A. Castro Villamor3,4
Laura Mordillo-Mateos1Juan José Bernal-Jiménez1Rosa Conty-Serrano6Miguel A. Castro Villamor3,4 Raúl López-Izquierdo3,4,7‡
Raúl López-Izquierdo3,4,7‡ Francisco Martín-Rodríguez3,4,8‡
Francisco Martín-Rodríguez3,4,8‡- 1Faculty of Health Sciences, Universidad de Castilla-la Mancha, Talavera de la Reina, Spain
- 2Technological Innovation Applied to Health Research Group (ITAS), Faculty of Health Sciences, University of Castilla-La Mancha, Talavera de la Reina, Spain
- 3Prehospital Early Warning Scoring-System Investigation Group, Valladolid, Spain
- 4Faculty of Medicine, Universidad de Valladolid, Valladolid, Spain
- 5Emergency Department, Hospital Clínico Universitario, Valladolid, Spain
- 6Faculty of Nursing, University of Castilla-La Mancha, Toledo, Spain
- 7Emergency Department, Hospital Universitario Rio Hortega, Valladolid, Spain
- 8Advanced Life Support, Emergency Medical Services (SACYL), Valladolid, Spain
Introduction: COVID-19 has initially been studied in terms of an acute-phase disease, although recently more attention has been given to the long-term consequences. In this study, we examined COVID-19 as an independent risk factor for long-term mortality in patients with acute illness treated by EMS (emergency medical services) who have previously had the disease against those who have not had the disease.
Methods: A prospective, multicenter, ambulance-based, ongoing study was performed with adult patients with acute disease managed by EMS and transferred with high priority to the emergency department (ED) as study subjects. The study involved six advanced life support units, 38 basic life support units, and five emergency departments from Spain. Sociodemographic inputs, baseline vital signs, pre-hospital blood tests, and comorbidities, including COVID-19, were collected. The main outcome was long-term mortality, which was classified into 1-year all-cause mortality and 1-year in- and out-of-hospital mortality. To compare both the patients with COVID-19 vs. patients without COVID-19 and to compare survival vs non-survival, two main statistical analyses were performed, namely, a longitudinal analysis (Cox regression) and a logistic regression analysis.
Results: Between 12 March 2020 and 30 September 2021, a total of 3,107 patients were included in the study, with 2,594 patients without COVID-19 and 513 patients previously suffering from COVID-19. The mortality rate was higher in patients with COVID-19 than in patients without COVID-19 (31.8 vs. 17.9%). A logistic regression showed that patients previously diagnosed with COVID-19 presented higher rates of nursing home residency, a higher number of breaths per minute, and suffering from connective disease, dementia, and congestive heart failure. The longitudinal analysis showed that COVID-19 was a risk factor for mortality [hazard ratio 1.33 (1.10–1.61); p < 0.001].
Conclusion: The COVID-19 group presented an almost double mortality rate compared with the non-COVID-19 group. The final model adjusted for confusion factors suggested that COVID-19 was a risk factor for long-term mortality.
Introduction
The current coronavirus disease 2019 (COVID-19) pandemic has been described as a novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a disease condition at the beginning characterized by a massive number of cases, leading to unplanned intensive care unit (ICU) admissions, pneumonia with the multiorgan disease, and related mortality (particularly before mass vaccination programs) (1).
At the peak of the pandemic, a drop in notifications to emergency call centers for life-threatening diseases was observed, with a significant decrease in incidents attended by the emergency medical services (EMS) and the emergency department (ED) (2). A marked decrease in cases of acute myocardial infarction, stroke, or traffic accidents has also been reported (3–5), prioritizing COVID-19 (2). EMS were called upon to respond to biohazard medical emergencies, monopolizing patients with COVID-19 and virtually all ambulance transfers. Pre-hospital care was initially provided under unfavorable circumstances, e.g., the use of personal protective equipment, excessive evacuation delays, and, above all, a general unawareness concerning the transmission of the virus (6, 7).
With rapid tests, vaccinations, and effective therapies, the current pandemic has been kept under control, and health systems have managed to deal with COVID-19. We hypothesize that COVID-19 has likely been one of the factors, but not the unique one, of the exacerbation of chronic pathologies and of the observed over-mortality compared to the historical time series. This excess of mortality may result from the lack of appropriate and timely attention to life-threatening diseases, excess mortality due to COVID-19, or a combination of both circumstances (8).
Over the course of the outbreak, health systems have changed from assisting patients with COVID-19 and focusing all efforts on controlling the virus to assisting patients with diseases associated with COVID-19. In other words, COVID-19 has changed from being the primary disease to being treated for a patient in need of urgent care to being part of the full set of pathologies that may negatively affect the prognosis of the patient as a whole (9).
The objective of the present study was to compare long-term mortality (1-year mortality by all-cause and in- and out-of-hospital) in cases managed by EMS and subsequently transferred with high priority to ED in the following two contrasting prospective cohorts: cases with the acute disease without past COVID-19 vs. cases with the acute disease after COVID-19.
Methods
Study design and settings
The present prospective, multicenter, ambulance-based, ongoing study included adult patients with acute disease managed by EMS and transferred with high priority to the ED, collected from two back-to-back prospective studies carried out under the same operative guideline from 12 March 2020 to 30 September 2021.
The study was carried out in four Spanish provinces, i.e., Burgos, Salamanca, Segovia, and Valladolid, covering 24/7 urban, suburban, and rural areas with a reference population of 1,166,746 inhabitants, involving the coordination center 1-1-2, six advanced life support units (ALSU), 38 basic life support units (BLSU), and five EDs, resources managed by the regional public health system (SACYL).
The study protocol was registered in the WHO International Clinical Trials Registry Platform (ISRCTN48326533 and ISRCTN49321933), was approved by the institutional review board of public health (reference: PI-049-19/PI-GR-19-1258), and followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) (Supplementary material) (10). Written informed consent was obtained from all the study participants at the EMS attendance. Patients without informed consent were excluded.
Population
In this study, two prospective cohorts were established. Cohort #01 included acute disease cases with no prior history of COVID-19. Cohort #2 was composed of acute disease cases who had been previously infected by COVID-19.
Adult patients (≥18 years) with acute disease, assisted consecutively by an ALSU and evacuated to ED by ALSU or BLSU, with a 1-year follow-up period were included. Those patients who present the following exclusion criteria were not considered in the study: patients with active COVID-19 cases (this exclusion criterion was selected to avoid the effect of acute infection and to focus on the long-term effects of the previous infection), patients aged <18 years, patients who had cardiorespiratory arrest (on the scene or en route), patients who were terminally ill (documented condition), pregnant women, cases discharged in situ, and patients with <1-year follow-up. The sample size was based on an opportunity sample method, i.e., selecting all the patients who met the criteria during the study time.
Outcome
The main outcome was long-term mortality, which was classified into 1-year all-cause mortality and 1-year in- and out-of-hospital mortality after the ambulance transfer. The 1-year follow-up period was in line with comparable studies (11, 12). The principal outcome was blinded to the clinical researchers responsible for collecting the data. As the electronic health record is linked to the community mortality registry, all deaths, even those that occurred out-of-hospital, were included in the study. The outcome was retrieved at the end of the study follow-up.
Measures
Sociodemographic inputs (sex, age, urban/rural area, nursing home residence, and evacuation way to the hospital) were collected by an ALSU emergency medical technician. Baseline vital signs (respiratory rate—number of breaths per minute, oxygen saturation, pulse oximetry saturation/fraction of inspired oxygen ratio, blood pressure, heart rate, temperature, and Glasgow Coma Scale) and pre-hospital blood tests (glucose, lactate, and creatinine) were picked up and recorded by the ALSU emergency registered nurse during the first contact with the patient, either at the scene or en route. Oxygen saturation, blood pressure (systolic, diastolic, and mean), and heart rate was obtained using LifePAK® 15 monitor-defibrillator (Physio-Control, Inc., Redmond, USA), and temperature using ThermoScan® PRO 6000 thermometer (Welch Allyn, Inc., Skaneateles Falls, USA). The analytical blood test was carried out using point-of-care testing epoc® Blood Analysis System (Siemens Healthcare GmbH, Erlangen, Germany). Finally, the ALSU physician compiled the pre-hospital advanced life support special follow-up procedures, namely, non-invasive respiratory support, invasive respiratory support, and/or use of vasoactive medications (norepinephrine), as well as the pre-hospital presumptive diagnosis, updated based on the 11th revision of the International Classification of Diseases.
To correctly match EMS and the electronic medical record of a hospital patient, we required the exact linkage of at least 5 identifiers, including date, admission time in ED, age, sex, ambulance code, name and surname, and/or healthcare card number. Upon data de-screening, an exact linkage failed with at least five identifiers out of 39 cases, which were excluded from the final analysis.
To assess in-hospital variables, an associate investigator assigned to each hospital (with pre-hospital care records blinded) captured the following at the end of follow-up: SARS-CoV-2 positives (polymerase chain reaction and/or rapid antigen test), 17 categories of comorbidities required to calculate the age-adjusted Charlson comorbidity index (aCCI) (myocardial infarction, congestive heart failure, peripheral vascular disease, stroke or transient ischemic attack, dementia, chronic obstructive pulmonary disease, connective tissue disease, peptic ulcer disease, mild liver disease, uncomplicated diabetes mellitus, hemiplegia, moderate to severe chronic kidney disease, diabetes mellitus with end-organ damage, localized solid tumor, leukemia, lymphoma, moderate to severe liver disease, metastatic solid tumor, and AIDS), hospitalization, ICU admission, and 1-year mortality (all-cause and in- and out-of-hospital). Finally, a data manager calculated the modified sequential organ failure assessment (mSOFA) (13) and aCCI scores (14).
Statistical analysis
Percentages were used to represent categorical variables, and the mean and standard deviation was used as continuous variables. All the comparisons followed the same procedure: first, a univariate comparison, followed by a multivariate regression using those variables with a p-value of <0.001. In particular, two main factors were used to compare groups: patients who had COVID-19 or patients without COVID-19 and mortality. This comparison was performed by considering the whole cohort, selecting only those patients who died or selecting those patients who previously suffered from COVID-19.
A comparison between patients with COVID-19 and patients without COVID-19 for the whole cohort and for those who died within the follow-up time was performed using the Mann-Whitney U test, T-test, or chi-squared test, when appropriate, followed by logistic regression with a forward and backward stepwise variable selection. The comparison for mortality was performed by the log rank followed by Cox regression. Furthermore, the survival according to patients with COVID-19 or patients without COVID-19 was obtained using the Kaplan-Meier method (KM).
Data were analyzed using our own codes and basic functions in R, version 4.2.1 (http://www.R-project.org; the R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 3,107 patients with acute disease managed by pre-hospital care and referred to the ED were included in the final evaluation: 2,594 in cohort #01 (non-COVID-19) and 513 in cohort #02 (COVID-19). We excluded 308 confirmed active COVID-19 cases in ED (Figure 1).
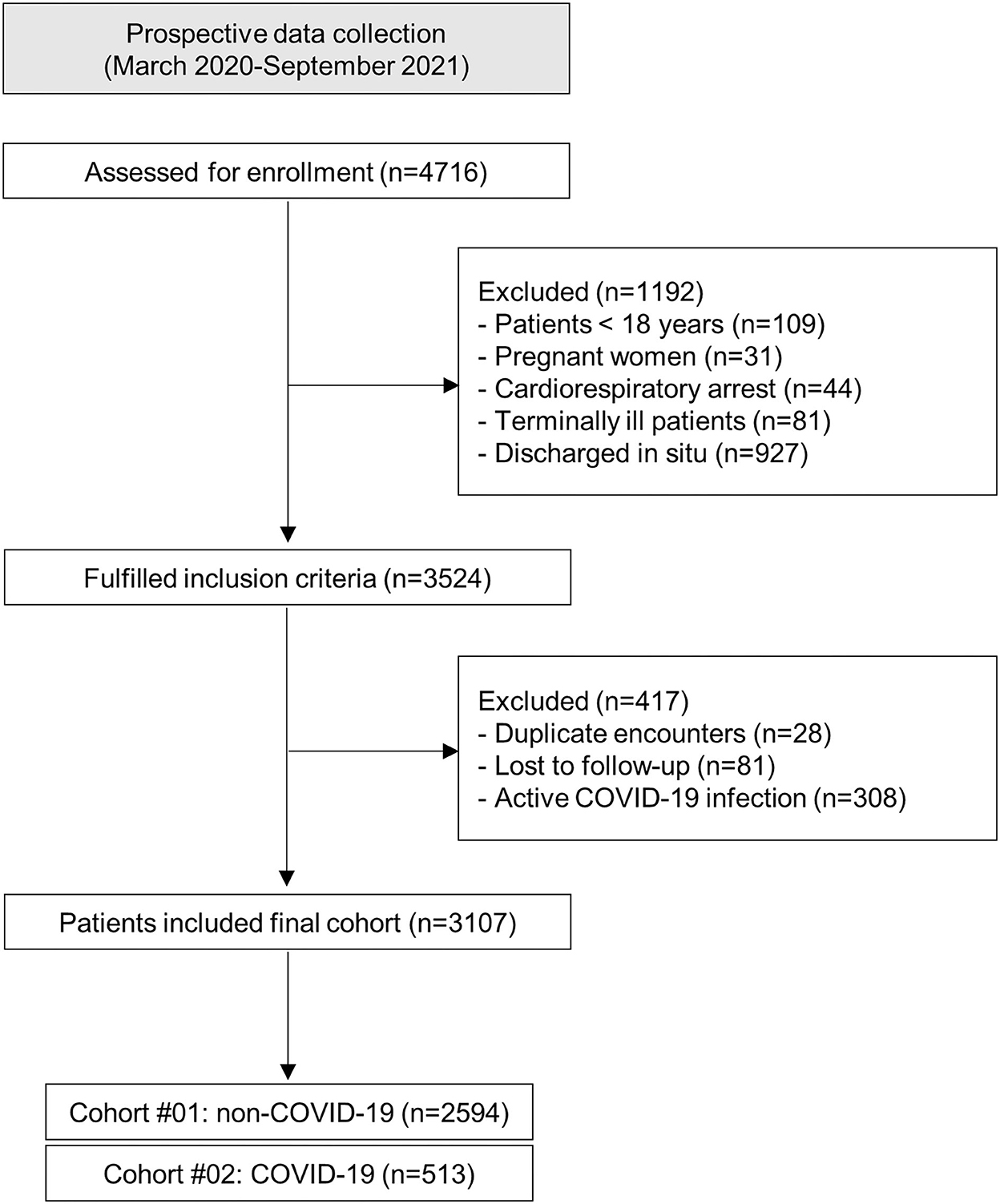
Figure 1. Study flowchart. COVID-19, coronavirus disease 2019.
The median age was 67 years (IQR (interquartile range): 50–81 years), with 41.8% women (1,299 cases). Demographic characterization by COVID-19 cohort included older adults evacuated by ALSU mainly from urban areas to ED and derived to a large extent from nursing homes, with a significant number of comorbidities (especially congestive heart failure, myocardial infarction, dementia, connective disease, and severe chronic kidney disease). The non-COVID-19 cohort exhibited a similar median age, with more middle-aged cases, significantly reduced comorbidities, and a lower nursing home origin. Clinically, both groups reported the same qSOFA, and a similar percentage of pre-hospital advanced life support special procedures, with comparable hospitalization and ICU admission rates (Tables 1, 2).
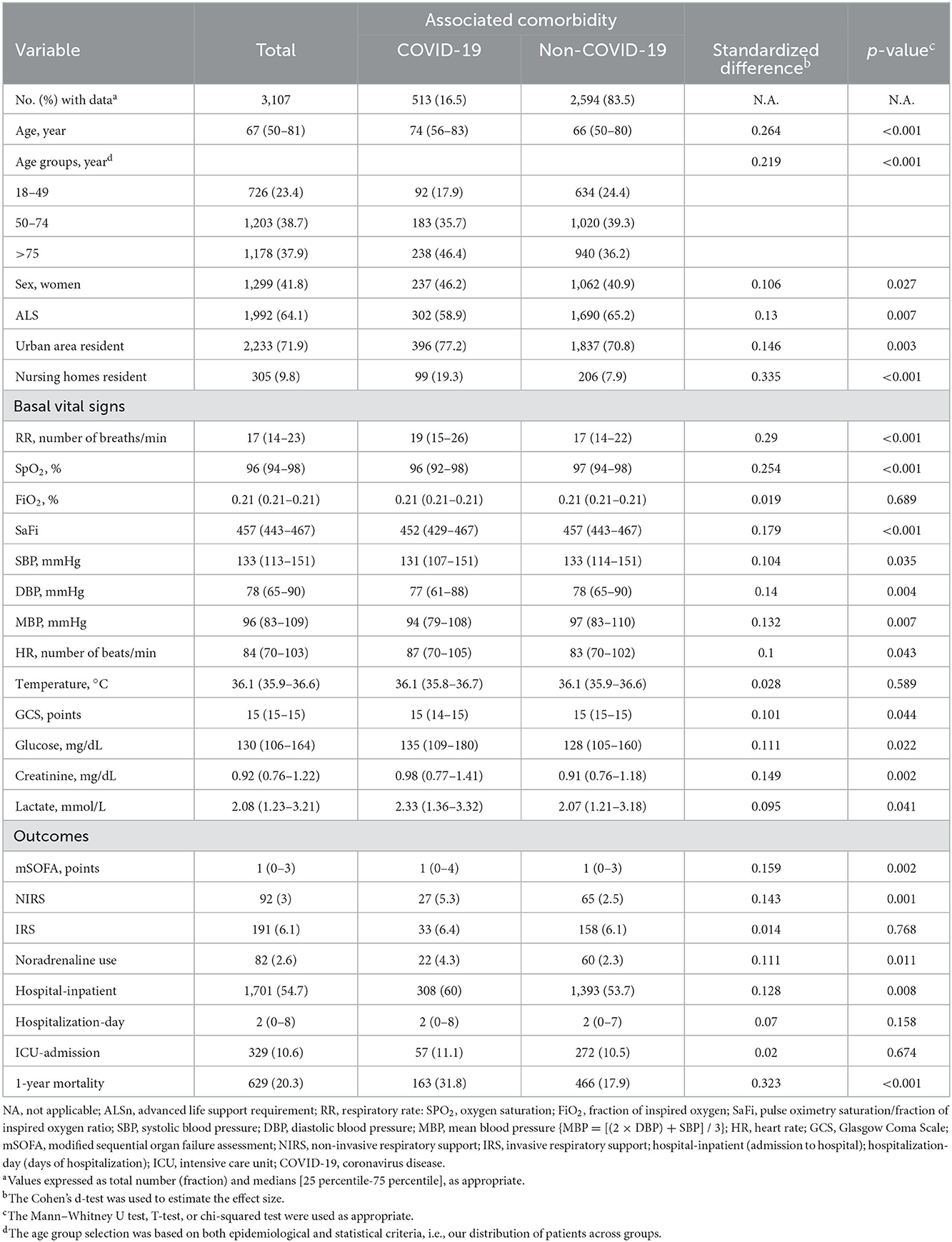
Table 1. Demographic characteristics.
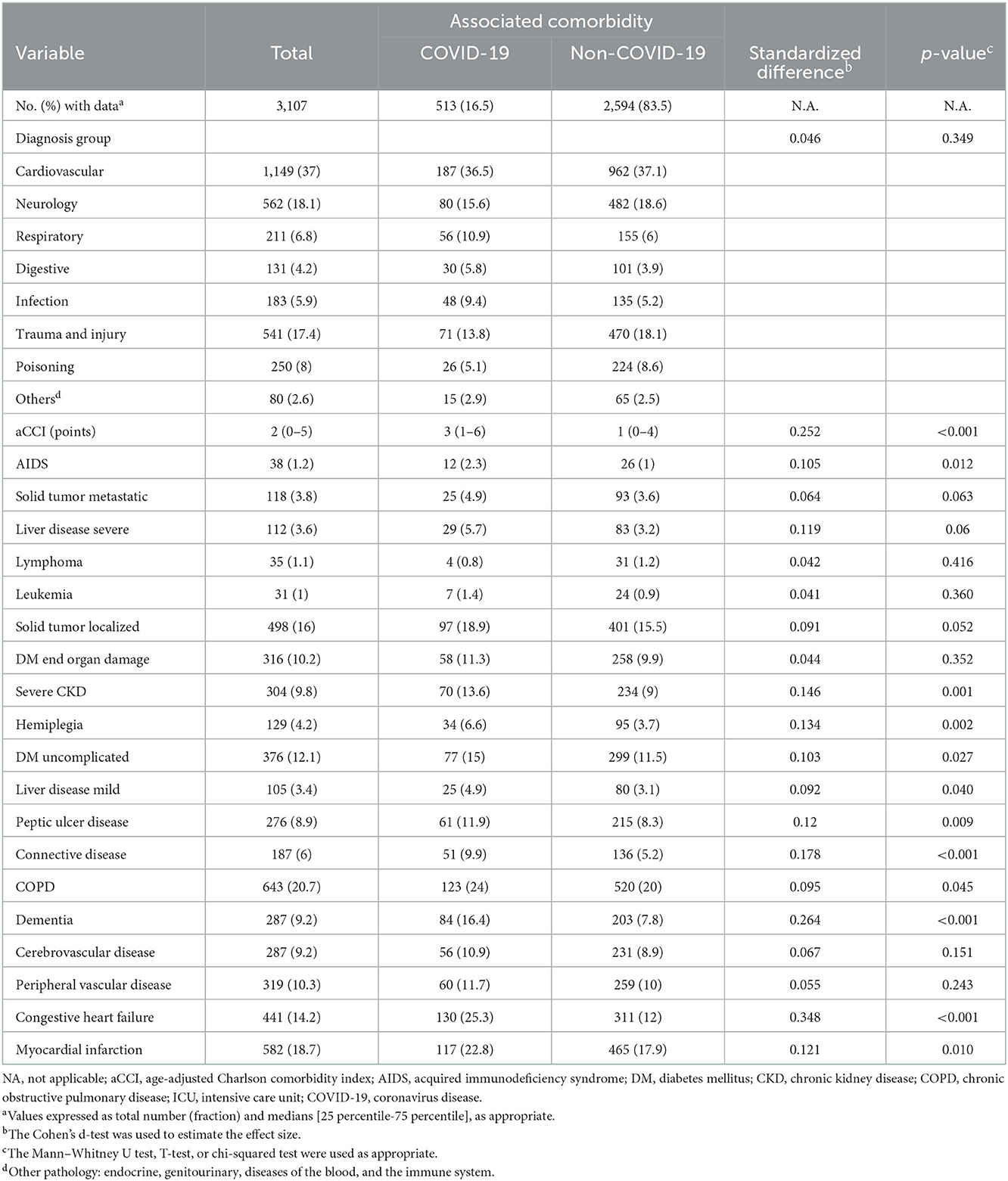
Table 2. Comorbidities of baseline patients and diagnosis group.
The overall 1-year mortality was 20.3% (629 cases). Comparing both cohorts, the mortality rate in the COVID-19 group was 13.9 points higher than the one in the non-COVID-19 group (31.8 vs. 17.9%). Cumulative mortality by time points, respectively, 1, 2, 7, 30, 90, 180, and 365 days, in the COVID-19 cohort increased consistently over all time points, exhibiting about double the cumulative mortality vs. the non-COVID-19 cohort for all the time points (Table 3). This result was corroborated by the KM curve (Figure 2); as can be observed, both groups remained parallel throughout the follow-up.
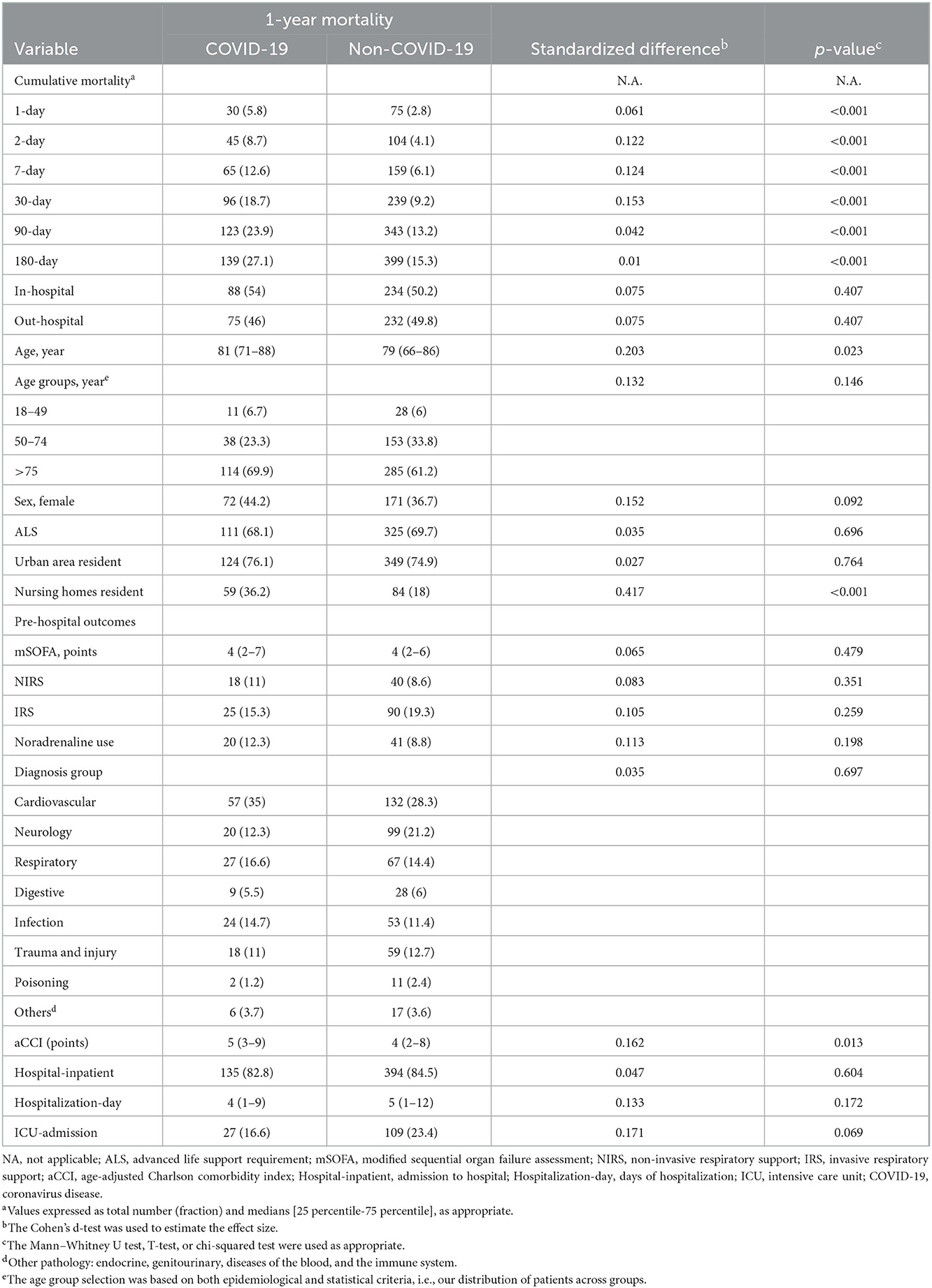
Table 3. Outcomes of long-term mortality patients.
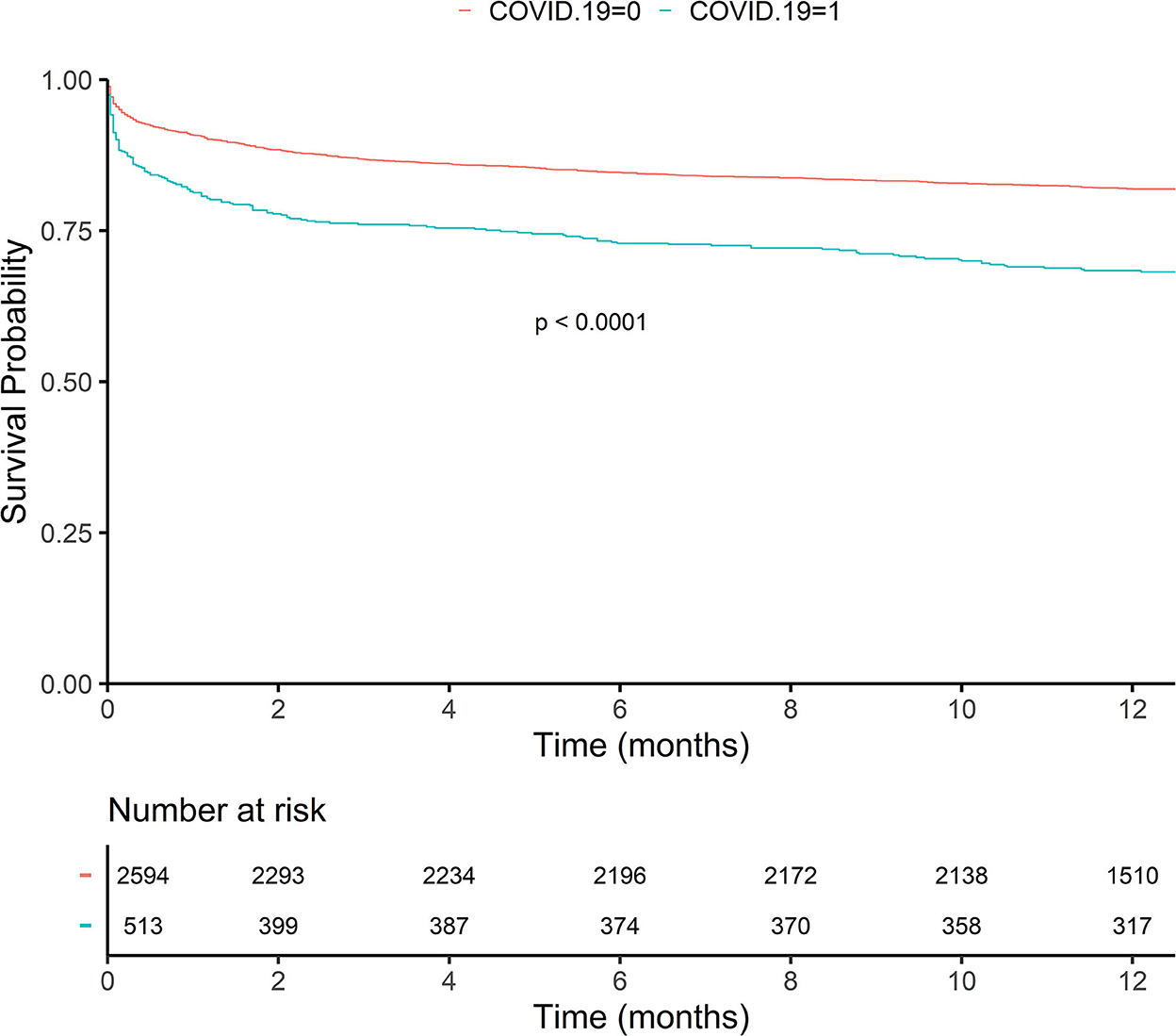
Figure 2. The Kaplan–Meier curve showing the survival probability for patients with and without COVID-19. The red line represents patients without COVID-19. The blue line represents patients with COVID-19.
When considering the whole cohort (Table 4A) or only those with 1-year mortality (Table 4B), the logistic multivariate analysis of COVID-19 vs. non-COVID-19 showed that the main characteristics of patients with COVID-19 were being in a nursing home and suffering from dementia or congestive heart failure. Additionally, when considering the whole cohort (Table 4A), patients with COVID-19 suffered from connective disease, presented a higher number of breaths per minute, and had higher 1-year mortality.
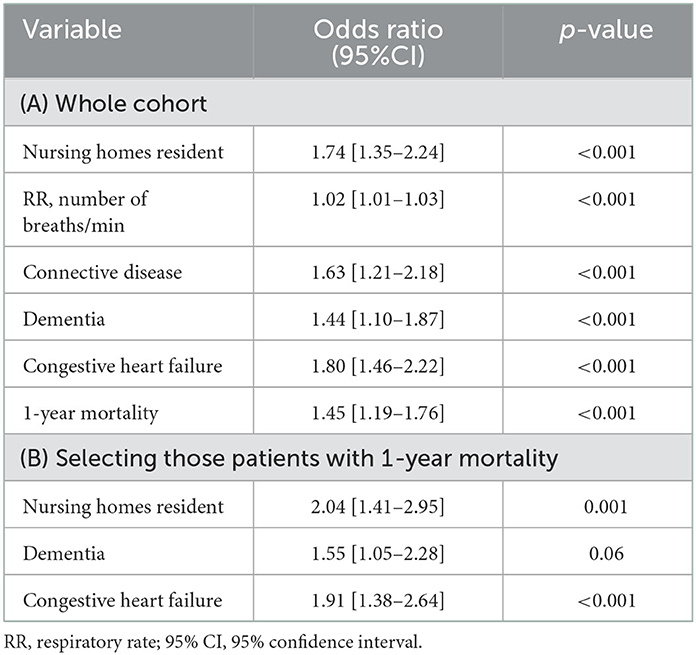
Table 4. Multivariate logistic regression for patients with COVID-19 vs. patients without COVID-19.
Similar to the comparison between patients with COVID-19 and patients without COVID-19, the longitudinal analysis of mortality for the whole cohort (Table 5) showed that factors associated with mortality included (results from Cox regression) age, respiratory support both invasive and non-invasive, noradrenaline administration, hospital admission, and hospital stay duration. The diagnosis groups that stood out as risk factors were respiratory, digestive, infection, and trauma and injury. Pathologies associated with mortality were a metastatic solid tumor, leukemia, and congestive heart failure. Those patients with COVID-19 presented a higher risk of mortality, a variable that remains statistically significant despite the high number of confounding factors. Finally, the mSOFA score was higher in those patients with a higher risk of mortality, suggesting its reliability in predicting clinical worsening even at long-term follow-ups. Further details of the results from this analysis can be found in Supplementary Table S1.
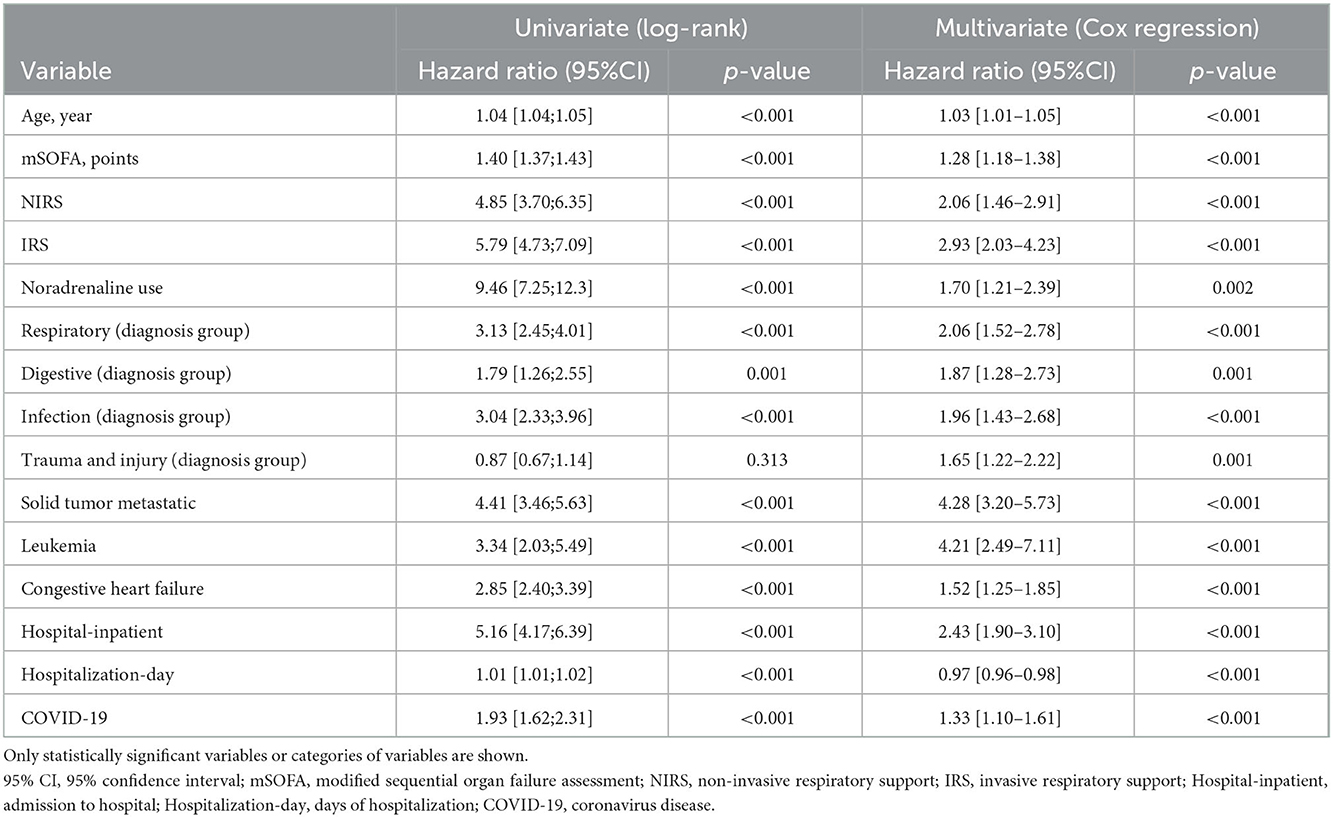
Table 5. Factors associated with mortality (univariate and multivariate by Cox regression) for the whole cohort.
To determine the factors critical for mortality for patients with COVID-19, the same procedure applied in the previous analysis was used for the cohort of patients with COVID-19 (Table 6); further details of these results can be found in Supplementary Table S2. Again, age, mSOFA, respiratory disease, metastatic solid tumor, leukemia, and congestive heart failure were risk factors for mortality. This more detailed analysis showed that hemiplegia, high aCCI, diastolic blood pressure, and FiO2 were critical factors for mortality within the COVID-19 group.
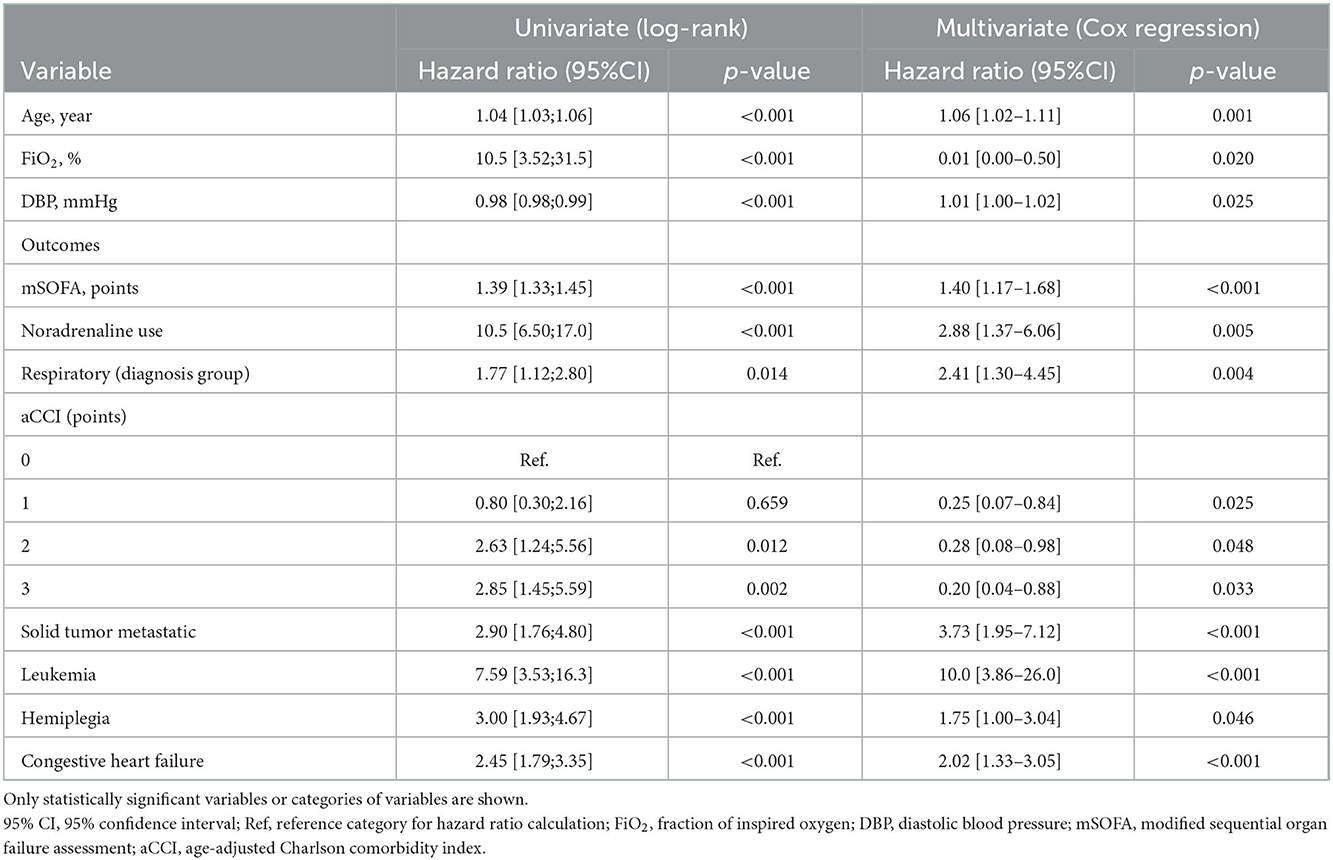
Table 6. Factors associated with mortality (univariate and multivariate by Cox regression) for those patients with COVID-19.
Discussion
The massive caseload caused by SARS-CoV-2 has consequently led to an increase in mortality rates, associated both with the pandemic and with the suboptimal support provided to non-COVID-19 disease at the start of the outbreak.
Patients treated by pre-hospital care without COVID-19 (cases with an acute disease that did not present the previous COVID-19) showed a 1-year mortality rate close to 18%. According to our results, 1-year mortality for those from the COVID-19 group (cases formerly infected by COVID-19) was 13.9 points higher. A longitudinal analysis showed that presenting COVID-19 as an antecedent is a risk factor for long-term mortality.
Chronic preexisting health conditions are well-documented to play a key role in long-term survival; the greater the number of pathologies, the lower the likelihood of survival and the higher the likelihood of in-patient hospitalization, rehospitalization, and ICU admission rates (15, 16). The number of pathologies was observed as a key factor for short-, medium-, and long-term related mortality since the beginning of the pandemic (17, 18). Different studies examined long-term mortality in post-COVID-19 patients (19–21), but to the best of our knowledge, no research has analyzed the impact of COVID-19 as a previous condition among acute disease patients managed in pre-hospital care.
This over-mortality, according to our study, appears to have a multi-causal explanation. The cases included were multi-pathological patients, such as cardiovascular and neurologic diseases or trauma and injury. Pre-hospital care was homogeneous among both cohorts in terms of assessment using the mSOFA (13) (pulse saturation/inspired oxygen fraction ratio, mean arterial pressure, Glasgow Coma Scale, creatinine, and lactate), although some advanced life support techniques were preferred in COVID-19 cohort, e.g., non-invasive mechanical ventilation and noradrenaline use (22). The rates of hospital-inpatient, hospitalization-day, and ICU admission were statistically equivalent.
The above results reinforce the argument that over-mortality could be caused by a combination of variables. Chronological age is an unquestionable biological factor. In addition, chronological age plays a pivotal role in chronic diseases, so the older the age, the increased the comorbidities (23, 24). Despite age showing significant differences between groups, we believe that comorbidity burden was the most decisive factor since age was not statistically significant in the multivariate logistic regression. The COVID-19 cohort exhibited a median aCCI of 3 points vs. 1 point in the non-COVID-19 cohort. A detailed analysis highlighted an increase observed in cardiovascular pathology (congestive heart failure and myocardial infarction) and dementia in the COVID-19 cohort, with data in line with similar studies (25–27), since those conditions are associated with common exacerbations, hospital-inpatient, and ultimately poor long-term outcomes. Other pulmonary diseases, such as chronic obstructive pulmonary disease, were not related to a significant increase in 1-year mortality with similar results in both cohorts (28).
Nursing home affiliation was a critical factor directly involved in the mortality of the COVID-19 cohort. Remarkably, at the start of the outbreak, unacceptable mortality rates associated with nursing homes were observed. Admittedly, patients are multi-pathological, with multiple comorbidities, and generally of elderly age, but the over-mortality described in nursing homes should give us a wake-up call to reconsider this fact as a healthcare system (29, 30). Nursing home mortality was two times as high as in the COVID-19 cohort compared to patients managed by EMS due to acute disease without COVID-19; this irrefutable observation flags nursing home affiliation as a critical factor underlying poor long-term outcomes (31).
The above-mentioned results suggest that COVID-19 plays an important role in this long-term mortality, and three main reasons could be argued for the importance of COVID-19 in long-term mortality: First, in the selection of patients, all the patients were selected based on an opportunity sample method, i.e., selecting all the patients who accomplished criteria during the study time. The difference between the COVID-19 and non-COVID-19 groups regarding age or comorbidities was due to chance rather than a consequence of having suffered from COVID-19. When using the above-mentioned confusion factors in the Cox regression (Table 5), none of them (and the other confusion factors) exclude COVID-19 as a risk factor for mortality. In addition, when all statistically significant factors (including age and aCCI) were adjusted in a regression model to determine the final model that described the difference between the COVID-19 and non-COVID-19 groups (Table 4), age and aCCI were automatically (by the regression algorithm) excluded from the final model, and only a few comorbidities alone were included. Epidemiological studies have shown an excess of mortality in patients with COVID-19 compared to analogous historical series (32, 33). Even though mortality also increased in patients without COVID-19 in the early stages of the pandemic, this trend has gradually normalized to previous levels as healthcare returned to pre-pandemic attention levels and due to the improvement of COVID-19 handling (34). Therefore, as the pandemic evolved, one should expect a reduction in mortality, which was not the case according to our results.
Our study is not free of limitations. First, a pure convenience sample was collected consecutively. To control for potential bias, data input was gathered 24/7 non-stop throughout the study period in ambulance stations located in urban, suburban, and rural areas, patients transferred to ED of different hospitals, and hospitals with different clinical qualifications, attempting to be a true cross-section of the analyzed population. Second, the data extractors were not blinded. To avoid cross-contamination, the EMS staff was unaware of the scores being estimated and interpreted, and as a double fail-safe, the research associates from each hospital were unaware of the pre-hospital parameters as well. Only the data manager and the principal investigator could access the master database. Third, confirmed cases of COVID-19 were taken as patients with a positive polymerase chain reaction and/or rapid antigen test, but an underestimation is possible. Currently, some people skip screening or do not report self-test results. At the onset of the outbreak, the availability of test kits was limited, even though the incidence rates should be treated with caution. In this sense, antibody tests for the non-COVID-19 group were not available, so it cannot be completely ruled out that they did not have COVID-19. Fourth, the study was carried out across different provinces, all of which comprise the same health system. To validate the findings, multicenter studies in different regions involving several institutions should be carried out. Fifth, in the present study, we did not consider all the patients who could present long-term mortality; this is because patients could reach the emergency department by their means without requiring assistance from EMS. However, this study aimed to focus on patients who required pre-hospital emergency care. Sixth, since this study has been developed in the pre-hospital scenario, critical factors related to the long-term consequences of COVID-19 have not been considered due to the impossibility to achieve them, for instance: the date of infection (hampering determining the time between infection and the EMS attendance), the severity of COVID-19, the treatment the COVID-19 (whether it required intensive therapy or invasive mechanical ventilation), and the treatment after COVID-19 hospitalization. Seventh, the duration or diagnostic time of comorbidities was not available; however, despite being important information regarding the status of the patients, it is not included in the commonly used comorbidity-based scores.
Conclusion
According to our results, the COVID-19 group presented a higher mortality rate than the non-COVID-19 group. The predictive model, when adjusted by confusion factors, showed COVID-19 as a relevant risk factor for mortality.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Research Review Board of each health area (reference: PI-049-19/PI-GR-19-1258). The patients/participants provided their written informed consent to participate in this study.
Author contributions
FM-R conceptualized the project, managed and coordinated the project, assisted with the design of methodology, analyzed data, and prepared the initial and final drafts of the manuscript. AS-G takes responsibility for the data and their analysis. LM-M, JB-J, RC-S, BP-L, CP, MC, and JM-C assisted with the management and coordination of the project, assisted with the design of methodology, and helped review the manuscript. RL-I conceptualized the project and helped review and comment on the initial and final drafts of the manuscript. All authors performed a critical review and approved the final manuscript for interpretation of the data and important intellectual input.
Funding
This study was supported by the Gerencia Regional de Salud, Public Health System of Castilla y León (Spain) [grant numbers GRS 1903/A/19 and GRS 2131/A/20]. Sponsors have no role in manuscript writing and reviewing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2022.1076627/full#supplementary-material
References
1. van Ginneken E, Webb E, Maresso A, Cylus J. Lessons learned from the COVID-19 pandemic. Health Policy. (2022) 116:348–54. doi: 10.1016/j.healthpol.2022.04.004
2. Syntia Munung N, Ujewe SJ, Afolabi MO. Priorities for global access to life-saving interventions during public health emergencies: crisis nationalism, solidarity or charity? Glob Public Health. (2022) 17:1785–94. doi: 10.1080/17441692.2021.1977973
3. Silva-Pozo A, Vallejos J, Almeida J, Martoni M, Martin RUS, Miranda M, et al. Impact of COVID-19 pandemic on stroke severity and mortality in the South-East of Santiago, Chile. J Stroke Cerebrovasc Dis. (2021) 30:105953. doi: 10.1016/j.jstrokecerebrovasdis.2021.105953
4. Yeo YH, Wang M, He X, Lv F, Zhang Y, Zu J, et al. Excess risk for acute myocardial infarction mortality during the COVID-19 pandemic. J Med Virol. (2022). doi: 10.1002/jmv.28187
5. Greco M, De Corte T, Ercole A, Antonelli M, Azoulay E, Citerio G, et al. Clinical and organizational factors associated with mortality during the peak of first COVID-19 wave: the global UNITE-COVID study. Intensive Care Med. (2022) 48:690–705. doi: 10.1007/s00134-022-06705-1
6. Satty T, Ramgopal S, Elmer J, Mosesso VN, Martin-Gill C. EMS responses and non-transports during the COVID-19 pandemic. Am J Emerg Med. (2021) 42:1–8. doi: 10.1016/j.ajem.2020.12.078
7. Eftekhar Ardebili M, Naserbakht M, Bernstein C, Alazmani-Noodeh F, Hakimi H, Ranjbar H. Healthcare providers experience of working during the COVID-19 pandemic: a qualitative study. Am J Infect Control. (2021) 49:547–54. doi: 10.1016/j.ajic.2020.10.001
8. COVID-19-Excess-Mortality-Collaborators. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020–21. Lancet. (2022) 399:1513–36. doi: 10.1016/S0140-6736(21)02796-3
9. Long B, Carius BM, Chavez S, Liang SY, Brady WJ, Koyfman A, et al. Clinical update on COVID-19 for the emergency clinician: presentation and evaluation. Am J Emerg Med. (2022) 54:46–57. doi: 10.1016/j.ajem.2022.01.028
10. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
11. Bergman J, Ballin M, Nordström A, Nordström P. Risk factors for COVID-19 diagnosis, hospitalization, and subsequent all-cause mortality in Sweden: a nationwide study. Eur J Epidemiol. (2021) 36:287–98. doi: 10.1007/s10654-021-00732-w
12. Ceccato A, Pérez-Arnal R, Motos A, Barbé F, Torres A. One-year mortality after ICU admission due to COVID-19 infection. Intensive Care Med. (2022) 48:366–8. doi: 10.1007/s00134-021-06611-y
13. Martín-Rodríguez F, Sanz-García A, Del Pozo Vegas C, Ortega GJ, Castro Villamor MA, López-Izquierdo R. Time for a pre-hospital-modified sequential organ failure assessment score: an ambulance-Based cohort study. Am J Emerg Med. (2021) 49:331–7. doi: 10.1016/j.ajem.2021.06.042
14. Shuvy M, Zwas DR, Keren A, Gotsman I. The age-adjusted Charlson comorbidity index: a significant predictor of clinical outcome in patients with heart failure. Eur J Intern Med. (2020) 73:103–4. doi: 10.1016/j.ejim.2019.12.030
15. Schluep M, Rijkenberg S, Stolker RJ, Hoeks S, Endeman H. One-year mortality of patients admitted to the intensive care unit after in-hospital cardiac arrest: a retrospective study. J Crit Care. (2018) 48:345–51. doi: 10.1016/j.jcrc.2018.09.029
16. Jiang Y, Luo Y, Lyu H, Li Y, Gao Y, Fu X, et al. Postoperative Complications of Geriatric Hip Fracture Patients from 2000 to 2019: results from a Hip Fracture Cohort in a Tertiary Hospital. Orthop Surg. (2021) 13:1890–8. doi: 10.1111/os.13142
17. Treskova-Schwarzbach M, Haas L, Reda S, Pilic A, Borodova A, Karimi K, et al. Pre-existing health conditions and severe COVID-19 outcomes: an umbrella review approach and meta-analysis of global evidence. BMC Med. (2021) 19:212. doi: 10.1186/s12916-021-02058-6
18. Ejaz H, Alsrhani A, Zafar A, Javed H, Junaid K, Abdalla AE, et al. COVID-19 and comorbidities: deleterious impact on infected patients. J Infect Public Health. (2020) 13:1833–9. doi: 10.1016/j.jiph.2020.07.014
19. Huang L, Yao Q, Gu X, Wang Q, Ren L, Wang Y, et al. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. Lancet. (2021) 398:747–58. doi: 10.1016/S0140-6736(21)01755-4
20. Zhang X, Wang F, Shen Y, Zhang X, Cen Y, Wang B, et al. Symptoms and health outcomes among survivors of COVID-19 infection 1 year after discharge from hospitals in Wuhan, China. JAMA Netw Open. (2021) 4:e2127403. doi: 10.1001/jamanetworkopen.2021.27403
21. Fang X, Ming C, Cen Y, Lin H, Zhan K, Yang S, et al. Post-sequelae one year after hospital discharge among older COVID-19 patients: a multi-center prospective cohort study. J Infect. (2022) 84:179–86. doi: 10.1016/j.jinf.2021.12.005
22. Solà-Muñoz S, Yuguero O, Azeli Y, Roig G, Prieto-Arruñada JA, Español J, et al. Impact on polytrauma patient prehospital care during the first wave of the COVID-19 pandemic: a cross-sectional study. Eur J Trauma Emerg Surg. (2021) 47:1351–8. doi: 10.1007/s00068-021-01748-3
23. Scrutinio D, Guida P, Aliani M, Castellana G, Guido P, Carone M. Age and comorbidities are crucial predictors of mortality in severe obstructive sleep apnoea syndrome. Eur J Intern Med. (2021) 90:71–6. doi: 10.1016/j.ejim.2021.04.018
24. Langsted SND, Dynesen JJ, Liesanth JY, Jessen MK, Mackenhauer J, Ahrensberg J, et al. How comorbidities impact Early Warning Score as a predictor of 7-day mortality. Eur J Emerg Med. (2020) 27:142–6. doi: 10.1097/MEJ.0000000000000633
25. Standl E, Schnell O. Heart failure outcomes and COVID-19. Diabetes Res Clin Pract. (2021) 175:108794. doi: 10.1016/j.diabres.2021.108794
26. Del Prete A, Conway F, Della Rocca DG, Biondi-Zoccai G, De Felice F, Musto C, et al. COVID-19, acute myocardial injury, and infarction. Card Electrophysiol Clin. (2022) 14:29–39. doi: 10.1016/j.ccep.2021.10.004
27. Liu L, Ni SY, Yan W, Lu QD, Zhao YM, Xu YY, et al. Mental and neurological disorders and risk of COVID-19 susceptibility, illness severity and mortality: a systematic review, meta-analysis and call for action. EClinicalMedicine. (2021) 40:101111. doi: 10.1016/j.eclinm.2021.101111
28. Halpin DMG, Criner GJ, Papi A, Singh D, Anzueto A, Martinez FJ, et al. Global initiative for the diagnosis, management, and prevention of chronic obstructive lung disease. The 2020 GOLD science committee report on COVID-19 and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. (2021) 203:24–36. doi: 10.1164/rccm.202009-3533SO
29. Ouslander JG, Grabowski DC. COVID-19 in nursing homes: calming the perfect storm. J Am Geriatr Soc. (2020) 68:2153–62. doi: 10.1111/jgs.16784
30. Martín-Rodríguez F, Sanz-García A, Melero Guijarro L, Ortega GJ, Gómez-Escolar Pérez M, Castro Villamor MA, et al. Comorbidity-adjusted NEWS predicts mortality in suspected patients with COVID-19 from nursing homes: multicentre retrospective cohort study. J Adv Nurs. (2022) 78:1618–31. doi: 10.1111/jan.15039
31. Wong R, Grullon JR, Lovier MA. COVID-19 risk factors and predictors for handwashing, masking, and social distancing among a national prospective cohort of US older adults. Public Health. (2022) 211:164–70. doi: 10.1016/j.puhe.2022.08.002
32. Friedman J, Calderón-Villarreal A, Bojorquez I, Vera Hernández C, Schriger DL, Tovar Hirashima E. Excess out-of-hospital mortality and declining oxygen saturation: the sentinel role of emergency medical services data in the COVID-19 crisis in Tijuana, Mexico. Ann Emerg Med. (2020) 76:413–26. doi: 10.1016/j.annemergmed.2020.07.035
33. Calderón-Larrañaga A, Vetrano DL, Rizzuto D, Bellander T, Fratiglioni L, Dekhtyar S. High excess mortality in areas with young and socially vulnerable populations during the COVID-19 outbreak in Stockholm Region, Sweden. BMJ Glob Health. (2020) 5:003595. doi: 10.1136/bmjgh-2020-003595
Keywords: clinical decision rules, COVID-19, emergency medical services, long-term mortality, pre-hospital care
Citation: Martín-Conty JL, Polonio-López B, Sanz-García A, del Pozo Vegas C, Mordillo-Mateos L, Bernal-Jiménez JJ, Conty-Serrano R, Castro Villamor MA, López-Izquierdo R and Martín-Rodríguez F (2023) COVID-19 as a risk factor for long-term mortality in patients managed by the emergency medical system: A prospective, multicenter, ambulance-based cohort study. Front. Public Health 10:1076627. doi: 10.3389/fpubh.2022.1076627
Received: 21 October 2022; Accepted: 15 December 2022;
Published: 10 January 2023.
Edited by:
Ramcés Falfán-Valencia, Instituto Nacional de Enfermedades Respiratorias-México (INER), MexicoReviewed by:
Brandon Bautista-Becerril, Instituto Politécnico Nacional (IPN), MexicoLuiz Gonzaga Francisco De Assis Barros D'Elia Zanella, University of São Paulo, Brazil
Touil Imen, University of Monastir, Tunisia
Camila Bruneli Do Prado, Federal University of Espirito Santo, Brazil
Copyright © 2023 Martín-Conty, Polonio-López, Sanz-García, del Pozo Vegas, Mordillo-Mateos, Bernal-Jiménez, Conty-Serrano, Castro Villamor, López-Izquierdo and Martín-Rodríguez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ancor Sanz-García,  YW5jb3Iuc2FuekBnbWFpbC5jb20=
YW5jb3Iuc2FuekBnbWFpbC5jb20=
†These authors share first authorship
‡These authors share last authorship